ISCHAEMIC CARDIAC TISSUE REPURFUSION WAS

ISCHAEMIC CARDIAC TISSUE REPURFUSION WAS. The result shows Ischaemic/Infarcted myocardium reperfused adequately and rapidly, with induction of mature.
Dec 30, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ISCHAEMIC CARDIAC TISSUE REPURFUSION WAS

The result shows
Ischaemic/Infarcted myocardium reperfused adequately and rapidly, with induction of mature capillary formation very early
Induction of angiogenic bud formation within 96 hrs.
Various routes of application attempted. All give adequate induction.I.V. route being the simplest.
Regenerating/reclaimed myocardial islands, very obvious.
Fibrous tissue zone(s), in acute infarct model, shows "Development of continuity". [ Significance to be studied further]
Cardiac Angiogenesis and Reperfusion

The healing --
Mode of induction of controllable angiogenesis is similaras in wound repair.
The molecule, being "natural", is non-toxic even in loading dose.
Cost of therapy is very low.
Now contrast this with the conventional mode(s) of therapy:
(CABG), angioplasty and stenting --- incidence of recurrenceis very high.
Cost of therapy is reasonably high in all approaches- conventional as well as upcoming e.g. gene therapy, stem-cell implantation, therapy through traditional angiogenic factors e.g. VEGF etc.

Normal sheep myocardium
Cardiac Angiogenesis and Reperfusion :-
Normal myocardium getting replaced byfibrous tissue in acute infarction model (surgical)
Histopathology of reperfused myocardium treated with amino acid lysine applied through I.V. route, showing extensive healthy blood filled capillaries, regenerated within three weeks of treatment.
? Regenerating/ Reclaimed Myocardium
Fibrous tissue showing a definite reversal towards continuity( ? regenerating / reclaimed myocardium )
Extensive network of regenerating capillaries
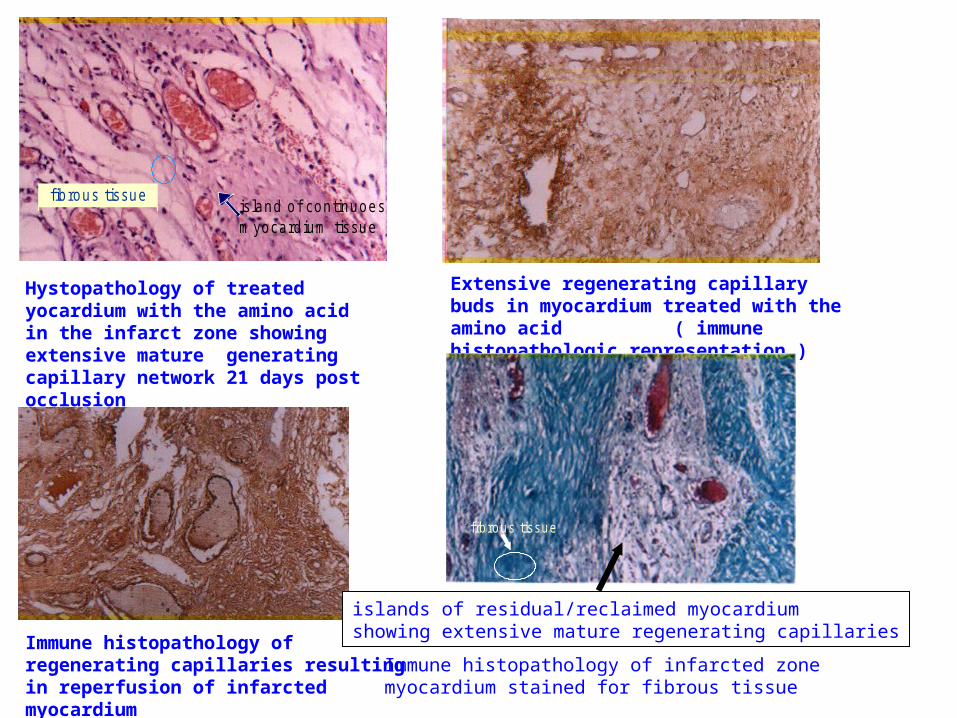
fibrous tissueisland of continuoesm yocardium tissue
Hystopathology of treated yocardium with the amino acid in the infarct zone showing extensive mature generating capillary network 21 days post occlusion
Extensive regenerating capillary buds in myocardium treated with the amino acid ( immune histopathologic representation )
Immune histopathology of regenerating capillaries resulting in reperfusion of infarcted myocardium
frbrous tissue
islands of residual/reclaimed myocardiumshowing extensive mature regenerating capillaries
Immune histopathology of infarcted zonemyocardium stained for fibrous tissue
Reclaiming Stroke Cases was never easier ………
ISCHAEMIC CEREBRAL / NEURAL TISSUE
Induction of Controllable Therapeutic Angiogenesis (CTA) caused rapid reperfusion of infarct mass in ( through i.v. route) the patients with various degree of paresis and paralysis, in
Tubercular Meningitis
Stroke
Time required for such induction and reperfusion was withinthe 240 hrs. from the onset of application of the molecule.
Induction of CTA was " Irreversible" through IV route.
Patients in various degrees of Paresis and Paralysis showed completerecovery within two (2) weeks in cases of Stroke.
Thrombosis and Embolism had more effects towards reperfusion.
Massive cerebral hemorrhages showed little delayed recovery.( Might be due to the "intereference" in the " Local Autocrine Effect(s)" induced by the molecule due to presence of Oedema.
*
*

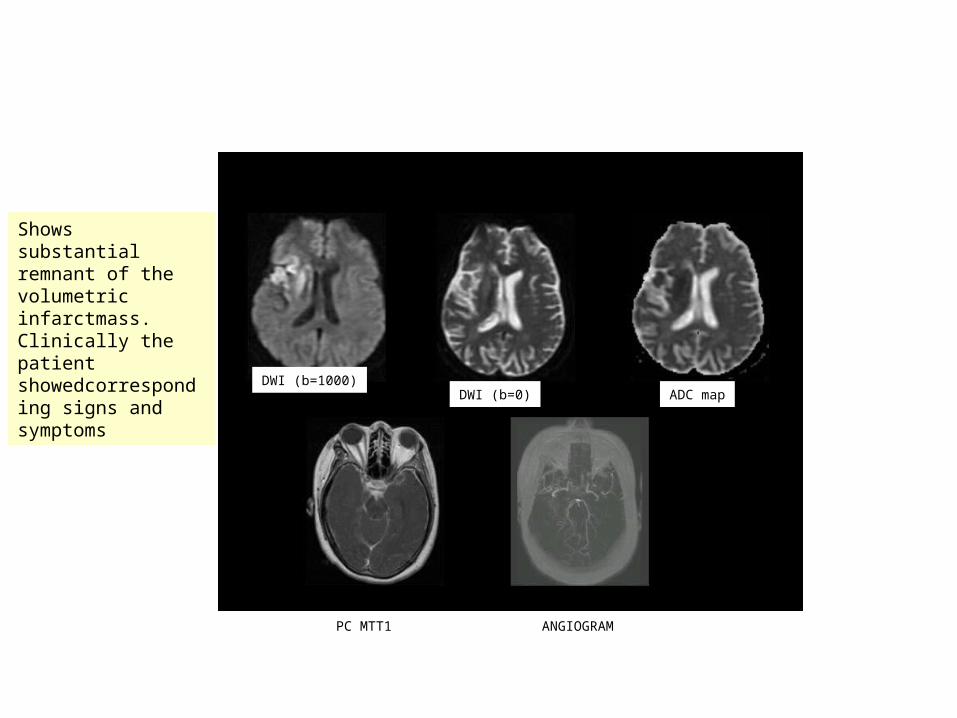
DWI (b=1000)DWI (b=0)
ADC map
PC MTT1
ANGIOGRAM
Site of obstruction
Diffusion weighted MRI in Panel1 ( in a case of TB Meningitis) showing volume infarct on the rightcerebral hemisphere
DAY 0 OBSERVATIONS
shows basal meningial inflamation (TB meningiatis)

DAY 10 OBSERVATIONS
showing totalresolution of theinfarct mass
DWI (b=1000) DWI (b=0) ADC map
ANGIOGRAM
PC MTT1
Near total resolution of inflammation

1st study 2nd study
3rd study
Views of Angiogram in Cerebral Stroke

Angiogram Study of Stroke Patients
Magnified Views of Angiogram in
Cerebral Stroke

DWI (b=1000)DWI (b=0)
DWI (b=0)
Control TB meningitis( not treated with the amino acid )
INFARCT TREATED CONVENTIONALLY, DAY 0
NOT TREATED WITH X MOLECULE, DAY 10
Shows substantialremnant of the volumetric infarctmass. Clinically the patient showedcorresponding signs and symptoms
DWI (b=1000)DWI (b=0) ADC map
ANGIOGRAMPC MTT1
THE MOLECULE
An essential amino acid - Lysine.
Although, it is present as one of the members in the blood amino acid pool
And
Angiogenic factor(s) are present in all conditions of Ischaemia/Infarction
The new found biochemical properties of the amino acidprobably require a "Window Concentration".
Metabolic role(s) of the molecule is obvious at the availableconcentrations (as in the amino acid pool),
Angiogenic property (and other newfound biochemical roles)is obvious at a much higher concentration
Current working hypothesis - On the possible mode of action
In a particular augmented concentration window, probably acts as a molecular bridge between cell-surface receptors and available angiogenic factor(s).
The molecule, only acts as a bridge, as long as required concentration of angiogenic factor(s) is available in a given anatomical location, under the ischaemic stress (Withdrawal of the molecule stops the process).
Induction of therapeutic angiogenesis is totally controllable
The two distinctive amino groups at two ends of themolecule (lysine), looks extremely attractive.
In conditions of ischaemia, when the tissue pH is more acidic, chances of protonation of these groups are high, leading to generation of - NH3+ groups, which are probably capable of generating "reasonable“ numbers of hydrogen bondings with other charged species (e.g. R- groups of amino acids in receptors as well as in angiogenic/growth factor(s)), which, probably, give the combination (of ligand and receptor), some sort of "stability" which is more than an usual hit-and-miss process of any ligand-receptor interaction and "just less" than a covalent linkage .

Key Issues: -
Titres of angiogenic factor(s), under a given condition of ischaemia /infarction
Not all subjects are equal producers of same amounts of angiogenic factor(s) under the same stress of ischaemia and infarction.
Therefore, important considerations :
a.Age of the patient.b.How old is the infarct/ ischaemia.
In cases where both a and /or b are advanced in nature, depending on the therapeutic requirements, a combination therapy may have to be instituted

CONCLUSION
The natural molecule-lysine-causes profuse induction of angiogenic response, in a timed way, in conditions of ischaemia and infarction.
The process of induction is an indirect phenomenon and depends on thepresence of available growth factor(s)/angiogenic factor(s) in the tissue.
The process is controllable and depends on: a.Availability of the amino acid in a given window concentration, and b.Availability of angiogenic factor(s) in adequate concentration, in the said tissues.
A number of clinical conditions can draw benefit from the observations. Cerebral and Cardiac Ischaemic (infarction) reperfusion was never this simple. Wound repair, of all types and durations, is much simple now. Possibilities in cosmetic surgery and other clinical conditions indicated.

Coronary Artery Bypass Graft:
“Over 500,000 CABG procedures are performed on an annual basis in the US. Approximately 8-10% of such grafts are less than optimal, leading to a 10% mortality rate for CABGs that are re-performed” ( Source:Medicure)
Cardiac Angina (Pectoris):
According to recent statistics from the American Heart association, more than six million Americans are diagnosed with angina and more women are affected than men.
Cardiac Stents:
Industry analysts estimate that the stent market, currently $ 2.3 billion, could easily double in size in the next three to four years as clinicians convert to coated stents that will fetch a hefty premium over bare metal stents. ( Source : Citritech)

Cardiac Catheterization Laboratory( Cath-lab)
Current Cardiac Drugs:Antiplatelet agents
Aspirin
Lipid lowering drugs
Statins
Trial Reports on Angiogenesis By :
Dr. K.M Cherian – Madras Medical Mission, Chennai
Dr. Rakesh Gupta: Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow
Trial Reports awaited on Angiogenesis By :
Dr. Nisith Azani – Azani Hospital, Siddhpur, Gujarat.
Dr. R.K. Sharma: Head of Nephrology, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow
Achievements :-
• Initial Acceptance by American Heart Association.
• International Society for heart Research - World Congress,
Brisbane, Australia
Report by Prof. Dr. KM Cherian

With an MBBS in 1964 and an MS in 1968, Dr K.M. Cherian headed for Australia to become a FRACS (Fellow of the Royal Australian College of Surgeons). He worked with the Railways and since then has devoted his life to serving humankind. Dr. Cherian has the rare distinction of having performed the first successful heart transplant in India in 1975. He has many more firsts to his name, including the first paediatric heart transplant and more recently, the first heart and lung transplant. He is the Director of the Institute of Cardio-Vascular diseases, Madras Medical Mission, Chennai.
He has held numerous positions both in India and abroad, including Visiting Professor at University of Oregon, USA; Senior Registrar of Greenlane Hospital, Royal Alexandria Hospital and St Vincent's Hospital, Sydney, Australia. He is the recipient of several honours including the Padmashri in 1991. He has authored several National and International publications and was the Honorary Surgeon to the President of India from 1990 to 1993. He has performed more than 17,000 operations. A very busy man and yet there is no end to the line of people wishing to consult him. He sees them all.
Dr. K. M. Cherian. Dedication personified.
Dr. K. M. CHERIAN
Acceptance by European Association for Cardio-Thoratic Surgery

Report from Prof. Dr. Rakesh Gupta

Thanks from . . . . . .
Prof. Dr. Debatosh Datta
Related Documents











