Fax +41 61 306 12 34 E-Mail [email protected] www.karger.com Original Paper Cerebrovasc Dis 2012;33:329–339 DOI: 10.1159/000335309 Thrombotic Stroke in the Anesthetized Monkey (Macaca mulatta) : Characterization by MRI – A Pilot Study Maxime Gauberti a Pauline Obiang a Pierre Guedin a, e Anne Balossier a, b Clément Gakuba a, c Anne Sophie Diependaele d Laurent Chazalviel a Denis Vivien a Alan R. Young a Véronique Agin a Cyrille Orset a a INSERM U919, Serine Proteases and Pathophysiology of the Neurovascular Unit, GIP Cyceron, Université de Caen-Basse Normandie, et b Service de Neurochirurgie, c Service d’anesthésie et réanimation, et d Laboratoire d’exploration fonctionnelle du système nerveux, CHU de Caen, Caen, et e Service de Neuroradiologie, Hôpital Lariboisière, Paris, France Physiological and biochemical parameters were monitored throughout the investigations. Results: Once standardized, the surgical procedure induced transient occlusion of the middle cerebral artery in all operated animals. All animals studied showed spontaneous reperfusion, which occurred some time between 2 h and 7 days post-ictus. Eighty percent of the studied animals showed diffusion/perfusion mis- match. The ischemic lesions at 24 h spared both superficial and profound territories of the MCA. Some animals present- ed hemorrhagic transformation at 7 days post-ictus. Conclu- sion: In this study, we developed a pre-clinically relevant model of embolic stroke in the anesthetized nonhuman pri- mate. Copyright © 2012 S. Karger AG, Basel Key Words Animal models Embolic stroke Focal ischemia Middle cerebral artery occlusion Methods Monkey MRI Thrombin Abstract Background: The lack of a relevant stroke model in large nonhuman primates hinders the development of innova- tive diagnostic/therapeutic approaches concerned with this cerebrovascular disease. Our objective was to develop a nov- el and clinically relevant model of embolic stroke in the anes- thetized monkey that incorporates readily available clinical imaging techniques and that would allow the possibility of drug delivery including strategies of reperfusion. Methods: Thrombin was injected into the lumen of the middle cere- bral artery (MCA) in 12 anesthetized (sevoflurane) male rhe- sus macaques (Macaca mulatta). Sequential MRI studies (in- cluding angiography, FLAIR, PWI, DWI, and gadolinium-en- hanced T1W imaging) were performed in a 3T clinical MRI. Received: June 14, 2011 Accepted: November 17, 2011 Published online: February 16, 2012 Prof. D. Vivien, PhD INSERM U919 Serine Proteases and Pathophysiology of the Neurovascular Unit GIP Cyceron, Bd H.-Becquerel, BP5229 FR–14074 Caen Cedex (France) Tel. +33 2 31 47 01 60, E-Mail vivien @ cyceron.fr © 2012 S. Karger AG, Basel 1015–9770/12/0334–0329$38.00/0 Accessible online at: www.karger.com/ced Maxime Gauberti, Pauline Obiang, Véronique Agin, and Cyrille Orset contributed equally to this work. Downloaded by: INSERM DISC IST 193.54.110.33 - 7/8/2013 12:07:50 PM

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Fax +41 61 306 12 34E-Mail [email protected]
Original Paper
Cerebrovasc Dis 2012;33:329–339 DOI: 10.1159/000335309
Thrombotic Stroke in the Anesthetized Monkey (Macaca mulatta) : Characterization by MRI – A Pilot Study
Maxime Gauberti a Pauline Obiang a Pierre Guedin a, e Anne Balossier a, b
Clément Gakuba a, c Anne Sophie Diependaele d Laurent Chazalviel a
Denis Vivien a Alan R. Young a Véronique Agin a Cyrille Orset a
a INSERM U919, Serine Proteases and Pathophysiology of the Neurovascular Unit, GIP Cyceron,Université de Caen-Basse Normandie, et b Service de Neurochirurgie, c Service d’anesthésie et réanimation, et d Laboratoire d’exploration fonctionnelle du système nerveux, CHU de Caen, Caen , et e Service de Neuroradiologie, Hôpital Lariboisière, Paris , France
Physiological and biochemical parameters were monitored throughout the investigations. Results: Once standardized, the surgical procedure induced transient occlusion of the middle cerebral artery in all operated animals. All animals studied showed spontaneous reperfusion, which occurred some time between 2 h and 7 days post-ictus. Eighty percent of the studied animals showed diffusion/perfusion mis-match. The ischemic lesions at 24 h spared both superficial and profound territories of the MCA. Some animals present-ed hemorrhagic transformation at 7 days post-ictus. Conclu-
sion: In this study, we developed a pre-clinically relevant model of embolic stroke in the anesthetized nonhuman pri-mate. Copyright © 2012 S. Karger AG, Basel
Key Words
Animal models � Embolic stroke � Focal ischemia � Middle cerebral artery occlusion � Methods � Monkey � MRI � Thrombin
Abstract
Background: The lack of a relevant stroke model in large nonhuman primates hinders the development of innova-tive diagnostic/therapeutic approaches concerned with this cerebrovascular disease. Our objective was to develop a nov-el and clinically relevant model of embolic stroke in the anes-thetized monkey that incorporates readily available clinical imaging techniques and that would allow the possibility of drug delivery including strategies of reperfusion. Methods: Thrombin was injected into the lumen of the middle cere-bral artery (MCA) in 12 anesthetized (sevoflurane) male rhe-sus macaques (Macaca mulatta). Sequential MRI studies (in-cluding angiography, FLAIR, PWI, DWI, and gadolinium-en-hanced T1W imaging) were performed in a 3T clinical MRI.
Received: June 14, 2011 Accepted: November 17, 2011 Published online: February 16, 2012
Prof. D. Vivien, PhD INSERM U919 Serine Proteases and Pathophysiology of the Neurovascular Unit GIP Cyceron, Bd H.-Becquerel, BP5229 FR–14074 Caen Cedex (France) Tel. +33 2 31 47 01 60, E-Mail vivien @ cyceron.fr
© 2012 S. Karger AG, Basel1015–9770/12/0334–0329$38.00/0
Accessible online at:www.karger.com/ced
Maxime Gauberti, Pauline Obiang, Véronique Agin, and Cyrille Orset contributed equally to this work.
Dow
nloa
ded
by:
INS
ER
M D
ISC
IST
193.
54.1
10.3
3 -
7/8/
2013
12:
07:5
0 P
M

Gauberti et al. Cerebrovasc Dis 2012;33:329–339330
Introduction
To date, there is no consensus on the nonhuman stroke model that most acutely mimics the human pathology. Primate models of cerebral ischemia may offer many ad-vantages over their rodent counterparts [1–5] , but such investigations are time-consuming and rely on a multi-disciplinary team, state-of-the-art imaging techniques, appropriate intensive care facilities, and a substantial fi-nancial commitment. Nonetheless, primate models of stroke offer full biochemical, physiological, and neuro-logical assessment of the animal during a prolonged pe-riod of survival.
It is not surprising, therefore, that new experimental models of stroke in the primate are sparse as it may be just too difficult to induce a major stroke in healthy young adolescent nonhuman primates without elaborate ma-nipulation of the cerebral vasculature. There are several models of stroke that have been used in nonhuman pri-mates; some are more severe than others in terms of the degree of neuropathological changes. Experimental tech-niques to occlude the middle cerebral artery (MCA) in-volve mechanical occlusions by using either electrocoag-ulation [6, 7] , a filament model [8, 9] , an intravascular balloon or cuff [2, 10–12] , microvascular clips [13–18] , or ligatures [19–21] . Other approaches use the intravascular route to inject autologous or heterologous preformed fi-brin, blood clots [3, 22, 23] , microemboli [24–26] , or, in some cases, by in situ clot formation by photothrombosis [27–29] . However, it is important to establish which, if any, of these models of focal cerebral ischemia can be considered to be the most representative of an acute stroke in humans.
We believe that an animal model of embolic stroke would be the most appropriate manner in which to in-duce focal brain ischemia as it allows the possibility of thrombolytic and/or neuroprotector therapy. Further-more, as the precise moment of MCA occlusion (MCAO) is known, the temporal evolution of the lesion and the time-to-treatment can be accurately determined through the use of MRI techniques, as in the present study.
The objective of the present study was to validate a model of thromboembolic stroke in anesthetized mon-keys and to follow the time course of the resulting lesion through the use of clinically relevant imaging techniques and diagnostic procedures over a 3-month interval. This study consists of two parts: in the first one, which in-volved 6 animals, we tried to standardize the surgical procedure. In the second one, we used the standardized procedure to characterize and test the reproducibility of
our model in 6 additional animals. The following is a re-sult of our findings and our attempt to compare them with documented clinical studies.
Methods
Experiments were performed in 12 male rhesus macaques (Macaca mulatta) aged 5–6 years and with body weights ranging from 7 to 11 kg. An experimental protocol was submitted (A.R.Y.) to the Regional Ethics Committee for Animal Experimentation (Normandy) and approval was granted to conduct the study (re-ferral No. N/02-03-08/03/02-11). Experiments were performed by licensed investigators (C.O., A.R.Y., L.C.) and in accordance with French ethical laws (act No. 87-848; Ministère de l’Agriculture et de la Forêt) and European Communities Council Directives (86/609/EEC and 2010/63/EU) guidelines for the care and use of laboratory animals. The animals were purchased directly from a French supplier (Station de primatologie – UPS 846, D56 – 13790 Rousset sur Arc). During the course of the present studies (2 years), the monkeys were housed at the Cyceron Research Centre (Establishment for Animal Experimentation, agreement No. B14118001) in individual cages maintained at 24 ° C with 50% rel-ative humidity on a 12-hour/12-hour light/dark cycle and were fed commercial chow supplemented with fresh fruits and water ad libitum. Throughout the duration of these studies a veterinary surgeon was available to oversee the well-being of the animals.
Anesthesia The monkeys were tranquilized with ketamine (Imogen � , 0.1
mg/kg, i.m.) and, subsequent to the placement of catheters in the external saphenous veins, anesthesia was induced by sevoflurane (Sevorane � , 2%) in 100% oxygen. Atracurium (Tracrium � , 0.5 mg/kg, i.v.) was used to achieve muscular relaxation and endotra-cheal intubation was performed. Monkeys were placed on inter-mittent positive pressure ventilation (Aestiva 5/MRI 7900; Gen-eral Electric, France) with a fixed respiratory rate (22 breaths per min). The tidal volume ( � 120 ml) was adjusted to maintain nor-mocapnia (P CO 2 38–42 mm Hg). Anesthesia was maintained with sevoflurane and 66% nitrous oxide in oxygen along with an intra-venous perfusion of atracurium (0.75 mg/kg/h). During surgical interventions, the sevoflurane concentration was increased (to � 3%, and sufentanyl 0.1 � g, i.v., was administered for further pain relief). Thereafter, and 30 min prior to the MRI studies, su-fentanyl was discontinued and the concentration of sevoflurane was reduced to around 1.5–2.0%. Prior to the placement and re-moval of the stereotaxic ear bars, atropine sulphate (0.25 mg, i.v.) was administered. At the end of each study, the monkey was de-curarized with neostigmine (Prostigmine � , 0.5 mg, i.v.), extubat-ed, and returned to its cage.
Post-Operative Recovery Systemic antibiotic treatment with cephamandole was contin-
ued over 5 days (Kefandol � , 15 mg/kg, i.m., daily). A local antibi-otic rifamycine (Rifocine � ; Merrel Dow) was also applied into and around the orbit. In case of pain, an injection of the anti-inflam-matory agent tolfedine 4% (Vétoquinol � , 4 mg/kg, i.m.) or the oripavine derivative buprenorphine (Buprecare � , 20 � g/kg, i.m.) was given as deemed necessary.
Dow
nloa
ded
by:
INS
ER
M D
ISC
IST
193.
54.1
10.3
3 -
7/8/
2013
12:
07:5
0 P
M

Thrombotic Stroke in the Anesthetized Monkey
Cerebrovasc Dis 2012;33:329–339 331
Surgical Procedures and Physiological Monitoring The transorbital approach to the right MCA, originally de-
scribed by Hudgins and Garcia [17] , was employed as modified by Young et al. [30] . Following enucleation, a craniectomy was made using a high-speed saline-cooled dental drill to expose the right MCA. The dura was opened and the arachnoid dissected to allow placement of the micropipette. Two sutures were positioned to isolate the M1 branch into which the micropipette was inserted and thrombin injected ( fig. 1 a, b). During this procedure, warm saline was used to reduce the possibility of vascular spasm. Re-construction of the orbit under aseptic conditions allowed com-plete post-operative recovery and permitted long-term survival in all animals. Arterial pressure and heart rate were measured con-tinuously, as was the temperature, end-tidal CO 2 levels, and Sa O 2 concentrations (In Vivo Magnitude 3150 MRI; Ademia, France). Following reconstructive surgery, the monkeys were immediately transferred to a 3T Philips MRI scanner (Philips Achieva) where physiological monitoring was continued. Basal physiological pa-rameters were obtained from the basal imaging performed before the day of the surgery.
Clot Formation and Injection The hematological micropipette was made using an electro-
physiology puller (PC-10; Narishige, USA) and calibrated (15 mm/ � l; Assistent � ref. 555/5; Hoechst, Sondheim-Rhoen, Ger-many). Just before surgery, the micropipette was connected to a syringe filled with human thrombin (final concentration 1 UI/ � l in PBS; Enzyme Research Laboratories, USA). Thrombin (total volume for the standardized procedure was 800 � l, 1 UI/ � l) was injected into the lumen of the designated MCA segment in a step-
by-step manner (firstly 6 ! 50 � l at 2-min intervals). Thereafter, the proximal suture was removed and 2 ! 100 � l were injected at 2-min intervals. Finally, the remaining thrombin (300 � l for the standardized procedure) was injected over 1–2 min after the distal suture was removed. The duration of the entire surgical procedure was ap proximately 3 h from endotracheal intubation to the end of reconstructive surgery.
The concentration of the thrombin solution was chosen ac-cording to the results obtained in rodent studies performed at our laboratory [31] . In the first set of monkeys operated, the total amount of thrombin injected was chosen to achieve a complete and stable arterial occlusion at the end of the thrombus formation procedure. Thereafter, we used this dose (800 UI) in the 6 other animals operated according to the standardized procedure.
In vivo MRI Acquisition Monkeys were studied in a 3T clinical MRI equipped with two
surface coils located on each side of the animal’s head (Philips Sense Flex M). Imaging was performed in the axial plane and in-cluded the following sequences (30 min total duration), 3D-time-of-flight angiography, T2-weighted, fluid attenuation inversion recovery (FLAIR), diffusion-weighted imaging (DWI), and pre- and post-contrast T1-weighted and perfusion-weighted imaging (PWI). This block of MRI sequences was repeated before and after surgery at 2 and 24 h, 7 and 21 days, and 3 months ( fig. 1 a). A bo-lus of 0.2 mmol/kg GdDOTA (Dotarem � ) was injected i.v. for PWI imaging. Immediately before (pre-scan) and 15 min after GdDOTA injection (post-scan), we performed a T1-weighted scan. Subtractions of pre-scan from post-scan were visually in-spected for BBB leakage at all imaging time points.
b
a
c
Fig. 1. a Time line for the experimental protocol. b Schema of the surgical proce-dure showing the craniotomy, the isolated segment of the MCA between the two su-tures and the pipette used to inject the thrombin to induce the cascade of clot for-mation ( c ).
Dow
nloa
ded
by:
INS
ER
M D
ISC
IST
193.
54.1
10.3
3 -
7/8/
2013
12:
07:5
0 P
M
Gauberti et al. Cerebrovasc Dis 2012;33:329–339332
Image Analysis Maps of relative hemodynamic indices from PWI data [time
to peak (TTP), mean transit time, relative cerebral blood volume, and relative cerebral blood velocity] were calculated using the console software (Philips Achieva v1.5). The apparent diffusion coefficient (ADC) was calculated from the diffusion data using MedINRIA software (v1.9). Registrations of ADC maps were per-formed using the Fusion tool of the MedINRIA software. Maps of infarction probability were computed from manually outlined in-farcted areas on registered DWI images using ImageJ software. For pixel-by-pixel analysis of perfusion/diffusion mismatch, we registered ADC maps (at 2 and 24 h) and TTP maps. Then, aregion of interest was drawn in a nonischemic area allowing nonischemic ADC and TTP values to be measured. Subsequently, we thresholded the images to measure the volume of the brain regions showing low ADC (a threshold of 75% of the nonischemic region was chosen according to Røhl et al. [32] ) and high TTP (a threshold of +3s compared to the nonischemic region was chosen because it provided the best estimate of the resulting ischemic le-sion at 24 h post-occlusion with our data).
Neurological Score Functional deficit was evaluated over the 3 months of the re-
covery period compared to the basal level before the MCA occlu-sion. The neurological score was obtained from observations of the animals’ behaviors (e.g. analysis of their spontaneous activities in the cages, hand use during feeding, interactions with animal caregivers) based on the following criteria: 0 = no apparent deficit; 1 = use of the left hand with noticeable deficits; 2 = no use of the left hand, and 3 = death. When the behaviors of the operated ani-mals precluded accurate evaluation of the neurological score (be-cause of altered consciousness, apathy, etc.), they were not tested. Evaluation of the neurological score was performed on videotapes in a blinded fashion by both basic scientists and clinicians.
Statistics Statistical analyses of the data presented in table 1 were per-
formed using the ANOVA test for multiple comparisons. p ! 0.05 was considered statistically significant.
Results
The schematic illustration of the surgical approach, placement of the micropipette, and the study protocol are illustrated in figure 1 . The embolization procedure was difficult and evolved during the course of the study. The first 6 monkeys allowed us to standardize the procedure (determination of the volume of thrombin used and how the injection is performed). Once the procedure was es-tablished, we performed it on 6 additional animals to de-termine the reproducibility of the model.
Physiological and Biochemical Data Anesthesia was regulated on an individual basis. The
surgical intervention, the timing of the MRI examina-tions, and the survival period were the same for each monkey studied. No significant differences were noted in the physiological data measured with respect to time (n = 12). These data are presented in table 1 .
Establishment of the Injection Procedure Because of methodological issues (mainly due to dys-
functional injection systems leading to a low quantity of injected thrombin) the first two monkeys showed no sig-nificant parenchymal infarction on MRI during the course of the study. The next two monkeys received the thrombin injection into the M1 segment of the MCA while the artery was patent. The example of m576 ( fig. 2 a) showed that, due to the diameter of the artery and the perfusion pressure, the clot did not remain in place. In-deed, there was visual evidence [later confirmed by mag-netic resonance angiography (MRA) at +2 h, fig. 2 a] that, immediately following the injection, the clot was flushed
Table 1. Physiological and biochemical parameters measured before and after controlled embolic stroke in anesthetized monkeys
Condition Baseline(n = 12)
M CAO
0 h +2 h +1 day +7 days +21 days +3 months(n = 12) (n = 12) (n = 12) (n = 9) (n = 9) (n = 9)
Heart rate, beats/min 137810 124813 127810 133811 140815 134813 12888MAP, mm Hg 80817 73814 7589 76811 78815 84820 69812ET pCO2, mm Hg 3783 3981 3882 3685 3882 3882 3783SpO2, % 9782 9782 9781 9682 9781 9782 9683Temperature, ° C 38.581.0 37.880.5 38.080.5 38.380.7 37.780.5 38.380.8 38.180.6Sevoflurane, % 1.680.4 1.980.3 1.880.2 1.880.3 1.980.3 1.880.3 1.880.3
Val ues are presented as means 8 SD. One-way ANOVAR using 95% confidence limits. Baseline = Control measurements made at least 2 weeks prior to surgery. Time: 0 h – MCAO; MAP = noninvasive mean arterial pressure; ET pCO2 = partial pressure of exhaled carbon dioxide; SpO2 = saturation of peripheral oxygen.
Dow
nloa
ded
by:
INS
ER
M D
ISC
IST
193.
54.1
10.3
3 -
7/8/
2013
12:
07:5
0 P
M

Thrombotic Stroke in the Anesthetized Monkey
Cerebrovasc Dis 2012;33:329–339 333
through the circulation to lodge at the boundary zones of the vascular tree or in small arterioles, leading to a corti-cal hyperintense signal that covered the entire MCA ter-ritory (T2 image at +24 h, fig. 2 a) with some involvement of the posterior aspect of the putamen. In the next mon-key (m586, fig. 2 b), a transient ligature of the distal part of the MCA was performed prior to the injection of thrombin into the MCA during blood flow interruption. This procedure resulted in an acute hyperintense signal on DWI that encompassed the putamen, the caudatenucleus, and the internal capsule (data not shown). The ischemic lesion was restricted to the basal ganglia region with sparing of the parasylvian cortex. The MRA showed a reduction in the apparent caliber of the MCA, but the MCA was by no means completely occluded ( fig. 2 b, MRA). Thus, the clot might have been flushed into len-ticulostriate arteries. At +24 h, the T2 hyperintense signal ( fig. 2 b, T2) clearly showed the presence of large areas of edematous tissue in deep brain regions. Without proxi-mal ligature the distal occlusion of the MCA preserves perfusion of the lenticulostriate arteries. This residual
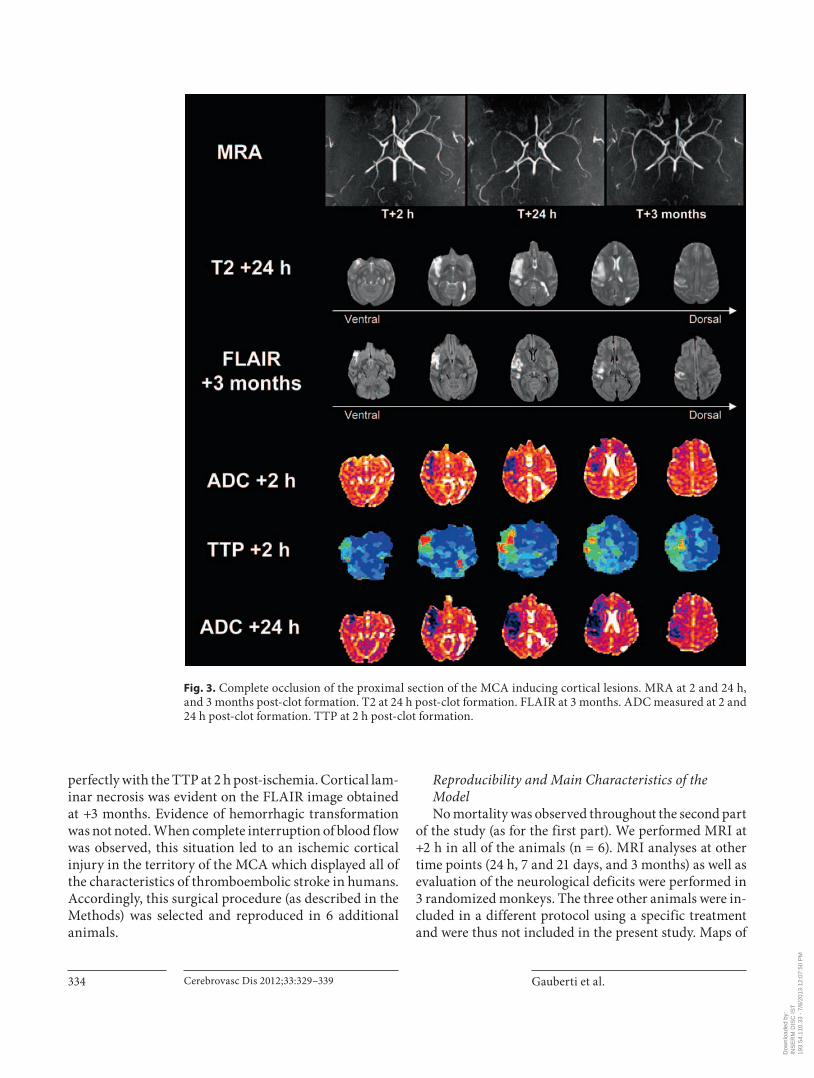
bloodstream drags the thrombin-induced clot from the proximal arteries to the deep brain. Then, occlusion of the striatal arteries leads to a persistent subcortical in-farct. In the next monkey (m488, fig. 3 ), the injection of thrombin was performed in the isolated M1 segment of the MCA (with both proximal and distal ligatures). This procedure induced complete occlusion of the artery as il-lustrated in figure 3 (MRA at 2 h post-injection). Partial spontaneous reperfusion occurred some time between +2 h and 1 day post-ictus. The T2 image at +24 h ( fig. 3 ) showed involvement of the pre-central gyrus with some preservation of the post-central gyrus which was in good agreement with the hypoperfused area detected at +2 h on the TTP image. Accordingly, MRI investigations highlighted a significant diffusion-perfusion mismatch ( fig. 3 ). There was a clear difference 2 h post-ischemia be-tween the area of reduced ADC (dark area) and the area of hypoperfusion (TTP; bright area) which may corre-spond to a brain zone in jeopardy. Twenty-four hours lat-er, this area was recruited by the infarct core as illustrated by the size of the reduced ADC signal which matched
a
b
Fig. 2. a MRA (+2 h) and T2-weighted imaging (+24 h) after the MCAO approach in m576. b MRA (+2 h) and T2-weighted imaging (+24 h) after the MCAO approach in m586.
Dow
nloa
ded
by:
INS
ER
M D
ISC
IST
193.
54.1
10.3
3 -
7/8/
2013
12:
07:5
0 P
M
Gauberti et al. Cerebrovasc Dis 2012;33:329–339334
perfectly with the TTP at 2 h post-ischemia. Cortical lam-inar necrosis was evident on the FLAIR image obtained at +3 months. Evidence of hemorrhagic transformation was not noted. When complete interruption of blood flow was observed, this situation led to an ischemic cortical injury in the territory of the MCA which displayed all of the characteristics of thromboembolic stroke in humans. Accordingly, this surgical procedure (as described in the Methods) was selected and reproduced in 6 additional animals.
Reproducibility and Main Characteristics of the Model No mortality was observed throughout the second part
of the study (as for the first part). We performed MRI at +2 h in all of the animals (n = 6). MRI analyses at other time points (24 h, 7 and 21 days, and 3 months) as well as evaluation of the neurological deficits were performed in 3 randomized monkeys. The three other animals were in-cluded in a different protocol using a specific treatment and were thus not included in the present study. Maps of
Fig. 3. Complete occlusion of the proximal section of the MCA inducing cortical lesions. MRA at 2 and 24 h, and 3 months post-clot formation. T2 at 24 h post-clot formation. FLAIR at 3 months. ADC measured at 2 and 24 h post-clot formation. TTP at 2 h post-clot formation.
Dow
nloa
ded
by:
INS
ER
M D
ISC
IST
193.
54.1
10.3
3 -
7/8/
2013
12:
07:5
0 P
M

Thrombotic Stroke in the Anesthetized Monkey
Cerebrovasc Dis 2012;33:329–339 335
infarction probability at 2 h (n = 6) and 24 h (n = 3) are shown in figure 4 a. Individual images of the 3 monkeys followed during 3 months are presented in figure 4 b. Im-portantly, all animals showed complete occlusion of the MCA on the MRA performed +2 h after thrombin in-jection ( fig. 5 a). At +24 h, 66% of the animals showed
arterial reperfusion and at +7 days, reperfusion had oc-curred in all animals ( fig. 5 a). Interestingly, pixel-by-pixel analysis revealed a perfusion mismatch at 2 h post-occlu-sion in 5 of 6 animals (not shown). Among the 3 animals which had MRI follow-up at +24 h and +7 days, 2 showed hemorrhagic transformation at +7 days (as il lustrated in
a
b
Fig. 4. a Probability infarction map calcu-lated from DWI at 2 and 24 h post-occlu-sion. b Longitudinal MRI findings of the 3 monkeys with the 3-month follow-up in-cluding MRA at 2 h, T2-weighted imaging at 24 h, and FLAIR at 3 months post-occlu-sion.
Dow
nloa
ded
by:
INS
ER
M D
ISC
IST
193.
54.1
10.3
3 -
7/8/
2013
12:
07:5
0 P
M

Gauberti et al. Cerebrovasc Dis 2012;33:329–339336
fig. 5 e). The mean lesion volume on DWI at +2 h was 1.82 cm 3 ( 8 1.08 SD). As expected, the lesion volume (DWI) increased between +2 and +24 h (mean: 4.02 cm 3 8 1.38 SD at +24 h , fig. 5 b). Pixel-by-pixel analysis revealed that most brain regions which infarcted between 2 and 24 h post-occlusion showed hemodynamic impairment on
PWI imaging at 2 h ( fig. 5 c). No reversal of ADC was seen in our study using the 80% threshold. Ischemic lesions (as assessed by DWI-weighted imaging at +2 h) involved sub-cortical (1 of 6) or both cortical and subcortical (5 of 6) areas. BBB opening was evident at +24 h and +7 days post-ictus in all animals studied ( fig. 5 d).
MCA occlusion led to a measurable functional deficit in the 3 animals tested 21 days after MCAO, as expected after the MRI evaluation of the lesion ( table 2 ). However, neurological deficit persisted at 3 months when the cau-date nucleus and the putamen were encompassed by the infarct (m889, m907).
Discussion
In accordance with the recommendations described in the updated STAIR report [33, 34] , we developed a novel model of embolic stroke in the anesthetized monkey. In
Table 2. N eurological score performed at 7, 21, and 90 days post-stroke
Animal Pre-MCAO 7 days 21 days 90 days
m862 0 NT 2 0m889 0 1 1 1m907 0 NT 2 2
N T = Not tested; 0 = no apparent deficit; 1 = use of the left hand with noticeable deficits; 2 = no use of the left hand; 3 = death.
c
d e
a b
Fig. 5. a Percentage of animals with MCA reperfusion at 2 and 24 h, and 7 days post-clot formation. b Lesion volume measured on DWI images 2 and 24 h post-clot forma-tion. c Representative images of the pixel-by-pixel analysis of the diffusion mis-match. d Representative image of BBB per-meability to gadolinium at 2 and 24 h, and 7 days post-clot formation. e Representa-tive image of hemorrhagic transformation (arrows).
Dow
nloa
ded
by:
INS
ER
M D
ISC
IST
193.
54.1
10.3
3 -
7/8/
2013
12:
07:5
0 P
M

Thrombotic Stroke in the Anesthetized Monkey
Cerebrovasc Dis 2012;33:329–339 337
this experimental model we observed many of the vascu-lar abnormalities noted in humans during and after a stroke: the clot remains in place at least over several hours inducing downstream ischemic damages, thus allowing the timely administration of drugs including thrombo-lytic agents such as tissue-type plasminogen activator (tPA; with or without a neuroprotector agent).
MRI techniques were used to evaluate the conse-quences of ischemic stroke as this technology is readily available in most stroke centers. Although MRI technol-ogy identifies regions of mismatch, the hypothesis that DWI and PWI allows precise identification of the ische-mic core and penumbra is still debated [35–37] . Nonethe-less, most neurologists select their patients who are eli-gible for thrombolysis [38–41] based on, among other fac-tors, PW- and DW-MRI. For this reason, we used the same diagnostic procedures as those performed in the stroke clinic to evaluate acute and chronic pathological changes associated with focal cerebral ischemia.
Among stroke models in nonhuman primates de-scribed so far, we consider that our present thrombotic model induced by local injection of thrombin displays most of the features of the clinical situation. For instance, in contrast to our present protocol, in models where au-tologous or heterologous preformed clots are used [22, 23, 42, 43] , the precise location of the arterial occlusion is not controlled (proximal or distal, middle or anterior MCA, involvement of the lenticulostriate arteries). In the pho-tothrombotic model [27, 28] , although the location of the clot is also controlled, concerns have been recently raised about the mechanism involved in clot formation in such models and its relevance in what happens in the ‘real-life situation’ [44] . In contrast, in our present model, throm-bus formation is triggered by a direct thrombin injection, thus mimicking the endogenous activation of thrombin mediated by the tissue factor, as could occur in humans during vascular thrombosis [45] . Thus, we believe thatour model acutely mimics the human pathology and ad-dresses some of the limitations of the previously de-scribed models.
This model could be relevant for future pre-clinical studies, either to validate strategies of brain protection, advance research on biomarkers, or for the development of new MRI sequences. In most nonhuman primate mod-els of stroke, there are some caveats that must be taken into account. The various methodologies used to occlude a major cerebral artery, most often the MCA, are de-scribed above. All of these techniques are feasible for the study of therapeutic efficacy, but few, apart from the ad-ministration of autologous blood clots, provide the repre-
sentative conditions of embolic stroke in humans. Nota-bly, successful treatment of experimental embolic stroke has rarely been achieved in nonhuman primate models [42, 43] . There is an urgent need for the development of new clinically relevant models of embolic stroke in the nonhuman primate. Our model of embolic stroke allows the direct induction of a single clot into the M1 segment of the MCA and permits localized occlusion of this major cerebral artery with, as in most humans experiencing ischemic stroke, spontaneous reperfusion in the follow-ing days.
It is difficult to accurately assess the time of onset of symptoms in a stroke patient. However, through the use of this novel experimental model we can accurately fol-low ischemic disturbances with respect to time and eval-uate the efficacy of thrombolysis after administration of the drug even beyond the 4.5-hour time window as cur-rently proposed [46, 47] .
One criterion of any model of focal cerebral ischemia is that it must have a reproducible lesion volume and thus a small number of ischemic animals could be compared to a treated group. We believe that variations in cerebro-vascular architecture are an inherent factor of variability in man and, as was noted in the present study during the surgical preparation, in the nonhuman primate. Fortu-nately, the present model allows us to obtain a priori an individual MRA of each monkey prior to the surgical in-tervention and to assess the best possible approach for the injection site of thrombin. Furthermore, it is possible with this model to perform long-term evaluations using MRI, a technique rarely performed in the chronic stage of stroke in humans since the lesion is normally consoli-dated within 48–72 h.
Several key points remain, however, to be clarified and improved. In the present experimental stroke model, thrombus formation is triggered by a large amount of re-combinant active thrombin. The injected thrombin could interact with the endothelium located downstream of the resulting thrombus and could trigger intracellular sig-naling unrelated to ischemia. However, in similar studies performed in rodents, intravascular thrombin did not produce any detectable side effects [48, 49] , suggesting that this mechanism is unlikely to significantly influence stroke outcome in the present model.
In contrast to other less invasive experimental stroke models, we performed enucleation to expose the MCA. Thus, ischemia-unrelated modifications of visual skills are expected and should be taken into account for neuro-logical evaluation in enucleated animals. The craniotomy performed during the transorbital approach was as small
Dow
nloa
ded
by:
INS
ER
M D
ISC
IST
193.
54.1
10.3
3 -
7/8/
2013
12:
07:5
0 P
M

Gauberti et al. Cerebrovasc Dis 2012;33:329–339338
References
1 Alonso de Leciñana M, Díez-Tejedor E, Car-celler F, Roda JM: Cerebral ischemia: from animal studies to clinical practice – should the methods be reviewed? Cerebrovasc Dis 2001; 11: 20–30.
2 del Zoppo GJ, Copeland BR, Harker LA, Waltz TA, Zyroff J, Hanson SR, Battenberg E: Experimental acute thrombotic stroke in baboons. Stroke 1986; 17: 1254–1265.
3 Kito G, Nishimura A, Susumu T, Nagata R, Kuge Y, Yokota C, Minematsu K: Experi-mental thromboembolic stroke in cynomol-gus monkey. J Neurosci Methods 2001; 105: 45–53.
4 Green RA, Odergren T, Ashwood T: Animal models of stroke: do they have value for dis-covering neuroprotective agents? Trends Pharmacol Sci 2003; 24: 402–408.
5 Young AR, Ali C, Duretete A, Vivien D: Neu-roprotection and stroke: time for a compro-mise. J Neurochem 2007; 103: 1302–1309.
6 Marshall JW, Duffin KJ, Green AR, Ridley RM: NXY-059, a free radical-trapping agent, substantially lessens the functional disabili-ty resulting from cerebral ischemia in a pri-mate species. Stroke 2001; 32: 190–198.
7 Strong AJ, Smith SE, Whittington DJ, Mel-drum BS, Parsons AA, Krupinski J, Hunter AJ, Patel S: Factors influencing the frequency of f luorescence transients as markers of peri-infarct depolarizations in focal cerebral is-chemia. Stroke 2000; 31: 214–221.
8 Bihel E, Pro-Sistiaga P, Letourneur A, Toutain J, Saulnier R, Insausti R, Bernaudin M, Roussel S, Touzani O: Permanent or tran-sient chronic ischemic stroke in the non-hu-man primate: behavioral, neuroimaging, histological, and immunohistochemical in-vestigations. J Cereb Blood Flow Metab 2010; 30: 273–285.
9 Freret T, Bouet V, Toutain J, Saulnier R, Pro-Sistiaga P, Bihel E, Mackenzie ET, Roussel S, Schuhmann-Bard P, Touzani O: Intralumi-nal thread model of focal stroke in the non-human primate. J Cereb Blood Flow Metab 2008; 28: 786–796.
10 Jungreis CA, Nemoto E, Boada F, Horowitz MB: Model of reversible cerebral ischemia in a monkey model. AJNR Am J Neuroradiol 2003; 24: 1834–1836.
11 Hamberg LM, Hunter GJ, Maynard KI, Owen C, Morris PP, Putman CM, Ogilvy C, González RG: Functional CT perfusion im-aging in predicting the extent of cerebral in-farction from a 3-hour middle cerebral arte-rial occlusion in a primate stroke model. AJNR Am J Neuroradiol 2002; 23: 1013–1021.
12 Zabramski JM, Spetzler RF, Selman WR, Roessmann UR, Hershey LA, Crumrine R, Macko R: Naloxone therapy during focal ce-rebral ischemia evaluation in a primate mod-el. Stroke 1984; 15: 621–627.
13 Frazee JG, Luo X, Luan GM, Hinton DS, Hovda DA, Shiroishi MS, Barcliff LT: Retro-grade transvenous neuroperfusion: a back door treatment for stroke. Stroke 1998; 29: 1912–1916.
14 Touzani O, Young AR, Derlon JM, Baron JC, MacKenzie ET: Progressive impairment of brain oxidative metabolism reversed by re-perfusion following middle cerebral artery occlusion in anaesthetized baboons. Brain Res 1997; 767: 17–25.
15 Michenfelder JD, Sundt TM: Cerebral ATP and lactate levels in the squirrel monkey fol-lowing occlusion of the middle cerebral ar-tery. Stroke 1971; 2: 319–326.
16 Crowell RM, Olsson Y, Klatzo I, Ommaya A: Temporary occlusion of the middle cerebral artery in the monkey: clinical and patholog-ical observations. Stroke 1970; 1: 439–448.
17 Hudgins WR, Garcia JH: Transorbital ap-proach to the middle cerebral artery of the squirrel monkey: a technique for experimen-tal cerebral infarction applicable to ultra-structural studies. Stroke 1970; 1: 107–111.
18 Symon L: Regional cerebrovascular respons-es to acute ischaemia in normocapnia and hypercapnia: an experimental study in ba-boons. J Neurol Neurosurg Psychiatry 1970; 33: 756–762.
19 Morawetz RB, DeGirolami U, Ojemann RG, Marcoux FW, Crowell RM: Cerebral blood flow determined by hydrogen clearance dur-ing middle cerebral artery occlusion in un-anesthetized monkeys. Stroke 1978; 9: 143–149.
20 Dodson RF, Aoyagi M, Chu LW: Ultrastruc-tural changes in subacute cerebral infarction following middle cerebral artery occlusion in the baboon. Cytobios 1975; 13: 97–108.
as possible and reconstruction of the orbit avoided a sig-nificant effect on the post-stroke intracranial pressure. Nevertheless, this surgical procedure could trigger local inflammation and could be confounding in some cases (such as investigation of inflammatory-related biomark-ers). Sham-operated animals would be needed as a con-trol group in such cases.
Another critical issue is the number of animals needed to detect any significant effect of a neuroprotective treat-ment in this model. Since the lesion volume at 24 h is ap-proximately twice the volume at 2 h, we can assume that neuroprotective treatments started 2 h after thrombus formation could reduce the ischemic lesion size by maxi-mum 50% at 24 h. Sample size calculation [standardized difference = 0.5 !(4.02/1.38) = 1.46] indicates that 8 an-imals per group are needed to detect the treatment effect on the lesion volume at 24 h with a power of 0.8 and a cutoff for statistical significance of 0.05 (t test). To detect
a more reasonable difference of 25% in lesion size at 24 h, 15 animals per group would be needed. Thus, a study in-vestigating a neuroprotective treatment in this model should involve 30 monkeys in order to be sufficiently powered.
Given that this model has most of the main character-istics of ischemic stroke in humans (i.e. arterial occlusion by a blood clot, diffusion/perfusion mismatch, and even-tually hemorrhagic transformation), together with a very low mortality rate, we believe that it fulfills all of the cri-teria for assessing the pre-clinical efficacy of a treatment.
Acknowledgements
This work was supported by grants from the INSERM, the University of Caen-Basse Normandie, and the Regional Council of Lower Normandy.
Dow
nloa
ded
by:
INS
ER
M D
ISC
IST
193.
54.1
10.3
3 -
7/8/
2013
12:
07:5
0 P
M

Thrombotic Stroke in the Anesthetized Monkey
Cerebrovasc Dis 2012;33:329–339 339
21 Ott EO, Abraham JA, Meyer JS, Tulleken CA, Mathew NT, Achari AN, Aoyagi M, Dodson RF: Regional cerebral blood flow measured by the gamma camera after direct injection of 133Xe into the distal stump of the occlud-ed middle cerebral artery. Stroke 1975; 6: 376–381.
22 Kuge Y, Yokota C, Tagaya M, Hasegawa Y, Nishimura A, Kito G, Tamaki N, Hashimoto N, Yamaguchi T, Minematsu K: Serial changes in cerebral blood flow and flow-me-tabolism uncoupling in primates with acute thromboembolic stroke. J Cereb Blood Flow Metab 2001; 21: 202–210.
23 Xie Y, Munekata K, Seo K, Hossmann KA: Effect of autologous clot embolism on re-gional protein biosynthesis of monkey brain. Stroke 1988; 19: 750–757.
24 Sato Y, Chin Y, Kato T, Tanaka Y, Tozuka Y, Mase M, Ageyama N, Ono F, Terao K, Yoshi-kawa Y, Hisatsune T: White matter activated glial cells produce BDNF in a stroke model of monkeys. Neurosci Res 2009; 65: 71–78.
25 Watanabe O, Bremer AM, West CR: Experi-mental regional cerebral ischemia in the middle cerebral artery territory in primates. 1. Angio-anatomy and description of an ex-perimental model with selective emboliza-tion of the internal carotid artery bifurca-tion. Stroke 1977; 8: 61–70.
26 Bremer AM, Watanabe O, Bourke RS: Arti-ficial embolization of the middle cerebral ar-tery in primates: description of an experi-mental model with extracranial technique. Stroke 1975; 6: 387–390.
27 Koketsu D, Furuichi Y, Maeda M, Matsuoka N, Miyamoto Y, Hisatsune T: Increased number of new neurons in the olfactory bulb and hippocampus of adult non-human pri-mates after focal ischemia. Exp Neurol 2006; 199: 92–102.
28 Furuichi Y, Maeda M, Moriguchi A, Sawa-moto T, Kawamura A, Matsuoka N, Mutoh S, Yanagihara T: Tacrolimus, a potential neu-roprotective agent, ameliorates ischemic brain damage and neurologic deficits after focal cerebral ischemia in nonhuman pri-mates. J Cereb Blood Flow Metab 2003; 23: 1183–1194.
29 Kaku S, Umemura K, Mizuno A, Yano S, Su-zuki K, Kawasaki T, Nakashima M: Evalua-tion of a GPIIb/IIIa antagonist YM337 in a primate model of middle cerebral artery thrombosis. Eur J Pharmacol 1998; 345: 185–192.
30 Young AR, Sette G, Touzani O, Rioux P, Der-lon JM, MacKenzie ET, Baron JC: Relation-ships between high oxygen extraction frac-tion in the acute stage and final infarction in reversible middle cerebral artery occlusion: an investigation in anaesthetized baboons with positron emission tomography. J Cereb Blood Flow Metab 1996; 16: 1176–1188.
31 Orset C, Macrez R, Young AR, Panthou D, Angles-Cano E, Maubert E, Agin V, Vivien D: Mouse model of in situ thromboembolic stroke and reperfusion. Stroke 2007; 38: 2771–2778.
32 Røhl L, Ostergaard L, Simonsen CZ, Vester-gaard-Poulsen P, Andersen G, Sakoh M, Le Bihan D, Gyldensted C: Viability thresholds of ischemic penumbra of hyperacute stroke defined by perfusion-weighted MRI and ap-parent diffusion coefficient. Stroke 2001; 32: 1140–1146.
33 Fisher M, Feuerstein G, Howells DW, Hurn PD, Kent TA, Savitz SI, Lo EH: Update of the stroke therapy academic industry round-table preclinical recommendations. Stroke 2009; 40: 2244–2250.
34 Recommendations for standards regarding preclinical neuroprotective and restorative drug development. Stroke 1999; 30: 2752–2758.
35 Sobesky J, Weber OZ, Lehnhardt FG, Hes-selmann V, Neveling M, Jacobs A, Heiss WD: Does the mismatch match the penumbra? Magnetic resonance imaging and positron emission tomography in early ischemic stroke. Stroke 2005; 36: 980–985.
36 Kranz PG, Eastwood JD: Does diffusion-weighted imaging represent the ischemic core? An evidence-based systematic review. AJNR Am J Neuroradiol 2009; 30: 1206–1212.
37 Kane I, Sandercock P, Wardlaw J: Magnetic resonance perfusion diffusion mismatch and thrombolysis in acute ischaemic stroke: a systematic review of the evidence to date. J Neurol Neurosurg Psychiatry 2007; 78: 485–491.
38 Chemmanam T, Campbell BC, Christensen S, Nagakane Y, Desmond PM, Bladin CF, Parsons MW, Levi CR, Barber PA, Donnan GA, Davis SM, EPITHET Investigators: Ischemic diffusion lesion reversal is uncom-mon and rarely alters perfusion-diffusion mismatch. Neurology 2010; 75: 1040–1047.
39 Donnan GA, Baron JC, Ma H, Davis SM: Penumbral selection of patients for trials of acute stroke therapy. Lancet Neurol 2009; 8: 261–269.
40 Ebinger M, De Silva DA, Christensen S, Par-sons MW, Markus R, Donnan GA, Davis SM: Imaging the penumbra – strategies to detect tissue at risk after ischemic stroke. J Clin Neurosci 2009; 16: 178–187.
41 Solling C, Hjort N, Ashkanian M, Oster-gaard L, Andersen G: Safety and efficacy of MRI-based selection for recombinant tissue plasminogen activator treatment: responder analysis of outcome in the 3-hour time win-dow. Cerebrovasc Dis 2009; 27: 223–229.
42 Susumu T, Yoshikawa T, Akiyoshi Y, Nagata R, Fujiwara M, Kito G: Effects of intra-arte-rial urokinase on a non-human primate thromboembolic stroke model. J Pharmacol Sci 2006; 100: 278–284.
43 Omura T, Tanaka Y, Miyata N, Koizumi C, Sakurai T, Fukasawa M, Hachiuma K, Mina-gawa T, Susumo T, Yoshida S, Nakaike S, Okuyama S, Harder DR, Roman RJ: Effect of a new inhibitor of the synthesis of 20-HETE on cerebral ischemia reperfusion injury. Stroke 2006; 37: 1307–1313.
44 Kleinschnitz C, Braeuninger S, Pham M, Austinat M, Nölte I, Renné T, Nieswandt B, Bendszus M, Stoll G: Blocking of plateletsor intrinsic coagulation pathway-driven thrombosis does not prevent cerebral infarc-tions induced by photothrombosis. Stroke 2008; 39: 1262–1268.
45 Owens AP 3rd, Mackman N: Tissue factor and thrombosis: the clot starts here. Thromb Haemost 2010; 104: 432–439.
46 Carpenter CR, Keim SM, Milne WK, Meurer WJ, Barsan WG: Thrombolytic therapy for acute ischemic stroke beyond three hours.J Emerg Med 2011; 40: 82–92.
47 del Zoppo GJ, Saver JL, Jauch EC, Adams HP Jr: Expansion of the time window for treat-ment of acute ischemic stroke with intrave-nous tissue plasminogen activator: a science advisory from the American Heart Associa-tion/American Stroke Association. Stroke 2009; 40: 2945–2948.
48 García-Yébenes I, Sobrado M, Zarruk JG, Castellanos M, Pérez de la Ossa N, Dávalos A, Serena J, Lizasoain I, Moro MA: A mouse model of hemorrhagic transformation by de-layed tissue plasminogen activator adminis-tration after in situ thromboembolic stroke. Stroke 2011; 42: 196–203.
49 Zhang Z, Zhang RL, Jiang Q, Raman SB, Cantwell L, Chopp M: A new rat model of thrombotic focal cerebral ischemia. J Cereb Blood Flow Metab 1997; 17: 123–135.
D
ownl
oade
d by
: IN
SE
RM
DIS
C IS
T19
3.54
.110
.33
- 7/
8/20
13 1
2:07
:50
PM
Related Documents