Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
-
TOBACCO CONTROLCOUNTRY PROFILES
-
The Tobacco Control Country Profiles is an initiative of the 11th World Conference on Tobacco OR Health.
Funding from SmithKline Beecham Consumer Healthcare andthe American Cancer Society supported the development of
the monograph. The World Health Organization and the Centers for Disease Control and Prevention provided, in kind, data and
personnel resources to the project.
-
TOBACCO CONTROLCOUNTRY PROFILES
The 11th World Conference on Tobacco OR Health
Editors:
Marlo Ann CorraoG. Emmanuel Guindon
Namita SharmaDorna Fakhrabadi Shokoohi
The American Cancer Society, Inc.Atlanta, Georgia
-
COPYRIGHT WAIVERBecause the Tobacco Control Country Profiles is intended to serve as a
reference book and a resource for tobacco control advocates, any part of the book may be reproduced without seeking copyright permission
from the editors or the American Cancer Society; citation as to source,however, is appreciated.
Suggested citation:Corrao MA, Guindon GE, Sharma N, Shokoohi DF (eds). Tobacco Control
Country Profiles, American Cancer Society, Atlanta, GA, 2000.
-
1
Foreword 3
Acknowledgments 4
Introduction 5
Methods 7
Regional SummariesAfrican Region 23Region of the Americas 27Eastern Mediterranean Region 30European Region 32South-East Asia Region 36Western Pacific Region 40
Regional MapsAfrican Region Plate 1Region of the Americas Plate 2Eastern Mediterranean Region Plate 3European Region Plate 4South-East Asia Region Plate 5Western Pacific Region Plate 6
Country and Territory ProfilesAfrican Region: 46–137Algeria, Angola, Benin, Botswana, Burkina Faso, Burundi, Cameroon, Cape Verde, Central African Republic, Chad, Comoros, Congo, Côte d’Ivoire, Democratic Republic of theCongo, Equatorial Guinea, Eritrea, Ethiopia, Gabon, Gambia, Ghana, Guinea, Guinea-Bissau,Kenya, Lesotho, Liberia, Madagascar, Malawi, Mali, Mauritania, Mauritius, Mozambique,Namibia, Niger, Nigeria, Rwanda, Sao Tome and Principe, Senegal, Seychelles, Sierra Leone,South Africa, Swaziland, Togo, Uganda, United Republic of Tanzania, Zambia, Zimbabwe
Region of the Americas: 138-209Antigua and Barbuda, Argentina, Bahamas, Barbados, Belize, Bolivia, Brazil, Canada, Chile,Colombia, Costa Rica, Cuba, Dominica, Dominican Republic, Ecuador, El Salvador, Grenada,Guatemala, Guyana, Haiti, Honduras, Jamaica, Mexico, Nicaragua, Panama, Paraguay, Peru, Puerto Rico (associate Member State), Saint Kitts and Nevis, Saint Lucia, Saint Vincent andthe Grenadines, Suriname, Trinidad and Tobago, United States of America, Uruguay, Venezuela (Bolivarian Republic of)
Table of Contents
-
2
Eastern Mediterranean Region: 210–255Afghanistan, Bahrain, Cyprus, Djibouti, Egypt, Iran (Islamic Republic of), Iraq, Jordan, Kuwait,Lebanon, Libyan Arab Jamahiriya, Morocco, Oman, Pakistan, Qatar, Saudi Arabia, Somalia,Sudan, Syrian Arab Republic, Tunisia, United Arab Emirates, Yemen, West Bank and Gaza Strip
European Region: 256–357Albania, Andorra, Armenia, Austria, Azerbaijan, Belarus, Belgium, Bosnia and Herzegovina, Bulgaria, Croatia, Czech Republic, Denmark, Estonia, Finland, France, Georgia, Germany,Greece, Hungary, Iceland, Ireland, Israel, Italy, Kazakhstan, Kyrgyzstan, Latvia, Lithuania,Luxembourg, Malta, Monaco, Netherlands, Norway, Poland, Portugal, Republic of Moldova,Romania, Russian Federation, San Marino, Slovakia, Slovenia, Spain, Sweden, Switzerland,Tajikistan, Turkey, The former Yugoslav Republic of Macedonia, Turkmenistan, Ukraine, United Kingdom of Great Britain and Northern Ireland, Uzbekistan, Yugoslavia
South-East Asia Region: 358–377Bangladesh, Bhutan, Democratic People’s Republic of Korea, India, Indonesia, Maldives,Myanmar, Nepal, Sri Lanka, Thailand
Western Pacific Region: 378–437Australia, Brunei Darussalam, Cambodia, China, Hong Kong (special administrative region ofChina), Taiwan (province of China), Cook Islands, Fiji, Japan, Kiribati, Lao People’s DemocraticRepublic, Malaysia, Marshall Islands, Micronesia (Federated States of), Mongolia, Nauru, NewZealand, Niue, Palau, Papua New Guinea, Philippines, Republic of Korea, Samoa, Singapore,Solomon Islands, Tokelau (associate Member State), Tonga, Tuvalu, Vanuatu, Viet Nam
Appendix A: List of Contributors 439
Appendix B: Legislation 443
-
In 1952, the American Cancer Society amended its officialstatement of purpose to include cooperation with other offi-cial and non-official organizations interested in cancer, any-where in the world, so that greater progress could be madein the fight against the disease. Today, the Tobacco ControlCountry Profiles project exemplifies this spirit of internationalcooperation in cancer surveillance, primarily through theaggregation of statistical information about the most signifi-cant risk factor for cancer: tobacco use. In the United States,tobacco use causes 30% of cancer deaths among men andwomen, and as the tobacco industry intensifies its marketingstrategies in developing countries, we can expect the propor-tion of tobacco-attributed deaths worldwide to increase. TheTobacco Control Country Profiles is one step in the develop-ment of an information system to support global tobaccocontrol efforts. More than 350 tobacco control advocates,representing over 130 countries and territories, contributedinformation to the Tobacco Control Country Profiles mono-graph, and in turn, to the emerging global information sys-tem for tobacco control. Since the American Cancer Societyrelies heavily on volunteers to administer many of its
programs nationwide, we appreciate the immensity of thisvolunteer effort. The individuals, organizations and govern-ments that assisted the development of the monograph, bysending data, completing questionnaires and lending theiradvice, share the American Cancer Society’s commitment tofighting the global smoking pandemic. It is our hope that themomentum against tobacco use apparent at the 11th WorldConference on Tobacco OR Health will continue to grow andwill result in overwhelming support for a global policy ontobacco control. Progress in decreasing tobacco-relatedmorbidity and mortality worldwide will require every nationto look beyond its geographic borders to develop new part-nerships against the tobacco industry and its advocates.
John R. Seffrin, PhDChief Executive OfficerAmerican Cancer Society
3
ForewordJohn R. Seffrin
-
This publication was prepared under the general direction ofthe American Cancer Society’s Department of Epidemiologyand Surveillance Research, headed by Dr. Michael J. Thun.Ms. Marlo Ann Corrao was the Program Manager for theTobacco Control Country Profiles project, supported by manymembers of the Surveillance Research Branch. Ms. Dorna F.Shokoohi managed the review and verification of all smokingprevalence information, while Dr. Phyllis Wingo, Dr. VilmaCokkinides, Ms. Cheryll Cardinez, and Dr. Robert Greenleeprovided guidance in epidemiologic and statistical analyses.Ms. April Harris, Ms. Emily Brouwer, and Ms. ChristyCianfrini provided assistance with data entry, data verifica-tion, and document management, while Mr. Jayson Crumpand Mr. Jeff Clements provided computer and library sup-port, respectively. Ms. Sherry Bolden, Ms. Mary Beth Hill-Harmon and Ms. Kate O’Brien also assisted withproofreading the final data. Mr. Steven Tobin, an economistand independent contractor to the American Cancer Society(ACS), was responsible for the electronic processing andmanagement of agricultural and trade data. Ms. SusanSummers, Ms. Janet Weaver, and Ms. Beverly Greene pro-vided monograph design, typesetting, and productionassistance.
ACS gratefully acknowledges ongoing support from itsprimary collaborators: the World Health Organization (WHO)and the Centers for Disease Control and Prevention (CDC).The Tobacco Free Initiative (WHO), headed by Dr. Derek Yach,and the Office on Smoking and Health (CDC), headed by Dr.Michael Eriksen, provided in-kind data and personnel supportto the project. Special thanks are due to Mr. G. EmmanuelGuindon of the Tobacco Free Initiative for coordinating thepreparation of all sociodemographic, economic, agricultural,and trade data included in this monograph. Mr. Guindonserved as a liason between the American Cancer Society andWHO regional offices, in addition to lending his expertise inthe economics of tobacco control to the project. ACS alsoacknowledges Ms. Namita Sharma of the Office on Smoking
and Health for her assistance, including facilitating theexchange of legislative and other essential data between theCDC and ACS and providing guidance in the selection of keyindicators.
The development of the Tobacco Control Country Profiles(Profiles) was made possible by collaborators in governmentand non-government organizations throughout the world thatprovided data and information for, and comments and cor-rections on, the drafts of the Profiles. A list of these collabo-rators and their countries or territories can be found inAppendix A. Special thanks are extended to two groups ofindividuals: 1) those who assisted in the selection of key indi-cators for the Profiles: Samira Asma, Simon Chapman, GregConnolly, Kourtney Johnston Davis, Allan Erickson, MichaelEriksen, Nigel Gray, Prakash Gupta, Alan Lopez, DavidSimpson, Ken Warner, and Derek Yach; 2) those who pro-vided the monograph’s Regional Summaries: Prakash Gupta(South-East Asia Region), Gonghaun Yang (Western PacificRegion), Margaretha Haglund (European Region), Vera Luizada Costa e Silva (Region of the Americas), Sherif Omar(Eastern Mediterranean Region), and Yussuf Saloojee(African Region).
The following organizations and individuals facilitateddata collection and analysis by providing access to their data:Mr. Joe Gitchell of PinneyAssociates, Dr. Judith Mackay ofthe Asian Consultancy on Tobacco Control, Mr. VasilyRomanovsky of the Industrial Statistics Section, UnitedNations Statistics Division, Mr. Thomas C. Capehart Jr. andMs. Arnella Trent of the United States Department ofAgriculture, and Véronique Pecenka of the United NationsIndustrial Development Organization.
The 11th World Conference offers a very special acknowl-edgment to SmithKline Beecham Consumer Healthcare forthe generous financial support that made this project pos-sible, in addition to the financial and human resourcescontributed by the American Cancer Society.
4
Acknowledgments
-
Tobacco Control Country ProfilesThis monograph provides the most current and comprehen-sive documentation of the status of the tobacco pandemic in197 countries and territories, virtually every country of theworld. Like the 1997 World Health Organization (WHO)report, Tobacco or Health: A Global Status Report, it reflectsthe vast continuing toll of deaths from tobacco in industrial-ized countries and the relentless increase in cigarette use andthe tobacco economy in developing countries. Monitoring thepandemic is an ongoing, multifaceted task. Three organiza-tions, the American Cancer Society (ACS), WHO, and theCenters for Disease Control and Prevention (CDC) collabo-rated to update these national and regional profiles oftobacco consumption, production, marketing, trade, anddisease burden from tobacco use.
A critical problem confronted by health advocates intobacco control, much like the challenge of preventinghuman immunodeficiency virus (HIV) infection and acquiredimmunodeficiency syndrome (AIDS), is how to communicatethe present and future human costs of an evolving pandemicto the public and to policy makers. The prolonged delaybetween the entrenchment of the causal agent, whether HIVinfection or widespread cigarette smoking and nicotineaddiction, and the disease and death caused by these agentscircumvents natural human alarm systems. At the societallevel, policymakers feel the immediate short-term appeal ofrevenue and employment from cigarette production andmarketing, whereas the diseases caused by tobacco are dis-tant and largely unseen. Health advocates have the dauntingchallenge of persuading policy makers to take preventiveactions decades before the full crisis emerges.
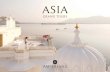
The conceptual framework that links the four stages ofthe cigarette epidemic as a continuum, rather than a series ofisolated events, is the WHO paradigm of the evolving ciga-rette epidemic in developed countries (Figure 1). The powerof this model, as proposed by Lopez and others is that itallows virtually every country to find itself in relation to thelarger pandemic. Stage 1, characterized by smoking preva-lence below 20% in men and minimal smoking in womenencompasses many countries in sub-Saharan Africa.Typically, these countries have not yet been drawn into theglobal tobacco economy, yet conditions can change rapidlydue to strategic expansion of transnational companies. Forexample, in several African countries, the acreage devoted totobacco growing has increased up to ten-fold since 1970,
with accompanying increases in the number of workersemployed in tobacco manufacture. Investments in infrastruc-ture invariably strengthen the political base for a tobaccoeconomy.
Stage 2 of the epidemic is characterized by increases insmoking prevalence to above 50% in men, an early increasein smoking prevalence among women, and rising death ratesfrom lung cancer among men. Many countries in Asia, NorthAfrica, and Latin America fit this pattern. Tobacco controlactivities are usually not well developed, the health risks oftobacco not widely understood, and there is relatively lowpublic and political support for the implementation of effec-tive tobacco control measures. Here, as in Stage 1 of theepidemic, regional and international collaboration is essentialto accelerate the development of effective tobacco control.
Stage 3 of the epidemic is characterized by a markeddownturn in smoking prevalence among men, a more grad-ual decline in women, and continued increases in mortalityfrom smoking. Many countries in Eastern and SouthernEurope are at this stage of the epidemic. Despite reductionsin the prevalence of current smoking, the increased numbersof ex-smokers in middle age, and the narrowing gap in smok-ing prevalence between the sexes, smoking attributabledeaths comprise 10% to 30% of all deaths, about three-quarters of these being in men. Health education and mediacoverage of diseases caused by smoking, begin to erodepublic acceptance of tobacco use. The educated populationincreasingly views smoking as socially undesirable ratherthan normal behavior. Public support grows for restrictionson smoking in public places and in transit.
Stage 4 of the epidemic is marked by further declines insmoking prevalence in men and women. Deaths attributableto smoking among men peak at 30% to 35% of all deaths(40% to 45% of deaths in middle aged men) and subse-quently decline. Among women, smoking-attributable deathsrise to about 20% to 25% of all deaths. Countries in Northernand Western Europe, North America, and Australia vary con-siderably in their continuing progress against tobacco.Finland achieved the largest and earliest reductions in ciga-rette use among men beginning in the 1970’s, due to vigor-ous national programs against heart disease. The subsequent25% decline in the death rate from all cancers combined inFinland from the intervals 1958-1962 to 1993-1997 was theearliest and largest decline in any industrialized country.Smoking prevalence has since stabilized in Finland at 27%
5
IntroductionMichael J. Thun, Derek Yach, Michael Eriksen
-
and 20% among adult men and women respectively, whereasit has continued to decrease in Sweden to 17.1% and 22.3%in men and women, respectively. Sustained national commit-ment to reduce tobacco use is essential for continuingprogress.
Thus, the challenge to health workers at the national levelis to translate the abstract indices of the tobacco pandemicinto terms that local policy makers will understand. Forexample, in many countries the retail price of cigarettes hasnot kept pace with inflation. Cigarettes have become cheaperrather than more expensive in real currency, despite theproven deterrent effect of higher prices on cigarette con-sumption, and despite the increased revenue that tobaccotaxes can bring to the state. This Monograph provides sev-eral resources that should facilitate the creation of strongernational tobacco control coalitions. It lists the names andaddresses of organizations involved in tobacco control withineach country. The information will be available online through
the WHO web site (http://tobacco.who.int) and CDC’sNational Tobacco Online Systems (NATIONS) (www.cdc.gov,keyword Office of Smoking and Health). While the currentMonograph provides adult smoking prevalence data on 158of 197 countries and territories and youth prevalence on 150countries and territories, residual gaps and inconsistencieswill doubtlessly stimulate further efforts to improve the qual-ity and representativeness of future data collection.
There are currently over 1.2 billion (thousand million)smokers worldwide and approximately four million deathsfrom tobacco annually. Global progress against tobacco willrequire rapid development and implementation of regulatorymeasures that cut across national boundaries. Crucial for thecontrol of this man-made epidemic are the full negotiationson the WHO Framework Convention on Tobacco Controlwhich begin in October 2000. The critical goal of these nego-tiations is to achieve universal support for the Convention nolater than May 2003.
6
Per
cent
age
of s
mok
ers
amon
g ad
ults
Per
cent
age
of d
eath
s ca
used
by
smok
ing
40
30
20
10
0
70
60
50
40
30
20
10
0
STAGE 4STAGE 3STAGE 2 STAGE 4STAGE 1
0 10 20 30 40 50 60 70 80 90 100
% malesmokers % female
smokers
% femaledeaths
% maledeaths
• sub-Saharan Africa
• China• Japan• Southeast Asia• Latin America• North Africa
• Eastern Europe• Southern Europe• Latin America
• Western Europe, UK• USA• Canada• Australia
Figure 1. 4 Stages of the Tobacco Epidemic
Source: Lopez AD, Collishaw NE, Piha T. (1994). A descriptive model of the cigarette epidemic in developed countries. Tobacco Control,3, 242-247.
Reproduced by permission of BMJ Publishing Group.
-
Monitoring the Tobacco Epidemic: Past, Present, and FutureIn 1997, the World Health Organization (WHO) responded tothe World Health Assembly’s 1989 and 1990 resolutions call-ing for periodic monitoring and reports on the “tobacco orhealth” situation in its Member States by publishing Tobaccoor Health: A Global Status Report.1 The report used stan-dardized indicators to analyze the tobacco situation atnational, regional, and global levels. The Global StatusReport consolidated a large amount of information about thetobacco epidemic during the late 1980s and the early 1990s,thus establishing a baseline for future global tobacco surveil-lance efforts.2
Following the Global Status Report and anticipating thedemand for an information system to support new tobaccocontrol efforts, WHO and the Centers for Disease Control andPrevention (CDC) initiated development of the NationalTobacco Information Online System (NATIONS) in December1998. Additional partners in this on-going project include theAmerican Cancer Society (ACS), the World Bank (WB), theUnited Nations Children’s Fund (UNICEF), and theInternational Union Against Cancer (UICC). When develop-ment is complete, NATIONS will be an electronic system thattracks country-specific information across a variety of indi-cators: smoking prevalence and tobacco consumption, lawsand regulations, morbidity and mortality, industrial organiza-tions, tobacco economics, and programmatic interventionsagainst tobacco use. NATIONS will report time trend data forsome of these topics, and the data will be updated periodi-cally and available on the Internet. NATIONS will help moni-tor the global tobacco epidemic by standardizing datacollection and distribution methods, providing the permanentelectronic framework necessary to update the data, and mak-ing information easily accessible to the public.3
This monograph, Tobacco Control Country Profiles(Profiles) updates the Global Status Report and provides pre-liminary data for NATIONS. Profiles reports on the currenttobacco situation in 197 countries and territories around theworld: 191 WHO Member States, 2 WHO associate MemberStates (Puerto Rico and Tokelau), Hong Kong (special admin-istrative region of China), Taiwan (province of China), theWest Bank and Gaza Strip (presented together). The Profileshas two overall objectives. First, it provides government and
non-government organizations with an updated, standard-ized reference source for information about tobacco and itsuse in their countries and territories. Second, it identifiesgaps where very little or no information exists and whereinformation does exist, but is not publicly accessible. Gaps inthe data highlight priorities for future data collection andtobacco surveillance efforts.
MethodsThe data in the Tobacco Control Country Profiles are orga-nized into six categories: sociodemographic situation, smok-ing prevalence, smoking-related disease impact, tobaccoeconomy, infrastructure for tobacco control, and availablepharmaceutical treatments for tobacco dependence. Theinformation presented in the Profiles includes the most cur-rent data available through May 2000. The data come from avariety of national and international sources, including datawarehouses, such as those maintained by the United Nations(UN) and the United States Department of Agriculture(USDA), government agencies, such as Ministries of Healthand national statistical offices, and individuals working in thefields of public health and tobacco control in each country.For some countries, data in one or more of the Profiles’ sixcategories are incomplete or missing. A short line (—) inplace of data signifies that no data were available for inclu-sion in the monograph. In addition, for some indicators suchas smoking prevalence and national legislation, differentsources yielded contradictory data. Where possible, conflict-ing data were reconciled by reviewing historic data related tothe indicators and consulting with experts in the country.Decisions about the reliability of each information sourcewere made on a case-by-case basis. Whenever possible,tobacco control experts and non-government organizations(NGOs) in each country or territory verified the data. Becausethe amount and the quality of data available in the Profilesvaries by country, we encourage readers to compare theircountry’s profile to their personal knowledge and impres-sions of their nation’s tobacco control situation. Readers whowish to contribute more recent data about their country tothe National Tobacco Information Online System should con-tact either the Tobacco Free Initiative at WHO or the Office onSmoking and Health at the CDC to become partners in theproject.4
7
MethodsMarlo Ann Corrao, G. Emmanual Guindon, Steven M. Tobin
-
Structure of the MonographThe methods section will provide readers with the informa-tion necessary to navigate the monograph, to reproduce datacalculations, and to locate the primary and secondarysources used to develop the country profiles. The methodsare divided into six sections, corresponding to the six cate-gories in the Profiles. Each section contains descriptions ofeach indicator and an outline of data collection methods andsources. If the data or additional information about sourcesis available through the Internet, readers will find the appro-priate Internet addresses in the reference section (p. 21). Themethods section also contains references for publicationsthat might supplement readers’ interpretation of the Profilesdata or provide insight into other topics that are important totobacco control.
Following the methods section, six tobacco controlexperts representing each of the WHO regions provide theirinsight into regional trends that may be inferred from thecountry-specific data in the Profiles. The WHO regions arethe African Region, the Region of the Americas, the EasternMediterranean Region, the European Region, the South-EastAsia Region, and the Western Pacific Region. The Table ofContents lists the countries and territories included in eachregion. Each regional summary includes an overview of avail-able data and noteworthy trends, discussion of recent victo-ries and setbacks in tobacco control activities, and adescription of future challenges to tobacco control.
Two appendices at the end of the monograph supplementthe information in the country profiles. Appendix A lists indi-viduals and organizations that contributed information or edi-torial guidance to the Profiles. Appendix B contains namesand short descriptions of the laws, regulations and voluntaryagreements included in each profile, in addition to theirsources.
Sociodemographic SituationPopulation. Population data by age and sex are presented forthe years 1995, 2000, 2025, and 2050. Figures in the tableare expressed in millions (1,000,000) and the data aredivided into two age groups: “All adults” (persons aged 15years and older) and “All youth” (persons aged 14 years andyounger). The number of females is shown under the total foreach population group. Figures for the years 2000, 2025, and2050 are projections generated by the UN PopulationDivision in the 1998 revision of “World Population Prospects:1950-2050.”5 The UN Population Division prepares thesefigures biannually for most countries in order to provide aconsistent set of population data for UN program planningand activities.6 Twenty-four countries and territories thatappear in the Profiles are not included in the UN population
database. They are Andorra, Antigua and Barbuda, CookIslands, Dominica, Grenada, Kiribati, Marshall Islands,Federated States of Micronesia, Monaco, Nauru, Niue, Palau,San Marino, Sao Tome and Principe, Seychelles, St. Kitts andNevis, St. Lucia, St. Vincent and the Grenadines, Taiwan(province of China), Tokelau, Tonga, Turkmenistan, Tuvalu,and West Bank and Gaza Strip. The alternative sources ofpopulation data for these countries and territories are listedbelow the corresponding table in their profiles.Real Gross Domestic Product. Real gross domestic productper capita derived from purchasing power parity calculations(GDP-PPP) or real GDP per capita without PPP adjustment ispresented for the years 1970, 1980, 1990, 1995, and 1998.GDP measures the total value of all final goods and servicesintended for use within the domestic territory of a givencountry, during a single year. GDP per capita is a measure ofthis output per person. GDP per capita serves as a guide tothe standard of living in the nation, and is correlated withother qualitative standard of living measures, such as healthstatus and literacy rates (although they are not directlyincluded in the GDP computation).7 Increase in GDP percapita over time suggests improvement in the nation’s eco-nomic health, and is likely to increase access to services likehealth care and public education. GDP figures derived fromPPP calculations use standardized international dollar priceweights rather than conversions at official currency exchangerates and provide a better comparison of economic healthamong countries. PPP adjusts output according to variationsin spending power. For instance, $1,000 converted at PPPrates will purchase the same amount of goods and servicesin the United Kingdom as it purchases in Austria. Conversely,GDP data derived from conversions at official currencyexchange rates can fluctuate as a result of domestic andinternational financial events that are mostly unrelated to thedomestic output of goods and services.
While there are four sources of GDP data in the Profiles,the primary source is the Penn World Tables.8 When coun-tries were not included in the Penn World Tables, the sourcefor GDP was the World Bank,9 followed by the UnitedNations,10 and lastly, the United States’ Central IntelligenceAgency.11 Whenever possible, real GDP-PPP per capita dataare presented for each country. When real GDP-PPP percapita data were not available, real GDP is presented withoutthe PPP conversion. Real GDP-PPP per capita data from thePenn World Tables are expressed in constant dollars, inter-national prices, base year 1985.12 Real GDP-PPP per capitadata from the World Bank or Central Intelligence Agency areexpressed in current dollars, international prices; the PPPconversion rates used in the calculations are based on theWorld Bank’s 1996 World Development Report.13 Because
8
-
there are three sources of real GDP-PPP per capita data,comparisons between countries whose GDP source is differ-ent are likely to be inaccurate. Furthermore, GDP per capitadata for several countries do not incorporate PPP conversionrates. The title of the GDP table in these country profiles is“GDP per capita, US Dollars” instead of “Real GDP per capita(PPP), US Dollars.” The source of these data is the UNStatistics Division-National Accounts Section, EconomicStatistics Branch. In cases where no GDP data were reportedin any of the years 1970, 1980, 1990, 1995, or 1998, a sta-tistic from the year closest to the missing year was used inits place to maintain a time series.
Other sociodemographic indicators relevant to theassessment of tobacco use include life expectancy, literacyrates, labor force structure, and human developmentindexes.14 Data related to these indicators are not presentedin the Profiles. Readers may wish to refer to the CentralIntelligence Agency’s World Factbook and the United Nations’Human Development Report to augment the sociodemo-graphic profiles presented in this monograph.15, 16
Smoking PrevalenceAs smoking is the most common form of tobacco use inmost countries, the extent of the tobacco epidemic can bereasonably measured through the prevalence of cigarette orother tobacco smoking. The prevalence of tobacco or ciga-rette smoking among adults, youth, and health professionals(physicians, nurses and/or medical students) is presented inthree separate tables. Smoking prevalence refers to the pro-portion (expressed as a percent) of the study population whoare smokers. Where possible, prevalence is presented sepa-rately for males and females within the adult, youth, andhealth professional populations. The age range that defines“adult” and “youth” and the year that the data were collectedappear in the title of each table, as these information differamong sources and across countries. The footnotes underthe prevalence tables include information about how the sur-vey defined “smokers,” where the survey was conducted (ifnot nationally representative), and the original source of theprevalence data. The source is provided so that readers canobtain a copy of the publication and independently assessdata quality and validity. Before comparing smoking preva-lence across several countries or territories, the followingquestions should be considered:• What type of tobacco do respondents report smoking? • What frequency of smoking defines a “smoker?”• What is the age range defining “adult” and “youth” and how
were the respondents selected?• Where was survey conducted? Was the survey conducted
throughout the country or territory?
• Is the survey conducted annually or less frequently?The first two questions relate to how the survey distin-
guished between smokers and non-smokers; smokingbehavior in two countries may not be comparable if theanswers to these questions are different. Whenever possible,survey data that adhered to the WHO definitions of smokingwere selected to increase comparability between studies. TheWHO guidelines state that respondents who report smokingat the time of the survey, or “current smokers” should be fur-ther categorized as “daily” or “occasional” smokers. “Daily”smokers are individuals who smoke any tobacco product atleast once a day, including those who smoke everyday exceptdays of religious fasting. “Occasional” smokers are individu-als who smoke any tobacco product, but not every day.17
The last three questions relate to the selection of surveyrespondents. Surveys vary in their ability to describe anentire nation’s smoking behavior depending on the sampledesign. The most reliable estimates of smoking prevalencecome from population-based, cross-sectional surveys andthat data can be inferred as representative of the country’spopulation at a given point in time. Specific criteria wereestablished for including smoking prevalence data in theProfiles, based on the principles of survey research. Prioritywas given to the most current and nationally representativeestimates of smoking prevalence in each country’s adult,youth, and health professional populations.
Smoking prevalence studies were collected from severalsources, including articles from Medline literature searches,personal contacts with investigators and non-governmentorganizations engaged in tobacco control, and reports fromMinistries of Health, national statistical offices, and WHOcountry representatives. Inclusion criteria for these preva-lence surveys required the following minimum information:1) date of the survey or its publication, 2) characteristics ofthe respondents (age and/or gender distribution), 3) detailsabout sampling techniques and data collection, and 4) somedescription of the questions used in assessing smokingbehavior. If several studies from the same country met thesecriteria, they were compared with respect to geographic cov-erage (national, regional or other), date of the study, samplesize, response rates, and methods. If different sourcesyielded contradictory data on prevalence, the authorsreviewed historical data and consulted with experts workingin the country. The most current and representative studiesof smoking prevalence were included.
Table 1 lists the countries and territories for which smok-ing prevalence information was available and the year inwhich the data were collected. Italicized years denote thepublication year and not the data collection year; the year ofdata collection for these studies is not known.
9
-
Countries and Territories Adult Youth Health Professional
Afghanistan — — —Albania 1995-1996 1990-1991 1990-1991Algeria 1997-1998 1999 1999Andorra 1997 1988 —Angola — — —Antigua and Barbuda — 1998 —Argentina 1999 1997 1997Armenia 1990s 1997 —Australia 1995 1996 1996Austria 1997 1998 1995
Azerbaijan 1999 — —Bahamas 1989 1987 —Bahrain 1995 1991 1994Bangladesh 1998 1991 1985Barbados 1993 — —Belarus 1999 1999 —Belgium 1999 1998 1991Belize — 1992 —Benin 1988 1988 —Bhutan — — —
Bolivia 1998 1992 1987Bosnia and Herzegovina 1995 — 1996Botswana 1988 — —Brazil 1995 1989 1996Brunei Darussalam 1979 1979 —Bulgaria 1996 1998 1996Burkina Faso — 1992 —Burundi — 1996 —Cambodia 1994 1994 1998-1999Cameroon — 1996 —
Canada 1999 1997 1994Cape Verde — — —Central African Republic — — —Chad 1994 1994 —Chile 1998 1998-1999 1992China 1996 1997 1996Hong Kong (special administrative region of China) 1998 1998 1987
Taiwan (province of China) 1996 1994 —Colombia 1997 1988-1989 1991
Comoros — — —Congo — — —Cook Islands 1978-1987 1980 —Costa Rica 1995 1995 1993-1994Côte d’Ivoire 1977 1990 —Croatia 1995 1995 1993Cuba 1995 1990 1995Cyprus 1997 1998 —Czech Republic 1998 1998 1998Democratic People’s Republic of Korea 1985 — —
Democratic Republic of the Congo 1998 1998 —Denmark 1998 1998 1996Djibouti 1999 — —Dominica — 1998 —Dominican Republic 1993 1986 1986Ecuador 1991 1994 —Egypt 1997 1998 1993El Salvador 1988 1988 —Equatorial Guinea — — —Eritrea — — —
Estonia 1996 1998 1982Ethiopia 1995 1997-1998 1985Fiji 1997 1994 1991Finland 1999 1998 1995France 1997 1998 1993Gabon — — —Gambia — — —Georgia 1999 1997 1996Germany 1997 1998 1992-1993Ghana 1980 1992 —
Countries and Territories Adult Youth Health Professional
Greece 1994 1998 1992Grenada — 1998 —Guatemala 1989 1989 1987Guinea 1998 — —Guinea-Bissau — — —Guyana — — —Haiti 1990 1990 —Honduras 1988 1989 —Hungary 1998-1999 1997 1995Iceland 1998 1998 2000
India 1985-1986 1991 1985Indonesia 1995 1995 1985Iran (Islamic Republic of) 1997-1998 1997-1998 1997-1998Iraq 1990 1990 —Ireland 1998 1998 1990Israel 1999 1998 1995-1996Italy 1998 1994 1996Jamaica 1994 1997 —Japan 1998 1990 1990Jordan 1996 1997 —
Kazakhstan 2000 — —Kenya 1995 1993 1986Kiribati 1978-1987 1981 —Kuwait 1996 1995 1990Kyrgyzstan 1998 1998 —Lao People’s Democratic Republic 1993 1997 1996Latvia 1998 1997 1993Lebanon 1997 1997 1999Lesotho 1992 1992 —Liberia — — —
Libyan Arab Jamahiriya 1997 — —Lithuania 1997 1998 1992Luxembourg 1998 1998 1991Madagascar — — 1993Malawi 1996 — —Malaysia 1996 1996 1991Maldives — — —Mali — — —Malta 1995 1995 1989Marshall Islands — — —
Mauritania — — —Mauritius 1998 — 1992Mexico 1998 1998 1997Micronesia (Federated States of) — — —Monaco — — —Mongolia 1999 1998 1990Morocco 1999 1992 1994-1995Mozambique — — —Myanmar 1992-1993 — —Namibia 1994 — —Nauru 1978-1987 1975 —
Nepal 1998 1987 —Netherlands 1998 1998 1989New Zealand 1998 1998 1996Nicaragua 1988 1988 —Niger — 1990s —Nigeria 1998 1994 1983Niue 1978-1987 1980 —Norway 1998 1997 1993Oman 1995 1995 —Pakistan 1990-1994 1990 1993
Palau 1997 1997 —Panama 1993 1996 1980Papua New Guinea 1990 1989-1990 1990Paraguay 1990 — 1989Peru 1998 1998 —Philippines 1999 1995 1987Poland 1998 1998 1995Portugal 1995-1996 1998 1991Puerto Rico 1998 1995 —Qatar — 1998 —
10
Table 1. Years of smoking prevalence statistics in the Profiles
-
Countries and Territories Adult Youth Health Professional
Republic of Korea 1996 1997 1998Republic of Moldova 1998 1998 1998Romania 1994 1994-1996 1997Russian Federation 1996 1998 1996-1999Rwanda 1992-1994 1998 —Saint Kitts and Nevis — — —Saint Lucia — — —Saint Vincent & Grenadines 1991 — —Samoa 1995 1994 1994San Marino 1990s — —
Sao Tome and Principe 1998 1998 —Saudi Arabia 1994 1993 1996Senegal 1998 1998 1989Seychelles 1994 1991 —Sierra Leone 1998 1994 —Singapore 1998 1987 1985Slovakia 1996 1998 1991Slovenia 1999 1999 1996Solomon Islands 1989 1989 —Somalia — — —South Africa 1998 1998 1986
Spain 1997 1994 1995Sri Lanka 1998 1995 —Sudan 1999 1992 1980Suriname — 1987-1988 —Swaziland 1994 1997 —Sweden 1998 1997 1996Switzerland 1997 1998 1989Syrian Arab Republic 1997-2000 1997 1997-1998Tajikistan — 1990s —Thailand 1999 1996 1989
The former Yugoslav Republic of Macedonia — — —
Togo — — —Tokelau 1991 1994 —Tonga 1991 1991 1994Trinidad and Tobago 1977-1986 1988 —Tunisia 1996 1999 1994Turkey 1997 1996 1993Turkmenistan 1990 — —Tuvalu 1975-1981 1975-1981 —
Uganda 1995 1995 —Ukraine 1995 1995 —United Arab Emirates 1995 1995 1991-1992United Kingdom of Great Britain and Northern Ireland 1996 1997-1998 1985 & 1997
United Republic of Tanzania 1992-1998 1995 —United States of America 1997 1998 1991Uruguay 1995 1993 1992Uzbekistan 1991 1989 —Vanuatu 1990 — —
Venezuela (Bolivarian Republic of) 1992 1984 1990Viet Nam 1995 1995 1997West Bank and Gaza Strip 1996 1996 1999Yemen 1997 — —Yugoslavia 1999 1984-1985 1989Zambia 1996 1996 —Zimbabwe 1993 1990-1991 —
Despite the focus on cigarette smoking in the Profiles, theprevalence of other smoking tobacco and oral tobacco usebetter reflects the tobacco situation in some countries andsub-regions within countries. The South-East Asia regionalsummary discusses bidis and other forms of tobacco usethat are more prevalent than cigarette smoking. Prevalenceestimates for tobacco use other than cigarette smoking arealso provided in this regional summary (p. 36).
Smoking-Related Disease ImpactThe Profiles includes estimates of smoking-attributed deathsin 44 developed countries. The data were prepared by theWHO Collaborating Center for Chronic Disease Control at theUniversity of Oxford, in collaboration with ACS, the ImperialCancer Research Fund and WHO. The estimates firstappeared in “Mortality from Smoking in DevelopedCountries, 1950-2000”18 and the original paper, includingdiscussion of the methods used to derive tobacco-attributedmortality, was published in Lancet.19 In the Profiles, the num-bers of deaths attributed to smoking in 1990 or 1995 are cat-egorized by cause, age group, and sex. Trends in totalsmoking-attributed mortality among men and women, aged35 to 69, between 1955 and 1995 are shown graphically.Only mortality during middle age (35 to 69 years) is pre-sented in the graph because in developed countries, smokingcauses few deaths before middle age, while it is responsiblefor about one-third of deaths among men during middle ageand a growing proportion of deaths among women duringmiddle age.20
The Profiles also includes smoking-attributed mortalityestimates for China, prepared by the Chinese Academy ofMedical Science, the Clinical Trial Service Unit andEpidemiological Studies Unit at Oxford University, CornellUniversity, and the Chinese Academy of PreventiveMedicine.21 Smoking-attributed mortality estimates, how-ever, were not calculated for other developing countries.
The Profiles presents the crude numbers of deaths andage-standardized mortality rates for diseases most com-monly associated with tobacco use. The CDC developed thislist of smoking-related diseases through previous analyses ofthe impact of cigarette smoking on mortality and years ofpotential life lost before age 65 in the United States.22Because this categorization of disease better reflects theproportion of deaths due to smoking in developed countriesthan in developing countries, some modifications were madeto the CDC’s list under the advice of the WHO and ACS.23 Thegoal of these changes was to “concentrate” on the effects oftobacco use in developing countries. First, pediatric diseases,such as low birth weight, respiratory distress, sudden infantdeath syndrome and burns were eliminated from the list sothat the mortality tables for developing countries include onlyadult diseases and mortality among persons in middle age.Second, acute respiratory infections, such as pneumonia andinfluenza, were eliminated from the list. In developing coun-tries, these conditions may have weaker associations withtobacco use. Those diseases for which the causal roles oftobacco use are well established and are likely to have at leastmoderate mortality rates attributable to tobacco wereselected from the remaining conditions.
11
-
Table 2 lists the disease categories, the conditionsincluded in each category, and the ICD-9 or ICD-10 codesthat correspond to the data in the World Health StatisticsAnnual. With the exception of five countries, the numericalcodes in the Annual correspond to ICD-9 codes. Data forCroatia, Republic of Korea, Malta, Qatar, and Thailand corre-spond to ICD-10 codes.
Table 2. Select smoking-attributed diseasesDisease Category Included Conditions ICD-9 ICD-10
Trachea, lung & bronchus Trachea, lung & cancer bronchus cancer, 101 162 TBL
Lip, oral cavity, and Lip, oral cavity, and pharynx cancer pharynx cancer, 08 140-149 LOP
Ischemic heart disease Acute myocardial infarction, 270 410-414 MYIOther ischemic heart disease, 279 ISC/CIH
Stroke Cerebrovasculardisease, 29 430-438 CEVEmbolism, thrombosis and other diseases of the arteries, arterioles & capillaries, 301 & 302 440-448 ARTAtherosclerosis, 300Phlebitis, thrombophlebitis,venous embolism & thrombosis, 303 451-453 PTV
Other diseases of the Hypertensive disease, 26 401-404 HYPcirculatory system Diseases of the pulmonary
circulation & other forms 415-417 PHDof heart disease, 28 420-429 HDD
Respiratory disease Bronchitis, chronic & unspecified, emphysema & asthma, 323 490-496 COPOther diseases of therespiratory system, 313- 519 EMP315, 319, 324-327, 329 AST
Total (All Causes) Total (All Causes) — —
Mortality data come from the World Health StatisticsAnnual, which reports the statistics submitted to WHO byindividual Member States.24 According to WHO, the data arelimited to those countries that report cause of death infor-mation in an appropriate format and have reasonably ade-quate death registration coverage. Where information wasavailable, death rates age-adjusted to the World standardpopulation and truncated to ages 35+ were calculated. It isvery important to note that in countries with low populationsize, small changes in the number of deaths can cause sub-stantial variability in rates from one year to another.Furthermore, WHO does not provide death rates for somecountries because of low coverage by their death registrationsystems. Thus, death rates for the following countries shouldbe interpreted with caution: Bahamas, Barbados, Belize,Brazil, Ecuador, Egypt, Guyana, Malta, Mongolia, Nicaragua,Paraguay, Philippines, and Qatar. Data for countries and ter-ritories whose reports to WHO were based on hospital or
institutional death registration are not included in theProfiles.
Cancer statistics for countries not in the “World HealthStatistics Annual” were derived from the InternationalAgency for Research on Cancer (IARC). These estimates ofannual cancer mortality in 1990 are available through theelectronic database, GLOBOCAN.25 The methods used toderive these estimates are described in the InternationalJournal of Cancer.26
Readers should not confuse these mortality statisticswith smoking-attributed mortality estimates. Mortality num-bers and rates provide valuable information about the differ-ential burden of disease around the world and allow somecomparison among countries; however, they do not reflectthe true burden of disease caused by smoking alone.
Tobacco EconomyThe Profiles presents data related to the economics oftobacco control, including trade and agricultural productionstatistics and tobacco prices, taxes and duties. Several pub-lications, listed below, may assist readers in interpreting thedata and provide a broader view of the economic issues sur-rounding the adoption of new tobacco control policies. Thesepublications also discuss the economic merits of tobaccocontrol and respond to arguments that tobacco control activ-ities might negatively impact nations’ economic health:• Chaloupka, FJ & Warner, KE. (forthcoming). The Economics
of Smoking. In Newhouse J, and Culyer (Eds.), The Hand-book of Health Economics. Amsterdam: North Holland.
• Warner, KE. (2000). The economics of tobacco: myths andrealities. Tobacco Control, 9, 78-89.
• The World Bank. (1999). Curbing the epidemic: govern-ments and the economics of tobacco control. Series:Development in practice. Washington, D.C.
Annual Trade and Agriculture Statistics. The Profiles pre-sents both tobacco leaf and cigarette import, export and pro-duction figures for 1970, 1980, 1990, 1995, and 1998. Twodatabases from the United Nations Statistical Division(UNSD) provided data for the Profiles. First, the CommodityTrade Statistics (COMTRADE) database contains trade(import and export) statistics for more than a dozen tobaccoproducts, to include cigarettes, cigars, manufactured andunmanufactured tobacco.27 The UNSD also collects com-modity production statistics through its IndustrialCommodity Production Statistics Database.28 These produc-tion data correspond to the information published in theIndustrial Commodity Statistics Yearbook.29 Similarly, theFood and Agricultural database (FAOSTAT) provides informa-tion related to the production of tobacco leaves, trade in cig-arettes, cigars, manufactured tobacco and tobacco leaves,
12
-
and the land area harvested annually in tobacco farming.30Apart from the UN, the USDA maintains tobacco-related pro-duction, trade and land statistics in an electronic database.When no data were available from COMTRADE, FAOSTAT orUSDA, figures from national statistical agencies and privateresearch firms were used.Land devoted to tobacco & Employment in tobacco manu-facturing. The amount of land devoted to tobacco growing ispresented both in total hectares and as a percent of the totalagricultural land in 1970, 1980, 1990, 1995, and 1998, whenavailable. The source of these data is the United Nations’Food and Agriculture Organization (FAO). Employment intobacco manufacturing is reported for 1970, 1980, 1990,1995, and 1998, when available. The employment figureswere taken from the United Nations Industrial DevelopmentOrganization’s (UNIDO) Industrial Statistics Database.UNIDO collects information from four sources in order tomaintain the database: 1) industry data from country ques-tionnaires, 2) national publications, including industrial cen-suses and annual surveys, 3) published and unpublishedinternational sources, and 4) national data compiled by stat-isticians working in each country.31
Annual per capita and total cigarette consumption. Totaland per capita cigarette consumption figures were calculatedusing production, import, and export figures found in theaforementioned databases. The best source for each coun-try’s indicators was selected according to the followingprocess. Production and trade data from the UNSD, FAO-STAT, USDA and ERC Statistics International32 were com-pared and contrasted. When the data were identical or verysimilar, the most complete source (the one with the mostdata points) was utilized. On a few occasions, similar datafrom different sources were merged to expand the data cov-erage. When data from any of the four sources conflictedwith another, they were compared and contrasted with datareported in Tobacco or Health: A Global Status Report, thePan American Health Organization’s Tobacco or Health:Status in the Americas33 and Market Tracking International.34If no consensus emerged, the data were not reported. On rareoccasions, cigarette consumption calculations yielded unre-alistic estimates (for instance, negative consumption num-bers). These estimates were also not reported.
The formulas for consumption calculations are asfollows:• Total Cigarette Consumption =
Production + Imports – Exports• Per Capita Cigarette Consumption =
(Production + Imports – Exports) / Population aged 15+For the purposes of the calculations, one cigarette stick
was equivalent to one gram in weight.
Table 3 lists the sources of production, import, and exportdata used in each country or territory’s cigarette consump-tion calculation.
Table 3. Sources used in caluculating cigarette consumptionCigarette Cigarette imports
Countries and Territories production & exports
Afghanistan No production FAOAlbania UN Not AvailableAlgeria UN FAOAndorra Not Available Not AvailableAngola UN/USDA FAOAntigua and Barbuda No production FAOArgentina USDA FAOArmenia UN FAOAustralia USDA USDAAustria UN/USDA UNAzerbaijan UN/USDA USDABahamas No production FAOBahrain No production UNBangladesh UN FAOBarbados UN FAOBelarus UN FAO
Belgium (Includes Luxembourg) UN UNBelize UN FAOBenin Not Available FAOBhutan No production FAOBolivia UN FAOBosnia and Herzegovina USDA FAOBotswana Not Available FAOBrazil UN/USDA FAOBrunei Darussalam No production FAOBulgaria UN FAOBurkina Faso UN FAOBurundi UN FAOCambodia UN FAOCameroon (Trade data exclude trade with Central African Republic, Congo and Gabon) UN/USDA FAO
Canada UN/ERC UNCape Verde Not Available FAOCentral African Republic (Trade data exclude trade with Cameroon, Congo and Gabon) UN FAO
Chad UN FAOChile UN FAOChina USDA FAOHong Kong (special administrative region of China) UN/ERC FAO/USDA
Taiwan (province of China) USDA USDAColombia UN FAOComoros Not Available FAOCongo UN FAOCook Islands Not Available FAOCosta Rica UN FAO
Côte d’Ivoire UN/USDA FAOCroatia UN/USDA USDACuba UN FAOCyprus UN UNCzech Republic UN/ERC UNDemocratic People’s Republic of Korea Not Available FAODemocratic Republic of the Congo(Trade data exclude trade with Cameroon,Central African Republic and Gabon) UN/ERC FAO
Denmark UN/USDA UNDjibouti Not Available FAODominica UN FAODominican Republic (Assumed negligible exports to estimate consumption priorto 1994) UN FAO/USDA
Ecuador UN FAO
13
-
Cigarette Cigarette importsCountries and Territories production & exports
Egypt UN FAOEl Salvador UN FAOEquatorial Guinea Not Available Not AvailableEritrea Not Available Not AvailableEstonia UN FAOEthiopia UN FAOFiji UN FAOFinland UN FAOFrance USDA USDAGabon (Trade data exclude trade with Cameroon, Central African Republicand Congo) UN FAO
Gambia Not Available FAO
Georgia UN Not AvailableGermany UN/USDA FAOGhana UN/ERC FAOGreece UN UNGrenada (Assumed negligible exports to estimate consumption) UN FAO
Guatemala UN FAOGuinea Not Available FAOGuinea-Bissau Not Available FAOGuyana UN FAOHaiti UN FAOHonduras UN FAOHungary UN FAO
Iceland No production UNIndia UN FAOIndonesia USDA FAOIran (Islamic Republic of) UN FAOIraq UN/USDA FAOIreland UN FAOIsrael UN FAOItaly UN UNJamaica UN/USDA FAOJapan USDA USDAJordan UN FAOKazakhstan UN FAOKenya UN FAO
Kiribati Not Available UNKuwait No production FAOKyrgyzstan UN ERCLao People’s Democratic Republic UN Not Available(Assumed negligible exports and imports to estimate consumption)
Latvia UN UNLebanon UN FAOLesotho Not Available Not AvailableLiberia UN FAOLibyan Arab Jamahiriya UN FAOLithuania UN Not AvailableLuxembourg Not Available Not Available
Madagascar UN FAOMalawi UN FAOMalaysia UN UNMaldives (Assumed negligible exports andproduction to estimate consumption) Not Available FAO
Mali UN UNMalta UN FAOMarshall Islands Not Available Not AvailableMauritania Not Available FAOMauritius UN FAOMexico UN FAOMicronesia (Federated States of) Not Available Not AvailableMonaco Not Available Not Available
Cigarette Cigarette importsCountries and Territories production & exports
Mongolia Not Available UNMorocco UN/ERC FAOMozambique UN FAOMyanmar UN Not AvailableNamibia Not Available Not AvailableNauru Not Available Not AvailableNepal UN FAONetherlands UN/USDA UNNew Zealand (Trade with the Cook Islands, Niue and Tokelau is excluded) UN FAO
Nicaragua UN/USDA FAONiger Not Available FAONigeria UN FAO
Niue Not Available Not AvailableNorway UN/USDA FAOOman Not Available FAOPakistan UN FAOPalau Not Available Not AvailablePanama UN UNPapua New Guinea Not Available FAOParaguay UN FAOPeru UN FAOPhilippines UN UNPoland UN FAOPortugal UN FAOPuerto Rico Not Available Not Available
Qatar No production FAORepublic of Korea USDA USDARepublic of Moldova UN/USDA USDARomania UN FAORussian Federation (Data for 1992 and 1993 refer to trade only with countries outside the area of the former USSR, while data for1994 refer to trade with all countries) UN FAO
Rwanda UN FAOSaint Kitts and Nevis (Includes Anguilla data) Not Available FAO
Saint Lucia Not Available FAOSaint Vincent and the Grenadines Not Available FAO
Samoa USDA USDASan Marino Not Available Not AvailableSao Tome and Principe Not Available FAOSaudi Arabia No production FAO/ERCSenegal UN FAOSeychelles UN FAOSierra Leone UN FAOSingapore UN/USDA UN/USDASlovakia UN/ERC FAOSlovenia UN FAOSolomon Islands No production FAOSomalia UN Not AvailableSouth Africa UN/ERC FAO/USDA
Spain UN UNSri Lanka UN FAOSudan UN FAOSuriname (Assumed negligible exports to estimate consumption) UN FAO/UN
Swaziland Not Available FAOSweden UN/USDA FAOSwitzerland UN UNSyrian Arab Republic UN FAOTajikistan UN Not AvailableThailand UN FAOThe former Yugoslav Republic of Macedonia Not Available FAO
14
Table 3. (cont.)
-
Cigarette Cigarette importsCountries and Territories production & exports
Togo Not Available FAOTokelau Not Available Not AvailableTonga Not Available FAOTrinidad and Tobago UN FAOTunisia UN FAOTurkey USDA USDATurkmenistan (Assumed negligible exports to estimate consumption) USDA USDA
Tuvalu Not Available FAOUganda UN FAOUkraine UN FAOUnited Arab Emirates Not Available FAOUnited Kingdom of Great Britain and Northern Ireland USDA USDA
United Republic of Tanzania UN FAOUnited States of America USDA USDAUruguay UN/ERC FAOUzbekistan USDA USDAVanuatu Not Available FAOVenezuela (Bolivarian Republic of) UN/USDA FAOViet Nam UN FAOWest Bank and Gaza Strip Not Available Not AvailableYemen UN FAOYugoslavia UN FAOZambia UN FAOZimbabwe UN/USDA FAO
The accuracy of the per capita consumption estimates islimited by the information not included in each country’s offi-cial trade and production statistics. The calculations in theProfiles did not account for factors that increase or decreasethe true volumes of trade and production, such as smugglingand tax exemption. The consumption formula does notaccount for the production of roll-your-own, bidi, and kretek
cigarettes, as only manufactured cigarettes are included inthe UN and USDA databases. In countries where the pre-ferred cigarette types are other than manufactured, the for-mula will underestimate the populations’ cigaretteconsumption. This is most relevant to the EasternMediterranean Region and Central and Southern Asia. Third,the calculation does not account for cigarette stocks held inreserve by cigarette wholesalers and retailers. This is lesssignificant because it would only become apparent when thenet change in stock volume is very large between years.Finally, the per capita consumption calculation includes onlyadults aged 15 years and older in its denominator, and thus,does not account for smokers younger than 15 years. Thisfactor is more important in selected developing countries,where the largest proportion of the population is youth under15 years of age. The advantages and disadvantages of calcu-lating tobacco consumption statistics are discussed at lengthin many publications.35
Manufactured Tobacco Consumption. Per capita manufac-tured tobacco consumption statistics provide some sense ofthe total volume of tobacco consumed, not only that of man-ufactured cigarettes. Based on the data available from the UNand USDA, only 24 countries had data sufficient to calculatemanufactured tobacco consumption. Table 4 presents theavailable data. Methods for making these estimates wereidentical to the per capita cigarette consumption calculations.
15
Table 4. Per Capita Consumption—Manufactured Tobacco (grams per person)1970 1980 1985 1990 1995 Production Source Trade Source
Algeria 454.4 744.7 — 735.4 476.51 UN FAOAustria 135.4 32.6 72.8 59.1 — UN FAOBelgium2 877.5 945.2 1527.7 1246.0 — UN FAOCanada 639.2 342.9 387.9 420.1 3 — UN FAODenmark 774.1 558.8 796.5 1002.1 631.2 UN UNEgypt 247.7 388.5 614.5 1045.6 1197.4 UN FAOFiji Islands 34.0 33.6 27.8 3.6 — UN FAOFinland 331.7 381.7 363.2 397.0 390.1 UN UN
Iceland 652.44 387.9 259.9 156.3 277.25 UN UNIran (Islamic Republic of) 313.7 221.7 230.3 157.8 98.3 UN FAOIsrael 66.9 45.5 24.2 42.86 — UN FAOItaly 86.4 28.8 14.5 32.1 67.1 UN UNMadagascar 460.2 448.7 202.9 93.3 — UN UNNew Zealand 541.6 215.7 140.9 248.6 305.8 UN FAONorway 1578.9 1433.3 1381.9 — — UN UNPhilippines 40.5 40.9 34.7 — — UN FAO
Portugal 54.8 29.5 26.3 22.3 30.6 UN FAOSouth Africa 937.8 641.0 476.9 365.9 246.47 UN FAOSpain 81.7 167.1 127.8 685.1 — UN FAOSweden 719.5 717.7 916.2 897.2 934.1 UN UNSwitzerland 372.1 346.6 339.7 624.1 256.2 UN UNUnited Kingdom of Great Britain and Northern Ireland 298.8 339.3 259.2 301.78 444.9 UN FAOUnited States 444.1 444.2 288.0 24.8 — USDA USDA
Note: 1. Denotes 1994. 2. Include data from Luxembourg. 3. Denotes 1989. 4. Denotes 1971. 5. Denotes 1994. 6. Denotes 1989. 7. Denotes 1993. 8. Denotes 1989.
-
Taxes & Duties. Tax and duty data are presented in a table onthe first page of each country or territory’s profile. Since mosttaxes and duties are established through legislation or regula-tions, more information about the imposition of tax and dutyfees may appear in Appendix B, the Legislative Appendix.Information regarding the taxes levied on cigarettes was gath-ered from three main sources, ERC, USDA, and the TobaccoMerchants Association (TMA).36 The information is brokendown into three categories. The first is excise tax that coverstaxes levied within each country on cigarettes, usually in theform of a value added per pack or per cigarette. The secondcategory covers any sales tax or value added taxes (VAT) onall goods and services that are also applicable to cigarettes.The third category covers any import duties associated withforeign cigarette brands sold in the domestic market.
The following units of measure and abbreviations areused in the tax section:
Cig(s) Cigarette(s)CIF Cost Including Freight chargesECU European Currency UnitETP Excise Tax in ProductsGST Goods and Services TaxLCU Local Currency Unitmax Maximummin Minimummm millimeter in lengthTVO Taxes sur la valeur ordinaireUS$ United States Dollars% PercentThe following abbreviations are used in the tax section to
describe associations among countries related to preferentialtrade status:
ANDEAN South American countries including Bolivia,Chile, Colombia, Ecuador, and Peru
APEC Asian Pacific Economic CooperationASEAN Association of Southeast Asian NationsCACU Central African Customs UnionCARICOM Caribbean Community and Common
MarketCEFTA Central European Free Trade AreaCOMESA Common Market for Eastern and Southern
AfricaECOWAS Economic Community of West African
StatesEEC European Economic CommunityEFTA European Free Trade AssociationEU European Union (formerly EEC)MERCOSUR Common Market of the South (Argentina,
Brazil, Paraguay, and Uruguay)MFN Most Favored NationsSA South American or South America
SACU South Africa Customs Union (Namibia,Botswana, Lesotho and Swaziland)
SADC South African Development CommunitySPARTECA South Pacific Regional Trade and Economic
Cooperation AgreementUEMOA Economic and Monetary Union of West
Africa UMA Union Maghreb Arabe (Libya, Mauritania,
Morocco and Tunisia)WTO World Trade Organization The tax tables in the country profiles do not reflect the
trade relationships among European Union (EU) memberstates and between the EU and countries that receive prefer-ential trade status from it. For trade within the EU among itsmember states, cigarettes are not subject to any importduties. The member states established a community inte-grated tariff system (TARIC), through which duties areapplied to imports from non-EU countries. TARIC was estab-lished by the 1958 Treaty of Rome as part of the EuropeanEconomic Community. The EU tariff schedule is based on theCustoms Cooperation Council Nomenclature, also called theHarmonized System. It was introduced to provide a standardtariff classification regime for all products imported andexported throughout the world. Under the Lome Convention,the EU also extends various preferential tariff treatments toimports from the developing countries in Africa, theCaribbean and the Pacific Rim. Tariff preferences also extendto over 100 developing countries (except China) under theGeneralized System of Preferences. This system of duty-freeand preferential trading in the EU is not noted separately ineach country’s tax and duty table.Prices. The Profiles presents the retail price of a single pack-age of domestic and imported manufactured cigarettes,including applicable taxes and duties. Prices in local currencyare converted to US dollars to allow comparison amongcountries. When a currency exchange rate was not available,the local price is presented alone. In most countries, twentycigarettes constitute a package of cigarettes; when this is notthe case, the title of the table includes the appropriate num-ber of cigarettes. Whenever possible, Marlboro brand ciga-rettes were selected to represent the price of foreigncigarettes in order to provide a measure of standardization.There are four main sources of retail price data in this mono-graph. The primary source is the Economist Intelligence Unit(EIU), an economic and market research firm based in theUnited Kingdom. The EIU surveys cigarette and pipe tobaccoprices biannually as part of its Cost of Living Survey in 129cities or a total of 82 countries.37 The EIU conducts pricesurveys during March (“Spring”) and September (“Autumn”)and reports prices for two types of cigarettes, Marlboro (apopular foreign brand) and a popular domestic brand. TheEIU survey is not limited to one retail location in each city, but
16
-
includes the price of the same product in three different retaillocations: a supermarket, a mid-price store, and a specializedshop. This survey method results in three price categories:low, middle, and high. For the purposes of the Profiles, theprice of foreign and domestic cigarettes is the average of thethree price categories in each survey. In cases where the EIUconducted its survey in two or more cities in the same coun-try, the average of the city prices serves as the country price.Table 5 lists the cities where the EIU conducted its surveys.
Table 5. EIU Survey Coverage, 1997-1999Countries and Territories Cities
Algeria AlgiersAngola LuandaArgentina Buenos AiresAustralia Adelaide, Brisbane, Melbourne, Perth,
and SydneyAustria ViennaAzerbaijan BakuBahamas Nassau Bahrain BahrainBangladesh DhakaBelgium BrusselsBotswana GaboroneBrazil Brasilia, Curitiba, Rio De Janeiro, and
Sao PauloBrunei Darussalam Bandar Seri Bagawan and BruneiBulgaria SofiaCambodia Phnom PenCameroon DoualaCanada Calgary, Montreal, Toronto, and Vancouver
Chile SantiagoChina Beijing, Dalian, Guangzhou, Qingdao,
Shanghai, Shenzhen, Tianjin, and XiamenHong Kong (special administrative region of China) Hong Kong
Taiwan (province of China) TaipeiColombia BogotaCongo BrazzavilleCosta Rica San JoseCote d’Ivoire AbidjanCroatia ZagrebCyprus NicosiaCzech Republic PragueDemocratic Republic of the Congo KinshasaDenmark CopenhagenEcuador QuitoEgypt CairoFinland HelsinkiFrance Lyon and Paris
Gabon LibrevilleGermany Berlin, Dusseldorf, Frankfurt, Hamburg,
and MunichGreece AthensGuatemala GuatemalaHungary BudapestIceland Reykjavik India Mumbai and New DelhiIndonesia JakartaIran (Islamic Republic of) TehranIraq BaghdadIreland DublinIsrael Jerusalem and Tel AvivItaly Milan and RomeJamaica KingstonJapan Osaka Kobe and TokyoJordan AmmanKenya NairobiKuwait Kuwait
Countries and Territories Cities
Lao People’s Democratic Republic VientianeLesotho MaseruLibyan Arab Jamahiriya TripoliLuxembourg LuxembourgMadagascar AntananarivoMalawi LilongweMalaysia Kuala LumpurMauritius Port LouisMexico Mexico City and MontereyMorocco CasablancaMozambique MaputoMyanmar YangonNetherlands Amsterdam and WillemstadNew Zealand Auckland and WellingonNicaragua ManaguaNigeria Lagos
Norway OsloOman MuscatPakistan KarachiPanama Panama CityPapua New Guinea Port MoresbyParaguay AsuncionPeru LimaPhilippines ManilaPoland WarsawPortugal Funchal and LisbonPuerto Rico San JuanQatar DohaRepublic of Korea SeoulRomania BucharestRussian Federation Moscow, Mumansk, St. Petersburg, and
Vladivosto
Saudi Arabia Al Khobar, Jeddah, and RiyadhSenegal DakarSingapore SingaporeSlovakia BratislavaSlovenia LjubljanaSouth Africa Johannesburg and PretoriaSpain Barcelona and MadridSri Lanka ColomboSudan KhartoumSwaziland MbabaneSweden StockholmSwitzerland Zurich and GenevaSyrian Arab Republic DamascusThailand BangkokTogo LomeTrinidad and Tobago Port of Spain
Tunisia TunisTurkey IstanbulUnited Arab Emirates Abu Dhabi and DubaiUnited Kingdom of Great Britain and Northern Ireland London and Manchester
United States of America Atlanta, Boston, Chicago, Denver, Detroit, Honolulu, Houston, Lexington, Los Angeles, Miami, Minneapolis, New York, Pittsburgh, San Francisco, Seattle, and Washington
Uruguay MontevideoUzbekistan TashkentVenezuela (Bolivarian Republic of) Caracas and Puerto OrdazViet Nam Hanoi and Ho Chi MinhZambia LusakaZimbabwe Harare
The second source of price data is ERC.38 Also a marketresearch firm, ERC compiles retail price data from its indus-try sources and publishes them annually in the series, “TheWorld Cigarette Market.” Prices from the ERC are deriveddirectly from this publication and not modified in any way.The third source of data is the TMA.39 Prices from the TMA
17
-
reflect the average cost of a pack of 20 cigarettes during asingle year. Domestic and imported cigaretts are not pre-sented separately in this case.
The final sources of price data in the Profiles are reportsfrom individuals living in each country. ACS and WHOenlisted help from NGOs and WHO country focal points for abiannual survey, beginning in March 2000. The survey asksfor the prices of packs of 20 cigarettes in three categories.The categories of cigarettes are 1) Marlboro King Size Filter,2) the most popular foreign brand if Marlboro was not avail-able, and 3) the most popular domestic brand. Table 6 liststhe countries and cities whose price reports come from the2000 ACS/WHO price survey. The name of the individual whoreported the price is also listed.
Table 6. ACS/WHO 2000 Price SurveyCountry City Date Participant
Antigua and Barbuda St. John’s 9-Mar Janice AlexanderBarbados Bridgetown 7-Mar Samuel DeaneBelarus Minsk 20-Mar Irina TioukhlovaBelize Belize 2-Mar Victor RosadoBosnia and Herzegovina Banja Luka 16-Mar Zivana GavricBrazil Rio de Janeiro Mar Vera Luiza da Costa e
SilvaBulgaria Sofia 27-Mar Kiril MilenkovBulgaria Sofia 10-Mar Tinka TroevaBulgaria Sofia 10-Mar George KotarovCambodia Phnom Penh 6-Mar Greg Hallen
Cook Islands Avarua 3-Mar Edwina TangardaDominica Roseau 4-MarEstonia Tallinn 7-Mar Andrus LipandGeorgia Tbilisi 4-Mar Revaz TataradzeGhana Accra 29-Feb Seth Koranteng Kazakhstan Astana 1-Mar Bruce HankeLebanon Beirut 20-Mar Norbert HirschhornLebanon Beirut 1-Mar Michel DaherLithuania Kaunas 7-Mar Tomas StanikasMalta Floriana 16-Mar Maria EllulMauritius Port Louis 2-Feb D. Carmagnoue
Mongolia Ulaanbaatar 1-Mar Mitsuaki ToyodaNepal Kathmandu 14-Jan Mrigendra Raj PandeyPalau Koror 14-Mar Annabel LymanRepublic of Moldova Kishinev 13-Mar Tudor VasilievRussian Federation Moscow 1-Mar Tatayana KamardinaSaint Vincent and the Grenadines Kingstown 3-Mar Hyacinth Bacchus
Slovakia Martin 1-Mar Elena KavcovaSolomon Islands Honiara 1-Apr Dennie IniakwalaSudan Khartoum 21-Mar Ali IdrisUnited Republic of Tanzania Moshi 2-Mar Nancy Tesha
Market share by cigarette manufacturer. The market shareof the top four manufacturers is presented for some coun-tries. The following abbreviations are used in place of somemanufacturers’ full names:
ATW Austria Tabak AGB & H Rothmans, Benson & Hedges (RBH)BAT British American TobaccoCNTC China National Tobacco CorporationFTR Fabriques de Tabac Réunies SA (Philip Morris SA)JT Japan TobaccoKT & G Korea Tobacco & Ginseng Corporation
MO Modi Group (local manager of Godfrey PhilipsIndia)
MTC Malaysian Tobacco Co. (subsidiary of BritishAmerican Tobacco)
OGT Organisation Generale de TabacsPM Philip MorrisPMI Philip Morris InternationalPWT PWT Augustow (BAT Polska)RJR R.J. ReynoldsSNTA Societe Nationle des Tabacs et AllumettesTTWMB Taiwan Tobacco and Wine MonopolyWWT WWT Poznan (Reemtsma)ZPT ZPT Krakow (Philip Morris)The data were derived from the ERC’s “The World
Cigarette Market,” the “Maxwell Consumer Report onInternational Tobacco,”39 the Tobacco Reporter’s secondarypublication of the “Maxwell Report,” and the TMA.40 The“Maxwell Report” was first developed in the mid-1960s, withemphasis on the European region. Currently, the report con-tains data on market shares and industry trends in 50 to 60countries.41 In 1993, the monthly trade magazine, TheTobacco Reporter, first included a portion of “The MaxwellConsumer Report” in its publication and it is now a biannualfeature in the magazine.
Infrastructure for Tobacco ControlGovernment and non-government organizations engagedin tobacco control & national tobacco control provisionsGovernment and non-government organizations engagedin tobacco control. For each country, the Profiles provides alist of up to nine government and non-government organiza-tions committed to tobacco control. In most countries, morethan nine national organizations are working towardstobacco control; however, due to space constraints in thetwo-page profile, not all organizations are listed. The inclu-sion or exclusion of organizations in no way reflects their rel-ative contributions and is not an endorsement by ACS, CDC,or WHO. In the development of each country or territory’slist, efforts were made to include both government and non-government organizations in the directory and to confirmthat the contact information was correct as of May 2000. Thenames of organizations are listed alone if contact informationcould not be verified.
The development of the contact lists began with searchesof public and private sources that provide information aboutorganizations involved in national tobacco control activities.GLOBALink’s members were the first audience for a Profilessurvey designed to measure the development of nationalorganizations devoted to tobacco control. The InternationalTobacco-Control Network (ITCN) or “GLOBALink” is man-aged by the UICC and serves as a virtual network for tobacco
18
-
control advocates on the Internet.42 All members were invitedto complete an online questionnaire asking respondents toidentify focal points for tobacco control efforts in their coun-try or territory and to describe activities in seven areas: advo-cacy in government, policy development, youth education(school-based), worksite education, media campaigns, ces-sation services, and programs with health professionals.Respondents were asked to categorize these activities aseither “national” or “local (sub-national)” efforts. When appli-cable, respondents also provided information about collabo-rative activities between government and non-governmentorganizations and the year that the activities commenced. Inaddition to GLOBALink members online, surveys were sent tomembers by mail and facsimile.
WHO country focal points for tobacco control, nationalcancer organizations, scholarship applicants to the 11thWorld Conference, Action on Smoking and Health (ASH)members and International Non Government CoalitionAgainst Tobacco (INGCAT) members were also asked torespond to the survey. Internet searches were used to iden-tify other organizations engaged in tobacco control. National Tobacco Control Provisions. National tobacco con-trol “provisions” refer to all national laws, ministerial, royaland presidential decrees, regulations, and voluntary codes ofpractice between industries, organizations, and the govern-ment. Throughout this section, the word “national” isintended to describe regional provisions in Hong Kong (spe-cial administrative region of China), provincial provisions inTaiwan (province of China) and territorial provisions in the
West Bank and Gaza Strip. The Profiles divides nationaltobacco provisions into six categories: prohibitions andrestrictions on advertising and sponsorship, health promo-tion and education efforts against tobacco, sales and distri-bution requirements, tobacco product regulations,smoke-free indoor air restrictions, and other provisions toinclude the formation of a national or territorial committee ontobacco control. One of four symbols appears beside the pro-visions if sources suggested that it is either included in leg-islation and regulations or voluntarily included in industry ororganizations’ codes of practice. Provisions without anysymbol beside them were not found in any source reviewedby the American Cancer Society; however, the absence of theprovision from these sources does not necessarily mean thatthe provision does not exist in a country. Furthermore, thepresence of a tobacco control provision in legislative text orsecondary reports from country representatives does notmean that the measure is enforced to the full extent of thelaw. Table 7 defines the symbols used in this section. Table 8provides a list of the provisions in each category, the sym-bols that could appear beside the provision, and an explana-tion of relationship between the provision and each symbol.
Table 7.Symbol Definition
B National legislation and/or regulations ban (prohibit) the conduct ofthe listed activity
R National legislation and/or regulations place restrictions on the con-duct of the listed activity
X Provision is included in national legislation and/or regulationsV Provision exists through voluntary action and is not included in
national legislation and/or regulations
19
Table 8.Category and Provisions Symbol Definition
Advertising and Sponsorship:Product advertising bans X Media type or advertising strategies can not be used to advertise tobacco in accordance with national legislation and/or
regulationsV Tobacco industry has absolutely suspended its use of media types or advertising strategies through a voluntary code of
practice Product advertising restrictions X Tobacco advertising is allowed, but national legislation and/or regulations govern its use
V Tobacco industry has restricted its use of media types or advertising strategies through a voluntary code of practice Sponsorship bans X Tobacco industry sponsorship of events is absolutely prohibited by national legislation and/or regulations
V Tobacco industry has absolutely suspended its sponsorship of events through a voluntary code of practiceSponsorship restrictions X Tobacco industry sponsorship of events is allowed, but national legislation and/or regulations govern the practice
V Tobacco industry has restricted its sponsorship of events through a voluntary code of practice
Health Promotion and Education:Health education curricula or programs X School education about the dangers of tobacco use is mandated by national legislation and/or regulations
V Schools include education about the dangers of tobacco use in their curriculums voluntarily, with assistance fromgovernment and/or non-government organizations (as reported by NGOs)
Public information initiatives X Public information initiatives about the dangers of tobacco use are mandated by national legislation and/or regulationsV National government and/or non-government organizations conduct regular public information initiatives about the dan-
gers of tobacco use without a legislative mandate from the government (as reported by NGOs)
Sales and Distribution:Free products or samples B Free products and industry sampling practices are absolutely prohibited by national legislation and/or regulations
R Free products and industry sampling practices are allowed, but national legislation and/or regulations govern thesepractices
V Tobacco industry has voluntarily restricted the distribution of free products or samples Tobacco sales restricted to certain X Retail tobacco sales are not permitted in some facilities and locations according to national legislation and/or locations regulations
-
20
Table 8. (cont.)Category and Provisions Symbol Definition
Sales and Distribution: (cont.)Tobacco sales restricted to certain V Tobacco industry voluntarily limits the locations were tobacco products are soldlocationsSales of smokeless tobacco prohibited X Retail sale or trade in smokeless tobacco products is not allowed by national legislation and/or regulationsSales/distribution to minors prohibited X Individuals under a certain age may not purchase cigarettes or another tobacco product according to national legislation
and/or regulationsVending machines B The sale of tobacco products through automatic vending machines is prohibited by national legislation and/or
regulationsR Tobacco products may be sold through automatic vending machines, but national legislation and/or regulations govern
these salesV All tobacco retailers and manufacturers have voluntarily suspended or restricted tobacco sales through automatic vend-
ing machines Other restrictions on tobacco sales X See Appendix B for details about nationally mandated restrictions
V See Appendix B for details about voluntary restrictions
Tobacco Product Regulations:Health warning on packaging X National laws and/or regulations mandate printed health warnings on tobacco product packaging
V Tobacco product manufacturers voluntarily print a health warning on tobacco product packagingIngredient control: maximum X The national government determined the maximum permissible yield of nicotine per cigarettenicotine yield V Tobacco manufactures voluntarily adhere to a standard nicotine yield Ingredient control: toxic constituents/ X The national government determined the maximum permissible yields of tar and other toxic constituents per cigarettemaximum tar yield V Tobacco manufactures voluntarily adhere to a standard yield of toxic contentsIngredient disclosure on packaging X National laws and/or regulations mandate printed disclosure of, at minimum, the tar and nicotine yields per cigarette on
tobacco product packagingV Tobacco product manufacturers voluntarily disclose, at minimum, the tar and nicotine yields per cigarette on tobacco
product packaging
Smoke-free Indoor Air:Aircraft (domestic flights) B Smoking is absolutely prohibited aboard aircraft during flights within national borders according to national legislation
and/or regulationsR Smoking is restricted to certain areas aboard aircraft during flights within national borders according to national legisla-
tion and/or regulationsV Airline voluntarily prohibits or restricts smoking aboard their aircraft during flights within national borders
Aircraft (international flights) B Smoking is absolutely prohibited aboard aircraft during flights between two countries according to national legislationand/or regulations
R Smoking is restricted to certain areas aboard aircraft during flights between two countries according to national legisla-tion and/or regulations
V Airline voluntarily prohibits or restricts smoking aboard their aircraft during flights between two countriesEducational facilities B Smoking is prohibited in educational facilities according to national legislation and/or regulations; facilities with a desig-
nated smoking area are included in this category if non-smoking areas must always remain uncontaminated by smokeR Smoking is restricted, but not prohibited in educational facilities according to national legislation and/or regulationsV Educational facilities voluntarily prohibit or restrict smoking in areas under their management
Government buildings B Smoking is prohibited in government buildings according to national legislation and/or regulations; facilities with a des-ignated smoking area are included in this category if non-smoking areas must always remain uncontaminated by smoke
R Smoking is restricted, but not prohibited in government buildings according to national legislation and/or regulationsV Government buildings voluntarily prohibit or restrict smoking in areas under their management
Health care facilities B Smoking is prohibited in health care facilities according to national legislation and/or regulations; facilities with a desig-nated smoking area are included in this category if non-smoking areas must always remain uncontaminated by smoke
R Smoking is restricted, but not prohibited in health care facilities according to national legislation and/or regulationsV Health care facilities voluntarily prohibit or restrict smoking in areas under their management
Public transportation B Smoking is absolutely prohibited in public transportation vehicles according to national legislation and/or regulationsR Smoking is restricted, but not prohibited in public transportation vehicles according to national legislation and/or
regulationsV Owners of public transportation vehicles voluntarily prohibit or restrict smoking in their vehicles
Workplaces B Smoking is prohibited in workplaces according to national legislation and/or regulations; facilities with a designatedsmoking area are included in this category if non-smoking areas must always remain uncontaminated by smoke
R Smoking is restricted, but not prohibited in workplaces according to national legislation and/or regulationsV Employers voluntarily prohibit or restrict smoking in areas under their management
Other public places X See Appendix B for information about smoking bans or restrictions in other public places in accordance with nationallegislation and/or regulations
V See Appendix B for information about smoking bans or restrictions in other public places in accordance with voluntaryagreements
Other Provisions:National committee on tobacco control X National regulations and/or regulations mandate the formation of a national committee to address issues specific to
tobacco controlV Government and non-government organizations voluntarily formed a national coalition to address issues related to
tobacco control (as reported by NGOs)
-
Legislative data for the Profiles were collected from sev-eral sources: WHO’s International Health Legislative Digest(IDHL),43 Ruth Roemer’s book, “Legislative Action to Combatthe World Tobacco Epidemic,”44 ERC’s “World CigaretteMarket,” the USDA, “The Maxwell Consumer Report,” theTMA and its industry sources45 and the aforementioned NGOsurveys collected by ACS. The CDC also gathered legislativedata by searching the following sources: 1) national govern-ment homepages and country-specific sites on the Internet,2) Lexis-Nexis International Tax Directory, 3) Library ofCongress, Global Information Legal Network, and 4) the per-sonal database of Dr. Judith Mackay of the Asian Consultancyon Tobacco Control.
In addition, requests for the full text of tobacco laws andregulations were made to WHO’s Health Legislative Unit andWHO Regional Offices. When the full text of the provisionwas available, characterization of its content was derivedsolely from the original text. The name of the organizationthat reviewed the text of the law is listed in Appendix B. Theappendix also provides the details and dates of implementa-tion of some tobacco control provisions.
Pharmaceutical Treatment for TobaccoDependenceData on pharmaceutical treatment for tobacco dependence inthe Profiles is limited to the pharmaceutical treatments cur-rently available in each country, the product’s dosage form,and legal and advertising status. Legal status refers towhether the product is sold only in pharmacies (with or with-out a prescription), sold over the counter (without a pre-scription from a doctor), or sold only with a doctor’sprescription. These data were provided by PinneyAssociates,a consultant firm to SmithKline Beecham ConsumerHealthcare and were collected from several commercial andinternal sources of retail sales and regulatory information. Toensure that the data reflected the worldwide availability of allpharmaceutical treatments for tobacco dependence (not onlynicotine replacement products), information from SmithKlinewas compared to information from other pharmaceuticalmanufacturers that have smoking cessation products.46 Thepharmaceutical data presented in the Profiles do not addressthe public’s level of access to the products or other non-phar-maceutical cessation methods. Determining the availability ofbehavioral treatments was beyond the scope of the Profilesproject.
ConclusionThe Profiles monograph is intended to serve as a referencetool for those working in the fields of tobacco control andsurveillance research. Readers should direct questions about
the data to either ACS-Department of Epidemiology andSurveillance Research,47 WHO-Tobacco Free Initiative orCDC-Office on Smoking and Health.
References
1. World Health Organization. (1997). Tobacco or health: a global statusreport. Geneva, Switzerland.2. Tobacco or health: a global st
Related Documents