Clinical Allergy, 1975, Volume 5, pages 145-157 The correlation between skin tests, bronchial provocation tests and the serum level of IgE specific for common allergens in patients with asthma D. H. BRYANT*, M. W. BURNS and L. LAZARUS Garvan Institute of Medical Research, St Vincent^s Hospital, Sydney, NSW, Australia Summary Cutaneous and bronchial immediate allergic reactivity and the serum level of IgE specific for each of four common inhalant allergens were determined for 153 asthmatic patients. Positive bronchial reactivity to an extract was not detected in any of the patients with a negative prick test reaction to that extract but did occur in 9'\, of the patients in whom the serum tests results for IgE specific to that allergen fell within the range regarded as negative. Highly significant correlation coefficients between the degree of bronchial and cutaneous allergic reactivity to the allergen extracts were found and these were slightly but significantly less than the correlation between the serum level of allergen specific IgE and the degree of bronchial allergic reactivity to the allergen extracts. These findings indicate that the results both of prick testing with appropriate extracts and estimation of the serum level of allergen specific IgE can be used to predict not only the presence of detectable bronchial reactivity to inhalant allergens but also the degree of this reactivity. However, for the routine investiga- tion of asthmatic patients measurement of the serum level of allergen specific IgE would appear to have little advantage over properly performed prick tests. Introduction It has been reported in several studies that there is a significant association between the presence of allergen specific IgE in patients' serum and both a clinical history suggestive of sensitivity to that allergen and also positive skin and nasal or bronchial provocation tests to extracts of that allergen {Aas & Johansson, 1971; Berg, Bennich & Johansson, 1971; Stenius et al., 1971; Ahlstedt et al., 1974). However, the nature of the relationship between the degree of the immediate allergic reactivity of different tissues with the serum level ofallergen specific IgE has not been clearly established. A statistically significant positive correlation has been reported between the serum level of allergen specific IgE and both the degree of cutaneous reactivity (Stenius et ai. Correspondence: Dr M. W. Burns, Garvan Institute of Medical Research, St Vincent's Hospital, Sydney. NSW, Australia. * Present address: Cardiothoracic Institute, Bromton Hospital, London SW3. 145

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Clinical Allergy, 1975, Volume 5, pages 145-157
The correlation between skin tests, bronchial provocationtests and the serum level of IgE specific for commonallergens in patients with asthma
D. H. BRYANT*, M. W. BURNS and L. LAZARUS
Garvan Institute of Medical Research, St Vincent^s Hospital, Sydney, NSW, Australia
SummaryCutaneous and bronchial immediate allergic reactivity and the serum level of IgEspecific for each of four common inhalant allergens were determined for 153 asthmaticpatients. Positive bronchial reactivity to an extract was not detected in any of thepatients with a negative prick test reaction to that extract but did occur in 9'\, of thepatients in whom the serum tests results for IgE specific to that allergen fell withinthe range regarded as negative. Highly significant correlation coefficients between thedegree of bronchial and cutaneous allergic reactivity to the allergen extracts were foundand these were slightly but significantly less than the correlation between the serumlevel of allergen specific IgE and the degree of bronchial allergic reactivity to theallergen extracts. These findings indicate that the results both of prick testing withappropriate extracts and estimation of the serum level of allergen specific IgE can beused to predict not only the presence of detectable bronchial reactivity to inhalantallergens but also the degree of this reactivity. However, for the routine investiga-tion of asthmatic patients measurement of the serum level of allergen specific IgEwould appear to have little advantage over properly performed prick tests.
IntroductionIt has been reported in several studies that there is a significant association betweenthe presence of allergen specific IgE in patients' serum and both a clinical historysuggestive of sensitivity to that allergen and also positive skin and nasal or bronchialprovocation tests to extracts of that allergen {Aas & Johansson, 1971; Berg, Bennich& Johansson, 1971; Stenius et al., 1971; Ahlstedt et al., 1974). However, the natureof the relationship between the degree of the immediate allergic reactivity of differenttissues with the serum level ofallergen specific IgE has not been clearly established. Astatistically significant positive correlation has been reported between the serum levelof allergen specific IgE and both the degree of cutaneous reactivity (Stenius et ai.Correspondence: Dr M. W. Burns, Garvan Institute of Medical Research, St Vincent's Hospital,Sydney. NSW, Australia.
* Present address: Cardiothoracic Institute, Bromton Hospital, London SW3.
145
146 D. H. Bryant, M. W. Burns and L. Lazarus
1971; Miyamoto et al., 1974), and the degree of leucocyte sensitization (Assem &McAllen, 1970; Norman, Ishizaka & Lichtenstein, 1973). and it has been mentionedin several reports that patients with a high serum level ofallergen specific IgE tendedto develop bronchial responses after the inhaiation of smaller amounts of allergenextract than did the patients with lower serum levels ofallergen specificlgE(Bergc/fl/..1971; Ahlstedt et al., 1974; Miyamoto et al., 1974). However, no statistical attemptwas made in those studies to relate the degree of bronchial allergic reactivity to thepatients' scrum level ofallergen specific IgE.
The aim of this study was to investigate a sample of asthmatic patients in orderto document the degree of cutaneous and bronchial reactivity to extracts of commonallergens and to measure the level of IgE in their serum which was specific for thoseallergens so that the correlation between these parameters could be determined.
Patients and methods
PatientsA group of 153 patients with asthma {eighty-three men and seventy women) whohad been referred to the Thoracic Outpatients Clinic at St Vincent's Hospital wereselected for the study. Patients were accepted as having asthma if they experiencedepisodes of breathlessness and wheezing with relative freedom from symptomsbetween attacks and if these symptoms were not attributable to cardiac disease.Patients were excluded from the study if they had had symptoms of chronic bronchitis(Ciba Guest Symposium, 1959) before the onset of symptoms of asthma, if they hadever had hyposensitization injections, or if they had a basal Forced Expiratory VolumeIn one second (FEV,) ofless than 2L.
The patients were said to have a history of house dust sensitivity if exposure tohouse dust caused a noticeable increase in symptoms. The history was graded asstrongly positive (+ +) if symptoms could be provoked by brief exposure to smallamounts of house dust, and positive (-I-) if more prolonged exposure was needed. Thepatients were said to have a history of pollen sensitivity if they had experienced anoticeable increase in symptoms during the spring months ofthe 2 preceding years.
Informed consent for the investigations was obtained from all patients.
MeihodsSkin tests. Skin tests were carried out by the prick method (Pepys, 1972) using
extracts of Dermatophagoides pteronyssinus (Commonwealth Serum Laboratories.Melbourne), rye grass pollen (Lolii/ni perenne), plantain pollen (Plantago lanceolata),and A.spergillus fumigatus (Hollister Stier, Washington), using Coca's solution as thecontrol. All tests were made using the full strength extracts* and three serial ten-folddilutions of those extracts. The tests were made on the volar aspect of the patients'forearms and the mean diameter of the weal responses were measured to the nearestmillimeter after 20 min. The reactions were graded as 0 if they were not different fromthe control, as + if the weal was less than 3 mm in diameter, and -I- if the weal was3 mm or more in diameter. That strength of an extract which produced a 3 mm wealwas arbitrarily defined as the threshold strength of that extract.
* Z). preroH^'i'j'imw—10,000 units/ml; rye grass pollen and plantain pollen—50 mg/ml: A.fumigatus10 mg/ml.
' Common allergens in asthma patients 147
The patients were instructed not to take any antihistamine-containing preparationsfor 5 days prior to the tests (Cooke et al., 1973; Galant ct al., 1973). To avoid anypossible effect of circadian changes in cutaneous reactivity the tests were all madebetween 9 a.m. and II a.m. (Cormia, 1952; Reinberg, Sidi & Ghata, 1965).
Blood was taken from each patient, allowed to clot, the serum was separated andstored at —20 C until needed.
Bronchial provocation tests. The patients were instructed not to take any sodiumcromoglycate or aerosol bronchodilator for 24 hr prior to the tests. These tests wereall begun at 9 a.m. and were not made unless the patients were symptom free at thetime of testing. The aerosols were produced in a DeViibiss 40 nebulizer (Drug Housesof Australia, Sydney), which, with an air fiow of 8 l/min, nebulized fluid at a rate of0 25 ml/min. Only one allergen was tested on anyone day. The patient's basal FEV,was determined and then the patient inhaled an aerosol of Coca's solution for 20 minin order to ensure that this alone did not produce a fall in FEV,. Provocation testswere carried out using nonglycerinated extracts from the same batches as those usedin the other tests. The tests were begun with that strength of extract which produceda 3 mm weal on prick testing as it had been found in preliminary studies that patientsrarely reacted to extracts more dilute than this unless the aerosol was inhaled for aprolonged period. Beginning with inhalation periods of i min the patients inhaled thisextract for increasingly long periods. The patients' FEV, was measured during the15 min after each inhalation. This was continued until a positive bronchial responseoccurred or until the patient had inhaled that strength of extract for 20 min. If noresponse occurred this procedure was carried out with progressively stronger extractsuntil a positive response occurred or until the full strength extract had been inhaledfor 20 min. A positive response was defined as a 20% fall in the patient's FEV,. Positiveresponses were reversed by having the patients inhale 016 mg isoprenaline sulphatefrom a metered aerosol. Hydrocortisone and aminophyiline were also kept availablefor immediate parenteral use but these were never required.
The bronchial threshold dose ofallergen extract was taken as the total amount ofextract which had to be nebulized to produce a 20% fall in the patients' FEV,. Theconsistency of this response was determined in twenty-two patients. These patients allhad a positive response to D. pteronyssinus extract and a second provocation test withthis allergen was performed 1 week after the first test and the values of the two deter-minations were compared.
Allergen specific IgE a.ssay. IgE antibodies to the allergen extracts being studiedwere estimated by radioallergosorbent (RAST) procedure of Wide, Bennich & Johans-son (1967). The allergen extracts were coupled to cyanogen bromide activated micro-crystalline cellulose (E. Merck A.G., Darmstadt) and were stored as I mg/ml solutionsin the assay buffer (0 075 M phosphate buffer with 1% Tween 20 and 0-5 mg/ml sheepgamma globulin, pH 7 4). The specific antibody was isolated from sheep F^-specificanti-human IgE serum (Pharmacia, Uppsala) by affinity chromatography using IgEprotein which had been coupled to cyanogen bromide activated Sepharose 4B(Pharmacia, Uppsala). This purified antibody was labelled with '^^I by the chlor-amine-T method of Hunter & Greenwood (1962) and had a specific activity ofbetween 45 and 65 uC/ug.
Using these reagents the RAST tests were carried out using the method describedby Aas & Johansson (1971). The allergen specific IgE content of the sera were ex-pressed in arbitrary units, the serum from a highly atopic subject being used as the
148 D. H. Bryant, M. W. Burns and L. Lazarus
reference serum and being defined as containing IOOO arbitrary units/! ml of IgEspecific for each of the allergens being tested.
Statistical analysis. The index of predictive association, AB (Hays, 1963) was usedto determine the predictive strength ofthe relationship between two variables thatwere significantly related using the Pearson y'^ test statistic (Hays, 1963). The logarithmsofthe serum IgE and bronchial threshold dose values were used in the calculation ofthe correlation coefficients.
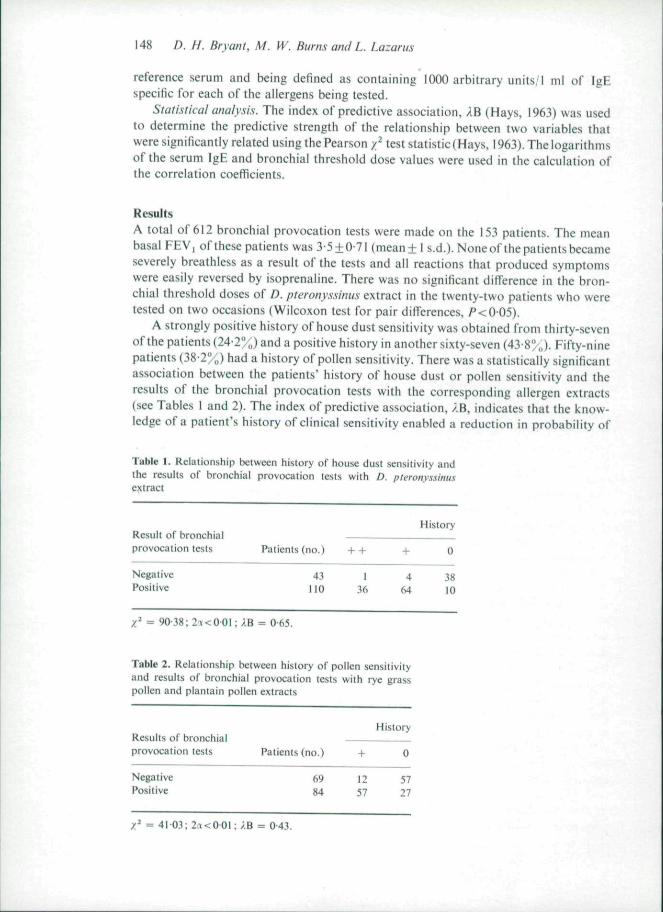
ResultsA total of 612 bronchial provocation tests were made on the 153 patients. The meanbasal FEV| of these patients was 3-5 + 0 71 (mean ± I s.d.). None of the patients becameseverely breathless as a result of the tests and all reactions that produced symptomswere easily reversed by isoprenaline. There was no significant difference in the bron-chial threshold doses of D. pteronyssinus extract in the twenty-two patients who weretested on two occasions (Wilcoxon test for pair differences. / ' <0 05).
A strongly positive history of house dust sensitivity was obtained from thirty-sevenof the patients (24-2^ „) and a positive history in another sixty-seven (43-8%). Fifty-ninepatients (38-2%) had a history of pollen sensitivity. There was a statistically significantassociation between the patients' history of house dust or pollen sensitivity and theresults of the bronchial provocation tests with the corresponding allergen extracts(see Tables I and 2). The index of predictive association. AB. indicates that the know-ledge of a patient's history of clinical sensitivity enabled a reduction in probability of
Table 1. Relationship between history of house dust sensitivity andthe results of bronchial provocation lesls with D. pteronyssimisextract
provocation tests
NegativePositive
Patients (no.)
43no
+ +
136
+
464
History
0
3810
: /B =
Table 2. Relationship beiween history of pollen sensilivityand results of bronchial provocation tests with rye grasspollen and plantain pollen extracts
provocation tests
NegativePositive
Patients (no.)
6984
+
1257
History
0
5727
^ = 41 03;2<T<00l:;iB = 043.
Common allergens in asthma patients 149
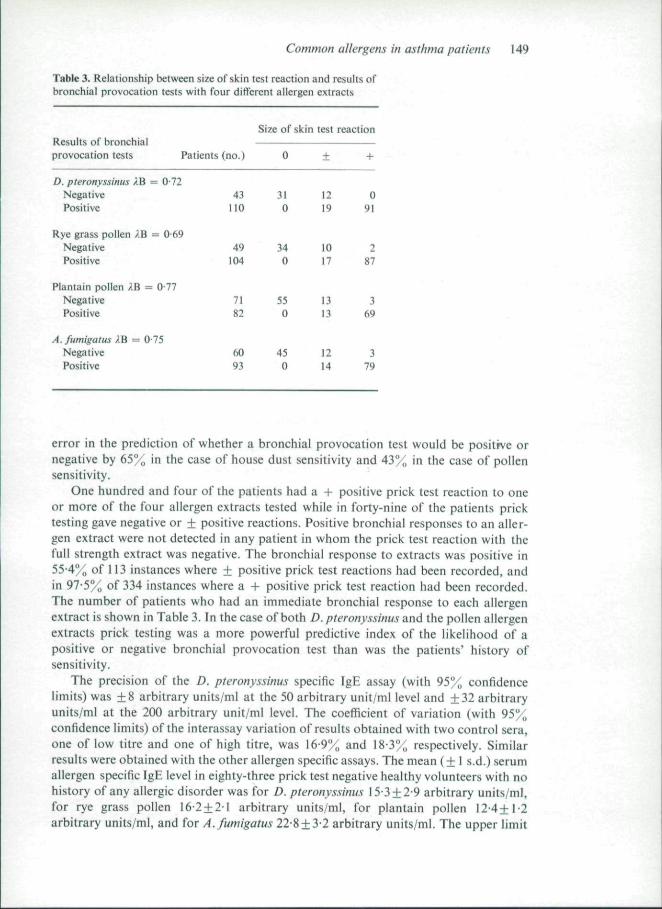
Table 3. Relationship beiween size of skin tesl reaction and results ofbronchial provocalion tests wilh four different ailergen extracts
Results of bronchialprovocation tests Patients
D. pteronyssinus XB = 0-72NegativePositive
Rye grass pollen i.B = 0 69NegativePositive
Plantain pollen ;.B = 077NegativePositive
A. fttmigatus AB = 0-75NegativePositive
(no.)
43
no
49104
7182
6093
Size of skin
0
310
340
550
450
test reaetion
±
1219
1017
1313
1214
+
091
287
369
379
error in the prediction of whether a bronchial provocation test would be positive ornegative by 65% in the case of house dust sensitivity and 43% in the case of pollensensitivity.
One hundred and four of the patients had a + positive prick test reaction to oneor more of the four allergen extracts tested while in forty-nine of the patients pricktesting gave negative or ± positive reactions. Positive bronchial responses to an aller-gen extract were not detected in any patient in whom the prick test reaction with thefull strength extract was negative. The bronchial response to extracts was positive in55-4% of 113 instances where ± positive prick test reactions had been recorded, andin 97-5% of 334 instances where a + positive prick test reaction had been recorded.The number of patients who had an immediate bronchia! response to each allergenextract is shown in Table 3. In thecase of both D. pteronyssinus and the pollen allergenextracts prick testing was a more powerful predictive index of the likelihood of apositive or negative bronchial provocation test than was the patients' history ofsensitivity.
The precision of the D. pteronyssinus specific IgE assay (with 95% confidencelimits) was ±8 arbitrary units/ml at the 50 arbitrary unit/ml level and ±32 arbitraryunits/ml at the 200 arbitrary unit/ml level. The coefficient of variation (with 95%confidence limits) ofthe interassay variation of results obtained with two control sera,one of low titre and one of high titre, was 16 9% and 18-3% respectively. Similarresults were obtained with the other allergen specific assays. The mean (± 1 s.d.) serumallergen specific IgE level in eighty-three prick test negative healthy volunteers with nohistory ofany allergic disorder was for D. pteronyssinus 15 3±2-9 arbitrary units/ml,for rye grass pollen 16 2 + 21 arbitrary units/ml, for plantain pollen 12 4+1-2arbitrary units/ml, and for A.fumigatus 22-8±3-2 arbitrary units/ml. The upper limit
150 D. H. Bryant, M. W. Burns and L. Lazaru.s
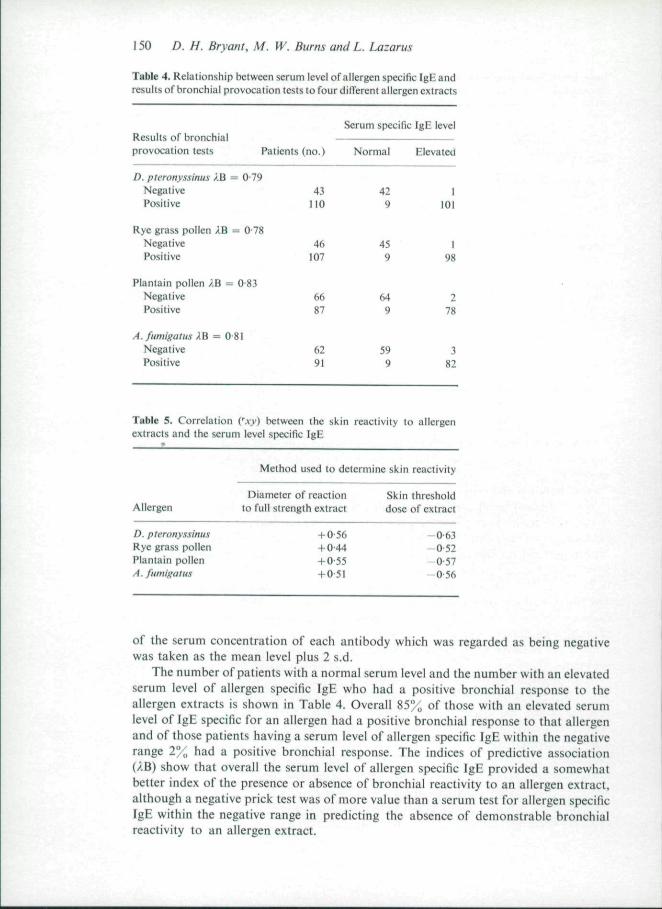
Table 4. Relationship between serum level of allergen specific IgE andresults of bronchial provocation lesls to four dilTerenl allergen extracts
Results of bronchialprovocation tests
D. pteronyssinus XB =NegativePositive
Rye grass pollen IB -NegativePositive
Plantain pollen ?,B =NegativePositive
Patients (no.)
= 0 7943
110
- 0 7846
107
0-836687
A. fumigatus XB = 081Negative 62Positive 91
Serum specific IgE level
Normal
429
459
649
599
Elevated
I101
198
278
382
Table 5. Correlation Cxy) between the skin reactivity to allergenextracts and the serum level specific IgE
Method used to determine skin reactivity
Diameter of reaction Skin thresholdAllergen to full strength extract dose of extraet
D. pteronys.simis +0 56 —0-63Rye grass pollen + 0 44 —0-52Plantain pollen -1-0 55 —0-57A. fumigatii.s +0 51 - 0 56
of the serum concentration of each antibody which was regarded as being negativewas taken as the mean level plus 2 s.d.
The number of patients with a normal serum level and the number with an elevatedserum level of allergen specific IgE who had a positive bronchial response to theallergen extracts is shown in Table 4. Overall 85% of those with an elevated serumlevel of IgE specific for an allergen had a positive bronchial response to that allergenand of those patients having a serum level of allergen specific IgE within the negativerange 2%, had a positive bronchial response. The indices of predictive association(AB) show that overall the serum level of allergen specific IgE provided a somewhatbetter index of the presence or absence of bronchial reactivity to an allergen extract,although a negative prick test was of more value than a serum test for allergen specificIgE within the negative range in predicting the absence of demonstrable bronchialreactivity to an allergen extract.
Common allergens in asthma patients 15!
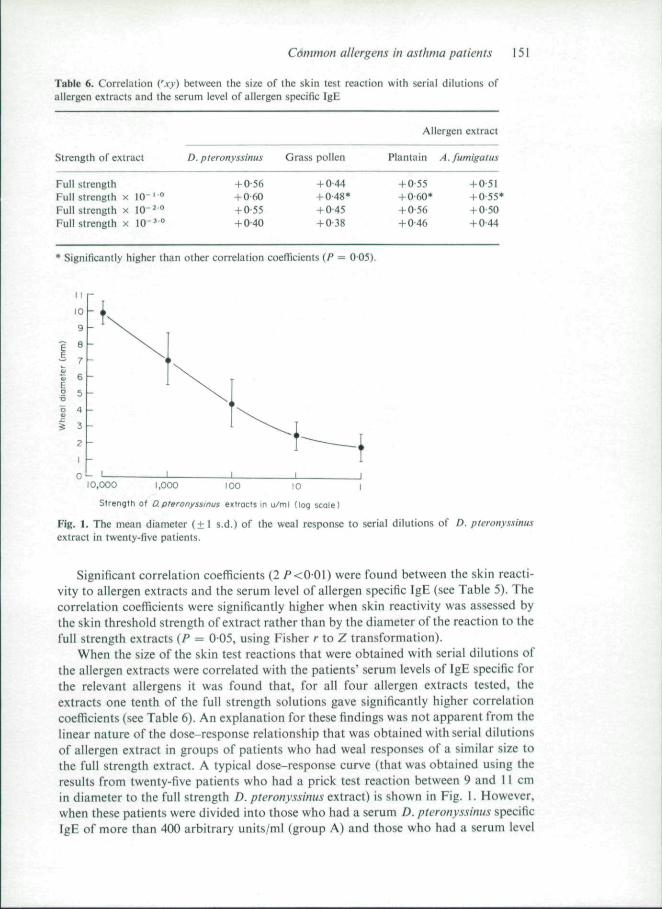
Table 6. Correlation Cxy) between the size of the skin test reaction with serial dilutions ofallergen extracts and the serum level of allergen specific IgE
Strength of extract
Full strengthFull strength x 10" '"Full strength x lO"''"Full strength x 10"^ °
D. pterony.ssinus
+ 0 56+ 0 60+ 0 55+ 0 40
Grass pollen
+ 0 44+ 0-48*+ 0 45+ 0-38
Allergen extract
Plantain A
+ 055+ 060*+ 0 56+ 0-46
. fumigatus
+ 051+ 055*+ 0 50+ 0 44
* Significantly higher than other correlation coefficients (P — 0 05).
10,000 1,000 (00 10 I
Strengtti of D.pferonyssinus eKtrocls in u/ml (log scale)
Fig. 1. The mean diameter (±1 s.d.) of the weal response to serial dilutions of D. pteronyssinusextract in twenty-five patients.
Significant correlation coefficients (2P<00\) were found between the skin reacti-vity to allergen extracts and the serum level of allergen specific IgE (see Table 5). Thecorrelation coefficients were significantly higher when skin reactivity was assessed bythe skin threshold strength of extract rather than by the diameter ofthe reaction to thefull strength extracts (P = 005, using Fisher r to Z transformation).
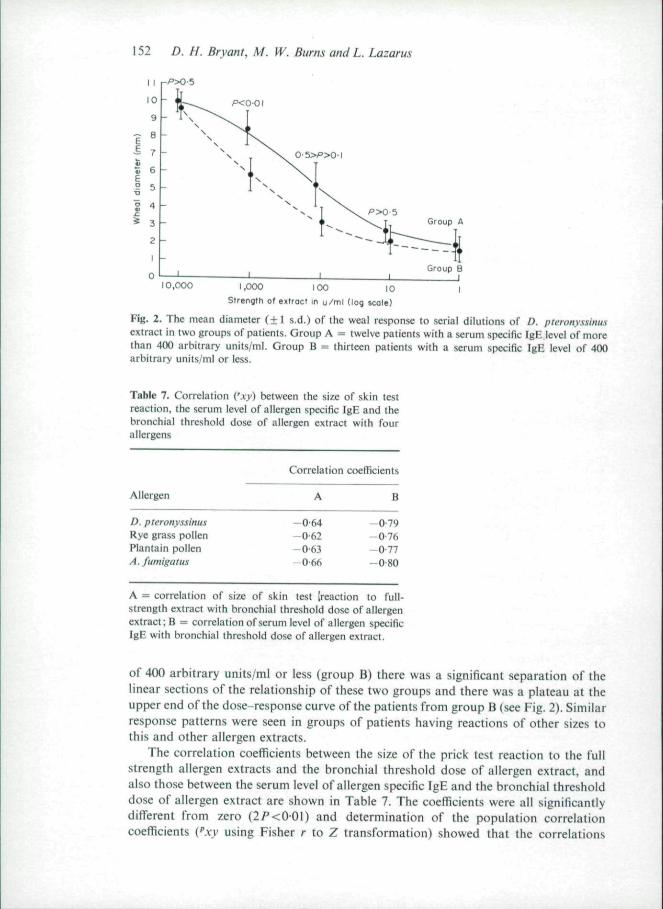
When the size ofthe skin test reactions that were obtained with serial dilutions ofthe allergen extracts were correlated with the patients" serum levels of IgE specific forthe relevant allergens it was found that, for all four allergen extracts tested, theextracts one tenth of the full strength solutions gave significantly higher correlationcoefficients (see Table 6). An explanation for these findings was not apparent from thelinear nature of the dose-response relationship that was obtained with serial dilutionsof allergen extract in groups of patients who had weal responses of a similar size tothe full strength extract. A typical dose-response curve (that was obtained using theresults from twenty-five patients who had a prick test reaction between 9 and 11 cmin diameter to the full strength D. pteronyssinus extract) is shown in Fig. 1. However,when these patients were divided into those who had a serum D. pteronyssinus specificIgE of more than 400 arbitrary units/ml (group A) and those who had a serum level
152 D. H. Bryant, M. W. Burns and L. Lazarus
Group A
10,000 1,000 100 10 1
Strength of extract m u /ml (log scole)
Fig. 2. The mean diameter (+1 s.d.) of ihe weal response to serial dilutions of D. pieronyssinusextract in two groups of patients. Group A = twelve patients with a serum specific IgE level of morethan 400 arbitrary units/ml. Group B = thirteen patients with a serum specific IgE level of 400arbitrary units/ml or less.
Table 7. Correlation ('J:^> between the size of skin testreaction, the serum level of allergen specific IgE and thebronchial threshold dose of allergen extract with fourallergens
Allergen
D. pteronyssinu-iRye gras.s pollenPlantain pollenA. fumigatus
Correlation coefficients
A
-0-64-0-62-0-63-0-66
B
-0-79- 0 7 6- 0 7 7- 0 8 0
A = correlation of size of skin test [reaction to full-strength extract with bronchial threshold dose of allergenextract; B = correlation of serum level of allergen specificIgE with bronchial threshold dose of allergen extract.
of 400 arbitrary units/ml or less (group B) there was a significant separation ofthelinear sections of the relationship of these two groups and there was a plateau at theupper end of the dose-response curve of the patients from group B (see Fig. 2). Similarresponse patterns were seen in groups of patients having reactions of other sizes tothis and other allergen extracts.
The correlation coefficients between the size of the prick test reaction to the fullstrength allergen extracts and the bronchial threshold dose of allergen extract, andalso those between the serum level of allergen specific IgE and the bronchial thresholddose of allergen extract are shown in Table 7. The coefficients were all significantlydifferent from zero (2/'<0-01} and determination of the population correlationcoefficients {"xy using Fisher r io Z transformation) showed that the correlations
Common allergens in asthma patients 153
obtained between the bronchial threshold and the serum level of allergen specific IgEwere all significantly higher than those between the bronchial threshold and the sizeofthe skin test reactions (2 P<005). The calculation ofthe coefficients of determina-tion (r^xy) showed that (depending on the allergen concerned) 38-44% ofthe variancein the bronchial threshold dose of allergen extract could be accounted for by theknowledge ofthe size ofthe skin test reaction to the full strength extract, and 59-65"'oof the variance could be accounted for by the knowledge of the serum level of allergenspecific IgE.
DiscussionEvidence that a bronchia! immediate allergic reaction to an inhaled allergen is apotential cause of symptoms in an asthmatic patient can be obtained by demonstratingthat airway obstruction is provoked in that patient by the inhalation of an aerosol ofa suitable extract ofthe allergen, provided that such a reaction is due to an imniuno-iogic response and not to a nonspecific bronchial response. In this study bronchialimmediate reactions have been termed immediate allergic reactions because positivebronchial responses were not detected in patients who had a negative prick test to thatallergen extract (although many of these patients had positive skin and bronchialresponses to other allergen extracts and had marked bronchial hyperreactivity tohistamine), because ofthe significant association between the results ofthe bronchialprovocation tests and both the patients' history of asthma after natural allergenexposure and the serum level of allergen specific IgE, and because of the ability ofsodium cromogiycate to inhibit these bronchial responses (Bryant, Burns & Lazarus,1975).
The results obtained in this study confirm the findings of Stenius et al. (1971) whoreported a significant correlation between the size of prick test reactions to allergenextracts and the serum level of allergen specific IgE. The significantly higher correlationthat was obtained when the skin threshold strength of allergen extract was used toassess cutaneous allergic reactivity is similar to that reported by Miyamoto et al.(1974). In the present study the use of allergen extracts more dilute than the fullstrength solutions produced reactions which showed, with some solutions, a signifi-cantly higher correlation with the serum level of allergen specific IgE although theseweaker extracts failed to produce positive responses in some patients who had onlyslightly elevated serum levels of allergen specific IgE. This pattern of reaction was alsonoted by Stenius et al. (1971).
These correlation patterns may be explained by the finding that, of those patientswho had similar sized weal reactions to the full strength extracts, those with higherserum antibody levels had significantly larger reactions to the weaker allergen extractsthan did those patients with lower serum antibody levels. In view ofthe highly signi-ficant correlation that Bruce et al. (1974) have reported between the skin thresholdstrength of allergen extract and the amount of allergen needed to cause 50/(, histaminerelease in leucocyte preparations from asthmatic patients it is of interest that thelateral displacement of the dose-response curves that was found in the present studyresembles the pattern of dose-response curves that are obtained in thestudy of allergen-induced histamine release using the leucocytes from different allergic patients (Lichten-stein & Osier, 1964; Sadan et aL 1969; Assem & McAllen, 1970). To what extent thislateral shift may be explained by the presence of different amounts of IgE on cells in thetissues and on the proposal by Levine of biochemically optimal allergen/antibody
154 D. H. Bryant, M. W. Burns and L. Lazarus
ratios on the surface of mast cells (Levine, 1965; Levine & Redmond, 1968), on differ-ences in the antigen binding capacity of different IgE molecules (Ishizaka & Ishizaka,1974), on the effect of allergen specific IgG antibody reducing histamine release athigher antigen concentrations (Sadan et al., 1969), on the negative feed-back exertedby discharged histamine on subsequent histamine release (Lichtenstein. 1974). and ondifferences in the tissue reactivity to vasoactive substances released in immediateallergic reactions remains speculative.
In this study a highly significant predictive association between the cutaneous andbronchial immediate allergic responses was found so that the knowledge that the skinreaction to the extract of an allergen was negative excluded delectable bronchialimmediate reactivity to that allergen extract, the knowledge of whether the skinreaction was positive or negative reduced the error in predicting the qualitative out-come of the bronchial provocation tests by between 69*',, and 77" „, while use ofthe cutaneous threshold strength of allergen extract enabled a 58-64% reduction in thevariance ofthe predicted quantitative bronchial threshold dose of allergen extract. Thenature of the relationship between skin and bronchial immediate allergic reactivitydepends on the criteria used for the selection of patients for testing and on the degreeof control over the variables (including the potency and purity of extracts, the tech-niques used to perform the tests, the sensitivity of the methods used to record theresponses and criteria used to define positive reactions) which affect the assessment ofcutaneous and bronchial reactivity. Because of differences in all these variables theresults obtained in this study cannot be validly compared with the results of manyprevious studies. Using the prick method of skin testing Pepys (1969) found that, asin this study, bronchial responses to extracts were not detected in patients in whomthe skin reaction was not bigger than the control response. Bronsky & Ellis (1969) andSpeetor & Farr (1973) recorded positive bronchial responses to extracts in 23% and3% respectively of patients in whom the prick test reaction had been graded asnegative. However, in both these reports prick tests were graded as negative when theweal was up to 2 mm in diameter and was accompanied by an area of erythema up to14 mm in diameter. Such reactions would have been graded as + in the present study.It is unlikely that many patients with significant bronchial immediate allergic reactivitywere missed in the present study as the maximal dose of allergen extract nebulizedbefore a bronchial provocation test was classed as negative was higher than in thesetwo other reports. The differences in the results between this study and those of Bron-sky & Ellis (1969) and Speetor & Parr (1973) may, therefore, be attributed to thedifferent criteria used to define positive skin test reactions.
These results are in marked contrast to those obtained with the intradermal methodof skin testing where positive bronchial responses have been found in a variablepercentage of patients with positive intradermal skin tests and in from I";, to 40% ofpatients in whom skin reactivity was classed as negative (Nilsson & Kaude, 1960;Colldahl. 1967; Aas, 1970; Maier, Orion & Deviller, 1970; Gayrard et al., 1972).However, as intradermal tests tend to produce more nonspecifically positive reactionsthan do prick tests (Pepys, 1972), as the criteria that were used in these studies to definepositive cutaneous and bronchial responses differed, and as the degree of control overthose variables which influence the assessment of cutaneous and bronchial reactivityvaried widely, these differences in the observed relationship between the allergicreactivity of the skin and the bronchi are not surprising. However, recent reportsindicate that if the sensitivity of the intradermal technique is increased by determining
Common allergens in asthma patients 155
the skin threshold strength of extracts then the correlation of these results with theserum level of allergen specific IgE is highly significant (Henderson & Gleich, 1974;Normal et al., 1973), and the correlation with the bronchial threshold dose of allergenextract may approach that reported in this study with prick testing (Bruce et al., 1974;Miyamoto et al., 1974).
As the measurement of serum allergen specific IgE is not influenced by the variableswhich afiect the assessment of the allergic reactivity of the skin, the serum level ofallergen specific IgE could be expected to have an even closer relationship withbronchial allergic reactivity than does cutaneous allergic reactivity. This hypothesis issupported by the results of this and other studies (Stenius & Wide, 1969; Aas &Johansson, 1971; Berg et al., 1971; Ahlstedt et al., 1974). However the number ofpatients tested in some of these studies have been small and the nature ofthe relation-ship between the parameters examined were not subjected to statistical analysis. Itwas reported that in between 60% and 80% ofthe patients studied either the serumlevel of allergen specific IgE was elevated and the bronchial provocation test waspositive or the serum test result for allergen specific IgE was within the negativerange and the bronchial provocation was negative. However, the expression of re-sults in this form gives no true indication of the ability to predict bronchial reactivityfrom the serum antibody level. In this study, by means of the index of predictive associ-alion (AB) it was apparent that the knowledge of whether a patient's serum test resultlor allergen specific IgE was within the negative range or elevated allowed a 78-83%(depending on the allergen) reduction in error in predicting whether the bronchialprovocation test would be positive or negative.
Aas & Johansson (1971) and Miyamoto c/a/. (1974) mentioned that in the patientsthey studied, a tendency was apparent for those patients with a high serum level of IgEspecific for an allergen to develop a positive bronchial response after exposure to onlysmall quantities of an extract of that allergen but they did not analyse the relationshipbetween these two parameters. The correlation between these two variables for thefour allergen extracts studied in this investigation indicated that use of the linearregression equation and the serum allergen specific IgH would reduce the variance ofthe predicted bronchial threshold dose of allergen extract by between 58% and 64%.
Of the patients in this study in whom a positive bronchial provocation test wasrecorded 9% had serum test results for allergen specific IgE within the negative range.In previously reported studies this response pattern has been seen in between 2%and 9%, of patients subjected to bronchial or nasal provocation tests (Aas & Johans-son, 1971; Berg et al., 1971; Stenius e/ al., 1971; Ahlstedt et al., 1974; Miyamotoet al., 1974). This type of response pattern could have been caused by the bronchialreaction being due to a nonspecific rather than an immediate allergic reaction. How-ever, many of the patients with this pattern of response in the present study had aclinical history suggesting allergen sensitivity, all had a positive prick test to theallergen extract concerned, and some had quite low bronchial threshold doses of theallergen extract. This indicates that the bronchial response in these patients mayhave been due to an immediate allergic reaction to the allergen aerosol but that theantibody concerned did not belong to the IgE class and may have been short termanaphylactic IgG antibody (Bryant et al., 1975), or it did belong to the IgE class butwas present in the serum in normal amounts only or was not recognized by the IgEassay.
The results of this study indicate that the patients' serum level of allergen specific
156 D. H. Bryatit, M. W. Burns and L. Lazarus
IgE provides a slightly but significantly better indication of the likely presence ofbronchial allergic reactivity and of the degree of this reactivity than do the results ofskin testing. However, they do not support the contention that bronchial provocationtests are essential for the assessment of asthmatic patients for bronchial immediateallergic reactivity to recognized common inhalant allergens (Colldahl, 1967; Aas,1970), nor do they indicate that skin prick tests should be replaced by the estimation ofthe serum level of allergen specific IgE for the routine investigation of asthmaticpatients, although in particular circumstances these additional investigations may beindicated.
Ack no wledgmentsThis work was supported by a grant from The Asthma Foundation of NSW. Wewould also like to thank Mr B. Polglase for technical assistance, Dr E. Kraegen forhelp with the statistical analysis, and the physicians ofthe Thoracic Unit at St Vincent'sHospital for permission to study their patients.
ReferencesAAS, K . (1970) Bronchial provocation tests in asthma. Archives of Diseases in Childhood, 45, 221.AAS, K . & JOHANSSON, S.G.O. (1971) The radioallergosorhcnt lesi In the in c/rro diagnosis of multiple
reaginic allergy. Jotmtal of Allergy ami Clinical Imnumohf^y. 48, 1.14.AHLSTEDT, S.. ERIKSSON, N . , LINDGREN. S. & ROTH, A. (1974) Specific IgE determination by RAST
compared wilh skill and provocation tests in allergy diagnosis wilh birch pollen, limolhy pollenand dog epithelium allergens. Clinical Allergy. 4. 131.
ASSEM, E . S . K . & McALt.EN, M.K.(1970)Serumreaginsand leucocyte response in patients with house-dust mite allergy. Briti.sh MedicalJournal, il, 504.
B E R G . T . , BENNICH, H . & JOHANSSON, S.G.O. (1971)/« r/fw diagnosis of alopic allergy. I. A compari-son between provocation tests and the radioallergosorbent lest. International Archiii:<i of Allergy.40, 770.
BRONSKY, E . & ELLIS, E . (1969) Inhalation bronchial challenge testing in asthmatic children. PaediatricClinics of North America, 16, 85.
BRUCE, C.A., ROSENTHAL, R.R., LICHTENSTEIN, L.M. & NORMAN, P.S. (1974) Diagnostic tests in
ragweed allergic asihma. Joitrmil of Allergy and Clinical Immunology, S3, 230.BRYANT, D.H., BURNS, M . W . & LAZARUS, L . (1975) The identification of IgG as a carrier of reaginic
activity in patients wilh asthma. JotirmI of Allergy and Clinical Immtmotogy (in press).DBA GUEST SYMPOSIUM (1959) Terminology, definitions, and a classification of chronic pulmonary
emphysema and related conditions. Thorax, 44, 286.COLLDAHL, H . { 1967) The importance of inhalation tests in the etiological diagnosis of allergic diseases
of the bronchi and in the evaluation of the effects of specific hyposensitisation treatment. Adaallergologiia. 22 (suppl. 8), 7.
CooKE, T.J., MACQUEEN, D.M.. WITTIG, H J . , THORNBV, J.L, LANTOS. R . L . & VIRTUE, C M . (1973)
Degree and duration of skin test suppression and side effects with antihistamines. Journal ofAllergy and Clinical Immunology^ 51, 71.
CoRMiA, E.F. (1952) Experimental histamine pruritis. I. Influence of physical and psychologicalfactors on threshold reactivity. Journal of Investigative Dermatology, 19, 21.
GALANT, S.P.. BULLOCK, J., WONG, D . & MAIBACH, H.I. (1973) The inhibitory etlect of anti-allergy
drugs on allergen and histamine induced weal and fiare response. Journal of Allergy and ClinicalI m m t i n o l o g y , 5 1 , I I .
GAYRARD. P., OREHEK, J., BOUTIN, C . & CHARPIN, J. (1972) Valeur du test de provocation par aller-gens inhales dans i'asthma. Acia allergologica, 11, 87.
HAYS, W . L . (1963) Statistics for Psychologist.s, p. 608. Holt, Rinehart and Winston, New York.HENDERSON, L . L . & GLEICH, G.J. (1974) Reagin antibodies and hypersensitisation in atopie disease.
In: Allergology (Ed. by Y. Yamamura, O. L. Frick, Y. Horiuchi, S. Kishimoto, T. Miyamoto,P. Naranjo and A. De Week), p. 54. Excerpta Medica, Amsterdam.
Cotntnon allergens in asthma patients 157
HUNTER, W.M. & GREENWOOD, F .C. (1962) Preparation of iodine—131 labelled human growthhormone of high specific activity. Nature, Lond., 194, 495.
ISHIZAKA. K. & ISHIZAKA, T. (1974) Mechanisms of reaginic hypersensitivily: IgE molecules ontarget cells. In: Allergology (Ed. by Y. Yamamura, O. L. Frick, Y. Horiuchi, S. Kishimoto,T. Miyamoto, P. Naranjo and A. De Week), p. 12. Excerpta Medica, Amsterdam.
LEVINE, B.B. (1965) The nature of antigen-antibody complexes initiating anaphylactic reactions.J o t i r n a t of I m n m n o l o g y , 9 4 , I I I .
LEVINE, B.B. & REDMOND, A.P. (1968) The nature of Ag-Ab complexes initiating the specific weal andflare reaction in sensitised man. Journal of Clinical Investigation, 47, 556.
LicHTENSTEiN, L.M. (1974) /// ('(Vro studies on the biochemical mechanisms and pharmacologic controlof atopie reactions. In: Allergology (Ed. by Y. Yamamura, O. L. Frick, Y. Horiuchi, S. Kishi-moto, T. Miyamoto, P. Naranjo and A. De Week), p. 294. Excerpta Medica, Amsterdam.
LICHTENSTEIN, L.M. &OSLER, A.G. (1964) Studies on the mechanisms of hypersensitivity phenomena.Journal of Experimental Medicine, 120, 507.
MAIER, A., ORION, B. & DEVILLER, C. (1970) Confrontation des tests cutanes et des tests de provoca-tion chez 200 asthmatiques. Revue Fran^aise d'Allergologie. 10, 221.
MIYAMOTO, T., JOHANSSON, S.G.O., ITO, K. & HORIUCHI, Y. (1974) Atopie allergy in Japanese sub-jects: Studies primarily with radioallergosorbent test. Journal of Allergy and Clinieal Immunology,53, 9.
Nii-SSON, H. & KAUDE, J. (1960) Inhalation and skin test in the diagnosis of asthma bronchiale.Diseases ofthe Chest, 37, 535.
NORMAN, P.S., ISHIZAKA, K. & LICHTENSTEIN, L.M. (1973) Specific IgE antibody measurement indiagnosis of ragweed hayfever. Journal of Allergy and Clinieal Immunology, 51, 112.
PHPYS, J. (1969) Hypersensilivily diseases ofthe lungs dtie lo fungi and organie dusts. S. Karger, Basle.PEPYS, J. (1972) Skin tests for immediate. Type I, allergic reactions. Proceedings of the Royal Society
of Medicine, 65, 271.REINBERG. A., SiDt, E. & GHATA, J. (1965) Orcadian reactivity, rhythms of human skin to histamine,
allergen and the adrenal cycle. Journal of Allergy, 36, 273.SADAN, N. , RHYNE, M.B., MELLITIS, D., GOLDSTEIN, E.O., LEVY, D.A. & LtCHTENSTEiN, L.M. (1969)
Immunotberapy of pollinosis in children: An investigation of the immunologic basis for clinicalimprovement. New England Journal of Medicine, 280, 623.
SPECTOR, S.L. & FARR, R.S. (1973) Inhalation challenge in aslhmatics. Journal of Allergy and ClinicalImmunology, 51, 87.
STENIUS, B. & WIDE, L. (1969) Reaginic antibody (IgE), skin and provocation tests to Dermaiopha-goides culinae and house dust in respiratory allergy. Lancet ii, 455.
STENIUS, B., WIDE, L., SEYMOUR, W.M., HOLFORO-STREVENS, V. & PEPYS. J. (1971) Clinical signifi-cance of specific IgE to common allergens. Clinical Allergy, 1, 37.
WIDE, L., BENNICH, H. & JOHANSSON. S.G.O. (1967) Diagnosis of allergy by an/« r/Vcy test for allergenantibodies. Laneei, ii, 1105.

Related Documents











