Thoracolumbar Fractures

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ThoracolumbarFractures

Thoracic and lumbar fractures account for 50% of all spinal traumatic fractures.
• Incidence.
4-5 per 100,000.
18 - 35 years.
Male\ Female = 4:1
Neurologic injury 25% of cases.
• 65% of TL#s occurs between the T9&L2 vertebrae.
(thoracolumbar Junction)


Functional spinal unit
Composed of: • 2 adjacent vertebrae • Facet joint• Inter vertebral disc • Intervening ligaments
4
This unit is responsible for Movement of spine

Thoracic Spine
• Kyphotic Curve.
• Ribs more stiffness, resist rotation.
• T11,T12 have floating ribs;
No costotransverse articulations.
No sternal attachement.
•Facet orientation limited flexion/extension.
•Canal is relatively small.

Lumbar Spine
• Lordotic Curve.
• Large discs More mobility
• Spinal canal wider.
• Spinal cord ended at L1.
• Facet orientation more
flexion/extension.

•Transition between the stiff kyphotic thoracic spine
and mobile lordotic lumbar spine.
• In trauma;
Thoracic spine deforms into kyphosis,
Lumbar spine into lordosis leaving,
Junction exposed to pure compression.
• T11, T12 are less stable less resistance to
rotation more stress.
Why Thoraco-lumbar junction is more succeptible?

ETIOLOGY
• High energy trauma (RTA 50%)
• Falls.
• Sports accident.
• Gunshot injury.
• Osteoporosis
• Tumors
• Weak bone(malnutrition,renal,RA,DM,endocrine).

– 16% major chest injury
– 10% major abdominal injury
– 8% long bone/ pelvic fractures
Spinal fracture should be suspected in;1. Comatosed patient.
2. High energy trauma.
3. Evidence of neurological deficit.
4. Multiple injuries:

Missed TL#s reach 5%, And reach 22% in cervical fractures.
The main causes are,
• Poly trauma.
• low level of suspicion.
• Intoxication \ unconsciousness
• Failure to take proper radiographs.
• Failure to interpret the x ray.

CLASSIFICATION

Three column theory
ANTERIOR COLUMN
MIDDLE COLUMN
POSTERIOR COLUMN

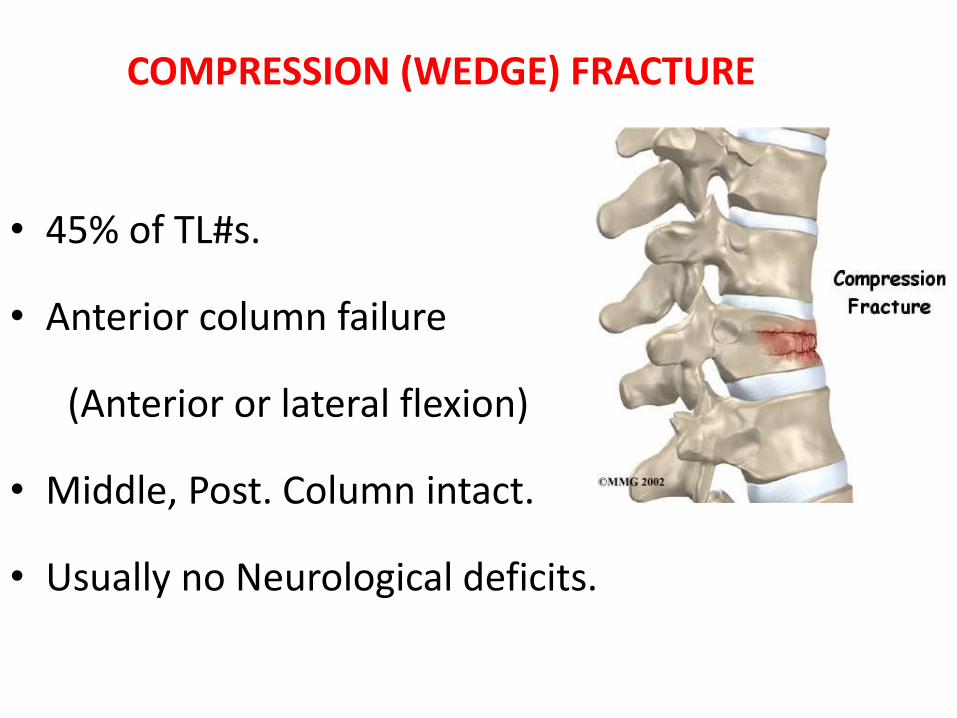
• 45% of TL#s.
• Anterior column failure
(Anterior or lateral flexion)
• Middle, Post. Column intact.
• Usually no Neurological deficits.
COMPRESSION (WEDGE) FRACTURE



Burst fractures
• 15 % of TL#s
• Anterior& middle column failure.
(Axial compression)
• Most common at T/L junction
• Neurological deficit.



FLEXION-DISTRACTION = SEAT-BELT-TYPE = CHANCE #
• Posterior &middle columns failure.
(hyperflexion then tension forces)
• Anterior column
- partial damage.
- functions like a hinge.



Fracture-Dislocation
• Failure of all columns (compression, tension,
rotation, or shear).
• anterior hinge is disrupted.
• Dislocation.
• Severe neurological deficit.



Approach to Spine
Trauma

Pre Hospital Care
• Proper extraction & Immobilization;
Cervical collar
Hard board (log roll)
Sand bag
Tape
• Airway protection.
• Rapid & safe transfer for suitable facilities.

Emergency Assessment
ABCs & Immobilization Hemodynamically stable
Secondary Survey:
1-Log roll technique
2-Remove the spinal board
3-Remove cervical collar carefully
4-Brief history (Mechanism, movement, position)

Inspection
• Clothes removed.
• Bleeding , abrasion or lacerations.
• Deformity, Swelling.
• Limb asymmetry (movements).
• Chest expansion, Paradoxical breathing.

Palpation
1. Tenderness.
2. Swelling.
3. Interspinous widening (>7mm).
4. Malialignement of spinouse process .
5. Step off.

Initial Neurological Assessment

Initial Assessment:Motor Examination

Initial Assessment:Motor Examination

Initial Assessment:Sensation
Initial Assessment:Reflexes
1. Babiniski sign.
2. Perianal/perineal sensation
3. Rectal tone
4. Cresmatic reflex

RADIOLOGICAL ASSESMENT

X-RAYS Lateral View
• Alignment.
• Contour of bodies.
• Disc spaces.
• Angulation.
• Encroachment on canal.
• Loss of vertebral body height.

X-RAYS Lateral View
• Measurement of degree of vertebral body compression.

• Look at how the ant.& post. aspects of the body line up.
X-RAYS Lateral View

X-RAYS Lateral View
• Measure Kyphosis.
• Measure from closest intact endplates.

• Alignment
• Symmetry/ Shape of pedicles
• Interpedicular distance
• Position of spinous process
• Contour of bodies
X-RAYS A-P view

X-RAYS A-P view
• Lateral vertebral body height.
• Interpedicular
distance.
• Distance between the spinousprocesses.

CT Scan
• Accurate assessment
of bone.
1- Comminution.
2- Canal compromise.
3- Dislocation.

MRI
• Accurate assessment
of soft tissue.
1- Neurological deficits.
2- Cord lesion.
3- Ligament injury.
4- Disc herniation.
5- Hematoma.

Treatment

Goals
1. Maximise neurological recovery .
2. Maintain or restore spinal alignment.
3. Obtain a healed and stable spinal column.
4. Prevent future deformity.

Spinal Cord Injury
Methylprednisolone
• 30mg/kg iv bolus over 15min.
• 5.4 mg/kg/h infusion over 23 hrs (first 3 hours).
• 5.4 mg/kg/h for 47hrs (if > 3 – 8 hrs passed).
Proton pump inhibitor & LMW Heparin

Non-operative treatment
Indications:• Ant. vertebral height loss < 40%.
• Canal compromise < 40%.
• kyphosis < 25 degrees.
Bed Rest• Strict bed rest for 3- 4 weeks.
• Avoid flexion, sit-ups, & spinal rotation.
• Avoid weight bearing.
• Bed rolling encouraged.

Bracing
• Treated with brace for 6-8 weeks.
• Wear on whenever upright.
• Ambulation & Transfers.
• Solid healing 8-12 weeks.

Operative treatment
Indications:• Ant. vertebral height loss > 40%.
• Canal compromise > 40%.
• Kyphosis > 25 degrees.
• Neural compression.
Aim
• Neural Decompression.
• Stabilization.
• Solid fusion.

Surgical options
Anterior FixationPosterior Fixation

Vertebroplasty

Kyphoplasty

Rehabilitation
• Physiotherapy.
• Bladder dysfunction: Intermittent cath.
Supra-pubic cath.
• Bowel dysfunction: high fluids, fibers, Prokinetic.
• Spasticity: Stretching exercises, Baclofen, surgical.
• DVT prevention.
• Chest physiotherapy.
• Bed sore prevention: Postural change/2h, Air mattress,
High protein diet.

Related Documents









![[Treatment options for problematic thoracic and lumbar osteoporotic fractures]](https://static.cupdf.com/doc/110x72/6339e0838308f0b2d3050ee7/treatment-options-for-problematic-thoracic-and-lumbar-osteoporotic-fractures.jpg)

