... <;;- - ~ Community Dental Health (2005) 22, 272-278 Received 10 February 2004; Accepted 10 October 2004 @ BASCD 2005 Fluoride intake and fractionaI urinary fluoride excretion of Colombian preschooI children ÁngelaM. Francol, Alexandra Saldarriaga2, Stefanía Martignon3, María Clara González3 and Alberto E. Villa4 lAntioquia University, Medellín, Colombia; 2CES University, Medellín, Colombia; 3El Bosque University, Bogotá, Colombia; 4lnstitute of Nutrition and Food Technology, INTA, University qf' Chile Aims The purpose of this study was to assess the total fluoride intake and the fractional urinary fluoride excretion (FUFE) relative to the custornary daily fluoride (F) ingestion in preschool children between 48-59 months of age. Design Total fluoride ingestion, from dietary and toothpaste samples wa.~determined in 120 young children, dwellers of four Colombian cities. A "duplicate plate" technique was used. In Colombia, table salt is fluoridated to a concentration ofbetween 180-220 mg F/kg. Individual (n=96) FUFE values were calculated as the ratio between the total amount of F excreted in the urine and the total amount of F ingested, over a 24-hour periodo Results The average daily F-intake was 0.098 mg F/kg/day; 95% C.I. = 0.085-0.111 mg F/kg/day. The proportion of fluoride ingestion from toothpa.~te to the total fluoride intake was higher than 66% in all cities. The average FUFE values of subjects from each of the four Colombian cities under study did not differ significantly (ANOV A; p >0.91). The average 24-hour FUFE value for preschool children was 0.33; 95% CJ. =0.29-0.37. Conclusions The results obtained suggest that preschool children residing in Colombian urban areas are ingesting amounts of fluoride above the upper limit of the proposed safe threshold. FUFE values are similar to those reported in previolL~ studies where daily F-doses were equal or higher than 0.064 mg F/kg. Key words: Fluoride, fluoride intake, preschool children, urinary excretion Introduction Several reports have pointed out a sustained increase in the prevalence of dental fluorosis in industrialised coun- tries, when compared to historical data (Driscoll et al., 1983; Szpunar and Burt, 1987; Clark, 1994; Heller et al., 1997; Ismail et al., 1998; Rozier, 1999). A similar trend seems to be occurring in developing countries (Villa and Guerro, 1996; Villa et al., 1998; Villa and Guerro, 2001; República de Colombia, 1999; lrigoyen et al., 1995; Akpata et al., 1997). lt is generally accepted that the increased use of fluoridated dental products during the f¡rst years of life together with ongoing systemic fluoridated programmes can be the cause of the undesirable increase of dental fluorosis (Pendrys and Starnm, 1990; Levy, 1994; Burt, 1992; Kumar and Swango, 1999). Information regarding the proportions that different fluoride sources contribute to the total fluoride intake of pre-schoolers is essential for taking appropriate actions to minimize enamel fluorosis risk. There have been rela- tively few studies on this issue. Studies in the USA (Rojas-Sanchez et al., 1999; Levy et al., 2001) and in New-Zealand (Guha-Chowdhury et al., 1996) reported different values for the total daily fluoride intake as well as for the contributions of diet (food and beverages), toothpastes and other sources to the total fluoride inges- tion. This type of information for developing countries with established community-delivered fluoride preventive programs was available very recently (Villa et al., 2000; Martínez-Mier et al., 2003; Paiva et al., 2003). In Colombia, a salt fluoridation programme was intro- duced in 1989. The target fluoride concentration lies in the range 180-220 mg/kg salt (Kellog Foundation, 1977; República de Colombia, 1984), fluoride dietary supple- ments are not recommended and are not commercially available, fluoridated mouth rinses are not being used widely at the domestic level and their coverage in school- children programmes is small. Fluoridated toothpastes were first introduced in the country in the 1970s. However, there has been a generalised belief among Colombian public dental health officers that due to cultural and socioeconomic reasons, children belonging to the low socioeconomic status (SES) have less access to fluoridated toothpastes than children of higher SES, although this situation has not been documented. lf this assumption were correct, low SES children would have less fluoride exposure compared to high SES children On the other hand, the National Oral Health Survey carried out in 1998 showed a global prevalence of enamel fluorosis of 25.7%, in children aged 6 and 7 years (República de Colombia, 1999). The proportion ofmoder- ate and severe scores (Dean's system) in the capital city, Bogotá, was 4.5% (República de Colombia, 1999). On the other hand, the assessment of the amount of fluoride excreted in urine is the usual method of estimat- ing fluoride exposure of a population or estimating the daily fluoride intake in children (Rugg-Guun et al., 1993; Marthaler, 1995, World Health Organization, 1999; Villa et al., 2000; Báez et al., 2000; Ketley and Lennon, 2001; Haftenberger et al., 2001; Ketley et al., 2002). However, evaluation of the fractional urinary fluoride excretion (FUFE), Le. the ratio of the amount of fluoride Correspondence to: Professor Alberto E. Villa, INTA, Universidad de Chile, Casilla 138-11, Santiago, Chile. E-mail: [email protected]

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

...
<;;- - ~Community Dental Health (2005) 22, 272-278Received 10 February 2004; Accepted 10 October 2004
@ BASCD 2005
Fluoride intake and fractionaI urinary fluoride excretion ofColombian preschooI children
ÁngelaM. Francol, Alexandra Saldarriaga2, Stefanía Martignon3, María Clara González3and Alberto E. Villa4
lAntioquia University, Medellín, Colombia; 2CES University, Medellín, Colombia; 3ElBosque University, Bogotá, Colombia; 4lnstituteof Nutrition and Food Technology, INTA, University qf' Chile
Aims The purpose of this study was to assess the total fluoride intake and the fractional urinary fluoride excretion (FUFE) relativeto the custornary daily fluoride (F) ingestion in preschool children between 48-59 months of age. Design Total fluoride ingestion,from dietary and toothpaste samples wa.~determined in 120 young children, dwellers of four Colombian cities. A "duplicate plate"technique was used. In Colombia, table salt is fluoridated to a concentration ofbetween 180-220 mg F/kg. Individual (n=96) FUFEvalues were calculated as the ratio between the total amount of F excreted in the urine and the total amount of F ingested, overa 24-hour periodo Results The average daily F-intake was 0.098 mg F/kg/day; 95% C.I. =0.085-0.111 mg F/kg/day. The proportion
of fluoride ingestion from toothpa.~te to the total fluoride intake was higher than 66% in all cities. The average FUFE values ofsubjects from each of the four Colombian cities under study did not differ significantly (ANOV A; p >0.91). The average 24-hourFUFE value for preschool children was 0.33; 95% CJ. =0.29-0.37. Conclusions The results obtained suggest that preschool childrenresiding in Colombian urban areas are ingesting amounts of fluoride above the upper limit of the proposed safe threshold. FUFEvalues are similar to those reported in previolL~ studies where daily F-doses were equal or higher than 0.064 mg F/kg.
Key words: Fluoride, fluoride intake, preschool children, urinary excretion
Introduction
Several reports have pointed out a sustained increase inthe prevalence of dental fluorosis in industrialised coun-tries, when compared to historical data (Driscoll et al.,1983; Szpunar and Burt, 1987; Clark, 1994; Heller et al.,1997; Ismail et al., 1998; Rozier, 1999). A similar trendseems to be occurring in developing countries (Villa andGuerro, 1996; Villa et al., 1998; Villa and Guerro, 2001;República de Colombia, 1999; lrigoyen et al., 1995; Akpataet al., 1997). lt is generally accepted that the increaseduse of fluoridated dental products during the f¡rst yearsof life together with ongoing systemic fluoridatedprogrammes can be the cause of the undesirable increaseof dental fluorosis (Pendrys and Starnm, 1990; Levy, 1994;Burt, 1992; Kumar and Swango, 1999).
Information regarding the proportions that differentfluoride sources contribute to the total fluoride intake of
pre-schoolers is essential for taking appropriate actionsto minimize enamel fluorosis risk. There have been rela-
tively few studies on this issue. Studies in the USA(Rojas-Sanchez et al., 1999; Levy et al., 2001) and inNew-Zealand (Guha-Chowdhury et al., 1996) reporteddifferent values for the total daily fluoride intake as wellas for the contributions of diet (food and beverages),toothpastes and other sources to the total fluoride inges-tion. This type of information for developing countrieswith established community-delivered fluoride preventiveprograms was available very recently (Villa et al., 2000;Martínez-Mier et al., 2003; Paiva et al., 2003).
In Colombia, a salt fluoridation programme was intro-
duced in 1989. The target fluoride concentration lies inthe range 180-220 mg/kg salt (Kellog Foundation, 1977;República de Colombia, 1984), fluoride dietary supple-ments are not recommended and are not commerciallyavailable, fluoridated mouth rinses are not being usedwidely at the domestic level and their coverage in school-children programmes is small. Fluoridated toothpasteswere first introduced in the country in the 1970s.However, there has been a generalised belief amongColombian public dental health officers that due tocultural and socioeconomic reasons, children belongingto the low socioeconomic status (SES) have less accessto fluoridated toothpastes than children of higher SES,although this situation has not been documented. lf thisassumption were correct, low SES children would haveless fluoride exposure compared to high SES children
On the other hand, the National Oral Health Surveycarried out in 1998 showed a global prevalence of enamelfluorosis of 25.7%, in children aged 6 and 7 years(República de Colombia, 1999). The proportion ofmoder-ate and severe scores (Dean's system) in the capital city,Bogotá, was 4.5% (República de Colombia, 1999).
On the other hand, the assessment of the amount offluoride excreted in urine is the usual method of estimat-
ing fluoride exposure of a population or estimating thedaily fluoride intake in children (Rugg-Guun et al., 1993;Marthaler, 1995, World Health Organization, 1999; Villa etal., 2000; Báez et al., 2000; Ketley and Lennon, 2001;Haftenberger et al., 2001; Ketley et al., 2002).
However, evaluation of the fractional urinary fluorideexcretion (FUFE), Le. the ratio of the amount of fluoride
Correspondence to: Professor Alberto E. Villa, INTA, Universidad de Chile, Casilla 138-11, Santiago, Chile. E-mail: [email protected]

'¡:' ;;
excreted with the urine to the amount of ingested fluoridein very young children and pre-schoolers has been rela-tively scarce and results were conflicting. Previouslyreported FUPE values in pre-school children cover a widerange: from 30-35% (Ketley and Lennon, 2000; 2001; Villaet al., 1999; 2000), 51.5% (Haftenberger et al., 2001), upto 80-85% (Brunetti and Newbrun, 1983; Zohouri andRugg-Gunn, 2000). This wide variability is rather unex-pected because it has been generally accepted that ageis the main FUPE determinant (Whitford, 1990), therefore,it could be anticipated that the average FUFE values forthis age group would lie within a relatively narrow range.Very recent studies (Villa, 2004; Villa et al., 2004) how-ever, pointed out that besides age other factors such asthe inverse of the fluoride dose and the rate of fluoride
urinary excretion might influence FUFE values.The above mentioned conflicting results on the FUFE
values for pre-school children represents a drawbackwhen carrying out epidemiological studies aimed to esti-mate the total daily fluoride intake (and daily fluoridedose) in this age group through 24-hour urine collection(World Health Organization, 1999). lf there were anaccepted average FUFE value for pre-schoolers, theassessment of the 24-hour fluoride excretion on a commu-
nity basis would allow the estimation of the daily fluoridedose (Villa et al., 2000). The daily fluoride dose obtainedby dividing the 24-hour fluoride excretionlbody weightby the average FUPE value for this age group wouldfacilitate making useful comparisons with the generallyaccepted "optimal" fluoride dose: 0.05-0.07 mg F/day/kgbody weight (Burt, 1992) in order to minimise the risk ofenamel fluorosis.
In light of the facts discussed above, this study wasundertaken in order to: (i) determine the total daily fluo-ride intake by young children from four salt-fluoridatedColombian cities, considering diet (including water) andtoothpaste use; (ii) assess their fractional urinary fluorideexcretion relative to the total daily fluoride ingestion undercustomary fluoride intake conditions, and (iii) evaluatewhether the socioeconomic status has any influence onthe total fluoride exposure.
Method
Prior to initiating this study, institutional approval fromthe Bioethics Committee of the Health Sciences Institute
(CES) was obtained. The study population consisted of120, 48-59 months old healthy children with similarlow-F drinking water supplies, both genders, from lowand high socio-economic status (SES), attending eitherthe Colombian Family Well-being Day-care Centres (DCC)(low SES) or private Day-care Centres (high SES) in thecities of Bogotá, Medellín, Manizales and Cartagena. Theparents were informed of the project and gave theirconsent for their children to participate.
For the low SES the sample was probabilistic, clus-tered and stratified: probabilistic, because each child fromthe studied universe had a known selection probability;by clusters constituted by the children concentrated in alimited number of DCC, in order to reduce costs, allowingfor a slight increase in the sample error; and stratified, bythe geographical localisation of the DCC in the citiesaccording to SESo For the high SES the type of sample
was non-probabilistic (convenience), because the datacollection required high cooperation from parents, whichin light of the past and current Colombian political situ-ation is not usual in the high SES of this country.
Four cities were selected for this study. Bogotálocated at 2,600 m above the sea level, Medellín andManizales located at 1,650 and 2,800 m above sea levelrespectively and Cartagena at sea level. Fluoride concen-trations in the drinking water of these four cities are ~0.08 mgIL
In order to determine the fluoride intake from foods
and beverages through the duplicate plate technique, aduplicated sample from all of the ingested foods andbeverages, was collected over three days (two weekdaysand one weekend day). In the case of cooked meals twosimilar portions were served on two separate plates. Whenthe children finished their portion comparable amounts offood were added or removed to the "duplicate" sample.The collection was done for each participating child byauxiliary personnel in the DCC and by their parents or theperson in charge in the child's house, both with previoustraining which consisted of a demonstration of theprocedure followed by supervision of the first duplica-tion done at home. The importance of keeping thechildren's usual diet was emphasised 10the parents. Urinecollection was carried out at home on the same weekend
day mentioned above in plastic flasks, over a 24-hourperiodo The parents and care givers were trained tocollect from the second urine passed on the study dayuntil the first urine of the following day. The instructionsprovided also included the importance of accompanyingthe child, keeping the collection flask in the refrigeratorwhen not being used and avoiding the attendanceto public places that could cause incomplete urinarycollections.
In order to determine the individuals' fluoride intake
from toothpastes the following steps were followed:1) The amount of toothpaste used was assessed byweighing the toothbrush and then the toothbrush withtoothpaste; 2) the amount of fluoride in the toothpasteused was determined by micro-diffusion analysis from atoothpaste sample used by each child; 3) the amount ofnon ingested fluoride was calculated from the recoveredrinsing solution; 4) the amount of recovered fluoride wassubtracted from the amount of fluoride used; the resultwas assumed to be the ingested amount; 5) the amountingested was multiplied by the number of tooth brushingsper day in order to estimate the daily F intake from thissource. Foods, beverages and recovered toothpastesolutions collected each day were separately stored inplastic containers at -150 C. The fluoride intake for eachchild is expressed as the total amount (mg F/day) and asthe ingested amount per kg body weight (mg F/kg b.w./day).
A questionnaire in the form of a structured interviewwas completed by the children's parents or person incharge. 1t included questions on social-demographicaldata, oral hygiene habits, fluoridated toothpaste use habitsand the instructions adults have received for the chil-
dren's oral careo A pilot test was conducted prior tothestudy in order to assess the precision and validity of thequestions. Results obtained at this stage were consid-ered for the final version of the applied questionnaire.
273
~ -
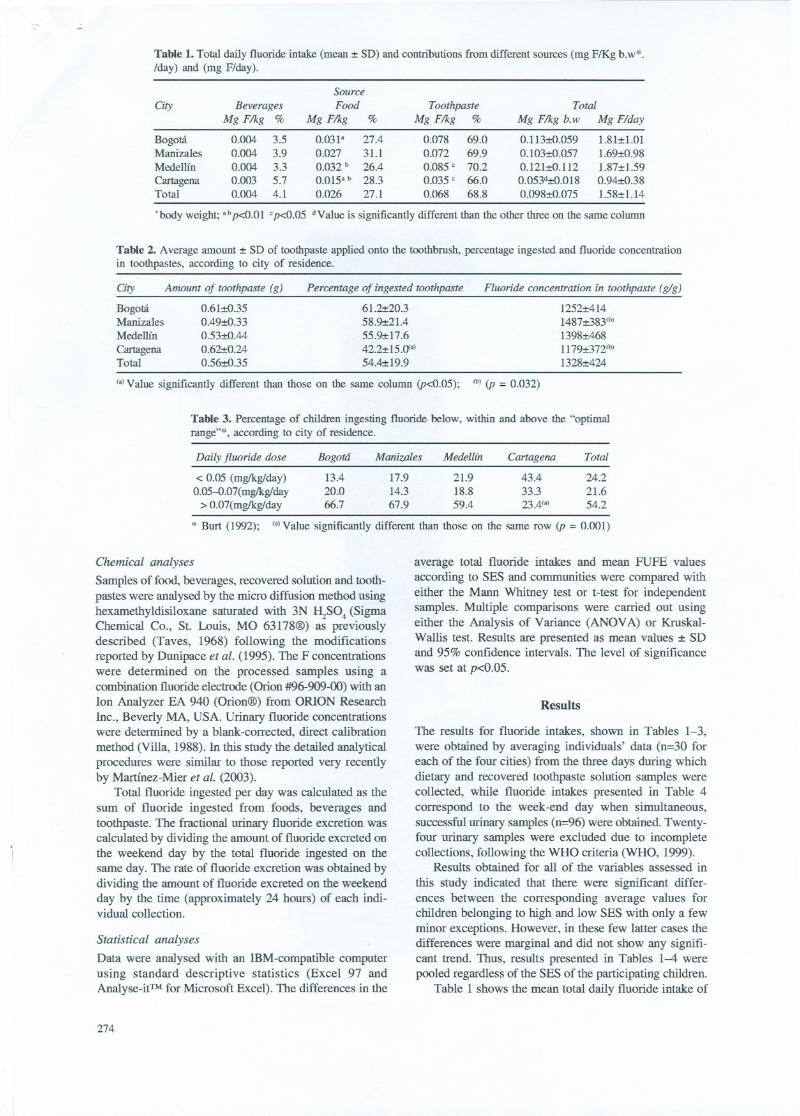
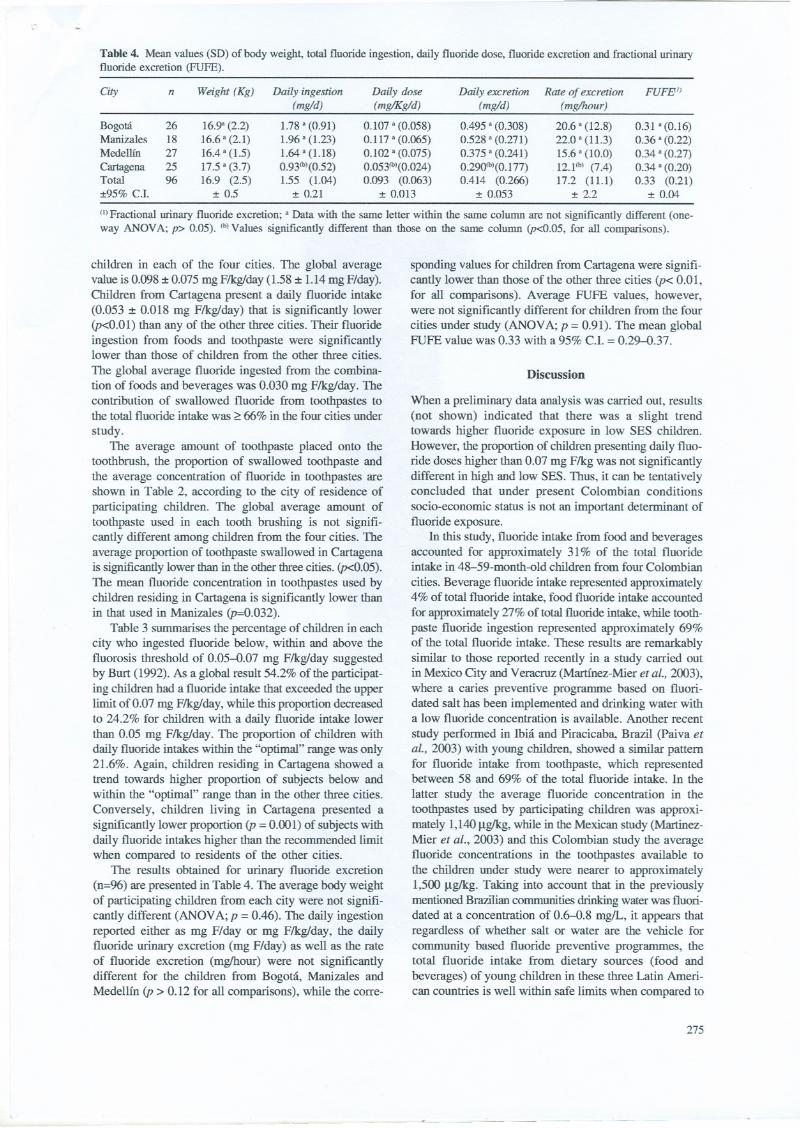
Table 1. Total daily fluoride intake (m.ean:t SD) and contributions from different sources (mg FlKg b.w*./day) and (mg F/day).
.body weight; ab p<O.OI cp<O.05 dValue is significantly different than the other three on the same column
Table 2. Average amount :t SD of toothpaste applied onto the toothbrush, percentage ingested and fluoride concentrationin toothpastes, according to city of residence.
Fluoride concentration in toothpaste (g/g)
1252:t4141487:t3831b)
1398:t4681179:t3721b)
1328:t424
(a)Value significantly different than those on the same column (p<0.05); lb)(p =0.032)
Table 3. Percentage of children ingesting fluoride below, within and above the "optimalrange"*, according to city of residence.
Chemical analy.<:es
Samples of food, beverages, recovered solution and tooth-pastes were analysed by the micro diffusion method usinghexamethyldisiloxane saturated with 3N l\S04 (SigmaChemical Co., Sto Louis, MO 63178@) as previouslydescribed (Taves, 1968) following the modificationsreported by Dunipace et al. (1995). The F concentrationswere determíned on the processed samples using acombination fluoride electrode (Orion #96-909-00) with anIon Analyzer EA 940 (Orion@) from ORlON ResearchInc., Beverly MA, USA. Urinary fluoride concentrationswere determíned by a blank-corrected, direct calibrationmethod (Villa, 1988). In this study the detailed analyticalprocedures were similar to those reported very recentIyby Martínez-Mier et al. (2003).
Total fluoride ingested per day was calculated as thesum of fluoride ingested from foods, beverages andtoothpaste. The fractional urinary fluoride excretion wascalculated by dividing the amount of fluoride excreted onthe weekend day by the total fluoride ingested on thesame day. The rate of fluoride excretion was obtained bydividing the amount of fluoride excreted on the weekendday by the time (approximately 24 hours) of each indi-vidual collection.
Statistical analyses
Data were analysed with an IBM -compatible computerusing standard descriptive statistics (Excel 97 andAnalyse-if1'Mfor Microsoft Excel). The differences in the
274
average total fluoride intakes and mean FUFE valuesaccording to SES and communities were compared witheither the Mann Whitney test or t-test for independentsamples. Multiple comparisons were carried out usingeither the Analysis of Yariance (ANOY A) or Kruskal-Wallis test. Results are presented as mean values :t SDand 95% confidence intervals. The level of significancewas set at p<0.05.
Results
The results for fluoride intakes, shown in Tables 1-3,were obtained by averaging individuals' data (n=30 foreach of the four cities) from the three days during whichdietary and recovered toothpaste solution samples werecollected, while fluoride intakes presented in Table 4correspond to the week -end day when simultaneous,successful urinary samples (n=96) were obtained. Twenty-four urinary samples were excluded due to incompletecollections, following the WHO criteria (WHO, 1999).
Results obtained for a1l of the variables assessed in
this study indicated that there were significant differ-ences between the corresponding average values forchildren belonging to high and low SES with only a fewminor exceptions. However, in these few latter cases thedifferences were marginal and did not show any signifi-cant trend. Thus, results presented in Tables 1-4 werepooled regardless of the SES of the participating children.
Table 1 shows the mean total daily fluoride intake of
SaurceCiry Beverages Food Toothpaste Total
Mg F/kg % Mg F/kg % Mg F/kg % Mg F/kg b.w Mg F/day
Bogotá 0.004 3.5 0.031" 27.4 0.078 69.0 0.113:tO.059 1.81:t1.01Manizales 0.004 3.9 0.027 31.1 0.072 69.9 0.103:tO.057 1.69:tO.98Medellín 0.004 3.3 0.032b 26.4 0.085 e 70.2 0.121:tO.112 1.87:t1.59Cartagena 0.003 5.7 0.015ab 28.3 0.035e 66.0 0.053d:tO.0l8 0.94:tO.38Total 0.004 4.1 0.026 27.1 0.068 68.8 0.098:tO.075 1.58:t1.14
Ciry Amount 01 toothpaste (g) Percentage of ingested toothpaste
Bogotá 0.61:tO.35 61.2:t20.3Manizales 0.49:t0.33 58.9:t21.4Medellín 0.53:tO.44 55.9:t17.6
Cartagena 0.62:t0.24 42.2:t15.<ya)Total 0.56:tO.35 54.4:t19.9
Daily fluoride dose Bogotá Manizales Medellín Cartagena Total
< 0.05 (mgikg/day) 13.4 17.9 21.9 43.4 24.20.05-O.07(mglkg/day 20.0 14.3 18.8 33.3 21.6
> 0.07(mgikg/day 66.7 67.9 59.4 23.4fa) 54.2
* Burt (1992); fa)Value significantly different than those on the same row (p =0.001)
-
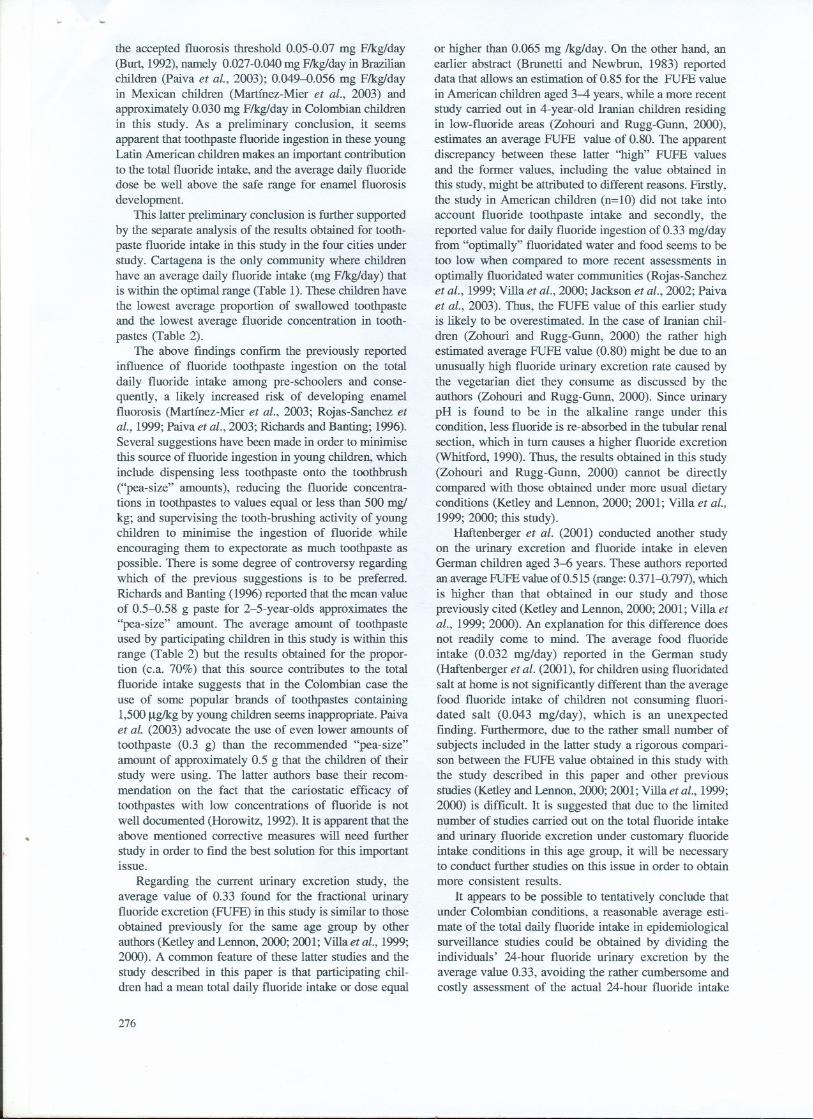
Table 4. Mean vaIues (SD) ofbody weight, total fIuoride ingestion, daily fIuoride dose, fIuoride excretion and fractionaI urinaryfIuoride excretion (FUFE).
Weight (Kg) FUFE1)City n Daily ingestion(mgld)
1.78 a (0.91)1.96 a (1.23)1.64 a (1.18)0.93(b)(0.52)1.55 (1.04)
:!: 0.21
Daily dose(mgIKgld)
0.107 a (0.058)
0.117 a (0.065)
0.102 a (0.075)
0.053(b)(0.024)
0.093 (0.063):!: 0.013
Rate of excretion(mglhour)
20.6 a (12.8)22.0 a (11.3)15.6 a (10.0)12.1(b) (7.4)
17.2 (11.1):!: 2.2
BogotáManizaIesMedellin
CartagenaTotal:!:95% CJ.
2618272596
16.9" (2.2)16.6 a (2.1)16.4 a(1.5)17.5 a (3.7)16.9 (2.5)
:!: 0.5
Daily excretion(mgld)
0.495 a (0.308)
0.528 a (0.271)
0.375 a (0.241)
0.29()tb)(0.177)
0.414 (0.266):!: 0.053
0.31 a (0.16)
0.36 a (0.22)
0.34 a (0.27)
0.34 a (0.20)
0.33 (0.21):!: 0.04
(I)FractionaI urinary fIuoride excretion; a Data with the same letter within the same column are not significantly different (one-way ANOV A; p> 0.05). (b)VaIues significantly different than those on the same column (p<O.05, for aIl comparisons).
children in each of the four cities. The global averagevalue is 0.098:!: 0.075 mg Flkg/day (1.58 :!:1.14 mg F/day).Children from Cartagena present a daily fluoride intake(0.053 :!: 0.018 mg F/kglday) that is significantly lower(p<0.01) than any of the other three cities. Their fluorideingestion from foods and toothpaste were significantlylower than those of children from the other three cities.
The global average fluoride ingested from the combina-tion of foods and beverages was 0.030 mg F/kglday. Thecontribution of swallowed fluoride from toothpastes tothe total fluoride intake was ~ 66% in the four cities under
study.The average amount of toothpaste placed onto the
toothbrush, the proportion of swallowed toothpaste andthe average concentration of fluoride in toothpastes areshown in Table 2, according to the city of residence ofparticipating children. The global average amount oftoothpaste used in each tooth brushing is not signifi-cantly different among children from the four cities. Theaverage proportion of toothpaste swallowed in Cartagenais significantly lower than in the other three cities. (p<O.05).The mean fluoride concentration in toothpastes used bychildren residing in Cartagena is significantly lower thanin that used in Manizales (p=O.032).
Table 3 surnmarises the percentage of children in eachcity who ingested fluoride below, within and above thefluorosis threshold of 0.05-0.07 mg F/kglday suggestedby Burt (1992). As a global result 54.2% of the participat-ing children had a fluoride intake that exceeded the upperlimit ofO.07 mg F/kglday, while this proportion decreasedto 24.2% for children with a daily fluoride intake lowerthan 0.05 mg F/kglday. The proportion of children withdaily fluoride intakes within the "optimal" range was only21.6%. Again, children residing in Cartagena showed atrend towards higher proportion of subjects below andwithin the "optimal" range than in the other three cities.Conversely, children living in Cartagena presented asignificantly lower proportion (p =0.001) of subjects with
daily fluoride intakes higher than the recommended limitwhen compared to residents of the other cities.
The results obtained for urinary fluoride excretion(n=96) are presented in Table 4. The average body weightof participating children from each city were not signifi-cantly different (ANOY A; p =0.46). The daily ingestionreported either as mg F/day or mg F/kglday, the dailyfluoride urinary excretion (mg F/day) as well as the rateof fluoride excretion (mglhour) were not significantlydifferent for the children from Bogotá. Manizales andMedellín (p > 0.12 for all comparisons), while the corre-
sponding values for children from Cartagena were signifi-cantly lower than those of the other three cities (p< 0.01,for a11comparisons). Average FUFE values, however,werenot significantly different for children from the fourcities under study (ANOY A; p = 0.91). The mean globalFUFE value was 0.33 with a 95% Cl. = 0.29-0.37.
Discussion
When a preliminary data anaIysis was carried out, results(not shown) indicated that there was a slight trendtowards higher fluoride exposure in low SES children.However, the proportion of children presenting daily fluo-ride doses higher than 0.07 mg F/kg was not significantlydifferent in high and low SES. Thus, it can be tentativelyconcluded that under present Colombian conditionssocio-economic status is not an important determinant offluoride exposure.
In this study, fluoride intake from food and beveragesaccounted for approxirnately 31% of the total fluorideintake in 48-59-month-old children from four Colombian
cities. Beverage fluoride intake represented approxirnately4% of total fluoride intake, food fluoride intake accountedfor approxirnately 27% of total fluoride intake, while tooth-paste fluoride ingestion represented approximately 69%of the total fluoride intake. These results are remarkablysimilar to those reported recently in a study carried outin Mexico City and Yeracruz (Martínez-Mier et al., 2003),where a caries preventive programme based on fluori-dated salt has been implemented and drinking water witha low fluoride concentration is available. Another recent
study performed in Ibiá and Piracicaba, Brazil (Paiva etal., 2003) with young children, showed a similar pattemfor fluoride intake from toothpaste, which representedbetween 58 and 69% of the total fluoride intake. In the
latter study the average fluoride concentration in thetoothpastes used by participating children was approxi-mately 1,140 11g/kg,while in the Mexican stndy (Martinez-Mier et al., 2003) and this Colombian stndy the averagefluoride concentrations in the toothpastes available tothe children under stndy were nearer to approximately1,500 I1g/kg. Taking inlo account that in the previouslymentioned Brazilian communities drinking water was fluori-dated at a concentration of 0.6-0.8 mg/L, it appears thatregardless of whether salt or water are the vehicle forcommunity based fluoride preventive programmes, fuetotal fluoride intake from dietary sources (food andbeverages) of young children in these three Latin Ameri-can countries is well within safe limits when compared to
275
~-~-- ~
\.o
the accepted fluorosis threshold 0.05-0.07 mg F/kg/day(Burt, 1992), namely 0.027-0.040 mg F/kg/day in Brazilianchildren (Paiva et al., 2003); 0.049-0.056 mg F/kg/dayin Mexican children (Martínez-Mier et al., 2003) andapproximately 0.030 mg F/kg/day in Colombian childrenin this study. As a preliminary conclusion, it seemsapparent that toothpaste fluoride ingestion in these youngLatin American children makes an important contributionto the total fluoride intake, and the average daily fluoridedose be well above the safe range for enamel fluorosisdevelopment.
This latter preliminary conclusion is further supportedby the separate analysis of the results obtained for tooth-paste fluoride intake in this study in the four cities understudy. Cartagena is the only community where childrenhave an average daily fluoride intake (mg F/kg/day) thatis within the optimal range (Table 1). These children havethe lowest average proportion of swallowed toothpasteand the lowest average fluoride concentration in tooth-pastes (Table 2).
The above findings confl.I111the previously reportedinfluence of fluoride toofupaste ingestion on the totaldaily fluoride intake among pre-schoolers and conse-quently, a likely increased risk of developing enamelfluorosis (Martínez-Mier et al., 2003; Rojas-Sanchez etal., 1999; Paiva et al., 2003; Richards and Banting; 1996).Several suggestions have been made in order to minimisethis source of fluoride ingestion in young children. whichinclude dispensing less toothpaste onto the toothbrush("pea-size" amounts), reducing the fluoride concentra-tions in toothpastes to values equal or less than 500 mg/kg; and supervising the tooth-brushing activity of youngchildren to minimise the ingestion of fluoride whileencouraging them to expectorate as much toothpaste aspossible. There.is some degree of controversy regardingwhich of the previous suggestions is to be preferred.Richards and Banting (1996) reported that the mean valueof 0.5-0.58 g paste for 2-5-year-olds approximates the"pea-size" amount. The average amount of toothpasteused by participating children in this study is within thisrange (Table 2) but the results obtained for the propor-tion (c.a. 70%) that this source contributes to the totalfluoride intake suggests that in the Colombian case theuse of some popular brands of toothpastes containing1,500 f..lg/kgby young children seems inappropriate. Paivaet al. (2003) advocate the use of even lower amounts oftoothpaste (0.3 g) than the recommended "pea-size"amount of approximately 0.5 g that the children of theirstudy were using. The latter authors base their recom-mendation on the fact that the carioslatic efficacy oftoothpastes with low concentrations of fluoride is notwell documented (Horowitz, 1992). 1t is apparent that theabove mentioned corrective measures will need further
study in order to find the best solution for this importantissue.
Regarding the current urinary excretion study, theaverage value of 0.33 found for the fractional urinaryfluoride excretion (FUFE) in this study is similar to thoseobtained previously for the same age group by otherauthors (Ketley and Lennon, 2000; 2001; Villa et al., 1999;2000). A common feature of these latter studies and thestudy described in this paper is that participating chil-dren had a mean total daily fluoride intake or dose equal
276
or higher than 0.065 mg /kg/day. On the other hand, anearlier abstract (Brunetti and Newbrun, 1983) reporteddata that allows an estimation of 0.85 for the FUFE value
in American children aged 3-4 years, while a more recentstudy carried out in 4-year-old lranian children residingin low-fluoride areas (Zohouri and Rugg-Gunn, 2000),estimates an average FUFE value of 0.80. The apparentdiscrepancy between these latter ''high'' FUFE valuesand the former values, including the value obtained inthis study, might be attributed to different reasons. Firstly,the study in American children (n=lO) did not take intoaccount fluoride toothpaste intake and secondly, thereported value for daily fluoride ingestion of 0.33 mg/dayfrom "optimally" fluoridated water and food seems to betoo low when compared to more recent assessments inoptimally fluoridated water communities (Rojas-Sanchezet al., 1999; Villa et al., 2000; Jackson et al., 2002; Paivaet al., 2003). Thus, the FUFE value of this earlier studyis likely to be overestimated. In the case of Iranian chil-dren (Zohouri and Rugg-Gunn, 2000) the rather highestimated average FUFE value (0.80) might be due to anunusually high fluoride urinary excretion rate caused bythe vegetarian diet they consume as discussed by theauthors (Zohouri and Rugg-Gunn, 2000). Since urinarypH is found to be in the alkaline range under thiscondition, less fluoride is re-absorbed in the tubular renalsection, which in tum causes a higher fluoride excretion(Whitford, 1990). Thus, the results obtained in this study(Zohouri and Rugg-Gunn, 2000) cannot be directlycompared with those obtained under more usual dietaryconditions (Ketley and Lennon, 2000; 2001; Villa et al.,1999; 2000; this study).
Haftenberger et al. (2001) conducted another studyon the urinary excretion and fluoride intake in elevenGerman children aged 3-6 years. These authors reportedan average FUFE value of 0.515 (range: 0.371-0.797), whichis higher than that obtained in our study and thosepreviously cited (Ketley and Lennon, 2000; 2001; Villa etal., 1999; 2000). An explanation for this difference doesnot readily come to mind. The average food fluorideintake (0.032 mg/day) reported in the German study(Haftenberger et al. (2001), for children using fluoridatedsalt at home is not significantly different than the averagefood fluoride intake of children not consuming fluori-dated salt (Q.043 mg/day), which is an unexpectedfinding. Furthermore, due to the rather small number ofsubjects included in the latter study a rigorous compari-son between the FUFE value obtained in this study withthe study described in this paper and other previousstudies (Ketley and Lennon, 2000; 2001; Villa et al., 1999;2000) is difficult. 1t is suggested that due to the limitednumber of studies carried out on the total fluoride intake
and urinary fluoride excretion under customary fluorideintake conditions in this age group, it will be necessaryto conduct further studies on this issue in order to obtainmore consistent results.
1t appears to be possible to tentatively conclude thatunder Colombian conditions, a reasonable average esti-mate of the total daily fluoride intake in epidemiologicalsurveillance studies could be obtained by dividing theindividuals' 24-hour fluoride urinary excretion by theaverage value 0.33, avoiding the rather cumbersome andcostly assessment of the actual 24-hour fluoride intake
'" '-'
from food, beverages, swallowed toothpaste, and anyother potential fluoride source.
The general features of fluoride (F) metabolism havebeen well described (Whitford, 1990). lt is generallyaccepted that F absorption is relatively high, accountingfor about 90% of total F intake (Ek:strand, 1996), whilefaecal excretion roughly amounts to 10% of F intake(Ek:strand, 1996). Two metabolic pathways are recognizedas the main factors that determine plasma F clearance,namely calcified tissue F retention and urinary F excretion(Whitford, 1990). Since the assessment of the amount offluoride retained in hard tissue is obviously difficult, theamount of fluoride excreted with the urine has beenconsidered a useful estimator of recent fluoride intake
(Marthaler et al., 1995). However, experimental conditionsfor urine collection are not standardised.
1n order to support the epidemiological surveillanceof community based fluoride preventive programmes theWorld Health Organization has recentIy published a help-fuI manual (WHO, 1999) that provides general guidelineson the different time-controlled urinary collection meth-ods and provisional standards for the ranges of amountand rate of 24-hour fluoride excretion that can be consid-
ered "optimal" in children.lt is interesting to compare our and others' results
with the values proposed in the above mentioned guide-lines on renal fluoride excretion in epidemiologicalsurveillance published by WHO (WHO, 1999). The WHOguidelines propose that an optimal range of daily fluorideurinary excretion for children aged 3-5 years would lie inthe 0.36-0.48 mg/day interval, and for 6-7-year-olds theproposed range is 0.48-0.60 mg/day. 1n a previous study(Villa et al., 2000), an average daily fluoride excretion of0.35 mg/day, which is slightIy below the lower limit
References
Akpata,E.s., Fakiha,Z. and Khan,N. (1997):DentalFluorosisin 12-15year-old rural children exposed to fluoride fromwell drinking water in the Haill region of Saudi Arabia.CommunityDentistryand Oral Epidemiology25,324--327.
Báez, RJ., Báez M.x. and Marthaler, T. M. (2000): Urinaryfluoride excretion by children 4-6 years old in a SouthTexas community.PanAmerican Journal of Public Health7, 242-248.
Brunetti, A. and Newbrun, E. (1983):Fluoride balance of chil-dren 3 and 4 years-old. Caries Research 17, 171 (abstract41).
Burt, B.A. (1992): The changingpatterns of systemic fluorideintake. Journal of Dental Research 71, 1228-1237.
Clark, D.C. (1994):Trends in prevalenceof dental fluorosis inNorth America.CommunityDentistryand Oral Epidemiol-ogy 22, 148-152.
Driscoll, W.S., Horowitz, H.S, Meyers, RJ., Heifetz, S.B.,Kingman. A. and ZimmermanE.R. (1983): Prevalence ofdental caries and dental fluorosis in area.~with optimal andabove-optimal water fluoride concentrations in drinkingwater.JournalofAmerican DentalAssociation 107,47-53.
Dunipace, A.J., Brizendine, EJ., Zhang, W., Wilson, M.E.,Miller, L., Katz, B.P., et al. (1995): Effect of aging onanimal response to chronic fluoride exposure. Journal ofDental Research 74, 358-368.
Ekstrand, J. (1996):Fluoride metabolismoIn: Fluoride in Den-tistry, 2ndedn.; eds. Fejerskov, O., Ekstrand, J. and Burt,B. Chapter 4..Copenhagen,Munksgaard;.
Guha-Chowdhury, N., Drummond, B.K. and Smillie, A.C.
proposed in the WHO guidelines, was found for pre-school children presenting an average daily fluoride doseof 0.064 mglkg/day. 1n the present study, an averagevalue for the daily fluoride urinary excretion of 0.414 mg/day was obtained. This value that lies in the "optimalrange" according to the WHO guidelines is connectedhowever, with an experimentally determined average dailyfluoride dose (0.093 mglkg/day), which is above therecommended safe threshold: 0.05-0.07 mglkg/day (Burt,1992). By contrast, the lranian children studied by Zohouriand Rugg-Gunn (2000), showed an average daily fluorideurinary excretion of 0.339 mg/day, which would almostcorrespond to an optimal fluoride intake according to theWHO proposed standards, while their actual fluorideingestion (0.426 mg/day or 0.028 mglkg/day) is well belowthe accepted range.
The above discussion illustrates the difficulties that
are currently associated with the relationship betweenthe optimal daily fluoride intake and the urinary fluorideexcretion among young children who might be at risk ofdeveloping enamel fluorosis. Considering the importanceof this subject on fluoride metabolism of young humansand on epidemiological surveillance of caries preventivefluoride programmes all over the world, it is clear thatadditional studies of this kind under different and
well controlled customary fluoride customary exposureconditions are needed in order to refine the currentlyrecommended standards.
Acknowledgements
We wish to thank the Colombian Association of Dental
Schools and Faculties for their support and Mr. GonzaloAlvarez for his statistical analyses.
(19%): Total fluoride intake in children aged 3-4 years -a longitudinal study. Journal (){Dental Research 69, 1828-1833.
Haftenberger, M., Viergutz, G., Neumeister, V. and Hetzer, G.(2001): Total fluoride intake and urinary excretion in Ger-man children aged ~ years. Caries Research 35, 451-457.
Heller, K.E., Eklund, S.A. and Burt, B.A. (1997): Dental cariesand dental fluorosis at varying water fluoride concentra-tions. Journal (){Public Health Dentistry 57, 136-143.
Horowitz, H.S. (1992): The needs for toothpa~tes with lowerthan conventional fluoride concentrations for pre-schoolaged children. Joumal (){Public Health Dentistry 52,216-221.
Irigoyen, M.E., Molina, N. and Luenga.~, 1. (1995): Prevalenceand severity of dental fluorosis in a Mexican communitywith above optimal fluoride concentration in Drinking water.Community Dentistry and Oral Epidemiology 23, 243-245.
Ismail, AJ., Messer, J.G. and Hornett, PJ. (1998): Prevalenceof dental caries and fluorosis in 7- to 12-year-old childrenin Northern Newfoundland and Forteau, Labrador. Cana-dian Dental Association Journal 64, 118-124.
Jacks(m, R.D., Brizendine, E.J., Kelly, S.A., Hinesly, R.,Stookey, G.K. and Dunipace, A.J. (2002): The fluoridecontent of food~ and beverages from negligibly and optimallyfluoridated communities. Community Dentistry and OralEpidemiology 30, 382-391.
KelIog Foundation (1977): Salt Fluoridation: An alternative forthe prevention of dental caries. lnternational Symposium on
277
'"~ .;;
1
,\
.....
salt fluoridation. Medellín, Colombia 1977. A Summaryreport.
Ketley, C.E. and Lennon, M.A. (2000): Urinary fluoride excre-tion in chi1dren drinking fluoridated schoo1 milk. [ntema-tional Joumal ol Paediatric Dentistry 10, 260-270.
Ketley, C.E. and Lennon, MA (2001): Determination of fluo-ride intake from urinary fluoride excretion data in chi1drendrinking fluoridated schoo1 mi1k. Caries Research 35, 252-257.
Ketley, C. E., Cochran, J. A., Lennon, M. A., O'Mullane, D.M. and Worthington, H. W. (2002): Urinary fluoride excre-tion of young children exposed to different fluoride regimes.Caries Research 19, 12-17.
Kumar, J.V. and Swango, P.A. (1999): Fluoride exposure anddental fluorosis in Newburgh and Kingston, New York:Po1icy Imp1ications. Community Dentistry and Oral Epide-miology 27, 171-180.
Levy, SM. (1994): Review offluoride exposures and ingestion.Community Dentistry and Oral Epidemiology 22,173-180.
Levy, SM., Warren J.J., Davis, C.S., Kirchner, L., Kanellis,M.J. and Wefe1, J.S. (2001): Patterns of fluoride intakefrom birth to 36 months. Joumal qlPublic Health Dentistry61, 70-77.
Marthaler, TM., Steiner, M., Menghini, G. and De Crousaz,P. (1995): Urinary fluoride excretion in chi1dren with 10wfluoride intake or consuming fluoridated salt. Caries Re-search 29, 26-34.
Martínez-Mier, E.A., Soto-Rojas, A.E., Ureña-Cirett, J.L.,Stookey, G.K and Dunipace, A.J. (2003): Fluoride intakefrom foods, beverages and toothpaste by chi1dren in Mexico.Community Dentistry and Oral Epidemiology 31, 221-230.
Paiva, S.M., Lima, Y.B.O. and Cury, J.A. (2003): Fluorideintake by Brazi1ian chi1dren from two communities withfluoridated water. Community Dentistry and Oral Epidemi-ology 31, 184-191.
Pendrys, D.G. and Stamm, J.W. (1990): Relationship of totalfluoride intake to beneficial effects and ename1 fluorosis.
Joumal ol Dental Research 69, 529-538.República de Colombia. Ministerio de Salud (1999): III Estudio
Nacional de Salud Bucal. Serie Documentos Técnicos Tomo
VII. Ministerio de Salud. Bogotá, 1999.República de Colombia (1984): Ministerio de Salud. Decreto
2024 de 1984.
Richards, A. and Banting, D.W. (1996): Fluoride metabolism.In: Fluoride in Dentistry, 2nd edn.; eds. Fejerskov, O.,Ekstrand, J. and Burt, B. Chapter 18. Copenhagen,Munksgaard;.
Rojas-Sánchez, F., Kelly, S.A., Drake, KM., Eckert, G.J,Stookey, G.K and Dunipace, A.J. (1999): Fluoride intakefrom foods, beverages and toothpaste by young chi1dren incommunities with neg1igib1eand optimal1y fluoridated wa-ter: a pi10t study. Community Dentistry and Oral Epidemi-ology 27, 288-297.
278
Rozier, G. (1999): The prevalence and severity of ename1fluorosis in North American chi1dren.Joumal ol PublicHealth Dentistry 59, 239-246.
Rugg-Gunn, A.J., Nunn, J.H., Ekanayake, L., Saparamadu,KD.G. and Wright, W.G. (1993): Urinary fluoride excre-tion in 4-year-01dchi1drenin Sri-Lankaand Eng1and.CariesResearch 27, 478-483.
Szpunar,S.M. and Burt, B.A. (1987):Trends in the prevalenceof dental fluorosis in the United States. Joumal ol PublicHealth Dentistry 47, 71-79.
Taves, D.R. (1968): Separation of fluoride by rapid diffusionusing hexamethy1disi10xane.Talanta 15, 969-974.
Villa, A.E. (1988): Rapid method for determining very 10wfluoride concentrations using an ion-se1ective e1ectrode.Analyst 113, 1299-1303.
Villa, A.E. and Guerrero, S. (1996): Caries experience andfluorosisprevalencein Chileanchildrenfromdifferentsocio-economic status. CommunityDentistry and Oral Epidemi-ology 24, 225-227.
Villa,A.E., Guerrero,S., !caza,G., Villalobos,J. and Anabalón,M. (1998): Dental fluorosis in Chi1eanChi1dren: Evalua-tion of Risk factors. Community Dentistryand Oral Epi-demiology 26, 310-315.
Villa, AE., Salazar,G., Anabalón,M. and Cabezas,L. (1999):Estimation of the fraction of an ingested dose of fluorideexcreted through urine in pre-schoo1chi1dren.CommunityDentistry and Oral Epidemiology 27, 305-312.
Villa, A.E., Anabalón, M. and Cabezas, L (2000): The frac-tional urinary fluoride excretion in young chi1drenunderstable fluoride intakeconditions.CommunityDentistryandOral Epidemiology 28, 344-355.
Villa, A.E. and Guerrero, S. (2001): Assessment of the effec-tiveness of water fluoridation in the Macu1District, San-tiago, Chile [In Spanish]. Odontología Chilena 49, 3-12.
Villa, A. E. (2004): Critical evaluationof previous1ypublisheddata on the fractional urinary fluoride excretion in youngchi1dren.Community Dental Health 21, 155-169.
Villa, A. E., Cabezas, L., Anabalon,M. and Garza, E. (2004):The fractionalurinary fluorideexcretionof ado1escentsandadults Ander customary fluoride intake conditions, in acommunitywith 0.6-mg F/L in its drinking water. Commu-nity Dental Health 21, 11-18.
Whitford, G.M. (1990): The physio10gicaland toxico10gicalcharacteristicsof fluoride. Joumal ol Dental Research 69(Spec Issue), 539-549.
Wor1dHealthOrganization(1999):Monitoring~lrenalfluorideexcretion in community preventive programmes on oralhealth. Ed. Marthaler,T.M. Geneva:World Hea1thOrgani-zation.
Zohouri, F.v. and Rugg-Gunn,A.J. (2000): Total fluoride in-take and urinary excretion in 4-year-01dIranian chi1drenresiding in 10w-fluorideareas. British Joumal ql Nutrition83, 15-25.
Related Documents