TB 101 Part II Brenda Mayes, R. N. March 2009

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

TB 101 Part II
Brenda Mayes, R. N. March 2009

TREATMENT TB DISEASE MDR XDR LATENT TB INFECTION

Who Is Responsible For TB Treatment?
See MMWR June 20,2003 pg 15 2.1 of Treatment of Tuberculosishttp://www.cdc.gov/tb/pubs/mmwr/maj_guide.htm
See TB Control Website VDH Standards of Care: Tuberculosis Controlhttp://www.vdh.virginia.gov/epidemiology/DiseasePrevention/Programs/Tuberculosis/Policies/

CDC and VIRGINIA GOALS forTREATMENT of ACTIVE TB
The initial TB interview conducted within 3 days for 95% of reported cases/suspects
90% will complete treatment in 12 months 100% of smear + TB will have appropriate
monitoring tests collected at appropriate intervals and will convert to culture negative within 90 days as evidenced by negative cultures on sputa collected on THREE separate days. Immediate investigation will be undertaken for cases that do not have culture conversion to identify cause

How Do We Treat Tuberculosis?
DIRECT OBSERVED THERAPY is the standard of care in Virginia
Every TB case in Virginia is assigned a PHN case manager

Antituberculosis Drugs Currently in Use in the US First-line Drugs
Isoniazid Rifampin Rifapentine Rifabutin Ethambutol Pyrazinamide
Second-line Drugs Cycloserine Ethionamide Levofloxacin Moxifloxacin Gatifloxacin P-Aminosalicylic acid Streptomycin Amikacin/kanamycin Capreomycin Linezolid

Treatment of MTB Case
Initial Phase – Direct Observed Therapy
7 d/wk for 56 doses or 5d/wk for 40 doses
(see page 3,4 and 5 of Treatment of TB)
INH Rifampin Ethambutol PZA

Treatment of MTB Case
CONTINUATION PHASE by DOT
Either 4 or 7 months
Daily 126 doses ( INH and RIF )
5X/wk 90 doses (INH and RIF )
2X/wk 36 doses (INH and RIF )
1X/wk 18 doses ( INH and RPT )
The 4 month continuation phase will
be used on most clients

Continuation Phase for 7 months
Cavitary pulmonary TB caused by drug-
susceptible organisms and whose sputum
culture obtained at completion of 2
month initial phase is positive No PZA in initial phase INH and Rifapentine 1X/wk whose
sputum culture is + at end of initial phase

Children with MTB
CXRs reveal different findings;
see MMWR 6-20-03 pg 55 section 8.2 Drug dosages are different Child = less than 40kg by weight or
less than 15 years old Not usually given ETH unless drug
resistance suspected or adult type cavitation on CXR
( visual acuity ) Younger than 4 start Tx ASAP

Drug Resistance
MDR (Multiple Drug Resistance)
INH AND Rifampin
XDR ( Extreme Drug Resistance)
INH and Rifampin plus any floroquinolone and
at least one of the three injectable second-line drugs (amikacin, kanamycin or capremycin)

Global Drug-Resistant TB: How Bad Is It?
2004 MDR TB estimates: 424,203 (4.3%)(estimate includes new and previously treated cases) 2000 MDR TB estimates: 272,906 (1.1%)(estimate includes new cases only)
Estimated 43% of global MDR TB cases have had prior treatment
China, India, and Russian Federation account for 62% of the MDR burden
Prevalence of XDR TB not known
Zignol, Dye et al, JID 2006:194


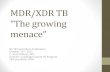
XDR TB Cases in the United States (Initial DST), 1993–2007*
2
1
1
8
11
2
1
2
NYC 16
New Jersey 31
* Preliminary data- not for distribution

Definitions
Primary drug resistance: Infected with TB which is already drug
resistant Secondary (acquired) drug resistance:
Drug resistance develops during treatment

What Causes Secondary Drug Resistance??
TREATMENT
FAILURE

Poor Patient Outcome Failure To Follow Principles Of Care
Providers should assess barriers to adherence and address them All patients should receive Directly Observed Therapy (DOT)
Acquired drug resistance may be associated with treatment failure (Clinical improvement? Reported? Serum levels?)
Repeat drug susceptibility studies should be ordered when cultures remain positive after three months
A single drug should never be added to a failing regimen
At least two and preferably three new drugs with proven or suspected susceptibility should be added
BS

Who Is At Higher Risk Of MDR-TB???
History of previous TB Tx especially if recent Foreign-born patients from countries or ethnicities
with high prevalence of MDR Poor response to standard 4 drug regimen Known exposure to MDR-TB case HIV+

Step 1Use any available
Begin with anyFirst line agents toWhich the isolate is Susceptible
Add aFluoroquinoloneAnd an injectableDrug based onsusceptibilities
Fluoroquinolones
Levofloxacin Moxifloxacin
Injectable agents
Amikacin Capreomycin Streptomycin Kanamycin
PLUSOne of these
One of these
First-line drugs
Pyrazinamide
Ethambutol
PLUS
BS

Step 1Use any available
Begin with anyFirst line agents toWhich the isolate is Susceptible
Add aFluoroquinoloneAnd an injectableDrug based onsusceptibilities
Fluoroquinolones
Levofloxacin Moxifloxacin
Injectable agents
Amikacin Capreomycin Streptomycin Kanamycin
PLUSOne of these
One of these
First-line drugs
Pyrazinamide
Ethambutol
PLUS
Step 2 Pick one or more of these
Oral second line drugs
Cycloserine Ethionamide PAS
Add 2nd line drugs until you have 4-6 drugs to which isolate is susceptible (which have not been used previously)

Step 3
Third line drugs
Imipenem Linezolid Macrolides Amoxicillin/Clavulanate
Consider use of these
If there are not 4-6 drugs available consider 3rd line in consult with MDRTB experts
Step 1Use any available
Begin with anyFirst line agents toWhich the isolate is Susceptible
Add aFluoroquinoloneAnd an injectableDrug based onsusceptibilities
Fluoroquinolones
Levofloxacin Moxifloxacin
Injectable agents
Amikacin Capreomycin Streptomycin Kanamycin
PLUSOne of these
One of these
First-line drugs
Pyrazinamide
Ethambutol
PLUS
Step 2 Pick one or more of these
Oral second line drugs
Cycloserine Ethionamide PAS
Add 2nd line drugs until you have 4-6 drugs to which isolate is susceptible (which have not been used previously)
BS

Criteria For Reporting TB Cases
All TB cases and suspects are required to be reported in Virginia (EPI 1) Positive smear Positive culture Clinical findings and/or treatment started
All children under age 4 found to have latent TB infection are required to be reported (EPI 1)

Counting Cases
Culture confirmed MTB Clinical TB Case
Keep on medicines for two months and if
there is clinical and radiographic improvement
and meets other CDC guidelines, can be
classified as a clinical case
Suspects

LTBI Treatment Regimens

Targeted Tuberculin Testing And Treatment Of Latent Tuberculosis Infection
MMWR June 9, 2000http://www.cdc.gov/tb/pubs/mmwr/maj_guide.htm
As tuberculosis (TB) disease rates in the United States (U.S.) decrease, finding and treating persons at high risk for latent TB infection (LTBI) has become a priority.

TB Risk Assessment
Use in conjunction with TST TB 512
CI risk assessment

STANDARDS OF CARECONTACTS
95% of all contacts of AFB smear + TB cases will be evaluated for disease and/or infection
CI will be initiated within 3 days of first notification and completed within 3 months
85% of contacts with MTB or LTBI will complete a full course of recommended treatment

Before Initiating Treatment
Rule out TB disease (i.e., wait for culture result if specimen obtained)
Determine prior history of treatment for LTBI or TB disease
Assess risks and benefits of treatment Determine current and previous drug therapy

Standards of Care:LTBI other than contacts
90% of clients screened for purposes other than CI will complete required f/u for evaluation of TB disease/infection
60% of clients recommended for treatment of LTBI will complete the recommended coarse of treatment thereby reducing their progression to active disease

Isoniazid Regimens 9-month regimen of isoniazid (INH) is the
preferred regimen (270 doses) 6-month regimen is less effective but may be
used if unable to complete 9 months May be given daily or intermittently (twice
weekly) Use directly observed therapy (DOT) for
intermittent regimen

Rifampin Regimens (1)
Rifampin (RIF) given daily for 4 months is an acceptable alternative when treatment with INH is not feasible.
In situations where RIF cannot be used (e.g., HIV-infected persons receiving protease inhibitors), rifabutin may be substituted.

Rifampin Regimens
RIF daily for 4 months (120 doses within 6 months)
RIF and PZA for 2 months should generally not be offered due to risk of severe adverse events

Completion of Therapy
Completion of therapy is based on the total number of doses administered, not on duration alone.

Who to Call
VDH DIVISION OF DISEASE PREVENTION
TB PROGRAM
Dr.Tipple 804-864-7916JANE MOORE (804) 864-7920
BRENDA MAYES (804) 864-7968

QUESTIONS?????????
Related Documents




![Preface XDR-TB Response Plan 2007-2008 · The Global Plan to Stop TB 2006-2015 [1]— and its companion piece, the Global MDR-TB and XDR-TB Response Plan 2007-2008 [2]—calls for](https://static.cupdf.com/doc/110x72/5e67e90334f19c1644738981/preface-xdr-tb-response-plan-2007-the-global-plan-to-stop-tb-2006-2015-1a-and.jpg)