Thorax 1994;49:121-127 Microvascular exudative hyperresponsiveness in human coronavirus-induced common cold Lennart Greiff, Morgan Andersson, Anders Akerlund, Per Wollmer, Christer Svensson, Ulf Alkner, Carl G A Persson Abstract Background - The inflammatory re- sponse of the airway microcirculation in rhinitis and asthma may be recorded as luminal entry of plasma macromolecules (mucosal exudation). This study ex- amines the exudative responsiveness of the subepithelial microvessels in subjects with and without common cold after inoculation with coronavirus. Methods - The airway mucosa was exposed to exudative concentrations of histamine (40 and 400,ug/ml) before and six days after inoculation. To assess whether mucosal penetration of a topi- cally applied agent was altered, nasal absorption of chromium-51 labelled ethylene diamine tetraacetic acid (5'Cr- EDTA, MW 372) was also examined. A nasal pool technique kept the challenge and tracer solutes in contact with the same ipsilateral mucosal surface. Con- centrations of albumin in lavage fluids were measured as an index of mucosal exudation of plasma. Nasal absorption of 5'Cr-EDTA was determined by the cumulated 24 hour urinary excretion of radioactivity. Results - Nine subjects developed com- mon cold after coronavirus inoculation and 10 remained healthy. Histamine pro- duced concentration dependent mucosal exudation of plasma in all subjects before and after coronavirus inoculation. In subjects with common cold, however, the histamine-induced mucosal exudation was significantly augmented compared with the group without common cold. This exudative hyperresponsiveness is not explained by an increased baseline exudation because the lavage regimen used produced comparably low baseline exudation in both groups of subjects, nor is it explained by an increased penetra- tion of topical histamine because the ability of the nasal mucosa to absorb 5'Cr-EDTA was not significantly increased in the subjects with common cold. Conclusions - An increased proclivity of the airway subepithelial microcircula- tion to respond with plasma exudation develops during coronavirus-induced common cold. This specific exudative hyperresponsiveness may be a feature of inflammatory airway diseases. (Thorax 1994;49:121-127) Several reports have suggested that rhinoviral infections may contribute to the development of non-specific bronchial hyperresponsive- ness.'2 The possibility that viral infections of the nose also produce nasal hyperresponsive- ness has not received attention. This seems unfortunate because nasal studies can be car- ried out with great specificity and yield in- formation of potential relevance both for the upper and lower airways.3 Changes in the sensitivity and function of different nasal end organs including the epi- thelial barrier, the secretory apparatus, the innervation, and the subepithelial microcircu- lation can be assessed in the nose.3 One end organ response - the mucosal exudation of plasma - may be of special interest. This response constitutes a significant mucosal defence reaction4 but may also produce many pathogenetic effects in the airways.5 In addi- tion, it can serve as a specific and quantitative index of the subepithelial inflammatory pro- cess.3 In allergic airway disease and coronavirus infection the inflammatory process is charac- terised by mucosal exudation of bulk plasma.67 Topical challenge with single mediators such as histamine also produces a reproducible mucosal exudation of bulk plasma.89 Using histamine as a challenge agent we have recently shown that an exudative hyperresponsiveness may develop during seasonal allergic rhinitis.'0 This increased vascular epithelial exudation response in allergy was not associated with increased mucosal absorption." It is not known whether the exudative responsiveness of the airway mucosa may be altered in other inflammatory respiratory diseases such as common cold. Viral infections are thought to damage the epithelium, resulting in increased tissue penetration of the challenge agent. This mechanism alone might produce exaggerated responses to airway challenges. In the present study we have measured histamine-induced mucosal exudation of plasma before and during human coronavirus- induced common cold. We have also examined the rate of nasal absorption of 51-chromium labelled ethylene diamine tetraacetic acid (5'Cr-EDTA, MW 372) to assess whether the normal barrier function of the mucosa is altered in the present virus-induced inflamma- tion. A nasal pool technique9 has been used both for histamine challenge and for adminis- tration of 5'Cr-EDTA. This technique ensures that the challenge and tracer solutes, respect- ively, are kept in contact with a large and well defined area of the nasal mucosal surface for a selected period of time. Department of Otorhinolaryngology L Greiff M Andersson A Akerlund C Svensson Department of Clinical Physiology P Wollmer Department of Clinical Pharmacology C G A Persson Lund University Hospital, S-221 85, Lund, Sweden Department of Bioanalysis, Astra Draco, Lund, Sweden U Alkner Reprint requests to: Dr L Greiff. Received 27 May 1993 Returned to authors 13 August 1993 Revised version received 15 November 1993 Accepted for publication 18 November 1993 121 on April 23, 2020 by guest. Protected by copyright. http://thorax.bmj.com/ Thorax: first published as 10.1136/thx.49.2.121 on 1 February 1994. Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Thorax 1994;49:121-127
Microvascular exudative hyperresponsiveness inhuman coronavirus-induced common cold
Lennart Greiff, Morgan Andersson, Anders Akerlund, Per Wollmer,Christer Svensson, Ulf Alkner, Carl G A Persson
AbstractBackground - The inflammatory re-sponse of the airway microcirculation inrhinitis and asthma may be recorded asluminal entry ofplasma macromolecules(mucosal exudation). This study ex-amines the exudative responsiveness ofthe subepithelial microvessels in subjectswith and without common cold afterinoculation with coronavirus.Methods - The airway mucosa wasexposed to exudative concentrations ofhistamine (40 and 400,ug/ml) before andsix days after inoculation. To assesswhether mucosal penetration of a topi-cally applied agent was altered, nasalabsorption of chromium-51 labelledethylene diamine tetraacetic acid (5'Cr-EDTA, MW 372) was also examined. Anasal pool technique kept the challengeand tracer solutes in contact with thesame ipsilateral mucosal surface. Con-centrations of albumin in lavage fluidswere measured as an index of mucosalexudation of plasma. Nasal absorptionof 5'Cr-EDTA was determined by thecumulated 24 hour urinary excretion ofradioactivity.Results - Nine subjects developed com-mon cold after coronavirus inoculationand 10 remained healthy. Histamine pro-duced concentration dependent mucosalexudation ofplasma in all subjects beforeand after coronavirus inoculation. Insubjects with common cold, however, thehistamine-induced mucosal exudationwas significantly augmented comparedwith the group without common cold.This exudative hyperresponsiveness isnot explained by an increased baselineexudation because the lavage regimenused produced comparably low baselineexudation in both groups of subjects, noris it explained by an increased penetra-tion of topical histamine because theability of the nasal mucosa to absorb5'Cr-EDTA was not significantlyincreased in the subjects with commoncold.Conclusions - An increased proclivity ofthe airway subepithelial microcircula-tion to respond with plasma exudationdevelops during coronavirus-inducedcommon cold. This specific exudativehyperresponsiveness may be a feature ofinflammatory airway diseases.
(Thorax 1994;49:121-127)
Several reports have suggested that rhinoviralinfections may contribute to the developmentof non-specific bronchial hyperresponsive-ness.'2 The possibility that viral infections ofthe nose also produce nasal hyperresponsive-ness has not received attention. This seemsunfortunate because nasal studies can be car-ried out with great specificity and yield in-formation of potential relevance both for theupper and lower airways.3Changes in the sensitivity and function of
different nasal end organs including the epi-thelial barrier, the secretory apparatus, theinnervation, and the subepithelial microcircu-lation can be assessed in the nose.3 One endorgan response - the mucosal exudation ofplasma - may be of special interest. Thisresponse constitutes a significant mucosaldefence reaction4 but may also produce manypathogenetic effects in the airways.5 In addi-tion, it can serve as a specific and quantitativeindex of the subepithelial inflammatory pro-cess.3
In allergic airway disease and coronavirusinfection the inflammatory process is charac-terised by mucosal exudation of bulk plasma.67Topical challenge with single mediators suchas histamine also produces a reproduciblemucosal exudation of bulk plasma.89 Usinghistamine as a challenge agent we have recentlyshown that an exudative hyperresponsivenessmay develop during seasonal allergic rhinitis.'0This increased vascular epithelial exudationresponse in allergy was not associated withincreased mucosal absorption." It is notknown whether the exudative responsivenessof the airway mucosa may be altered in otherinflammatory respiratory diseases such ascommon cold. Viral infections are thought todamage the epithelium, resulting in increasedtissue penetration of the challenge agent. Thismechanism alone might produce exaggeratedresponses to airway challenges.
In the present study we have measuredhistamine-induced mucosal exudation ofplasma before and during human coronavirus-induced common cold. We have also examinedthe rate of nasal absorption of 51-chromiumlabelled ethylene diamine tetraacetic acid(5'Cr-EDTA, MW 372) to assess whether thenormal barrier function of the mucosa isaltered in the present virus-induced inflamma-tion. A nasal pool technique9 has been usedboth for histamine challenge and for adminis-tration of 5'Cr-EDTA. This technique ensuresthat the challenge and tracer solutes, respect-ively, are kept in contact with a large and welldefined area of the nasal mucosal surface for aselected period of time.
Department ofOtorhinolaryngologyL GreiffM AnderssonA AkerlundC Svensson
Department ofClinical PhysiologyP Wollmer
Department ofClinicalPharmacologyC G A Persson
Lund UniversityHospital, S-221 85,Lund, Sweden
Department ofBioanalysis, AstraDraco, Lund, SwedenU Alkner
Reprint requests to:Dr L Greiff.Received 27 May 1993Returned to authors13 August 1993Revised version received15 November 1993Accepted for publication18 November 1993
121
on April 23, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.49.2.121 on 1 F
ebruary 1994. Dow
nloaded from

Greiff, Andersson, Akerlund, Wollmer, Svensson, Alkner et al.
MethodsSUBJECTSNineteen healthy men of mean age 24 (range20-27 years) participated in the study. Thesubjects had no history of general, nasal, orallergic disease, and no history of recent drugtreatment or recent vaccination. Absence ofallergy was verified by a negative history and anegative skin prick test (Phazett, Pharmacia,Uppsala, Sweden). The study was performedin May 1991 and was approved by the localethics committee and informed consent wasobtained.The subjects were isolated and lodged four
by four in five separate two bedroom apart-ments. They were instructed not to meetpeople other than their lodge mates at a rangecloser than 10 metres. Outdoor activities wereotherwise not restricted. All meals were de-livered to the apartments. In order to ensurethat the subjects were not infected at the startof the study, they were observed for the firsttwo days of isolation. During this time none ofthe subjects developed symptoms of commoncold so all were inoculated with coronavirus.Subjects not developing infection after corona-virus inoculation were used as control subjects.
NASAL CORONAVIRUS INOCULATIONHuman coronavirus 229E was diluted in phos-phate buffered saline at 4°C to a concentrationof 100 TCID,0/ml (tissue culture infective dose50 - that is, the dose that produced infection in50% of cultures). With the subjects in a supineand extended neck position 0 5 ml of thissolution was administered into each nasalcavity two days after isolation (study day zero).In order to avoid infectious contaminationduring the study the investigators in contactwith the subjects wore aprons, surgical gloves,and face masks. The non-disposable equip-ment used by the investigators was soaked inethanol (70%) or boiled water for two minutesbetween use. The clinical course, includingdaily measurements of symptoms and mucosaltemperature, is reported elsewhere.7
DETERMINATION OF COMMON COLDTo distinguish between subjects with andwithout common cold a clinical evaluation wasperformed daily by an otolaryngologist. Asymptom and clinical sign score, based onsymptoms presented on direct questions andclinical signs on physical examination includ-ing an anterior rhinoscopy, was given twicedaily according to the method of Beare et al.'2The criteria for the development of commoncold was a total score of more than 16 points,and a convincing progress of symptoms andsigns on the second to fifth days after inocula-tion - that is, a four point increase for at leasttwo consecutive days. In support of the clinicalevaluation an ELISA techique was used forserological analysis. Preinoculation sera werecompared with convalescent sera obtainedthree to four weeks after inoculation. A greaterthan fourfold increase in the titre was con-
sidered as seroconversion and as a suggestionof recent coronavirus-induced infection.
NASAL POOL TECHNIQUEA nasal pool technique was used for concom-itant histamine challenge and lavage, and foradminstration of the absorption tracer, re-spectively.9 The nasal pool device is a com-pressible plastic container equipped with anasal adapter. The adapter is inserted into oneof the nostrils (in the present study the rightnostril) and the container is compressed by thesubject sitting in a 60° forward flexed neckposition. The nasal pool fluid (in the presentstudy 14 ml) is then instilled and maintained incontact with a large and defined area of thenasal mucosal surface for an extended periodof time. When the pressure on the device isreleased the fluid returns into the container.
MEASUREMENT OF MUCOSAL EXUDATION OFPLASMAMeasurement of histamine-induced mucosalexudation of albumin was performed onemonth before and six days after coronavirusinoculation. Isotonic saline and histamine (40and 400 pg/ml) were introduced in sequenceinto the nasal cavity by the nasal pool tech-nique. The fluid was maintained in the nasalcavity for 10 minutes, and 20 minutes elapsedbetween each instillation. To prevent hist-amine from being retained in the airway themucosal surface was irrigated with saline for30 seconds using the nasal pool technique,immediately after each 10 minute challenge.These lavage fluids were not collected. Therecovered fluids were centrifuged (105g, 10minutes, 4°C) and samples were obtained fromthe supernatant and frozen (- 20°C) whileawaiting analysis. The concentration of albu-min was measured in the recovered lavagefluids with a radioimmunoassay techniquesensitive to 6-25 ng/ml. The intra- and inter-assay coefficients of variation were 5% and10%, respectively.Five days after inoculation the effect of
repeated saline lavages without histamine onlavage fluid levels of albumin was examined inthe group with common cold. Two consec-utive saline lavages, each of 10 minutesduration, were performed, followed by a thirdlavage 30 minutes later. The concentration ofalbumin was measured in the recovered lavagefluids as described above.
MEASUREMENT OF NASAL ABSORPTION OF5'Cr-EDTAMeasurement of nasal absorption of 51Cr-EDTA was performed one month before andfour days after coronavirus inoculation.'3 5GCr-EDTA (about 5 MBq) in isotonic saline wasintroduced into the nasal cavity by the nasalpool technique. The fluid was maintained inthe nasal cavity for 15 minutes. Two additional30 second saline lavages were then promptlycarried out to prevent absorption of any tracerretained on the mucosal surface. The nasal
122
on April 23, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.49.2.121 on 1 F
ebruary 1994. Dow
nloaded from
Microvascular exudative hyperresponsiveness in common cold
absorption of 5"Cr-EDTA during the 15minute exposure was determined by samplingthe urine produced during 24 hours after theinstillation procedure. Three samples (each3-0 ml) taken from the pooled 24 hour urinecollection were counted in a well counter for2000 seconds. Two samples (each 3 0 ml) of a
standard solution, prepared by diluting 0 1 mlof the instillate to 100 ml, were countedtogether with the urine samples. The amountabsorbed was expressed as the correspondingvolume of the nasal instillate - that is, the urinecount rate multiplied by the pooled urinevolume, divided by the standard solutioncount rate corrected for dilution.
STATISTICSThe Friedman and Wilcoxon signed rank testswere used to examine differences in albuminconcentrations between the three lavages per-
formed on subjects with common cold fivedays after inoculation. The Wilcoxon signedrank test was used to examine differences inhistamine-induced albumin concentrationsand differences in absorbed volumes of 5"Cr-EDTA before and after inoculation within thegroups, with and without common cold. TheMann-Whitney U test was used to examinedifferences in histamine-induced albumin con-
centrations between the groups with and with-out common cold. A regression analysis ofindividual values was used to examine thecorrelation between histamine-induced muco-
sal exudation of plasma on day six andabsorption of 51Cr-EDTA on day four afterinoculation. A p value <0 05 was consideredsignificant. Data are presented as means (SE).
ResultsNine subjects developed common cold as
judged by scores of symptoms and clinicalsigns (table), two of whom failed to showseroconversion. Because of a convincing de-velopment of symptoms, however, all ninesubjects were included in the group with com-
mon coldi. A total number of nine subjectsshowed seroconversion, two of whom were
without convincing symptoms or clinical signsof common cold. The latter subjects wereincluded in the group without common cold.
Before inoculation the albumin concentra-tion in the saline lavage fluid obtained was lowin subjects who subsequently developed or didnot develop common cold (11-8 (3-5) tg/mland 22 3 (5-1) jig/ml, respectively). Six daysafter inoculation the group without commoncold also exhibited a relatively low albuminconcentration (34 6 (8 5) gtg/ml) in the salinelavage fluid obtained, whereas the albuminconcentration was significantly elevated (137 2(30 7) jg/ml) in the group with common cold(p < 0 01) reflecting an ongoing mucosalexudation of plasma. The initial saline lavagefluid obtained five days after inoculation (theday before the saline/histamine challengeseries) in subjects developing common coldexhibited an almost equally elevated levelof albumin concentration (83-3 (31-8) gg/ml;p < 0 05), again demonstrating ongoing muco-
sal exudation in the subjects with common
cold. However, in the second saline lavagefluid taken on day five a low baseline levelof albumin (34 1 (11 2)glg/ml) was obtained(Friedman test, p< 005; Wilcoxon's signedrank test, p < 0 01 ) compared with the concen-tration of albumin in the first saline lavagefluid. Furthermore, in the third saline lavagefluid obtained 30 minutes later the level ofalbumin remained low (36 1 (13 5) gg/ml) sug-gesting that, with the present technique ofrepeated challenge and lavage experiments,changes in baseline concentrations of albuminwould not invalidate the measurement of hist-amine-induced exudation in subjects whodeveloped common cold.
Histamine produced a concentration de-pendent mucosal exudation of albumin in bothgroups before and six days after coronavirusinoculation (fig 1). Furthermore, the effect ofhistamine was increased in the group withcommon cold after inoculation compared withits effect before inoculation (histamine 40 gg/ml (p <0 05) and 400 gg/ml (p <0 05)). In con-trast, the effect of histamine was unchanged inthe group without common cold after inocula-tion compared with before inoculation. The
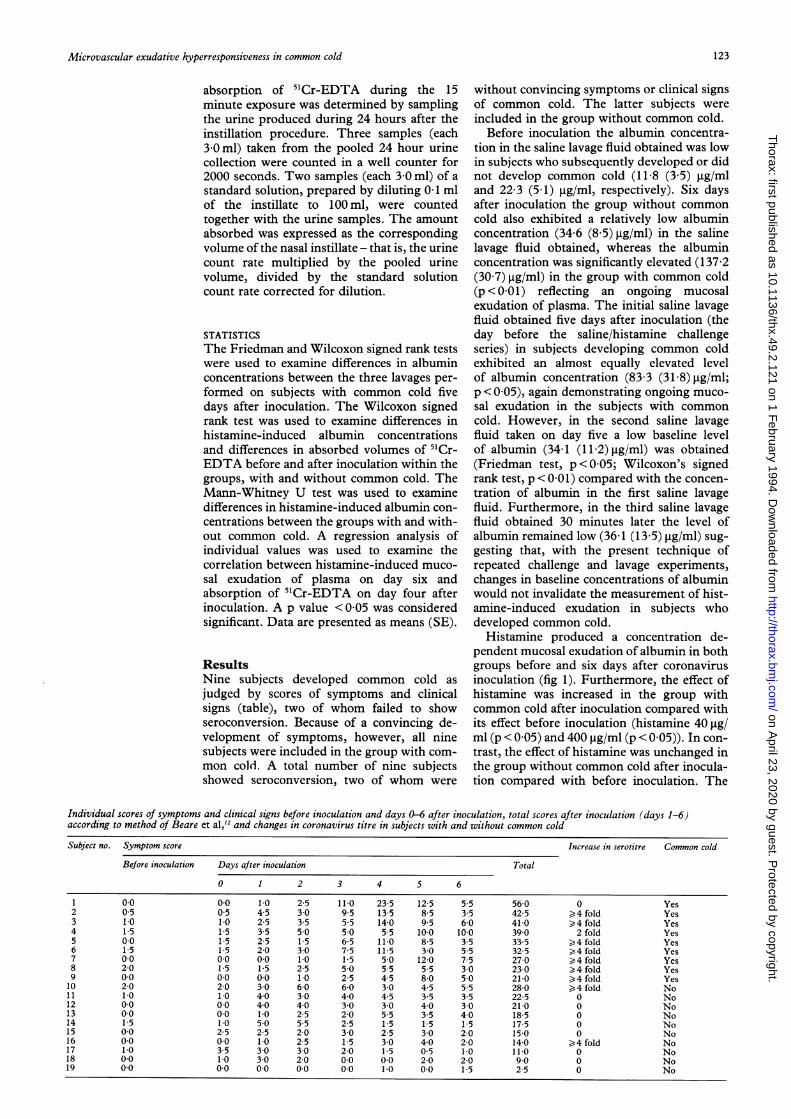
Individual scores of symptoms and clinical signs before inoculation and days 0-6 after inoculation, total scores after inoculation (days 1-6)according to method of Beare et al,'2 and changes in coronavirus titre in subjects with and without common cold
Subject no. Symptom score Increase in serotitre Common cold
Before inoculation Days after inoculation Total
0 1 2 3 4 5 6
1 00 0.0 1-0 25 110 235 125 55 560 0 Yes2 0 5 0 5 4 5 3 0 9 5 13-5 8 5 3-5 42-5 )4 fold Yes3 1.0 1.0 2-5 3 5 5 5 14-0 9 5 6-0 41.0 >4 fold Yes4 1-5 15 35 50 50 5 5 10.0 100 390 2 fold Yes5 00 15 25 1-5 65 110 85 35 335 >4 fold Yes6 15 15 2 0 3-0 7 5 115 3 0 5-5 32-5 )4 fold Yes7 00 00 00 10 15 5.0 120 75 270 4 fold Yes8 20 15 15 25 50 55 55 30 230 4 fold Yes9 00 00 0-0 10 25 45 80 50 210 4 fold Yes10 20 2.0 30 60 60 30 4-5 55 280 4 fold No11 10 10 40 30 40 45 3-5 35 225 0 No12 00 00 40 40 30 30 40 30 210 0 No13 0 0 0 0 10 2 5 2-0 5.5 3 5 4 0 18 5 0 No14 15 10 50 55 25 15 1.5 15 175 0 No15 00 25 2-5 2-0 30 25 30 20 15.0 0 No16 00 00 10 25 1.5 30 40 20 140 >4 fold No17 1.0 35 30 30 20 1.5 05 1.0 11.0 0 No18 00 10 3-0 20 00 00 20 20 90 0 No19 0.0 00 00 00 0.0 10 00 15 25 0 No
123
on April 23, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.49.2.121 on 1 F
ebruary 1994. Dow
nloaded from
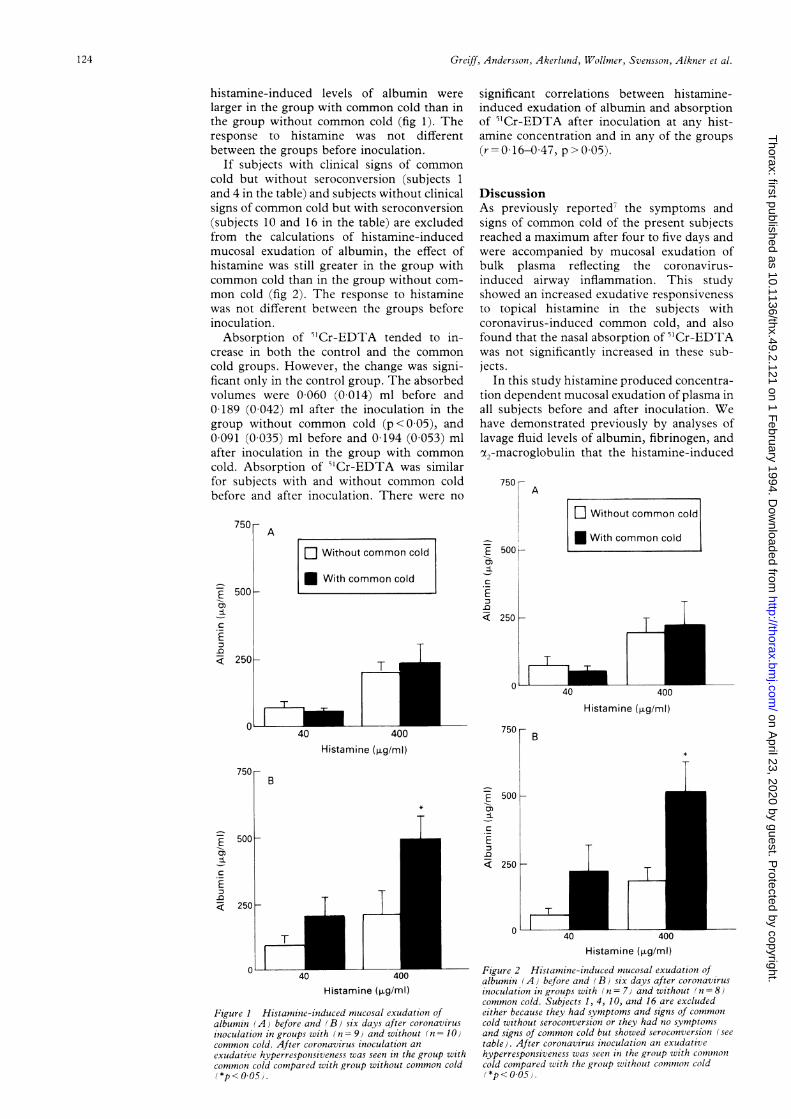
Greiff, Andersson, Akerlund, Wollmer, Svensson, Alkner et al.
histamine-induced levels of albumin werelarger in the group with common cold than inthe group without common cold (fig 1). Theresponse to histamine was not differentbetween the groups before inoculation.
If subjects with clinical signs of commoncold but without seroconversion (subjects 1and 4 in the table) and subjects without clinicalsigns of common cold but with seroconversion(subjects 10 and 16 in the table) are excludedfrom the calculations of histamine-inducedmucosal exudation of albumin, the effect ofhistamine was still greater in the group withcommon cold than in the group without com-mon cold (fig 2). The response to histaminewas not different between the groups beforeinoculation.Absorption of 5"Cr-EDTA tended to in-
crease in both the control and the commoncold groups. However, the change was signi-ficant only in the control group. The absorbedvolumes were 0 060 (0 014) ml before and0 189 (0 042) ml after the inoculation in thegroup without common cold (p < 0-05), and0 091 (0 035) ml before and 0 194 (0 053) mlafter inoculation in the group with commoncold. Absorption of 'Cr-EDTA was similarfor subjects with and without common coldbefore and after inoculation. There were no
E 500 -
-E
.E
< 250
0
A
[1 Without common cold
* With common cold
T
significant correlations between histamine-induced exudation of albumin and absorptionof 51Cr-EDTA after inoculation at any hist-amine concentration and in any of the groups(r= 0 16-0 47, p>005).
DiscussionAs previously reported/ the symptoms andsigns of common cold of the present subjectsreached a maximum after four to five days andwere accompanied by mucosal exudation ofbulk plasma reflecting the coronavirus-induced airway inflammation. This studyshowed an increased exudative responsivenessto topical histamine in the subjects withcoronavirus-induced common cold, and alsofound that the nasal absorption of 51Cr-EDTAwas not significantly increased in these sub-jects.
In this study histamine produced concentra-tion dependent mucosal exudation of plasma inall subjects before and after inoculation. Wehave demonstrated previously by analyses oflavage fluid levels of albumin, fibrinogen, andot,-macroglobulin that the histamine-induced
A
O Without common cold
* With common cold
T- T
-E
-3
.EQ
250
o 40 400
Histamine (1ig/ml)
40 400Histamine ([.g/ml)
750 B
D
E
.E
40 400Histamine (pg/mI)
Figure I Histami ne-induced mucosal exudation ofalbumin (A) before and (B) six days after coronavirus
inoculation in groups with (n = 9J and without (n = 10Icommon cold. After coronavirus inoculation an
exudative hyperresponsiveness was seen in the group withcommon cold compared with group without common cold
(*p<o0O5.
iT500 -
I250 H
o0 440Histamine (fig/ml)
Figure 2 Histamine-induced mucosal exudatiotn ofalbumin (A) before and (B) six days after coronavirusinoculation in groups with ( n = 7) and without (n = 8)common cold. Subjects 1, 4, 10, and 16 are excludedeither because they had symptoms and signs of commoncold without seroconversion or they had no symptomsand signs of common cold but showed seroconversion (seetable). After coronavirus inoculation an exudativehyperresponsiveness was seen in the group with comtmoncold compared with the group without conimon cold(*p< 0.5)
E-iC
.EQ0
500 e
250 H
T1
0
124
on April 23, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.49.2.121 on 1 F
ebruary 1994. Dow
nloaded from

Microvascular exudative hyperresponsiveness in common cold
exudation of albumin corresponds to mucosalexudation of non-sieved bulk plasma.310 Wehave also observed, in human nasal airways'3and in guinea pig tracheobronchial airways,'4that histamine-induced mucosal exudation ofplasma is not associated with any change in theabsorption permeability of the airway mucosa.
Interestingly, the histamine-induced exuda-tion of plasma was significantly greater insubjects with common cold than in those with-out common cold. The response in the formergroup was significant. For comparison, about afivefold greater concentration of histaminemay be required to produce the same degree ofplasma exudation in healthy subjects.9 Theincreased response in subjects with commoncold may not reflect a high baseline concentra-tion of albumin because control experimentscarried out five days after inoculation showedthat the high baseline is already lost after theinitial saline lavage. Furthermore, the resultsobtained on day five showed that albumin doesnot accumulate significantly on the mucosalsurface for the period of 30 minutes that waschosen in the present challenge and lavageregimen. The baseline levels obtained on dayfive thus strongly suggest that the abnormallyincreased concentrations of albumin after thetwo histamine challenge doses in subjects withcommon cold reflect an exudative hyper-responsiveness of the airway mucosa. Thishyperresponsiveness is similar in magnitude tothat recently found in seasonal allergic rhin-itis."' Hence, both allergen-induced and virus-induced airway inflammation appear to be as-sociated with exudative hyperresponsiveness.We have suggested that exudative indices maydirectly reflect the intensity of the subepithe-lial airway inflammation.3 One consequence ofan increased exudative responsiveness, asobserved in the present study, is that themucosal exudation response would be an evenmore sensitive measure of airway inflamma-tion than previously suggested.3
In a series of studies involving human andguinea pig airways we have examined mechan-isms of mucosal exudation of plasma.31516 Posi-tioned just beneath the epithelial lining is anetwork of capillary venular microvessels.Active separation of endothelial cells of post-capillary venules is induced by actions of in-flammatory mediators on these cells. Throughthe open gaps in the venular wall bulk plasmais extravasated along a hydrostatic pressuregradient. We have suggested that the extrava-sated plasma moves up between epithelial cellsand exerts a hydrostatic pressure load on baso-lateral aspects of the cells.315 This load mayproduce a transient separation of the junctionsbetween the epithelial cells so that a paracellu-lar pathway for the clearance ofplasma into thelumen is created. In guinea pig tracheal tubepreparations we have shown that an increase inserosal hydrostatic pressure of about 5 cm H20is sufficient to move macromolecules from theserosal to the mucosal aspect of the prepara-tion.'6 Furthermore, the luminal entry in vitrois not affected by the presence of exudativemediators on the mucosa,16 suggesting that thephysical pressure effect alone, without the aid
of any mediator-induced epithelial effect, ac-counts for the passage. Luminal entry of bulkplasma may thus occur along a small hydro-static pressure gradient, and even if mucosalexudation of plasma is pronounced it mayoccur without generation of oedemal7 orincreased lymph protein transport.'8 Mucosalexudation of plasma is produced by thresholdinflammatory challenges.'9 Hence, the move-ment of extravasated plasma into the airwaylumen may not be hindered greatly by thenormal epithelial lining and may not involvepharmacological effects on the epithelial cells.We therefore suggest that the increased exud-ative responsiveness to histamine challengein coronavirus-induced airway inflammationdoes not reflect an abnormal responsiveness ofthe epithelial lining, but is the result of anincreased responsiveness of the subepithelialmicrocirculation.Mucosal exudation of plasma is strictly
unidirectional and the baseline absorptionability of the mucosa is not affected by theexudation process.'3 1420 In the present studynasal absorption of 5'Cr-EDTA was not signi-ficantly changed in subjects with common coldat the height of infection, suggesting that sig-nificant epithelial destruction had not oc-curred. Since mucosal exudation of plasmamay occur without damage to the epitheliallining, this process may be considered a firstline respiratory defence also in common cold.Mucosal exudation of plasma is induced by
inflammatory mediators,819 allergen,61921 occu-pational factors,'9 and infection.7 The intensityand time course of the plasma exudation re-sponse can be monitored by analysing theconcentration ofplasma proteins/tracers in air-way mucosal surface liquids. Mucosal exud-ation of bulk plasma has been found in allergicrhinitis2' and in allergic asthma.6 Furthermore,increased concentrations of both albumin andfibrinogen have been shown in airway mucosalsurface liquids after nasal coronavirus inocula-tion, indicating that mucosal exudation of bulkplasma is ongoing in subjects with commoncold,722 particularly late at night and in theearly morning hours.22 In the present study thefirst saline lavages carried out on days five andsix in subjects with common cold revealedabnormally high levels of albumin, confirmingthe inflammatory exudative nature of this dis-ease.The mechanism of the exudative hyper-
responsiveness has not yet been clarified. Inthe present study the nasal absorption of 5'Cr-EDTA (a small polar solute like histamine) wasnot significantly changed in subjects with com-mon cold. It therefore seems that increasedpenetration of histamine to the subepithelialmicrovascular target can be excluded as animportant mechanism. Although it has beensuggested that epithelial disruption andincreased absorption across the mucosa is afeature of airway inflammation and airwayhyperresponsiveness,23-25 this is not stronglysupported by actual observations made inasthmatic subjects,2627 and in experimentalstudies involving human nasal airways andanimal tracheobronchial airways.3 1420 We
125
on April 23, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.49.2.121 on 1 F
ebruary 1994. Dow
nloaded from

Greiff, Andersson, Akerlund, Wollmer, Svensson, Alkner et al.
have shown that absorption across the nasalmucosa may even be reduced in seasonal aller-gic rhinitis late into the birch pollen season.'1During the course of the present study theabsorption rate was slightly increased both inhealthy individuals and in those with commoncold. This effect may be a result of the frequentlavages that were carried out in these subjectsduring the course of the entire experimentcomprising seven days.7 It is less likely thatcoronavirus inoculation in itself may have con-tributed to the increased absorption that wasrecorded in subjects who did not develop com-mon cold.
Bronchial hyperresponsiveness to topicalhistamine has been shown during virus infec-tion,' but it is not known what mechanisms areinvolved in this response. Indeed, if the muco-sal thickness is increased this could in theoryexplain an increased "obstructive" responsive-ness to any fixed bronchoconstrictor stimulus.Thus, methacholine and histamine have pre-viously been employed to study non-specificresponsiveness in asthma (and rhinitis). In thepresent study we have used histamine specific-ally to examine the ability of the subepithelialmicrocirculation to respond with plasma exu-dation. The presently observed increasedmucosal responsiveness may be one of severalspecific end organ functions of the airways thatcan potentially be altered in airway inflamma-tion. Other important functions include sens-ory nerve responsiveness and secretory res-ponsiveness, both of which may increase inairway diseases.3
It is difficult to examine plasma exudationand solute absorption across the human tra-cheobronchial mucosa in vivo with acceptablespecificity. The distribution of absorptiontracers and challenge factors may not be wellcontrolled, and it may be difficult to distin-guish between airway and alveolar absorptionprocesses in the human lung. In a series ofstudies on human nasal and guinea pig tra-cheobronchial airways we have found verysimilar responses to inflammatory challengesbetween the upper and the lower airways,particularly concerning effects on plasma exu-dation and solute absorptionrates.'131428 Thepossibility that an exudative hyperresponsive-ness may also be present in inflammation of thelower airways cannot therefore be excluded.Studies on exudative responsiveness may beparticularly warranted in asthma whereexuded plasma is considered a multipotentialdisease mechanism.5
It is possible that altered airway end organfunctions may be important and specific char-acteristics of inflammatory airway diseases orof subgroups of patients within a particulardisease. Our observation of increased exudat-ive responsiveness in both virus-induced (thisstudy) and allergen-induced'0 inflammationsuggests a generality of this particular altera-tion in mucosal function. However, we do notyet know any details of the development ofincreased exudative responsiveness or its rolein the disease process. It is an intriguing, butas yet unproven, possibility that this specific
responsiveness may be modulated by anti-inflammatory drug intervention.We conclude that coronavirus-induced
common cold is characterised by an increasedproclivity of the subepithelial microcirculationto respond with plasma exudation. Thisexudative hyperresponsiveness may not beexplained by increased mucosal penetration ofhistamine, as the absorption permeability ofthe airway was not significantly changed in thesubjects with common cold.
This study was supported by the Swedish Medical ResearchCouncil (Projects 8308 and 2872), the Medical Faculty of LundUniversity, the Swedish Association against Asthma andAllergy, and Skaraborg County Council.
Empey DW, Laitinen LA, Jacobs L, Gold WM, Nadel JA.Mechanisms of bronchial hyperreactivity in normal sub-jects after respiratory tract infection. Am Rev Respir Dis1976;113:131-9.
2 Bardin PG, Johnston SL, Pattemore PK. Viruses as precip-itants of asthma symptoms. II. Physiology and mechan-isms. Clin Exp Allergy 1992;22:809-22.
3 Persson CGA, Svensson C, Greiff L, Anderson M,Wollmer P, Alkner U, et al. Use of the nose to study theinflammatory response in the respiratory tract. Thorax1992;47:993-1000.
4 Persson CGA, Erjefilt I, Alkner U, Baumgarten C, GreiffL, Gustafsson B, et al. Plasma exudation as a first linerespiratory mucosal defence. Clin Exp Allergy1991;21:17-24.
5 Persson CGA. Role of plasma exudation in asthmatic air-ways. Lancet 1986;ii:1126-9.
6 Salomonsson P, Gronneberg R, Gilljam H, Andersson 0,Billing B, Enander I, et al. Bronchial exudation of bulkplasma at allergen challenge in allergic asthma. Am RevRespir Dis 1992;146:1535-42.
7 Akerlund A, Greiff L, Andersson M, Bende M, Alkner U,Persson CGA. Mucosal exudation of fibrinogen in cor-onavirus-induced common cold. Acta Otolaryngol(Stockh) 1993;113:642-8.
8 Svensson C, Baumgarten CR, Pipkorn U, Alkner U, Pers-son CGA. Reversibility and reproducibility of histamineinduced plasma leakage in nasal airways. Thorax1989;44:13-8.
9 Greiff L, Pipkorn U, Alkner U, Persson CGA. The "nasalpool-device" applies controlled concentrations of soluteson human nasal airway mucosa and samples its surfaceexudation/secretions. Clin Exp Allergy 1990;20:253-9.
10 Persson CGA, Greiff L, Svensson C, Andersson M, Aker-lund A, Wollmer P, et al. Exudative hyperresponsivenessof the airway microcirculation in allergic rhinitis andcommon cold (abstract). Am Rev Respir Dis 1993;147:A833.
11 Greiff L, Wollmer P, Svensson C, Andersson M, PerssonCGA. Effects of seasonal allergic rhinitis on airway mu-cosal absorption of chromium-51 labelled EDTA. Thorax1993;48:648-50.
12 Beare A, Reed S. The study of anti-viral compounds involunteers. In: Oxford JS, ed. Chemoprophylaxis and virusinfections of the respiratory tract. Vol 2. Cleveland: CRCPress, 1977:28-55.
13 GreiffL, Wollmer P, Pipkorn U, Persson CGA. Absorptionof "Cr-EDTA across the human nasal mucosa in thepresence of topical histamine. Thorax 1991;46:630-2.
14 Greiff L, Erjefilt I, Wollmer P, Pipkorn U, Persson CGA.Effects of histamine, ethanol, and a detergent on exuda-tion and absorption across the guinea pig airway mucosain vivo. Thorax 1991;46:700-5.
15 Persson CGA. Permeability changes in obstructive airwaydisease. In: Sluiter HJ, Van der Lende R, eds. BronchitisIV. Assen: Van Gorcum, 1989:236-46.
16 Persson CGA, ErjefiltI, Gustafsson B, Luts A. Subepithe-lial hydrostatic pressure may regulate plasma exudationacross the mucosa. Int Arch Allergy Appl Immunol1990;92: 148-53.
17 Erjefilt I. Plasma exudation in tracheobronchial airways: aphysiological and pharmacological study in the guinea pig.Thesis, Lund University, Sweden: 1991.
18 Erjefalt I, Luts A, Persson CGA. The appearance of airwayexudation and absorption tracers in guinea pig tracheo-bronchial lymph nodes. J Appl Physiol 1993;74:817-24.
19 Erjefalt I, Persson CGA. Inflammatory passage of plasmamacromolecules into airway wall and lumen. PulmonolPharmacol 1989;2:93-102.
20 Erjefalt I, Persson CGA. Allergen, bradykinin, and cap-saicin increase outward but not inward macromolecularpermeability of guinea-pig tracheobronchial mucosa. ClinExp Allergy 1991;21:217-24.
21 Svensson C, Klementsson H, Alkner U, Pipkorn U, Pers-son CGA. A topical glucocorticoid reduces the level offibrinogen and bradykinins on the allergic nasal mucosa
during natural pollen exposure. Allergy 1993 (in press).22 Persson CGA, Greiff L, Akerlund A, Andersson M, Svens-
son C, Alkner U. The mucosal inflammatory process isnoctumal in coronavirus-induced common cold(abstract). Am Rev Respir Dis 1993;147:A66.
126
on April 23, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.49.2.121 on 1 F
ebruary 1994. Dow
nloaded from
Microvascular exudative hyperresponsiveness in common cold
23 Buckle FG, Cohen AB. Nasal mucosal hyperpermeability tomacromolecules in atopic rhinitis and extrinsic asthma.JAllergy Clin Immunol 1975;55:213-21.
24 Hogg JC, Eggleston PA. Is asthma an epithelial disease? AmRev Respir Dis 1984;129:207-8.
25 Laitinen LA, Heino M, Laitinen A, Kava T, Haahtela T.Damage of the airway epithelium and bronchial reactivityin patients with asthma. Am Rev Respir Dis 1985;131:599-606.
26 Elwood RK, Kennedy S, Belzberg A, Hogg JC, Pare PD.
Respiratory mucosal permeability in asthma. Am RevRespir Dis 1983;128:523-7.
27 O'Byme PM, Dolovich M, Dirks R, Roberts RS,Newhouse MT. Lung epithelial permeability: relation tonon-specific airway responsiveness. Appl Physiol1984;57:77-84.
28 Greiff L, Wollmer P, Erjefilt I, Pipkorn U, Persson CGA.Clearance of 99mTc-DTPA from guinea pig nasal,tracheobronchial, and bronchoalveolar airways. Thorax1990;45:841-5.
127
on April 23, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.49.2.121 on 1 F
ebruary 1994. Dow
nloaded from
Related Documents











