Downloaded from https://journals.lww.com/internat-ophthalmology by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AWnYQp/IlQrHD3toxqoobVJlY7QxzbwcW58lEx82IvsAg18ccq7+R+k2A= on 11/14/2019 Tumors of the Optic Nerve and its Sheath Lilangi S. Ediriwickrema, MD Neil R. Miller, MD ’ Introduction Tumors that affect the optic nerve (ON) may arise within the nerve itself, from its surrounding optic nerve sheath (ONS), or from a distant location and spread to the nerve. Regardless of their origin, both primary and secondary ON tumors produce a variety of clinical manifestations and imaging findings. In addition, the management of patients with these lesions differs depending on multiple factors, including the age and health of the patient, the symptoms and signs produced by the tumor, the presence or absence of progression, and the management options available. Herein, we review the settings, clinical manifestations, imaging findings, pathology, and management options for patients with the most common and some uncommon primary tumors of the ON and sheath (Table 1). Although the ON can be compressed and/or infiltrated by a number of secondary tumors such as carcinomas and lymphoreticular neoplasms, these will be discussed only very briefly in this chapter. ’ Primary ON Tumors Optic Nerve Gliomas (ONGs) Optic pathway gliomas comprise tumors that affect the precortical visual pathway. Some of these tumors affect only the ON and, thus, are referred to as ONGs. ONGs usually become symptomatic in childhood, typically in the first decade of life and account for about 65% of all intrinsic ON tumors. 1 Rush et al 2 reviewed a series of 33 patients with ONGs and found an age range of 2 to 46 years with a median age of 6.5 years, whereas 52 patients with chiasmal gliomas had an age range of 0.75 to 50 years with a median range of 11 years. Although some authors INTERNATIONAL OPHTHALMOLOGY CLINICS Volume 58, Number 2, 237–260 Copyright © 2018 Wolters Kluwer Health, Inc. All rights reserved. www.internat-ophthalmology.com | 237 Copyright r 2018 Wolters Kluwer Health, Inc. All rights reserved.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Dow
nloadedfrom
https://journals.lww.com
/internat-ophthalmology
byBhD
Mf5ePH
Kav1zEoum1tQ
fN4a+kJLhEZgbsIH
o4XMi0hC
ywCX1AW
nYQp/IlQ
rHD3toxqoobVJlY7Q
xzbwcW
58lEx82IvsAg18ccq7+R+k2A=
on11/14/2019
Downloadedfromhttps://journals.lww.com/internat-ophthalmologybyBhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AWnYQp/IlQrHD3toxqoobVJlY7QxzbwcW58lEx82IvsAg18ccq7+R+k2A=on11/14/2019
Tumors of the Optic Nerve andits Sheath
Lilangi S. Ediriwickrema, MDNeil R. Miller, MD
’ Introduction
Tumors that affect the optic nerve (ON) may arise within the nerveitself, from its surrounding optic nerve sheath (ONS), or from a distantlocation and spread to the nerve. Regardless of their origin, both primaryand secondary ON tumors produce a variety of clinical manifestationsand imaging findings. In addition, the management of patients withthese lesions differs depending on multiple factors, including the age andhealth of the patient, the symptoms and signs produced by the tumor, thepresence or absence of progression, and the management optionsavailable. Herein, we review the settings, clinical manifestations, imagingfindings, pathology, and management options for patients with the mostcommon and some uncommon primary tumors of the ON and sheath(Table 1). Although the ON can be compressed and/or infiltrated by anumber of secondary tumors such as carcinomas and lymphoreticularneoplasms, these will be discussed only very briefly in this chapter.
’ Primary ON Tumors
Optic Nerve Gliomas (ONGs)
Optic pathway gliomas comprise tumors that affect the precorticalvisual pathway. Some of these tumors affect only the ON and, thus, arereferred to as ONGs. ONGs usually become symptomatic in childhood,typically in the first decade of life and account for about 65% of allintrinsic ON tumors.1 Rush et al2 reviewed a series of 33 patients withONGs and found an age range of 2 to 46 years with a median age of6.5 years, whereas 52 patients with chiasmal gliomas had an age range of0.75 to 50 years with a median range of 11 years. Although some authors
INTERNATIONAL OPHTHALMOLOGY CLINICSVolume 58, Number 2, 237–260Copyright © 2018 Wolters Kluwer Health, Inc. All rights reserved.
www.internat-ophthalmology.com | 237
Copyright r 2018 Wolters Kluwer Health, Inc. All rights reserved.

Table 1. Neuroimaging and Histopathologic Features of Optic Nerve and Sheath TumorsOptic nerve glioma
Malignant optic glioma
Ganglioglioma Medulloepithelioma Hemangioblastoma Oligodendroglioma Optic Nerve Sheath Meningioma
Magnetic Resonance Imaging characteristics
If non NF1, most often fusiform enlargement of nerve; T1 hypo or iso-intensity, T2 hyperintensity;enhances with gadolinium contrast; if NF1, most often diffuse enlargement of nerve with kinking; both can have pseudo-CSF sign
Fusiform, homogenous enhancement;rapid growth
Can be cystic and non-enhancing with contrast
Fusiform enlargement Fusiform enlargement, increased homogenous enhancement
Generalized enlargement; enhancement
Three patterns: 1) Diffuse homogenous enhancement on T1 weighted post contrast fat suppressed images with a characteristic “tram-track” sign. (Computed tomography may show calcification); 2) hypointense nerve surrounded by hyperintense, enhancing fusiform mass with “fingers” extending; 3) apparent extra-axial mass adjacent to nerve
Histopathologic features
Pink, eosinophilic collections known as Rosenthal
Increased mitotic index, hyperchromatic nuclei, variable cellular pleomorphism, necrosis, hemorrhage
Reactivity to synaptophysin and neurofilament protein
Hyperchromatic cells, high mitotic figures, hyaluronidase-positive confirmed via Alcian blue stain, presence of differentiated cells (i.e. neuroglial, ganglion, Flexner-Wintersteinerrosettes), and rarely heteroplasmic elements (i.e. cartilage, striated muscle)
Endothelial cells and pericytes, vascular channels, and stromal lipid
Compact masses of swollen oligodendrocytes separated by scanty and delicate supporting stroma of blood vessels and collagen
Whorls of spindle cells with interspersed hyalinized calcium deposits known as psammoma bodies, and/or sheets of polygonal cells separated by vasculature
CSF indicates cerebrospinal fluid; NF1, neurofibromatosis type 1.
238
’Ediriw
ickremaandMille
r
www.internat-ophthalm
ology.com

consider these lesions “hamartomas,” they are, according to the 2016World Health Organization (WHO), most often low-grade I juvenilepilocytic astrocytomas or grade II diffuse fibrillary astrocytomas.3
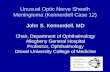
ONGs tend to be benign and slow growing. They can present in avariety of ways. The “anterior” presentation is characterized by signs ofan anterior optic neuropathy with variably decreased visual acuity,reduced color vision, a relative afferent pupillary defect, strabismus thatusually is vertical, painless proptosis, and optic disc swelling (Fig. 1). The“posterior” presentation presents in similar manner, except that the opticdisc appears normal or pale (Fig. 2). Nystagmus can occur in the affectedeye if visual loss is severe. The nystagmus typically is low-frequency andcan have a low or high amplitude. It is always vertical and monocular,thus differentiating it from the high-frequency, low-amplitude unilateral,or asymmetric spasmus nutans that be seen in some patients with gliomasthat involve the optic chiasm and surrounding structures. This nystag-mus, also known as the Hiemann-Bielschowsky phenomenon, is notlimited to patients with an ONG; it can be present in any patient withacquired monocular visual loss; however, in the appropriate setting, anONG should be suspected.4 Rarely, an ONG may produce venous stasisretinopathy, a central retinal vein occlusion (CRVO), retinal-choroidalshunt vessels, or neovascular glaucoma.5
Although most cases of ONG are sporadic, there is a clear geneticrelationship with neurofibromatosis type 1 (NF1), an autosomal domi-nantly inherited disorder that occurs in 1 in 3000 individuals. It is causedby a mutation in the tumor suppressor gene for neurofibromin onchromosome 17 and is fully penetrant. About 15% of NF1 patients haveONGs, with reports in the literature ranging from 8% to 31%.Conversely, 10% to 70% of patients with ONGs have NF1.6 Themechanism for tumorigenesis depends on the activation of the retro-virus-associated sequence (RAS) oncogene (via loss of inhibition byneurofibromin) and the B1 homolog of the retrovirus-associated function(BRAF) oncogene that, in turn, upregulates mammalian target ofrapamycin pathways, leading to increased protein synthesis and glial
Figure 1. “Anterior” presentation optic nerve glioma. A, External photograph of a child showingright proptosis and vertical strabismus. B, The patient has optic disc swelling. Note lack of hemorrhagesor exudates.
Optic Nerve and Sheath Tumors ’ 239
www.internat-ophthalmology.com
Copyright r 2018 Wolters Kluwer Health, Inc. All rights reserved.

cell proliferation. ONGs also can occur in children with NF2, althoughmuch less frequently.7
Imaging of ONGs typically shows 1 of 2 patterns. The most commonis that of fusiform enlargement of the ON (Fig. 3A). The appearance onmagnetic resonance imaging (MRI) is one of T1 hypointensity orisointensity, T2 hyperintensity, and enhancement after intravenousinjection of a paramagnetic substance such as gadolinium. In some cases,the subarachnoid space (SAS) surrounding the nerve is enlarged andappears to be filled with cerebrospinal fluid (CSF) (Fig. 3B); however,ultrasonography in such cases typically reveals evidence of solid tissue inthe SAS, indicating that the enlargement is due not to trapped CSF but,rather, to spread of tumor into the SAS (the “pseudo-CSF sign”).8Regardless of whether or not there is tumor in the SAS surroundingthe nerve, the nerve usually has a clearly demarcated, smooth margin
Figure 2. “Posterior” presentation of an optic nerve glioma. The child presented with decreasedvisual acuity and reduced color vision in the right eye, associated with a right relative afferentpupillary defect. A, External photograph; note that there is no proptosis or ocular misalignment. B,The right optic disc is pale.
Figure 3. Magnetic resonance imaging characteristics of an optic nerve glioma. A, AxialT2-weighted image shows diffuse fusiform enlargement of the orbital portion of right optic nerve.B, Coronal T2-weighted image shows generalized enlargement of both the nerve and the SASsurrounding the nerve. Although the enlarged SAS could be from increased cerebrospinal fluid in theSAS, it is more likely due to extension of the glioma beyond the confines of the pia-arachnoid; that is,“pseudo-CSF sign.” CSF indicates cerebrospinal fluid; SAS, subarachnoid space.
240 ’ Ediriwickrema and Miller
www.internat-ophthalmology.com
Copyright r 2018 Wolters Kluwer Health, Inc. All rights reserved.

due to an intact ONS [unlike the appearance of an optic nerve sheathmeningioma (ONSM), see below].
A second, less common imaging appearance of an ONG is that of athickened, kinked nerve,6,7 again with what appears to be CSF in anexpanded SAS surrounding the nerve. However, as in the case of ONGswith a fusiform appearance, this phenomenon is due to extension of thetumor into the SAS (Fig. 4). It has been suggested that this appearanceis most often seen in patients with NF1, whereas fusiform enlargementis most often seen in patients with sporadic ONG9; however, bothpatterns can occur in patients with and without NF1 and, thus, neitherpattern is diagnostic.
Some ONGs are associated with ipsilateral enlargement of the opticcanal that may or may not be a sign of intracranial extension. MRI ismuch better than computed tomographic (CT) scanning in identifyingintracranial spread of tumor (Fig. 5). Spicer et al10 found that even ONGsthat appear not to have spread intracranially by MRI as well as by directobservation at the time of nerve resection have done so when ahistopathologic examination is performed on a resected nerve.
On gross inspection, ONGs appear solid or gelatinous and maycontain intraneural hemorrhages. Histopathologically, they most oftenshow the typical features of a low-grade pilocytic astrocytoma, with anincreased number of benign-appearing astrocytes and varying numbersof degenerating astrocytes called Rosenthal fibers6 (Fig. 6). As notedabove, these tumors almost always remain within the dural sheath but notinfrequently spread into the SAS surrounding the nerve.6
The diagnosis of an ONG usually is made on the basis of the clinicalsetting and the appearance of the lesion on imaging. Although other
Figure 4. Axial T2-weighted magnetic resonance image of bilateral optic nerve gliomas in a patientwith neurofibromatosis type 1. Both nerves are thickened and kinked, and there is extension of tumorinto the subarachnoid space surrounding the nerves (the “pseudo-CSF sign”). CSF indicatescerebrospinal fluid.
Optic Nerve and Sheath Tumors ’ 241
www.internat-ophthalmology.com
Copyright r 2018 Wolters Kluwer Health, Inc. All rights reserved.

lesions can mimic ONGs (see below), characteristic findings on imagingusually preclude the need for a diagnostic biopsy. In addition, the biopsyitself could result in permanent visual loss,11 precisely what one is tryingto avoid.
The management of patients with presumed ONGs should betailored to the patient. As noted above, these tumors tend to grow very
Figure 6. Histopathologic appearance of an optic nerve glioma. The tumor is composed of benign-appearing astrocytes and eosinophilic, degenerating astrocytes (Rosenthal fibers), consistent with a low-grade pilocytic astrocytoma. Inset shows Rosenthal fibers at higher power.
Figure 5. Axial T1-weighted, postcontrast magnetic resonance image of a left optic nerve gliomashows a diffusely enlarged, enhancing left optic nerve extending intracranially through an enlargedoptic canal.
242 ’ Ediriwickrema and Miller
www.internat-ophthalmology.com
Copyright r 2018 Wolters Kluwer Health, Inc. All rights reserved.

slowly and may even regress spontaneously. Thus, observation withoutintervention is often indicated, particularly in patients with good visionor at least stable visual function.12,13 For children who present with poorvision and particularly for those whose vision appears to worsen or whosetumors grow on serial imaging, a number of options are available.
Surgery generally is reserved for patients who have cosmeticallyunacceptable proptosis associated with severe visual loss and generallyinvolves resection or debulking of the affected ON14,15 (Fig. 6). In somecases, the ONS can be opened to release trapped CSF or loose tumor.16,17Although some authors recommend resection of ONGs to preventextension to the chiasm, this approach is rarely indicated and, as notedabove, tumor cells are often present beyond the apparent limitssuggested by MRI.10
Radiotherapy is appropriate for some patients with ONGs and can beused as adjunctive therapy or as an alternative to surgery.18,19 It usually isreserved for patients above 5 years of age and, ideally, for patients afterpuberty. The authors of 2 early studies claimed that radiation treatmentproduced shrinkage of both the intraorbital and intracranial portions ofONGs, with subsequent reduction of proptosis, improvement in vision,reduction in optic disc swelling,20 and arrest of progressive visual loss orimprovement of vision.21 However, in a subsequent study, radiation ofONGs did not seem to improve the overall course when compared withsurgery or observation alone.2 In addition, children who undergoradiation therapy have an increased risk of behavior problems, endo-crinologic disturbances, vascular changes (eg, moyamoya-like), andpostradiation malignancies. Most radiation therapy is performed by astereotactic-fractionated technique using photons; there are no long-term data on the use of proton beam therapy (PBT) for ONGs.
Chemotherapy is sometimes used to treat ONGs associated withprogressive visual loss. It may be particularly useful in children below5 years of age. A number of chemotherapeutic agents have beenrecommended, including vincristine, carboplatin, vinblastine, and temo-zolomide. Although none of these agents is consistently effective, impres-sive results have been seen in some cases.22 In addition, over 60% of ONGsin patients without NF1 have a tandem duplication at the BRAF locus thatproduces a fusion gene between KIAA1549 (an uncharacterized gene) andBRAF.23–26 Increased BRAF in astrocytes causes activation of extracellularsignal-related kinase (ERK) and mitogen-activated protein (MAP) kinasedownstream, leading to the development of pilocytic astrocytomas. Thus,chemotherapeutic agents that target the MAP/ERK pathway, such asdabrafenib, may be the appropriate treatment in at least some patientswith ONGs.
In addition to chemotherapy, treatment with topical nerve growthfactor has been found to result in improvement in vision in patients withknown or presumed ONGs. Falsini et al27 treated 5 children with ONGs
Optic Nerve and Sheath Tumors ’ 243
www.internat-ophthalmology.com
Copyright r 2018 Wolters Kluwer Health, Inc. All rights reserved.

and severe optic disc pallor with a 10-day course of topical murine nervegrowth factor. After treatment, all 5 showed an increase in visual evokedpotential amplitudes that persisted for 90 days. The amplitudes declinedby 180 days but still remained above baseline. During this period, MRIshowed no change in tumor size.
Malignant ONGs
Malignant gliomas of the ON are rare and aggressive tumors,resulting in significant morbidity such as severe vision loss, neurologicalsequelae, and death within 1 to 2 years of diagnosis.28 These tumors areWHO grade III (anaplastic astrocytomas) or WHO grade IV (glioblas-toma, gliosarcoma) and typically affect older adults.1,6,28 A retrospectivecase series review of 66 patients revealed a mean age of onset of 57 years,with a range between 22 and 83 years of age, with an approximatelyequal sex distribution.29 Malignant ONGs usually present with rapidlyprogressive monocular visual loss, often associated with retrobulbar pain,simulating acute optic neuritis. Ophthalmoscopy may reveal a normalappearing fundus or, in some cases, a CRVO that may appear relativelymild despite the associated severe visual loss.6,29 One case has been reportedthat was associated with intravitreal seeding of tumor.29 Imaging findingstend to be nonspecific, although in most cases MRI reveals a diffuselythickened nerve that enhances heterogenously (Fig. 7A).6,29–32
Unlike the typical histologic findings in an ONG that occurs inchildhood (see above), the histologic appearance of a malignant ONG is
Figure 7. Malignant optic nerve glioma. The patient was a 67-year-old man with rapidlyprogressive severe visual loss in the right eye, associated with a fundus picture consistent with a centralretinal vein occlusion. A, Axial T1-weighted, postcontrast magnetic resonance image shows a diffuselythickened, markedly enhancing right optic nerve. Because of the rapidly progressive visual loss, thepatient underwent a biopsy of the nerve. B, Histologic examination of the biopsy specimen revealscellular pleomorphism, hyperchromatic nuclei, areas of necrosis, increased vascularity, and a highmitotic index, consistent with a high-grade glioma. The patient died 6 months after diagnosis despitetreatment with both chemotherapy and radiation therapy.
244 ’ Ediriwickrema and Miller
www.internat-ophthalmology.com
Copyright r 2018 Wolters Kluwer Health, Inc. All rights reserved.

that of a high-grade glioma, with cellular pleomorphism, hyperchromaticnuclei, increased vascularity, areas of necrosis, and a high mitotic index(Fig. 7B).6,31,32 Treatment consists of radiotherapy, chemotherapy, or both;however, the prognosis for survival, not to mention vision, is extremelypoor. Molecular profiling for markers such as isocitrate dehydrogenase 1(IDH1) and the alpha-thalassemia/mental retardation syndrome x-linked(ATRX) protein will likely become important in developing more effective,targeted therapies in the future.1
Gangliogliomas
Comprised of both ganglion cells and astrocytes separated byconnective tissue, gangliogliomas are rare, WHO grade I tumors thathave been reported to arise in the ON.1,6,33–36 Although the imagingappearance of an ON ganglioglioma can easily be mistaken for that of abenign ONG, unlike benign ONGs, ON gangliogliomas typically do notenhance on MRI after intravenous injection of gadolinium.33 Despite thisdifference in enhancement, the diagnosis of ON gangliogliomas usually ismade at the time of biopsy or resection of the affected nerve (Fig. 8).
Treatment of an ON ganglioglioma, largely based on anecdotalevidence or results of the treatment of intracranial gangliogliomas, usuallyconsists of a partial nerve resection, with or without adjuvant radiation, ora total resection in a blind or nearly blind eye. There is minimal evidenceregarding the utility of chemotherapy in the literature.33
Medulloepitheliomas
ON medulloepitheliomas, like other tumors of the ON, can presentwith proptosis, disc swelling, and orbital congestion, or simply as
Figure 8. Optic nerve ganglioglioma. A, Axial computed tomographic image shows a diffuselyenlarged left optic nerve. Because of progressive visual loss, the patient underwent a biopsy of thelesion. B, The biopsy specimen shows numerous large cells scattered among an increased population ofglia. The findings are most consistent with a ganglioglioma.
Optic Nerve and Sheath Tumors ’ 245
www.internat-ophthalmology.com
Copyright r 2018 Wolters Kluwer Health, Inc. All rights reserved.

progressive visual loss associated with an optic disc that initially appearsnormal but later becomes pale. Imaging initially may suggest an ONG asthese tumors often produce fusiform enlargement of the ON6 (Fig. 9A).As is the case with other rare tumors of the ON, the diagnosis of an ONmedulloepithelioma usually is made at the time of surgery.
Medulloepitheliomas of the ON have a histopathologic appearanceidentical with that of intracranial and intraocular medulloepitheliomas,with hyperchromatic cells with many mitotic figures (Fig. 9B). The cells arearranged in tubes and cords separated by hyaluronidase-sensitive materialthat stains positively with Alcian blue, resulting in an interconnected web ofcells.6,37,38 Some tumors have more differentiated cells, which may bearranged in rosettes (Fig. 9C). Rare “teratoid variants” have heteroplasmicelements such as cartilage or striated muscle.6,37 Standard treatment isresection of the affected ON. Despite apparent complete resection,recurrences, and metastases can still occur. Thus, most patients are treatedwith adjuvant radiotherapy, chemotherapy, or both.6,38
Figure 9. Optic nerve medulloepithelioma. A, Axial computed tomographic image reveals fusiformenlargement of the left optic nerve with flattening as well as indentation of the back of the left globe.Because of this unusual appearance, the patient underwent an enucleation. B, The enucleationspecimen shows a markedly cellular tumor with hyperchromatic nuclei. The cells, some of which showmitoses, are arranged in tubes and cords, separated by hyaluronidase-sensitive material. C, A subset oftumor cells are more differentiated, exhibiting rosette formation. The histopathologic findings are mostconsistent with a medulloepithelioma.
246 ’ Ediriwickrema and Miller
www.internat-ophthalmology.com
Copyright r 2018 Wolters Kluwer Health, Inc. All rights reserved.

Hemangioblastomas
Like gangliogliomas and medulloepitheliomas, ON hemangioblasto-mas are extremely rare. Kerr et al39 reviewed a series of 10 patients, 5 ofwhom were male, ranging in age from 15 to 44 years. All presented withvision loss, with occasional headaches or pain with eye movement, andsome had proptosis associated with optic disc swelling or pallor. As is thecase with hemangioblastomas elsewhere in the body, ON hemangioblas-tomas may occur as a sporadic phenomenon or in association with vonHippel-Lindau disease. The MRI characteristics of ON hemangioblasto-mas are similar to those of ONGs, but hemangioblastomas tend to enhancemuch more vividly and homogenously than ONGs, similar to theircounterparts in the brain and spinal cord (Fig. 10A). Histologically, thesetumors are typical hemangioblastomas, composed of endothelial cells andpericytes, the juxtaposition of which with intervening vascular channelsand stromal lipid deposits results in histopathologic variability amonglesions (Fig. 10B). It also should be noted that the term “hemangioblas-toma,” is somewhat of a misnomer, as these lesions are benign and rarelyinfiltrate, metastasize, or recur after complete resection.6
Oligodendrogliomas
Oligodendrogliomas constitute between 4% and 12% of all intracranialtumors.40 Both sexes are equally affected. The highest incidence is in thefourth and fifth decades of life, but they may occur in infancy and are notuncommon in childhood and adolescence.41 Most oligodendrogliomasoccur in the cerebral hemispheres, especially the frontal lobes, but they
Figure 10. Optic nerve hemangioblastoma. A, Axial T1-weighted, postcontrast magnetic resonanceimage shows a focal area of homogenous, vivid enhancement within the right optic nerve. Because ofthe unusual appearance of the lesion combined with rapidly progressive visual loss in the right eye, thepatient underwent a biopsy of the right optic nerve. At surgery, this area was noted to be dark red. B,Histologic examination of the biopsy specimen reveals endothelial cells, pericytes, vascular channels,and stromal lipid deposits, consistent with a diagnosis of a hemangioblastoma.
Optic Nerve and Sheath Tumors ’ 247
www.internat-ophthalmology.com
Copyright r 2018 Wolters Kluwer Health, Inc. All rights reserved.

occasionally occur in the region of the third ventricle, cerebellum, rarelywithin the spinal cord, and very rarely in the brainstem.41 Oligodendro-gliomas are composed primarily of compact masses of swollen oligoden-drocytes separated by a scanty and rather delicate supporting stroma ofblood vessels and collagen. There are many areas where the cells are notswollen; in these areas, the cells lie in small clusters with the spaces betweenthe groups of cells bridged by their processes, producing a cobwebappearance. In all cellular areas, mitoses are generally rare, althoughmitotic foci are numerous in some tumors.40
Whether or not ON oligodendrogliomas truly exist is unclear.Lucarini et al42 reported a case in an adult who also had orbital non-Hodgkin lymphoma. According to the report, the affected enlarged ONwas resected and showed histologic changes that “appeared to be”consistent with an oligodendroglioma; however, the authors did notspecify what these changes were, nor did they provide any histologicphotographs. A more informative case was reported by Offret et al.43These authors described a 14-year-old girl who developed proptosis,decreased vision, and ocular motor palsies in the left eye. CT scanningand MRI revealed a large fusiform expansion of the left ON withoutintracranial involvement. The entire ON was resected, and microscopicsections demonstrated changes consistent with an oligodendroglioma.
’ Primary ON Sheath Tumors
Although a number of tumors, such as schwannomas and solitaryfibrous tumors can be tightly adherent to the ONS, there is only 1 tumorthat arises from the sheath itself—the ONSM.
Primary ONSMs
ONSMs account for 2% of all orbital tumors and may be primary orsecondary.44–46 Primary meningiomas arise from the cap cells of thearachnoid that surrounds the intraorbital or intracanalicular portions ofthe ON. Secondary meningiomas arise from the sphenoid ridge, anteriorclinoid process, tuberculum sellae, olfactory groove, or other intracranialregions, and subsequently extend into the space between the dura andarachnoid. Both types can involve the orbital, canalicular, and intra-cranial portions of the ON as they extend along the ONS, graduallyobliterating the pial vasculature, to encircle and, in some cases, infiltratethe nerve by growing along the fibrovascular pial septae.6 Schick et al47proposed a classification system consisting of 3 types of ONSMs. Type IONSMs are limited to the orbital portion of the ON and have acharacteristic fusiform, tubular, or, rarely, globular (ie, exophytic,mimicking an extrinsic lesion such as a cavernous angioma or solitary
248 ’ Ediriwickrema and Miller
www.internat-ophthalmology.com
Copyright r 2018 Wolters Kluwer Health, Inc. All rights reserved.

fibrous tumor) appearance. Type II ONSMs extend through the opticcanal or supraorbital fissure, sometimes with invasion of the cavernoussinus. Type III ONSMs have intracranial extension > 1 cm, includingextension to the optic chiasm or across the planum sphenoidale to thecontralateral ON.
The epidemiology of ONSMs is well-defined. Dutton44 reviewed aseries of 5000 orbital meningiomas and found that 90% were secondaryto intracranial extension (ie, secondary ONSMs), whereas about 10%were primary ONSMs, with the vast majority of these (92%) originatingwithin the orbit and the remaining tumors (8%) arising within the opticcanal. ONSMs almost always are unilateral, but they may be bilateral,particularly in patients with NF2.48 They most often occur in middle-aged women but may develop at any age and in men.
Patients with ONSMs usually present with painless, slowly progres-sive, monocular vision loss associated with reduced color vision. Somepatients have transient obscurations of vision, particularly in eccentricgaze. The clinical findings in patients with an ONSM include not onlyvariably reduced visual acuity and color vision but also a visual fielddefect that can be of any type and severity, an ipsilateral relative afferentpupillary defect, and an optic disc that may appear normal, swollen, orpale, depending on the location of the tumor and the duration of visualsymptoms.6,44–46 Proptosis is often present, but the degree is extremelyvariable and depends in large part on the volume of the lesion. Patientswith fusiform enlargement and patients with the rare globular type oftumor tend to have moderate proptosis, whereas patients with thetubular type may have no proptosis or only 1 or 2mm. About one third ofpatients with ONSMs have retinal-choroidal vessels that shunt venousblood from the retina to the choroid due to compression of the centralretinal vein.6,44,46 When associated with decreased acuity and optic discpallor, these vessels are almost pathognomonic of an ONSM (Fig. 11).49
As noted above, ONSMs have several appearances on imaging. CTscanning typically reveals fusiform or tubular enlargement of the affectedON, the sheath of which appears thickened and enhances. In some casesthe sheath is partially calcified (ie, the “tram-track” sign) (Fig. 12). MRI ismore revealing than CT scanning, as it shows that the apparently enlargedON is actually normal in diameter and is hypointense on T1-weightedimages, whereas it is the ONS that is thickened and markedly enhanced(Fig. 13). In addition, unlike ONGs that, as noted above, have a smoothdural outline, ONSMs always show small, thin extensions from the affectedsheath into the orbit44–46 (Fig. 14). Although this appearance is notpathognomonic for an ONSM, as it rarely may be seen in patients withsarcoid affecting the ON, it is extremely suggestive. Thus, as is the casewith children with presumed ONGs (see above), the combination of theclinical setting, history, examination findings, and imaging results usuallyleads to the correct diagnosis without the need for a biopsy.
Optic Nerve and Sheath Tumors ’ 249
www.internat-ophthalmology.com
Copyright r 2018 Wolters Kluwer Health, Inc. All rights reserved.

Histopathologically, ONSMs usually are characterized by concentricwhorls of spindle cells with interspersed hyalinized calcium depositsknown as psammoma bodies (Fig. 15). A second pattern consists of sheetsof polygonal cells that are separated by tumor vessels.6,44,46
As in patients with ONGs, the management of patients with ONSMsmust be individualized. These tumors are not a threat to life or neurologicalfunction, and primary ONSMs rarely extend intracranially across theplanum sphenoidale to compromise the contralateral ON. Thus, their onlymorbidity is that related to visual loss from damage to the affected ON.
Not everyone with an ONSM requires treatment. Observation isappropriate if the patient has no significant visual dysfunction, there is nosignificant documented progression of visual loss, and there is no
Figure 11. Optic disc photograph in a 45-year-old woman with a 6-month history of progressivevisual loss in the left eye. The left optic disc is pale and there are several retinochoroidal shunt vessels(previously called “optociliary shunt vessels”). In the setting of progressive visual loss and optic discpallor, these vessels are pathognomonic of an optic nerve sheath meningioma.
Figure 12. Axial computed tomographic image shows evidence of peripheral calcification along anenlarged left optic nerve. This “tram-track sign” is pathognomonic of an optic nerve sheathmeningioma.
250 ’ Ediriwickrema and Miller
www.internat-ophthalmology.com
Copyright r 2018 Wolters Kluwer Health, Inc. All rights reserved.

significant intracranial extension. We believe that patients being observedshould be examined every 3 to 6 months and undergo imaging (preferablyMRI) every 6 to 12 months. Such patients also should be told to contact theophthalmologist if they believe that their vision is worsening.
Figure 13. Axial T1-weighted, postcontrast magnetic resonance images in patients with presumedoptic nerve sheath meningiomas. A, A diffusely enlarged right optic nerve shows irregular peripheralenhancement (the “tram-track sign”). B, A low-density right optic nerve that is normal in diameter issurrounded by an enhancing fusiform mass. C, There is a mildly enhancing mass adjacent to a rightoptic nerve, associated with an enhancing “dural tail” medially along the nerve and lateral peripheralenhancement of the nerve that extends from the globe to the orbital apex.
Figure 14. Coronal T1-weighted, postcontrast magnetic resonance image of a patient with apresumed right optic nerve sheath meningioma reveals thin extensions from the affected sheath into thesurrounding orbital fat.
Optic Nerve and Sheath Tumors ’ 251
www.internat-ophthalmology.com
Copyright r 2018 Wolters Kluwer Health, Inc. All rights reserved.

There is no proven medical treatment for ONSMs. Becausemeningioma cells often express a variety of hormone receptors, mostcommonly estrogen and progesterone receptors,50 and because they canincrease in size during pregnancy,51,52 it might be expected that treat-ment with estrogen or progesterone antagonists (eg, tamoxifen, mefipri-stone) would result in destruction of the tumor or at least reduction in itssize and extent, but this does not seem to be the case. Similarly, althoughhydroxyurea has been said to be helpful in some cases of intracranialmeningioma, we are aware of only 1 case report in which the treatment ofan ONSM with hydroxyurea resulted in visual improvement.53
As noted above, the major morbidity of an ONSM is loss of vision inthe affected eye. For this reason, and because ONSMs are intimatelyrelated to the ON and its blood supply, surgery to excise the tumorusually is not indicated because in most cases of attempted excision, thepatient is rendered blind following surgery, precisely the complicationone is trying to avoid. In addition, disturbances of eyelid function and eyemovement can occur postoperatively.44–46 The only exceptions areONSMs that are primarily extradural. In such cases, the bulk of thetumor can be excised,54 although rarely if ever can the entire tumor beremoved; at least some of the tumor remains behind in the subdural orSAS surrounding the nerve. In other cases, particularly those with acutevisual loss, some authors recommend opening the ONS to decompressthe nerve.55,56 We believe that this procedure should be used only iffollowed by fractionated radiation therapy (see below). Otherwise, thevisual improvement is only temporary, and, in addition, the tumorsubsequently may spread throughout the orbit.
The standard of care for ONSMs that require treatment is radiationtherapy.44–46 This may be delivered in 1 of 5 ways: (1) conventional
Figure 15. Histologic appearance of an optic nerve sheath meningioma. There are concentricwhorls of spindle cells with interspersed hyalinized calcium bodies; that is, psammoma bodies. Note theintimate association of the tumor with the optic nerve sheath.
252 ’ Ediriwickrema and Miller
www.internat-ophthalmology.com
Copyright r 2018 Wolters Kluwer Health, Inc. All rights reserved.

fractionated radiation therapy; (2) single-dose stereotactic radiosurgery(SRS); (3) hypofractionated SRS; (4) PBT; and (5) stereotactic-fractio-nated radiotherapy (SFR).
In 2002, Turbin et al57 reported a retrospective series of 64 patientswith ONSMs managed with either observation alone, surgery, surgerywith radiation, or radiation alone. The study included patients from theoriginal report of Kennerdell et al.58 The follow-up in the study byTurbin and colleagues ranged from 51 months to 516 months, with amean follow-up of 150 months, and revealed that treatment withradiation alone resulted in the best long-term visual outcome eventhough about one third of patients treated in this manner developedcomplications from radiation, including radiation retinopathy, retinalvascular occlusion, persistent iritis, and temporal lobe atrophy. The studydid not describe which radiation technique was used, but given the eraduring which the study was conducted and the length of time the patientswere followed, it is likely that the majority of the patients were treatedwith conventional radiation.
Conventional radiation therapy for ONSMs usually consists of 5000cGy given in doses of 180 to 200 cGy daily fractions. The main advantageof this technique is that it can be performed by almost any radiationcenter. The disadvantage is the potential toxicity that can result fromradiation damage to adjacent normal tissue, including the retina(particularly if the tumor extends up to or very near the globe) and thepituitary gland (for tumors that extend intracranially).
The threshold for radiation damage to the ON has been estimated tobe 80 to 100 cGy for a single dose.59 Because lower doses of radiation arethought to have a more uncertain effect on benign tumors such asONSMs, and a large, single dose of radiation is associated with a high riskof tissue damage,60 single-dose SRS is not widely used to treat ONSMs.Nevertheless, several patients have been reported in whom visualfunction stabilized or improved after this treatment.61,62
A variant of single-dose SRS is hypofractionated SRS. This consists ofa 5-consecutive day regimen that delivers a total dose of 250 cGy (50 cGyper session). Two large series using this technique have been reported todate.63,64 The largest series consisted of 25 patients who had a meanfollow-up of 27 months (range, 11 to 68mo).64 Among the 21 patientswho had vision before treatment (4 were already blind), visual acuityimproved in 27%, visual field improved in 35%, and, perhaps mostimportantly, no patient experienced worsening of acuity or field.
As is the case with hypofractionated SRS, there are little dataconcerning the efficacy of PBT in the treatment of ONSMs. Theoret-ically, it should be less likely to produce damage to surrounding normaltissue because of the shape of the Bragg peak for protons compared withphotons; however, there also is the risk that the focus could be so limitedthat cells at the apparent proximal and distal extents of the tumor could
Optic Nerve and Sheath Tumors ’ 253
www.internat-ophthalmology.com
Copyright r 2018 Wolters Kluwer Health, Inc. All rights reserved.

survive and subsequently grow. Nevertheless, Moyal et al65 reported theresults of PBT in 15 patients: 13 women and 2 men. Among these 15individuals, 4 received PBT after a period of observation, 5 were treatedafter surgery, and 6 underwent PBT as a primary procedure. All received52.2 cGy equivalents in 29 daily fractions of 1.8 cGy equivalents. Over amean follow-up period of 22.4 months (range, 8 to 79mo), visual acuityimproved in 3, remained stable in 11, and deteriorated in 1. Tumor sizeremained stable in all patients by MRI. There were no adverse effects.The conclusion of the authors was that PBT is both a safe and an effectivetreatment for ONSMs.
Despite the encouraging short-term results from other forms ofradiation therapy, the current standard of care for patients with ONSMsthat require treatment is SFR.66,67 This technique appears to offer thepotential for delivering a sufficient amount of radiation to an ONSM in amanner more focused than that of conventional fractionated radiationtherapy, thus minimizing the complications from exposure of thesurrounding tissue to high doses of radiation.
SFR requires complex planning, which is facilitated by sophisticatedsoftware and 3-dimensional imaging. Linear accelerator units, such as theCyberknife, use a tracking system that eliminates the need for rigidimmobilization during pretreatment imaging and treatment. Thesesystems deliver the radiation in noncoplanar fields that take into accountthe characteristics of the surrounding tissue. Every beam is size-adjustedand shape-adjusted by different devices, with microleaf collimators beingthe most advanced way of achieving a high degree of conformality to thetumor. Patients in whom SFR is used to treat an ONSM usually receive 50to 54 Gy in 180 cGy daily fractions.
Patients with ONSMs treated with SFR generally have an excellentshort-term and long-term prognosis characterized by sustained visualimprovement or stability with minimal complications.66–73 Combining thedata from published studies, it would appear that about 95% of patients withpresumed or biopsy-proven ONSMs treated with SFR show either improve-ment or stability of their visual function (Fig. 16). Improvement in visualfunction generally begins within 3 months after treatment in the majority ofthe cases and in some cases, within a few weeks after completion ofradiation.45 Posttreatment imaging generally shows no change in tumor sizeor extent, although some tumors, particularly those with a fusiform orglobular appearance, demonstrate a reduction in volume over time.
Acute effects of SFR include headache, nausea, local erythema, andfocal alopecia. None of these complications tends to be severe orpermanent. Rare patients experience a transient worsening of visionduring SFR that usually responds dramatically to treatment with systemiccorticosteroids.
SFR is not without potential permanent visual complications. Radia-tion retinopathy is the most common, usually developing between
254 ’ Ediriwickrema and Miller
www.internat-ophthalmology.com
Copyright r 2018 Wolters Kluwer Health, Inc. All rights reserved.

14 months and 4 years following treatment with at least 50Gy of radiation.Patients in whom this complication occurs may be asymptomatic, but someauthors have reported loss of vision ranging from 20/25 to lightperception.74 We believe that patients with ONSMs involving the proximalpart of the ON adjacent to the globe are at the greatest risk of developingradiation-induced retinopathy, and this potential complication thus shouldbe considered when deciding whether or not to treat such patients.
Figure 16. Results of visual field testing (Humphrey automated perimeter) before and aftertreatment of a patient with a left optic nerve sheath meningioma using stereotactic-fractionatedradiation. Note marked improvement in the visual field (B, D) compared with pretreatment (A, C).
Optic Nerve and Sheath Tumors ’ 255
www.internat-ophthalmology.com
Copyright r 2018 Wolters Kluwer Health, Inc. All rights reserved.

Other late ophthalmic complications of SFR include cataract, dry eye,and iritis, with dry eye being the most common.66–73 Although radiationoptic neuropathy is a potential complication of SFR, it appears to occurrarely; in fact, there has never been a case reported at our institution.Finally, some patients continue to lose vision from tumor progressiondespite SFR, although this should not be considered a complication of thetreatment.
Late nonocular side effects of SFR include pituitary dysfunction andpunctate white-matter lesions in the cerebral hemispheres, presumablyfrom the effects of radiation on cerebral blood flow. Both findings are apotential concern after irradiation of posteriorly located ONSMs,particularly those with mild but definite intracranial extension. Intervalmonitoring of pituitary function in such patients thus is appropriate.
On the basis of the results of published studies, we believe that SFR isthe best option for most cases of progressive or advanced disease.However, because of improved imaging, patients with presumed ONSMsassociated with mild progressive or stable visual loss are being diagnosedearlier, and the choice between observation and radiation has becomemore difficult.
’ Secondary ON and Sheath Tumors
A variety of tumors can damage the ON, usually by infiltration,compression, or both. Secondary tumors that can infiltrate or compressthe nerve include carcinomas, lymphomas, and other rare neoplasms.The clinical manifestations and management of the tumor depend inpart on the location of the damage and in part on the natural history ofthe neoplasm. The most common tumor that affects the ONS is thesecondary ONSM. As noted above, this is a meningioma that arises notfrom the sheath of the nerve but, rather, from the intracranial arachnoidcap cells along the planum sphenoidale, tuberculum sellae, or anteriorclinoid process and extends into the optic canal where it is intimatelyassociated with the ONS. If a secondary ONSM has a significantintracranial component, that component can be resected; however, oncethe tumor has extended into the optic canal, the canal can be unroofed toprovide some relief from ON compression, but radiation therapy isrequired to halt further tumor growth.
’ Summary
Tumors of the ON and ONS are diverse in etiology. Diagnosis of themore common ONGs and ONSMs are usually made clinically, based onpresentation and imaging characteristics. Biopsy and histologic analysis,however, may be required in the setting of progressive symptoms or
256 ’ Ediriwickrema and Miller
www.internat-ophthalmology.com
Copyright r 2018 Wolters Kluwer Health, Inc. All rights reserved.

aggressive tumors, to rule out malignant subtypes or mimickers. Treatmentparadigms are largely tailored to the type of tumor and clinical profile ofthe patient. Whereas optic pathway gliomas can usually be monitoredclinically, and symptomatic ONSM are treated with SFR, other tumors mayrequire surgical resection, radiation, chemotherapy, immunomodulatorytherapy, or a combination of these modalities. Overall prognosis dependson the tumor pathology, and will largely be affected by the evolvinglandscape of molecular profiling and multimodal drug design.
The authors declare that they have no conflicts of interest to disclose.
’ References
1. Dutton JJ. Gliomas of the anterior visual pathway. Surv Ophthalmol. 1994;38:427–452.2. Rush JA, Younge BR, Campbell RJ, et al. Optic glioma: long-term follow-up of 85
histologically verified cases. Ophthalmology. 1982;89:1213–1219.3. Louis DN, Perry A, Reifenberger G, et al. The 2016 World Health Organization
classification of tumors of the central nervous system: a summary. Acta Neuropathol.2016;131:803–820.
4. Smith JL, Flynn JT, Spiro HJ. Monocular vertical oscillations of amblyopia. TheHeimann-Bielschowsky phenomenon. J Clin Neuroophthalmol. 1982;2:85–91.
5. Miller NR. Optic gliomas: past, present, and future. J Neuroophthalmol. 2016;36:460–473.6. Miller NR. Primary tumours of the optic nerve and its sheath. Eye. 2004;18:1026–1037.7. Brodsky MC. The Apparently Blind Infant In Pediatric Neuro-Ophthalmology. New York,
NY: Springer; 2016:34–43.8. Brodsky MC. The “pseudo-CSF” signal of orbital optic glioma on magnetic resonance
imaging: a signature of neurofibromatosis. Surv Ophthalmol. 1993;38:213–218.9. Stern J, Jakobiec FA, Housepian EM. The architecture of optic nerve gliomas with and
without neurofibromatosis. Arch Ophthalmol. 1980;98:505–511.10. Spicer GJ, KazimM, Glass LR, et al. Accuracy of MRI in defining tumor-free margin in
optic nerve glioma surgery. Ophthal Plast Reconstr Surg. 2013;29:277–280.11. Revere KE, Katowitz WR, Katowitz JA, et al. Childhood optic nerve glioma: vision loss
due to biopsy. Ophthal Plast Reconstr Surg. 2017;33:S107–S109.12. Tow SL, Chandela S, Miller NR, et al. Long-term prognosis in children with gliomas of
the anterior visual pathway. Pediatr Neurol. 2003;28:262–270.13. Parsa CF, Hoyt WF, Lesser RL, et al. Spontaneous regression of optic gliomas. Thirteen
cases documented by serial neuroimaging. Arch Ophthalmol. 2001;119:516–529.14. Wolter JR. Large optic nerve glioma removed by the transconjunctival approach.
J Pediatr Ophthalmol. 1973;10:142–146.15. Althekair FY. Debulking optic nerve gliomas for disfiguring proptosis: a globe-sparing
approach by lateral orbitotomy alone. Presented as a poster at the 42nd AnnualMeeting of the North American Neuro-Ophthalmology Society, Tucson, AZ. February28, 2016.
16. Vanderveen DK, Nihalani BR, Barron P, et al. Optic nerve sheath fenestration for anisolated optic nerve glioma. J AAPOS. 2009;13:88–90.
17. Chen A, Yoon MK, Haugh S, et al. Surgical management of an optic nerve glioma withperineural arachnoidal gliomatosis growth pattern. J Neuroophthalmol. 2013;33:51–53.
Optic Nerve and Sheath Tumors ’ 257
www.internat-ophthalmology.com
Copyright r 2018 Wolters Kluwer Health, Inc. All rights reserved.

18. McDonnell P, Miller NR. Chiasmatic and hypothalamic extension of optic nerveglioma. Arch Ophthalmol. 1983;101:1412–1415.
19. Marwaha G, Macklis R, Singh AD. Radiation therapy: orbital tumors. Dev Ophthalmol.2013;52:94–101.
20. Taveras JM, Mount LA, Wood EH. The value of radiation therapy in the managementof glioma of the optic nerves and chiasm. Radiology. 1956;66:518–528.
21. Throuvalas N, Bataini P, Ennuyer A. Les gliomes du chiasma et du nerf optique:L’apport de la radiotherapie transcutanée dans leur traitement [Gliomas of the chiasmand optic nerve: The role of external radiation therapy in their treatment].Bull Assoc Etude Cancer. 1969;56:231–264.
22. Parentin F, Rabusin M, Zannaro F, et al. Chemotherapy for optic nerve glioma in achild with neurofibromatosis type-1. Neuro-Ophthalmology. 2008;32:159–162.
23. Pfister S, Janzarik WG, Remke M, et al. BRAF gene duplication constitutes amechanism of MAPK pathway activation in low-grade astrocytomas. J Clin Invest. 2008;118:1739–1749.
24. Rodriguez FJ, Lim KS, Bowers D, et al. Pathological and molecular advances inpediatric low-grade astrocytoma. Annu Rev Pathol Mech Dis. 2013;8:361–379.
25. Yu J, Deshmukh H, Gutmann RJ, et al. Alterations of BRAF and HIPK2 locipredominate in sporadic pilocytic astrocytoma. Neurology. 2009;73:1526–1531.
26. Rodriguez FJ, Ligon AH, Horkayne-Szakaly I, et al. BRAF duplications and MAPKpathway activation are frequent in gliomas of the optic nerve proper. J Neuropathol ExpNeurol. 2012;71:789–794.
27. Falsini B, Chiaretti A, Barone G, et al. Total nerve growth factor as a visual rescuestrategy in pediatric optic gliomas: a pilot study including electrophysiology. Neuro-rehabil Neural Repair. 2011;25:512–520.
28. Cimino PJ, Sychev Y, Gonzalez-Cuyar LF, et al. Primary gliosarcoma of the optic nerve:a unique adult optic pathway glioma. Ophthal Plast Reconstr Surg. 2017;33:e88–e92.
29. Spoor TC, Kennerdell JS, Martinez Z, et al. Malignant gliomas of the optic nervepathways. Am J Ophthalmol. 1980;89:284–292.
30. Chong VF. The orbits in cancer imaging. Cancer Imaging. 2006;6:S27–S31.31. Brodovsky S, ten Hove MW, Pinkerton RM, et al. An enhancing optic nerve lesion:
malignant glioma of adulthood. Can J Ophthalmol. 1997;32:409–413.32. Taphoorn MJB, de Vries-Knoppert WAEJ, Ponssen H, et al. Malignant optic glioma
in adults. Case report. J Neurosurg. 1989;70:277–279.33. Rolston JD, Han SJ, Cotter JA, et al. Gangliogliomas of the optic pathway. J Clin
Neurosci. 2014;21:2244–2249.34. Gritzman MCD, Snyckers FD, Proctor NS. Ganglioglioma of the optic nerve. A case
report. S Afr Med J. 1983;63:863–865.35. Bergin DJ, Johnson TE, Spencer WH, et al. Ganglioglioma of the optic nerve. Am J
Ophthalmol. 1988;105:146–149.36. Sadun F, Hinton DR, Sadun AA. Rapid growth of an optic nerve ganglioglioma in a
patient with neurofibromatosis 1. Ophthalmology. 1996;103:794–799.37. Chidambaram B, Santosh V, Balasubramanian V. Medulloepithelioma of the optic
nerve with intradural extension: report of two cases and a review of the literature.Childs Nerv Syst. 2000;16:329–333.
38. Chavez M, Mafee MF, Castillo B, et al. Medulloepithelioma of the optic nerve. J PediatrOphthalmol Strabismus. 2004;41:48–52.
39. Kerr DJ, Scheithauer BW, Miller GM, et al. Hemangioblastoma of the optic nerve: casereport. Neurosurgery. 1995;36:573–581.
40. McLendon RE, Kros JM, Bruner J, et al. Oligodendrogliomas. In: McLendon RE,Rosenblum MK, Bigner DD, eds. Russell and Rubinstein’s Pathology of Tumors of theNervous System, 7th ed. London: Hodder Arnold; 2006:167–186.
258 ’ Ediriwickrema and Miller
www.internat-ophthalmology.com
Copyright r 2018 Wolters Kluwer Health, Inc. All rights reserved.

41. Hedges TR III. Tumors of neuroectodermal origin. In: Miller NR, Newman NJ,Biousse V, Kerrison JB, eds. Walsh and Hoyt’s Clinical Neuro-Ophthalmology, 6th ed.Philadelphia, PA: Lippincott Williams & Wilkins; 2005;2:1439–1442.
42. Lucarini C, Tomei G, Gaini SM, et al. A case of optic nerve oligodendroglioma associated withan orbital non-Hodgkin’s lymphoma in adult. Case report. J Neurosurg Sci. 1990;34:319–321.
43. Offret H, Gregoire-Cassoux N, Frau E, et al. Solitary oligodendroglioma of the opticnerve. Apropos of a case. J Fr Ophtalmol. 1995;18:158–163.
44. Dutton JJ. Optic nerve sheath meningiomas. Surv Ophthalmol. 1992;37:167–183.45. Miller NR. New concepts in the diagnosis and management of optic nerve sheath
meningioma. J Neuroophthalmol. 2006;26:200–208.46. Shapey J, Sabin HI, Danesh-Meyer HV, et al. Diagnosis and management of optic
nerve sheath meningiomas. J Clin Neurosci. 2013;20:1045–1056.47. Schick U, Dott U, Hassler W. Surgical management of meningiomas involving the
optic nerve sheath. J Neurosurg. 2004;101:951–959.48. Bosch MM, Wichmann WW, Boltshauser E, et al. Optic nerve sheath meningiomas in
patients with neurofibromatosis type 2. Arch Ophthalmol. 2006;124:379–385.49. Frisén L, Hoyt WF, Tengroth BM. Optociliary veins, disc pallor and visual loss. Acta
Ophthalmol. 1973;51:241–249.50. ThomM, Martinian L. Progesterone receptors are expressed with higher frequency by
optic nerve sheath meningiomas. Clin Neuropathol. 2002;21:5–8.51. Wright JE, Call NB, Liarcos S. Primary optic nerve sheath meningioma. Br J
Ophthalmol. 1980;64:553–558.52. Berete R, Vignal-Clermont C, Boissonnet H, et al. Optic nerve sheath meningioma:
diagnosis and new treatment options, a case study of monocular blindness duringpregnancy [in French]. J Fr Ophtalmol. 2006;29:426–431.
53. Paus S, Klockgether T, Urbach H, et al. Meningioma of the optic nerve sheath:treatment with hydroxyurea. J Neurol Neurosurg Psychiatry. 2003;74:1348–1350.
54. Mark LE, Kennerdell JS, Maroon JC, et al. Microsurgical removal of a primaryintraorbital meningioma. Am J Ophthalmol. 1978;86:704–709.
55. Saeed P, Rootman J, Nugent RA, et al. Optic nerve sheath meningiomas. Ophthalmology.2003;110:2019–2030.
56. Turbin RE, Pokorny K. Diagnosis and treatment of orbital optic nerve sheathmeningioma. Cancer Control. 2004;11:334–341.
57. Turbin RE, Thompson CR, Kennerdell JS, et al. A long-term visual outcomecomparison in patients with optic nerve sheath meningioma managed with observation,surgery, radiotherapy, or surgery and radiotherapy. Ophthalmology. 2002;109:890–899.
58. Kennerdell JS, Maroon JC, Malton M, et al. The management of optic nerve sheathmeningiomas. Am J Ophthalmol. 1988;106:450–457.
59. Parsons JT, Bova FJ, Fitzgerald CR, et al. Radiation optic neuropathy aftermegavoltage external-beam irradiation: analysis of time-dose factors. Int J Radiat OncolBiol Phys. 1994;30:755–763.
60. Girkin CA, Comey CH, Lunsford LD, et al. Radiation optic neuropathy afterstereotactic radiosurgery. Ophthalmology. 1997;104:1634–1643.
61. Kwon Y, Bae JS, Kim JM, et al. Visual changes after gamma knife surgery for opticnerve tumors. Report of three cases. J Neurosurg. 2005;102(suppl):43–46.
62. Klink DF, Miller NR, Williams J. Preservation of residual vision 2 years afterstereotactic radiosurgery for a presumed optic nerve sheathmeningioma. J Neuroophthalmol.1998;18:117–120.
63. Romanelli P, Wowra B, Muacevic A. Multisession CyberKnife radiosurgery for opticnerve sheath meningiomas. Neurosurg Focus. 2007;23:E11–E16.
64. Marchetti M, Bianchi S, Milanesi I, et al. Multisession radiosurgery for optic nervesheath meningiomas—an effective option: preliminary results of a single-centerexperience. Neurosurgery. 2011;69:1116–1122.
Optic Nerve and Sheath Tumors ’ 259
www.internat-ophthalmology.com
Copyright r 2018 Wolters Kluwer Health, Inc. All rights reserved.

65. Moyal L, Vignal-Clermont C, Boissonnet H, et al. Results of fractionated targetedproton beam therapy in the treatment of optic nerve sheath meningioma. J FrOphtalmol. 2014;37:288–295.
66. Liu JK, Forman S, Hershewe GL, et al. Optic nerve sheath meningiomas: visualimprovement after stereotactic radiotherapy. Neurosurgery. 2002;50:950–957.
67. Richards JC, Roden D, Harper CS. Management of sight-threatening optic nervesheath meningioma with fractionated stereotactic radiotherapy. Clin Exp Ophthalmol.2005;33:137–141.
68. Pitz S, Becker G, Schiefer U, et al. Stereotactic fractionated irradiation of optic nervesheath meningioma: a new treatment alternative. Br J Ophthalmol. 2002;86:1265–1268.
69. Andrews DW, Faroozan R, Yang BP, et al. Fractionated stereotactic radiotherapy forthe treatment of optic nerve sheath meningiomas: preliminary observations of 33 opticnerves in 30 patients with historical comparison to observation with or without priorsurgery. Neurosurgery. 2002;51:890–902.
70. Narayan S, Cornblath WT, Sandler HM, et al. Preliminary visual outcomes after three-dimensional conformal radiation therapy for optic nerve sheath meningioma. Int JRadiat Oncol Biol Phys. 2003;56:537–543.
71. Baumert BG, Villa S, Studer G, et al. Early improvements in vision after fractionatedstereotactic radiotherapy for primary optic nerve sheath meningioma. Radiother Oncol.2004;72:169–174.
72. Lesser RL, Knisely JP, Wang SL, et al. Long-term response to fractionated radio-therapy of presumed optic nerve sheath meningioma. Br J Ophthalmol. 2010;94:559–563.
73. Metellus P, Kapoor S, Kharkar S, et al. Fractionated conformal radiotherapy of opticnerve sheath meningiomas: long-term outcomes of tumor control and visual functionat a single institution. Int J Radiat Oncol Biol Phys. 2011;80:185–192.
74. Subramanian PS, Bressler NM, Miller NR. Radiation retinopathy after fractionatedstereotactic radiotherapy for optic nerve sheath meningioma. Ophthalmology. 2004;111:565–567.
260 ’ Ediriwickrema and Miller
www.internat-ophthalmology.com
Copyright r 2018 Wolters Kluwer Health, Inc. All rights reserved.
Related Documents