Toxic Alcohols John Kashani D.O. Attending, St. Joseph’s Emergency Department Staff Toxicologist, New Jersey Poison Center

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Toxic AlcoholsJohn Kashani D.O.
Attending, St. Joseph’s Emergency Department
Staff Toxicologist, New Jersey Poison Center

Case
• An 18 year old male is brought into the ED by his mother when he was difficult to awaken in the AM
• He was partying the night before, he is not able to provide a history
• He becomes progressively more obtunded while in the ED

Case
• A 22 year old frustrated medical student drinks a bottle of formaldehyde he stole from gross anatomy lab
• He complains of throat and esophageal irritation and has had multiple episodes of emesis

Case
• A 65 year old man is found comatosed
• His wife states that he has been depressed recently and has been drinking heavily
• An empty bottle of antifreeze was found in his kitchen garbage can

Case
• A 17 year old female ingests a bottle of rubbing alcohol
• She appears drunk, has multiple episodes of emesis and complains of abdominal pain

Case
• A 25 year old man presents to the ED with blurry vision
• For the past few days he has been feeling “cruddy”
• He admits to the ingestion of homemade everclear 3 days prior

Objectives
• Outline the “toxic” alcohols and potentially toxic alcohols
• Discuss the pharmacology, kinetics and pathophysiology of the toxic alcohols
• Discuss the clinical manifestations, diagnosis and management of patients poisoned by these agents

Introduction
• Alcohols are hydrocarbons that contain a hydroxyl group
• A compound with two hydroxyl groups is called a diol or a glycol
• Toxic alcohols commonly refer to methanol, ethylene glycol and isopropyl alcohol

Introduction
• Less common but potentially toxic alcohols include diethylene glycol, benzyl alcohol and the glycol ethers


Ethylene Glycol
• Coolant mixtures
• Antifreeze
• Air craft de-icing solutions
• Solvent (inks, pesticides and adhesives)
• Brake fluid
• Heat exchangers and condensers
• Glycerin substitute
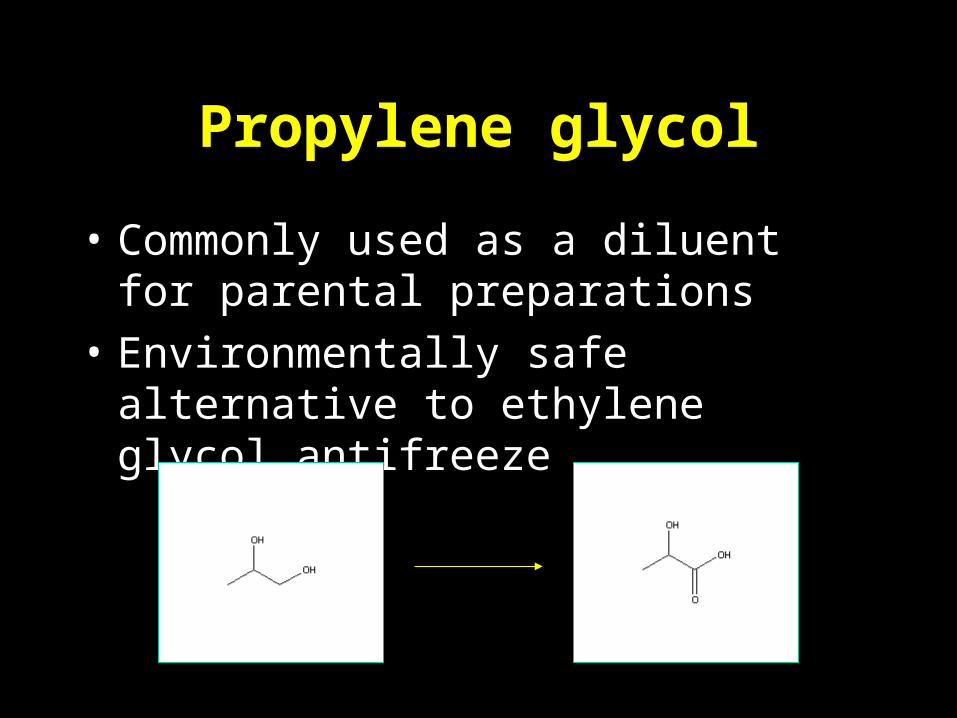
Propylene glycol
• Commonly used as a diluent for parental preparations
• Environmentally safe alternative to ethylene glycol antifreeze

Benzyl alcohol
+

Methanol
• Antifreeze (window washer fluid)
• Anti icing agent
• Octane booster
• Ethanol denaturant
• Extraction agent
• Solvent
• Fuel source

Methanol
• Varnish and paint removers
• Industrial solvent
• Manufacture of acetic acid, formaldehyde and inorganic acids

Isopropanol
• Synthesis of acetone, glycerin
• Solvent for oils, gums and resins
• Deicing agent
• Rubbing alcohol
• Hair care products, skin lotion and aerosols

Diethylene glycol
• Solvent
• Sprinkler antifreeze
• Paints, cosmetics
+ HEAA

Glycol ethers
• Solvents
• Semiconductor industry
• Fingernail polishes and removers
• Dyes, ink, cleaners, degreasers
• Brake fluid, car wax, injector cleaner
• Various household cleaning products

Pharmacology and Kinetics
• Exposure may occur dermally, pulmonary and GI
– Pulmonary absorption depends on vapor pressure
• Rapidly absorbed by the gastrointestinal route

Pharmacology and Kinetics
• Time to peak concentration
– Ethylene glycol = 1 - 4 hrs
– Methanol, isopropyl alcohol = 30 - 60 minutes
• VD is 0.6L/kg

Pharmacology and Kinetics
• Ethylene glycol and methanol are metabolized by alcohol dehyrogenase and aldehyde dehydrogenase
• Isopropanol is metabolized by alcohol dehydrogenase
• Binding affinities for
– ethanol>methanol>ethylene glycol

Pharmacology and Kinetics
• Methanol metabolism may be delayed (up to 72 hours)
• The volatility of methanol contributes to its pulmonary excretion (10-20%)
• Ethylene glycol is metabolized over 3 – 8 hours
– Undergoes multiple oxidations

Pharmacology and Kinetics
• Ethylene glycol is not appreciably excreted by the lungs
• Isopropanol is rapidly metabolized to acetone via alcohol dehyrogenase
• 20% is excreted unchanged
• Acetone is predominantly renally excreted

(CH2OH)2
CH2OHCHO
Ethylene glycol
Glycoaldehyde
CH2OHCOOH Glycolic Acid
CHOCOOH Glyoxylic Acid
Glycine + Benzoic Acid
Hippuric Acid
Oxalic Acid
Alpha-hydroxy-beta-ketoadipic acid
thiamine
Mg++
B6
ADH
ADH
ADH

CH3OH
CH2O
CHOOH
CO2 + H2O
Methanol
Formaldehyde
Formic Acid
Folate
ADH
ADH

Isopropyl alcohol
CH3CHOHCH3
ADH
CH3COCH3 Acetone

The Usual Suspects

Formic acid
• Metabolic acidosis
• Inhibits cytochrome oxidase:
– Decreased ATP production
• Increased anaerobic glycolysis & lactate

R-OH
NAD+ NADH + H+
ADH

Pyruvate Lactate
Acetyl-CoA
CO2
NAD+
NADH H+
NADH H+ NAD+
NADH
NAD+

Clinical Manifestations
• Clinical manifestations may be related to the parent compound or metabolites
• There may be an initial asymptomatic period
• Inebriation (unreliable)
– Isopropyl>ethylene glycol>methanol

Clinical Manifestations
• Vasodilation – hypotension and reflex tachycardia
• Hypoglycemia
• Anion gap acidosis
– Methanol and ethylene glycol
• Visual disturbances (”snow Field”)
– Formic acid is a retinal toxin

Clinical Manifestations
• ATN may develop secondary to calcium oxalate crystalluria
• Cranial nerve deficits have been reported with ethylene glycol

Clinical Manifestations
• Ispopropanol ingestion usually does not cause major toxicity unless a large amount is ingested
– CNS depression, hemorrhagic gastritis and tracheobronchitis

Diagnosis
• Both ethylene glycol and methanol result in an anion gap acidosis
• Isopropyl alcohol usually does not result in an anion gap acidosis
• Hypocalcemia may be seen in ethylene glycol intoxication– Chelation of calcium by oxalate –
calcium oxalate crystals

Diagnosis
• The absence of crystals is an unreliable finding
• The urine of a patient with ethylene glycol ingestion may fluoresce
– Short lived, unreliable

Calcium oxalate Crystals
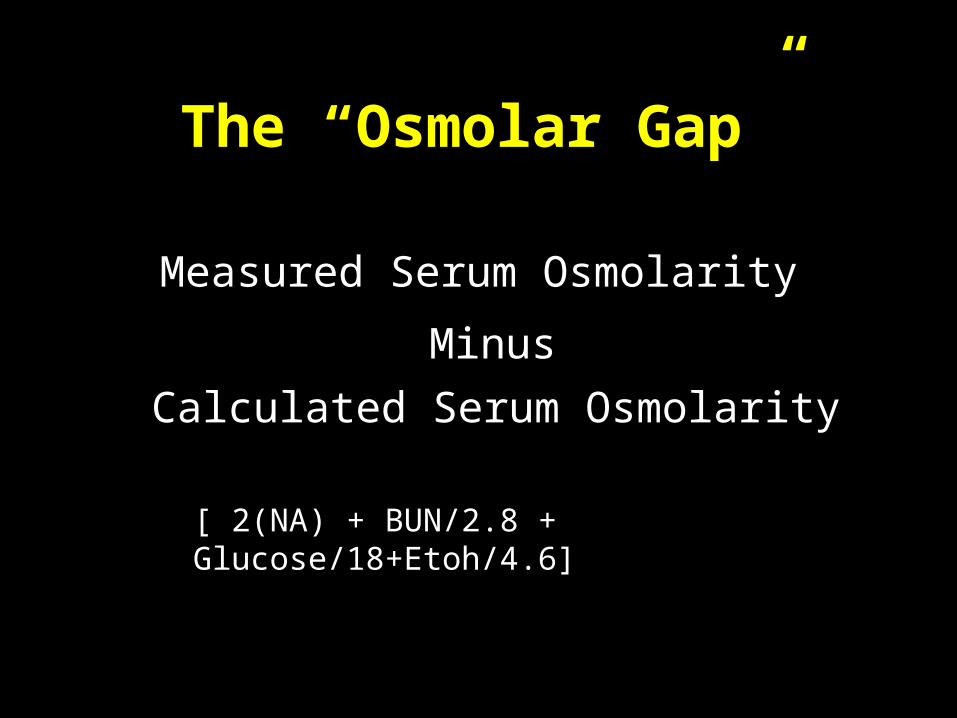
The “Osmolar Gap”
Measured Serum Osmolarity
Minus
Calculated Serum Osmolarity
[ 2(NA) + BUN/2.8 + Glucose/18+Etoh/4.6]

Substance Mole Wgt mOsm/L*
Methanol 32 34
Ethanol 46 23
Ethylene glycol 62 19
Acetone 58 18
Isopropanol 60 18
Salicylate 180 6
* At 100 mg/dl

0
50
100
150
200
250
0 100 200 300 400 500 600 700 800
Concentration (mg/dl)
osm
ola
r g
ap methanol
ethanol
ethylene glycol
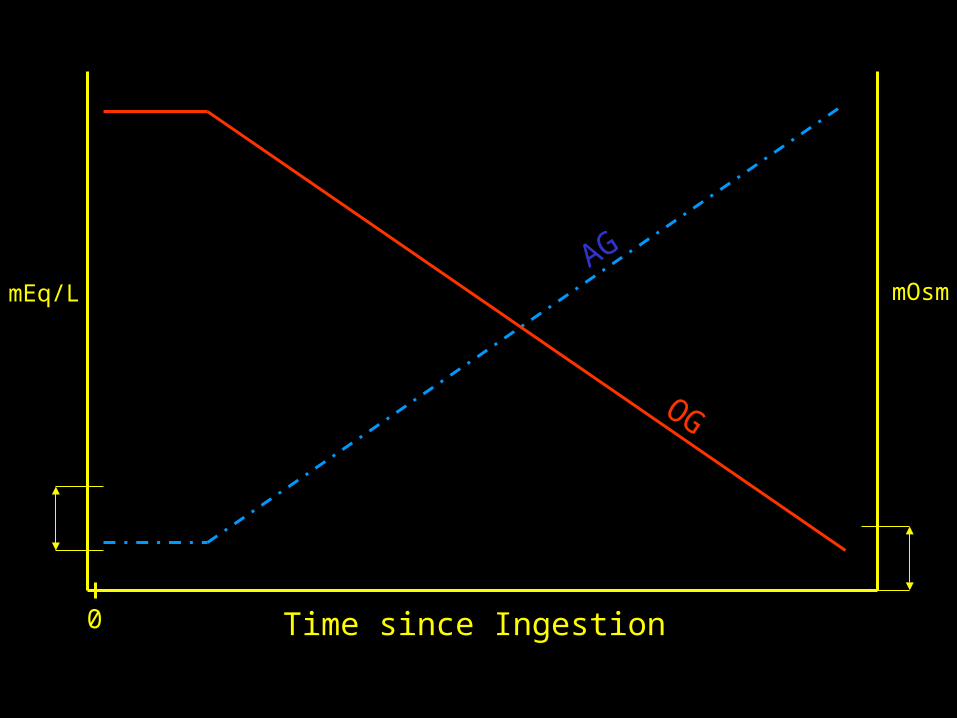
0 Time since Ingestion
mEq/L mOsmAG
OG

Quantitative testing
• If quantitative levels are readily available they can be used to determine proper management
• Best method is gas chromatography with flame ionization
– Subject to false positives
Management
• ABC’s
• +/---- NGT aspiration
• AC/ipecac/lavage = Bad move
• Thiamine and pyridoxine in the setting of ethylene glycol toxicity
• Folic acid in the setting of methanol toxicity

Management
• Sodium bicarbonate as needed
• Inhibition of Alcohol dehydrogenase
– Ethanol
– Fomepizole

Ethanol vs Fompepizole
Ethanol:- Oral or IV- CNS depression- Difficult titration- Frequent levels- Hypoglycemia
Fomepizole:- IV- No CNS depression- Easy dosing- No levels to monitor- More predictable pharmacokinetcs- No Hypoglycemia- Cost

Fomepizole…because shit happens

(CH2OH)2
CH2OHCHO
Ethylene glycol
Glycoaldehyde
CH2OHCOOH Glycolic Acid
CHOCOOH Glyoxylic Acid
Glycine + Benzoic Acid
Hippuric Acid
Oxalic Acid
Alpha-hydroxy-beta-ketoadipic acid
Thiamine 100 mg IV/day
Mg++
B6 100 mg/day
ADH
ADH
ADH
X

CH3OH
CH2O
CHOOH
CO2 + H2O
Methanol
Formaldehyde
Formic Acid
Folate
ADH
ADH
X
Case
• An 18 year old male is brought into the ED by his mother when he was difficult to wake up in the AM
• Apparently he was partying the night before, he is not able to provide a history
• He becomes progressively more obtunded while in the ED

Case
• A 22 year old frustrated medical student drinks a bottle of formaldehyde he stole from gross anatomy lab
• He complains of throat and esophageal irritation and has had multiple episodes of emesis

Case
• A 65 year old man is found comatosed
• His wife states that he has been depressed recently and has been drinking heavily
• An empty bottle of antifreeze was found in his kitchen garbage can

Case
• A 17 year old female ingests a bottle of rubbing alcohol
• She appears drunk, has multiple episodes of emesis and complain of abdominal pain

Case
• A 25 year old man presents to the ED with blurry vision
• For the past few days he has been feeling “cruddy”
• He admits to the ingestion of homemade everclear 3 days prior

Toxic alcohol Pearls
• Calcium oxalate crystals, renal failure = ethylene glycol
• “Snow field vision” = methanol• Methanol has a slower metabolism and
there may be a significant lag until the onset of symptoms
• A “normal” osmolar gap does not rule out the diagnosis

Toxic alcohol Pearls
• “ketosis without acidosis” = isopropyl alcohol
• Inhibition of alcohol dehydrogenase with fomepizole

The End
Related Documents











