Research Article The Immunological Plasmodium falciparum Malaria Characteristics of Children in Tajikistan Republic Nighina M. Khodzhaeva, 1 Alla M. Baranova , 2 and Anatoly K. Tokmalaev 3 1 Ibn Sina Tajik State Medical University, Dushanbe, Tajikistan 2 Sechenov First Moscow State Medical University, Moscow, Russia 3 e Peoples’ Friendship University of Russia, Moscow, Russia Correspondence should be addressed to Alla M. Baranova; [email protected] Received 23 January 2019; Revised 27 April 2019; Accepted 21 May 2019; Published 12 June 2019 Guest Editor: Faham Khamesipour Copyright © 2019 Nighina M. Khodzhaeva et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. e epidemiological situation in Tajikistan Republic deteriorated in the 1990s, when an influx of refugees from Afghanistan resulted in mass importation of Plasmodium vivax and Plasmodium falciparum malaria to Khatlon region. e National Programme of Malaria Control was successful and malaria transmission was interrupted in 2009. Background. e aim of this study was to investigate the mechanisms of immunological response in Tajik children with tropical Plasmodium falciparum malaria. Materials and Methods. We examined 124 patients with P. falciparum malaria at the age of 6 months up to 14 years that were hospitalized in Clinical Infectious Diseases Hospital in Dushanbe city and in Regional hospital of Khatlon region in the period 2000-2007. In most cases, they were school-age children (56%). e peak incidence was recorded in July-October. Verification of the diagnosis was based on clinical, epidemiological data, and the results of blood microscopy. In all patients, along with the standard, clinical, and laboratory tests, a number of indicators of the immune status were performed that include the T-immunity, the content of serum immunoglobulins of three main classes, the level of circulating immune complexes (CIC), C3 complement, and the concentration of key serum cytokines that have been studied in the dynamics of infectious process. Finding. e study of cellular and humoral immunity in patients with Plasmodium falciparum malaria is an obvious additional criterion in assessing the severity of infection. e imbalance of cytokine profile is an important pathogenic factor in the development of severe and recurrent forms of the disease, since the formation of a defective immune response to parasitic antigens contributes to adverse outcomes. Conclusions. Plasmodium falciparum malaria was characterized by depression of cellular and humoral immunity, the degree of which depended on the severity of the pathological process. 1. Background e Plasmodium falciparum malaria was registered in Tajik- istan Republic, the only in the European Region of World Health Organization. e epidemiological situation in the newly independent Tajikistan deteriorated further in 1993, when an influx of refugees from malaria endemic regions of Afghanistan resulted in mass importation of Plasmodium vivax and Plasmodium falciparum malaria to malaria genic areas of Khatlon region, bordering Afghanistan. In 1997, at the peak of the epidemic, 29794 malaria cases were officially reported in the country. Considerable financial, scientific, and practical support from the government and various international organizations played a crucial role in controlling the malaria epidemic [1]. e health system is structured in accordance with the administrative districts of the country. Primary health care services in urban and rural areas are provided by the Primary Health Centre, which offers diagnosis and treatment, curative and preventive measures, immunization, health education, and mother and child health protection measures. Various epidemic control measures in the stable malaria foci were used: mass drug administration of population by primaquine (14 days), indoor residual spraying (IRS) with cypermethrin, larvivorous fish Gambusia affinis in breading sites, insecticide-treated nets (ITNs), and personnel training resulting in a rapid decrease of malaria morbidity. e P. falciparum malaria patients received radical treatment by artesunate + sulphadoxine/pyrimethamine. In 2000-2008, Hindawi Journal of Tropical Medicine Volume 2019, Article ID 5147252, 6 pages https://doi.org/10.1155/2019/5147252

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Research ArticleThe Immunological Plasmodium falciparum MalariaCharacteristics of Children in Tajikistan Republic
Nighina M Khodzhaeva1 Alla M Baranova 2 and Anatoly K Tokmalaev3
1 Ibn Sina Tajik State Medical University Dushanbe Tajikistan2Sechenov First Moscow State Medical University Moscow Russia3The Peoplesrsquo Friendship University of Russia Moscow Russia
Correspondence should be addressed to Alla M Baranova barallamailru
Received 23 January 2019 Revised 27 April 2019 Accepted 21 May 2019 Published 12 June 2019
Guest Editor Faham Khamesipour
Copyright copy 2019 NighinaM Khodzhaeva et alThis is an open access article distributed under the Creative Commons AttributionLicensewhichpermits unrestricteduse distribution and reproduction in anymedium provided the original work is properly cited
The epidemiological situation in Tajikistan Republic deteriorated in the 1990s when an influx of refugees fromAfghanistan resultedin mass importation of Plasmodium vivax and Plasmodium falciparum malaria to Khatlon region The National Programme ofMalaria Control was successful and malaria transmission was interrupted in 2009 Background The aim of this study was toinvestigate the mechanisms of immunological response in Tajik children with tropical Plasmodium falciparummalaria Materialsand Methods We examined 124 patients with P falciparummalaria at the age of 6 months up to 14 years that were hospitalized inClinical Infectious Diseases Hospital in Dushanbe city and in Regional hospital of Khatlon region in the period 2000-2007 In mostcases they were school-age children (56) The peak incidence was recorded in July-October Verification of the diagnosis wasbased on clinical epidemiological data and the results of blood microscopy In all patients along with the standard clinical andlaboratory tests a number of indicators of the immune status were performed that include the T-immunity the content of serumimmunoglobulins of three main classes the level of circulating immune complexes (CIC) C3 complement and the concentrationof key serum cytokines that have been studied in the dynamics of infectious process Finding The study of cellular and humoralimmunity in patients with Plasmodium falciparummalaria is an obvious additional criterion in assessing the severity of infectionThe imbalance of cytokine profile is an important pathogenic factor in the development of severe and recurrent forms of the diseasesince the formation of a defective immune response to parasitic antigens contributes to adverse outcomesConclusions Plasmodiumfalciparummalaria was characterized by depression of cellular andhumoral immunity the degree ofwhich depended on the severityof the pathological process
1 Background
The Plasmodium falciparum malaria was registered in Tajik-istan Republic the only in the European Region of WorldHealth Organization The epidemiological situation in thenewly independent Tajikistan deteriorated further in 1993when an influx of refugees from malaria endemic regionsof Afghanistan resulted in mass importation of Plasmodiumvivax and Plasmodium falciparum malaria to malaria genicareas of Khatlon region bordering Afghanistan In 1997at the peak of the epidemic 29794 malaria cases wereofficially reported in the country Considerable financialscientific and practical support from the government andvarious international organizations played a crucial role in
controlling the malaria epidemic [1] The health system isstructured in accordance with the administrative districts ofthe country Primary health care services in urban and ruralareas are provided by the PrimaryHealthCentre which offersdiagnosis and treatment curative and preventive measuresimmunization health education andmother and child healthprotection measures Various epidemic control measures inthe stablemalaria foci were usedmass drug administration ofpopulation by primaquine (14 days) indoor residual spraying(IRS) with cypermethrin larvivorous fishGambusia affinis inbreading sites insecticide-treated nets (ITNs) and personneltraining resulting in a rapid decrease of malaria morbidityThe P falciparummalaria patients received radical treatmentby artesunate + sulphadoxinepyrimethamine In 2000-2008
HindawiJournal of Tropical MedicineVolume 2019 Article ID 5147252 6 pageshttpsdoiorg10115520195147252
2 Journal of Tropical Medicine
1
10
100
1000
10000
100000
P vivax (autochthonous cases)P falciparum (autochthonous cases)
1990
1992
1994 19
9619
9820
0020
02 2004
2006
2008 20
10 2012
2014
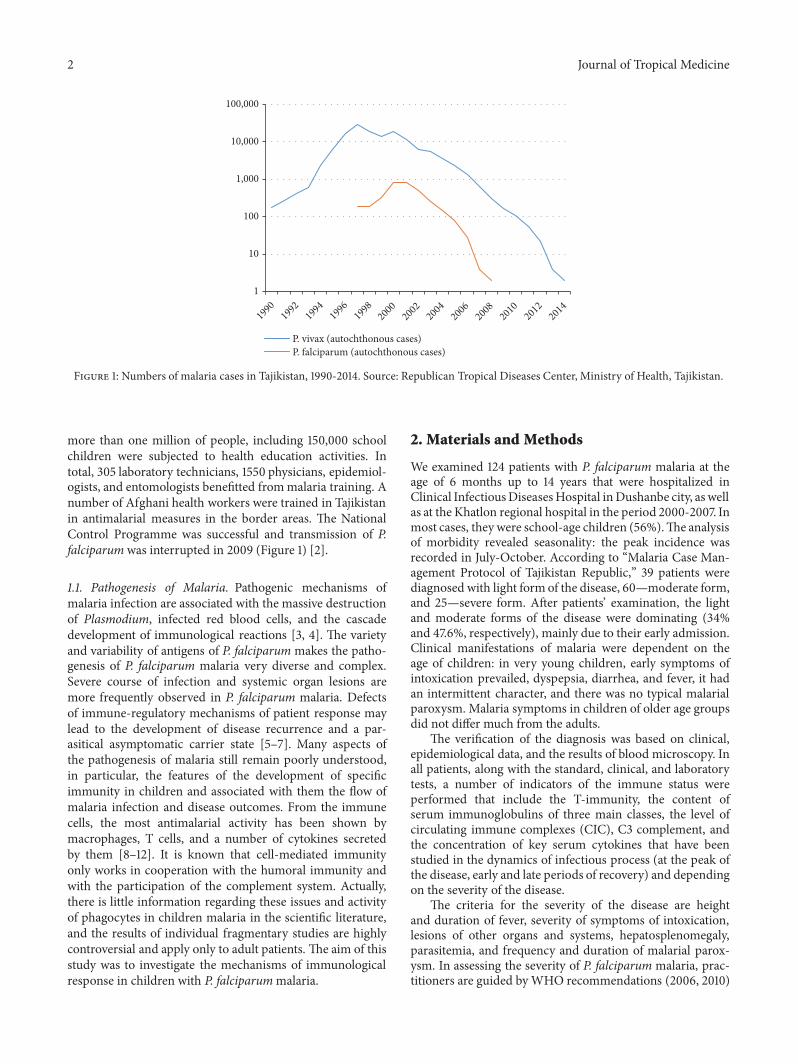
Figure 1 Numbers of malaria cases in Tajikistan 1990-2014 Source Republican Tropical Diseases Center Ministry of Health Tajikistan
more than one million of people including 150000 schoolchildren were subjected to health education activities Intotal 305 laboratory technicians 1550 physicians epidemiol-ogists and entomologists benefitted frommalaria training Anumber of Afghani health workers were trained in Tajikistanin antimalarial measures in the border areas The NationalControl Programme was successful and transmission of Pfalciparum was interrupted in 2009 (Figure 1) [2]
11 Pathogenesis of Malaria Pathogenic mechanisms ofmalaria infection are associated with the massive destructionof Plasmodium infected red blood cells and the cascadedevelopment of immunological reactions [3 4] The varietyand variability of antigens of P falciparum makes the patho-genesis of P falciparum malaria very diverse and complexSevere course of infection and systemic organ lesions aremore frequently observed in P falciparum malaria Defectsof immune-regulatory mechanisms of patient response maylead to the development of disease recurrence and a par-asitical asymptomatic carrier state [5ndash7] Many aspects ofthe pathogenesis of malaria still remain poorly understoodin particular the features of the development of specificimmunity in children and associated with them the flow ofmalaria infection and disease outcomes From the immunecells the most antimalarial activity has been shown bymacrophages T cells and a number of cytokines secretedby them [8ndash12] It is known that cell-mediated immunityonly works in cooperation with the humoral immunity andwith the participation of the complement system Actuallythere is little information regarding these issues and activityof phagocytes in children malaria in the scientific literatureand the results of individual fragmentary studies are highlycontroversial and apply only to adult patients The aim of thisstudy was to investigate the mechanisms of immunologicalresponse in children with P falciparummalaria
2 Materials and Methods
We examined 124 patients with P falciparum malaria at theage of 6 months up to 14 years that were hospitalized inClinical InfectiousDiseasesHospital inDushanbe city as wellas at the Khatlon regional hospital in the period 2000-2007 Inmost cases they were school-age children (56)The analysisof morbidity revealed seasonality the peak incidence wasrecorded in July-October According to ldquoMalaria Case Man-agement Protocol of Tajikistan Republicrdquo 39 patients werediagnosed with light form of the disease 60mdashmoderate formand 25mdashsevere form After patientsrsquo examination the lightand moderate forms of the disease were dominating (34and 476 respectively) mainly due to their early admissionClinical manifestations of malaria were dependent on theage of children in very young children early symptoms ofintoxication prevailed dyspepsia diarrhea and fever it hadan intermittent character and there was no typical malarialparoxysm Malaria symptoms in children of older age groupsdid not differ much from the adults
The verification of the diagnosis was based on clinicalepidemiological data and the results of blood microscopy Inall patients along with the standard clinical and laboratorytests a number of indicators of the immune status wereperformed that include the T-immunity the content ofserum immunoglobulins of three main classes the level ofcirculating immune complexes (CIC) C3 complement andthe concentration of key serum cytokines that have beenstudied in the dynamics of infectious process (at the peak ofthe disease early and late periods of recovery) and dependingon the severity of the disease
The criteria for the severity of the disease are heightand duration of fever severity of symptoms of intoxicationlesions of other organs and systems hepatosplenomegalyparasitemia and frequency and duration of malarial parox-ysm In assessing the severity of P falciparum malaria prac-titioners are guided byWHO recommendations (2006 2010)
Journal of Tropical Medicine 3
and ICD-10 (International Classification of Diseases) whichdistinguish uncomplicated severe and complicated malariaIn the NIS countries including the Republic of Tajikistan inthe classification of P falciparummalaria the only differencefrom the WHO classification is that in uncomplicated formthere are two degrees of severity light (low-symptomatic)andmedium (clinically expressed withmoderate intoxicationsyndrome mild anemia and hepatosplenomegaly) the restcomplies with the recommendations of WHO and ICD-10
For quantification of CD4+ CD8+ and B lymphocytes(CD20+) the commercial kits of monoclonal antibodies ofthe company ORTON (USA) were used and the determina-tion was performed on the cytometry counter (FACSbAN)Serum levels of immunoglobulin classes A M G andthe third component of complement were determined byradial immunodiffusion in gel circulating concentrationsof immune complexes (CIC) in the blood serum wereperformed in the reaction with polyethylene glycol
The study of cytokines in pgml was determined bythe competitive and enzyme-linked immunosorbent assay(ELISA) using commercial ldquoProConrdquo companyrsquos test systemsSaint Petersburg measurement of the optical density wasperformed on Multiscan MCC-340 ldquoLabsystemsrdquo (Finland)IFN-g was also tested by ELISA using Biosource test system(USA)
Statistical analysis was performed by the method ofvariation statistics on the PC using the application packageldquoStatistica 60rdquo (StatSoft Inc USA) for the absolute valuesof calculated average values and the error of the mean(mplusmnm) Pair comparisons of absolute values were carriedout according to the Mann-Whitney U-test which is usedto compare independent samples and Wilcoxon T-test fordependent samples The differences were statistically consid-ered significant at plt005
3 Results
The study of the immune response dynamics in P falci-parum malaria revealed disturbances of immunoregulatorymechanisms in the different periods of the disease and theirseverity depends on the severity of the disease The studyof cellular and humoral protective factors revealed that inpatients with mild form of P falciparum malaria indicatorsof cellular immunity at all stages of the disease did not differfrom those of the control group (546 plusmn 80 567 plusmn 85 and591 plusmn 100 respectively in the peak of disease during theearly and late recovery) (pgt 005) but the immunoregulatoryindex (IRI) in the peak of disease was reduced (20) Lowproduction of early antibodies (IgMmdash105 plusmn 09 versus 18 plusmn07 gl in control) in the early stages of the disease contributedto the reduction of the index of antibody activity (IAA) Highlevels of IgG (136 plusmn 07 against 112 plusmn 035 gl in controlP lt001) and CIC (24 plusmn 013 vs 084 plusmn 004 gl in thecontrol p lt0001) decreased gradually toward recovery butalso at late stage of recovery in the absence of parasites inthe peripheral blood are still significantly higher than thecontrol level (098 plusmn 004 gl) In the peak of the light form oftropical malaria in the composition of CIC immunoglobulinG was dominated which apparently was associated with
a more active IgG binding of the antigenic determinantsof Plasmodium falciparum This was also reflected in thesignificant increase in the level of the absolute content of Bcells in the period of the disease (307 plusmn 60 vs 139 plusmn 35p lt005) which is obviously connected with the expressedneoantigenic stimulation of B cell part of the immune systemThe values of C3 blood serum in all periods of the diseaseremained normal The dynamics of cellular and humoralimmunity in patients with mild form of P falciparummalariashowed a weak immune restructuring of the organism dueto brief irritation of the immune system by antigens of theparasite Obviously it is linked to more frequent occurrenceof relapses and repeated cases of the disease after sufferingfrommild form of P falciparummalaria (773)
Changes of the immune status in the moderate formof P falciparum malaria were significantly different fromthose of the light form The most pronounced changes wereobserved at the peak of decease and early recovery theabsolute number of T-lymphocytes was significantly reduced(431 plusmn 64 and 494 plusmn 70 respectively versus 667 plusmn 47 incontrol p lt0001) and CD4 + (186 plusmn 50 and 281 plusmn 63 gl vs463 plusmn 50 in control p lt001) In these stages of the diseasethe activation of humoral immunity was observed which wasexpressed in a significant increase in IgM concentrations of18 plusmn 03 and 16 plusmn 058 gl against 102 plusmn 007 gl in thecontrol p lt001 and the IAA index of 24 In the peak ofmoderate form in the composition of the CIC large-sizedcomplexes containing IgM were dominated Active immunerestructuring determines a favorable outcome of the diseasethat is evidenced by the absence of cases of relapses and theformation of asymptomatic carriage with moderate course ofillness
Severe form of P falciparum malaria was characterizedby almost the same quantitative and qualitative changes ofcellular immunity as well as in cases of moderate flow butthere was a significant reduction of IRI during the crisisperiod (196 versus 277 in the control p lt001) Indicatorsof humoral immunity did not differ from those of healthychildren indicating the low production of antibodies M andG class with this form of disease severity In the peak of thedisease a significant increase of CIC was observed (243 plusmn 02vs 084 plusmn 004 gl p lt0001) and as in the moderate formimmune complexes of large dimensions prevailed in theircomposition containing IgM The obvious depression of cellhumoral protective factors and of high CIC values requiresimmunotherapy As a result studies have found a significantincrease of proinflammatory cytokines in almost all periodsof the disease with a tendency of reduced rates in the periodof late recovery but not reaching the control values (p lt005)(Table 1)
An exception is the content of IFN-120574 in the peakof disease it was found at low level (p lt005) with anincrease in value in the period of recovery which is a majorfactor activating macrophages and promoting more effectivedestruction of intracellular pathogens The findings suggesta substantial suppression of specific antiparasitic immunityin P falciparum malaria The level of the studied cytokinescorrelated with the severity of the disease the highest rates
4 Journal of Tropical Medicine
Table 1 Contents of plasma cytokines in Plasmodium falciparum malaria in children (Pgml)
Periods of disease n TNF-120572 IL-1120573 IL-6 IFN-120574 IL-2 IL-4Peak of diseaseI 24 428 plusmn 17lowast lowast lowast 616 plusmn 58lowast lowast lowast 764 plusmn 25lowast lowast lowast 93 plusmn 06 203 plusmn 23 1358plusmn71lowast lowast lowastII 24 1021plusmn 156lowast lowast lowast 1202 plusmn107lowast lowast lowast 1081 plusmn 62lowast lowast lowast 68 plusmn 04lowast 184 plusmn 11 2339plusmn 224lowast lowast lowastIII 24 3329plusmn489lowast lowast lowast 4668 plusmn514lowast lowast lowast 3062 plusmn 71lowast lowast lowast 54 plusmn 01lowast 135 plusmn 16 4585 plusmn167lowast lowast lowastAll patients 1505 plusmn 63lowast lowast lowast 2162 plusmn401lowast lowast lowast 1606 plusmn 34lowast lowast lowast 72 plusmn 02lowast 163 plusmn 17 2711 plusmn 94lowast lowast lowastEarly recoveryI 24 294 plusmn 12lowastlowast 433 plusmn 12lowast lowast lowast 492 plusmn 17lowast lowast lowast 104 plusmn 11 1084 plusmn132lowast lowast lowast 466 plusmn 39lowast lowast lowastII 24 402 plusmn 24lowastlowast 888 plusmn 26lowast lowast lowast 581 plusmn 35lowast lowast lowast 129 plusmn 15 829 plusmn 52lowast lowast lowast 721 plusmn 29lowast lowast lowastIII 24 1226 plusmn32lowast lowast lowast 1359 plusmn 47lowast lowast lowast 1024 plusmn 42lowast lowast lowast 121 plusmn 13 463 plusmn 37 lowast lowast lowast 2004 plusmn 34lowast lowast lowastAll patients 607 plusmn 21lowast lowast lowast 891 plusmn 87lowast lowast lowast 682 plusmn 23lowast lowast lowast 112 plusmn 12 722 plusmn 37lowast lowast lowast 1046 plusmn 57lowast lowast lowastLate recoveryI 18 209 plusmn 11 249 plusmn 22 312 plusmn 11 147 plusmn 13 2022 plusmn115lowast lowast lowast 324 plusmn 42lowastlowastII 20 223 plusmn 14 306 plusmn 16 394 plusmn 22 189 plusmn 22lowastlowast 1885plusmn123lowast lowast lowast 391 plusmn 16lowast lowast lowastIII 17 291 plusmn 28lowastlowast 398 plusmn 32lowast 465 plusmn 18lowast 176 plusmn 11lowastlowast 244 plusmn 19lowast lowast lowast 443 plusmn 29lowast lowast lowastAll patients 234 plusmn 13 314 plusmn 25lowast 388 plusmn 15lowast 168 plusmn 13lowast 1304 plusmn 96lowast lowast lowast 326 plusmn 22lowast lowast lowastControl 30 203 plusmn 11 244 plusmn 35 323 plusmn 041 1131 plusmn 07 122 plusmn 003 208 plusmn 022Note I a mild form II moderate form and III severe formlowastp lt005 lowastlowastp lt001 lowast lowast lowastp lt0001mdashsignificant differences compared with the control
were found in severe tropical malaria perhaps due to exces-sive activity of monocytesmacrophages responsible for theproduction of proinflammatory components of regulationas well as the release of reactive radicals The involvementof the monocyte-macrophage cells followed by the activeelaboration of the whole complex of biologically activesubstances contributing to cellular and circulatory disorderscan be traced withmoderate and severe P falciparummalariait is probably one of the pathological links of severe anemiabrain damage and nonspecific inflammation In consideringthe role of cytokines in the development of these or otherdisturbances one has to take into account the diversity oftheir spectrum of biological activity [6 7] It is known thatIFN-120574 naturally called immune interferon also has the abilityto suppress the proliferation of erythrocyte germ cells [3] Ofparticular interest is the study of proinflammatory cytokineantagonistsmdashIL-4 produced by Th2-cells The concentrationof this cytokine was significantly greater than control valuesin all periods of the disease the highest content was duringthe peak of P falciparum malaria (p lt001) suggesting animbalance of immunoregulatory mechanisms of Th2 typeThe predominance of Th2-pathway immune response deter-mines the suppression of cell-mediated immunity in the earlystages of the disease In addition the imbalance of cell-cell interactions and the reduction of immunomodulatoryproperties indicate failure of stimulation of own adequateimmune response as a reaction to malarial infection causedby P falciparum Although replicative P falciparum malariapathogen activity must be an inductor of interferon produc-tion it does not happen due to lack of effective immunolog-ical response to various stimuli including proinflammatorycytokines pathogen itself and its products of metabolismThis may lead to severe course with the development of seri-ous complications and the concentration of these cytokines
may be a predictor of it It should be noted that imbalanceof immune mechanisms is short and in the recovery periodthe dominance of Th1-type immune response is observedthat is induced by IFN-120574 production as well as lower levelsof proinflammatory cytokines that exacerbate cardiovascularand autoimmune processes Increasing concentrations of IL-4 have compensatory rather than active counterregulatorycharacter to proinflammatory cytokines that implies morestabilizing function in the inflammatory response Togetherthese identified features demonstrate the complexity anddiversity of processes of immune cytokines in P falciparummalaria
4 Discussion
The Plasmodium falciparum malaria is characterized bydepression of T cell immunity the extent of which dependedon the severity of malaria infection Please note the lowlevels of T-lymphocytes in moderate and severe forms of thedisease a significant reduction of T helpers relatively intactlevel of T suppressors and suppression of humoral immu-nity These changes are most pronounced in the moderateform of the disease moreover they are accompanied by asubstantial increase in the functional activity of cells havingkiller cytotoxic activity The study of cellular and humoralimmunity in patients with tropical malaria is an obviousadditional criterion in assessing the severity of infection Theimbalance of cytokine profile in P falciparum malaria is animportant pathogenetic factor in the development of severeand recurrent forms of the disease since the formation of adefective immune response to parasitic antigens contributesto adverse outcomes
In parallel and at the same time the above-mentionedindicators of the immune status and cytokine profile were
Journal of Tropical Medicine 5
0
50
100
150
200
315207
204
1505
607234
203
Pgml
Stage of disease
Note 1 ndash Peak of disease 2 ndash Early recovery 3 ndash Late recovery 4 ndash Сontrol
TNF-
P vivaxP falciparumcontrol
Figure 2 Dynamics of indicators of proinflammatory cytokines(TNF-120572) in children with malaria
0
100
200
300
345 283 267
2162
891314
244
Pgml
Stage of diseaseNote 1 ndash Peak of disease 2 ndash Early recovery 3 ndash Late recovery 4 ndash
control
IL-1
P vivaxP falciparumcontrl
Figure 3Dynamics of indicators of proinflammatory cytokines (IL-1120573) in children with malaria
carried out in children with P vivax (mean severityndash59patients severendash21) It was found that the nature of immuno-logical disorders in the tertian malaria in contrast to the Pfalciparum malaria is due to the high level of CIC in theircomposition of IgM in combination with a decrease in theabsolute number of peripheral blood lymphocytes Immuno-logical reactions are not prolonged in time and reflect theadequacy of the immune response The tertian malaria ischaracterized by the predominance of Th1-pathway immuneresponse which contributes to the earliest elimination ofinfected red blood cells and pathogens from the body andthe adequacy of the mechanisms of immunological responseIn P falciparummalaria as noted above Th2-pathway of theimmune response prevails in the early stages of the diseasewith a switch in the period of convalescence toTh1-characterof lymphocytic reactions (Figures 2ndash7)The persistent imbal-ance in theTh1Th2 cytokine systemobserved inP falciparummalaria is a predictor of the severe complicated course ofthe disease since the formation of an inadequate immuneresponse to parasitic antigens contributes to the developmentof adverse outcomes
The study of cellular and humoral immunity in patientswith P falciparummalaria is an objective additional criterionin assessing the severity of the infectious process
050
100150200
455367 331
1606
682388
323
Pgml
Stage of diseaseNote 1 ndash Peak of disease 2 ndash Early recovery 3 ndash Late recovery 4 ndash control
IL-6
P vivaxP falciparumcontrol
Figure 4 Dynamics of indicators of proinflammatory cytokines(IL-6) in children with malaria
16 164129
72112
168
113
0
5
10
15
20
25
30
35Pgml
Stage of diseaseNote 1 ndash Peak of disease 2 ndash Early recovery 3 ndash Late recovery 4 ndash control
INF-
controlP falciparumP vivax
Figure 5 Dynamics of indicators of proinflammatory cytokinesantagonists (IFN-120574) in children with malaria
0
100
200
300
400 3764
1328
518163 722 1304122
Pgml
Stage of diseaseNote 1 ndash Peak of disease 2 ndash Early recovery 3 ndash Late recovery 4 ndash control
IL-2
P vivaxP falciparumcontrol
Figure 6 Dynamics of indicators of proinflammatory cytokinesantagonists (IL-2) in children with malaria
6 Journal of Tropical Medicine
050
100150200250300
208
1142
296
2711
1046
326 208
Pgml
Stage of diseaseNote 1 ndash Peak of disease 2 ndash Early recovery 3 ndash Late recovery 4 ndash control
IL-4
P vivaxP falciparumcontrol
Figure 7 Dynamics of indicators of proinflammatory cytokinesantagonists (IL-4) in children with malaria
5 Conclusions
Plasmodium falciparummalaria was characterized by depres-sion of cellular and humoral immunity the degree of whichdepended on the severity of the pathological process Pleasepay attention to the low rates of T-lymphocytes in moderateand severe forms of the disease and the significant decreasein T-lymphocytes-helpers with a relatively stable level of T-lymphocytes-suppressors The most pronounced changes inthe moderate form of the disease are accompanied by asignificant increase in the functional activity of cells withkiller cytotoxic activity and activation of humoral protectionfactors
Data Availability
The data used to support the findings of this study areavailable from the corresponding author upon request
Conflicts of Interest
The authors declare that they have no conflicts of interestregarding the publication of this paper
Authorsrsquo Contributions
Nighina M Khodzhaeva developed the study of protocoland wrote part of the manuscript Alla M Baranova partic-ipated in the epidemiological and clinical diagnoses and dataanalysis Anatoly K Tokmalaev developed the protocol andwrote part of the manuscript All authors approved the finalmanuscript
References
[1] D S Saiburhonov S S Karimov D S Kadamov and A MBaranova ldquoDistribution of Plasmodium falciparum malaria inthe Republic of Tajikistan 1994-2008rdquo Meditsinskaya Parazi-tologiya (Mosk) vol 1 pp 3ndash6 2015 (Russian)
[2] Malaria in the WHO European Region on the Road to Elim-ination 2000-2015 vol 40 World Health Organization 2018
httpwwweurowhointenhealth-topicscommunicable-diseas-esvector-borne-and-parasitic-diseasespublications2018ma-laria-in-the-who-european-region-on-the-road-to-elimination-20002015-summary-2018
[3] V P Sergiev N D Yushchuk U Y Vengerow and V DZavoykin ldquoTropical diseaserdquoManual for Physicians PublishingHouse BINOM vol 640 2015 (Russian)
[4] L Schofield and G E Grau ldquoImmunological processes inmalaria pathogenesisrdquo Nature Reviews Immunology vol 5 no9 pp 722ndash735 2005
[5] M Y Boiro S Boumbali O K Konstantinov S KalivoguiM Koulibali and A S Bah ldquoIndices of immune responsein patients of P falciparum malaria in Republic of GuineardquoInfection and Immunity (Russian Journal Infektsiya i Immunitet)vol 6 no 2 pp 151ndash156 2016 (Russian)
[6] E M Riley S Wahl D J Perkins and L Schofield ldquoRegulatingimmunity to malariardquo Parasite Immunology vol 28 no 1-2 pp35ndash49 2006
[7] S Blair Trujillo G Alvarez Sanchez A Villa Restrepo JCarmona Fonseca and L Rıos Osorio ldquoNutritional status andimmunoglobulin and cytokine concentrations in children withmalariardquo Anales de Pediatrıa (Barcelona Spain) vol 58 no 5pp 418ndash424 2003
[8] N M Khodzhaeva N F Fayzulloev and A K TokmalaevldquoCytokine profile of children to malariardquoMeditsinskaya Parazi-tologiya vol 4 pp 22ndash26 2008 (Russian)
[9] A P F do Rosario T Lamb P Spence et al ldquoIL-27 promotes IL-10 production by effectorTh1CD4+T cells a criticalmechanismfor protection from severe immunopathology during malariainfectionrdquoThe Journal of Immunology vol 188 no 3 pp 1178ndash1190 2012
[10] E B Belachew ldquoImmune response and evasion mechanismsof plasmodium falciparum parasitesrdquo Journal of ImmunologyResearch vol 2018 Article ID 6529681 6 pages 2018
[11] B Dinko and G Pradel ldquoImmune evasion by Plasmodiumfalciparum parasites converting a host protection mechanismfor the parasite1015840s benefitrdquo Advances in Infectious Diseases vol6 no 2 pp 82ndash95 2016
[12] P S Gomes J Bhardwaj J Rivera-Correa C G Freire-De-Lima and A Morrot ldquoImmune escape strategies of malariaparasitesrdquo Frontiers in Microbiology vol 7 article no 1617 2016
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom
2 Journal of Tropical Medicine
1
10
100
1000
10000
100000
P vivax (autochthonous cases)P falciparum (autochthonous cases)
1990
1992
1994 19
9619
9820
0020
02 2004
2006
2008 20
10 2012
2014
Figure 1 Numbers of malaria cases in Tajikistan 1990-2014 Source Republican Tropical Diseases Center Ministry of Health Tajikistan
more than one million of people including 150000 schoolchildren were subjected to health education activities Intotal 305 laboratory technicians 1550 physicians epidemiol-ogists and entomologists benefitted frommalaria training Anumber of Afghani health workers were trained in Tajikistanin antimalarial measures in the border areas The NationalControl Programme was successful and transmission of Pfalciparum was interrupted in 2009 (Figure 1) [2]
11 Pathogenesis of Malaria Pathogenic mechanisms ofmalaria infection are associated with the massive destructionof Plasmodium infected red blood cells and the cascadedevelopment of immunological reactions [3 4] The varietyand variability of antigens of P falciparum makes the patho-genesis of P falciparum malaria very diverse and complexSevere course of infection and systemic organ lesions aremore frequently observed in P falciparum malaria Defectsof immune-regulatory mechanisms of patient response maylead to the development of disease recurrence and a par-asitical asymptomatic carrier state [5ndash7] Many aspects ofthe pathogenesis of malaria still remain poorly understoodin particular the features of the development of specificimmunity in children and associated with them the flow ofmalaria infection and disease outcomes From the immunecells the most antimalarial activity has been shown bymacrophages T cells and a number of cytokines secretedby them [8ndash12] It is known that cell-mediated immunityonly works in cooperation with the humoral immunity andwith the participation of the complement system Actuallythere is little information regarding these issues and activityof phagocytes in children malaria in the scientific literatureand the results of individual fragmentary studies are highlycontroversial and apply only to adult patients The aim of thisstudy was to investigate the mechanisms of immunologicalresponse in children with P falciparummalaria
2 Materials and Methods
We examined 124 patients with P falciparum malaria at theage of 6 months up to 14 years that were hospitalized inClinical InfectiousDiseasesHospital inDushanbe city as wellas at the Khatlon regional hospital in the period 2000-2007 Inmost cases they were school-age children (56)The analysisof morbidity revealed seasonality the peak incidence wasrecorded in July-October According to ldquoMalaria Case Man-agement Protocol of Tajikistan Republicrdquo 39 patients werediagnosed with light form of the disease 60mdashmoderate formand 25mdashsevere form After patientsrsquo examination the lightand moderate forms of the disease were dominating (34and 476 respectively) mainly due to their early admissionClinical manifestations of malaria were dependent on theage of children in very young children early symptoms ofintoxication prevailed dyspepsia diarrhea and fever it hadan intermittent character and there was no typical malarialparoxysm Malaria symptoms in children of older age groupsdid not differ much from the adults
The verification of the diagnosis was based on clinicalepidemiological data and the results of blood microscopy Inall patients along with the standard clinical and laboratorytests a number of indicators of the immune status wereperformed that include the T-immunity the content ofserum immunoglobulins of three main classes the level ofcirculating immune complexes (CIC) C3 complement andthe concentration of key serum cytokines that have beenstudied in the dynamics of infectious process (at the peak ofthe disease early and late periods of recovery) and dependingon the severity of the disease
The criteria for the severity of the disease are heightand duration of fever severity of symptoms of intoxicationlesions of other organs and systems hepatosplenomegalyparasitemia and frequency and duration of malarial parox-ysm In assessing the severity of P falciparum malaria prac-titioners are guided byWHO recommendations (2006 2010)
Journal of Tropical Medicine 3
and ICD-10 (International Classification of Diseases) whichdistinguish uncomplicated severe and complicated malariaIn the NIS countries including the Republic of Tajikistan inthe classification of P falciparummalaria the only differencefrom the WHO classification is that in uncomplicated formthere are two degrees of severity light (low-symptomatic)andmedium (clinically expressed withmoderate intoxicationsyndrome mild anemia and hepatosplenomegaly) the restcomplies with the recommendations of WHO and ICD-10
For quantification of CD4+ CD8+ and B lymphocytes(CD20+) the commercial kits of monoclonal antibodies ofthe company ORTON (USA) were used and the determina-tion was performed on the cytometry counter (FACSbAN)Serum levels of immunoglobulin classes A M G andthe third component of complement were determined byradial immunodiffusion in gel circulating concentrationsof immune complexes (CIC) in the blood serum wereperformed in the reaction with polyethylene glycol
The study of cytokines in pgml was determined bythe competitive and enzyme-linked immunosorbent assay(ELISA) using commercial ldquoProConrdquo companyrsquos test systemsSaint Petersburg measurement of the optical density wasperformed on Multiscan MCC-340 ldquoLabsystemsrdquo (Finland)IFN-g was also tested by ELISA using Biosource test system(USA)
Statistical analysis was performed by the method ofvariation statistics on the PC using the application packageldquoStatistica 60rdquo (StatSoft Inc USA) for the absolute valuesof calculated average values and the error of the mean(mplusmnm) Pair comparisons of absolute values were carriedout according to the Mann-Whitney U-test which is usedto compare independent samples and Wilcoxon T-test fordependent samples The differences were statistically consid-ered significant at plt005
3 Results
The study of the immune response dynamics in P falci-parum malaria revealed disturbances of immunoregulatorymechanisms in the different periods of the disease and theirseverity depends on the severity of the disease The studyof cellular and humoral protective factors revealed that inpatients with mild form of P falciparum malaria indicatorsof cellular immunity at all stages of the disease did not differfrom those of the control group (546 plusmn 80 567 plusmn 85 and591 plusmn 100 respectively in the peak of disease during theearly and late recovery) (pgt 005) but the immunoregulatoryindex (IRI) in the peak of disease was reduced (20) Lowproduction of early antibodies (IgMmdash105 plusmn 09 versus 18 plusmn07 gl in control) in the early stages of the disease contributedto the reduction of the index of antibody activity (IAA) Highlevels of IgG (136 plusmn 07 against 112 plusmn 035 gl in controlP lt001) and CIC (24 plusmn 013 vs 084 plusmn 004 gl in thecontrol p lt0001) decreased gradually toward recovery butalso at late stage of recovery in the absence of parasites inthe peripheral blood are still significantly higher than thecontrol level (098 plusmn 004 gl) In the peak of the light form oftropical malaria in the composition of CIC immunoglobulinG was dominated which apparently was associated with
a more active IgG binding of the antigenic determinantsof Plasmodium falciparum This was also reflected in thesignificant increase in the level of the absolute content of Bcells in the period of the disease (307 plusmn 60 vs 139 plusmn 35p lt005) which is obviously connected with the expressedneoantigenic stimulation of B cell part of the immune systemThe values of C3 blood serum in all periods of the diseaseremained normal The dynamics of cellular and humoralimmunity in patients with mild form of P falciparummalariashowed a weak immune restructuring of the organism dueto brief irritation of the immune system by antigens of theparasite Obviously it is linked to more frequent occurrenceof relapses and repeated cases of the disease after sufferingfrommild form of P falciparummalaria (773)
Changes of the immune status in the moderate formof P falciparum malaria were significantly different fromthose of the light form The most pronounced changes wereobserved at the peak of decease and early recovery theabsolute number of T-lymphocytes was significantly reduced(431 plusmn 64 and 494 plusmn 70 respectively versus 667 plusmn 47 incontrol p lt0001) and CD4 + (186 plusmn 50 and 281 plusmn 63 gl vs463 plusmn 50 in control p lt001) In these stages of the diseasethe activation of humoral immunity was observed which wasexpressed in a significant increase in IgM concentrations of18 plusmn 03 and 16 plusmn 058 gl against 102 plusmn 007 gl in thecontrol p lt001 and the IAA index of 24 In the peak ofmoderate form in the composition of the CIC large-sizedcomplexes containing IgM were dominated Active immunerestructuring determines a favorable outcome of the diseasethat is evidenced by the absence of cases of relapses and theformation of asymptomatic carriage with moderate course ofillness
Severe form of P falciparum malaria was characterizedby almost the same quantitative and qualitative changes ofcellular immunity as well as in cases of moderate flow butthere was a significant reduction of IRI during the crisisperiod (196 versus 277 in the control p lt001) Indicatorsof humoral immunity did not differ from those of healthychildren indicating the low production of antibodies M andG class with this form of disease severity In the peak of thedisease a significant increase of CIC was observed (243 plusmn 02vs 084 plusmn 004 gl p lt0001) and as in the moderate formimmune complexes of large dimensions prevailed in theircomposition containing IgM The obvious depression of cellhumoral protective factors and of high CIC values requiresimmunotherapy As a result studies have found a significantincrease of proinflammatory cytokines in almost all periodsof the disease with a tendency of reduced rates in the periodof late recovery but not reaching the control values (p lt005)(Table 1)
An exception is the content of IFN-120574 in the peakof disease it was found at low level (p lt005) with anincrease in value in the period of recovery which is a majorfactor activating macrophages and promoting more effectivedestruction of intracellular pathogens The findings suggesta substantial suppression of specific antiparasitic immunityin P falciparum malaria The level of the studied cytokinescorrelated with the severity of the disease the highest rates
4 Journal of Tropical Medicine
Table 1 Contents of plasma cytokines in Plasmodium falciparum malaria in children (Pgml)
Periods of disease n TNF-120572 IL-1120573 IL-6 IFN-120574 IL-2 IL-4Peak of diseaseI 24 428 plusmn 17lowast lowast lowast 616 plusmn 58lowast lowast lowast 764 plusmn 25lowast lowast lowast 93 plusmn 06 203 plusmn 23 1358plusmn71lowast lowast lowastII 24 1021plusmn 156lowast lowast lowast 1202 plusmn107lowast lowast lowast 1081 plusmn 62lowast lowast lowast 68 plusmn 04lowast 184 plusmn 11 2339plusmn 224lowast lowast lowastIII 24 3329plusmn489lowast lowast lowast 4668 plusmn514lowast lowast lowast 3062 plusmn 71lowast lowast lowast 54 plusmn 01lowast 135 plusmn 16 4585 plusmn167lowast lowast lowastAll patients 1505 plusmn 63lowast lowast lowast 2162 plusmn401lowast lowast lowast 1606 plusmn 34lowast lowast lowast 72 plusmn 02lowast 163 plusmn 17 2711 plusmn 94lowast lowast lowastEarly recoveryI 24 294 plusmn 12lowastlowast 433 plusmn 12lowast lowast lowast 492 plusmn 17lowast lowast lowast 104 plusmn 11 1084 plusmn132lowast lowast lowast 466 plusmn 39lowast lowast lowastII 24 402 plusmn 24lowastlowast 888 plusmn 26lowast lowast lowast 581 plusmn 35lowast lowast lowast 129 plusmn 15 829 plusmn 52lowast lowast lowast 721 plusmn 29lowast lowast lowastIII 24 1226 plusmn32lowast lowast lowast 1359 plusmn 47lowast lowast lowast 1024 plusmn 42lowast lowast lowast 121 plusmn 13 463 plusmn 37 lowast lowast lowast 2004 plusmn 34lowast lowast lowastAll patients 607 plusmn 21lowast lowast lowast 891 plusmn 87lowast lowast lowast 682 plusmn 23lowast lowast lowast 112 plusmn 12 722 plusmn 37lowast lowast lowast 1046 plusmn 57lowast lowast lowastLate recoveryI 18 209 plusmn 11 249 plusmn 22 312 plusmn 11 147 plusmn 13 2022 plusmn115lowast lowast lowast 324 plusmn 42lowastlowastII 20 223 plusmn 14 306 plusmn 16 394 plusmn 22 189 plusmn 22lowastlowast 1885plusmn123lowast lowast lowast 391 plusmn 16lowast lowast lowastIII 17 291 plusmn 28lowastlowast 398 plusmn 32lowast 465 plusmn 18lowast 176 plusmn 11lowastlowast 244 plusmn 19lowast lowast lowast 443 plusmn 29lowast lowast lowastAll patients 234 plusmn 13 314 plusmn 25lowast 388 plusmn 15lowast 168 plusmn 13lowast 1304 plusmn 96lowast lowast lowast 326 plusmn 22lowast lowast lowastControl 30 203 plusmn 11 244 plusmn 35 323 plusmn 041 1131 plusmn 07 122 plusmn 003 208 plusmn 022Note I a mild form II moderate form and III severe formlowastp lt005 lowastlowastp lt001 lowast lowast lowastp lt0001mdashsignificant differences compared with the control
were found in severe tropical malaria perhaps due to exces-sive activity of monocytesmacrophages responsible for theproduction of proinflammatory components of regulationas well as the release of reactive radicals The involvementof the monocyte-macrophage cells followed by the activeelaboration of the whole complex of biologically activesubstances contributing to cellular and circulatory disorderscan be traced withmoderate and severe P falciparummalariait is probably one of the pathological links of severe anemiabrain damage and nonspecific inflammation In consideringthe role of cytokines in the development of these or otherdisturbances one has to take into account the diversity oftheir spectrum of biological activity [6 7] It is known thatIFN-120574 naturally called immune interferon also has the abilityto suppress the proliferation of erythrocyte germ cells [3] Ofparticular interest is the study of proinflammatory cytokineantagonistsmdashIL-4 produced by Th2-cells The concentrationof this cytokine was significantly greater than control valuesin all periods of the disease the highest content was duringthe peak of P falciparum malaria (p lt001) suggesting animbalance of immunoregulatory mechanisms of Th2 typeThe predominance of Th2-pathway immune response deter-mines the suppression of cell-mediated immunity in the earlystages of the disease In addition the imbalance of cell-cell interactions and the reduction of immunomodulatoryproperties indicate failure of stimulation of own adequateimmune response as a reaction to malarial infection causedby P falciparum Although replicative P falciparum malariapathogen activity must be an inductor of interferon produc-tion it does not happen due to lack of effective immunolog-ical response to various stimuli including proinflammatorycytokines pathogen itself and its products of metabolismThis may lead to severe course with the development of seri-ous complications and the concentration of these cytokines
may be a predictor of it It should be noted that imbalanceof immune mechanisms is short and in the recovery periodthe dominance of Th1-type immune response is observedthat is induced by IFN-120574 production as well as lower levelsof proinflammatory cytokines that exacerbate cardiovascularand autoimmune processes Increasing concentrations of IL-4 have compensatory rather than active counterregulatorycharacter to proinflammatory cytokines that implies morestabilizing function in the inflammatory response Togetherthese identified features demonstrate the complexity anddiversity of processes of immune cytokines in P falciparummalaria
4 Discussion
The Plasmodium falciparum malaria is characterized bydepression of T cell immunity the extent of which dependedon the severity of malaria infection Please note the lowlevels of T-lymphocytes in moderate and severe forms of thedisease a significant reduction of T helpers relatively intactlevel of T suppressors and suppression of humoral immu-nity These changes are most pronounced in the moderateform of the disease moreover they are accompanied by asubstantial increase in the functional activity of cells havingkiller cytotoxic activity The study of cellular and humoralimmunity in patients with tropical malaria is an obviousadditional criterion in assessing the severity of infection Theimbalance of cytokine profile in P falciparum malaria is animportant pathogenetic factor in the development of severeand recurrent forms of the disease since the formation of adefective immune response to parasitic antigens contributesto adverse outcomes
In parallel and at the same time the above-mentionedindicators of the immune status and cytokine profile were
Journal of Tropical Medicine 5
0
50
100
150
200
315207
204
1505
607234
203
Pgml
Stage of disease
Note 1 ndash Peak of disease 2 ndash Early recovery 3 ndash Late recovery 4 ndash Сontrol
TNF-
P vivaxP falciparumcontrol
Figure 2 Dynamics of indicators of proinflammatory cytokines(TNF-120572) in children with malaria
0
100
200
300
345 283 267
2162
891314
244
Pgml
Stage of diseaseNote 1 ndash Peak of disease 2 ndash Early recovery 3 ndash Late recovery 4 ndash
control
IL-1
P vivaxP falciparumcontrl
Figure 3Dynamics of indicators of proinflammatory cytokines (IL-1120573) in children with malaria
carried out in children with P vivax (mean severityndash59patients severendash21) It was found that the nature of immuno-logical disorders in the tertian malaria in contrast to the Pfalciparum malaria is due to the high level of CIC in theircomposition of IgM in combination with a decrease in theabsolute number of peripheral blood lymphocytes Immuno-logical reactions are not prolonged in time and reflect theadequacy of the immune response The tertian malaria ischaracterized by the predominance of Th1-pathway immuneresponse which contributes to the earliest elimination ofinfected red blood cells and pathogens from the body andthe adequacy of the mechanisms of immunological responseIn P falciparummalaria as noted above Th2-pathway of theimmune response prevails in the early stages of the diseasewith a switch in the period of convalescence toTh1-characterof lymphocytic reactions (Figures 2ndash7)The persistent imbal-ance in theTh1Th2 cytokine systemobserved inP falciparummalaria is a predictor of the severe complicated course ofthe disease since the formation of an inadequate immuneresponse to parasitic antigens contributes to the developmentof adverse outcomes
The study of cellular and humoral immunity in patientswith P falciparummalaria is an objective additional criterionin assessing the severity of the infectious process
050
100150200
455367 331
1606
682388
323
Pgml
Stage of diseaseNote 1 ndash Peak of disease 2 ndash Early recovery 3 ndash Late recovery 4 ndash control
IL-6
P vivaxP falciparumcontrol
Figure 4 Dynamics of indicators of proinflammatory cytokines(IL-6) in children with malaria
16 164129
72112
168
113
0
5
10
15
20
25
30
35Pgml
Stage of diseaseNote 1 ndash Peak of disease 2 ndash Early recovery 3 ndash Late recovery 4 ndash control
INF-
controlP falciparumP vivax
Figure 5 Dynamics of indicators of proinflammatory cytokinesantagonists (IFN-120574) in children with malaria
0
100
200
300
400 3764
1328
518163 722 1304122
Pgml
Stage of diseaseNote 1 ndash Peak of disease 2 ndash Early recovery 3 ndash Late recovery 4 ndash control
IL-2
P vivaxP falciparumcontrol
Figure 6 Dynamics of indicators of proinflammatory cytokinesantagonists (IL-2) in children with malaria
6 Journal of Tropical Medicine
050
100150200250300
208
1142
296
2711
1046
326 208
Pgml
Stage of diseaseNote 1 ndash Peak of disease 2 ndash Early recovery 3 ndash Late recovery 4 ndash control
IL-4
P vivaxP falciparumcontrol
Figure 7 Dynamics of indicators of proinflammatory cytokinesantagonists (IL-4) in children with malaria
5 Conclusions
Plasmodium falciparummalaria was characterized by depres-sion of cellular and humoral immunity the degree of whichdepended on the severity of the pathological process Pleasepay attention to the low rates of T-lymphocytes in moderateand severe forms of the disease and the significant decreasein T-lymphocytes-helpers with a relatively stable level of T-lymphocytes-suppressors The most pronounced changes inthe moderate form of the disease are accompanied by asignificant increase in the functional activity of cells withkiller cytotoxic activity and activation of humoral protectionfactors
Data Availability
The data used to support the findings of this study areavailable from the corresponding author upon request
Conflicts of Interest
The authors declare that they have no conflicts of interestregarding the publication of this paper
Authorsrsquo Contributions
Nighina M Khodzhaeva developed the study of protocoland wrote part of the manuscript Alla M Baranova partic-ipated in the epidemiological and clinical diagnoses and dataanalysis Anatoly K Tokmalaev developed the protocol andwrote part of the manuscript All authors approved the finalmanuscript
References
[1] D S Saiburhonov S S Karimov D S Kadamov and A MBaranova ldquoDistribution of Plasmodium falciparum malaria inthe Republic of Tajikistan 1994-2008rdquo Meditsinskaya Parazi-tologiya (Mosk) vol 1 pp 3ndash6 2015 (Russian)
[2] Malaria in the WHO European Region on the Road to Elim-ination 2000-2015 vol 40 World Health Organization 2018
httpwwweurowhointenhealth-topicscommunicable-diseas-esvector-borne-and-parasitic-diseasespublications2018ma-laria-in-the-who-european-region-on-the-road-to-elimination-20002015-summary-2018
[3] V P Sergiev N D Yushchuk U Y Vengerow and V DZavoykin ldquoTropical diseaserdquoManual for Physicians PublishingHouse BINOM vol 640 2015 (Russian)
[4] L Schofield and G E Grau ldquoImmunological processes inmalaria pathogenesisrdquo Nature Reviews Immunology vol 5 no9 pp 722ndash735 2005
[5] M Y Boiro S Boumbali O K Konstantinov S KalivoguiM Koulibali and A S Bah ldquoIndices of immune responsein patients of P falciparum malaria in Republic of GuineardquoInfection and Immunity (Russian Journal Infektsiya i Immunitet)vol 6 no 2 pp 151ndash156 2016 (Russian)
[6] E M Riley S Wahl D J Perkins and L Schofield ldquoRegulatingimmunity to malariardquo Parasite Immunology vol 28 no 1-2 pp35ndash49 2006
[7] S Blair Trujillo G Alvarez Sanchez A Villa Restrepo JCarmona Fonseca and L Rıos Osorio ldquoNutritional status andimmunoglobulin and cytokine concentrations in children withmalariardquo Anales de Pediatrıa (Barcelona Spain) vol 58 no 5pp 418ndash424 2003
[8] N M Khodzhaeva N F Fayzulloev and A K TokmalaevldquoCytokine profile of children to malariardquoMeditsinskaya Parazi-tologiya vol 4 pp 22ndash26 2008 (Russian)
[9] A P F do Rosario T Lamb P Spence et al ldquoIL-27 promotes IL-10 production by effectorTh1CD4+T cells a criticalmechanismfor protection from severe immunopathology during malariainfectionrdquoThe Journal of Immunology vol 188 no 3 pp 1178ndash1190 2012
[10] E B Belachew ldquoImmune response and evasion mechanismsof plasmodium falciparum parasitesrdquo Journal of ImmunologyResearch vol 2018 Article ID 6529681 6 pages 2018
[11] B Dinko and G Pradel ldquoImmune evasion by Plasmodiumfalciparum parasites converting a host protection mechanismfor the parasite1015840s benefitrdquo Advances in Infectious Diseases vol6 no 2 pp 82ndash95 2016
[12] P S Gomes J Bhardwaj J Rivera-Correa C G Freire-De-Lima and A Morrot ldquoImmune escape strategies of malariaparasitesrdquo Frontiers in Microbiology vol 7 article no 1617 2016
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

Journal of Tropical Medicine 3
and ICD-10 (International Classification of Diseases) whichdistinguish uncomplicated severe and complicated malariaIn the NIS countries including the Republic of Tajikistan inthe classification of P falciparummalaria the only differencefrom the WHO classification is that in uncomplicated formthere are two degrees of severity light (low-symptomatic)andmedium (clinically expressed withmoderate intoxicationsyndrome mild anemia and hepatosplenomegaly) the restcomplies with the recommendations of WHO and ICD-10
For quantification of CD4+ CD8+ and B lymphocytes(CD20+) the commercial kits of monoclonal antibodies ofthe company ORTON (USA) were used and the determina-tion was performed on the cytometry counter (FACSbAN)Serum levels of immunoglobulin classes A M G andthe third component of complement were determined byradial immunodiffusion in gel circulating concentrationsof immune complexes (CIC) in the blood serum wereperformed in the reaction with polyethylene glycol
The study of cytokines in pgml was determined bythe competitive and enzyme-linked immunosorbent assay(ELISA) using commercial ldquoProConrdquo companyrsquos test systemsSaint Petersburg measurement of the optical density wasperformed on Multiscan MCC-340 ldquoLabsystemsrdquo (Finland)IFN-g was also tested by ELISA using Biosource test system(USA)
Statistical analysis was performed by the method ofvariation statistics on the PC using the application packageldquoStatistica 60rdquo (StatSoft Inc USA) for the absolute valuesof calculated average values and the error of the mean(mplusmnm) Pair comparisons of absolute values were carriedout according to the Mann-Whitney U-test which is usedto compare independent samples and Wilcoxon T-test fordependent samples The differences were statistically consid-ered significant at plt005
3 Results
The study of the immune response dynamics in P falci-parum malaria revealed disturbances of immunoregulatorymechanisms in the different periods of the disease and theirseverity depends on the severity of the disease The studyof cellular and humoral protective factors revealed that inpatients with mild form of P falciparum malaria indicatorsof cellular immunity at all stages of the disease did not differfrom those of the control group (546 plusmn 80 567 plusmn 85 and591 plusmn 100 respectively in the peak of disease during theearly and late recovery) (pgt 005) but the immunoregulatoryindex (IRI) in the peak of disease was reduced (20) Lowproduction of early antibodies (IgMmdash105 plusmn 09 versus 18 plusmn07 gl in control) in the early stages of the disease contributedto the reduction of the index of antibody activity (IAA) Highlevels of IgG (136 plusmn 07 against 112 plusmn 035 gl in controlP lt001) and CIC (24 plusmn 013 vs 084 plusmn 004 gl in thecontrol p lt0001) decreased gradually toward recovery butalso at late stage of recovery in the absence of parasites inthe peripheral blood are still significantly higher than thecontrol level (098 plusmn 004 gl) In the peak of the light form oftropical malaria in the composition of CIC immunoglobulinG was dominated which apparently was associated with
a more active IgG binding of the antigenic determinantsof Plasmodium falciparum This was also reflected in thesignificant increase in the level of the absolute content of Bcells in the period of the disease (307 plusmn 60 vs 139 plusmn 35p lt005) which is obviously connected with the expressedneoantigenic stimulation of B cell part of the immune systemThe values of C3 blood serum in all periods of the diseaseremained normal The dynamics of cellular and humoralimmunity in patients with mild form of P falciparummalariashowed a weak immune restructuring of the organism dueto brief irritation of the immune system by antigens of theparasite Obviously it is linked to more frequent occurrenceof relapses and repeated cases of the disease after sufferingfrommild form of P falciparummalaria (773)
Changes of the immune status in the moderate formof P falciparum malaria were significantly different fromthose of the light form The most pronounced changes wereobserved at the peak of decease and early recovery theabsolute number of T-lymphocytes was significantly reduced(431 plusmn 64 and 494 plusmn 70 respectively versus 667 plusmn 47 incontrol p lt0001) and CD4 + (186 plusmn 50 and 281 plusmn 63 gl vs463 plusmn 50 in control p lt001) In these stages of the diseasethe activation of humoral immunity was observed which wasexpressed in a significant increase in IgM concentrations of18 plusmn 03 and 16 plusmn 058 gl against 102 plusmn 007 gl in thecontrol p lt001 and the IAA index of 24 In the peak ofmoderate form in the composition of the CIC large-sizedcomplexes containing IgM were dominated Active immunerestructuring determines a favorable outcome of the diseasethat is evidenced by the absence of cases of relapses and theformation of asymptomatic carriage with moderate course ofillness
Severe form of P falciparum malaria was characterizedby almost the same quantitative and qualitative changes ofcellular immunity as well as in cases of moderate flow butthere was a significant reduction of IRI during the crisisperiod (196 versus 277 in the control p lt001) Indicatorsof humoral immunity did not differ from those of healthychildren indicating the low production of antibodies M andG class with this form of disease severity In the peak of thedisease a significant increase of CIC was observed (243 plusmn 02vs 084 plusmn 004 gl p lt0001) and as in the moderate formimmune complexes of large dimensions prevailed in theircomposition containing IgM The obvious depression of cellhumoral protective factors and of high CIC values requiresimmunotherapy As a result studies have found a significantincrease of proinflammatory cytokines in almost all periodsof the disease with a tendency of reduced rates in the periodof late recovery but not reaching the control values (p lt005)(Table 1)
An exception is the content of IFN-120574 in the peakof disease it was found at low level (p lt005) with anincrease in value in the period of recovery which is a majorfactor activating macrophages and promoting more effectivedestruction of intracellular pathogens The findings suggesta substantial suppression of specific antiparasitic immunityin P falciparum malaria The level of the studied cytokinescorrelated with the severity of the disease the highest rates
4 Journal of Tropical Medicine
Table 1 Contents of plasma cytokines in Plasmodium falciparum malaria in children (Pgml)
Periods of disease n TNF-120572 IL-1120573 IL-6 IFN-120574 IL-2 IL-4Peak of diseaseI 24 428 plusmn 17lowast lowast lowast 616 plusmn 58lowast lowast lowast 764 plusmn 25lowast lowast lowast 93 plusmn 06 203 plusmn 23 1358plusmn71lowast lowast lowastII 24 1021plusmn 156lowast lowast lowast 1202 plusmn107lowast lowast lowast 1081 plusmn 62lowast lowast lowast 68 plusmn 04lowast 184 plusmn 11 2339plusmn 224lowast lowast lowastIII 24 3329plusmn489lowast lowast lowast 4668 plusmn514lowast lowast lowast 3062 plusmn 71lowast lowast lowast 54 plusmn 01lowast 135 plusmn 16 4585 plusmn167lowast lowast lowastAll patients 1505 plusmn 63lowast lowast lowast 2162 plusmn401lowast lowast lowast 1606 plusmn 34lowast lowast lowast 72 plusmn 02lowast 163 plusmn 17 2711 plusmn 94lowast lowast lowastEarly recoveryI 24 294 plusmn 12lowastlowast 433 plusmn 12lowast lowast lowast 492 plusmn 17lowast lowast lowast 104 plusmn 11 1084 plusmn132lowast lowast lowast 466 plusmn 39lowast lowast lowastII 24 402 plusmn 24lowastlowast 888 plusmn 26lowast lowast lowast 581 plusmn 35lowast lowast lowast 129 plusmn 15 829 plusmn 52lowast lowast lowast 721 plusmn 29lowast lowast lowastIII 24 1226 plusmn32lowast lowast lowast 1359 plusmn 47lowast lowast lowast 1024 plusmn 42lowast lowast lowast 121 plusmn 13 463 plusmn 37 lowast lowast lowast 2004 plusmn 34lowast lowast lowastAll patients 607 plusmn 21lowast lowast lowast 891 plusmn 87lowast lowast lowast 682 plusmn 23lowast lowast lowast 112 plusmn 12 722 plusmn 37lowast lowast lowast 1046 plusmn 57lowast lowast lowastLate recoveryI 18 209 plusmn 11 249 plusmn 22 312 plusmn 11 147 plusmn 13 2022 plusmn115lowast lowast lowast 324 plusmn 42lowastlowastII 20 223 plusmn 14 306 plusmn 16 394 plusmn 22 189 plusmn 22lowastlowast 1885plusmn123lowast lowast lowast 391 plusmn 16lowast lowast lowastIII 17 291 plusmn 28lowastlowast 398 plusmn 32lowast 465 plusmn 18lowast 176 plusmn 11lowastlowast 244 plusmn 19lowast lowast lowast 443 plusmn 29lowast lowast lowastAll patients 234 plusmn 13 314 plusmn 25lowast 388 plusmn 15lowast 168 plusmn 13lowast 1304 plusmn 96lowast lowast lowast 326 plusmn 22lowast lowast lowastControl 30 203 plusmn 11 244 plusmn 35 323 plusmn 041 1131 plusmn 07 122 plusmn 003 208 plusmn 022Note I a mild form II moderate form and III severe formlowastp lt005 lowastlowastp lt001 lowast lowast lowastp lt0001mdashsignificant differences compared with the control
were found in severe tropical malaria perhaps due to exces-sive activity of monocytesmacrophages responsible for theproduction of proinflammatory components of regulationas well as the release of reactive radicals The involvementof the monocyte-macrophage cells followed by the activeelaboration of the whole complex of biologically activesubstances contributing to cellular and circulatory disorderscan be traced withmoderate and severe P falciparummalariait is probably one of the pathological links of severe anemiabrain damage and nonspecific inflammation In consideringthe role of cytokines in the development of these or otherdisturbances one has to take into account the diversity oftheir spectrum of biological activity [6 7] It is known thatIFN-120574 naturally called immune interferon also has the abilityto suppress the proliferation of erythrocyte germ cells [3] Ofparticular interest is the study of proinflammatory cytokineantagonistsmdashIL-4 produced by Th2-cells The concentrationof this cytokine was significantly greater than control valuesin all periods of the disease the highest content was duringthe peak of P falciparum malaria (p lt001) suggesting animbalance of immunoregulatory mechanisms of Th2 typeThe predominance of Th2-pathway immune response deter-mines the suppression of cell-mediated immunity in the earlystages of the disease In addition the imbalance of cell-cell interactions and the reduction of immunomodulatoryproperties indicate failure of stimulation of own adequateimmune response as a reaction to malarial infection causedby P falciparum Although replicative P falciparum malariapathogen activity must be an inductor of interferon produc-tion it does not happen due to lack of effective immunolog-ical response to various stimuli including proinflammatorycytokines pathogen itself and its products of metabolismThis may lead to severe course with the development of seri-ous complications and the concentration of these cytokines
may be a predictor of it It should be noted that imbalanceof immune mechanisms is short and in the recovery periodthe dominance of Th1-type immune response is observedthat is induced by IFN-120574 production as well as lower levelsof proinflammatory cytokines that exacerbate cardiovascularand autoimmune processes Increasing concentrations of IL-4 have compensatory rather than active counterregulatorycharacter to proinflammatory cytokines that implies morestabilizing function in the inflammatory response Togetherthese identified features demonstrate the complexity anddiversity of processes of immune cytokines in P falciparummalaria
4 Discussion
The Plasmodium falciparum malaria is characterized bydepression of T cell immunity the extent of which dependedon the severity of malaria infection Please note the lowlevels of T-lymphocytes in moderate and severe forms of thedisease a significant reduction of T helpers relatively intactlevel of T suppressors and suppression of humoral immu-nity These changes are most pronounced in the moderateform of the disease moreover they are accompanied by asubstantial increase in the functional activity of cells havingkiller cytotoxic activity The study of cellular and humoralimmunity in patients with tropical malaria is an obviousadditional criterion in assessing the severity of infection Theimbalance of cytokine profile in P falciparum malaria is animportant pathogenetic factor in the development of severeand recurrent forms of the disease since the formation of adefective immune response to parasitic antigens contributesto adverse outcomes
In parallel and at the same time the above-mentionedindicators of the immune status and cytokine profile were
Journal of Tropical Medicine 5
0
50
100
150
200
315207
204
1505
607234
203
Pgml
Stage of disease
Note 1 ndash Peak of disease 2 ndash Early recovery 3 ndash Late recovery 4 ndash Сontrol
TNF-
P vivaxP falciparumcontrol
Figure 2 Dynamics of indicators of proinflammatory cytokines(TNF-120572) in children with malaria
0
100
200
300
345 283 267
2162
891314
244
Pgml
Stage of diseaseNote 1 ndash Peak of disease 2 ndash Early recovery 3 ndash Late recovery 4 ndash
control
IL-1
P vivaxP falciparumcontrl
Figure 3Dynamics of indicators of proinflammatory cytokines (IL-1120573) in children with malaria
carried out in children with P vivax (mean severityndash59patients severendash21) It was found that the nature of immuno-logical disorders in the tertian malaria in contrast to the Pfalciparum malaria is due to the high level of CIC in theircomposition of IgM in combination with a decrease in theabsolute number of peripheral blood lymphocytes Immuno-logical reactions are not prolonged in time and reflect theadequacy of the immune response The tertian malaria ischaracterized by the predominance of Th1-pathway immuneresponse which contributes to the earliest elimination ofinfected red blood cells and pathogens from the body andthe adequacy of the mechanisms of immunological responseIn P falciparummalaria as noted above Th2-pathway of theimmune response prevails in the early stages of the diseasewith a switch in the period of convalescence toTh1-characterof lymphocytic reactions (Figures 2ndash7)The persistent imbal-ance in theTh1Th2 cytokine systemobserved inP falciparummalaria is a predictor of the severe complicated course ofthe disease since the formation of an inadequate immuneresponse to parasitic antigens contributes to the developmentof adverse outcomes
The study of cellular and humoral immunity in patientswith P falciparummalaria is an objective additional criterionin assessing the severity of the infectious process
050
100150200
455367 331
1606
682388
323
Pgml
Stage of diseaseNote 1 ndash Peak of disease 2 ndash Early recovery 3 ndash Late recovery 4 ndash control
IL-6
P vivaxP falciparumcontrol
Figure 4 Dynamics of indicators of proinflammatory cytokines(IL-6) in children with malaria
16 164129
72112
168
113
0
5
10
15
20
25
30
35Pgml
Stage of diseaseNote 1 ndash Peak of disease 2 ndash Early recovery 3 ndash Late recovery 4 ndash control
INF-
controlP falciparumP vivax
Figure 5 Dynamics of indicators of proinflammatory cytokinesantagonists (IFN-120574) in children with malaria
0
100
200
300
400 3764
1328
518163 722 1304122
Pgml
Stage of diseaseNote 1 ndash Peak of disease 2 ndash Early recovery 3 ndash Late recovery 4 ndash control
IL-2
P vivaxP falciparumcontrol
Figure 6 Dynamics of indicators of proinflammatory cytokinesantagonists (IL-2) in children with malaria
6 Journal of Tropical Medicine
050
100150200250300
208
1142
296
2711
1046
326 208
Pgml
Stage of diseaseNote 1 ndash Peak of disease 2 ndash Early recovery 3 ndash Late recovery 4 ndash control
IL-4
P vivaxP falciparumcontrol
Figure 7 Dynamics of indicators of proinflammatory cytokinesantagonists (IL-4) in children with malaria
5 Conclusions
Plasmodium falciparummalaria was characterized by depres-sion of cellular and humoral immunity the degree of whichdepended on the severity of the pathological process Pleasepay attention to the low rates of T-lymphocytes in moderateand severe forms of the disease and the significant decreasein T-lymphocytes-helpers with a relatively stable level of T-lymphocytes-suppressors The most pronounced changes inthe moderate form of the disease are accompanied by asignificant increase in the functional activity of cells withkiller cytotoxic activity and activation of humoral protectionfactors
Data Availability
The data used to support the findings of this study areavailable from the corresponding author upon request
Conflicts of Interest
The authors declare that they have no conflicts of interestregarding the publication of this paper
Authorsrsquo Contributions
Nighina M Khodzhaeva developed the study of protocoland wrote part of the manuscript Alla M Baranova partic-ipated in the epidemiological and clinical diagnoses and dataanalysis Anatoly K Tokmalaev developed the protocol andwrote part of the manuscript All authors approved the finalmanuscript
References
[1] D S Saiburhonov S S Karimov D S Kadamov and A MBaranova ldquoDistribution of Plasmodium falciparum malaria inthe Republic of Tajikistan 1994-2008rdquo Meditsinskaya Parazi-tologiya (Mosk) vol 1 pp 3ndash6 2015 (Russian)
[2] Malaria in the WHO European Region on the Road to Elim-ination 2000-2015 vol 40 World Health Organization 2018
httpwwweurowhointenhealth-topicscommunicable-diseas-esvector-borne-and-parasitic-diseasespublications2018ma-laria-in-the-who-european-region-on-the-road-to-elimination-20002015-summary-2018
[3] V P Sergiev N D Yushchuk U Y Vengerow and V DZavoykin ldquoTropical diseaserdquoManual for Physicians PublishingHouse BINOM vol 640 2015 (Russian)
[4] L Schofield and G E Grau ldquoImmunological processes inmalaria pathogenesisrdquo Nature Reviews Immunology vol 5 no9 pp 722ndash735 2005
[5] M Y Boiro S Boumbali O K Konstantinov S KalivoguiM Koulibali and A S Bah ldquoIndices of immune responsein patients of P falciparum malaria in Republic of GuineardquoInfection and Immunity (Russian Journal Infektsiya i Immunitet)vol 6 no 2 pp 151ndash156 2016 (Russian)
[6] E M Riley S Wahl D J Perkins and L Schofield ldquoRegulatingimmunity to malariardquo Parasite Immunology vol 28 no 1-2 pp35ndash49 2006
[7] S Blair Trujillo G Alvarez Sanchez A Villa Restrepo JCarmona Fonseca and L Rıos Osorio ldquoNutritional status andimmunoglobulin and cytokine concentrations in children withmalariardquo Anales de Pediatrıa (Barcelona Spain) vol 58 no 5pp 418ndash424 2003
[8] N M Khodzhaeva N F Fayzulloev and A K TokmalaevldquoCytokine profile of children to malariardquoMeditsinskaya Parazi-tologiya vol 4 pp 22ndash26 2008 (Russian)
[9] A P F do Rosario T Lamb P Spence et al ldquoIL-27 promotes IL-10 production by effectorTh1CD4+T cells a criticalmechanismfor protection from severe immunopathology during malariainfectionrdquoThe Journal of Immunology vol 188 no 3 pp 1178ndash1190 2012
[10] E B Belachew ldquoImmune response and evasion mechanismsof plasmodium falciparum parasitesrdquo Journal of ImmunologyResearch vol 2018 Article ID 6529681 6 pages 2018
[11] B Dinko and G Pradel ldquoImmune evasion by Plasmodiumfalciparum parasites converting a host protection mechanismfor the parasite1015840s benefitrdquo Advances in Infectious Diseases vol6 no 2 pp 82ndash95 2016
[12] P S Gomes J Bhardwaj J Rivera-Correa C G Freire-De-Lima and A Morrot ldquoImmune escape strategies of malariaparasitesrdquo Frontiers in Microbiology vol 7 article no 1617 2016
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

4 Journal of Tropical Medicine
Table 1 Contents of plasma cytokines in Plasmodium falciparum malaria in children (Pgml)
Periods of disease n TNF-120572 IL-1120573 IL-6 IFN-120574 IL-2 IL-4Peak of diseaseI 24 428 plusmn 17lowast lowast lowast 616 plusmn 58lowast lowast lowast 764 plusmn 25lowast lowast lowast 93 plusmn 06 203 plusmn 23 1358plusmn71lowast lowast lowastII 24 1021plusmn 156lowast lowast lowast 1202 plusmn107lowast lowast lowast 1081 plusmn 62lowast lowast lowast 68 plusmn 04lowast 184 plusmn 11 2339plusmn 224lowast lowast lowastIII 24 3329plusmn489lowast lowast lowast 4668 plusmn514lowast lowast lowast 3062 plusmn 71lowast lowast lowast 54 plusmn 01lowast 135 plusmn 16 4585 plusmn167lowast lowast lowastAll patients 1505 plusmn 63lowast lowast lowast 2162 plusmn401lowast lowast lowast 1606 plusmn 34lowast lowast lowast 72 plusmn 02lowast 163 plusmn 17 2711 plusmn 94lowast lowast lowastEarly recoveryI 24 294 plusmn 12lowastlowast 433 plusmn 12lowast lowast lowast 492 plusmn 17lowast lowast lowast 104 plusmn 11 1084 plusmn132lowast lowast lowast 466 plusmn 39lowast lowast lowastII 24 402 plusmn 24lowastlowast 888 plusmn 26lowast lowast lowast 581 plusmn 35lowast lowast lowast 129 plusmn 15 829 plusmn 52lowast lowast lowast 721 plusmn 29lowast lowast lowastIII 24 1226 plusmn32lowast lowast lowast 1359 plusmn 47lowast lowast lowast 1024 plusmn 42lowast lowast lowast 121 plusmn 13 463 plusmn 37 lowast lowast lowast 2004 plusmn 34lowast lowast lowastAll patients 607 plusmn 21lowast lowast lowast 891 plusmn 87lowast lowast lowast 682 plusmn 23lowast lowast lowast 112 plusmn 12 722 plusmn 37lowast lowast lowast 1046 plusmn 57lowast lowast lowastLate recoveryI 18 209 plusmn 11 249 plusmn 22 312 plusmn 11 147 plusmn 13 2022 plusmn115lowast lowast lowast 324 plusmn 42lowastlowastII 20 223 plusmn 14 306 plusmn 16 394 plusmn 22 189 plusmn 22lowastlowast 1885plusmn123lowast lowast lowast 391 plusmn 16lowast lowast lowastIII 17 291 plusmn 28lowastlowast 398 plusmn 32lowast 465 plusmn 18lowast 176 plusmn 11lowastlowast 244 plusmn 19lowast lowast lowast 443 plusmn 29lowast lowast lowastAll patients 234 plusmn 13 314 plusmn 25lowast 388 plusmn 15lowast 168 plusmn 13lowast 1304 plusmn 96lowast lowast lowast 326 plusmn 22lowast lowast lowastControl 30 203 plusmn 11 244 plusmn 35 323 plusmn 041 1131 plusmn 07 122 plusmn 003 208 plusmn 022Note I a mild form II moderate form and III severe formlowastp lt005 lowastlowastp lt001 lowast lowast lowastp lt0001mdashsignificant differences compared with the control
were found in severe tropical malaria perhaps due to exces-sive activity of monocytesmacrophages responsible for theproduction of proinflammatory components of regulationas well as the release of reactive radicals The involvementof the monocyte-macrophage cells followed by the activeelaboration of the whole complex of biologically activesubstances contributing to cellular and circulatory disorderscan be traced withmoderate and severe P falciparummalariait is probably one of the pathological links of severe anemiabrain damage and nonspecific inflammation In consideringthe role of cytokines in the development of these or otherdisturbances one has to take into account the diversity oftheir spectrum of biological activity [6 7] It is known thatIFN-120574 naturally called immune interferon also has the abilityto suppress the proliferation of erythrocyte germ cells [3] Ofparticular interest is the study of proinflammatory cytokineantagonistsmdashIL-4 produced by Th2-cells The concentrationof this cytokine was significantly greater than control valuesin all periods of the disease the highest content was duringthe peak of P falciparum malaria (p lt001) suggesting animbalance of immunoregulatory mechanisms of Th2 typeThe predominance of Th2-pathway immune response deter-mines the suppression of cell-mediated immunity in the earlystages of the disease In addition the imbalance of cell-cell interactions and the reduction of immunomodulatoryproperties indicate failure of stimulation of own adequateimmune response as a reaction to malarial infection causedby P falciparum Although replicative P falciparum malariapathogen activity must be an inductor of interferon produc-tion it does not happen due to lack of effective immunolog-ical response to various stimuli including proinflammatorycytokines pathogen itself and its products of metabolismThis may lead to severe course with the development of seri-ous complications and the concentration of these cytokines
may be a predictor of it It should be noted that imbalanceof immune mechanisms is short and in the recovery periodthe dominance of Th1-type immune response is observedthat is induced by IFN-120574 production as well as lower levelsof proinflammatory cytokines that exacerbate cardiovascularand autoimmune processes Increasing concentrations of IL-4 have compensatory rather than active counterregulatorycharacter to proinflammatory cytokines that implies morestabilizing function in the inflammatory response Togetherthese identified features demonstrate the complexity anddiversity of processes of immune cytokines in P falciparummalaria
4 Discussion
The Plasmodium falciparum malaria is characterized bydepression of T cell immunity the extent of which dependedon the severity of malaria infection Please note the lowlevels of T-lymphocytes in moderate and severe forms of thedisease a significant reduction of T helpers relatively intactlevel of T suppressors and suppression of humoral immu-nity These changes are most pronounced in the moderateform of the disease moreover they are accompanied by asubstantial increase in the functional activity of cells havingkiller cytotoxic activity The study of cellular and humoralimmunity in patients with tropical malaria is an obviousadditional criterion in assessing the severity of infection Theimbalance of cytokine profile in P falciparum malaria is animportant pathogenetic factor in the development of severeand recurrent forms of the disease since the formation of adefective immune response to parasitic antigens contributesto adverse outcomes
In parallel and at the same time the above-mentionedindicators of the immune status and cytokine profile were
Journal of Tropical Medicine 5
0
50
100
150
200
315207
204
1505
607234
203
Pgml
Stage of disease
Note 1 ndash Peak of disease 2 ndash Early recovery 3 ndash Late recovery 4 ndash Сontrol
TNF-
P vivaxP falciparumcontrol
Figure 2 Dynamics of indicators of proinflammatory cytokines(TNF-120572) in children with malaria
0
100
200
300
345 283 267
2162
891314
244
Pgml
Stage of diseaseNote 1 ndash Peak of disease 2 ndash Early recovery 3 ndash Late recovery 4 ndash
control
IL-1
P vivaxP falciparumcontrl
Figure 3Dynamics of indicators of proinflammatory cytokines (IL-1120573) in children with malaria
carried out in children with P vivax (mean severityndash59patients severendash21) It was found that the nature of immuno-logical disorders in the tertian malaria in contrast to the Pfalciparum malaria is due to the high level of CIC in theircomposition of IgM in combination with a decrease in theabsolute number of peripheral blood lymphocytes Immuno-logical reactions are not prolonged in time and reflect theadequacy of the immune response The tertian malaria ischaracterized by the predominance of Th1-pathway immuneresponse which contributes to the earliest elimination ofinfected red blood cells and pathogens from the body andthe adequacy of the mechanisms of immunological responseIn P falciparummalaria as noted above Th2-pathway of theimmune response prevails in the early stages of the diseasewith a switch in the period of convalescence toTh1-characterof lymphocytic reactions (Figures 2ndash7)The persistent imbal-ance in theTh1Th2 cytokine systemobserved inP falciparummalaria is a predictor of the severe complicated course ofthe disease since the formation of an inadequate immuneresponse to parasitic antigens contributes to the developmentof adverse outcomes
The study of cellular and humoral immunity in patientswith P falciparummalaria is an objective additional criterionin assessing the severity of the infectious process
050
100150200
455367 331
1606
682388
323
Pgml
Stage of diseaseNote 1 ndash Peak of disease 2 ndash Early recovery 3 ndash Late recovery 4 ndash control
IL-6
P vivaxP falciparumcontrol
Figure 4 Dynamics of indicators of proinflammatory cytokines(IL-6) in children with malaria
16 164129
72112
168
113
0
5
10
15
20
25
30
35Pgml
Stage of diseaseNote 1 ndash Peak of disease 2 ndash Early recovery 3 ndash Late recovery 4 ndash control
INF-
controlP falciparumP vivax
Figure 5 Dynamics of indicators of proinflammatory cytokinesantagonists (IFN-120574) in children with malaria
0
100
200
300
400 3764
1328
518163 722 1304122
Pgml
Stage of diseaseNote 1 ndash Peak of disease 2 ndash Early recovery 3 ndash Late recovery 4 ndash control
IL-2
P vivaxP falciparumcontrol
Figure 6 Dynamics of indicators of proinflammatory cytokinesantagonists (IL-2) in children with malaria
6 Journal of Tropical Medicine
050
100150200250300
208
1142
296
2711
1046
326 208
Pgml
Stage of diseaseNote 1 ndash Peak of disease 2 ndash Early recovery 3 ndash Late recovery 4 ndash control
IL-4
P vivaxP falciparumcontrol
Figure 7 Dynamics of indicators of proinflammatory cytokinesantagonists (IL-4) in children with malaria
5 Conclusions
Plasmodium falciparummalaria was characterized by depres-sion of cellular and humoral immunity the degree of whichdepended on the severity of the pathological process Pleasepay attention to the low rates of T-lymphocytes in moderateand severe forms of the disease and the significant decreasein T-lymphocytes-helpers with a relatively stable level of T-lymphocytes-suppressors The most pronounced changes inthe moderate form of the disease are accompanied by asignificant increase in the functional activity of cells withkiller cytotoxic activity and activation of humoral protectionfactors
Data Availability
The data used to support the findings of this study areavailable from the corresponding author upon request
Conflicts of Interest
The authors declare that they have no conflicts of interestregarding the publication of this paper
Authorsrsquo Contributions
Nighina M Khodzhaeva developed the study of protocoland wrote part of the manuscript Alla M Baranova partic-ipated in the epidemiological and clinical diagnoses and dataanalysis Anatoly K Tokmalaev developed the protocol andwrote part of the manuscript All authors approved the finalmanuscript
References
[1] D S Saiburhonov S S Karimov D S Kadamov and A MBaranova ldquoDistribution of Plasmodium falciparum malaria inthe Republic of Tajikistan 1994-2008rdquo Meditsinskaya Parazi-tologiya (Mosk) vol 1 pp 3ndash6 2015 (Russian)
[2] Malaria in the WHO European Region on the Road to Elim-ination 2000-2015 vol 40 World Health Organization 2018
httpwwweurowhointenhealth-topicscommunicable-diseas-esvector-borne-and-parasitic-diseasespublications2018ma-laria-in-the-who-european-region-on-the-road-to-elimination-20002015-summary-2018
[3] V P Sergiev N D Yushchuk U Y Vengerow and V DZavoykin ldquoTropical diseaserdquoManual for Physicians PublishingHouse BINOM vol 640 2015 (Russian)
[4] L Schofield and G E Grau ldquoImmunological processes inmalaria pathogenesisrdquo Nature Reviews Immunology vol 5 no9 pp 722ndash735 2005
[5] M Y Boiro S Boumbali O K Konstantinov S KalivoguiM Koulibali and A S Bah ldquoIndices of immune responsein patients of P falciparum malaria in Republic of GuineardquoInfection and Immunity (Russian Journal Infektsiya i Immunitet)vol 6 no 2 pp 151ndash156 2016 (Russian)
[6] E M Riley S Wahl D J Perkins and L Schofield ldquoRegulatingimmunity to malariardquo Parasite Immunology vol 28 no 1-2 pp35ndash49 2006
[7] S Blair Trujillo G Alvarez Sanchez A Villa Restrepo JCarmona Fonseca and L Rıos Osorio ldquoNutritional status andimmunoglobulin and cytokine concentrations in children withmalariardquo Anales de Pediatrıa (Barcelona Spain) vol 58 no 5pp 418ndash424 2003
[8] N M Khodzhaeva N F Fayzulloev and A K TokmalaevldquoCytokine profile of children to malariardquoMeditsinskaya Parazi-tologiya vol 4 pp 22ndash26 2008 (Russian)
[9] A P F do Rosario T Lamb P Spence et al ldquoIL-27 promotes IL-10 production by effectorTh1CD4+T cells a criticalmechanismfor protection from severe immunopathology during malariainfectionrdquoThe Journal of Immunology vol 188 no 3 pp 1178ndash1190 2012
[10] E B Belachew ldquoImmune response and evasion mechanismsof plasmodium falciparum parasitesrdquo Journal of ImmunologyResearch vol 2018 Article ID 6529681 6 pages 2018
[11] B Dinko and G Pradel ldquoImmune evasion by Plasmodiumfalciparum parasites converting a host protection mechanismfor the parasite1015840s benefitrdquo Advances in Infectious Diseases vol6 no 2 pp 82ndash95 2016
[12] P S Gomes J Bhardwaj J Rivera-Correa C G Freire-De-Lima and A Morrot ldquoImmune escape strategies of malariaparasitesrdquo Frontiers in Microbiology vol 7 article no 1617 2016
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

Journal of Tropical Medicine 5
0
50
100
150
200
315207
204
1505
607234
203
Pgml
Stage of disease
Note 1 ndash Peak of disease 2 ndash Early recovery 3 ndash Late recovery 4 ndash Сontrol
TNF-
P vivaxP falciparumcontrol
Figure 2 Dynamics of indicators of proinflammatory cytokines(TNF-120572) in children with malaria
0
100
200
300
345 283 267
2162
891314
244
Pgml
Stage of diseaseNote 1 ndash Peak of disease 2 ndash Early recovery 3 ndash Late recovery 4 ndash
control
IL-1
P vivaxP falciparumcontrl
Figure 3Dynamics of indicators of proinflammatory cytokines (IL-1120573) in children with malaria
carried out in children with P vivax (mean severityndash59patients severendash21) It was found that the nature of immuno-logical disorders in the tertian malaria in contrast to the Pfalciparum malaria is due to the high level of CIC in theircomposition of IgM in combination with a decrease in theabsolute number of peripheral blood lymphocytes Immuno-logical reactions are not prolonged in time and reflect theadequacy of the immune response The tertian malaria ischaracterized by the predominance of Th1-pathway immuneresponse which contributes to the earliest elimination ofinfected red blood cells and pathogens from the body andthe adequacy of the mechanisms of immunological responseIn P falciparummalaria as noted above Th2-pathway of theimmune response prevails in the early stages of the diseasewith a switch in the period of convalescence toTh1-characterof lymphocytic reactions (Figures 2ndash7)The persistent imbal-ance in theTh1Th2 cytokine systemobserved inP falciparummalaria is a predictor of the severe complicated course ofthe disease since the formation of an inadequate immuneresponse to parasitic antigens contributes to the developmentof adverse outcomes
The study of cellular and humoral immunity in patientswith P falciparummalaria is an objective additional criterionin assessing the severity of the infectious process
050
100150200
455367 331
1606
682388
323
Pgml
Stage of diseaseNote 1 ndash Peak of disease 2 ndash Early recovery 3 ndash Late recovery 4 ndash control
IL-6
P vivaxP falciparumcontrol
Figure 4 Dynamics of indicators of proinflammatory cytokines(IL-6) in children with malaria
16 164129
72112
168
113
0
5
10
15
20
25
30
35Pgml
Stage of diseaseNote 1 ndash Peak of disease 2 ndash Early recovery 3 ndash Late recovery 4 ndash control
INF-
controlP falciparumP vivax
Figure 5 Dynamics of indicators of proinflammatory cytokinesantagonists (IFN-120574) in children with malaria
0
100
200
300
400 3764
1328
518163 722 1304122
Pgml
Stage of diseaseNote 1 ndash Peak of disease 2 ndash Early recovery 3 ndash Late recovery 4 ndash control
IL-2
P vivaxP falciparumcontrol
Figure 6 Dynamics of indicators of proinflammatory cytokinesantagonists (IL-2) in children with malaria
6 Journal of Tropical Medicine
050
100150200250300
208
1142
296
2711
1046
326 208
Pgml
Stage of diseaseNote 1 ndash Peak of disease 2 ndash Early recovery 3 ndash Late recovery 4 ndash control
IL-4
P vivaxP falciparumcontrol
Figure 7 Dynamics of indicators of proinflammatory cytokinesantagonists (IL-4) in children with malaria
5 Conclusions
Plasmodium falciparummalaria was characterized by depres-sion of cellular and humoral immunity the degree of whichdepended on the severity of the pathological process Pleasepay attention to the low rates of T-lymphocytes in moderateand severe forms of the disease and the significant decreasein T-lymphocytes-helpers with a relatively stable level of T-lymphocytes-suppressors The most pronounced changes inthe moderate form of the disease are accompanied by asignificant increase in the functional activity of cells withkiller cytotoxic activity and activation of humoral protectionfactors
Data Availability
The data used to support the findings of this study areavailable from the corresponding author upon request
Conflicts of Interest
The authors declare that they have no conflicts of interestregarding the publication of this paper
Authorsrsquo Contributions
Nighina M Khodzhaeva developed the study of protocoland wrote part of the manuscript Alla M Baranova partic-ipated in the epidemiological and clinical diagnoses and dataanalysis Anatoly K Tokmalaev developed the protocol andwrote part of the manuscript All authors approved the finalmanuscript
References
[1] D S Saiburhonov S S Karimov D S Kadamov and A MBaranova ldquoDistribution of Plasmodium falciparum malaria inthe Republic of Tajikistan 1994-2008rdquo Meditsinskaya Parazi-tologiya (Mosk) vol 1 pp 3ndash6 2015 (Russian)
[2] Malaria in the WHO European Region on the Road to Elim-ination 2000-2015 vol 40 World Health Organization 2018
httpwwweurowhointenhealth-topicscommunicable-diseas-esvector-borne-and-parasitic-diseasespublications2018ma-laria-in-the-who-european-region-on-the-road-to-elimination-20002015-summary-2018
[3] V P Sergiev N D Yushchuk U Y Vengerow and V DZavoykin ldquoTropical diseaserdquoManual for Physicians PublishingHouse BINOM vol 640 2015 (Russian)
[4] L Schofield and G E Grau ldquoImmunological processes inmalaria pathogenesisrdquo Nature Reviews Immunology vol 5 no9 pp 722ndash735 2005
[5] M Y Boiro S Boumbali O K Konstantinov S KalivoguiM Koulibali and A S Bah ldquoIndices of immune responsein patients of P falciparum malaria in Republic of GuineardquoInfection and Immunity (Russian Journal Infektsiya i Immunitet)vol 6 no 2 pp 151ndash156 2016 (Russian)
[6] E M Riley S Wahl D J Perkins and L Schofield ldquoRegulatingimmunity to malariardquo Parasite Immunology vol 28 no 1-2 pp35ndash49 2006
[7] S Blair Trujillo G Alvarez Sanchez A Villa Restrepo JCarmona Fonseca and L Rıos Osorio ldquoNutritional status andimmunoglobulin and cytokine concentrations in children withmalariardquo Anales de Pediatrıa (Barcelona Spain) vol 58 no 5pp 418ndash424 2003
[8] N M Khodzhaeva N F Fayzulloev and A K TokmalaevldquoCytokine profile of children to malariardquoMeditsinskaya Parazi-tologiya vol 4 pp 22ndash26 2008 (Russian)
[9] A P F do Rosario T Lamb P Spence et al ldquoIL-27 promotes IL-10 production by effectorTh1CD4+T cells a criticalmechanismfor protection from severe immunopathology during malariainfectionrdquoThe Journal of Immunology vol 188 no 3 pp 1178ndash1190 2012
[10] E B Belachew ldquoImmune response and evasion mechanismsof plasmodium falciparum parasitesrdquo Journal of ImmunologyResearch vol 2018 Article ID 6529681 6 pages 2018
[11] B Dinko and G Pradel ldquoImmune evasion by Plasmodiumfalciparum parasites converting a host protection mechanismfor the parasite1015840s benefitrdquo Advances in Infectious Diseases vol6 no 2 pp 82ndash95 2016
[12] P S Gomes J Bhardwaj J Rivera-Correa C G Freire-De-Lima and A Morrot ldquoImmune escape strategies of malariaparasitesrdquo Frontiers in Microbiology vol 7 article no 1617 2016
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

6 Journal of Tropical Medicine
050
100150200250300
208
1142
296
2711
1046
326 208
Pgml
Stage of diseaseNote 1 ndash Peak of disease 2 ndash Early recovery 3 ndash Late recovery 4 ndash control
IL-4
P vivaxP falciparumcontrol
Figure 7 Dynamics of indicators of proinflammatory cytokinesantagonists (IL-4) in children with malaria
5 Conclusions
Plasmodium falciparummalaria was characterized by depres-sion of cellular and humoral immunity the degree of whichdepended on the severity of the pathological process Pleasepay attention to the low rates of T-lymphocytes in moderateand severe forms of the disease and the significant decreasein T-lymphocytes-helpers with a relatively stable level of T-lymphocytes-suppressors The most pronounced changes inthe moderate form of the disease are accompanied by asignificant increase in the functional activity of cells withkiller cytotoxic activity and activation of humoral protectionfactors
Data Availability
The data used to support the findings of this study areavailable from the corresponding author upon request
Conflicts of Interest
The authors declare that they have no conflicts of interestregarding the publication of this paper
Authorsrsquo Contributions
Nighina M Khodzhaeva developed the study of protocoland wrote part of the manuscript Alla M Baranova partic-ipated in the epidemiological and clinical diagnoses and dataanalysis Anatoly K Tokmalaev developed the protocol andwrote part of the manuscript All authors approved the finalmanuscript
References
[1] D S Saiburhonov S S Karimov D S Kadamov and A MBaranova ldquoDistribution of Plasmodium falciparum malaria inthe Republic of Tajikistan 1994-2008rdquo Meditsinskaya Parazi-tologiya (Mosk) vol 1 pp 3ndash6 2015 (Russian)
[2] Malaria in the WHO European Region on the Road to Elim-ination 2000-2015 vol 40 World Health Organization 2018
httpwwweurowhointenhealth-topicscommunicable-diseas-esvector-borne-and-parasitic-diseasespublications2018ma-laria-in-the-who-european-region-on-the-road-to-elimination-20002015-summary-2018
[3] V P Sergiev N D Yushchuk U Y Vengerow and V DZavoykin ldquoTropical diseaserdquoManual for Physicians PublishingHouse BINOM vol 640 2015 (Russian)
[4] L Schofield and G E Grau ldquoImmunological processes inmalaria pathogenesisrdquo Nature Reviews Immunology vol 5 no9 pp 722ndash735 2005
[5] M Y Boiro S Boumbali O K Konstantinov S KalivoguiM Koulibali and A S Bah ldquoIndices of immune responsein patients of P falciparum malaria in Republic of GuineardquoInfection and Immunity (Russian Journal Infektsiya i Immunitet)vol 6 no 2 pp 151ndash156 2016 (Russian)
[6] E M Riley S Wahl D J Perkins and L Schofield ldquoRegulatingimmunity to malariardquo Parasite Immunology vol 28 no 1-2 pp35ndash49 2006
[7] S Blair Trujillo G Alvarez Sanchez A Villa Restrepo JCarmona Fonseca and L Rıos Osorio ldquoNutritional status andimmunoglobulin and cytokine concentrations in children withmalariardquo Anales de Pediatrıa (Barcelona Spain) vol 58 no 5pp 418ndash424 2003
[8] N M Khodzhaeva N F Fayzulloev and A K TokmalaevldquoCytokine profile of children to malariardquoMeditsinskaya Parazi-tologiya vol 4 pp 22ndash26 2008 (Russian)
[9] A P F do Rosario T Lamb P Spence et al ldquoIL-27 promotes IL-10 production by effectorTh1CD4+T cells a criticalmechanismfor protection from severe immunopathology during malariainfectionrdquoThe Journal of Immunology vol 188 no 3 pp 1178ndash1190 2012
[10] E B Belachew ldquoImmune response and evasion mechanismsof plasmodium falciparum parasitesrdquo Journal of ImmunologyResearch vol 2018 Article ID 6529681 6 pages 2018
[11] B Dinko and G Pradel ldquoImmune evasion by Plasmodiumfalciparum parasites converting a host protection mechanismfor the parasite1015840s benefitrdquo Advances in Infectious Diseases vol6 no 2 pp 82ndash95 2016
[12] P S Gomes J Bhardwaj J Rivera-Correa C G Freire-De-Lima and A Morrot ldquoImmune escape strategies of malariaparasitesrdquo Frontiers in Microbiology vol 7 article no 1617 2016
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom
Related Documents











