REGULAR ARTICLE Thromboxane and prostacyclin biosynthesis in patients with acute spontaneous intracerebral hemorrhage Pertti Saloheimo a, * , Seppo Juvela a,b , Asko Riutta a,c , Juhani Pyhtinen a,d , Matti Hillbom a a Department of Neurology, Oulu University Central Hospital, Oulu, Finland b Department of Neurosurgery, Helsinki University Central Hospital, Helsinki, Finland c Department of Pharmacological Sciences, University of Tampere and Tampere University Hospital, Tampere, Finland d Department of Diagnostic Radiology, Oulu University Central Hospital, Oulu, Finland Received 19 April 2004; received in revised form 18 August 2004; accepted 24 August 2004 Available online 30 September 2004 Abstract Objective: Elevated levels of 11-dehydrothromboxane B 2 (11-dehydro-TXB 2 ) excreted in urine have been observed in acute ischemic stroke. This marker of platelet activation has not been investigated in patients with acute spontaneous intracerebral hemorrhage (ICH). Methods: We examined 43 patients with sponta- neous ICH and 23 controls. Urinary excretion rates of 11-dehydro-TXB 2 , 2,3-dinor- thromboxane B 2 (2,3 dinor-TXB 2 ) and 2,3-dinor-6-ketoprostaglandin F 1a (2,3-dinor- PGF 1a ) during the first week and at 3 months after ICH were compared between patients who had or had not used aspirin and controls. Results: On admission, ICH patients without aspirin use had significantly higher urinary levels of 11-dehydro- TXB 2 ( pb0.001), 2,3-dinor-TXB 2 ( pb0.001) and 2,3-dinor-PGF 1a ( p=0.019) than controls. Aspirin users had significantly lower urinary levels of these metabolites than nonusers. The metabolite levels of aspirin users on admission did not significantly differ from those of controls. The differences between aspirin users and nonusers leveled off during the following 3—5 days, however, as the blocking 0049-3848/$ - see front matter D 2004 Elsevier Ltd. All rights reserved. doi:10.1016/j.thromres.2004.08.026 Abbreviations: ICH, spontaneous intracerebral hemorrhage; 11-dehydro-TXB 2 , 11-dehydrothromboxane B 2 ; 2,3-dinor-TXB 2 , 2,3- dinor-thromboxane B 2 ; 2,3-dinor-PGF 1a , 2,3-dinor-6-ketoprostaglandin F 1a ; TXA 2 , thromboxane A 2 ; PGI 2 , prostacyclin. * Corresponding author. Tel.: +358 9 6188 5224; fax: +358 9 6188 5259. E-mail addresses: [email protected] (P. Saloheimo)8 [email protected] (S. Juvela)8 [email protected] (A. Riutta)8 [email protected] (J. Pyhtinen)8 [email protected] (M. Hillbom). KEYWORDS Cerebral hemorrhage; Hemostasis; Platelets; Thromboxane; Prostacyclin; Aspirin Thrombosis Research (2005) 115, 367 — 373 intl.elsevierhealth.com/journals/thre

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

intl.elsevierhealth.com/journals/thre
REGULAR ARTICLE
Thromboxane and prostacyclin biosynthesisin patients with acute spontaneousintracerebral hemorrhage
Pertti Saloheimoa,*, Seppo Juvelaa,b, Asko Riuttaa,c,Juhani Pyhtinena,d, Matti Hillboma
aDepartment of Neurology, Oulu University Central Hospital, Oulu, FinlandbDepartment of Neurosurgery, Helsinki University Central Hospital, Helsinki, FinlandcDepartment of Pharmacological Sciences, University of Tampere and Tampere University Hospital,Tampere, FinlanddDepartment of Diagnostic Radiology, Oulu University Central Hospital, Oulu, Finland
Received 19 April 2004; received in revised form 18 August 2004; accepted 24 August 2004Available online 30 September 2004
0049-3848/$ - see front matter D 200doi:10.1016/j.thromres.2004.08.026
Abbreviations: ICH, spontaneous idinor-thromboxane B2; 2,3-dinor-PGF1
* Corresponding author. Tel.: +358E-mail addresses: pertti.saloheimo
[email protected] (J. Pyhtinen)8
KEYWORDSCerebral
hemorrhage;Hemostasis;Platelets;Thromboxane;Prostacyclin;Aspirin
Abstract
Objective: Elevated levels of 11-dehydrothromboxane B2 (11-dehydro-TXB2)excreted in urine have been observed in acute ischemic stroke. This marker ofplatelet activation has not been investigated in patients with acute spontaneousintracerebral hemorrhage (ICH). Methods: We examined 43 patients with sponta-neous ICH and 23 controls. Urinary excretion rates of 11-dehydro-TXB2, 2,3-dinor-thromboxane B2 (2,3 dinor-TXB2) and 2,3-dinor-6-ketoprostaglandin F1a (2,3-dinor-PGF1a) during the first week and at 3 months after ICH were compared betweenpatients who had or had not used aspirin and controls. Results: On admission, ICHpatients without aspirin use had significantly higher urinary levels of 11-dehydro-TXB2 ( pb0.001), 2,3-dinor-TXB2 ( pb0.001) and 2,3-dinor-PGF1a ( p=0.019) thancontrols. Aspirin users had significantly lower urinary levels of these metabolitesthan nonusers. The metabolite levels of aspirin users on admission did notsignificantly differ from those of controls. The differences between aspirin usersand nonusers leveled off during the following 3—5 days, however, as the blocking
Thrombosis Research (2005) 115, 367—373
4 Elsevier Ltd. All rights reserved.
ntracerebral hemorrhage; 11-dehydro-TXB2, 11-dehydrothromboxane B2; 2,3-dinor-TXB2, 2,3-
a, 2,3-dinor-6-ketoprostaglandin F1a; TXA2, thromboxane A2; PGI2, prostacyclin.9 6188 5224; fax: +358 9 6188 [email protected] (P. Saloheimo)8 [email protected] (S. Juvela)8 [email protected] (A. Riutta)[email protected] (M. Hillbom).

P. Saloheimo et al.368
effect of aspirin on the production of TXA2 and PGI2 ceased. Three months after ICH,the metabolite excretion levels in all the patients were similar to those in nonusersof aspirin on admission. On admission, aspirin users had longer bleeding times( p=0.032) than nonusers, but aspirin use did not associate with impaired recovery orhematoma enlargement. Conclusions: Urinary excretion levels of 11-dehydro-TXB2,2,3-dinor-TXB2 and 2,3-dinor-PGF1a were higher in patients with acute ICH than incontrols. The levels in aspirin users were equally low as in controls but rose to thelevels of the other patients within a few days. The metabolite levels remained high 3months after ICH in all patients. Prior use of aspirin did not seem to cause hematomaenlargement.D 2004 Elsevier Ltd. All rights reserved.
Introduction
Platelet activation is increased in patients withischemic stroke and myocardial infarction, andelevated levels of thromboxane A2 (TXA2) metabo-lites excreted in urine have been observed in suchpatients [1,2,3]. However, TXA2 metabolites asmarkers of platelet activation have not beeninvestigated specifically in acute spontaneousintracerebral hemorrhage (ICH), which accountsfor about 10% of all strokes. TXA2 and prostacyclin(PGI2) are the major products of arachidonic acidmetabolism in platelets [4] and vascular endothe-lium [5], respectively. TXA2 is a potent stimulatorof platelet activation [6] and vasoconstriction [7],while PGI2 inhibits platelet aggregation and inducesvasodilation [8]. Endogenous TXA2 and PGI2 biosyn-thesis can be quantitated reliably by measuringtheir metabolites (11-dehydrothromboxane B2, 2,3-dinor-thromboxane B2 and 2,3-dinor-6-ketoprosta-glandin F1a) in urine [9].
We measured the urinary excretion of 11-dehydrothromboxane B2 (11-dehydro-TXB2), 2,3-dinor-thromboxane B2 (2,3-dinor-TXB2) and 2,3-dinor-6-ketoprostaglandin F1a (2,3-dinor-PGF1a)and bleeding times on admission and thereafterdaily for 1 week in patients with spontaneous ICHas well as 3 months after the stroke. We comparedthe levels of these metabolites between patientswho had or had not been using aspirin during theweek preceding the onset of ICH and healthycontrols. We hypothesized that the onset of ICHmay modify the biosynthesis of TXA2 and PGI2.
Patients and methods
Ethics
The study protocol was approved by the ethicscommittee of the Medical Faculty, University of
Oulu. Informed consent was obtained from all thesubjects. The data and permission for the studyweregiven by a proxy if the patient was too ill tocooperate. The study was conducted in the Depart-ment of Neurology, Oulu University Hospital, Fin-land. The investigation conforms with the principlesoutlined in the Declaration of Helsinki [10].
Clinical and radiological assessments
Our prospective study included 43 patients withspontaneous ICH admitted into the stroke unit ofthe Department of Neurology, Oulu UniversityHospital. The location and volume of ICH wereverified by head CT scanning on admission in allcases. We excluded the patients who had a braintumor, saccular arterial aneurysm, arteriovenousmalformation, or head trauma and those who wereon anticoagulant therapy. Every patient’s aspirinmedication was discontinued on admission, andnone of the patients used aspirin between theacute phase and the control visit 3 months later.
Information was gathered by using a structuredquestionnaire including items on the subjects’ useof medicines, previous diseases, and height andbody weight. In the case of ICH patients who wereconfused, unconscious, or dysphasic, family mem-bers were interviewed. To avoid recall bias,previous hospital records were also reviewed toverify diseases, medications, and blood pressurehistories.
The subjects were considered to be hypertensiveif their blood pressure readings preceding the indexstroke had repeatedly exceeded 160/95 mm Hg orif they were taking antihypertensive medication.The patients who had, unsupervised, discontinuedtheir antihypertensive medication were also classi-fied as having hypertension. Previous hemorrhagicstrokes (ICH and subarachnoid hemorrhage) as wellas ischemic strokes were recorded. Patients with ahistory of hematuria or epistaxis were classified ashaving a bleeding tendency. The coronary heart

Thromboxane and prostacyclin biosynthesis 369
disease category also included patients with pre-vious myocardial infarction, and all diabetics wereon drug treatment.
The patient’s clinical condition was assessed onadmission and 1 week after the ICH by using theGlasgow Coma Scale (GCS) score [11] and theprognostic score of the Scandinavian Stroke Scale(SSS-PRG), which includes consciousness, gazepalsy, and limb strength [12]. If the score oneither of these scales was higher after 1 weekthan on admission, the patient was classified asimproved. Outcome was assessed 3 months afterthe bleeding episode by using the Glasgow Out-come Scale (GOS) [13]. Impaired outcome wasdefined as moderate-to-severe disability, vegeta-tive state or death. The patients underwentrepeated head CT scanning 2—14 days (median,7 days) after admission to verify possible hema-toma enlargement or hydrocephalus. The CT scanswere analyzed and the locations and volumes ofhematomas were measured by a neuroradiologist(J.P.). The volume of each hematoma was meas-ured on a workstation by encircling its boundarieswith a pointer slice by slice and thereby deter-mining its area. The area was then multiplied bythe slice thickness (5 or 10 mm) to get thevolume. The presence of intraventricular bleedingwas recorded. The neuroradiologist was blindedto the patients’ clinical condition and use ofaspirin when measuring the volume and enlarge-ment of the hematomas.
Laboratory procedures
Urine was collected for the determination of 11-dehydrothromboxane B2 (11-dehydro-TXB2), 2,3-dinor-thromboxane B2 (2,3-dinor-TXB2) and 2,3-dinor-6-ketoprostaglandin F1a (2,3-dinor-PGF1a)during the night (10 p.m. to 6 a.m.) after admission,during the nights of the first week after admission,and during one night at the control visit. Controldata of prostanoid excretion from 23 healthy sub-jects aged 29—59 (mean 45F8.1) years were avail-able for comparison. The samples of urine werefrozen immediately after collection and stored at�708 C until extraction. 11-Dehydro-TXB2, 2,3-dinor-TXB2 and 2,3-dinor-PGF1a were determinedafter solid-phase extraction by radioimmunoassay aspreviously reported [14—16]. In order to avoiddifferences due to inter- and intraindividual varia-tions in diuresis, the excretion of prostanoids wascorrelated with the excretion of creatinine, whichwas determined from the urine samples spectro-photometrically by the picric acid method using acommercial assay kit (Orion, Espoo, Finland). The
urinary excretion rates were expressed as pico-grams per micromole of creatinine. Bleeding timeswere assessed by the Ivy method [17,18] onadmission (within 0—3 days after the onset of thestroke), daily during the first week after admission,and at the control visit 3 months after the ICH. Theinvestigator of the laboratory parameters (A.R.)was blinded to the patients’ clinical condition anduse of aspirin.
Statistical analysis
Fisher’s exact two-tailed test, Pearson’s v2 test,Mann—Whitney U-test, Student’s t-test, analysisof variance (ANOVA) with corrected multiplecomparisons in pairs by use of the Bonferronimethod and Spearman’s rank correlation coeffi-cients (rs) were used as appropriate. Univariateand multivariate odds ratios (OR) with 95%confidence intervals (CI) were calculated bylogistic regression (maximum likelihood method).Stepwise logistic regression (pb0.1 for entry limitand pN0.15 for removal limit) was used to findout significant independent risk factors forimpaired outcome after ICH. Adjustments ofORs were made for all the parameters listed inthe tables by using logistic regression models. Inthe patients with a complete set of samples, theeffect of the time elapsed after ICH and thedifferent grouping variables on TXA2 and PGI2metabolites were compared by repeated-meas-ures ANOVA. For ANOVA, the values for prosta-noid variables were analyzed after logarithmictransformation if necessary, to obtain equality ofvariances between the different groups. A two-tailed p-value below 0.05 was considered toindicate statistical significance.
Results
The patients’ baseline characteristics on admissionare shown in Table 1. There were 13 regular and 8occasional aspirin users. The median daily dose ofthe regular users was 250 mg (range 250—600 mg).The maximum dose of aspirin consumed by theoccasional users amounted to 1500 mg (median 500mg) during the week preceding the ICH. The aspirinusers had more frequently hypertension in theirhistory than the nonusers. History of ischemicstroke, bleeding tendency, coronary heart diseaseand hematomas in basal ganglia were also morecommon among the aspirin users than the otherpatients, but these differences were not statisti-cally significant. Hematoma volumes as well as GCS

Table 1 Baseline characteristics of 43 patients with spontaneous ICH
Variable Total Nonusersof aspirin
Aspirin users
Sex (female/male) 20/23 13/9 7/14Mean (SD) age, years 66.3 (11.0) 64.5 (11.7) 67.6 (10.2)Mean (SD) BMI, kg/m2 26.0 (4.1) 25.1 (4.4) 27.0 (3.7)Hypertension (%) 27 (62.8) 10 (45.4) 17 (80.9)*Ischemic stroke (%) 9 (20.9) 2 (9.1) 7 (33.3)y
Hemorrhagic stroke (%) 5 (11.6) 2 (9.1) 3 (14.3)Bleeding tendency (%) 15 (34.9) 5 (22.7) 10 (47.6)z
Coronary heart disease (%) 13 (30.2) 5 (22.7) 9 (42.9)Diabetes (%) 4 (9.3) 2 (9.1) 2 (9.5)Location of hematomaSubcortex 10 5 5Basal ganglia 19 7 12Thalamus 8 5 3Cerebellum 3 2 1Pons 3 2 0Median hematoma volume (25,75 percentiles) 11 (5,30) 12 (6,28) 9 (4,33)Median GlasgowComa Scale score (25,75 percentiles)
15 (13,15) 15 (13,15) 15 (13,15)
Median SSS Prognostic score (25,75 percentiles) 19 (10,21) 18 (10,21) 20 (15,21)
BMI=body mass index. SSS=Scandinavian Stroke Scale.* p=0.050 for difference between aspirin users and nonusers.y p=0.069 for difference between aspirin users and nonusers.z p=0.087 for difference between aspirin users and nonusers.
P. Saloheimo et al.370
and SSS-PRG scores on admission were similar in thetwo groups.
The levels of 11-dehydro-TXB2, 2,3-dinor-TXB2and 2,3-dinor-PGF1a excretion into urine onadmission (0—3 days after the onset of ICH) inthe patients and controls are shown in Table 2.The levels were significantly higher in thepatients without prior use of aspirin than thecontrols. The mean urinary excretion rates of 11-dehydro-TXB2, 2,3-dinor-TXB2 and 2,3-dinor-PGF1ain the aspirin users on admission did not signifi-cantly differ from those of the controls (p=0.6,0.5, and 1.0, respectively).
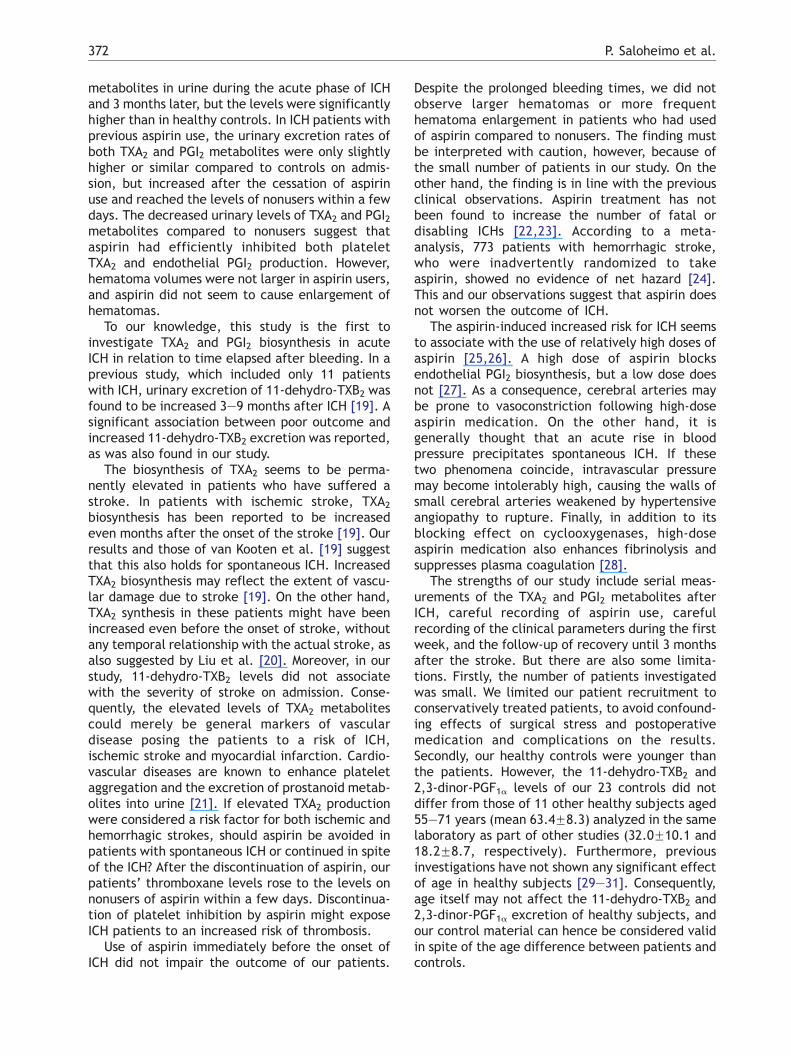
Fig. 1 shows the mean levels and 95% CIs of 11-dehydro-TXB2 and 2,3-dinor-PGF1a excretion intourine in the users and nonusers of aspirin day by dayduring the first week after the onset of ICH and atthe control visit. 11-dehydro-TXB2 excretion intourine was significantly (p=0.048) lower in the users
Table 2 Urinary excretion of 11-dehydro-TXB2, 2,3-dinor-onset of ICH) of patients according to aspirin use and contr
Metabolite Nonusers of aspirin(n=21)
11-Dehydro-TXB2 129.4 (91.5—167.3)2,3-Dinor-TXB2 69.3 (41.7—97.0)2,3-Dinor-PGF1a 31.6 (21.0—42.3)11-Dehydro-TXB2/2,3-dinor-PGF1a 6.18 (2.93—9.43)
Metabolite levels are expressed as pg/Amol creatinine (mean and 9* Nonusers of aspirin vs. controls.
than nonusers of aspirin on day 3 after the onset ofICH, but on days 1 and 2 the difference did notreach statistical significance because the numberof samples from those days was small. When theurinary values of 11-dehydro-TXB2 on days 1—2 and5—6 were compared, the values increased signifi-cantly ( p=0.007) as more time elapsed, andsignificant interactions between the groups andtime were also observed (p=0.028) (i.e., the valueschanged differently over time, depending onaspirin use). The levels of 2,3-dinor-PGF1a obtainedon the first day after the onset of ICH weresignificantly (p=0.001) lower in the aspirin usersthan in nonusers. The difference disappearedduring the following few days. When the urinaryvalues of 2,3-dinor-PGF1a on days 1—2 and 5—6were compared, there was a significant (p=0.015)effect of the interaction between aspirin use andthe time of sampling on 2,3-dinor-PGF1a excretion
TXB2 and 2,3-dinor-PGF1a on admission (0—3 days afterols
Aspirin users(n=19)
Controls(n=23)
P*
52.9 (24.9—81.0) 27.9 (14.9—40.9) b0.00131.3 (16.7—45.9) 19.7 (11.9—27.5) b0.00116.2 (9.7—22.7) 16.1 (7.7—24.5) 0.0193.52 (2.48—4.56) 2.17 (1.57—2.77) 0.009
5% CI).
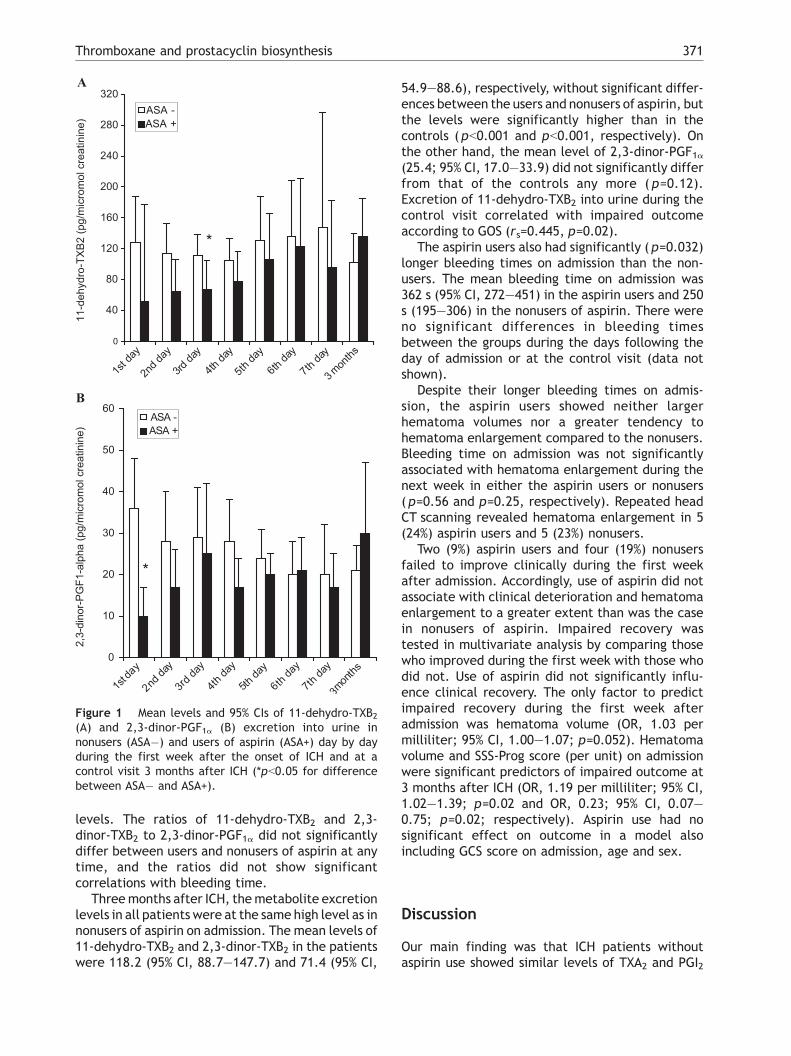
Figure 1 Mean levels and 95% CIs of 11-dehydro-TXB2(A) and 2,3-dinor-PGF1a (B) excretion into urine innonusers (ASA�) and users of aspirin (ASA+) day by dayduring the first week after the onset of ICH and at acontrol visit 3 months after ICH (*pb0.05 for differencebetween ASA� and ASA+).
Thromboxane and prostacyclin biosynthesis 371
levels. The ratios of 11-dehydro-TXB2 and 2,3-dinor-TXB2 to 2,3-dinor-PGF1a did not significantlydiffer between users and nonusers of aspirin at anytime, and the ratios did not show significantcorrelations with bleeding time.
Threemonths after ICH, themetabolite excretionlevels in all patients were at the same high level as innonusers of aspirin on admission. The mean levels of11-dehydro-TXB2 and 2,3-dinor-TXB2 in the patientswere 118.2 (95% CI, 88.7—147.7) and 71.4 (95% CI,
54.9—88.6), respectively, without significant differ-ences between the users and nonusers of aspirin, butthe levels were significantly higher than in thecontrols (pb0.001 and pb0.001, respectively). Onthe other hand, the mean level of 2,3-dinor-PGF1a(25.4; 95% CI, 17.0—33.9) did not significantly differfrom that of the controls any more ( p=0.12).Excretion of 11-dehydro-TXB2 into urine during thecontrol visit correlated with impaired outcomeaccording to GOS (rs=0.445, p=0.02).
The aspirin users also had significantly (p=0.032)longer bleeding times on admission than the non-users. The mean bleeding time on admission was362 s (95% CI, 272—451) in the aspirin users and 250s (195—306) in the nonusers of aspirin. There wereno significant differences in bleeding timesbetween the groups during the days following theday of admission or at the control visit (data notshown).
Despite their longer bleeding times on admis-sion, the aspirin users showed neither largerhematoma volumes nor a greater tendency tohematoma enlargement compared to the nonusers.Bleeding time on admission was not significantlyassociated with hematoma enlargement during thenext week in either the aspirin users or nonusers(p=0.56 and p=0.25, respectively). Repeated headCT scanning revealed hematoma enlargement in 5(24%) aspirin users and 5 (23%) nonusers.
Two (9%) aspirin users and four (19%) nonusersfailed to improve clinically during the first weekafter admission. Accordingly, use of aspirin did notassociate with clinical deterioration and hematomaenlargement to a greater extent than was the casein nonusers of aspirin. Impaired recovery wastested in multivariate analysis by comparing thosewho improved during the first week with those whodid not. Use of aspirin did not significantly influ-ence clinical recovery. The only factor to predictimpaired recovery during the first week afteradmission was hematoma volume (OR, 1.03 permilliliter; 95% CI, 1.00—1.07; p=0.052). Hematomavolume and SSS-Prog score (per unit) on admissionwere significant predictors of impaired outcome at3 months after ICH (OR, 1.19 per milliliter; 95% CI,1.02—1.39; p=0.02 and OR, 0.23; 95% CI, 0.07—0.75; p=0.02; respectively). Aspirin use had nosignificant effect on outcome in a model alsoincluding GCS score on admission, age and sex.
Discussion
Our main finding was that ICH patients withoutaspirin use showed similar levels of TXA2 and PGI2
P. Saloheimo et al.372
metabolites in urine during the acute phase of ICHand 3 months later, but the levels were significantlyhigher than in healthy controls. In ICH patients withprevious aspirin use, the urinary excretion rates ofboth TXA2 and PGI2 metabolites were only slightlyhigher or similar compared to controls on admis-sion, but increased after the cessation of aspirinuse and reached the levels of nonusers within a fewdays. The decreased urinary levels of TXA2 and PGI2metabolites compared to nonusers suggest thataspirin had efficiently inhibited both plateletTXA2 and endothelial PGI2 production. However,hematoma volumes were not larger in aspirin users,and aspirin did not seem to cause enlargement ofhematomas.
To our knowledge, this study is the first toinvestigate TXA2 and PGI2 biosynthesis in acuteICH in relation to time elapsed after bleeding. In aprevious study, which included only 11 patientswith ICH, urinary excretion of 11-dehydro-TXB2 wasfound to be increased 3—9 months after ICH [19]. Asignificant association between poor outcome andincreased 11-dehydro-TXB2 excretion was reported,as was also found in our study.
The biosynthesis of TXA2 seems to be perma-nently elevated in patients who have suffered astroke. In patients with ischemic stroke, TXA2biosynthesis has been reported to be increasedeven months after the onset of the stroke [19]. Ourresults and those of van Kooten et al. [19] suggestthat this also holds for spontaneous ICH. IncreasedTXA2 biosynthesis may reflect the extent of vascu-lar damage due to stroke [19]. On the other hand,TXA2 synthesis in these patients might have beenincreased even before the onset of stroke, withoutany temporal relationship with the actual stroke, asalso suggested by Liu et al. [20]. Moreover, in ourstudy, 11-dehydro-TXB2 levels did not associatewith the severity of stroke on admission. Conse-quently, the elevated levels of TXA2 metabolitescould merely be general markers of vasculardisease posing the patients to a risk of ICH,ischemic stroke and myocardial infarction. Cardio-vascular diseases are known to enhance plateletaggregation and the excretion of prostanoid metab-olites into urine [21]. If elevated TXA2 productionwere considered a risk factor for both ischemic andhemorrhagic strokes, should aspirin be avoided inpatients with spontaneous ICH or continued in spiteof the ICH? After the discontinuation of aspirin, ourpatients’ thromboxane levels rose to the levels onnonusers of aspirin within a few days. Discontinua-tion of platelet inhibition by aspirin might exposeICH patients to an increased risk of thrombosis.
Use of aspirin immediately before the onset ofICH did not impair the outcome of our patients.
Despite the prolonged bleeding times, we did notobserve larger hematomas or more frequenthematoma enlargement in patients who had usedof aspirin compared to nonusers. The finding mustbe interpreted with caution, however, because ofthe small number of patients in our study. On theother hand, the finding is in line with the previousclinical observations. Aspirin treatment has notbeen found to increase the number of fatal ordisabling ICHs [22,23]. According to a meta-analysis, 773 patients with hemorrhagic stroke,who were inadvertently randomized to takeaspirin, showed no evidence of net hazard [24].This and our observations suggest that aspirin doesnot worsen the outcome of ICH.
The aspirin-induced increased risk for ICH seemsto associate with the use of relatively high doses ofaspirin [25,26]. A high dose of aspirin blocksendothelial PGI2 biosynthesis, but a low dose doesnot [27]. As a consequence, cerebral arteries maybe prone to vasoconstriction following high-doseaspirin medication. On the other hand, it isgenerally thought that an acute rise in bloodpressure precipitates spontaneous ICH. If thesetwo phenomena coincide, intravascular pressuremay become intolerably high, causing the walls ofsmall cerebral arteries weakened by hypertensiveangiopathy to rupture. Finally, in addition to itsblocking effect on cyclooxygenases, high-doseaspirin medication also enhances fibrinolysis andsuppresses plasma coagulation [28].
The strengths of our study include serial meas-urements of the TXA2 and PGI2 metabolites afterICH, careful recording of aspirin use, carefulrecording of the clinical parameters during the firstweek, and the follow-up of recovery until 3 monthsafter the stroke. But there are also some limita-tions. Firstly, the number of patients investigatedwas small. We limited our patient recruitment toconservatively treated patients, to avoid confound-ing effects of surgical stress and postoperativemedication and complications on the results.Secondly, our healthy controls were younger thanthe patients. However, the 11-dehydro-TXB2 and2,3-dinor-PGF1a levels of our 23 controls did notdiffer from those of 11 other healthy subjects aged55—71 years (mean 63.4F8.3) analyzed in the samelaboratory as part of other studies (32.0F10.1 and18.2F8.7, respectively). Furthermore, previousinvestigations have not shown any significant effectof age in healthy subjects [29—31]. Consequently,age itself may not affect the 11-dehydro-TXB2 and2,3-dinor-PGF1a excretion of healthy subjects, andour control material can hence be considered validin spite of the age difference between patients andcontrols.

Thromboxane and prostacyclin biosynthesis 373
Acknowledgement
This study was supported in part by the OuluMedical Foundation, the Neurology Foundationand the Maire Taponen Foundation (P.S.).
References
[1] Van Kooten F, Ciabattoni G, Patrono C, Schmitz PIM, van GijnJ, Koudstaal PJ. Evidence for episodic platelet activation inacute ischemic stroke. Stroke 1994;25:278—81.
[2] Koudstaal PJ, Ciabattoni G, van Gijn J, Nieuwenhuis K, deGroot PG, Sixma JJ, et al. Increased thromboxane biosyn-thesis in patients with acute cerebral ischemia. Stroke1993;24:219—23.
[3] Henriksson P, Wennmalm A, Edhag O, Vesterqvist O, GreenK. In vivo production of prostacyclin and thromboxane inpatients with acute myocardial infarction. Br Heart J1986;55:543—8.
[4] Hammarstrfm S, Falardeau P. Resolution of prostaglandinendoperoxide synthase and thromboxane synthase ofhuman platelets. Proc Natl Acad Sci U S A 1977;74:3691—5.
[5] Marcus AJ, Weksler BB, Jaffe EA. Enzymatic conversion ofprostaglandin endoperoxide H2 and arachidonic acid toprostacyclin by cultured human endothelial cells. J BiolChem 1978;253:7138—41.
[6] Svensson J, Hamberg M, Samuelsson B. On the formationand effects of thromboxane A2 in human platelets. ActaPhysiol Scand 1976;98:285—94.
[7] Ellis EF, Oelz O, Roberts II LJ, Payne NA, Sweetman BJ, NiesAS, et al. Coronary arterial smooth muscle contraction by asubstance released from platelets: evidence that it isthromboxane A2. Science 1976;193:1135—7.
[8] Bunting S, Gryglewski R, Moncada S, Vane JR. Arterial wallsgenerate from prostaglandin endoperoxides a substance(prostaglandin X) which relaxes strips of mesenteric andceliac arteries and inhibits platelet aggregation. Prosta-glandins 1976;12:897—913.
[9] FitzGerald GA, Pedersen AK, Patrono C. Analysis ofprostacyclin and thromboxane biosynthesis in cardiovascu-lar disease. Circulation 1983;67:1174—7.
[10] World Medical Association Declaration of Helsinki. Recom-mendations guiding physicians in biomedical researchinvolving human subjects C. Cardiovasc Res 1997;35:2—3.
[11] Teasdale G, Jennett B. Assessment of coma and impairedconsciousness: a practical scale. Lancet 1974;2:81—94.
[12] Scandinavian Stroke Study Group. Multicentre trial ofhemodilution in ischaemic stroke: background and studyprotocol. Stroke 1985;16:885—90.
[13] Jennett B, Bond M. Assessment of outcome after severebrain damage: a practical scale. Lancet 1975;1:480—4.
[14] Riutta A, Mucha I, Vapaatalo H. Solid-phase extraction ofurinary 11-dehydrothromboxane B2 for reliable determi-nation with radioimmunoassay. Anal Biochem 1992;202:299—305.
[15] Numminen H, Kobayashi M, Uchiyama S, Iwata M, Ikeda Y,Riutta A, et al. Effects of alcohol and the evening meal on
shear-induced platelet aggregation and urinary excretion ofprostanoids. Alcohol Alcohol 2000;35:594—600.
[16] Riutta A, Nurmi E, Weber C, Hansson G, Vapaatalo H, MuchaI. Selective solid-phase extraction of urinary 2,3-dinor-6-ketoprostaglandin F1a for determination with radioimmuno-assay. Anal Biochem 1994;220:351—9.
[17] Ivy AC, Nelson D, Bucher G. The standardization of certainfactors in cutaneous bvenostasisQ bleeding time technique.J Lab Clin Med 1941;26:1812—22.
[18] Mielke Jr CH, Kaneshiro MM, Maher IA, Weiner JM, RapaportSI. The standardized normal Ivy bleeding time and itsprolongation by aspirin. Blood 1969;34:204—15.
[19] van Kooten F, Ciabattoni G, Koudstaal PJ, Dippel DW,Patrono C. Increased platelet activation in the chronicphase after cerebral ischaemia and intracerebral hemor-rhage. Stroke 1999;30:546—9.
[20] Liu L, Lin Z, Shen Z, Zhang G, Li S, Cao P. Platelethyperfunction exists in both acute non-haemorrhagic andhaemorrhagic stroke. Thromb Res 1994;75:485—90.
[21] Catella F, FitzGerald GA. Paired analysis of urinary throm-boxane B2 metabolites in humans. Thromb Res 1987;47:647—56.
[22] Juntti-Patinen L, Neuvonen PJ. Drug-related deaths in auniversity central hospital. Eur J Pharmacol 2002;58:479—82.
[23] The Medical Research Council’s General Practice ResearchFramework. Thrombosis prevention trial: randomised trialof low-intensity oral anticoagulation with warfarin and low-dose aspirin in the primary prevention of ischaemic heartdisease in men at increased risk. Lancet 1998;351:233—41.
[24] Chen ZM, Sandercock P, Pan HC, Counsell C, Collins R, LiuLS, et al. Indications for early aspirin use in acute ischemicstroke. A combined analysis of 40000 randomized patientsfrom the Chinese acute stroke trial and the internationalstroke trial. Stroke 2000;31:1240—9.
[25] Saloheimo P, Juvela S, Hillbom M. Use of aspirin, epistaxis,and untreated hypertension as risk factors for primaryintracerebral hemorrhage in middle-aged and elderlypeople. Stroke 2001;32:399—404.
[26] Thrift AG, McNeil JJ, Forbes A, Donnan GA. Risk of primaryintracerebral haemorrhage associated with aspirin andnon-steroidal anti-inflammatory drugs: case-control study.Br Med J 1999;318:759—64.
[27] Tohgi H, Konno S, Tamura K, Kimura B, Kawano K. Effects oflow to high doses of aspirin on platelet aggregability andmetabolites of thromboxane A2 and prostacyclin. Stroke1992;23:1400—4.
[28] Patrono C, Coller B, Dalen JE, FitzGerald GA, Fuster V, GentM, Hirsh J, Roth G. Platelet-active drugs: the relationshipsamong dose, effectiveness, and side effects. Chest 2001;119(1 Suppl.):S39.
[29] McDonnel JP, Cheryk LA, Durocher A, Bruno A, Bang NU,Fleck JD, et al. Urinary 11-dehydro-thromboxane B2 andcoagulation activation markers measured within 24 h ofhuman acute ischemic stroke. Neurosci Lett 2001;313:88—92.
[30] R3ngemark C, Benthin G, Granstrfm EF, Persson L, Winell S,Wennmalm 2. Tobacco use and urinary excretion ofthromboxane A2 and prostacyclin metabolites in womenstratified by age. Circulation 1992;86:1495—500.
[31] Reilly IA, Fitzgerald GA. Eicosanoid biosynthesis and plateletfunction with advancing age. Thromb Res 1986;15:545—54.
Related Documents











