..................................................................................................................................................................................... ..................................................................................................................................................................................... Sympathetic denervation is associated with microvascular dysfunction in non-infarcted myocardium in patients with cardiomyopathy Mischa T. Rijnierse 1,2 , Cornelis P. Allaart 1,2 , Stefan de Haan 1,2 , Hendrik J. Harms 3 , Marc C. Huisman 3 , LiNa Wu 1,2 , Aernout M. Beek 1,2 , Adriaan A. Lammertsma 3 , Albert C. van Rossum 1,2 , and Paul Knaapen 1,2 * 1 Department of Cardiology, VU University Medical Center, De Boelelaan 1117, PO Box 7057, Amsterdam, HV 1081, The Netherlands; 2 Institute for Cardiovascular Research (ICaR-VU), VU University Medical Center, Amsterdam, The Netherlands; and 3 Department of Radiology and Nuclear Medicine, VU University Medical Center, Amsterdam, The Netherlands Received 11 November 2014; accepted after revision 19 January 2015 Aims Sympathetic denervation typically occurs in the infarcted myocardium and is associated with sudden cardiac death. Impaired innervation was also demonstrated in non-infarcted myocardium in ischaemic and dilated cardiomyopathy (ICMP and DCMP). Factors affecting sympathetic nerve integrity in remote myocardium are unknown. Perfusion abnor- malities, even in the absence of epicardial coronary artery disease, may relate to sympathetic dysfunction. This study was aimed to assess the interrelations of myocardial blood flow (MBF), contractile function, and sympathetic innervation in non-infarcted remote myocardium. Methods and results Seventy patients with ICMP or DCMP and LVEF ≤35% were included. [ 15 O]H 2 O- and [ 11 C]hydroxyephedrine (HED) PET was performed to quantify resting MBF, hyperaemic MBF, and sympathetic innervation. Cardiovascular mag- netic resonance (CMR) imaging was performed to assess left ventricular function, mass, wall thickening, and scar size. Wall thickening, [ 11 C]HED retention index (RI), and MBF were assessed in remote segments without scar, selected on CMR. [ 11 C]HED RI was correlated with resting MBF (r ¼ 0.41, P , 0.001) and hyperaemic MBF (r ¼ 0.55, P , 0.001) in remote myocardium in both ICMP and DCMP. In addition, LV volumes (r ¼ 20.40, P ¼ 0.001), LV mass (r ¼ 20.31, P ¼ 0.008), and wall thickening (r ¼ 0.45, P , 0.001) correlated with remote [ 11 C]HED RI. Multivariable analysis revealed that hyper- aemic MBF (B ¼ 0.79, P , 0.001), wall thickening (B ¼ 0.01, P ¼ 0.03), and LVEDV (B ¼ 20.03, P ¼ 0.02) were inde- pendent predictors for remote [ 11 C]HED RI. Conclusion Hyperaemic MBF is independently associated with sympathetic innervation in non-infarcted remote myocardium in patients with ICMP and DCMP. This suggests that microvascular dysfunction might be an important factor related to sympathetic nerve integrity. Whether impaired hyperaemic MBF is the primary cause of this relation remains unclear. ----------------------------------------------------------------------------------------------------------------------------------------------------------- Keywords positron emission tomography † cardiovascular magnetic resonance † cardiomyopathy † sympathetic innervation † myocardial perfusion imaging Introduction Impaired cardiac sympathetic innervation in cardiomyopathy is asso- ciated with progression of heart failure and increased mortality. 1 Fur- thermore, it was recently demonstrated that the total denervation size as assessed with [ 11 C]Hydroxyephedrine positron emission tomography ([ 11 C]HED PET) predicts sudden cardiac death in patients with ischaemic cardiomyopathy (ICMP). 2 Sympathetic denervation typically results from myocardial infarction (MI) and often exceeds infarct size as myocardial nerves are more susceptible to ischaemia than myocardium itself. 2 – 6 Indeed, patients with chronic multivessel coronary artery disease (CAD) but without MI * Corresponding author. Tel: +31 20 4442441; Fax: +31 20 4442446, E-mail: [email protected] Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2015. For permissions please email: [email protected]. European Heart Journal – Cardiovascular Imaging doi:10.1093/ehjci/jev013 European Heart Journal - Cardiovascular Imaging Advance Access published February 21, 2015 by guest on February 25, 2015 Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Sympathetic denervation is associated withmicrovascular dysfunction in non-infarctedmyocardium in patients with cardiomyopathyMischa T. Rijnierse1,2, Cornelis P. Allaart1,2, Stefan de Haan1,2, Hendrik J. Harms3,Marc C. Huisman3, LiNa Wu1,2, Aernout M. Beek1,2, Adriaan A. Lammertsma3,Albert C. van Rossum1,2, and Paul Knaapen1,2*
1Department of Cardiology, VU University Medical Center, De Boelelaan 1117, PO Box 7057, Amsterdam, HV 1081, The Netherlands; 2Institute for Cardiovascular Research (ICaR-VU),VU University Medical Center, Amsterdam, The Netherlands; and 3Department of Radiology and Nuclear Medicine, VU University Medical Center, Amsterdam, The Netherlands
Received 11 November 2014; accepted after revision 19 January 2015
Aims Sympathetic denervation typically occurs in the infarcted myocardium and is associated with sudden cardiac death.Impaired innervation was also demonstrated in non-infarcted myocardium in ischaemic and dilated cardiomyopathy(ICMP and DCMP). Factors affecting sympathetic nerve integrity in remote myocardium are unknown. Perfusion abnor-malities, even in the absence of epicardial coronary artery disease, may relate to sympathetic dysfunction. This study wasaimed to assess the interrelations of myocardial blood flow (MBF), contractile function, and sympathetic innervation innon-infarcted remote myocardium.
Methodsand results
Seventy patients with ICMP or DCMP and LVEF ≤35% were included. [15O]H2O- and [11C]hydroxyephedrine(HED) PET was performed to quantify resting MBF, hyperaemic MBF, and sympathetic innervation. Cardiovascular mag-netic resonance (CMR) imagingwas performed toassess left ventricular function,mass, wall thickening, and scar size.Wallthickening, [11C]HED retention index (RI), and MBF were assessed in remote segments without scar, selected on CMR.[11C]HED RI was correlated with resting MBF (r ¼ 0.41, P , 0.001) and hyperaemic MBF (r ¼ 0.55, P , 0.001) in remotemyocardium in both ICMP and DCMP. In addition, LV volumes (r ¼ 20.40, P ¼ 0.001), LV mass (r ¼ 20.31, P ¼ 0.008),and wall thickening (r ¼ 0.45, P , 0.001) correlatedwith remote [11C]HED RI. Multivariable analysis revealed that hyper-aemic MBF (B ¼ 0.79, P , 0.001), wall thickening (B ¼ 0.01, P ¼ 0.03), and LVEDV (B ¼ 20.03, P ¼ 0.02) were inde-pendent predictors for remote [11C]HED RI.
Conclusion Hyperaemic MBF is independently associated with sympathetic innervation in non-infarcted remote myocardium inpatients with ICMP and DCMP. This suggests that microvascular dysfunction might be an important factor relatedto sympathetic nerve integrity. Whether impaired hyperaemic MBF is the primary cause of this relation remainsunclear.
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -Keywords positron emission tomography † cardiovascular magnetic resonance † cardiomyopathy † sympathetic innervation
† myocardial perfusion imaging
IntroductionImpaired cardiac sympathetic innervation in cardiomyopathy is asso-ciated with progression of heart failure and increased mortality.1 Fur-thermore, it was recently demonstrated that the total denervationsize as assessed with [11C]Hydroxyephedrine positron emission
tomography ([11C]HED PET) predicts sudden cardiac death inpatients with ischaemic cardiomyopathy (ICMP).2 Sympatheticdenervation typically results from myocardial infarction (MI) andoften exceeds infarct size as myocardial nerves are more susceptibleto ischaemia thanmyocardium itself.2– 6 Indeed, patients with chronicmultivessel coronary artery disease (CAD) but without MI
* Corresponding author. Tel: +31 20 4442441; Fax: +31 20 4442446, E-mail: [email protected]
Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2015. For permissions please email: [email protected].
European Heart Journal – Cardiovascular Imagingdoi:10.1093/ehjci/jev013
European Heart Journal - Cardiovascular Imaging Advance Access published February 21, 2015by guest on F
ebruary 25, 2015D
ownloaded from
demonstrate ischaemia-induced regional areas of denervation aswell.7,8 As most studies have focused on denervation in infarcted or is-chaemic areas, sympathetic innervation of non-infarcted remotemyocardium has not been studied extensively. Nonetheless, the in-tegrity of the innervation system in remote myocardium mayprovide important prognostic information and is related to cardiacremodelling.9– 11 In addition, these observations are not precludedto patients with ICMP but can similarly be observed in patientswith dilated cardiomyopathy (DCMP).12,13 It has been suggestedthat heterogeneity of sympathetic innervation may serve as anarrhythmic substrate preceding sudden cardiac death.14,15 It is there-fore of interest to gain more insight into factors influencing sympa-thetic nerve integrity in remote non-infarcted myocardium.Perfusion abnormalities, even in the absence of obstructive epicardialCAD, may play a role as a causal agent of sympathetic dysfunction. Infact, impaired perfusion has also been linked to an unfavourable prog-nosis in both ICMPand DCMP.16– 18 The aim of the present study wastherefore to explore the interrelations between myocardial perfu-sion, contractile function, and sympathetic innervation in non-infarcted remote myocardium in patients with ICMP and DCMP.
Methods
Study populationPatients with ICMP (n ¼ 52) and DCMP (n ¼ 18) with left ventricularejection fraction (LVEF) ≤35% were prospectively included. Patientswith a cardiac rhythm other than sinus rhythm were excluded. None ofthe patients displayed ischaemia or viability amenable to (further) revas-cularization at time of inclusion in the current study. All patients under-went [15O]H2O and [11C]HED PET imaging to assess resting MBF,hyperaemic MBF, and cardiac sympathetic innervation. Furthermore,late gadolinium-enhanced cardiovascular magnetic resonance imaging(LGE-CMR) was performed. The study was approved by the Ethics Com-mittee of the VU University Medical Center, in accordance with the Dec-laration of Helsinki, and written informed consent was obtained from allpatients.
CMR image acquisitionCMR studies were performed as described previously.19 In short, a clin-ical 1.5-T MRI scanner was used with a dedicated phased-array body coil.After survey scans, cine imaging was performed using a retrospectivelyECG-gated, steady-state free precession sequence during breath holdsin mild expiration. Standard four-, three-, and two-chamber orientationswere obtained, and subsequently, a stack of 10–12 consecutive short-axis slices was acquired, fully covering the left ventricle. Approximately10–15 min after administration of 0.2 mmol kg21 gadolinium, LGEimages were acquired in similar orientations as the cine images, using atwo-dimensional segmented inversion-recovery prepared gradientecho sequence. In case of difficulties with breath holding during LGEimaging, a single-shot sequence was used instead of a segmentedsequence.
CMR image analysisImages were analysed using dedicated software packages MASS (Massv.5.1 2010-EXP beta, Medis, Leiden, the Netherlands) and QMass(QMass v.7.5, Medis). Volumes, mass, and function were calculated onthe end-diastolic and end-systolic phases of the cine images. In addition,regional wall thickening was calculated as the percentage increase inwall thickness during the systole. Infarct size was calculated on LGE
images by using the full-width-at-half-maximum method.20 All segmentalanalyses were quantified according to the 17-segment American HeartAssociation model,21 excluding the apex. Using segmental LGE results,myocardial remote segments without scar were selected. Regional LVfunction in non-infarcted myocardium was calculated as the mean LVwall thickening in myocardial remote segments.
PET protocol and image acquisitionAll PET studieswereperformed using aPET/CTdevice (PhilipsGemini TF64, Philips Healthcare, Best, The Netherlands). Patients were instructedto refrain from intake of products containing caffeine or xanthine 24 hprior to the scan. All patients received a radial artery catheter for arterialblood sampling during the [11C]HED PET scan. The scanning protocolconsisted of two dynamic [15O]H2O scans, followed by a [11C]HEDscan. A 5 mL (0.8 mL.s21) bolus injection of [15O]H2O (370 MBq) fol-lowed by a 35 mL saline flush (2 mL.s21) was administered simultaneous-ly with the start of a 6-min emission scan. To correct for attenuation, arespiration-averaged low-dose CT scan was performed immediatelyafter the dynamic scan (55 mAs; rotation time, 1.5 s; pitch, 0.825; collima-tion, 64 × 0.625; acquiring 20 cm in 11 s) during normal breathing. Aftera 10-min interval to allow for decay of radioactivity, an identical PET se-quence was performed under infusion of intravenous adenosine(140 mg.kg21.min21). Adenosine infusion was started 2 min prior tothe start of the dynamic stress scan and was terminated after thelow-dose CT. Dynamic images were reconstructed into 22 frames(1 × 10, 8 × 5, 4 × 10, 2 × 15, 3 × 20, 2 × 30, and 2 × 60 s) usingthe three-dimensional row-action maximum likelihood algorithm (3DRAMLA), applying all appropriate corrections. After an interval of�15 min, a 5 mL (0.8 mL.s21) bolus [11C]HED (370 MBq) followed bya 35 mL saline flush (2 mL.s21) was injected simultaneously with thestart of a 60-min emission scan. During this scan, 7 mL arterial sampleswere collected manually at 2.5, 5, 10, 20, 30, 40, and 60 min to determineplasma and whole blood activity concentrations, and radiolabelledplasma [11C]HED metabolites. The dynamic scan was immediately fol-lowed by a respiration-averaged low-dose CT scan. Images were recon-structed into 36 frames (1 × 10, 8 × 5, 4 × 10, 3 × 20, 5 × 30, 5 × 60,4 × 150, 4 × 300, and 2 × 600 s) using the 3D RAMLA with applicationof all appropriate corrections.
PET image analysisPET image analysis was performed using in-house developed software.For both [15O]H2O and [11C]HED, image-derived input functionswere derived by placing 1 cm diameter regions of interest (ROIs) overthe ascending aorta in at least five transaxial planes showing the firstpass of the injected bolus. These ROIs were combined in one volumesof interest (VOI) for the ascending aorta. Furthermore, a right ventricularVOI was obtained by drawing a second set of ROIs in at least three trans-axial planes over the right ventricle. Subsequently, both VOIs were trans-ferred to the full dynamic images to obtain arterial whole blood and rightventricular time-activity curves (TACs). For [11C]HED image analysis,parent fractions and ratios of plasma/whole blood concentrationsderived from the manual blood samples were fitted to a sigmoid function.Subsequently, the arterial whole blood TAC was multiplied by the fittedplasma/whole blood ratio and parent fraction curves. For MBF analysis,parametric images of MBF, anatomic tissue fraction, perfusable tissuefraction (PTF), and arterial and venous blood volume fractions were gen-erated as previously described.22,23 Subsequently, segmental VOIs weredefined manually according to the 17-segment model of the AmericanHeart Association21 on short-axis images. For MBF analysis, short-axisPTF images were used, whereas for [11C]HED analysis, segmental VOIswere drawn on short-axis images in the final frame of the dynamic
M.T. Rijnierse et al.Page 2 of 11
by guest on February 25, 2015
Dow
nloaded from
scan. Finally, for MBF analysis, segmental VOI templates were projectedonto the entire dynamic emission scans to extract segmental TACsthat were fitted to a single tissue compartment model.
MBF was expressed in mL.min21.g21 of perfusable tissue. Coronaryflow reserve (CFR) was defined as the ratio of hyperaemic and restingMBF. Myocardial [11C]HED uptake was expressed using the retentionindex (RI) which was calculated as the uptake at the last frame(50260 min) divided by the integral of the arterial plasma-correctedTAC. Mean resting MBF, hyperaemic MBF, CFR, and [11C]HED RI wereassessed in myocardial segments without scar, selected duringLGE-CMR image analysis (excluding the apex). In case no enhancementwas present in patients with DCMP, global myocardium was consideredthe remote area.
Statistical analysisContinuous data are presented as means with standard deviations (SD),whereas categorical data are expressed as frequencies with percentages.Medians with inter-quartile range (IQR) were presented for non-parametric data. Histograms were used to evaluate whether continuousdata were normally distributed. Patient groups were compared usingunpaired Student’s t-tests for continuous data andx2 tests for categoricaldata. Levene’s test was used to verify whether the equal variancesassumption of the unpaired Student’s t-test was appropriate. In addition,non-parametric Mann–Whitney U test was used when appropriate. Forcomparisonsof paired continuous data, paired samples t-testwasapplied.The association between two continuous variables was analysed usingthe Pearson’s correlation coefficient. To assess the association of alldemographic and imaging variables with [11C]HED RI in remote
myocardium, univariate linear regression analyses were performed. Fur-thermore, a multivariable linear regression analysis was performed usinga backward selection procedure including all variables that were asso-ciated with [11C]HED RI in remote myocardium in univariate analysis(with P-value ,0.1). LVEDV and LVESV were analysed in separatemodels due to the interdependency (Model 1 and Model 2, respectively).Furthermore, as preserved innervation may result in preserved regionalwall thickening, a third multivariable analysis was performed excludingremote wall thickening and LVESV (Model 3). All tests were performedtwo-sided and were considered statistically significant if P-value ,0.05.All statistical analyses were performed using SPSS software package(SPSS 20.0, IBM Corporation, Chicago, IL, USA).
Results
Study populationA total of 70 patients were included in this study. Clinical baselinecharacteristics are presented in Table 1. Fifty-two (74%) patientssuffered from ICMP, whereas 18 (26%) patients were classifiedas DCMP. Patients with ICMP were more likely to be male (89vs. 61%, P ¼ 0.03) and more frequently use statins (90 vs. 39%,P , 0.001). Figure 1 shows examples of PET and CMR imaging intwo ICMP patients.
PETTable 2 summarizes haemodynamic parameters of all patientsduring PET at baseline and hyperaemic conditions. Overall, during
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
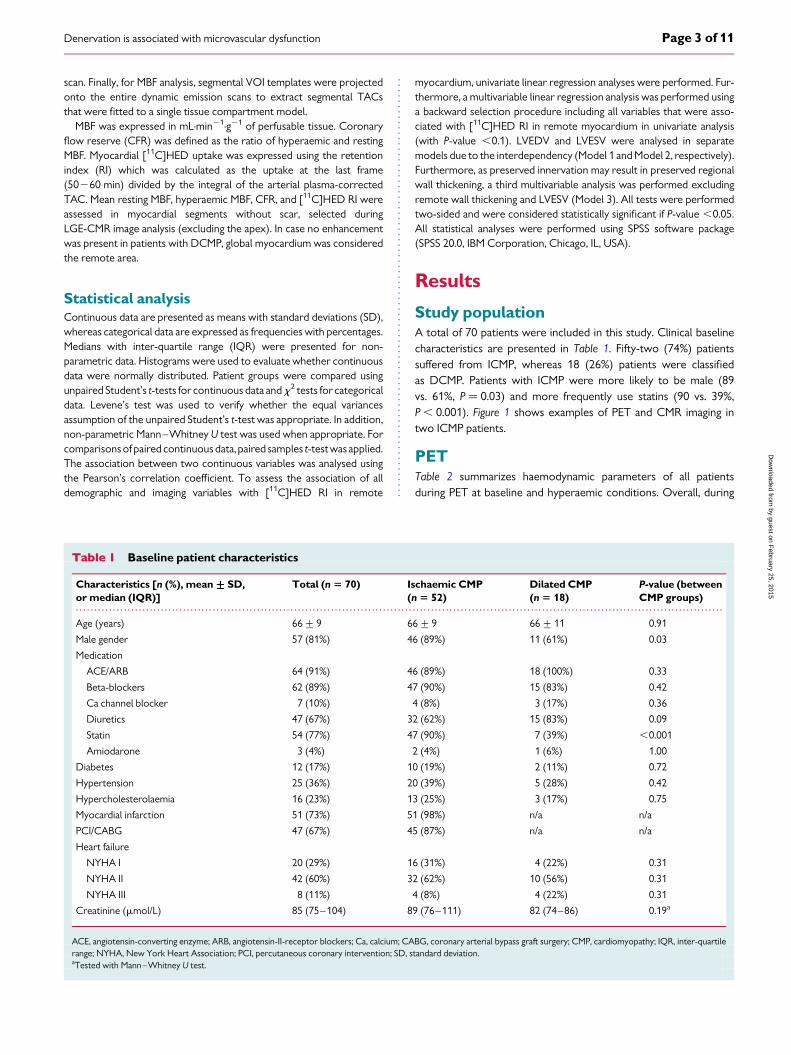
Table 1 Baseline patient characteristics
Characteristics [n (%), mean+++++SD,or median (IQR)]
Total (n 5 70) Ischaemic CMP(n 5 52)
Dilated CMP(n 5 18)
P-value (betweenCMP groups)
Age (years) 66+9 66+9 66+11 0.91
Male gender 57 (81%) 46 (89%) 11 (61%) 0.03
Medication
ACE/ARB 64 (91%) 46 (89%) 18 (100%) 0.33
Beta-blockers 62 (89%) 47 (90%) 15 (83%) 0.42
Ca channel blocker 7 (10%) 4 (8%) 3 (17%) 0.36
Diuretics 47 (67%) 32 (62%) 15 (83%) 0.09
Statin 54 (77%) 47 (90%) 7 (39%) ,0.001
Amiodarone 3 (4%) 2 (4%) 1 (6%) 1.00
Diabetes 12 (17%) 10 (19%) 2 (11%) 0.72
Hypertension 25 (36%) 20 (39%) 5 (28%) 0.42
Hypercholesterolaemia 16 (23%) 13 (25%) 3 (17%) 0.75
Myocardial infarction 51 (73%) 51 (98%) n/a n/a
PCI/CABG 47 (67%) 45 (87%) n/a n/a
Heart failure
NYHA I 20 (29%) 16 (31%) 4 (22%) 0.31
NYHA II 42 (60%) 32 (62%) 10 (56%) 0.31
NYHA III 8 (11%) 4 (8%) 4 (22%) 0.31
Creatinine (mmol/L) 85 (75–104) 89 (76–111) 82 (74–86) 0.19a
ACE, angiotensin-converting enzyme; ARB, angiotensin-II-receptor blockers; Ca, calcium; CABG, coronary arterial bypass graft surgery; CMP, cardiomyopathy; IQR, inter-quartilerange; NYHA, New York Heart Association; PCI, percutaneous coronary intervention; SD, standard deviation.aTested with Mann–Whitney U test.
Denervation is associated with microvascular dysfunction Page 3 of 11
by guest on February 25, 2015
Dow
nloaded from

Figure 1: Examples of PET and CMR imaging in two patients (A–D and E–H) with ischaemic cardiomyopathy. Both patients demonstrated a largemyocardial infarction at LGE-CMR (D and H) with corresponding PET perfusion and sympathetic innervation defects (A–C and E–G). QuantitativePET results of Patient 2 (E–H) revealed a relatively preserved hyperaemic MBF (E) and sympathetic innervation (F) in the non-infarcted remotemyocardium compared with hyperaemic MBF and sympathetic innervation of Patient 1 (A and B, respectively). Note the difference in MBF and[11C]HED RI scaling.
M.T. Rijnierse et al.Page 4 of 11
by guest on February 25, 2015
Dow
nloaded from
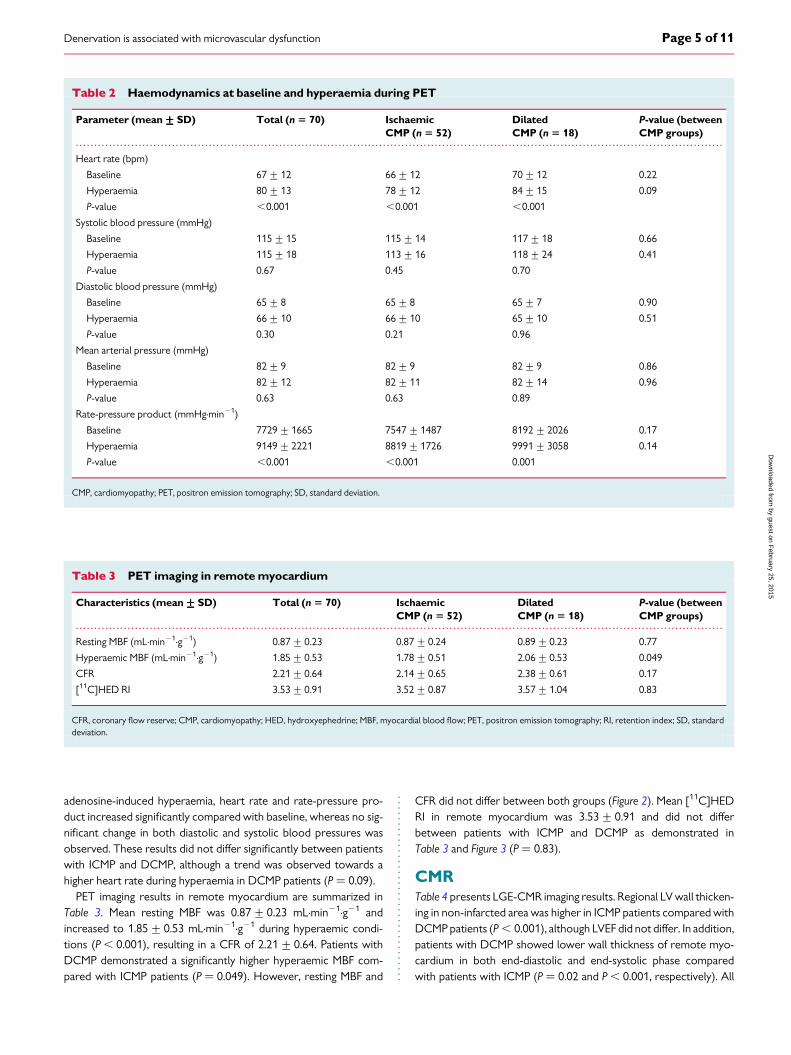
adenosine-induced hyperaemia, heart rate and rate-pressure pro-duct increased significantly compared with baseline, whereas no sig-nificant change in both diastolic and systolic blood pressures wasobserved. These results did not differ significantly between patientswith ICMP and DCMP, although a trend was observed towards ahigher heart rate during hyperaemia in DCMP patients (P ¼ 0.09).
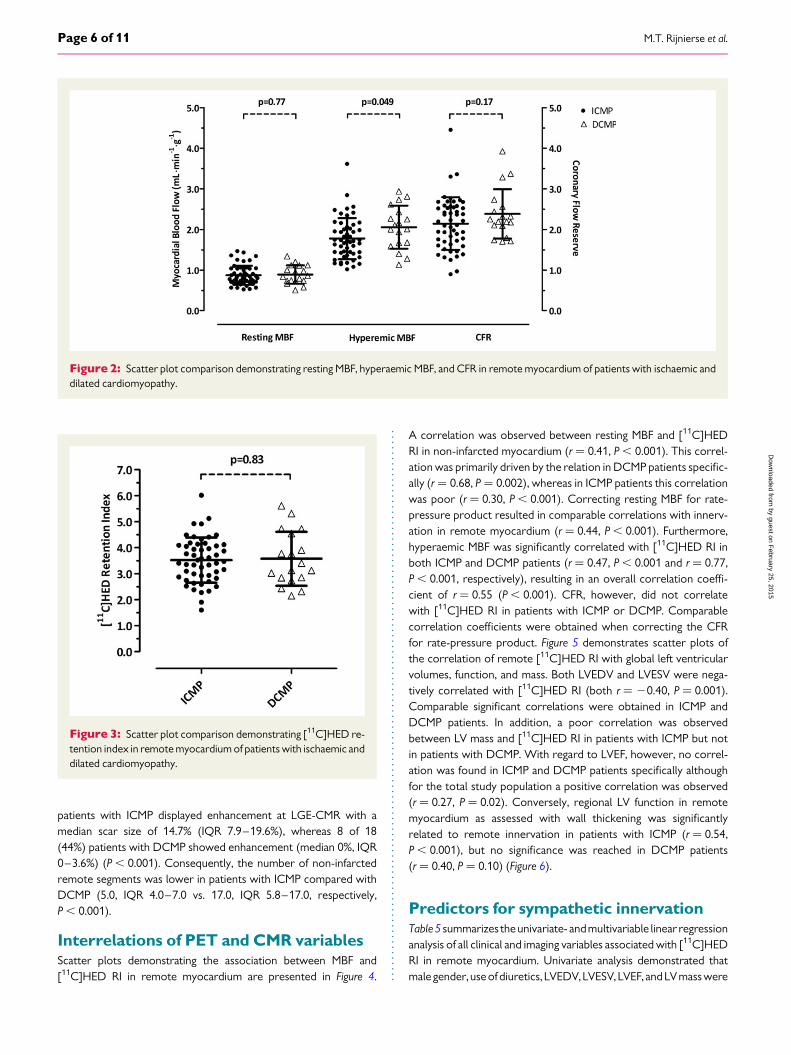
PET imaging results in remote myocardium are summarized inTable 3. Mean resting MBF was 0.87+0.23 mL.min21.g21 andincreased to 1.85+ 0.53 mL.min21.g21 during hyperaemic condi-tions (P , 0.001), resulting in a CFR of 2.21+0.64. Patients withDCMP demonstrated a significantly higher hyperaemic MBF com-pared with ICMP patients (P ¼ 0.049). However, resting MBF and
CFR did not differ between both groups (Figure 2). Mean [11C]HEDRI in remote myocardium was 3.53+ 0.91 and did not differbetween patients with ICMP and DCMP as demonstrated inTable 3 and Figure 3 (P ¼ 0.83).
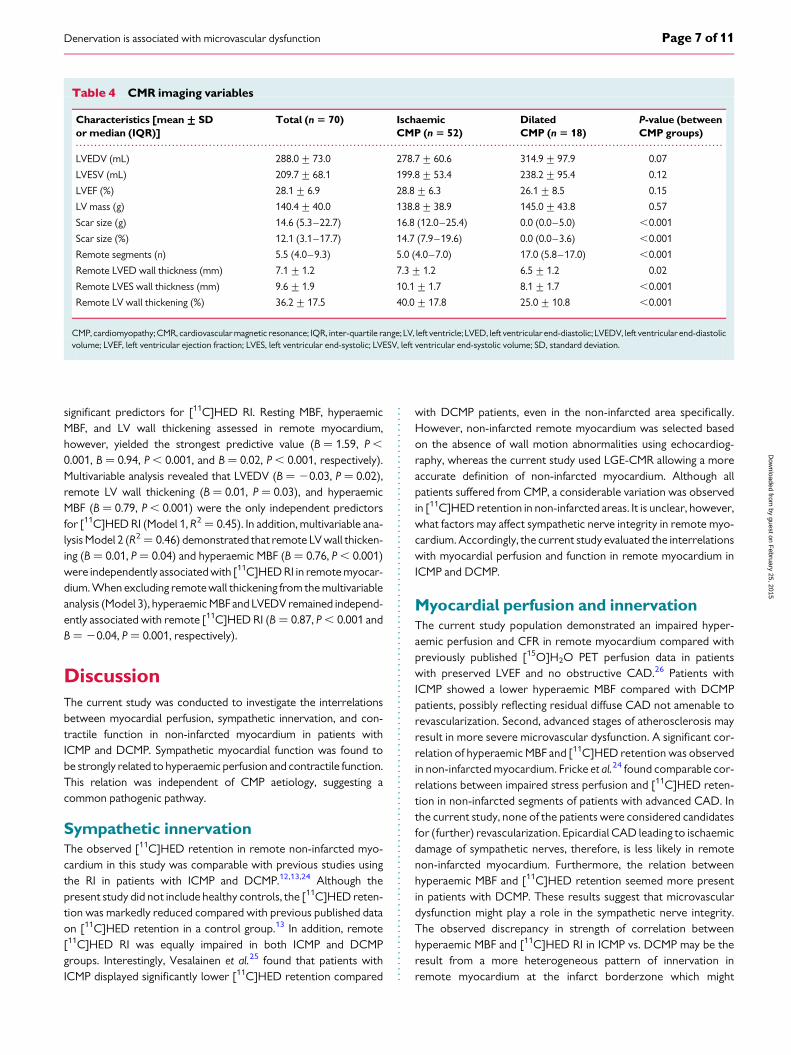
CMRTable 4 presents LGE-CMR imaging results. Regional LV wall thicken-ing in non-infarcted area was higher in ICMP patients compared withDCMP patients (P , 0.001), although LVEF did not differ. In addition,patients with DCMP showed lower wall thickness of remote myo-cardium in both end-diastolic and end-systolic phase comparedwith patients with ICMP (P ¼ 0.02 and P , 0.001, respectively). All
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 2 Haemodynamics at baseline and hyperaemia during PET
Parameter (mean+++++SD) Total (n 5 70) IschaemicCMP (n 5 52)
DilatedCMP (n 5 18)
P-value (betweenCMP groups)
Heart rate (bpm)
Baseline 67+12 66+12 70+12 0.22
Hyperaemia 80+13 78+12 84+15 0.09
P-value ,0.001 ,0.001 ,0.001
Systolic blood pressure (mmHg)
Baseline 115+15 115+14 117+18 0.66
Hyperaemia 115+18 113+16 118+24 0.41
P-value 0.67 0.45 0.70
Diastolic blood pressure (mmHg)
Baseline 65+8 65+8 65+7 0.90
Hyperaemia 66+10 66+10 65+10 0.51
P-value 0.30 0.21 0.96
Mean arterial pressure (mmHg)
Baseline 82+9 82+9 82+9 0.86
Hyperaemia 82+12 82+11 82+14 0.96
P-value 0.63 0.63 0.89
Rate-pressure product (mmHg.min21)
Baseline 7729+1665 7547+1487 8192+2026 0.17
Hyperaemia 9149+2221 8819+1726 9991+3058 0.14
P-value ,0.001 ,0.001 0.001
CMP, cardiomyopathy; PET, positron emission tomography; SD, standard deviation.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 3 PET imaging in remote myocardium
Characteristics (mean+++++SD) Total (n 5 70) IschaemicCMP (n 5 52)
DilatedCMP (n 5 18)
P-value (betweenCMP groups)
Resting MBF (mL.min21.g21) 0.87+0.23 0.87+0.24 0.89+0.23 0.77
Hyperaemic MBF (mL.min21.g21) 1.85+0.53 1.78+0.51 2.06+0.53 0.049
CFR 2.21+0.64 2.14+0.65 2.38+0.61 0.17
[11C]HED RI 3.53+0.91 3.52+0.87 3.57+1.04 0.83
CFR, coronary flow reserve; CMP, cardiomyopathy; HED, hydroxyephedrine; MBF, myocardial blood flow; PET, positron emission tomography; RI, retention index; SD, standarddeviation.
Denervation is associated with microvascular dysfunction Page 5 of 11
by guest on February 25, 2015
Dow
nloaded from
patients with ICMP displayed enhancement at LGE-CMR with amedian scar size of 14.7% (IQR 7.9–19.6%), whereas 8 of 18(44%) patients with DCMP showed enhancement (median 0%, IQR0–3.6%) (P , 0.001). Consequently, the number of non-infarctedremote segments was lower in patients with ICMP compared withDCMP (5.0, IQR 4.0–7.0 vs. 17.0, IQR 5.8–17.0, respectively,P , 0.001).
Interrelations of PET and CMR variablesScatter plots demonstrating the association between MBF and[11C]HED RI in remote myocardium are presented in Figure 4.
A correlation was observed between resting MBF and [11C]HEDRI in non-infarcted myocardium (r ¼ 0.41, P , 0.001). This correl-ation was primarily driven by the relation in DCMP patients specific-ally (r ¼ 0.68, P ¼ 0.002), whereas in ICMP patients this correlationwas poor (r ¼ 0.30, P , 0.001). Correcting resting MBF for rate-pressure product resulted in comparable correlations with innerv-ation in remote myocardium (r ¼ 0.44, P , 0.001). Furthermore,hyperaemic MBF was significantly correlated with [11C]HED RI inboth ICMP and DCMP patients (r ¼ 0.47, P , 0.001 and r ¼ 0.77,P , 0.001, respectively), resulting in an overall correlation coeffi-cient of r ¼ 0.55 (P , 0.001). CFR, however, did not correlatewith [11C]HED RI in patients with ICMP or DCMP. Comparablecorrelation coefficients were obtained when correcting the CFRfor rate-pressure product. Figure 5 demonstrates scatter plots ofthe correlation of remote [11C]HED RI with global left ventricularvolumes, function, and mass. Both LVEDV and LVESV were nega-tively correlated with [11C]HED RI (both r ¼ 20.40, P ¼ 0.001).Comparable significant correlations were obtained in ICMP andDCMP patients. In addition, a poor correlation was observedbetween LV mass and [11C]HED RI in patients with ICMP but notin patients with DCMP. With regard to LVEF, however, no correl-ation was found in ICMP and DCMP patients specifically althoughfor the total study population a positive correlation was observed(r ¼ 0.27, P ¼ 0.02). Conversely, regional LV function in remotemyocardium as assessed with wall thickening was significantlyrelated to remote innervation in patients with ICMP (r ¼ 0.54,P , 0.001), but no significance was reached in DCMP patients(r ¼ 0.40, P ¼ 0.10) (Figure 6).
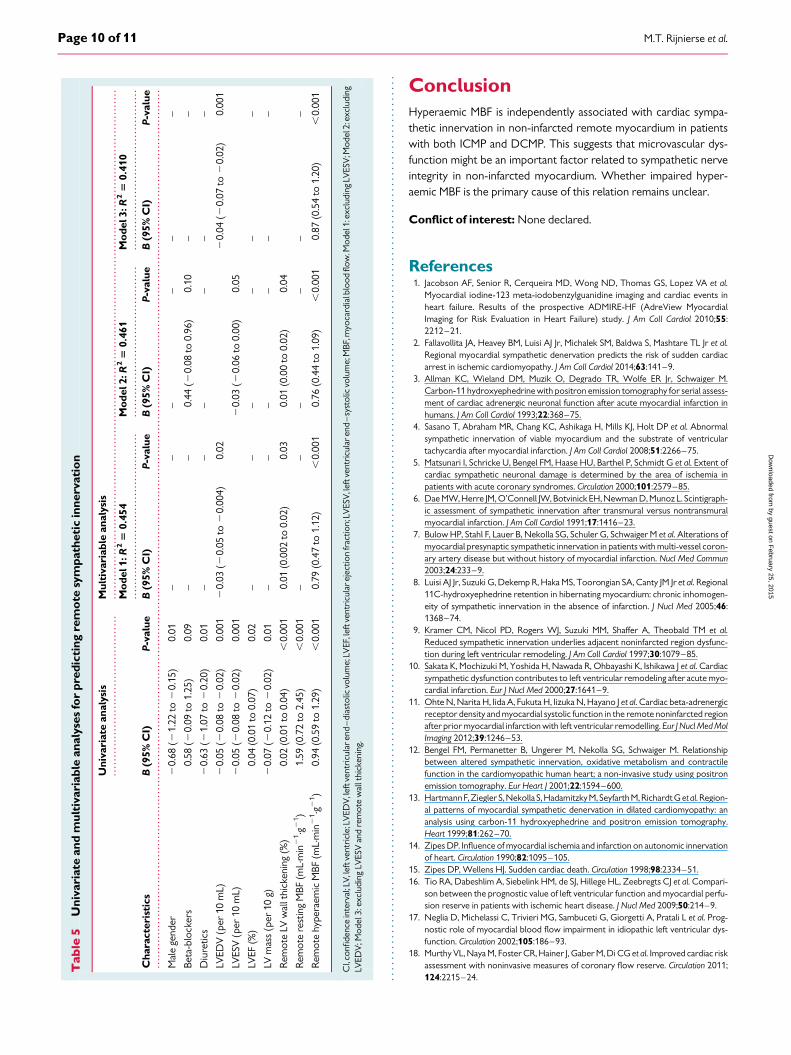
Predictors for sympathetic innervationTable5 summarizes the univariate- andmultivariable linear regressionanalysis of all clinical and imaging variables associated with [11C]HEDRI in remote myocardium. Univariate analysis demonstrated thatmale gender, use of diuretics, LVEDV, LVESV, LVEF, and LVmass were
Figure 3: Scatter plot comparison demonstrating [11C]HED re-tention index in remote myocardium of patients with ischaemic anddilated cardiomyopathy.
Figure 2: Scatter plot comparison demonstrating resting MBF, hyperaemic MBF, and CFR in remote myocardium of patients with ischaemic anddilated cardiomyopathy.
M.T. Rijnierse et al.Page 6 of 11
by guest on February 25, 2015
Dow
nloaded from
significant predictors for [11C]HED RI. Resting MBF, hyperaemicMBF, and LV wall thickening assessed in remote myocardium,however, yielded the strongest predictive value (B ¼ 1.59, P ,
0.001, B ¼ 0.94, P , 0.001, and B ¼ 0.02, P , 0.001, respectively).Multivariable analysis revealed that LVEDV (B ¼ 20.03, P ¼ 0.02),remote LV wall thickening (B ¼ 0.01, P ¼ 0.03), and hyperaemicMBF (B ¼ 0.79, P , 0.001) were the only independent predictorsfor [11C]HED RI (Model 1, R2 ¼ 0.45). In addition, multivariable ana-lysis Model 2 (R2 ¼ 0.46) demonstrated that remote LV wall thicken-ing (B ¼ 0.01, P ¼ 0.04) and hyperaemic MBF (B ¼ 0.76, P , 0.001)were independently associated with [11C]HED RI in remote myocar-dium. When excluding remote wall thickening from the multivariableanalysis (Model 3), hyperaemic MBF and LVEDV remained independ-ently associated with remote [11C]HED RI (B ¼ 0.87, P , 0.001 andB ¼ 20.04, P ¼ 0.001, respectively).
DiscussionThe current study was conducted to investigate the interrelationsbetween myocardial perfusion, sympathetic innervation, and con-tractile function in non-infarcted myocardium in patients withICMP and DCMP. Sympathetic myocardial function was found tobe strongly related to hyperaemic perfusion and contractile function.This relation was independent of CMP aetiology, suggesting acommon pathogenic pathway.
Sympathetic innervationThe observed [11C]HED retention in remote non-infarcted myo-cardium in this study was comparable with previous studies usingthe RI in patients with ICMP and DCMP.12,13,24 Although thepresent study did not include healthy controls, the [11C]HED reten-tion was markedly reduced compared with previous published dataon [11C]HED retention in a control group.13 In addition, remote[11C]HED RI was equally impaired in both ICMP and DCMPgroups. Interestingly, Vesalainen et al.25 found that patients withICMP displayed significantly lower [11C]HED retention compared
with DCMP patients, even in the non-infarcted area specifically.However, non-infarcted remote myocardium was selected basedon the absence of wall motion abnormalities using echocardiog-raphy, whereas the current study used LGE-CMR allowing a moreaccurate definition of non-infarcted myocardium. Although allpatients suffered from CMP, a considerable variation was observedin [11C]HED retention in non-infarcted areas. It is unclear, however,what factors may affect sympathetic nerve integrity in remote myo-cardium. Accordingly, the current study evaluated the interrelationswith myocardial perfusion and function in remote myocardium inICMP and DCMP.
Myocardial perfusion and innervationThe current study population demonstrated an impaired hyper-aemic perfusion and CFR in remote myocardium compared withpreviously published [15O]H2O PET perfusion data in patientswith preserved LVEF and no obstructive CAD.26 Patients withICMP showed a lower hyperaemic MBF compared with DCMPpatients, possibly reflecting residual diffuse CAD not amenable torevascularization. Second, advanced stages of atherosclerosis mayresult in more severe microvascular dysfunction. A significant cor-relation of hyperaemic MBF and [11C]HED retention was observedin non-infarcted myocardium. Fricke et al.24 found comparable cor-relations between impaired stress perfusion and [11C]HED reten-tion in non-infarcted segments of patients with advanced CAD. Inthe current study, none of the patients were considered candidatesfor (further) revascularization. Epicardial CAD leading to ischaemicdamage of sympathetic nerves, therefore, is less likely in remotenon-infarcted myocardium. Furthermore, the relation betweenhyperaemic MBF and [11C]HED retention seemed more presentin patients with DCMP. These results suggest that microvasculardysfunction might play a role in the sympathetic nerve integrity.The observed discrepancy in strength of correlation betweenhyperaemic MBF and [11C]HED RI in ICMP vs. DCMP may be theresult from a more heterogeneous pattern of innervation inremote myocardium at the infarct borderzone which might
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 4 CMR imaging variables
Characteristics [mean+++++SDor median (IQR)]
Total (n 5 70) IschaemicCMP (n 5 52)
DilatedCMP (n 5 18)
P-value (betweenCMP groups)
LVEDV (mL) 288.0+73.0 278.7+60.6 314.9+97.9 0.07
LVESV (mL) 209.7+68.1 199.8+53.4 238.2+95.4 0.12
LVEF (%) 28.1+6.9 28.8+6.3 26.1+8.5 0.15
LV mass (g) 140.4+40.0 138.8+38.9 145.0+43.8 0.57
Scar size (g) 14.6 (5.3–22.7) 16.8 (12.0–25.4) 0.0 (0.0–5.0) ,0.001
Scar size (%) 12.1 (3.1–17.7) 14.7 (7.9–19.6) 0.0 (0.0–3.6) ,0.001
Remote segments (n) 5.5 (4.0–9.3) 5.0 (4.0–7.0) 17.0 (5.8–17.0) ,0.001
Remote LVED wall thickness (mm) 7.1+1.2 7.3+1.2 6.5+1.2 0.02
Remote LVES wall thickness (mm) 9.6+1.9 10.1+1.7 8.1+1.7 ,0.001
Remote LV wall thickening (%) 36.2+17.5 40.0+17.8 25.0+10.8 ,0.001
CMP, cardiomyopathy; CMR, cardiovascular magnetic resonance; IQR, inter-quartile range; LV, left ventricle; LVED, left ventricular end-diastolic; LVEDV, left ventricular end-diastolicvolume; LVEF, left ventricular ejection fraction; LVES, left ventricular end-systolic; LVESV, left ventricular end-systolic volume; SD, standard deviation.
Denervation is associated with microvascular dysfunction Page 7 of 11
by guest on February 25, 2015
Dow
nloaded from

contain small areas of denervation in ICMP patients. However, assegments were carefully selected that did not show any scarduring LGE-CMR, the influence of heterogeneity at the infarctborder on the total remote [11C]HED retention is limited. No cor-relation of CFR and [11C]HED retention was demonstrated whichis most likely the result of the poor but significant correlation
between resting MBF and [11C]HED retention in remote myocar-dium. This might be explained by severe microvascular dysfunctionwhich may even be apparent in the assessment of resting MBF.In addition, the influence of flow-dependent tracer delivery of[11C]HED could be involved in this relation.
LV function and innervationThe population in the present study was characterized byan impairedLVEF in both ICMP and DCMP groups. Regional LV function inremotemyocardiumwas morepreserved in ICMPpatients, reflectingthe more globally impaired contractility in DCMP, whereas the func-tion impairment in ICMP is predominantly present in the infarct area.[11C]HED retention in remote myocardium was correlated withglobal LV volumes, consistent with the findings from Aoki et al.27 Inaddition, a poor correlation between global LVEF and [11C]HED re-tention was found in the total study population as consistentlydemonstrated in prior studies.12,13,27,28 However, most studies didnot focus on sympathetic innervation in remote myocardium specif-ically. Regional wall thickening in non-infarcted myocardium wasfound to correlate with [11C]HED retention predominantly inICMP patients, whereas no significance was reached in DCMPpatients. As previously mentioned, the contractility of remote myo-cardium in ICMP is relatively preserved compared with DCMP whichmight explain the observed discrepancy. Consistently, Bengel et al.12
found only a poor correlation between regional LV function and[11C]HED RI in patients with DCMP. In patients with ICMP,however, Aoki et al.27 demonstrated a stronger relation betweenregional LV function and [11C]HED RI non-infarcted myocardium.Furthermore, sympathetic innervation is importantly related to LVremodelling after MI.9,10
Predictors of sympathetic nerve integrityThe present study showed relations of sympathetic innervation inremote myocardium with LV volumes, wall thickening, resting perfu-sion, and hyperaemic perfusion. However, hyperaemic perfusion, re-gional wall thickening, and LVEDV were the only independentpredictors for [11C]HED retention in remote myocardium. In par-ticular, hyperaemic MBF demonstrated the strongest relation with[11C]HED retention, suggesting that microvascular dysfunctionplays an important role in sympathetic innervation in remote myo-cardium. Previous studies have demonstrated that impaired hyper-aemic perfusion independently predict mortality in patients DCMPand ICMP.16– 18 Furthermore, a relation was found between ventri-cular arrhythmia inducibility and impaired hyperaemic MBF, evenwhen assessing in remote non-infarcted areas.19 Impaired sympa-thetic innervation related to hyperaemic MBF might contribute tothe relation with electrical instability resulting in a higher risk of(sudden) cardiac death.
LimitationsThere are several limitations in this study. First, no cause–effect rela-tion between hyperaemic MBFand innervation was established in thisstudy. Consequently, whether impaired hyperaemic MBF is theprimary cause of impaired sympathetic innervation in remote myo-cardium remains unclear. Left ventricular remodelling may affectboth hyperaemic MBF and innervation. However, after correctionfor markers of LV remodelling in a multivariable analysis, hyperaemic
Figure 4: Scatter plots demonstrating the association of remote[11C]HED retention index with resting MBF (A), hyperaemic MBF(B), and CFR (C ) assessed in remote myocardium in patients withischaemic and dilated cardiomyopathy.
M.T. Rijnierse et al.Page 8 of 11
by guest on February 25, 2015
Dow
nloaded from

MBFremainedassociated with remote innervation. Secondly, compar-isons of smaller regions of remote myocardium in each patient mightprovide additional important correlative information. However, as
all imaging data were not exactly aligned, the current study exploredthe relation of mean innervation and perfusion in the total non-infarcted tissue to minimize the influence of misalignment betweenCMR, [11C]HED PET, and [15O]H2O PET. Thirdly, Harms et al.29
demonstrated that calculation of the volume of distribution of[11C]HED using a single tissue compartment model allows absolutequantification of [11C]HED activity which may be a more sophisti-cated way to describe the measured tracer activity compared withthe semi-quantitative RI from a technical point of view. However,as this model has not been clinically validated yet, it remainsunclear whether the single tissue compartment model leads to abetter assessment of actual presynaptic sympathetic nerve activity.The clinical importance of this model, therefore, remains unclear asmost clinical studies have used the RI to assess sympathetic innerv-ation.2– 4,12,13,25,27,28,30 In addition, due to the lack of a controlgroup, normal vs. abnormal remote innervation could not be distin-guished. Nonetheless, usage of the RI allowed comparisons with pre-vious published data that used the RI in CMP patients as well as incontrol groups. Finally, the partial volume effect is a limitation ofPET imaging, especially for [11C]HED quantification and may beinvolved in the current study as patients have enlarged ventricleswhich are thin walled. However, the extent of the partial volumeeffects on the assessed uptake of [11C]HED in remote myocardiumis unclear.
Figure5: Scatter plots demonstrating the association of remote [11C]HED retention indexwith LVEDV (A), LVESV (B), LVEF (C), and LV mass (D)in patients with ischaemic and dilated cardiomyopathy.
Figure 6: Scatter plot demonstrating the association of remote[11C]HED retention index with regional LV wall thickening in non-infarcted myocardium in patients with ischaemic and dilated cardio-myopathy.
Denervation is associated with microvascular dysfunction Page 9 of 11
by guest on February 25, 2015
Dow
nloaded from
ConclusionHyperaemic MBF is independently associated with cardiac sympa-thetic innervation in non-infarcted remote myocardium in patientswith both ICMP and DCMP. This suggests that microvascular dys-function might be an important factor related to sympathetic nerveintegrity in non-infarcted myocardium. Whether impaired hyper-aemic MBF is the primary cause of this relation remains unclear.
Conflict of interest: None declared.
References1. Jacobson AF, Senior R, Cerqueira MD, Wong ND, Thomas GS, Lopez VA et al.
Myocardial iodine-123 meta-iodobenzylguanidine imaging and cardiac events inheart failure. Results of the prospective ADMIRE-HF (AdreView MyocardialImaging for Risk Evaluation in Heart Failure) study. J Am Coll Cardiol 2010;55:2212–21.
2. Fallavollita JA, Heavey BM, Luisi AJ Jr, Michalek SM, Baldwa S, Mashtare TL Jr et al.Regional myocardial sympathetic denervation predicts the risk of sudden cardiacarrest in ischemic cardiomyopathy. J Am Coll Cardiol 2014;63:141–9.
3. Allman KC, Wieland DM, Muzik O, Degrado TR, Wolfe ER Jr, Schwaiger M.Carbon-11 hydroxyephedrine with positron emission tomography for serial assess-ment of cardiac adrenergic neuronal function after acute myocardial infarction inhumans. J Am Coll Cardiol 1993;22:368–75.
4. Sasano T, Abraham MR, Chang KC, Ashikaga H, Mills KJ, Holt DP et al. Abnormalsympathetic innervation of viable myocardium and the substrate of ventriculartachycardia after myocardial infarction. J Am Coll Cardiol 2008;51:2266–75.
5. Matsunari I, Schricke U, Bengel FM, Haase HU, Barthel P, Schmidt G et al. Extent ofcardiac sympathetic neuronal damage is determined by the area of ischemia inpatients with acute coronary syndromes. Circulation 2000;101:2579–85.
6. Dae MW, Herre JM, O’Connell JW, Botvinick EH, Newman D, Munoz L. Scintigraph-ic assessment of sympathetic innervation after transmural versus nontransmuralmyocardial infarction. J Am Coll Cardiol 1991;17:1416–23.
7. Bulow HP, Stahl F, Lauer B, Nekolla SG, Schuler G, Schwaiger M et al. Alterations ofmyocardial presynaptic sympathetic innervation in patients with multi-vessel coron-ary artery disease but without history of myocardial infarction. Nucl Med Commun2003;24:233–9.
8. Luisi AJ Jr, Suzuki G, Dekemp R, Haka MS, Toorongian SA, Canty JM Jr et al. Regional11C-hydroxyephedrine retention in hibernating myocardium: chronic inhomogen-eity of sympathetic innervation in the absence of infarction. J Nucl Med 2005;46:1368–74.
9. Kramer CM, Nicol PD, Rogers WJ, Suzuki MM, Shaffer A, Theobald TM et al.Reduced sympathetic innervation underlies adjacent noninfarcted region dysfunc-tion during left ventricular remodeling. J Am Coll Cardiol 1997;30:1079–85.
10. Sakata K, Mochizuki M, Yoshida H, Nawada R, Ohbayashi K, Ishikawa J et al. Cardiacsympathetic dysfunction contributes to left ventricular remodeling after acute myo-cardial infarction. Eur J Nucl Med 2000;27:1641–9.
11. Ohte N, Narita H, Iida A, Fukuta H, Iizuka N, Hayano J et al. Cardiac beta-adrenergicreceptor density and myocardial systolic function in the remote noninfarcted regionafter prior myocardial infarction with left ventricular remodelling. Eur J Nucl Med MolImaging 2012;39:1246–53.
12. Bengel FM, Permanetter B, Ungerer M, Nekolla SG, Schwaiger M. Relationshipbetween altered sympathetic innervation, oxidative metabolism and contractilefunction in the cardiomyopathic human heart; a non-invasive study using positronemission tomography. Eur Heart J 2001;22:1594–600.
13. HartmannF, Ziegler S, Nekolla S, Hadamitzky M, Seyfarth M,RichardtG et al. Region-al patterns of myocardial sympathetic denervation in dilated cardiomyopathy: ananalysis using carbon-11 hydroxyephedrine and positron emission tomography.Heart 1999;81:262–70.
14. Zipes DP. Influence of myocardial ischemia and infarction on autonomic innervationof heart. Circulation 1990;82:1095–105.
15. Zipes DP, Wellens HJ. Sudden cardiac death. Circulation 1998;98:2334–51.16. Tio RA, Dabeshlim A, Siebelink HM, de SJ, Hillege HL, Zeebregts CJ et al. Compari-
son between the prognostic value of left ventricular function and myocardial perfu-sion reserve in patients with ischemic heart disease. J Nucl Med 2009;50:214–9.
17. Neglia D, Michelassi C, Trivieri MG, Sambuceti G, Giorgetti A, Pratali L et al. Prog-nostic role of myocardial blood flow impairment in idiopathic left ventricular dys-function. Circulation 2002;105:186–93.
18. Murthy VL, Naya M, Foster CR, Hainer J, Gaber M, Di CG et al. Improved cardiac riskassessment with noninvasive measures of coronary flow reserve. Circulation 2011;124:2215–24.
....
....
....
....
....
....
....
....
....
....
...
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
..
....
....
....
....
....
....
....
....
....
....
....
...
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
.
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
.
Tab
le5
Uni
vari
ate
and
mul
tiva
riab
lean
alys
esfo
rpr
edic
ting
rem
ote
sym
path
etic
inne
rvat
ion
Uni
vari
ate
anal
ysis
Mul
tiva
riab
lean
alys
is
Mo
del1
:R2
50.
454
Mo
del2
:R2
50.
461
Mo
del3
:R2
50.
410
Cha
ract
eris
tics
B(9
5%C
I)P-
valu
eB
(95%
CI)
P-va
lue
B(9
5%C
I)P-
valu
eB
(95%
CI)
P-va
lue
Mal
ege
nder
20.
68(2
1.22
to2
0.15
)0.
01–
––
––
–
Beta
-blo
cker
s0.
58(2
0.09
to1.
25)
0.09
––
0.44
(20.
08to
0.96
)0.
10–
–
Diu
retic
s2
0.63
(21.
07to
20.
20)
0.01
––
––
––
LVED
V(p
er10
mL)
20.
05(2
0.08
to2
0.02
)0.
001
20.
03(2
0.05
to2
0.00
4)0.
022
0.04
(20.
07to
20.
02)
0.00
1
LVES
V(p
er10
mL)
20.
05(2
0.08
to2
0.02
)0.
001
20.
03(2
0.06
to0.
00)
0.05
LVEF
(%)
0.04
(0.0
1to
0.07
)0.
02–
––
––
–
LVm
ass
(per
10g)
20.
07(2
0.12
to2
0.02
)0.
01–
––
––
–
Rem
ote
LVw
allt
hick
enin
g(%
)0.
02(0
.01
to0.
04)
,0.
001
0.01
(0.0
02to
0.02
)0.
030.
01(0
.00
to0.
02)
0.04
Rem
ote
rest
ing
MBF
(mL.
min
21. g
21)
1.59
(0.7
2to
2.45
),
0.00
1–
––
––
–
Rem
ote
hype
raem
icM
BF(m
L.m
in2
1. g
21)
0.94
(0.5
9to
1.29
),
0.00
10.
79(0
.47
to1.
12)
,0.
001
0.76
(0.4
4to
1.09
),
0.00
10.
87(0
.54
to1.
20)
,0.
001
CI,
confi
denc
ein
terv
al;L
V,l
eftv
entr
icle
;LV
EDV
,lef
tven
tric
ular
end
–di
asto
licvo
lum
e;LV
EF,l
eftv
entr
icul
arej
ectio
nfr
actio
n;LV
ESV
,lef
tven
tric
ular
end
–sy
stol
icvo
lum
e;M
BF,m
yoca
rdia
lblo
odflo
w.M
odel
1:ex
clud
ing
LVES
V;M
odel
2:ex
clud
ing
LVED
V;M
odel
3:ex
clud
ing
LVES
Van
dre
mot
ew
allt
hick
enin
g.
M.T. Rijnierse et al.Page 10 of 11
by guest on February 25, 2015
Dow
nloaded from
19. Rijnierse MT, de Haan S, Harms HJ, Robbers LF, Wu L, Danad I et al. Impaired hyper-emic myocardial blood flow is associated with inducibility of ventricular arrhythmiain ischemic cardiomyopathy. Circ Cardiovasc Imaging 2014;7:20–30.
20. Flett AS, Hasleton J, Cook C, Hausenloy D, Quarta G, Ariti Cet al. Evaluation of tech-niques for the quantification of myocardial scar of differing etiology using cardiacmagnetic resonance. JACC Cardiovasc Imaging 2011;4:150–6.
21. Cerqueira MD, Weissman NJ, Dilsizian V, Jacobs AK, Kaul S, Laskey WK et al.Standardized myocardial segmentation and nomenclature for tomographic imagingof the heart. A statement for healthcare professionals from the Cardiac ImagingCommittee of the Council on Clinical Cardiology of the American Heart Associ-ation. Circulation 2002;105:539–42.
22. Harms HJ, de Haan S, Knaapen P, Allaart CP, Lammertsma AA, Lubberink M. Para-metric images of myocardial viability using a single 15O-H2O PET/CT scan. J NuclMed 2011;52:745–9.
23. Harms HJ, Knaapen P, de Haan S, Halbmeijer R, Lammertsma AA, Lubberink M.Automatic generation of absolute myocardial blood flow images using [15O]H2Oand a clinical PET/CT scanner. Eur J Nucl Med Mol Imaging 2011;38:930–9.
24. Fricke E, Fricke H, Eckert S, Zijlstra S, Weise R, Lindner O et al. Myocardial sympa-thetic innervation in patients with chronic coronary artery disease: is reduction incoronary flow reserve correlated with sympathetic denervation? Eur J Nucl MedMol Imaging 2007;34:206–11.
25. Vesalainen RK, Pietila M, Tahvanainen KU, Jartti T, Teras M, Nagren K et al. Cardiacpositron emission tomography imaging with [11C]hydroxyephedrine, a specifictracer for sympathetic nerve endings, and its functional correlates in congestiveheart failure. Am J Cardiol 1999;84:568–74.
26. Danad I, Raijmakers PG, Appelman YE, Harms HJ, de Haan S, van den Oever ML et al.Coronary risk factors and myocardial blood flow in patients evaluated for coronaryartery disease: a quantitative [15O]H2O PET/CT study. Eur J Nucl Med Mol Imaging2012;39:102–12.
27. Aoki H, Matsunari I, Nomura Y, Fujita W, Komatsu R, Miyazaki Y et al. Myocardialsympathetic innervation, function, and oxidative metabolism in non-infarcted myo-cardium in patients with prior myocardial infarction. Ann Nucl Med 2013;27:523–31.
28. Matsunari I, Aoki H, Nomura Y, Takeda N, Chen WP, Taki J et al. Iodine-123 metaio-dobenzylguanidine imaging and carbon-11 hydroxyephedrine positron emissiontomography compared in patients with left ventricular dysfunction. Circ CardiovascImaging 2010;3:595–603.
29. Harms HJ, De Haan S, Knaapen P, Allaart CP, Rijnierse MT, Schuit RC et al. Quanti-fication of [11C]-meta-hydroxyephedrine uptake in human myocardium. EJNMMIResearch 2014;4:0.
30. Bengel FM, Permanetter B, Ungerer M, Nekolla SG, Schwaiger M. Alterations of thesympathetic nervous system and metabolic performance of the cardiomyopathicheart. Eur J Nucl Med Mol Imaging 2002;29:198–202.
Denervation is associated with microvascular dysfunction Page 11 of 11
by guest on February 25, 2015
Dow
nloaded from
Related Documents











