Mardin mazhar Shanga ismail Hawnaz hamasalh Hwda mhamad

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Mardin mazhar
Shanga ismail
Hawnaz hamasalh
Hwda mhamad
Second largest endocrine gland in body,Small butterfly shaped gland located at base of neck below the sternocleidomastoid muscles
Thyroid is controlled by the hypothalmus
and pituitary
Weighs 18-60gms in adults,Histologically it is made up of follicular and parafollicular cells.
Introduction of thyrodgland
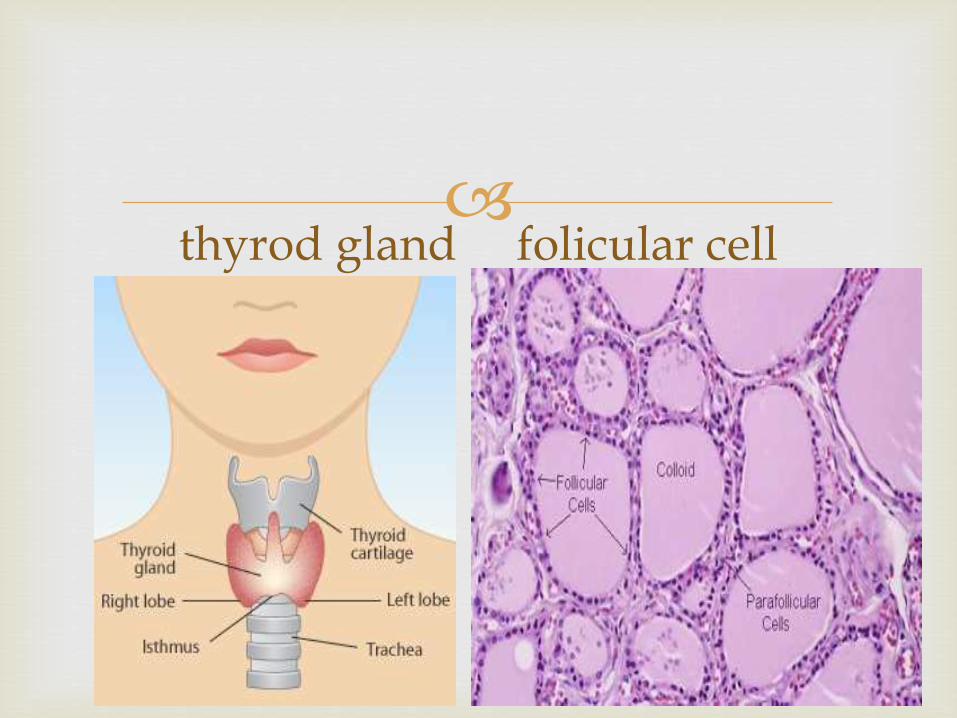
thyrod gland folicular cell
Stimulates & maintains metabolic processes
Produces thyroid hormones T3-triiodothyronine and T4-thyroxine
These hormones regulate metabolism & affect the growth and function of other systems in the body
Secretes calcitonin to lower serum calcium levels
Parathyroid gland secretes PTH to raise serum calcium levels
function
Metabolic stimulants of:
Neural and skeletal development
Oxygen consumption at rest
Stimulating bone turnover by increasing formation and resorption
Promoting chronitropic and ionotropic effects
Increasing number of catecholamine receptors in heart
Increasing production of RBC
Altering the metabolism of carbs, fats, and protein
Function cont……..

T3 (Triiodothyronine) & T4
(Tetraiodothyronine Stored in Follicles (round sacs) in the thyroid filled
with thyroglobulin, a thyroid protein. Dietary iodine enters follicles where they are stored as
T3 and T4
T4 is converted to T3 by peripheral organs such as kidney, liver, and spleen
T3 is 10x more active than T 4
Only 20% of total T3 is secreted by thyroid
Hormones: T3 & T4
T4-thyroxine contains 4 iodine atoms
It is a slow-acting pre-hormone
T4 takes 4 days to peak in blood
Half-life 7 days
Overall effects take 6 weeks
T3 is the active and faster-acting hormone
The immediate effects of T3 last 1-2 days
Half-life 1.5 days
Hormones: T4
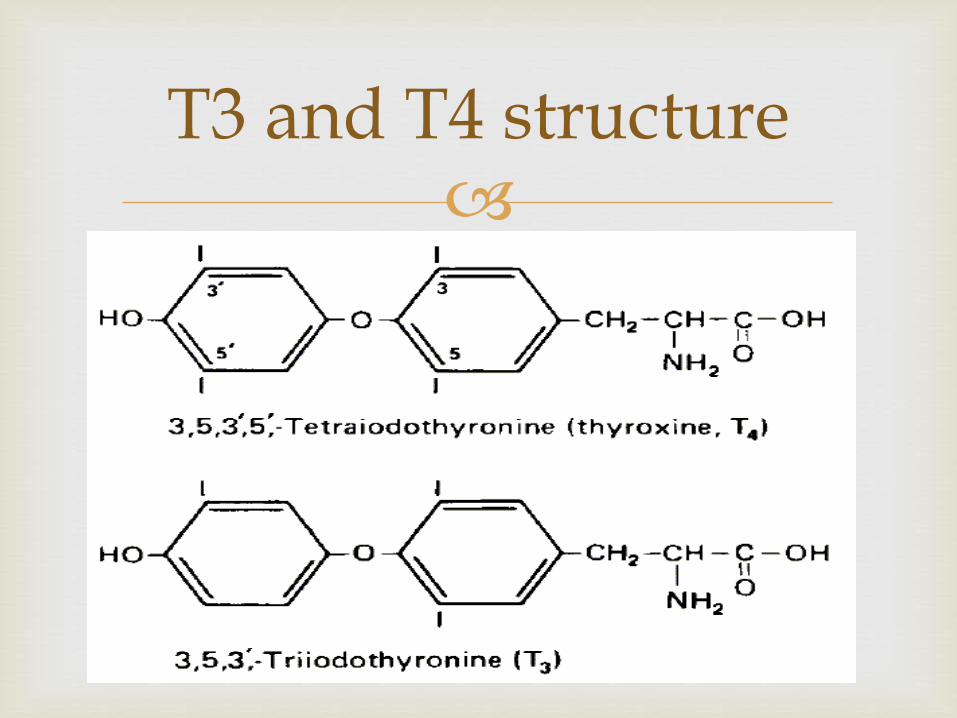
T3 and T4 structure
Dietary Iodide is removed from the bloodstream by
means of an active pump
The pump can concentrate iodide in the follicular sacs at 350x greater than the blood concentration
Oxidation of iodide by thyroid peroxidase converts iodide iodine
Peripheral de-iodination of T4 to T3 is regulated by many factors including health, nutritional status, and other hormones
Iodine
TSH
TSH is a pituitary hormone
Controlled by TRH-thyrotropin releasing hormone from hypothalamus
Functions to stimulate thyroid hormone production
May enlarge thyroid (goiter) when under producing
Labs:
High TSH indicates low thyroid hormone= hypo
Low TSH indicates high thyroid hormone = hyper
Hormones- TSH
Produced by thyroid to regulate serum calcium
levels
Calcitonin stimulates movement of calcium into bone
Parathyroid hormone (PTH) opposite effect of calcitonin
Hormones-Calcitonin & PTH

Negative Feedback System
TRH
T3 & T4 Thyroid
TSH
The disruption of any of these mechanisms can cause abnormal levels of T3 and T4 leading to thyroid disease
Primary Hypothyroidism
Disease of the thyroid gland
Secondary Hypothyroidism
Hypothalamic-pituitary diseases (reduced TSH)
Hypothyroidism
PRIMARY
Congenital Agenesis
Ectopic thyroid remnants
Defects of hormone synthesis Iodine deficiency
Dyshormonogenesis
Antithyroid drugs
Other drugs (e.g. lithium, amiodarone, interferon)
Causes of Hypothyroidism
Autoimmune Atrophic thyroiditis
Hashimoto's thyroiditis
Postpartum thyroiditis
Infective Post-subacute thyroiditis
Causes of Hypothyroidism
Iatrogenic Radioactive iodine therapy External neck irradiation post-surgery
Infiltration amyloidosis, sarcoidosis, hemochromatosis,
scleroderma
Causes of Hypothyroidism
SECONDARY
Hypopituitarism: tumors, pituitary surgery or irradiation, infiltrative disorders, Sheehan's syndrome, trauma, genetic forms of combined pituitary hormone deficiencies
Isolated TSH deficiency or inactivity
Hypothalamic disease: tumors, trauma, infiltrative disorders, idiopathic
Although anyone can develop hypothyroidism, you're at an increased risk if you:
Are a woman older than age 60 Have an autoimmune disease Have a close relative, such as a parent or grandparent, with an
autoimmune disease Have been treated with radioactive iodine or anti-thyroid
medications Received radiation to your neck or upper chest Have had thyroid surgery (partial thyroidectomy) Have been pregnant or delivered a baby within the past six
months
Risk factor
Fatigue Increased sensitivity to cold Constipation Dry skin Unexplained weight gain Puffy face Hoarseness Muscle weakness Elevated blood cholesterol level Muscle aches, tenderness and stiffness Pain, stiffness or swelling in your joints Heavier than normal or irregular menstrual periods Thinning hair Slowed heart rate Depression Impaired memory
signs and symptom
Diagnosis of hypothyroidism is based on your
symptoms and the results of blood tests that measure the level of TSH and sometimes the level of the thyroid hormone thyroxine. A low level of thyroxineand high level of TSH indicate an underactive thyroid. That's because your pituitary produces more TSH in an effort to stimulate your thyroid gland into producing more thyroid hormone.
diagnosis
Replacement therapy with levothyroxine (thyroxine, i.e. T4) is given for life. In the young and fit, 100 - 150 μg daily is suitable.
thyroid function tests after at least 2 months on a steady dose
the aim is to restore T4 and TSH to well within the normal range
An annual thyroid function test is recommended .
Treatment
Excessive amounts of the hormone can cause side
effects, such as:
Increased appetite
Insomnia
Heart palpitations
Shakiness
Goiter. Constant stimulation of your thyroid to release
more hormones may cause the gland to become larger —a condition known as a goiter.
Heart problems. Hypothyroidism may also be associated with an increased risk of heart disease, primarily because high levels of low-density lipoprotein (LDL) cholesterol — the "bad" cholesterol — can occur in people with an underactive thyroid.
Mental health issues. Depression may occur early in hypothyroidism and may become more severe over time. Hypothyroidism can also cause slowed mental functioning.
Complication
Peripheral neuropathy. Long-term uncontrolled hypothyroidism can
cause damage to your peripheral nerves — the nerves that carry information from your brain and spinal cord to the rest of your body,
Myxedema. This rare, life-threatening condition is the result of long-term, undiagnosed hypothyroidism. Its signs and symptoms include intense cold intolerance and drowsiness followed by profound lethargy and unconsciousness.
Infertility. Low levels of thyroid hormone can interfere with ovulation, which impairs fertility.
Birth defects. Babies born to women with untreated thyroid disease may have a higher risk of birth defects than may babies born to healthy mothers. These children are also more prone to serious intellectual and developmental problems. Infants with untreated hypothyroidism present at birth are at risk of serious problems with both physical and mental development.
Hyperthyroidism - result of excessive thyroid
function
major etiologies of thyrotoxicosis are hyperthyroidism caused by Graves' disease, toxic MNG, and toxic adenomas
Hyperthyrodism
Common
Graves' disease (autoimmune)
Toxic multinodular goitre
Solitary toxic nodule/adenoma
Causes of hyperthyroidism
Graves' disease. Graves' disease, an autoimmune
disorder in which antibodies produced by your immune system stimulate your thyroid to produce too much T-4, is the most common cause of hyperthyroidism.
Hyperfunctioning thyroid nodules (toxic adenoma, toxic multinodular goiter, Plummer's disease). This form of hyperthyroidism occurs when one or more adenomas of your thyroid produce too much T-4. An adenoma is a part of the gland that has walled itself off from the rest of the gland, forming noncancerous (benign) lumps that may cause an enlargement of the thyroid. Not all adenomas produce excess T-4, and doctors aren't sure what causes some to begin producing too much hormone.
Reasons for too much thyroxine (T-4)

Thyroiditis. Sometimes your thyroid gland can
become inflamed for unknown reasons. The inflammation can cause excess thyroid hormone stored in the gland to leak into your bloodstream. One rare type of thyroiditis, known as subacutethyroiditis, causes pain in the thyroid gland. Other types are painless and may sometimes occur after pregnancy (postpartum thyroiditis).
Cont……
Hyperthyrodism
Clinical features: due to
Hypermetabolic state
Overactivity of sympathetic nervous system

Symptoms
Weight loss
Increased appetite
Irritability
Tremor
Goiter
Restlessness
Stiffness
Muscle weakness
Breathlessness
Palpitation
Heat intolerance
Excessive sweating
Itching
Thirst
Vomiting
Diarrhoea
Oligomenorrhoea
Loss of libido
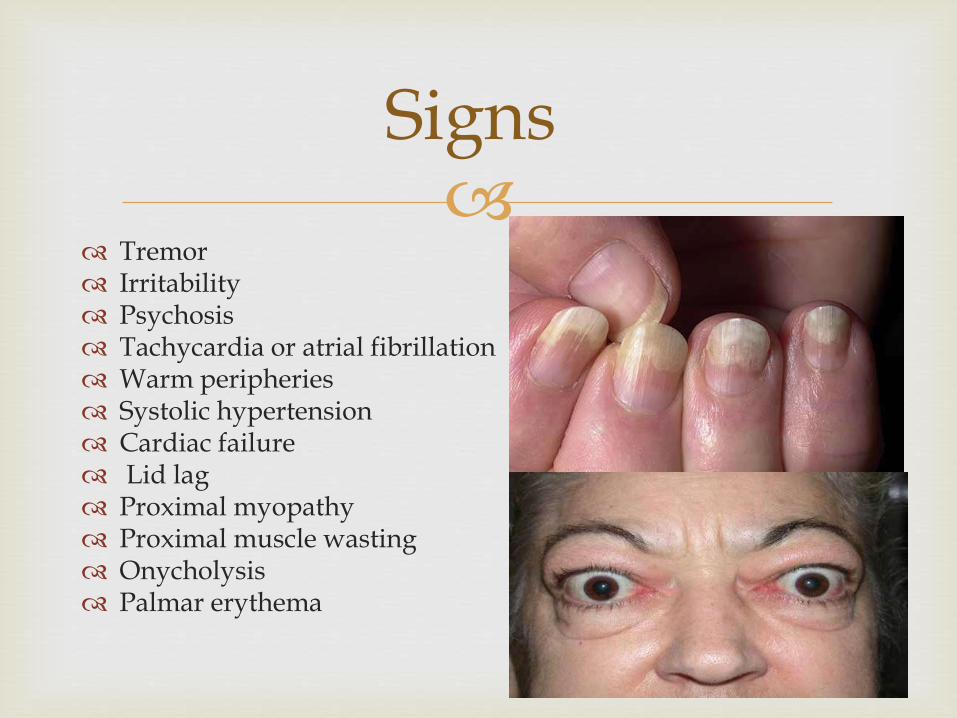
Signs
Tremor Irritability Psychosis Tachycardia or atrial fibrillation Warm peripheries Systolic hypertension Cardiac failure Lid lag Proximal myopathy Proximal muscle wasting Onycholysis Palmar erythema
Medical history and physical exam. During the exam your doctor may try to detect a slight tremor in your fingers when they're extended, overactive reflexes, eye changes and warm, moist skin. Your doctor will also examine your thyroid gland as you swallow.
Blood tests. A diagnosis can be confirmed with blood tests that measure the levels of thyroxine and TSH in your blood. High levels of thyroxine and low or nonexistent amounts of TSH indicate an overactive thyroid.
diagnosis
Radioactive iodine uptake test. For this test, you take a
small, oral dose of radioactive iodine (radioiodine). Over time, the iodine collects in your thyroid gland because your thyroid uses iodine to manufacture hormones. You'll be checked after two, six or 24 hours — and sometimes after all three time periods — to determine how much iodine your thyroid gland has absorbed.
A high uptake of radioiodine indicates your thyroid gland is producing too much thyroxine. The most likely cause is either Graves' disease or hyperfunctioning nodules.
If blood tests indicate hyperthyroidism, your doctor may recommend one of the following tests to help determine why your thyroid is
overactive:
Thyroid scan. During this test, you'll have a
radioactive isotope injected into the vein on the inside of your elbow or sometimes into a vein in your hand. You then lie on a table with your head stretched backward while a special camera produces an image of your thyroid on a computer screen.
The time needed for the procedure may vary, depending on how long it takes the isotope to reach your thyroid gland. You may have some neck discomfort with this test, and you'll be exposed to a small amount of radiation.

Treatment
Antithyroid drugs:
1. Carbimazole.
2. Propylthiouracil.
These drugs inhibit the formation of thyroid hormones
common side effects - rash, urticaria, fever, and arthralgia
Rare but major side effects include hepatitis; an SLE-like syndrome; and, most important, agranulocytosis
Treatment
Radioactive iodine
RAI accumulates in the thyroid and destroys the gland by local radiation.
It takes several months to be fully effective.
Surgery:
subtotal thyroidectomy
Only in patient who have previously been rendered euthyroid.
Goiter
Goiter refers to an enlarged thyroid gland
Biosynthetic defects, iodine deficiency, autoimmune disease, and nodular diseases can each lead to goiter
diffuse nontoxic goiter - diffuse enlargement of the thyroid occurs in the absence of nodules and hyperthyroidism
Worldwide, diffuse goiter is most commonly caused by iodine deficiency and is termed endemic goiter
Congenital Thyroid Diseases
Agenesis /Aplasia
Hypoplasia
Accessory or aberrant thyroid glands
Thyroglossal duct cyst
Thyroglossal Duct Cyst
A thyroglossal duct cyst is a neck mass or lump that develops from cells and tissues remaining after the formation of the thyroid gland during embryonic development.
Children
Failure of regression
Neck, medial
Squamous or columnar lining
often appears after an upper respiratory infection when it enlarges and becomes painful.
Complications: inflammation,
sinus tracts
History: A 50 year old housewife complains of progressive
weight gain of 20 pounds in 1 year, fatigue, postural dizziness, loss of memory, slow speech, deepening of her voice, dry skin, constipation, and cold intolerance.
Physical examination: Vital signs include a temperature 96.8oF, pulse 58/minute and regular, BP 110/60. She is moderately obese and speaks slowly and has a puffy face, with pale, cool, dry, and thick skin. The thyroid gland is not palpable. The deep tendon reflex time is delayed.
Laboratory studies: CBC and differential WBC are normal. The serum T4 concentration is 3.8 ug/dl (N=4.5-12.5), the serum TSH is 1 uU/ml (N=0.2-3.5), and the serum cholesterol is 255 mg/dl (N<200)
Case with hypothyrodism

History: A 35 year old nurse complained of nervousness, mood
swings, weakness, and palpitations with exertion for the past 6 months. Recently, she noticed excessive sweating and wanted to sleep with fewer blankets than her husband. She used oral contraceptives and her menstrual periods were regular.
Physical examination: Pulse was 92/minute and BP was 130/60. She appeared anxious, with a smooth, warm, and moist skin, a fine tremor, a bounding cardiac apical impulse, and she couldn't rise from a deep knee bend without aid. Her thyroid was diffusely enlarged, soft, mobile, without nodularity and there was no lymphadenopathy. Her eyes were not prominent (proptotic) and she had no focal skin thickening.
Laboratory studies: Serum T4=15.6 ug/dl and serum T3=210 ng/dl.
Case with hyperthyrodism
Thank you
Related Documents











