Therapeutic Drug Monitoring Sandeep.B, M.Pharm, II Semester, Department of Pharmacy Practice

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Therapeutic Drug Monitoring
Sandeep.B,M.Pharm, II Semester,
Department of Pharmacy Practice
Contents:
Introduction Necessity of TDM Objectives Criteria for TDM Drugs requiring TDM Sampling Examples Factors influencing plasma drug concentration Analytical techniques used in TDM Clinical interpretation of results Role of Pharmacist in TDM Limitations References
Introduction:
Therapeutic drug monitoring is defined as a “a process of assessing concentration of the drug in biological fluids such that it is maintained within the therapeutic range.”
It aims at individualizing the dose for a patient to obtain maximum benefit.
TDM closely observes the changes in the signs and symptoms of patient and the related laboratory data as well which affect the clinical outcome of the therapy.
TDM establishes safety and effectiveness of therapy.

Time
Pla
sma d
rug c
once
ntr
ati
on
MEC
MSCTherapeutic Range
Toxic Level
Subtherapeutic Level
Plasma drug Concentration Vs Time Plot

Necessity for TDM:
TDM is necessary for certain drugs having narrow therapeutic range or non-linear pharmacokinetics, where the dosage individualization becomes difficult.
It is useful in assessing the variability between the individual patient’s response to drug therapy which arises due to differences between:
Dose of the drug and its plasma concentration (Pharmacokinetic variability)
Concentration of the drug at the receptor site and its response (Pharmacodynamic variability)
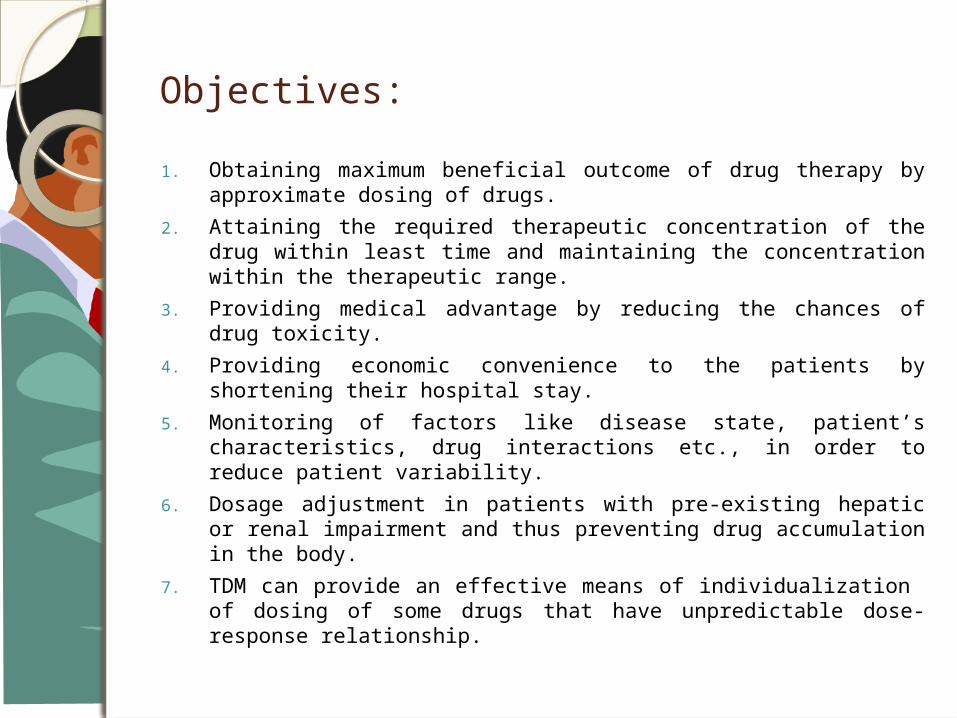
Objectives:
1. Obtaining maximum beneficial outcome of drug therapy by approximate dosing of drugs.
2. Attaining the required therapeutic concentration of the drug within least time and maintaining the concentration within the therapeutic range.
3. Providing medical advantage by reducing the chances of drug toxicity.
4. Providing economic convenience to the patients by shortening their hospital stay.
5. Monitoring of factors like disease state, patient’s characteristics, drug interactions etc., in order to reduce patient variability.
6. Dosage adjustment in patients with pre-existing hepatic or renal impairment and thus preventing drug accumulation in the body.
7. TDM can provide an effective means of individualization of dosing of some drugs that have unpredictable dose-response relationship.

Criteria for TDM:
The criteria for obtaining a valid TDM which is clinically effective is:
1. A well established correlation among concentration of drug in plasma and its therapeutic response and toxicity.
2. Meagre correlation between concentration of drug in plasma and its dose.
3. An acceptable evidence for performing TDM i.e., no response of the patient to the drug therapy, patient’s non-compliance, signs and symptoms of toxicity.
4. Availability of specific and well established methodology.
5. Collection of biological samples at regular intervals.
6. There should be sufficient clinical data which permits rapid and accurate interpretation of clinical outcome.
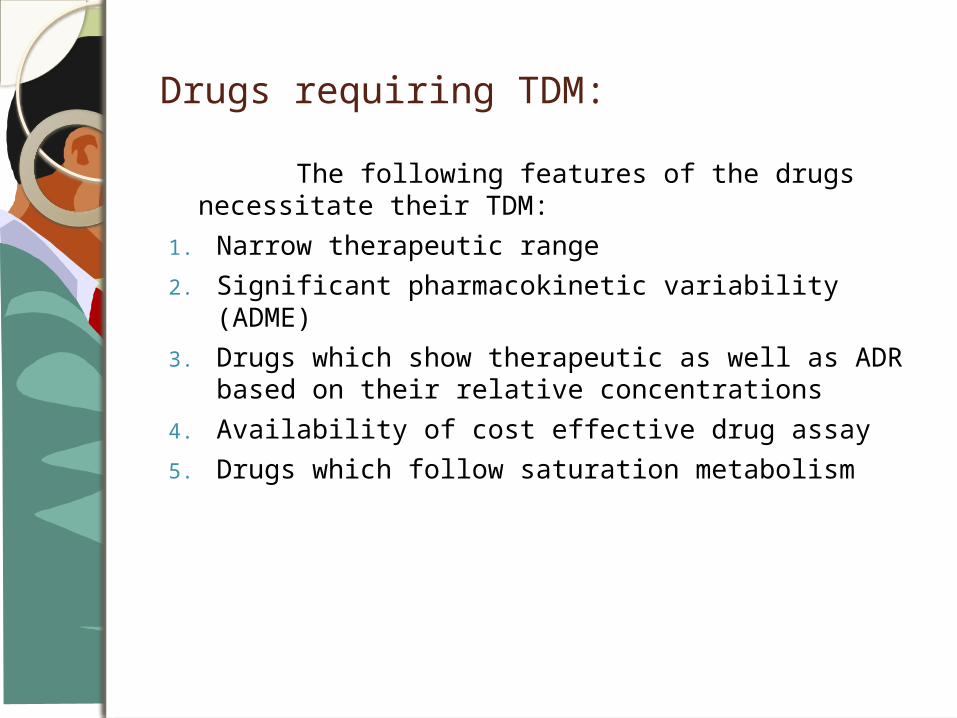
Drugs requiring TDM:
The following features of the drugs necessitate their TDM:
1. Narrow therapeutic range
2. Significant pharmacokinetic variability (ADME)
3. Drugs which show therapeutic as well as ADR based on their relative concentrations
4. Availability of cost effective drug assay
5. Drugs which follow saturation metabolism

1. Anticancer drugs- Paclitaxel, Cisplatin, Methotrexate
2. Antiepileptics- Phenytoin, Fosphenytoin, Valproic acid, Carbamazepin
3. Cardiotonics- Digoxin
4. Immunosupressants- Cyclosporin, Tacrolimus
5. Antibiotics- Ampicilline, Vancomycin
6. Antiarrythmics- Amiadarone, Lidocaine
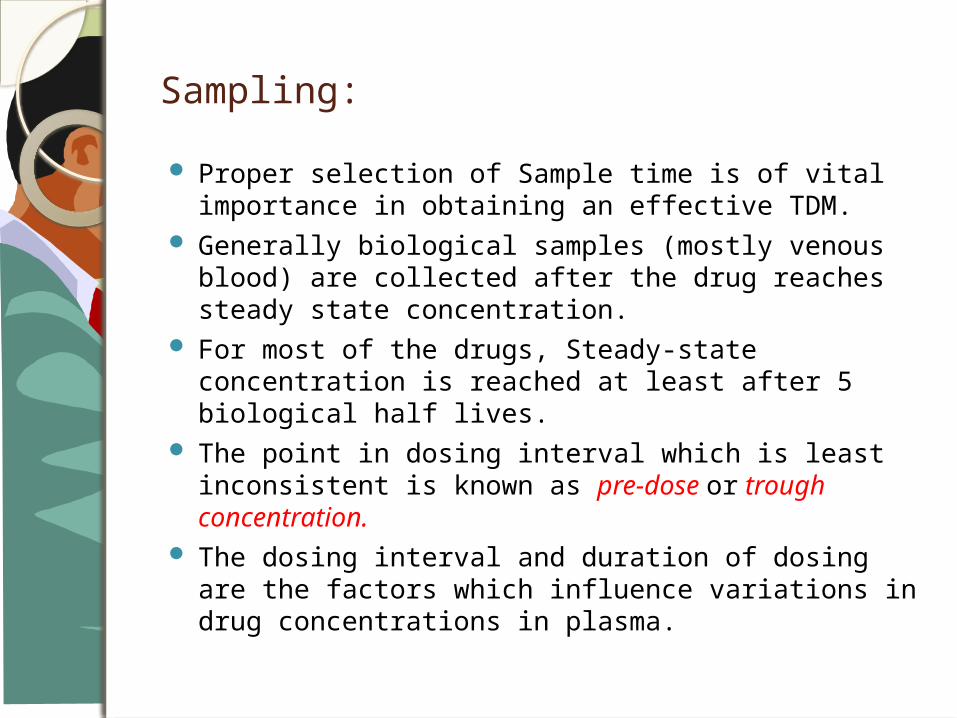
Sampling:
Proper selection of Sample time is of vital importance in obtaining an effective TDM.
Generally biological samples (mostly venous blood) are collected after the drug reaches steady state concentration.
For most of the drugs, Steady-state concentration is reached at least after 5 biological half lives.
The point in dosing interval which is least inconsistent is known as pre-dose or trough concentration.
The dosing interval and duration of dosing are the factors which influence variations in drug concentrations in plasma.
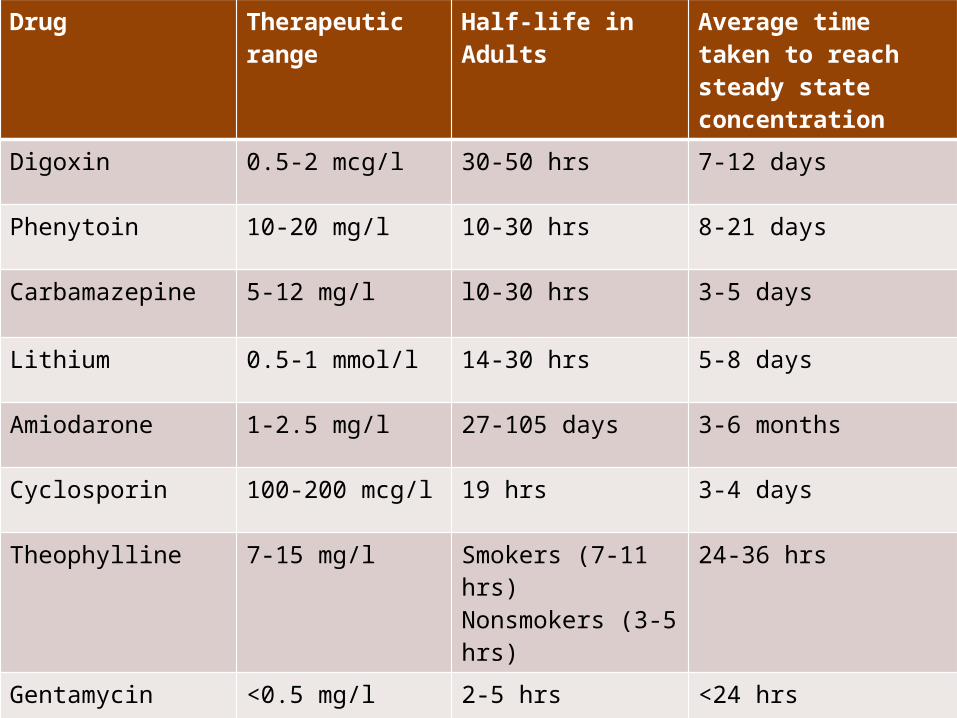
Drug Therapeutic range
Half-life in Adults
Average time taken to reach steady state concentration
Digoxin 0.5-2 mcg/l 30-50 hrs 7-12 days
Phenytoin 10-20 mg/l 10-30 hrs 8-21 days
Carbamazepine 5-12 mg/l l0-30 hrs 3-5 days
Lithium 0.5-1 mmol/l 14-30 hrs 5-8 days
Amiodarone 1-2.5 mg/l 27-105 days 3-6 months
Cyclosporin 100-200 mcg/l 19 hrs 3-4 days
Theophylline 7-15 mg/l Smokers (7-11 hrs)Nonsmokers (3-5 hrs)
24-36 hrs
Gentamycin <0.5 mg/l 2-5 hrs <24 hrs
Vancomycin 5-15 mg/l 3-8 hrs 24-48 hrs
Valproate 50-100 mg/l 6-20 hrs 3-5 days

Factors influencing plasma drug concentration:
1. Patient characteristics
2. Patient compliance
3. Dosage regimen and Duration of therapy
4. Time of sampling
5. Alteration in Protein binding
6. Alteration in elimination of drugs
7. Pathological characteristics
8. Drug interactions
9. Smoking and alcohol consumption
10. Sampling and Laboratory errors

Analytical techniques used in TDM:
The techniques chiefly employed for detection of drugs in a TDM laboratory are:
1. HPLC
2. GC/MS
3. LC/MS
4. RIA
5. PETINIA
6. EIA
7. EMIT
8. FPIA
9. CEDIA
10. Chemiluminiscence
11. One-step Dry Chemistry Technique
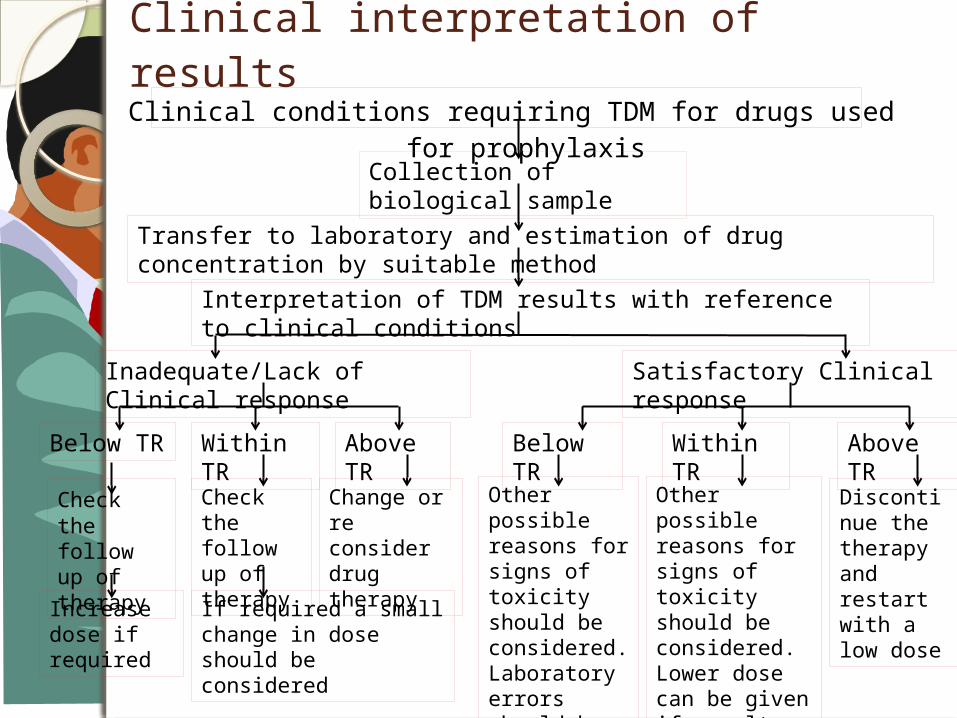
Clinical interpretation of resultsClinical conditions requiring TDM for drugs used for
prophylaxisCollection of biological sample
Transfer to laboratory and estimation of drug concentration by suitable method
Interpretation of TDM results with reference to clinical conditions
Inadequate/Lack of Clinical response
Satisfactory Clinical response
Below TR Within TR
Above TR
Check the follow up of therapy
Increase dose if required
If required a small change in dose should be considered
Change or re consider drug therapy
Check the follow up of therapy
Below TR
Within TR
Above TR
Other possible reasons for signs of toxicity should be considered. Laboratory errors should be checked
Other possible reasons for signs of toxicity should be considered. Lower dose can be given if result indicates the relief of disease
Discontinue the therapy and restart with a low dose
Role of Pharmacist in TDM:
A clinical pharmacist may assist other health care professionals by advising them about correct use if TDM- sampling time, sampling technique and interpretation of results.
They also may be engaged in:
1. Selecting initial drug dosage regimen-dose, dosing interval, route of administration, dosage form.
2. Depending upon the TDM results and patient’s response, revision and adjustment of dosage regimen should be done.
3. Assessing various other reasons for unexpected results like patient’s non-compliance, medication or laboratory errors, DDIs etc.
4. Evaluating and adjusting dosage for patients on haemodialysis.
5. Managing acute drug interactions.
Limitations of TDM:
Scientific accuracy of drug assays Laboratory variability in reporting Validity of suggested target ranges. Active metabolites which contribute to the
therapeutic response cannot be measured.
References
1. Birkett DJ. Therapeutic drug monitoring. Aust Prescr 1997;20:9-11
2. Therapeutic Drug Monitoring (TDM), An Educational Guide. www.siemens.com/diagnostics
3. Summers, K. K., T. C. Hardin, S. J. Gore, and J. R. Graybill. 1997. Therapeutic drug monitoring of systemic antifungal therapy. J. Antimicrob. Chemother. 40:753-764.
4. Schumacher GE. Clinical pharmacokinetics and therapeutic drug monitoring. Comprehensive pharmacy review; 7:732-741
5. Flexner D. Update on HIV pharmacology and therapeutic drug monitoring. Perspectives - Pharmacology and therapeutic drug monitoring Vol 9 Issue 3 July 2001
THANK YOU…
Related Documents