Journal of Psychosomaric Research, Vol. 33, No. 5, pp. 537-547, 1989. 0022-3999/89 $3.00 + 00 Printed in Great Britain. Pergamon Press pk THE EFFECTS OF EXERCISE TRAINING ON MOOD AND PERCEIVED COPING ABILITY IN ANXIOUS ADULTS FROM THE GENERAL POPULATION ANDREW STEPTOE,* SARA EDWARDS, JENNIFER MOSES? and ANDREW MATHEWS% (Received 22 November 1988; accepted in revised form 15 March 1989) Abstract-A comparison was carried out of the psychological effects of a moderate aerobic training programme (n = 24) and an attention-placebo strength and flexibility training programme (n = 23) in previously inactive anxious adults from the general population. Training consisted of one supervised and three unsupervised sessions per week for 10 weeks. Effects were assessed with the Profile of Mood States, the State-Trait Anxiety Inventory and questionnaires indexing perceived coping ability. Seven participants dropped out of each condition during the training period. Expectations of benefit assessed pre-training, and satisfaction assessed post-training, did not differ between conditions. The moderate exercise programme led to significant improvements in aerobic fitness, and was associated with significantly greater reductions in tension-anxiety, depression and other moods than the attention-placebo condition, together with increases in perceived ability to cope with stress. Psychological responses were not correlated with changes in fitness assessed with bicycle ergometry or the 12 min walk/run test. These effects were maintained on 3 month follow up. INTRODUCTION EXERCISE training is thought to have a beneficial effect on psychological well-being [I, 21. Positive results have been reported using aerobic training with volunteers from the general population, people with stress-related problems and depressed patients [3-51. However, studies in this area suffer from a number of methodological deficiencies, including non-random assignment of participants and failure to control for subject expectation, attention, encouragement and the non-specific effect of taking part in a structured course of activity with the achievement of progressive goals [6]. The implications for public health have also been limited by the use of costly, intensively supervised programs, requiring therapist or trainer involvement several times a week. An experiment was therefore carried out with psychologically healthy volunteers from the general population, in which aerobic training at a high intensity was compared with moderate intensity training, an attention-placebo condition and wait-list control [7]. The aerobic programmes were based on walking and jogging at individually determined rates designed to elevate heart rate to 70--75% Department of Psychology, St Georges Hospital Medical School, University of London, London, U.K. *Address correspondence to: Andrew Steptoe, Department of Psychology, St George’s Hosp. Med. Sch., Cranmer Terrace, London SW17 ORE, U.K. tSub-Department of Clinical Psychology, University of Liverpool, Liverpool, U.K. IDepartment of Psychology, Louisiana State University, Baton Rouge, Louisiana, U.S.A. 537

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Journal of Psychosomaric Research, Vol. 33, No. 5, pp. 537-547, 1989. 0022-3999/89 $3.00 + 00 Printed in Great Britain. Pergamon Press pk
THE EFFECTS OF EXERCISE TRAINING ON MOOD AND PERCEIVED COPING ABILITY IN ANXIOUS ADULTS FROM THE GENERAL
POPULATION
ANDREW STEPTOE,* SARA EDWARDS,
JENNIFER MOSES? and ANDREW MATHEWS%
(Received 22 November 1988; accepted in revised form 15 March 1989)
Abstract-A comparison was carried out of the psychological effects of a moderate aerobic training programme (n = 24) and an attention-placebo strength and flexibility training programme (n = 23) in previously inactive anxious adults from the general population. Training consisted of one supervised and three unsupervised sessions per week for 10 weeks. Effects were assessed with the Profile of Mood States, the State-Trait Anxiety Inventory and questionnaires indexing perceived coping ability. Seven participants dropped out of each condition during the training period. Expectations of benefit assessed pre-training, and satisfaction assessed post-training, did not differ between conditions. The moderate exercise programme led to significant improvements in aerobic fitness, and was associated with significantly greater reductions in tension-anxiety, depression and other moods than the attention-placebo condition, together with increases in perceived ability to cope with stress. Psychological responses were not correlated with changes in fitness assessed with bicycle ergometry or the 12 min walk/run test. These effects were maintained on 3 month follow up.
INTRODUCTION
EXERCISE training is thought to have a beneficial effect on psychological well-being [I, 21. Positive results have been reported using aerobic training with volunteers from the general population, people with stress-related problems and depressed patients [3-51. However, studies in this area suffer from a number of methodological deficiencies, including non-random assignment of participants and failure to control for subject expectation, attention, encouragement and the non-specific effect of taking part in a structured course of activity with the achievement of progressive goals [6]. The implications for public health have also been limited by the use of costly, intensively supervised programs, requiring therapist or trainer involvement several times a week. An experiment was therefore carried out with psychologically healthy volunteers from the general population, in which aerobic training at a high intensity was compared with moderate intensity training, an attention-placebo condition and wait-list control [7]. The aerobic programmes were based on walking and jogging at individually determined rates designed to elevate heart rate to 70--75%
Department of Psychology, St Georges Hospital Medical School, University of London, London, U.K. *Address correspondence to: Andrew Steptoe, Department of Psychology, St George’s Hosp. Med.
Sch., Cranmer Terrace, London SW17 ORE, U.K. tSub-Department of Clinical Psychology, University of Liverpool, Liverpool, U.K. IDepartment of Psychology, Louisiana State University, Baton Rouge, Louisiana, U.S.A.
537
538 ANDREW STEPTOE el al.
(high intensity condition) or 60% (moderate intensity condition) of maximum. The attention-placebo programme was based on strength and flexibility exercises, and was devised to match the other conditions for all factors associated with exercise training apart from the aerobic component. Significant reductions in psychological tension were seen after the moderate exercise programme, but not after the high exercise or attention-placebo programmes. This effect was maintained at follow-up, at which time perceived coping ability was also greater in the moderate exercise group than in other conditions.
These results suggest that aerobic training does have a favourable effect on psychological well-being that is not accounted for by non-specific factors such as selection, expectations or attention. However, benefits are not directly related to improvements in cardiorespiratory fitness, and intensive aerobic programmes may have aversive components that counter improvements in mood. The conclusion that moderate exercise training is effective has important implications for the use of physical conditioning programs in health care. Accordingly, one of the principle aims of the present study was to replicate the finding that moderate exercise training leads to improvement in mood and perceived coping ability. A comparison was made with a strength and flexibility programme in order to control for attentional and other placebo factors. It should be noted that the demands of this schedule were light, and were not therefore equivalent to the intensive anaerobic training routines recently evaluated in the literature [5, 8,9]. Predominantly home-based self-monitored train- ing programmes were again employed, in order to reduce the impact of therapist contact to a low level, and to assess schedules that do not rely on intensive trainer involvement.
The second aim of the study was to assess the effects of training on volunteers from the general population who suffer from moderate elevations in tension and anxiety. Little information is available concerning the chronic effects of aerobic exercise on anxious individuals. However, exercise training has been found effective in reducing anxiety levels in non-anxious groups [7, lo] and women reporting stress at work [ 1 I], and in helping people to cope with stressful events [3, 121. Simons and Birkimer [ 121 reported that improvements in mood were correlated with level of negative mood pre-training. Participants in the current study were therefore selected on the basis of high levels of self-reported tension and anxiety.
METHOD
One hundred and ninety-three adults responded to advertisements in local newspapers inviting participation in a ‘Health and Fitness Programme’. Respondents were screened by postal questionnaire, and were considered eligible if they reported high levels of tension and anxiety, were aged between 20 and 60, reported low levels of habitual activity, no medical problems likely to interfere with training, absence of hypertension and psychiatric history, and if they were not more than 25% above their ideal weight (based on the Metropolitan Height and Weight Tables). The anxiety criterion was that participants should score within the ‘borderline’ or ‘definite’ range for clinically significant anxiety as indexed by the Hospital Anxiety and Depression Scale (HAD [14]), and/or have a score on the tension-anxiety scale of the Profile of Moods States (POMS [IS]) that was one standard deviation or more above the mean found in an earlier study on this local population [7]. Previous experience suggested an adherence rate of 75% might be anticipated, and recruitment was based on the goal of ending the trial with 15.-20 participants in each condition. Fifty-three volunteers were selected and were allocated to moderate exercise (n = 27) and attention-placebo (n = 26) conditions matched for age, sex, bodyweight, habitual activity level and initial
Exercise and anxiety 539
anxiety level. The volunteers selected were representative of the total number who fulfilled entry criteria with respect to age, sex and other factors. Participants were not informed that selection was based on anxiety reports.
Training programmes
Training m both conditions consisted of a IO-week course with one supervised and three unsupervised sessions per week. Each course was structured so that individuals began at an activity level appropriate for their initial fitness, and progressed towards more demanding levels over the programme. Sessions in the two conditions included identical warm-up and cool-down exercises lasting 510 min, but differed during the training phase.
Moderate aerobic training. This condition involved aerobic exercise at a level expected to produce marginal improvements in cardiorespiratory fitness on the criteria recommended by the American College of Sports Medicine [16]. It was based on sessions of 20 min continuous walking or jogging at an intensity sufficient to elevate heart rate to 60% but not above 65% of estimated maximum (HRmax).
Attention-placebo condition. Participants in this condition performed strength, mobility and flexibility exercises during the training phase of each session, performing discontinuous exercise for at least 20 min at an intensit.y that was not expected to elevate heart rate about 50% HRmax.
Participants were provided with detailed training manuals that outlined the rationales and structures of the programmes. Careful attention was paid in each group to helping participants to integrate training into their daily routine. Immediate and long-term goals were set in terms of improvements in endurance in the moderate exercise condition, and flexibility and suppleness in the attention-placebo condition, Participants were taught to monitor their own heart rates in order to ensure that they remained within prescribed training limits. Weekly diaries were distributed in which details of the duration of each training session were listed, together with ratings of exertion on the Borg scale [17]. These diaries were discussed at supervised training sessions and used to adjust activity levels and to identify problems of adherence.
Measures
Psychological measures. The principle measure used to evaluate the effects of experimental conditions was a modification of the POMS. This consisted of a 72 adjective inventory in which the participant rated each item on a five point scale ranging from 0 = ‘not at all’ to 4 = ‘extremely’. The 6 mood factors of the POMS-tension-anxiety, depression-dejection, anger-hostility, mental vigour, mental fatigue and mental confusion-were each represented by the six highest loading items on the original POMS, as published in the Manual [15]. The other 36 items were introduced in order to assess perceived coping ability. Using factor analysis, Moses et al. [7] identified three factors labelled ‘coping assets’ (14 items such as competent, self-confident), ‘coping deficits’ (10 items such as run-down, easily upset), and perceived ‘physical well-being’ (six items, including supple, refreshed). Scores on all scales were standardized so as to range from a minimum of 0 to a maximum of 24. The trait scale of the State Trait Anxiety Inventory (STAI [IS]) was used as an additional outcome measure.
Expectations concerning the programme were assessed with five questions, asking participants to what extent they believed that training would improve their level of fitness, sense of well-being, and health, the extent to which they expected to enjoy participating, and whether they would recommend the programme to a friend. Each item was rated on a five-point scale with higher scores representing more positive expectations. At the end of the study, satisfaction was assessed using the last three of these questions.
Psychological state prior to participation was assessed with the HAD; a score of 8-10 on the anxiety subscale indicates ‘borderline’, and 11 or more ‘probable’ case status. Habitual activity level (HAL) during work and leisure time was assessed using the questionnaire developed for the H.I.P. study of coronary heart disease [19].
Fitness measures. Two measures of aerobic fitness were obtained during the study. First, participants underwent a sub-maximal graded exercise test on a Monark 864 weight cycle ergometer. The electro- cardiogram and respiratory parameters were monitored on-line during four min trials at four workloads: 25, 50, 75 and 100 W. Heart rate and oxygen consumption over the last two mins of each workload were entered into a regression analysis in order to predict VO,max [20].
The second measure of physical fitness was the 12 min walk-run test [21]. Participants were asked to walk or run as far as they could within a 12 min period on an all-weather running track. The distance completed was converted using standardized scales to a predicted VO,max corrected for age and sex.
Other measures. Body weight and height were recorded. Percent body fat was assessed by using Holtain calipers to measure skin fold thickness from the biceps, triceps, subscapula and supra-iliac sites. Values were summed and converted to percent body fat in relation to age and sex using standard formulae [22].
Procedure
Participants were assessed individually before and after the training programme in the laboratory. Psychological measures were administered and the sub-maximal exercise test was carried out. In addition,

540 ANDREW STEPTOE et al
participants carried out a series of mental stress tests during which cardiovascular, respiratory and electrodermal parameters were monitored. The results of the psychophysiological testing will be presented elsewhere. In the pre-training session, participants were provided with a detailed summary of the experimental condition to which they had been assigned after assessments were completed. When this had been read, participants rated their expectations of benefit.
Pre-training laboratory assessment for each experimental group was conducted over a 223 week period. The group then met in an orientation session in which the details of the programme were elaborated, and practical questions concerning location, equipment and clothing were discussed. The first of the ten supervised sessions was conducted at a local running track, and the pre-treatment 12 min test was carried out on this occasion. Supervised sessions 2-9 were conducted in a gym, and the post-training 12 min test carried out during the 10th supervised session at the running track. Participants then returned to the laboratory for the post-training assessment over the next 2-3 weeks. Ratings of satisfaction were obtained during the post-treatment session. Participants in both groups were recontacted 3 months after the programme and asked to complete further psychological assessments, report on their activities over the intervening period, and carry out a further 12 min test.
Data reduction and analysis
Two of the POMS scales (depression-dejection and anger-hostility) were negative skewed due to a predominance of low scores. These scales were therefore log transformed before analysis. The remaining POMS and three coping scales were scored to produce responses ranging from O-24.
Volunteers were considered to have completed the programme if their diary records and attendance at supervised sessions indicated that they had completed 70% of scheduled assignments. Adherence was assessed by analysing diary records of home practise in terms of number of sessions per week and average duration of sessions in minutes, comparing weeks l--5 with weeks 610 in repeated measures analyses of variance (ANOVA). One way ANOVAs were used to compare the characteristics of groups pre-treatment. Responses to training were assessed with repeated measures ANOVA, and with analysis of co-variance (ANCOVA) of post-training and follow-up data using pre-treatment as the co-variate. The Green houseeGeisser adjustment to the degrees of freedom was applied where appropriate. In view of the predominance of women in the study, analyses were carried out on the entire sample and on women separately. However, the results were similar in the two cases, so data from the entire sample are reported here.
RESULTS
Group characteristics and adherence to training
Three members of each group dropped out of the study before training
commenced, leaving 24 in the moderate exercise and 23 in the attention-placebo
conditions. A further seven dropped out of each group over the training period--fiv-e
moved house or job and were thereby prevented from continuing, four gave medical reasons (pregnancy, hospital admission etc) while five gave no special explanation. A comparison of participants who completed the programme with those who dropped out revealed no significant differences in sex, age, physical characteristics, smoking, anxiety, depression. POMS and perceived coping ratings, habitual activity level, VO,max or expectations about training. The analysis is therefore based on 17 moderate exercise and 16 attention-placebo participants.
The initial characteristics of the two groups who completed the programme arc summarized in Table T. There were no significant differences between the groups in sex distribution, age, height, weight. body fat or physical fitness. There were seven smokers in the moderate exercise and two in the attention-placebo condition. Ratings of habitual activity at work and in leisure time did not differ significa.ntly between groups. The mean anxiety score on the HAD scale indicates a level on the margin of probable case status, while depression scores averaged at the upper limit of the normal range. Expectations of benefit were high (max. score 25). and there were no differences between the groups in this respect. Ratings of satisfaction taken post- training again showed no differences between groups, indicating that the conditions
Exercise and anxiety 541
TABLE I.--GROUP CHARACTERISTICS PRE-TRAININGMEAN (SD)
Moderate Attention- exercise placebo
n Sex Age (yr) Height (cm) Weight (kg) Body fat (%)
Hospital Anxiety and Depression Scale:
Anxiety Depression
Trait anxiety (STAI) Tension/Anxiety (POMS) Max oxygen consumption- Lab (ml/kg/min) Max oxygen consumption- 12 min test (ml/kg/min) Expectancy rating
17 16 14 F/3 M 14 F/2 M
35.4 (8.3) 38.7 (10.3) 168.2 i6.5) 172.1 (6.9) 64.4 (9.4) 63.4 (9.3) 27.8 (7.5) 30.7 (5.2)
10.4 (2.4) 10.8 (3.1) 6.2 (2.7) 7.4 (3.2)
50.0 (10.9) 50.6 (9.1) 10.2 (4.5) 10.8 (2.6)
41.0 (11.0) 41.7 (10.3)
28.8 (8.8) 29.5 (5.0) 22.6 (3.9) 21.3 (3.4)
were well matched in terms of enjoyability and subject expectations (overall mean 12.0, max. score 15).
Adherence to unsupervised practice sessions was assessed by analysing information provided in the weekly training diaries completed by participants. The mean number of sessions carried out each week was averaged for the first (weeks 1-5) and second (weeks 6-10) halves of the training programme. There was a significant main effect of time [F( 1,30) = 8.73, p < 0.011, with the average number of sessions completed per week dropping from 3.49 in l-5 weeks to 3.12 in weeks 6-10. There was also a significant main effect of groups [F(1,30) = 4.45, p < 0.051, participants in the moderate aerobic exercise programme completing more sessions than those in the attention-placebo condition (3.45 vs 3.13). On the other hand, the mean duration of sessions was significantly longer in the attention-placebo than moderate exercise conditions (44.8 .vs 33.0 mins, F(1,30) = 50.0, p < O.OOOl), indicating that the lower practice rate in the attention-placebo group was more than compensated by longer training (overall average weekly practice was 113.9 min in the moderate exercise, and 140.2 min in the attention-placebo condition).
Aerobic jitness changes
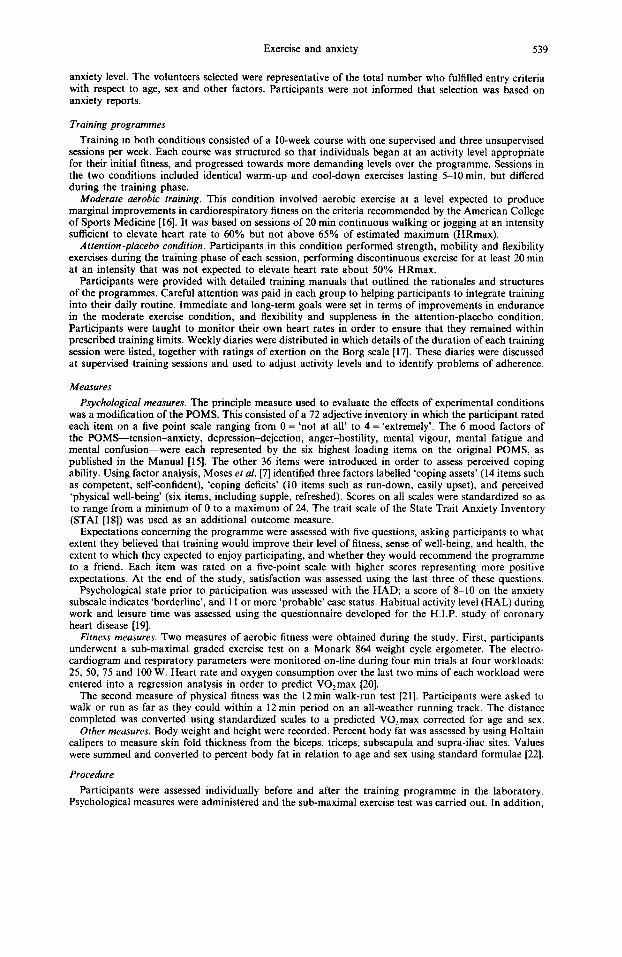
Changes in fitness were assessed using repeated measures ANOVA with experi- mental group as the between-subject factor and session (pre-training, post-training) as the within-subject factor. Analysis of VO,max derived from the laboratory test reveal a significant group by session interaction [F(1,3 1) = 12.1, p < 0.0021, shown in Fig. 1. The moderate exercise group produced an increase of 7.04 ml/kg/min over the training period, while there was no change in the attention-placebo condition. A similar interaction was observed on VO,max estimates derived from the 12 min
test [F(1,29) = 19.9, p < O.OOOl] (two members of the attention-placebo group failed to attend the 12 min test and were excluded from the analysis). As can be seen in Fig. 1, the average improvement in VO,max on the 12 min test was 7.4 ml/kg/min in the moderate exercise, and 1.5 ml/kg/min in the attention-placebo group. It is
542 ANDREW STEPTOE rt al
FITNESS RESPONSE
LABORATORY TEST 12 MIN TEST
:;I /// ; /
Pre Post Pre Post
FIG. I. Mean VO,max in ml/kg/min estimated from the bicycle ergometry test (left panel) and I2 min walk/run test (right panel). assessed pre and post the IO week training period. e--e Moderate exercise
group. 0 0 Attention-placebo group.
evident that the training conditions produced appropriate modifications in fitness. with a 17% improvement on the laboratory tests in the moderate aerobic training group, and virtually no change in the attention-placebo condition. Across the entire sample, there was a strong association between changes in VOzmax estimated from the laboratory and 12min test (r = 0.91, p < 0.0001). There were no significant alterations in body weight across the training period.
Ps_vchoIogicul results
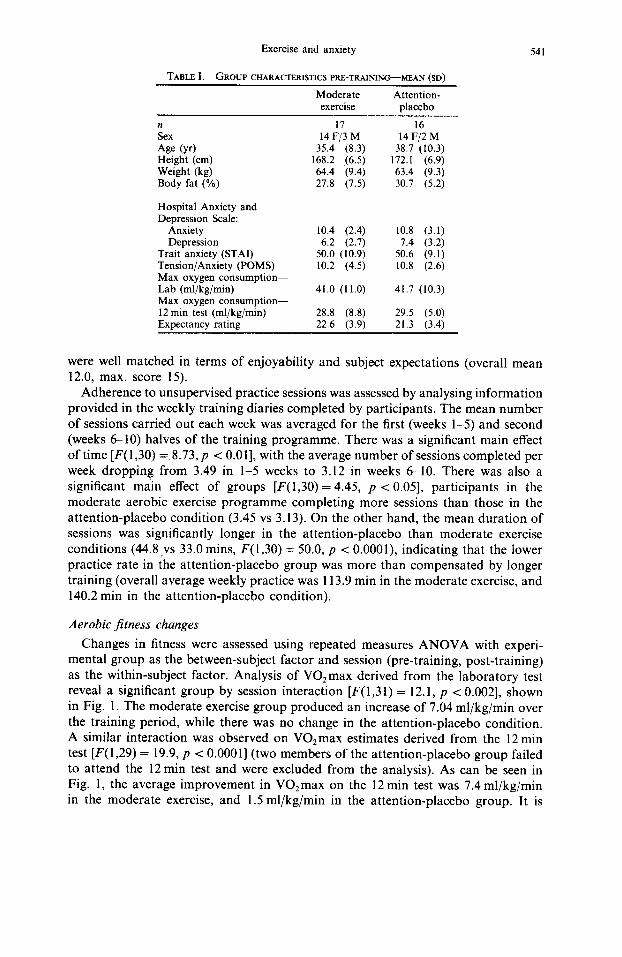
The two groups did not differ on anxiety, depression or any other psychological measures prior to training. Psychological responses post-training were assessed by ANCOVA and results are summarized in Table II. There were significant group differences post-training on POMS tension-anxiety, mental confusion and on per- ceived coping assets [F( 1,30) = 6.29, 4.48 and 4.20 respectively, p < 0.051. These effects are illustrated in Fig. 2, where it can be seen that there were greater reductions in tension-anxiety and improvements in perceived coping ability in the moderate
TABLE II.-PSYC‘HOLOGICAL (‘HANGES ACROSS THETRAINING PERIOD. (MEANS WITH STAS-
DAK” DEVIATIONS IN PARENTHESES) I_
Moderate exercise Attention-placebo
Pre- (’ T *‘) Post- Pre- (‘I = 16) Post- training training training training
Tension-anxiety 9.6 (4.5) 6.6 (3.7) X.5 (2.6) x.9 (4.4) Mental confusion 7.7 (2.9) 6.2 (4.4) x.3 (3.8) 9.X (4.6) Depression (log) 0.77 (0.26) 0.58 (0.38) 0.63 (0.30) 0.60 (0.35) Mental fatigue 13.5 (4.7) 6.4 (4.2) I I .4 (X.0) 9.7 (6.1) Mental vigour 9.9 (4.4) 14.0 (4.0) X.3 (4.8) 10.8 (4.X) Anger (log) 0.92 (0.32) 0.86 (0.3 I ) 0.90 (0.13) 0.82 (0.29) Coping assets x.4 (4.5) 12.8 (4.2) 9.0 (4.2) 10.8 (4.1) Coping deficits 11.1 (4.3) 7.5 (3.8) 9.4 (4. I) X.6 (4.1) Physical wellbeing 7.2 (6.0) 13.4 (3.9) 6.3 (3.9) Il.5 (3.7) Trait anxiety 49.7 (11.2) 42.3 (11.5) 51.3 (8.9) 46.5 (9.1)
lo-
9.
$ = d
E 8 p”
7.
TENSION-ANXIETY
Exercise and anxiety
PSYCHOLOGICAL RESPONSE
MENTAL CONFUSION COPING ASSETS
‘Or 13r
9- / 12.
11 -
8
7- \
10.
g- k
543
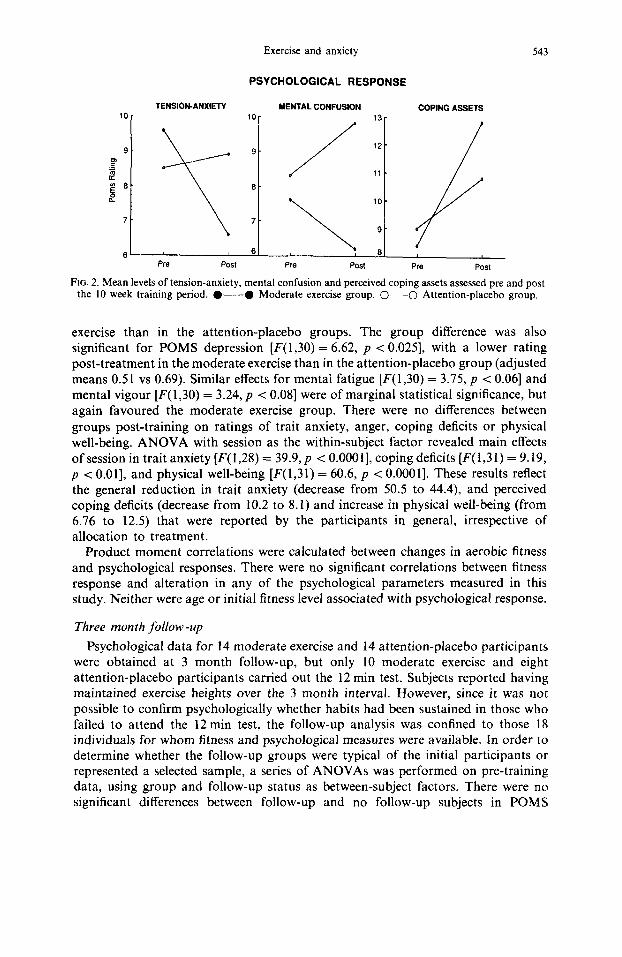
6’ , 6 ‘: *I f PW POSI PK3 Post Pr.3 Post
FIG. 2. Mean levels of tension-anxiety, mental confusion and perceived coping assets assessed pre and post the 10 week training period. O---O Moderate exercise group. O---O Attention-placebo group.
exercise than in the attention-placebo groups. The group difference was also significant for POMS depression [F(1,30) = 6.62, p < 0.0251, with a lower rating post-treatment in the moderate exercise than in the attention-placebo group (adjusted means 0.51 vs 0.69). Similar effects for mental fatigue [F(1,30) = 3.75, p < 0.061 and mental vigour [F( 1,30) = 3.24, p < 0.081 were of marginal statistical significance, but again favoured the moderate exercise group. There were no differences between
groups post-training on ratings of trait anxiety, anger, coping deficits or physical well-being. ANOVA with session as the within-subject factor revealed main effects of session in trait anxiety [F( 1,28) = 39.9, p < O.OOOl], coping deficits [F( I,3 1) = 9.19, p < 0.011, and physical well-being [F(1,31) = 60.6, p < O.OOOl]. These results reflect the general reduction in trait anxiety (decrease from 50.5 to 44.4) and perceived coping deficits (decrease from 10.2 to 8.1) and increase in physical well-being (from 6.76 to 12.5) that were reported by the participants in general, irrespective of allocation to treatment.
Product moment correlations were calculated between changes in aerobic fitness and psychological responses. There were no significant correlations between fitness response and alteration in any of the psychological parameters measured in this study. Neither were age or initial fitness level associated with psychological response.
Three month follow -up
Psychological data for 14 moderate exercise and 14 attention-placebo participants were obtained at 3 month follow-up, but only 10 moderate exercise and eight attention-placebo participants carried out the 12 min test. Subjects reported having maintained exercise heights over the 3 month interval. However, since it was not possible to confirm psychologically whether habits had been sustained in those who failed to attend the 12 min test, the follow-up analysis was confined to those 18 individuals for whom fitness and psychological measures were available. In order to determine whether the follow-up groups were typical of the initial participants or represented a selected sample, a series of ANOVAs was performed on pre-training data, using group and follow-up status as between-subject factors. There were no significant differences between follow-up and no follow-up subjects in POMS
544 ANDREW STEPTCJE ct al.
FITNESS RESPONSES - 12 MIN TEST
36
36
30
28 PR? Post Follow-up
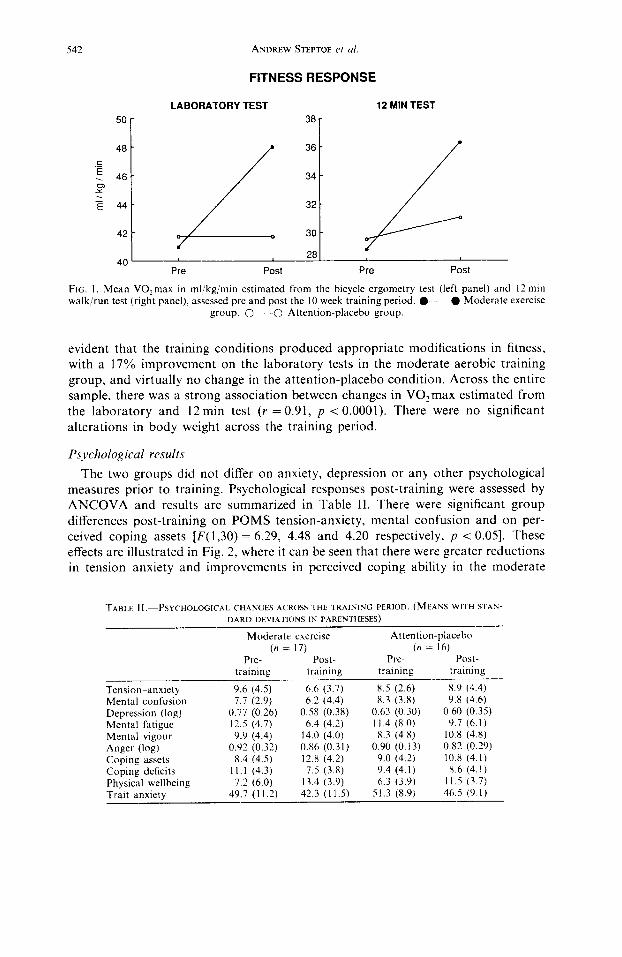
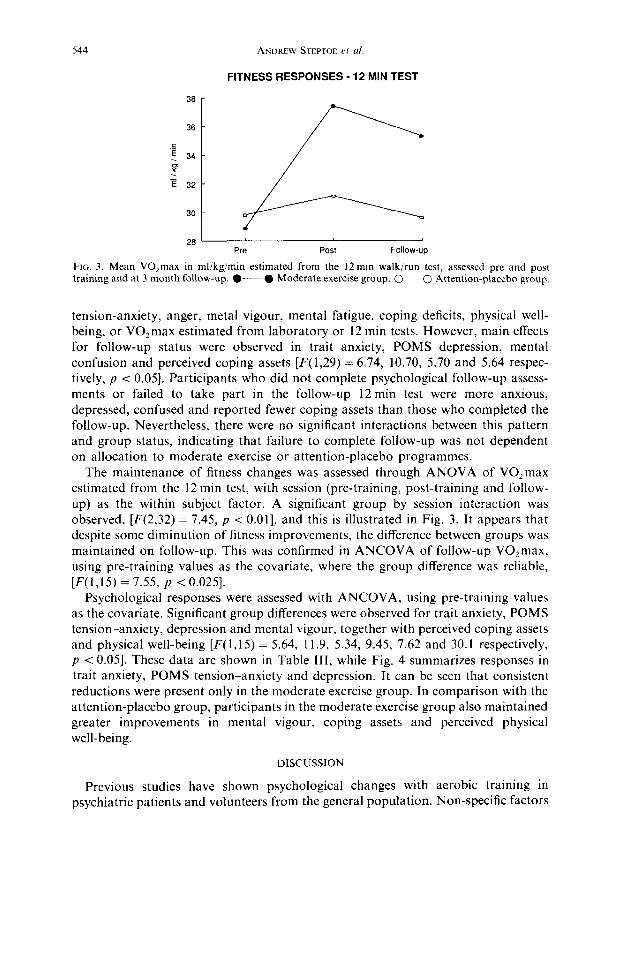
FIG. 3. Mean VOzmax in ml/kgjmin estimated from the 12 min walk/run test. assessed pre and post training and at 3 month follow-up. O---O Moderate exercise group. O~~P~~O Attention-placebo group.
tension-anxiety, anger, metal vigour, mental fatigue, coping deficits, physical well- being, or VO,max estimated from laboratory or 12 min tests. However, main effects for follow-up status were observed in trait anxiety, POMS depression, mental confusion and perceived coping assets [F(l,29) = 6.74, 10.70, 5.70 and 5.64 respec- tively, p < 0.051. Participants who did not complete psychological follow-up assess- ments or failed to take part in the follow-up 12 min test were more anxious, depressed, confused and reported fewer coping assets than those who completed the follow-up. Nevertheless, there were no significant interactions between this pattern and group status, indicating that failure to complete follow-up was not dependent on allocation to moderate exercise or attention-placebo programmes.
The maintenance of fitness changes was assessed through ANOVA of VO,max estimated from the 12 min test, with session (pre-training, post-training and follow- up) as the within subject factor. A significant group by session interaction was observed, [F(2,32) = 7.45, p < 0.011, and this is illustrated in Fig. 3. It appears that despite some diminution of fitness improvements, the difference between groups was maintained on follow-up. This was confirmed in ANCOVA of follow-up VOzmax, using pre-training values as the covariate, where the group difference was reliable, [F( 1,15) = 7.55, p < 0.0251.
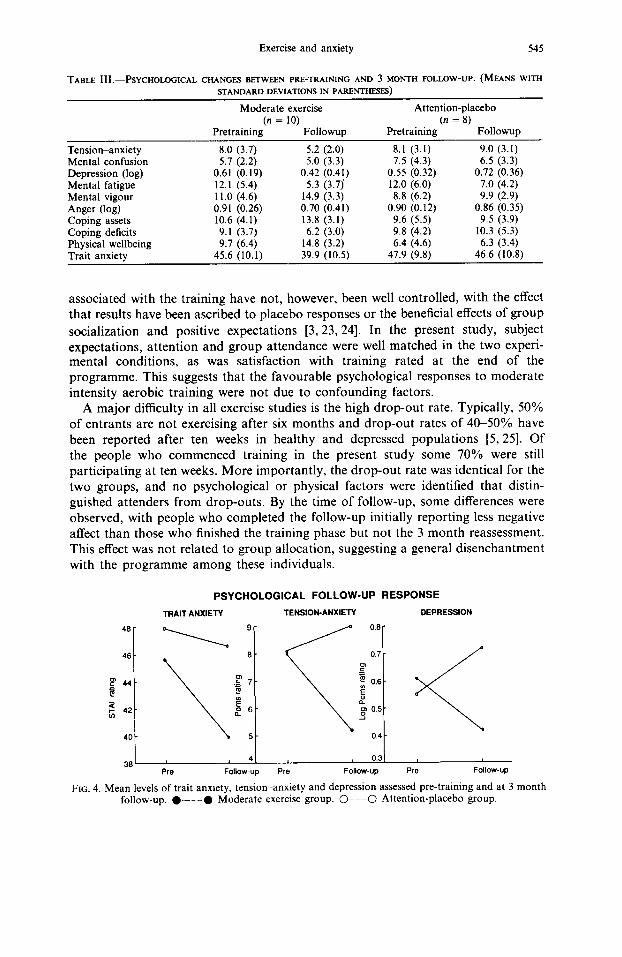
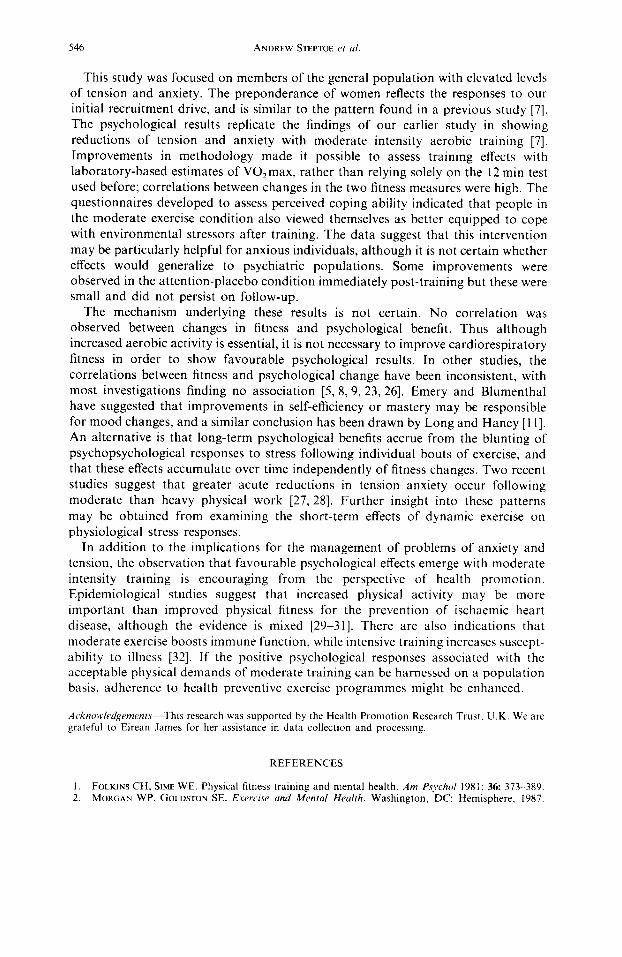
Psychological responses were assessed with ANCOVA, using pre-training values as the covariate. Significant group differences were observed for trait anxiety, POMS tension-anxiety, depression and mental vigour, together with perceived coping assets and physical well-being [F(l,l5) = 5.64, 11.9, 5.34, 9.45, 7.62 and 30.1 respectively, p < 0.051. These data are shown in Table III, while Fig. 4 summarizes responses in trait anxiety, POMS tension-anxiety and depression. It can be seen that consistent reductions were present only in the moderate exercise group. In comparison with the attention-placebo group, participants in the moderate exercise group also maintained greater improvements in mental vigour, coping assets and perceived physical well-being.
DISCUSSION
Previous studies have shown psychological changes with aerobic training in psychiatric patients and volunteers from the general population. Non-specific factors
Exercise and anxiety 545
TABLE III.-PSYCHOLOGICAL CHANGES BETWEEN PRE-TRAINING AND 3 MONTH FOLLOW-UP. (MEANS WITH
STANDARDDEVIATIONSINPARENTHE?5ES)
Moderate exercise
Pretraining(n = lo) Followup
Attention-placebo
Pretraining (’ = ‘) Followup
Tension-anxiety Mental confusion Depression (log) Mental fatigue Mental vigour Anger (log) Coping assets Coping deficits Physical wellbeing Trait anxietv
8.0 (3.7) 5.7 (2.2)
0.61 (0.19) 12.1 (5.4) 11.0 (4.6) 0.91 (0.26) 10.6 (4.1) 9.1 (3.7) 9.7 (6.4)
45.6 (10.1)
5.2 (2.0) 5.0 (3.3)
0.42 (0.41) 5.3 (3.7)
14.9 (3.3) 0.70 (0.41) 13.8 (3.1) 6.2 (3.0)
14.8 (3.2) 39.9 (10.5)
8.1 (3.1) 7.5 (4.3)
0.55 (0.32) 12.0 (6.0) 8.8 (6.2)
0.90 (0.12) 9.6 (5.5) 9.8 (4.2) 6.4 (4.6)
47.9 (9.8)
9.0 (3.1) 6.5 (3.3)
0.72 (0.36) 7.0 (4.2) 9.9 (2.9)
0.86 (0.35) 9.5 (3.9)
10.3 (5.3) 6.3 (3.4)
46.6 (10.8)
associated with the training have not, however, been well controlled, with the effect that results have been ascribed to placebo responses or the beneficial effects of group
socialization and positive expectations [3, 23,241. In the present study, subject expectations, attention and group attendance were well matched in the two experi- mental conditions, as was satisfaction with training rated at the end of the programme. This suggests that the favourable psychological responses to moderate intensity aerobic training were not due to confounding factors.
A major difficulty in all exercise studies is the high drop-out rate. Typically, 50% of entrants are not exercising after six months and drop-out rates of 4&50% have been reported after ten weeks in healthy and depressed populations [5,25]. Of the people who commenced training in the present study some 70% were still participating at ten weeks. More importantly, the drop-out rate was identical for the two groups, and no psychological or physical factors were identified that distin- guished attenders from drop-outs. By the time of follow-up, some differences were observed, with people who completed the follow-up initially reporting less negative affect than those who finished the training phase but not the 3 month reassessment. This effect was not related to group allocation, suggesting a general disenchantment with the programme among these individuals.
PSYCHOLOGICAL FOLLOW-UP RESPONSE
TRAIT ANXIETY TENSIOKANXIETY DEPRESSION
38 ( 4 , 0.3
PN3 Follow-up PW Follow-up PW Follow-up
FIG. 4. Mean levels of trait anxiety, tension-anxiety and depression assessed pre-training and at 3 month follow-up, l -e Moderate exercise group. O---O Attention-placebo group.
546 ANDREW QEPTOE et 01
This study was focused on members of the general population with elevated levels of tension and anxiety. The preponderance of women reflects the responses to our initial recruitment drive, and is similar to the pattern found in a previous study [7]. The psychological results replicate the findings of our earlier study in showing reductions of tension and anxiety with moderate intensity aerobic training [7]. Improvements in methodology made it possible to assess training effects with laboratory-based estimates of VOzmax, rather than relying solely on the 12 min test used before; correlations between changes in the two fitness measures were high. The questionnaires developed to assess perceived coping ability indicated that people in the moderate exercise condition also viewed themselves as better equipped to cope with environmental stressors after training. The data suggest that this intervention may be particularly helpful for anxious individuals, although it is not certain whether effects would generalize to psychiatric populations. Some improvements were observed in the attention-placebo condition immediately post-training but these were small and did not persist on follow-up.
The mechanism underlying these results is not certain. No correlation was observed between changes in fitness and psychological benefit. Thus although increased aerobic activity is essential, it is not necessary to improve cardiorespiratory fitness in order to show favourable psychological results. In other studies, the correlations between fitness and psychological change have been inconsistent, with most investigations finding no association [5, 8,9,23,26]. Emery and Blumenthal have suggested that improvements in self-efficiency or mastery may be responsible for mood changes, and a similar conclusion has been drawn by Long and Haney [ 1 I]. An alternative is that long-term psychological benefits accrue from the blunting of psychopsychological responses to stress following individual bouts of exercise, and that these effects accumulate over time independently of fitness changes. Two recent studies suggest that greater acute reductions in tension-anxiety occur following moderate than heavy physical work [27,28]. Further insight into these patterns may be obtained from examining the short-term effects of dynamic exercise on physiological stress responses.
In addition to the implications for the management of problems of anxiety and tension, the observation that favourable psychological effects emerge with moderate intensity training is encouraging from the perspective of health promotion. Epidemiological studies suggest that increased physical activity may be more important than improved physical fitness for the prevention of ischaemic heart disease, although the evidence is mixed [29%31]. There are also indications that moderate exercise boosts immune function, while intensive training increases suscept- ability to illness [32]. If the positive psychological responses associated with the acceptable physical demands of moderate training can be harnessed on a population basis, adherence to health preventive exercise programmes might be enhanced.
A[,knolr,/~d~rmenrs~This research was supported by the Health Promotion Research Trust. U.K. We are grateful to Eirean James for her assistance in data collection and processmg.
REFERENCES
1. FOLKINS CH, SIME WE. Physical fitness training and mental health. Am Psycho/ 1981; 36: 373- 389. 2. MORGAN WP. GOLDSTON SE. Exercise and Mental Healrh. Washington, DC: Hemisphere, 1987.
Exercise and anxiety 541
3.
4.
5.
6.
1.
8.
9.
10.
11.
12.
13.
14. 15.
16.
17. 18.
19.
20. 21. 22.
23.
24. 25.
26.
21. 28.
29.
30.
31.
32.
JASNOSKI MI, HOLMES DS, SOLOMON S, AG~JIAR C. Exercise, changes in aerobic capacity, and changes in self-perceptions: an experimental investigation. J Res Person 1981; 15: 46&466. MARTINSEN EW, MEDHUS A, SANDVIK L. Effect of aerobic exercise on depression: a controlled trial. Er med J 1985; 291: 109. DOYNE EJ, OSSIP-KLEIN DJ, BOWMAN ED, OSBORN KM, MCDOUGAI.L-WILSON IB, NEIMEYER RA. Running vs weight lifting in the treatment of depression. J consult c/in Psycho1 1987; 55: 748.--754. HUGHES JR. Psychological effects of habitual aerobic exercise: a critical review. Preuenf Med 1984: 13: 6678. MOSES J, STEPTOE A, MATHEWS A, EDWARDS S. The effects of exercise training on mental well-being in the normal population: a controlled trial. J psychosom Res 1989; 33: 47-61. E~~IERY CF, BLUMENTHAL JA. Effects of exercise training on psychological functioning in healthy Type A men. Psycho1 Hlth 1988; 2: 367-319. KING AC, TAYLOR CB, HASKELL WL, DEBUSK RF. The influence of regular aerobic exercise on psychological health: a randomised, controlled trial of healthy middle-aged adults. Health Psychol, in press. LONG BC. Aerobic conditioning and stress inoculation: a comparison of stress-management interventions. Cog Ther Res 1984; 8: 517-542. LANG BC, HARVEY CH. Coping strategies for working women: aerobic exercise and relaxation interventions. Behav. Ther 1988; 19: 75-83. ROTH DL, HOLMES DS. Influence of aerobic exercise training and relaxation training on physical and psychological health following stressful life events. Psychosom Med 1987; 49: 355.-365. SIMON CW, BIRKIMER JC. An exploration of factors predicting the effects of aerobic conditioning on mood state. J psychosom Res 1988; 32: 63-15. ZIGMOND AS, SNAITH RP. The Hospital Anxiety and Depression Scale. Acfa psych& 1983; 86: l-7. MCNAIR DM, LORR N, DROPPLEMAN LF. Manual for the Profile of Mood States. San Diego: Education and Industrial Testing Service, 1981. American College of Sports Medicine. Guidelines for Exercise Testing and Prescription, 3rd Edn. Philadelphia: Lea and Febiger, 1986. BORG GA. Psychophysical bases of perceived exertion. Med Sci Sports Exercise 1982; 14: 377-38 1. SPIELBERGER CD. Manual for the State-Trait Anxiety Inuenfory (Form Y). Palo Alto: Consulting Psychologists Press, 1983. SHAPIRO S, WEINBLAIT E, FRANK CW, SAGER RF. Study of incidence and prognosis of coronary heart disease. J chron Dis 1965; 18: 527-558. ASTRAND P-O, RODAHL K. Textbook of Work Physiology, 3rd Edn. New York: McGraw-Hill, 1986. COOPER KH. A means of assessing maximal oxygen intake. J Am med Ass 1968; 203: 135-138. DURNIN JVGA, WOMERSLEY J. Body fat assessed from total body density and its estimation from skinfold thickness: measurements on 481 men and women aged 1672 years. Er J Nut& 1984; 32: 71-79. HUGHES JR, CASAL DC, LEON AS. Psychological effects of exercise: a randomised crossover trial. J psychosom Res 1986; 30: 355-360. SOLOMON HA. The Exercise Myth. New York: Harcourt Brace Jovanovich, 1984. WARD A, MORGAN WP. Adherence patterns of healthy men and women enrolled in an adult exercise program. J cardiac Rehab 1984; 4: 143-152. JASNOSKI NL, HOLMES DS, BANKS DL. Changes in personality associated with changes in aerobic and anaerobic fitness in women and men. J psychosom Res 1988; 32: 273-276. STEPTOE A, Cox S. Acute effects of aerobic exercise on mood. Hlth Psychoi 1988; 7: 329-340. STEPTOE A, BOLTON J. The short-term influence of high and low intensity physical exercise on mood. Psycho1 Hlth 1988; 2: 91-106. LAPORTE RE, ADAMS LL, SAVAGE DD, BRENES G, DEARWATER S, C&K T. The spectrum of activity, cardiovascular disease and health: an epidemiologic perspective. Am J Epidemiol 1984; 120: 507-517. LEON AS, CONNETT J, JACOBS DR, RAURAMAA R. Leisure-time physical activity levels and risk of coronary heart disease and health. J. Am med Ass 1987; 258: 2388-2395. SOBOLSKI J, KONITZER M, DE BACKER G, DRAMAIX M, ABRAMOWICZ M, DEGRE S, DENOLIN H. Protection against ischaemic heart disease in the Belgium Physical Fitness Study: physical fitness rather than physical activity? Am J Epidemiol 1987; 125: 60-610. FITZGERALD L. Exercise and the immune system. Immunol Today 1988; 9: 337-339.
Related Documents











