1 1 Joannes-Boyau O SAR II CHU Bordeaux Joannes-Boyau O SAR II CHU Bordeaux Suppléance hépatique Introduction Recherche de méthodes de suppléance hépatique depuis 50 ans Plus que jamais d’actualité Pronostic particulièrement sombre des défaillances hépatiques aiguës Sur foie sain sur pathologie préexistante Introduction Greffe hépatique reste le TTT de choix Inadéquation : malade / greffon Traitement immunosuppresseur lourd Suppléance hépatique temporaire 3 Transplantation Insuffisance hépatique Suppléance ou “Bridge” Récuperation Principes de suppléance Plusieurs groupes de techniques : Perfusion extracorporelle de foies animaux et/ou humains. Hépatocytes dans des systèmes de foie bioartificiels. Méthodes de détoxification mécanique sans matériel cellulaire. Toutes ces techniques peuvent être combinées. Principes de suppléance Suppléance des fonctions déficientes: Détoxification Toxines dans le sang, non filtrables. Portées par des protéines de transport dont l’albumine Substances hydrosolubles (urée, créatinine, ammoniaque) Substances liées à l’albumine (phénols, acides biliaires, bilirubine, etc.). Synthèse de différents produits Métabolisme du « diazépam » Glucuronoconjugaison Synthèse de l’urée Contrôle de l’inflammation Historique Recherche de suppléance de la fonction hépatique = une longue liste d’échec. Hémodialyse pour traiter l’hyperammoniémie en 1955 Kiley JE et al . N Engl J Med. 1958 l’hémofiltration, l’hémoperfusion et la plasmaperfusion sur des membranes adsorbantes Gazzard BG et al. Lancet. 1974 O'Grady JG et al. Gastroenterology. 1988 Stockmann HB et al. Ann Surg. 2000 Nyberg SL et al. Am J Surg. 1993

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
1Joannes-Boyau OSAR II CHU Bordeaux
Joannes-Boyau OSAR II CHU Bordeaux
Suppléance hépatique Introduction
� Recherche de méthodes de suppléance
hépatique depuis 50 ans
� Plus que jamais d’actualité
� Pronostic particulièrement sombre des
défaillances hépatiques aiguës � Sur foie sain
� sur pathologie préexistante
Introduction
� Greffe hépatique reste le TTT de choix
� Inadéquation : malade / greffon
� Traitement immunosuppresseur lourd
� Suppléance hépatique temporaire
3
Transplantation
Insuffisance hépatique Suppléance ou
“Bridge” Récuperation
Principes de suppléance
� Plusieurs groupes de techniques :� Perfusion extracorporelle de foies animaux et/ou
humains.
� Hépatocytes dans des systèmes de foie bioartificiels.
� Méthodes de détoxification mécanique sans matériel cellulaire.
� Toutes ces techniques peuvent être combinées.
Principes de suppléance
� Suppléance des fonctions déficientes:� Détoxification
� Toxines dans le sang, non filtrables.
� Portées par des protéines de transport dont l’albumine
� Substances hydrosolubles (urée, créatinine, ammoniaque)
� Substances liées à l’albumine (phénols, acides biliaires, bilirubine, etc.).
� Synthèse de différents produits � Métabolisme du « diazépam »
� Glucuronoconjugaison
� Synthèse de l’urée
� Contrôle de l’inflammation
Historique
� Recherche de suppléance de la fonction hépatique = une longue liste d’échec.
� Hémodialyse pour traiter l’hyperammoniémie en 1955 Kiley JE et al . N Engl J Med. 1958
� l’hémofiltration, l’hémoperfusion et la plasmaperfusion sur des membranes adsorbantes Gazzard BG et al. Lancet. 1974 O'Grady JG et al. Gastroenterology. 1988Stockmann HB et al. Ann Surg. 2000 Nyberg SL et al. Am J Surg. 1993

2
Historique
Technique de suppléance N° patients Amélioration neurologique Survie
Hémodialyse 65 33 (51%) 17 (26%)
Hémofiltration 15 10 (67%) 8 (53%)
Echanges sanguins 48 24 (50%) 9 (19%)
Echanges plasmatiques 32 15 (47%) 7 (22%)
Hémoperfusion sur résine 9 5 (56%) 0 (0%)
Hémoperfusion sur colonne de charbon 278 73 (26%) 116 (42%)
Total 447 160 (36%) 157 (35%)
Stockmann HB Ann Surg. 2000 (3)88
Circulation croisée avec chien
Liver failure patient
reactor
WarmerRoller pump
Metabolic circuit
Healthy dogs
Splenic artery
Splenic vein
Cross dialysis treatment using four living dogs Hori et al; 1958
99
Perfusion sur Foie ex vivo
The Venovenous Circuit for ex Vivo Pig-Liver Perfusion
Chari RS et al, N. Engl J Med 1994
Historique
� Dernière décennie : intensification des recherches dans ce domaine.
� Biocompatibilité des matériaux.
� Pouvoir de détoxification du dispositif par accrétion d’élément toxiques.
� Association avec un dialysat.
� Avènement des foies bioartificiels� Après la relative inefficacité des méthodes artificielles.
� Travaux majeurs de certaines équipes nord-américaines.
Techniques bioartificielles
� Quatre techniques en phase d’évaluation dans de nombreux centres (stoppées actuellement)
� L’extracorporeal liver assist device (ELAD (Vitagen))
� Le système HepatAssist (Circe Biomedical)
� le Bioartificial Liver Support System (BLSS (ExcorpMedical))
� le Bioartificial extracorporeal Liver Support (BELS (Gerlach))
L’extracorporeal liver assist device (ELAD
(Vitagen))

3
Etude ELAD
� 24 patients � 17 avec potentiel de récupération spontanée
� 7 listés pour la greffe
� Randomisés en 2 groupes� Traité par ELAD pendant 72 heures
� Groupe contrôle
� Encéphalopathie < dans le groupe traité
� Survie identique 78% contre 75%� Ellis AJ et al. Hepatology. 1996
Techniques bioartificielles
� Quatre techniques actuellement en phase d’évaluation dans de nombreux centres.
� L’extracorporeal liver assist device (ELAD (Vitagen))
� Le système HepatAssist (Circe Biomedical)
� le Bioartificial Liver Support System (BLSS (Excorp Medical))
� le Bioartificial extracorporeal Liver Support (BELS (Gerlach))
Hepatassist

4
1919
Hepatasist :Resultats cliniques Phase 1
� 36 patients en IHA:
� 21 patients ont pu bénéficier d’une Tx hépatique� 19 en HAG
� 2 en AoCLF
� 6 ont récupèré sans Tx H
� 9 patients sont décédés
Samuel D. et al transplantation 200220
Etude prospective multicentrique
� METHODS:
� 171 patients (86 contrôle et 85 BAL :hépatite aigue fulminante ou sub
fulminante ou dysfonction primaire du greffon.
� RESULTATS:
� Survie globale à 30 jours: 71% pour le Bal et 62% groupe contrôle
� Dans le groupe HAG: la survie est de 73% pour le BAL versus 59% dans
le groupe contrôle (n = 147; P = 0.12). (risk ratio = 0.56; P = 0.048).
� CONCLUSIONS: 1ére étude prospective, randomisée, contrôlée,
démontrant la sûreté de la méthode et l’amélioration de la survie chez
des patients avec une hépatite fulminante/subfulminante .
Demetriou AA Ann Surg. 2004
Techniques bioartificielles
� Quatre techniques actuellement en phase d’évaluation dans de nombreux centres.
� L’extracorporeal liver assist device (ELAD (Vitagen))
� Le système HepatAssist (Circe Biomedical)
� le Bioartificial Liver Support System (BLSS (Excorp Medical))
� le Bioartificial extracorporeal Liver Support (BELS (Gerlach))
Bioartificial Liver Support System (BLSS (Excorp Medical))
Techniques bioartificielles
� Quatre techniques actuellement en phase d’évaluation dans de nombreux centres.
� L’extracorporeal liver assist device (ELAD (Vitagen))
� Le système HepatAssist (Circe Biomedical)
� le Bioartificial Liver Support System (BLSS (Excorp Medical))
� le Bioartificial extracorporeal Liver Support (BELS (Gerlach))
BELS
5
25
B.A.L.: le futur
�Les législation européenne sur lesxenotransplantation interdisent l’utilisationd’hépatocytes animaux dans les applicationscliniques des BAL.
�Pb des hepatocytes issus d’hépatoblastome
�Le futur des BAL est le développement et laculture de lignées cellulaires d’hépatocyteshumain.
27
Techniques artificielles
2828
La dialyse simple: SPAD
� (SPAD) dialyse à l’albumine utilisant une machine de d’hémofiltration rénale conventionnelle:
� Le sang du patient traverse un circuit avec une membrane à fibre creuse identique à celle du MARS en polysulfone.
� Le dialysat circulant à contre courant est une solution d’Albumine qui est jetée après le passage dans le filtre.
� Résultats controversés
29
SPAD et Prismaflex
Membrane en polysulfone HF 1400Hémosol et albumine
Techniques artificielles
� Nombreuses techniques, purement artificielles, apparues depuis vingt ans
� 3 Principaux
� MARS (molecular adsorbents recycling system)
(Gambro)
� biologic-DT (HemoCleanse Inc.)
� Prometheus (Fresenius)
6
31
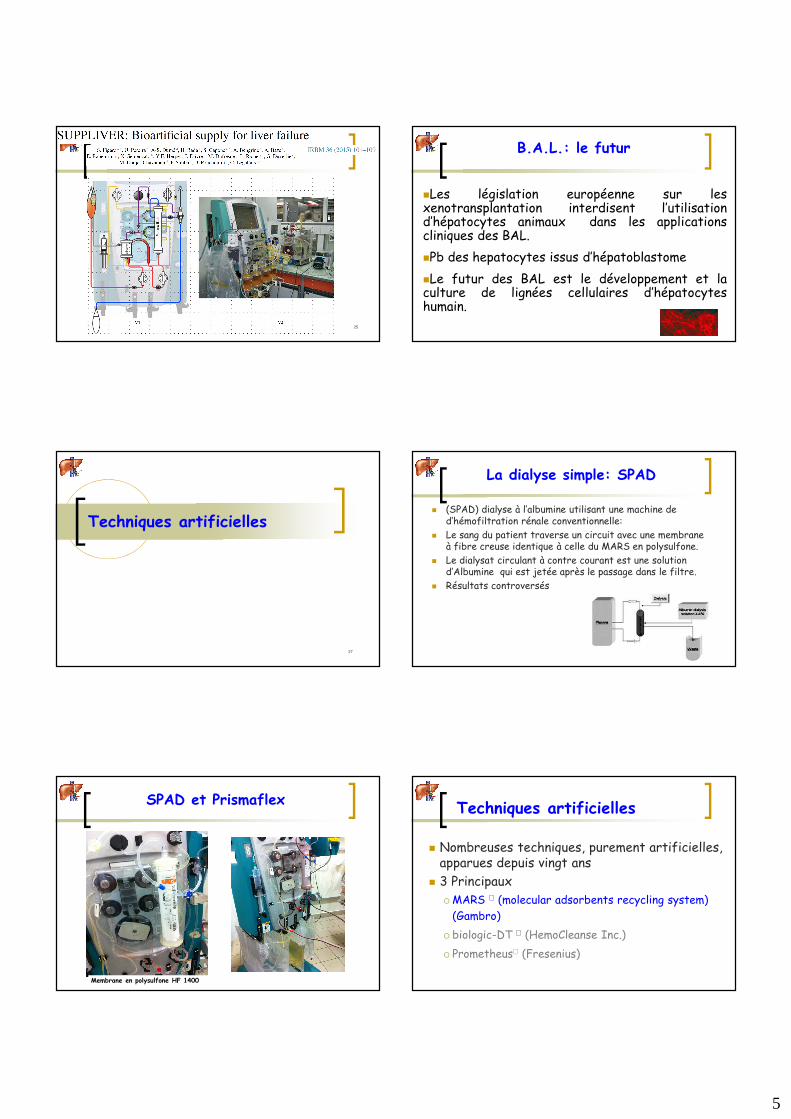
MARS
Blood circuit Dialysate circuitAlbumin circuit
MARS®FLUXdialyzer
diaFLUX dialyzer
diaMARS ® AC250 adsorber(Activated carbon adsorber)
diaMARS ® IE250 adsorber(Anionic exchanger) 32
MARS
33
La Membrane MARS
34
MOLECULES EPUREES
TOXINES
� Bilirubine
� Acides biliaires
� Ammoniac
� Benzodiazépines endogènes
� Digoxine
� Tryptophane
� NO
MEDICAMENTS
� Diazépam
� Furosémide
� Halopéridol
35
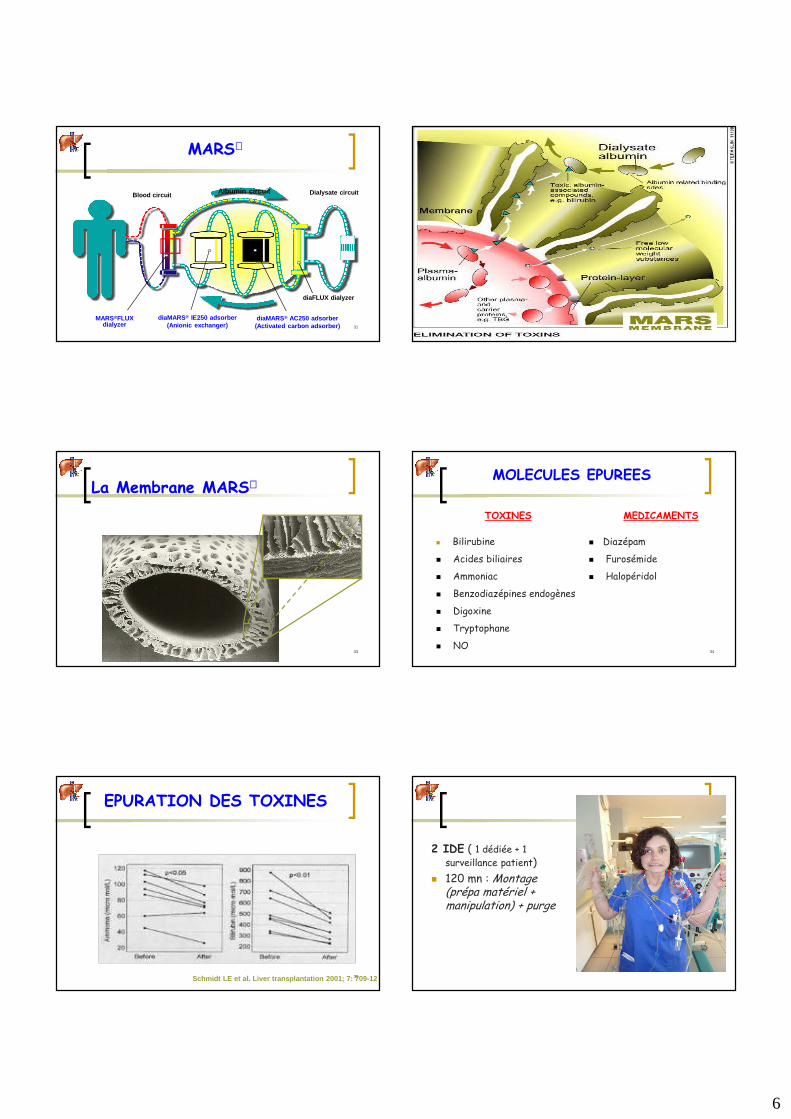
EPURATION DES TOXINES
Schmidt LE et al. Liver transplantation 2001; 7: 709-12
2 IDE ( 1 dédiée + 1
surveillance patient)
� 120 mn : Montage (prépa matériel + manipulation) + purge
7
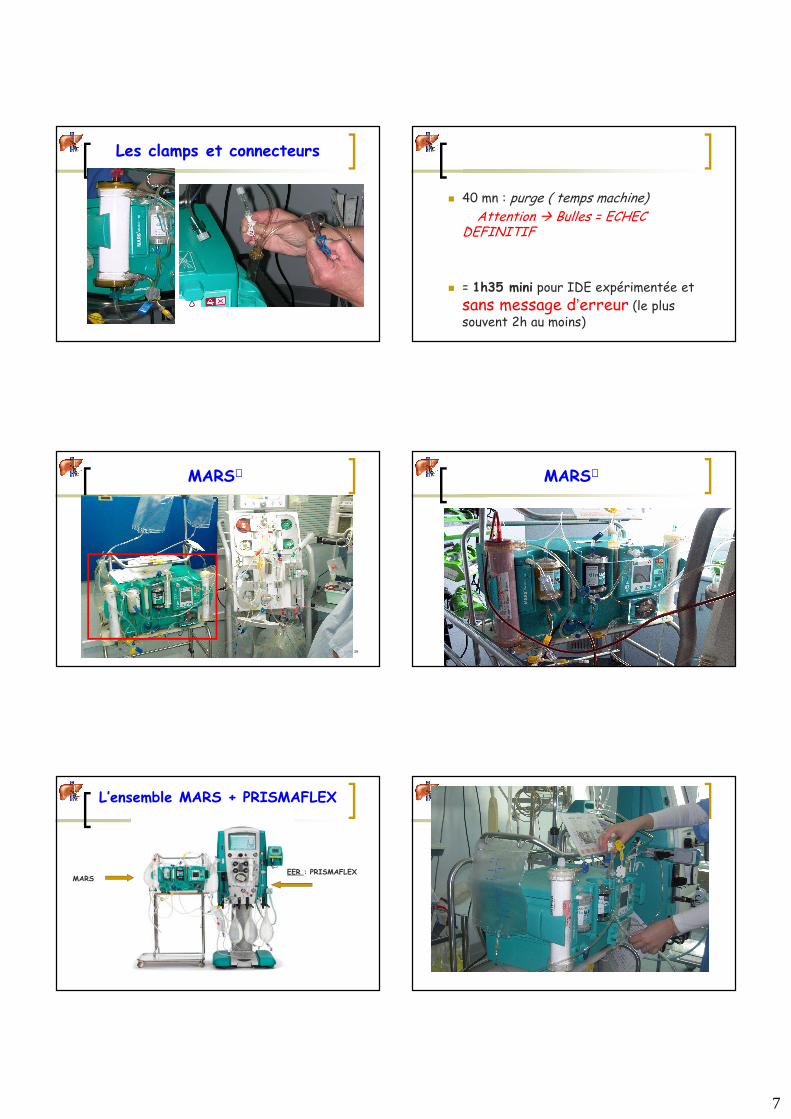
Les clamps et connecteurs
� 40 mn : purge ( temps machine)Attention � Bulles = ECHEC
DEFINITIF
� = 1h35 mini pour IDE expérimentée et
sans message d’erreur (le plus souvent 2h au moins)
39
MARS
40
MARS
L’ensemble MARS + PRISMAFLEX
MARSEER : PRISMAFLEX

8
Suppléance hépatique
45
Bilirubine adsorbée
46
MARS
Techniques artificielles
� Nombreuses techniques, purement artificielles, apparues depuis vingt ans
� 3 Principaux
� MARS (molecular adsorbents recycling system)
(Gambro)
� biologic-DT (HemoCleanse Inc.)
� Prometheus (Fresenius)
biologic-DT
9
Techniques artificielles
� Nombreuses techniques, purement artificielles, apparues depuis vingt ans
� 3 Principaux
� MARS (molecular adsorbents recycling system)
(Teraklin)
� biologic-DT (HemoCleanse Inc.)
� Prometheus (Fresenius)
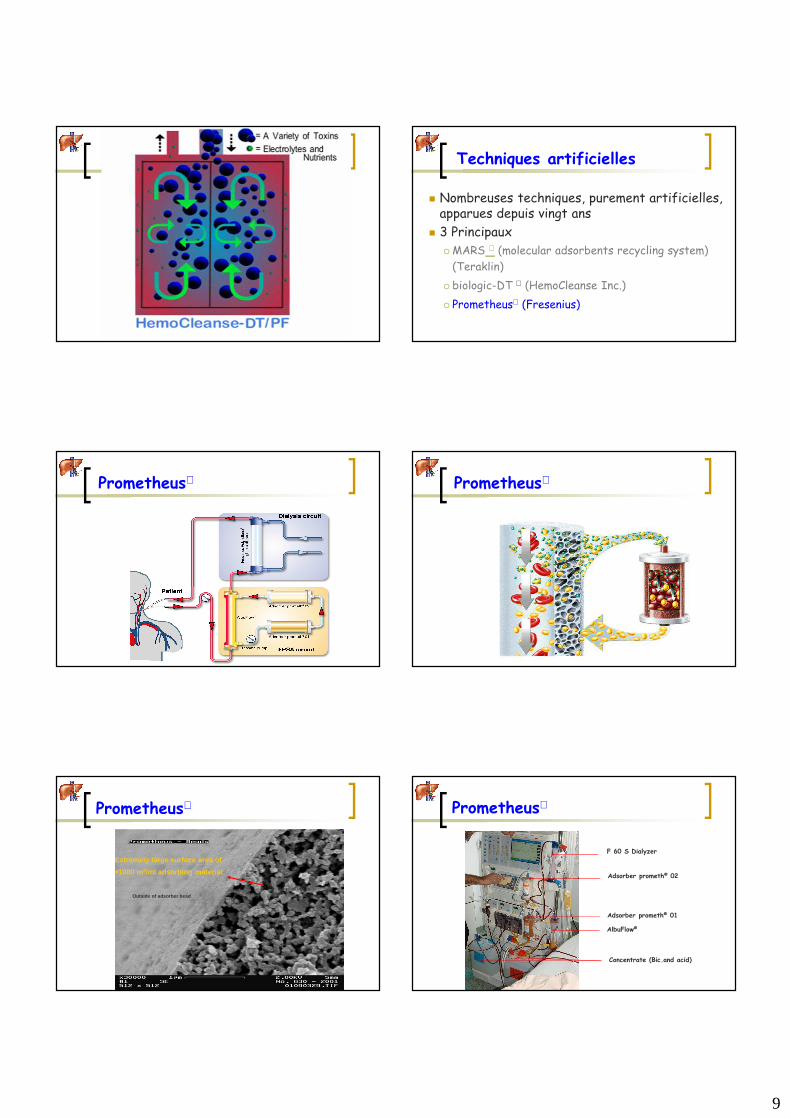
Prometheus Prometheus
Prometheus
Extremely large surface area of
>1000 m2/ml adsorbing material
Inside of adsorber bead
Outside of adsorber bead
Edge of break
Prometheus
AlbuFlow®
Adsorber prometh® 01
Adsorber prometh® 02
F 60 S Dialyzer
Concentrate (Bic.and acid)

10
Suppléance hépatique
Blood circuit
Dialysate circuit
Albumin circuit
MARS®FLUX
dialyzer
diaFLUXdialyzer
diaMARS® AC250 adsorber (Activated carbon adsorber)
diaMARS® IE250 adsorber (Anionic
exchanger)
Prometheus ®
MARS®
Techniques artificielles
� Traitement des hépatites aiguës et
chroniques acutisées
� Plusieurs études en cours et terminées
� Etude FULMAR / Etude Helios
� Attente des évaluations en cours
57
Prometheus: résultats
Evenepoel P. et al Blood purif 2005
58
Etude Helios
� 145 patients with ACLF were randomized to either SMT or additive treatment with Prometheus.
� Prometheus therapy was initiated for 3 weeks, and the primary end points were 28- and 90-day survival.
� Results
� There were no significant differences in baseline characteristics concerningMELD score, age or etiology of underlying chronic liver disease.
� In the intention-to-treat analysis, survival on day 28 was 66 versus 63% (p = 0.70; SMT plus Prometheus vs SMT) and on day 90 was 47 versus 38% (p = 0.35), respectively.
� In a predefined subgroup analysis, a significant survival benefit was observedunder FPSA therapy in patients with HRS type I (p = 0.04) or MELD score more than 30 (p = 0.02
Rifai K, Kribben A, Gerken G et al. Extracorporeal liver support by fractionated plasma separation and absorption (Prometheus®) in patients with acute-on-chronic liver failure
(HELIOS study): a prospective randomized controlled multicenter study. J. Hepatol. 2010
227 publications
64 Reviews & Comments17 animal studies
146 publications of use ofMARS in humans
126 uncontrolled studies- 57 case reports- 69 case series
20 controlled studies
8 randomized studieswith 178 patients (~ 4 %)
12 non-randomizedstudies
Approx. 15.000 treatmentsin > 4.500 patients
MARS
60
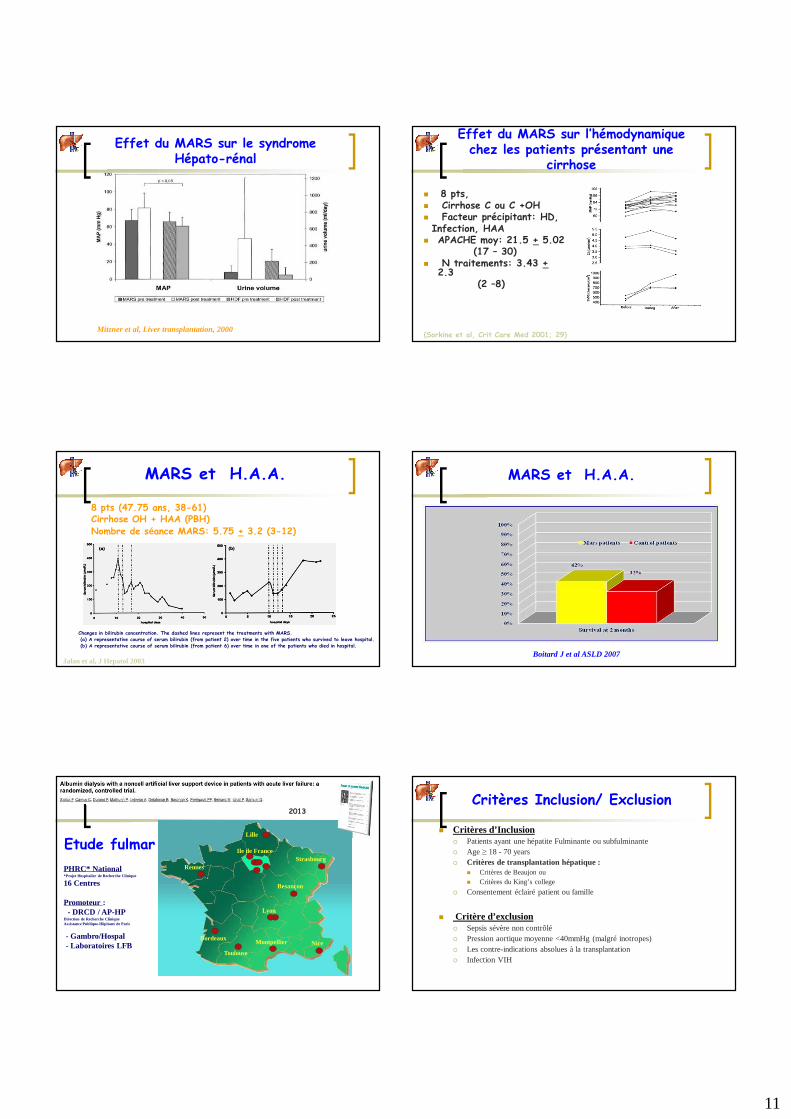
Effet du MARS sur le syndrome Hépato-rénal
Mitzner et al, Liver transplantation, 2000
Etude contrôlée randomisée: 13 patients avec HRS
8 traités par MARS et 5 par HDF
11
61
Effet du MARS sur le syndrome Hépato-rénal
Mitzner et al, Liver transplantation, 2000 62
� 8 pts, � Cirrhose C ou C +OH� Facteur précipitant: HD, Infection, HAA
� APACHE moy: 21.5 + 5.02 (17 – 30)
� N traitements: 3.43 +2.3
(2 –8)
(Sorkine et al, Crit Care Med 2001; 29)
Effet du MARS sur l’hémodynamique chez les patients présentant une
cirrhose
63
MARS et H.A.A.
8 pts (47.75 ans, 38-61)Cirrhose OH + HAA (PBH)Nombre de séance MARS: 5.75 + 3.2 (3-12)
Jalan et al, J Hepatol 2003
Changes in bilirubin concentration. The dashed lines represent the treatments with MARS.(a) A representative course of serum bilirubin (from patient 2) over time in the five patients who survived to leave hospital.(b) A representative course of serum bilirubin (from patient 6) over time in one of the patients who died in hospital.
64
MARS et H.A.A.
Boitard J et al ASLD 2007
65
Etude fulmarIle de France
Lille
StrasbourgRennes
Lyon
Bordeaux
Toulouse
Montpellier Nice
Besançon
PHRC* National*Projet Hospitalier de Recherche Clinique
16 Centres
Promoteur : - DRCD / AP-HP
Direction de Recherche CliniqueAssistance Publique-Hôpitaux de Paris
- Gambro/Hospal- Laboratoires LFB
2013
66
Critères Inclusion/ Exclusion
� Critères d’Inclusion� Patients ayant une hépatite Fulminante ou subfulminante� Age ≥ 18 - 70 years� Critères de transplantation hépatique :
� Critères de Beaujon ou� Critères du King’s college
� Consentement éclairé patient ou famille
� Critère d’exclusion� Sepsis sévère non contrôlé� Pression aortique moyenne <40mmHg (malgré inotropes)� Les contre-indications absolues à la transplantation� Infection VIH
12
67
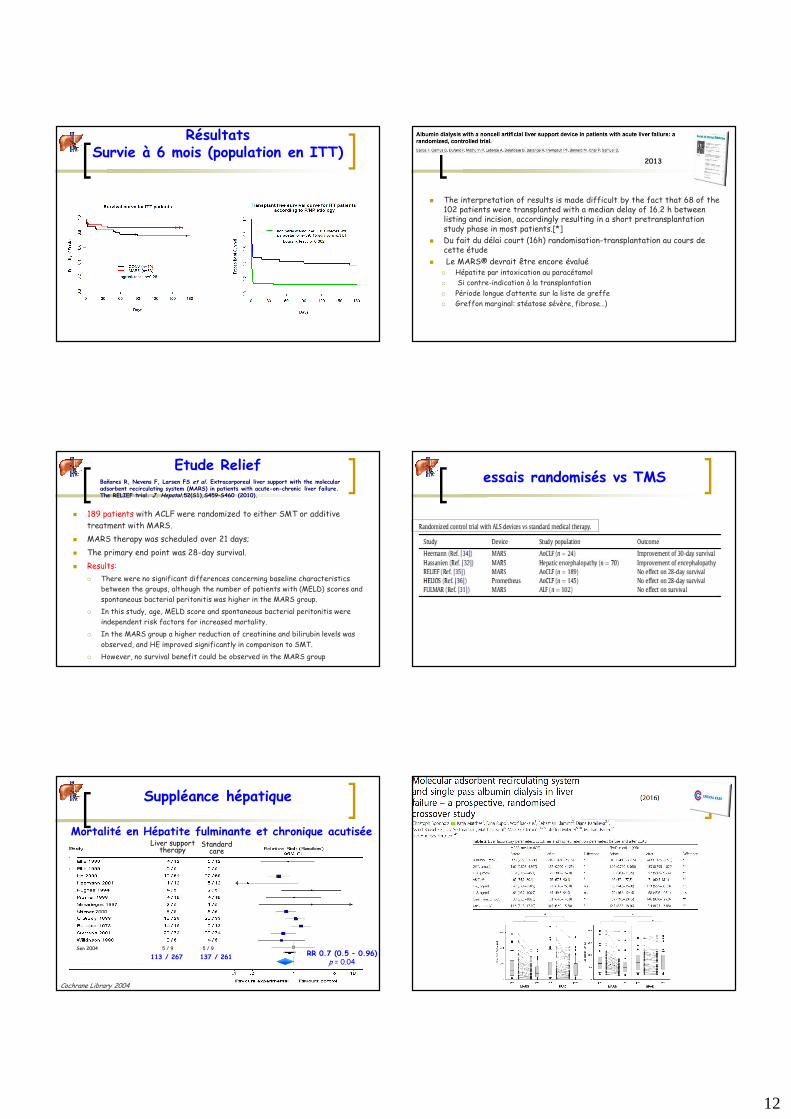
Résultats Survie à 6 mois (population en ITT)
68
� The interpretation of results is made difficult by the fact that 68 of the 102 patients were transplanted with a median delay of 16.2 h betweenlisting and incision, accordingly resulting in a short pretransplantationstudy phase in most patients.[*]
� Du fait du délai court (16h) randomisation-transplantation au cours de cette étude
� Le MARS® devrait être encore évalué� Hépatite par intoxication au paracétamol
� Si contre-indication à la transplantation
� Période longue d’attente sur la liste de greffe
� Greffon marginal: stéatose sévère, fibrose…)
2013
69
Etude Relief
� 189 patients with ACLF were randomized to either SMT or additive
treatment with MARS.
� MARS therapy was scheduled over 21 days;
� The primary end point was 28-day survival.
� Results:
� There were no significant differences concerning baseline characteristics
between the groups, although the number of patients with (MELD) scores and
spontaneous bacterial peritonitis was higher in the MARS group.
� In this study, age, MELD score and spontaneous bacterial peritonitis were
independent risk factors for increased mortality.
� In the MARS group a higher reduction of creatinine and bilirubin levels was
observed, and HE improved significantly in comparison to SMT.
� However, no survival benefit could be observed in the MARS group
Bañares R, Nevens F, Larsen FS et al. Extracorporeal liver support with the molecularadsorbent recirculating system (MARS) in patients with acute-on-chronic liver failure. The RELIEF trial. J. Hepatol.52(S1),S459–S460 (2010).
70
essais randomisés vs TMS
71
Mortalité en Hépatite fulminante et chronique acutisée
Cochrane Library 2004
RR 0.7 (0.5 – 0.96)p = 0.04
113 / 267 137 / 261
Sen 2004 5 / 9 5 / 9
Suppléance hépatique
Standard care
Liver support therapy
72

13
73 74
75 76
2015
77Time
Liver
func
tion
0%
100% Acute LF
Time
Liver
func
tion
0%
100%
Time
Liver
func
tion
0%
100%
Time
Liver
func
tion
0%
100% Acute on chronic LF Endstage liver disease
60 % 30 %
5 %5 %
SurgerySmall for size
Liver supportConclusion
� La suppléance hépatique est une voie de recherche très active
� Pathologie grevée d’une mortalité extrêmement élevée
� Potentiel de récupération de la fonction hépatique :
� Elevée
� Aléatoire
� Critères pronostiques et décisionnels ?
14
� Grand intérêt de suppléance fonctionnelle� Foie bioartificielle : L ’hépatite fulminante
� Stade développement et recherche, Infrastructures lourde
Plus pragmatique
� Dispositifs artificiels temporaires� Hépatopathie : Chronique accutisée, prurit +++, aiguë ?
� Hypoxies hépatique : Bas débit, résection…
« Bridge » vers la Greffe
� Intoxication par les inhibiteurs calciques
Conclusion
Related Documents