Special Section: International Voices 2010 The Cultural Context of End-of-Life Ethics: A Comparison of Germany and Israel SILKE SCHICKTANZ, AVIAD RAZ, and CARMEL SHALEV End-of-life (EoL) decisions concerning euthanasia, stopping life-support ma- chines, or handling advance directives are very complex and highly disputed in industrialized, democratic countries. A main controversy is how to balance the patient’s autonomy and right to self-determination with the doctor’s duty to save life and the value of life as such. These EoL dilemmas are closely linked to legal, medical, religious, and bioethical discourses. In this paper, we examine and deconstruct these linkages in Germany and Israel, moving beyond one- dimensional constructions of ethical statements as ‘‘social facts’’ to their conflict- ing and multifaceted embedding within professional, religious, and cultural perspectives. 1 Why Compare Germany and Israel? Germany and Israel constitute opposing examples of professional culture in relation to biomedicine, especially in all questions pertaining to the beginning of life. By adding to this comparison a new focus on end-of-life biomedical dilemmas, several new insights can be gained. First, so far the bioethical comparison between Germany and Israel has generally shown Germany to be more restrictive and Israel to be more per- missive. Various studies have shown that German and Israeli professionals, such as genetic counselors, ethicists, and physicians, differ strongly in their moral assessment of various biomedical issues including preimplantation and prenatal genetic diagnosis (PND), stem cell research, and elective abortion. German geneticists expressed extreme caution regarding the use of PND for selective abortion, whereas Israeli geneticists advocated it. 2 Israeli law allows eugenic abortions, even after viability (under certain administrative restrictions), whereas the latest version of the German Criminal Law under which abortion is regulated does not allow them. 3 Does the same opposition also characterize EoL ethics in both countries? On the face of it, German and Israeli bioethical statements concerning EoL dilemmas stand in stark contrast to previous comparisons, as in this context Germany appears to be more permissive and Israel more restrictive. Second, because Germany and Israel have been shown to constitute such professional opposites, their juxtaposition is expected to highlight the context of cultural variation and pluralism in the moral assessment and evaluation of EoL dilemmas. Such differences are often attributed to the prevalent religions in each country. In the case of biomedical dilemmas pertaining to the beginning of life, the differences between Germany and Israel are often attributed to Christian versus Jewish positions toward the moral status of the embryo. Similarly, Judaism and Christianity are also expected to provide opposing influences on national Cambridge Quarterly of Healthcare Ethics (2010), 19, 381–394. Ó Cambridge University Press, 2010. 0963-1801/10 $20/00 doi:10.1017/S0963180110000162 381

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Special Section: International Voices 2010
The Cultural Context of End-of-Life Ethics:A Comparison of Germany and Israel
SILKE SCHICKTANZ, AVIAD RAZ, and CARMEL SHALEV
End-of-life (EoL) decisions concerning euthanasia, stopping life-support ma-chines, or handling advance directives are very complex and highly disputed inindustrialized, democratic countries. A main controversy is how to balance thepatient’s autonomy and right to self-determination with the doctor’s duty to savelife and the value of life as such. These EoL dilemmas are closely linked to legal,medical, religious, and bioethical discourses. In this paper, we examine anddeconstruct these linkages in Germany and Israel, moving beyond one-dimensional constructions of ethical statements as ‘‘social facts’’ to their conflict-ing and multifaceted embedding within professional, religious, and culturalperspectives.1
Why Compare Germany and Israel?
Germany and Israel constitute opposing examples of professional culture inrelation to biomedicine, especially in all questions pertaining to the beginning oflife. By adding to this comparison a new focus on end-of-life biomedicaldilemmas, several new insights can be gained.
First, so far the bioethical comparison between Germany and Israel hasgenerally shown Germany to be more restrictive and Israel to be more per-missive. Various studies have shown that German and Israeli professionals, suchas genetic counselors, ethicists, and physicians, differ strongly in their moralassessment of various biomedical issues including preimplantation and prenatalgenetic diagnosis (PND), stem cell research, and elective abortion. Germangeneticists expressed extreme caution regarding the use of PND for selectiveabortion, whereas Israeli geneticists advocated it.2 Israeli law allows eugenicabortions, even after viability (under certain administrative restrictions), whereasthe latest version of the German Criminal Law under which abortion is regulateddoes not allow them.3 Does the same opposition also characterize EoL ethics inboth countries? On the face of it, German and Israeli bioethical statementsconcerning EoL dilemmas stand in stark contrast to previous comparisons, as inthis context Germany appears to be more permissive and Israel more restrictive.
Second, because Germany and Israel have been shown to constitute suchprofessional opposites, their juxtaposition is expected to highlight the context ofcultural variation and pluralism in the moral assessment and evaluation of EoLdilemmas. Such differences are often attributed to the prevalent religions in eachcountry. In the case of biomedical dilemmas pertaining to the beginning of life,the differences between Germany and Israel are often attributed to Christianversus Jewish positions toward the moral status of the embryo. Similarly, Judaismand Christianity are also expected to provide opposing influences on national
Cambridge Quarterly of Healthcare Ethics (2010), 19, 381–394.� Cambridge University Press, 2010. 0963-1801/10 $20/00doi:10.1017/S0963180110000162 381

positions in Israel and Germany concerning EoL dilemmas.4 For example, theCatholic Church allows both withholding and withdrawing of futile EoL therapy if itis burdensome, although active euthanasia is never allowed, and palliative care is tobe offered. The Evangelical Lutheran church in Germany has developed advancedirectives for EoL choices but similarly rejects active euthanasia. Jewish law (halacha)differentiates between active and passive euthanasia and does not allow thewithdrawal of life-support measures. As in Christianity, active euthanasia orphysician-assisted suicide is prohibited in Judaism, even if the patient has requestedit. However, rather than separating the religious influences, we ask how thesereligious differences have shaped and been assimilated into the multifaceted culturalcontext underlying the national discourse and the law in Germany and Israel.
Third, another important point of reference for bioethical analyses of theGerman–Israeli juxtaposition is the Holocaust and the role of the medical systemduring the Nazi regime. Especially in the German EoL debate, the holocaust andthe ‘‘Nazi doctors’’ have played an enormous argumentative role.5 Contempo-rary discussions of EoL treatment and advance directives that mention the termeuthanasia are therefore difficult to accept because of the association of this termwith the Nazis. The German National Ethics Council introduced the term criminaleuthanasia to classify this murdering under the more general label of euthanasia(which literally means ‘‘good death’’), internationally used to denote mercykilling or killing on request. Moreover, the experience of the political instrumen-talization of medical experts as well as the impact of sociobiological and racistideologies on medical practice are often raised in the German discourse ashistorical evidence for sustaining slippery slope arguments. Interestingly, theattitudes of Israeli Holocaust survivors concerning euthanasia were found to beopposed to those of German professionals. Israeli Holocaust survivors arguedthat profound differences existed between Nazi Germany practices and sociallyassisted dying. They saw the latter, in contrast to the Holocaust, as somethingthat can be morally and ethically justified and therefore cautioned againstcomparisons between the Holocaust and other human behaviors.6 We thereforeask how the historical background of the Holocaust affects the cultural in-terpretation of euthanasia as part of EoL dilemmas in Germany and Israel.
Methods
A comparative investigation of the ethical debate on EoL decisions in Israel andGermany has not been done before. In this study, we focus on the expertdiscourse of two national ethics committees, both found in a politically powerfulposition. We compare, on the one hand, the 2002 Israeli Report of the PublicCommittee on the Care of Dying Patients (the so-called Steinberg Committee)7 withthe 2006 German National Ethics Council’s Opinion Report on Self-Determination andCare at the End of Life.8 Our analysis here concentrates on these official statementsalong the following research questions: (a) What are the main ethical principlesmentioned? (b) What are the main problems identified? (c) What role do culturaland historical factors play? By deconstructing each of the statements, exposingthe basic elements of their discourses, and comparing them cross-culturally, thismethodology aims at uncovering the embedding of ethics within multifacetedand conflicting cultural narratives. In such a manner, we offer a subversiveanalysis of ethical declarations as presenting an illusion of being monolithic and
Silke Schicktanz, Aviad Raz, and Carmel Shalev
382

consensual ‘‘social facts.’’9 Our analysis concentrates on differences regardingactive and passive euthanasia, decisionmaking processes, and normative justifi-cations.
The German National Ethics Council (NEC) was appointed by the Germanchancellor Gerhard Schroder in 2001 with the general mandate to discuss urgentbioethical issues and to advise the chancellor, the Parliament, and the public. TheIsraeli committee was appointed by the minister of health, Shlomo Benezri, in2000 with the specific mandate to propose legislation on EoL medical care.Whereas the German NEC is constructed as a long-term institution (now undera law also regularly adopted by the German Parliament in 2007 and renamed theGerman Ethics Council with a new list of members), the Israeli committee wasestablished as an ad hoc committee with the mandate to discuss the issue of endof life and to develop a bill. At the end of 2005, the bill proposed by the Steinbergcommittee was adopted by the Knesset without major revision.
Both committees were comprised of an interdisciplinary membership. At thetime of its EoL report, the German Committee consisted of 25 members (pro-fessional philosophers, lawyers, medical scientists, patient representatives, pol-iticians, and Catholic and Protestant religious authorities) and was chaired by thelawyer and politician Christiane Weber-Hassemer. The Israeli Committee con-sisted of 59 expert members, making it the largest public committee ever es-tablished in Israel, and it was chaired by the pediatric neurologist and halakhicmedical ethicist Avraham Steinberg.10 Both national committees aimed for a finalconsensus statement that was achieved in the main part, but both also offer somedissenting statements.
Results and Discussion: Comparative Analysis of the Statements
Legal Backgrounds
In both countries, to the date of the reports no specific law existed. However, inIsrael, there were Ministry of Health guidelines (1996) and the Patient Rights Law(1996) and several court decisions that indicated recognition of certain legalprinciples (e.g., the patient’s right to refuse treatment, the prohibition of activeeuthanasia, in dubio pro vitae).11 In Germany, there existed sections in the criminallaw that were relevant to end-of-life decisions as well as articles in theConstitution, such as Article 1, which protects the individual right to life andphysical integrity, and Article 2(2), which protects the right to free developmentof the personality and was construed to include autonomous decisions inshaping the dying process. Likewise, the predominant view in Germany wasthat suicide falls within the purview of freedom of action (Article 2 (1)); there isno obligation for citizens to stay alive because the individual takes precedenceover the state.12 However, there remained considerable legal questions about thedoctor’s role as a guarantor of life and a large degree of ambivalence as regardsthe doctor’s duties.
Main Similarities and Differences
The main recommendations in both expert statements can be summarized withrespect to their similar articulation of the following five points:
End-of-Life Ethics in Germany and Israel
383

d There is a duty to administer palliative care, which is understood as theappropriate treatment for patients in an EoL stage to relieve associated painand suffering.
d There is duty to administer basic care, which includes hygiene, social care,and treatment, to assuage feelings of starving and of thirst.
d Killing on request (so called active euthanasia) should be legally forbidden.d Both statements clearly state that no doctors or other persons should be
allowed to kill a patient (e.g., by applying a deadly dose of a substance), evenon the patient’s voiced wish.
d In case of doubt or uncertainty about the patient’s will, a decision in favor oflife ought to be made: In the absence of an explicit statement or advancedirective by the patient, and if the relatives seem to be unclear orcontradictory as to the patient’s presumed wishes, physicians and caregiversshould preserve life and not stop life-sustaining care.
Despite these similarities, the two reports differ in two major respects. The firstdiscrepancy concerns the moral acceptance of letting die (synonymously used for‘‘passive euthanasia’’). In the German report, a strong consensus is expressed that‘‘letting die’’ encompasses both forms of withholding and withdrawing medicaltreatment. As long as letting die is in accordance with the patient’s explicit wish,the NEC supported it. In contrast, the Israeli report stands out from mostinternational reports and laws by stressing that there is a significant distinctionbetween interrupting (withdrawing) and refraining from (withholding) medicaltreatment, because of psychological, philosophical, and religious (halakhic) aspectsassociated with the former. Hence, the report concludes, withholding or refrainingfrom any kind of medical treatment is morally acceptable if in accordance with thepatient’s explicit voiced wish. However, interrupting a continuous treatment suchas artificial respiration or artificial feeding is seen as morally unacceptable even ifthe patient so wishes. At the same time, the commentary of the Israeli reportsuggests a compromise in the form of a technical device, such as a timer, that couldtransform a continuous treatment into a discontinuous one (like medication,dialysis, chemotherapy, etc.) and by which each cycle of treatment may be regardedas a new procedure that can be withheld (see below).
The second interesting divergence between the reports concerns the discussionand conclusion about physician-assisted suicide (e.g., by prescribing a deadlydose of a poison). The Israeli expert committee expressed a strong consensus thatassisted suicide is morally unacceptable and should be legally forbidden. Incontrast, the German expert committee did not reach a consensus on this issue. Itformulated two positions: the one morally condemning assisted suicide becauseof apparently religious reasons and the other expressing a liberal empathy forpatients who want to control their own death by committing suicide.
Cultural Diversity of Moral Key Elements in the Argumentation
The main ethical principles that served as presumptions in the reports aresummarized in Table 1. It is noteworthy that balancing between various,sometimes opposing values seems to be the key element in EoL decisionsaccording to both committees’ statements. Value balancing entails a twofoldproblem: First, one has to justify the main ethical principles; second, some
Silke Schicktanz, Aviad Raz, and Carmel Shalev
384
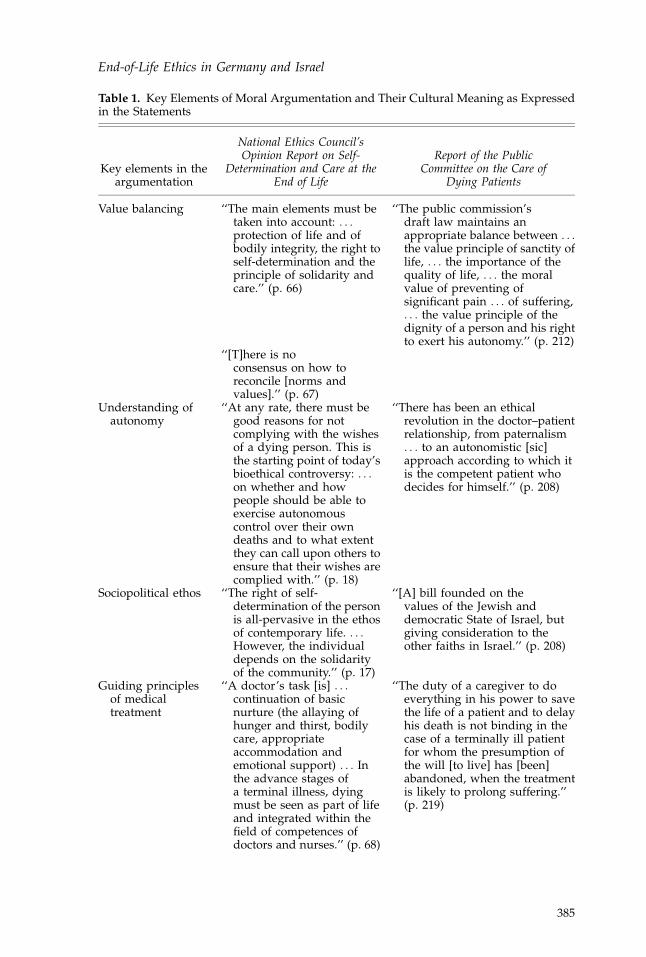
Table 1. Key Elements of Moral Argumentation and Their Cultural Meaning as Expressedin the Statements
Key elements in theargumentation
National Ethics Council’sOpinion Report on Self-
Determination and Care at theEnd of Life
Report of the PublicCommittee on the Care of
Dying Patients
Value balancing ‘‘The main elements must betaken into account: . . .protection of life and ofbodily integrity, the right toself-determination and theprinciple of solidarity andcare.’’ (p. 66)
‘‘The public commission’sdraft law maintains anappropriate balance between . . .the value principle of sanctity oflife, . . . the importance of thequality of life, . . . the moralvalue of preventing ofsignificant pain . . . of suffering,. . . the value principle of thedignity of a person and his rightto exert his autonomy.’’ (p. 212)
‘‘[T]here is noconsensus on how toreconcile [norms andvalues].’’ (p. 67)
Understanding ofautonomy
‘‘At any rate, there must begood reasons for notcomplying with the wishesof a dying person. This isthe starting point of today’sbioethical controversy: . . .on whether and howpeople should be able toexercise autonomouscontrol over their owndeaths and to what extentthey can call upon others toensure that their wishes arecomplied with.’’ (p. 18)
‘‘There has been an ethicalrevolution in the doctor–patientrelationship, from paternalism. . . to an autonomistic [sic]approach according to which itis the competent patient whodecides for himself.’’ (p. 208)
Sociopolitical ethos ‘‘The right of self-determination of the personis all-pervasive in the ethosof contemporary life. . . .However, the individualdepends on the solidarityof the community.’’ (p. 17)
‘‘[A] bill founded on thevalues of the Jewish anddemocratic State of Israel, butgiving consideration to theother faiths in Israel.’’ (p. 208)
Guiding principlesof medicaltreatment
‘‘A doctor’s task [is] . . .continuation of basicnurture (the allaying ofhunger and thirst, bodilycare, appropriateaccommodation andemotional support) . . . Inthe advance stages ofa terminal illness, dyingmust be seen as part of lifeand integrated within thefield of competences ofdoctors and nurses.’’ (p. 68)
‘‘The duty of a caregiver to doeverything in his power to savethe life of a patient and to delayhis death is not binding in thecase of a terminally ill patientfor whom the presumption ofthe will [to live] has [been]abandoned, when the treatmentis likely to prolong suffering.’’(p. 219)
End-of-Life Ethics in Germany and Israel
385
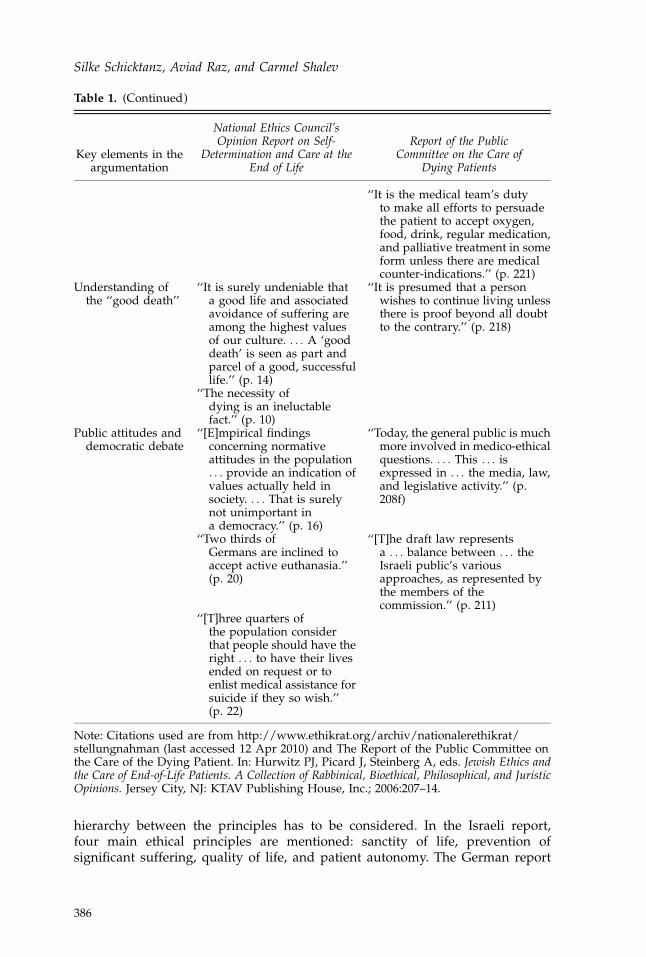
hierarchy between the principles has to be considered. In the Israeli report,four main ethical principles are mentioned: sanctity of life, prevention ofsignificant suffering, quality of life, and patient autonomy. The German report
Table 1. (Continued)
Key elements in theargumentation
National Ethics Council’sOpinion Report on Self-
Determination and Care at theEnd of Life
Report of the PublicCommittee on the Care of
Dying Patients
‘‘It is the medical team’s dutyto make all efforts to persuadethe patient to accept oxygen,food, drink, regular medication,and palliative treatment in someform unless there are medicalcounter-indications.’’ (p. 221)
Understanding ofthe ‘‘good death’’
‘‘It is surely undeniable thata good life and associatedavoidance of suffering areamong the highest valuesof our culture. . . . A ‘gooddeath’ is seen as part andparcel of a good, successfullife.’’ (p. 14)
‘‘It is presumed that a personwishes to continue living unlessthere is proof beyond all doubtto the contrary.’’ (p. 218)
‘‘The necessity ofdying is an ineluctablefact.’’ (p. 10)
Public attitudes anddemocratic debate
‘‘[E]mpirical findingsconcerning normativeattitudes in the population. . . provide an indication ofvalues actually held insociety. . . . That is surelynot unimportant ina democracy.’’ (p. 16)
‘‘Today, the general public is muchmore involved in medico-ethicalquestions. . . . This . . . isexpressed in . . . the media, law,and legislative activity.’’ (p.208f)
‘‘Two thirds ofGermans are inclined toaccept active euthanasia.’’(p. 20)
‘‘[T]he draft law representsa . . . balance between . . . theIsraeli public’s variousapproaches, as represented bythe members of thecommission.’’ (p. 211)
‘‘[T]hree quarters ofthe population considerthat people should have theright . . . to have their livesended on request or toenlist medical assistance forsuicide if they so wish.’’(p. 22)
Note: Citations used are from http://www.ethikrat.org/archiv/nationalerethikrat/stellungnahman (last accessed 12 Apr 2010) and The Report of the Public Committee onthe Care of the Dying Patient. In: Hurwitz PJ, Picard J, Steinberg A, eds. Jewish Ethics andthe Care of End-of-Life Patients. A Collection of Rabbinical, Bioethical, Philosophical, and JuristicOpinions. Jersey City, NJ: KTAV Publishing House, Inc.; 2006:207–14.
Silke Schicktanz, Aviad Raz, and Carmel Shalev
386
refers to self-determination and protecting bodily integrity as part of patientautonomy, then protection of life, and solidarity with vulnerable persons.However, ‘‘protection of life’’ as opposed to ‘‘sanctity of life’’ has a less religiousand less absolute connotation. Obviously, the German committee ranks the rightof self-determination higher than the other principles because it is understood asthe ethos of contemporary life. In contrast, the Israeli report starts with a generalpresumption that autonomy, as the democratic value, has to be balanced withother, Jewish religious values—of which ‘‘sanctity of life’’ is the most importantone. This can be demonstrated by the nonliberal (socially prescriptive)recommendation of the Israeli committee that caregivers have a duty not towithdraw medical treatment and to persuade patients to accept oxygen, food,drink, and regular medicine.
The Role of Individual and Social Decisionmaking Processes
Furthermore, we examine what is identified by each committee as the reason forethical discussion and legal change. Both statements start with the observationthat recent progress in medical technology to prolong life can become a burden ifthere is no improvement of quality of life and alleviation of suffering for thepatient. But there are interesting differences in the subsequent discussions.
According to the German report, death remains a very individualized event,although nowadays 90% of Germans die in hospitals or nursing homes. It isimportant to note that the German report stresses that the idea of having controlover one’s death is embedded in German society. Nearly half of the report consistsof the summary of already existing opinion polls and quantitative surveysconcerning public attitudes toward EoL decisions (while in Israel, notably, therehas not been any significant such public deliberation). The German report also usesthe case of suicide as a moral reference for several arguments; for example, ifsuicide (without any assistance) is deemed immoral, positions toward letting dieand assisted suicide will also be negative. In the end, the German NEC does notcome to a consensus but shows dissent on this question: One view morallycondemns suicide in general (while sympathizing with individual situations),referring in particular to Christian religious argumentation. The other view under-stands the suicide of a mentally capable person who is terminally ill as morallylegitimate so long as it is an ultima ratio. In contrast, the Israeli statement does notreport a controversy in its deliberation concerning the moral and legal acceptance ofsuicide, presenting instead a strong consensus in condemning suicide.
The role of experts represents a key element in both committees. The Israelireport delegates the responsibility for conflict resolution to medical and health-care experts. Local, institutional ethics expert committees should moderate andalso decide in conflicting situations between the involved parties. In the case ofunresolved dissent in the institutional ethics committee, a national committeeshould be authorized to decide. On the same issue, a debate developed in theGerman committee, although its report generally remains imprecise regardingwho should balance the norms and values. The answer can be found in anotherOpinion Report of the German NEC on advance directives, where they state thatin the event of conflict—in particular concerning the interpretation of the advancedirective—the Court of Guardianship should decide. Hence, the cultural alloca-tion of expert responsibility is quite different: In Israel healthcare experts are seen
End-of-Life Ethics in Germany and Israel
387
as best equipped to solve EoL dilemmas, whereas in Germany decisionmakingpower is put in the hands of legal experts. This is reflected also in the expertise ofthe two heads of the respective committees: in Germany, a lawyer-philosopher; inIsrael a physician-cleric.
Religious and Historical Factors
In addition to the two above mentioned parameters, the cultural diversity of theethical statements under study is also influenced by religion and history (seeTable 2). The influence of religion can be seen in the discussions about thedistinction between withholding and withdrawing treatment (passive and activeeuthanasia). This distinction was the subject of fierce controversy in the in-ternational bioethics community, especially until the mid-1990s.13 However, mostinternational statements on passive euthanasia nowadays agree that there is nosubstantial moral or legal distinction between the two, in light of consequentialistand intentional considerations. Correspondingly, the German Report emphasizesthat there is no morally relevant distinction between removing a continuingmedical treatment or not applying it. The examples mentioned are artificialfeeding and respiration. The NEC report concludes that the morally relevantaction is the omission of unwanted treatment, although it acknowledges that it is‘‘psychologically understandable if the doctor . . . is more reluctant to interveneactively—by removing a feeding tube or turning off a respirator—than simply donothing.’’14 According to it, the intention and outcome of the action are what ismorally relevant, so the distinction between actively doing and omitting was seenas inherently unjustified.
In contrast, the moral distinction between withholding and withdrawingplayed an important role in the Israeli report. The supporting argument isexplained by the Chair Steinberg: ‘‘According to relevant halakhic principles and theactual rulings of these prominent rabbis, preserving life is one of the most importantvalues, but it is not an infinitive or an absolute value. Any act that shortens life ishalakhically considered as murder, even at the very end of life. . . . Therefore, activeeuthanasia, physician-assisted suicide or the withdrawal of a continuous treatmentsuch as a pacemaker or a respirator is absolutely forbidden.’’15
This argumentation leads to a novel distinction on the level of technology (asopposed to the level of action theory about doing and allowing): a distinctionbetween ‘‘continuous’’ and ‘‘discontinuous, serial’’ treatment. This distinction isbased on the idea that medical treatment can be seen as either one act ora sequence of acts: For example, the administration of dialysis is seen asa sequence of single, equivalent acts, whereas artificial respiration over severalmonths is seen as only one act.
As Ravitsky—a bioethicist and a member of the Steinberg committee—hascommented, this moral distinction was criticized by various (secular) ethicistsand lawyers as unethical and inconsistent with the previous case law.16 Judges,legal scholars, and philosophers maintained that there was no logical differencebetween such omission or action in accordance with the international agreement.From a patients’ rights perspective, it was argued that just as informed consent isrequired before the administration of medical treatment, so too treatment maynot be continued against the will of the patient, because in both cases the forcedtreatment is a violation of the right to bodily integrity and amounts technically to
Silke Schicktanz, Aviad Raz, and Carmel Shalev
388
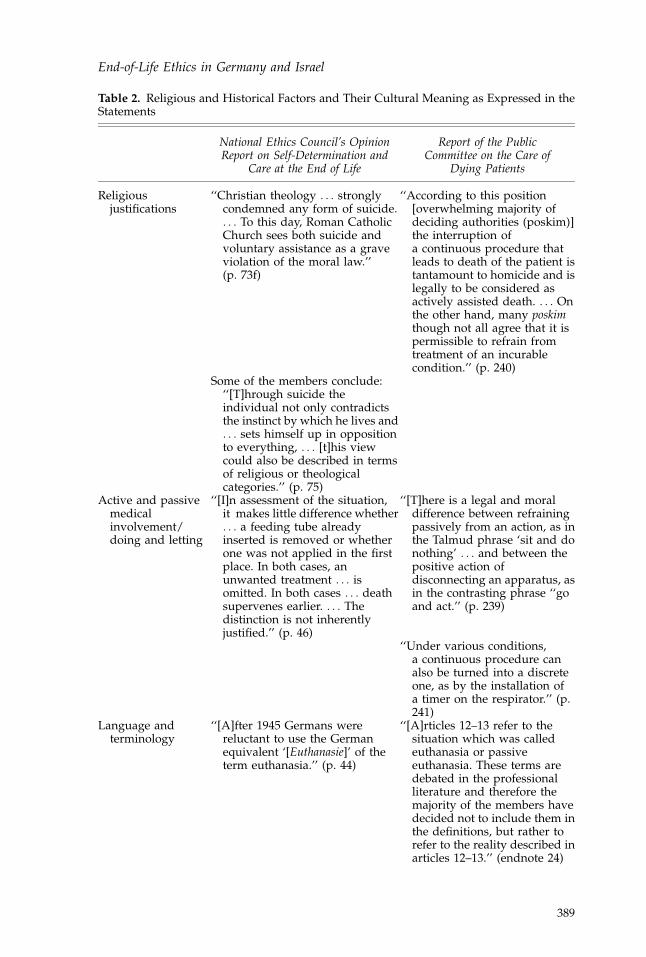
Table 2. Religious and Historical Factors and Their Cultural Meaning as Expressed in theStatements
National Ethics Council’s OpinionReport on Self-Determination and
Care at the End of Life
Report of the PublicCommittee on the Care of
Dying Patients
Religiousjustifications
‘‘Christian theology . . . stronglycondemned any form of suicide.. . . To this day, Roman CatholicChurch sees both suicide andvoluntary assistance as a graveviolation of the moral law.’’(p. 73f)
‘‘According to this position[overwhelming majority ofdeciding authorities (poskim)]the interruption ofa continuous procedure thatleads to death of the patient istantamount to homicide and islegally to be considered asactively assisted death. . . . Onthe other hand, many poskimthough not all agree that it ispermissible to refrain fromtreatment of an incurablecondition.’’ (p. 240)
Some of the members conclude:‘‘[T]hrough suicide theindividual not only contradictsthe instinct by which he lives and. . . sets himself up in oppositionto everything, . . . [t]his viewcould also be described in termsof religious or theologicalcategories.’’ (p. 75)
Active and passivemedicalinvolvement/doing and letting
‘‘[I]n assessment of the situation,it makes little difference whether. . . a feeding tube alreadyinserted is removed or whetherone was not applied in the firstplace. In both cases, anunwanted treatment . . . isomitted. In both cases . . . deathsupervenes earlier. . . . Thedistinction is not inherentlyjustified.’’ (p. 46)
‘‘[T]here is a legal and moraldifference between refrainingpassively from an action, as inthe Talmud phrase ‘sit and donothing’ . . . and between thepositive action ofdisconnecting an apparatus, asin the contrasting phrase ‘‘goand act.’’ (p. 239)
‘‘Under various conditions,a continuous procedure canalso be turned into a discreteone, as by the installation ofa timer on the respirator.’’ (p.241)
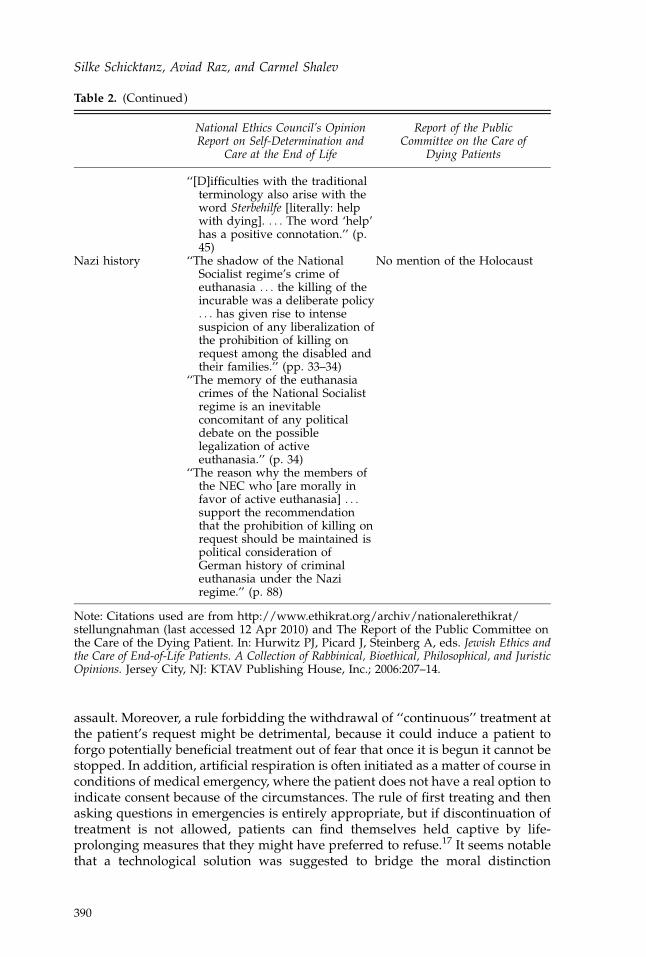
Language andterminology
‘‘[A]fter 1945 Germans werereluctant to use the Germanequivalent ‘[Euthanasie]’ of theterm euthanasia.’’ (p. 44)
‘‘[A]rticles 12–13 refer to thesituation which was calledeuthanasia or passiveeuthanasia. These terms aredebated in the professionalliterature and therefore themajority of the members havedecided not to include them inthe definitions, but rather torefer to the reality described inarticles 12–13.’’ (endnote 24)
End-of-Life Ethics in Germany and Israel
389
assault. Moreover, a rule forbidding the withdrawal of ‘‘continuous’’ treatment atthe patient’s request might be detrimental, because it could induce a patient toforgo potentially beneficial treatment out of fear that once it is begun it cannot bestopped. In addition, artificial respiration is often initiated as a matter of course inconditions of medical emergency, where the patient does not have a real option toindicate consent because of the circumstances. The rule of first treating and thenasking questions in emergencies is entirely appropriate, but if discontinuation oftreatment is not allowed, patients can find themselves held captive by life-prolonging measures that they might have preferred to refuse.17 It seems notablethat a technological solution was suggested to bridge the moral distinction
Table 2. (Continued)
National Ethics Council’s OpinionReport on Self-Determination and
Care at the End of Life
Report of the PublicCommittee on the Care of
Dying Patients
‘‘[D]ifficulties with the traditionalterminology also arise with theword Sterbehilfe [literally: helpwith dying]. . . . The word ‘help’has a positive connotation.’’ (p.45)
Nazi history ‘‘The shadow of the NationalSocialist regime’s crime ofeuthanasia . . . the killing of theincurable was a deliberate policy. . . has given rise to intensesuspicion of any liberalization ofthe prohibition of killing onrequest among the disabled andtheir families.’’ (pp. 33–34)
No mention of the Holocaust
‘‘The memory of the euthanasiacrimes of the National Socialistregime is an inevitableconcomitant of any politicaldebate on the possiblelegalization of activeeuthanasia.’’ (p. 34)
‘‘The reason why the members ofthe NEC who [are morally infavor of active euthanasia] . . .support the recommendationthat the prohibition of killing onrequest should be maintained ispolitical consideration ofGerman history of criminaleuthanasia under the Naziregime.’’ (p. 88)
Note: Citations used are from http://www.ethikrat.org/archiv/nationalerethikrat/stellungnahman (last accessed 12 Apr 2010) and The Report of the Public Committee onthe Care of the Dying Patient. In: Hurwitz PJ, Picard J, Steinberg A, eds. Jewish Ethics andthe Care of End-of-Life Patients. A Collection of Rabbinical, Bioethical, Philosophical, and JuristicOpinions. Jersey City, NJ: KTAV Publishing House, Inc.; 2006:207–14.
Silke Schicktanz, Aviad Raz, and Carmel Shalev
390

between continuous and serial treatment.18 The reliance on a technologicalsolution could be explained in the broader context of the Israeli–Jewish affinitytoward science and technology, if one considers the Jewish use of timers in orderto bypass the laws of the Sabbath.19 The solution, used to contrive a consensusbetween secular and religious parts of the committee, was the installation ofa timer on a respiratory machine, which automatically switches off the respiratorevery day or so and has to be intentionally turned on by someone again. Thisresetting of the clock would be routine care unless patients explicitly expresstheir wish not to turn it on again. Such technology may be very useful forovercoming the understandable reluctance to pull the plug, but it raises variousquestions. For example, if it is morally wrong to discontinue life support, whatdifference does it make how we perform the act? Secular lawyers and ethicistsasked whether a change of technique can make right something that is wrong.
Toward the end of the Steinberg committee report, under the section entitled‘‘reservations,’’ several committee members expressed a minority view that thedistinction between continuous and discontinuous treatment had no legal orethical justification and should be abolished in order to allow the cessation ofmedical treatment in both cases. These members primarily represented the liberaland secular perspective of legal bioethics experts (Professor Amos Shapira,Justice Moshe Talgam, Dr. Carmel Shalev, Attorney Na’ama Wieczener), as wellas one medical expert (Professor Avinoam Reches). This unresolved tensionbetween the onstage presentation of a broad consensus and backstage reserva-tions illustrates the impact of religion on the Jewish–Israeli bioethics discourse. Itwas the Jewish Orthodox view that defined the major problem (withholding vs.withdrawing treatment) and also proffered the practical solution (the timer). Themajority in the Israeli committee accepted this perspective and strove fora consensus even at the cost of liberal principles.
Whereas religious considerations played a central role in the Israeli debate, theinfluence of historical considerations came up only in the German NEC, when itsmembers discussed the ethical and social dimension of killing on request. Thosemembers of the NEC who considered killing on request as ethically acceptablenevertheless supported the recommendation that it should be kept legally for-bidden because of political considerations. These considerations could be de-scribed as taking historical responsibility for the criminal euthanasia practicedunder the Nazi regime. In the Israeli report we cannot find any comparableexpression or reference.
Conclusions
People in Germany and Israel have a wide range of views concerning EoLdecisions. However, a comparison of the two expert committees shows system-atic differences that could be explained by a culturally sensitive analysis.Compared to its general permissiveness in the beginning-of-life discourse, theIsraeli view on EoL was found to be much more restrictive. This contrast betweenthe beginning and end of life could be explained by a twofold view thatcharacterizes Israeli society,20 namely, that there is a separation between the preborn(i.e., the moral status of the embryo is acquired gradually) and the already born (fullmoral status), whereas in Germany, full moral status is already attributed to thehuman embryo from the moment of conception. The relative permissiveness of
End-of-Life Ethics in Germany and Israel
391
Germany in the context of EoL can be seen to represent different conceptions ofadult life, with a Christian–German emphasis on self-determination (reflected in theprivileged moral status of the autonomous individual) as opposed to a Jewish–Israeli focus on the sanctity of life as a social value and prescription. There arecomplex religious and cultural influences in each of these claims.
We would like to refine our own generalization by offering a more differen-tiated understanding of the term ‘‘restrictive.’’ Indeed, the Israeli stance con-cerning passive euthanasia is more restrictive in two respects: (a) Patients shouldbe persuaded to accept life-supporting machines and artificial feeding and (b)patients’ expressed wishes for withdrawing life support are overridden ina paternalistic manner. However, the practical solution of the timer might softenthe restriction, at least as regards competent patients, depending on who willhave the power to decide whether the timer is set up again, the patient (as, e.g.,suggested by Shalev21) or the physicians and caregivers (as the committeesuggested). It is worth noting that this kind of practical solution is a characteristicIsraeli construct of negotiating a resolution between Jewish law and secularmodernism and between rabbis and doctors. Some may regard the timer as a figleaf for existing moral problems. It has also been regarded as ‘‘the displacementof ethics by trickery.’’22 But one could see it as a pragmatic way out to allowindividual solutions for existing cultural conflicts.23 Other scholars have seen thisdifference as representing a religious gap between Judaism and Catholicism/Protestantism.24
With respect to the issue of physician-assisted suicide, the Israeli consensusagainst was also more restrictive than the German approach. In both reports,assisted suicide and killing on request are forbidden. In contrast to theconsensual Israeli stance against assisted suicide, the German statement didnot reach consensus on the matter. Corresponding to the liberal view of some ofthe German committee experts regarding the advantages of assisted suicide, inGermany there is a growing public debate on allowing it—as is now commonin Germany’s neighbor countries such as Belgium, Switzerland, and theNetherlands. Furthermore, also in Germany we observe a practical solution tothe tension between personal and societal–political interests, because someGerman patients travel abroad for assistance in suicide, as part of the recentlyobserved phenomenon labeled as bio-tourism. In Israel no such phenomenon hasbeen documented.
The Israeli proscription of both assisted suicide and withdrawal of continuoustreatment can be attributed to the primacy of the ‘‘sanctity of life’’ in the hierar-chy of orthodox Jewish ethics.25 It should be noted, though, that the expert state-ment regarding this stance is not automatically generalizable to Israeli culture ingeneral. Indeed, in a crosscultural survey on attitudes toward EoL care, it wasfound that physicians and patients who were Jewish regarded quality of life asmore important than the value of life, as compared to the importance reported byCatholics.26 In addition, Israel is a democracy with a legal system in whichpatient autonomy plays an important role. And Jewish scholars such as LeonardKravitz claim that the statements in the Steinberg committee’s report do notpresent any universalistic position of Jewish thinking.27 Therefore, the consensusof the Israeli committee could be seen as creating a political status quo betweenJudaism and the State, which might be considered as a ‘‘triumph of religion’’ overliberal principles of secular law.
Silke Schicktanz, Aviad Raz, and Carmel Shalev
392
In the German debate, too, there is a powerful religious impact. Christianauthorities also refer to the sanctity of life and the moral unacceptability ofterminating human life, seen as a gift from God. However, the religious positionis seen as only one voice among many others. Moreover, because the mandate ofthe German NEC was to deliberate, rather than to propose legislation, there wasno need to reach a final political consensus, so that two or three final voices couldbe presented in parallel.
The special role that historical arguments play in the German statement, butnot in the Israeli debate, is also noteworthy. It is not the first time that we find ina statement of a bioethics committee in Germany a reference to the crimes underthe National Socialist regime. For example, in the final report of the GermanParliamentary Interim Committee of Law and Ethics in Modern Medicine, theabsolute, universalistic character of Article 1 of the German constitution with itsnotion of human dignity and the main guiding principle of informed consent arejustified as legal tools to impede any future events that are comparable to thosethat took place during the National Socialist regime.28 As more and morebioethical statements are constructed and presented to the public, it would beequally important to accompany their dissemination with a careful and criticalanalysis of how they are embedded in conflicting and multifaceted cultural,political, and religious perspectives.
Notes
1. Turner L. From the local to the global. Bioethics and the concept of culture. Journal of Medicine and
Philosophy 2005;30:305–20.2. Wertz DC, Fletcher JC, eds. Ethics and Human Genetics: A Cross Cultural Perspective. Berlin: Springer;
1989.3. Hashiloni-Dolev Y. A Life (Un)Worthy of Living: Reproductive Genetics in Israel and Germany.
Dordrecht: Springer; 2007.4. Bulow H-H. The world’s major religions’ points of view on end-of-life decisions in the intensive
care unit. Intensive Care Medicine 2008;34:423–30.5. Schmuhl H-W. Nationalsozialismus als Argument im aktuellen Medizinethik-Diskurs. Eine
Zwischenbilanz [Euthanasia and the recent debate. Historical backgrounds of medical ethics].In: Frewer A, Eickhoff C, eds. Euthanasie und die aktuelle Sterbehilfe-Debatte. Die historischenHintergrunde medizinischer Ethik. Frankfurt a. M.: Campus; 2000:385–407.
6. Leichtentritt RD, Rettig K. Meanings and attitudes towards end-of-life preferences in Israel. Death
Studies 1999;23:323–58.7. The Report of the Public Committee on the Care of the Dying Patient. In: Hurwitz PJ, Picard J,
Steinberg A, eds. Jewish Ethics and the Care of End-of-Life Patients. A Collection of Rabbinical, Bioethical,
Philosophical, and Juristic Opinions. Jersey City, NJ: KTAV Publishing House, Inc.; 2006:207–14.8. National Ethics Council. German (Nationaler Ethikrat): Selbstbestimmung Fursorge am
Lebensende [Self-determination and Care in End of Life]. Berlin 2006.9. Haimes E, Williams R. Sociology, ethics, and the priority of the particular: Learning from a case
study of genetic deliberations. British Journal of Sociology 2007;58(3):457–76.10. Steinberg A. A law proposal in Israel regarding the patient at the end of life. In: Hurwitz PJ, Picard
J, Steinberg A, eds. Jewish Ethics and the Care of End-of-Life Patients. A Collection of Rabbinical,
Bioethical, Philosophical, and Juristic Opinions. Jersey City, NJ: KTAV Publishing House, Inc.;2006:99–104.
11. Shalev C. Paternalism and autonomy in end-of-life decision-making: The Israeli normativeambivalence. Israel Yearbook on Human Rights 2000;29:121–36.
12. See note 8, National Ethics Council 2006.13. Steinbock B, Norcross A, eds. Killing and Letting Die, 2nd ed. New York: Fordham University Press;
1994; Howard-Snyder D. Doing vs. allowing harm. In: Stanford Encyclopedia of Philosophy; 2006,available at http://plato.stanford.edu/entries/doing-allowing/ (last accessed 12 Apr 2010).
End-of-Life Ethics in Germany and Israel
393
14. See note 8, National Ethics Council 2006:47.15. See note 10, Steinberg 2006:103.16. Ravitsky V. Dying with dignity in a Jewish-democratic state. In: Hurwitz PJ, Picard J, Steinberg A,
eds. Jewish Ethics and the Care of End-of-Life Patients. A Collection of Rabbinical, Bioethical,
Philosophical, and Juristic Opinions. Jersey City, NJ: KTAV Publishing House, Inc.; 2006:105–18.17. Shalev C. End-of-life care in Israel—The Dying Patient Law 2005. Israel Law Review 2009;42(2):279–
305.18. Barilan MY. Is the clock ticking for terminally ill patients in Israel? Preliminary comment on
a proposal for a bill of rights for the terminally ill. Journal for Medical Ethics 2004;30:353–7.19. Wahrman MZ. Brave New Judaism: When Science and Scripture Collide. Hanover, MA: Brandeis
University Press; 2002; Prainsack B, Firestine O. ‘‘Science for survival’’: Biotechnology regulationin Israel. Science and Public Policy 2006;33(1):33–46.
20. Raz A. ‘‘Important to test, important to support’’: Attitudes toward disability rights and prenataldiagnosis among leaders of support groups for genetic disorders in Israel. Social Science and
Medicine 2004;59:1857–66.21. See note 17, Shalev 2009:289–290.22. Barilan MY. Revisiting the problem of Jewish bioethics: The case of terminal care. Kennedy Institute
of Ethics Journal 2003;13(2):141–68.23. Shapira A. Law and bioethics in Israel: Between liberal ethical values and Jewish religious norms.
Journal International de Bioethique 2006;17(1–2):115–23.24. See note 4, Bulow 2008.25. Ganz F, Benbenishty J, Hersch M, Fischer A, Gurman G, Sprung CL. The impact of regional culture
on intensive care end of life decision making: An Israeli perspective from the ETHICUS study.Journal for Medical Ethics 2006;32:196–9.
26. Sprung CL, Sara C, Baras M, Cohen SL, Maia P, Beishuizen A, et al. Attitudes of Europeanphysicians, nurses, patients, and families regarding end-of-life decisions: The ETHICATT study.Intensive Care Medicine 2007;33(1):104–10.
27. Kravitz LS. ‘‘Some’’ reflections on Jewish tradition and the end-of-life patient. In: Hurwitz PJ,Picard J, Steinberg A, eds. Jewish Ethics and the Care of End-of-Life Patients. A Collection of Rabbinical,
Bioethical, Philosophical, and Juristic Opinions. Jersey City, NJ: KTAV Publishing House, Inc.;2006:75–98.
28. Enquete-Kommission, Recht und Ethik der Modernen Medizin [Law and ethics of modernmedicine – Final Report]. Schlussbericht. Berlin: Deutscher Bundestag; 2002.
Silke Schicktanz, Aviad Raz, and Carmel Shalev
394
Related Documents