
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
The Swiss Paraplegic Center inNottwil, which opened inOctober 1990, is a NationalCenter of Competence that pro-vides comprehensive care toparaplegic and quadriplegicpatients who come not only fromSwitzerland, but from all overEurope (and, indeed, the world).The more than 1,000 centeremployees use the latest in med-icine, social services, vocationaltraining, education, and technol-ogy to restore patients to thehighest possible level of inde-pendent function and participa-tion. Patients can be managedfrom the time of onset of spinaldamage through vocational
training and finding a new placeto live or a new job. In 2005,almost 300 patients began theirtreatment with a stay in theintensive care unit that averaged7.4 days and more than 15,000days of artificial ventilation were delivered.
An institute within the center isdevoted to research aimed atmaking care even better in thefuture. In contrast to years past,when accidents were the princi-pal cause of spinal-cord injury,almost half of today’s patients atthe center have an illness such asvascular disease or cancer as thecause of their impairment. As a
result, the patients tend to beolder (and thus to have morecomorbidities) than patients seenin earlier years.
On average, almost 800 patientsare receiving some type of treat-ment at the center on any givenday. Much of this treatment is inthe form of care for the decubitusulcers, genitourinary infectionsand incontinence, respiratorycomplications, and neuropathicpain that are so prevalent afterspinal-cord injuries. Patients,however, also can practice in on-site homelike environments tomaximize their ability to copewhen they leave the facility.Some learn to walk on up-to-datetraining equipment such as theLokomat or participate in equinetherapy, sports activities, or psy-chotherapy to help them adjustto their new circumstances. Theindividuals who will care for thepatients once they leave the cen-ter also receive training.
Not all education at the center isfor patients and their families. Aprogram has been established toprepare new prostheticists toserve patients with spinal-cord
injuries. Employees can alsoattend foreign-language classes,and health care professionalsfrom all over the world attendconferences and seminars. Helpis provided to patients in findingthe necessary financial aid fortheir specialized care.
The condition of the patients andthe support equipment they sooften require create unique chal-lenges for the radiology depart-ment, even with its technologi-cally sophisticated equipment.Well over 5,000 MRI examina-tions are performed annually,and the center has the firstSiemens Sensation 40 multide-tector-array CT scanner to beinstalled in Europe. A new acqui-sition is the Swissray ddRCombiTrauma system, which the centerhelped the company develop. Itreplaced a computed radiogra-phy (CR) system and is usedmostly for inpatients, althoughsome outpatients and referralsalso are imaged.
According to Markus F. Berger,MD, senior consultant in radiolo-gy, the complexity of the center'scases means that 15 to 20
SWISS PARAPLEGIC CENTER:
IN SEARCH OF
THE MALLEABLE MACHINE
By Judith Gunn Bronson, MS
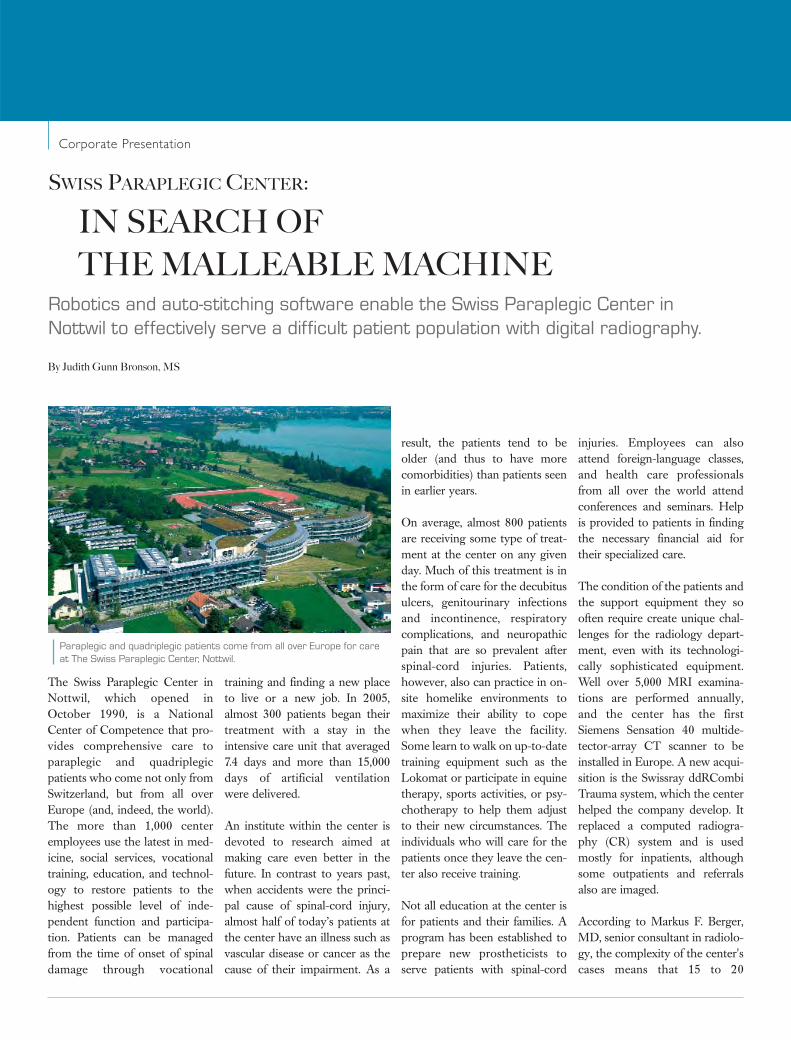
Robotics and auto-stitching software enable the Swiss Paraplegic Center inNottwil to effectively serve a difficult patient population with digital radiography.
Paraplegic and quadriplegic patients come from all over Europe for careat The Swiss Paraplegic Center, Nottwil.
Corporate Presentation

patients are examined per day.This is not as many as would beseen in a typical radiographypractice, so the features of theddRCombi Trauma system areespecially helpful. Most of thetime required for a study is con-sumed by the difficulties of mov-ing the paraplegic or quadriplegicpatient from the wheelchair orbed to the table. Nevertheless,“The room time has decreased,”Berger reports. “Once the proce-dure begins, we can have animage on the screen in 5 seconds.”
The center has found the imagequality to be better with the newsystem than with the CR system itreplaced. “We confirmed the high-er resolution with line-pair trials;the resolution can be as high as 3.5line pairs per mm. Also, with win-dowing, leveling, zoom, and such,even bad images can often befixed, which is helpful for thesedifficult patients and reduces ourretake rate,” Berger says.
Some other features of theddRCombi Trauma system proved
helpful. “With film-screen radiog-raphy, it was difficult to get theexposures of whole-spine imagesto match because of the differ-ences in the tissues in the differentareas, such as the pelvis and thethorax," Berger notes. "TheAutoStitching function makessuperb whole-spine images easy toobtain. We also measured the radi-ation dose, which is a serious con-cern in this population becausethey require so many imagingstudies, and we found it was halfthat of our previous CR system.”
The center converted to an all-electronic information-manage-ment environment eight yearsago, and Berger described theintegration of the ddRCombiTrauma into the network asexceptionally smooth. The cen-ter also has found the system tobe highly robust. Its PanelProtection program, combiningthe ability to halt system move-ment if an obstacle is detectedwith shock-absorbing features,helps protect it from damageduring these difficult cases.Swissray guarantees 99% uptime.
“In the last few years, our systemwas upgraded regularly,” Bergersays. “We now have equipmentthat is extraordinarily robust,almost never fails, and deliversimage quality second to none.Anyone in the market for directdigital radiography should haveSwissray on their short list ofpossible vendors.”
Judith Gunn Bronson, MS, is a contribut-ing writer for Imaging Economics.
The Swissray ddRCombi Trauma system has enabled the center to reduce room time.
Markus F. Berger, MD
ECRI’s focus is medical device technology, healthcare risk and qualitymanagement, and health technology assessment. It provides informationservices and technical assistance to more than 5,000 hospitals, health-care organisations, ministries of health, government and planning agen-cies, voluntary sector organisations and accrediting agencies worldwide.Its databases (over 30), publications, information services and technicalassistance services set the standard for the healthcare community.
More than 5,000 healthcare organisations worldwide rely on ECRIInstitute’s expertise in patient safety improvement, risk and quality man-agement, healthcare processes, devices, procedures and drug technolo-gy. ECRI Institute is one of only a handful of organisations designated asboth a Collaborating Centre of the World Health Organisation and anevidence-based practice centre by the US Agency for healthcareresearch and quality.
For more information, visit www.ecri.org
Publication of all submitted data is not possible: for further information please contact ECRI or [email protected].
ECRI Institute, a non-profit organisation, dedicates itself tobringing the discipline of applied scientific research in health-care to uncover the best approaches to improving patientcare. As pioneers in this science for nearly 40 years, ECRIInstitute marries experience and independence with theobjectivity of evidence-based research.
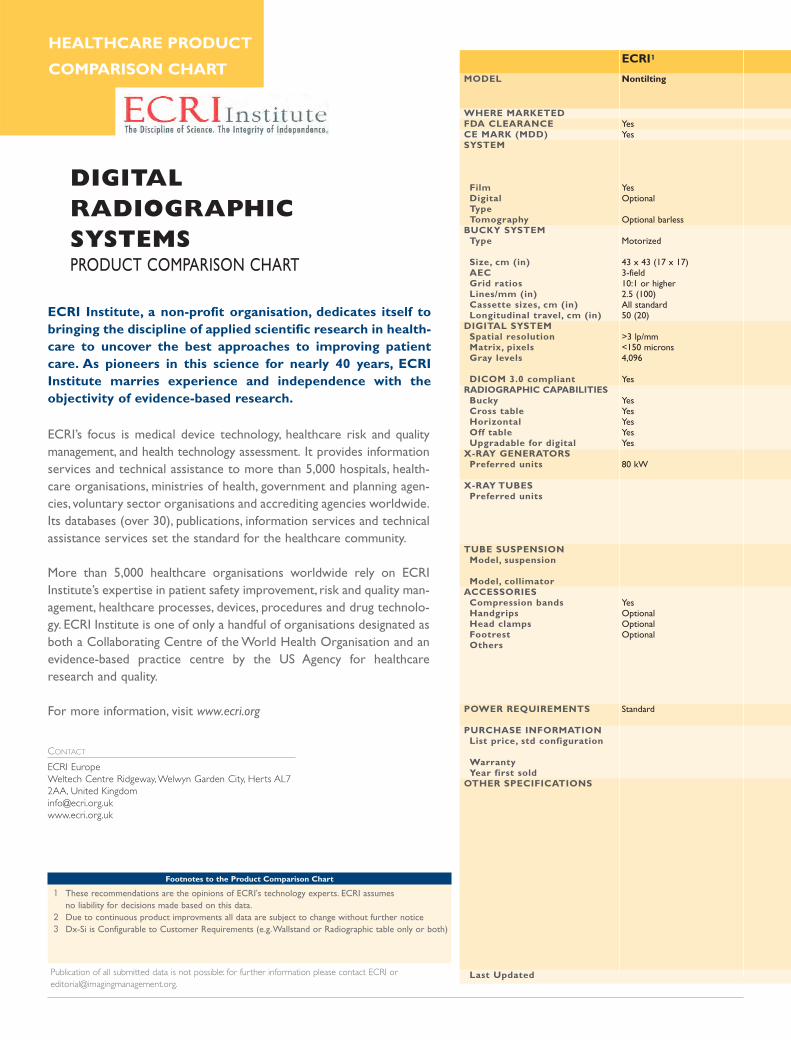
DIGITAL RADIOGRAPHIC SYSTEMSPRODUCT COMPARISON CHART
Footnotes to the Product Comparison Chart
1 These recommendations are the opinions of ECRI's technology experts. ECRI assumes no liability for decisions made based on this data.
2 Due to continuous product improvments all data are subject to change without further notice3 Dx-Si is Configurable to Customer Requirements (e.g.Wallstand or Radiographic table only or both)
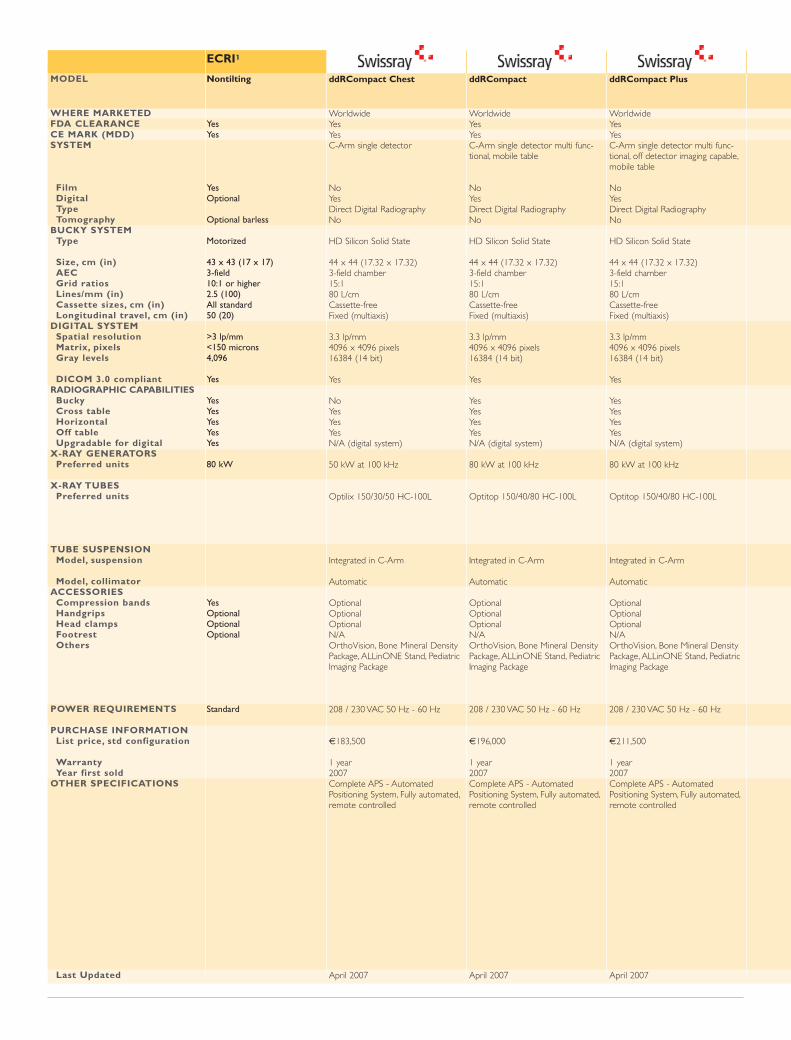
ECRI1
Nontilting
Yes Yes
Yes Optional
Optional barless
Motorized
43 x 43 (17 x 17) 3-field 10:1 or higher 2.5 (100) All standard 50 (20)
>3 lp/mm <150 microns 4,096
Yes
Yes Yes Yes Yes Yes
80 kW
Yes Optional Optional Optional
Standard
MODEL
WHERE MARKETEDFDA CLEARANCE CE MARK (MDD) SYSTEM
FilmDigital Type Tomography
BUCKY SYSTEMType
Size, cm (in) AEC Grid ratios Lines/mm (in) Cassette sizes, cm (in) Longitudinal travel, cm (in)
DIGITAL SYSTEM Spatial resolution Matrix, pixels Gray levels
DICOM 3.0 compliant RADIOGRAPHIC CAPABILITIES
Bucky Cross table Horizontal Off table Upgradable for digital
X-RAY GENERATORS Preferred units
X-RAY TUBESPreferred units
TUBE SUSPENSION Model, suspension
Model, collimatorACCESSORIES
Compression bands Handgrips Head clampsFootrest Others
POWER REQUIREMENTS
PURCHASE INFORMATIONList price, std configuration
Warranty Year first sold
OTHER SPECIFICATIONS
Last Updated
CONTACT
ECRI EuropeWeltech Centre Ridgeway, Welwyn Garden City, Herts AL72AA, United [email protected]
HEALTHCARE PRODUCT
COMPARISON CHART
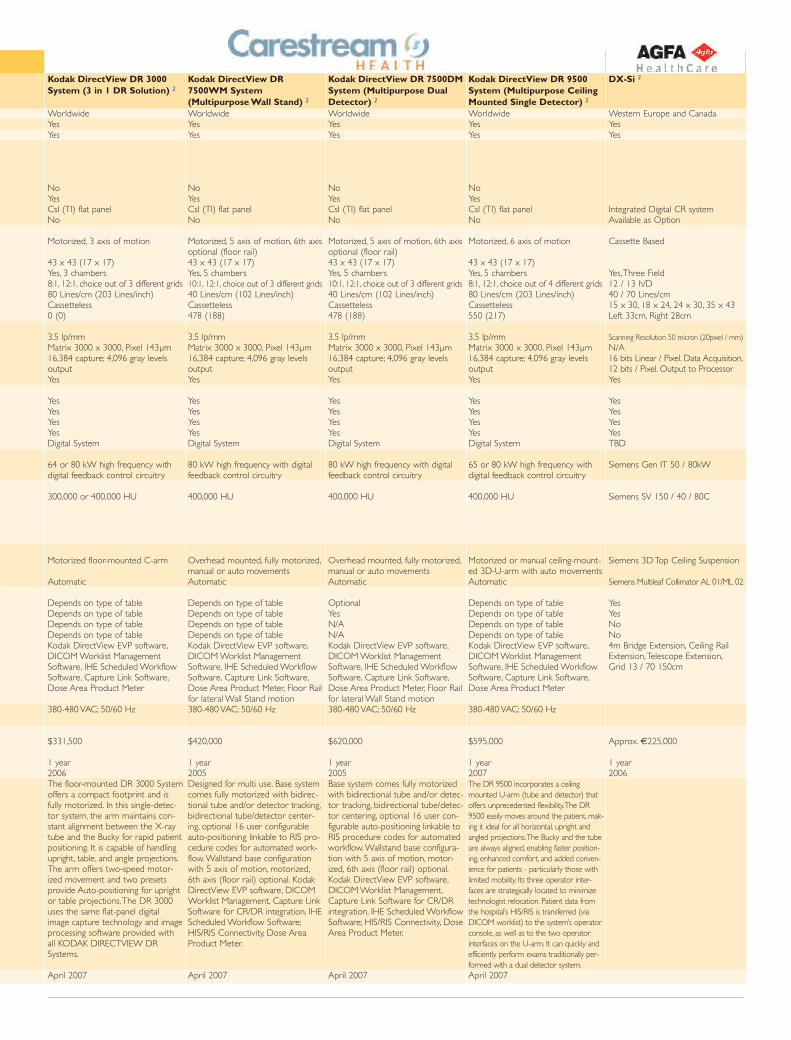
Kodak DirectView DR7500WM System(Multipurpose Wall Stand) 2
WorldwideYesYes
NoYesCsI (TI) flat panel No
Motorized, 5 axis of motion, 6th axisoptional (floor rail)43 x 43 (17 x 17) Yes, 5 chambers10:1, 12:1, choice out of 3 different grids40 Lines/cm (102 Lines/inch) Cassetteless 478 (188)
3.5 lp/mm Matrix 3000 x 3000, Pixel 143µm16,384 capture; 4,096 gray levelsoutputYes
YesYesYesYesDigital System
80 kW high frequency with digitalfeedback control circuitry
400,000 HU
Overhead mounted, fully motorized,manual or auto movementsAutomatic
Depends on type of tableDepends on type of tableDepends on type of tableDepends on type of tableKodak DirectView EVP software,DICOM Worklist ManagementSoftware, IHE Scheduled WorkflowSoftware, Capture Link Software,Dose Area Product Meter, Floor Railfor lateral Wall Stand motion380-480 VAC; 50/60 Hz
$420,000
1 year2005Designed for multi use. Base systemcomes fully motorized with bidirec-tional tube and/or detector tracking,bidirectional tube/detector center-ing, optional 16 user configurableauto-positioning linkable to RIS pro-cedure codes for automated work-flow.Wallstand base configurationwith 5 axis of motion, motorized,6th axis (floor rail) optional. KodakDirectView EVP software, DICOMWorklist Management, Capture LinkSoftware for CR/DR integration, IHEScheduled Workflow Software;HIS/RIS Connectivity, Dose AreaProduct Meter.
April 2007
Kodak DirectView DR 7500DMSystem (Multipurpose DualDetector) 2
Worldwide YesYes
No YesCsI (TI) flat panel No
Motorized, 5 axis of motion, 6th axisoptional (floor rail)43 x 43 (17 x 17) Yes, 5 chambers10:1, 12:1, choice out of 3 different grids40 Lines/cm (102 Lines/inch) Cassetteless 478 (188)
3.5 lp/mm Matrix 3000 x 3000, Pixel 143µm16,384 capture; 4,096 gray levelsoutput Yes
YesYesYesYesDigital System
80 kW high frequency with digitalfeedback control circuitry
400,000 HU
Overhead mounted, fully motorized,manual or auto movementsAutomatic
Optional YesN/AN/AKodak DirectView EVP software,DICOM Worklist ManagementSoftware, IHE Scheduled WorkflowSoftware, Capture Link Software,Dose Area Product Meter, Floor Railfor lateral Wall Stand motion380-480 VAC; 50/60 Hz
$620,000
1 year2005Base system comes fully motorizedwith bidirectional tube and/or detec-tor tracking, bidirectional tube/detec-tor centering, optional 16 user con-figurable auto-positioning linkable toRIS procedure codes for automatedworkflow.Wallstand base configura-tion with 5 axis of motion, motor-ized, 6th axis (floor rail) optional.Kodak DirectView EVP software,DICOM Worklist Management,Capture Link Software for CR/DRintegration, IHE Scheduled WorkflowSoftware; HIS/RIS Connectivity, DoseArea Product Meter.
April 2007
Kodak DirectView DR 9500System (Multipurpose CeilingMounted Single Detector) 2
Worldwide YesYes
NoYesCsI (TI) flat panel No
Motorized, 6 axis of motion
43 x 43 (17 x 17) Yes, 5 chambers8:1, 12:1, choice out of 4 different grids80 Lines/cm (203 Lines/inch)Cassetteless 550 (217)
3.5 lp/mm Matrix 3000 x 3000, Pixel 143µm16,384 capture; 4,096 gray levelsoutput Yes
YesYesYesYesDigital System
65 or 80 kW high frequency withdigital feedback control circuitry
400,000 HU
Motorized or manual ceiling-mount-ed 3D-U-arm with auto movementsAutomatic
Depends on type of tableDepends on type of tableDepends on type of tableDepends on type of tableKodak DirectView EVP software,DICOM Worklist ManagementSoftware, IHE Scheduled WorkflowSoftware, Capture Link Software,Dose Area Product Meter
380-480 VAC; 50/60 Hz
$595,000
1 year2007The DR 9500 incorporates a ceilingmounted U-arm (tube and detector) thatoffers unprecedented flexibility.The DR9500 easily moves around the patient, mak-ing it ideal for all horizontal, upright andangled projections.The Bucky and the tubeare always aligned, enabling faster position-ing, enhanced comfort, and added conven-ience for patients - particularly those withlimited mobility. Its three operator inter-faces are strategically located to minimizetechnologist relocation. Patient data fromthe hospital’s HIS/RIS is transferred (viaDICOM worklist) to the system’s operatorconsole, as well as to the two operatorinterfaces on the U-arm. It can quickly andefficiently perform exams traditionally per-formed with a dual detector system.April 2007
DX-Si 3
Western Europe and CanadaYesYes
Integrated Digital CR systemAvailable as Option
Cassette Based
Yes,Three Field12 / 13 h/D40 / 70 Lines/cm15 x 30, 18 x 24, 24 x 30, 35 x 43Left 33cm, Right 28cm
Scanning Resolution 50 micron (20pixel / mm)N/A16 bits Linear / Pixel. Data Acquisition,12 bits / Pixel. Output to ProcessorYes
YesYesYesYesTBD
Siemens Gen IT 50 / 80kW
Siemens SV 150 / 40 / 80C
Siemens 3D Top Ceiling Suspension
Siemens Multileaf Collimator AL 01/ML 02
YesYesNoNo4m Bridge Extension, Ceiling RailExtension,Telescope Extension,Grid 13 / 70 150cm
Approx. €225,000
1 year2006
Kodak DirectView DR 3000System (3 in 1 DR Solution) 2
WorldwideYes Yes
No Yes CsI (TI) flat panel No
Motorized, 3 axis of motion
43 x 43 (17 x 17) Yes, 3 chambers8:1, 12:1, choice out of 3 different grids80 Lines/cm (203 Lines/inch)Cassetteless 0 (0)
3.5 lp/mm Matrix 3000 x 3000, Pixel 143µm16,384 capture; 4,096 gray levelsoutputYes
Yes Yes Yes Yes Digital System
64 or 80 kW high frequency withdigital feedback control circuitry
300,000 or 400,000 HU
Motorized floor-mounted C-arm
Automatic
Depends on type of tableDepends on type of tableDepends on type of tableDepends on type of tableKodak DirectView EVP software,DICOM Worklist ManagementSoftware, IHE Scheduled WorkflowSoftware, Capture Link Software,Dose Area Product Meter
380-480 VAC; 50/60 Hz
$331,500
1 year2006The floor-mounted DR 3000 Systemoffers a compact footprint and isfully motorized. In this single-detec-tor system, the arm maintains con-stant alignment between the X-raytube and the Bucky for rapid patientpositioning. It is capable of handlingupright, table, and angle projections.The arm offers two-speed motor-ized movement and two presetsprovide Auto-positioning for uprightor table projections.The DR 3000uses the same flat-panel digitalimage capture technology and imageprocessing software provided withall KODAK DIRECTVIEW DRSystems.
April 2007
ECRI1
Nontilting
Yes Yes
Yes Optional
Optional barless
Motorized
43 x 43 (17 x 17) 3-field 10:1 or higher 2.5 (100) All standard 50 (20)
>3 lp/mm <150 microns 4,096
Yes
Yes Yes Yes Yes Yes
80 kW
Yes Optional Optional Optional
Standard
MODEL
WHERE MARKETEDFDA CLEARANCE CE MARK (MDD) SYSTEM
FilmDigital Type Tomography
BUCKY SYSTEMType
Size, cm (in) AEC Grid ratios Lines/mm (in) Cassette sizes, cm (in) Longitudinal travel, cm (in)
DIGITAL SYSTEM Spatial resolution Matrix, pixels Gray levels
DICOM 3.0 compliant RADIOGRAPHIC CAPABILITIES
Bucky Cross table Horizontal Off table Upgradable for digital
X-RAY GENERATORS Preferred units
X-RAY TUBESPreferred units
TUBE SUSPENSION Model, suspension
Model, collimatorACCESSORIES
Compression bands Handgrips Head clampsFootrest Others
POWER REQUIREMENTS
PURCHASE INFORMATIONList price, std configuration
Warranty Year first sold
OTHER SPECIFICATIONS
Last Updated
ddRCompact Chest
WorldwideYesYesC-Arm single detector
NoYesDirect Digital RadiographyNo
HD Silicon Solid State
44 x 44 (17.32 x 17.32)3-field chamber15:180 L/cmCassette-freeFixed (multiaxis)
3.3 lp/mm 4096 x 4096 pixels16384 (14 bit)
Yes
NoYesYesYesN/A (digital system)
50 kW at 100 kHz
Optilix 150/30/50 HC-100L
Integrated in C-Arm
Automatic
OptionalOptionalOptionalN/AOrthoVision, Bone Mineral DensityPackage, ALLinONE Stand, PediatricImaging Package
208 / 230 VAC 50 Hz - 60 Hz
€183,500
1 year2007Complete APS - AutomatedPositioning System, Fully automated,remote controlled
April 2007
ddRCompact
WorldwideYesYesC-Arm single detector multi func-tional, mobile table
NoYesDirect Digital RadiographyNo
HD Silicon Solid State
44 x 44 (17.32 x 17.32)3-field chamber15:180 L/cmCassette-freeFixed (multiaxis)
3.3 lp/mm 4096 x 4096 pixels16384 (14 bit)
Yes
YesYesYesYesN/A (digital system)
80 kW at 100 kHz
Optitop 150/40/80 HC-100L
Integrated in C-Arm
Automatic
OptionalOptionalOptionalN/AOrthoVision, Bone Mineral DensityPackage, ALLinONE Stand, PediatricImaging Package
208 / 230 VAC 50 Hz - 60 Hz
€196,000
1 year2007Complete APS - AutomatedPositioning System, Fully automated,remote controlled
April 2007
ddRCompact Plus
WorldwideYesYesC-Arm single detector multi func-tional, off detector imaging capable,mobile table
NoYesDirect Digital RadiographyNo
HD Silicon Solid State
44 x 44 (17.32 x 17.32)3-field chamber15:180 L/cmCassette-freeFixed (multiaxis)
3.3 lp/mm 4096 x 4096 pixels16384 (14 bit)
Yes
YesYesYesYesN/A (digital system)
80 kW at 100 kHz
Optitop 150/40/80 HC-100L
Integrated in C-Arm
Automatic
OptionalOptionalOptionalN/AOrthoVision, Bone Mineral DensityPackage, ALLinONE Stand, PediatricImaging Package
208 / 230 VAC 50 Hz - 60 Hz
€211,500
1 year2007Complete APS - AutomatedPositioning System, Fully automated,remote controlled
April 2007
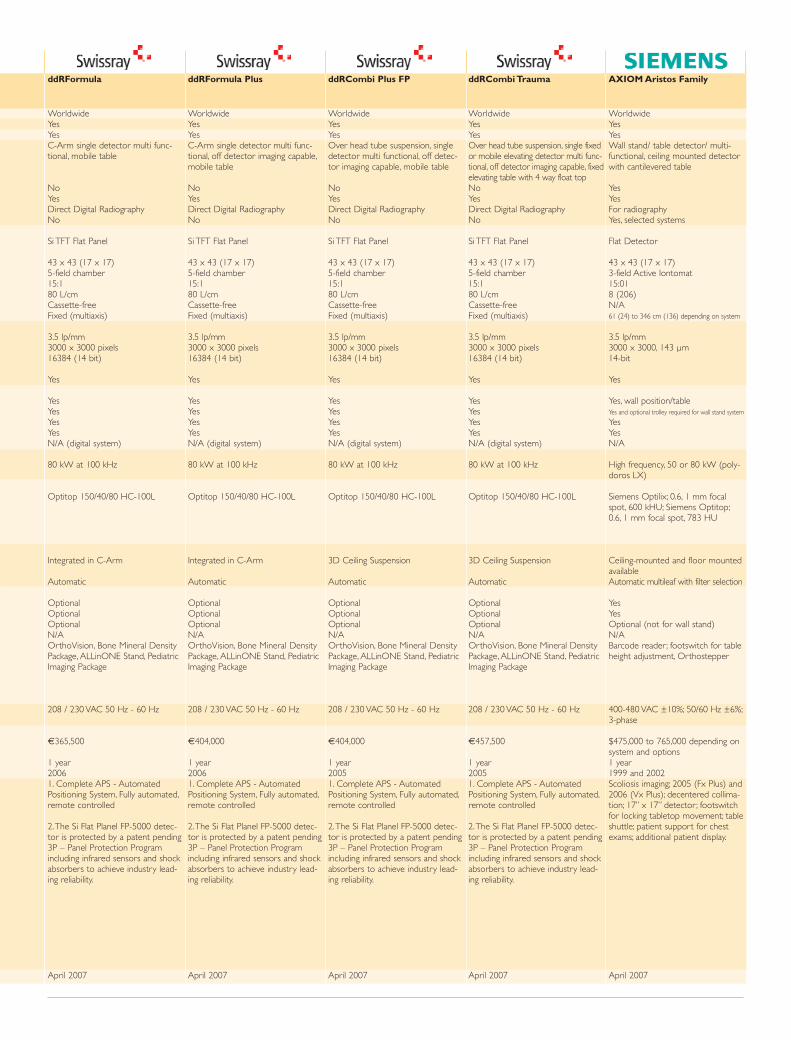
ddRFormula Plus
WorldwideYesYesC-Arm single detector multi func-tional, off detector imaging capable,mobile table
NoYesDirect Digital RadiographyNo
Si TFT Flat Panel
43 x 43 (17 x 17)5-field chamber15:180 L/cmCassette-freeFixed (multiaxis)
3.5 lp/mm3000 x 3000 pixels16384 (14 bit)
Yes
YesYesYesYesN/A (digital system)
80 kW at 100 kHz
Optitop 150/40/80 HC-100L
Integrated in C-Arm
Automatic
OptionalOptionalOptionalN/AOrthoVision, Bone Mineral DensityPackage, ALLinONE Stand, PediatricImaging Package
208 / 230 VAC 50 Hz - 60 Hz
€404,000
1 year20061. Complete APS - AutomatedPositioning System, Fully automated,remote controlled
2.The Si Flat Planel FP-5000 detec-tor is protected by a patent pending3P – Panel Protection Programincluding infrared sensors and shockabsorbers to achieve industry lead-ing reliability.
April 2007
ddRCombi Plus FP
WorldwideYesYesOver head tube suspension, singledetector multi functional, off detec-tor imaging capable, mobile table
NoYesDirect Digital RadiographyNo
Si TFT Flat Panel
43 x 43 (17 x 17)5-field chamber15:180 L/cmCassette-freeFixed (multiaxis)
3.5 lp/mm3000 x 3000 pixels16384 (14 bit)
Yes
YesYesYesYesN/A (digital system)
80 kW at 100 kHz
Optitop 150/40/80 HC-100L
3D Ceiling Suspension
Automatic
OptionalOptionalOptionalN/AOrthoVision, Bone Mineral DensityPackage, ALLinONE Stand, PediatricImaging Package
208 / 230 VAC 50 Hz - 60 Hz
€404,000
1 year20051. Complete APS - AutomatedPositioning System, Fully automated,remote controlled
2.The Si Flat Planel FP-5000 detec-tor is protected by a patent pending3P – Panel Protection Programincluding infrared sensors and shockabsorbers to achieve industry lead-ing reliability.
April 2007
ddRCombi Trauma
WorldwideYesYesOver head tube suspension, single fixedor mobile elevating detector multi func-tional, off detector imaging capable, fixedelevating table with 4 way float topNoYesDirect Digital RadiographyNo
Si TFT Flat Panel
43 x 43 (17 x 17)5-field chamber15:180 L/cmCassette-freeFixed (multiaxis)
3.5 lp/mm3000 x 3000 pixels16384 (14 bit)
Yes
YesYesYesYesN/A (digital system)
80 kW at 100 kHz
Optitop 150/40/80 HC-100L
3D Ceiling Suspension
Automatic
OptionalOptionalOptionalN/AOrthoVision, Bone Mineral DensityPackage, ALLinONE Stand, PediatricImaging Package
208 / 230 VAC 50 Hz - 60 Hz
€457,500
1 year20051. Complete APS - AutomatedPositioning System, Fully automated,remote controlled
2.The Si Flat Planel FP-5000 detec-tor is protected by a patent pending3P – Panel Protection Programincluding infrared sensors and shockabsorbers to achieve industry lead-ing reliability.
April 2007
AXIOM Aristos Family
WorldwideYesYesWall stand/ table detector/ multi-functional, ceiling mounted detectorwith cantilevered table
YesYesFor radiographyYes, selected systems
Flat Detector
43 x 43 (17 x 17)3-field Active Iontomat15:018 (206)N/A61 (24) to 346 cm (136) depending on system
3.5 lp/mm3000 x 3000, 143 µm14-bit
Yes
Yes, wall position/tableYes and optional trolley required for wall stand system
YesYesN/A
High frequency, 50 or 80 kW (poly-doros LX)
Siemens Optilix; 0.6, 1 mm focalspot, 600 kHU; Siemens Optitop;0.6, 1 mm focal spot, 783 HU
Ceiling-mounted and floor mountedavailableAutomatic multileaf with filter selection
YesYesOptional (not for wall stand)N/ABarcode reader; footswitch for tableheight adjustment, Orthostepper
400-480 VAC ±10%; 50/60 Hz ±6%;3-phase
$475,000 to 765,000 depending onsystem and options1 year1999 and 2002Scoliosis imaging; 2005 (Fx Plus) and2006 (Vx Plus); decentered collima-tion; 17” x 17” detector; footswitchfor locking tabletop movement; tableshuttle; patient support for chestexams; additional patient display.
April 2007
ddRFormula
WorldwideYesYesC-Arm single detector multi func-tional, mobile table
NoYesDirect Digital RadiographyNo
Si TFT Flat Panel
43 x 43 (17 x 17)5-field chamber15:180 L/cmCassette-freeFixed (multiaxis)
3.5 lp/mm 3000 x 3000 pixels16384 (14 bit)
Yes
YesYesYesYesN/A (digital system)
80 kW at 100 kHz
Optitop 150/40/80 HC-100L
Integrated in C-Arm
Automatic
OptionalOptionalOptionalN/AOrthoVision, Bone Mineral DensityPackage, ALLinONE Stand, PediatricImaging Package
208 / 230 VAC 50 Hz - 60 Hz
€365,500
1 year20061. Complete APS - AutomatedPositioning System, Fully automated,remote controlled
2.The Si Flat Planel FP-5000 detec-tor is protected by a patent pending3P – Panel Protection Programincluding infrared sensors and shockabsorbers to achieve industry lead-ing reliability.
April 2007
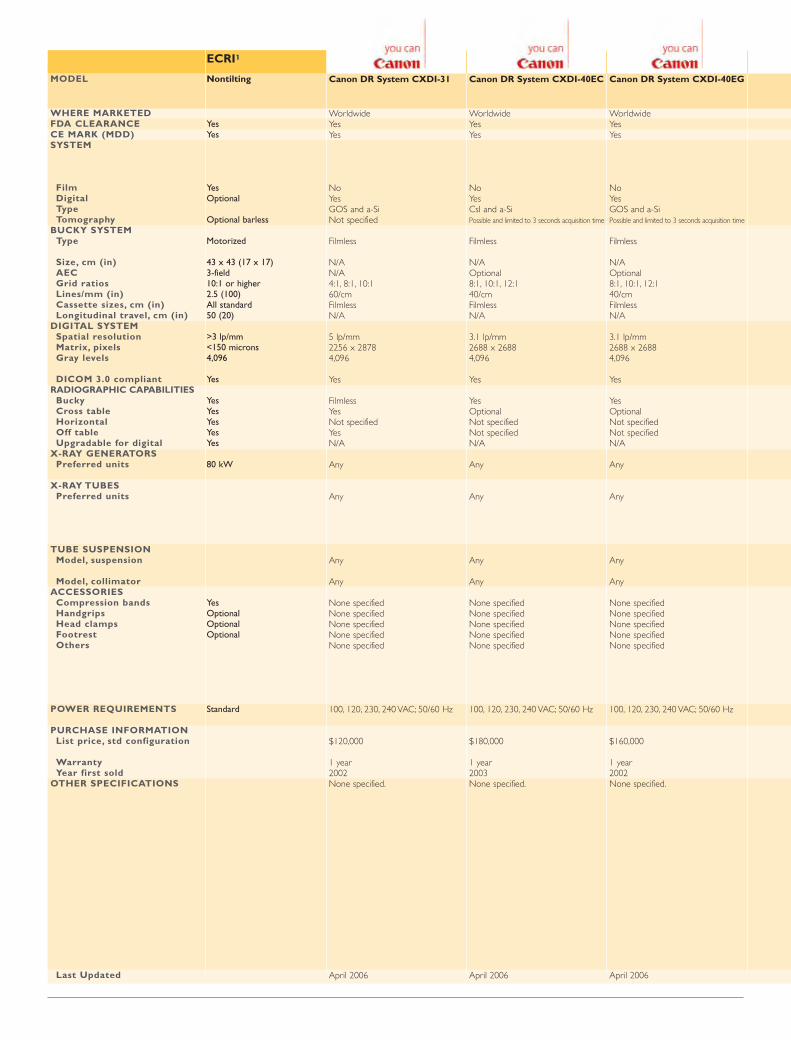
ECRI1
Nontilting
Yes Yes
Yes Optional
Optional barless
Motorized
43 x 43 (17 x 17) 3-field 10:1 or higher 2.5 (100) All standard 50 (20)
>3 lp/mm <150 microns 4,096
Yes
Yes Yes Yes Yes Yes
80 kW
Yes Optional Optional Optional
Standard
MODEL
WHERE MARKETEDFDA CLEARANCE CE MARK (MDD) SYSTEM
FilmDigital Type Tomography
BUCKY SYSTEMType
Size, cm (in) AEC Grid ratios Lines/mm (in) Cassette sizes, cm (in) Longitudinal travel, cm (in)
DIGITAL SYSTEM Spatial resolution Matrix, pixels Gray levels
DICOM 3.0 compliant RADIOGRAPHIC CAPABILITIES
Bucky Cross table Horizontal Off table Upgradable for digital
X-RAY GENERATORS Preferred units
X-RAY TUBESPreferred units
TUBE SUSPENSION Model, suspension
Model, collimatorACCESSORIES
Compression bands Handgrips Head clampsFootrest Others
POWER REQUIREMENTS
PURCHASE INFORMATIONList price, std configuration
Warranty Year first sold
OTHER SPECIFICATIONS
Last Updated
Canon DR System CXDI-31
Worldwide YesYes
No YesGOS and a-Si Not specified
Filmless
N/AN/A4:1, 8:1, 10:1 60/cmFilmless N/A
5 lp/mm 2256 x 2878 4,096
Yes
Filmless YesNot specified YesN/A
Any
Any
Any
Any
None specified None specified None specified None specified None specified
100, 120, 230, 240 VAC; 50/60 Hz
$120,000
1 year2002None specified.
April 2006
Canon DR System CXDI-40EC
Worldwide YesYes
NoYesCsI and a-Si Possible and limited to 3 seconds acquisition time
Filmless
N/AOptional8:1, 10:1, 12:1 40/cm Filmless N/A
3.1 lp/mm 2688 x 2688 4,096
Yes
Yes Optional Not specified Not specified N/A
Any
Any
Any
Any
None specified None specified None specified None specified None specified
100, 120, 230, 240 VAC; 50/60 Hz
$180,000
1 year2003None specified.
April 2006
Canon DR System CXDI-40EG
Worldwide YesYes
NoYesGOS and a-Si Possible and limited to 3 seconds acquisition time
Filmless
N/AOptional8:1, 10:1, 12:1 40/cm Filmless N/A
3.1 lp/mm 2688 x 2688 4,096
Yes
YesOptionalNot specifiedNot specifiedN/A
Any
Any
Any
Any
None specified None specified None specified None specified None specified
100, 120, 230, 240 VAC; 50/60 Hz
$160,000
1 year2002None specified.
April 2006
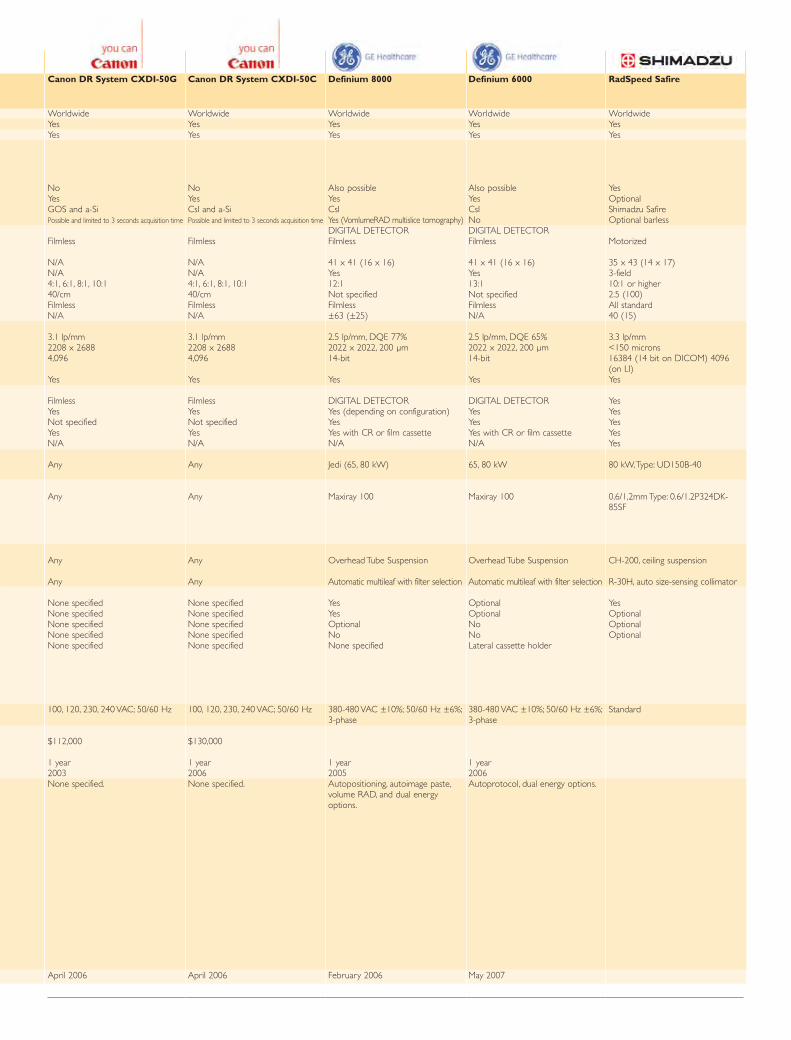
Canon DR System CXDI-50C
Worldwide YesYes
NoYesCsI and a-Si Possible and limited to 3 seconds acquisition time
Filmless
N/AN/A4:1, 6:1, 8:1, 10:1 40/cm Filmless N/A
3.1 lp/mm 2208 x 2688 4,096
Yes
Filmless YesNot specifiedYesN/A
Any
Any
Any
Any
None specified None specified None specified None specified None specified
100, 120, 230, 240 VAC; 50/60 Hz
$130,000
1 year2006None specified.
April 2006
Definium 8000
WorldwideYesYes
Also possibleYesCsIYes (VomlumeRAD multislice tomography)DIGITAL DETECTOR Filmless
41 x 41 (16 x 16)Yes12:1Not specified Filmless ±63 (±25)
2.5 lp/mm, DQE 77% 2022 x 2022, 200 µm14-bit
Yes
DIGITAL DETECTOR Yes (depending on configuration)YesYes with CR or film cassetteN/A
Jedi (65, 80 kW)
Maxiray 100
Overhead Tube Suspension
Automatic multileaf with filter selection
YesYesOptionalNoNone specified
380-480 VAC ±10%; 50/60 Hz ±6%;3-phase
1 year2005Autopositioning, autoimage paste,volume RAD, and dual energyoptions.
February 2006
Definium 6000
WorldwideYesYes
Also possibleYesCsINoDIGITAL DETECTORFilmless
41 x 41 (16 x 16)Yes13:1Not specifiedFilmlessN/A
2.5 lp/mm, DQE 65% 2022 x 2022, 200 µm 14-bit
Yes
DIGITAL DETECTORYesYesYes with CR or film cassetteN/A
65, 80 kW
Maxiray 100
Overhead Tube Suspension
Automatic multileaf with filter selection
OptionalOptionalNoNoLateral cassette holder
380-480 VAC ±10%; 50/60 Hz ±6%;3-phase
1 year2006Autoprotocol, dual energy options.
May 2007
RadSpeed Safire
WorldwideYes Yes
Yes OptionalShimadzu SafireOptional barless
Motorized
35 x 43 (14 x 17) 3-field 10:1 or higher 2.5 (100) All standard 40 (15)
3.3 lp/mm<150 microns 16384 (14 bit on DICOM) 4096(on LI)Yes
Yes YesYesYesYes
80 kW,Type: UD150B-40
0,6/1,2mm Type: 0.6/1.2P324DK-85SF
CH-200, ceiling suspension
R-30H, auto size-sensing collimator
Yes OptionalOptionalOptional
Standard
Canon DR System CXDI-50G
Worldwide YesYes
NoYesGOS and a-Si Possible and limited to 3 seconds acquisition time
Filmless
N/AN/A4:1, 6:1, 8:1, 10:1 40/cm Filmless N/A
3.1 lp/mm 2208 x 2688 4,096
Yes
Filmless YesNot specified YesN/A
Any
Any
Any
Any
None specified None specified None specified None specified None specified
100, 120, 230, 240 VAC; 50/60 Hz
$112,000
1 year2003None specified.
April 2006
ECRI1
Nontilting
Yes Yes
Yes Optional
Optional barless
Motorized
43 x 43 (17 x 17) 3-field 10:1 or higher 2.5 (100) All standard 50 (20)
>3 lp/mm <150 microns 4,096
Yes
Yes Yes Yes Yes Yes
80 kW
Yes Optional Optional Optional
Standard
MODEL
WHERE MARKETEDFDA CLEARANCE CE MARK (MDD) SYSTEM
FilmDigital Type Tomography
BUCKY SYSTEMType
Size, cm (in) AEC Grid ratios Lines/mm (in) Cassette sizes, cm (in) Longitudinal travel, cm (in)
DIGITAL SYSTEM Spatial resolution Matrix, pixels Gray levels
DICOM 3.0 compliant RADIOGRAPHIC CAPABILITIES
Bucky Cross table Horizontal Off table Upgradable for digital
X-RAY GENERATORS Preferred units
X-RAY TUBESPreferred units
TUBE SUSPENSION Model, suspension
Model, collimatorACCESSORIES
Compression bands Handgrips Head clampsFootrest Others
POWER REQUIREMENTS
PURCHASE INFORMATIONList price, std configuration
Warranty Year first sold
OTHER SPECIFICATIONS
Last Updated
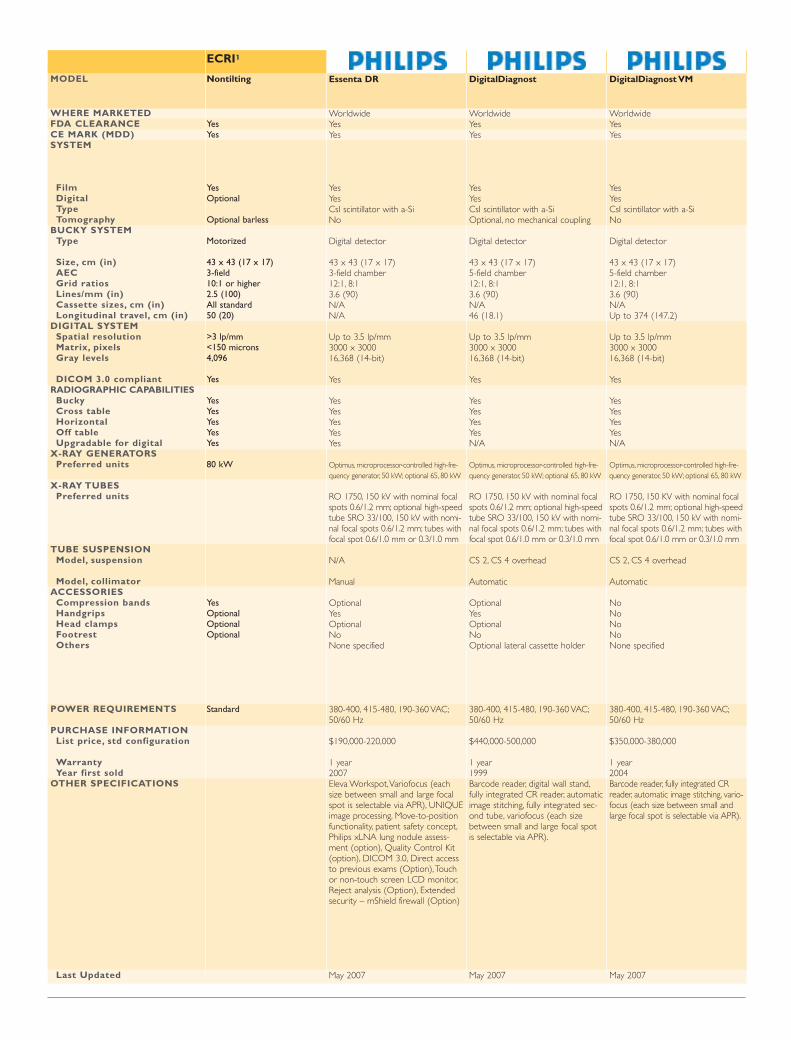
Essenta DR
Worldwide YesYes
Yes YesCsI scintillator with a-Si No
Digital detector
43 x 43 (17 x 17) 3-field chamber 12:1, 8:1 3.6 (90) N/AN/A
Up to 3.5 lp/mm 3000 x 3000 16,368 (14-bit)
Yes
YesYesYesYesYes
Optimus, microprocessor-controlled high-fre-quency generator, 50 kW; optional 65, 80 kW
RO 1750, 150 kV with nominal focalspots 0.6/1.2 mm; optional high-speedtube SRO 33/100, 150 kV with nomi-nal focal spots 0.6/1.2 mm; tubes withfocal spot 0.6/1.0 mm or 0.3/1.0 mm
N/A
Manual
Optional Yes Optional No None specified
380-400, 415-480, 190-360 VAC;50/60 Hz
$190,000-220,000
1 year 2007Eleva Workspot,Variofocus (eachsize between small and large focalspot is selectable via APR), UNIQUEimage processing, Move-to-positionfunctionality, patient safety concept,Philips xLNA lung nodule assess-ment (option), Quality Control Kit(option), DICOM 3.0, Direct accessto previous exams (Option),Touchor non-touch screen LCD monitor,Reject analysis (Option), Extendedsecurity – mShield firewall (Option)
May 2007
DigitalDiagnost
Worldwide YesYes
Yes Yes CsI scintillator with a-Si Optional, no mechanical coupling
Digital detector
43 x 43 (17 x 17) 5-field chamber 12:1, 8:1 3.6 (90) N/A46 (18.1)
Up to 3.5 lp/mm 3000 x 3000 16,368 (14-bit)
Yes
YesYesYesYesN/A
Optimus, microprocessor-controlled high-fre-quency generator, 50 kW; optional 65, 80 kW
RO 1750, 150 kV with nominal focalspots 0.6/1.2 mm; optional high-speedtube SRO 33/100, 150 kV with nomi-nal focal spots 0.6/1.2 mm; tubes withfocal spot 0.6/1.0 mm or 0.3/1.0 mm
CS 2, CS 4 overhead
Automatic
Optional Yes Optional No Optional lateral cassette holder
380-400, 415-480, 190-360 VAC;50/60 Hz
$440,000-500,000
1 year 1999Barcode reader, digital wall stand,fully integrated CR reader, automaticimage stitching, fully integrated sec-ond tube, variofocus (each sizebetween small and large focal spot is selectable via APR).
May 2007
DigitalDiagnost VM
Worldwide YesYes
YesYesCsI scintillator with a-Si No
Digital detector
43 x 43 (17 x 17) 5-field chamber 12:1, 8:1 3.6 (90) N/AUp to 374 (147.2)
Up to 3.5 lp/mm 3000 x 3000 16,368 (14-bit)
Yes
YesYesYesYesN/A
Optimus, microprocessor-controlled high-fre-quency generator, 50 kW; optional 65, 80 kW
RO 1750, 150 KV with nominal focalspots 0.6/1.2 mm; optional high-speedtube SRO 33/100, 150 kV with nomi-nal focal spots 0.6/1.2 mm; tubes withfocal spot 0.6/1.0 mm or 0.3/1.0 mm
CS 2, CS 4 overhead
Automatic
No No No No None specified
380-400, 415-480, 190-360 VAC;50/60 Hz
$350,000-380,000
1 year 2004Barcode reader, fully integrated CRreader, automatic image stitching, vario-focus (each size between small andlarge focal spot is selectable via APR).
May 2007
AUTHORS
Thomas J.Vogl (above)M.G. Mack T. Lehnert
Department of RadiologyInstitute of Diagnostic andInterventional RadiologyJohann Wolfgang GoetheUniversity Frankfurt, Germany
Progress in Digital RadiographyDigital detectors have come a long way since the initialDigital Subtraction Angiography (DSA) systems in the
1970’s, which were rapidlyfollowed by CR in the eight-ies, DR in the nineties andlater on, flat panel technolo-gy. Today, digital radiogra-phy offers many advantagesand possibilities, includingthe reconstruction and refor-matting of images, easierimage processing, a widerange of acquisition, rapidstorage and retrieval, better
distribution and more controlled viewing and analysis,amongst others. What this adds up to finally, isimproved image management.
There is much research and study taking place across Europeto anticipate the advent of the digital hospital. Since imaging isat the heart of medical healthcare services, it makes sensethat studies need to take place now, in anticipation of theneeds of a fully-electronic imaging department, to ensure thatthe patient receives the best possible services. One of theways we can do this is to make our facility as efficient as possi-ble, examining the steps necessary in the workflow to improvethroughput. In this article, I will present the results of a studythat took place with the support of Kodak/Carestream Health,in cooperation with the Centre for Biomedical Engineering(CBME) and the Technical University of Frankfurt.This studyexamined not only the comparison of the latest CR and DRsystems to check which is the best future contender, it alsoexamined what happens to the quality of the image when thedose is reduced. Can we cope equally well with a lower dose?
Results of a Study of Workflow and Dose Reduction
MAKING
DIGITAL RADIOGRAPHYMORE EFFICIENT
CR Vs. DR – SummaryComputed Radiography (CR), uses photo-stimulablephosphor plates to obtain digital images, and can beimplemented by updating the cassettes you use in yourcurrent x-ray system. Digital Radiography (DR)requires the use of newer x-ray systems with an inte-grated digital detector. Presently, the latter option ismore expensive though it enhances workflow due tothe added advantage that it is no longer necessary tohandle the cassettes. Thus, while the most commonsolution is to use CR with mobile systems, there arealready mobile x-ray units with an integrated flat paneldigital detector on the market using a phosphor plate.
Although digital imaging systems have the poten-tial for dose reduction, the most common out-come is that this dose reduction is not realised,since over-exposure goes undetected, unlike withfilm where the image turns dark or black. In dig-ital imaging, by contrast, the image becomesclearer when it is over-exposed. Also, there is atendency to take more images than necessary.Exams levels per patient seem to increase with theuse of digital systems. Further, it is very easy todelete images, and technologists tend to repeatexposure if the image is not satisfactory. Thus dig-ital imaging is likely to increase not only the num-ber of exposures but also patient dose.
What’s on the Market?Digital radiography’s current array of technolo-gies, which are being examined by the differentmanufacturers, include CR, PhotoconductorDrum, Direct DR, Indirect DR and ChargedCoupled Device (CCD) DR. Manufacturers arecompeting to provide the most efficient system.As well as Fuji, AGFA and Kodak/CarestreamHealth, Hologic, Toshiba, Canon, GE, Philips,Siemens, Imix, Swissray, Imaging Dynamics, andDelft Diagnostic Imaging are involved in thedevelopment of a variety of different technologiesusing storage phosphor plates, flat-panel detectorsand CCD in different combinations.
The main technology driving CCD-based digitalradiography (DR) systems is the CCD camerasthemselves. Currently, there are several CCD-based digital x-ray systems available with the pri-mary technological difference between the CCD-based systems being the number of CCD camerasthat each system uses. Among those companiesopting for the multiple CCD configuration are
Swissray, which uses four CCD cameras and WuestecMedical Inc., which uses two CCD cameras in its cur-rent system. Companies that use a single CCD config-uration include Nucletron B.V., Imix, Trex Medicaland Imaging Dynamics.
Workflow ComparisonsAs with any new technology, digital detectors havetheir disadvantages. Aside from the cost of digitaldetectors, one must also account for the cost of con-verting previous records to digital, the inconvenienceof learning to use the concept and the fact that this sys-tem can produce more images than are actuallyrequired. Also, it is the consensus that for digital detec-tors, higher doses result in a better image quality.
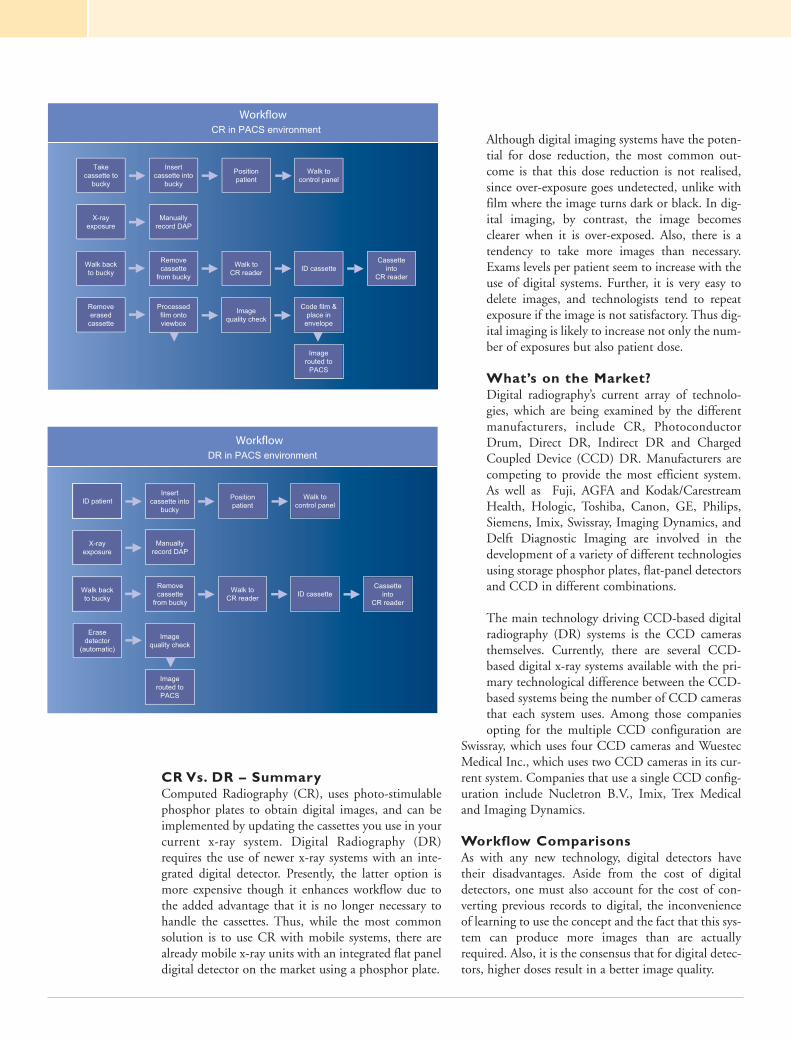
However, we set out to clarify what exactly was the out-come when comparing workflow across three differentsystems: in conventional film screen systems in day-light processing, CR in a PACS environment and DRin a PACS environment, of which the latter involvedthe least number of steps in routine workflow.
Creating the Winning Formula: DoseReduction and Digital RadiographyAs noted above, there is a certain consensus that with-out a higher dose, digital radiography does not per-form to its best. Part of our trials involved shatteringthis myth to clarify whether DR systems are the best future investment option for medical healthcarefacilities. This study on the dose reduction rate up to the limit of diagnostic utilisation compared Philips Horizontal Diagnost H, a screen-film systemusing Kodak/Carestream Health’s skeletal insight SC 200/SC 400 and Kodak/Carestream Health’sDirectView DR 7100
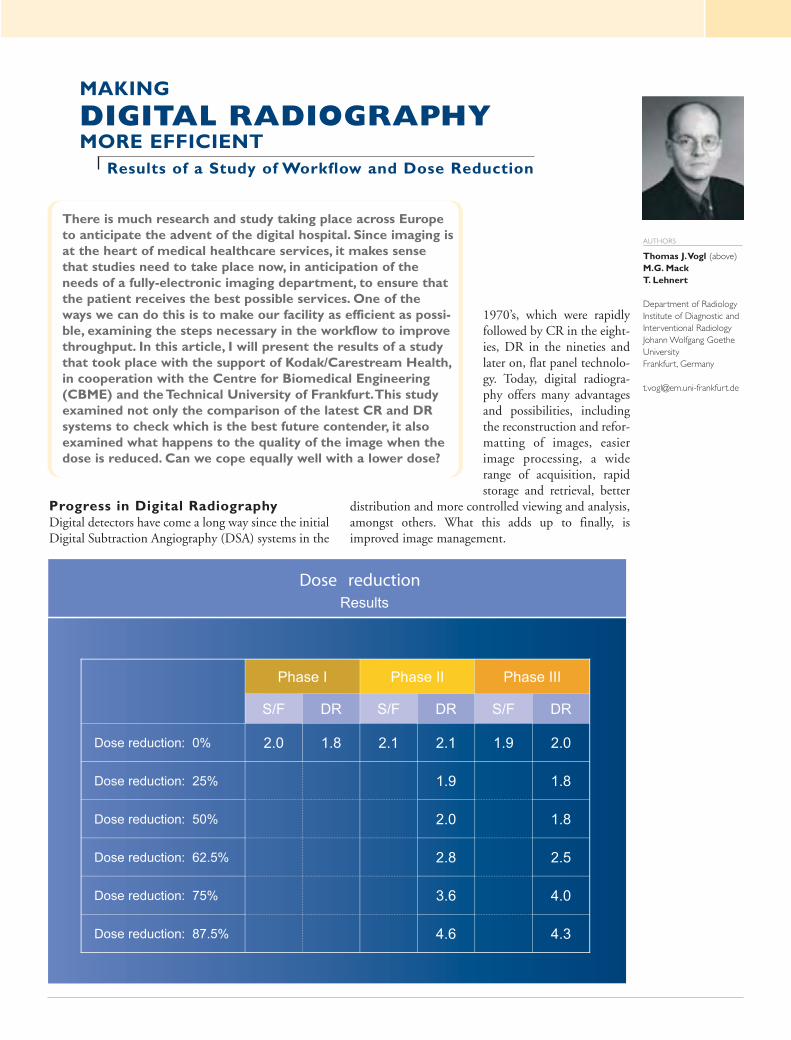
The three-phase trial was designed to evaluate imagequality advantages in digital equipment versus ana-logue equipment. In phase one, the objective was todo exactly this, using a contrast-detail phantom trial.In phase two we then aimed to evaluate the mini-mum required dose to obtain acceptable images fordiagnostic purposes which was performed on extrem-ities from cadavers and finally we repeated this on 85 patients.
Resolution and EvaluationA total of eight radiologic technicians worked on theproject, examining key areas such as resolution, con-trast, articulation and soft tissue areas, to assesswhether with DR one could reduce the dose and stillachieve an acceptable image. Through the exampleswe used, we could still ensure a quality image with arelatively low dose per study and no loss of detail. Inour research laboratory we then used post-processingsteps to fine-tune the images and provide the bestdetail. With this key step involved, we were able toimplement a 50% dose reduction without overall lossof quality.
ConclusionAs this study proved, it is paramount to analyse work-flow as otherwise, potential benefits to the workflowmay be unrecognised. It is also important to includethe patient’s needs in the study protocol. It is highlypossible to implement DR and using fine tuning toincorporate a significant dose reduction. We are gain-ing expertise all the time.
Corporate Presentation
IntroductionDoctor Roentgen, winner of the first NobelPrize, discovered X-rays in 1895. In 1896,the following year, the son of ShimadzuCorporation's founder Genzo Shimadzu Jr.became the first person in Japan to succeedin capturing X-ray images. Based on X-raytechnology accumulated over more than acentury since the corporation was founded,Shimadzu continues to pursue the R&D forthe most advanced technology in this field,providing high added value and reliabilitydiagnostic imaging systems and solutions toadvanced medical facilities. Our challengeto develop the world’s first Direct-conver-sion flat panel detector(FPD) for both stillimages and moving images which nobodycould provide still now is also the one thatwas made from such pioneer spirits and richclinical and X-ray field experiences of ours.
If we look at the history of X-rays, we cansee that the evolution of X-ray technologycan be divided into two general areas: stillimages and fluoroscopic (moving) images.The development of still-image technology,of course, is tied to the history of film-screen systems. Even in this digital age, filmimaging is used widely for radiographybecause of its high image quality. The histo-ry of fluoroscopy began with fluorescentscreens. This was followed by the historical
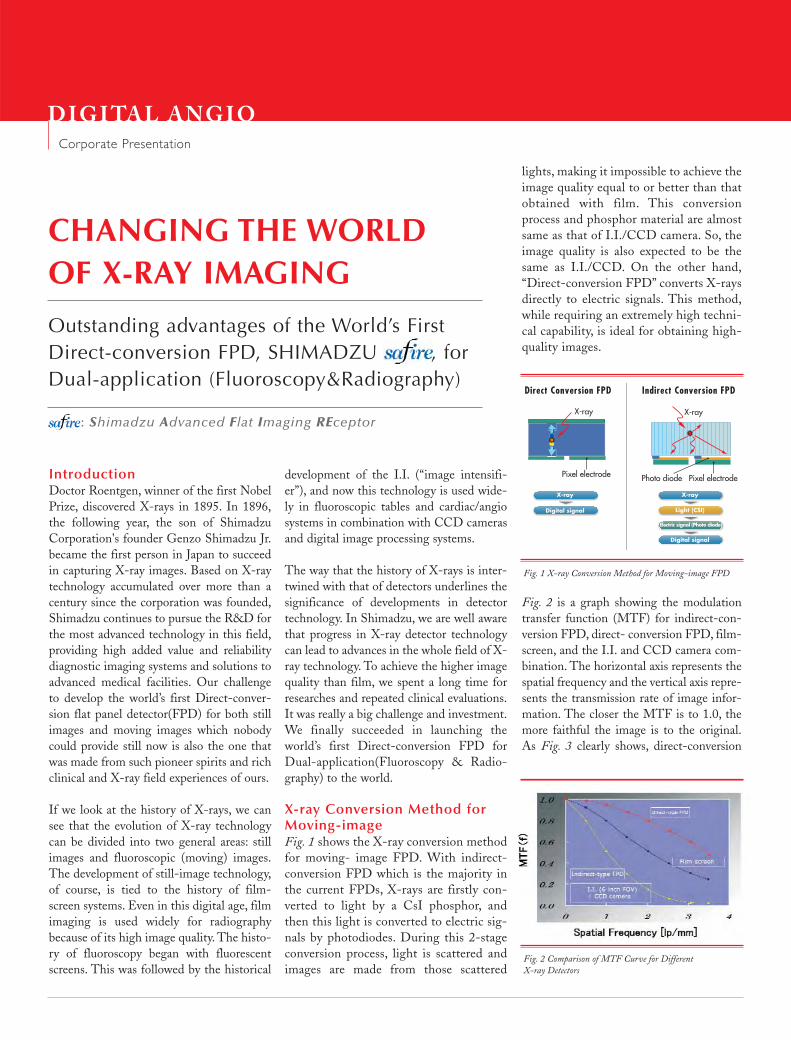
lights, making it impossible to achieve theimage quality equal to or better than thatobtained with film. This conversionprocess and phosphor material are almostsame as that of I.I./CCD camera. So, theimage quality is also expected to be thesame as I.I./CCD. On the other hand,“Direct-conversion FPD” converts X-raysdirectly to electric signals. This method,while requiring an extremely high techni-cal capability, is ideal for obtaining high-quality images.
Fig. 2 is a graph showing the modulationtransfer function (MTF) for indirect-con-version FPD, direct- conversion FPD, film-screen, and the I.I. and CCD camera com-bination. The horizontal axis represents thespatial frequency and the vertical axis repre-sents the transmission rate of image infor-mation. The closer the MTF is to 1.0, themore faithful the image is to the original.As Fig. 3 clearly shows, direct-conversion
development of the I.I. (“image intensifi-er”), and now this technology is used wide-ly in fluoroscopic tables and cardiac/angiosystems in combination with CCD camerasand digital image processing systems.
The way that the history of X-rays is inter-twined with that of detectors underlines thesignificance of developments in detectortechnology. In Shimadzu, we are well awarethat progress in X-ray detector technologycan lead to advances in the whole field of X-ray technology. To achieve the higher imagequality than film, we spent a long time forresearches and repeated clinical evaluations.It was really a big challenge and investment.We finally succeeded in launching theworld’s first Direct-conversion FPD forDual-application(Fluoroscopy & Radio-graphy) to the world.
X-ray Conversion Method forMoving-imageFig. 1 shows the X-ray conversion methodfor moving- image FPD. With indirect-conversion FPD which is the majority inthe current FPDs, X-rays are firstly con-verted to light by a CsI phosphor, andthen this light is converted to electric sig-nals by photodiodes. During this 2-stageconversion process, light is scattered andimages are made from those scattered
CHANGING THE WORLDOF X-RAY IMAGING
Outstanding advantages of the World’s FirstDirect-conversion FPD, SHIMADZU , forDual-application (Fluoroscopy&Radiography)
: Shimadzu Advanced Flat Imaging REceptor
DIGI TAL ANGIO
Fig. 1 X-ray Conversion Method for Moving-image FPD
Fig. 2 Comparison of MTF Curve for Different X-ray Detectors
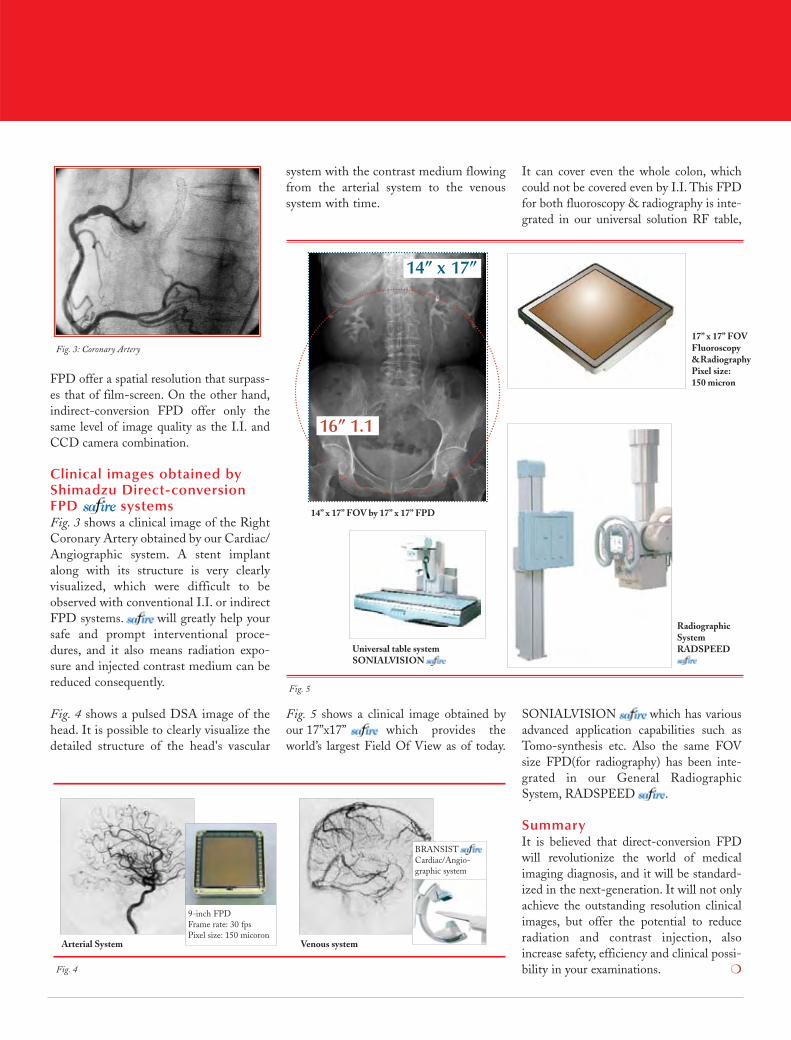
It can cover even the whole colon, whichcould not be covered even by I.I. This FPDfor both fluoroscopy & radiography is inte-grated in our universal solution RF table,
SONIALVISION which has variousadvanced application capabilities such asTomo-synthesis etc. Also the same FOVsize FPD(for radiography) has been inte-grated in our General RadiographicSystem, RADSPEED .
SummaryIt is believed that direct-conversion FPDwill revolutionize the world of medicalimaging diagnosis, and it will be standard-ized in the next-generation. It will not onlyachieve the outstanding resolution clinicalimages, but offer the potential to reduceradiation and contrast injection, alsoincrease safety, efficiency and clinical possi-bility in your examinations. ❍
system with the contrast medium flowingfrom the arterial system to the venoussystem with time.
Fig. 5 shows a clinical image obtained byour 17”x17” , which provides theworld’s largest Field Of View as of today.
FPD offer a spatial resolution that surpass-es that of film-screen. On the other hand,indirect-conversion FPD offer only thesame level of image quality as the I.I. andCCD camera combination.
Clinical images obtained byShimadzu Direct-conversionFPD systemsFig. 3 shows a clinical image of the RightCoronary Artery obtained by our Cardiac/Angiographic system. A stent implantalong with its structure is very clearlyvisualized, which were difficult to beobserved with conventional I.I. or indirectFPD systems. will greatly help yoursafe and prompt interventional proce-dures, and it also means radiation expo-sure and injected contrast medium can bereduced consequently.
Fig. 4 shows a pulsed DSA image of thehead. It is possible to clearly visualize thedetailed structure of the head's vascular
Fig. 3: Coronary Artery
14” x 17” FOV by 17” x 17” FPD
17” x 17” FOVFluoroscopy&RadiographyPixel size:150 micron
Radiographic SystemRADSPEED Universal table system
SONIALVISION
Fig. 4
Fig. 5
Arterial System Venous system
9-inch FPD Frame rate: 30 fpsPixel size: 150 micoron
BRANSISTCardiac/Angio-graphic system
14” x 17”
16” 1.1
Related Documents











