NEOPLASMS OF MEDIASTINUM THEODORE D. LIWONGAN 1. ANATOMY The mediastinum comprises an anatomic space located between the thoracic inlet and the diaphragm, and bordered on the left and right sides by the pleural cavities. This central anatomic location houses or borders vital structures of almost every major organ system including the heart and great vessels of the circulatory system, the esophagus, and major airways of the aerodigestive tract, the thymus of the immune system, and important nerves such as the phrenic and vagus nerves. Further, various endocrine organs may project into it, distant malignancies may metastasize to it, and infectious processes can manifest themselves within it. 2. EPIDEMIOLOGY AND INCIDENCE The incidence and type of primary mediastinal neoplasms varies with patient age. In combined series totaling 3017 mostly adult patients, the incidence of mediastinal masses in decreasing frequency were thymomas and thymic cysts (26.5%), neurogenic tumors (20.2%), germ cell tumors (GCTs) (13.8%), lymphomas (12.7%), foregut cysts (10.3%), and pleuropericardial cysts (6.6%). In children, combined series totaling 718 patients demonstrated that neurogenic tumors were most common (41.6%), followed by GCTs (13.5%), foregut cysts (13.4%), lymphomas (13.4%), angiomas and lymphangiomas (6.1%), and thymic tumors or cysts (4.9%).2 In general, the incidence of anterior lesions is higher in adults, and posterior lesions predominate in children. Further, the incidence of malignancy differs among primary mediastinal masses arising in each of the different compartments. In one of the largest series, Davis and colleagues demonstrated that among patients with mediastinal masses, malignancy was found in 59% of those in the anterior mediastinum, 29% of those in the middle mediastinum, and 16% of those in the posterior mediastinum. Mediastinal masses are often incidentally detected on imaging studies obtained for other reasons. An estimate of the frequency of “incidental” mediastinal masses has been provided by a large lung cancer screening study. In 9263 individuals at high risk for lung cancer who underwent a computed tomography (CT) screening examination, a mediastinal mass was found in 71 patients (0.77%). The majority of these incidental masses were thymic and most were treated successfully with a conservative approach. 3. DIAGNOSIS Mediastinal masses rarely cause chest pain. Most attract attention by compression of normal structures or are found incidentally on chest X-ray. Signs suggesting mediastinal tumors are dyspnea from retrosternal goiter, hoarseness, and brassy cough from compression of the recurrent laryngeal nerve, Horner syndrome (unilateral ptosis, miosis, and anhidrosis) from involvement of the superior cervical ganglion, edema of the arms and neck with cyanosis from obstruction of the SVC, and chylous

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
NEOPLASMS OF MEDIASTINUM THEODORE D. LIWONGAN
1. ANATOMY
The mediastinum comprises an anatomic space located between the thoracic inlet and
the diaphragm, and bordered on the left and right sides by the pleural cavities.
This central anatomic location houses or borders vital structures of almost every
major organ system including the heart and great vessels of the circulatory system,
the esophagus, and major airways of the aerodigestive tract, the thymus of the
immune system, and important nerves such as the phrenic and vagus nerves. Further,
various endocrine organs may project into it, distant malignancies may metastasize
to it, and infectious processes can manifest themselves within it.
2. EPIDEMIOLOGY AND INCIDENCE
The incidence and type of primary mediastinal neoplasms varies with patient age. In
combined series totaling 3017 mostly adult patients, the incidence of mediastinal
masses in decreasing frequency were thymomas and thymic cysts (26.5%), neurogenic
tumors (20.2%), germ cell tumors (GCTs) (13.8%), lymphomas (12.7%), foregut cysts
(10.3%), and pleuropericardial cysts (6.6%). In children, combined series totaling
718 patients demonstrated that neurogenic tumors were most common (41.6%), followed
by GCTs (13.5%), foregut cysts (13.4%), lymphomas (13.4%), angiomas and
lymphangiomas (6.1%), and thymic tumors or cysts (4.9%).2 In general, the incidence
of anterior lesions is higher in adults, and posterior lesions predominate in
children. Further, the incidence of malignancy differs among primary mediastinal
masses arising in each of the different compartments. In one of the largest series,
Davis and colleagues demonstrated that among patients with mediastinal masses,
malignancy was found in 59% of those in the anterior mediastinum, 29% of those in
the middle mediastinum, and 16% of those in the posterior mediastinum.
Mediastinal masses are often incidentally detected on imaging studies obtained for
other reasons. An estimate of the frequency of “incidental” mediastinal masses
has been provided by a large lung cancer screening study. In 9263 individuals at
high risk for lung cancer who underwent a computed tomography (CT) screening
examination, a mediastinal mass was found in 71 patients (0.77%). The majority of
these incidental masses were thymic and most were treated successfully with a
conservative approach.
3. DIAGNOSIS
Mediastinal masses rarely cause chest pain. Most attract attention by compression
of normal structures or are found incidentally on chest X-ray. Signs suggesting
mediastinal tumors are dyspnea from retrosternal goiter, hoarseness, and brassy
cough from compression of the recurrent laryngeal nerve, Horner syndrome (unilateral
ptosis, miosis, and anhidrosis) from involvement of the superior cervical ganglion,
edema of the arms and neck with cyanosis from obstruction of the SVC, and chylous
pleural effusion. Lymph nodes are enlarged in Hodgkin disease, non-Hodgkin lymphoma,
carcinoma, germ cell tumors, or tuberculosis. Other locations of neoplastic tissue
are retrosternal goiter, thymoma, and teratoma (dermoid cyst). When a dermoid forms
a tracheal fistula, it may produce trichoptysis, coughing up of hair.
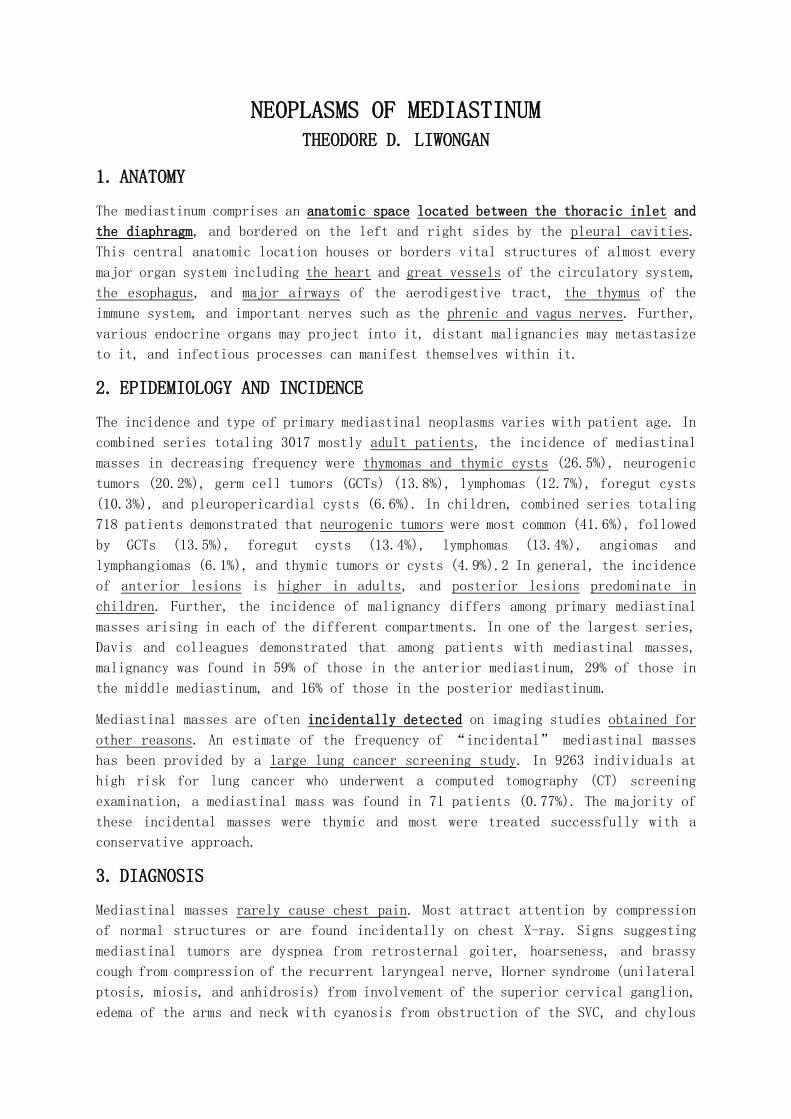
4. ANTERIOR MEDIASTINUM TUMORS 4.1. THYMOMA
4.1.1. PATHOLOGY
Thymomas are neoplasms of thymic epithelial cells. They almost always
occur in adult life and most (80%) are benign.
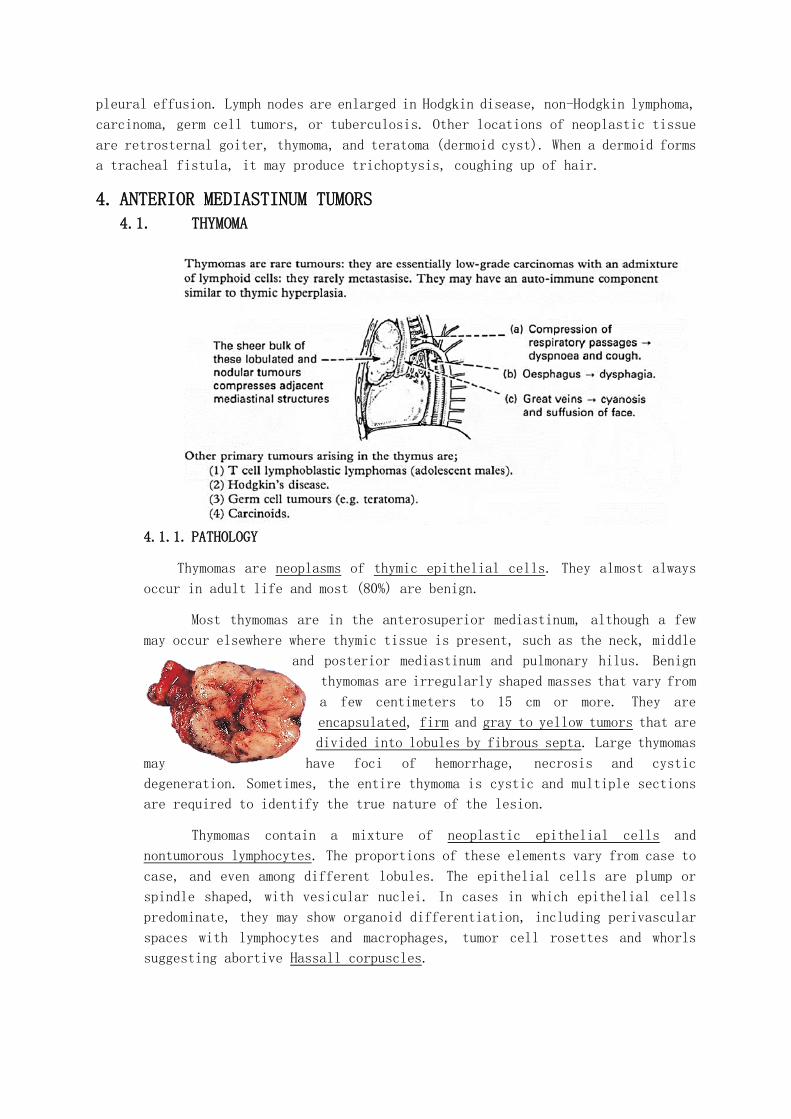
Most thymomas are in the anterosuperior mediastinum, although a few
may occur elsewhere where thymic tissue is present, such as the neck, middle
and posterior mediastinum and pulmonary hilus. Benign
thymomas are irregularly shaped masses that vary from
a few centimeters to 15 cm or more. They are
encapsulated, firm and gray to yellow tumors that are
divided into lobules by fibrous septa. Large thymomas
may have foci of hemorrhage, necrosis and cystic
degeneration. Sometimes, the entire thymoma is cystic and multiple sections
are required to identify the true nature of the lesion.
Thymomas contain a mixture of neoplastic epithelial cells and
nontumorous lymphocytes. The proportions of these elements vary from case to
case, and even among different lobules. The epithelial cells are plump or
spindle shaped, with vesicular nuclei. In cases in which epithelial cells
predominate, they may show organoid differentiation, including perivascular
spaces with lymphocytes and macrophages, tumor cell rosettes and whorls
suggesting abortive Hassall corpuscles.

MALIGNANT THYMOMAS INVADE LOCALLY AND MAY METASTASIZE. One fourth of
thymomas are not encapsulated and show malignant features.
Type I malignant thymoma is the most common cancer of the thymus, and
is virtually indistinguishable histologically from encapsulated, benign
thymomas. However, it penetrates the capsule, implants on pleural or
pericardial surfaces and metastasizes to lymph nodes, lung, liver and bone.
Type II malignant thymoma is a very uncommon invasive tumor, also
called thymic carcinoma. Its morphology is highly variable and it resembles
squamous carcinomas, lymphoepithelioma-like carcinomas (identical to those
in the oropharynx), sarcomatoid variants (carcinosarcoma) and other rare
patterns. These variants share a distinct epithelial appearance and a
mediastinal tumor that lacks this feature is probably not thymic carcinoma.
4.1.2. CLINICAL PRESENTATION AND DIFFERENTIAL DIAGNOSIS
Carcinoid tumors, lipomas, and thymic cysts also may
produce radiographic masses. After combination
chemotherapy for another malignancy, teenagers and
young adults may develop a rebound thymic
hyperplasia in the first few months after treatment.
Granulomatous inflammatory diseases (tuberculosis,
sarcoidosis) can produce thymic enlargement.
Thymomas are most common in the fifth and sixth
decades, are uncommon in children, and are
distributed evenly between men and women.
About 40–50% of patients are asymptomatic; masses are detected
incidentally on routine chest radiographs. When symptomatic, patients
may have cough, chest pain, dyspnea, fever, wheezing, fatigue, weight
loss, night sweats, or anorexia. Occasionally, thymomas may obstruct the
superior vena cava. Pericardial effusion may be present. About 40% of
patients with thymoma have another systemic autoimmune illness related
to the thymoma. About 30% of patients with thymoma have myasthenia gravis,
5–8% have pure red cell aplasia, and ~5% have hypogammaglobulinemia.
Thymoma with hypogammaglobulinemia also is called Good’s syndrome.
Among patients with myasthenia gravis, ~10–15% have a thymoma. Thymoma
more rarely may be associated with polymyositis, systemic lupus
erythematosus, thyroiditis, Sjögren’s syndrome, ulcerative colitis,
pernicious anemia, Addison’s disease, stiff person syndrome,
scleroderma, and panhypopituitarism. In one series, 70% of patients with
thymoma were found to have another systemic illness.
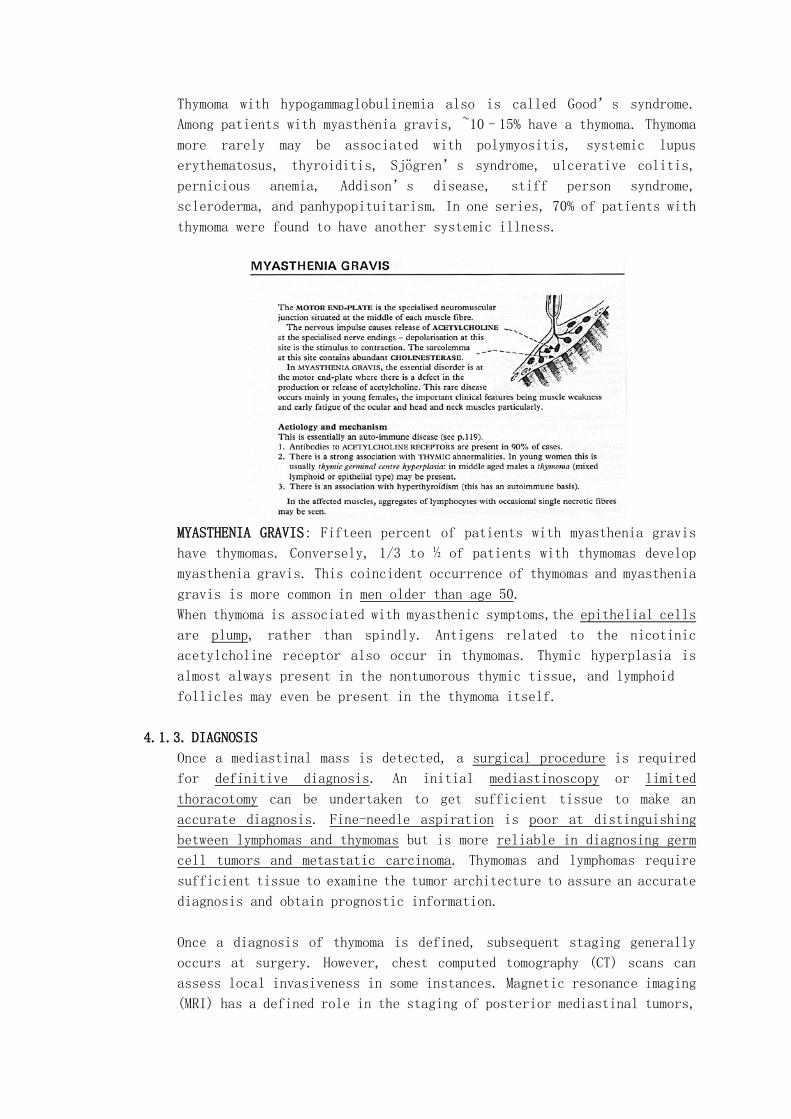
MYASTHENIA GRAVIS: Fifteen percent of patients with myasthenia gravis
have thymomas. Conversely, 1/3 to ½ of patients with thymomas develop
myasthenia gravis. This coincident occurrence of thymomas and myasthenia
gravis is more common in men older than age 50.
When thymoma is associated with myasthenic symptoms,the epithelial cells
are plump, rather than spindly. Antigens related to the nicotinic
acetylcholine receptor also occur in thymomas. Thymic hyperplasia is
almost always present in the nontumorous thymic tissue, and lymphoid
follicles may even be present in the thymoma itself.
4.1.3. DIAGNOSIS
Once a mediastinal mass is detected, a surgical procedure is required
for definitive diagnosis. An initial mediastinoscopy or limited
thoracotomy can be undertaken to get sufficient tissue to make an
accurate diagnosis. Fine-needle aspiration is poor at distinguishing
between lymphomas and thymomas but is more reliable in diagnosing germ
cell tumors and metastatic carcinoma. Thymomas and lymphomas require
sufficient tissue to examine the tumor architecture to assure an accurate
diagnosis and obtain prognostic information.
Once a diagnosis of thymoma is defined, subsequent staging generally
occurs at surgery. However, chest computed tomography (CT) scans can
assess local invasiveness in some instances. Magnetic resonance imaging
(MRI) has a defined role in the staging of posterior mediastinal tumors,
but it is not clear that it adds important information to the CT scan
in anterior mediastinal tumors. Somatostatin receptor imaging with
indium-labeled somatostatin analogues may be of value. If invasion is
not distinguished by noninvasive testing, an effort to resect the entire
tumor should be undertaken. If invasion is present, neoadjuvant
chemotherapy may be warranted before surgery.
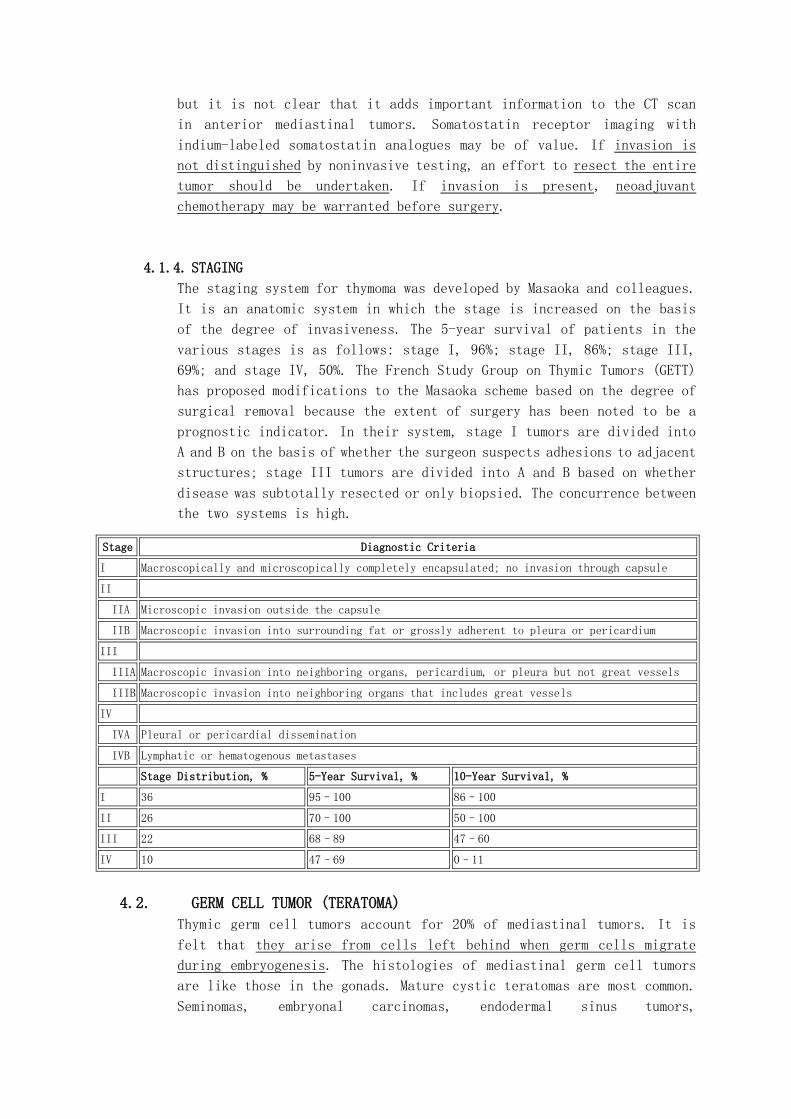
4.1.4. STAGING
The staging system for thymoma was developed by Masaoka and colleagues.
It is an anatomic system in which the stage is increased on the basis
of the degree of invasiveness. The 5-year survival of patients in the
various stages is as follows: stage I, 96%; stage II, 86%; stage III,
69%; and stage IV, 50%. The French Study Group on Thymic Tumors (GETT)
has proposed modifications to the Masaoka scheme based on the degree of
surgical removal because the extent of surgery has been noted to be a
prognostic indicator. In their system, stage I tumors are divided into
A and B on the basis of whether the surgeon suspects adhesions to adjacent
structures; stage III tumors are divided into A and B based on whether
disease was subtotally resected or only biopsied. The concurrence between
the two systems is high.
Stage Diagnostic Criteria
I Macroscopically and microscopically completely encapsulated; no invasion through capsule
II
IIA Microscopic invasion outside the capsule
IIB Macroscopic invasion into surrounding fat or grossly adherent to pleura or pericardium
III
IIIA Macroscopic invasion into neighboring organs, pericardium, or pleura but not great vessels
IIIB Macroscopic invasion into neighboring organs that includes great vessels
IV
IVA Pleural or pericardial dissemination
IVB Lymphatic or hematogenous metastases
Stage Distribution, % 5-Year Survival, % 10-Year Survival, %
I 36 95–100 86–100
II 26 70–100 50–100
III 22 68–89 47–60
IV 10 47–69 0–11
4.2. GERM CELL TUMOR (TERATOMA)
Thymic germ cell tumors account for 20% of mediastinal tumors. It is
felt that they arise from cells left behind when germ cells migrate
during embryogenesis. The histologies of mediastinal germ cell tumors
are like those in the gonads. Mature cystic teratomas are most common.
Seminomas, embryonal carcinomas, endodermal sinus tumors,
teratocarcinomas, immature teratomas and choriocarcinomas all occur.
Mixed germ cell histologies are common. Mediastinal germ cell tumors may
on occasion show somatic-type malignant components of sarcoma, carcinoma
or hematologic malignancies. Save for mature cystic teratoma, which
affects both sexes equally, the other tumors occur mostly in males.
Thymic seminomas arise only in men. Prognosis is like that for comparable
gonadal tumors, although mediastinal nonseminomatous germ cell tumors
are more aggressive. Other lesions include benign and malignant stromal
tumors. Thymolipomas are benign, well-circumscribed masses of mature
adipose tissue and unremarkable thymic parenchyma. Thymic stromal
sarcomas are low-grade malignant mesenchymal tumors with variable
morphology, but frequently of a liposarcomatous nature. Nonneoplastic
masses include thymic, mesothelial and enteric-type cysts.
4.3. LIMFOMA MALIGNUM
Lymphomas are malignant proliferations of lymphocytes. B-cell, T-cell and
NK-cell lymphomas may be immature (derived from precursor cells; lymphoblasts)
or mature (derived from mature effector cells). The latter are more common.
While all lymphomas are malignant, they show a wide spectrum of clinical
behavior: some follow an indolent clinical course (and may not even require
treatment), while others are very aggressive (and can cause death in a short
time, if untreated). Lymphomas mostly affect lymph nodes, but any tissue
or organ may be involved (e.g., GI tract, thyroid, liver, skin, lungs, brain).
If lymphoma cells are present in the peripheral blood and/or bone marrow,
the tumor is “leukemic” or “peripheralized.” Beyond the broad categories
of B-cell, T-cell and NKcell types, lymphomas are further classified by
their postulated cells of origin, normal cellular counterparts,
immunophenotypes, molecular/genetic alterations, clinical features and
morphology. Further, Hodgkin lymphomas (HLs) are classified separately from
non-Hodgkin lymphomas (NHLs). The WHO classification of lymphoid tumors takes
all of these parameters into account and is currently used by pathologists
and clinicians alike.
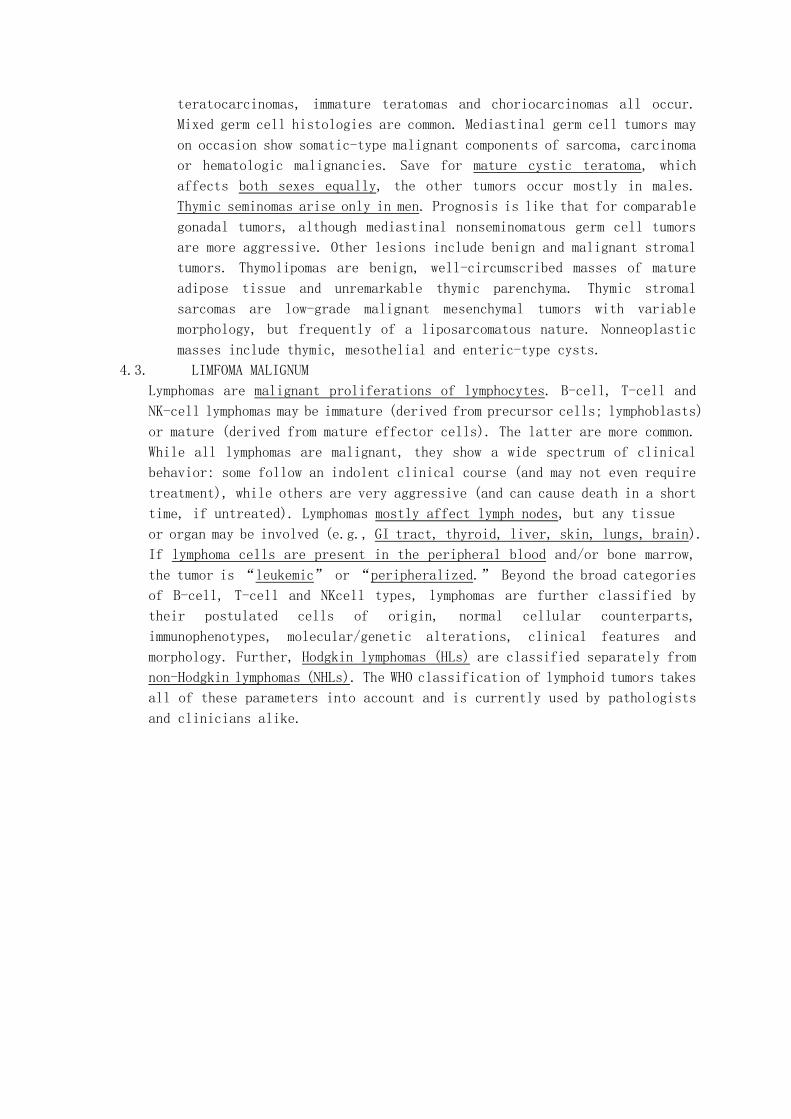
5. POSTERIOR MEDIASTINUM TUMORS (NEUROGENIC TUMORS)
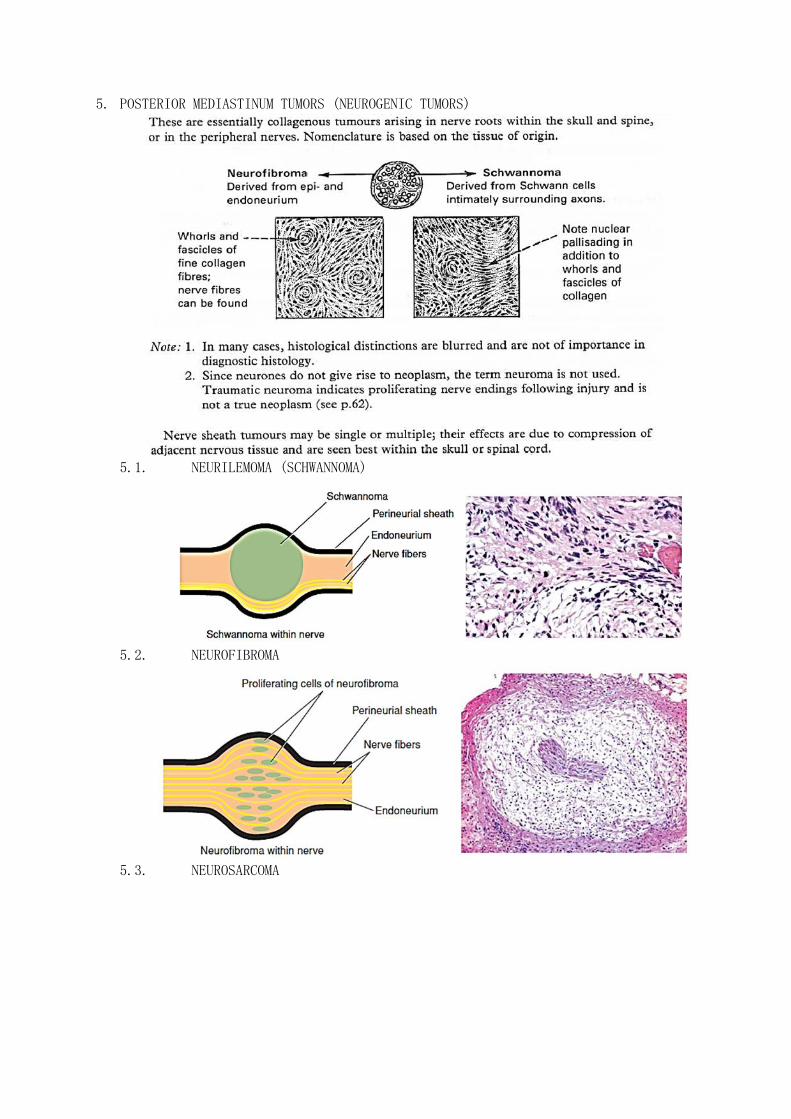
5.1. NEURILEMOMA (SCHWANNOMA)
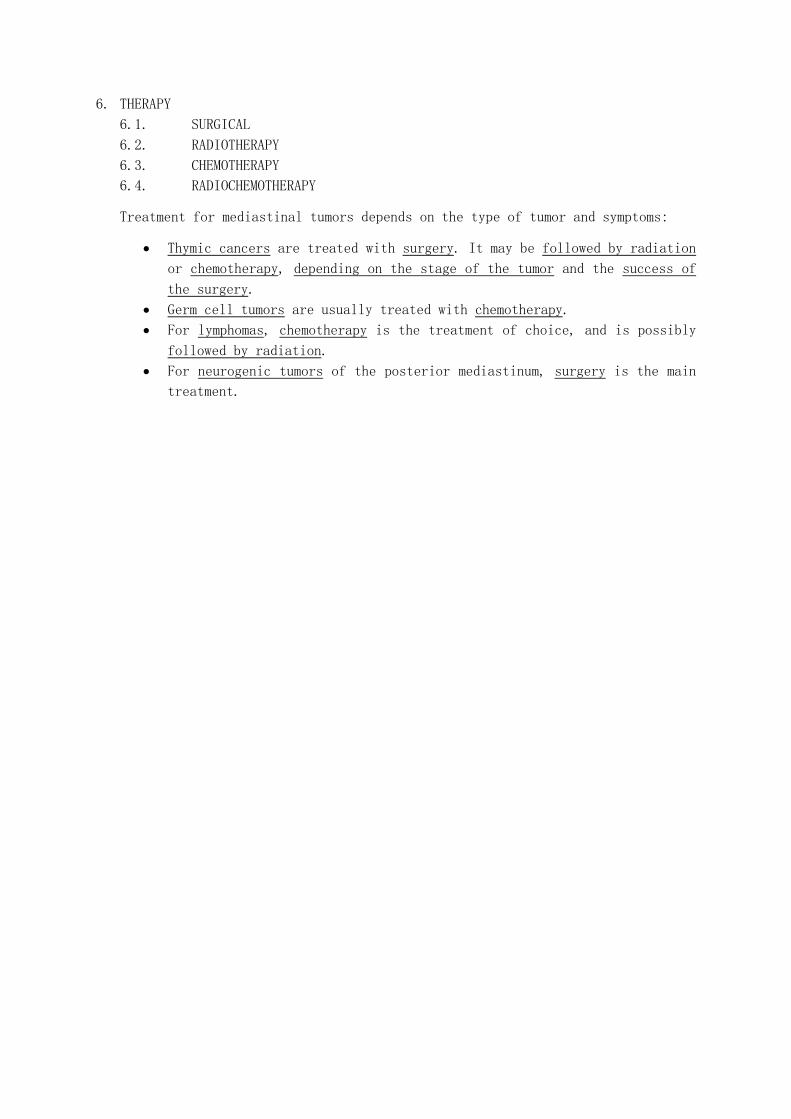
5.2. NEUROFIBROMA
5.3. NEUROSARCOMA
6. THERAPY
6.1. SURGICAL
6.2. RADIOTHERAPY
6.3. CHEMOTHERAPY
6.4. RADIOCHEMOTHERAPY
Treatment for mediastinal tumors depends on the type of tumor and symptoms:
Thymic cancers are treated with surgery. It may be followed by radiation
or chemotherapy, depending on the stage of the tumor and the success of
the surgery.
Germ cell tumors are usually treated with chemotherapy.
For lymphomas, chemotherapy is the treatment of choice, and is possibly
followed by radiation.
For neurogenic tumors of the posterior mediastinum, surgery is the main
treatment.
ATTACHMENT
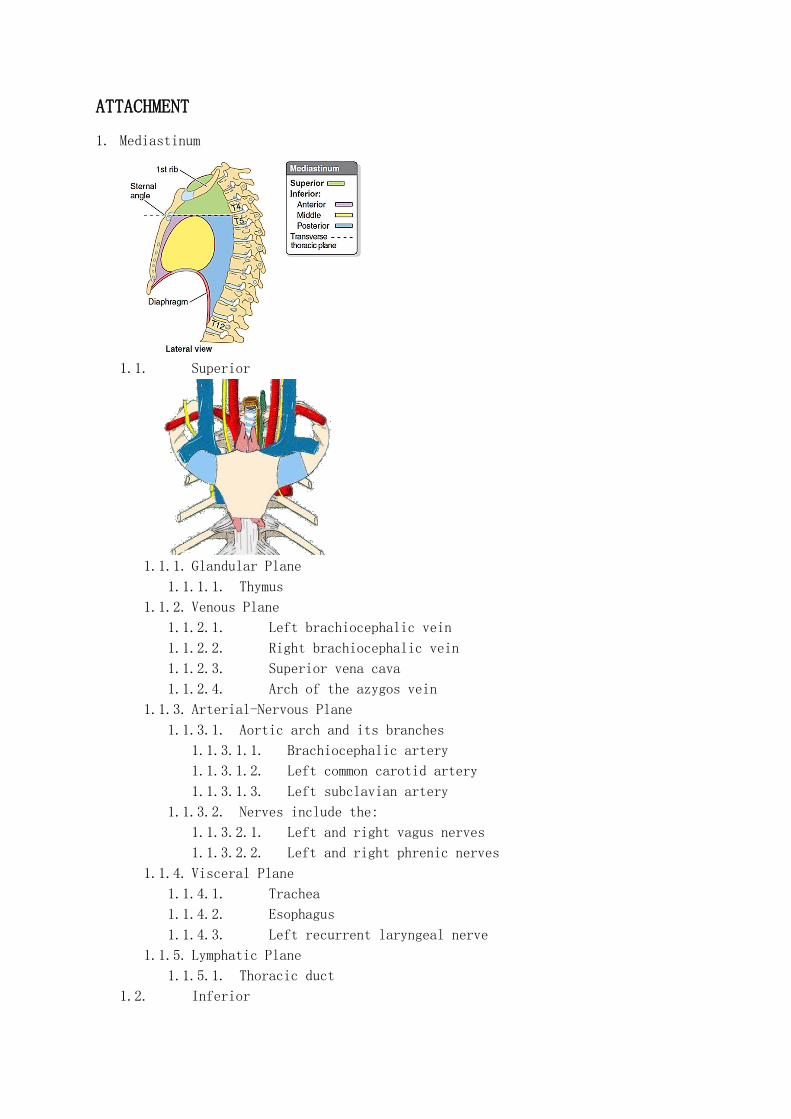
1. Mediastinum
1.1. Superior
1.1.1. Glandular Plane
1.1.1.1. Thymus
1.1.2. Venous Plane
1.1.2.1. Left brachiocephalic vein
1.1.2.2. Right brachiocephalic vein
1.1.2.3. Superior vena cava
1.1.2.4. Arch of the azygos vein
1.1.3. Arterial-Nervous Plane
1.1.3.1. Aortic arch and its branches
1.1.3.1.1. Brachiocephalic artery
1.1.3.1.2. Left common carotid artery
1.1.3.1.3. Left subclavian artery
1.1.3.2. Nerves include the:
1.1.3.2.1. Left and right vagus nerves
1.1.3.2.2. Left and right phrenic nerves
1.1.4. Visceral Plane
1.1.4.1. Trachea
1.1.4.2. Esophagus
1.1.4.3. Left recurrent laryngeal nerve
1.1.5. Lymphatic Plane
1.1.5.1. Thoracic duct
1.2. Inferior

1.2.1. Anterior
1.2.1.1. Loose areolar tissue
1.2.1.2. Lymphatic vessels which ascend from the convex surface of the
liver
1.2.1.3. Two or three anterior mediastinal lymph nodes
1.2.1.4. The small mediastinal branches of the internal thoracic artery
1.2.1.5. Thymus (involuted in adults)
1.2.2. Media
1.2.2.1. Pericardium
1.2.2.2. Heart
1.2.3. Posterior
1.2.3.1. Artery
1.2.3.1.1. Thoracic part of the descending aorta
1.2.3.2. Veins
1.2.3.2.1. Azygos vein
1.2.3.2.2. The hemiazygos vein and the accessory hemiazygos vein
1.2.3.3. Nerves
1.2.3.3.1. Vagus nerve
1.2.3.3.2. Splanchnic nerves
1.2.3.3.3. Sympathetic chain
1.2.3.4. Esophagus
1.2.3.5. Thoracic duct
1.2.3.6. Some lymph glands
Structures Common Lesions Rare Lesions
Anterior compartment
Thymus Thymomas Thymic carcinoma; benign thymic tumors
Fat and lymphatics Lymphomas Vascular lesions
Internal mammary vessels Germ cell tumors
(teratoma) Mesenchymal tumors
Thyroid (occasional) Endocrine tumors (e.g., ectopic
parathyroid, goiter)
Castleman’s disease
Middle compartment
Heart Foregut cysts Pleural and pericardial cysts
Pericardium Lymphoma Castleman disease
Aorta
Superior and inferior
vena cava
Trachea and main bronchi
Lymph nodes
Posterior compartment
Descending aorta Nerve sheath tumors Vascular tumors
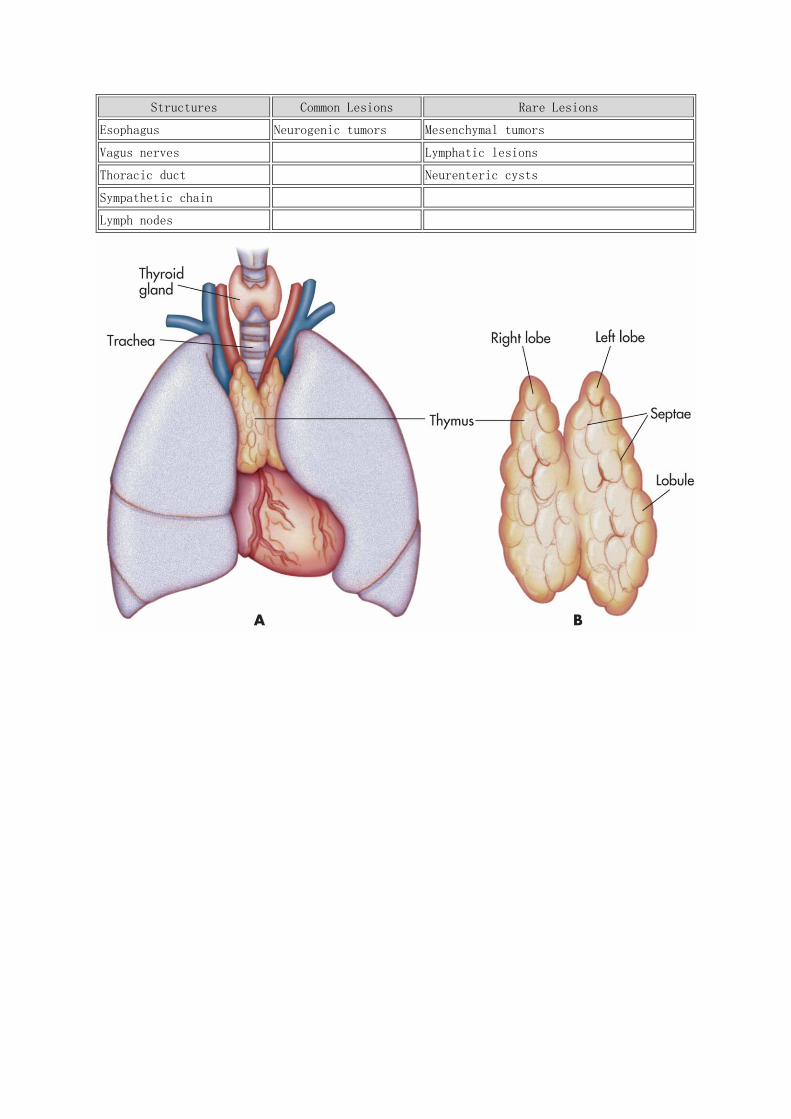
Structures Common Lesions Rare Lesions
Esophagus Neurogenic tumors Mesenchymal tumors
Vagus nerves Lymphatic lesions
Thoracic duct Neurenteric cysts
Sympathetic chain
Lymph nodes
Resources:
LeBlond RF, Brown DD, Suneja M, Szot JF. The Chest: Chest Wall, Pulmonary, and
Cardiovascular Systems; The Breasts. In: LeBlond RF, Brown DD, Suneja M, Szot JF.
eds. DeGowin’s Diagnostic Examination, 10e. New York, NY: McGraw-Hill; 2015
Burt BM, Shrager JB. Benign and Malignant Neoplasms of the Mediastinum. In: Grippi
MA, Elias JA, Fishman JA, Kotloff RM, Pack AI, Senior RM, Siegel MD. eds.
Fishman's Pulmonary Diseases and Disorders, Fifth Edition. New York, NY: McGraw-
Hill; 2015
Essential Clinical Anatomy 5th ed Moore
Colour Atlas of Anatomical Pathology Robin A. Cooke, Brian Stewart
Rubin’s Pathology
Pathology Illustrated
http://www.wesnorman.com/thoraxlesson5.htm
https://www.nlm.nih.gov/medlineplus/ency/article/001086.htm
Related Documents











