NEUROCARDIOGENIC SYNCOPE: CURRENT STATUS WITH EVIDENCE ON RATE DROP PACING DR DEVINDER KUMAR

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

NEUROCARDIOGENIC SYNCOPE:
CURRENT STATUS WITH EVIDENCEON RATE DROP PACING
DR DEVINDER KUMAR
SYNCOPE
Defined as brief and self-limited period of loss ofconsciousness due to transient global cerebralhypoperfusion.


NEUROCARDIOGENIC SYNCOPE
Refers to heterogeneous group of conditions inwhich cardiovascular reflexes that are normallyuseful in controlling the circulation becomeintermittently inappropriate, in response to atrigger, resulting in vasodilatation and/orbradycardia.

VVS
• Magnitude of the problem
• Often encountered in young otherwisehealthy patients, but may occur in all agegroups, and is generally unassociated withcardiovascular or neurologic diseases.

VVS
• Common triggers: Unpleasant sights, pain,extreme emotion, and prolonged standing.
• Autonomic activation (eg, flushing andsweating) in the premonitory phase stronglysuggests a vasovagal origin.
• Typical presentations occur in about 40% ofpresumed vasovagal syncope, but less often inolder patients.

PATHOPYSIOLOGY OF VVS
• Incompletely understood.
• Afferent pathway remains uncertain (nohuman recordings of baroreceptor signalsduring syncope have been made).
• Experimental data from cats.
• It consists of paradoxic impulses from ahypercontractile, empty left ventricle, whichare conducted by unmyelinated vagalafferents to the brain stem.

• The efferent response is transient vagalstimulation of the heart and widespreadsympathetic withdrawal.


Extrapolating this data to humans?
• Feline reflex, recorded under general anesthesia and major instrumentation, to the conscious human, with the knowledge that cats do not faint
• There is evidence to suggest that humans can have VVS after cardiac transplantation
Fitzpatrick AP, Banner N, Cheng A, et al. J Am Coll Cardiol 1993;21:1132–7
Scherrer U, Vissing S, Morgan BJ, et al. N Engl J Med 1990;322:602–4

Extrapolating this data to humans?
• Mechanism when the stimulus is central ? (eg, blood–injection–injury phobia)
• Echocardiography during tilt

DIAGNOSIS
• History
• Physical examination
• ECG
• ECHOCARDIOGRAPHY

DIAGNOSIS
• HUTT
• ILRs

PHYSIOLOGIC IMPACT OF UPRIGHT POSTURE
• Initially, as upright posture is achieved, 500 to800 ml blood is shifted to the lower part ofthe body.
• Most of this redistribution occurs in the first10 seconds.

PHYSIOLOGIC IMPACT OF UPRIGHT POSTURE
• Subsequently, in normal individuals, anadditional 700 ml protein-free fluid is filteredinto the interstitial space in the next 10minutes.
• The result of these two actions is markedreduction of venous return and stroke volume.
PHYSIOLOGIC IMPACT OF UPRIGHT POSTURE
• These are compensated by both ↑ HR &constriction of resistance and capacitancevessels.
• If compensatory cardiovascular responsemaintains MAP atleast 60 mmHg ormore………………..no syncope.

PHYSIOLOGIC IMPACT OF UPRIGHT POSTURE
• In susceptible individuals, an inappropriate setof neural reflex responses appear to betriggered - i.e. vasodilatation and bradycardia -the vasovagal response.
• It is this latter possible outcome that formsthe basis for the use of tilt testing in theevaluation of patients with suspectedvasovagal syncope.

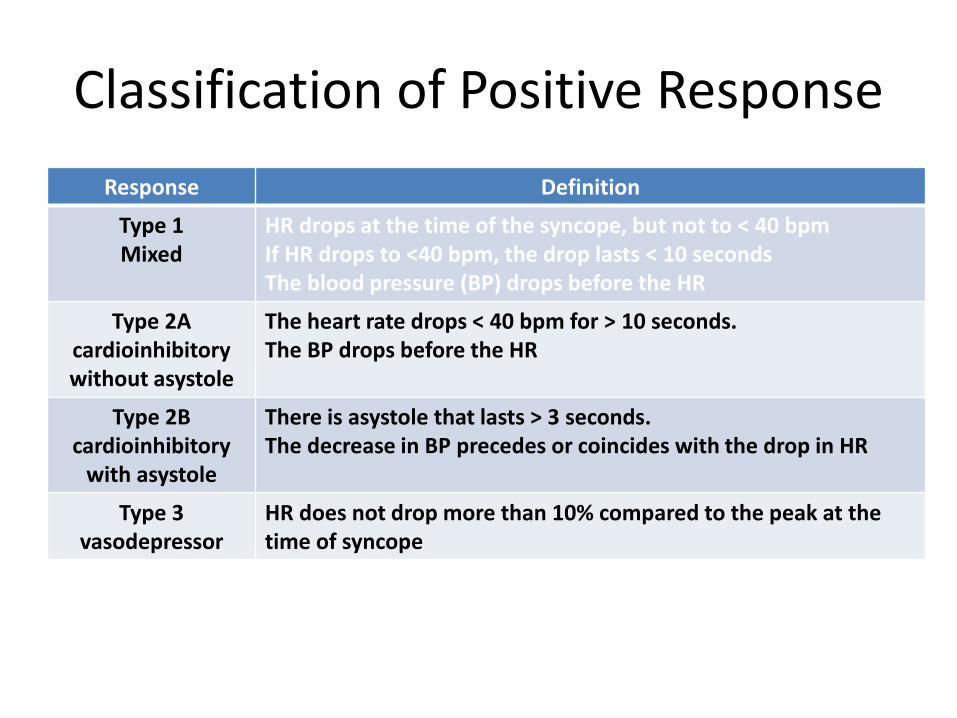
Classification of Positive Response
Response Definition
Type 1Mixed
HR drops at the time of the syncope, but not to < 40 bpmIf HR drops to <40 bpm, the drop lasts < 10 secondsThe blood pressure (BP) drops before the HR
Type 2A cardioinhibitorywithout asystole
The heart rate drops < 40 bpm for > 10 seconds. The BP drops before the HR
Type 2B cardioinhibitory
with asystole
There is asystole that lasts > 3 seconds. The decrease in BP precedes or coincides with the drop in HR
Type 3 vasodepressor
HR does not drop more than 10% compared to the peak at the time of syncope


HUTT
• Is HUTT indicated in every patient suspectedof VVS?
• Are we better placed after HUTT and if sohow?

SENSITIVITY
• No definite evidence based clinical definitionof neurocardiogenic syncope.
• In fact, it is a syndrome defined by a test,rather than a test that diagnoses a syndrome.
• There is a lack of the validation of tilt tabletesting against populations with definedcauses of syncope (hence difficult to knowsensitivity of tilt table tests).
SPECIFICITY
• Life time prevalence of VVS 20-40% of generalpopulation.
• It is not known how many control subjects aresimply people who have not yet fainted but willat some later time (hence difficult to assess truespecificity).
• Also the specificity decreases withpharmacological provocation.

METHODOLOGICAL ROBUSTNESS
• In HUTT, the likelihood of positive tests depends on whether
Intravenous cannulation is used,
The angle and duration of head-up tilt,
Whether, how and which drug challenge is used,
The number of head-up iterations during the test,
The volume status of the subject,
Subject’s age

REPRODUCIBILITY
• Tilt table tests are 70% to 87% reproducibleover periods of days to months.
• The degree of bradycardia and hypotensionduring tilt table tests is only modestlyreproducible, suggesting that patients cannotbe classified based on the hemodynamicchanges seen on a single positive tilt tabletest.
REPRODUCIBILITY
International Study on Syncope of UncertainEtiology (ISSUE) investigators concluded that thedegree of bradycardia during a positive tilt tabletest does not correlate with the degree ofbradycardia recorded in an ILR during asubsequent spontaneous syncopal spell in thecommunity.

PROGNOSTIC VALUE
• Tilt table test outcomes do not predict clinicaloutcome.
• Patients with negative and positive tests havesimilar symptoms, similar symptom burdens,similar clinical outcomes in the 3 yearsfollowing the tilt table test.
Sheldon R, Rose S, Connolly S, et al. Eur Heart J 2006;27:344–50
Sheldon R, Rose S, Koshman ML. Am J Cardiol 1997;80:581–5
SELECTING THERAPIES
• The need for isoproterenol to induce syncopedoes not predict a clinical response to beta-blockers.
• Positive during tilt table testing does notpredict a clinical response to pacemakers.
Sheldon R, Connolly S, Rose S, et al. Circulation 2006;113:1164–70
Sud S, Massel D, Klein GJ, et al. Am J Med 2007;120:54–62

USEFULLNESS OF HUTT
• Positive test indicates susceptibility to neurallymediated syncope.
• They have provided the inclusion criteria fordiagnostic and long-term observational studiesand randomized clinical trials.
• Tilt table tests have been used as platforms forphysiologic studies and pilot treatment studies.
USEFULLNESS OF HUTT
• Added reassurance.
• For education to early identification ofpremonitory symptoms.
• For tilt training.
• For psychogenic syncope.

ILRs
• Are small devices implanted subcutaneously inthe left hemithorax.
• Have no intravascular leads, thereby avoidingmost complications caused by pacemakers.
• Last about 3 years.


ILRs
ECG findings during syncopal spells within eachpatient are highly reproducible, indicating that asingle syncopal spell suffices to provide useablediagnostic information.

ILRs
The overall likelihood of establishing a diagnosiswithin the 2- to 3-year lifetime of an ILR istherefore in the range of 40%, which agrees wellwith the likelihood of at least 1 syncoperecurrence in numerous observational andrandomized clinical trials.
Brignole M, Vardas P, Hoffman E, et al. Europace 2009;11:671–87

Carotid Sinus Syndrome
• CSS tends to occur most often in older men,and is especially associated with concomitantatherosclerotic disease.
• The most common symptoms attributed toCSH are dizziness (presyncope) and syncope.
• Classical provocative maneuvers: headturning, shaving, or the wearing of tight neckcollars.

PATHOPHYSIOLOGY
Neurodegenerative process in medullary nucleii,which may in turn be associated with impairedbaroreceptor regulation.

CSM
• The procedure should be done with thepatient in both the supine and uprightpositions.
• Continuous ECG and BP monitoring.
• Following baseline measurements, CSM isperformed for 5 to 10 seconds at the anteriormargin of the sternocleidomastoid muscle atthe level of the cricoid cartilage.

• CICSH is defined as greater than or equal to 3seconds asystole during carotid massage.
• Vasodepressor CSH is defined as greater than orequal to 50 mm Hg decrease in blood pressure inresponse to carotid sinus massage.
• Mixed CSH is diagnosed by the presence of agreater than or equal to 3-second pause, alongwith a decrease in systolic blood pressure of atleast 50 mm Hg upon rhythm resumption.
• If a positive result is not obtained, theprocedure is then repeated on the oppositeside after an interval of 1 to 2 minutes.
• One-third of patients have a positive responseonly in the upright position.
• If a cardioinhibitory response is elicited,atropine may be administered beforerepeating massage to determine the degree ofcontributory vasodepression.

THERAPY FOR VASOVAGAL SYNCOPE

TREATMENT GOALS?
• Prevention of recurrence.
• Prevention of associated injuries.
• Improvement of quality of life.
• Not to prolong survival, as this is a benigncondition.
NONPHARMACOLOGICAL
• Education and counselling.
• Salt and water increase.
• Orthostatic training.
• Counterpressure maneuvers.
Education and counselling
• Reassurance about benign nature of thecondition.
• Help in identifying prodromal symptoms early (soas to implement counterpressure maneuvers)and potential known triggers (venipuncture,volume depletion, environmental triggers) whichcould be avoided.
Salt and Water Increase
• Volume expansion: First line therapy andcornerstone of treatment.
• Improves orthostatic tolerance in patientswith recurrent VVS.
• Beneficial effects are reported in mostsubjects within 1 week.

Orthostatic Training
• Patients stand with their upper back positionedagainst a wall or a corner without moving theirarms or legs.
• Starting at 5 mins twice daily, gradually increasedover a period of 6-8 weeks to 40 mins twice daily.
• Orthostatic training can also be achieved by tilttraining.

Orthostatic Training
• Physiologic objective: Reset baroreceptorreflexes, improving gravitational stressresponse by leading to more efficientvasoconstriction.
Orthostatic Training
• Patients with recurrent VVS were randomizedto treatment with propranolol, disopyramide,or tilt training. On repeat tilt table test,pharmacologic therapy was not effective atpreventing syncope (32% propranolol, 26%disopyramide). In contrast, tilt training washighly efficient and prevented syncope in 92%of patients.
Abe H, et al. Pacing Clin Electrophysiol 2002;25:1454–8

Orthostatic Training
Patients with VVS refractory to standardmedical therapy were randomized to a controlor orthostatic training group.
After a mean follow-up of 18 months,recurrent syncope was experienced by 56.5% inthe controlled group, compared with no syncoperecurrences in the orthostatic training group.
Di Girolamo E, et al.k. Circulation 1999;100:1798–801

Orthostatic Training
• Compliance is poor.
• Three RCTs comparing either orthostatictraining or tilt training have failed to confirmreductions in long-term syncope recurrence.
1. Reybrouck T, Heidbu¨chel H, Van De Werf F, et al. Pacing Clin Electrophysiol 2002;25:1441–6
2. Gajek J, Zysko D, Mazurek W. Kardiol Pol 2006;64:602–8
3. Duygu H, Zoghi M, Turk U, et al. Pacing Clin Electrophysiol2008;31:592–6
Orthostatic Training
Progressively prolonged periods ofenforced orthostatic training may reducesyncope recurrence in highly motivated youngpatients when prodromal symptoms are presentand reproducible.

Counterpressure Maneuvers (CPMs)
• Younger patients: VVS is preceded byprodromal symptoms and early recognitionprovides enough time to implement CPMs.
• Isometric CPMs of legs (leg crossing) or arms(hand grip and arm tensing) are able toinduce a significant BP increase during thephase of impending VVS.

Counterpressure Maneuvers (CPMs)

Counterpressure Maneuvers (CPMs)
• By increase in sympathetic nerve dischargeand vascular resistance during maneuvers andby mechanical compression of the venousvascular bed in the legs and abdomen.
Counterpressure Maneuvers (CPMs)
• The Physical Counterpressure Maneuvers Trial(PC-Trial) was a multicenter, prospective,randomized clinical trial evaluating theeffectiveness of CPMs in 223 patients withrecurrent VVS and recognizable prodromalsymptoms.

During a mean follow-up period of 14months, the occurrence of syncope wassignificantly lower in the group trained in CPMs(50.9% of the patients receiving conventionaltreatment vs 31.6% of those trained in CPMs;P<.005)
CPMs are effective, feasible, safe, and wellaccepted by patients in daily life and should beadvised as first-line treatment in youngerpatients presenting with VVS and recognizableprodromal symptoms.
PHARMACOLOGICAL TREATMENT
• Beta blockers
• Adrenergic agonists
• Fludrocortisone
• SSRIs
• Experimental therapies

Beta blockers
• Based on the initial understanding of themechanism of VVS, b-blockers were used asfirst-line therapy.
• Early observational studies showed significantreductions in recurrence of syncope, mostlyassessed by repeated tilt testing.

Beta blockers
• RCTs have failed to show beneficial effects ofb-blockers in unselected patients withrecurrent VVS.
• POST(Prevention Of Syncope Trial): largemulticenter, randomized, placebo-controlled,double-blind study.
• Metoprolol (25 to 200 mg) vs placebo in VVS.

Beta blockers
• No differences in the primary outcome (firstrecurrence of syncope) were seen betweenthe groups.
• Subgroup analysis in POST: in patients olderthan 42 years, metoprolol may be effectivebased on a 48% relative risk reduction (RRR) intime to first recurrence of syncope.

Beta blockers
• The latest ESC guidelines do not recommendbeta-blockers for the routine treatment ofrecurrent VVS and might be beneficial inpatients older than 42 years.

Alpha agonists
Potent vasoconstrictors that amelioratethe reduction in peripheral resistanceresponsible for venous pooling andvasodepression, and therefore result in anincrease systolic and diastolic blood pressure.

Alpha agonists
• Etilefrine was the first a-agonist tested fortreatment of VVS.
• The Vasovagal Syncope International Study(VASIS), was a large, multicenter, placebo-controlled, double-blinded study – nosignificant differences in the recurrence ofsyncope and time for first syncopal episodecompared with placebo.

MIDODRINE
Midodrine, a specific alpha 1-agonistcompared with placebo, provides beneficialeffects in symptom frequency, symptoms duringhead-up tilt, and quality of life.
A recent meta-analysis of 6 randomizedclinical trials evaluating alpha-agonists fortreatment of VVS included 329 patients. Thismeta-analysis reported a large effect favoringmidodrine compared with placebo (odds ratio,0.21; 95% CI, 0.06–0.77; P = 0.02).
Liao Y, Li X, Zhang Y, et al. Acta Paediatr 2009;98:1194–2000

• Midodrine is reasonably well tolerated, but itsuse is not recommended in patients withhypertension or heart failure.
• Midodrine should be administered 3 times perday and titrated to a maximum dose of 40 mg.
FLUDROCORTISONE
• Corticosteroid with marked mineralocorticoidactivity that increases sodium and fluidretention and, consequently, intravascularvolume expansion.
• It upregulates alpha-adrenergic receptors andmay prevent vasodilatation during neurallymediated reflex responses.

FLUDROCORTISONE
• The second POST trial (POST II) randomized213 patients to fludrocortisone (0.1 to 0.4 mgdaily) or placebo.
• The primary outcome of the study was time tothe first recurrence of syncope, which was notsignificantly reduced by fludrocortisone.

FLUDROCORTISONE
• Available evidence does not show a significantreduction in syncope recurrence withfludrocortisone in unselected patients withVVS.
• Further analysis of the POST II population mayidentify subgroups that benefit from thistherapy.
SSRIs
• Fluoxetine vs propranolol: no differences insyncope-free period.
• A significant improvement in quality of lifewas observed with fluoxetine.
Theodorakis GN, Leftheriotis D, Livanis EG, et al. Europace 2006;8:193–8.
SSRIs
• Paroxetine 20 mg/d or placebo.
• After 1 month of treatment, the responserates (negative tilt) were 61.8% versus 38.2%(P<.001) in the paroxetine and placebogroups, respectively.
Di Girolamo E, Di Iorio C, Sabatini P, et al. J Am Coll Cardiol 1999;33:1227–30

• Paroxetine significantly improved symptomscompared with placebo (17.6% vs 52.9,P<.0001).
• SSRIs are rarely the first choice in thetreatment of neurally mediated reflex syncope

Patients in whom standard therapies areineffective, poorly tolerated, or contraindicatedmight be prescribed SSRIs, which may beparticularly useful in patients with associatedanxiety and panic disorders
PACING IN SYNCOPE
• Only treatable component- BRADYCARDIA.
• With the use of tilt testing, several authorsanalyzed the role of pacing in preventingsyncope induced during tilt testing.

SPECIAL PACING ALGORITHMS
• Rate drop response (RDR) algorithm.
• Closed loop stimulation (CLS).
RATE DROP RESPONSE (RDR)
Two detection elements that can beactivated simultaneously and triggerintervention therapy independently from eachother
Drop-detect method
Low-rate detect method

DROP DETECT METHOD

LOW RATE DETECTION METHOD
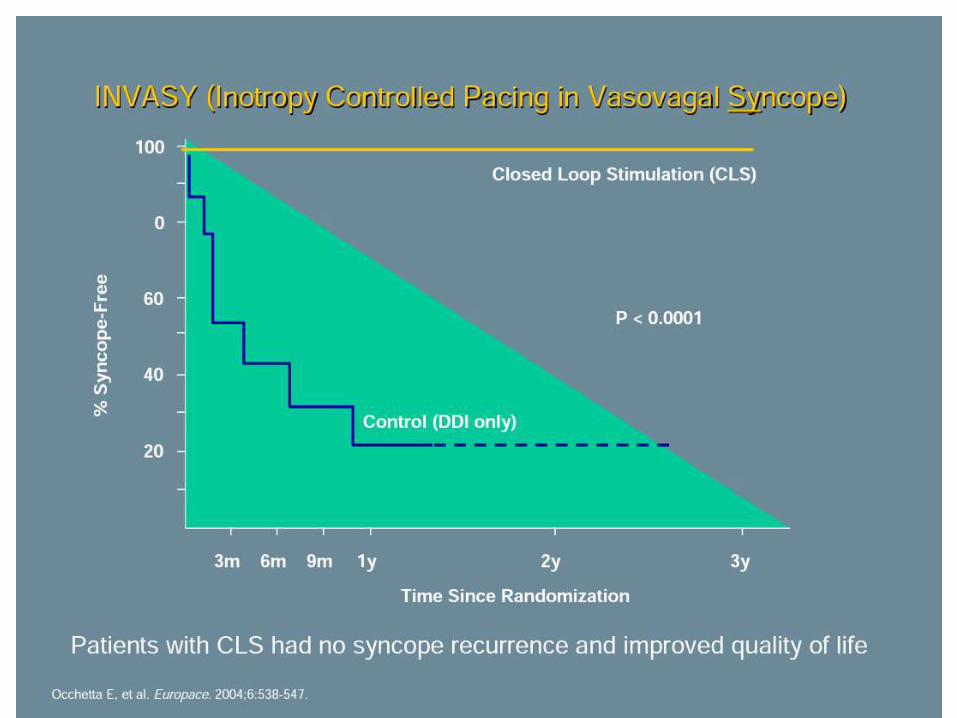
CLOSED LOOP STIMULATION (CLS)
• This pacing system tracks the variations inintracardiac impedance during the systolicphase of the cardiac cycle on a beat-to-beatbasis.
• Changes in intracardiac impedance are closelycorrelated with both right and left ventricularcontractility.
Based on that relationship, CLS transfersthe detected changes in myocardial contractiondynamics into individual pacing rates.

In the very first days following programmeimplementation, CLS is adjusted to eachindividual patient: a reference curve is createdand continuously updated with beat-to-beatimpedance measurements.
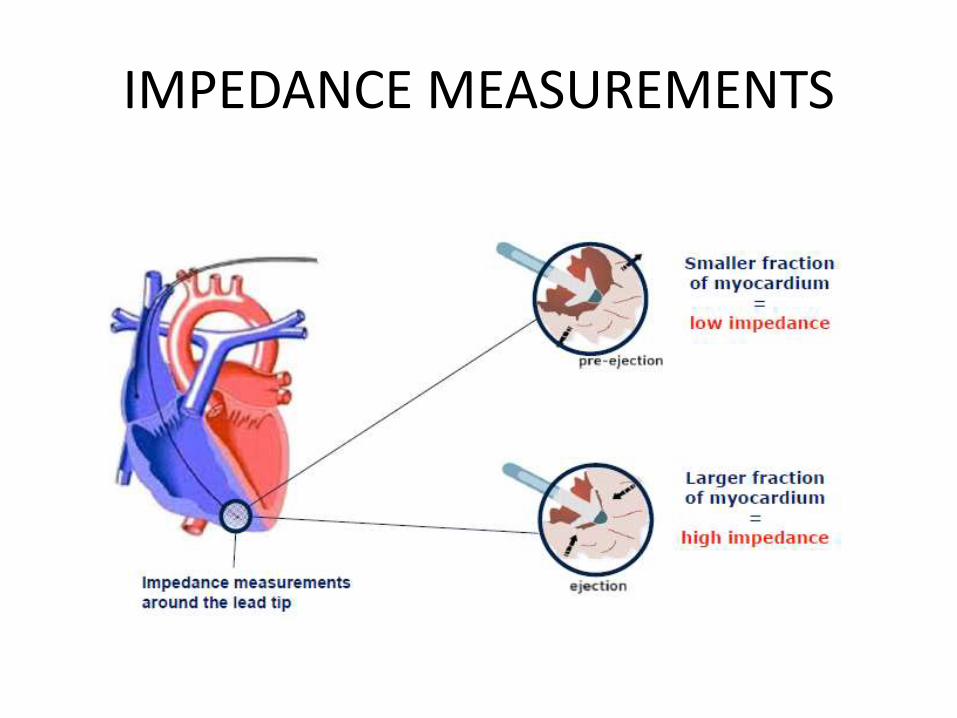
IMPEDANCE MEASUREMENTS
CLS-Reference Vs Load curve
• With each heartbeat, CLS determines theimpedance curve (VIMP) during ventricularcontraction (load curve) and compares it to itsreference curve at rest (rest curve).

REFERENCE Vs LOAD CURVE

PACING IN RESPONSE TO CONTRACTION DYNAMICS

NONBLINDED STUDIES

RANDOMIZED BLINDED STUDIES

DISCREPANCIES IN STUDIES
• PLACEBO effect.
• The vasodepressor and cardioinhibitorycomponents may vary in each patient withdifferent episodes and 50% to 83% of syncopalepisodes may not have a cardioinhibitorycomponent ((Sheldon & Connolly, 2003).

SUMMARY
• Neurocardiogenic syncope is a commonproblem with significant burden.
• Most important for the diagnosis is history.
• Present therapeutic approaches not stronglysupported by randomized clinical trials.

SUMMARY
• Pacing in patients with neurocardiogenic syncope is adifficult decision and requires careful judgement.
• Treatment success is dependent on the underlyingmechanism of neurocardiogenic syncope.
• Use of an ILR can improve identification of patientswith neurocardiogenic syncope, in whom pacemakertreatment is helpful, esp. those with spontaneousasystolic episodes.

SUMMARY
• Do not expect miracles.
• Patience by both physician and the patient.

Status of Pacing in VVS
• Perception of pacing for VVS changing:– VVS with +HUT and cardioinhibitory response a Class IIb indication1
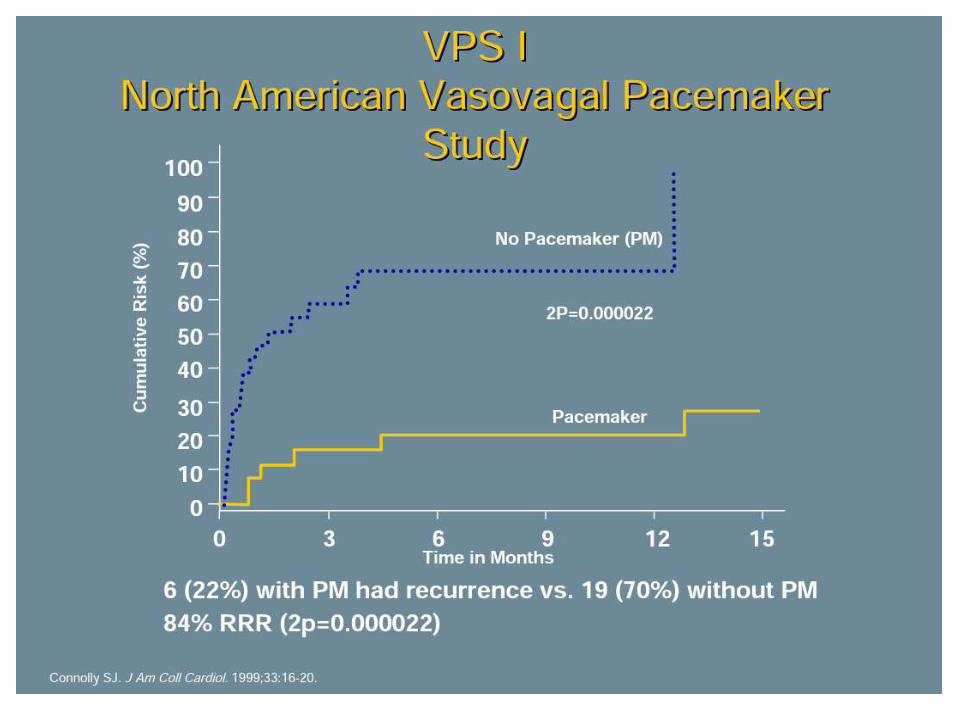
• Recent clinical studies demonstrated benefits of pacing in select VVS patients:– VPS I
– VASIS
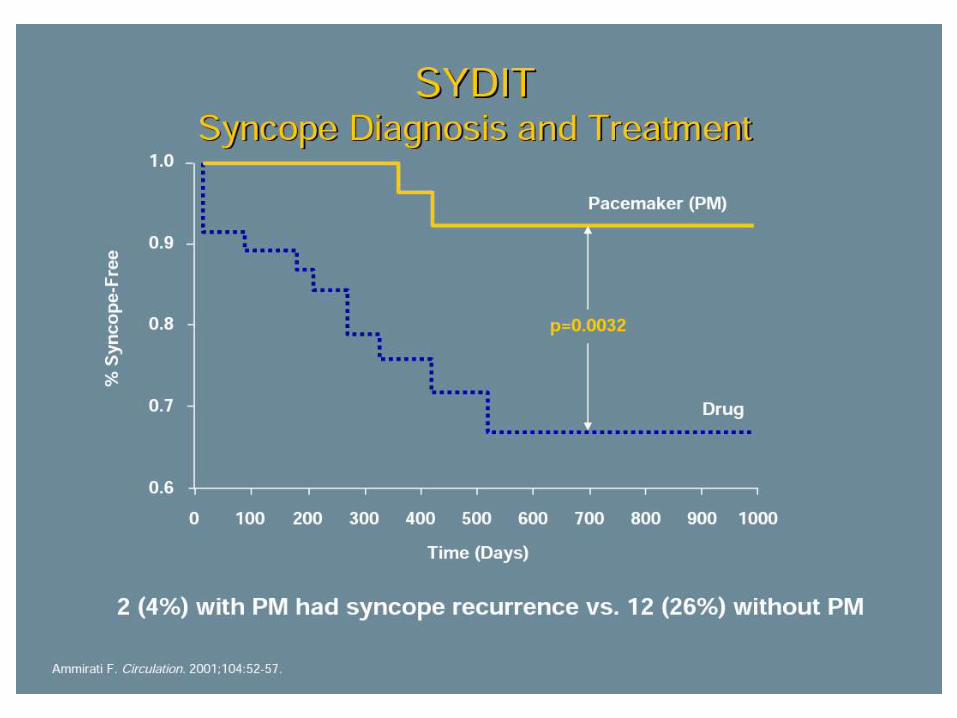
– SYDIT
– VPS II –Phase I
– ROME VVS Trial
1Gregoratos G, et al. ACC/AHA Guidelines for Implantation of Cardiac Pacemakers and Antiarrhythmic Devices. Circulation. 1998; 97:
1325-1335.

Status of Pacing in VVS
• Benefits of specific device features evolving:– Some success with DDD/DDI hysteresis 1
• “False positives” may result in prolonged high rate intervention
• Tied to lower rate intervention
– Rate drop therapies designed for treating VVS syncope appear to be successful 2-4
1 Sutton R, et al. Circulation. 2000; 102:294-299.
2 Connolly S, et al. J Am Coll Cardiol 1999; 33:16-20.
3 Ammirati F, et al. Circulation. 2002; 104: 52-57.
4 Ammirati F, et al. NASPE Abstract #307. PACE, Vol. 24, April 2002, Part II.
VPS-IVasovagal Pacemaker Study I
Connolly S, et al. J Am Coll Cardiol 1999; 33: 16-20.
Study Design:54 patients randomized, prospective, single center
_ 27 DDD pacemaker with rate drop response (RDR)
_ 27 no pacemaker
Patient Inclusion Criteria:6 syncopal events ever (median lifetime history of 35 episodes (no
pacemaker) and 14 episodes (pacemaker).
+HUT
Relative bradycardia*
*a trough heart rate <60/min if no isoproterenol used,
<70/min if up to 2 mcg/min isoproterenol used, or <80/min
if over 2 mcg/min isoproterenol used

VPS-I
• Conclusion:
Dual-chamber pacing with rate drop response
reduces the likelihood of syncope in patients
with recurrent VVS.
Connolly S, et al. J Am Coll Cardiol 1999; 33: 16-20.

VASIS Vasovagal Syncope International Study
Sutton, R, et al. Circulation. 2000; 102:294-299.
Study Design: 42 patients, randomized, prospective, multicenter
_ 19 DDI pacemaker (80 bpm) with rate hysteresis (45 bpm)
_ 23 no pacemaker
Patient Inclusion Criteria: > 3 syncopal events in 2 years and last event occurring within 6 months of
enrollment and,
Positive VASIS type 2A or 2B cardioinhibitory response to HUT and,
Age > 40 years or drug refractory if < 40 years


VASIS
• Conclusion:
Dual-chamber pacing (at a rate of 80 bpm ) with rate hysteresis reduces the likelihood of syncope in patients with tilt-positive, cardioinhibitory syncope.
Sutton, R, et al. Circulation. 2000; 102:294-299.

SYDIT Syncope Diagnosis and Treatment Study
• Study Design:
– 93 patients randomized, prospective, multicenter
• 46 DDD pacemaker with rate drop response (RDR)
• 47 Atenolol 100 MG/D
• Patient Inclusion Criteria:
– > 55 yrs
– > 3 syncopal episodes in 2 years
– + HUT with relative bradycardia (trough HR <60 bpm)
Ammirati F, et al. Circulation. 2001; 104:52-57.

SYDIT
• Conclusion:
Dual-chamber pacing + RDR is superior to Atenolol in prevention of recurrent syncope in highly symptomatic patients with relative bradycardia during tilt-induced syncope.
Ammirati F, et al. Circulation. 2001; 104:52-57.

VPS-II: Phase IVasovagal Pacemaker Study-II
• Study Design:– 100 patients, randomized, prospective, multicenter
• 50 DDD pacemaker with rate drop response (RDR)
• 50 ODO pacemaker (inactive mode)
• Patient Inclusion Criteria:– > 6 syncope events ever or > 3 syncope events in 2
years or > 1 syncope event in 6 months and,
– Positive HUT with syncope or presyncope and aheart rate blood pressure product <9000.
Presented at the 23rd Annual Scientific Sessions of the North American Society of Pacing and Electrophysiology. Late Breaking
Clinical Trials, May 11, 2002.


VPS-II: Phase I
Conclusions:
Lower than anticipated syncope event rate in the control arm.
Higher than anticipated event rate in the treatment group.
Consequence: treatment effect was less than VPS-I.
Results favored pacing but the treatment effect was not statistically significant.
Presented at the 23rd Annual Scientific Sessions of the North American Society of Pacing and Electrophysiology. Late Breaking
Clinical Trials, May 11, 2002.

VVS Pacing Trials Conclusions
DDD pacing reduces the risk of syncope
in patients with recurrent, refractory,
highly-symptomatic, cardioinhibitory
vasovagal syncope.

SAFE PACE Study Design
• Randomized controlled trial (N=175):
– Pacing (87) vs. No Pacing (88)
• Single center: Royal Victoria Infirmary, Newcastle, UK
• Recruitment began: April 1998
• 12 month follow-up per patient
• Study concluded: May 2000
Kenny RA, J Am Coll Cardiol 2001; 38:1491-1496.

SAFE PACE Inclusion Criteria
• Consecutive adults attending accident and emergency department
• > 50 Years
- Experienced non-accidental fall
•Positive response to CSM
Kenny RA, J Am Coll Cardiol 2001; 38:1491-1496.
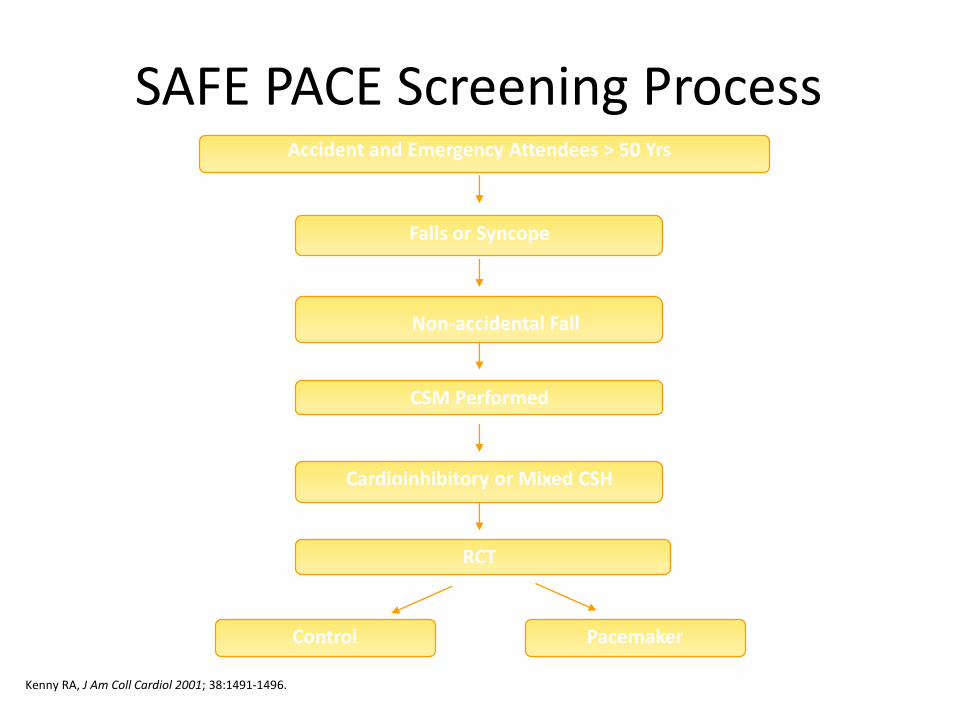
SAFE PACE Screening ProcessAccident and Emergency Attendees > 50 Yrs
Falls or Syncope
Non-accidental Fall
CSM Performed
Cardioinhibitory or Mixed CSH
RCT
Control Pacemaker
Kenny RA, J Am Coll Cardiol 2001; 38:1491-1496.

SAFE PACE Screening Results
RCT (n=175)
Control (n=88)
Pacemaker (n=87)
• No pacing intervention • Medtronic Thera DR(Rate Drop ResponseAlgorithm)
Kenny RA, J Am Coll Cardiol 2001; 38:1491-1496.

SAFE PACE ResultsNumber of Falls
Control
n=87
Pacemaker
n=84
% Participants
w/Falls
60% 58%
Total Number of
Falls*
699 216
Mean Number of
Falls**
9.3 4.1
* Falls during 12 months post randomization
** Crude adjustment calculation
Kenny RA, J Am Coll Cardiol 2001; 38:1491-1496.
70%Reduction[OR 0.42; 95%CI: 0.23, 0.75]
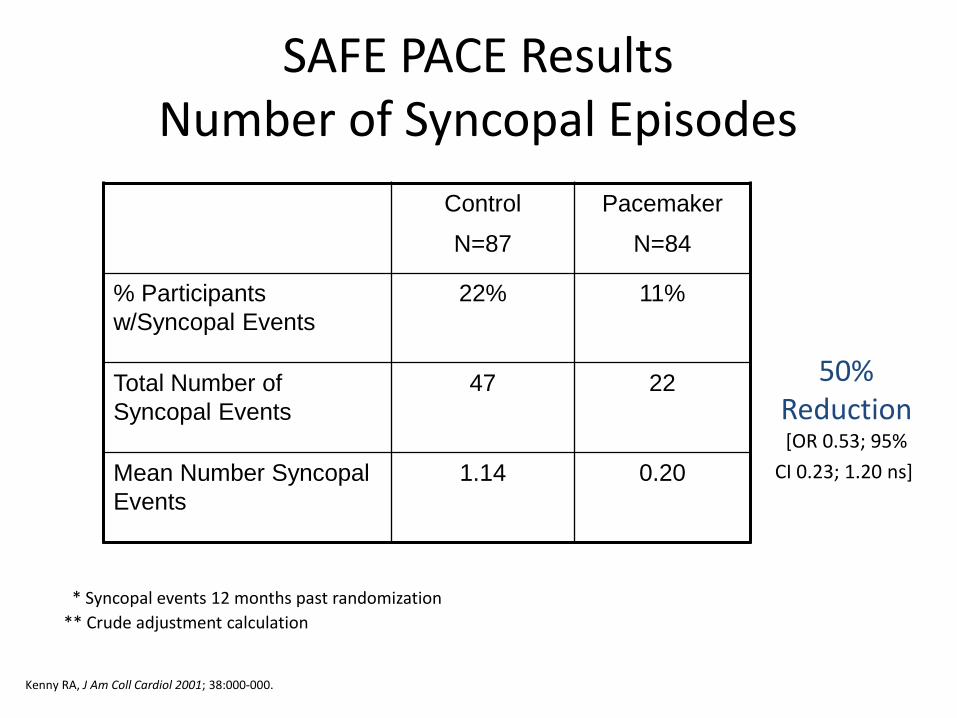
Control
N=87
Pacemaker
N=84
% Participants
w/Syncopal Events
22% 11%
Total Number of
Syncopal Events
47 22
Mean Number Syncopal
Events
1.14 0.20
SAFE PACE ResultsNumber of Syncopal Episodes
50%Reduction[OR 0.53; 95%
CI 0.23; 1.20 ns]
* Syncopal events 12 months past randomization
** Crude adjustment calculation
Kenny RA, J Am Coll Cardiol 2001; 38:000-000.
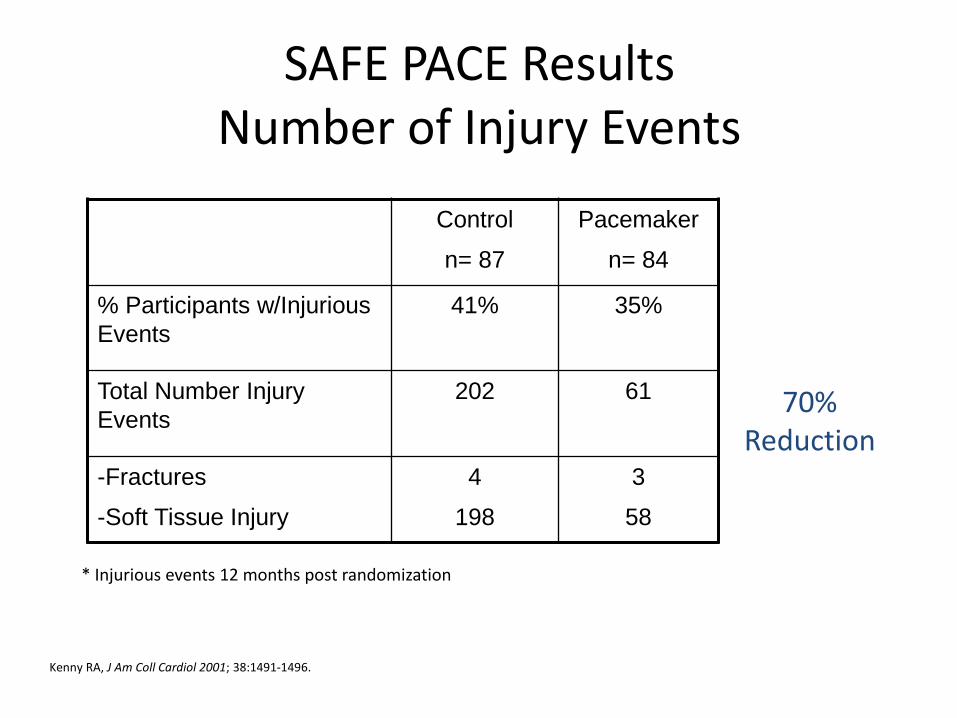
Control
n= 87
Pacemaker
n= 84
% Participants w/Injurious
Events
41% 35%
Total Number Injury
Events
202 61
-Fractures
-Soft Tissue Injury
4
198
3
58
SAFE PACE ResultsNumber of Injury Events
70%Reduction
* Injurious events 12 months post randomization
Kenny RA, J Am Coll Cardiol 2001; 38:1491-1496.

SAFE PACE Conclusions
In patients with unexplained falls and a
diagnosis of Cardioinhibitory CSH, cardiac
pacing reduced the total number of:
• Falls by 70%
• Syncopal events by 53%
• Injurious events by 70%
Kenny RA, J Am Coll Cardiol 2001; 38:1491-1496.
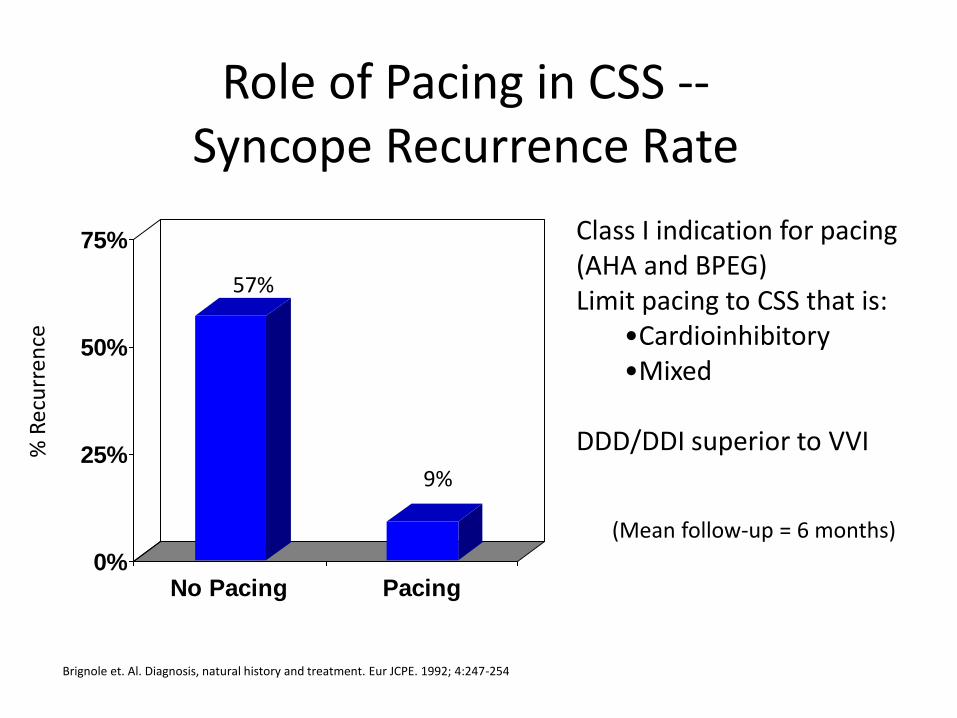
Role of Pacing in CSS --Syncope Recurrence Rate
Brignole et. Al. Diagnosis, natural history and treatment. Eur JCPE. 1992; 4:247-254
0%
25%
50%
75%
No Pacing Pacing
57%
%6Class I indication for pacing (AHA and BPEG)Limit pacing to CSS that is:
•Cardioinhibitory•Mixed
DDD/DDI superior to VVI
(Mean follow-up = 6 months)




2008 ACC/AHA GUIDELINES

2012 ACCF/HRS GUIDELINES

THANK YOU
Related Documents

![Syncope AHD[1]](https://static.cupdf.com/doc/110x72/577d36611a28ab3a6b92ec10/syncope-ahd1.jpg)