ORIGINAL ARTICLE Suppressive effect of low-level laser therapy on tracheal hyperresponsiveness and lung inflammation in rat subjected to intestinal ischemia and reperfusion Flávia Mafra de Lima & Luana Vitoretti & Fernando Coelho & Regiane Albertini & Ana Cristina Breithaupt-Faloppa & Wothan Tavares de Lima & Flávio Aimbire Received: 20 September 2011 / Accepted: 15 March 2012 / Published online: 5 May 2012 # Springer-Verlag London Ltd 2012 Abstract Intestinal ischemia and reperfusion (i-I/R) is an insult associated with acute respiratory distress syndrome (ARDS). It is not known if pro- and anti-inflammatory mediators in ARDS induced by i-I/R can be controlled by low-level laser therapy (LLLT). This study was designed to evaluate the effect of LLLT on tracheal cholinergic reactivity dysfunction and the release of inflammatory mediators from the lung after i-I/R. Anesthetized rats were subjected to superior mesenteric artery occlusion (45 min) and killed after clamp release and preestablished periods of intestinal reperfusion (30 min, 2 or 4 h). The LLLT (660 nm, 7.5 J/ cm 2 ) was carried out by irradiating the rats on the skin over the right upper bronchus for 15 and 30 min after initiating reperfusion and then euthanizing them 30 min, 2, or 4 h later. Lung edema was measured by the Evans blue extravasation technique, and pulmonary neutrophils were determined by myeloperoxidase (MPO) activity. Pulmo- nary tumor necrosis factor-α (TNF-α), interleukin-10 (IL- 10), intercellular adhesion molecule-1 (ICAM-1), and iso- form of NO synthase (iNOS) mRNA expression were analyzed by real-time PCR. TNF-α, IL-10, and iNOS proteins in the lung were measured by the enzyme-linked immunoassay technique. LLLT (660 nm, 7.5 J/cm 2 ) re- stored the tracheal hyperresponsiveness and hyporespon- siveness in all the periods after intestinal reperfusion. Although LLLT reduced edema and MPO activity, it did not do so in all the postreperfusion periods. It was also observed with the ICAM-1 expression. In addition to reducing both TNF-α and iNOS, LLLT increased IL-10 in the lungs of animals subjected to i-I/R. The results indicate that LLLT can control the lung's inflammatory response and the airway reactivity dysfunction by simulta- neously reducing both TNF-α and iNOS. Keywords Gut ischemia . Acute lung inflammation . Airway smooth muscle . Adhesion molecule . Cytokines . Phototherapy F. M. de Lima : R. Albertini Department of Rehabilitation Sciences, Universidade Nove de Julho, UNINOVE, Rua Vergueiro, 235, São Paulo, SP, Brazil L. Vitoretti : W. T. de Lima Laboratório de Fisiopatologia Experimental, Departamento de Farmacologia, Universidade de São Paulo – USP, Av. Prof. Lineu Prestes, 1524, CEP: 05508-900 São Paulo, SP, Brazil F. Coelho Laboratório de Radicais Livres, Departamento de Bioquímica, Instituto de Química, Av. Prof. Lineu Prestes, 748, CEP: 05508-00 São Paulo, Brazil A. C. Breithaupt-Faloppa Laboratório de Cirurgia Cardiovascular e Fisiopatologia da Circulação (LIM-11), Hospital das Clínicas - FMUSP, Av. Dr. Arnaldo, 445, CEP: 01246-093 São Paulo, Brazil F. Aimbire (*) Department of Science and Technology, Federal University of São Paulo, UNIFESP, São José dos Campos, São Paulo, Brazil e-mail: [email protected] Lasers Med Sci (2013) 28:551–564 DOI 10.1007/s10103-012-1088-1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ORIGINAL ARTICLE
Suppressive effect of low-level laser therapy on trachealhyperresponsiveness and lung inflammation in rat subjectedto intestinal ischemia and reperfusion
Flávia Mafra de Lima & Luana Vitoretti &Fernando Coelho & Regiane Albertini &Ana Cristina Breithaupt-Faloppa &
Wothan Tavares de Lima & Flávio Aimbire
Received: 20 September 2011 /Accepted: 15 March 2012 /Published online: 5 May 2012# Springer-Verlag London Ltd 2012
Abstract Intestinal ischemia and reperfusion (i-I/R) is aninsult associated with acute respiratory distress syndrome(ARDS). It is not known if pro- and anti-inflammatorymediators in ARDS induced by i-I/R can be controlled bylow-level laser therapy (LLLT). This study was designed to
evaluate the effect of LLLT on tracheal cholinergic reactivitydysfunction and the release of inflammatory mediators fromthe lung after i-I/R. Anesthetized rats were subjected tosuperior mesenteric artery occlusion (45 min) and killedafter clamp release and preestablished periods of intestinalreperfusion (30 min, 2 or 4 h). The LLLT (660 nm, 7.5 J/cm2) was carried out by irradiating the rats on the skinover the right upper bronchus for 15 and 30 min afterinitiating reperfusion and then euthanizing them 30 min, 2,or 4 h later. Lung edema was measured by the Evans blueextravasation technique, and pulmonary neutrophils weredetermined by myeloperoxidase (MPO) activity. Pulmo-nary tumor necrosis factor-α (TNF-α), interleukin-10 (IL-10), intercellular adhesion molecule-1 (ICAM-1), and iso-form of NO synthase (iNOS) mRNA expression wereanalyzed by real-time PCR. TNF-α, IL-10, and iNOSproteins in the lung were measured by the enzyme-linkedimmunoassay technique. LLLT (660 nm, 7.5 J/cm2) re-stored the tracheal hyperresponsiveness and hyporespon-siveness in all the periods after intestinal reperfusion.Although LLLT reduced edema and MPO activity, it didnot do so in all the postreperfusion periods. It was alsoobserved with the ICAM-1 expression. In addition toreducing both TNF-α and iNOS, LLLT increased IL-10in the lungs of animals subjected to i-I/R. The resultsindicate that LLLT can control the lung's inflammatoryresponse and the airway reactivity dysfunction by simulta-neously reducing both TNF-α and iNOS.
Keywords Gut ischemia . Acute lung inflammation .
Airway smooth muscle . Adhesion molecule . Cytokines .
Phototherapy
F. M. de Lima : R. AlbertiniDepartment of Rehabilitation Sciences,Universidade Nove de Julho, UNINOVE,Rua Vergueiro, 235,São Paulo, SP, Brazil
L. Vitoretti :W. T. de LimaLaboratório de Fisiopatologia Experimental, Departamento deFarmacologia, Universidade de São Paulo – USP,Av. Prof. Lineu Prestes, 1524,CEP: 05508-900 São Paulo, SP, Brazil
F. CoelhoLaboratório de Radicais Livres, Departamento de Bioquímica,Instituto de Química,Av. Prof. Lineu Prestes, 748,CEP: 05508-00 São Paulo, Brazil
A. C. Breithaupt-FaloppaLaboratório de Cirurgia Cardiovascular e Fisiopatologia daCirculação (LIM-11), Hospital das Clínicas - FMUSP,Av. Dr. Arnaldo, 445,CEP: 01246-093 São Paulo, Brazil
F. Aimbire (*)Department of Science and Technology,Federal University of São Paulo, UNIFESP,São José dos Campos, São Paulo, Brazile-mail: [email protected]
Lasers Med Sci (2013) 28:551–564DOI 10.1007/s10103-012-1088-1

Introduction
Abdominal trauma that causes intestinal ischemia and reper-fusion (i-I/R) may induce remote organ injury, with the lungbeing the first organ injured [1]. Intestinal I/R is also asso-ciated with the induction of systemic inflammatory re-sponse, which may indicate a causal link betweenmediators released during systemic inflammation and pul-monary dysfunction in acute respiratory distress syndrome(ARDS) [2]. ARDS is a critical illness characterized byacute lung injury, which leads to pulmonary permeability,edema, and respiratory failure, in addition to the massiverelease of inflammatory mediators [1, 2]. There is no spe-cific therapy for ARDS, and mortality resulting from thisdisease still remains high [3]. Many inflammatory media-tors, such as tumor necrosis factor-α (TNF-α), interleukin-10 (IL-10) and nitric oxide (NO), as well as intercellularadhesion molecule-1 (ICAM-1), are released during i-I/R[4]. Among them, the TNF-α, a pro-inflammatory cytokinewith a wide spectrum of activities, is involved in circulatoryshock, sepsis, and multiple organ failure. TNF also plays apivotal role in local and remote inflammatory responsesevoked by i-I/R [5, 6].
Several studies have demonstrated that IL-10 modulatespro-inflammatory cytokine production and tissue injury fol-lowing ischemia and reperfusion injury [7]. There is an evi-dence that the imbalance between TNF-α and IL-10production determines tissue injury and lethality during i-I/R[8], and it has been shown that treatment with anti IL-10 isassociated with increased TNF-α concentration, tissue injury,and lethality, demonstrating a role for the endogenous pro-duction of IL-10 in modulating exacerbated tissue pathologyand lethality [9].
An intestinal ischemic event culminates in mesentericvascular hyporesponsiveness mediated by intestinal expres-sion of the inducible isoform of NO synthase (iNOS) [10].Moreover, NO-dependent pulmonary inflammation occursduring i-I/R [11]. NO seems to mediate systemic reactionssuch as hypotension, vascular hyporesponsiveness to vaso-constricting agents, and mucosal intestinal injury and par-ticipates in the ensuing lung microvascular injury [12].Indeed, it is known that lung-generated NO plays a regula-tory role in airway smooth muscle tonus, in both healthy andinflammatory conditions [13].
Considering the above cited studies collectively, it is clearthat the strategies that stimulate IL-10 production and/or pre-vent TNF-α generation or function are effective in preventingi-I/R-induced lung injury. Furthermore, the exacerbated mod-ulation of NO synthesis can contribute strongly to controlreactive airways dysfunction syndrome.
Traditional ARDS and asthma treatments include avariety of pharmacological corticosteroids, methotrexate,and other disease-modifying agents such as cyclosporine
and intravenous immunoglobulin, as well as novel treat-ments such as TNF-α and IL-1β [14, 15]. Low-levellaser therapy (LLLT) has been used in inflammatorypathologies as a new anti-inflammatory therapy, which,in principle, would not be associated with any sideeffects [16, 17]. In fact, diverse authors have demon-strated that LLLT afforded a significant improvement inthe course of bronchial asthma, allowing for outpatienttreatment and rehabilitation, recovery of bronchial sen-sitivity to sympathomimetics and xanthine derivatives,lower glucocorticoid doses, shorter hospital stays, andreduced bronchial asthma-related disability [18, 19].
Recently, we showed a dual effect of LLLT on anti- andpro-inflammatory cytokines in a model of the acute lunginflammation induced by intestinal ischemia and reperfu-sion [20]. This result revealed that low-level laser irradi-ation can exert its biomodulatory effect on differentcytokines (TNF-α and IL-10) independently of each oneand at the same time. Based on data, our motivation in thecurrent study was to investigate if this inhibitory approachof laser irradiation on acute lung inflammation and anti-and pro-inflammatory mediators can be also efficient inrelieving the airway smooth muscle dysfunction (hyper-responsiveness or hyporresponsiveness). Moreover, hereinwe tested the laser irradiation in a different experimentaldesign with an innovative approach in which the efficien-cy of laser irradiation on Th1/Th2 cytokines, the induciblenitric oxide synthase (iNOS), and adhesion molecule indifferent periods of intestinal reperfusion were boarded. Inview of the above, the present work sought to identify apossible action of LLLT in relationship between airwayreactivity dysfunction and pulmonary inflammation afterintestinal ischemia and reperfusion.
Material and methods
Experimental animals
Male adult Wistar rats weighing 180–200 g were suppliedby the University of São Paulo, Department of Pharmacol-ogy. The animals were housed in artificially lighted roomswith controlled temperature (21–23 °C) and humidity (45–65 %) and a 12 h-12 h light/dark cycle (lights on at7:00 a.m.) with free access to food and water. The food isan extruded type, and its composition is protein (22 %),ether extract (4 %), fibrous matter (8 %), mineral matter(10 %), calcium (1.40 %), and phosphorus (0.80 %). Theanimals' housing and use were in accordance with the guide-lines of the Committee on Care and Use of LaboratoryAnimal Resources of the University of São Paulo, Instituteof Biomedical Sciences, which are similar to the guidelinesof the Canadian Council of Animal Care.
552 Lasers Med Sci (2013) 28:551–564

i-I/R rat model
The animals were preanesthetized with butorphanol (ace-promazine, 0.1 mg/kg) in which the acepromazine is theactive compound,, and shortly thereafter the animalswere anesthetized with Zoletil (zolazepam chlorhydrate0.1 mg/kg+tiletamine chlorhydrate 0.1 mg/kg; Invitro-gen, São Paulo, Brazil) that associates a new compoundof the family of feniciclidinas—the tiletamine—and acompound of the family of benzodiazepines—the zola-zepam—in a 1:1 ratio. The anesthetic properties ofacepromazine describe that it is not a sedative (calmingis not one) but neuroleptic and tranquilizing, ideal forpreanesthesia. The anesthetic properties of Zoletil com-pound describe that it allows a general anesthesia, safeand effective with minimal side effects. Posteriorly toanesthesia, the superior mesenteric artery was exposedthrough a midline abdominal incision and occluded using amicrosurgical clamp shaped very similarly to a number 1001-531 Vascu-Statt clamp (Scanlan International, MN, USA).After 45 min of arterial occlusion, the clamp was removed,and intestinal perfusion was established. The animals werekilled 30 min, 2, and 4 h later, still under anesthesia, byexsanguination of the abdominal aorta. With regard to thepossible interference of anesthesia in laser effects on bronchialand lung tissue, the more important point is that all animalswere anesthetized, and clearly, it did not interfere in inflam-matory response of animals from any group studied herein.The response of bronchial muscle and lung tissue to lipopoly-saccharide (LPS) was not altered by anesthesia; it proves thatanesthesia has no anti-inflammatory effect and oppositelyprovides evidences that laser is the responsible for attenuatingthe tracheal hyperresponsiveness and the lung inflammationafter i-I/R.
Laser irradiation
A CW laser diode module (MM Optics, São Paulo, Brazil)with an output power of 30 mW and a wavelength of660 nm was employed. The spot size was 0.08 cm2, andoptical power density was 31.25 mW/cm2. The opticalpower was calibrated using a Newport 1835 C multifunc-tion optical power meter (Equipland, Oklahoma Road, SaoJose, CA, USA). Laser beam pointing stability duringlaser irradiation was measured by collecting light with apartial reflection (4 %). The laser irradiation dose was setat 5.4 J for 3 min. The animals reperfused for 30 minreceived laser treatment 15 min after the beginning ofreperfusion, while those reperfused for 2 or 4 h receivedlaser irradiation 30 min after the beginning of reperfusion.The animals were irradiated once on the skin over theupper bronchus.
Experimental groups
The rats were divided into the following five groups (n07 pergroup): The naive group consisted of nonmanipulated rats.The sham group consisted of rats subjected to the samesurgical procedures, including mesenteric artery dissection,but not to arterial occlusion (ischemia) or reperfusion. Thei-I/R group consisted of rats subjected to occlusion of thesuperior mesenteric artery and reperfusion. The laser groupconsisted of nonmanipulated rats irradiated with laser. Lastly,the i-I/R+laser group consisted of rats subjected to i-I/R andlaser irradiation.
Preparation of isolated trachea segments
The rats were exsanguinated by sectioning the abdominalaorta under anesthesia. The thorax was opened, and thetrachea was removed. Tracheal segments were isolated anddissected out of the surrounding tissues. Tracheal rings werefixed with the aid of two steel hooks in a glass chamberfilled with 10 mL of Krebs–Henseleit buffer composed of(in mM): NaCl, 115.0; KCl, 4.6; CaCl2·2H2O, 2.5: KH2PO4,1.2; MgSO4·7H2O, 2.5; NaHCO3, 25.0; and glucose, 11.0.All reagents used to prepare the Krebs–Henseleit buffersolution were purchased from Invitrogen, São Paulo, Brazil.The solution was aerated continuously (95 % oxygen and5 % carbon dioxide) and kept at 37 °C. The tissues wereallowed to equilibrate for 60 min under a tension of 500 mg.During this period, the bath solution was replaced at 10-minintervals. The dose–response curves to increasing doses ofmethacholine were constructed with a data acquisition sys-tem (PowerLab, ADInstruments, Colorado Springs, CO,USA). Thereafter, the responsiveness to the cholinergicagonist methacholine (MCh; Sigma-Aldrich, St. Louis,MO, USA) was evaluated in tracheal tissues taken from ratssubjected to i-I/R and i-I/R+laser or from sham-operatedand nonmanipulated rats.
Pulmonary myeloperoxidase activity
Neutrophil recruitment to the lung was assessed by measur-ing myeloperoxidase (MPO) activity in the lung. Samples oflung were removed from rats killed 30 min, 2, and 4 h afterintestinal reperfusion and processed. The thorax wasopened, and the lungs were perfused with saline solution(PBS, pH 7.0; Invitrogen, São Paulo, Brazil) via the pulmo-nary artery. The whole lung was then homogenized usingBrinkmann tissue homogenizer (Polytron, Maryland, USA)(1×40 s, at a setting of 30, using 3 mL g−1 of PBS contain-ing 0.5 % of hexadecyltrimethylammonium bromide and5 mM EDTA, pH 6.0). The homogenized samples weresonicated (Vibra-Cell, Sonics & Materials, Newtown, CT,USA) for 3×2 min at 40 Hz and then centrifuged at 37,000×g
Lasers Med Sci (2013) 28:551–564 553

for 15 min. Lung myeloperoxidase activity was measured inthe supernatant by the method described by Henson andcoworkers [21]. Briefly, the samples of lung homogenateswere incubated with H2O2 and orthodianisidine, and the reac-tion was stopped after 15 min by adding NaNO3 (1 %).Absorbance was determined by fluorimeter (Edmund OpticsInc., Barrington, NJ, USA) at an optical density (O.D.) of460 nm.
Pulmonary microvascular leakage
Pulmonary vascular permeability was assessed by Evans bluedye extravasation. In brief, Evans blue dye (25 mg kg−1;Sigma, St. Louis, MO, USA) was administered intravenously5 min before the animals were killed. At the different timesafter reperfusion commenced (30 min, 2, and 4 h), the ratswere killed, the lungs were perfused as described above, andtwo samples of parenchyma were removed. Both sampleswere weighed, and then one was placed in formamide(4 mL g−1 wet weight; Invitrogen, São Paulo) at 20 °C for24 h, and the other was oven dried (60 °C) until it reached aconstant weight. The concentration of Evans blue dyeextracted in formamide was determined by spectrophotometryat a wavelength of 620 nm, using a standard dilution of Evansblue in formamide (0.3–100 μg mL−1). The fresh weight/dryweight ratio of each lung sample was determined (edemaindex) and used in the final calculation of Evans blue/gramdry weight of tissue, to avoid underestimating changes due toedema.
Real-time PCR
Elapsed 30 min, 2, and 4 h after beginning intestinal reper-fusion, the thoracic cavity of the rats was exposed, and theheart and lungs were removed en bloc. The pulmonaryartery was cannulated, after which the pulmonary vascula-ture was perfused with ice-cold sterile PBS using a peristal-tic pump (Thermo Fisher Scientific, Suwanee, GA, USA) toremove the intravascular blood. Lung fragments were cutinto 5-mm pieces using a tissue chopper, flash frozen inliquid nitrogen, and stored at −80 °C for real-time PCR (RT-PCR; Agilent Technologies, NW, USA) analysis of geneexpression. After 30 min, 2, and 4 h of intestinal reperfu-sion, the lungs were removed and processed for RT-PCR. Tothis end, total RNAwas isolated from the lung using TRIzolreagent (Gibco BRL, Gaithersburg, MD), following themanufacturer's protocol. RNA was subjected to DNase Idigestion, followed by reverse transcription to cDNA, aspreviously described by Cayla and colleagues [22]. PCRwas performed in a 7000 Sequence Detection System (ABIPrism, Applied Biosystems, Foster City, CA, USA) usingthe SYBR® Green core reaction kit (Applied Biosystems).
All the primers were purchased from R&D Systems, Min-neapolis, MN, USA. The primers used for ICAM-1 mRNAquantification were ICAM-1 forward 5′-AGACACAAG-CAAGAGAAGAAAAGG-3′ and reverse primer 5′-TTGGGAACAAAGGTAGGAATGTAT-3′ (GenBankTM
accession number NW047658), while the primers forTNF-α mRNA quantification were TNF forward 5′-AAATGGGCTCCCTCTATCAGTTC-3′ and reverse primer5′-TCTGCTTGGTGGTTTGCTACGAC-3′ (GenBankTM
accession number D00475). The primers for IL-10 mRNAquantification were forward primer 5′-TGACAATAACTGCACCCACTT-3′ and reverse primer 5′-TCATTCATGGCCTTGTAGACA-3′ (GenBankTM accession numberNW036214). The primers used for iNOS mRNA quantifi-cation were forward primer 5′-AAGTCCCTCACCCTCCCAAAAG-3′ and reverse primer 5′-GGCTGGACTTTTCACTGC-3′ (GenBankTM accession number J00691).GAPDH-3474-3570 (GenBankTM accession numberJ00691) forward primer 5′-AAGTCCCTCACCCTCCCAAAAG-3′ and reverse primer 5′-AAGCAATGCTCACCTTCCC-3′) as naive were also used. Quantitativevalues for ICAM-1, TNF-α, IL-10, and GAPDH mRNAtranscription were obtained from the threshold cycle num-ber, where the increase in the signal associated with theexponential growth of PCR products begins to becomedetectable. Melting curves were generated at the end ofevery run to ensure product uniformity. The relative targetgene expression level was normalized on the basis ofGAPDH expression as endogenous RNA control. ΔCt val-ues of the samples were determined by subtracting theaverage Ct value of ICAM-1, TNF-α, IL-10, and iNOSmRNA from the average Ct value of the internal controlGAPDH. Because ΔCt is not usually employed as relativedata due to this logarithmic characteristic, the 2−ΔCt param-eter was used to express the relative expression data. Theresults are expressed as a ratio relative to the sum ofGAPDH transcription level as an internal control.
Enzyme-linked immunoassay absorbance
Protein levels in lung the homogenates were measured byspecific rat TNF-α and IL-10 enzyme-linked immunoassay(ELISA) kit (R&D Systems, Minneapolis, MN, USA),according to manufacturer's instructions.
Statistical analysis
Statistical differences were evaluated by analysis of varianceand the Tukey–Kramer multiple comparisons test to deter-mine differences between groups. The results were consid-ered significant when p<0.05.
554 Lasers Med Sci (2013) 28:551–564
Results
Effect of i-I/R on tracheal reactivity
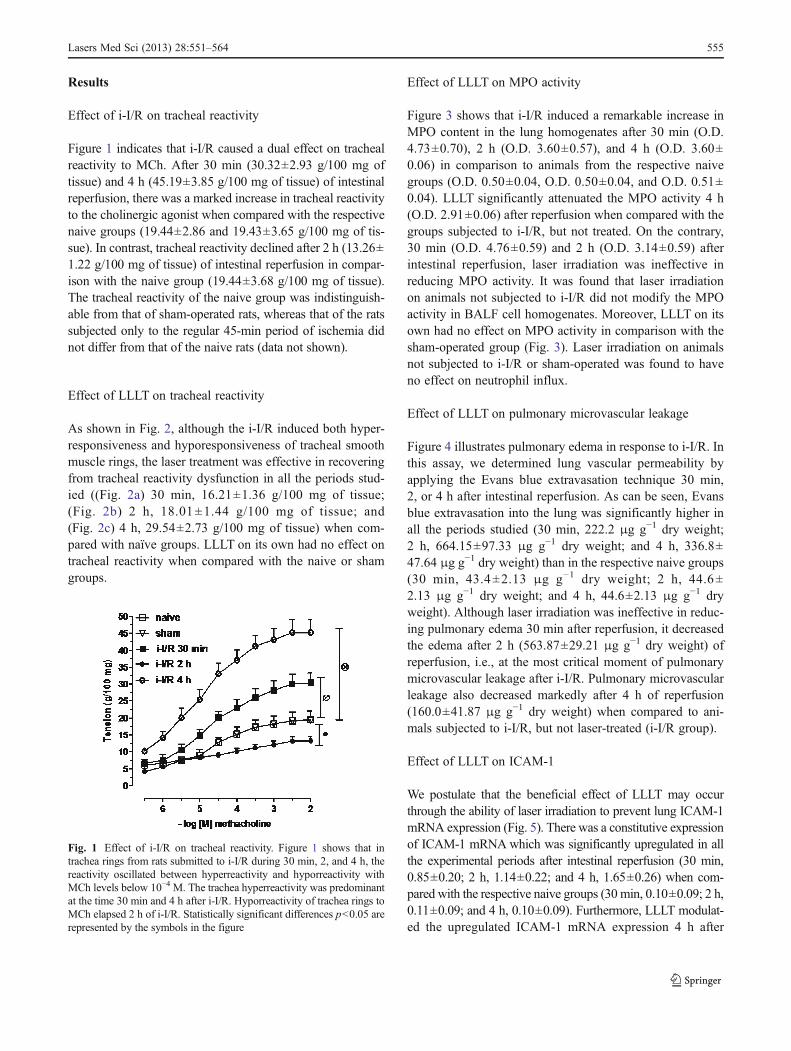
Figure 1 indicates that i-I/R caused a dual effect on trachealreactivity to MCh. After 30 min (30.32±2.93 g/100 mg oftissue) and 4 h (45.19±3.85 g/100 mg of tissue) of intestinalreperfusion, there was a marked increase in tracheal reactivityto the cholinergic agonist when compared with the respectivenaive groups (19.44±2.86 and 19.43±3.65 g/100 mg of tis-sue). In contrast, tracheal reactivity declined after 2 h (13.26±1.22 g/100 mg of tissue) of intestinal reperfusion in compar-ison with the naive group (19.44±3.68 g/100 mg of tissue).The tracheal reactivity of the naive group was indistinguish-able from that of sham-operated rats, whereas that of the ratssubjected only to the regular 45-min period of ischemia didnot differ from that of the naive rats (data not shown).
Effect of LLLT on tracheal reactivity
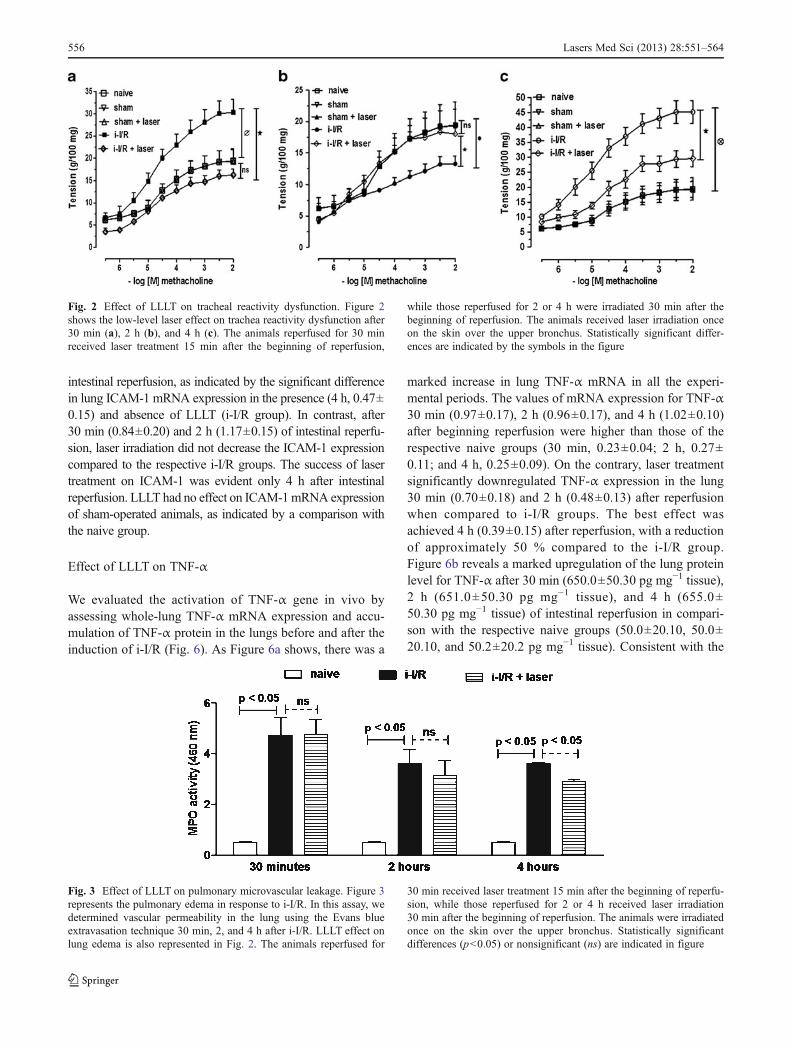
As shown in Fig. 2, although the i-I/R induced both hyper-responsiveness and hyporesponsiveness of tracheal smoothmuscle rings, the laser treatment was effective in recoveringfrom tracheal reactivity dysfunction in all the periods stud-ied ((Fig. 2a) 30 min, 16.21±1.36 g/100 mg of tissue;(Fig. 2b) 2 h, 18.01±1.44 g/100 mg of tissue; and(Fig. 2c) 4 h, 29.54±2.73 g/100 mg of tissue) when com-pared with naïve groups. LLLT on its own had no effect ontracheal reactivity when compared with the naive or shamgroups.
Effect of LLLT on MPO activity
Figure 3 shows that i-I/R induced a remarkable increase inMPO content in the lung homogenates after 30 min (O.D.4.73±0.70), 2 h (O.D. 3.60±0.57), and 4 h (O.D. 3.60±0.06) in comparison to animals from the respective naivegroups (O.D. 0.50±0.04, O.D. 0.50±0.04, and O.D. 0.51±0.04). LLLT significantly attenuated the MPO activity 4 h(O.D. 2.91±0.06) after reperfusion when compared with thegroups subjected to i-I/R, but not treated. On the contrary,30 min (O.D. 4.76±0.59) and 2 h (O.D. 3.14±0.59) afterintestinal reperfusion, laser irradiation was ineffective inreducing MPO activity. It was found that laser irradiationon animals not subjected to i-I/R did not modify the MPOactivity in BALF cell homogenates. Moreover, LLLT on itsown had no effect on MPO activity in comparison with thesham-operated group (Fig. 3). Laser irradiation on animalsnot subjected to i-I/R or sham-operated was found to haveno effect on neutrophil influx.
Effect of LLLT on pulmonary microvascular leakage
Figure 4 illustrates pulmonary edema in response to i-I/R. Inthis assay, we determined lung vascular permeability byapplying the Evans blue extravasation technique 30 min,2, or 4 h after intestinal reperfusion. As can be seen, Evansblue extravasation into the lung was significantly higher inall the periods studied (30 min, 222.2 μg g−1 dry weight;2 h, 664.15±97.33 μg g−1 dry weight; and 4 h, 336.8±47.64 μg g−1 dry weight) than in the respective naive groups(30 min, 43.4±2.13 μg g−1 dry weight; 2 h, 44.6±2.13 μg g−1 dry weight; and 4 h, 44.6±2.13 μg g−1 dryweight). Although laser irradiation was ineffective in reduc-ing pulmonary edema 30 min after reperfusion, it decreasedthe edema after 2 h (563.87±29.21 μg g−1 dry weight) ofreperfusion, i.e., at the most critical moment of pulmonarymicrovascular leakage after i-I/R. Pulmonary microvascularleakage also decreased markedly after 4 h of reperfusion(160.0±41.87 μg g−1 dry weight) when compared to ani-mals subjected to i-I/R, but not laser-treated (i-I/R group).
Effect of LLLT on ICAM-1
We postulate that the beneficial effect of LLLT may occurthrough the ability of laser irradiation to prevent lung ICAM-1mRNA expression (Fig. 5). There was a constitutive expressionof ICAM-1 mRNAwhich was significantly upregulated in allthe experimental periods after intestinal reperfusion (30 min,0.85±0.20; 2 h, 1.14±0.22; and 4 h, 1.65±0.26) when com-pared with the respective naive groups (30 min, 0.10±0.09; 2 h,0.11±0.09; and 4 h, 0.10±0.09). Furthermore, LLLT modulat-ed the upregulated ICAM-1 mRNA expression 4 h after
Fig. 1 Effect of i-I/R on tracheal reactivity. Figure 1 shows that intrachea rings from rats submitted to i-I/R during 30 min, 2, and 4 h, thereactivity oscillated between hyperreactivity and hyporreactivity withMCh levels below 10−4 M. The trachea hyperreactivity was predominantat the time 30 min and 4 h after i-I/R. Hyporreactivity of trachea rings toMCh elapsed 2 h of i-I/R. Statistically significant differences p<0.05 arerepresented by the symbols in the figure
Lasers Med Sci (2013) 28:551–564 555
intestinal reperfusion, as indicated by the significant differencein lung ICAM-1 mRNA expression in the presence (4 h, 0.47±0.15) and absence of LLLT (i-I/R group). In contrast, after30 min (0.84±0.20) and 2 h (1.17±0.15) of intestinal reperfu-sion, laser irradiation did not decrease the ICAM-1 expressioncompared to the respective i-I/R groups. The success of lasertreatment on ICAM-1 was evident only 4 h after intestinalreperfusion. LLLT had no effect on ICAM-1mRNA expressionof sham-operated animals, as indicated by a comparison withthe naive group.
Effect of LLLT on TNF-α
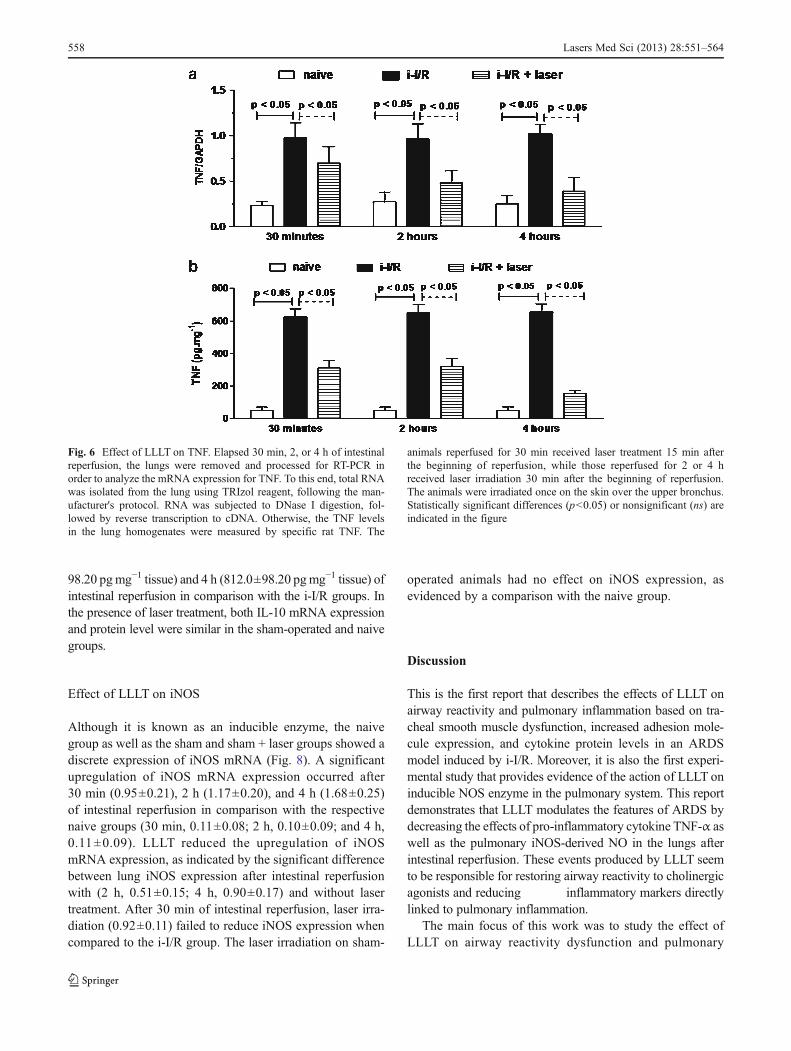
We evaluated the activation of TNF-α gene in vivo byassessing whole-lung TNF-α mRNA expression and accu-mulation of TNF-α protein in the lungs before and after theinduction of i-I/R (Fig. 6). As Figure 6a shows, there was a
marked increase in lung TNF-α mRNA in all the experi-mental periods. The values of mRNA expression for TNF-α30 min (0.97±0.17), 2 h (0.96±0.17), and 4 h (1.02±0.10)after beginning reperfusion were higher than those of therespective naive groups (30 min, 0.23±0.04; 2 h, 0.27±0.11; and 4 h, 0.25±0.09). On the contrary, laser treatmentsignificantly downregulated TNF-α expression in the lung30 min (0.70±0.18) and 2 h (0.48±0.13) after reperfusionwhen compared to i-I/R groups. The best effect wasachieved 4 h (0.39±0.15) after reperfusion, with a reductionof approximately 50 % compared to the i-I/R group.Figure 6b reveals a marked upregulation of the lung proteinlevel for TNF-α after 30 min (650.0±50.30 pg mg−1 tissue),2 h (651.0±50.30 pg mg−1 tissue), and 4 h (655.0±50.30 pg mg−1 tissue) of intestinal reperfusion in compari-son with the respective naive groups (50.0±20.10, 50.0±20.10, and 50.2±20.2 pg mg−1 tissue). Consistent with the
Fig. 3 Effect of LLLT on pulmonary microvascular leakage. Figure 3represents the pulmonary edema in response to i-I/R. In this assay, wedetermined vascular permeability in the lung using the Evans blueextravasation technique 30 min, 2, and 4 h after i-I/R. LLLT effect onlung edema is also represented in Fig. 2. The animals reperfused for
30 min received laser treatment 15 min after the beginning of reperfu-sion, while those reperfused for 2 or 4 h received laser irradiation30 min after the beginning of reperfusion. The animals were irradiatedonce on the skin over the upper bronchus. Statistically significantdifferences (p<0.05) or nonsignificant (ns) are indicated in figure
Fig. 2 Effect of LLLT on tracheal reactivity dysfunction. Figure 2shows the low-level laser effect on trachea reactivity dysfunction after30 min (a), 2 h (b), and 4 h (c). The animals reperfused for 30 minreceived laser treatment 15 min after the beginning of reperfusion,
while those reperfused for 2 or 4 h were irradiated 30 min after thebeginning of reperfusion. The animals received laser irradiation onceon the skin over the upper bronchus. Statistically significant differ-ences are indicated by the symbols in the figure
556 Lasers Med Sci (2013) 28:551–564

mRNA expression data, LLLT reduced the TNF-α protein inthe lung after 30 min (310.0±50.10 pg mg−1 tissue) and 2 h(321.0±50.10 pg mg−1 tissue) of intestinal reperfusion whencompared to the i-I/R groups. When the TNF-α protein levelin the lung was measured 4 h after intestinal reperfusion, theresults demonstrated that LLLT (153.0±21.0 pg mg−1 tis-sue) induced an almost fivefold greater reduction than thevalues obtained in the i-I/R group. In the presence of laser,the TNF-α mRNA expression and the protein level weresimilar in both the sham-operated and naive groups.
Effect of LLLT on IL-10
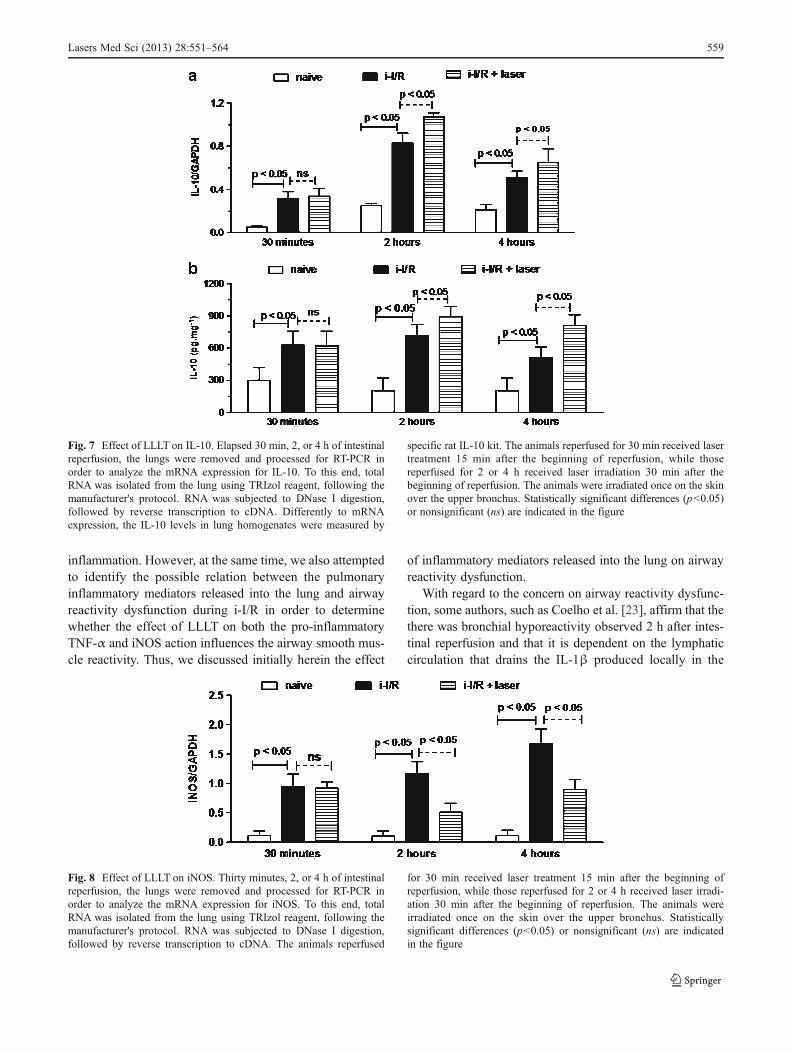
In this study, IL-10 mRNA and protein level were detectedconstitutively and were upregulated after i-I/R (Fig. 7). Asshown in Fig. 7a, the mRNA expression for IL-10 remainedconstantly higher after intestinal reperfusion (30 min, 0.32±
0.06; 2 h, 0.83±0.09; and 4 h, 0.51±0.06) than in therespective naive groups (0.15±0.06, 0.25±0.02, and 0.21±0.05). LLLT appeared to have had no effect on increased IL-10 expression 30 min (0.34±0.07) after i-I/R, whereas lasertreatment appeared to have an additive effect on the upregu-lated IL-10 mRNA expression 2 h (1.07±0.04) and 4 h(0.65±0.13) after intestinal reperfusion. With regard to theIL-10 protein level, Fig. 7b shows a significant upregulationof this cytokine in the lungs after 30 min (625.1±133.10 pg mg−1 tissue), 2 h (720.0±98.20 pg mg−1 tissue),and 4 h (510.0±98.20 pg mg−1 tissue) of intestinal reperfu-sion when compared to the respective naive groups (300.0±121.60, 200.0±121.60, and 205.2±122.1 pg mg−1 tissue).Consistent with the mRNA data, LLLT did not reduce theupregulated level of IL-10 protein after 30 min of i-I/R(622.10±133.10 pg mg−1 tissue). However, the laser treatmentfurther increased the IL-10 in the lungs after 2 h (890.0±
Fig. 5 Effect of LLLT on ICAM-1. Elapsed 30 min, 2, or 4 h ofintestinal reperfusion, the lungs were removed and processed for RT-PCR in order to analyze the mRNA expression for ICAM-1. To thisend, total RNA was isolated from the lung using TRIzol reagent,following the manufacturer's protocol. RNA was subjected to DNaseI digestion, followed by reverse transcription to cDNA. The animals
reperfused for 30 min received laser treatment 15 min after the begin-ning of reperfusion, while those reperfused for 2 or 4 h received laserirradiation 30 min after the beginning of reperfusion. The animals wereirradiated once on the skin over the upper bronchus. Statisticallysignificant differences (p<0.05) or nonsignificant (ns) are indicatedin the figure
Fig. 4 Effect of LLLT on MPO activity. Neutrophil recruitment to thelung was assessed by measuring MPO activity in the lung. Samples oflung were removed from rats killed 30 min, 2, and 4 h after i-I/R andprocessed. Lung myeloperoxidase activity was measured in the super-natant, and it was determined at an optical density (O.D.) of 460 nm.The animals reperfused for 30 min received laser treatment 15 min
after the beginning of reperfusion, while those reperfused for 2 or 4 hreceived laser irradiation 30 min after the beginning of reperfusion.The animals were irradiated once on the skin over the upper bronchus.Statistically significant differences (p<0.05) or nonsignificant (ns) areindicated in the figure
Lasers Med Sci (2013) 28:551–564 557
98.20 pgmg−1 tissue) and 4 h (812.0±98.20 pgmg−1 tissue) ofintestinal reperfusion in comparison with the i-I/R groups. Inthe presence of laser treatment, both IL-10 mRNA expressionand protein level were similar in the sham-operated and naivegroups.
Effect of LLLT on iNOS
Although it is known as an inducible enzyme, the naivegroup as well as the sham and sham + laser groups showed adiscrete expression of iNOS mRNA (Fig. 8). A significantupregulation of iNOS mRNA expression occurred after30 min (0.95±0.21), 2 h (1.17±0.20), and 4 h (1.68±0.25)of intestinal reperfusion in comparison with the respectivenaive groups (30 min, 0.11±0.08; 2 h, 0.10±0.09; and 4 h,0.11±0.09). LLLT reduced the upregulation of iNOSmRNA expression, as indicated by the significant differencebetween lung iNOS expression after intestinal reperfusionwith (2 h, 0.51±0.15; 4 h, 0.90±0.17) and without lasertreatment. After 30 min of intestinal reperfusion, laser irra-diation (0.92±0.11) failed to reduce iNOS expression whencompared to the i-I/R group. The laser irradiation on sham-
operated animals had no effect on iNOS expression, asevidenced by a comparison with the naive group.
Discussion
This is the first report that describes the effects of LLLT onairway reactivity and pulmonary inflammation based on tra-cheal smooth muscle dysfunction, increased adhesion mole-cule expression, and cytokine protein levels in an ARDSmodel induced by i-I/R. Moreover, it is also the first experi-mental study that provides evidence of the action of LLLT oninducible NOS enzyme in the pulmonary system. This reportdemonstrates that LLLT modulates the features of ARDS bydecreasing the effects of pro-inflammatory cytokine TNF-α aswell as the pulmonary iNOS-derived NO in the lungs afterintestinal reperfusion. These events produced by LLLT seemto be responsible for restoring airway reactivity to cholinergicagonists and reducing inflammatory markers directlylinked to pulmonary inflammation.
The main focus of this work was to study the effect ofLLLT on airway reactivity dysfunction and pulmonary
Fig. 6 Effect of LLLT on TNF. Elapsed 30 min, 2, or 4 h of intestinalreperfusion, the lungs were removed and processed for RT-PCR inorder to analyze the mRNA expression for TNF. To this end, total RNAwas isolated from the lung using TRIzol reagent, following the man-ufacturer's protocol. RNA was subjected to DNase I digestion, fol-lowed by reverse transcription to cDNA. Otherwise, the TNF levelsin the lung homogenates were measured by specific rat TNF. The
animals reperfused for 30 min received laser treatment 15 min afterthe beginning of reperfusion, while those reperfused for 2 or 4 hreceived laser irradiation 30 min after the beginning of reperfusion.The animals were irradiated once on the skin over the upper bronchus.Statistically significant differences (p<0.05) or nonsignificant (ns) areindicated in the figure
558 Lasers Med Sci (2013) 28:551–564
inflammation. However, at the same time, we also attemptedto identify the possible relation between the pulmonaryinflammatory mediators released into the lung and airwayreactivity dysfunction during i-I/R in order to determinewhether the effect of LLLT on both the pro-inflammatoryTNF-α and iNOS action influences the airway smooth mus-cle reactivity. Thus, we discussed initially herein the effect
of inflammatory mediators released into the lung on airwayreactivity dysfunction.
With regard to the concern on airway reactivity dysfunc-tion, some authors, such as Coelho et al. [23], affirm that thethere was bronchial hyporeactivity observed 2 h after intes-tinal reperfusion and that it is dependent on the lymphaticcirculation that drains the IL-1β produced locally in the
Fig. 8 Effect of LLLT on iNOS. Thirty minutes, 2, or 4 h of intestinalreperfusion, the lungs were removed and processed for RT-PCR inorder to analyze the mRNA expression for iNOS. To this end, totalRNA was isolated from the lung using TRIzol reagent, following themanufacturer's protocol. RNA was subjected to DNase I digestion,followed by reverse transcription to cDNA. The animals reperfused
for 30 min received laser treatment 15 min after the beginning ofreperfusion, while those reperfused for 2 or 4 h received laser irradi-ation 30 min after the beginning of reperfusion. The animals wereirradiated once on the skin over the upper bronchus. Statisticallysignificant differences (p<0.05) or nonsignificant (ns) are indicatedin the figure
Fig. 7 Effect of LLLT on IL-10. Elapsed 30 min, 2, or 4 h of intestinalreperfusion, the lungs were removed and processed for RT-PCR inorder to analyze the mRNA expression for IL-10. To this end, totalRNA was isolated from the lung using TRIzol reagent, following themanufacturer's protocol. RNA was subjected to DNase I digestion,followed by reverse transcription to cDNA. Differently to mRNAexpression, the IL-10 levels in lung homogenates were measured by
specific rat IL-10 kit. The animals reperfused for 30 min received lasertreatment 15 min after the beginning of reperfusion, while thosereperfused for 2 or 4 h received laser irradiation 30 min after thebeginning of reperfusion. The animals were irradiated once on the skinover the upper bronchus. Statistically significant differences (p<0.05)or nonsignificant (ns) are indicated in the figure
Lasers Med Sci (2013) 28:551–564 559

intestine and carries it into pulmonary circulation. Still aboutbronchial hyporeactivity, Coelho et al. [23] stated that intes-tinal reperfusion-derived IL-1β can stimulate pulmonaryiNOS and that iNOS-derived NO is responsible for decreas-ing the contractile response of the airway smooth muscle tocholinergic agonists.
Reports about the effects of NO in i-I/R have beendescribed by Cuzzocrea et al. [11], who showed that inresponse to i-I/R, NO causes hypotension and hyporespon-siveness to vasoconstricting agents. In this sense, Ameredesand colleagues [24] demonstrated that enhanced NO pro-duction is associated with airway hyporesponsiveness in theabsence of IL-10 and that this effect is reversed by theinhibition of NO. In this condition, cNOS-derived NOseems to be responsible for airway hyporesponsiveness tomethacholine. In the absence of IL-10, which is also able tominimize TNF-α-induced airway hyperreactivity [24], theproduction of NO is increased as a compensatory mechanismto control the airway tonus against hyperresponsiveness.
Regarding the involvement of NO in lung inflammation,Cavriani and colleagues [10] indicated that during intestinalischemia/reperfusion, both constitutive and inducible NOSisoforms are called to exert a differential modulatory effect.Further evidence of the role of iNOS-derived NO in i-I/Rwas reported by Cavriani and colleagues [11], who foundthat the inhibition of NO synthesis by L-NAME significantlyincreased the mortality rate of rats subjected to 2 h ofintestinal reperfusion. On the other hand, during intestinalreperfusion, there is a substantial production and release ofiNOS-derived NO. Moreover, Cavriani and colleagues [10]demonstrated a significant reduction of lung edema fromrats pretreated with different doses of iNOS inhibitor andsubjected to intestinal reperfusion.
Our results suggest that the protection of the airwaysafforded by pulmonary cNOS-derived NO reported byCavriani and coworkers [10] is not very effective in control-ling tracheal hyperreactivity observed after 30 min of i-I/R.This indicates that it is possible that the effect of NO derivedfrom iNOS is responsible for the airway hyperreactivity ob-served 4 h after reperfusion, since iNOS mRNA expressionwas significantly augmented in this period.
With regard to the effect of anti-inflammatory cytokineIL-10 and NO on airway reactivity dysfunction, Ameredesand coworkers [22] demonstrated that enhanced NO pro-duction is associated with airway hyporesponsiveness in theabsence of IL-10 and that this effect was reversed by NOinhibition. Our results showed a significant increase in IL-10 protein and mRNA expression after intestinal reperfusionin all the experimental periods. The same was observed iniNOS mRNA expression. As expected, IL-10 protein andmRNA levels remained high in all the experimental periodsafter intestinal reperfusion, since the pro-inflammatorymediators are a principal stimulus to production of IL-10.
Curiously, 2 h after intestinal reperfusion, the production ofthis anti-inflammatory cytokine was higher than at the othertimes studied here. This may be explained by the absence ofcNOS-derived NO, since Coelho et al. [22] demonstratedthat after 2 h of intestinal reperfusion, pulmonary cNOSexpression did not increase and that the pulmonary systemattempted to control the airway dysfunction by increasingIL-10 production, which is able to modulate exacerbatediNOS-derived NO synthesis.
Finally, 4 h after intestinal reperfusion, tracheal reactivityreturned to much higher levels than those presented 30 minafter reperfusion, i.e., more pronounced airway hyperres-ponsiveness. At this time, pulmonary IL-10 protein andmRNA expression were high but lower than those observed2 h after reperfusion. With a lower concentration of IL-10,tracheal reactivity tends to increase. Our results show that i-I/R-induced smooth muscle dysfunction culminated in trachealhyperreactivity.
iNOS-derived NO is related to functional changes oftracheal reactivity, and our results suggest that it may bean adaptive response of the pulmonary system to i-I/R,which modulates the smooth muscle tone. Our results alsosuggest that iNOS participated in the hyperresponsivenessobserved 30 min and 4 h after intestinal reperfusion but thatIL-10 played an important role in the compensatory re-sponse to counterbalance the increase in airway reactivityobserved 2 h after reperfusion. Four hours after intestinalreperfusion, tracheal hyperresponsiveness became acute,probably because of the continuing high levels of bothTNF-α and iNOS and the fact that IL-10 protein and mRNAexpression, which are able to control the effect of pro-inflammatory cytokines, were reduced to lower levels incomparison to the other reperfusion periods.
With regard to lung inflammation, ICAM-1 mRNA expres-sion has been evidenct in experimental i-I/R models by severalauthors [25, 26]. The results of the current study are consistentwith those of the above cited authors, since they revealed asignificant increase in ICAM-1 mRNA expression and proteinin all the experimental periods after intestinal reperfusion. Aresult that strongly suggests that the decline in pulmonaryneutrophils elicited by lasermay be related directly to the effectof this therapy on the interaction of leukocytes with endothelialcells is the fact that LLLT markedly reduced ICAM-1 mRNAexpression in the lung after i-I/R. This was observed only 4 hafter intestinal reperfusion. Based on these results, it is reason-able to suggest that LLLT attenuates lung inflammation by amechanism driven by leukocyte–endothelium interaction pro-moted by TNF generation in lungs.
A significant increase in MPO activity has been describedas an indirect measure of neutrophil influx in different periodsafter intestinal reperfusion [27]. The intestinal I/R events inthe pulmonary vasculature augmented the pulmonary vascularpermeability, culminating in microvascular leakage and
560 Lasers Med Sci (2013) 28:551–564

facilitating the migration of pro-inflammatory cells into thelungs. Our results are consistent with those of Cavriani et al.[28], who demonstrated that 2 or 4 h after intestinal reperfu-sion, neutrophil influx and pulmonary microvascular leakagewere considerably increased compared to those of healthyanimals. The abovementioned authors found no a change inMPO activity or lung edema 30 min after intestinal reperfu-sion. In contrast, our results demonstrated a significant in-crease in both MPO activity and lung edema in the initialphase of reperfusion. These results converge with those ofSouza et al. [27], who also reported changes in both MPOactivity and lung edema shortly after intestinal reperfusion.This increase in MPO activity is probably more related toactivated mast cells and alveolar macrophages that can releaseTNF-α, an important chemoattractant for neutrophils that issubsequently recruited to the lungs. Recently, we demonstrat-ed a significant damage in pulmonary endothelial cells fromrats after intestinal reperfusion, characterized by endothelialcytoskeleton retraction with loss of cell-to-cell contact (datanot shown). Consequently, this further compromises the pul-monary vascular permeability.
Some studies have attempted to determine which cellularsignal is responsible for the anti-inflammatory effect of LLLTon airway reactivity dysfunction and pulmonary inflammationin different experimental models. In the condition of TNF-induced airway dysfunction, we demonstrated that laser ther-apy restored the relaxation capacity of rat bronchi segments byincreasing cAMP [29]. We have shown the effectiveness ofLLLT both in reducing airway hyperreactivity and in restoringthe ability of smooth muscle to relax when stimulated by β2-adrenergic agonist through a NF-κB-dependent mechanism[30]. In TNF-α-induced ARDS, LLLT reduced bronchialhyperreactivity through a mechanism that involves dimin-ished calcium sensitivity as well as the expression of inositoltriphosphate (IP3) receptor [31].
With regard to lung inflammation and the beneficialeffects of LLLT, we have demonstrated, in ARDS elicitedby immune-complex reaction in rat, that laser reduces MPOactivity and TNF-α levels and also attenuates hemorrhagicpulmonary lesion [32, 33]. In LPS-induced ARDS, LLLTdecreases pulmonary microvascular leakage, neutrophil in-flux, and IL-1β levels in the airway and lungs of ratssubjected to LPS-induced inflammation [34]. Moreover,laser treatment decreases levels of lung neutrophil antiapop-totic factors in a model of rat lung inflammation induced byintravenous injection of LPS from Escherichia coli [35]. Wehave also demonstrated in vivo that LLLT reduces lungedema and neutrophil influx and that in vitro it attenuatesthe disruption of the pulmonary endothelial barrier, restoringendothelial integrity [36].
The findings of our present work revealed that laser irradi-ation applied noninvasively can control airway smooth muscledysfunction and pulmonary inflammation induced by i-I/R.
Laser treatment reduced tracheal hyperresponsiveness as wellas hyporesponsiveness to the cholinergic agonist. Moreover,laser therapy also reduced both myeloperoxidase activity andlung edema.
As expected for an in vivo treatment, the laser does notaffect MPO activity or lung edema 30 min after intestinalreperfusion. This is probably because 30 min is not anenough time for the laser to interact with the lung andproduce a beneficial effect. Nevertheless, LLLT reducedboth TNF-α protein and mRNA expression in the same timeperiod, i.e., 30 min after intestinal reperfusion. Despite theineffectiveness of laser treatment on edema and MPO activ-ity 30 min after intestinal reperfusion, this does not meanthat laser irradiation cannot act on inflammatory mediatorsreleased by cells in the lungs after intestinal reperfusion,particularly activated alveolar macrophages. Lastly, i.e., 4 hafter intestinal reperfusion, the laser-irradiated animals pre-sented significantly lower MPO activity than the animalssubjected only to i-I/R. These preliminary results allow us tohypothesize that LLLT may interfere with one of the pro-cesses linked to cellular migration. In addition, the effect ofLLLT on MPO activity observed 4 h after intestinal reper-fusion may have been due to late cellular response againstTNF-α production by alveolar macrophages (resident cells)stimulated after reperfusion.
As for the effect of LLLT on TNF-α production inducedby intestinal reperfusion, our results demonstrated thatLLLT reduced TNF-α mRNA expression in inflamed lungtissue after i-I/R. mRNA expression measured by the RT-PCR technique does not detect the presence of the protein inthe lung because, although mRNAwas expressed, there is anatural delay in the protein synthesis. Therefore, this studyalso evaluated the concentration of TNF-α and IL-10 pro-tein in the lung homogenates assessed by ELISA, whichindicated that LLLT is truly effective in reducing thesecytokines. An interesting study by Frangogiannis andcoworkers [37] showed that mast cells are an importantearly source of TNF-α during ischemia and reperfusion.In this regard, an initial tissue release of TNF-α, possiblymast cell-derived, may be essential and sufficient for anearly wave of neutrophil influx to occur, after which afeedback process is established in which neutrophil influxfacilitates TNF-α production, which in turn facilitatesneutrophil influx. The results described herein indicatethat laser irradiation was more effective in influencingTNF-α expression and protein than in interfering in MPOactivity. This suggests that the reduction of neutrophilinflux by LLLT is, at least in part, a mechanism whoseaction is dependent on TNF-α. Therefore, we cannotdiscard the hypothesis that the beneficial effect of LLLTin reducing the neutrophil influx observed later (4 h afterreperfusion) could be initiated by the reduction of TNF-αproduced by mast cells in an early phase of i-I/R.
Lasers Med Sci (2013) 28:551–564 561

Our findings concerning IL-10 mRNA expression in thelung from animals subjected to i-I/R showed that this cyto-kine was significantly increased in comparison with in-flamed but nonirradiated animals. The same response wasobserved in IL-10 protein in the lung homogenates. Theseresults are consistent with those reported by Souza andcolleagues [38], who demonstrated the enhancement of thisanti-inflammatory cytokine in the lungs of animals sub-jected to severe i-I/R. Surprisingly, LLLT induced an in-crease in IL-10 to a higher concentration than that found inanimals with II/R-induced lung inflammation. These resultsare interesting because, as mentioned earlier, the presence ofTNF-α in conditions of inflammation causes IL-10 to in-crease in order to counteract the deleterious effect of TNF-α. Moreover, most of the studies using animal modelsrecognize that an increase in TNF-α is usually accompaniedby increased IL-10 [9]. Our results corroborate the findingsof these authors, since we observed that both TNF-α and IL-10 increased 4 hx after reperfusion. In view of this fact, itwas expected that the IL-10 level would also decline afterLLLT, since with less TNF-α, the anti-inflammatory IL-10in the lung also could be reduced. However, LLLT presentedthe opposite outcome. This result indicates the beneficialeffect of LLLT in i-I/R by another mechanism. The fact thatLLLT reduces the TNF-α level while simultaneously in-creasing IL-10 in the lungs seems to suggest a dual effectof laser therapy on these cytokines. In fact, it is possible thatLLLT acts by a distinct mechanism on each one. Recently,we demonstrated that LLLT presents a modulatory action onsome chemical mediators involved in lung inflammationsince it was able to restore the balance between Th1/Th2cytokines in acute lung inflammation induced by i-I/R [20].
It is well known that IL-10 can modulate MPO activityand pulmonary edema by controlling the effects of the pro-inflammatory cytokine TNF-α [9]. An interesting findingwas the upregulation of IL-10 anti-inflammatory cytokineby laser treatment. IL-10 upregulation after LLLT was evi-denct 2 and 4 h after intestinal reperfusion. The upregulationof IL-10 anti-inflammatory cytokine may be responsible forthe beneficial effect of laser on the tracheal reactivity andlung inflammation studied here. By upregulating IL-10,LLLT may indirectly reduce either TNF-α mRNA expres-sion or protein such as iNOS mRNA expression. Still withrespect to the effects of LLLT on pulmonary inflammationinduced by i-I/R, although ICAM-1 mRNA expression wassignificantly decreased, this occurred only 4 h after intesti-nal reperfusion. This period corresponds to the best effect ofLLLT on MPO activity and lung edema. Therefore, it ispossible that the beneficial effect of laser on MPO activityand lung edema observed 2 h after intestinal reperfusion isnot linked to the expression of adhesion molecules in endo-thelial pulmonary cells. It should be noted that in this study,we did not evaluate the effect of LLLT on inflammatory
mediators produced in tracheal segments. Thus, we cannotdiscard the possibility that laser controls tracheal reactivitydysfunction while simultaneously acting directly on airwaysmooth muscle. In addition, we did not evaluate the partic-ipation of serum TNF-α levels in i-I/R, in part, becauseCavriani and colleagues [28] found no correlation betweenserum TNF-α levels and lung edema. However, using dif-ferent models of pulmonary inflammation, we have shownpreviously that laser is not effective in reducing inflamma-tory mediators in serum [33]. Although, localized lasertherapy appears to be advantageous because it reaches onlythe airways and lungs, thus allowing for a better control oreven avoidance of a possible toxic effect of LLLT. Ourresults reinforce the proposal of localized treatment of lunginflammation with laser irradiation.
Concern on the time intervals of 15 and 30 min chosenafter initiating reperfusions for laser irradiation, we agreethat building a strategy of treatment with laser to try tocontrol the airway reactivity dysfunction and the lung in-flammation is a crucial point for obtaining beneficial effects.However, we recognized that the temporal course of induc-ing both bronchial hyperreactivity and lung inflammationvia intestinal reperfusion is an excellent experimental modelto mimic the acute lung inflammation, but it is not easy towork with laser because it has a short period of reperfusion(30 min) where it is possible to observe inflammatory cellsand mediators. However, it is a period very short for induc-ing a beneficial effect of laser therapy particularly when it isapplied in vivo. We applied laser shortly thereafter inductionof lung inflammation, and it was evident that laser does nothave the same efficacy. Otherwise, when we applied thelaser in a period very proximal to the final of reperfusion,it was not also able to control the lung inflammation. There-fore, we chose 15 min after intestinal reperfusion, i.e., thehalf of total period for irradiating the animals. With regardon the time of 2 and 4 h after intestinal reperfusion, thethought was the same explained anteriorly, but principallyherein, we irradiated the animals 30 min after reperfusion inorder to investigate how long is the laser able to control thebronchial reactivity dysfunction and lung inflammation inthese studied periods.
Although the results presented here were obtained froman experimental model, they provide information that justi-fies the proposal of laser therapy as an adjuvant in thenoninvasive treatment of acute lung inflammation. The ev-idence of the beneficial effects of laser therapy for patientswhose airways and lungs are compromised by acute inflam-mation cannot be discarded, despite the fact that there islittle information about how light can modulate the pulmo-nary inflammatory process by means of a few minutes ofradiation. With this in mind, it is clear that an understandingof the LLLT mechanism of action on acute lung injury afteri-I/R would be useful for the development of laser
562 Lasers Med Sci (2013) 28:551–564

irradiation as a novel adjuvant therapeutic strategy thatlimits lung injury caused by reperfusion. Moreover, its easyavailability, good reproducibility, cost-effectiveness, ab-sence of side effects, and safety make LLLT one of the mostpromising nonpharmacological therapies for I/R-related pul-monary diseases.
Generally, the compounds existing in the animal bodymay have a nonnegligible influence on the interaction of thelaser radiation with the animal's tissues. In fact, it is wellestablished that the physiological composition of both tissueand the corporal fluid interferes with physical parameters oflaser irradiation, such as for example absorption and scat-tering influences directly the quantity of light that attain thetarget tissue. Admitting that low-level laser can be widelyused as a coadjuvant therapy in clinical treatment of lungdisorders, the physiological composition of both tissue andthe corporal fluid will be a reality present all the time. Wehave experimentally demonstrated that LLLT reduces thelung inflammation and the airway hyperresponsivenessthrough a noninvasive way. Therefore, if the diode laser,the dosimetry, and strategy of treatment used for treatmentare appropriate, the target cellular is reached making viablethe beneficial effects with LLLT.
In conclusion, our general hypothesis is that LLLT con-trols tracheal reactivity and pulmonary inflammation bydownregulating the release of TNF-α pro-inflammatory cy-tokine and iNOS mRNA expression and upregulating IL-10anti-inflammatory cytokine in the lungs. Further studies inthis novel area of LLLT research are justified to determine ifthe action of laser irradiation in balancing pro- and anti-inflammatory cytokines and iNOS occurs by an independentmechanism.
Acknowledgments The authors acknowledge the financial supportof FAPESP (São Paulo State Research Foundation) through Grants2008/08048-4 and 2008/08838-5.
References
1. Ito K, Osaka H, Kojima N, Miura M (2003) Pharmacologicalpreconditioning protects lung injury induced by intestinal ische-mia/reperfusion in rat. Shock 19:462–468
2. Van Soeren M, Diehl-Jones W, Maykut R, Haddara W (2000)Pathophysiology and implications for treatment of acute respirato-ry distress syndrome. AACN Clin Issues 11:179–197
3. Tsushima K, King L, Aggarwal N, De Gorordo A, D’Alessio F,Kubo K (2009) Acute lung injury. Inter Med 48:621–630
4. Carden D, Granger D (2000) Pathophysiology of ischaemia-reperfusion injury. J Pathol 190:255–266
5. Van der Poll T, Lowry S (1995) Tumor necrosis factor in sepsis:mediator of multiple organ failure or essential part of host defense?Shock 3:1–12
6. Koksoy C, Kuzu M, Kuzu I, Ergun H, Gurhan I (2001) Role oftumour necrosis factor in lung injury caused by intestinalischaemia-reperfusion. Br J Surg 88:464–468
7. Yamamoto S, Tanabe M, Wakabayashi G, Shimazu M, MatsumotoK, Kitajima M (2001) The role of tumor necrosis factor-α andinterleukin-1β in ischemia/reperfusion injury of the rat small in-testine. J Surg Res 99:134–141
8. Oliveira-Junior I, Pinheiro B, Silva I, Salomão R, Zollner R,Beppu O (2003) Pentoxifylline decreases tumor necrosis factorand interleukin-1 during high tidal volume. Braz J Med Bio Res36:1349–1357
9. Souza D, Teixeira M (2005) The balance between the productionof tumor necrosis factor-alpha and interleukin-10 determines tissueinjury and lethality during intestinal ischemia and reperfusion.Mem Inst Oswaldo Cruz 100(Sup 1):59–66
10. Cavriani G, Oliveira-Filho R, Trezena A, da Silva Z, Domingos H,de Arruda M, Jancar S, Tavares de Lima W (2004) Lung micro-vascular permeability and neutrophil recruitment are differentlyregulated by nitric oxide in a rat model of intestinal ischemia-reperfusion. Eur J Pharmacol 494:241–249
11. Cuzzocrea S, Chatterjee P, Mazzon E, Dugo L, De Sarro L, Van deLoo A, Fons A, Caputi A, Thiemermann C (2002) Role of inducednitric oxide in the initiation of the inflammatory response after postischemic injury. Shock 18:169–176
12. Ke-seng Z, Huang X, Liu J, Huang Q, Jin C, Jiang J, Yong Z,Guiling Z (2002) New approach to treatment of shock—restitutionof vasoreactivity. Shock 18:189–192
13. Ricciardolo F, Di Stefano A, Sabatini F, Folkerts G (2006) Reac-tive nitrogen species in the respiratory tract. Eur J Pharmacol533:240–252
14. Tsushima K, King L, Aggarwal N, De Gorordo A, D’Alessio A,Kubo K (2009) Acute lung injury. Inter Med 48:621–630
15. Cazzola M, Polosa R (2006) Anti-TNF-alpha and Th1 cytokine-directed therapies for the treatment of asthma. Curr Opin AllergyClin Immunol 6:43–50
16. Bjordal J, Johnson M, Iversen V, Aimbire F, Lopes-Martins R(2006) Photoradiation in acute pain: a systemic review of possiblemechanisms of action and clinical effects in randomized placebo-controlled trials. Photomed Laser Surg 24:158–168
17. Chow R, Johnson M, Lopes-Martins R, Bjordal J (2009) Efficacyof low-level laser therapy in the management of neck pain: asystematic review and meta-analysis of randomised placebo oractive-treatment controlled trials. Lancet 374:1897–908
18. Ostronosova N (2006) Outpatient use of laser therapy in bronchialasthma. Ter Arkh 78:41–44
19. Nikitin A, Esaulenko I, Shatalova O (2008) Effectiveness of laserpuncture in elderly patients with bronchial asthma accompanied bychronic rhinosinusitis. Adv Gerontol 21:424–426
20. Henson P, Zanolari B, Schwartzman N, Hong S (1978) Intracellu-lar control of human neutrophil secretion. I. C5a-induced stimulus-specific desensitization and the effects of cytochalasin. J Immunol121:851–855
21. Cayla C, Merino V, Cabrini D, Silva A Jr, Pesquero P, Bader M(2002) Structure of the mammalian kinin receptor gene locus. IntImmunopharmacol 2:1721–1727
22. Coelho F, Cavriani G, Soares A, Teixeira A, Almeida P, Sudo-Hayashi L, Muscará M, Oliveira-Filho R, Vargaftig B, Tavares deLima W (2007) Lymphatic-borne IL-1β and the inducible isoformof nitric oxide synthase trigger the bronchial hyporresponsivenessafter intestinal ischemia/reperfusion in rats. Shock 28:694–699
23. Ameredes B, Zamora R, Sethi J, Liu H, Kohut L, Gligonic A, ChoiA, Calhoun W (2005) Alterations in nitric oxide and cytokineproduction with airway inflammation in the absence of IL-10. JImmunol 175:1206–1213
24. Guiqi G (2011) Pre-treatment with glutamine attenuates lung inju-ry in rats subjected to intestinal ischaemia–reperfusion. Injury41:72–77
25. Tian X, Yao J, Zhang X, Feng B, Yang C, Zheng S (2006) Effect ofnuclear factor kappa B on intercellular adhesion molecule-1
Lasers Med Sci (2013) 28:551–564 563

expression and neutrophil infiltration in lung injury induced byintestinal ischemia/reperfusion in rats. World J Gastroenterol12:388–392
26. Souza D, Lomez E, Pinho V, Pesquero J, Bader M, Pesquero M,Teixeira M (2004) Role of bradykinin B2 and B1 receptors in thelocal, remote, and systemic inflammatory responses that followintestinal ischemia and reperfusion injury. J Immunol 172:2542–2548
27. Cavriani G, Domingos H, Soares A, Trezena A, Ligeiro-OliveiraA, Oliveira-Filho R, Sudo-Hayashi L, Tavares de Lima W (2005)Lymphatic system as a path underlying the spread of ischemia/reperfusion in rats. Shock 23:330–336
28. Aimbire F, Bjordal J, Iversen V, Albertini R, Frigo L, Pacheco M,Castro-Faria-Neto H, Chavantes M, Labat R, Lopes-Martins R(2006) Low-level laser therapy partially restores trachea musclerelaxation response in rats with tumor necrosis factor alpha-mediated smooth airway muscle dysfunction. Lasers Surg Med38:773–778
29. Mafra de Lima F, Costa M, Albertini R, Silva J Jr, Aimbire F (2009)Low level laser therapy (LLLT): attenuation of cholinergic hyperre-activity, β2-adrenergic hyporesponsiveness and TNF-α mRNA ex-pression in rat bronchi segments in E. coli lipopolysaccharide-induced airway inflammation by a NF-κB dependent mechanism.Lasers Surg Med 41:68–74
30. Aimbire F, de Lima F, Costa M, Albertini R, Correa J, Iversen V,Bjordal J (2009) Effect of low level laser therapy on bronchialhyper-responsiveness. Lasers Med Sci 24:557–576
31. Aimbire F, Lopes-Martins R, Albertini R, Pacheco M, Castro-Faria-Neto H, Martins P, Bjordal J (2007) Effect of low-level lasertherapy on hemorrhagic lesions induced by immune complex in ratlungs. Photomed Laser Surg 25:112–117
32. Aimbire F, Albertini R, Pacheco M, Castro-Faria-Neto H, Leo-nardo P, Iversen V, Lopes-Martins R, Bjordal J (2006) Low-level laser therapy induces dose-dependent reduction of TNFal-pha levels in acute inflammation. Photomed Laser Surg 24:33–37
33. Aimbire F, Ligeiro de Oliveira A, Albertini R, Corrêa J, Ladeira deCampos C, Lyon J, Silva J Jr, Costa M (2008) Low level lasertherapy (LLLT) decreases pulmonary microvascular leakage, neu-trophil influx and IL-1β levels in airway and lung from rat sub-jected to LPS-induced inflammation. Inflammation 31:189–197
34. Aimbire F, Santos F, Albertini R, Castro-Faria-Neto H, MittmannJ, Pacheco-Soares C (2008) Low-level laser therapy decreaseslevels of lung neutrophils anti-apoptotic factors by a NF-kappaBdependent mechanism. Int Immunopharmacol 8:603–605
35. Mafra de Lima F, Naves K, Machado A, Albertini R, Villaverde A,Aimbire F (2009) Lung inflammation and endothelial cell damageare decreased after treatment with laser therapy (PhT) in a model ofacute lung injury induced by Escherichia coli lipopolysaccharidein the rat. Cell Biol Int 33:1212–1221
36. Frangogiannis N, Smith C, Entman M (2002) The inflammatoryresponse in myocardial infarction. Cardiovasc Res 53:31–47
37. Souza D, Fagundes F, Amaral F, Cisalpino D, Sousa L, Vieira A,Pinho V, Nicoli J, Vieira L, Fierro I, Teixeira M (2007) Therequired role of endogenously produced lipoxin A4 and annexin-1 for the production of IL-10 and inflammatory hyporesponsive-ness in mice. J Immunol 179:8533–8543
38. de Lima F, Villaverde A, Albertini R, Corrêa J, Carvalho R, MuninE, Araújo T, Silva J Jr, Aimbire F (2011) Dual effect of low-levellaser therapy (LLLT) on the acute lung inflammation induced byintestinal ischemia and reperfusion: action on anti- and pro-inflammatory cytokines. Lasers Surg Med 43:410–420
564 Lasers Med Sci (2013) 28:551–564
Related Documents











