CASE STUDY ON: Total Thyroidectomy

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

CASE STUDY ON:Total
Thyroidectomy

Introduction
A colloid goiter, sometimes known as a colloid nodular goiter or an endemic goiter, is a thyroid gland which has become enlarged due to a lack of iodine. Situated at the front of the neck, the thyroid gland makes thyroid hormones which regulate metabolism, affecting heart rate, temperature, digestion, energy levels and other bodily functions.

Colloid goiters occur most frequently in areas where there is little iodine in the soil. This means that food grown in the soil and then eaten by the local population is likely to be deficient in iodine.

Prevalence Rates:6.7% in 7 years old and above and
4.9% overall. In the mountainous regions, the
prevalence is as high as 90% and cretinism is said to have been reported.
It has the highest prevalence among pregnant women 13-20 years old. One out 10 pregnant women has iodine deficiency.
Prevalence Rates:
Thyroid cancer is within the list of top 10 (no. 8) cancers. It is within the top 5 (no. 5) cancers in females. It comprises about 4% of all cancers and about 5% of all cancers in females.
Reasons why we chose the case:
increase in occurrence to create an awareness to those living
in areas where there scarcity of Iodine supplement.
opportunity to learn more about the condition in order to enhance our skills and knowledge so that in the future we can render better care to our clients.

Scope And Limitation:
we only focus on our patient’s condition while he is admitted in the PACU. Due to time constraints our case study is theory-based.

Clients Profile
This is a case of Patient JC, 69-years old, female, who was admitted at Capitol University Medical City (CUMC) with a diagnosis of Multiple Colloid Goiter. She was scheduled for an operation of Total Thyroidectomy last January 5, 2011.
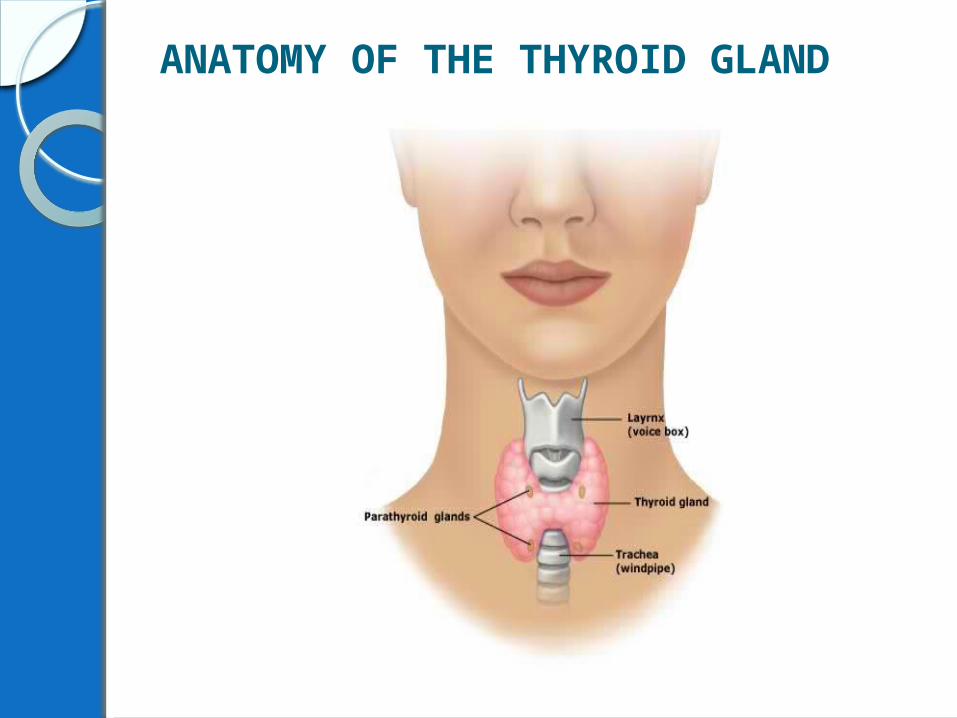
ANATOMY OF THE THYROID GLAND
The thyroid is a butterfly-shaped gland that sits low on the front of the neck. Your thyroid lies below your Adam’s apple, along the front of the windpipe. The thyroid has two side lobes, connected by a bridge (isthmus) in the middle. The thyroid is usually larger in women than men. The total weight of the thyroid is approximately 20-25 grams but is smaller in parts of the world where supplies of iodine are abundant.

The thyroid is a very vascular organ and is surrounded by a sheath. This sheath attaches the thyroid to the larynx and the trachea.
Anteriorly, the sternohyoid and sternothyroid muscles overlie each of the lobes. A pyramidal lobe is also often present and it projects upwards from the isthmus. A fibrous or muscular band frequently connects the pyramidal lobe to the hyoid bone.

Brownish-red in color, the thyroid is rich with blood vessels. Nerves important for voice quality also pass through the thyroid.

The thyroid secretes several hormones, collectively called thyroid hormones. The main hormone is thyroxine, also called T4. Thyroid hormones act throughout the body, influencing metabolism, growth and development, and body temperature. During infancy and childhood, adequate thyroid hormone is crucial for brain development.

PATHOPHYSIOLOGYLegend:
Predisposing Factors
Manifestation
Precipitating Factors
Pathophysiology
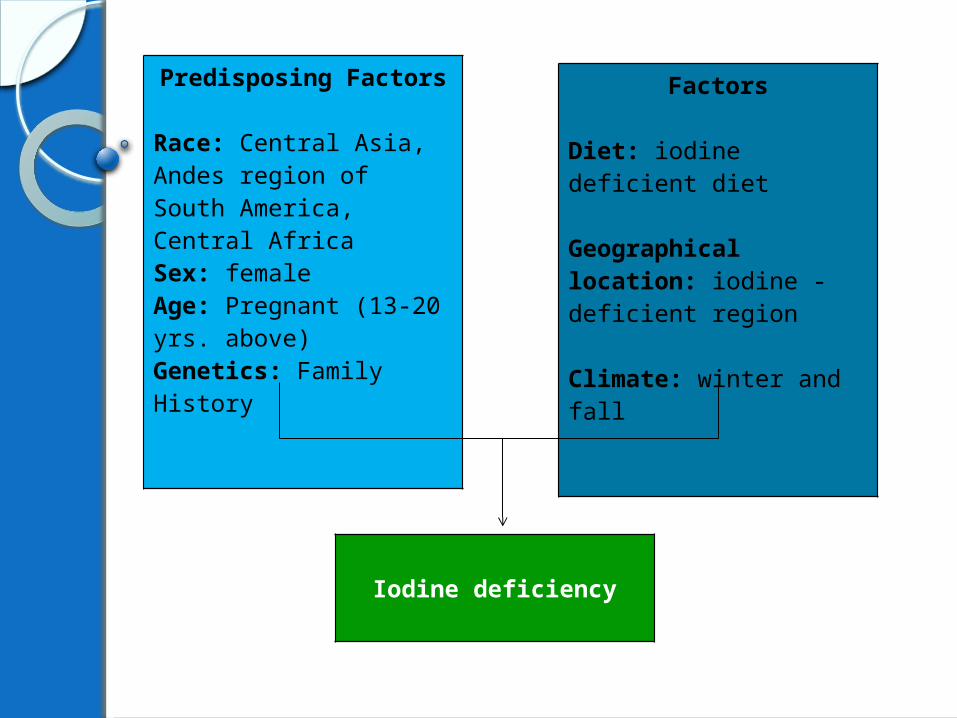
Predisposing Factors
Race: Central Asia, Andes region of South America, Central AfricaSex: femaleAge: Pregnant (13-20 yrs. above)Genetics: Family History
Factors
Diet: iodine deficient diet
Geographical location: iodine -deficient region
Climate: winter and fall
Iodine deficiency

Decreased synthesis of thyroid hormones
Increased TRH influence
Increased cellularity of the thyroid glands

Hyperplasia of the thyroid glands
Visible swelling of the neck

Operation Performed:
Total Thyroidectomy is the total surgical removal of the thyroid gland. Both sections (lobes) of the thyroid gland are removed.
Conventional Thyroidectomy In a conventional thyroidectomy, a
3- to 4-inch incision will be made through the skin in the low collar area of the neck (the lower front portion of the neck, above the collar bones and breast bone).
Next, a vertical cut will be made through the strap-like muscles located just below the skin, and these muscles will be spread aside to reveal the thyroid gland and other deeper structures.
The blood supply to the portion of the thyroid gland that is to be removed is clamped off. Then, the whole part of the thyroid gland will be cut free from surrounding tissues and removed.

During the entire procedure, the surgeon will be very careful to preserve the parathyroid glands (two pairs of small glands located near the thyroid) and to avoid damaging important nerves and blood vessels in the neck.
After your thyroid gland is removed, a drain (a soft plastic tube that drains fluid out of the area) may be placed before the incision is closed.

Then, one or two stitches will be used to bring the neck muscles together again. Then the deeper layer of your incision will be closed with stitches, and the skin will be closed with sterile paper tapes.
Following surgery, the patient will be taken to a recovery room, where he/she will be monitored for several hours until patient is stable enough to return to hospital room.
After about 24 hours, the drain will be removed from patient’s neck. Most patients go home one or two days after the surgery.

PERIOPERATIVE MANAGEMENT
Immediate Preoperative ManagementObtain and review signed informed
consent attached in the chart.Greet patient by name, and positioned
comfortably on the stretcher or bed.The patient changes into a hospital gown
that is left untied and open in the back. The patient with long hair may braid it, remove hairpins, and cover the head completely with a disposable paper cap.
PREOPERATIVE MANAGEMENT
• The mouth is inspected, and dentures or plates are removed. If left in the mouth, these items could easily fall to the back of the throat during induction of anesthesia and cause respiratory obstruction.
• Jewelry is not worn to the OR; wedding rings and jewelry of body piercings should be removed to prevent injury. All articles of value, including assistive devices, dentures, glasses, and prosthetic devices, are given to family members or are labeled clearly with the patient's name and stored in a safe and secure place according to the institution's policy.
PREOPERATIVE MANAGEMENT
All patients (except those with urologic disorders) should void immediately before going to the OR to promote continence during low abdominal surgery and to make abdominal organs more accessible. Urinary catheterization is performed in the OR as necessary.
Administering pre-anesthetic medication.Observe the patient for any untoward
reaction to the medications. The immediate surroundings are kept quiet to promote relaxation.

PREOPERATIVE MANAGEMENT
Maintaining the preoperative record. Preoperative checklists contain critical elements that must be checked and verified preoperatively and must be completed.
All wires and plugs are inspected for correct attachment. All equipments are checked.
INTRAOPERATIVE MANAGEMENT
•Identify the client, the operation to be performed (thyroidectomy), and the operative site (neck).•Position (dorsal recumbent) the client comfortably on the operating table.•Skin preparation is done along with any other procedures that must be completed (e.g. catheterization).•Gathering of additional and special supplies.

INTRAOPERATIVE MANAGEMENT
Draping and creation of sterile field. Perform “Time-Out”.Surgical counting before initial incision
is done, during the surgery, and immediately before the incision is closed.
Maintain surgical asepsis. Keep patient warm as possible.

INTRAOPERATIVE MANAGEMENT
Monitor for any emergencies.Wipe off any excess blood especially
on the neck or the operative site.Documentation of the intraoperative
care.Maintain safety in transporting the
patient.
Immediate Post-operative ManagementProper transferring and positioning on
bed from stretcher. Patient is placed in supine position.
Assessment of the ABCs and sensorium.Ensure patent airway.Reorient the patient. Maintain safety all the time. Keep all
cardio-resuscitating equipments readily available at bed side.
Monitor vital signs every 15 minutes.

Immediate Post-operative ManagementMonitor for any complications or
any signs/symptoms of shock.Administer any ordered drug
(analgesics).Promote comfort to the patient.Document all appropriate
information thoroughly.Endorse and refer patient
accordingly.

Nursing Care PlanProblem no.1Risk for aspiration related to
impaired swallowing secondary to neck surgery.
Goals:• At the end of 2 hours of nursing
interventions, the patient will be able to:Experience no aspiration as evidenced by clear breath sounds and odorless secretions.

Interventions:1. Monitor level of consciousness..
R – A decreased level of consciousness is a prime risk factor for aspiration.
2. Monitor swallowing ability.R - Choking indicates aspiration.
3. Auscultate bowel sounds to evaluate bowel motility.R - Decreased gastrointestinal motility increases the risk of aspiration because

food or fluids accumulate in the stomach. Elderly patients have a decrease in esophageal motility, which delays esophageal emptying. When combined with the weaker gag reflex of elderly patients, aspiration is a higher risk.
4. Assess for presence of nausea or vomiting.R – to be able to turn the patient to sides.
5. Keep suction setup readily available.R -- This is necessary to maintain a patent airway.

Problem no. 2Risk for ineffective breathing
pattern secondary to anesthetics side effects
Goals:Within 1-2 hours of nursing care and
intervention, the patient will be able to maintain an effective breathing pattern and show no signs of respiratory distress or hypoxia.
Nursing Care Plan
Interventions:• Maintain patent airway (by head tilt,
hyperextension, oral pharyngeal airway).
R- to prevent airway obstruction.Auscultate breath sounds and note for
any abnormalities.R- this may indicate obstruction.
Observe respiratory rate and depth, chest expansion, use of accessory muscle.R- Abnormalities of the following indicates respiratory distress.

• Monitor vital signs continuously.R- Note for any changes like increased respiration, tachycardia or bradycardia may suggest hypoxia.
Teach patient deep breathing exercises.R- to facilitate mobilization of respiratory secretions and lung expansion.
Administer supplemental oxygen as needed and indicated.

• Elevate head of the bed as appropriate to surgical procedure, if possible get patient out of bed as soon as possible. R- This promotes maximal lung expansion and decreasing risk of pulmonary complications.
Evaluation:Goals met, patient showed no signs of
hypoxia and was able to maintain an effective breathing pattern as evidenced by RR=16 and O2 saturation= 99%.

Problem no. 3Acute pain related to tissue trauma
Cues:Facial Grimacing notedHesitancy to move notedPain scale: 9/10
Goals:Within 30 minutes of nursing care and
interventions, patient will manifest decreased level of pain as evidenced by absence of facial grimace.
Interventions:Assess vital signs noting an increase of
HR, BP, and PR.R: changes in this vital signs often indicate pain and discomfort.
Evaluate pain regularly (every 15 minutes) noting characteristics, location and intensity.R: This provides information about need for effectiveness of interventions.

• Note presence of anxiety/fear and relate with and preparation for procedure.
R: Concerns about the unknown and or inadequate preparation can increase patient perception of pain.• Provide information about transitory nature
of discomfort as appropriate.R: Understanding the discomfort provides the patient emotional reassurance.
• Provide additional comfort measures (back rub, heat cold app. Etc) R: improves circulation, reduces muscle tension and anxiety associated with pain.
• Encourage use of relaxation techniques (deep breathing exercises, guided imagery, visualization, music, etc.)R: to divert attention away from pain and enhances self control and may improve coping skills.
• Administer pain medication as indicated.R: To manage pain pharmacologically
Evaluation:Goals met, after 30 minutes of nursing
care and interventions the patient was able to display absence of facial grimace.

Problem no. 4Risk for deficient fluid volume
related to blood loss during the operation.
Risk Factor:Estimated blood loss 280 mlGoals:Within 2 hours of nursing care
intervention, patient will demonstrate adequate fluid for circulation as evidenced by normal vital signs and absence of cyanosis.

Interventions:Measure and record I&O(including
tube and drains)R: Accurate documentation helps identify fluid loss/ replacement need and influences choice of interventions.
Monitor v/s noting changes in BP, HR, RR. Calculate pulse pressure.R: decrease in BP and an increase in HR and RR may indicate fluid deficit.

Monitor skin temperature and palpate peripheral pulses.R: Cool clammy skin, weak pulse indicates decreased peripheral circulation and needs for additional fluid replacement.
Administer intravenous fluids and blood products or plasma expanders as indicated.R: this helps replace fluid loss and decrease potential complications of fluid deficit (electrolyte imbalance. Dehydration, cardiovascular collapse, etc.)

• Note presence of nausea and vomiting. R: usually occurs 12-24 hrs post operatively due to side effects of anesthesia.
Administer antiemetic medications as ordered.
Evaluation:Goals met, after 8 hours of nursing
care and interventions the patient was able to demonstrate adequate fluid for circulation as evidenced by normal vital signs and absence of cyanosis
Problem no. 5Anxiety related unfamiliarity with
environment and change in health status after operation.
Cues:Increased tension notedInability to focusUneasiness notedFrequently expresses concern regarding
changes.

Goals:Within 2 hours of nursing care and
intervention, the patient will be able to report a decrease level in anxiety, acknowledge feelings and identify health ways to deal with them.

Interventions:• Provide preoperative education, discuss/demonstrate routine procedures/ process that may contribute to anxiety. (mask, lights, IV’s, electrodes, etc.) R: this provides reassurance and alleviates pt. anxiety, as well as provide information for formulating intra operative care.
Inform pt/SO if nurses intraoperative advocate role.R: develops trust/ appropriately, decreasing fear of loss control in the environment.
Introduce patient to staff at time of transfer to operating room.R: establishes trust/rapport and psychological comfort with operative team.
Control external stimuli.R: extraneous noises and commotion may increase anxiety.

Allow the patient to express her feelings and give feed back.R: this allows nurses to explore clients concern and giving feedbacks may help decrease anxiety.
Evaluation:Goals met, after 2 hrs of nursing care
and interventions the patient appeared relaxed and was able to report a decrease in anxiety.

PROGNOSIS Goiter
Results vary depending on the underlying condition. The early stages of goiter often respond well to medication (hormone therapy); a marked reduction in size or complete resolution can occur within 3 to 6 months.
When nodules are present, only about one-third of individuals see a reduction in gland size after hormone therapy. Surgery (thyroidectomy) is generally effective. Even in cases in which the goiter regresses with treatment, it may recur in months or years. Undiagnosed progressive thyroid cancer can be fatal.

ThyroidectomyThe prognosis of a thyroidectomy
is excellent, with a mortality rate of almost 0% (“Thyroidectomy”). All individuals undergoing a total thyroidectomy, and some of those undergoing a partial thyroidectomy, will require lifelong treatment with thyroid hormone replacement.

END
Related Documents











