
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1.Introduction
2.Classifications
3.Mechanism of action
4.Spectrum of activity
5.Dosages
6.Adverse reactions
7.Drug interactions
8.Use in Special Populations
9.Patient counselling
Objectives
Tetracyclines is a group of antibiotics that include
Tetracycline ; it was discovered in 1948 , exhibitedactivity against a wide range of microorganismsincluding gram-positive and gram-negative bacteria,Chlortetracycline was the first Tetracycline to beidentified. . Since then five additional tetracyclineshave been isolated or derived (oxytetracycline,tetracycline, Demeclocycline, Doxycycline andminocycline ).
1.Introduction
Tetracyclines retain important roles in both human and veterinary medicine.
The favorable antimicrobial properties of these agents and the absence of major adverse side effects has led to their extensive use in the therapy of human and animal infections but the emergence of microbial resistance has limited their effectiveness.
They are also inexpensive antibiotics, therefore have
been used extensively in the prophlylaxis and therapy of human and animal infections also at subtherapeutic levels in animal feed as growth promoters.
Doxycycline and minocycline are the most frequently prescribed .
The improved understanding of tetracycline resistance mechanisms has provided opportunities for the recent discovery of a new generation of tetracyclines, the GLYCYLCYCLINES.
2.1 According to source: Naturally occurring
Tetracycline Chlortetracycline Oxytetracycline Demeclocycline
Semi-synthetic Doxycycline Lymecycline Meclocycline Methacycline Minocycline Rolitetracycline
2.Classifications
2.2.According to duration of action:
Short-acting (Half-life is 6-8 hrs) Tetracycline
Chlortetracycline
Oxytetracycline
Intermediate-acting (Half-life is ~12 hrs) Demeclocycline
Methacycline
Long-acting (Half-life is 16 hrs or more) Doxycycline
Minocycline
Tigecycline
Tigecycline may also be considered a tetracycline antibiotic, though it is usually classified as a glycylcyclineantibiotic.
tetracyclines bind reversibly to the 30S ribosomal
subunit at a position that blocks the binding of the
aminoacyl-tRNA to the acceptor site on the mRNA-ribosome complex. Protein synthesis is ultimately inhibited, leading to a bacteriostatic effect .
3.Mechanism of action
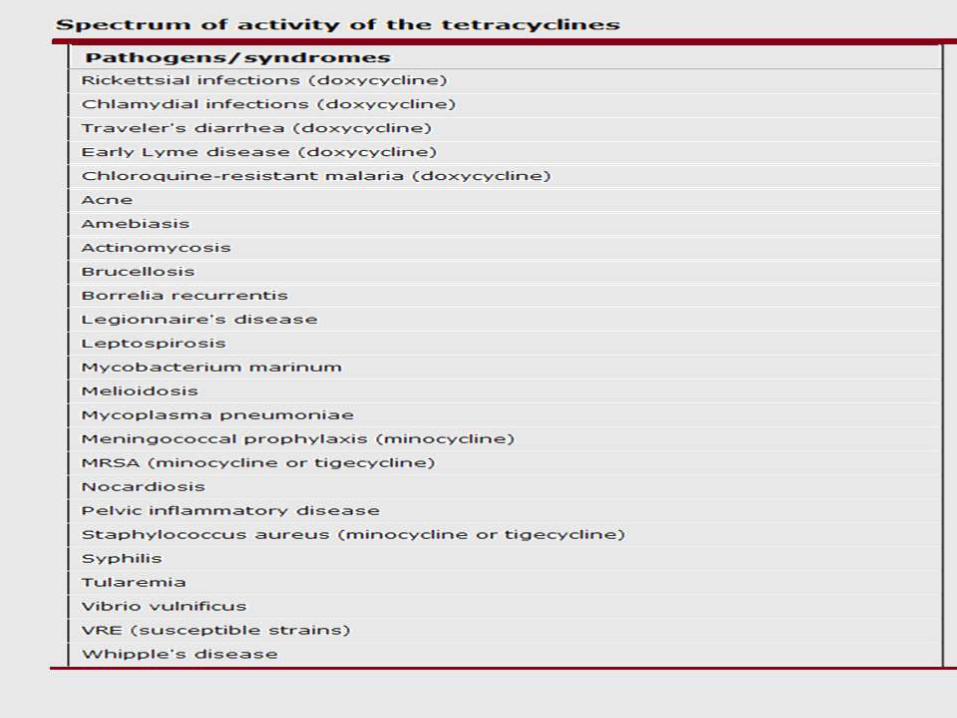
4.Spectrum of activity
The antimicrobial activity of all the tetracyclines is essentially the same although some differences in the relative degree of activity against certain pathogens do exist among the various agents.
As an example, minocycline appears to be the most active of the compounds due to its slight increase in lipid solubility; Doxycycline follows closely behind.
The tetracyclines are considered broad-spectrum
bacteriostatic antibiotics that are used to treat infection caused by many aerobic gram-positive and gram-negative bacteria. However, they also have activity against many atypical pathogens.
These drugs have little activity against fungi and viruses .
Against N. gonorrhoeae, the 2006 Gonococcal Isolate
Surveillance Project (GISP) report shows that 25.6 percent
of isolates collected in 2006 were resistant to Tetracycline,. Therefore, use of tetracyclines for the treatment of N. gonorrhoeae in the US is NOT recommended
by the CDC.
Doxycycline is effective for patients with
nongonococcal urethritis caused by Chlamydia trachomatis; however, recurrent urethritis in patients previously treated with doxycycline may be the result of tetracycline-resistant U. urealyticum. Doxycycline is an alternative agent in the treatment of genital Chlamydial infections [11].
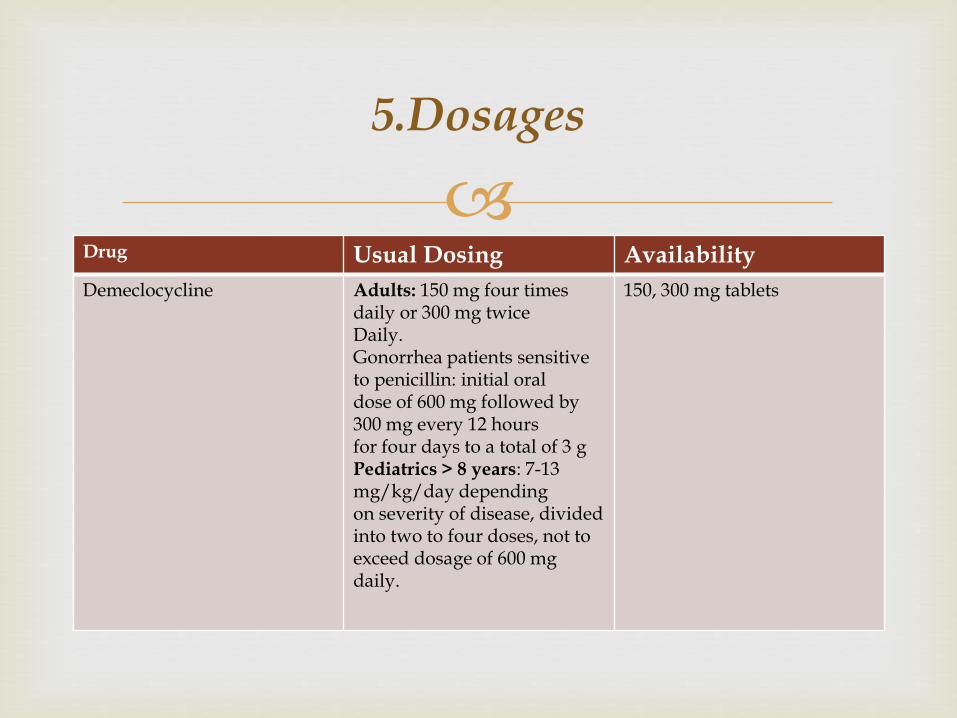
Drug Usual Dosing Availability
Demeclocycline Adults: 150 mg four times daily or 300 mg twiceDaily.Gonorrhea patients sensitive to penicillin: initial oraldose of 600 mg followed by 300 mg every 12 hoursfor four days to a total of 3 gPediatrics > 8 years: 7-13 mg/kg/day dependingon severity of disease, divided into two to four doses, not to exceed dosage of 600 mg daily.
150, 300 mg tablets
5.Dosages
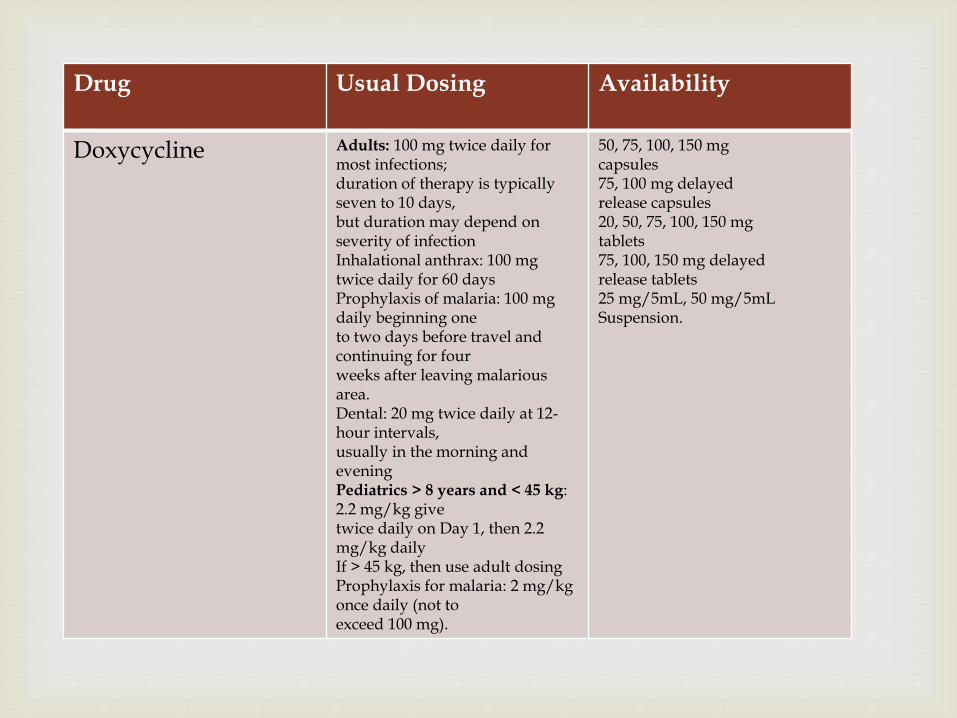
Drug Usual Dosing Availability
Doxycycline Adults: 100 mg twice daily for most infections;duration of therapy is typically seven to 10 days,but duration may depend on severity of infectionInhalational anthrax: 100 mg twice daily for 60 daysProphylaxis of malaria: 100 mg daily beginning oneto two days before travel and continuing for fourweeks after leaving malariousarea.Dental: 20 mg twice daily at 12-hour intervals,usually in the morning and eveningPediatrics > 8 years and < 45 kg: 2.2 mg/kg givetwice daily on Day 1, then 2.2 mg/kg dailyIf > 45 kg, then use adult dosingProphylaxis for malaria: 2 mg/kg once daily (not toexceed 100 mg).
50, 75, 100, 150 mgcapsules75, 100 mg delayedrelease capsules20, 50, 75, 100, 150 mgtablets75, 100, 150 mg delayedrelease tablets25 mg/5mL, 50 mg/5mLSuspension.
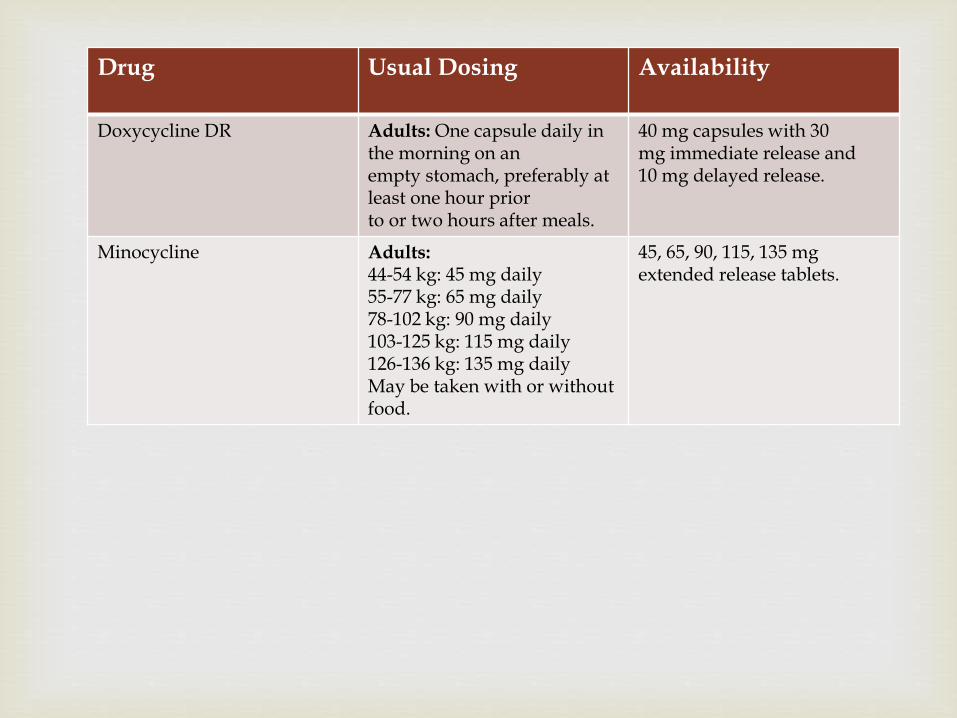
Drug Usual Dosing Availability
Doxycycline DR Adults: One capsule daily in the morning on anempty stomach, preferably at least one hour priorto or two hours after meals.
40 mg capsules with 30mg immediate release and10 mg delayed release.
Minocycline Adults:44-54 kg: 45 mg daily55-77 kg: 65 mg daily78-102 kg: 90 mg daily103-125 kg: 115 mg daily126-136 kg: 135 mg dailyMay be taken with or without food.
45, 65, 90, 115, 135 mgextended release tablets.
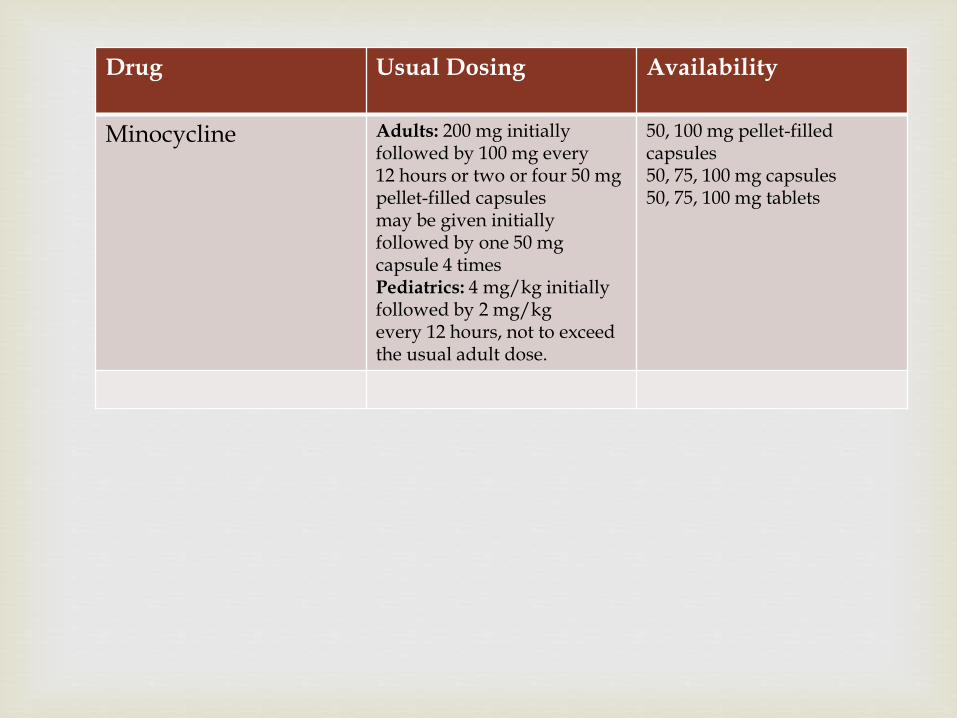
Drug Usual Dosing Availability
Minocycline Adults: 200 mg initially followed by 100 mg every12 hours or two or four 50 mg pellet-filled capsulesmay be given initially followed by one 50 mgcapsule 4 timesPediatrics: 4 mg/kg initially followed by 2 mg/kgevery 12 hours, not to exceed the usual adult dose.
50, 100 mg pellet-filledcapsules50, 75, 100 mg capsules50, 75, 100 mg tablets
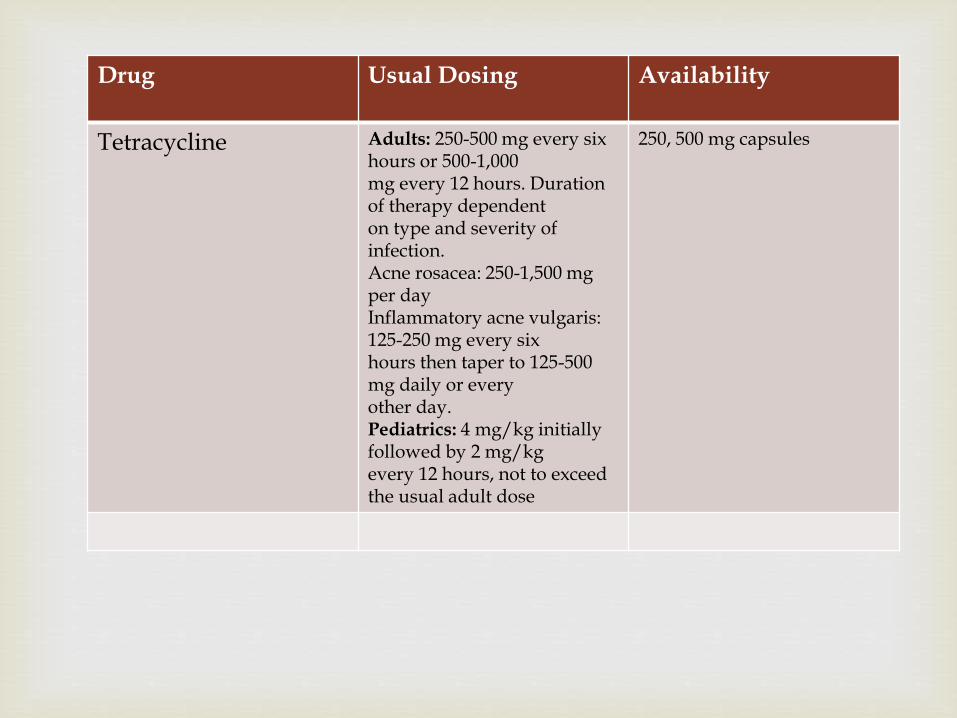
Drug Usual Dosing Availability
Tetracycline Adults: 250-500 mg every six hours or 500-1,000mg every 12 hours. Duration of therapy dependenton type and severity of infection.Acne rosacea: 250-1,500 mg per dayInflammatory acne vulgaris: 125-250 mg every sixhours then taper to 125-500 mg daily or everyother day.Pediatrics: 4 mg/kg initially followed by 2 mg/kgevery 12 hours, not to exceed the usual adult dose
250, 500 mg capsules
Tetracyclines are generally safe drugs, but some
adverse effects can occur.
6.1. Gastrointestinal
Dose-related gastrointestinal side effects are the most common complaint in patients taking oral tetracyclines . These include abdominal discomfort, epigastric pain, nausea, vomiting and anorexia. Food may decrease these symptoms but also may decrease the absorption of tetracycline by 50 percent. Food does not affect the absorption of doxycycline
6.ADVERSE REACTIONS
Tetracyclines may alter gut flora to cause large
bulky stools and diarrhea. Diarrhea usually subsides once the agent is stopped. A patient with continued diarrhea, fever, and a rising white blood count should be evaluated for antibiotic associated diarrhea caused by Clostridium difficile. Esophageal ulcerations and strictures have been reported with tetracyclines but can be prevented by taking the drugs with plenty of water and not before bedtime.
Allergic and skin reactions:
Hypersensitivity reactions can occur with tetracyclines but are uncommon. If a patient is allergic to one tetracycline, they should be considered allergic to all. Photosensitivity reactions can occur, ranging from a red rash to blistering on areas exposed to the sun. These reactions are most common with demeclocycline but can occur with all analogues. Photosensitivity can be decreased by avoiding direct sunlight or wearing protective clothing with sunscreen.
Teeth and bone:
Tetracyclines can cause a brown to yellow discoloration of the teeth in children under the age of eight that is sometimes associated with hypoplasia of the enamel. The darkening effect on the permanent teeth appears to be dose related and does not occur in adults. These agents generally should be avoided in children under the age of eight; however if they must be used, doxycycline may be the preferred agent. Tetracyclines may also deposit in the bone likely due to chelate formation with calcium, thus adding another reason to avoid these agents in children with developing bone formation.
Liver and renal :
Hepatotoxicity with tetracyclines is rare but can be fatal. This occurs more commonly with tetracycline and minocycline and less often with doxycycline.
Tetracyclines inhibit protein synthesis and may exacerbate preexisting renal failure by increasing the azotemia from amino acid metabolism. Demeclocycline can cause a nephrogenicdiabetes insipidus, a side effect that is used therapeutically to treat the syndrome of inappropriate antidiuretic hormone secretion (SIADH). The use of outdated tetracyclines has been associated with a reversible Fanconi-like syndrome and renal tubular acidosis; however, current formulations, which do not contain citric acid as an excipient, have virtually eliminated this possibility.
The absorption of tetracyclines can be impaired by
co-administered minerals and antacids (eg, calcium, magnesium, iron), lanthanum, and dairy including milk. Tetracyclines can interact with oral isotretinoin, beta-lactams, and a variety of other drugs
7.DRUG INTERACTIONS
Pediatrics:
Use of tetracycline products in children less than eight years of age is not recommended due to the potential for tooth discoloration. Safety and effectiveness of minocycline ER (Solodyn) in children less than 12 years of age have not been established.
Pregnancy:All agents in this class are Pregnancy Category D.
8.Use in Special Populations
Nursing Mothers:
The American Academy of Pediatrics considers ciprofloxacin and tetracyclines including doxycyclineto be usually compatible with breastfeeding because the amount of drug absorbed by infants is small, but little is known about the safety of long-term use. Mothers concerned about the use of ciprofloxacin or doxycycline for antimicrobial prophylaxis should consider expressing and then discarding breast milk so that breastfeeding can be resumed when antimicrobial prophylaxis is completed.
Renal Impairment
If renal impairment is present, minocycline doses may need to be adjusted to avoid
excessive systemic accumulation of the drug and possible liver toxicity.
Take your medicine with a full glass of water. These medicines are best taken on an empty stomach (either 1 hour before or 2 hours after meals). unless manufacturer specify or if stomach upset occurs.
Avoid exposure to direct sunlight.
Do not take milk, other dairy products, antacids or iron within 2 hours of taking these medicines
9.Patient counselling
The course of antibiotics should be completed even if you feel better after a few days, and DO NOT forget to keep the medicine out of reach of children
http://www.uptodate.com
http://www.micromedexsolutions.com/micromedex2/librarian?partner=true
www.clinicalpharmacology.com.
Toxicology and Applied Pharmacology
References
Thanks
Related Documents











