PROMOTING MANAGEMENT AND LEADERSHIP IN MEDICAL IMAGING V OLUME 7 I SSUE 5 / 2007 D ECEMBER - J ANUARY ISSN = 1377-7629 MIR 2007 Congress Review Are PACS Requirements Too High? Radiology in Finland Role of DICOM in Therapy CHANGE MANAGEMENT CHANGE MANAGEMENT www.imagingmanagement.org www.imagingmanagement.org RADIOLOGY ■ CARDIOLOGY ■ INTERVENTION ■ SURGERY ■ IT MANAGEMENT ■ EUROPE ■ ECONOMY ■ TRENDS ■ TECHNOLOGY

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

PROMOTING MANAGEMENT
AND LEADERSHIP
IN MEDICAL IMAGING
VOLUME 7 I SSUE 5 / 2007 DECEMBER - JANUARY
ISSN = 1377-7629
MIR 2007Congress Review
Are PACS RequirementsToo High?
Radiologyin Finland
Role of DICOMin Therapy
CHANGEMANAGEMENTCHANGEMANAGEMENT
www.imagingmanagement.orgwww.imagingmanagement.org
RADIOLOGY ■ CARDIOLOGY ■ INTERVENTION ■ SURGERY ■ IT MANAGEMENT ■ EUROPE ■ ECONOMY ■ TRENDS ■ TECHNOLOGY
E d i t o r i a lChange Management
E D I T O R I A L
Dear readers,
Much has been written on the management ofchange across a variety of industries and services.Change is an integral feature of radiology, which hasevolved and integrated a number of different imag-ing modalities of increasing sophistication, com-plexity and clinical effectiveness. Every time a newpiece of equipment is installed in a department itrequires re-evaluation of working practices, clinicalapplications and workflow, costs and income.
It is also important to ensure that changes thatresult from new equipment implementation orwork practices are patient-focused. The emphasisshould be primarily on clinical effectiveness withcost and staff considerations being important butnevertheless secondary. There are many recentexamples of changes that require careful manage-ment including the introduction of MR, thereplacement of old single-slice CT scanners withmulti-slice CT systems that have massivelyincreased throughput but have brought time-con-suming data analysis and huge storage capacityrequirements. However, the development that hasaffected the imaging department and indeed thewhole hospital has been digital archiving and datatransmission. These PACS systems have requiredre-engineering of clerical, radiographic, radiologicstaff and pan-hospital information delivery andusage and storage of imaging data.
Many papers have been written about the man-agement of the implementation of these systems -the key seems to be very careful planning and
inclusion of all staff from inception to implemen-tation. Discussion of the implications, well-organised re-training and a transparent and orderly plan as well as the removal from an earlystage of all uncertainty are also factors in the success of projects. It is also desired that both staffand patients are persuaded of the benefit to themof the proposed changes.
This edition’s cover story includes three articles ondifferent scenarios in change management. Onearticle emphasises the steps required for successfulchange management in any healthcare setting. Asecond paper discusses the natural resistance ofstaff to change which they perceive, rightly orwrongly, to be threatening to their way of work-ing. The third paper discusses the implications ofmergers & consolidation, and emphasises theneed for all parties to have an understanding ofthe goals of the merger, an agreement on the gov-ernance structure and the creation of a new cul-ture. It is to be hoped that these papers will provideuseful messages. The journal would also welcomecontributions from those of you who have man-aged departmental reengineering whether theywere stress-free or whether they generated lessonsfrom any confrontations that may have occurredduring the transition period.
Please send your responses to myself or to ManagingEditor Dervla Gleeson at [email protected].
Prof. Iain McCall
Prof. Iain McCall
Editor-in-Chief
H AV E YO U R S AY !Letters to the Editor at [email protected]
IMAGING MANAGEMENT: THE OFF IC IAL VOICE OF THE EUROPEAN IMAGING INIT IAT IVE 1

EDITOR-IN-CHIEFProf. Iain McCall (UK)
EDITORIAL BOARDProf. Hans Blickman (The Netherlands)Prof. Georg Bongartz (Switzerland)Prof. Nevra Elmas (Turkey)Prof. Guy Frija (France)Prof. Paolo Inchingolo (Italy)Prof. Lars Lonn (Sweden)Prof. Heinz U. Lemke (Germany)
Prof. Jarl A. Jakobsen (Norway)Prof. Mieczyslaw Pasowicz (Poland)Prof. Udo Sechtem (Germany)Prof. Rainer Seibel (Germany)Dr Nicola H. Strickland (UK)Prof. Henrik S.Thomsen (Denmark)Prof.Vlastimil Valek (Czech Republic)Prof. Berthold Wein (Germany)
CORRESPONDENTSProf. Frank Boudghene (France)Prof. Davide Caramella (Italy)Nicole Denjoy (France)Johan De Sutter (Belgium)Prof.Adam Mester (Hungary)Sergei Nazarenko (Estonia)Dr Hanna Pohjonen (Finland)
GUEST AUTHORSDr J.AhovuoDr S. M. ErturkDr I. E. GilDr J. HodlerDr R. LooseJ. Launders
Dr E. NathansonDr S. Ondategui-ParraDr H. OteroDr J.P. PelageDr P. RosDr P. Ruotsalainen
FEATURES This issue’s features include:
28 Are Technical and Legal Standards for PACS too High?:Results from Mainz Meeting Indicate a Need for ChangeProf. R. Loose
31 The Role of DICOM in Therapy: Coping with Rise in Demand for Surgical ServicesDr H. U. Lemke
33 Focus on Interventional Radiology Equipment:Technology Drives Clinical PracticeJ. Launders
COVER STORY Change Management
16 Six Steps for Successful Change Management:What Works and What Doesn’tProf. M. Goyen
20 IT & Change Management: Dealing with Staff Resistance to PACS IntegrationProf. J. Hodler
24 Academic Medical Centres & Mergers: Consolidation Leads to Increased CompetitivenessProf. P. Ros, Dr S. Ondategui-Parra, Dr S. M. Erturk, Dr H. Otero, Dr I. E. Gil, Dr E. Nathanson
ContentIMAGING Management
Volume 7 Issue 5 / 2007, December - January
1 EditorialBy Editor-in-Chief Prof. Iain McCall
4 MIR Congress ReviewReview of recently-held ‘Management in Radiology’ (MIR) Congress, Oxford, UK
8 Association NewsLatest updates from leading European associations
12 EU NewsSeventh framework programme for research and technological development
14 Industry NewsCoverage of corporate news and updates
44 How To… Assess Staff Performance in the Imaging DepartmentAdvice from Prof. H. Blickman
46 My OpinionInterview with Dr J.P. Pelage
48 Conference AgendaUpcoming seminars in Europe and beyond
COUNTRY FOCUSRadiology in Finland
38 Overview of the Healthcare System in FinlandFinnish Medical Association
40 Management Challenges for Radiology in Finland:Reorganising Departmental Activities for Greater EffectivenessDr J. Ahovuo
42 Finnish National EHR Project: An Interoperable Infrastructure for eHealthDr P. Ruotsalainen

with a particular focus on issues facing thecongress host country, the United Kingdom.The opening session was dedicated to high-lighting imaging management issues in theUK as a direct result of feedback receivedfrom MIR’s congress last year held inBudapest, Hungary, where requests weremade for delegates to be informed aboutthe MIR host country’s imaging issues.
During this first session on Wednesday after-noon, Dr. John Somers spoke amusingly butsincerely about the difficulties in managing“difficult” Trusts in the UK government’snational “Connecting for Health” (CfH)PACS programme, such as resistance tochange. He provided a true recent exampleof mismanagement and overspend experi-enced during one particular PACS imple-mentation across two hospitals, which hedescribed as a ‘bloody’ merger. Many jokingreferences were made in particular to theorthopaedic surgeons involved in the transi-tion, who resisted the change most stronglythrough complaints and indefatigablerequests for unnecessarily expensive addi-tions. His advice, on how to manage thesesorts of expectations, was clearly based onpersonal experience and was well received.
Organised and chaired by Dr NicolaStrickland, consultant radiologist atLondon’s Imperial College Healthcare NHSTrust, this year’s annual Management inRadiology (MIR) congress, a professionalmeeting aimed at leaders, managers andadministrators of imaging departmentsworldwide, was held from 10 - 13 Octoberin Oxford, UK.The congress attracted 137professionals from 29 countries. With 64invited lectures and proffered papers, and52 international lecturers, the event, heldfor the 10th year, was welcomed by partic-ipants and this year had a particularly inno-vative programme.
Sessions Shed Light on Managementin the UKThe congress addressed critical managerialchallenges encountered in the daily work ofrunning the medical imaging department,
This was followed by a presentation by DrNicholas Hollings on managing the problemscreated when implementing PACS in a geo-graphically dispersed and economically chal-lenged region (Cornwall in South WestEngland), including maintaining connectivity,and how solutions such as voice recognitiontechnology and digital dictation can over-come this.
ESR Request Coding SessionAt the specific request of the ESRProfessional Organisations Committee(POC), Dr. Strickland included in this year’sMIR programme, a special session dedicatedto imaging study coding issues and howgreater standardisation can be achievedthrough a set of national codes. It exploredthe management process necessary toupdate those codes and guidelines forimplementation.“A new system is an enablerfor change”, explained speaker Dr RhidianBramley, who discussed the benefits of com-mon code sets such as simplified deploy-ment of systems and the improved interop-erability of systems with more consistentdata collection.The ensuing post-session dis-cussion provoked much comment anddebate. “Payment by results will bring
4 PROMOTING TEAMWORK ACROSS DIFFERENT DISC IPL INES
MIR Congress Review
Dr Nicola StricklandChairman
Dr Nicola Strickland, with Prof. Georg Bongartz
MIR 2007 Congress ReviewReinforcing the Message of Management in Medical Imaging
accountability”, said Dr. Strickland,“We needto ensure that all work performed will drawfunds from the National Health System inthe UK, and in order to achieve this we needto identify how much each item of work isactually costing, and to use radiological pro-cedure coding to make sure that the sameimaging procedures are identified and paidfor uniformly across the UK, and hopefullyacross Europe”. It was also noted that in theUS, there are highly trained coding specialistswho are dedicated to the task of coding, butthe question of who in European hospitalswill be responsible for this, remains.
10 Commandments for Managing anImaging DepartmentOne of the most compelling and entertainingsessions held during the course of the con-gress, the ten commandments for managing animaging department, kicked off with soundadvice from Prof. Philip Gishen who at onepoint, broke into song to express his disdain of
6 PROMOTING TEAMWORK ACROSS DIFFERENT DISC IPL INES
MIR Congress Review
the eternal refrain of radiologists everywhere‘we’re short of staff ’, before proceeding todebate whether or not the field of medicalimaging actually suffers a shortage of trainedstaff. Having worked hard to achieve no wait-ing lists and no delays in reporting in hisdepartment, Prof. Gishen was ideally placed toprovide some key pointers for participants,such as the need to work smarter, so that thegovernment does not continue to farm outroutine radiological work, thus risking thefuture of radiology as a specialty.
Prof. Guy Frija also contributed to this ses-sion with advice on leadership, defining keystrategic goals and targets and dealing withproblems in radiology reporting. Anotherleading speaker, Prof. Henrik Thomsen, urged“visibility, openness and engagement” as thekeys to leading a successful department. Allspeakers were in agreement that peoplemanagement was one of the top factors in
contributing to this success. The results ofthis session will be summarised in a futureedition of IMAGING Management.
Future Congresses and WorkshopsMIR organises a congress each year and awinter course at a variety of European loca-tions. The next winter course on "ApplyingIndustry Leadership Concepts toHealthcare" will be held from 10 - 12January, 2008 in Bad Gastein,Austria, and thenext congress will take place in Athens,Greece, in October 2008.
The workshop programme in particular,will explore key concepts required toenhance a manager's ability to work effec-tively within an organisation. It will furtherexplore concepts such as emotional intel-ligence, why high performance teams arecritical for success and the top keys to suc-cessful communication.
The MIR Congress presentations and pic-tures are available at:www.imagingmanagement.org.To register for the upcoming workshopplease visit: www.mir-online.org.The following edition of IMAGING Managementincludes a cover story highlighting in more detailthe leading presentations from the congress.
Prof. Guy Frija speaking during the congress
Prof. Michael J. Pentecost
Dates Announced for 2008EuroPACS Meeting Next year’s EuroPACS meeting is to be heldJune 25 - 28, 2008, Barcelona, Spain, in con-junction with CARS. The conference pro-
gramme will offer information on the latestand most significant developments in clinicalpractice, research and education within digi-tal radiology, including:
• PACS Planning and Purchasing Strategies• PACS Beyond Radiology (Cardiology,
Endoscopy, Opthalmology, etc.)• Image Distribution, Storage
and Archiving Strategies
• Workflow and Data Flow in Radiology • PACS/RIS/HIS Integration Issues• Regional PACS and Teleradiology• Security and Privacy, Quality Assurance,
Legal Aspects• Standardisation (DICOM, HL7, IHE)• PACS and E-Learning in Radiology and
Medical Sciences
www.europacs.org
A s s o c i a t i o n N e w sAssociat ion News
Participants will benefit from the success ofprevious events, to ensure that interoper-ability remains a hot topic and to ensure thefuture success of their systems in regards tointeroperability.
The IHE ConnectathonIHE provides a detailed implementation andtesting process to promote the adoption ofstandards-based interoperability by vendorsand users of healthcare information systems.The process culminates in the Connectathon,a weeklong interoperability-testing event. TheConnectathon provides the most detailed val-
idation of the participants' integration work.Participating companies prepare for the eventusing testing software - the MESA test tools -developed for this purpose.
IHE is an initiative by healthcare profession-als and industry to improve the way com-puter systems in healthcare share informa-tion. IHE promotes the coordinated use ofestablished standards such as DICOM andHL7 to address specific clinical needs in sup-port of optimal patient care.
www.ihe-europe.org
Registration Open for 2008IHE Europe ConnectathonRegistration for the next IHE EuropeConnectathon, to be held at St Catherine’sCollege in Oxford, UK will close December7, 2007. The Connectathon itself will takeplace Monday, April 7 to Friday, April 11,2008, while the traditional participants’workshop will be held on both February 6and 7, 2008.
8 PROMOTING TEAMWORK ACROSS DIFFERENT DISC IPL INES
Abstract Submission Openfor 2008 CARS Congress andExhibition Abstract submissions for presenters at theforthcoming CARS 2008 22nd InternationalCongress and Exhibition will be accepteduntil January 10, 2008. Chaired by Prof.Stanley Baum and Co-chaired by Prof. LuisDonoso Bach, this year’s edition takes placesin Barcelona, Spain from June 25 – 28, 2008.Programme topics will include:
• Medical Imaging, e.g., CT, MR, US,SPECT, etc.
• Computer Assisted Cardiovascular Imaging
• Image Processing and Display• Medical Workstations• Interventional Radiology • Minimally Invasive Spinal Therapy• Image Guided Diagnosis and Therapy
of the Prostate• Tumour Ablation Therapies• Image Guided Radiation Therapy• Telemedicine, e-Health and Multimedia EPR
The CARS meeting will also host the annu-al conference of the International Society for
Computer Aided Surgery, the InternationalWorkshop on Computer-Aided Diagnosis,the annual EuroPACS meeting and theComputed Maxillofacial Imaging Congress.
And finally, the 7th CARS/SPIE JointWorkshop on Surgical PACS and the DigitalOperating Room, chaired by ProfessorHeinz Lemke (University of SouthernCalifornia) and Dr. Osman Ratib (Universityof Geneva) was successfully held on theclosing day of CARS 2007.
www.cars-int.org

WHO Redesignates ECRIInstitute as a PAHO/WHOCollaborating CentreECRI Institute, an independent nonprofitbody that researches the best approaches to improving patient care, announced that the World Health Organization (WHO) hasredesignated ECRI Institute as aPAHO/WHO Collaborating Centre forPatient Safety, Risk Management, andHealthcare Technology.
WHO Collaborating Centres are part of aninter-institutional network designed tostrengthen resources in terms of informa-tion, services, research, and training in sup-port of national health development. As aPAHO/WHO Collaborating Centre, ECRIInstitute’s activities include coordinating amedical device safety programme, providingtraining in technology assessment, identifyinghealthcare standards and guidelines, andsupporting global patient safety efforts.
“We are gratified to again earn designationas a PAHO/WHO Collaborating Centre,”
says Ronni P. Solomon, J.D., ECRI Institute’sExecutive Vice President. “As a nonprofitorganisation, we are committed to findingthe most effective ways to improve patientcare and to sharing that information with theinternational healthcare community.”
Since its first PAHO/WHO CollaboratingCentre designation in 1987, ECRI Institutehas worked on a range of health technologyissues around the world.
www.ecri.org.uk
Update from CIRSE 2007With over 4,700 participants and a recordlevel of abstract submissions, this year’sannual congress of the Cardiovascular andInterventional Radiological Society ofEurope (CIRSE) proved a great success.Abstract submission for CIRSE 2007reached an all time high surpassing the 1,000benchmark for the first time in CIRSE histo-ry.The strong increase in submissions to theCIRSE meeting as well as the increasingnumber of late-breaking abstract submis-sions shows once again that CIRSE is notonly an important educational congress, butalso an outstanding meeting for the presen-tation of new scientific findings.
Scientific ProgrammeThe programme put together by Prof.Michael Lee and his scientific programmecommittee comprised more than 100 hoursof lectures and hands-on workshops.CIRSE’s new format streamlined around fivemajor topics (Vascular Interventions, Non-Vascular Interventions, TranscatheterEmbolisation, Interventional Oncology and
Clinical Practice) facilitated itinerary planningand enabled participants to follow a specificarea of interest without overlap. The newformat will be continued for CIRSE 2008.
The CIRSE Foundation Courses, designedfor young doctors to illustrate the basic prin-ciples of a specific procedure, focused onembolisation and peripheral vascular dis-ease.These sessions were complemented bya self-assessment test based on the ESR toolwhich had been adapted for CIRSE by JoséIgnacio Bilbao.The test could be carried outindividually by the participants or in a specialsession which allowed for Q and A.
The ‘CIRSE meets…’ session was dedicatedto the European Society for CardiovascularSurgery (ESVS) and China, a country ofalmost unlimited potential for IR. ProfessorKe Xu and other distinguished members ofthe Chinese Society of InterventionalRadiology (CSIR) gave a very interestinginsight into the current status of IR in Chinaas well as into the state of specific proce-dures and conditions in their home country.
The CIRSE 2007 exhibition comprised3,000m2 of exhibition space, where morecompanies than ever chose to present their
latest developments and many launchedtheir latest products. Numerous companiesalso offered Learning Centres to the partic-ipants. The industry satellite symposia, com-prising a newly introduced breakfast slot,also enjoyed great popularity.
Apart from the usual highlights of the CIRSEsocial programme, such as the highly popu-lar CIRSE Foundation Party, this year’s meet-ing also featured two new events; the CIRSEFun Run and the first CIRSE Soccer Cup.Both events met with a very positiveresponse, and will become regular featuresof future CIRSE meetings.
Abstract Submissions CIRSE 2008!Upon their arrival from Athens, the mem-bers of the CIRSE Scientific ProgrammeCommittee have already started puttingtogether the topics and sessions for CIRSE2008 to take place in CopenhagenSeptember 13 - 17. Abstract submission forCIRSE 2008 will be possible from December4, 2007 until February 12, 2008. Please referto www.cirse.org or contact CIRSE CentralOffice at [email protected] to stay updated onCIRSE 2008 and all other CIRSE initiatives.
www.cirse.org
10 PROMOTING TEAMWORK ACROSS DIFFERENT DISC IPL INES
A s s o c i a t i o n N e w sAssociat ion News

The Seventh Framework Programme forResearch and Technological Development(FP7) is the European Union's maininstrument for funding research inEurope. Running from 2007 to 2013, itwill execute a budget during that periodof €50.5 billion and an additionalEuratom budget for the next five years of€2.7 billion. FP7 is designed to supportresearch in selected priority areas.
How is FP7 made up? FP7 is made up of four main specific pro-grammes under the headings Cooperation,Ideas, People and Capacities, plus a fifth spe-cific programme on nuclear research. Herewe assess the most relevant ones.
Cooperation With a budget of €32 billion, the “Cooper-ation” programme will provide research sup-port to international cooperation projectsacross the European Union and beyond. Itsten thematic areas, corresponding to majorfields in science and research will promotethe progress of knowledge and technology.Research will be supported and strength-ened to address European social, economic,environmental, public health and industrialchallenges, serve the public good and sup-port developing countries.
Health Research ProgrammeWith a budget of €6 billion, the healthresearch programme aims to improve thehealth of European citizens, and increase andstrengthen the competitiveness and innova-tive capacity of European health-relatedindustries and businesses. Global health
cancer, cardiovascular disease, diabetes/-obesity, rare diseases, other chronic diseasesincluding rheumatoid diseases, arthritis and muscoskeletal diseases
• Optimising the delivery of healthcare to European citizens
• Translation of clinical outcome into clinical practice
• Quality, efficiency and solidarity of health care systems including transitional health care systems and home care strategies
• Enhanced disease prevention and better use of medicines
• Appropriate use of new health therapies and technologies
“People” Programme SupportsCareers in Research With a budget of €4.7 billion, the “People”programme offers individuals training andcareer development in research. It aims toencourage European researchers to stay inEurope and attract the best researchers inthe world to European research excellenceand infrastructures.The “People” programmeshould encourage individuals to enter theprofession of researcher ; structure theirresearch training by offering options; and,encourage mobility within the same sector.The mobility of researchers is not only keyto the career development of researchersbut also vital to the sharing and transfer ofknowledge between countries and sectors.
During FP7, a series of EU research fundedactions will support the on-going training,research and mobility of highly qualified sci-entists and encourage the proliferation ofcentres of excellence in the EU and their
issues, like emerging epidemics, will also beaddressed. European collaboration withdeveloping countries will allow those coun-tries to develop research capacities. Itsemphasis will be put on translationalresearch (i.e. the translation of basic discover-ies in clinical applications), the developmentand validation of new therapies, methods forhealth promotion and prevention includingthe promotion of healthy ageing, diagnostictools and medical technologies, and sustain-able and efficient healthcare systems.
Clinical research will tackle a number of dis-eases such as cancer, cardiovascular, infec-tious, mental and neurological diseases, andin particular those linked with ageing, such asAlzheimers and Parkinsons diseases.Throughinternational multi-centre trials involving therequired number of patients, new drugs andtreatments would be developed in a shortertime frame. European-funded healthresearch will focus on:• Biotechnology, generic tools and medical
technologies for human health• High-throughput research• Detection, diagnosis and monitoring• Prediction of suitability, safety and efficacy
of therapies• Innovative therapeutic approaches
and intervention • Translating research for human health -
Integration of biological data and processes • Research on the brain and related
diseases, human development and ageing• Translational research in infectious diseases
(HIV/AIDS, malaria, tuberculosis, SARS,avian influenza)
• Translational research in major diseases:
Dervla GleesonManaging EditorIMAGING [email protected]
EU News
SEVENTH FRAMEWORK PROGRAMMEFOR RESEARCH AND TECHNOLOGICAL DEVELOPMENT
12 PROMOTING TEAMWORK ACROSS DIFFERENT DISC IPL INES

contribution in new areas of research andtechnology. This will be carried out throughinitiatives such as lifelong training and careerdevelopment through individual fellowshipsand co-financing programmes at interna-tional, national and regional level and inter-national outgoing and incoming fellowshipsaiming to increase research talent outsideEurope and fostering mutually beneficialresearch collaboration with researchersfrom outside Europe. The activity will alsoinclude measures to counterbalance "braindrain" and create networks of Europeanresearchers working abroad.
Capacities With a budget of €4.2 billion, the“Capacities” programme will optimise theuse and development of research infrastruc-tures, while enhancing the innovative capaci-ties of SMEs to benefit from research. Theprogramme is designed to support regionalresearch-driven clusters and at the sametime unlock the research potential in theEU’s convergence and outermost regions.
Four Countries Sign Agreement toJoin FP7Croatia, Serbia, the former Yugoslav Republicof Macedonia and Turkey all recently signedagreements that enable their eligibility tocompete on an equal footing with EUMember States in the Seventh FrameworkProgramme (FP7), following the signature ofMemoranda of Understanding with theEuropean Commission.
These countries will now be able to partici-pate in all the FP7 calls for proposals andenjoy the same rights for participation as EUMember States in all the research cooperationand supported actions funded under FP7.
Science and Research Commissioner JanezPotocnik has noted the importance of theagreement in view of these countries' appli-cation to join the EU. 'Research cooperationwith Europe's scientific community is a toolwhich can smooth the way for the integra-tion process of candidate and potential can-didate countries into the European Union,'he said.
Further Readinghttp://cordis.europa.eu/fp7http://www.dti.gov.uk/science/uk-intl-engagement/euro-programmes/fp7/page38886.htmlhttp://europa.eu/scadplus/leg/en/lvb/i23022.htm
Montenegro has also requested to becomeassociated with FP7 and it is expected that adecision will be taken once Stabilisation andAssociation Agreement (SAA) negotiationshave come to a head. Albania, Bosnia-Herzegovina, Israel and Switzerland are alsoexpected to join soon.
EU News

ORBIS via the patient interface.The roll-outof the DMS to two more hospitals of theMKO-holding, the St. Franziskus-HospitalHarderberg and the Krankenhaus St.Raphael Ostercappeln, is planned to becompleted by the end of 2008.
HologicStudy Rates Performance of DirectDigital Over Film MammographyThe Vestfold County Study, comparing theresults of a particular digital mammographytechnology to women screened with filmwas published in European Radiology inAugust 2007. Researchers compared can-cer detection and recall rates of 18,239women screened with a Hologic Seleniadigital mammography system to the resultsof 324,763 women screened with film overa two year period. Researchers reportedthat the detection rate for ductal carcinomain situ (DCIS) and the positive predictivevalue for cancer (PPV) were statistically sig-nificantly higher and the technical recall ratewas statistically lower for Selenia over film.
CarestreamCarestream Adds to Molecular ImagingProduct LineCarestream Molecular Imaging is introduc-ing new large Stokes shift dyes for fluores-cent in-vivo imaging applications. The dyesare designed to enable researchers and sci-entists to maximise fluorescent signal andminimise autofluorescence issues during in-vivo imaging. Kodak X-Sight dyes will beavailable in 2008 for preclinical use.
PhilipsPhilips Seeks to Reduce Time fromHeart Attack to TreatmentRoyal Philips Electronics recently demon-strated its HeartStart MRx Monitor/-Defibrillator, which enables paramedics totransmit patient data from the ambulanceto the hospital’s emergency department tohelp clinicians use ECG data to beginorganising its resources before the patientarrives.The HeartStart MRx also integrateswith the hospital’s ECG management system
Industr y News
TraceMasterVue, enabling critical patientinformation to be seen where it’s needed.
E-Z-EME-Z-EM Announces Financial Results 2007E-Z-EM, Inc. has announced financial resultsfor its fiscal 2007 fourth quarter and fiscalyear. Highlights for the quarter included:• Net sales from continuing operations of
$36.7 million • Earnings from continuing operations of
$2.8 million • Receipt of 510(k) regulatory approval
for EmpowerMRTM • Receipt of $8 million follow-on order
for RSDL from the DoD
Sales were led by CT imaging products,which increased 8% over the prior-yearquarter. Injector system sales were up 20%,while CT contrast sales were flat comparedto the prior-year period. Sales of virtualcolonoscopy and X-ray fluoroscopy prod-ucts grew 22% and 7%, respectively. Grossprofit for the current quarter increased10% to $17.1 million from $15.6 million inthe prior-year quarter.
ConfirmaConfirma Expands Extensive Education ProgrammeConfirma has announced that it hasawarded an educational grant to theInternational Centre for PostgraduateMedical Education (ICPME) to develop anew curriculum of continuing medicaleducation for breast MRI.The breast MRIcurriculum includes two separate pro-grammes supported by the educationalgrant from Confirma.The first is “Decisionsin Medical Imaging – Breast MRI Analysisand Interpretation with CAD,” a series ofonline case reviews using CAD to aid theradiologist in the analysis and interpreta-tion of breast MRI studies.The second is afull-day course of instruction and trainingfor radiologists and interventional radiolo-gists, “Breast MR Imaging, Interpretationand Intervention.”
Siemens Siemens Expand VascularAnalysis OfferingNew functions for vascular analysis areavailable for Siemens Medical Solution’sclient-server solution for computed tomog-raphy (CT), the syngo WebSpace. syngoWebSpace allows users to access andmanipulate CT images via an internet orother network connection. Improved algo-rithms and additional tools in the new soft-ware version aid physicians to more quick-ly analyse small vessels as well as documentreports. For example, computer-supportedmeasurements for stenoses and compar-isons of vessel cross-sections are now partof the package.
MatroxMatrox Releases SmartCamera/Software Package Matrox Imaging has launched its Iris E-Series with new Design Assistant, a smartcamera/software package. It enables usersto instruct the Matrox Iris E-Series camerato intuitively grab, process and display, per-form measurements, analyse image dataand read machine codes. This potentiallyeliminates the need for programming andscripting and users benefit from simplifiedapplication development.The developmentenvironment is fully self-contained for bothapplication development and deployment,and the integrated HTML editor and layouttool gives users more flexibility to create acustom web-based operator view for mon-itoring the application.
AGFAAgfa HealthCare Announces LiveOperation of HYDMedia Solution Agfa HealthCare has announced the instal-lation of its HYDMedia Archiving andDocument Management System (DMS) atthe Marienhospital in Osnabrück, part ofthe Management Katholischer Kranken-häuser der Region Osnabrück (MKO) hold-ing, in northern Germany. The HYDMediasolution was installed at the hospital over aperiod of four months and is connected to
14 PROMOTING TEAMWORK ACROSS DIFFERENT DISC IPL INES
How should we implement change? It is a simpleenough question; surely there is a simple answer - espe-cially since we do it so often. Every time we implementa new system or install a new process, we are imple-menting change. Therefore, surely there are somethings that work, and some things that fail?
The Only Person That Likes Change is a Wet BabyWhen change is considered or promoted, there willalways be a conflict between those supporting the sta-tus quo and those supporting change. Among the sup-porters of change there may be conflict as to the extentand the nature of change that is desired. There is anassumption that there is a clear solution and theprocess is only a matter of finding that solution. Theprogression follows a linear process, namely deciding ifchange is necessary, and if so, what change will bemade. Healthcare is an area in which change is character-istically slow. In addition, healthcare organisations oftenlook at issues in a very narrow, short term way. However,in healthcare there may not be a clear, single solution orbest choice. There may be as large a group that supportsthe status quo as there is promoting change.
Views on Change ManagementChange management can be viewed from two perspec-tives – from those implementing the change and from
the recipients of change. Your view of change man-agement varies dramatically if you are the executivedemanding the change versus the front-line employ-ee who may be unsure why a change is even needed.
In many cases at the onset of a new change, neitherthe executive nor the front-line employee is knowl-edgeable about managing change. Executives wantthe change to happen now; employees are simplydoing their job. It is the project managers, consult-ants or members of the project team that first learnabout the necessity for change management. Theyare the first to realise the two dimensions of changemanagement: the top-down managers’ perspectiveand the bottom-up perspective.
The result is a potentially dangerous mix of differentpriorities, different knowledge sets and differentdriving forces. If the change is not managed proper-ly, these different values and driving forces clash,resulting in unfortunate outcomes for the business.Many healthcare organisations learn the hard waythrough failed projects. They learn that change man-agement is not something addressed after the fact.Change management must start at the beginning ofthe project and be integrated into all steps. Both per-spectives of change management must be addressed:the managers’ and the employees’.
The way hospitals address and manage change cansubstantially influence employees' willingness to com-mit to the process.Today, the question is not whetherto change, but how we manage the transformation ina way that also motivates employees and unifies thehealthcare organisation. On the one hand, change isdemanding and stressful. On the other hand it pro-vides an exciting and challenging area that is respon-sible not only for the existence of but also for theenjoyment of our jobs.
16 PROMOTING TEAMWORK ACROSS DIFFERENT DISC IPL INES
AUTHOR
Prof. Mathias GoyenAssistant ProfessorChief CommunicationOfficerUniversity Medical CentreHamburg-EppendorfHamburg, [email protected]
What Works and What Doesn’t
SIX STEPS FOR SUCCESSFULCHANGE MANAGEMENT
Cover Story Change Management

IMAGING MANAGEMENT: THE OFF IC IAL VOICE OF THE EUROPEAN IMAGING INIT IAT IVE 17
The Managers’ Perspective The managers’ perspective on change is results-orient-ed. Managers are very aware of the issues facing thedepartment or institution and are accountable for itsfinancial performance. When a change is deemed nec-essary, quick action is required. Primary concernsinclude:• When can the change be completed? • How much will this improve the processes
of the hospital?• How will this change impact financial performance?• What is the required investment?• How will it impact participants within the process
(e.g. patients, referring physicians, etc.)
The Employees’ Perspective Now consider the perspective of front-line employeesin hospitals. They are the ones who must ultimatelyimplement the change. In general, they do not have anoverview of the department’s or institution’s strategicgoals. Serving patients and getting the job done on aday-to-day basis are their primary areas of interest.When changes are made, many employees lack thebroader context or knowledge base of why the changeis being made. They also do not share the sameaccountabilities as managers. They question, therefore,how the change will impact them personally.
Six Steps for Implementing ChangeGiven the above-described model or framework forchange management, you can break down the requiredelements to effectively manage change.
I - Understand status quoCreating something new is always an act of destruc-tion. When implementing change you replace the oldstatus quo known to everyone, with a mere vision of agoal in the future. Having respect for the existing sta-tus quo builds respect for you. Some status quos havebeen around for only a few months, others for years.The older the status quo, the more likely it will be dif-ficult to remove. The older a status quo, the more it hasbeen proven as being valid. Let us respect the statusquo, but not be afraid of change.
II - Understand the need for changeBefore you implement change, it is crucial that youunderstand all the reasons for it. You must become anexpert in the change being proposed or reacted to,
because people will look to you for answers. Theymight even look to you for guidance. At the very least,"Is the change necessary?" will be asked by everyoneimpacted by it. It would be nice to have an answer.
III - Create desire to changeThis phase draws on all your management and leader-ship abilities. The more people who come to believethat the change is necessary, the easier the changeprocess. Imposing on them what to believe is not theanswer. Describing the problem, creating a vision of thefuture, and allowing them to contribute to the details ofwhat the solution might be, creates a common groundfor support and commitment to the change.
IV - Get operationalThe move takes place, the layoffs happen, the new sys-tem is made live. Getting the operational details to goas smoothly as possible, through good managementpractices, adds to the ease with which the change isassimilated.
V - Reinforce new behaviourMost attempts that are prepared well and implement-ed properly will result in sustained success. Not allattempts will result in failure. Each one of those suc-cesses should be rewarded. Employees initially hesitantto the respective change need special attention to guidethem to appreciation.
VI - CelebrateCelebration is both personal and peer recognition thatyou are of value to the progress of our department orinstitution. People like to be appreciated, and a cele-bration is a powerful way to communicate that mes-sage. Celebrating does not require a huge financialbudget. It does require an attitude, however, that peo-ple work better when their efforts are appreciated.
Implementing a support structure to assist peoplethrough a significant change is not just a matter ofovercoming your reluctance to leave the comfort of theold status quo; it is an attempt to support and promotethe determination and courage necessary to movetowards the next one. Especially in healthcare organi-sations, change management approaches are often ratherrandom instead of strategically driven. However, astrategic management of change for healthcare organisa-tions is needed to face the challenges of the future. ����
Cover Story Change Management
It was a bold decision for VestfoldHospital in Norway to establish anall-digital breast care unit in 2002. Digital breast imaging was in itsinfancy, and few breast centers inScandinavia, indeed few in theworld, were completely digital.
The center had originally plannedto purchase one digital mammog-raphy system and a computed
radiography system. However, a financial analysis found thesite could more than break even with two digital mammog-raphy systems and a prone breast biopsy system. One digitalmammography unit would be dedicated to breast screening;the second would be reserved for diagnostic cases.
The addition of a prone biopsy table would ensure that opti-mal patient care could be achieved. Criteria and motivationswere diverse. Hospital radiologists wanted to acquire the bestimage quality and give optimal patient comfort.
The hospital administrators wanted a system that wouldevolve as the Center’s patient population grew while puttingup with very heavy usage for the Norwegian Breast CancerScreening Program. After a thorough review of the available technologies, Vestfold chose the Hologic Selenia digitalmammography system. The decision to go with Hologic tech-nology was based on the quality of their selenium detectorimages and the size of their detector (the system’s field ofview is one of the largest available).
“We believe strongly in the [Hologic Selenia] detector,” said Dr.Einar Vigeland, the leading consultant radiologist at the breastcare unit in Vestfold. “We have a strong belief that we have cho-sen the right system and that this is the solution for the future.”
Also important was the integration of mammography into the radiology department’s existing PACS. At Vestfoldmammograms are both archived and presented on soft copyworkstations using the PACS. They are made available elec-tronically throughout the radiology department.Dr. Vigeland is particularly impressed with the Selenia system’s ability to visualize microcalcifications. “For micro-calcifications, digital is clearly superior to analog.” The centerreceives analog images from many referrers, enabling aneasy comparison with digitally captured pictures. “We cannotsee anything on film better than we can with digital,” he said.
In August 2007, European Radiology published the results of astudy by Dr. Vigeland and his colleagues. The study looked atcancer detection and recall rates for 18,239 women screenedwith the Selenia systems at Vestfold Hospital compared to theresults of 324,763 women screened with film in other hospitalsinvolved with the Norwegian breast screening program.
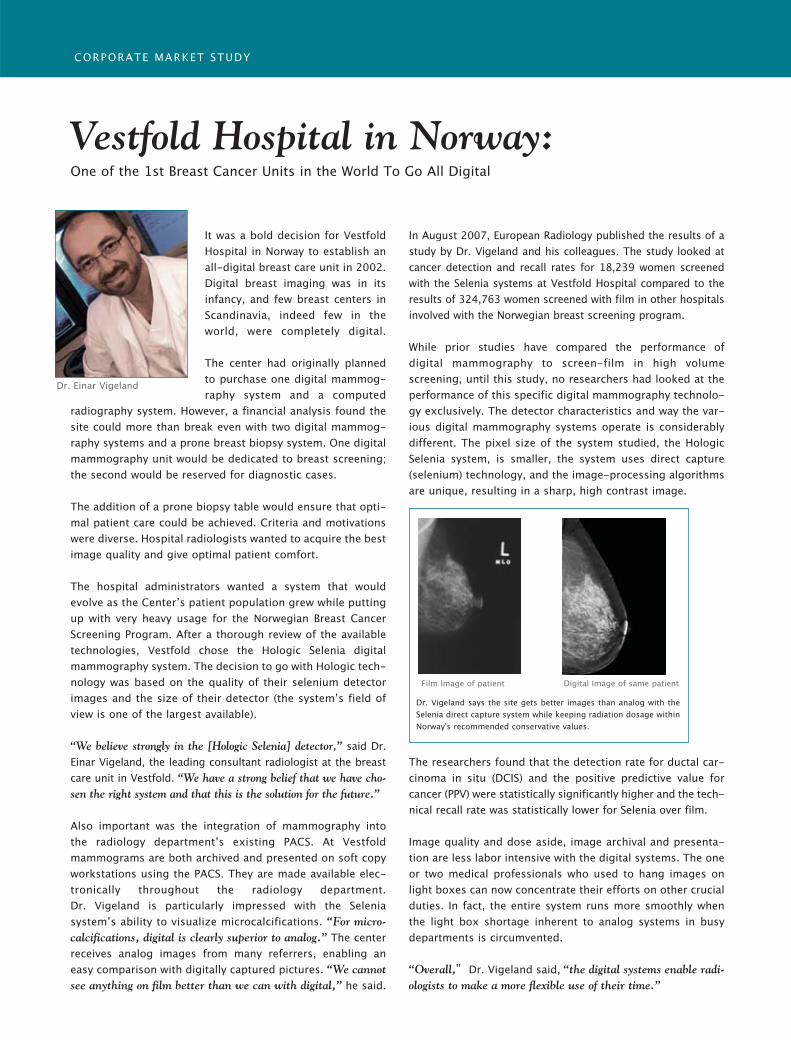
While prior studies have compared the performance of digital mammography to screen-film in high volume screening, until this study, no researchers had looked at theperformance of this specific digital mammography technolo-gy exclusively. The detector characteristics and way the var-ious digital mammography systems operate is considerablydifferent. The pixel size of the system studied, the HologicSelenia system, is smaller, the system uses direct capture(selenium) technology, and the image-processing algorithmsare unique, resulting in a sharp, high contrast image.
The researchers found that the detection rate for ductal car-cinoma in situ (DCIS) and the positive predictive value forcancer (PPV) were statistically significantly higher and the tech-nical recall rate was statistically lower for Selenia over film.
Image quality and dose aside, image archival and presenta-tion are less labor intensive with the digital systems. The oneor two medical professionals who used to hang images onlight boxes can now concentrate their efforts on other crucialduties. In fact, the entire system runs more smoothly whenthe light box shortage inherent to analog systems in busydepartments is circumvented.
“Overall,” Dr. Vigeland said, “the digital systems enable radi-ologists to make a more flexible use of their time.”
Vestfold Hospital in Norway:One of the 1st Breast Cancer Units in the World To Go All Digital
CORPORATE MARKET STUDY
Dr. Vigeland says the site gets better images than analog with theSelenia direct capture system while keeping radiation dosage withinNorway's recommended conservative values.
Film Image of patient Digital Image of same patient
Dr. Einar Vigeland
Cover Story Change Management
20 PROMOTING TEAMWORK ACROSS DIFFERENT DISC IPL INES
The project team was aware that introducing a PACSwas not only an informatics project but that it wouldchange a number of processes both within radiologyand in the clinics. After planning, tendering, decision-making and securing of financing the PACS wentonline in May 2002. An extensive training programmewas initiated, and there was extensive internal promo-tion of the new PACS.
Post-installation ReviewA review of the PACS project was performed threemonths after installation. The result was generallypositive on the technical side, in terms of systemreliability and functionality, as well as interfaces withthe HIS and network capacity. However, the DVDjukebox installed for long-term storage was alreadyslow during heavy outpatient clinics, though mostexams were still available via hard disk-based short-term storage. The special equipment required for the
operation theatre had long delivery times and wasnot yet installed.
On the human side, the new PACS was quickly accept-ed as an additional tool, for instance as a back-up solu-tion when hardcopies were not available or for slideproduction. However, total integration was provingdifficult, as the cost of film was decreasing more slow-ly than anticipated, in part due to an increasing num-ber of MR exams performed after installation of a sec-ond scanner, but also due to the unwillingness of manyclinicians to reduce hardcopies. Workflow changes werefelt to be extensive, even for the department of radiolo-gy, which had been most closely involved in the project.
Tough Measures to Ensure PACS UptakeThe following guidelines were implemented to increasethe uptake of PACS and to discourage dependency onhardcopies:
Dealing with Staff Resistance to PACS Integration
IT & CHANGEMANAGEMENT
In 2006, the Orthopaedic University Hospital Balgrist in Zurichtreated more than 4,000 inpatients, saw approximately 40,000 clin-ical outpatients and performed approximately 42,000 radiologicalexams.The hospital is part of the university healthcare system.Orthopaedic surgery is the dominant clinical discipline. In addition,there are departments for paraplegiology, rheumatology andrehabilitation medicine, anaesthesiology and internal medicine. In2000, a decision was made to install a PACS.This article deals withthe varying degrees of resistance met with from internal staff, andhow we overcame these management concerns.
AUTHOR
Prof. Juerg Hodler ChairmanDepartment of RadiologyOrthopaedic UniversityHospital BalgristZurich, [email protected]
Table 1: Goals of the PACS process
Goal Expected contribution of PACSImprove quality of care • Improvement of image availability
• Faster radiology service• New opportunities for quality control
Marketing • Positioning of the hospital as early adopter of new technology• Faster service than competitors
Cost savings • Reduction of printing and mailing cost• No replacement of auto-alternators
Productivity • Reduction of workload for printing and handling of hardcopies• Improved workflow
Scientific documentation • Electronic administration of studies• 100% availability of documents
Teaching • Electronic organisation and retrieval of teaching files

• No hardcopy printing for non-orthopaedic clinics.• Pushing for individual commitments to use PACS
in orthopaedic surgery.• For reluctant surgeons, printing of hardcopy was
performed only on individual request.• Publication of statistics regarding percentage of
exams documented on hardcopies.• Absolutely no reprinting of lost hardcopies.• Continuous PACS training, including thorough
induction of new employees. • Continuous internal promotion of PACS during
morning conferences, with flyers, posters and electronic mailing.
• Refusal to handle any hardcopies by the depart-ment of radiology, such as mailing and storage, in contrast to the support provided for electronic data handling.
As expected, resistence against the PACS increased, fol-lowing these activities. We encountered many of thewell-known problems occurring in change manage-ment situations (Lewin 1951, Beckhard 1969).
Change ManagementChange management “manages the people side ofchange and realises it effectively” (Hiatt and Creasey,2003). According to Strebel (1998), there are four typ-ical reactions to major change, as outlined in table 2(see below).
Another approach to innovation is provided by theEverett Rogers’ “diffusion of innovations” theory(1962), which differentiates five categories of productadopters, as outlined in table 3 (see below).
During our PACS project, a mixture of these personal-ity types was found. Early adopters included radiolo-gists, technicians and the informatics team. These per-
sons were treated preferentially with regards to hard-ware and software upgrades, training and support. Themajority of the employees adapted to PACS sooner orlater, including most physicians, secretaries, nurses andthe administration. This group had standard equip-ment, training and support.
Finally, there was a small group of traditionalists andresistors who complained about details such as spellingerrors in the web viewer entry page. A negligible num-ber of persons spread unfounded rumours about thelack of legal basis for running a PACS or regarding thereliability and technical quality of the PACS manufac-turer. The comments of traditionalists and resistorswere disregarded.
PACS Review: Four Years LaterApproximately four years after the installation of PACS,our hospital was filmless. Retrieval times were withinrequirements after the replacement of the DVD jukeboxby a hard disk RAID. A number of teleradiology proj-ects had been started. On the other hand, hardwarecosts increased more than anticipated, due to increasingrequirements for processor and RAM for the web view-er used by clinicians. On the human side, PACS waswidely accepted within the hospital. The majority ofexternal referring physicians, however, still requiredfilm, preventing complete replacement of hardcopies.
ConclusionA PACS project is a change management projectwith an important people side. There are manyobstacles which can be overcome with persistence,good project management, fast and competent sup-port as well as permanent communication. Majorproblems must be solved. Details, however, oftenhave to wait, especially when only important to tra-ditionalists and resistors. ����
Table 2. Four typical reactions to major change
Change Agents Respond actively to change, see it as an opportunity for development of their personality rather than a time-consuming problem.
Bystanders In principal agree with the necessity of change, but demonstrate a lack of initiative
Traditionalists See no need to change, are comfortable with the present, focus on security and react passively
Resistors Fear high losses, use power politics, focus on their position
Innovators Venturesome, educated, multiple info sources, greater propensity to take risk
Early adopters Social leaders, popular, educated Early majority Deliberate, many informal social contactsLate majority Skeptical, traditional, lower socio-
economic statusLaggards Neighbours and friends are main info
sources, fear of debt
Table 3. Five Categories of Product Adopters
Cover Story Change Management
IMAGING MANAGEMENT: THE OFF IC IAL VOICE OF THE EUROPEAN IMAGING INIT IAT IVE 21

Corporate Presentation
IntroductionOpened in 1959, Hachiya OrthopaedicHospital is committed to providing superi-or medical care. In keeping with this com-mitment, we digitalised our ordering sys-tem in 1996, completed image digitalisa-tion in 1998, and added a urology depart-ment in 2004 to maintain a continuouslyhigh level of medical service. Our hospitalis a 52-bed acute care hospital that con-ducts over 550 operations per year, includ-ing leading-edge treatments such as mini-mally invasive artificial joint surgery andendoscopic surgery.
Metal implants, plates and screws are com-monly employed during orthopaedic sur-gery. These frequently cause problems withmetal artifacts during CT or MRI examina-tions of bone union and in post-surgical fol-
Clinical ImagesClinical Image 1: Post-surgicalimages of bilateral total hip replacement The left joint was replaced in a 73-year-oldfemale patient 11 years after bilateral totalhip replacement surgery, due to looseness ofthe stem.
The bilateral hip replacement post-surgicalCT image in Fig.1 b) includes significantartifacts due to the implant between theacetabulum and trochanter.
The shift-and-add method image in Fig.1c) exhibits no effects of artifacts, whereasthe FBP image in Fig.1 d) exhibits artifactsin the tube-shift direction and at theboundary of the implant.
Clinical Image 2: Fracture after kneereplacement A 59-year-old female who had undergoneknee replacement surgery due toosteoarthritis of the knee suffered a fractureof the lateral tibial plateau due to a fall. TheCT image in Fig.2 b) exhibits effects of theimplant artifacts to the lateral side of thetibia. However, these effects do not extend tothe lateral side in the shift and add methodimage or the FBP image (Fig.2 c, 2 d).
Clinical Image 3: Follow-up of ante-rior fusion of cervical vertebraeAfter surgery for a cervical hernia on a 39-year-old male, anterior fusion was con-ducted from the 3rd to the 6th cervicalvertebrae, as shown in Fig.3. Periodic fol-low-up observations were requiredbecause of delays in bone union at thebone graft periphery on the 5th and 6thcervical vertebrae. Tomosynthesis wasused, due to its lower X-ray dose than CTexaminations.
low-up observations. This is a report on theuse of tomosynthesis to restrict metal arti-facts in images.
Current Tomosynthesis StatusSince introducing a flat-panel detector(FPD) in August 2005, we have conductedtomosynthesis examinations on 35 artificialjoint cases (20 hip, 10 knee, 5 elbow), 8spondylodesis cases, 3 arthrodesis cases, and4 osteosynthesis cases.
Evaluation of Clinical ImagesTomosynthesis images created by the shift-and-add and filtered back projection (FBP)method were compared to CT imagesusing the Shimadzu Sonialvision SafireR/F system with TomosynthesisWorkstation option and the Company A6-slice CT.
CHANGING THE WORLDOF X-RAY IMAGING
Outstanding Qualities of the World’s First Direct-Conversion R/F-FPD SHIMADZU FPD
: Shimadzu Advanced Flat Imaging REceptor
DIGI TAL ANGIO
Fig. 1
a) X-P b) CT image c) Shift-add method image d) FBP image
The Effective Use of Tomosynthesis in Orthopaedic Surgery: Follow-up after Procedures using MetalAuthor: Dr. Hiroyasu Yano, Hachiya Orthopaedic Hospital
Examining these topics and efficientlyapplying digital image technologies totake even better images in the futureshould make tomosynthesis an effectivemeans of post-operative follow-up. ❍
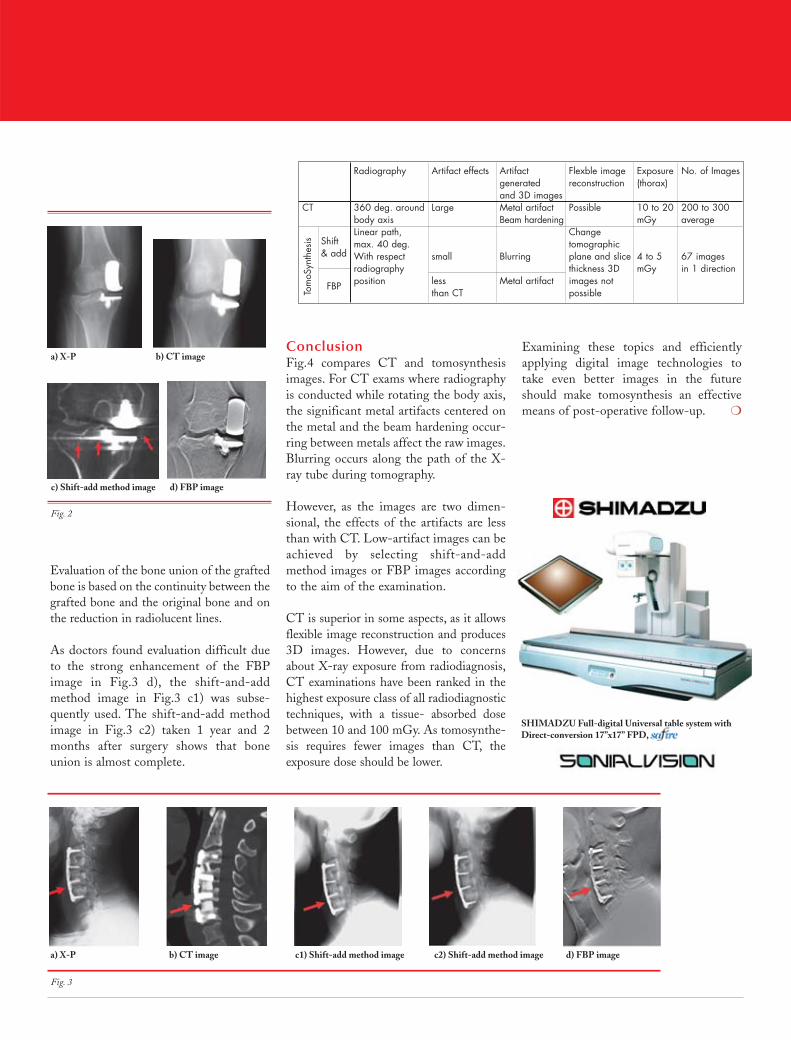
ConclusionFig.4 compares CT and tomosynthesisimages. For CT exams where radiographyis conducted while rotating the body axis,the significant metal artifacts centered onthe metal and the beam hardening occur-ring between metals affect the raw images.Blurring occurs along the path of the X-ray tube during tomography.
However, as the images are two dimen-sional, the effects of the artifacts are lessthan with CT. Low-artifact images can beachieved by selecting shift-and-addmethod images or FBP images accordingto the aim of the examination.
CT is superior in some aspects, as it allowsflexible image reconstruction and produces3D images. However, due to concernsabout X-ray exposure from radiodiagnosis,CT examinations have been ranked in thehighest exposure class of all radiodiagnostictechniques, with a tissue- absorbed dosebetween 10 and 100 mGy. As tomosynthe-sis requires fewer images than CT, theexposure dose should be lower.
Evaluation of the bone union of the graftedbone is based on the continuity between thegrafted bone and the original bone and onthe reduction in radiolucent lines.
As doctors found evaluation difficult dueto the strong enhancement of the FBPimage in Fig.3 d), the shift-and-addmethod image in Fig.3 c1) was subse-quently used. The shift-and-add methodimage in Fig.3 c2) taken 1 year and 2months after surgery shows that boneunion is almost complete.
Fig. 2
Fig. 3
a) X-P b) CT image c1) Shift-add method image c2) Shift-add method image d) FBP image
a) X-P
SHIMADZU Full-digital Universal table system withDirect-conversion 17”x17” FPD,
b) CT image
c) Shift-add method image d) FBP image
Radiography Artifact effects Artifact Flexble image Exposure No. of Imagesgenerated reconstruction (thorax)and 3D images
CT 360 deg. around Large Metal artifact Possible 10 to 20 200 to 300body axis Beam hardening mGy averageLinear path, Change max. 40 deg. tomographicWith respect small Blurring plane and slice 4 to 5 67 imagesradiography thickness 3D mGy in 1 directionposition less Metal artifact images not
than CT possibleTom
oSyn
thes
is Shift & add
FBP
24 PROMOTING TEAMWORK ACROSS DIFFERENT DISC IPL INES
In the US in the 1970s, both federal and state govern-ments enacted various regulations and laws resulting ina shift from expansion to cost control. This altered theincentive for lengthy inpatient admissions and createda decline in demand for inpatient services. Also, thechanging environment in healthcare delivery and reim-bursement in the late 1980s and ‘90s sparked a majoroverhaul in the organisational structure of healthcareinstitutions, emphasising primary care physicians overspecialists and introducing price competition into themarketplace. Factors that influenced this change were:• Medicare moved from a cost-based to prospective,
fixed-price payment system;• Technological advances enabled more treatment to
be provided in a lower-cost outpatient setting;• Increases in managed care and selective contract-
ing restrained reimbursement rates, enabling close monitoring of service necessity.
Academic Medical Centres Adapt toMarket DemandsAcademic medical centres faced enormous challengesin this new economic environment. Due to the highcost of the service delivered by them, referrals to aca-demic medical centres from community physiciansand hospitals began to decline. As volumes dropped, sodid clinical revenues. As the clinical subsidies that sup-ported teaching and research missions declined, thefinancial structure that supported the whole academicmedical system was threatened. Moreover, academicmedical centres also faced reductions in Medicarespending in the mid-to-late 1990s.
The academic medical community investigated a num-ber of strategies to overcome the challenges it faced. In
this regard, Harrison et al reported three alternatives:1. “Do it alone” by creating a self-contained integrateddelivery system;2. Consolidate by forming networks or mergers;3. Separate the college of medicine from the teachinghospital by selling the hospital to a for-profit company.
Perhaps the most hyped merger strategy was consolida-tion of highly specialised, high-cost programmes andequipment to result in significant savings, enhancedbargaining power to further reduce costs and the pool-ing of the patient base and increased referrals or mar-ket share to support operations.
Three Elements for Success Three key elements play a critical role in achieving suc-cessful merger of health institutions: the consensus of fun-damental goals and direction of merger by key leaders,agreement of governance structure and cultural resolution.
The first element crystallises the need for senioradministrators from both institutions to reach consen-sus on the goals and pathways needed to achieve aviable merger. Both strategic direction and day-to-dayoperations of large organisations like hospitals dependon the skills, visions and team abilities of senior execu-tives. Thus, once corporate-level issues are resolved,departmental leaders can act as liaisons in these discus-sions to facilitate communication between institution-al leaders and clinical departments.
A second element is governance structure. The partiesinvolved need to agree on the level of involvement orautonomy between them. The purpose of a centralgovernance body of a nonprofit organisation is to pro-
AUTHORS
Sukru Mehmet ErturkHansel OteroIleana E. GillEric NathansonPablo R. Ros (above)Silvia Ondategui-Parra
Radiology ManagementGroupDepartment of Radiology & Department of HospitalAdministrationBrigham and Women’sHospital/Harvard MedicalSchoolBoston, MA, [email protected]
Consolidation Leads to Increased Competitiveness
ACADEMIC MEDICAL CENTRES & MERGERS
Concerns over rising healthcare costs have motivated hospitalsto seek ways to increase efficiency, decrease costs and improvequality. Hospitals have recognised that consolidation mightaccomplish these goals.Academic medical centres are especiallyvulnerable to a changing economic environment, as their teach-ing and research responsibilities increase the cost of their servicesand many found that re-organisation and consolidation put themin a more competitive position.This article examines the back-ground, causes, benefits, and pitfalls of hospital mergers.We alsoanalyse related managerial and organisational challenges.
Cover Story Change Management
Cover Story Change Management
vide strategic guidance and support but requires con-stant and proactive communication. In mergers wherecommunication is a priority, more thorough and time-ly consolidation between departments is achieved.
A third key element to mergers is cultural resolution.Institutional leaders need to reach a consensus regard-ing cultural merger between two entities. Will theyfacilitate merger between two institutions by creating anew culture, where the perceptions of “us” versus“them” are minimised or will they retain former cultur-al practices? When entities retain an “us” versus “them”mentality, a destructive tendency against successfulmerger between the two departments emerges.
Radiology Departments and MergersThere are several advantages for radiology departmentsto merge early during the process. Firstly, radiology is aprocedure-based specialty and largely patient inde-pendent and therefore may have less departmentalidiosyncrasies. Secondly, there are a sizeable number ofradiological exams that are location independent, dueto ease of electronic imaging relay systems. In addition,there is considerable investment in the property andequipment of radiology, making it extremely capital
and space intensive, enabling departments to enjoy thebenefits of economic scale. Finally, the level ofadvanced technology also has a significant impact onthe clinical and educational components of academicmedical centres.
Partners HealthCare System, Inc.Brigham and Women’s Hospital and Massachussett’sGeneral Hospital were among the first academic med-ical centres to merge in the US. Both are teaching hos-pitals of Harvard Medical School and were interested inestablishing a holding company while preserving theirnames and identities. A neutral name was selected forthe new organisation: Partners HealthCare System, Inc.,(PHS). The ultimate power to decide policy for the cor-poration was given to Partners’ Board of Trustees.Accomplishments of the new corporation include:• The formation of Partners Community Healthcare
Inc., (PCHI), a subsidiary corporation that estab-lished a network of over 1,000 primary care physi-cians to serve practices and conduct negotiations with insurers;
• Partners and Dana Farber Cancer Institute to form Partners/Dana Farber Cancer Care for joint clinical,research, and educational programmes in oncology;
“Consolidation of servicesin another location mayresult in loss of a signifi-cant percentage ofpatients needed to sup-port the operation”
• Partners’ joint continuing medical education programmes and research projects;
• Merging of half of the residency programmes and one-third of the fellowship programmes into singletraining programmes across both institutions. Executives of Partners are housed in Boston, MA, midway between both hospitals, and manage a consolidated administrative structure that includesfinance, budgeting, information systems, invest-ments, legal issues, marketing, etc.
Avoiding Staff & Patient LossElements that typically lead to the failure of a mergerinclude:• Allowing anxiety of downsizing or demotion to
permeate throughout both hospitals and depart-ments leading to staff departures;
• Retaining separate financial records, information systems, billing systems, and marketing services;
• Merging with an entity geographically far from your institution.
An overwhelming number of mergers do result in lay-offs of both managers and rank-and-file staff, so manyemployees have good cause to feel uneasy in times ofchange. To many employees, an impending mergerspells an uncertain situation with implicit risks. Even ifthe merger does not eliminate their positions, it willchange the way they perform their jobs. A simplememo indicating the will of the leadership to accom-plish the merger with as little impact on employmentas possible can be helpful.
Particularly for patient referral, the location of an insti-tution is often a critical factor. Consequently, the con-solidation of services in another location may result inloss of a significant percentage of patients than wereanticipated, to support the operation. ����
Cover Story Change Management


Here are some examples of the regulations for PACSusage that were challenged at the Mainz meeting:• PACS is the most critical application of an enter-
prise. The up-time must be more than 99.9% with a 24h/365d service.
• All aspects of storage, data security and availability of PACS images must be increased 100 times, if possible 1,000 times above film-based radiology.
• All images must be archived even if they are only for temporary use without clinical relevance.
• A PACS system is mandatory to store all thin slices if a Multi Detector CT (MDCT) is operated.
• Film-based use of MDCT is not allowed. • No image may be lossy compressed, even if the
difference between original and compressed image is less than the difference in quantum noise between two sequential exposures.
• Storage has to be done locally, with high security Storage Area Network systems (SAN) and Network Attached Storage (NAS). External archiving by Application Service Providers (ASP) is not an option.
Is PACS a Critical Application?At the Mainz meeting, radiologists were asked “Do youclassify PACS as a critical application?” Two answeredwith “yes”, eight with “no”. PACS vendors were asked“Do you provide a 24h/365d service in Germany?”One vendor provides this service in 5% of cases, allothers in 0% of the installed base.
In our 2,500 bed hospital, the consensus of theChairmen of thirty clinical departments was thatPACS is not the most critical application. All agreedthat the availability of HIS, network and laboratory
data are critical, requiring a 24h/365d service. ForPACS, we provide several fallback and security mecha-nisms. Most new radiological modalities are preparedto store image data from three to fourteen days. Thistime should be sufficient to fix any PACS problems.Paper or film-based printing is available in most hospi-tals. A quick film reading of emergency cases can beperformed at the primary or secondary modality con-sole. In our PACS system the web-server for all clinicaldepartments can be accessed directly by all modalities.During the last six years, these methods have beenmore than sufficient.
On a typical 8 AM to 6 PM day with high PACSworkload, any problems can be fixed within hours bythe PACS vendor or IT department. Saturday,Sunday, on holidays and at night-time, the PACSworkload is low and radiologists on duty can use pre-scribed fallback mechanisms. Critical applications interms of patient safety are CT, radiography, ultra-sound and in some environments, angiography. Noservice contract guarantees the 100% uptime of a CTscanner, hence these critical modalities must be dou-bly available.
Are Safety Requirements too High?It is often argued that PACS downtime may not exceed0.1%. Solutions are often high-level expensive SANsystems with fast image access. Long-term archiving isperformed with tape or optical robot systems or hierar-chical storage management systems (HSM). Retrievalof these older images often takes up to a half hourdepending on the daily workload, speed of the archivesystem and the quality of the prefetching and autorout-ing implementation.
AUTHOR
Prof. Reinhard R.W.LooseChairmanInstitute for Diagnostic andInterventional RadiologyHospital Nuremberg-NorthNuremberg, [email protected]
PACS systems offer many proven benefits compared to film-based services in clinical environments. However, have we setthe benchmarks for its implementation and regulation toohigh? This question was discussed with PACS experts at theHIS/RIS/PACS/DICOM meeting June 6 – 7, 2007 in Mainz,Germany (http://www.unimainz.de/FB/Medizin/Radiologie/agit/Welcome.html).This article follows up by presenting thecase for a relaxation of certain significant rules for PACS usage.
Results from Mainz Meeting Indicate a Need for Change
ARE TECHNICAL AND LEGAL
STANDARDS FOR PACS TOO HIGH?
28 PROMOTING TEAMWORK ACROSS DIFFERENT DISC IPL INES
Features
FAX
BA
CK
TO
+3
2 2
28
6 8
50
8Subscr ip t ion Formfor Imaging Management
Title & First Name:
Surname:
Job title:
Institution:
Address:
Postcode & City:
Country:
Telephone:
Email:
Medical Doctors (respond below)1. What is your occupation? (check only one)
❏ Diagnostic Radiologist❏ Other Physician (please specify)
1a. What is your radiology sub-specialty? (check only one)❏ General Radiology❏ Neuroradiology❏ Nuclear Medicine❏Vascular & Interventional❏ Nuclear Radiology❏ Cardiovascular Diseases❏ Paediatric Radiology❏ Other (please specify)
1b. I am Chief of my Department❏Yes❏ No
Non-physic ian profess ionals (respond below)1c. What is your occupation? (check only one)
Administrator/Manager:❏ Radiology Administrator❏ Radiology Business Manager❏ PACS Administrator
Executive❏ Chief Information Officer / IT Manager❏ Chairman / Managing Director / Executive Director❏ Chief Financial Officer / other executive titles
Other❏ Medical Physicist❏ Academic❏ Chief Technologist / Senior Radiographer❏ Manufacturer❏ Business Consultant❏ Distributor / Dealer
All respondents reply to the questions below2. In what type of facility do you work? (check only one)
❏ Private clinic❏ Hospital (check number of beds)❏ More than 500 beds❏ 400-499 beds❏ 300-399 beds
3. With what technologies or disciplines do you work? (check all that apply)❏ Diagnostic X-ray❏ Nuclear Imaging❏ Interventional Radiology❏ CT❏ Ultrasound❏ MRI❏ Mammography❏ Bone Densitometry❏ PACS/Teleradiology❏ Cardiac Imaging❏ PET❏ Echography❏ Angio/Fluoroscopy
Subscription Rates (6 Issues / Year)One year ❏ Europe 85 Euros ❏ Overseas 105 EurosTwo years ❏ Europe 150 Euros ❏ Overseas 180 Euros
How to Subscribe?• Send an email with name and address to [email protected];• Complete this form and post it to 28, rue de la Loi - B-1040 Brussels - Belgium;• Complete this form and fax it to +32 2 286 8508.

and lossy compression is not used at all. There arevarious legal reasons for this. In Germany the“Röntgenverordnung” allows a compression (loss-less or lossy) “as long as there is no loss of diagnos-tic quality”. The responsible radiologist has todecide what is diagnostic or not. Hence PACS ven-dors provide lossy DICOM JPEG2000/Waveletcompressions but PACS users need a common con-sensus which lossy compression rates are safe andacceptable.
At the Hospital Nuremberg we compress all imagesafter “no touch” for six months with intelligent PACSrules depending on modality and type of study withcompression rates between 1:2.5 and 1:10. With thisdelay all film readings and clinical conferences are per-formed with original images as well as external long-term archiving close to exam time. This compressionreduces online storage volume by a factor of eight,compared to uncompressed data, or 3.2 compared tolossless compression.
At the Mainz meeting radiologists were asked “If thereis a consensus of radiologists on safe lossy compressionfactors, would you use lossy compression?” Tenanswered yes, one said no and I was the only one actu-ally using lossy compression.
External Archiving by ApplicationService ProvidersAt our hospital, the concept to store everythingonline (EOL) between five to six years had a stronginfluence on the decision for long-term archiving.This reduces the slow offline archive from a “workingarchive” to a “depository under legal aspects” whereimages must be retrievable in “appropriate time”(legal regulation in Germany “Röntgenverordnung” <24 hours). Hence, we decided to cooperate with anexternal ASP. The upload is not time-critical and thedownload of < 1% requires no high speed WAN con-nections. Of course the decision for ASP modelsdepends on legal regulations which vary from countryto country.
At the Mainz meeting radiologists were asked “Wouldyou use ASP for long-term storage?” Ten answered yes.I was again the only individual present using ASP stor-age. Clearly the results of the Mainz meeting indicatethat is time to think and act differently in future whenplanning or expanding a PACS system. ����
The future is clearly fast online storage and accesspreferably for four to six years. This reduces access toimages in the long-term archive far below 1%. At theHospital Nuremberg we provide fast online storagewith a less expensive solution over six years based onstandard IDE and SATA RAID systems. This storage isinstalled in two independent server rooms with anautomatic switchover of the IP address if one systemfails. All images over six years are accessible in 1 - 2 sec-onds. The need for retrieval of images older than sixyears is nearly zero.
Should we Archive all Images?The answer is clearly no. The preferable system is asfollows:• Thick slices are sent to PACS by the modality;
multiple thin slices go to a workstation. Here theyare used for post-processing in a first-in, first-out (FIFO) buffer and are deleted after several days or weeks. If archiving of thin slices is necessary, stor-age in the PACS has to be done manually. This solution involves time-consuming interaction between technicians and physicians.
• New MDCT scanners provide scan protocols that include the reconstruction of angulated images without displaying the thin slices. Hence, thick slices go to PACS or workstations only if flagged by the scan protocol.
• These algorithms could be included in PACS rules, for example “if thin slice datasets (e.g. >200 slices, <1 mm slice thickness) were used for recon-struction of diagnostic datasets that are also storedin the same study, there was no access to this study for >6 month and no “don’t delete” flag exists, images can be deleted automatically”. This procedure keeps the online archive fast and small but does not exclude archiving of all images in thelong-term archive that is normally done close to the exam date.
When asked “Do you want thin CT-slices to bearchived if they are only used for reconstruction ofdiagnostic thick slices?”, only one radiologist at theMainz meeting answered yes, eight answered no, andthere was one abstention.
Why are we Afraid of Lossy Image Compression?Lossless compression which reduces the amount ofdata by a factor of about 2.5 is not generally used
30 PROMOTING TEAMWORK ACROSS DIFFERENT DISC IPL INES
Features
Appropriate integration technologies require correla-tive IT infrastructure as well as communication andinterface standards, such as DICOM, to allow datainterchange between surgical system components inthe OR. Such an infrastructure system, called a“Therapy Imaging and Model Management System”(TIMMS) supports the essential functions that enableand advance images. A TIMMS provides the infra-structure necessary for surgical/interventional work-flow management in the Digital Operating Room(DOR). The design of a TIMMS should be based on asuitable DICOM extension for data, image, informa-tion, model and tool communication in order to clari-fy the position of interfaces and relevant standards forSAS and their specific components.
Therapy Imaging and ModelManagement System and its InterfacesThe DICOM standard comes closest to providing thebasis for the design of TIMMS interfaces. DICOMstandardisation aims at providing support to fulfildesign criteria derived from software engineering prin-ciples when realising ICT systems for medical activities.
Engineering of ICT systems for the assistance of surgi-cal interventional activities implies the specification,design, implementation and testing of ComputerAssisted Surgery (CAS) or IGT systems. A number ofcomponents for such systems have been developed inacademic and industrial settings and are applied in var-ious surgical disciplines. In most cases, however, theyare standalone systems with specific ad hoc propriety
or vendor interfaces.They can be consideredas islands of IT enginesand repositories withvarying degrees of modu-larisation and intercon-nection.
Such a system needs to bedesigned to provide ahighly modular structure.Modules may be defined
on different granulation levels. A first list of compo-nents (e.g. high and low level modules) comprisingengines and repositories of an SAS, which should beintegrated by a TIMMS, is currently being compiledwithin the DICOM WG 24 “DICOM in Surgery”.
Fig. 1 (page 32), demonstrates a high-level genericmodular structure for an SAS. High-level modules areabstracted from many specific CAS/IGT systems thathave been developed in recent years. In general, a com-bination of these can be found in most R&D andcommercial SAS systems. The “Kernel for workflow,knowledge and decision management” in Fig. 1 pro-vides the strategic intelligence for preoperative plan-ning and intraoperative execution. Often this mod-ule or parts thereof is integrated into other engines,as required.
Steps Towards DICOM in SurgeryMedical imaging and communication standards arewell defined by DICOM and are an integral part ofTIMMS. Most of the Image and PresentationStates (IOD), defined in DICOM, etc. are also rel-evant to surgery.
However, models and associated management havenot been considered in DICOM intensively, exceptthrough some work done in DICOM WG 07, WG17 and WG 22. Modelling and simulation in sur-gery however, are key functions for SAS pre- andintra-operatively. The interfacing of tools support-ing these functions represents a new scope forDICOM.
Features
AUTHOR
Prof. Heinz U. LemkeChairmanDICOM Working Group 24 DICOM in [email protected]
A recent report predicted the rise in demand for surgicalservices to be up to 47% by 2020. Difficulties that are alreadyapparent in the Operating Room (OR), such as the lack ofseamless integration of Surgical Assist Systems (SAS) intoworkflow, will be amplified in the near future.There are manySAS in development or employed in the OR, though their rou-tine use is impeded by the absence of appropriate integrationtechnology and standards.This article explores efforts todevelop strategies for improving surgical and interventionalworkflow assisted by surgical systems and technologies.
Coping with Rise in Demand for Surgical Services
THE ROLE OF DICOMIN THERAPY
IMAGING MANAGEMENT: THE OFF IC IAL VOICE OF THE EUROPEAN IMAGING INIT IAT IVE 31
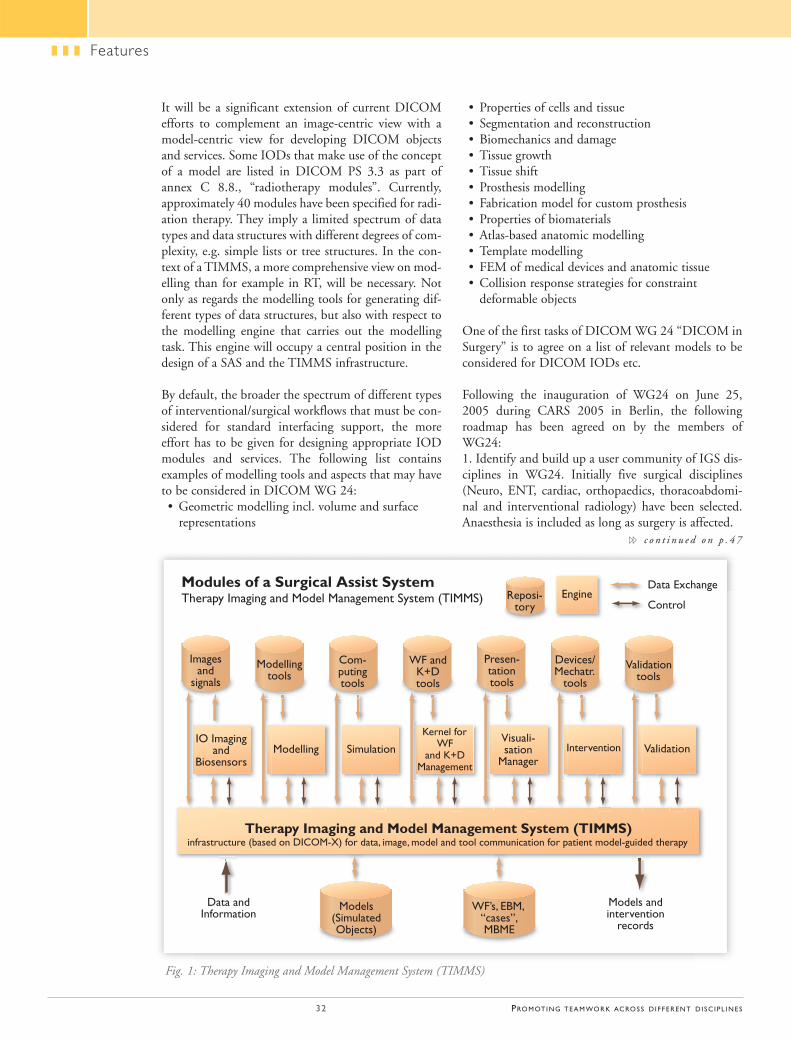
Reposi-tory
EngineData Exchange
Control
Validation tools
Devices/Mechatr.
tools
Presen-tationtools
WF andK+Dtools
Com-putingtools
Modellingtools
Images and
signals
IO Imaging and
Biosensors
Data and Information
WF’s, EBM,“cases”,MBME
Models(Simulated Objects)
Models and intervention
records
Modelling Simulation
Kernel forWF
and K+DManagement
Visuali-sation
ManagerIntervention Validation
Therapy Imaging and Model Management System (TIMMS)infrastructure (based on DICOM-X) for data, image, model and tool communication for patient model-guided therapy
Modules of a Surgical Assist SystemTherapy Imaging and Model Management System (TIMMS)
32 PROMOTING TEAMWORK ACROSS DIFFERENT DISC IPL INES
It will be a significant extension of current DICOMefforts to complement an image-centric view with amodel-centric view for developing DICOM objectsand services. Some IODs that make use of the conceptof a model are listed in DICOM PS 3.3 as part ofannex C 8.8., “radiotherapy modules”. Currently,approximately 40 modules have been specified for radi-ation therapy. They imply a limited spectrum of datatypes and data structures with different degrees of com-plexity, e.g. simple lists or tree structures. In the con-text of a TIMMS, a more comprehensive view on mod-elling than for example in RT, will be necessary. Notonly as regards the modelling tools for generating dif-ferent types of data structures, but also with respect tothe modelling engine that carries out the modellingtask. This engine will occupy a central position in thedesign of a SAS and the TIMMS infrastructure.
By default, the broader the spectrum of different typesof interventional/surgical workflows that must be con-sidered for standard interfacing support, the moreeffort has to be given for designing appropriate IODmodules and services. The following list containsexamples of modelling tools and aspects that may haveto be considered in DICOM WG 24:• Geometric modelling incl. volume and surface
representations
• Properties of cells and tissue• Segmentation and reconstruction• Biomechanics and damage• Tissue growth• Tissue shift• Prosthesis modelling• Fabrication model for custom prosthesis• Properties of biomaterials• Atlas-based anatomic modelling• Template modelling• FEM of medical devices and anatomic tissue• Collision response strategies for constraint
deformable objects
One of the first tasks of DICOM WG 24 “DICOM inSurgery” is to agree on a list of relevant models to beconsidered for DICOM IODs etc.
Following the inauguration of WG24 on June 25,2005 during CARS 2005 in Berlin, the followingroadmap has been agreed on by the members ofWG24:1. Identify and build up a user community of IGS dis-ciplines in WG24. Initially five surgical disciplines(Neuro, ENT, cardiac, orthopaedics, thoracoabdomi-nal and interventional radiology) have been selected.Anaesthesia is included as long as surgery is affected.
Features
Fig. 1: Therapy Imaging and Model Management System (TIMMS)
�� c o n t i n u e d o n p . 4 7
IMAGING MANAGEMENT: THE OFF IC IAL VOICE OF THE EUROPEAN IMAGING INIT IAT IVE 33
Features
Flat Panel TechnologyFor many years, image intensifiers mounted on a C-arm have provided useful service and this technologycan be considered mature. However, image intensifiersare not only bulky but are also susceptible to image dis-tortion and have limited dynamic range. Flat paneldetectors offer a number of advantages.
Electronic flat panel detectors were first developed toprovide digital radiography without the need to trans-port image cassettes between the patient and the imageplate reader, as is necessary with computed radiogra-phy. Cutting out the transport step means that imagesare available within about ten seconds of an exposure,so efficiency is greatly improved. The next develop-ment was to modify the radiographic detectors for flu-oroscopic use. To achieve this modification two signif-icant differences needed to be addressed: fluoroscopyuses much lower x-ray dose rates and image read timesof up to 60 frames per second are necessary.
Adoption of Flat Panel TechnologyThe first commercial flat panel detector was intro-duced in the late 1990’s by Marconi (previously knownas Picker, now part of Philips) as an add-on to theMx8000 CT system. The FACTS (Fluoro-AssistComputed Tomography) was designed to help CT-guided interventional procedures by allowing greateraccess to the patient than is possible with CT.However, the concept never gained wide clinicalacceptance. In 2000, GE Healthcare introduced a car-diology interventional system, the Innova 2000. Thiswas truly the first fluoroscopy flat panel to gain wide-spread acceptance for an interventional application.Cardiology was chosen first since a relatively small
detector is sufficient. Cardiologistsquickly recognised the advantagesof the flat panel, for example, thelack of distortion and even imagequality. What is more, the flat pan-els are physically smaller, so theyare less obtrusive. So, despite thehigher cost (about $200,000 ormore), flat panel-based cardiologysystems quickly replaced imageintensifier based systems.Technical issues, in particular thedetector size issue and the highercost, meant that general radiologyinterventional systems were not yet
available. However, as the detectors improved it wasinevitable that image intensifier based interventionalradiology would become obsolete.
Reduced Radiation DoseAt the same time the greater computer power becom-ing widely available enabled manufacturers to improvecapabilities. Some developments were made that signif-icantly reduced radiation exposure. For example, lastimage hold, virtual collimators, and fluoroscopy stor-age all help reduce the amount of fluoroscopy timeand, therefore, the radiation dose.
Image Processing Presents More InformationAll fluoroscopy images are two-dimensional. Anatomy,however, is three-dimensional. In applications in whichmore 3D information is essential, the traditionalapproach was to use a biplane system. The resultingtwo orthogonal views help neuroradiologists and pae-diatric cardiologists gain an accurate understanding ofvasculature. The other solution is to use CT. CT fluo-roscopy is widely used, particularly for biopsies.However, the limited coverage (present day CT sys-tems have a maximum of 4 cm), the high doses to theoperator, and the limited access to the patient, meanthat CT fluoroscopy is limited. Also, judging by thevery limited adoption of the FACTS system mentionedabove, neither is a combined CT and fluoroscopy sys-tem a practical solution.
3D AngiographyHowever, this increased computer power enabled thedevelopment of rotational angiography. The idea is
Interventional radiology (IR) refers to a wide range of minimally invasive procedures in which radiologyequipment is used to guide interventions, such asstenting, biopsy, embolisation, and ablation.Whileguidance can be achieved with various radiologicmodalities, including fluoroscopy, ultrasound, comput-ed tomography, and magnetic resonance, the terminterventional radiology usually refers to the use of x-ray fluoroscopy-based equipment. In recent years anumber of technological developments have increasedthe usefulness of IR.This article will review theimprovements in IR equipment and the possibilitiesfor the future.
Technology Drives Clinical Practice
FOCUS ON INTERVENTIONALRADIOLOGY EQUIPMENT
AUTHOR
Jason LaundersSenior Project OfficerECRI [email protected]
�� c o n t i n u e d o n p . 4 5
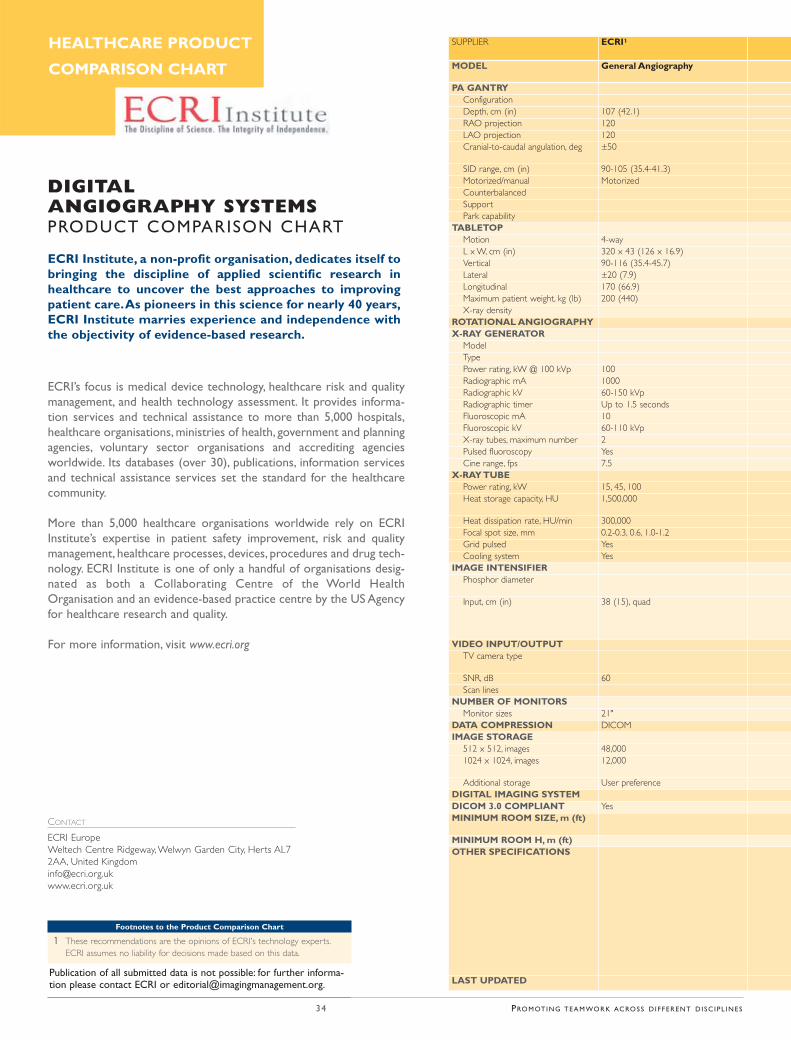
ECRI’s focus is medical device technology, healthcare risk and qualitymanagement, and health technology assessment. It provides informa-tion services and technical assistance to more than 5,000 hospitals,healthcare organisations, ministries of health, government and planningagencies, voluntary sector organisations and accrediting agenciesworldwide. Its databases (over 30), publications, information servicesand technical assistance services set the standard for the healthcarecommunity.
More than 5,000 healthcare organisations worldwide rely on ECRIInstitute’s expertise in patient safety improvement, risk and qualitymanagement, healthcare processes, devices, procedures and drug tech-nology. ECRI Institute is one of only a handful of organisations desig-nated as both a Collaborating Centre of the World HealthOrganisation and an evidence-based practice centre by the US Agencyfor healthcare research and quality.
For more information, visit www.ecri.org
Publication of all submitted data is not possible: for further informa-tion please contact ECRI or [email protected].
ECRI Institute, a non-profit organisation, dedicates itself tobringing the discipline of applied scientific research inhealthcare to uncover the best approaches to improvingpatient care.As pioneers in this science for nearly 40 years,ECRI Institute marries experience and independence withthe objectivity of evidence-based research.
DIGITAL ANGIOGRAPHY SYSTEMSPRODUCT COMPARISON CHART
Footnotes to the Product Comparison Chart
1 These recommendations are the opinions of ECRI's technology experts.ECRI assumes no liability for decisions made based on this data.
CONTACT
ECRI EuropeWeltech Centre Ridgeway, Welwyn Garden City, Herts AL72AA, United [email protected]
HEALTHCARE PRODUCT
COMPARISON CHART
SUPPLIER ECRI1
MODEL General Angiography
PA GANTRY ConfigurationDepth, cm (in) 107 (42.1) RAO projection 120LAO projection 120Cranial-to-caudal angulation, deg ±50
SID range, cm (in) 90-105 (35.4-41.3) Motorized/manual Motorized CounterbalancedSupportPark capability
TABLETOPMotion 4-way L x W, cm (in) 320 x 43 (126 x 16.9) Vertical 90-116 (35.4-45.7) Lateral ±20 (7.9) Longitudinal 170 (66.9) Maximum patient weight, kg (lb) 200 (440) X-ray density
ROTATIONAL ANGIOGRAPHY X-RAY GENERATOR
ModelType Power rating, kW @ 100 kVp 100Radiographic mA 1000Radiographic kV 60-150 kVpRadiographic timer Up to 1.5 seconds Fluoroscopic mA 10Fluoroscopic kV 60-110 kVp X-ray tubes, maximum number 2Pulsed fluoroscopy YesCine range, fps 7.5
X-RAY TUBE Power rating, kW 15, 45, 100 Heat storage capacity, HU 1,500,000
Heat dissipation rate, HU/min 300,000Focal spot size, mm 0.2-0.3, 0.6, 1.0-1.2 Grid pulsed YesCooling system Yes
IMAGE INTENSIFIER Phosphor diameter
Input, cm (in) 38 (15), quad
VIDEO INPUT/OUTPUTTV camera type
SNR, dB 60Scan lines
NUMBER OF MONITORS Monitor sizes 21"
DATA COMPRESSION DICOM IMAGE STORAGE
512 x 512, images 48,0001024 x 1024, images 12,000
Additional storage User preference DIGITAL IMAGING SYSTEM DICOM 3.0 COMPLIANT YesMINIMUM ROOM SIZE, m (ft)
MINIMUM ROOM H, m (ft) OTHER SPECIFICATIONS
LAST UPDATED
34 PROMOTING TEAMWORK ACROSS DIFFERENT DISC IPL INES
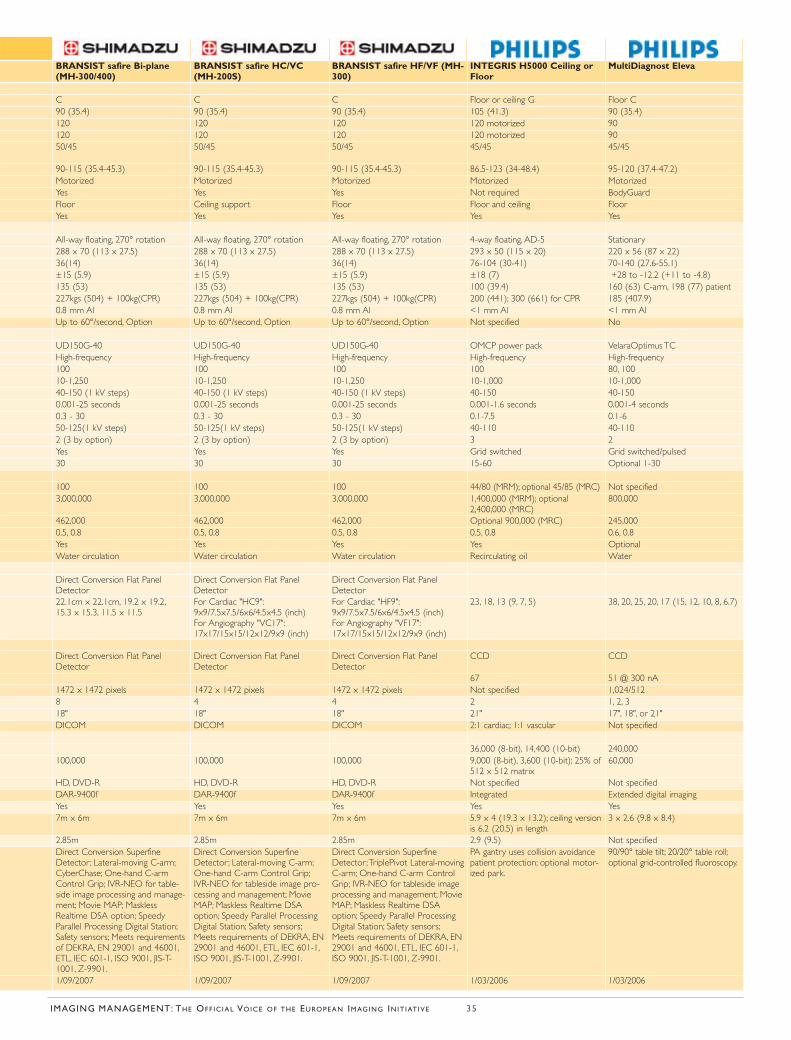
BRANSIST safire Bi-plane(MH-300/400)
BRANSIST safire HC/VC(MH-200S)
BRANSIST safire HF/VF (MH-300)
INTEGRIS H5000 Ceiling orFloor
MultiDiagnost Eleva
C C C Floor or ceiling G Floor C 90 (35.4) 90 (35.4) 90 (35.4) 105 (41.3) 90 (35.4) 120 120 120 120 motorized 90120 120 120 120 motorized 9050/45 50/45 50/45 45/45 45/45
90-115 (35.4-45.3) 90-115 (35.4-45.3) 90-115 (35.4-45.3) 86.5-123 (34-48.4) 95-120 (37.4-47.2) Motorized Motorized Motorized Motorized Motorized Yes Yes Yes Not required BodyGuard Floor Ceiling support Floor Floor and ceiling Floor Yes Yes Yes Yes Yes
All-way floating, 270° rotation All-way floating, 270° rotation All-way floating, 270° rotation 4-way floating, AD-5 Stationary 288 x 70 (113 x 27.5) 288 x 70 (113 x 27.5) 288 x 70 (113 x 27.5) 293 x 50 (115 x 20) 220 x 56 (87 x 22) 36(14) 36(14) 36(14) 76-104 (30-41) 70-140 (27.6-55.1) ±15 (5.9) ±15 (5.9) ±15 (5.9) ±18 (7) +28 to -12.2 (+11 to -4.8) 135 (53) 135 (53) 135 (53) 100 (39.4) 160 (63) C-arm, 198 (77) patient 227kgs (504) + 100kg(CPR) 227kgs (504) + 100kg(CPR) 227kgs (504) + 100kg(CPR) 200 (441); 300 (661) for CPR 185 (407.9) 0.8 mm Al 0.8 mm Al 0.8 mm Al <1 mm Al <1 mm Al Up to 60°/second, Option Up to 60°/second, Option Up to 60°/second, Option Not specified No
UD150G-40 UD150G-40 UD150G-40 OMCP power pack VelaraOptimus TC High-frequency High-frequency High-frequency High-frequency High-frequency100 100 100 100 80, 100 10-1,250 10-1,250 10-1,250 10-1,000 10-1,000 40-150 (1 kV steps) 40-150 (1 kV steps) 40-150 (1 kV steps) 40-150 40-150 0.001-25 seconds 0.001-25 seconds 0.001-25 seconds 0.001-1.6 seconds 0.001-4 seconds 0.3 - 30 0.3 - 30 0.3 - 30 0.1-7.5 0.1-6 50-125(1 kV steps) 50-125(1 kV steps) 50-125(1 kV steps) 40-110 40-110 2 (3 by option) 2 (3 by option) 2 (3 by option) 3 2Yes Yes Yes Grid switched Grid switched/pulsed 30 30 30 15-60 Optional 1-30
100 100 100 44/80 (MRM); optional 45/85 (MRC) Not specified 3,000,000 3,000,000 3,000,000 1,400,000 (MRM); optional
2,400,000 (MRC) 800,000
462,000 462,000 462,000 Optional 900,000 (MRC) 245,0000.5, 0.8 0.5, 0.8 0.5, 0.8 0.5, 0.8 0.6, 0.8 Yes Yes Yes Yes Optional Water circulation Water circulation Water circulation Recirculating oil Water
Direct Conversion Flat PanelDetector
Direct Conversion Flat PanelDetector
Direct Conversion Flat PanelDetector
22.1cm x 22.1cm, 19.2 x 19.2,15.3 x 15.3, 11.5 x 11.5
For Cardiac "HC9":9x9/7.5x7.5/6x6/4.5x4.5 (inch)For Angiography "VC17":17x17/15x15/12x12/9x9 (inch)
For Cardiac "HF9":9x9/7.5x7.5/6x6/4.5x4.5 (inch)For Angiography "VF17":17x17/15x15/12x12/9x9 (inch)
23, 18, 13 (9, 7, 5) 38, 20, 25, 20, 17 (15, 12, 10, 8, 6.7)
Direct Conversion Flat PanelDetector
Direct Conversion Flat PanelDetector
Direct Conversion Flat PanelDetector
CCD CCD
67 51 @ 300 nA 1472 x 1472 pixels 1472 x 1472 pixels 1472 x 1472 pixels Not specified 1,024/512 8 4 4 2 1, 2, 3 18" 18" 18" 21" 17", 18", or 21" DICOM DICOM DICOM 2:1 cardiac; 1:1 vascular Not specified
36,000 (8-bit), 14,400 (10-bit) 240,000100,000 100,000 100,000 9,000 (8-bit), 3,600 (10-bit); 25% of
512 x 512 matrix 60,000
HD, DVD-R HD, DVD-R HD, DVD-R Not specified Not specified DAR-9400f DAR-9400f DAR-9400f Integrated Extended digital imaging Yes Yes Yes Yes Yes 7m x 6m 7m x 6m 7m x 6m 5.9 x 4 (19.3 x 13.2); ceiling version
is 6.2 (20.5) in length 3 x 2.6 (9.8 x 8.4)
2.85m 2.85m 2.85m 2.9 (9.5) Not specified Direct Conversion SuperfineDetector; Lateral-moving C-arm;CyberChase; One-hand C-armControl Grip; IVR-NEO for table-side image processing and manage-ment; Movie MAP; MasklessRealtime DSA option; SpeedyParallel Processing Digital Station;Safety sensors; Meets requirementsof DEKRA, EN 29001 and 46001,ETL, IEC 601-1, ISO 9001, JIS-T-1001, Z-9901.
Direct Conversion SuperfineDetector; Lateral-moving C-arm;One-hand C-arm Control Grip;IVR-NEO for tableside image pro-cessing and management; MovieMAP; Maskless Realtime DSAoption; Speedy Parallel ProcessingDigital Station; Safety sensors;Meets requirements of DEKRA, EN29001 and 46001, ETL, IEC 601-1,ISO 9001, JIS-T-1001, Z-9901.
Direct Conversion SuperfineDetector;TriplePivot Lateral-movingC-arm; One-hand C-arm ControlGrip; IVR-NEO for tableside imageprocessing and management; MovieMAP; Maskless Realtime DSAoption; Speedy Parallel ProcessingDigital Station; Safety sensors;Meets requirements of DEKRA, EN29001 and 46001, ETL, IEC 601-1,ISO 9001, JIS-T-1001, Z-9901.
PA gantry uses collision avoidancepatient protection; optional motor-ized park.
90/90° table tilt; 20/20° table roll;optional grid-controlled fluoroscopy.
1/09/2007 1/09/2007 1/09/2007 1/03/2006 1/03/2006
IMAGING MANAGEMENT: THE OFF IC IAL VOICE OF THE EUROPEAN IMAGING INIT IAT IVE 35
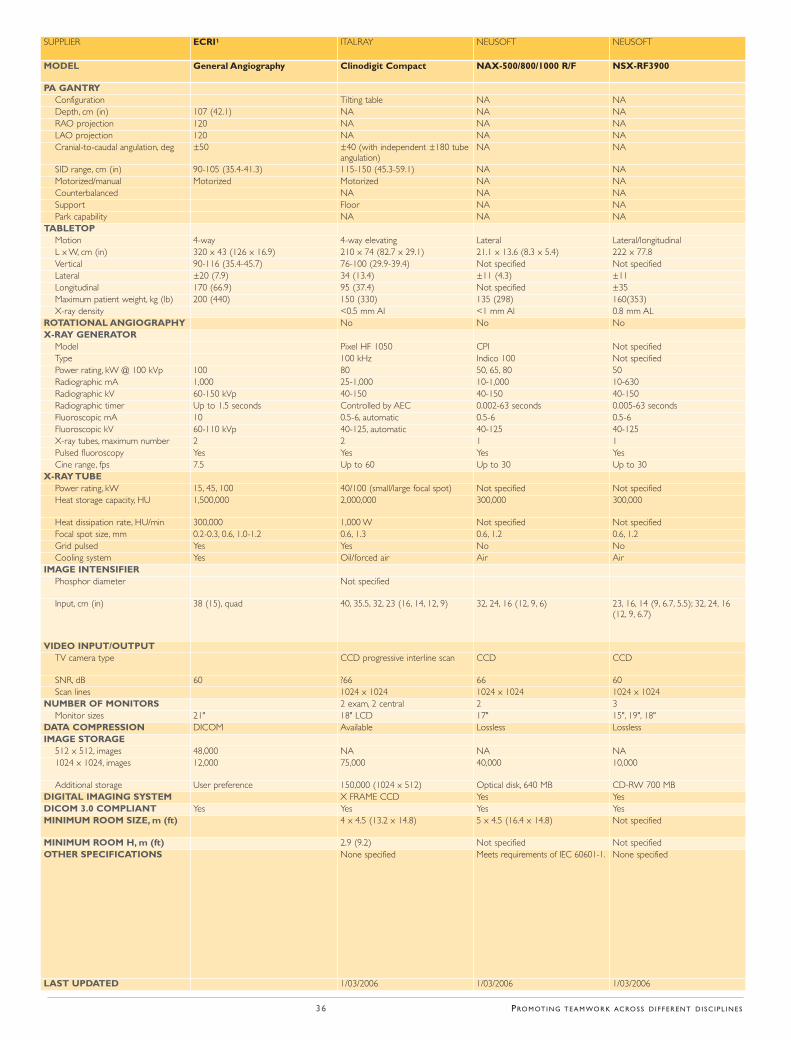
SUPPLIER ECRI1 ITALRAY NEUSOFT NEUSOFT
MODEL General Angiography Clinodigit Compact NAX-500/800/1000 R/F NSX-RF3900
PA GANTRY Configuration Tilting table NA NADepth, cm (in) 107 (42.1) NA NA NARAO projection 120 NA NA NALAO projection 120 NA NA NACranial-to-caudal angulation, deg ±50 ±40 (with independent ±180 tube
angulation) NA NA
SID range, cm (in) 90-105 (35.4-41.3) 115-150 (45.3-59.1) NA NAMotorized/manual Motorized Motorized NA NACounterbalanced NA NA NASupport Floor NA NAPark capability NA NA NA
TABLETOPMotion 4-way 4-way elevating Lateral Lateral/longitudinal L x W, cm (in) 320 x 43 (126 x 16.9) 210 x 74 (82.7 x 29.1) 21.1 x 13.6 (8.3 x 5.4) 222 x 77.8 Vertical 90-116 (35.4-45.7) 76-100 (29.9-39.4) Not specified Not specified Lateral ±20 (7.9) 34 (13.4) ±11 (4.3) ±11 Longitudinal 170 (66.9) 95 (37.4) Not specified ±35 Maximum patient weight, kg (lb) 200 (440) 150 (330) 135 (298) 160(353) X-ray density <0.5 mm Al <1 mm Al 0.8 mm AL
ROTATIONAL ANGIOGRAPHY No No No X-RAY GENERATOR
Model Pixel HF 1050 CPI Not specified Type 100 kHz Indico 100 Not specified Power rating, kW @ 100 kVp 100 80 50, 65, 80 50Radiographic mA 1,000 25-1,000 10-1,000 10-630 Radiographic kV 60-150 kVp 40-150 40-150 40-150 Radiographic timer Up to 1.5 seconds Controlled by AEC 0.002-63 seconds 0.005-63 seconds Fluoroscopic mA 10 0.5-6, automatic 0.5-6 0.5-6Fluoroscopic kV 60-110 kVp 40-125, automatic 40-125 40-125 X-ray tubes, maximum number 2 2 1 1Pulsed fluoroscopy Yes Yes Yes Yes Cine range, fps 7.5 Up to 60 Up to 30 Up to 30
X-RAY TUBE Power rating, kW 15, 45, 100 40/100 (small/large focal spot) Not specified Not specified Heat storage capacity, HU 1,500,000 2,000,000 300,000 300,000
Heat dissipation rate, HU/min 300,000 1,000 W Not specified Not specifiedFocal spot size, mm 0.2-0.3, 0.6, 1.0-1.2 0.6, 1.3 0.6, 1.2 0.6, 1.2 Grid pulsed Yes Yes No NoCooling system Yes Oil/forced air Air Air
IMAGE INTENSIFIER Phosphor diameter Not specified
Input, cm (in) 38 (15), quad 40, 35.5, 32, 23 (16, 14, 12, 9) 32, 24, 16 (12, 9, 6) 23, 16, 14 (9, 6.7, 5.5); 32, 24, 16(12, 9, 6.7)
VIDEO INPUT/OUTPUTTV camera type CCD progressive interline scan CCD CCD
SNR, dB 60 ?66 66 60Scan lines 1024 x 1024 1024 x 1024 1024 x 1024
NUMBER OF MONITORS 2 exam, 2 central 2 3Monitor sizes 21" 18" LCD 17" 15", 19", 18"
DATA COMPRESSION DICOM Available Lossless Lossless IMAGE STORAGE
512 x 512, images 48,000 NA NA NA 1024 x 1024, images 12,000 75,000 40,000 10,000
Additional storage User preference 150,000 (1024 x 512) Optical disk, 640 MB CD-RW 700 MB DIGITAL IMAGING SYSTEM X FRAME CCD Yes Yes DICOM 3.0 COMPLIANT Yes Yes Yes Yes MINIMUM ROOM SIZE, m (ft) 4 x 4.5 (13.2 x 14.8) 5 x 4.5 (16.4 x 14.8) Not specified
MINIMUM ROOM H, m (ft) 2.9 (9.2) Not specified Not specifiedOTHER SPECIFICATIONS None specified Meets requirements of IEC 60601-1. None specified
LAST UPDATED 1/03/2006 1/03/2006 1/03/2006
36 PROMOTING TEAMWORK ACROSS DIFFERENT DISC IPL INES
Author Guidelinesfor Imaging Management
�
CONTENT
IMAGING Management welcomes submissions from qualified, experi-
enced professionals active in the imaging industry, related technology
companies and medical healthcare professionals with an interest in imag-
ing-related topics and themes. We are particularly interested in articles
focusing on management or practice issues and therefore accept scientif-
ic papers with a clear connection to these areas. Articles must be written
by independent authorities, and any sponsors for research named. Our
editorial policy means that articles must present an unbiased view, and
avoid ‘promotional’ or biased content from manufacturers.
SUBMISSION GUIDELINES
Authors are responsible for all statements made in their work, including
changes made by the editor, authorised by the submitting author. The
text should be provided as a word document via e-mail to editorial@
imagingmanagement.org. Please provide a contact e-mail address for cor-
respondence. Following review, a revised version, which includes editor’s
comments, is returned to the author for authorisation. Articles may be a
maximum 700 words per published page, but may include up to 1,500
words in total.
STRUCTURE
Article texts must contain:
✓ names of authors with abbreviations for the highest academic degree;
✓ affiliation: department and institution, city and country;
✓ main authors are requested to supply a portrait photo (see specifica-
tions below);
✓ one contact name for correspondence and an e-mail address which
may be published with the article;
✓ acknowledgements of any connections with a company
or financial sponsor;
✓ authors are encouraged to include checklists, tables and/or guidelines,
which summarise findings or recommendations;
✓ references or sources, if appropriate, as specified below.
IMAGES
Main authors are invited to supply a portrait photo for publication with
their article, as well as other images and visuals. This and any other rele-
vant images for publication with an article should be sent by e-mail as
separate files (only high resolution images with 300dpi) and their order
of placement in the article must be clearly indicated. Only the electronic
formats _.tif_ or _.jpeg_ can be used for images, i.e. not Microsoft Word
or PowerPoint. Images must be no smaller than 9cm x 9cm at 100%
scale. Only images meeting these specifications can be published. If an
image has been published before, permission to reproduce the material
must be obtained by the author from the copyright holder and the origi-
nal source acknowledged in the text, e.g. © 2004 Dervla Gleeson.
FORMAT FOR REFERENCES
Please use the Harvard reference system. Citations within the text for a sin-
gle author reference should include the author surname and year of publica-
tion; for a citation with two authors include both author surnames and year
of publication; for more than two authors, include the first author surname
followed by "et al." and the year of publication. Multiple citations should be
separated by a semicolon, and listed in alphabetical order.
Example of within text citation: (Gleeson 2007; Gleeson and Miller
2002; Miller et al. 2003).
The format for listing references in submitted articles should follow
the Harvard reference system. Example of standard journal reference:
Sydow Campbell, K. (1999) "Collecting information; qualitative research
methods for solving workplace problems", Technical communication,
46 (4) 532-544. Readers will be provided with an e-mail contact for ref-
erences, which will be kept on file and supplied on request. Authors are
responsible for the accuracy of the references they cite.
ACCEPTANCE
It is at the discretion of our editorial board to accept or refuse submis-
sions. We will respond to submissions within four weeks of receipt. We
reserve the right to revise the article or request the author to edit the con-
tents, and to publish all texts in any EMC Consulting Group journal or
related website, and to list them in online literature databases.
For further details or to request a copy of the 2007 editorial planner,
with topics and focus areas included, please email
Thank you,
The IMAGING Management Editorial Team
IMAGING MANAGEMENT: THE OFF IC IAL VOICE OF THE EUROPEAN IMAGING INIT IAT IVE 37
The child mortality rate in Finland is one of the low-est in the world; the infant mortality rate is below4%. The life expectancy for women is 81 years, for aman, 73 years. The life expectancy of Finnish men isimpaired by cardiovascular disease, excessive con-sumption of alcohol and accidents. Cardiovascularmortality has declined in response to effective healthand nutritional education in recent decades but exces-sive blood cholesterol levels and obesity remain com-mon in Finland. Smoking and drug abuse are signifi-cantly less frequent in Finland than in Europe onaverage. Prevention receives particular emphasis inprimary healthcare.
Primary Healthcare in FinlandFinland is divided into some 450 municipalities. Eachmunicipality is responsible for arranging healthcarefor its inhabitants. Primary healthcare is provided byhealth centres established by a single municipality orjointly by neighbouring municipalities.Municipalitieshave the right to buy services from other municipali-ties or from the private sector. Health centre servicesinclude medical consultations and provision of dentalcare, preventive care and environmental healthcare.Health centres run maternity and child health clinics,and arrange school and occupational health services.
Finnish municipalities have switched from a primaryhealthcare system to a family doctor system. Each fam-ily doctor is responsible for about 2,000 patients. Theaim is for a patient to be able to contact her or his doc-tor and have needs for treatment assessed within three
38 PROMOTING TEAMWORK ACROSS DIFFERENT DISC IPL INES
working days. This system has proved very successful.
Benefits of long-term treatment relationships includea reduced need for hospital exams and reducedhealthcare costs. Outpatient care is also provided byoccupational and private healthcare units. Employersare under an obligation to arrange occupationalhealthcare for employees which can be arrangedthrough municipal health centres or private practi-tioners. About 4% of Finnish doctors work in occu-pational healthcare, offering both preventive servicesand primary healthcare.
Specialist Care Finland is divided into 20 hospital districts, each pro-viding specialist consultation and care for its popula-tion. Local municipal authorities are responsible forfunding specialist treatment for inhabitants of theirareas. Each hospital district has a central hospital withdepartments for main specialties. Finland has five uni-versity hospitals. These provide the most advancedmedical care, including highly specialised surgery andtreatment for rare diseases. The university hospitals arealso mainly responsible for the clinical training of med-ical students, and for medical research. In comparisonwith the situation in other countries, the number ofhospital beds in Finland is fairly high.
There has been a trend towards reducing the numberof hospital beds by grading of care, which means thatmilder cases are treated in outpatient care and healthcentres and more severe cases in hospitals. Other ways
The aim of Finnish health policy is to lengthen the active andhealthy lifespan of citizens, to improve quality of life, and todiminish differences in health between population groups. In2002 there were more than 19,000 doctors in Finland.Almost1,000 Finnish doctors of working age live abroad and some 200foreign doctors practice in Finland under temporary licences.About half of the Finnish medical profession is female.
PROVIDED BY:
Finnish MedicalAssociationHelsinki, Finland [email protected]
Overview of National Healthcare Services
HEALTHCARE AND
THE MEDICAL PROFESSIONIN FINLAND
Countr y Focus Finland
tion to health insurance is compensationfor sick leave and parental leave. Alllicensed Finnish doctors are covered by thereimbursement system, which is adminis-tered by the social insurance institution
Medical Education in FinlandIn Finland, basic medical education isgiven in five universities (Helsinki,Tampere, Turku, Oulu, and Kuopio).There is substantial competition for placesin medical schools. The number of appli-cants is four or five times higher than the
number admitted. The FMA has tried to persuade theauthorities to bring numbers of students into corre-spondence with numbers of doctors needed. The viewof the FMA is that adequate supply of doctors shouldbe ensured by improving remuneration and workingconditions of doctors rather than by increasing num-bers of students. Studies have traditionally involved aninitial two-year preclinical period of mainly theoreticalcourses in anatomy, biochemistry, pharmacology, etc.However, students now have contact with patientsfrom the beginning of their studies.
A problem-based learning method has been intro-duced. All medical schools have research programmesfor students who wish to undertake scientific work.Inclusion of clinical cases in various courses and pre-clinical subjects is becoming common. During theclinical period of their courses, students participate inthe work of various hospital and health centre depart-ments, learning necessary medical skills. After eachclinical course, students have to pass a final examina-tion in the specialty. Basic medical education lasts forsome six and a half years and leads to the degree ofLicentiate of Medicine. ����
of reducing the number of hospital beds include intro-ducing short-term postoperative treatment and trans-ferring patients, for example those receiving psychiatrictreatment, to receive outpatient care. The number ofemergency units has also been reduced in an effort tosave costs and reduce the workloads of doctors.
Costs of Public Healthcare Health services are available to all in Finland, regardlessof their financial situation. Public health services aremainly financed from tax revenues; partly municipal,partly state tax. Central government’s contribution tomunicipal healthcare is determined by populationnumbers, age structures and morbidity statistics. Anumber of other factors also affect its computation.Finland spends less than 7% of its gross national prod-uct on healthcare, one of the lowest among EU mem-ber states. The public sector finances 76% of totalhealthcare expenditure, users of services 20% and oth-ers 4%. Other contributors include employers, privateinsurance and benefit societies.
Private Healthcare Private medical treatment is provided by municipalitiesand the state. Particularly in cities, many doctors, den-tists, and physiotherapists offer private care. There arealso a few small private hospitals. Only about 8% ofFinnish doctors earn their living solely as private prac-titioners. However, about one third of doctors run aprivate practice in addition to working in a hospital orhealth centre. Most private practitioners now work ingroup practices.
Everyone in Finland is covered by obligatory sicknessinsurance, funded through taxes by the state, munici-palities, employers and the insured population. Thesickness insurance scheme reimburses fees paid bypatients to private doctors, costs of medicines pre-scribed, and transportation costs arising from treat-ment of illness. By far the greatest expenditure in rela-
IMAGING MANAGEMENT: THE OFF IC IAL VOICE OF THE EUROPEAN IMAGING INIT IAT IVE 39
Countr y Focus Finland
Table 1: Facts about Finland (2002)
Facts about Finland (2002)Area 338,145 km2
Population 5.2 million Population density 17/km2
Capital Helsinki Inhabitants 560,000 Official languages Finnish 92%, Swedish 6% Major religions Lutheran 85%, Orthodox 1% GDP per head 26,000 EurosNumber of doctors 19,336 Inhabitants/doctor 269
“Adequate supply ofdoctors should beensured by improvingworking conditionsrather than increasingstudent numbers”
40 PROMOTING TEAMWORK ACROSS DIFFERENT DISC IPL INES
Countr y Focus Finland
AUTHOR
Juhani AhovuoManaging Director HUS Helsinki MedicalImaging CentreHelsinki, [email protected]
Since 2004, the HUS Helsinki Medical ImagingCentre (HMIC) is responsible for the provision ofradiological services for the hospital district of Helsinkiand Uusimaa. HMIC offers radiological services tofourteen hospitals.
Municipality owners also have their own primaryhealthcare organisations, which have been equippedwith conventional radiographic and ultrasonograph-ic tools since the 1970’s. When the Hospital District ofHelsinki and Uusimaa was established, Helsinki Cityhanded over its primary healthcare radiological servic-es to HMIC. After that, many other municipalitiestook the same decision, and today HMIC offers pri-mary radiological services in sixteen of its thirty-oneowner municipalities. The integration of specialty andprimary radiological services reduces overlapping activ-ities, increases the use of radiological equipment anddecreases the number of radiological exams, generatingcost savings for the municipalities.
Financial Facts about HMICThe 2007 budget of HMIC is 68.7 million Euros. Pre-and post-tax profits are forecasted to be 1 millionEuros. The number of employees is 790, of which 171are radiologists, 466 radiographers, and 153 other staff.The number of radiological exams is 800,000 per year.Conventional radiography accounts for 69% of allexams, CT 10%, ultrasound 13%, and MRI 5%.
The annual investment level is under 10 millionEuros. There are nine MRI scanners, of which one isa 3T unit, as well as thirty ultrasound scanners and
fifteen CT scanners, of which two are 64-slice scan-ners. The organisation also has fourteen DR andtwenty CR systems for conventional radiography.
Protocols that Serve Patients and DoctorsHMIC operates on the principal of the patient’sright to be examined with the right radiologicalequipment based on careful clinical tests done forthe patient and patient’s disease history. The rightimaging protocol is also provided. Exam results mustbe available when the referring doctor needs themfor treatment decision-making. In big organisationslike HMIC, there are very varied pools of radiologi-cal knowledge. Networking this knowledge results inmore accurate radiological diagnoses and enablesquicker consultations. The patients can choose thedepartment where the exam is done, except for MRIand CT exams.
Uniform ProcessesIn order to efficiently manage a big organisation,processes must work fluidly. With fourteen radiolog-ical departments and studies carried out in 30 differ-ent buildings, core and supportive processes cross allHMIC departments in order to achieve uniformity.The two core processes are diagnostics andresearch/teaching. HMIC has four diagnosticprocesses: conventional radiography; ultrasonogra-phy; CT and MRI; fluoroscopy, angiography andradiological interventions. The purpose is to do theradiological exam in a uniform way across the wholeorganisation. With this in mind, each of the four-
Municipalities in Finland are responsible for arranging health-care services for the people living in their area.The hospitaldistrict of Helsinki and Uusimaa, owned by thirty-one membermunicipalities, is a publicly-funded specialised medical careorganisation. Helsinki city is the biggest municipality owner of the group, providing services to over 1.5 million people.The University of Helsinki is also an owner of this organisa-tion, and includes fifteen hospitals, of which eleven have uni-versity hospital status.
Reorganising Departmental Activities for Greater Effectiveness
MANAGEMENT CHALLENGESFOR RADIOLOGY IN FINLAND
ca. 180 km
ca. 80 km
Hospital District of Helsinki and Uusima
FINLAND
IMAGING MANAGEMENT: THE OFF IC IAL VOICE OF THE EUROPEAN IMAGING INIT IAT IVE 41
teen radiological sites are networked. The integra-tion of radiological services between these buildingsis supported by the HUSPacs IT solution and adomestic RIS. HUSPacs is one the biggest regionalPACS in Europe.
The owner of each diagnostic process is responsiblefor developing, planning, and coordinating theirprocess and for planning investments in radiologicalequipment. The target is to allocate scarce resourcesin an efficient way between the different depart-ments. When planning radiological investments,attention is paid to the utilisation capacity of theinvestment. Process owners also participate in allo-cating the use of human resources.
Economic BackgroundHMIC is a non-profit or low-profit public organisa-tion, which finances its activities from money comingfrom services given to patients and paid for by theresponsible municipalities. The economic situation ofthe municipalities determines the targets and framesfor HMIC. HMIC uses so much capital for its hugerunning costs that global business models are followedto ensure smooth management. Much attention is paidto cost-control. HMIC’s size gives it synergies andexcellent opportunities to utilise scale of economies,for example in investments.
Human ResourcesIn Finland, there is a shortage of radiologists. Publichospitals have difficulties in hiring radiologists, and theworkload for those in employment is high. In HMIC,the additional challenge is to balance the workload ofradiologists and radiographers between differentdepartments. HMIC has hired private sector radiolo-gists to read and report exams to assist in this. In pub-lic hospitals, the incentives for personnel are fewer than
in private practices. However, the trend is to increaseincentives in public hospitals also. As a hospital withuniversity status, HMIC pays attention to educatingpersonnel. The interesting nature of radiological workat the university hospital appeals to many radiologistsand radiographers.
Management HMIC is an organisation of many kinds of profes-sionals. This presents a challenge in leading andmanaging the enterprise. Having university hospitalstatus does not make it easier. The essential role ofthe managing director is to be visionary. Changes inradiological business are rapid and must be noted inthe development and planning of activities. At thesame time, increasing healthcare costs cause addi-tional challenges for management. The main task ofthe managing director is to ensure that economic andfunctional targets, assessed by the HMIC board andthe Council of the Hospital District of Helsinki andUusimaa, are achieved.
Radiological departments are run by chief radiologistsand chief radiographers responsible for arranging dailywork in their departments. Department chiefs mustnegotiate with process owners for daily investment andhuman resource needs. The role of the headquarters ofHMIC is planning, development and coordination of
radiological activities within the wholeHMIC organisation.
AchievementsEvery year we see positive results from ourtight managerial procedures. The orderedexams have been carried out at the righttime, within time limits set by Finnishstandards. Costs have been within targetbudgets. An annual decrease in indexedcosts has been at the level of 3%. This hasresulted in a good price stability, and forthe three last years, the nominal priceshave remained unchanged.
Future ChallengesUntil the present time, HMIC has con-centrated on expanding and taking over
integrated radiological services in the HospitalDistrict of Helsinki and Uusimaa. In the near future,the target is to reorganise radiological activities toachieve additional synergies, economies of scale andcost savings and to secure regional radiological serv-ices for patients. When reorganising HMIC’s activi-ties, identifying and balancing the interests of thestakeholders is crucial. In the near future, furtherdevelopment of processes is required. ����
Countr y Focus Finland
“Adequate supply of doctors should beensured by improvingworking conditions rather than increasingstudent numbers”
42 PROMOTING TEAMWORK ACROSS DIFFERENT DISC IPL INES
AUTHOR
Pekka RuotsalainenNational Research andDevelopment Centre forWelfare and Health Stakes Unit for eHealthand eWelfareHelsinki, [email protected]
The national communication platform is financedboth by the Ministry of Social Affairs and Health andpublic and private service providers. The platform willstart its service in Spring 2008 and should be fullyoperational by the end of 2011. The platform offersboth promises and challenges. Using the nationaleArchive it is possible to create one virtual lifelong per-sonal health record for every citizen which can be usedfor profiling, prevention and prediction of the futurehealth status and risks.
Typical eHealth services available via the internet arebooking and information services, disease and lifestylemanagement and home care. The eArchive also offerscitizens access to his or her own EHR and audit logsgenerated by the eArchive. Because all official eHealthservices will use the national web service platform, it isalso a natural platform for future consumer-orientedeHealth services.
Background – Digitisation in FinlandThe first eHealth strategy established by the Ministryof Social Affairs and Health was published in May1996 built around the principle of secure informationsharing and ICT support for seamless citizen-centredcare. This strategy was updated in 1998 with the fol-lowing targets: adoption of EHRs in all levels of care,nationwide interoperability, high-level security andprivacy protection and citizens’ access to their records
via the internet. This strategywas realised by the implementa-tion of regional cooperativeEHR systems (RHIS) with com-mon middleware services. RHISsupported the transmission ofeReferrals, eConsultation mes-sages and digitalised images.
Structure of the Finnish EHRIn Finland every health organi-sation has the responsibility tomanage and archive healthrecords. Inside the service organ-
isation the health record is personal and lifelong. Basedon national regulations health records must bearchived up to 100 years and images should bearchived for 20 years.
In Finland the collection of care information is based ondocuments. Those documents represent snap-shots ofthe dynamic care process. For security and confidentiali-ty, after every care episode, the responsible physicianmust sign the EHR. The internal organisation of theFinnish health record is very close to the structuredefined in the open EHR standard. The EHR has fold-ers for every specialty and inside a folder there is a set ofcumulative episodes. Episodes are organised under head-ings. Each headed section is lifelong and cumulative.
Securing the Future of HealthcareIn 2001, the Finnish government launched thenational programme for securing the future ofhealthcare. One of the eighteen projects of the pro-gramme concerns the implementation of national,interoperable EHRs. Messaging methods are basedon HL7 CDA and DICOM messages for communi-cation. A national core data set was created forsemantic interoperability.
The long term tradition in Finland has been todevelop both strategy and supporting legislation inparallel. A new act regulating the management and
Launched in 2001, the Finnish EHR project defines thebasic level of semantic interoperability of EHRs and thenational communication infrastructure for eHealth.Themain building blocks of this architecture are eArchivingservices and a national communication platform.Thisplatform integrates all local EHR systems and theeArchive.The eArchive preserves not only narrative EHRsbut also images and also supports gross organisationalseamless care by disclosing health records. First nationaleHealth services are e-prescribing and the preservationand distribution of EHRs and digitalised images.A new lawallows all EHR systems storing digitalised EHRs to usenational services after 2011.
An Interoperable Infrastructure for eHealth
FINNISH NATIONAL EHR PROJECT
Countr y Focus Finland

IMAGING MANAGEMENT: THE OFF IC IAL VOICE OF THE EUROPEAN IMAGING INIT IAT IVE 43
use of electronic health information has been devel-oped. This act regulates the collection and disclosureof EHRs and sets minimum security and privacyprotection rules. The updated eHealth strategy andnew legislation form the road-map for the imple-mentation of future eHealth services in Finland.
The national communication architecture is targetedto support both the technical and semantic interoper-ability of EHRs and to solve the problem of the long-term availability and usability of EHRs. Security serv-ices are also one of the key functions of the platform.In the architecture, the web-service platform acts as anintegration machine. Information between legacy sys-tems and common services are transferred in the formof documents. Citizens and patient are connected tothe eArchive via web services.
Technical interoperability is achieved using stan-dardised messages. Messages accepted at the presenttime are HL7CDA R2 and DICOM. ePrescriptionsare transferred in the form of HL7 v.3 messages. Allmessages have a header with harmonised meta-dataand a structured body section supporting the previ-ously-mentioned EHR structure.
Semantic interoperability is archived by making theuse of national core data sets, selected classificationsand EHR headings mandatory. All terms and classi-fications can be downloaded from the term codeserver. Long-term availability of records is achievedby the development of a centralised EHR archive.For security, all documents are signed electronicallyand transferred in a Simple Object Access Protocol(SOAP) envelope. Healthcare persons and entitiesare identified and authorised using the commonPKI-service. All health professionals have a healthprofessional smart card.
Common ServicesKey common services are registration of EHRs,eArchive, consent management, certification serviceand code and term service. The registering service isthe key tool to locate and manage EHRs.
The role of the eArchive is to preserve, disclose anddestroy records. The disclosure of EHRs is based on pol-icy rules. In Finland, preconditions for any EHR disclo-
sure are the presence of doctor-patient relationship,patient’s consent or explicit legislation. It is the respon-sibility of legacy systems to create the relationship cre-dential and consent document. A policy engine has beenincluded to the SOA service layer to control the disclo-sure of EHRs. The eArchive has to prove the availabili-ty and security of records during preservation.
The main task of the eArchive is to preserve narra-tive EHRs, pictures, images and bio-signals. ExistingPACS/RIS systems send pictures selected for longterm preservation or disclosure in DICOM docu-ment format to the eArchive. The national consentservice stores all consent documents. Patients main-tain the right to check and change their active con-sent profile. The eArchive must check consent beforeany data disclosure. National certification servicesare intended both for healthcare entities and healthpersons. There is also a national certification servicefor citizens.
Requirements for the Users of National ServicesThe main users of common services are legacy sys-tems and patients. Present legacy systems are notready to be connected to common services. Theyshould be updated and new services should also bedeveloped for citizens. All computer systems con-nected to the national platform should be certifiedagainst functionality, interoperability and security.
Legacy systems should implement the following newservices before the use of national services:1. A data entering application to support commonheadings, terms, classifications and the core data set;2. Creation of consent document and relationshipcredentials;3. Capturing data from the local database;4. Creation of HL7CDA and DICOM messages; 5. Creation, preservation and access requests whichare sent to the eArchive;6. Viewing received EHR-messages; and,7. Generating audit logs.
A secure web service will be developed for citizensaccessing the eArchive via the inter-net. A smart cit-izen card and certification services should be usedfor security. ����
Countr y Focus Finland
44 PROMOTING TEAMWORK ACROSS DIFFERENT DISC IPL INES
Implementing good staff assess-ments in the medical imagingdepartment begins at recruit-ment level. Making sound hiringdecisions in the first placeensures as few later difficulties aspossible. Don’t hire anyone whoisn’t well qualified or who hasquestionable career history, isthe first piece of advice; it makesassessing staff afterwards muchmore straightforward.
One of the main challenges in recruitingmedical imaging staff in Europe is posedby the national variations in standardsthroughout Europe and beyond, on whatconstitutes an adequately qualified radiol-
ogist. For example, in Russia it takes amere three years to become a practicingradiologist, with not even a fixed curricu-lum for residents by which to assess whatareas an applicant has covered. This is incomplete contrast to countries such as theUnited Kingdom and Germany, wherecurricula are highly regulated. Personalityis also important – making sure an appli-cant has the right personality and canengage effectively in cooperation andteamwork will make their place in yourdepartment much smoother.
Keeping Abreast of Evolving ProceduresA candidate’s initial education, whileimportant, must be backed up by con-tinuing medical education to ascertainwhether or not they are up-to-date withcurrent practice. The US is furtherevolved in this respect, due in part tothe rise in malpractice suits and a morelitigious culture. US board examina-tions, while not mandatory, are general-ly taken by all, as no decent hospital willhire a radiologist who has not taken andpassed these exams. There, radiologistsview board exams as a desirable additionto their resumé, an attitude similar tothe one in the UK.
The US has also developed e-Learning asa tool to offer continuing specialty-basedexams that are again not mandatory, butdemonstrate that a medical professional isactively ensuring their education is rele-
AUTHORS
Prof. Hans BlickmanChairmanDepartment of RadiologyNijmegen,The [email protected]
vant. It is inevitable that Europe must fol-low the US in these practices and for-malise continuing education with ahomogenised set of standards.
For example, in Europe, many medicalstaff attend such courses, but due to alack of regulation, it is possible for themto obtain the relevant CME creditswithout actually attending the course.Big meetings such as the ECR havetaken steps to regulate this absenteeism,but smaller courses don’t have a formalstructure in place to ensure that absentparticipants are not credited for coursesthey have not in fact attended.
Evaluating Underachieving StaffDocument, document, document! It isessential to maintain a comprehensivedossier on complaints about all employ-ees to back up any formal proceduresthat may eventually take place when amember of staff underperforms or isinvolved in a negative situation withpatients or other staff members.
An annual review is a great forum forthrashing out any workplace issues –with a positive ‘how can we help you’attitude, where one can give a warningthat an incident or behaviour/attitudein the department was inappropriate.This is the generally accepted formalsetting for dealing with underachievingstaff. The informal way is to evaluate
HOW TO...
ASSESS STAFF PERFORMANCE IN THE IMAGING DEPARTMENT
�How To...�

�� c o n t i n u e d f r o m p . 3 3
IMAGING MANAGEMENT: THE OFF IC IAL VOICE OF THE EUROPEAN IMAGING INIT IAT IVE 45
performance amongst peers within thedepartment. In our department, col-leagues send each other their cases forsecond opinion so that at the end of theyear we are then able to say how manyjudgement calls are valid, and howmany if at all, adversely affectedpatients. We hope to formalise thisprocess and I believe it will be a valuabletool in assessing staff.
Other Evaluation ToolsJob descriptions are broken down intosecondary task lists for each individualteam member. At the annual review, thisallows us to compare results to the orig-
inal standard document. We also main-tain a coordinating member of staff foreach modality, for example, MR, andtheir role in this task is also up for annu-al evaluation to talk about the changesthey have experienced over the past year,if they are satisfied with the way they aregoing and if there are any future changesthey wish to implement. It allows us todevelop a realistic and fulfilling careerpath for all members of staff.
Using Staff InformationResponsiblyConfidentiality is key in staff assess-ment. We can use information about
staff to inform our decisions in hiring,extending contracts or reviewing per-formance. We can let it be known toother members of staff if we have a gen-eral feeling of reservation about a certainindividual, but sharing negative infor-mation is clearly discriminatory andmust be avoided. All records from staffreviews are held in a central repositoryonly accessible by the record keeper, theboard of directors and the Chairman toensure complete confidentiality. ����
that the C-arm can rotate 180∞ aroundthe patient while capturing multipleimages. The images can then be back-projected, in much the same way as inCT, to produce a 3D depiction of theanatomy. Angiography was the firstapplication of this, since it is inherentlyhigh contrast, on account of the contrastmedia, allowing the use of low x-raydoses. The earliest implementations werelimited due to the five minutes neededfor reconstruction. As more computingpower was added and the algorithmsimproved, this delay has been signifi-cantly reduced, so that a few seconds isall that is required.
The 3D angiography technique has nowbeen extended to produce more CT-likeimage performance: in other words, bettersoft tissue contrast. The idea is that CT-like images can be acquired during aninterventional procedure without havingto take the patient to a CT scanner mid-procedure. The images, while of insuffi-cient quality for diagnosis, are goodenough to guide therapeutic applications.
In fact, while interventional CT imagesdon’t have the same contrast resolutionfound in diagnostic CT, the spatial resolu-tion is better.
Flat Panels BecomeNecessary for IRWhile these applications are theoreticallypossible with image intensifier-basedequipment, the wider dynamic range,high uniformity, and distortion-freeimage quality mean that flat panel sys-tems are necessary. So, flat panel detectorscan now be found on interventional radi-ology systems from all major manufactur-ers. More recently, healthcare facilitieshave a greater variety of biplane flat panelsystems to choose from. So, the use ofimage intensifiers is shrinking. It is main-ly due to cost considerations that theradiographic/fluoroscopic systems used indiagnostic applications are still equippedwith image intensifiers.
What About the future?Minimally invasive procedures arebecoming increasingly important. Flat
panel technology will improve, allowingfurther dose savings and higher resolu-tion imaging. The present limitations onframe rate will be improved. But the areawith the most benefit to patients will bethe addition of more robotic technologyand other automated guidance tech-niques. For example, one technique thatalready exists is magnetic guidance ofcatheters in cardiology. Such a techniquewould be impossible with an imageintensifier on account of the magneticfields. But with 3D data sets it is possi-ble to guide a catheter through the tor-tuous vasculature with far greater preci-sion and, therefore, safety.
Another example is the addition of an x-ray imager on an MR system. MR can-not provide real-time images and makesit extremely difficult to access thepatient. But MR does provide soft tissuecontrast that is simply unobtainablewith x-ray-based imaging. So, combin-ing the two modalities promises signifi-cant advantages. ����

46 PROMOTING TEAMWORK ACROSS DIFFERENT DISC IPL INES
are rare in experienced hands. Differentcost analysis, performed both in NorthAmerica and in Europe, show that UFEcompares favourably with hysterectomyand myomectomy despite the cost of thepre- and post-procedural MRI and theneed for single use devices such ascatheters.
� Is UFE one of the main proceduresperformed by interventional radiologists?Due to the high percentage of women pre-senting with fibroid-related symptoms, wemay expect UFE to be a commonly per-formed procedure. However, it is stillmainly available in big hospitals and uni-versities where trained radiologists andspecialised fibroid centres are present. Insome centres like ours, UFE is one of themany embolisations for gynaecological andobstetric disorders. We treat pelvic arterio-venous malformations, cancer-relatedbleeding, adenomyosis, and post-operativeor post-partum haemorrhage. In fact, UFEis very helpful to train young radiologiststo perform all kind of emergency pelvicembolisations.
� How can we ensure that gynaecolo-gists be informed about UFE so thatthey can present this procedure as atreatment option?Most gynaecologists are now well awareabout UFE even if they aren’t as familiarwith its indications. Scientific meetingsand publications will help. Family doctorshave so many clinical conditions to man-age that it is difficult for them to knowabout new treatments. We try to informthem through local meetings and publica-tions. The CIRSE UFE website has a sec-tion for doctors presenting the variousaspects of the technique, indications,results and follow-up. An updated list ofpublications is also available. For patients,the website seems very promising since it isavailable in different languages. For
INTERVIEWEE
Dr Jean-Pierre PelageHopital Ambroise ParéParis, France
dards of practice committee that pub-lished joint recommendations with theAmerican Society of InterventionalRadiology on UFE. I also got involved inthe set up and monitoring of the UFEregistry, promoted by the CIRSEFoundation. Finally, CIRSE created aUFE taskforce of which I am Chairman.
We have gathered a group of radiologistsand gynaecologists from differentEuropean countries with the goal of pro-moting UFE. The first objective has beenrecently achieved with the launch of theUFE website, which will be progressivelyavailable in different languages to helppatients to better understand about uterinefibroids, available treatments and theirprinciples, advantages and side-effects. Asection entitled “Find a doctor near you”will provide the list of centres per countrywhere embolisation is available. We havealso just started a UFE advisory group ded-icated to promotion, training and researchin the field.
� How does UFE compare with thealready “established” treatments?From scientific publications includinglarge prospective studies and randomisedcontrolled studies versus surgery, we knowthat UFE is a valuable alternative to hys-terectomy and multiple myomectomy.UFE is usually not a first line treatment asan alternative to a single myomectomy,particularly by laparoscopy or hys-teroscopy. All studies show that embolisa-tion is very effective to control heavy men-strual bleeding and bulk-related symp-toms. Volume reductions both for theuterus and the fibroids range between 30and 60% after treatment. Hospital staysare minimal, one or two nights in mostcases. Some well-organised centres evenoffer UFE as an outpatient procedure.Recovery is short and most women willstay out of work for a week. Complications
� Please tell us about your back-ground in the area of UFE.I was trained as a resident and performedmy first UFE procedure in the HôpitalLariboisière, a University Hospital of Parisunder the supervision of Dr. Le Dref, oneof the pioneers in this field, in December1993. This is also where the first case ofUFE was performed by Prof. Jean-JacquesMerland. I then performed a four-yearclinical fellowship in interventional radiol-ogy in the same hospital.
The Hôpital Lariboisière has a long tradi-tion of interventional radiology both forneuroradiology and peripheral radiology. Itwas then the reference hospital for themanagement of gynaecological and obstet-ric emergencies such as postpartum haem-orrhage. I got involved in women’s inter-ventions and set up a specialised consulta-tion for candidates for UFE, ovarian veinembolisation or tubal procedures. I thenmoved to another university hospital, ParisOuest, where I was promoted to AssociateProfessor of Radiology in 2003 and thenfull Professor of Radiology in 2006. Wehave adopted the same way of workingclosely with the gynaecologists withpluridisciplinary discussions of all cases ofpatients with uterine fibroids.
� How are you involved with CIRSEand the UFE taskforce?I am a member of CIRSE since my fellow-ship and have been progressively involvedin different committees. First, the stan-
INTERVIEW WITH PROF. JEAN-PIERRE PELAGEHopital Ambroise Paré, Paris, France
�My Opinion�

�� c o n t i n u e d f r o m p . 3 2
� What does the future hold for UFEand how is the treatment being devel-oped to grow safer and more effective? I think that UFE may become a first-linetreatment in young patients trying to con-ceive, particularly if the only treatment onoffer is hysterectomy and multiplemyomectomy. More studies addressing theissue of fertility should be conducted toverify this statement. The best proof thatUFE is a global and effective treatment isthat surgeons try to mimic its mechanismof action. Laparoscopic clipping of theuterine artery and transvaginal uterineartery clamping are being investigated asan alternative to UFE. ����
Erratum:In the last edition of IMAGING Management,we incorrectly published a picture of the“Gaiffe” machine of 1907, instead of thereferred-to CT machine of 1974 in the MyOpinion interview. The picture is availableupon request.
� How can one manage pain in thebest possible way?The best way to avoid complications isgood patient selection, best done as a teamwith radiologists and gynaecologistsinvolved. Some types of fibroids may notrespond well to embolisation or may beassociated with an increased risk of com-plications. Patients’ expectations should beevaluated before embolisation to avoidproblems: very large uteri will neverbecome normal despite satisfactory devas-cularisation of all fibroids and patientsshould be informed.
Different protocols are used to reducepatients’ discomfort during and afterembolisation. Administration of NSAIDs,analgesics, use of PCA pumps or spinalanalgesia are commonly performed tomanage pain which may be intense during6 - 12 hours post-embolisation. We arecurrently investigating the value of emboli-sation microspheres loaded with painkillers progressively released in the bloodcirculation at the site of embolisation.
patients who don’t speak English it issometimes difficult to get information onthe internet.
� What trials are available comparingsurgical and non-surgical options, andwhat do they tell us about the safety andeffectiveness of UFE as an alternative?There are different high-quality studies inthe literature. In particular, the results oftwo multi-centre randomised controlledstudies conducted in the UK (RESTstudy) and the Netherlands (EMMY trial)have been recently published. Both studiescompared outcomes from therapies inpatients randomly assigned to UFE or sur-gery and confirm that UFE is equivalent tohysterectomy in terms of quality of lifeafter treatment. Minor complications areslightly higher after embolisation andmajor complications after surgery.Hospital stay, length of recovery and costare in favour of embolisation. Not surpris-ingly, when comparing a conservativetreatment to hysterectomy, the rate of re-intervention is higher after UFE, particu-larly in case of clinical failure.
2. Encourage experts from vendor andacademic institutions to join WG24.Vendors of endoscopic and microscopicdevices as well as implants (templates)should be included in addition to theclassic vendors of medical imaging and PACS.3. Compile a representative set of surgicalworkflows (with a suitable high level ofgranularity and appropriate workflowmodelling standards and surgical ontolo-gies) as a work reference for the scope ofWG24. Initially, three to five workflows,characteristic for each discipline, shouldbe recorded with sufficient level of detail. 4. Derive potential DICOM servicesfrom these surgical workflows.
5. Design an information/knowledgemodel based on electronic medical record(EMR) related work and identify IODextensions to DICOM. 6. Take account of the special image com-munication (1D - 5D) requirements forsurgery and mechatronic devices. 7. Work in close cooperation withDICOM experts from radiology, cardiolo-gy, radiotherapy and related fields repre-sented in WG1 - WG23.8. Encourage close cooperation withworking groups in international societieswith an interest in this area.9. Disseminate knowledge gained follow-ing the roadmap through workshops, con-ferences and special seminars.
10. Connect to integration profiles speci-fied for surgery by IHE activities.
ConclusionIn the process of realising a standard fortherapy imaging and model managementin surgery, it can be expected that sur-geons, interventional radiologists, hospitalmanagers as well as buyers and vendors ofOR equipment, will become aware of thenew business potential made possible by asuitable DICOM standard. By using thestandard, their business situation willimprove not least by more streamlinedworkflows, but also by a safer and higherquality patient care. ����
IMAGING MANAGEMENT: THE OFF IC IAL VOICE OF THE EUROPEAN IMAGING INIT IAT IVE 47

Agenda
Key Seminars & Conferences
© Imaging Management is published five times per year.The publisher isto be notified of cancellations six weeks before the end of the subscrip-tion.The reproduction of (parts of) articles is prohibited without the con-sent of the publisher.The publisher does not accept liability for unsolicit-ed material.The publisher retains the right to republish all contributionsand submitted materials via the Internet and other media.
LEGAL DISCLAIMERThe Publishers, Editor-in-Chief, Editorial Board, Correspondents andEditors make every effort to ensure that no inaccurate or misleading data,opinion or statement appears in this publication. All data and opinionsappearing in the articles and advertisements herein are the sole respon-sibility of the contributor or advertiser concerned. Therefore thePublishers, Editor-in-Chief, Editorial Board, Correspondents and Editorsand their respective employees accept no liability whatsoever for the con-sequences of any such inaccurate of misleading data, opinion or statement.
IMAGING Management28/7, RUE DE LA LOI
B-1040 BRUXELLES, BELGIUM
T: +32/2/ 286 85 00F: +32/2/ 286 85 08WWW.IMAGINGMANAGEMENT.ORG
PUBLISHERCHRISTIAN MAROLT
MANAGING EDITORDERVLA GLEESON
INTERNATIONAL EDITOREDWARD SUSMAN
EDITORSCAROLINE HOMMEZ
SHERRY SCHARFF
GLOBAL COMMUNICATIONSDR DON I. IDREES
JOURNAL MANAGEMENTKATYA MITREVA
CREATIVE DIRECTORASTRID MENTZIK
PRODUCTION AND PRINTINGPPS, PRINT RUN: 13,000 ISSN = 1377-7629
JUNE 2008
5 - 8 25TH INTERNATIONAL CONGRESS OF RADIOLOGY (ICR)Marrakesh, Morocco www.icr2008.org
10 - 13 EUROPEAN SOCIETY OF GASTRO-INTESTINAL AND ABDOMINAL RADIOLOGY (ESGAR) 2008 ANNUAL MEETING AND POSTGRADUATE COURSEIstanbul,Turkeywww.esgar.org
25 - 28 EUROPACS ANNUAL CONGRESSBarcelona, Spainwww.europacs.org
25 - 28 CARS ANNUAL CONGRESSBarcelona, Spainwww.cars-international.org
SEPTEMBER 2008
11 - 13 9TH ESGAR HANDS-ON WORK- SHOP ON CT-COLONOGRAPHYBerlin, Germanywww.esgar.org
11 - 14 ESUR 2008 ANNUAL CONGRESSMunich, Germanywww.esur2008.Org
13 - 17 CIRSE 2008 ANNUAL CONGRESSCopenhagen, Norwaywww.cirse.org
17 - 21 11TH ESH CONGRESS: HYPNOSIS & HYPNOTHERAPY:TRAUMA AND PAINVienna, Austriawww.emdr-netzwerk.at
18 - 21 EUROPEAN SOCIETY OF NEURORADIOLOGY (ESNR)XXXIII CONGRESS AND 17TH
ADVANCED COURSEKrakow, Polandwww.esnr.org
DECEMBER 2007
13 - 16 30TH ANNUAL SAN ANTONIO BREAST CANCER SYMPOSIUMSan Antonio,TX, USAwww.sabcs.org
14 COURSE ON 'LIFE AFTER PACS'London, UKwww.hhnt.org/hcc/conferences/life_after_pacs/index.htm
JANUARY 2008
10 - 12 “APPLYING INDUSTRY LEADER-SHIP CONCEPTS TO HEALTH-CARE” MIR WORKSHOP Bad Gastein, Austriawww.mir-online.org
FEBRUARY 2008
1 - 4 MRI IN PRACTICESydney, Australiawww.aaedpro.org
17 - 21 14TH INTERNATIONAL POSTGRADUATE COURSE ON ADVANCES IN CARDIAC ULTRASOUNDDavos, Switzerlandwww.echodavos.info/info.htm
MARCH 2008
7 - 11 EUROPEAN SOCIETY OF RADIOLOGY (ESR) ANNUAL CONGRESSVienna, Austriawww.myesr.org
15 - 20 SOCIETY OF INTERVENTIONAL RADIOLOGY (SIR) 2008 ANNUAL SCIENTIFIC MEETING Washington, DC, USAwww.sirmeeting.org
APRIL 2008
7 - 11 IHE CONNECTATHONOxford, UKwww.ihe-europe.org
23 - 26 INTERNATIONAL SOCIETY FOR RADIOGRAPHERS AND RADIO-LOGICAL TECHNOLOGISTS (ISRRT) 15TH WORLD CONGRESSDurban, South Africawww.isrrt.org
48 PROMOTING TEAMWORK ACROSS DIFFERENT DISC IPL INES
Verified Circulationaccording to the standards of InternationalBusiness Press Audits
IMAGING Management is independentlyaudited by Accountskantoor Closset onbehalf of MIR
The Management Journalfor Cardiologists
Cardiology Management is the only hard-copy
journal focusing on best practice in management
in cardiology departments across the world.
Distributed four times per year, this journal is tai-
lored to meet your information needs on the lat-
est best practices in management topics, such as
staff, financial and IT-related management issues.
Sections include:
• EU News – Covers developments at an EU
level that are relevant to cardiologists
• Industry News – The latest updates from
industry mergers, acquisitions and new
technology propositions
• Cover Story – Addresses hot topics such as
patient safety, quality assessments, staff
training and performance and managing
financial resources
• Features – Updates from cardiology
managers around the world
• Management – Practical and informative
guides to the latest management practices
• My Opinion – Interviews with leading
experts in cardiology management
Please submit all management-related abstracts to Managing Editor Dervla Gleeson at [email protected] before December 15, 2007. A full list of desired topics is available from our website.
Visit us at w w w. c a r d i o l o g y m a n a g e m e n t . e u
C a l l f o r A b s t r a c t s !
Volume 1 - Issue 1, November-December 2007
Coming in 2008!
Related Documents











