Transcranial Doppler monitoring during head upright tilt table testing in patients with suspected neurocardiogenic syncope Gasto´nAlbina a, ) , Lucı ´a Fernandez Cisneros b ,Rube´nLain ˜o a , Ulises L. Nobo b , Daniel Ortega a , Elena Schwarz b , Luis Barja a , Roberto Lagos b , Alberto Giniger a , Sebastia ´n F. Ameriso b a Cardiovascular Institute of Buenos Aires (ICBA), Blanco Encalada 1543, (1428) Buenos Aires, Argentina b Institute for Neurological Research (FLENI), Buenos Aires, Argentina Submitted 21 January 2003, and accepted after revision 14 September 2003 – Abstract The aim of the present study was to evaluate the mechanism of cerebro- vascular autoregulation in patients with neurocardiogenic syncope using bilateral transcranial Doppler (TCD) monitoring during head upright tilt table testing (HUT). Two hundred and six patients were prospectively studied. One hundred and fifty-nine subjects (77%) had a prior history of syncope and 47 (23%) had presyncope. Ninety- nine patients (48%) had syncope or presyncope during HUT with a 76% fall in diastolic middle cerebral artery blood flow velocity (D-MCA-BFV). Systolic MCA-BFV (S-MCA- BFV) fell by 33%. Deepening of the dicrotic notch in the Doppler waveform always preceded the fall in D-MCA-BFV. Patients without syncope or presyncope (n ¼ 96) had smaller changes in cerebral blood flow velocities during HUT and only twenty- two subjects had transient deepening of the dicrotic notch. Eleven subjects had pre- syncope during HUT due to an exaggerated response to nitrates with progressive arterial hypotension without bradycardia and changes during TCD monitoring that were intermediate between positive and negative HUT. In conclusion, patients with neurocardiogenic syncope have changes in cere- bral blood flow during the event. TCD monitoring during HUT helps to assess these alterations. ª 2003 Published by Elsevier Ltd on behalf of The European Society of Cardiology. KEYWORDS syncope; head upright tilt table test; transcranial Doppler – Introduction Syncope is a transient loss of consciousness with in- ability to maintain postural tone due to cerebral hypoperfusion. Recovery is typically spontaneous. The most frequent cause of syncope is a dysfunction ) Corresponding author. Tel.: C54-4787-7500; fax: C54-577- 3209. E-mail address: [email protected] (G. Albina). Europace (2004) 6, 63e69 1099-5129/$30 ª 2003 Published by Elsevier Ltd on behalf of The European Society of Cardiology. doi:10.1016/j.eupc.2003.09.009 by guest on August 20, 2016 Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Europace (2004) 6, 63e69
by guest on August 20, 2016
Dow
nloaded from
Transcranial Doppler monitoring during headupright tilt table testing in patients withsuspected neurocardiogenic syncope
Gaston Albinaa,), Lucıa Fernandez Cisnerosb, Ruben Lainoa,Ulises L. Nobob, Daniel Ortegaa, Elena Schwarzb, Luis Barjaa,Roberto Lagosb, Alberto Ginigera, Sebastian F. Amerisob
aCardiovascular Institute of Buenos Aires (ICBA), Blanco Encalada 1543, (1428) Buenos Aires, ArgentinabInstitute for Neurological Research (FLENI), Buenos Aires, Argentina
Submitted 21 January 2003, and accepted after revision 14 September 2003
–––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––
Abstract The aim of the present study was to evaluate the mechanism of cerebro-vascular autoregulation in patients with neurocardiogenic syncope using bilateraltranscranial Doppler (TCD) monitoring during head upright tilt table testing (HUT).Two hundred and six patients were prospectively studied. One hundred and fifty-ninesubjects (77%) had a prior history of syncope and 47 (23%) had presyncope. Ninety-nine patients (48%) had syncope or presyncope during HUTwith a 76% fall in diastolicmiddle cerebral artery blood flow velocity (D-MCA-BFV). Systolic MCA-BFV (S-MCA-BFV) fell by 33%. Deepening of the dicrotic notch in the Doppler waveform alwayspreceded the fall in D-MCA-BFV. Patients without syncope or presyncope (n ¼ 96)had smaller changes in cerebral blood flow velocities during HUT and only twenty-two subjects had transient deepening of the dicrotic notch. Eleven subjects had pre-syncope during HUT due to an exaggerated response to nitrates with progressivearterial hypotension without bradycardia and changes during TCD monitoring thatwere intermediate between positive and negative HUT.
In conclusion, patients with neurocardiogenic syncope have changes in cere-bral blood flow during the event. TCD monitoring during HUT helps to assess thesealterations.ª 2003 Published by Elsevier Ltd on behalf of The European Society of Cardiology.
KEYWORDSsyncope;head upright tilt table
test;transcranial Doppler
–––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––
) Corresponding author. Tel.: C54-4787-7500; fax: C54-577-3209.
E-mail address: [email protected] (G. Albina).
1099-5129/$30 ª 2003 Published by Elsevier Ltd on behalf of Thedoi:10.1016/j.eupc.2003.09.009
Introduction
Syncope is a transient loss of consciousness with in-ability to maintain postural tone due to cerebralhypoperfusion. Recovery is typically spontaneous.Themost frequent cause of syncope is a dysfunction
European Society of Cardiology.
64 G. Albina et al.
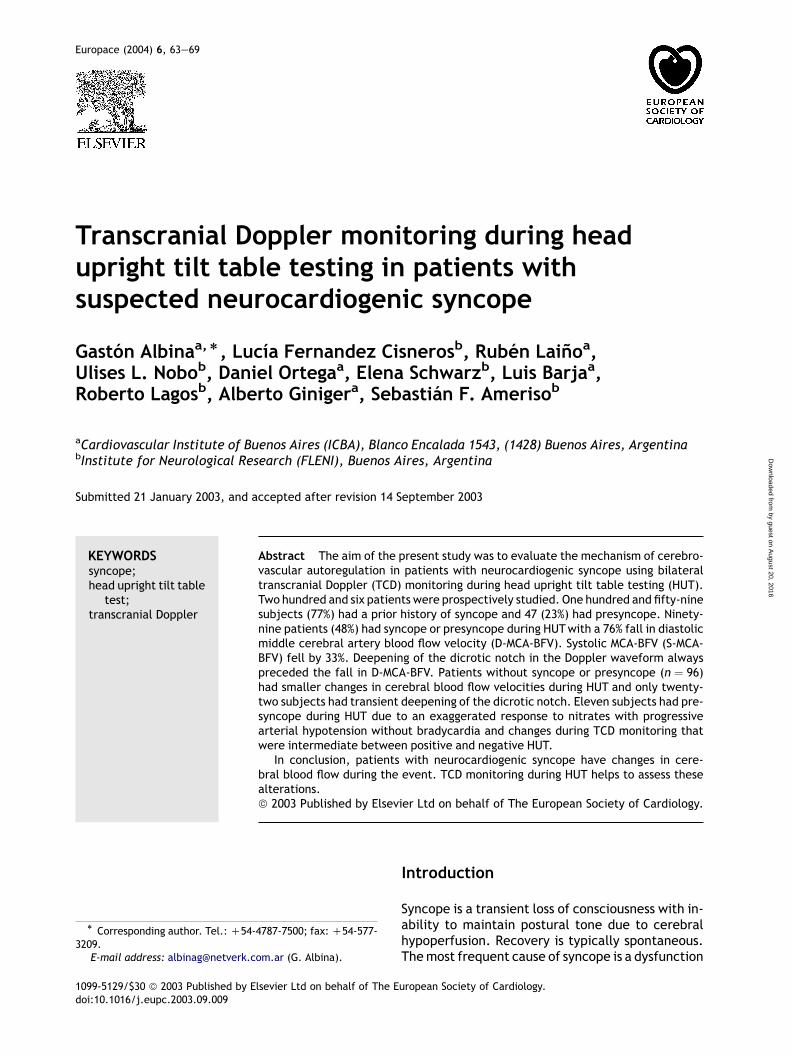
Figure 1 MeanG SD of percentage fall from baseline indiastolic (gray bars) and systolic (white bars) MCA-BFVduring HUT. P, positive test patients; N, negative testpatients; E, exaggerated response to nitrates patients.*p! 0:0001 vs. N and E, **p! 0:0001 vs. N.
of the autonomic nervous system (i.e., neurocardio-genic syncope) [1]. Its pathophysiological mecha-nisms are not fully understood. Syncope is theresultoftransientarterialhypotension,withorwith-out bradycardia, after triggering of sympatheticinhibition and adrenomedular discharge, associ-ated or not with parasympathetic upregulation[2]. This autonomic pattern may be mediated byperipheral mechanisms involving the BezoldeJarish reflex or central mechanisms with release ofserotonin or endogenous opiates. A rapid decreasein venous return associated with increased ventric-ular inotropism triggers most episodes [3e5].
The head upright tilt table test (HUT) objectivelyhelps to identify patients with neurocardiogenicsyncope. The pathophysiology of neurocardiogenicsyncope still poses several unanswered questions.One of them is the role of cerebral autoregulation.
In 1982, Aaslid et al. [6] introduced a transcranialDoppler technique that allowed real time assess-ment of blood flow velocities in intracranial cere-bral arteries. This technique provides anatomical
by guest on August 20, 2016
Dow
nloaded from
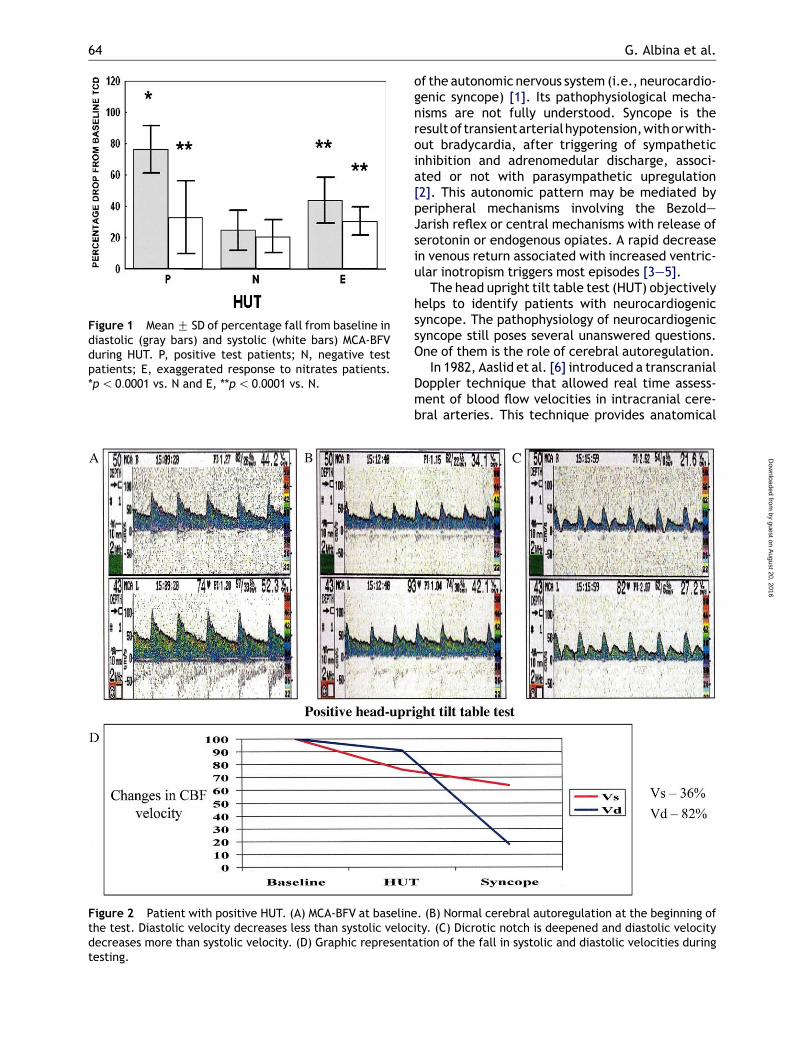
Figure 2 Patient with positive HUT. (A) MCA-BFV at baseline. (B) Normal cerebral autoregulation at the beginning ofthe test. Diastolic velocity decreases less than systolic velocity. (C) Dicrotic notch is deepened and diastolic velocitydecreases more than systolic velocity. (D) Graphic representation of the fall in systolic and diastolic velocities duringtesting.
Cerebral blood flow in reflex syncope 65
as well as functional information including cerebralautoregulation [7].
We evaluated cerebral blood flow dynamics usingtranscranial Doppler during HUT in patients withsuspected neurocardiogenic syncope.
Methods
Two hundred and six patients with a suspected diag-nosis of neurocardiogenic syncope referred to ourlaboratory between August 1999 and December2001 were analyzed. Syncope was defined as a sud-den transient loss of consciousness with inability tomaintain postural tone, with spontaneous recov-ery. Presyncope was defined as the presence ofpremonitory symptoms (i.e., dizziness, sweating,and nausea) not followed by loss of consciousness.All patients received a detailed medical history
including neurological and cardiological clinicalexaminations and electrocardiogram (ECG). Ancil-lary diagnostic tests were performed when medi-cally indicated. A photoplethysmographic device(Colin 7000, San Antonio, TX, USA) allowed accuratecontinuous noninvasive monitoring of systolic anddiastolic blood pressure and heart rate during theprocedure.
HUT was performed following a 3-h fasting peri-od. After baseline measurements of heart rate andblood pressure, each patient was positioned at anangle of 60( from supine on the tilt table for as longas 45 min. If syncope did not occur during the initialtilt, patients received 2.5 mg of sublingual isosor-bide dinitrate [8e14]. A positive test was definedas syncope associated with hypotension with orwithout bradycardia. Positive tests were classifiedas: Type 1 (mixed), blood pressure fall with heartrate reduction to no lower than 40 beats perminute;
by guest on August 20, 2016
Dow
nloaded from
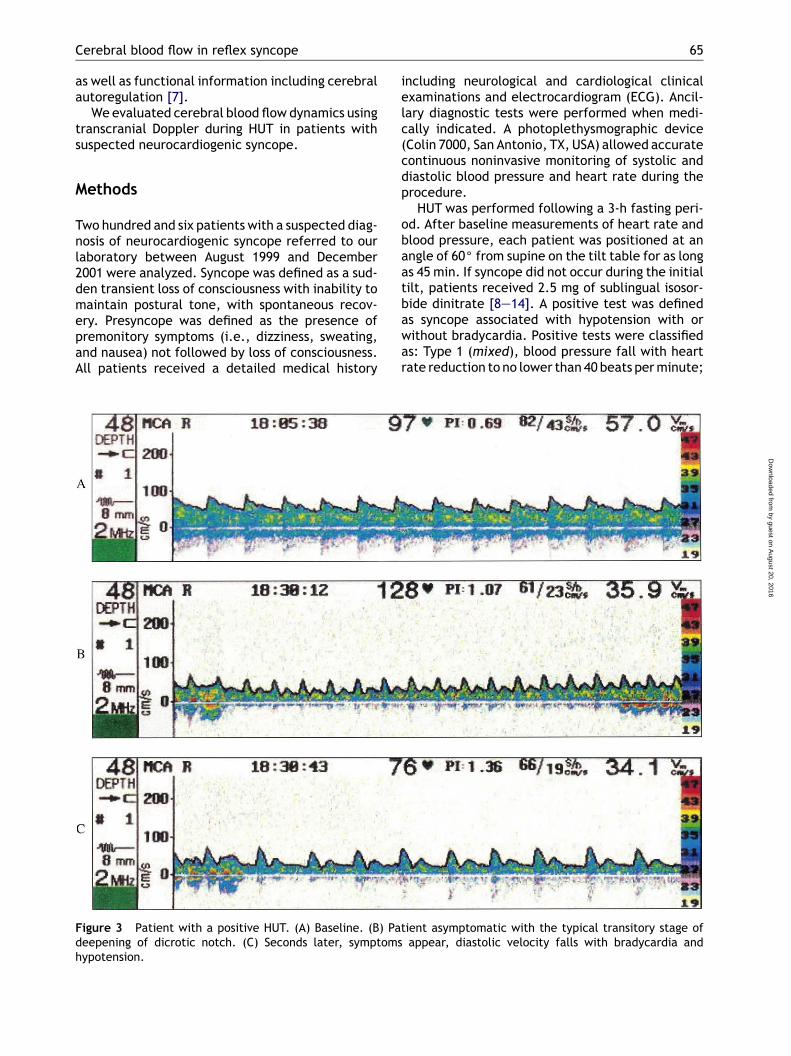
Figure 3 Patient with a positive HUT. (A) Baseline. (B) Patient asymptomatic with the typical transitory stage ofdeepening of dicrotic notch. (C) Seconds later, symptoms appear, diastolic velocity falls with bradycardia andhypotension.
66 G. Albina et al.
Type 2 (cardioinhibition), heart rate fall to aventricular rate less than 40 beats per minute;and Type 3 (vasodepressor), blood pressure fallwithout bradycardia [15].
Blood flow velocities of both middle cerebralarteries (MCA-BFV) were continuously monitoredat a depth of 55 mm through the transtemporalwindow using a transcranial Doppler device (MultiDop X4, Sipplingen, Germany). We recorded sys-tolic and diastolic MCA-BFV (S-MCA-BFV andD-MCA-BFV). For data analysis purposes, we selec-ted recordings from the side with the best ultra-sonic signal.
We analyzed the data using standard statisticalprocedures. We compared percent change in BFVduring HUT using paired t-tests. Comparisons ofpercent change in MCA-BFV during HUT betweenpositive test, negative test, and exaggerated re-sponse to nitrates groups were done usingStudent’s t-test for unpaired data. All statisticallevels quoted (p values) are two-sided. Resultsare given as meanG SD and were considered statis-tically significant when the p value was !0.05.
Results
We studied 206 consecutive subjects, aged 40G 22years (range 5e85 years). There were 129 femalesand 77 males. One hundred and fifty-nine subjectshad a history of syncope and 47 had presyncope. Onaverage, subjects had 5:7G 6:1 episodes (1:5G 2:0episodes in the previous 30 days). Dizziness wasthe most frequent prodromal symptom (n ¼ 110).Thirty patients had abnormal movements (seizure-like activity) during the episode, 48 sustainedtrauma, 26 had urinary incontinence, and 32 lostconsciousness without a prodrome. No patient hada history of cardiac disease or ECG abnormalities.
HUT was positive in 99 patients (48%), negativein 96 (47%) and the remaining 11 (5%) had an exag-gerated response to nitrates. Systolic and diastolicMCA-BFV fell significantly in the three groups. How-ever, the magnitude of the fall, especially in dia-stolic values, was larger in patients with positivetests (Fig. 1). Test responses in the positive groupwere vasodepressor in 19, cardioinhibitory in 12,and mixed in 68 cases.
by guest on August 20, 2016
Dow
nloaded from
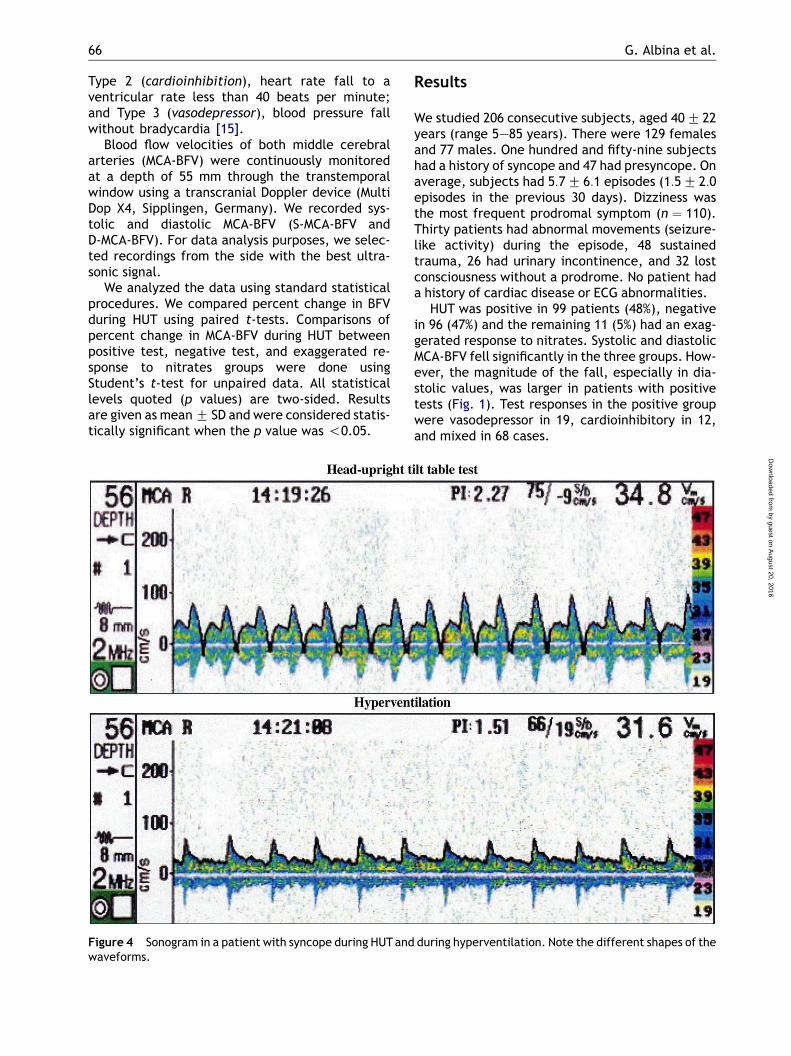
Figure 4 Sonogram in a patient with syncope during HUTand during hyperventilation. Note the different shapes of thewaveforms.
Cerebral blood flow in reflex syncope 67
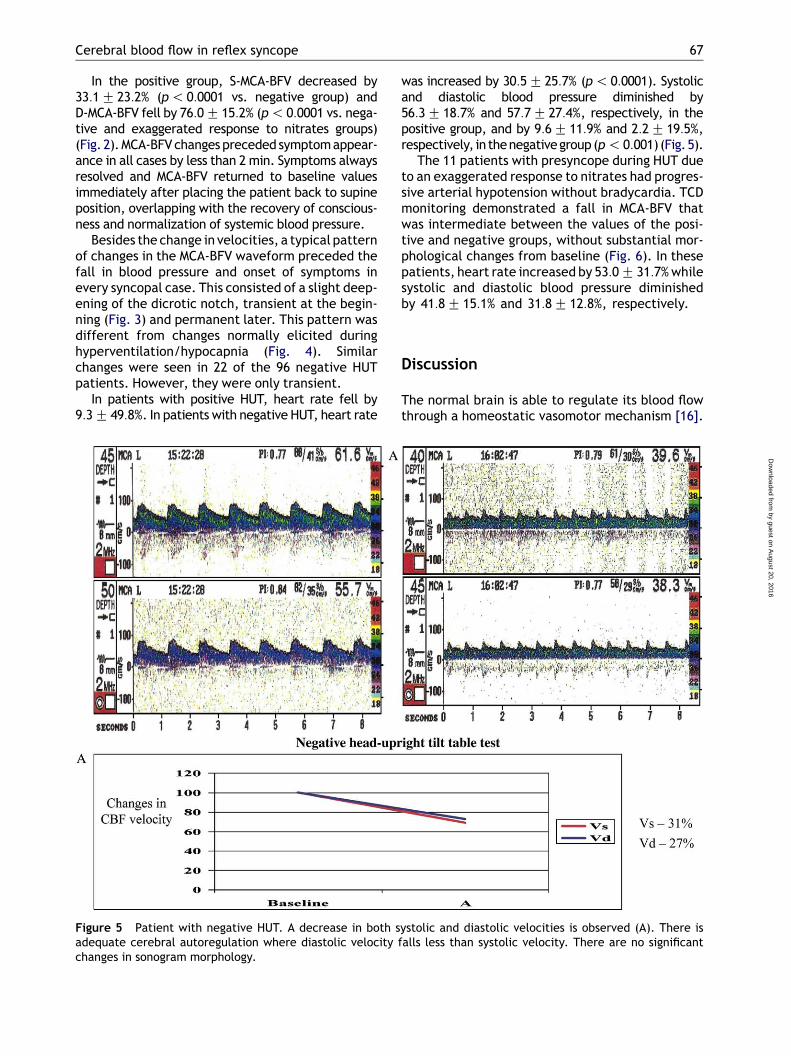
In the positive group, S-MCA-BFV decreased by33:1G 23:2% (p! 0:0001 vs. negative group) andD-MCA-BFV fell by 76:0G 15:2% (p! 0:0001 vs. nega-tive and exaggerated response to nitrates groups)(Fig. 2).MCA-BFVchangespreceded symptomappear-ance in all cases by less than 2 min. Symptoms alwaysresolved and MCA-BFV returned to baseline valuesimmediately after placing the patient back to supineposition, overlapping with the recovery of conscious-ness and normalization of systemic blood pressure.
Besides the change in velocities, a typical patternof changes in the MCA-BFV waveform preceded thefall in blood pressure and onset of symptoms inevery syncopal case. This consisted of a slight deep-ening of the dicrotic notch, transient at the begin-ning (Fig. 3) and permanent later. This pattern wasdifferent from changes normally elicited duringhyperventilation/hypocapnia (Fig. 4). Similarchanges were seen in 22 of the 96 negative HUTpatients. However, they were only transient.
In patients with positive HUT, heart rate fell by9:3G 49:8%. In patients with negative HUT, heart rate
was increased by 30:5G 25:7% (p! 0:0001). Systolicand diastolic blood pressure diminished by56:3G 18:7% and 57:7G 27:4%, respectively, in thepositive group, and by 9:6G 11:9% and 2:2G 19:5%,respectively, in thenegativegroup(p! 0:001) (Fig.5).
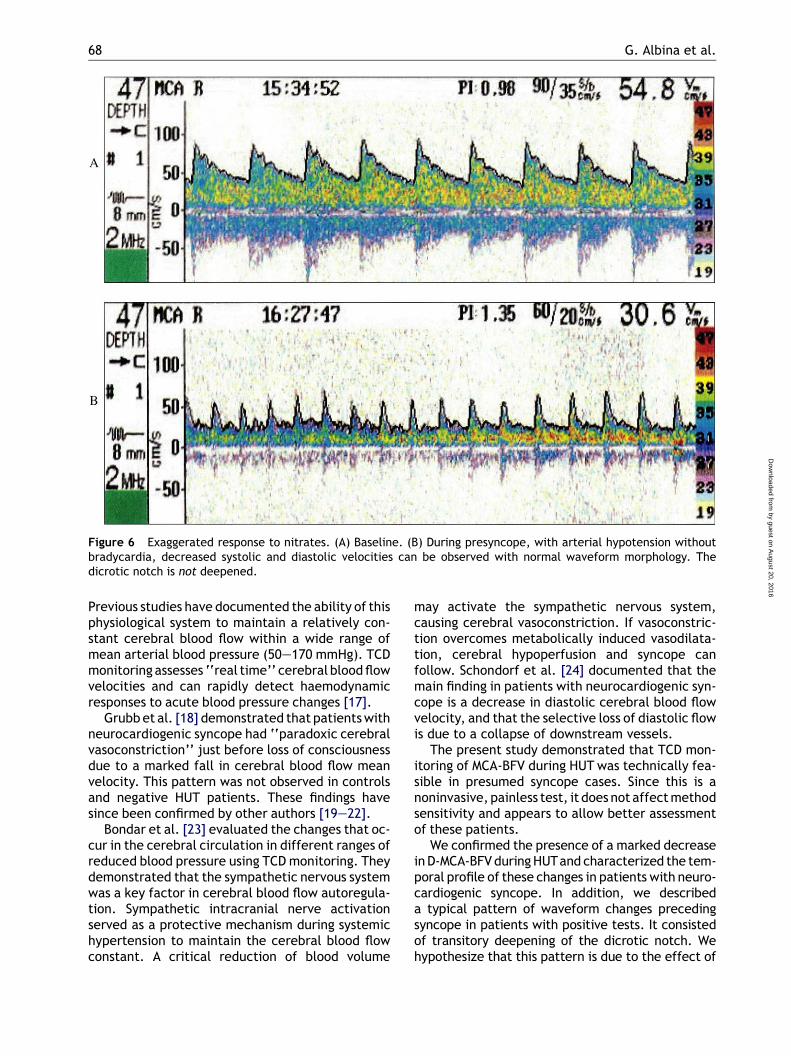
The 11 patients with presyncope during HUT dueto an exaggerated response to nitrates had progres-sive arterial hypotension without bradycardia. TCDmonitoring demonstrated a fall in MCA-BFV thatwas intermediate between the values of the posi-tive and negative groups, without substantial mor-phological changes from baseline (Fig. 6). In thesepatients, heart rate increased by 53:0G 31:7%whilesystolic and diastolic blood pressure diminishedby 41:8G 15:1% and 31:8G 12:8%, respectively.
Discussion
The normal brain is able to regulate its blood flowthrough a homeostatic vasomotor mechanism [16].
by guest on August 20, 2016
Dow
nloaded from
Figure 5 Patient with negative HUT. A decrease in both systolic and diastolic velocities is observed (A). There isadequate cerebral autoregulation where diastolic velocity falls less than systolic velocity. There are no significantchanges in sonogram morphology.
68 G. Albina et al.
by guest on August 20, 2
Dow
nloaded from
Figure 6 Exaggerated response to nitrates. (A) Baseline. (B) During presyncope, with arterial hypotension withoutbradycardia, decreased systolic and diastolic velocities can be observed with normal waveform morphology. Thedicrotic notch is not deepened.
016
Previous studies have documented the ability of thisphysiological system to maintain a relatively con-stant cerebral blood flow within a wide range ofmean arterial blood pressure (50e170 mmHg). TCDmonitoring assesses ‘‘real time’’ cerebral bloodflowvelocities and can rapidly detect haemodynamicresponses to acute blood pressure changes [17].
Grubbet al. [18] demonstrated that patientswithneurocardiogenic syncope had ‘‘paradoxic cerebralvasoconstriction’’ just before loss of consciousnessdue to a marked fall in cerebral blood flow meanvelocity. This pattern was not observed in controlsand negative HUT patients. These findings havesince been confirmed by other authors [19e22].
Bondar et al. [23] evaluated the changes that oc-cur in the cerebral circulation in different ranges ofreduced blood pressure using TCDmonitoring. Theydemonstrated that the sympathetic nervous systemwas a key factor in cerebral blood flow autoregula-tion. Sympathetic intracranial nerve activationserved as a protective mechanism during systemichypertension to maintain the cerebral blood flowconstant. A critical reduction of blood volume
may activate the sympathetic nervous system,causing cerebral vasoconstriction. If vasoconstric-tion overcomes metabolically induced vasodilata-tion, cerebral hypoperfusion and syncope canfollow. Schondorf et al. [24] documented that themain finding in patients with neurocardiogenic syn-cope is a decrease in diastolic cerebral blood flowvelocity, and that the selective loss of diastolic flowis due to a collapse of downstream vessels.
The present study demonstrated that TCD mon-itoring of MCA-BFV during HUT was technically fea-sible in presumed syncope cases. Since this is anoninvasive, painless test, it does not affectmethodsensitivity and appears to allow better assessmentof these patients.
We confirmed the presence of a marked decreaseinD-MCA-BFVduringHUTand characterized the tem-poral profile of these changes in patients with neuro-cardiogenic syncope. In addition, we describeda typical pattern of waveform changes precedingsyncope in patients with positive tests. It consistedof transitory deepening of the dicrotic notch. Wehypothesize that this pattern is due to the effect of
Cerebral blood flow in reflex syncope 69
by guest on August 20, 2016
Dow
nloaded from
the respiratory cycle on the cerebral blood flowvelocities during conditions of relative hypovolemiaas seen during the Valsalva manoeuvre, especiallyin susceptible patients. Patients with negative testsdid not exhibit this waveform pattern except for 22subjects, who did so transiently. The recognition ofthis pattern has 2 important implications: (1) itshows objective evidence of altered cerebral bloodflow regulation preceding systemic haemodynamicchanges; and (2) it identifies patients who may laterhave neurocardiogenic syncope.
TCD monitoring also allowed for better identifi-cation of patients with exaggerated response tonitrate stimuli. Despite a moderate fall in S- andD-MCA-BFV velocities, this group did not exhibitthe typical deepening of the dicrotic notch foundin positive HUT patients. We believe that this fea-ture may help to differentiate these patients fromthose with true vasodepressor syncope.
Thedisproportionatechange indiastoliccomparedwith systolic velocities suggests that simply monitor-ing the mean MCA-BFV may not reflect the actualmagnitude and quality of changes in cerebral circula-tion. Cerebral vessels of patients with neurocardio-genic syncope may have impaired reactivity, makingthem susceptible to sustain transient hypoperfusion.Theevidence for thiswas thefindingof anearly deep-ening of the dicrotic notch with lowering of D-MCA-BFV preceding changes in blood pressure.
In conclusion, patients with neurocardiogenicsyncope have changes in cerebral blood flow regu-lation during the event. TCD monitoring during HUThelps to assess these alterations. Since TCD changesprecede the fall in blood pressure, heart rateand symptoms, this technique may, in the future,allow early interruption of HUT before symptomsarise, preventing the unpleasant experience forthepatients. TCDmonitoringmay also help to differ-entiate patients with exaggerated response tonitrates fromthosewith trueneurocardiogenic vaso-depressor syncope.TCDduringHUTmay improve thewell-known usefulness of the method for the diag-nosis of neurocardiogenic syncope.
References
[1] Lempert T, Bauer M, Schmidt D. Syncope: a videometricanalysis of 56 episodes of transient cerebral hypoxia. AnnNeurol 1994;36:233e7.
[2] Grubb BP, Olshansky B. Syncope: mechanisms and manage-ment. In: Grubb BP, editor. Neurocardiogenic syncope.Futura Publishing Company; 1998. p. 73e106.
[3] Grimm DR. Neurally mediated syncope: a review of cardiacand arterial receptors. J Clin Neurophysiol 1997;14:170e82.
[4] Sutton R, Petersen M. The clinical spectrum of neurocardio-genic syncope. J Cardiovasc Electrophysiol 1995;6:569e76.
[5] Wallbridge DR, MacIntyre HE, Gray CE, Denvir MA, OldroydKG, Rae AP, et al. Increase in plasma b endorphins precedesvasodepressor syncope. Br Heart J 1994;71:597e9.
[6] Aaslid R, Markwalder T-M, Nornes H. Non-invasive trans-cranial Doppler ultrasound recording of flow velocity inbasal cerebral arteries. J Neurosurg 1982;57:769e74.
[7] Petty GW, Wiebers DO, Meissner I. Transcranial Dopplerultrasonography: clinical applications in cerebrovasculardisease. Mayo Clin Proc 1990;65:1350e64.
[8] Benditt DG, Remole S, Bailin S, Dunnigan A, Asso A, MilsteinS. Tilt table testing for evaluation of neurally mediated(cardioneurogenic) syncope: rationale and proposed proto-cols. Pacing Clin Electrophysiol 1991;14:1528e37.
[9] Fitzpatrick AP, Sutton R. Tilting towards a diagnosis inrecurrent unexplained syncope. Lancet 1989;1:658e60.
[10] Raviele A, Gasparini G, Di Pede F, et al. Nitroglycerininfusion during upright tilt: a new test for the diagnosis ofvasovagal syncope. Am Heart J 1994;127:103e11.
[11] Raviele A, Menozzi C, Brignole M, et al. Value of head-up tilttesting potentiated with sublingual nitroglycerin to assessthe origin of unexplained syncope. Am J Cardiol 1995;76:267e72.
[12] Zung Chuunyu, Zher Zhining, Hu Wenhui, et al. Value ofsublingual isosorbide dinitrate before isoproterenol tilt testfor diagnosis of neurally mediated syncope. Am J Cardiol1999;83:1059e63.
[13] Ammirati F, Colvicchi F, Biffi A, Mageis B, Pandozi C, SantiniM. Head-up tilt testing potentiated with low-dose sub-lingual isosorbide dinitrate. A simplified time-savingapproach for the evaluation of unexplained syncope.Am Heart J 1998;135:671e6.
[14] Del Rosso A, Bartoli P, Bertoletti A. Shortened head-up tilttesting potentiated with sublingual nitroglycerin in patientswith unexplained syncope. Am Heart J 1998;135:564e70.
[15] Sutton R, Petersen M, Brignole M, Raviele A, Menozzi C,Giani P. Proposed classification for tilt induced vasovagalsyncope. Eur J Card Pacing Electrophysiol 1992;2:180e3.
[16] Aaslid RP, Lindegaard KF, Sorteberg W, Nornes H. Cerebralautoregulation dynamics in humans. Stroke 1989;20:45e52.
[17] Tiecks FP, Lam AM, Aaslid R, Newell D. Comparison of staticand dynamic cerebral autoregulation measurements.Stroke 1995;26:1014e9.
[18] Grubb BP, Gerard G, Roush K, et al. Cerebral vasoconstric-tion during head-upright tilt-induced vasovagal syncope.A paradoxic and unexpected response. Circulation 1991;84:1157e64.
[19] Fredman CS, Bierman KM, Patel V, Uppstrom EL, Auer AI.Transcranial Doppler ultrasonography during head-uprighttilt-table testing. Ann Intern Med 1995;123:848e9.
[20] Sung RY, Du ZD, Yu CW, YamMC, Fok TF. Cerebral blood flowduring vasovagal syncope induced by active standing orhead up tilt. Arch Dis Child 2000;82:154e8.
[21] Grubb BP, Samoil D, Kosinski D, Wolfe D, Arewster P, ElliottL, et al. Cerebral syncope: loss of consciousness associatedwith cerebral vasoconstriction in the absence of systemichypotension. Pacing Clin Electrophysiol 1998;21:652e8.
[22] Dan D, Hoag JB, Ellenbogen KA, Wood MA, Eckberg DL,Gilligan DM. Cerebral blood flow velocity declines beforearterial pressure in patients with orthostatic vasovagalpresyncope. J Am Coll Cardiol 2002;39:1039e45.
[23] Bondar RL, Kassan MS, Stein F, Dunphy PT, Fortney S,Riedesel ML. Simultaneous cerebrovascular and cardiovas-cular responses during syncope and presyncope. Stroke1995;26:1794e800.
[24] Schondorf R, Benoit J, Wein T. Cerebrovascular andcardiovascular measurements during neurally mediatedsyncope induced by head-up tilt. Stroke 1997;28:1564e8.
Related Documents











