TREATMENT TREATMENT RECOMMENDATIONS RECOMMENDATIONS FOR MANAGING THE POST FOR MANAGING THE POST STROKE UPPER LIMB STROKE UPPER LIMB 7 YEARS LATER: HAS ANYTHING CHANGED? Susan Barreca, MSc. PT [email protected]

TREATMENT RECOMMENDATIONS FOR MANAGING THE POST STROKE UPPER LIMB 7 YEARS LATER: HAS ANYTHING CHANGED? Susan Barreca, MSc. PT [email protected].
Dec 28, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

TREATMENT TREATMENT RECOMMENDATIONS RECOMMENDATIONS
FOR MANAGING THE POST FOR MANAGING THE POST STROKE UPPER LIMBSTROKE UPPER LIMB
7 YEARS LATER:
HAS ANYTHING CHANGED?Susan Barreca, MSc. PT

Focus of today’s talkFocus of today’s talk
Examine the uptake of the treatment recommendations of the 2001 Consensus Panel by revisiting the same questions:
What is the most effective way for individuals to regain function in their paretic upper limb? Who benefits most?
Discuss the controversy around the Panel’s premises that there should be different treatment goals for individuals whose arms and hands are at varying levels of motor impairment
Consensus panel membersConsensus panel membersFunded by Ministry of Health and Long-Term Care of Funded by Ministry of Health and Long-Term Care of Ontario & Heart and Stroke Foundation of OntarioOntario & Heart and Stroke Foundation of Ontario
Panel Members Dr. Steve Wolf Dr. Richard Bohannon Dr. Susan Fasoli Prof. Ann Charness Dr. Vlasta Hajek Prof. Kelley Gowland Maria Huijbregts Jeremy Griffiths
ModeratorMary Ann O’Brien
MethodologistDr. Andy Willan

Consensus exercise Consensus exercise processprocess
Thorough literature review
Conducted series of meta-analyses
Developed 6 common clinical scenarios
Used Chedoke McMaster Stages
Sackett’s level of evidence (1-IV)
Formulated treatment recommendations
Panel voted independently by e-mail
Recommendations underwent external review
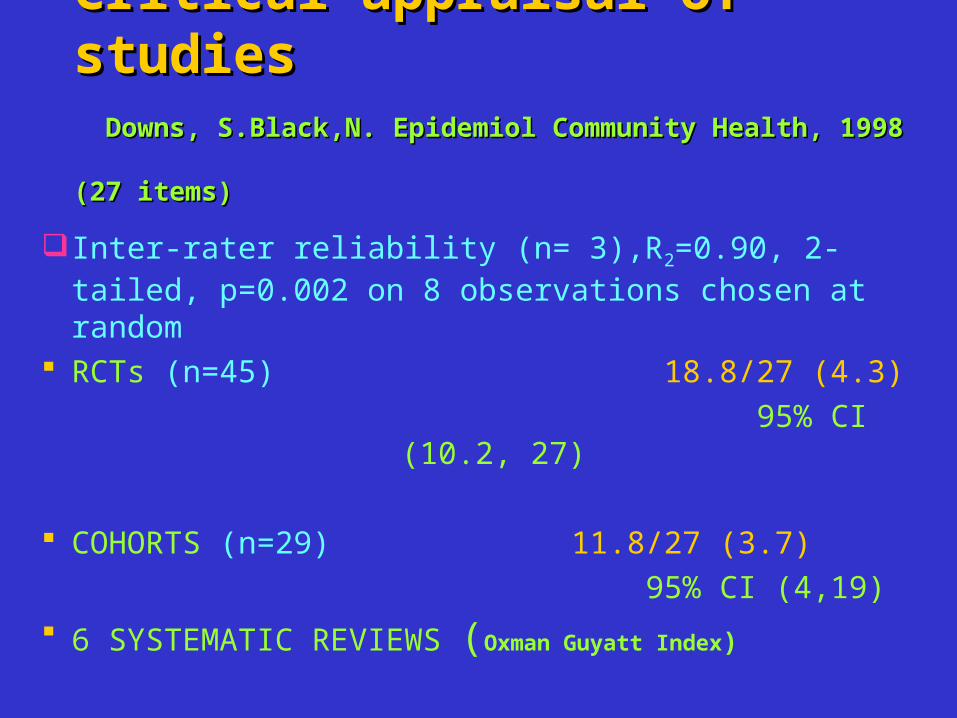
Critical appraisal of studiesCritical appraisal of studies Downs, S.Black,N. Epidemiol Community Health, 1998 Downs, S.Black,N. Epidemiol Community Health, 1998
(27 items)(27 items)
Inter-rater reliability (n= 3),R2=0.90, 2-tailed, p=0.002 on 8 observations chosen at random
RCTs (n=45) 18.8/27 (4.3)
95% CI (10.2, 27)
COHORTS (n=29) 11.8/27 (3.7)
95% CI (4,19)
6 SYSTEMATIC REVIEWS (Oxman Guyatt Index)
Evaluation of Consensus Evaluation of Consensus ExerciseExercise
Scored 80% by independent SCORE reviewers using AGREE
Awarded highest standards of excellence by Physiotherapy Evidence Based Database (PedRO) http://www.pedrp.fhs.usyd.edu/index.htl
Placed on the CMA Infobase Web http://mdm.ca/cpgs/search/english/results.asp
Supported by Ottawa Panel Evidence Based Clinical Practice Guidelines (Topics in Stroke Rehab, 2006)
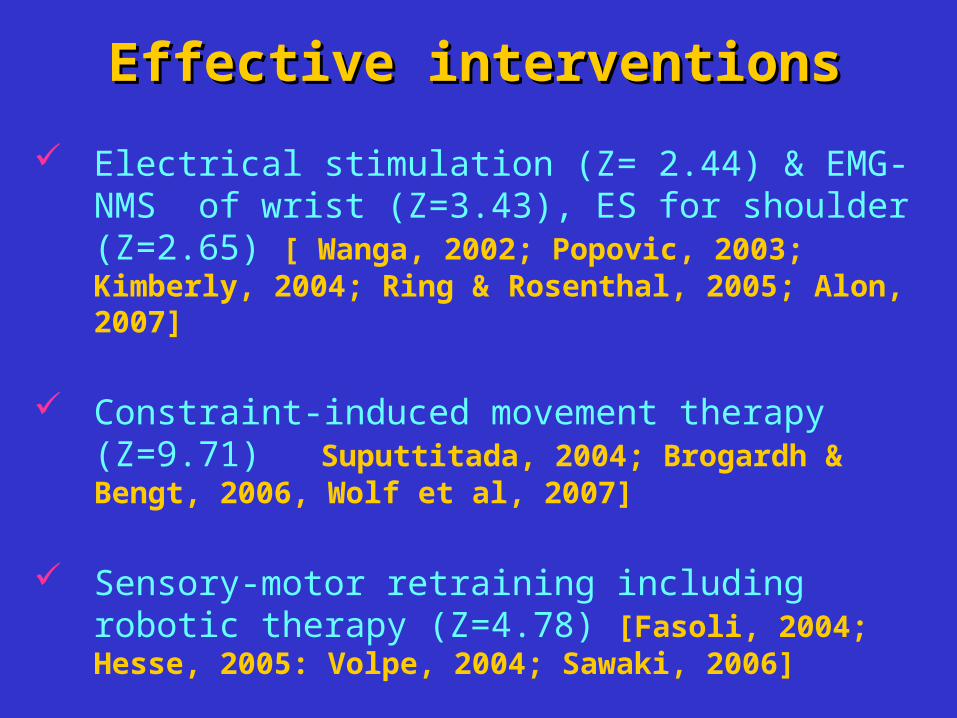
Effective interventionsEffective interventions
Electrical stimulation (Z= 2.44) & EMG-NMS of wrist (Z=3.43), ES for shoulder (Z=2.65) [ Wanga, 2002; Popovic, 2003; Kimberly, 2004; Ring & Rosenthal, 2005; Alon, 2007]
Constraint-induced movement therapy (Z=9.71) Suputtitada, 2004; Brogardh & Bengt, 2006, Wolf et al, 2007]
Sensory-motor retraining including robotic therapy (Z=4.78) [Fasoli, 2004; Hesse, 2005: Volpe, 2004; Sawaki, 2006]

Effective interventionsEffective interventions
Home exercises over no treatment (Home exercises over no treatment (Z=2.22)
Movement+elevation for hand edema (Z=3.2)
Shoulder strapping decreasing pain (Z=6.11)
OT + imagery (Z=3.34) [Dijkerman, 2004, Lui, 2005]
Repetitive training (Z=2.07): [French, 2007 appears unsupported]
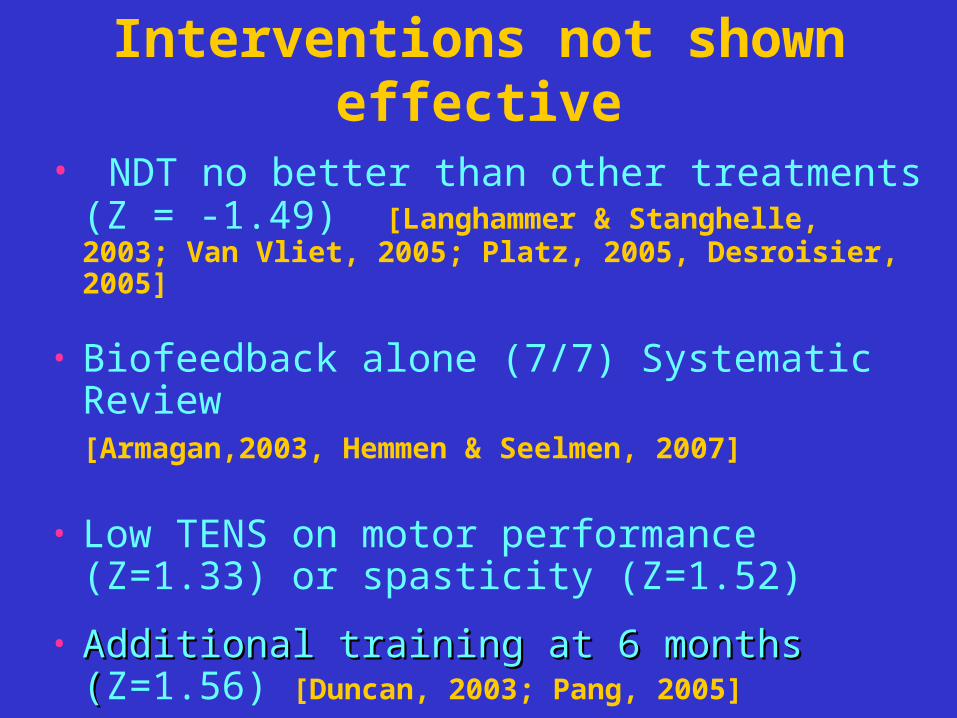
• NDT no better than other treatments (Z = -1.49) [Langhammer & Stanghelle, 2003; Van Vliet, 2005; Platz, 2005, Desroisier, 2005]
• Biofeedback alone (7/7) Systematic Review [Armagan,2003, Hemmen & Seelmen, 2007]
• Low TENS on motor performance (Z=1.33) or spasticity (Z=1.52)
• Additional training at 6 months (Additional training at 6 months (Z=1.56) [Duncan, 2003; Pang, 2005]
Interventions not shown effective
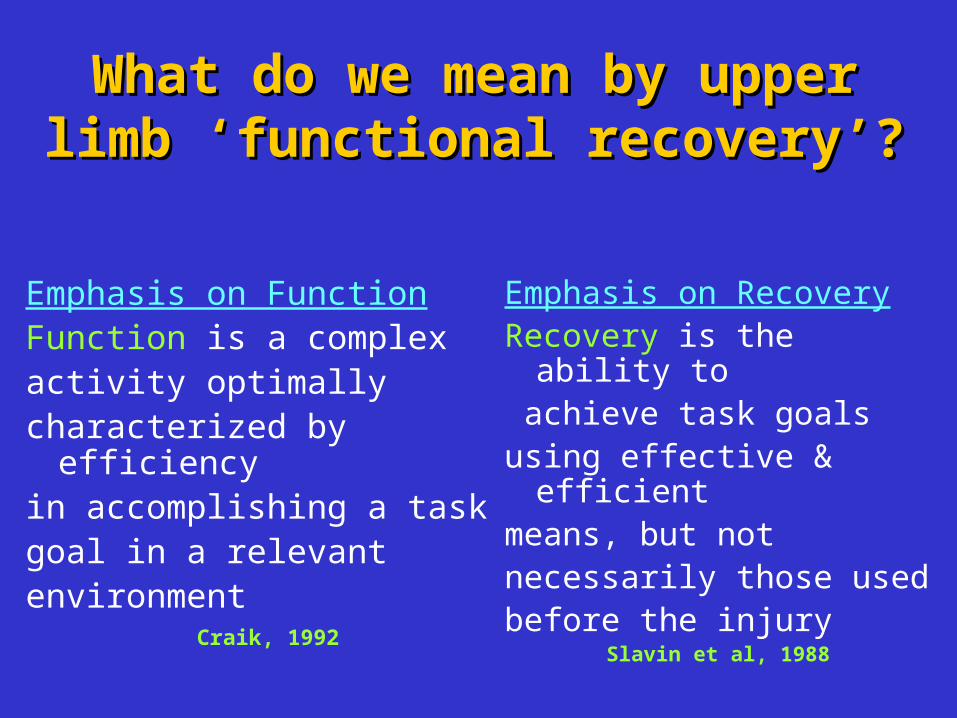
What do we mean by upper What do we mean by upper limb ‘functional recovery’?limb ‘functional recovery’?
Emphasis on FunctionFunction is a complex activity optimallycharacterized by efficiencyin accomplishing a taskgoal in a relevant environment
Craik, 1992
Emphasis on RecoveryRecovery is the ability to achieve task goals using effective & efficient means, but not necessarily those used before the injury
Slavin et al, 1988

Premise1:Therapeutic goals Premise1:Therapeutic goals for the arm & hand Stage 4 for the arm & hand Stage 4 or higheror higherProvide every opportunity to reduce motor impairment & improve function
Sensory motor training (level 1 evidence)
EMG-NMS or ES of wrist/forearm (level l evidence)
Engage in challenging, repetitive & intense use of novel tasks in order to acquire the necessary motor skills (level I evidence)

PREMISE 2: Therapeutic goals for the arm & hand < Stage 3
Maintain a comfortable, pain-free, mobile arm & handproper positioning, support (AHCPR), careful
handling (level IV evidence) teaching the client to perform self-ranging (Expert
Opinion)avoid overhead pulleys (level 11 evidence)ES (Level I evidence) may reduce shoulder
subluxation in the short term (mean 5 wks)
Maximize recovery using compensatory & environmental adaptations

Definition of upper limb Definition of upper limb functionfunction
The arm & hand moves as
an integrated unit in various
directions to stabilize, reach,
grasp & manipulate objects of
various sizes & weights repeatedly (Barreca et al, 2004)
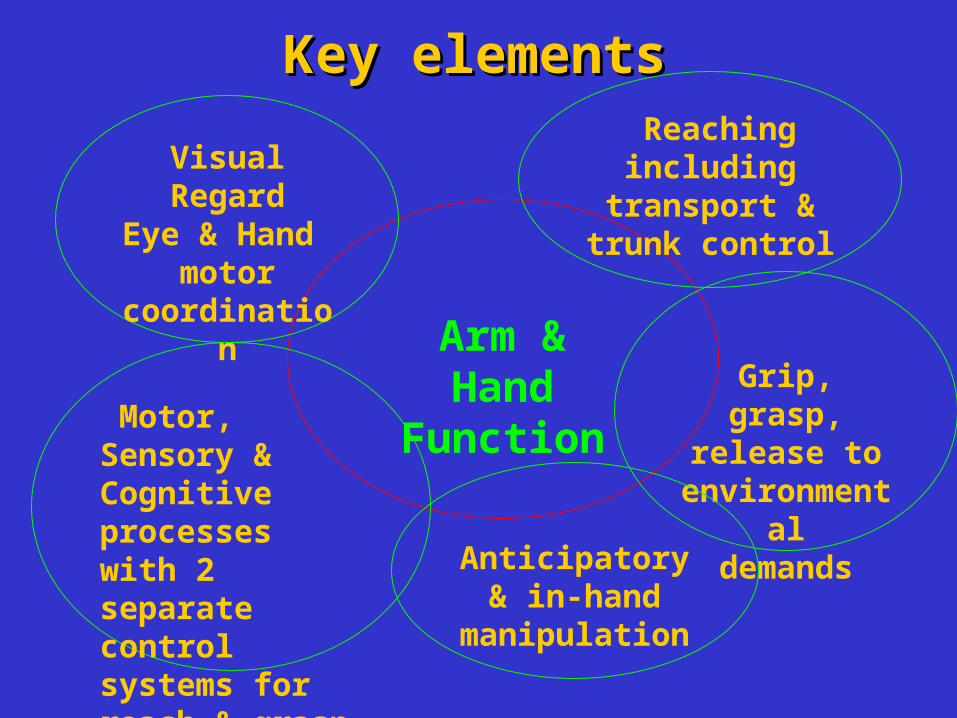
Key elementsKey elements
Arm & Hand Function
Reaching including
transport & trunk control
Visual RegardEye & Hand
motor coordination
Grip, grasp, release to
environmentaldemands
Motor, Sensory & Cognitiveprocesses with 2 separate controlsystems for reach & grasp
Anticipatory & in-hand
manipulation

Since our recommendationsSince our recommendations Positive response but many clinicians still practice
only NDT, unfamiliar with FES, EMG- FES, have difficulty managing shoulder pain, experience time restraints (SCORE addressing these issues)
Upper limb research still hot but since 2001…..
Twice as many studies conducted during chronic phase post stroke vs. subacute stage
50% of studies examined new interventions not readily translated into our current inpatient rehabilitation practice, e.g. CIT, robotics, virtual reality
Why different remedial Why different remedial goals for the arm & hand goals for the arm & hand Stage 3 or less may not be Stage 3 or less may not be readily acceptedreadily accepted
Personal values An individual’s confidence in the findings French versus Utilitarian philosophical approach
(equality vs. greatest good for the greatest number)
Professional values

Professional valuesProfessional values
Inherent flexibility and adaptability of neural system to respond to many factors
Lack of task specific intensive training to utilize alternative cortical pathways
Validity of predicting outcomes in the arm & hand
Changes in persons whose upper limb is labeled severe or chronic
ResponseResponse
Motor learning texts For task orientated training, clients need
some hand muscle activity Carr & Shepherd, 2003; Shumway-Wollacutt & Cook, 2005
Recent task specific training studies Cochrane review showed statistical
significance for task specific training for the lower extremity, not the upper limb (French, 2007)
ResponseResponse
Relationship of U/L sensory motor impairments to activity
U/L strength isometrics of shoulder, elbow,
wrist, grip (n=93) explained 87% variance of CAHAI, a measure of functional arm & hand performance (Harris & Eng, 2007)
Active ROM & isometric force production were the most common predictors of reaching during first 3 months post stroke (Wagner et al, 2007)
ResponseResponse
VECTORS: Phase II trial: CIT x 2 hrs, 6 hrs.
constraint vs. CIT, 3 hrs. 90% constraint, 9.4 days
post-stroke, 22.5 on ARAT: high intensity had worse scores Dromerick, 2007
Enhanced Exercise: Only those with moderateimpairments improved Duncan, 2004; Winstein, 2004; Pang,
2006 (n=92, 64, 63 respectively)
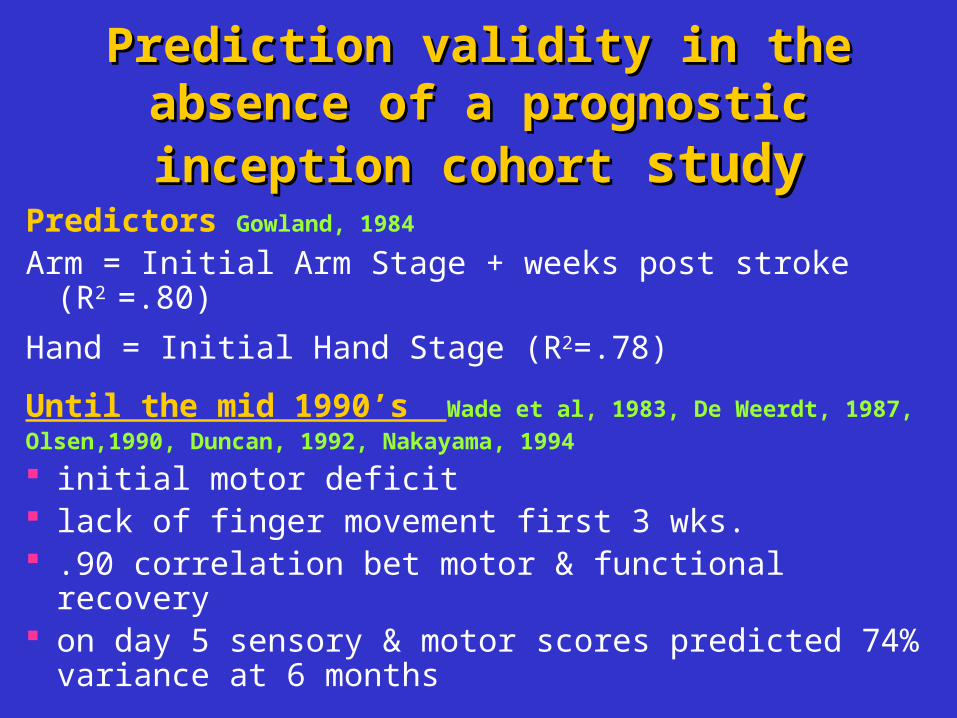
Prediction validity in the Prediction validity in the absence of a prognostic absence of a prognostic inception cohortinception cohort study study
Predictors Gowland, 1984
Arm = Initial Arm Stage + weeks post stroke (R2 =.80)
Hand = Initial Hand Stage (R2=.78)
Until the mid 1990’s Wade et al, 1983, De Weerdt, 1987,
Olsen,1990, Duncan, 1992, Nakayama, 1994
initial motor deficit lack of finger movement first 3 wks. .90 correlation bet motor & functional recovery on day 5 sensory & motor scores predicted 74%
variance at 6 months
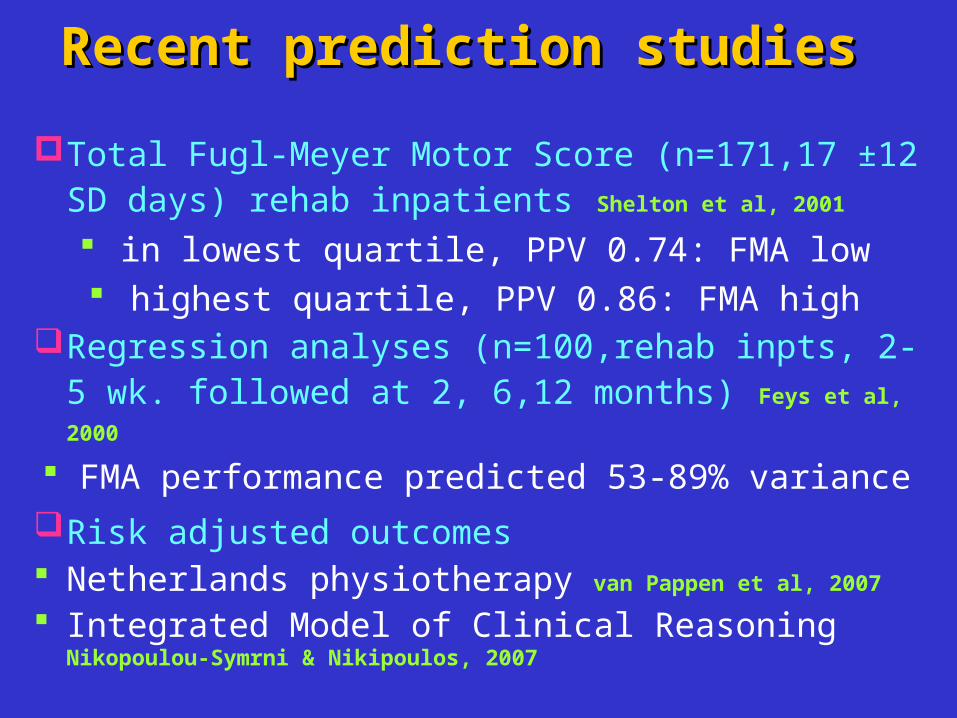
Recent prediction studies Recent prediction studies
Total Fugl-Meyer Motor Score (n=171,17 ±12 SD days) rehab inpatients Shelton et al, 2001
in lowest quartile, PPV 0.74: FMA low highest quartile, PPV 0.86: FMA high
Regression analyses (n=100,rehab inpts, 2-5 wk. followed at 2, 6,12 months) Feys et al, 2000
FMA performance predicted 53-89% variance
Risk adjusted outcomes Netherlands physiotherapy van Pappen et al, 2007
Integrated Model of Clinical Reasoning Nikopoulou-Symrni & Nikipoulos, 2007
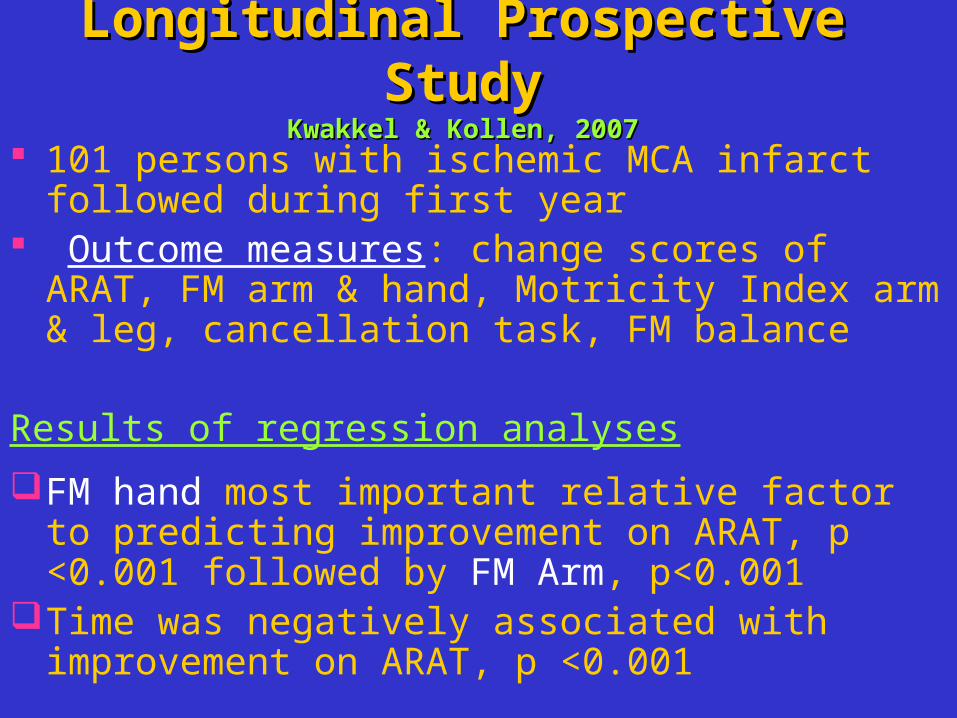
Longitudinal Prospective Longitudinal Prospective StudyStudy
Kwakkel & Kollen, 2007Kwakkel & Kollen, 2007 101 persons with ischemic MCA infarct followed
during first year Outcome measures: change scores of ARAT, FM arm
& hand, Motricity Index arm & leg, cancellation task, FM balance
Results of regression analyses
FM hand most important relative factor to predicting improvement on ARAT, p <0.001 followed by FM Arm, p<0.001
Time was negatively associated with improvement on ARAT, p <0.001
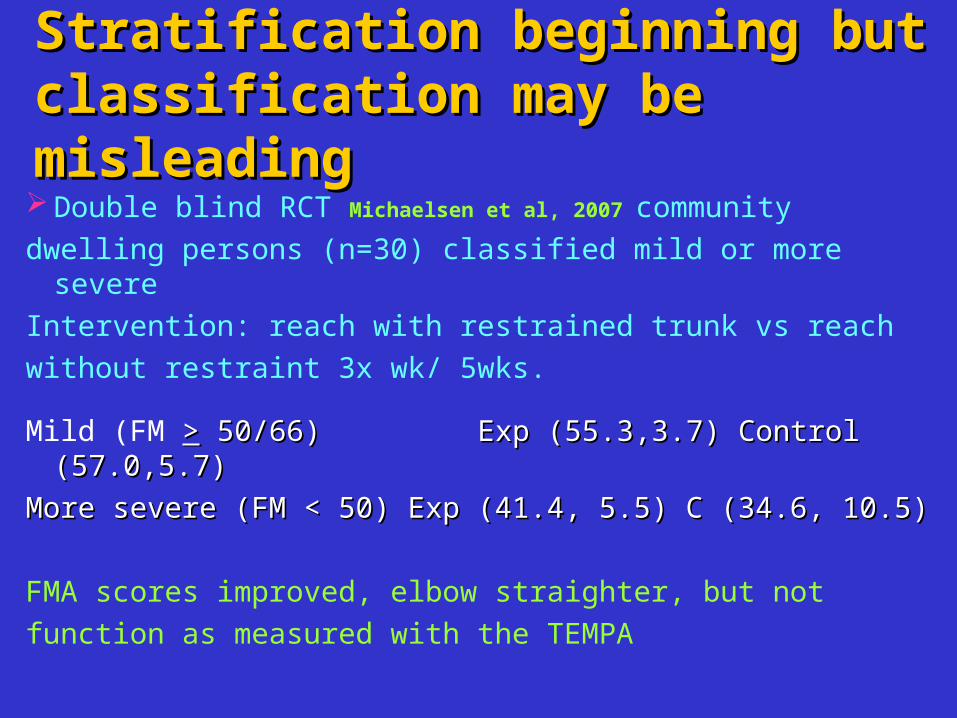
Stratification beginning but Stratification beginning but classification may be classification may be misleadingmisleading Double blind RCT Michaelsen et al, 2007 community
dwelling persons (n=30) classified mild or more severe
Intervention: reach with restrained trunk vs reach
without restraint 3x wk/ 5wks.
Mild (FM >> 50/66) Exp (55.3,3.7) Control (57.0,5.7) 50/66) Exp (55.3,3.7) Control (57.0,5.7)
More severe (FM < 50) Exp (41.4, 5.5) C (34.6, 10.5) More severe (FM < 50) Exp (41.4, 5.5) C (34.6, 10.5)
FMA scores improved, elbow straighter, but not
function as measured with the TEMPA
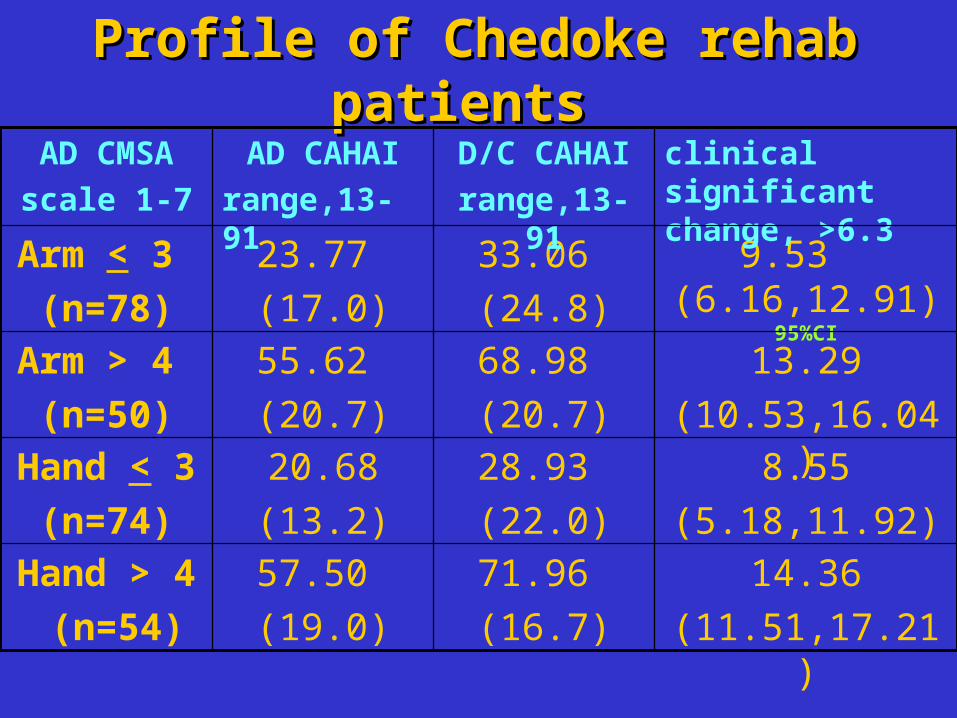
Profile of Chedoke rehab Profile of Chedoke rehab patientspatients
14.36
(11.51,17.21)
71.96
(16.7)
57.50
(19.0)
Hand > 4
(n=54)
8.55
(5.18,11.92)
28.93
(22.0)
20.68
(13.2)
Hand < 3
(n=74)
13.29
(10.53,16.04)
68.98
(20.7)
55.62
(20.7)
Arm > 4
(n=50)
9.53 (6.16,12.91) 95%CI
33.06
(24.8)
23.77
(17.0)
Arm < 3
(n=78)
clinical significant change, >6.3
D/C CAHAI
range,13- 91
AD CAHAI
range,13- 91
AD CMSA
scale 1-7
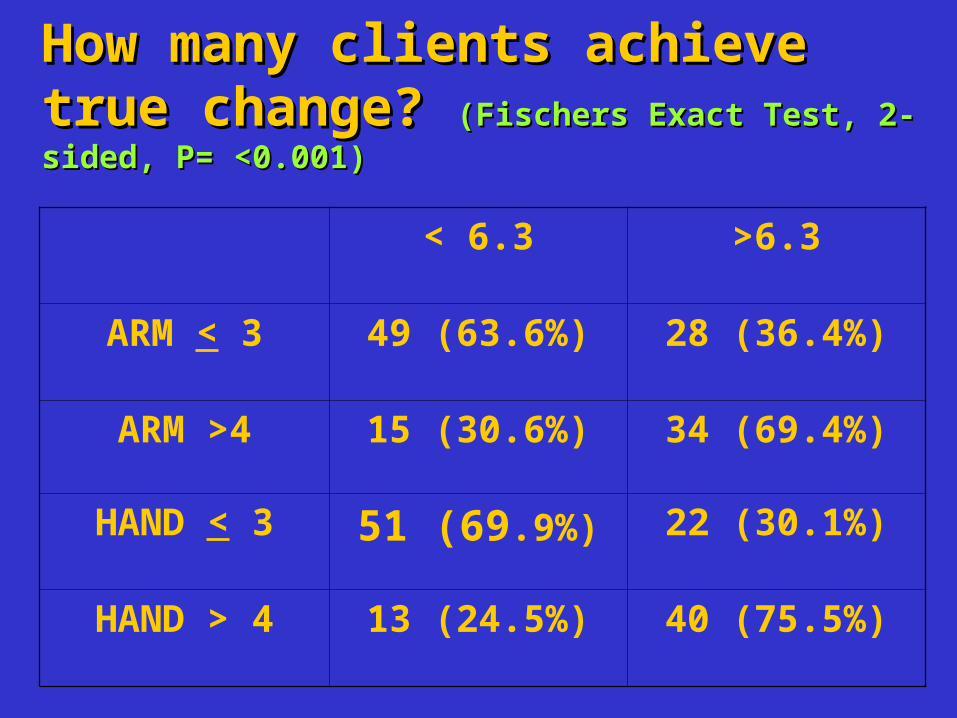
How many clients achieve How many clients achieve true change? true change? (Fischers Exact Test, 2-(Fischers Exact Test, 2-sided, P= <0.001)sided, P= <0.001)
< 6.3 >6.3
ARM < 3 49 (63.6%) 28 (36.4%)
ARM >4 15 (30.6%) 34 (69.4%)
HAND < 3 51 (69.9%) 22 (30.1%)
HAND > 4 13 (24.5%) 40 (75.5%)

Meaningful change? For whom?
Research-Practice Gap (Schuster et al, 1998; Grol, 2001)
30-40% patients do not receive treatments of proven effectiveness
20-25% patients get care that is not needed or potentially harmful
In US, two camps
Altruistic where the individual decides what is
meaningful
Realistic what the healthcare system will bear
Meaningful change? For whom?
Survey of former patients identified 2 major factors in recovering arm & hand function: (i) using their paretic upper limb in daily activities; (ii) not having enough movement to work with Baker, 2007
Need to consider how we help patients adjust to their deficits
“Although hope facilitates positive coping (during
rehab), total denial of possible long term
limitations is a negative strategy during this first
stage of living after stroke” (Sabari, 2001)
This is an exciting time for upper limb research
Many of the 2001 Consensus Panel treatment recommendations have been accepted
Controversy still exists over different therapeutic goals for individuals with differing levels of motor impairments
Defining concepts such as function, recovery, severity, chronicity would help prevent misunderstandings and foster universal research practices
ConcludingConcluding remarks remarks
Related Documents