Service Agreements Mike Davies, MD Mark Murray and Associates

Service Agreements Mike Davies, MD Mark Murray and Associates Mike Davies, MD Mark Murray and Associates.
Dec 26, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Service AgreementsService Agreements
Mike Davies, MDMark Murray and Associates
Mike Davies, MDMark Murray and Associates

Other IndustriesOther Industries
•“Live and die” on the product
•Define the timelines and handoffs
•Define expectations of each party
•Constantly measure conformity to expectations
•Refine and improve handoffs
•“Live and die” on the product
•Define the timelines and handoffs
•Define expectations of each party
•Constantly measure conformity to expectations
•Refine and improve handoffs

Big System FlowBig System Flow
TestTest
SCSC SurgerySurgery
External DemandExternal Demand
PCPC
TestTest

“We Are All Related”“We Are All Related”

Definition of a Service Agreement:Definition of a Service Agreement:
Understanding or agreement between any 2 parties, one of which sends work
to another, defining work flow rules.
Understanding or agreement between any 2 parties, one of which sends work
to another, defining work flow rules.

AgreementAgreement
•Sender – sends the right work packaged the right way
•Receiver – is accessible for performing the right work right away
•Sender – sends the right work packaged the right way
•Receiver – is accessible for performing the right work right away

Why are Service Agreements Important?
Why are Service Agreements Important?
•Define relationships between primary and specialty care
•Reduce demand for specialists
• Improve referral process
•Decrease delay in care
•Define relationships between primary and specialty care
•Reduce demand for specialists
• Improve referral process
•Decrease delay in care

Who are the stakeholders in the referral relationship?
Who are the stakeholders in the referral relationship?
PatientsPatients
•Reassurance
•Expectation for the process
•Knowledge of the process
•Certainty
•Speed
•Quality of the care and the experience
•Appropriate referral
•Reassurance
•Expectation for the process
•Knowledge of the process
•Certainty
•Speed
•Quality of the care and the experience
•Appropriate referral
Primary CarePrimary Care
•Access to SC
•Speed
•Know SC expectations
•Simple process
•Certainty of appointment
•Questions answered
•Let my people go
•Access to SC
•Speed
•Know SC expectations
•Simple process
•Certainty of appointment
•Questions answered
•Let my people go

Specialty CareSpecialty Care
•Knowledge of which doctor is referring
•Right patients sent with right information
•Patient expectations
•PC expectations
• (When do I) let the people go?
•Knowledge of which doctor is referring
•Right patients sent with right information
•Patient expectations
•PC expectations
• (When do I) let the people go?

Common InterestsCommon Interests
•PC and PatientsSpeed
Certainty of appointment
Answers
•SC and PCExpectations of each other
•PC and PatientsSpeed
Certainty of appointment
Answers
•SC and PCExpectations of each other

Four Components to Service Agreement
Four Components to Service Agreement
1.Define and discuss the work – Who? What? How much?
2.Sender – sends right work packaged the right way
3.Receiver – does right work right “right away”
4.Referee – monitors agreement
1.Define and discuss the work – Who? What? How much?
2.Sender – sends right work packaged the right way
3.Receiver – does right work right “right away”
4.Referee – monitors agreement

1. Define and Discuss the Work
1. Define and Discuss the Work
What is the work?
Who is sending it?
How much work exists?
What is the work?
Who is sending it?
How much work exists?

Sample of Consult Rate Q2 ‘02Sample of Consult Rate Q2 ‘02
Consults 2ndQuarter 02Provider
Consults 2ndQuarter 02Provider
Neu
rolo
gyN
euro
logy
Ort
hope
dics
Ort
hope
dics
Psyc
hiat
ryPs
ychi
atry
Uro
logy
Uro
logy
Car
diol
ogy
Car
diol
ogy
Der
mat
olog
yD
erm
atol
ogy
ENT
ENT
Neu
rolo
gyN
euro
logy
11 00 1212 1818 99 11 11 22 0022 00 00 22 11 00 00 00 0033 00 11 00 00 00 00 00 0044 00 22 11 11 00 00 00 0055 66 1111 1414 77 22 00 44 6666 00 00 00 00 00 00 00 0077 11 22 1515 66 00 66 22 1188 22 66 44 1010 00 00 22 2299 00 11 00 00 00 00 00 00
1010 1212 88 1515 66 11 66 33 12121111 44 88 77 99 22 44 44 441212 33 44 3030 77 11 66 22 331313 00 11 22 00 00 22 00 001414 55 1515 1111 1010 11 55 33 551515 44 22 1717 99 00 1313 33 44
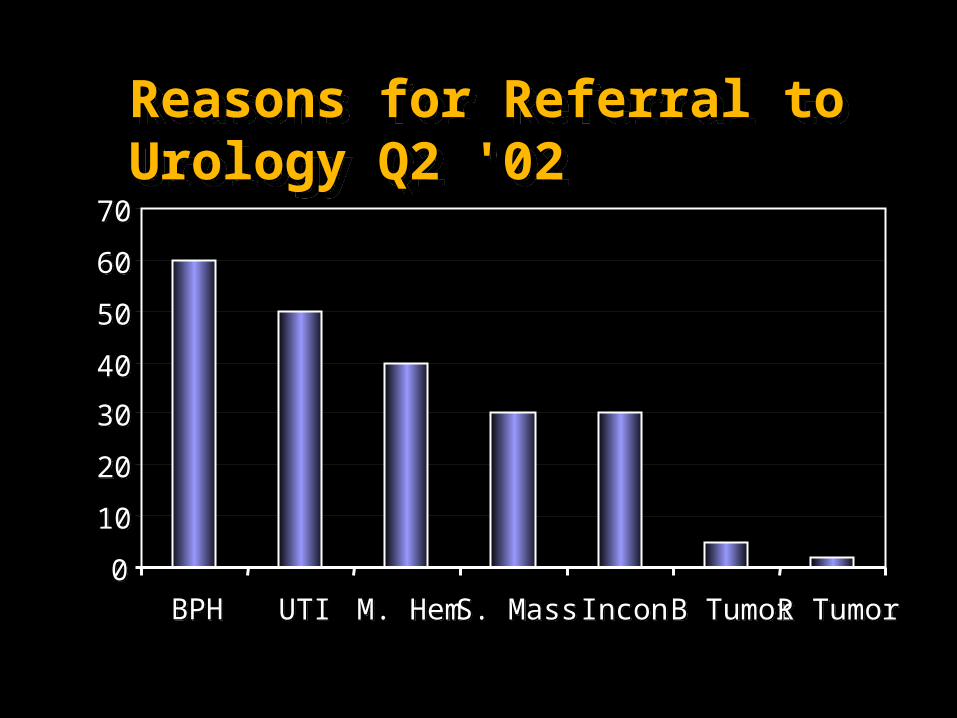
Reasons for Referral to Urology Q2 '02Reasons for Referral to Urology Q2 '02
00
1010
2020
3030
4040
5050
6060
7070
BPHBPH UTIUTI M. HemM. Hem S. MassS. Mass InconIncon B TumorB Tumor R TumorR Tumor
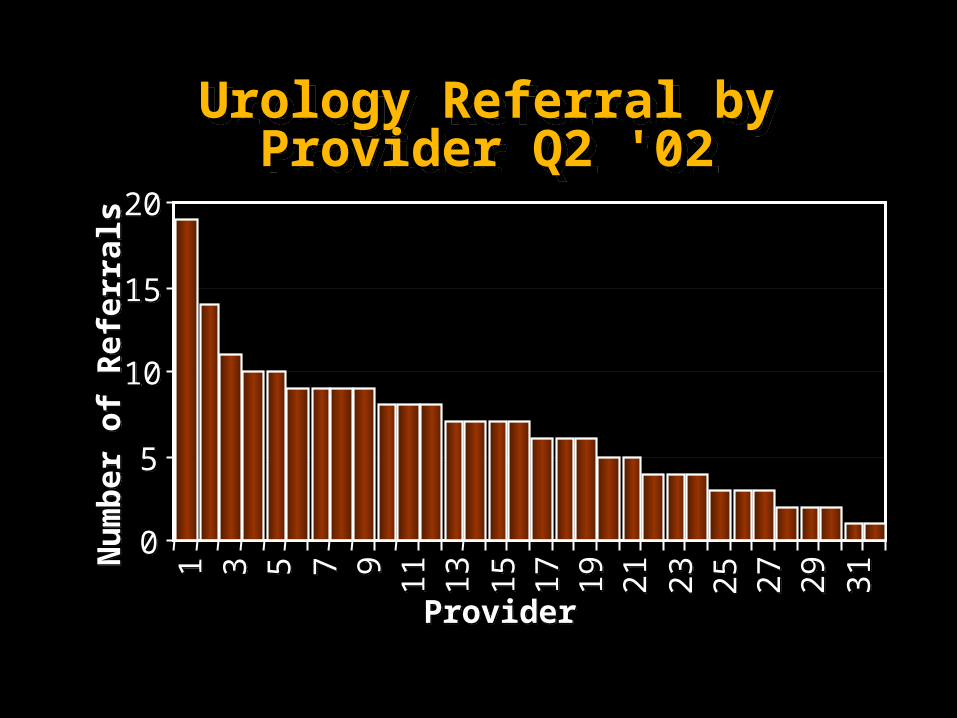
Urology Referral by Provider Q2 '02
Urology Referral by Provider Q2 '02
00
55
1010
1515
202011 33 55 77 99 1111 1313 1515 1717 1919 2121 2323 2525 2727 2929 3131
ProviderProvider
Num
ber o
f Ref
erra
lsN
umbe
r of R
efer
rals
Areas to Target for SAAreas to Target for SA
•High volume diagnosis•High volume diagnosis
Areas to Target for Focused EducationAreas to Target for Focused Education
•High volume referring providers

Face-to-Face Communication Needed at This Point!Face-to-Face Communication Needed at This Point!
•Organize all service members or key representatives to a meeting – facilitated if necessary
•Present the data
•Discuss the data, practices, history, problems, potential solutions and recommendations
•Organize all service members or key representatives to a meeting – facilitated if necessary
•Present the data
•Discuss the data, practices, history, problems, potential solutions and recommendations
Halt!Halt!

Draft Improvement IdeasDraft Improvement Ideas
•Draft list of appropriate reasons for referral
•Draft list of work up needed before the specialty appointment
•Circulate the proposal to everyone affected and consider all comments
•Draft list of appropriate reasons for referral
•Draft list of work up needed before the specialty appointment
•Circulate the proposal to everyone affected and consider all comments

2. Sender Sends Right Work (Packaged) the Right Way
2. Sender Sends Right Work (Packaged) the Right Way

What is the right work?System-wide BPH Referral Guidelines – Refer When:
What is the right work?System-wide BPH Referral Guidelines – Refer When:
1. Medical failure – symptoms not controlled, residual urine not reduced.
2. Adverse reaction to recommended medication
3. Possible obstructive uropathy – elevated BUN/Creat – not improved with medication
4. Patient desire for definitive surgical treatment.
1. Medical failure – symptoms not controlled, residual urine not reduced.
2. Adverse reaction to recommended medication
3. Possible obstructive uropathy – elevated BUN/Creat – not improved with medication
4. Patient desire for definitive surgical treatment.

a. Physician Factorsb. Referral Processc. Patient Experience
a. Physician Factorsb. Referral Processc. Patient Experience
2. Sender Sends Right Work (Packaged) the Right Way
2. Sender Sends Right Work (Packaged) the Right Way

Physician FactorsPhysician Factors
Packaging the referralPackaging the referral

Physician Factors: Package Right Way
Physician Factors: Package Right Way
•Refer the “right” problem
•“Sell” the consult to the patient (closing the visit)
•Clarify expectations
•Provide the right information to the specialist
•Refer the “right” problem
•“Sell” the consult to the patient (closing the visit)
•Clarify expectations
•Provide the right information to the specialist

Microscopic Hematuria – Refer With:Microscopic Hematuria – Refer With:
1.Verify presence of three UA’s with at least six RCBs/HPF
2.Negative C & S of urine
3. IVP or Renal Ultrasound (if renal insufficiency or contrast allergy) prior to consult.
1.Verify presence of three UA’s with at least six RCBs/HPF
2.Negative C & S of urine
3. IVP or Renal Ultrasound (if renal insufficiency or contrast allergy) prior to consult.

Structured ConsultStructured Consult
Tool to assist packaging the right way…
Tool to assist packaging the right way…


Referral ProcessConsult Flow
Patient Flow
Referral ProcessConsult Flow
Patient Flow

ColonoscopyOrdered
ColonoscopyOrdered
Chart reviewed by RNto find indications/
contraindications andlast exam
Chart reviewed by RNto find indications/
contraindications andlast exam
Chart Reviewedby Surgeon
Chart Reviewedby Surgeon
MeetsCriteriaMeets
Criteria
Call to Providerto Clarify
Call to Providerto Clarify
RN Calls patient toschedule and educate
Rn sends prep
RN Calls patient toschedule and educate
Rn sends prep
YESYESNONO
.15 to 2 hours X 25/wk.15 to 2 hours X 25/wk= 6 to 50 hours= 6 to 50 hours
5 to 205 to 20minmin X 25/wk X 25/wk= 2 to 4 hours per week= 2 to 4 hours per week

ProviderOrders
Colonoscopy
ProviderOrders
Colonoscopy
Provider fills outstructured consultProvider fills out
structured consult
Surgery schedules test,educates, sends prep
Surgery schedules test,educates, sends prep
5 min X 2/week5 min X 2/week
= 10 minutes= 10 minutes

Ideal Patient ExperienceIdeal Patient Experience
• Has clear understanding about and buy-in for referral from PCP
• PC Clerk reinforces expectations for referral negotiates ideal time and place for referral within 5 daysschedules specialty appointment at the time of check out from PCP
• Patient receives reminder material or call before appointment
• Has clear understanding about and buy-in for referral from PCP
• PC Clerk reinforces expectations for referral negotiates ideal time and place for referral within 5 daysschedules specialty appointment at the time of check out from PCP
• Patient receives reminder material or call before appointment

Ideal Patient Experience (cont)Ideal Patient Experience (cont)
• Specialty clerk warmly welcomes patientmentions who referred the patientReinforces reason for and expectations from referral
• Specialty provideris familiar with key historical factsis able to provide needed care in 1 or 2 visitsfacilitates smooth hand back to PCP
• Specialty clerk warmly welcomes patientmentions who referred the patientReinforces reason for and expectations from referral
• Specialty provideris familiar with key historical factsis able to provide needed care in 1 or 2 visitsfacilitates smooth hand back to PCP

3. Receiver: Is accessible for doing the right work right away
3. Receiver: Is accessible for doing the right work right away
Ways for Specialists to be AccessibleWays for Specialists to be Accessible
•Measure access parameters (wait, supply, demand, no-show, etc)
•Work down backlog
•Balance supply and demand
•Telephone
•“Question only” consults
•Measure access parameters (wait, supply, demand, no-show, etc)
•Work down backlog
•Balance supply and demand
•Telephone
•“Question only” consults

Wait Time for UrologyWait Time for Urology
00
1010
2020
3030
4040
5050
6060
1st Qtr1st Qtr 2nd Qtr2nd Qtr 3rd Qtr3rd Qtr 4th Qtr4th Qtr
Days to3ed nextDays to3ed next

Now Make and Agreement….Now Make and Agreement….
• “Primary Care will send the right patients appropriately worked up……in return, the specialists will be available to primary care anytime they are not in the OR and see patients quickly”
• “Primary Care will send the right patients appropriately worked up……in return, the specialists will be available to primary care anytime they are not in the OR and see patients quickly”

4. Referee – monitors for fair play
4. Referee – monitors for fair play
Audit: How we know it’s workingAudit: How we know it’s working

Develop measures (audit) for:Develop measures (audit) for:
•Wait time
•Audit of work (who is referring what?)
•Audit of important parts of process
•Wait time
•Audit of work (who is referring what?)
•Audit of important parts of process

Service Agreement Audit Quarter 4 '04 GIService Agreement Audit Quarter 4 '04 GI
GI Question #1: Receiver saw patient in agreed timeframeGI Question #1: Receiver saw patient in agreed timeframeGI Question #2: Sender referred the right casesGI Question #2: Sender referred the right casesGI Question #3: Sender provided the right informationGI Question #3: Sender provided the right information
Grp. 1
Grp. 1
Grp. 2
Grp. 2
Grp. 3
Grp. 3
Grp. 4
Grp. 4
Grp. 5
Grp. 5
Grp. 6
Grp. 6
Grp. 7
Grp. 7
Grp. 8
Grp. 8
System
Total
System
Total
120%120%
0%0%20%20%40%40%60%60%80%80%
100%100%
% C
om
pli
ance
% C
om
pli
ance

How to do it…How to do it…

Ideal Service Agreement Implementation Steps
Ideal Service Agreement Implementation Steps
1. Volume, reason, and source of existing referrals are measured and shared
2. Consultation scheduling process is flow-mapped
3. Face-to-face discussion between PC and Specialists occurs
Discuss current data
Discuss referral process
Small group tasked to work out agreement
1. Volume, reason, and source of existing referrals are measured and shared
2. Consultation scheduling process is flow-mapped
3. Face-to-face discussion between PC and Specialists occurs
Discuss current data
Discuss referral process
Small group tasked to work out agreement

Ideal Service Agreement Implementation Steps (Cont)Ideal Service Agreement
Implementation Steps (Cont)
4.One or 2 specific topics for future SA’s are chosen.
5.Simple SA is drafted
6.Consensus is reached among PC and SC providers for SA content, scheduling process, and audit criteria
7.Agreement is formally adopted by medical executive committee
4.One or 2 specific topics for future SA’s are chosen.
5.Simple SA is drafted
6.Consensus is reached among PC and SC providers for SA content, scheduling process, and audit criteria
7.Agreement is formally adopted by medical executive committee
8. SA implementation tools (structured consults, patient education, etc.) are implemented
9. Audit measures are tasked to be done periodically
10.Results of audit regularly discussed in face-to-face meeting of PC and Specialty providers
Ideas for improvement considered and adopted as needed
8. SA implementation tools (structured consults, patient education, etc.) are implemented
9. Audit measures are tasked to be done periodically
10.Results of audit regularly discussed in face-to-face meeting of PC and Specialty providers
Ideas for improvement considered and adopted as needed
Ideal Service Agreement Implementation Steps (Cont)Ideal Service Agreement
Implementation Steps (Cont)

Specialty ACA FacultySpecialty ACA Faculty
receive for preliminaryreceive for preliminary
reviewreview
Amb Care SLMAmb Care SLM
assign team toassign team to
review servicereview service
agreementsagreements
PC Team reviewsPC Team reviews
TAT 4 weeksTAT 4 weeks
ConsensusConsensus
requiredrequired
1. Accept w/o revision1. Accept w/o revision
2. Accept w/ minor revision2. Accept w/ minor revision
3. Not accepted3. Not accepted
Accepted?Accepted?
Signed by PC SLMSigned by PC SLM
& Specialty Chief& Specialty Chief
and distributedand distributed
Returned toReturned to
Specialty sectionSpecialty section
w/ recommendedw/ recommended
changes &changes &
rationalerationale
Annual review bySpecialty and PC
for concurrence and/oramendment
Annual review bySpecialty and PC
for concurrence and/oramendment
Make minorMake minor
revisions ifrevisions if
needed, getneeded, get
concurrencesconcurrences
YesYes
NoNo

Approval ProcessApproval Process
• Agreement by subspecialists and Primary Care
• Signatures by Specialty Care Chief and Primary Care Chief
• Approval by Executive Committee of the Medical Staff
• Agreement by subspecialists and Primary Care
• Signatures by Specialty Care Chief and Primary Care Chief
• Approval by Executive Committee of the Medical Staff

Individual Focused EducationIndividual Focused Education
•Find the most frequent referrers to the service
•One-on-one, or facilitated discussion about reasons for referral
•Measure before and after discussion
•Find the most frequent referrers to the service
•One-on-one, or facilitated discussion about reasons for referral
•Measure before and after discussion

Service AgreementService Agreement
Effect of Strategies on Demand Reduction in Specialty Care
Effect of Strategies on Demand Reduction in Specialty Care
Focused Education
0022446688
101012121414161618182020
Each Bar Represents 1 MDEach Bar Represents 1 MD
Mean 8.6Mean 8.6
SA Example SA Example
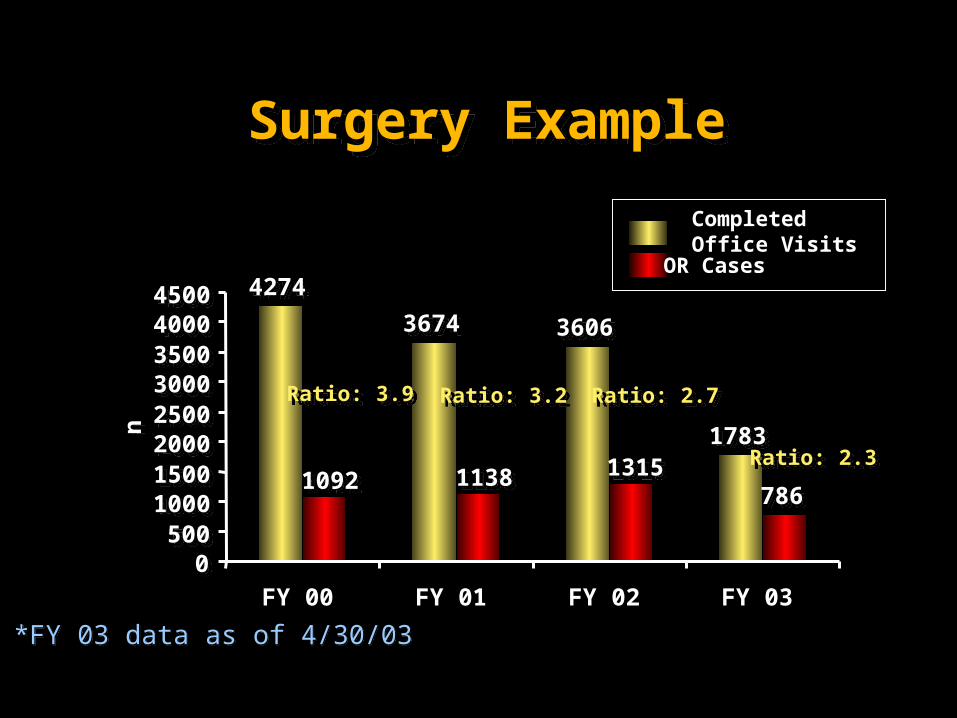
Surgery ExampleSurgery Example
*FY 03 data as of 4/30/03*FY 03 data as of 4/30/03
42744274
36743674 36063606
17831783
78678610921092 11381138 13151315
00500500
1000100015001500200020002500250030003000350035004000400045004500
FY 00 FY 01 FY 02 FY 03
nn
Completed Office Visits
OR Cases
Ratio: 3.9Ratio: 3.9 Ratio: 3.2Ratio: 3.2 Ratio: 2.7Ratio: 2.7
Ratio: 2.3Ratio: 2.3

Major Cases, FY 94-02Major Cases, FY 94-02
00
200200
400400
600600
800800
10001000
12001200
Maj
or C
ases
Maj
or C
ases
19941994 19951995 19961996 19971997 19981998 19991999 20002000 20012001 20022002 FYFY
Bivariate Line Chart, Major Cases vs Fiscal YearBivariate Line Chart, Major Cases vs Fiscal YearGrouping Variable: ServiceGrouping Variable: ServiceData Sources: Surgical Service Summary Report; Special Procedures LogbookData Sources: Surgical Service Summary Report; Special Procedures Logbook
764846 835
927869
916 953 958
1100
UrologyOrthopedicsOphthalmologyNeurosurgeryENT5C Services

AGREEMENT BETWEEN PRIMARY CARE AND GASTROENTEROLOGY
• To facilitate patient care by reducing waiting time to obtain a screening colonoscopy.
• To facilitate patient care by increasing the percentage of patients who are appropriately screened for colorectal carcinoma.
1. To facilitate patient care by decreasing the interval between a positive test for blood in the feces and initiation of therapy for colorectal carcinoma.
AGREEMENT BETWEEN PRIMARY CARE AND GASTROENTEROLOGY
• To facilitate patient care by reducing waiting time to obtain a screening colonoscopy.
• To facilitate patient care by increasing the percentage of patients who are appropriately screened for colorectal carcinoma.
1. To facilitate patient care by decreasing the interval between a positive test for blood in the feces and initiation of therapy for colorectal carcinoma.
Oklahoma Example AgreementOklahoma Example Agreement
1. Issue hemoccult cards to each non-screened patient over 50 who is not terminal and agrees to screening.
2. Evaluate those patients who have positive result. This colonoscopy, to fully inform patient about risks and benefits of a colonoscopy, and to set up appointment including ordering preparatory medications.
3. Adjust anticoagulant therapy as needed for those patients on warfarin.
4. Enter pre-colonoscopy note in the record.5. Call patients prior to scheduled exam to reduce no-
show rates.
1. Issue hemoccult cards to each non-screened patient over 50 who is not terminal and agrees to screening.
2. Evaluate those patients who have positive result. This colonoscopy, to fully inform patient about risks and benefits of a colonoscopy, and to set up appointment including ordering preparatory medications.
3. Adjust anticoagulant therapy as needed for those patients on warfarin.
4. Enter pre-colonoscopy note in the record.5. Call patients prior to scheduled exam to reduce no-
show rates.
Primary Care WillPrimary Care Will

1. Maintain enough open capacity to accommodate scheduling within 2- 4 weeks.
2. Enter reports including CPT codes into the record.
3. Recommend appropriate follow-up for patients after colonoscopy.
4. Open appointment capability so that Primary Care may schedule directly following guidelines.
5. Educate clinicians regarding appropriate screening intervals and techniques.
1. Maintain enough open capacity to accommodate scheduling within 2- 4 weeks.
2. Enter reports including CPT codes into the record.
3. Recommend appropriate follow-up for patients after colonoscopy.
4. Open appointment capability so that Primary Care may schedule directly following guidelines.
5. Educate clinicians regarding appropriate screening intervals and techniques.
Gastroenterology WillGastroenterology Will

Clarify the Pathways:Back Pain Example
Clarify the Pathways:Back Pain Example
•Services that treat back pain
Physical Therapy
Neurology
Neurosurgery
Physiatry
Orthopedics
•Services that treat back pain
Physical Therapy
Neurology
Neurosurgery
Physiatry
Orthopedics

SummarySummary
•Define and discuss the work: Who is sending it and what it is
•Sender sends the right work the right way
•Receiver does today’s work today – and is accessible to the sender
•Referee audits agreement
•Define and discuss the work: Who is sending it and what it is
•Sender sends the right work the right way
•Receiver does today’s work today – and is accessible to the sender
•Referee audits agreement

National Database “Mining” (Audit)
National Database “Mining” (Audit)
Bill BarrBill Barr


Eye Care carries a large proportion of Established Patients in its Case Load.
Eye Care carries a large proportion of Established Patients in its Case Load.
Related Documents











