Should we be evaluating patients in the hospital for gastropareis? If so, who?

Should we be evaluating patients in the hospital for gastropareis? If so, who?
Dec 18, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Should we be evaluating patients in the hospital for gastropareis?
If so, who?
Patient 1
• 47 y/of F with Type I DM who has a history of recurrent admissions for abdominal pain and intractable N/V who presents with a recurrence of these symptoms – requiring admission because of her pain and inability to keep down fluids

Patient 2
• 60 y/o obese M with Type II DM who presents with osteo of his foot.
• During the evaluation he reports post-prandial bloating and nausea which cause him to occasionally need to lie quietly after meals until the symptoms resolve.
Patient 3
• 50 y/o F with Type II DM who is admitted with CAP.• She reports that she and her PCP have not been
able to get good control of her DM as an outpatient.• As an inpatient she has widely fluctuating BS –
ranging from 38 ( at which point she is symptomatic) to greater than 200.
• Despite repeated appropriate adjustments in her insulin regimen and an Endo consult her BS continues to fluctuate significantly.
Questions:
• Which of these patients should have an inpatient work-up for gastroparesis?
• For Patient 1, how should we treat her abdominal pain?
Goals of the talk:
• Review normal gastric physiology related to meal ingestion and emptying
• Overview of the pathophysiology of gastroparesis
• Review typical etiologies of gastroparesis• Presentation of gastroparesis• Diagnostic work-up of gastroparesis – and
limitations.• Discuss acute management of pain in patients
with gastroparesis.

Main points to take away from the presentation:
• Gastroparesis is a common problem which is manifested in a variety of ways both with respect to clinical presentation and pathophysiology.
• Diagnosis of gastroparesis should at a minimum an evaluation for proof of delayed gastric emptying as well as an evaluation for alternative causes of delayed gastric emptying such as obstruction, cancer, or peptic ulcer disease.
• The diagnosis of gastroparesis is made when other causes of delayed gastric emptying are ruled out and delayed gastric emptying is demonstrated – preferably through obtaining a gastric emptying study showing > than 60% retention of a low fat meal after 2 hours and > 10% retention after 4 hours. (the 2 hour mark is more specific and the 4 hour mark more sensitive –
• Gastroparesis may cause unexpectedly wide variations in blood sugar in some diabetics without presenting any of the more typical symptoms of the condition.
Normal Physiology• As food enters the stomach the muscles in the proximal stomach relax to
accommodate solids.• Liquids will enter the proximal small bowel first. The presence of
nutrients – especially fats and sugar will result in release of hormones and neural feedback to cause relaxation of the fundus of the stomach, suppressing of antral contractions and stimulates tonic pyloric activity. Effectively this allows the stomach to fill and food to be stored as processing begins.
• When feedback from the small bowel is reduced antral activity increases in response to electrical slow waves which originate from a gastric pacemaker near the esophagus and spreads through the layer of circular gastric muscle– the fundus remains relaxed, though tone increases over time and the pylorus continues tonic and phasic contractions. The overall effect is that food is delivered in a controlled fashion to the antrum and pylorus where it is ground and sieved to be delivered to the small bowel. The rate is mediated by feedback from the small bowel.

Pathophysiology of Gastroparesis
• The pathophysiology of gastroparesis has not been fully developed and the condition is not homogenous – even amongst the various subgroups who characteristically develop gastroparesis. So, not all diabetics will exhibit the same mechanism. However the final pathway to symptoms seems to be dysregulation of normal gastric emptying physiology so that the proximal stomach or fundus may not relax normally, the antrum may not relax or it might not increase its activity as it should, the pylorus may not maintain its normal tone – or it might have elevated tone. The various treatments which are tried are aimed at different potential mechanisms.
Abdominal pain in gastroparesis – does not correlate with other symptoms
• The cause of pain in patients with gastroparesis is not well understood. Pain does not seem to correlate with resolution of the other symptoms.
• A small study in diabetics with gastroparesis showed that they had an exaggerated pain response evoked by gastric distension suggesting that there may be a yet to be defined sensory nerve component which produces a heightened sensitivity to noxious stimuli.
• • Samsom M., Vermeijden J.R., Smout A.J., et al: Prevalence of
delayed gastric emptying in diabetic patients and relationship to dyspeptic symptoms: a prospective study in unselected diabetic patients. Diabetes Care 26. 3116-3122.2003;
Abdominal pain in gastroparesis - continued
• Pain is a common presenting complaint of gastroparesis. Treatment of pain associated with gastroparesis has not been studied in any clinical trials. Various medications such as tricyclics, opiods, and NSAIDs have all been used. None have been shown to be superior.
• Given the lack of data, pain management varies significantly. We will discuss our personal approaches at the end of the talk.

Some diabetics may only manifest poor glycemic control
• In fact, there is poor correlation between all the typical symptoms of gastroparesis and demonstration of delayed gastric emptying. So, there is, especially amongst diabetics, a subset of patients who have significantly delayed gastric emptying, but none of the typical symptoms. These patients may manifest only episodes of unexplained hypo- or hyperglycemia, or difficult to control diabetes.
• • Annese V, Bassotti G, Caruso N, et al. Gastrointestinal motor• dysfunction, symptoms, and neuropathy in noninsulin-
dependent• (type 2) diabetes mellitus. J Clin Gastroenterol 1999;29:171e7.
Etiologyof gastroparesis
• Major causes • Idiopathic • Diabetes mellitus • Postsurgical• • Less common causes • Connective tissue disease • Ischemia • Cancer • Neurologic disease (including Parkinson's) • Eating disorders • Metabolic/endocrine conditions • Medications (e.g. anticholinergics, calcium channel antagonists and opiates) • Critical illness
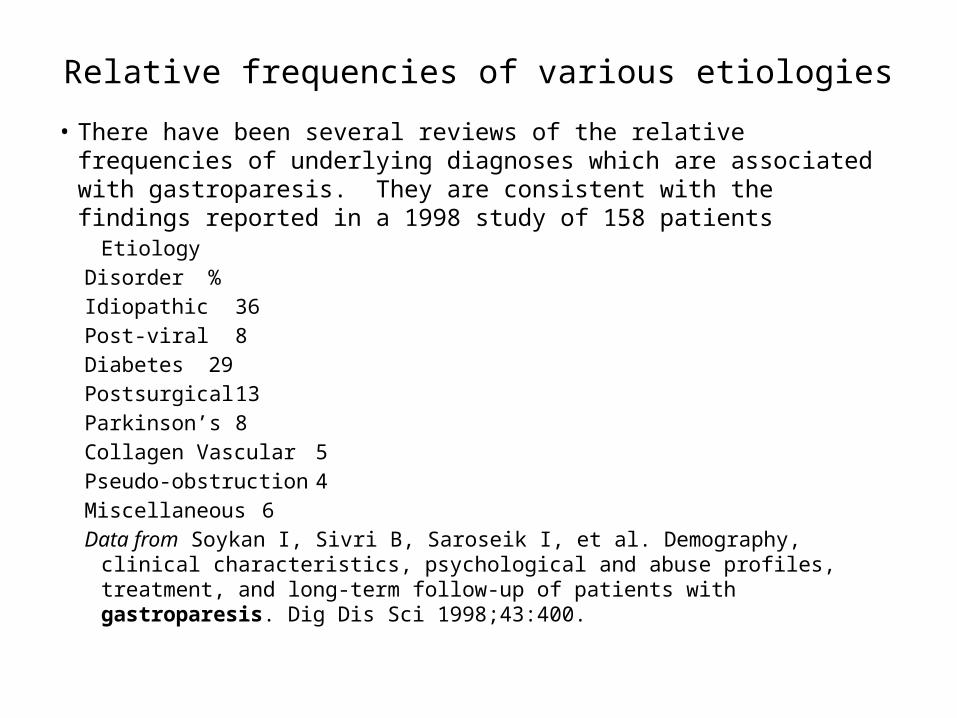
Relative frequencies of various etiologies• There have been several reviews of the relative frequencies of underlying
diagnoses which are associated with gastroparesis. They are consistent with the findings reported in a 1998 study of 158 patients
EtiologyDisorder %Idiopathic 36Post-viral 8Diabetes 29Postsurgical 13Parkinson’s 8Collagen Vascular 5Pseudo-obstruction 4Miscellaneous 6Data from Soykan I, Sivri B, Saroseik I, et al. Demography, clinical characteristics,
psychological and abuse profiles, treatment, and long-term follow-up of patients with gastroparesis. Dig Dis Sci 1998;43:400.
Typical presentation
• Patients will present with:• Nausea 92%• Vomiting 84%• Bloating 75%• Early satiety 60%• Pain 46 - 89%• The pain in gastroparesis is usually epigastric, worse at night or after meals and
burning or cramping. Frequently the pain is constant, but sometimes colicky.• • Exam is usually non-specific. Depending on duration of symptoms and ability
to keep down food or fluids patients may demonstrate evidence of dehydration.
• Patients may have diffuse abdominal tenderness, but lack peritoneal signs.• • Hoogerwerf WA, Pasricha PJ, Kalloo AN, et al. Pain: the overlooked symptom in
gastroparesis. Am J Gastroenterol 1999;94:1029–33

Lab studies
• Also non-specific.• Occasionally patients with Type I DM will
present with DKA.• Also in diabetics patients may present with
either marked hypo- or hyperglycemia.• There may be electrolyte disturbances such as
hypokalemia.• Non-specific markers of systemic
inflammation, such as CRP, may be elevated as well.
Radiographic studies
• Initial radiographic studies should be aimed at investigating the possibility of intestinal obstruction or perforation.
• KUB and upright of the abdomen are usually recommended, though a CT to evaluate for appendicitis, colitis, abscess, or neoplasm may also be warranted early in the work-up - especially for patients in whom pain is one of the primary complaints.
• A barium swallow, with small bowel follow through may be useful in identifying structural abnormalities as well as delayed emptying - and this has been suggested as sufficient evidence to make the diagnosis of gastroparesis and for initiation of therapy in one study.
• Clincal Radiology, 2008 Apr;63(4):407-14. Epub 2007 Dec 20.• An 8-year review of barium studies in the diagnosis of gastroparesis.
Levin AA, Levine MS, Ruibesin SE, Lauger I.

Next (or eventual step)
• However, the American Gastroenterological Association recommendations are to obtain upper endoscopy as the next test rather than barium swallow. There is the rationale from the proceduralists that an endoscopy affords the opportunity to obtain biopsies if warranted. And, if the patient does have significantly delayed gastric emptying this more definitive test may be delayed while waiting for the barium to clear sufficiently.
• While upper endoscopy cannot diagnose gastroparesis, retained food after an overnight fast suggests gastroparesis.
• • GASTROENTEROLOGY 2004;127:1592–1622

Gastic Emptying Study• The gold standard for demonstration of delayed
gastric emptying is the nuclear gastric emptying study. In this test the patient is fed a low fat diet with solid food that has been tagged with Technetium 99 sulfur colloid (usually scrambled eggs or Egg Beaters). The meal must be low fat because fat can delay gastric emptying. The test is usually performed with a solid meal because liquids may pass the pylorus even in the absence of normal gastric motility (a similar study using a liquid meal is sometimes used when dumping syndrome is suspected).
Interpretation of Gastic Emptying Study
• The patient is then imaged at 1, 2 and 4 hours to evaluate the percentage of tagged food which remains in the stomach.
• Though there is not universal standardization of criteria (because gastroparesis may affect either the early phase of gastric emptying or the later phases) it is generally accepted that 60% of the meal retained in the stomach at 2 hours or 10% at 4 hours is consistent with a diagnosis of delayed gastric emptying.
Factors which may affect the accuracy of a gastric emptying study
• Patients who are on medications which slow gastric motility (calcium channel blockers, opiates, TCA, antihistamines, fiber, PPIs, nicotine patch, etc.).
• Smoking can delay gastric emptying.• High blood sugar (> 270 mg/dL) delays gastric emptying.• Patients with sepsis, hypocalcemia, anemia.• These patients may have a false positive tests.• • Some medications accelerate gastric emptying:
Betablockers, macrolides, Reglan.• Patients on these medications may have a false negative
test.

• Given that the gastric emptying test is considered the gold standard - it is the test with which other potential tests are compared to evaluate their accuracy - do we need others?
• Perhaps...the test is more expensive than some other options and the patient does have to go to a center which has the capability to perform the test. There is also some concern about exposure to radiation, but this is minimal and the only subset of patients who are recommended to not have the test because of the risk of radiation exposure are pregnant women.
• The biggest concern with the gastric emptying test is the lack of standardization - though this does not prevent the test from being recommended by the American College of Gastroenterology.
•
• Quick Review of some other tests which might be used to diagnose delayed gastric emptying

. Gastroduodenal manometry
• Addresses the issue of radiation exposure. However, it is more expensive and it is invasive. It does offer the potential that it has been shown to be useful in predicting the patient's ability to tolerate tube feeding.
• Thumshirn M, Bruninga K, Camilleri M. Simplifying the evaluation of postprandial antral motor function in patients with suspected gastroparesis. Am J Gastroenterol 1997;92:1496e500.
Transabdominal ultrasound
• it is neither invasive nor does it involve radiation, but it is expensive, can only be done in centers where the procedure is available, and requires a high degree of technical expertise. Transabdominal ultrasound, carried out correctly correlates very well with gastric emptying studies.
• • Undeland KA, Hausken T, Svebak S, et al. Wide gastric antrum
and low vagal tone in patients with diabetes mellitus type 1 compared to patients with functional dyspepsia and healthy
• individuals. Dig Dis Sci 1996;41:9e16.

Breath Test
• Use of breath tests to identify the relative concentrations of non-radioactive carbon isotopes.
• C-13 is incorporated into a meal. The meal is ingested and then breath tests are taken at regular intervals. The relative concentrations of C-13 in expired air will demonstrate the time from ingestion to metabolism - the rate limiting step in the process is gastric emptying. This gives a valid representation of gastric emptying (in diabetics) and has been shown to be reliable enough to demonstrate improved gastric motility in patients given erythromycin.
• The test is relatively cheap, is non-invasive, avoids exposure to radiation and can be performed in an office.
• The limitations to the test are primarily related to the unknown variable of how valid it is in patients with pancreatic, liver, or lung.
• • Szarka LA, Camilleri M, Vella A, et al. A stable isotope breath• test with a standard meal for abnormal gastric emptying of solids• in the clinic and in research. Clin Gastroenterol Hepatol• 2008;6:635e43 e1.

So, what should we do in the hospital?• The recommended approach is to make the
diagnosis before initiating treatment.• However because of the nature of the
patient’s presentation they may not be able to have the testing done.
• Who should we test?• Who should we treat without completion of
the diagnostic work-up?

• There are five groups of patients who might be in the hospital with gastroparesis:
• • 1. Patients at risk, but with no symptoms.• 2. Patients who present for reasons other than the typical
symptoms of gastroparesis but who have a review of systems that raises suspicion.
• 3. Patients who develop symptoms suggestive of gastroparesis while hospitalized for some other problem.
• 4. Patients who come to the hospital with symptoms suggestive of gastroparesis as their presenting complaints.
• 5. Diabetics with unexplained widely fluctuating blood sugar.

• What do we do with patients who have known gastroparesis and present as the patient discussed above wher pain is one of the main complaints?
Related Documents











