1 Role of Private Duty in Healthcare Reform : Integrated Chronic Care Management ©2010 Beth Hennessey, All rights reserved Management 6 th Annual Private Duty Leadership Summit & Exposition January 24, 2011 Objectives Highlight the business case for integrated chronic care management as a strategic focus of private duty homecare and healthcare reform healthcare reform. Describe the foundation & tenets of a patient focused evidenced based care delivery model. Identify the “retooling” necessary for replication & success ©2010 Beth Hennessey, All rights reserved replication & success. Discuss the importance of private duty homecare demonstrating value and partnerships for transitions of care, community based teams, and ACOs.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1
Role of Private Duty in Healthcare Reform :
Integrated Chronic Care Management
©2010 Beth Hennessey, All rights reserved
Management
6th Annual Private Duty Leadership Summit & ExpositionJanuary 24, 2011
ObjectivesHighlight the business case for integrated chronic care management as a strategic focus of private duty homecare and healthcare reformhealthcare reform.
Describe the foundation & tenets of a patient focused evidenced based care delivery model. Identifythe “retooling” necessary for replication & success
©2010 Beth Hennessey, All rights reserved
replication & success.
Discuss the importance of private duty homecare demonstrating value and partnerships for transitions of care, community based teams, and ACOs.

2
Journey to Excellence
©2010 Beth Hennessey, All rights reserved
Our Patients’ Healthcare Experience
©2010 Beth Hennessey, All rights reserved

3
IOM Quality Chasm ReportConclusions
C t h lth t • Current healthcare systems cannot do the job
• Trying harder will not work• Changing care systems
will work
©2010 Beth Hennessey, All rights reserved
will work• Make the right thing to do
the easy thing to do
Innovative Leadership:
Looking at your business through a different lens
©2010 Beth Hennessey, All rights reserved

4
A New Way of Seeing:Reversing the Flow of Healthcare
Current Flow Reversed Flow
Policy & Regulation Policy & Regulation
Payment Methodology Payment Methodology
©2010 Beth Hennessey, All rights reserved
Provider Practices Provider Practices
Patient’s Health Needs
Chronic Disease• “Non communicable illnesses that are
prolonged in duration, do not resolve t l d l d spontaneously, and are rarely cured
completely. “ (CDC) • Most costly are heart conditions, cancer,
COPD, asthma, mental disorders, & trauma related disorders.
©2010 Beth Hennessey, All rights reserved
• Bulk of expenditures are on hospitalizations and physician services
IOM “ the Role of Human Factors in Home Care : Workshop Summary” © 2010
5
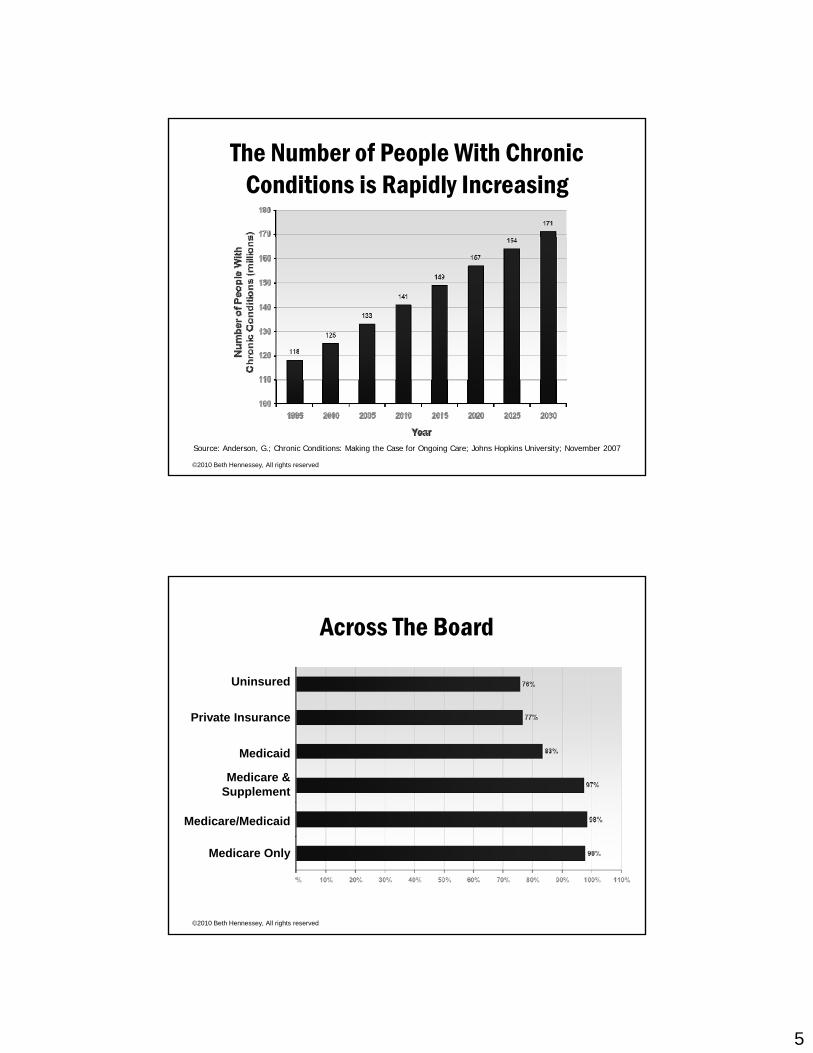
The Number of People With Chronic Conditions is Rapidly Increasing
©2010 Beth Hennessey, All rights reserved
Source: Anderson, G.; Chronic Conditions: Making the Case for Ongoing Care; Johns Hopkins University; November 2007
Across The Board
Uninsured
Private Insurance
Medicaid
Medicare & Supplement
©2010 Beth Hennessey, All rights reserved
Medicare/Medicaid
Medicare Only
6
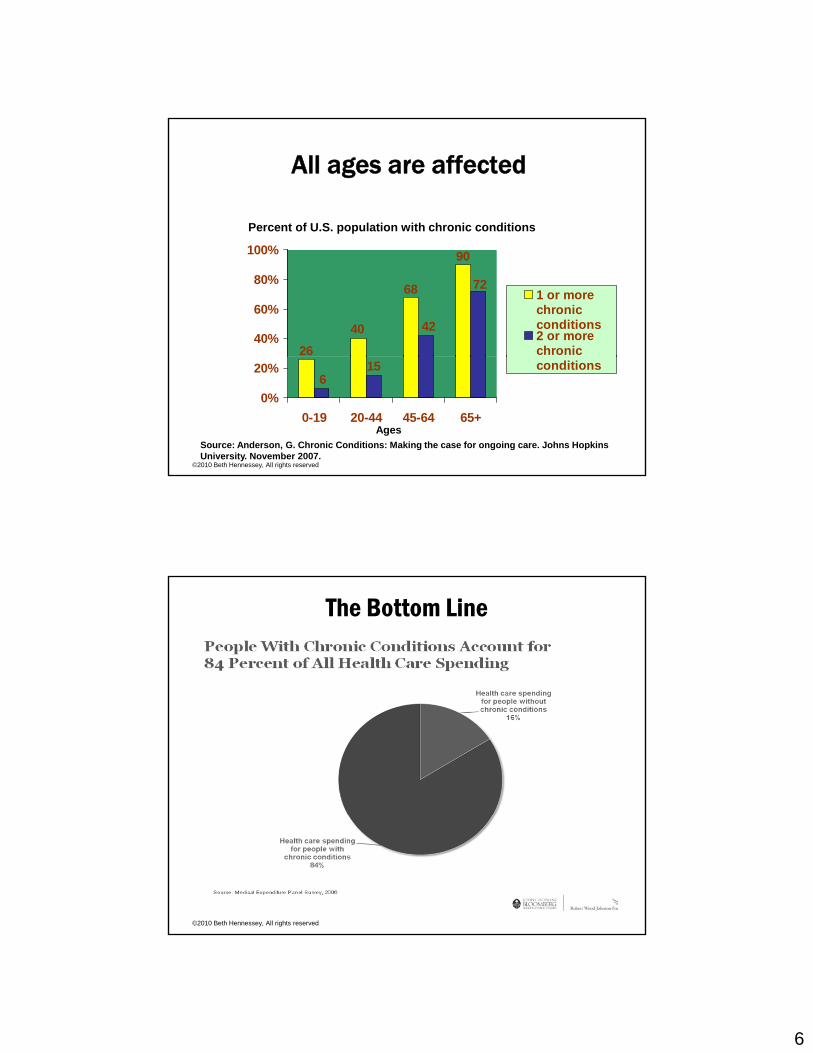
All ages are affected
Percent of U.S. population with chronic conditions
2640
68
90
42
72
40%
60%
80%
100%
1 or morechronicconditions2 or morechronic
©2010 Beth Hennessey, All rights reserved
615
0%
20%
0-19 20-44 45-64 65+
conditions
AgesSource: Anderson, G. Chronic Conditions: Making the case for ongoing care. Johns Hopkins University. November 2007.
The Bottom Line
©2010 Beth Hennessey, All rights reserved

7
So what about coordination?
©2010 Beth Hennessey, All rights reserved
Uncoordinated Care
©2010 Beth Hennessey, All rights reserved
8
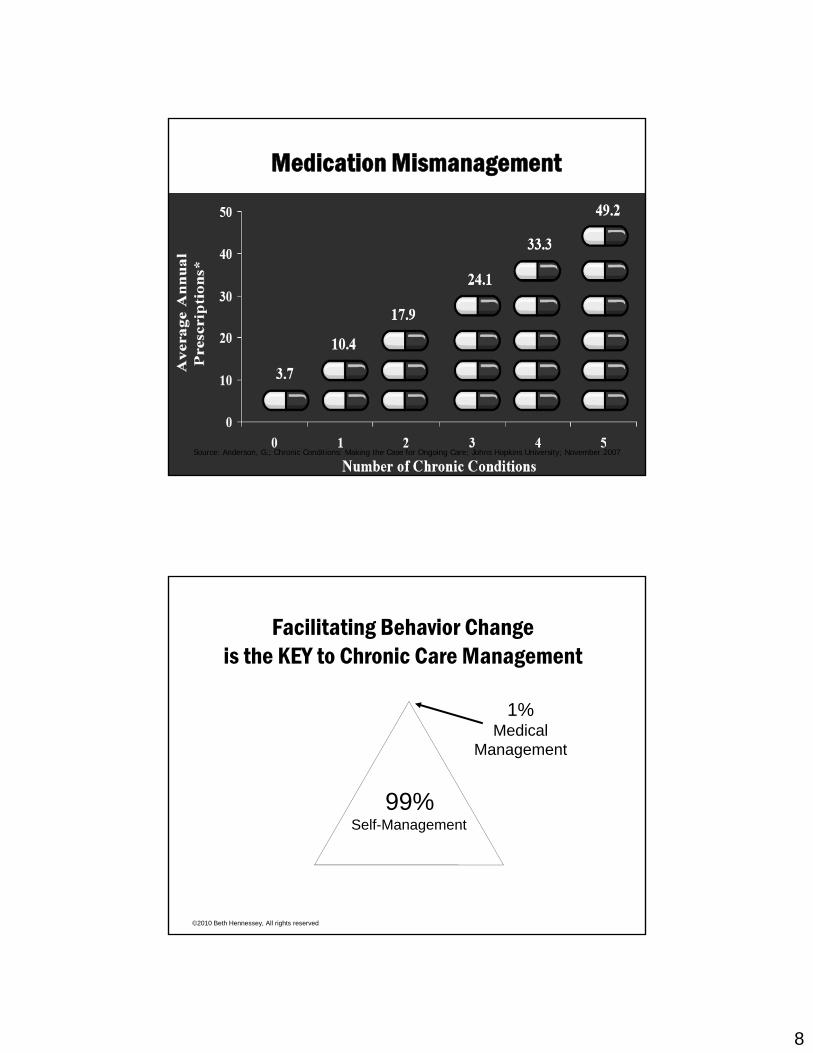
Medication Mismanagement
©2010 Beth Hennessey, All rights reserved
Source: Anderson, G.; Chronic Conditions: Making the Case for Ongoing Care; Johns Hopkins University; November 2007
Facilitating Behavior Changeis the KEY to Chronic Care Management
99%
1% Medical
Management
©2010 Beth Hennessey, All rights reserved
Self-Management
9
“Patients can
Complexity :Behavior Change Required
undo a month’s worth of
expensive and intensive care just
going home
©2010 Beth Hennessey, All rights reserved
g gand going about
their normal routines.”
John Charde, MDVP Strategic Development, Enhanced Care
Initiatives, Inc (April 2006)
Non-adherence: significant for those with chronic conditions
Non-adherence contributes to:– Increase in number and length of acute care visits
(25% of hospitalizations due to medication errors)– Increase in ED visits– Unnecessary changes in treatment
©2010 Beth Hennessey, All rights reserved
– Overuse of scarce and expensive medical resources– Loss of productivity and decreased quality of life
10
• Multiple medications • Multiple physicians
B i t
On the Front Lines
• Barriers to care coordination
• Gaps in transitions of care• Poorly controlled disease• Inconsistent evidence-based
©2010 Beth Hennessey, All rights reserved
care• “Non-compliant” patients• “We will see this pt again”
Bottom Line : Home Care
• Our business success is linked to our success i idi hi h lit i th hin providing high quality care in the home
• Our success in providing high quality care in the home is linked to our success in the management of chronic disease
• Our success in providing high quality CCM in
©2010 Beth Hennessey, All rights reserved
• Our success in providing high quality CCM in the home has resulted from the change in our care delivery prompted by HBCCM

11
Bottom line:Across the Healthcare Continuum
• Healthcare systems are designed for short-term acute rather than long-term chronic care
©2010 Beth Hennessey, All rights reserved
rather than long term chronic care• Chronic care management models must support the
individual in the environment where they face their daily challenges
Source: “Improving Primary Care for Patients with Chronic Illness” Bodenheimer, Wagner, Grumbach, JAMA , October 9, 2002 Vol. 288, No. 14
Our Iceberg is Meltingby John Kotter and Holger Rathgeber
©2010 Beth Hennessey, All rights reserved
The “acute care iceberg” is melting, and from our perspective there is urgency for change .
12
©2010 Beth Hennessey, All rights reserved
Patient Centered + Evidenced Based
Desperately Seeking a Solution
• Literature search: nothing for homecareD t ti j t l l d• Demonstration projects: lessons learned
• Extracted best practices from other fields (adult education, behavior change theory, etc.)
• Dr. Wagner’s Chronic Care Model
©2010 Beth Hennessey, All rights reserved
• Combined experience from across the healthcare continuum
• “We’ll have to build our own model.”
13
We CAN do this!
©2010 Beth Hennessey, All rights reserved© 2010 Beth Hennessey and Paula Suter (ALL RIGHTS RESERVED)
Leaders are visionaries with a poorly developed sense of fear
and no concept of the odds against them.Robert Jarvik
Medicine: Some Viable Solutions
• Traditional DM & M di l H lth Medical Health Support Programs
• Models focusing on care transitions
• Wagner’s Chronic
©2010 Beth Hennessey, All rights reserved
• Wagner s Chronic Care Model
• Guided Care Model
14
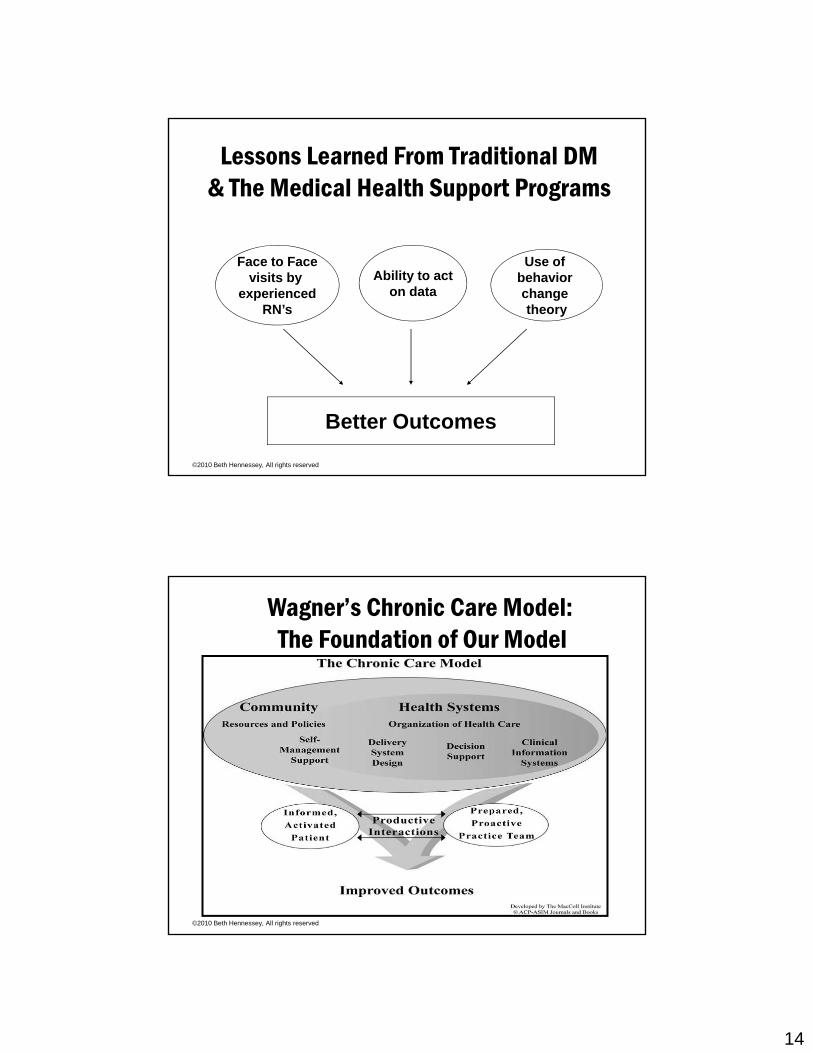
Lessons Learned From Traditional DM & The Medical Health Support Programs
Face to Facevisits by
experiencedRN’s
Use of behavior change theory
Ability to acton data
©2010 Beth Hennessey, All rights reserved
Better Outcomes
Wagner’s Chronic Care Model:The Foundation of Our Model
©2010 Beth Hennessey, All rights reserved
15
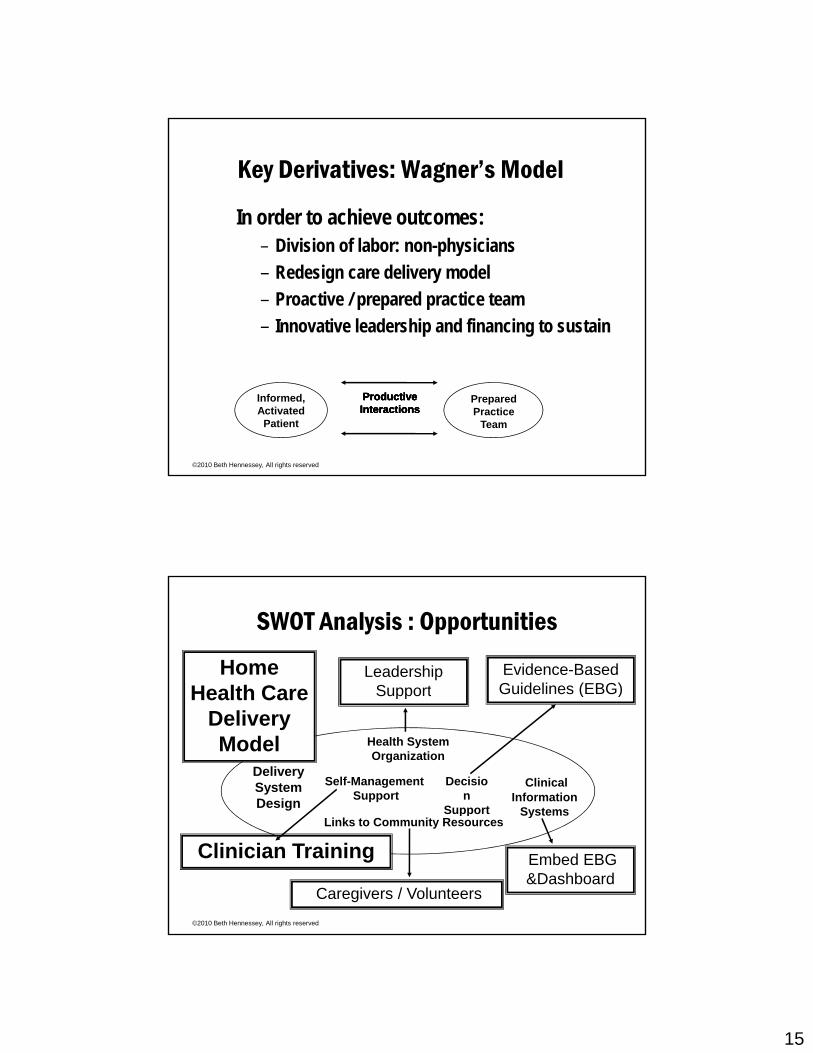
Key Derivatives: Wagner’s Model
In order to achieve outcomes:– Division of labor: non-physicians – Redesign care delivery model– Proactive / prepared practice team– Innovative leadership and financing to sustain
©2010 Beth Hennessey, All rights reserved
Informed,Activated
Patient
ProductiveProductiveInteractionsInteractionsProductiveProductiveInteractionsInteractions
PreparedPractice
Team
Leadership Support
Evidence-Based Guidelines (EBG)
Home Health Care
SWOT Analysis : Opportunities
Delivery SystemDesign
Decision
Support
Clinical Information
Systems
Self-ManagementSupport
Health System Organization
Support ( )Health Care Delivery Model
©2010 Beth Hennessey, All rights reserved
pp SystemsLinks to Community Resources
Embed EBG &Dashboard
Clinician Training
Caregivers / Volunteers

16
Areas for Focused ImprovementSelf – Management Support:
• Emphasizes pt’s central role in managing health• Use effective SMS goal setting (SMART goals), action
planning & problem solvingDecision Support:
• Embed evidence-based guidelines into practice• Share guidelines with patients
©2010 Beth Hennessey, All rights reserved
Delivery System Redesign:• Prepared proactive practice team
• Care coordination across healthcare system• Long term partnership with patient
Behavior Change is HARD
Are you “non ycompliant?”
©2010 Beth Hennessey, All rights reserved

17
The Home Based Chronic Care Model
Building Relationships Changing Behavior
©2010 Beth Hennessey, All rights reserved
Accessing Expertise Maximizing Technology
HBCCM PillarsHigh Touch:•Holistic assessments including barriers to self managementT t b ildi•Trust building
•Patient engagement•Front load visits
Self-management support (SMS):•Pt specific SMART goals
©2010 Beth Hennessey, All rights reserved
•Motivational Interviewing•Facilitation of behavior change
•Build skills & confidence•Provide reinforcement
•Problem Solving
18
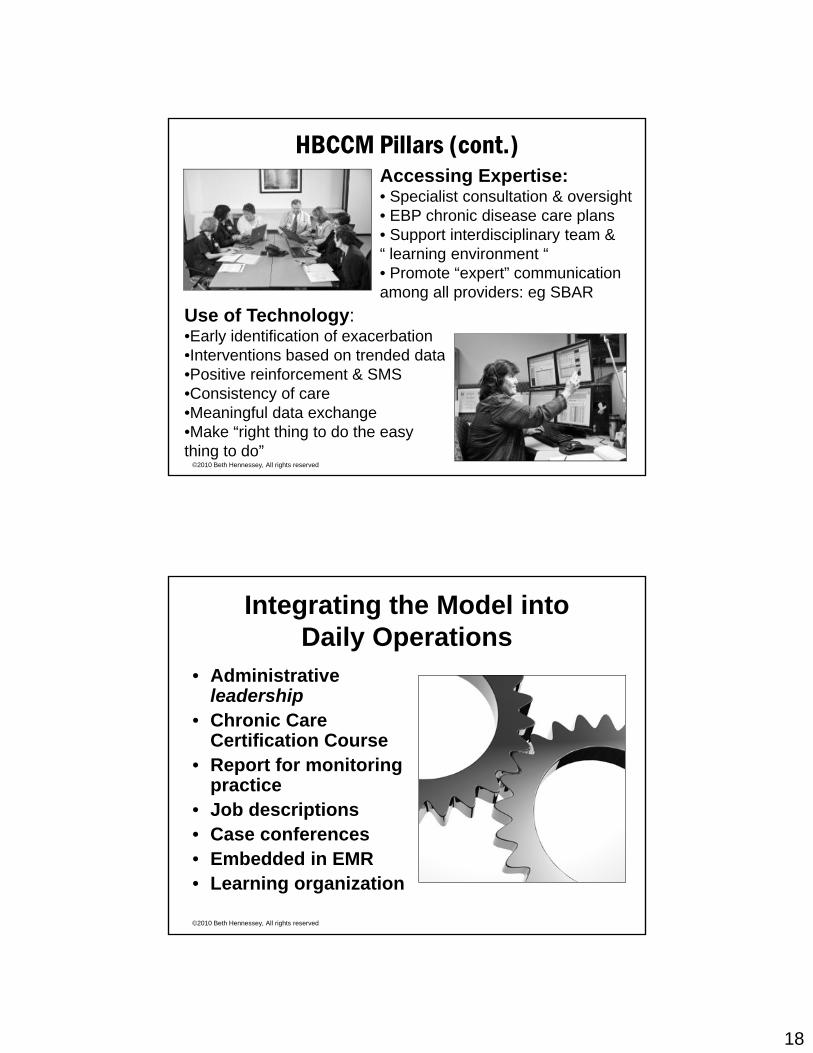
HBCCM Pillars (cont.)Accessing Expertise:• Specialist consultation & oversight• EBP chronic disease care plans • Support interdisciplinary team &Support interdisciplinary team & “ learning environment “• Promote “expert” communication among all providers: eg SBAR
Use of Technology:•Early identification of exacerbation•Interventions based on trended data
©2010 Beth Hennessey, All rights reserved
Interventions based on trended data•Positive reinforcement & SMS•Consistency of care•Meaningful data exchange•Make “right thing to do the easy thing to do”
Integrating the Model into Daily Operations
• Administrative leadershipleadership
• Chronic Care Certification Course
• Report for monitoring practice
• Job descriptions
©2010 Beth Hennessey, All rights reserved
Job descriptions• Case conferences• Embedded in EMR• Learning organization

19
Outcomes Experienced With Model
CLINICAL
Decrease in hospitalizations
FINANCIAL
Volume Increase
Increase in net
SATISFACTION
Pt Satisfaction
©2010 Beth Hennessey, All rights reserved
REGULATORY/ SAFETY
TJC : transitions
Employee engagement
INFORMATION SYSTEMS
Meaningful data exchange
IT : Meaningful Data Exchange
©2010 Beth Hennessey, All rights reserved
SMART Goal: I will meter once a day forthe next week
MD Follow-up Appts: 7/20/10 10am Dr T (PCP)
7/23/10 2pm Dr. G (Endo)
6/1/10- 6/6/10 BMC LR: UTI & Sepsis

20
Customer Satisfaction• Patients• Staff• Staff• Leadership• Physicians• Stakeholders
– Providers
©2010 Beth Hennessey, All rights reserved
Providers– Payers– Policymakers
Value to StakeholdersAcross the Healthcare Continuum
Valued Hospital Partner
Valued PhysicianPartner
Valued SystemPartner
©2010 Beth Hennessey, All rights reserved
•Reduce LOS/ Rehospitalizations/ ED•Reduce avoidable EOL
care expense •Improve Care
Transitions
• Physician Access • Transitions across providers•Physician extenders as a pro-active practice team• PQRI data • Pt-Centered Medical Home
• Payment reform models : bundled
payments to ACOS•Delivery reform: State
& Fed demos : Community Based
Transitions

21
Potentially preventable 30-day readmission rates
Type of Number of potentiallyPercent
readmittedAverage Medicare Total spending on
Initial condition
Type of hospital
admission
Number of potentially preventable 30-day
readmissions(in thousands)
readmitted within 30
days*
Medicare payment for
readmissions
Total spending on potentially preventable
readmissions(in millions) Heart failure Medical 139.2 19.1% $6,490 $903 COPD Medical 85.1 16.5 6,491 552 Pneumonia Medical 86.4 13.3 6,681 577 AMI Medical 30.5 18.7 6,540 199 CABG Surgical 26.6 18.1 8,085 215 PTCA Surgical 68.2 14.7 8,342 569 Other vascular Surgical 30.0 18.6 10,061 302 Total for seven 465 9 $3 318
©2010 Beth Hennessey, All rights reserved
conditions 465.9 $3,318
Total for all DRGs 1,715.5 $12,008 Percent of total 27.2% 27.6%
*30-day readmission rates are calculated based on the set of cases that are potentially eligible for an initial readmission, thus they exclude readmissions and people that died in the hospital from the denominator.
Source: 3M analysis of 2005 Medicare discharge claims data.
Targeted for Improvement Nationwide: Care Transitions
• Quality Improvement Organizations (QIO)Quality Improvement Organizations (QIO)• Special Interest Groups : H2H• Pilots / Demonstrations / Grants• Hospitals : Hospital Compare
©2010 Beth Hennessey, All rights reserved
• TJC: patient safety / culture of safety• Payors : federal / state / and private insurers
22
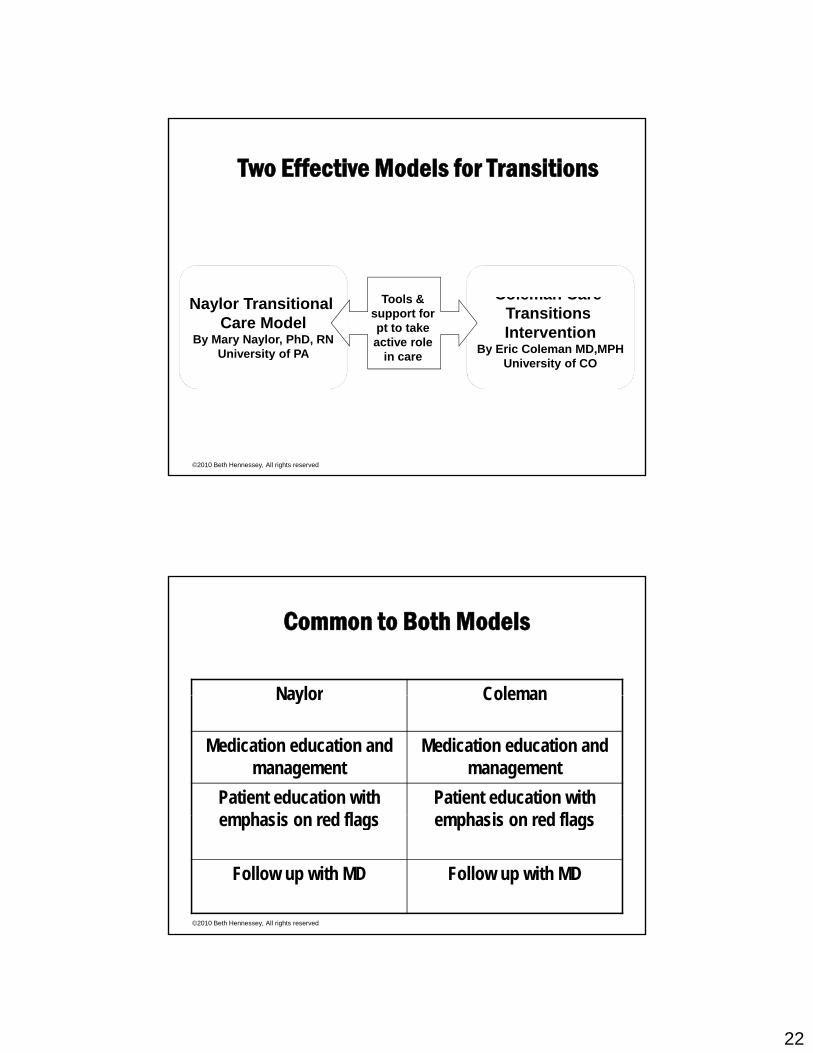
Two Effective Models for Transitions
Coleman Care Transitions Intervention
By Eric Coleman MD,MPH
Naylor Transitional Care Model
By Mary Naylor, PhD, RNUniversity of PA
Tools & support for pt to take active role
in care
©2010 Beth Hennessey, All rights reserved
University of COUniversity of PA in care
Common to Both Models
Naylor ColemanNaylor Coleman
Medication education and management
Medication education and management
Patient education with h i d fl
Patient education with h i d fl
©2010 Beth Hennessey, All rights reserved
emphasis on red flags emphasis on red flags
Follow up with MD Follow up with MD

23
Pt familiar & competent
MedicationManagement have access
di i
Three Question Focus “AND”
Appt scheduled within a week
competent
Early Follow-up AND
to medications
ability to get there
©2010 Beth Hennessey, All rights reserved
Comprehend S&S that require
attention
Symptom Management
whom to contact
Source: American College of Cardiology and the Institute for Healthcare Improvement, Hospital to Home Campaign
Pt familiar & competent
MedicationManagement have access
di i
Three Question Focus + AND + Homecare’s Unique AND
adherence & perseverance
Appt scheduled within a week
competent
Early Follow-up AND
to medications
ability to get there AND
access as needed in between
scheduled appts
perseverance
©2010 Beth Hennessey, All rights reserved
Comprehend S&S that require
attentionSymptom
Managementwhom to contact
Problem solve & behavior change

24
The Call for Innovative Leadership in Healthcare
• Great crises produce great leaders• Three-quarters of innovative
solutions come from “outsiders” • Vision sustains progress in the
midst of difficulties• Tenets of HBCCM offers a model
for transformational change
©2010 Beth Hennessey, All rights reserved
for transformational change
Building Upon A Strong Foundation“ Dombi, with the National Association forNational Association for Home Care and Hospice, said Baptist’s model is a ‘modernization’ of what homehealth agencies have done for more
©2010 Beth Hennessey, All rights reserved
have done for more than a century.”
Home-health program seen as national model
BY CAROLYNE PARK ARKANSAS DEMOCRAT-GAZETTE
25
NEW STRENGTHSHomecare retooled to deliver CCM is a perfect fit as both
• Pt centered goals• Pt engagement
pthe “health coach” AND the “prepared proactive practice team.”
©2010 Beth Hennessey, All rights reserved
• Pt engagement• Self mgt support• Uniform best practices• Health data exchange
Financing to Sustain:Redesigned care delivery supported by new
payment models (PPACA)M f l b d • Move from a volume-based reimbursement system to a value-based reimbursement system
• Achieve greater accountability for both
©2010 Beth Hennessey, All rights reserved
accountability for both efficiency, quality, and slow spending
26
Center for Medicare & Medicaid Innovation (CMI) Planned Opportunities for Chronic Care Mgt
Financing Opportunities within PPACA
Planned Opportunities for Chronic Care Mgt
• Geriatric assessment and care plans for beneficiaries with multiple chronic conditions and 2 ADLs
• Care coordination enabled by health information networks including telehealth
©2010 Beth Hennessey, All rights reserved
• Home health providers offering chronic care management via interdisciplinary teams
• Community-based teams to assist PCP with chronic care management
ACO’s will require delivery reformSupport for Clinical Transformation:
Cli i l t f ti i th li h i f ACO’ • Clinical transformation is the linchpin of ACO’s success, and it does not happen automatically by simply changing payment arrangements and measuring performance.
• Requires effective investment in infrastructure, process and organizational redesign to achieve delivery reform
©2010 Beth Hennessey, All rights reserved
and organizational redesign to achieve delivery reform.• Examples: Chronic disease management & care
transitions“A National Strategy To Put Accountable Care Into Practice” McClellan, A., Lewis, J., Roski, J, & Fisher, E, Health affairs, May 2010, 29:5

27
Private Duty’s Unique Role inMeaningful Healthcare Reform
• Fill the gaps of community based care needed g p y• Cost effective care• Located where patients want their care• “Army at the ready” for:
– Transitions of care– Patient Centered
©2010 Beth Hennessey, All rights reserved
– Patient Centered Medical Home
– Long term CCM– Value based partnerships– ACOs
Value to StakeholdersAcross the Healthcare Continuum
Valued Hospital Partner
Valued PhysicianPartner
Valued SystemPartner
©2010 Beth Hennessey, All rights reserved
•Reduce LOS/ Rehospitalizations/ ED•Reduce avoidable EOL
care expense •Improve Care Transitions
• Physician Access • Provider transitions• Physician extenders as a pro-active practice team• PQRI data • Pt-Centered Medical Home
• Payment reform models : bundled
payments to ACOS•Delivery reform: demos on State &
Federal Level

28
A Golden Opportunity Knocks
• To spark meaningful healthcare reform
• Make pts’ needs & providers’ expertise the drivers of reform
• Lead our organizations in a new way of delivering careT d t t fi ll
©2010 Beth Hennessey, All rights reserved
• To demonstrate a fiscally sensible & sustainable solution for CCM , transitions of care, PCMH & ACOs
Change has a considerable psychological impact on the human mind. To the fearful it is threatening because it means that things may get
worse.To the hopeful it is encouraging because things may get better.
To the confident it is inspiring because the challenge exists to make things better.
King Whitney, Jr.
©2010 Beth Hennessey, All rights reserved© 2010 Beth Hennessey and Paula Suter (ALL RIGHTS RESERVED)

29
Answering the Call
• If we can envision...A patient-centered h lth t th t i ibl ff d bl healthcare system that is accessible, affordable, sustainable and provides the best care in the world, and…
• If we can embrace...A blueprint for genuine reform that has immediate real world
©2010 Beth Hennessey, All rights reserved
reform that has immediate, real-world applicability with specific action steps for today, as well as clearly defined long-term objectives for the future, and…
Answering the Call• If we can embark…On a journey with colleagues
in the pursuit of excellence for those we are pprivileged to serve, and…
• If we can propose...That homecare providers are in a unique position to reform healthcare delivery by starting with integrated chronic care management
©2010 Beth Hennessey, All rights reserved
management…When we succeed, we will have delivered
meaningful healthcare reform and restored hope for those we are committed to serve.

30
The Journey BeckonsThe Journey Beckons
©2010 Beth Hennessey, All rights reserved
Related Documents











