Statistics for the Interventionist Gregory J. Dehmer, MD Professor of Medicine, Texas A&M College of Medicine Director, Cardiology Division Scott & White Clinic Statistics means never having to say your certain

Statistics for the Interventionist Gregory J. Dehmer, MD Professor of Medicine, Texas A&M College of Medicine Director, Cardiology Division Scott & White.
Jan 02, 2016
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Statistics for the InterventionistStatistics for the InterventionistGregory J. Dehmer, MD
Professor of Medicine, Texas A&M College of Medicine
Director, Cardiology DivisionScott & White Clinic
Gregory J. Dehmer, MDProfessor of Medicine, Texas A&M College of
MedicineDirector, Cardiology Division
Scott & White Clinic
Statistics means never having to say your certain

SCAI Interventional Cardiology Fellows Course2007
Gregory J. Dehmer, MD, FSCAI
I have no relevant financial disclosures to make.

Expectations - HypothesisExpectations - Hypothesis
• You will completely understand statistics at the end of this brief talk
• This is inherently boring materialand I can’t fix that
• Provide some comments about studies and statistics that I hope are helpful
• You will completely understand statistics at the end of this brief talk
• This is inherently boring materialand I can’t fix that
• Provide some comments about studies and statistics that I hope are helpful
p=1.0
p<0.000000001

Some Things Are Just Really Bad IdeasSome Things Are Just Really Bad Ideas
Another Questionable CombinationAnother Questionable Combination
Hazardous equipment – Don’t operate unless you know what you are doing
+
The busy interventional cardiologist Statistics-in-a- Box“SYSTAT has every statistical
procedure you need”

You Will Be ReviewedYou Will Be Reviewed
• Many papers now undergo formal statistical review• Many papers now undergo formal statistical review
StatisticalConsultants
NEJMCirculationCirc Res
JACCetc . . .

Evolution of EvidenceEvolution of Evidence
Primary Evidence
Randomized
controlled trial
Observational studies
Uncontrolled trials
Descriptive studies
Case reports
Synthesized quantitativeData (meta-analyses)
Systematic reviews
Summary reviews
Opinions of respectedauthorities
Secondary Evidence

Evolution of EvidenceEvolution of Evidence
Primary Evidence
Randomized
controlled trial
Observational studies
Uncontrolled trials
Descriptive studies
Case reports
• Issues related to RTCs
– Exclusions
– Missing data
– Power calculations
– Confidence intervals
– Confusing endpoints “Non-inferiority”
• Issues related to RTCs
– Exclusions
– Missing data
– Power calculations
– Confidence intervals
– Confusing endpoints “Non-inferiority”

• Exclusion of cases is a major weakness (during analysis)
– Most common reason is a desire to ensure that all patients are “adequately treated”
– Awkward to retain a patient in the analysis who died during the 1st week of therapy or were unwilling to stick with the therapy
• Exclusion of cases is a major weakness (during analysis)
– Most common reason is a desire to ensure that all patients are “adequately treated”
– Awkward to retain a patient in the analysis who died during the 1st week of therapy or were unwilling to stick with the therapy
RTCs Problem 1: ExclusionsRTCs Problem 1: Exclusions

RTCs Problem 1: ExclusionsRTCs Problem 1: Exclusions
Exclusions more likely in: - the “aggressive treatment” arm or the “high-risk” group
• Likely to have more non-adherent patients
• Non-adherent patients are a higher risk group
• Exclusion of high-risk patients improved the average of the remaining patients
• If exclusions are permitted, the more aggressive arm appears artificially better
• Likely to have more non-adherent patients
• Non-adherent patients are a higher risk group
• Exclusion of high-risk patients improved the average of the remaining patients
• If exclusions are permitted, the more aggressive arm appears artificially better
Standard Therapy
More aggressive than standard therapyR
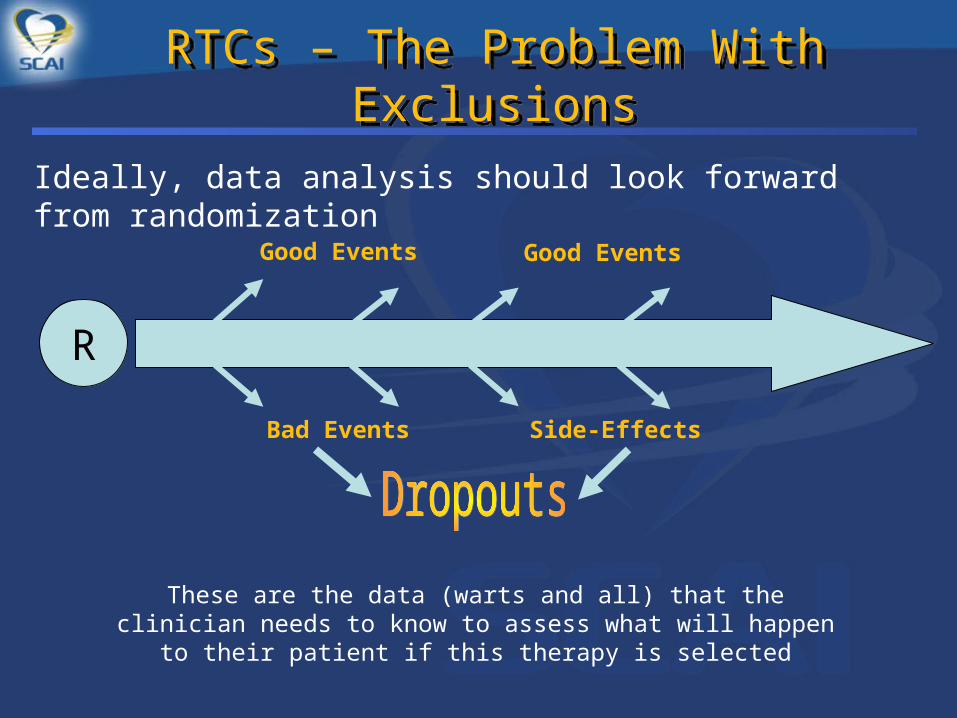
RTCs – The Problem With ExclusionsRTCs – The Problem With Exclusions
Ideally, data analysis should look forward from randomization
R
Good Events Good Events
Bad Events Side-Effects
These are the data (warts and all) that the clinician needs to know to assess what will happen to their patient if this therapy is selected

RTCs – The Problem With ExclusionsRTCs – The Problem With Exclusions
Data analysis when cases of inadequate treatment are excluded it like looking backward through rose-colored glasses
R
Good Events Good Events
Bad Events Side-Effects
Data Analysis
Excluding bad events and focusing only on the good results of the remaining cases may look impressive, but is not of practical value to clinicians who need to make
prospective therapy decisions for their patients.

RTC Lesson 1 – Avoid ExclusionsRTC Lesson 1 – Avoid Exclusions
Beware of potential bias
Check to see if the size of the analyzed groups are similar
R
n = 4932 n = 4931
n = 4100
Standard therapy New therapy
n = 4932

RTCs Problem 2: Missing DataRTCs Problem 2: Missing Data
45
50
55
60
65
70
Baseline 6 months 12 months 18 months 24 months
45
50
55
60
65
70
Baseline 6 months 12 months 18 months 24 months
LVE
F
Missing random data weakens the study, but is not a serious concern
However when data are missing because of aspects of treatment or disease, major bias can arise. Patients missing outcomes observations are more likely those with poor outcomes
# of patients: 200 120 50
Higher-risk ptsdon’t tolerate the therapy, drop out
leaving the low-riskpts who naturallyhave higher EFs

RTC Problem 2 - Beware of Missing DataRTC Problem 2 - Beware of Missing Data
•Make every effort to have data values at all key time points
– Can use “imputed values”
Carry previous measure forward
Inserting a conservative value
Averaging adjacent values
Computer models which use similar patients with complete information
•Make every effort to have data values at all key time points
– Can use “imputed values”
Carry previous measure forward
Inserting a conservative value
Averaging adjacent values
Computer models which use similar patients with complete information
RTC Problem 2 - Beware of Missing DataRTC Problem 2 - Beware of Missing Data
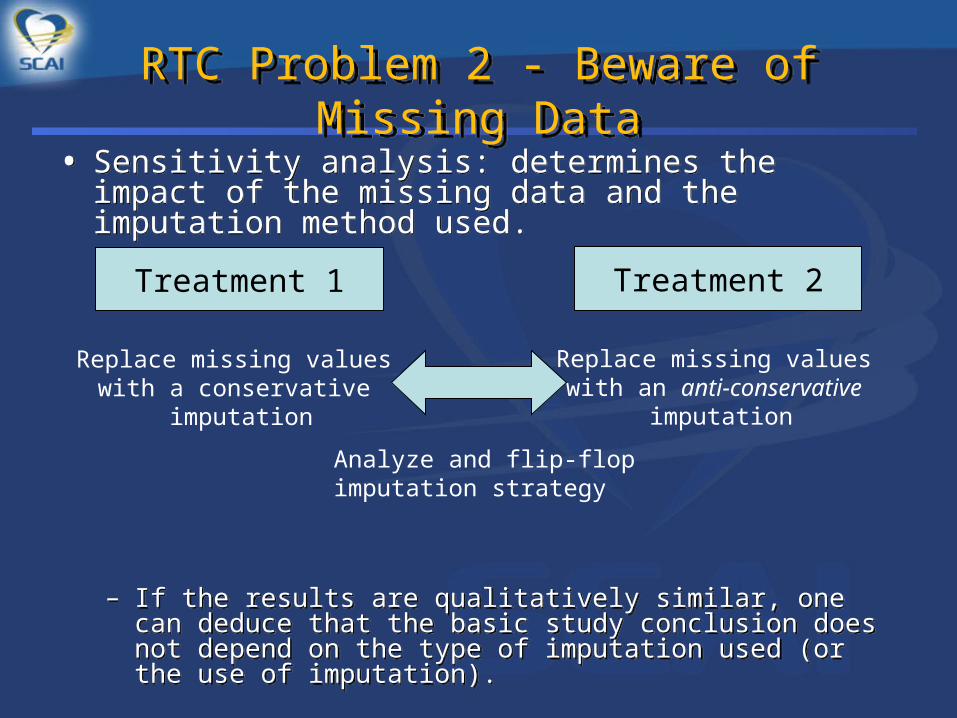
• Sensitivity analysis: determines the impact of the missing data and the imputation method used.
– If the results are qualitatively similar, one can deduce that the basic study conclusion does not depend on the type of imputation used (or the use of imputation).
• Sensitivity analysis: determines the impact of the missing data and the imputation method used.
– If the results are qualitatively similar, one can deduce that the basic study conclusion does not depend on the type of imputation used (or the use of imputation).
Treatment 1 Treatment 2
Replace missing values with a conservative
imputation
Replace missing values with an anti-conservative
imputation
Analyze and flip-flopimputation strategy

RTC Lesson 2 – Avoid Missing Data
RTC Lesson 2 – Avoid Missing Data
Rule of ThumbIf the proportion of cases excluded or with missing data in the size
of the treatment difference reported,the study is likely unreliable
Consolidated Standards for Reporting Trials
Lancet. 2001;357:1191–1194

RTCs Problem 3: Power CalculationsRTCs Problem 3: Power Calculations
Power calculation
• Determine what is a clinically meaningful difference between the two groups. (10%)
Would anyone care if the difference in restenosis was 2%?
• Amount of variation in the measurement of the endpoint (standard deviation)
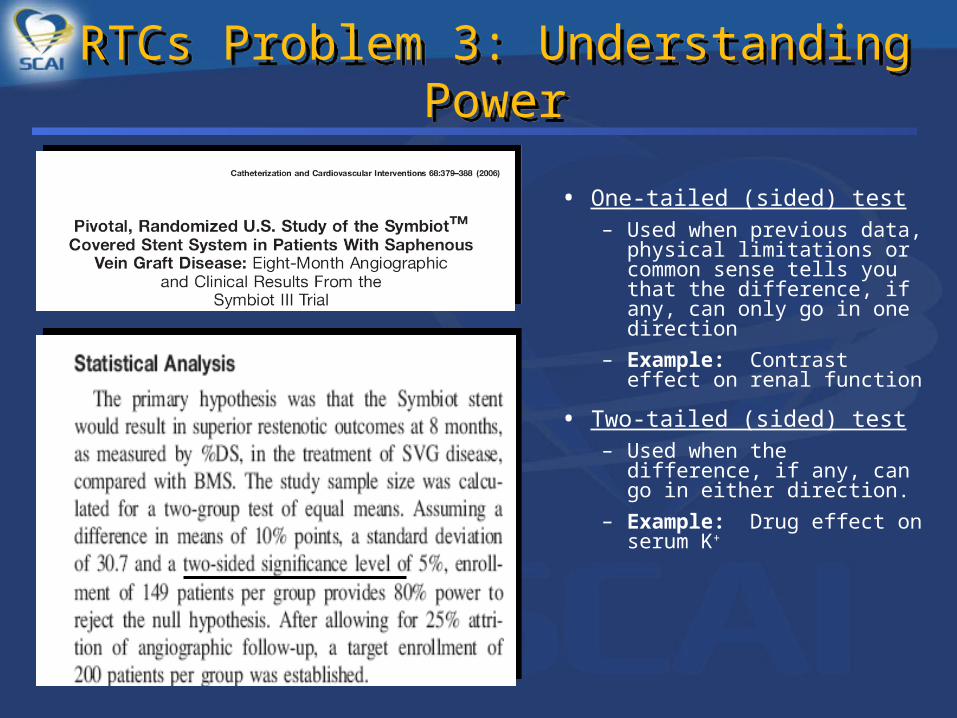
• One-tailed (sided) test– Used when previous data,
physical limitations or common sense tells you that the difference, if any, can only go in one direction
– Example: Contrast effect on renal function
• Two-tailed (sided) test– Used when the difference,
if any, can go in either direction.
– Example: Drug effect on serum K+
RTCs Problem 3: Understanding PowerRTCs Problem 3: Understanding Power
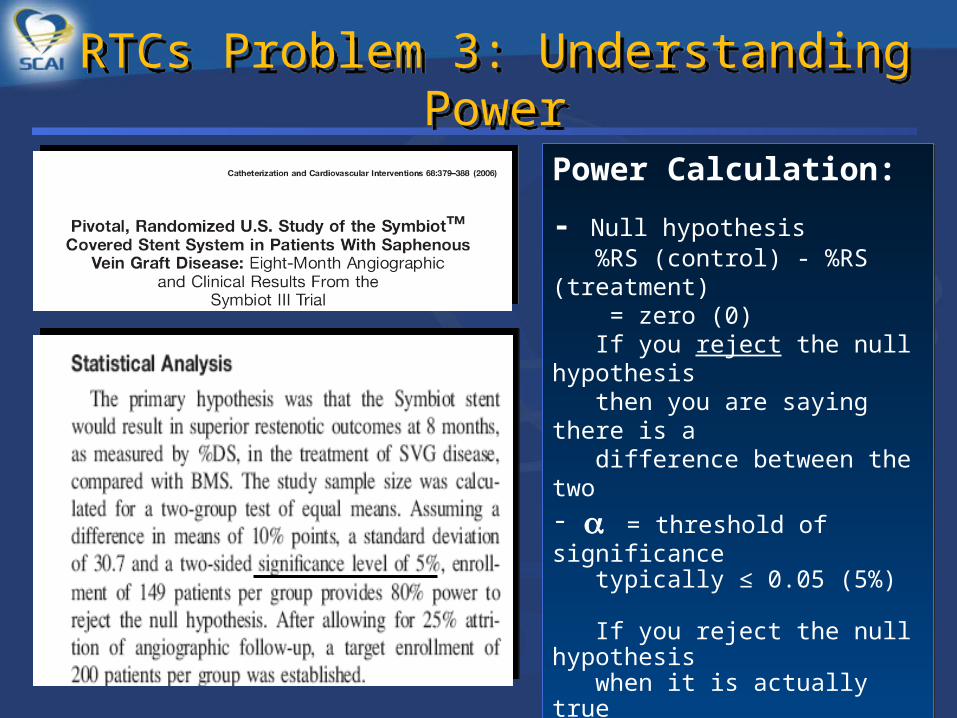
Power Calculation:
- Null hypothesis %RS (control) - %RS (treatment)
= zero (0) If you reject the null hypothesis then you are saying there is a difference between the two - = threshold of significance typically ≤ 0.05 (5%) If you reject the null hypothesis when it is actually true Type I error There is a ≤ 5% chance that there no difference, but your analysis concludes there is Probability of a Type I error =
Power Calculation:
- Null hypothesis %RS (control) - %RS (treatment)
= zero (0) If you reject the null hypothesis then you are saying there is a difference between the two - = threshold of significance typically ≤ 0.05 (5%) If you reject the null hypothesis when it is actually true Type I error There is a ≤ 5% chance that there no difference, but your analysis concludes there is Probability of a Type I error =
RTCs Problem 3: Understanding PowerRTCs Problem 3: Understanding Power

Power Calculation:- = threshold of significance typically ≤ 0.05
Saying there is a difference when there is none
- = the level you are willing to accept for the chance of missing an important difference when there really is one (20%) (Type II error)
Accepting the null hypothesis when it is, in fact, false
Power = 1 - 1 – 0.20 = 0.80 or 80%
RTCs Problem 3: Understanding PowerRTCs Problem 3: Understanding Power

RTC Lesson 3 – Know What Power MeansRTC Lesson 3 – Know What Power Means

RTCs Problem 4: Understanding CIsRTCs Problem 4: Understanding CIs
• Standard deviation– Relates to one data set
Fasting cholesterol of everyone in this room
Mean (average) SD is an expression of how
much spread there is around the mean value
• Equation for SD
• Standard deviation– Relates to one data set
Fasting cholesterol of everyone in this room
Mean (average) SD is an expression of how
much spread there is around the mean value
• Equation for SD SD mark the limits of scatter
Approximately 68% are within 1 SDApproximately 95% are within 2 SD
RTCs Problem 4: Understanding CIsRTCs Problem 4: Understanding CIs
• Confidence intervals
– Relate to populations (consider this room a population)
– Measure cholesterol in a sample of the population (n = 10)
– How well does the sample mean represent the population mean?
– 95% CI tells you that the mean of the population has a 95% chance (19 out of 20 times) of being within the range of the sample mean
• Confidence intervals
– Relate to populations (consider this room a population)
– Measure cholesterol in a sample of the population (n = 10)
– How well does the sample mean represent the population mean?
– 95% CI tells you that the mean of the population has a 95% chance (19 out of 20 times) of being within the range of the sample mean

RTCs Problem 4: Understanding CIsRTCs Problem 4: Understanding CIs

RTCs Lesson 4: Know Your CIsRTCs Lesson 4: Know Your CIs
• Confidence intervals– Each sample has a mean
and SD
– SEM = SD/ √n
– The 95% CI is ± 1.96 x SEM
– There is only a 5% chance that this range of values excludes the true population mean value
• Confidence intervals– Each sample has a mean
and SD
– SEM = SD/ √n
– The 95% CI is ± 1.96 x SEM
– There is only a 5% chance that this range of values excludes the true population mean value
0.0 0.3 0.5 0.8 1.0 1.3 1.5 1.8 2.0
#1
#2
#3
#4
Variable
RTCs Lesson 5: OR & RR Are Not the Same
RTCs Lesson 5: OR & RR Are Not the Same
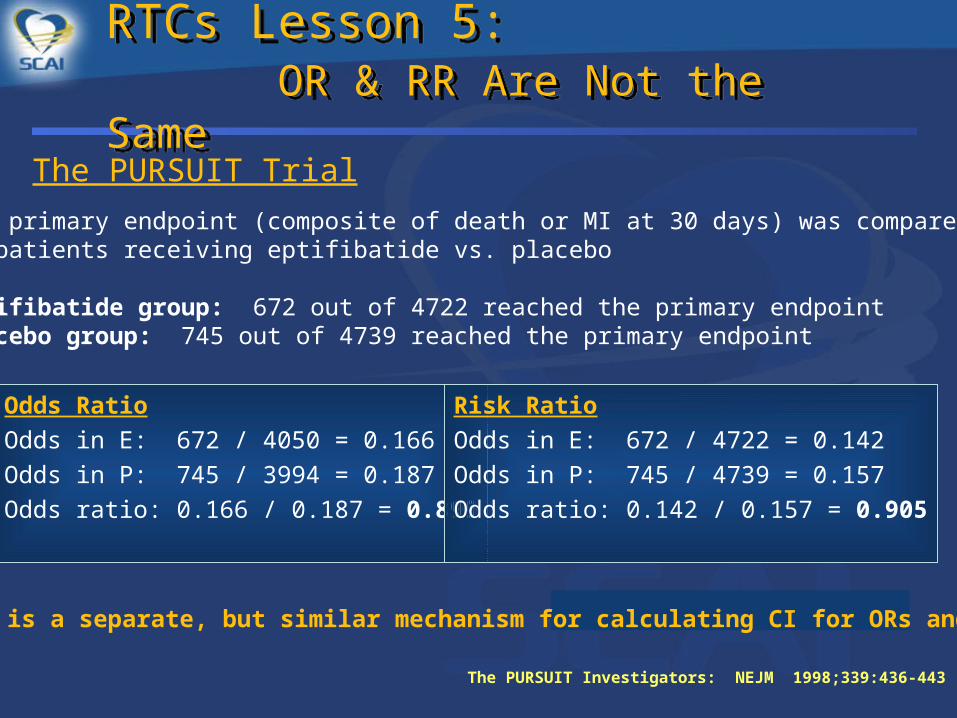
The PURSUIT Trial
The primary endpoint (composite of death or MI at 30 days) was comparedin patients receiving eptifibatide vs. placebo
Eptifibatide group: 672 out of 4722 reached the primary endpointPlacebo group: 745 out of 4739 reached the primary endpoint
Odds Ratio
Odds in E: 672 / 4050 = 0.166
Odds in P: 745 / 3994 = 0.187
Odds ratio: 0.166 / 0.187 = 0.899
Risk Ratio
Odds in E: 672 / 4722 = 0.142
Odds in P: 745 / 4739 = 0.157
Odds ratio: 0.142 / 0.157 = 0.905
The PURSUIT Investigators: NEJM 1998;339:436-443
There is a separate, but similar mechanism for calculating CI for ORs and RRs

RTCs Problem 5: Ratio ConfusionRTCs Problem 5: Ratio Confusion
Relationship between ORs and RRs for studies assessing harm
Each line on the graph relates to a different baseline prevalence, or event rate in the control group
When the prevalence of the event is low, say 1%, the RR is a good approximation of the OR For example, when the OR is 10, the RR is 9, an error of 10%
We can use this graph to get a grasp of how misleading it could be to interpret ORs as if they were RRs.
Rel
ativ
e R
isk
Odds Ratio

RTCs Problem 5: Ratio ConfusionRTCs Problem 5: Ratio ConfusionR
elat
ive
Ris
k
Odds Ratio
Relationship between OR and RR for studies which are assessing benefit
Each line on the graph relates to a different baseline prevalence, or event rate in the control group
When event rates are very low the approximation is close, but breaks down as event rates increase
For example, if the event rate is 50% and there is a 20% reduction in the odds, the relative risk adjustment will be little over 10%
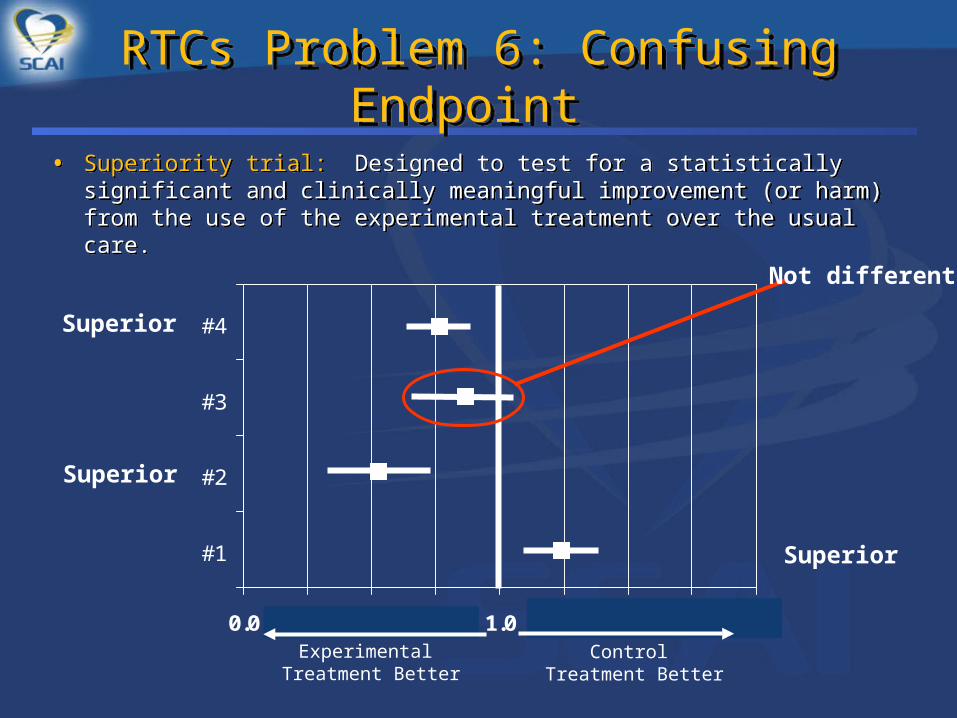
RTCs Problem 6: Confusing Endpoint RTCs Problem 6: Confusing Endpoint
• Superiority trial: Designed to test for a statistically significant and clinically meaningful improvement (or harm) from the use of the experimental treatment over the usual care.
• Superiority trial: Designed to test for a statistically significant and clinically meaningful improvement (or harm) from the use of the experimental treatment over the usual care.
0.0 0.3 0.5 0.8 1.0 1.3 1.5 1.8 2.0
#1
#2
#3
#4
Experimental Treatment Better
Control Treatment Better
Superior
Superior
Superior
Not different
RTCs Problem 6: Confusing Endpoint RTCs Problem 6: Confusing Endpoint
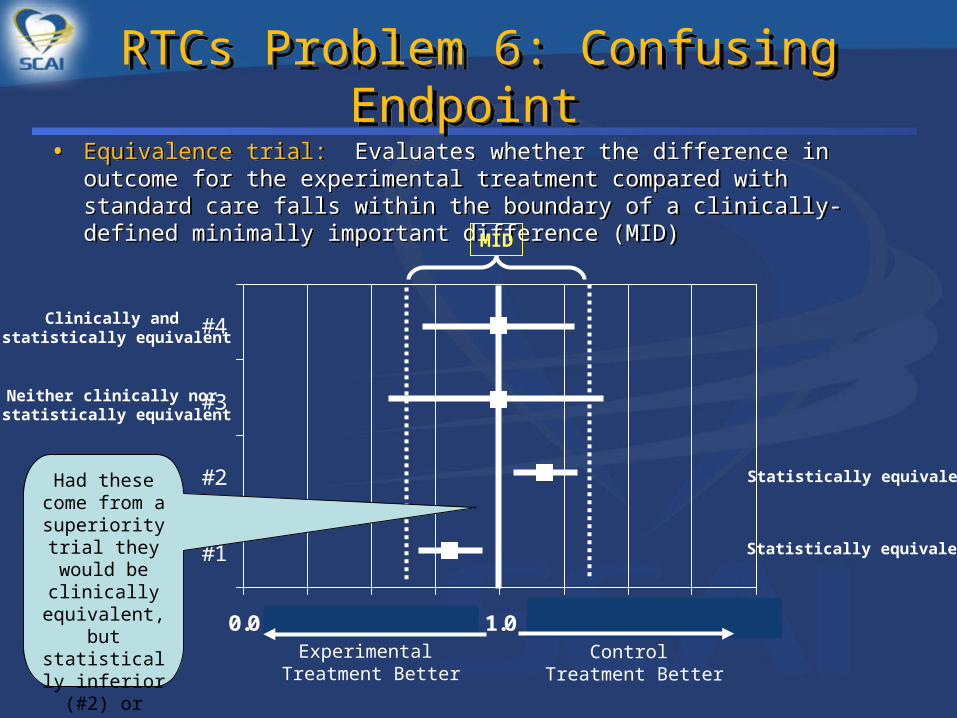
• Equivalence trial: Evaluates whether the difference in outcome for the experimental treatment compared with standard care falls within the boundary of a clinically-defined minimally important difference (MID)
• Equivalence trial: Evaluates whether the difference in outcome for the experimental treatment compared with standard care falls within the boundary of a clinically-defined minimally important difference (MID)
0.0 0.3 0.5 0.8 1.0 1.3 1.5 1.8 2.0
#1
#2
#3
#4
Experimental Treatment Better
Control Treatment Better
MID
Clinically and statistically equivalent
Neither clinically nor statistically equivalent
Statistically equivalent
Statistically equivalent
Had these come from a
superiority trial they would be
clinically equivalent, but
statistically inferior (#2) or superior (#1)

RTCs Problem 6: Confusing Endpoint RTCs Problem 6: Confusing Endpoint
• Noninferiority trial: Results are evaluated assuming that the experimental treatment is not worse than the standard treatment by a clinically-meaningful amount.
• Noninferiority trial: Results are evaluated assuming that the experimental treatment is not worse than the standard treatment by a clinically-meaningful amount.
0.0 0.2 0.4 0.6 0.8 1.0 1.2 1.4 1.6 1.8 2.0
#1
#2
#3
#4
Experimental Treatment Better
Control Treatment Better
Not inferior
Not inferior
CI does not crossthe MID
CI too wide for any conclusions
CI crosses MIDindicating
inferiority of the experimental Rx
MID

ResourcesResources
• http://www.jr2.ox.ac.uk/bandolier/
• http://www.statsoft.com/textbook/stathome.html
• http://www.bettycjung.net/Statsites.htm
• http://www.tufts.edu/~gdallal/bmj.htm– Link to Br Med J series of papers on statistics
• 2006-2007 Circulation series “Statistical Primer for Cardiovascular Research”
• Motulsky H. Intutitive Statistics. Oxford University Press 1995
A statistician is a person who comes to the rescue of figures that cannot lie for themselves
RememberRemember
Statistics are like a bikini. What they reveal is suggestive, but what they conceal is vital
Related Documents









![Stuctural Analysis of Molecular Networks: AMES Mutagenicityworldcomp-proceedings.com/proc/p2011/BIC4306.pdf · Dehmer et al. [Dehmer et al., 2010] used entropy-based descriptors [Dehmer](https://static.cupdf.com/doc/110x72/5f2f3c342f6dda55bc19971c/stuctural-analysis-of-molecular-networks-ames-mutagenicityworldcomp-dehmer-et.jpg)

