THYROID GLAND MJ Noon 2014-57

THYROID GLAND MJ Noon 2014-57. Anatomy of the thyroid gland Light brown, firm organ 15 – 20 gms in weight Two lateral lobes connected by an isthmus 4.
Dec 22, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
THYROID GLANDTHYROID GLAND
MJ Noon 2014-57MJ Noon 2014-57

Anatomy of the thyroid glandAnatomy of the thyroid gland
•Light brown, firm organ•15 – 20 gms in weight•Two lateral lobes connected by an isthmus•4 x 2 cm in dimension; 20 – 40 mm thickness•Pyramidal lobe present in 80% of normal persons; usually left of midline•Four parathyroid glands closely related•Recurrent laryngeal nerves on both sides
•Light brown, firm organ•15 – 20 gms in weight•Two lateral lobes connected by an isthmus•4 x 2 cm in dimension; 20 – 40 mm thickness•Pyramidal lobe present in 80% of normal persons; usually left of midline•Four parathyroid glands closely related•Recurrent laryngeal nerves on both sides

Anatomy of the thyroid glandAnatomy of the thyroid gland
Biosynthesis of T4 and T3Biosynthesis of T4 and T3
The process includes• Dietary iodine (I) ingestion• Active transport and uptake of iodide (I-) by
thyroid gland• Oxidation of I- and iodination of
thyroglobulin (Tg) tyrosine residues • Coupling of iodotyrosine residues (MIT and
DIT) to form T4 and T3
• Proteolysis of Tg with release of T4 and T3
into the circulation
The process includes• Dietary iodine (I) ingestion• Active transport and uptake of iodide (I-) by
thyroid gland• Oxidation of I- and iodination of
thyroglobulin (Tg) tyrosine residues • Coupling of iodotyrosine residues (MIT and
DIT) to form T4 and T3
• Proteolysis of Tg with release of T4 and T3
into the circulation
4
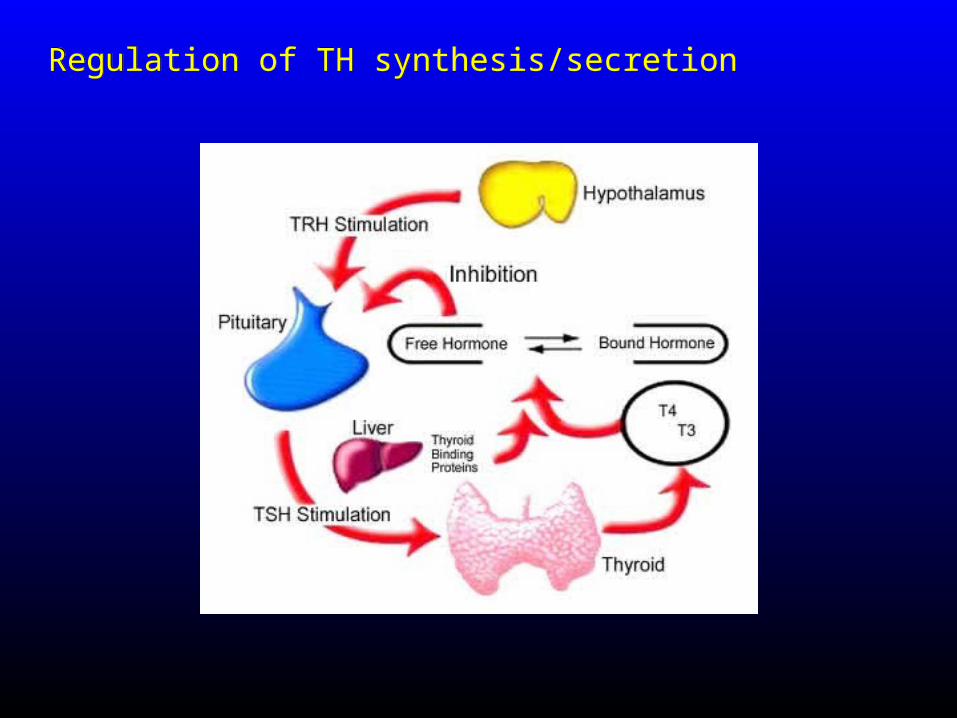
Regulation of TH synthesis/secretionRegulation of TH synthesis/secretion
Normal circulatory concentrationsNormal circulatory concentrations
– T4 4.5-11 g/dL
– T3 60-180 ng/dL (~100-fold less than T4)
– T4 4.5-11 g/dL
– T3 60-180 ng/dL (~100-fold less than T4)
6
Carriers for Circulating Thyroid Hormones
Carriers for Circulating Thyroid Hormones
• More than 99% of circulating T4 and T3 is bound to plasma carrier proteins– Thyroxine-binding globulin (TBG), binds
about 75%– Transthyretin (TTR), also called thyroxine-
binding prealbumin (TBPA), binds about 10%-15%
– Albumin binds about 7%– High-density lipoproteins (HDL), binds
about 3%
• Carrier proteins can be affected by physiologic changes, drugs, and disease
• More than 99% of circulating T4 and T3 is bound to plasma carrier proteins– Thyroxine-binding globulin (TBG), binds
about 75%– Transthyretin (TTR), also called thyroxine-
binding prealbumin (TBPA), binds about 10%-15%
– Albumin binds about 7%– High-density lipoproteins (HDL), binds
about 3%
• Carrier proteins can be affected by physiologic changes, drugs, and disease
7
Thyroid Hormone Plays a Major Role in Growth and DevelopmentThyroid Hormone Plays a Major
Role in Growth and Development
• Thyroid hormone initiates or sustains differentiation and growth– Stimulates formation of proteins– Is essential for normal brain development
• Essential for childhood growth– Untreated congenital hypothyroidism or
chronic hypothyroidism during childhood can result in incomplete development and mental retardation
• Thyroid hormone initiates or sustains differentiation and growth– Stimulates formation of proteins– Is essential for normal brain development
• Essential for childhood growth– Untreated congenital hypothyroidism or
chronic hypothyroidism during childhood can result in incomplete development and mental retardation
8
Thyroid Hormones and the Central Nervous System (CNS)
Thyroid Hormones and the Central Nervous System (CNS)
• Thyroid hormones are essential for neural development and maturation and function of the CNS
• Decreased thyroid hormone concentrations may lead to alterations in cognitive function– Patients with hypothyroidism may
develop impairment of attention, slowed motor function, and poor memory
– Thyroid-replacement therapy may improve cognitive function when hypothyroidism is present
• Thyroid hormones are essential for neural development and maturation and function of the CNS
• Decreased thyroid hormone concentrations may lead to alterations in cognitive function– Patients with hypothyroidism may
develop impairment of attention, slowed motor function, and poor memory
– Thyroid-replacement therapy may improve cognitive function when hypothyroidism is present 9

Thyroid Hormone Influences the Female Reproductive System
Thyroid Hormone Influences the Female Reproductive System
• Normal thyroid hormone function is important for reproductive function
– Hypothyroidism may be associated with menstrual disorders, infertility, risk of miscarriage, and other complications of pregnancy
• Normal thyroid hormone function is important for reproductive function
– Hypothyroidism may be associated with menstrual disorders, infertility, risk of miscarriage, and other complications of pregnancy
10

Thyroid Hormone is Critical for Normal Bone Growth
Thyroid Hormone is Critical for Normal Bone Growth
– T3 also may participate in osteoblast
differentiation and proliferation, and chondrocyte maturation leading to bone ossification
– T3 also may participate in osteoblast
differentiation and proliferation, and chondrocyte maturation leading to bone ossification
11

Thyroid Hormone Regulates Mitochondrial Activity
Thyroid Hormone Regulates Mitochondrial Activity
• T3 is considered the major regulator of mitochondrial activity
– A potent T3-dependent transcription
factor of the mitochondrial genome induces early stimulation of transcription and increases transcription factor (TFA) expression
– T3 stimulates oxygen consumption by the
mitochondria
• T3 is considered the major regulator of mitochondrial activity
– A potent T3-dependent transcription
factor of the mitochondrial genome induces early stimulation of transcription and increases transcription factor (TFA) expression
– T3 stimulates oxygen consumption by the
mitochondria
12
Thyroid Hormones Stimulate Metabolic Activities in Most
Tissues
Thyroid Hormones Stimulate Metabolic Activities in Most
Tissues
• Thyroid hormones (specifically T3)
regulate rate of overall body
metabolism– T3 increases basal metabolic rate
• Calorigenic effects– T3 increases oxygen consumption by most
peripheral tissues
– Increases body heat production
• Thyroid hormones (specifically T3)
regulate rate of overall body
metabolism– T3 increases basal metabolic rate
• Calorigenic effects– T3 increases oxygen consumption by most
peripheral tissues
– Increases body heat production
13

Evaluation of patients with Thyroid gland disorder
Evaluation of patients with Thyroid gland disorder
THREE MAIN CATEGORIES• HYPOFUNCTION• HYPERFUNCTION• ENLARGMENTS/GOITER– DIFFUSE ENLARGMENT– NODULAR ENLARGMENT
THREE MAIN CATEGORIES• HYPOFUNCTION• HYPERFUNCTION• ENLARGMENTS/GOITER– DIFFUSE ENLARGMENT– NODULAR ENLARGMENT
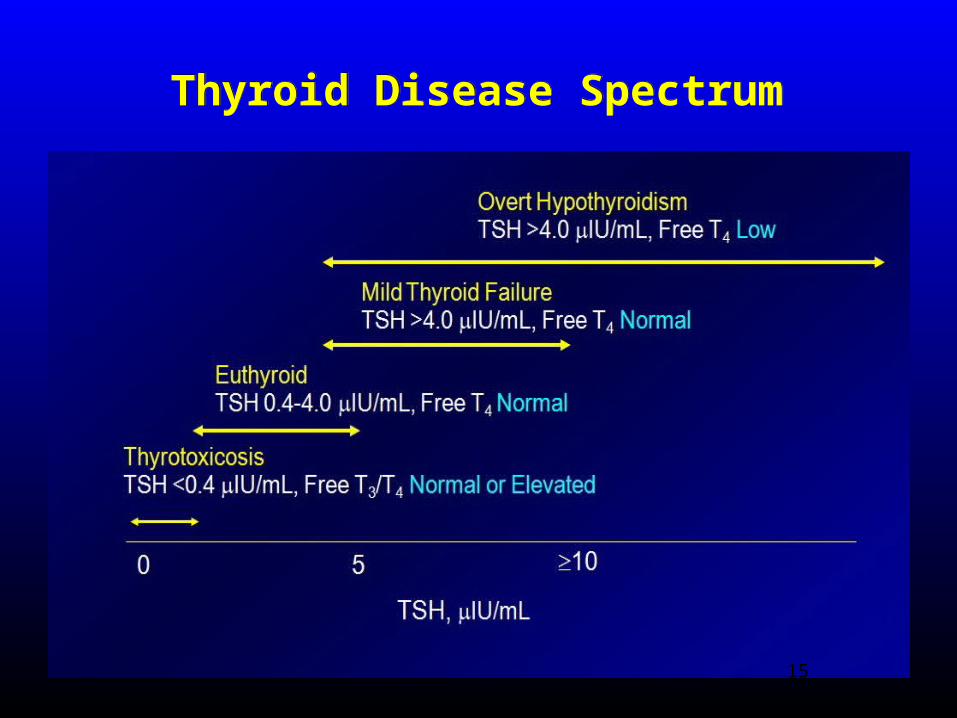
Thyroid Disease SpectrumThyroid Disease Spectrum
15
Clinical evaluationClinical evaluation• HISTORY AND PHYSICAL EXAMINATION• Clinical manifestations:
– HYPERFUNCTION• Weight loss, irritability, heat intolerance, thinning of hair,
palpitations, tachycardia– HYPOFUNCTION
• Weight gain, lethargy, coarse hair, cold intolerance, thick skin, slowed muscle reflex, constipation, slow mentation
– GOITER• Anterior neck mass that moves on deglutition is thyroid
gland in origin unless proven otherwise; enlarged thyroid gland
• Physical Examination:– Accurate description of the thyroid gland and mass– Appreciate presence or absence of associated cervical
lymphadenopathy
• HISTORY AND PHYSICAL EXAMINATION• Clinical manifestations:
– HYPERFUNCTION• Weight loss, irritability, heat intolerance, thinning of hair,
palpitations, tachycardia– HYPOFUNCTION
• Weight gain, lethargy, coarse hair, cold intolerance, thick skin, slowed muscle reflex, constipation, slow mentation
– GOITER• Anterior neck mass that moves on deglutition is thyroid
gland in origin unless proven otherwise; enlarged thyroid gland
• Physical Examination:– Accurate description of the thyroid gland and mass– Appreciate presence or absence of associated cervical
lymphadenopathy
Thyroid Function TestsThyroid Function Tests• T3 AND T4 LEVELS
• Serum TSH and TRH
• Free and bound ratio
• Plain films; X-Rays(chest/thoracic inlet;clinical evidence of tracheal deviation,compression,retrosternal extension)
• Ultrasonography(solid/cystic)or radioisotope scanning(99mTc-sodium pertechnate) for differentiating between
A. HOT nodules (actively functioning)
B. COLD nodules (non-functioning)
C. COOL (normaly functioning) MRI and CT (EXTENT OF GOITRE) FNAC(nature of thyroid nodules) Thyroid antibodies
• T3 AND T4 LEVELS
• Serum TSH and TRH
• Free and bound ratio
• Plain films; X-Rays(chest/thoracic inlet;clinical evidence of tracheal deviation,compression,retrosternal extension)
• Ultrasonography(solid/cystic)or radioisotope scanning(99mTc-sodium pertechnate) for differentiating between
A. HOT nodules (actively functioning)
B. COLD nodules (non-functioning)
C. COOL (normaly functioning) MRI and CT (EXTENT OF GOITRE) FNAC(nature of thyroid nodules) Thyroid antibodies
HYPERTHYROIDISMHYPERTHYROIDISM• Clinical syndrome of excess
thyroid hormone in the circulation
• Two dominant types or causes:
– Grave’s disease
– Toxic multinodular or solitary nodular goiter (Plummer’s disease)
• Can be PRIMARY (increased Thyroid hormone independent of TSH) or SECONDARY (increased in hormone due to increased TSH)
• Clinical syndrome of excess thyroid hormone in the circulation
• Two dominant types or causes:
– Grave’s disease
– Toxic multinodular or solitary nodular goiter (Plummer’s disease)
• Can be PRIMARY (increased Thyroid hormone independent of TSH) or SECONDARY (increased in hormone due to increased TSH)
HYPERTHYROIDISM/THYROTOXICOSIS
HYPERTHYROIDISM/THYROTOXICOSIS
SIGNSI. sinus
TachycardiaII. Hot,moist
palmsIII.ExosphthalmosIV.Lid lagV. AgitationVI.Thyroid goitre
SIGNSI. sinus
TachycardiaII. Hot,moist
palmsIII.ExosphthalmosIV.Lid lagV. AgitationVI.Thyroid goitre
SYMPTOMSI. TirednessII.Emotional labilityIII.Heat intoleranceIV.Wt.lossV.Excessive
appetiteVI.palpitations
SYMPTOMSI. TirednessII.Emotional labilityIII.Heat intoleranceIV.Wt.lossV.Excessive
appetiteVI.palpitations
19
Graves’ disease (diffuse toxic goiter)Graves’ disease (diffuse toxic goiter)• Most common cause of primary hyperthyrodism• Female dominant autoimmune disease• Inciting events; infection, steroid withdrawal,
postpartum, iodide excess• Anti-TSH receptor antibodies(IgG),type2
hypersensitivity• TSI can cross placenta so neonatal thyrotoxicosis
can occur• LABS;
A. Raised T3,T4
B. Low TSH
C. TSH producing response to TRH is absent because of atrophy of pituitary TSH producing cells
• Most common cause of primary hyperthyrodism• Female dominant autoimmune disease• Inciting events; infection, steroid withdrawal,
postpartum, iodide excess• Anti-TSH receptor antibodies(IgG),type2
hypersensitivity• TSI can cross placenta so neonatal thyrotoxicosis
can occur• LABS;
A. Raised T3,T4
B. Low TSH
C. TSH producing response to TRH is absent because of atrophy of pituitary TSH producing cells

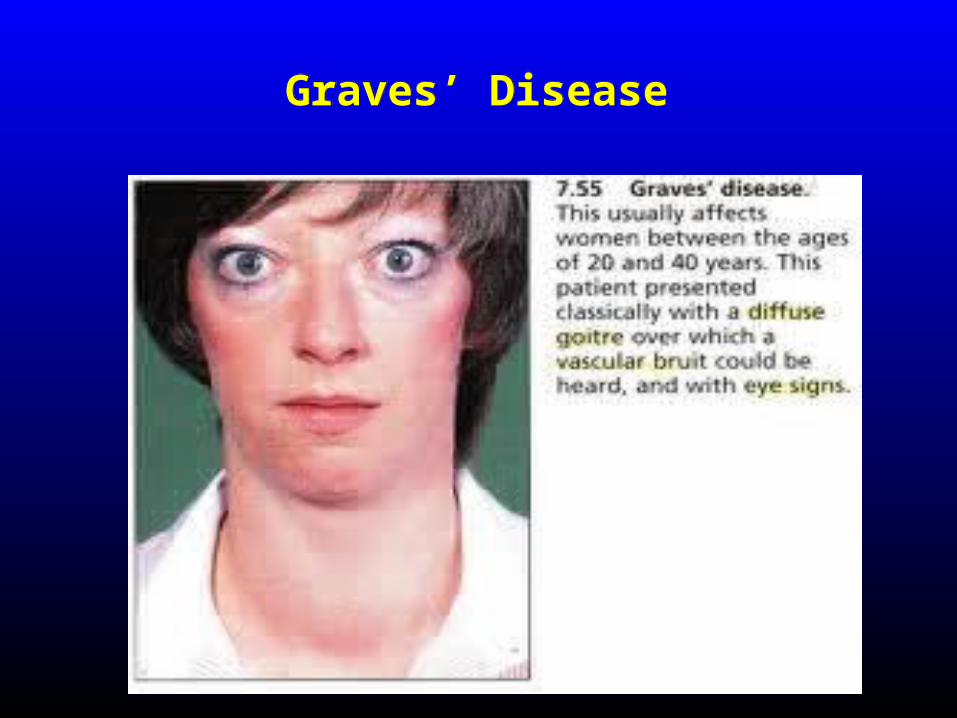
Graves’ DiseaseGraves’ Disease• CLINACAL FEATURES; INFILTRATIVE OPHTHALMOPATHY Proptosis of eye(volume of retro-orbital connective
tissue is increased; inflamation,GAGS,fatty infiltration;orbital fibroblasts have TSH receptor and become targets of antibody attack)
Pretibial myxedema( GAGS in dermis) Thyroid acropachy;
a) Digital swelling
b) Finger clubbing
• Cardiac problems;CHF,AF• Apathy,muscle weakness• thyromegaly
• CLINACAL FEATURES; INFILTRATIVE OPHTHALMOPATHY Proptosis of eye(volume of retro-orbital connective
tissue is increased; inflamation,GAGS,fatty infiltration;orbital fibroblasts have TSH receptor and become targets of antibody attack)
Pretibial myxedema( GAGS in dermis) Thyroid acropachy;
a) Digital swelling
b) Finger clubbing
• Cardiac problems;CHF,AF• Apathy,muscle weakness• thyromegaly
21
Graves’ DiseaseGraves’ Disease
22
Graves’ DiseaseGraves’ Disease
• Manage graves by 1)anti-thyroid drugs and,2)radioactive iodine ablation<CI in preg.> 3)surgery; subtotal-thyroidectomy
• Manage graves by 1)anti-thyroid drugs and,2)radioactive iodine ablation<CI in preg.> 3)surgery; subtotal-thyroidectomy
23
Multinodular Toxic Goiter (Plummer’s disease)Multinodular Toxic Goiter (Plummer’s disease)
• One or more thyroid nodules trapping and organifying more iodine and increase secretion of hormone independent of TSH control; autonomously functioning nodule/s
• No exophthalmos or pretibial myxoedema (Milder with no extrathyroidal manifestations)• Demonstrate increased uptake or radioactive iodine I131
localized to the nodule/s • Hot nodules on scan• Poor response to radioactive iodine treatment; surgery
is the choice of management
• One or more thyroid nodules trapping and organifying more iodine and increase secretion of hormone independent of TSH control; autonomously functioning nodule/s
• No exophthalmos or pretibial myxoedema (Milder with no extrathyroidal manifestations)• Demonstrate increased uptake or radioactive iodine I131
localized to the nodule/s • Hot nodules on scan• Poor response to radioactive iodine treatment; surgery
is the choice of management
Thyroid StormThyroid Storm• Rare but life-threatening complication of hyperthyroidism• Induced by thyroidal or non-thyroidal surgery; can be induced by
infection or other forms of stress (eg. Labor & delivery, pulmonary infection, after RAI treatment)
• Signs and symptoms of severe thyrotoxicosis– Hyperpyrexia, severe tachycardia, irritability, vomiting,
diarrhea, and proximal muscle weakness; cause of death due to high cardiac output
• Management:– Prevention is the best management– Immediate control of tachycardia, mechanical cooling, oxygen
and volume resuscitation– Steroids– Intravenous beta-blockers (propranolol)– Anti-thyroid drugs and Iodine solution– Peritoneal dialysis in extreme cases
• Rare but life-threatening complication of hyperthyroidism• Induced by thyroidal or non-thyroidal surgery; can be induced by
infection or other forms of stress (eg. Labor & delivery, pulmonary infection, after RAI treatment)
• Signs and symptoms of severe thyrotoxicosis– Hyperpyrexia, severe tachycardia, irritability, vomiting,
diarrhea, and proximal muscle weakness; cause of death due to high cardiac output
• Management:– Prevention is the best management– Immediate control of tachycardia, mechanical cooling, oxygen
and volume resuscitation– Steroids– Intravenous beta-blockers (propranolol)– Anti-thyroid drugs and Iodine solution– Peritoneal dialysis in extreme cases
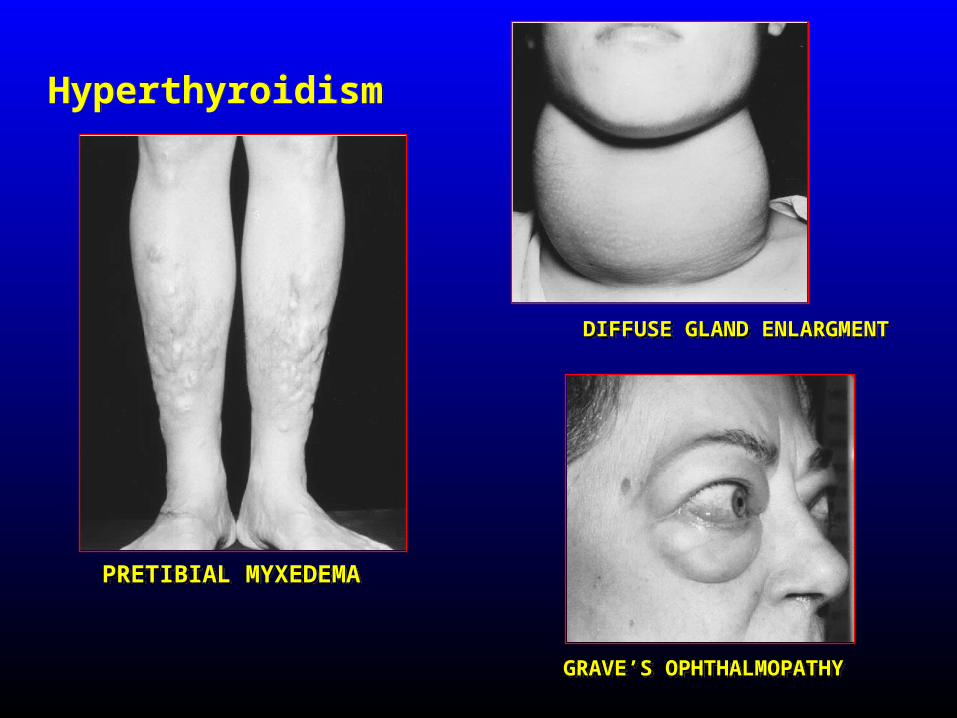
HyperthyroidismHyperthyroidism
PRETIBIAL MYXEDEMAPRETIBIAL MYXEDEMA
DIFFUSE GLAND ENLARGMENTDIFFUSE GLAND ENLARGMENT
GRAVE’S OPHTHALMOPATHYGRAVE’S OPHTHALMOPATHY
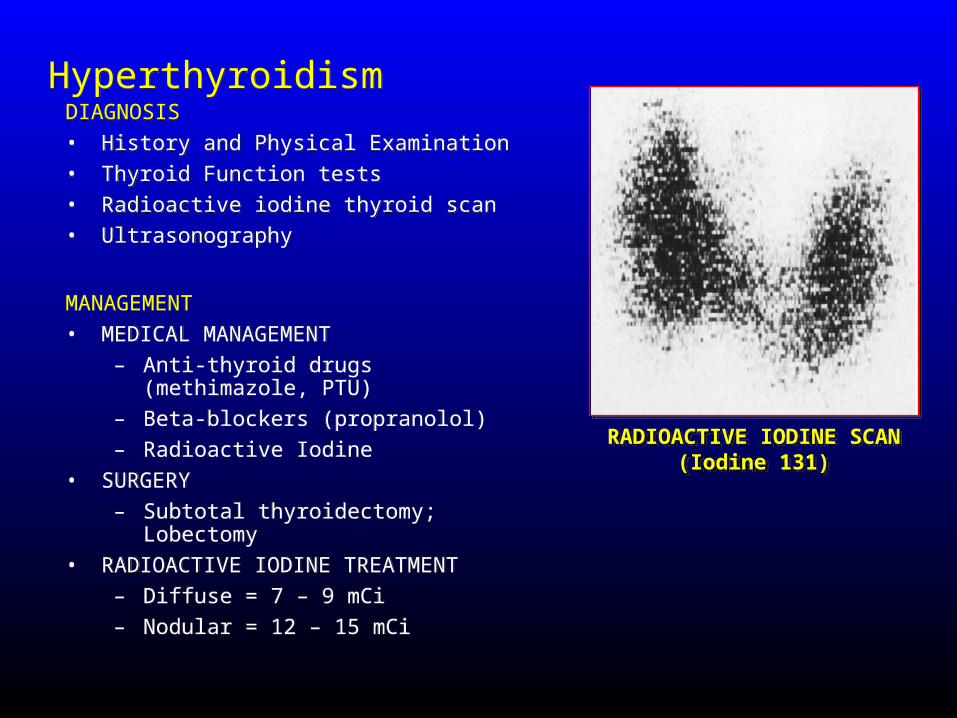
HyperthyroidismHyperthyroidismDIAGNOSIS• History and Physical Examination• Thyroid Function tests• Radioactive iodine thyroid scan• Ultrasonography
MANAGEMENT• MEDICAL MANAGEMENT
– Anti-thyroid drugs (methimazole, PTU)
– Beta-blockers (propranolol)– Radioactive Iodine
• SURGERY– Subtotal thyroidectomy; Lobectomy
• RADIOACTIVE IODINE TREATMENT– Diffuse = 7 – 9 mCi– Nodular = 12 – 15 mCi
DIAGNOSIS• History and Physical Examination• Thyroid Function tests• Radioactive iodine thyroid scan• Ultrasonography
MANAGEMENT• MEDICAL MANAGEMENT
– Anti-thyroid drugs (methimazole, PTU)
– Beta-blockers (propranolol)– Radioactive Iodine
• SURGERY– Subtotal thyroidectomy; Lobectomy
• RADIOACTIVE IODINE TREATMENT– Diffuse = 7 – 9 mCi– Nodular = 12 – 15 mCi
RADIOACTIVE IODINE SCAN(Iodine 131)
RADIOACTIVE IODINE SCAN(Iodine 131)
HYPOTHYROIDISMHYPOTHYROIDISM
• Syndrome of deficient circulating levels of thyroid hormone
• Cretinism in neonates – neurological impairment and mental retardation
• Clinical manifestations:– Myxedema (severe
form)– Bradycardia &
cardiomegaly• Laboratory:
– Decreased T3 and T4; Elevated TSH
• Management:– Thyroxine replacement
• Syndrome of deficient circulating levels of thyroid hormone
• Cretinism in neonates – neurological impairment and mental retardation
• Clinical manifestations:– Myxedema (severe
form)– Bradycardia &
cardiomegaly• Laboratory:
– Decreased T3 and T4; Elevated TSH
• Management:– Thyroxine replacement
THYROID CANCERTHYROID CANCER
• The most common endocrine malignancy that requires surgery
• Included in the top 10 sites of malignancy for both sexes in the Philippines
• Generally slow-growing and indolent malignancy
• AGE – considered the most important prognostic factor
• Certain types are also aggressive malignancy and potentially fatal disease
• The most common endocrine malignancy that requires surgery
• Included in the top 10 sites of malignancy for both sexes in the Philippines
• Generally slow-growing and indolent malignancy
• AGE – considered the most important prognostic factor
• Certain types are also aggressive malignancy and potentially fatal disease
THYROID CANCERTHYROID CANCER• MAJOR HISTOLOGIC TYPES
• PAPILLARY THYROID CANCER– Most common (70%); well-differentiated– Slow-growing; lymphatic spread– Good prognosis• FOLLICULAR THYROID CANCER– Well-differentiated; 2nd most common
(10%)– More aggressive; vascular invasion and
spread• MIXED PAPILLARY-FOLLICULAR THYROID
CANCER– Behaves and managed as papillary
carcinoma• HURTHLE-CELL TUMOR– 5% incidence; intermediate differentiation– Behaves like follicular carcinoma but
spread by lymphatics
• MAJOR HISTOLOGIC TYPES• PAPILLARY THYROID CANCER
– Most common (70%); well-differentiated– Slow-growing; lymphatic spread– Good prognosis• FOLLICULAR THYROID CANCER– Well-differentiated; 2nd most common
(10%)– More aggressive; vascular invasion and
spread• MIXED PAPILLARY-FOLLICULAR THYROID
CANCER– Behaves and managed as papillary
carcinoma• HURTHLE-CELL TUMOR– 5% incidence; intermediate differentiation– Behaves like follicular carcinoma but
spread by lymphatics
THYROID CANCERTHYROID CANCER• MAJOR HISTOLOGIC TYPES
• LYMPHOMA (5%)– Usually in females; history of previous
hashimoto’s– Surgery for compressive symptoms– Chemo and radiation sensitive• MEDULLARY THYROID CANCER– Aggressive; calcitonin producing tumor– 90% sporadic; 10% part of the MEN II
syndrome– Does not uptake I131
– Poor prognosis; undifferentiated carcinoma• ANAPLASTIC THYROID CANCER– Worst prognosis; very aggressive– 30% developed from well-differentiated
cancer (degeneration)– Chemo and radiation treatment– Palliatve surgery
• MAJOR HISTOLOGIC TYPES• LYMPHOMA (5%)
– Usually in females; history of previous hashimoto’s
– Surgery for compressive symptoms– Chemo and radiation sensitive• MEDULLARY THYROID CANCER– Aggressive; calcitonin producing tumor– 90% sporadic; 10% part of the MEN II
syndrome– Does not uptake I131
– Poor prognosis; undifferentiated carcinoma• ANAPLASTIC THYROID CANCER– Worst prognosis; very aggressive– 30% developed from well-differentiated
cancer (degeneration)– Chemo and radiation treatment– Palliatve surgery

• MANAGEMENT• SURGERY• LOBECTOMY + ISTHMUSECTOMY• TOTAL THYROIDECTOMY• INDICATED NECK DISSECTION
• ADJUVANT TREATMENT• POSTOPERAIVE RADIOACTIVE IODINE
TREATMENT• EXTERNAL BEAM RADIATION• CHEMOTHERAPY (emerging)
• MANAGEMENT• SURGERY• LOBECTOMY + ISTHMUSECTOMY• TOTAL THYROIDECTOMY• INDICATED NECK DISSECTION
• ADJUVANT TREATMENT• POSTOPERAIVE RADIOACTIVE IODINE
TREATMENT• EXTERNAL BEAM RADIATION• CHEMOTHERAPY (emerging)
THYROID CANCERTHYROID CANCER
INDICATIONS FOR THE PERFORMANCE OF THYROID
SURGERY
INDICATIONS FOR THE PERFORMANCE OF THYROID
SURGERY
• Thyroid enlargement (Goiter) causing compression symptoms (dysphagia, dyspnea)• Certain types of Hyperthyroidism• Thyroid Nodule/s or Thyroid Cancer• Cosmetic indication
• Thyroid enlargement (Goiter) causing compression symptoms (dysphagia, dyspnea)• Certain types of Hyperthyroidism• Thyroid Nodule/s or Thyroid Cancer• Cosmetic indication
Types of thyroid surgeriesTypes of thyroid surgeries
• SUBTOTAL-THYROIDECTOMY• TOTAL-THYROIDECTOMY(bilateral
lobectomy)• ISTHMUSECTOMY• NEAR-TOTAL THYROIDECTOMY(total thyroid
lobectomy on affected side with conservation of 1-2grm of thyroid on contralateral side to preserve blood flow to parathyroids
• SUBTOTAL-THYROIDECTOMY• TOTAL-THYROIDECTOMY(bilateral
lobectomy)• ISTHMUSECTOMY• NEAR-TOTAL THYROIDECTOMY(total thyroid
lobectomy on affected side with conservation of 1-2grm of thyroid on contralateral side to preserve blood flow to parathyroids
34
HAEMORRHAGE NERVE DAMAGE HYPOTHYROIDISM HYPOPARATHYROIDISM Wound infection(abscess must be drained) Respiratory obstruction(kinking of trachea,laryngeal
oedema,trauma during intubation)
HAEMORRHAGE NERVE DAMAGE HYPOTHYROIDISM HYPOPARATHYROIDISM Wound infection(abscess must be drained) Respiratory obstruction(kinking of trachea,laryngeal
oedema,trauma during intubation)
Complications of thyroid surgeryComplications of thyroid surgery
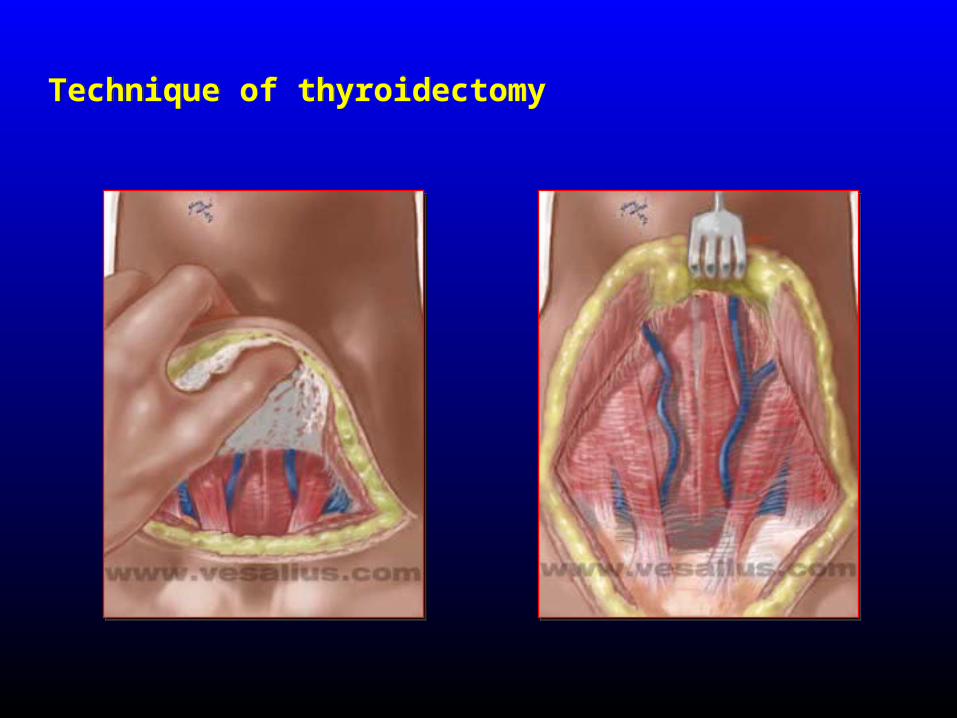
Technique of thyroidectomyTechnique of thyroidectomy
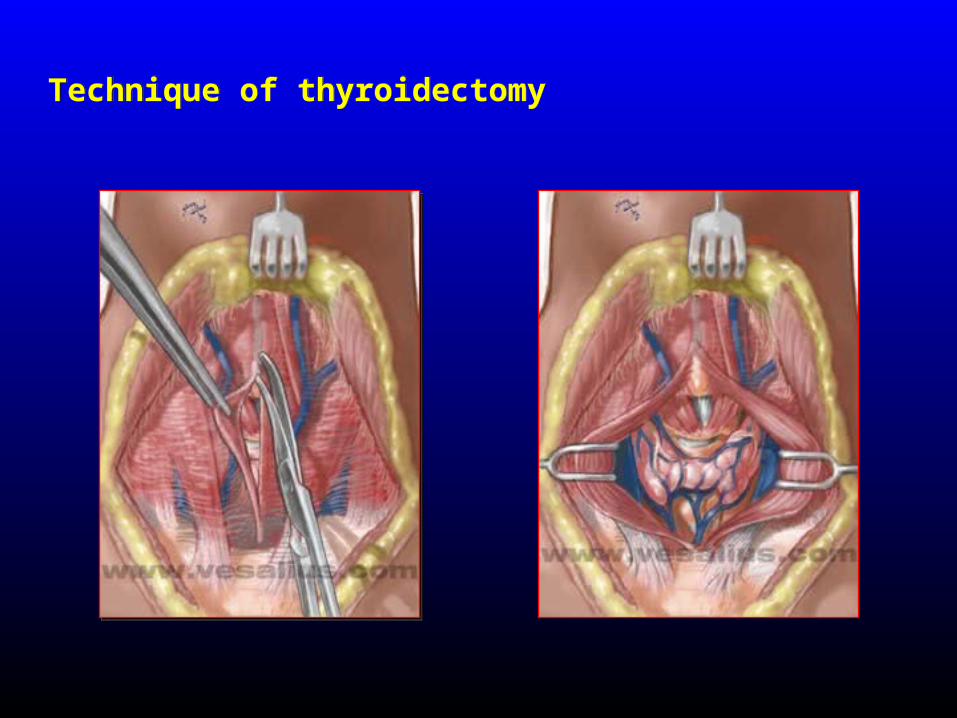
Technique of thyroidectomyTechnique of thyroidectomy

Technique of thyroidectomyTechnique of thyroidectomy
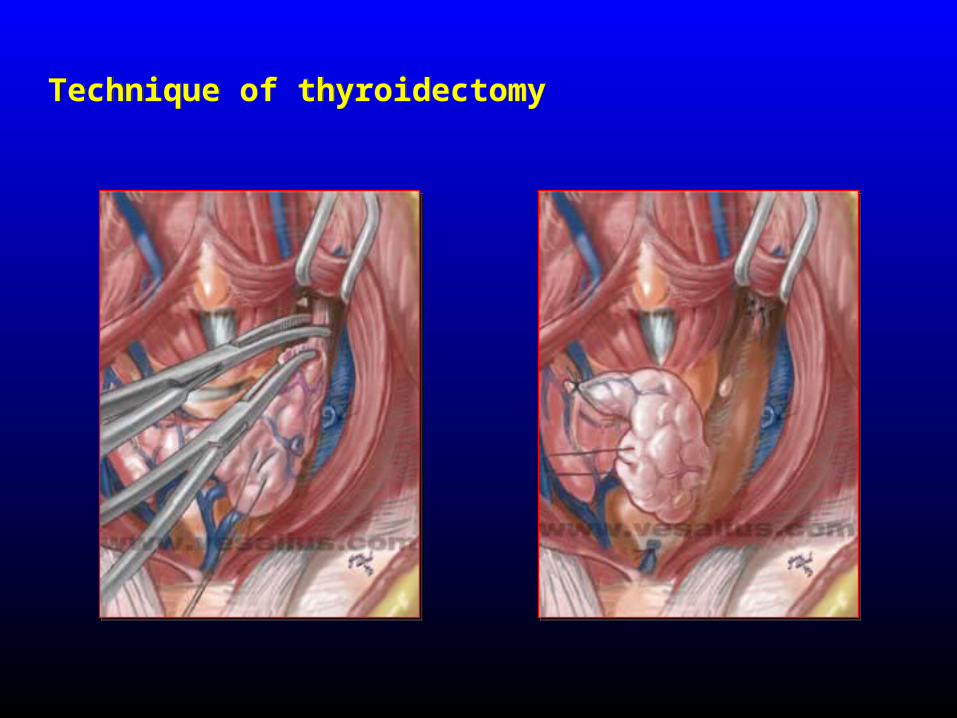
Technique of thyroidectomyTechnique of thyroidectomy
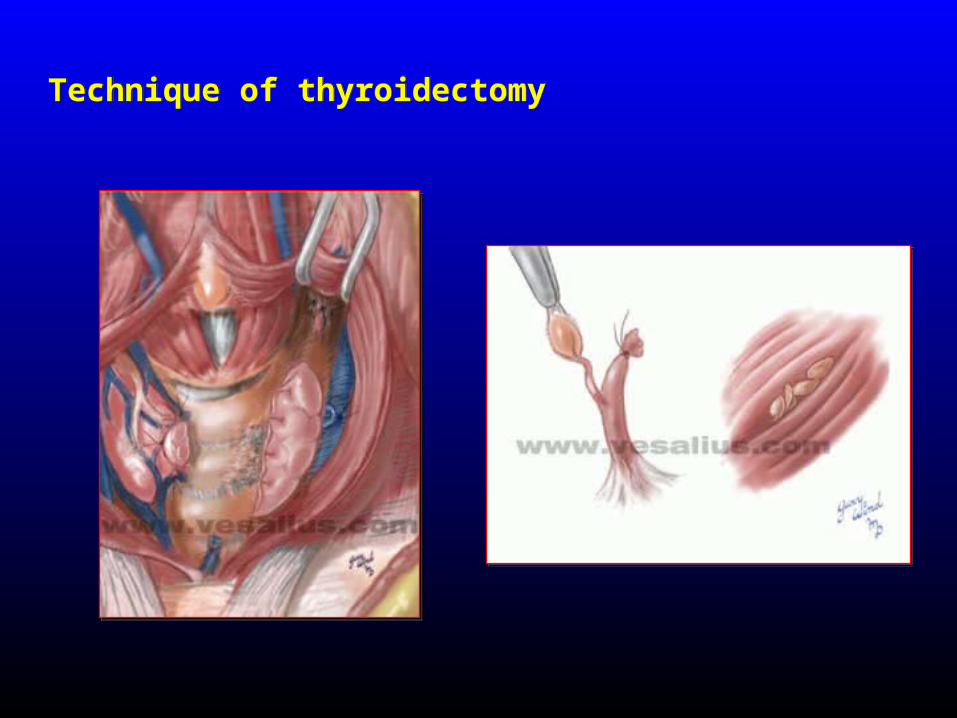
Technique of thyroidectomyTechnique of thyroidectomy
THANK YOUTHANK YOU
Related Documents