Sequestration of MBNL1 in tissues of patients with myotonic dystrophy type 2 Z. Luka ´s ˇ a,⇑,1 , M. Falk b,⇑,1 , J. Feit a , O. Souc ˇek a , I. Falkova ´ a,b , L. S ˇ tefanc ˇı ´kova ´ b , E. Janous ˇova ´ c , L. Fajkusova ´ d , J. Zaora ´lkova ´ a , R. Hraba ´lkova ´ a a Institute of Pathology, Brno Faculty Hospital, Brno, Czech Republic b Institute of Biophysics, Academy of Sciences of the Czech Republic, Brno, Czech Republic c Institute of Biostatistics and Analyses, Faculty of Medicine and Faculty of Science, Masaryk University, Brno, Czech Republic d Centre of Molecular Biology and Gene Therapy, Brno Faculty Hospital, Brno, Czech Republic Received 9 January 2012; received in revised form 2 March 2012; accepted 6 March 2012 Abstract The pathogenesis of myotonic dystrophy type 2 includes the sequestration of MBNL proteins by expanded CCUG transcripts, which leads to an abnormal splicing of their target pre-mRNAs. We have found CCUG exp RNA transcripts of the ZNF9 gene associated with the formation of ribonuclear foci in human skeletal muscle and some non-muscle tissues present in muscle biopsies and skin excisions from myotonic dystrophy type 2 patients. Using RNA-FISH and immunofluorescence-FISH methods in combination with a high-res- olution confocal microscopy, we demonstrate a different frequency of nuclei containing the CCUG exp foci, a different expression pattern of MBNL1 protein and a different sequestration of MBNL1 by CCUG exp repeats in skeletal muscle, vascular smooth muscle and endo- thelia, Schwann cells, adipocytes, and ectodermal derivatives. The level of CCUG exp transcription in epidermal and hair sheath cells is lower compared with that in other tissues examined. We suppose that non-muscle tissues of myotonic dystrophy type 2 patients might be affected by a similar molecular mechanism as the skeletal muscle, as suggested by our observation of an aberrant insulin receptor splicing in myotonic dystrophy type 2 adipocytes. Ó 2012 Elsevier B.V. All rights reserved. Keywords: Myotonic dystrophy; Transcription of ZNF9; CCUG repeat expansion; Sequestration of MBNL1 protein; Ribonuclear foci; Insulin receptor alternative splicing 1. Introduction Both myotonic dystrophy type 1 (DM1) and myotonic dystrophy type 2 (DM2) share a similar pathogenetic pattern beginning with an expansion of CTG and CCTG nucleotide repeats due to mutation in the genes encoding dystrophia myotonica protein kinase (DMPK) and zinc- finger protein 9 (ZNF9), respectively. Taneja et al. [1] were the first to describe and illustrate intranuclear foci contain- ing CTG repeat expansions in skeletal muscle and fibro- blasts of DM1 patients; the most of transcripts with expanded repeats remain retained in the nuclei of cells. Consequently, DMPK protein levels are reduced [2]. Miller et al. [3] demonstrated recruitment of RNA-binding proteins to the CUG exp foci in DM1 patients. Liquori et al. [4] showed that the second form of DM2 is also caused by an expansion, concretely of a CCTG repeat in the first intron of the ZNF9 gene. Consequently, co-localization 0960-8966/$ - see front matter Ó 2012 Elsevier B.V. All rights reserved. http://dx.doi.org/10.1016/j.nmd.2012.03.004 ⇑ Corresponding authors. Addresses: Department of Pathology, Brno Faculty Hospital, Jihlavska ´ 20, CZ-625 00 Brno, Czech Republic. Tel.: +420 532233837 (Z. Luka ´s ˇ); Laboratory of Chromatin Function, Damage and Repair, Dept. of Molecular Cytology and Cytometry, Institute of Biophysics, Academy of Sciences of CR, Kralovopolska 135, 61265 Brno, Czech Republic. Tel.: +420 541517165; mobile: +420 728 084060 (M. Falk). E-mail addresses: [email protected], [email protected] (Z. Luka ´s ˇ), [email protected] (M. Falk). 1 The first and second author contributed equally. www.elsevier.com/locate/nmd Available online at www.sciencedirect.com Neuromuscular Disorders xxx (2012) xxx–xxx ARTICLE IN PRESS Please cite this article in press as: Luka ´s ˇ Z et al., Sequestration of MBNL1 in tissues of patients with myotonic dystrophy type 2, Neuromuscul Disord (2012), http://dx.doi.org/10.1016/j.nmd.2012.03.004

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Available online at www.sciencedirect.com
ARTICLE IN PRESS
www.elsevier.com/locate/nmd
Neuromuscular Disorders xxx (2012) xxx–xxx
Sequestration of MBNL1 in tissues of patients with myotonicdystrophy type 2
Z. Lukas a,⇑,1, M. Falk b,⇑,1, J. Feit a, O. Soucek a, I. Falkova a,b, L. Stefancıkova b,E. Janousova c, L. Fajkusova d, J. Zaoralkova a, R. Hrabalkova a
a Institute of Pathology, Brno Faculty Hospital, Brno, Czech Republicb Institute of Biophysics, Academy of Sciences of the Czech Republic, Brno, Czech Republic
c Institute of Biostatistics and Analyses, Faculty of Medicine and Faculty of Science, Masaryk University, Brno, Czech Republicd Centre of Molecular Biology and Gene Therapy, Brno Faculty Hospital, Brno, Czech Republic
Received 9 January 2012; received in revised form 2 March 2012; accepted 6 March 2012
Abstract
The pathogenesis of myotonic dystrophy type 2 includes the sequestration of MBNL proteins by expanded CCUG transcripts, whichleads to an abnormal splicing of their target pre-mRNAs. We have found CCUGexp RNA transcripts of the ZNF9 gene associated withthe formation of ribonuclear foci in human skeletal muscle and some non-muscle tissues present in muscle biopsies and skin excisionsfrom myotonic dystrophy type 2 patients. Using RNA-FISH and immunofluorescence-FISH methods in combination with a high-res-olution confocal microscopy, we demonstrate a different frequency of nuclei containing the CCUGexp foci, a different expression patternof MBNL1 protein and a different sequestration of MBNL1 by CCUGexp repeats in skeletal muscle, vascular smooth muscle and endo-thelia, Schwann cells, adipocytes, and ectodermal derivatives. The level of CCUGexp transcription in epidermal and hair sheath cells islower compared with that in other tissues examined. We suppose that non-muscle tissues of myotonic dystrophy type 2 patients might beaffected by a similar molecular mechanism as the skeletal muscle, as suggested by our observation of an aberrant insulin receptor splicingin myotonic dystrophy type 2 adipocytes.� 2012 Elsevier B.V. All rights reserved.
Keywords: Myotonic dystrophy; Transcription of ZNF9; CCUG repeat expansion; Sequestration of MBNL1 protein; Ribonuclear foci; Insulin receptoralternative splicing
1. Introduction
Both myotonic dystrophy type 1 (DM1) and myotonicdystrophy type 2 (DM2) share a similar pathogenetic
0960-8966/$ - see front matter � 2012 Elsevier B.V. All rights reserved.
http://dx.doi.org/10.1016/j.nmd.2012.03.004
⇑ Corresponding authors. Addresses: Department of Pathology, BrnoFaculty Hospital, Jihlavska 20, CZ-625 00 Brno, Czech Republic. Tel.:+420 532233837 (Z. Lukas); Laboratory of Chromatin Function, Damageand Repair, Dept. of Molecular Cytology and Cytometry, Institute ofBiophysics, Academy of Sciences of CR, Kralovopolska 135, 61265 Brno,Czech Republic. Tel.: +420 541517165; mobile: +420 728 084060 (M.Falk).
E-mail addresses: [email protected], [email protected] (Z. Lukas),[email protected] (M. Falk).
1 The first and second author contributed equally.
Please cite this article in press as: Lukas Z et al., Sequestration of MBNL1 in(2012), http://dx.doi.org/10.1016/j.nmd.2012.03.004
pattern beginning with an expansion of CTG and CCTGnucleotide repeats due to mutation in the genes encodingdystrophia myotonica protein kinase (DMPK) and zinc-finger protein 9 (ZNF9), respectively. Taneja et al. [1] werethe first to describe and illustrate intranuclear foci contain-ing CTG repeat expansions in skeletal muscle and fibro-blasts of DM1 patients; the most of transcripts withexpanded repeats remain retained in the nuclei of cells.
Consequently, DMPK protein levels are reduced [2].Miller et al. [3] demonstrated recruitment of RNA-bindingproteins to the CUGexp foci in DM1 patients. Liquori et al.[4] showed that the second form of DM2 is also caused byan expansion, concretely of a CCTG repeat in the firstintron of the ZNF9 gene. Consequently, co-localization
tissues of patients with myotonic dystrophy type 2, Neuromuscul Disord

2 Z. Lukas et al. / Neuromuscular Disorders xxx (2012) xxx–xxx
ARTICLE IN PRESS
of MBNL1 protein with DMPK expanded repeat tran-scripts in DM1 and DM2 cells was confirmed in vivo byFardaei et al. [5].
The current model of the disease process in DM includesinteraction of CUGexp or CCUGexp mRNAs with CUG-binding proteins, which leads to their sequestration at thevolume of ribonuclear foci and, in turn, to an abnormalregulation of transcription and alternative splicing of theirtarget pre-mRNAs.
There are two groups of CUG-binding proteins: muscle-blind proteins bind pre-mRNA through an evolutionaryconserved tandem CCCCH zinc-finger domain. Humanmuscleblind homologues MBNL1, MBNL2, and MBNL3promote inclusion or exclusion of specific exons on differentpre-mRNAs by antagonizing the activity of the secondgroup of binding proteins – CUG-BP and ETR 3-like fac-tors (CELF proteins). The MBNL1 protein from theMBNL family promotes transition of splicing from foetalto adult exons (reviewed in Pascual et al. [6]), while CUG-binding protein (CUG-BP1) helps to retain foetal exons.
CUG-BP1 binds to single-stranded RNA and does notlocalize to nuclear foci either in DM1 or DM2 [7–10].Adult mouse skeletal muscle overexpressing CUG-BP1reproduces molecular and physiological defects of DM1tissue; the results of the study [10] suggest that CUG-BP1also plays a role in the developmental regulation of abnor-mal splicing in DM1. On the other hand, in DM2, MBNL1is sequestered on expanded CCUG repeat RNA whichaccumulates in nuclear foci like CUG repeat RNA, butCUG-BP1 is not overexpressed, suggesting that DM2 isprimarily a disease of MBNL1 depletion [10]. This multi-step model, common to both DM1 and DM2 [11,12], iswell explored in skeletal muscle, but not in other cell typesor tissues.
MBNL proteins have no general effect on alternativesplicing but rather regulate splicing of only specific targets[8]. Consequently, an inappropriate splicing of selectedtranscripts leads to the characteristic phenotype of DM1and DM2 patients. For instance, the loss of MBNL1results in an altered splicing of ClC-1 mRNA, expressionof non-functional ClC-1 protein, and subsequently to thedisruption of chloride conductance in muscle membrane[13,14]; this is manifested as myotonia, the characteristicsymptom of myotonic dystrophies. Another core featureof DM1 observed in skeletal muscles is insulin resistancedue to an altered splicing of the insulin receptor mRNA[15]. The list of the genes and exons known to be affectedby spliceopathy in DM1 skeletal muscle, brain and heartis increasing [9]; similar results could be reasonablyexpected also in DM2, since gene expression analysis indi-cated no essential differences between processing of theClC1 and insulin receptor pre-mRNAs in the muscle tissueof both DM1 and DM2 patients [12,16]. The splicing pat-tern of the insulin receptor, directly related to the DM2phenotype, was described to be altered in in vitro differen-tiated DM2 myoblasts [17]. From the opposite point ofview, DM1/2 presents a potential target for small molecule
Please cite this article in press as: Lukas Z et al., Sequestration of MBNL1 in(2012), http://dx.doi.org/10.1016/j.nmd.2012.03.004
therapy; since the pathogenesis of these disorders involvessequestration of splicing factors such as MBNL1 andCUG-BP1, caused by an RNA gain-of-function mutation,an agent that antagonizes this process could potentially beused therapeutically. Indeed, Pentamidine was proved toreverse the splicing defects associated with myotonic dys-trophy [18].
The structural organization and composition of the fociis still incompletely known. Recently, the spatial relationsof the components of the splicing apparatus and theMBNL1-containing ribonuclear foci in cell nuclei havebeen explored using immunohistochemical and electron-microscopic methods. The RNA-containing nuclear fociare round electron dense spaces which contain RNPs andproved to be immunopositive for MBNL1. These nucleardomains are surrounded by perichromatin fibrils (PFs), amorphological equivalent of hnRNP (heterogeneousnuclear ribonucleoproteins – complexes of RNA and pro-tein present in the cell nucleus during gene transcriptionand subsequent post-transcriptional modification of thenewly synthesized pre-mRNA), and by perichromatingranules (PG), small nuclear RNPs (snRNP). ThesesnRNP as well as hnRNP co-localize in the nuclear fociwith MBNL1 protein. The 3rd nuclear RNA-containingstructure, interchromatin granules (IG, nuclear speckles)do not co-localize – unlike IG in DM1 – with the PF andPG in DM2 [19,20]. The sequestration of splicing factorsinvolved in early phases of pre-mRNA processing supportsthe hypothesis of general alteration in the maturation ofseveral mRNAs, which could lead to pathological dysfunc-tion in dystrophic patients.
To better understand the role of the influence of CUG/CCUG repeat expression on the development of DM1/DM2 pathology, it is necessary to establish the identityof the tissues and cell types in which the expanded mRNAsand RNA-binding proteins are expressed.
DMPK mRNA was found to be expressed in a range ofadult mouse tissues that show pathology in DM1, but alsoin the intestinal epithelium, liver and cartilage, which hadnot been reported to show abnormalities in DMPK�/�mice. DMPK RNA was not found in the ovary, pancreasand kidney [21]. To date, there are still no comprehensivedata about the expression of DMPK or ZNF9 genes inhuman tissues. DMPK transcripts were detected in foetaleyes and in adult conjunctival and corneal epithelia, uvea,cellular layers of the retina, optic nerve, and in the sclera [22].
There are only several reports about CUGexp-containingfoci in human non-muscle tissues: Mankodi et al. [23] illus-trated ribonuclear intranuclear foci present in a smoothmuscle cell of an intramuscular arteriole of a patient withDM1. Sequestration of muscleblind proteins in the nuclearfoci of mutant CUGexp RNA and deregulated alternativesplicing in cortical and subcortical neurons was reportedby Jiang et al. [24]. Nuclear CUGexp RNA foci were alsodescribed in DM1 cardiomyocytes [25], subsynaptic nucleiof muscle fibres and in motor neurons of DM1 neuromus-cular junction [26]. In addition, expression of mutant
tissues of patients with myotonic dystrophy type 2, Neuromuscul Disord

Z. Lukas et al. / Neuromuscular Disorders xxx (2012) xxx–xxx 3
ARTICLE IN PRESS
DMPK mRNA was shown to be accumulated in foci in thegallbladder smooth muscle cells of DM1 patients [27].Finally, Bonifazi et al. [28] demonstrated by RNA-FISHanalysis the presence of CUGexp RNA foci in the nucleiof amniotic cells of a DM1 foetus.
The ZNF9 gene is ubiquitously expressed but the level of theZNF9 post-transcriptional modification of the newly synthe-sized RNA (pre-mRNA) or ZNF9 protein in human tissues isnot known. To date, the expression of CCUGexp RNA or co-localization of CCUGexp RNA foci with MBNL1 protein onlyin muscle tissue and cell cultures has been reported [5,23,29,30].
In this report, we examine the presence of CCUGexp
RNA transcripts of the ZNF9 gene associated with the for-mation of ribonuclear foci in human muscle and non-muscletissues present in muscle biopsies and skin excisions frompatients with DM2. We also study the expression ofMBNL1 protein, quantify the frequency of nuclei contain-ing the CCUGexp and MBNL1 foci, and determine the rateof co-localization, i.e. possible sequestration of the MBNL1within CCUGexp repeats in the tissues examined.
Based on our analysis of the insulin receptor splicing inadipocytes taken from a DM2 patient, we show that the co-localization of the expanded repeats with the MBNL1 proteinhas functional consequences and may disturb some MBNL1functions, such as splicing activity. Therefore, we speculatethat the co-localization of the expanded repeats with theMBNL1 protein may result in alteration of some MBNL1functions and, consequently, non-muscle tissues included inthe DM2 phenotype may theoretically be affected by the sameor a similar molecular mechanism as the skeletal muscle.
2. Materials and methods
2.1. Tissue samples
Diagnostic muscle biopsies and skin excisions of 12patients with DM2 (9 muscle biopsies, 4 skin excisions)and 9 non-DM controls (6 muscle biopsies, 3 skin excisions)were collected after obtaining the written informed consent.The numbers of nuclei in tissues examined of DM2 patientsand non-DM controls are listed in Table 1. The sampleswere deep-frozen and the histopathological and histochem-ical examination [31] as well as fluorescence in situ hybrid-ization (FISH) and immunohistochemical (IHC) orimmunofluorescence (IFL) methods were applied on frozensections. The tissue cells in the biopsies were identified by thegeneral texture of the section and, in some cases, by theimmunohistochemical reactivity of the cell types (neurofila-ment proteins, smooth muscle actin, S100 protein, CD34).
The diagnosis of DM2 was confirmed by mutation anal-ysis of blood samples, using the “Tetraplet-primed PCR”
method modified from Triplet-primed PCR [32,33].
2.2. Immunofluorescence
Immunofluorescence (IFL) was performed according toHolt et al. [34]. Briefly, fresh frozen sections (6 lm thick)
Please cite this article in press as: Lukas Z et al., Sequestration of MBNL1 in(2012), http://dx.doi.org/10.1016/j.nmd.2012.03.004
were placed on Superfrost� Plus microscope glasses(Menzel-Glaser), dried, fixed by acetone–methanol (1:1)at room temperature (RT), washed in PBS at RT, and incu-bated for 1 h at 37 �C with the primary mouse antibodyMB1a [19] diluted 1:3 in diluting buffer as described below.Alternatively, namely for the high-resolution confocalmicroscopy (see the particular paragraph), the slides werespatially fixed in 4% paraformaldehyde in PBS for 5 minat RT, and incubated with the MB1a primary antibodyas in the case of the acetone–methanol fixation.
Subsequently, the sections were washed in PBS at RTand incubated with the secondary antibody labelled withAlexa Fluor� 488 (Alexa Fluor� 488 Goat Anti-MouseSFX Kit, Molecular Probese, Invitrogen) for 1 h at 37 �C.
Following incubation, the slides were washed in PBS atRT and mounted in Vectashield Mounting Medium (Vec-tor Laboratories, USA). Nuclear chromatin was counter-stained with 0.075 lg/ml diamino-2-phenylindole (DAPI).The image acquisition and evaluation of the results wereperformed on a Leica DMRXA2 fluorescence microscope.
2.3. Fluorescence in situ hybridization
Fluorescence in situ hybridization (FISH) of frozen mus-cle sections for CUG repeats was performed according toHolt et al. [34]. Frozen sections (6 lm) were placed ontoSuperFrost Plus slides (Menzel-Glaser), air-dried at roomtemperature (RT) for 30 min, fixed in modified Carnoy’s fix-ative (73% ethanol; 25% acetic acid; 2% formalin (Sigma))for 30 min at 4 �C, and washed in PBS at RT followed byPBS at RT. The sections were incubated in prehybridizationbuffer (30% formamide (Sigma) in 2� SSC (Eppendorf)) atRT, and thereafter hybridized with the probe (1 ng/ll) at37 �C in hybridization buffer (30% formamide, 2� SSC,0.02% BSA (Invitrogen), 66 ng/ll yeast tRNA (Invitrogen),2 mM vanadyl complex (Sigma)). Probe for DM1 was 50-CAG CAG CAG CAG CAG CAG CAG-3020–O-Me-RNA50Fl, for DM2: 50-CAG GCA GGC AGG CAGGCA GG-3020–O-Me-RNA50Fl (both Generi Biotech,Czech Republic).
The sections were washed in a post-hybridization wash(30% formamide; 2� SSC) for 30 min at 45 �C followedby 1� SSC washing for 30 min at RT. Finally, the sectionswere mounted by DAPI (Vectashield Mounting Medium,Vecor Laboratories, USA). The slides were observed in aLeica DMRXA2 fluorescence microscope.
2.4. Combined immunofluorescence and in situ hybridization
For combined immunofluorescence and in situ hybrid-ization (IFL-FISH), the same antibodies, dilutions andprocedures as for the immunohistochemistry were used.The sections were dried, fixed by acetone–methanol (1:1)at RT, and incubated with the primary mouse antibodyfor 1 h at 37 �C. The secondary antibody was labelled withAlexa Fluor� 488 (Alexa Fluor� 488 Goat Anti-MouseSFX Kit, Molecular Probese, Invitrogen).
tissues of patients with myotonic dystrophy type 2, Neuromuscul Disord

Table 1The numbers of cell nuclei examined in DM2 patients and non-DM controls for the particular tissue.
Diagnosis Skeletal muscle Vascular media Endothelium Adipocytes Schwann cells Epidermis Hair sheath Sweat gland
Patient
P1 DM2 228 50 84 12 104P2 DM2 51P3 DM2 443 410 307 280 234 606 30 85P4 DM2 97 259 83 30 72P5 DM2 88 23 30P6 DM2 118 13 36P7 DM2 23 18P8 DM2 157 3 22P9 DM2 173 41 36 19 51P10 DM2 26 18 979 491 228P11 DM2 255 33 28 6 275 184 112P12 DM2 27 16 4 160 293 48
R 1559 959 678 351 461 2020 998 473
Control
C1 Muscular dystrophy 20 50 27 7 13C2 Neural atrophy 56C3 Muscle, normal 10 25 31 14 72C4 Skin, prurigo 17 6 46 16 40C5 Neural atrophy 10C6 Varices cruris 9 76 10C7 Myogenic disorder 46 21 18C8 Myositis 37 12 17 18C9 Erythema nodosum 19 90 122 78
R 133 133 115 56 118 212 138 128
P: patients with DM2; C: non-DM controls.Notes: skin excisions were examined outside the lesion.
4 Z. Lukas et al. / Neuromuscular Disorders xxx (2012) xxx–xxx
ARTICLE IN PRESS
Following the incubation, the slides were washed, fixedin 4% paraformaldehyde PBS at RT, and prehybridizedin 30% formamide in 2� SSC. Next, the tissue sectionswere hybridized for 16 h at 37 �C with 1 ng/ll of a 50-endcy3-labelled RNA probe, containing either CUG or CCUGrepeats (OPC-purified 20-O-Me-RNA, 50-20mers, GeneriBiotech), in a hybridization buffer consisting of 30% form-amide, 2� SSC, 0.02% BSA, 66 lg/ml yeast rRNA, and2 mM vanadyl complex. Afterwards, the slides werewashed in 1� SSC for 30 min (RT) and mounted in Vecta-shield Mounting Medium (Vector Laboratories, USA).Nuclear chromatin was counterstained with DAPI. BothRNA foci and MBNL1 protein were visualized on a LeicaDM RXA2 fluorescence microscope, alternatively using ahigh-resolution confocal regime as described below.
2.5. Image acquisition and confocal microscopy
Image acquisition and confocal microscopy were per-formed on an automated Leica DM RXA fluorescencemicroscope in a wide-field or confocal, high-resolutionregime. This configuration enabled us to inspect cell nucleiin 3D-space, which allowed us to discriminate between truereaction signals, lipofuscin and autofluorescence, as well asto confirm mutual co-localization of MBNL1 and CCUGexp
foci in all the three planes (Fig. 1). For confocal imageacquisition, the microscope was equipped with a CSU10aNipkow disc (Yokogawa, Japan) for confocal imaging, a
Please cite this article in press as: Lukas Z et al., Sequestration of MBNL1 in(2012), http://dx.doi.org/10.1016/j.nmd.2012.03.004
CoolSnap HQ CCD-camera (Photometrix, Tucson, AZ,USA), an Ar/Kr-laser (Innova 70C, Coherent, Palo Alto,CA, USA), and an oil immersion Plan Fluotar objective(100�/NA1.3) [35]. Automated exposure, image qualitycontrol, and other procedures were performed using FISH2.0 software [36]. The exposure time and dynamic range ofthe camera in the red, green and blue channels were adjustedto the same values for all slides to obtain quantitatively com-parable images. Up to forty serial optical slices (according tothe thickness of tissue sections) were captured at 0.2 lmintervals along the z-axis at a constant temperature of 26 �C.
2.6. Image analysis
The count of positive nuclei was determined in each tissuetype as the rate between the number of signal-bearing nucleiand the number of all evaluable nuclei (PN/RN) present in ahigh-power field (HPF). For each tissue type the values werecalculated from at least 10 HPF or 100 nuclei (Table 1). Thetissue cells in the biopsies were identified by the general tex-ture of the section, in some cases by the immunohistochem-ical reactivity of the cell types (neurofilament proteins,smooth muscle actin, S100 protein, CD34). The numbersof CCUGexp and MBNL1 foci per nucleus were determinedby visual inspection of maximal images composed of indi-vidual confocal slices. Co-localization of MBNL1 andCCUGexp foci was determined in confocal regime as a>50% overlay (Fig. 1) of the particular signals at original
tissues of patients with myotonic dystrophy type 2, Neuromuscul Disord

Fig. 1. Co-localization of CCUGexp RNA and MBNL1 protein foci as determined by the IFL-FISH method in combination with a high-resolutionconfocal microscopy. The main panel shows three nuclei of DM2 skeletal muscle (TOPRO-3, artificially blue), two of them with ribonuclear CCUGexp
(red) and MBNL1 foci (green); the maximal image in the X–Y coordinate plane, composed from 20 optical confocal slices with a z-step of 2 lm, isdisplayed. Right panels demonstrate, at single confocal slices, spatial preservation of nuclei after their fixation with paraformaldehyde (see Section 2) andco-localization of CCUGexp and MBNL1 foci in all the three planes (X–Y, X–Z, and Y–Z) (the middle nucleus from the main maximal image is displayed).The bottom panel shows images in separated red and green channels (red: CCUGexp foci, green: MBNL1 protein).
Z. Lukas et al. / Neuromuscular Disorders xxx (2012) xxx–xxx 5
ARTICLE IN PRESS
images (without deconvolution). The size of the foci wasdetermined in pixels (1 pix = 165 � 165 nm), after manualdemarcation of the signal area on the maximal image.
2.7. Statistical analysis of the data
A comparison of the percentages of CCUGexp andMBNL1 positive nuclei in different tissues was performed.Positive nuclei were further examined to analyse the num-ber and size of CCUGexp and MBNL1 foci.
The percentage of CCUGexp and MBNL1 positivenuclei in each tissue was computed as a mean of the percent-ages of positive nuclei in each microscopic field weighted bythe number of nuclei in the microscopic field. Generalizedlinear mixed models were used for the analysis of the percent-age of positive nuclei, the number and size of foci in differenttissues to account for the correlation of microscopic fields
Please cite this article in press as: Lukas Z et al., Sequestration of MBNL1 in(2012), http://dx.doi.org/10.1016/j.nmd.2012.03.004
from one patient. Differences in the size of CCUGexp
foci according to the categories of the size of MBNL1 fociwere tested using a Kruskal–Wallis ANOVA test. Alevel of statistical significance a = 0.05 was used. Theanalyses were performed in the statistical software PASW
Statistics 19 and software R. The results of comparison ofthe size of CCUGexp and MBNL1 foci were visualized usingbox plots prepared in the software STATISTICA for
Windows 9.1.
2.8. Semiquantitative PCR for insulin receptor
The expression analysis of the insulin receptor isoform Aand B (IR-A, IR-B) mRNAs, respectively, was performed inskeletal muscle and adipose tissue, according to Savkur et al.[15], with small adaptations. A High Pure RNA IsolationKit (Roche, #11828665001) was employed for isolation of
tissues of patients with myotonic dystrophy type 2, Neuromuscul Disord

6 Z. Lukas et al. / Neuromuscular Disorders xxx (2012) xxx–xxx
ARTICLE IN PRESS
total RNA from the homogenized skeletal muscle tissue, anRNeasy Lipid Tissue Mini Kit (Qiagen, #704804) for isola-tion from the adipose tissue. Altogether 200 ng of RNA andthe Transcriptor First-Strand cDNA Synthesis Kit (Roche)were used for reverse transcription with the primer 50-TTGGGGAAAGCTGCCACCGT-30. By using a Hot StartMaster Mix Kit (Qiagen), PCR analysis was accomp-lished from 5 ll of cDNA in a total volume of 50 ll, witha primer pair (50-CCAAAGACAGACTCTCAGAT-30
and 50-AACATCGCCAAGGGACCTGC-30) [15] flankingthe exons 10 and 12. Thirty cycles consisting of 95 �C/30 s,60 �C/30 s, and 72 �C/30 s were followed by a finalextension at 72 �C for 10 min. Ten ll of PCR productswas separated on 10% PAGE gel (acrylamide:bis-acrylam-ide 29:1) in TBE buffer. The size of PCR products was131 bp (IR isoform A) and 167 bp (IR isoform B).
Fig. 2. Demonstration of CCUGexp RNA and MBNL1 protein foci in skeletaland MBNL1 protein foci (green) were simultaneously detected by IFL-FISH(panel B): adipocytes, Schwann cells and epidermis of DM2 patients. The fociimages: wide-field views on the tissue; inserts: selected nuclei (identified by thindicated. For selected nuclei (panel B), green channel of MBNL1 and redlocalization; Chromatin was counterstained with DAPI (artificially blue); max0.2 lm wide. Abbreviations: I, fascicle of interstitial cells with intranuclear foci(SM); L, lipofuscin; M, media; E, endothelium.
Please cite this article in press as: Lukas Z et al., Sequestration of MBNL1 in(2012), http://dx.doi.org/10.1016/j.nmd.2012.03.004
3. Results
3.1. Confirmation of DM2 diagnosis of the samples
examined
The diagnosis of DM2 was confirmed by mutation anal-ysis of blood samples, using the “Tetraplet-primed PCR”
method. In all DM2 cases, an expanded allele [(CCTG)n
> 50–100] of the ZNF9 gene was detected (Suppl. Table1), while it was absent in non-DM controls.
3.2. Histopathological features of muscle biopsies in DM2
patients
Our histopathological findings correspond to the data pre-viously published (reviewed in [37,38]). In two cases, however,
muscle and non-muscle tissues of DM2 patients. CCUGexp RNA foci (red)method in (panel A): skeletal muscles, vascular media and endothelium,were not observed in non-DM control tissues (panels A and B). The maine red arrow at wide-field images), multiplied from the original image aschannel of CCUGexp are displayed separately to demonstrate their co-
imal microscopic images displayed were composed from 10 confocal slices(presumably capillary endothelium and nerve fibres) between muscle fibres
tissues of patients with myotonic dystrophy type 2, Neuromuscul Disord

Z. Lukas et al. / Neuromuscular Disorders xxx (2012) xxx–xxx 7
ARTICLE IN PRESS
an inflammatory infiltration of the endomysium by T cells,and in one case a picture indistinguishable from the congenitalfibre type disproportion, were found [39].
3.3. The presence of nuclear foci containing ZNF9
transcripts in human tissues
We have first analyzed the retention of expanded CCUGmRNA (further termed CCUGexp) in the foci in cross-stri-ated muscle fibres (skeletal muscle also served as a positivecontrol tissue) obtained from genetically confirmed DM2patients and non-DM controls. By employing the simpleRNA-FISH or combined IFL-FISH method, the CCUGexp
foci were directly visualized in situ in 66.4% nuclei in theskeletal muscle of DM2 patients (Figs. 1–3). In other tis-sues, the proportion of the nuclei that contained CCUGexp
foci differed: in sweat gland, adipocytes, Schwann cells,endothelial cells, and vascular smooth muscle the valuesfluctuated from 57.9% to 76.8% (Fig. 3) (for the significanceof these differences see Suppl. Table 2). In epidermal andfollicular keratinocytes the number of positive nuclei wasmarkedly lower, 30.8% and 47.6% respectively (Figs. 2and 3 and Suppl. Table 2).
These results thus provide unequivocal evidence that thetranscription of the expanded repeats of the ZNF9 genetakes place at a level ascertainable by the in situ hybridiza-tion method also in non-muscle tissues which may beinvolved in DM2 pathology [40]; hence, these tissues maytheoretically be also affected by the same molecularpathological mechanism as skeletal muscles; however, thetranscription levels of the ZNF9 gene in the tissues studieddiffer (see later).
As expected, the foci were completely absent from thenuclei of all non-DM2 control muscle fibres and other tis-sues analyzed.
86 4 86 5 87 5 89.2 91.9 91.5100
68.1
59.0
30.8
47.6
62.166.4
76.8
57.9
83.3 86.479.9
86.5 87.5
0
10
20
30
40
50
60
70
80
90
es el s et s e d a
% p
ositi
ve n
ucle
i
Adipoc
ytes
Endothe
l
Epiderm
is
Hair sh
eet
Schwan
n cell
s
Skelet
al mus
cle
Sweat g
land
Vascu
lar m
edia
Tissue
A B
Fig. 3. The percentage of CCUGexp and MBNL1 positive nuclei comparedexamination of MBNL1 foci were fixed either using acetone–methanol (panelblack bars: nuclei containing CCUGexp foci. See Suppl. Table 2 for a significa
Please cite this article in press as: Lukas Z et al., Sequestration of MBNL1 in(2012), http://dx.doi.org/10.1016/j.nmd.2012.03.004
3.4. Frequency of nuclei containing MBNL 1 protein and
comparison with the frequency of CCUGexp – positive nuclei
in DM2 tissues
As follows from the IFL staining, MBNL1 protein wasexpressed in a high frequency of nuclei in all tissues studied(Figs. 2 and 3). This is a further evidence that humanMBNL1 is not muscle-specific [34].
A comparison of the frequency of MBNL-positive withCCUGexp-positive nuclei (Figs. 2 and 3) indicates that a num-ber of MBNL1-positive nuclei do not contain CCUGexp
ZNF9 transcript. These results hold both for the tissues fixedwith acetone–methanol or formaldehyde, although slightlydifferent values of MBNL1-positive nuclei were obtained bythese two methods (Figs. 3A and B, respectively).
The frequency of MBNL1-positive nuclei in otherexamined tissues varied between 79.9% and 91.9% forthe acetone–methanol fixation (Fig. 3A and Suppl. Table3) or between 86.7% and 99.3% for the formaldehyde(Fig. 3B and Suppl. Table 4); the differences observedbetween these two methods can be attributed to the factthat cross-linking of tissue polypeptide chains by formal-dehyde generally contributes to a higher retention of pro-teins in tissue sections (Fig. 4). Anyway, in both cases thisprovides evidence of a high level of expression of theMBNL1 protein in all (i.e. also non-muscle) tissues stud-ied. Only skeletal muscles and the epidermis, with thehighest and lowest percentage of MBNL1 positive nucleiafter formaldehyde fixation, respectively, provided statisti-cally significant differences from other tissues (Suppl.Table 4).
In non-DM controls, the proportion of the cells express-ing MBNL1 protein in all tissues examined was very simi-lar compared to that in patients with DM2. Table 2 showsthat the differences in the percentage of MBNL1 positive
86.793.4
86 2
95.7 97.5 99.3
89.296.8
90
100
68.1
59.0
30.8
47.6
62.166.4
76.8
57.9
86.7 86.2
0
10
20
30
40
50
60
70
80
90
tes hel is et lls le nd dia
% p
ositi
ve n
ucle
i
CCUGexp
MBNL1
Adipoc
ytes
Endoth
e
Epiderm
is
Hair sh
eet
Schwan
n cell
s
Skelet
al mus
cle
Sweat g
land
Vascu
lar m
edia
Tissue
for skeletal muscle and other soft tissues of DM2 patients. Tissues forA) or formalin (panel B). Grey bars: nuclei positive for MBNL1 protein,nce of differences.
tissues of patients with myotonic dystrophy type 2, Neuromuscul Disord
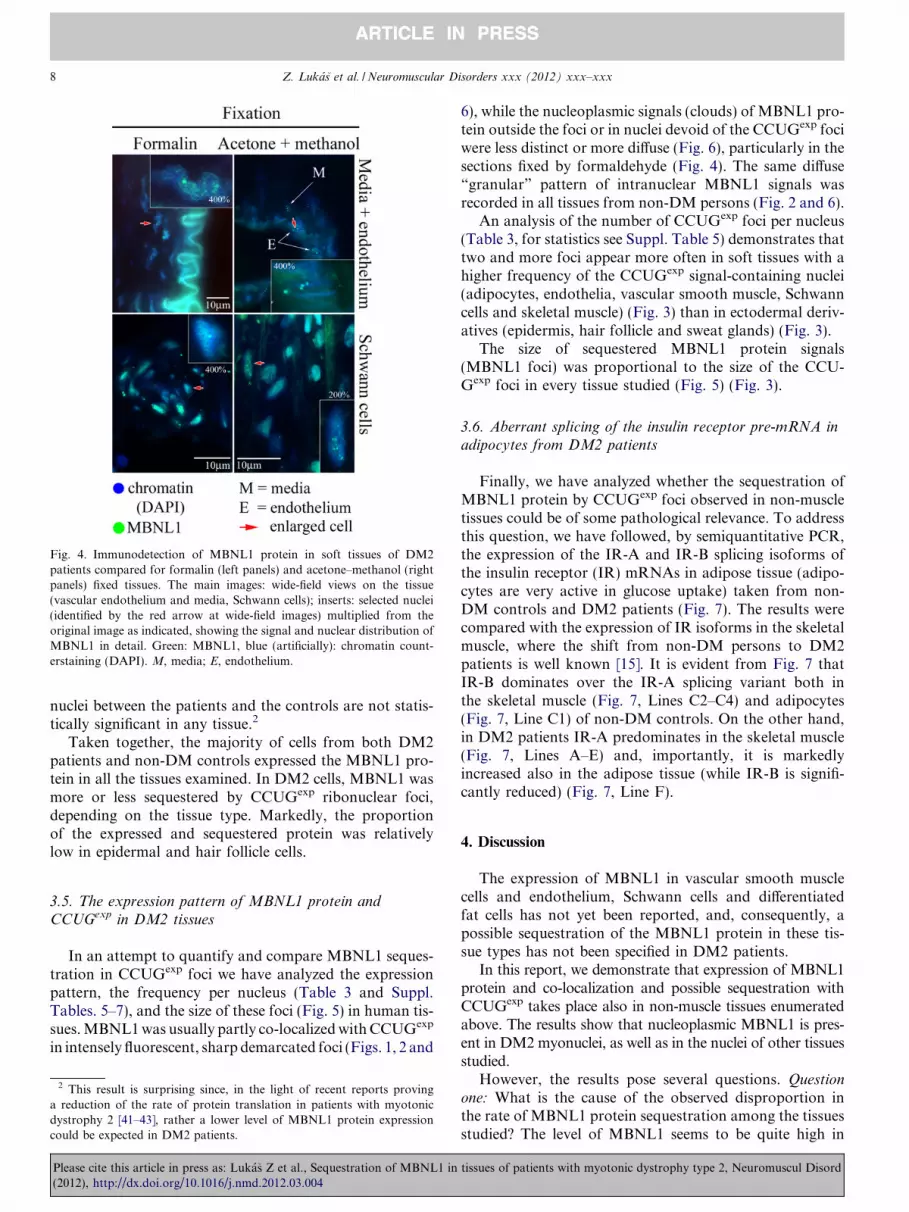
Fig. 4. Immunodetection of MBNL1 protein in soft tissues of DM2patients compared for formalin (left panels) and acetone–methanol (rightpanels) fixed tissues. The main images: wide-field views on the tissue(vascular endothelium and media, Schwann cells); inserts: selected nuclei(identified by the red arrow at wide-field images) multiplied from theoriginal image as indicated, showing the signal and nuclear distribution ofMBNL1 in detail. Green: MBNL1, blue (artificially): chromatin count-erstaining (DAPI). M, media; E, endothelium.
8 Z. Lukas et al. / Neuromuscular Disorders xxx (2012) xxx–xxx
ARTICLE IN PRESS
nuclei between the patients and the controls are not statis-tically significant in any tissue.2
Taken together, the majority of cells from both DM2patients and non-DM controls expressed the MBNL1 pro-tein in all the tissues examined. In DM2 cells, MBNL1 wasmore or less sequestered by CCUGexp ribonuclear foci,depending on the tissue type. Markedly, the proportionof the expressed and sequestered protein was relativelylow in epidermal and hair follicle cells.
3.5. The expression pattern of MBNL1 protein andCCUGexp in DM2 tissues
In an attempt to quantify and compare MBNL1 seques-tration in CCUGexp foci we have analyzed the expressionpattern, the frequency per nucleus (Table 3 and Suppl.Tables. 5–7), and the size of these foci (Fig. 5) in human tis-sues. MBNL1 was usually partly co-localized with CCUGexp
in intensely fluorescent, sharp demarcated foci (Figs. 1, 2 and
2 This result is surprising since, in the light of recent reports provinga reduction of the rate of protein translation in patients with myotonicdystrophy 2 [41–43], rather a lower level of MBNL1 protein expressioncould be expected in DM2 patients.
Please cite this article in press as: Lukas Z et al., Sequestration of MBNL1 in(2012), http://dx.doi.org/10.1016/j.nmd.2012.03.004
6), while the nucleoplasmic signals (clouds) of MBNL1 pro-tein outside the foci or in nuclei devoid of the CCUGexp fociwere less distinct or more diffuse (Fig. 6), particularly in thesections fixed by formaldehyde (Fig. 4). The same diffuse“granular” pattern of intranuclear MBNL1 signals wasrecorded in all tissues from non-DM persons (Fig. 2 and 6).
An analysis of the number of CCUGexp foci per nucleus(Table 3, for statistics see Suppl. Table 5) demonstrates thattwo and more foci appear more often in soft tissues with ahigher frequency of the CCUGexp signal-containing nuclei(adipocytes, endothelia, vascular smooth muscle, Schwanncells and skeletal muscle) (Fig. 3) than in ectodermal deriv-atives (epidermis, hair follicle and sweat glands) (Fig. 3).
The size of sequestered MBNL1 protein signals(MBNL1 foci) was proportional to the size of the CCU-Gexp foci in every tissue studied (Fig. 5) (Fig. 3).
3.6. Aberrant splicing of the insulin receptor pre-mRNA inadipocytes from DM2 patients
Finally, we have analyzed whether the sequestration ofMBNL1 protein by CCUGexp foci observed in non-muscletissues could be of some pathological relevance. To addressthis question, we have followed, by semiquantitative PCR,the expression of the IR-A and IR-B splicing isoforms ofthe insulin receptor (IR) mRNAs in adipose tissue (adipo-cytes are very active in glucose uptake) taken from non-DM controls and DM2 patients (Fig. 7). The results werecompared with the expression of IR isoforms in the skeletalmuscle, where the shift from non-DM persons to DM2patients is well known [15]. It is evident from Fig. 7 thatIR-B dominates over the IR-A splicing variant both inthe skeletal muscle (Fig. 7, Lines C2–C4) and adipocytes(Fig. 7, Line C1) of non-DM controls. On the other hand,in DM2 patients IR-A predominates in the skeletal muscle(Fig. 7, Lines A–E) and, importantly, it is markedlyincreased also in the adipose tissue (while IR-B is signifi-cantly reduced) (Fig. 7, Line F).
4. Discussion
The expression of MBNL1 in vascular smooth musclecells and endothelium, Schwann cells and differentiatedfat cells has not yet been reported, and, consequently, apossible sequestration of the MBNL1 protein in these tis-sue types has not been specified in DM2 patients.
In this report, we demonstrate that expression of MBNL1protein and co-localization and possible sequestration withCCUGexp takes place also in non-muscle tissues enumeratedabove. The results show that nucleoplasmic MBNL1 is pres-ent in DM2 myonuclei, as well as in the nuclei of other tissuesstudied.
However, the results pose several questions. Question
one: What is the cause of the observed disproportion inthe rate of MBNL1 protein sequestration among the tissuesstudied? The level of MBNL1 seems to be quite high in
tissues of patients with myotonic dystrophy type 2, Neuromuscul Disord

Table 2Comparison of the percentage of MBNL1 positive nuclei in skeletal muscles and soft tissues of DM2 patients and non-DM controls, fixed either withacetone–methanol (left panel) or formalin (right panel).
Acetone–methanol fixation Formalin fixation
% Positive nuclei in tissue of patients/%positive nuclei in tissue of controls
p-Value % Positive nuclei in tissue of patients/%positive nuclei in tissue of controls
p-Value
Adipocytes 83.3%/83.9% 0.955 86.7%/83.3% 0.832Endothelium 86.4%/93.2% 0.606 93.4%/100.0% 0.335Epidermis 79.9%/73.6% 0.340 86.2%/83.0% 0.996Hair sheet 86.5%/75.0% 0.465 95.7%/91.8% 0.192Schwann cells 87.5%/83.6% 0.979 97.5%/92.2% 0.279Skeletal muscle 89.2%/80.6% 0.471 99.3%/97.0% 0.561Sweat gland 91.9%/75.0% 0.454 89.2%/99.0% 0.115Vascular media 91.5%/89.3% 0.740 96.8%/96.4% 0.928
Table 3The summary of the number of CCUGexp foci per nucleus in DM2 tissues.
Tissue Number of CCUGexp foci per nucleus
1 focus 2 and more foci Total
Adipocytes 1 (6.7%) 14 (93.3%) 15 (100.0%)Endothelium 3 (9.7%) 28 (90.3%) 31 (100.0%)Epidermis 70 (85.4%) 12 (14.6%) 82 (100.0%)Hair follicle 62 (82.7%) 13 (17.3%) 75 (100.0%)Media 12 (33.3%) 24 (66.7%) 36 (100.0%)Schwann cells 12 (30.8%) 27 (69.2%) 39 (100.0%)Skeletal muscle 18 (33.3%) 36 (66.8%) 54 (100.0%)Sweat gland 52 (72.2%) 20 (27.8%) 72 (100.0%)
Z. Lukas et al. / Neuromuscular Disorders xxx (2012) xxx–xxx 9
ARTICLE IN PRESS
all the cell types studied, despite some variation of thepercentage of MBNL1 positive nuclei in the tissues. Conse-quently, the level of MBNL1 sequestration mostly dependson the expression level of the ZNF9 gene (i.e. CCUGexp
repeats), which differs in individual tissues. The propor-tion of CCUGexp-negative cells in the skeletal muscle, othersoft tissues, and in sweat glands is lower than that in epi-dermal and hair follicle/sheath cells (Fig. 3). For compari-son, we have found only one report on the rate ofexpression of nuclear foci in DM2 skeletal muscle – the fociwere recorded in >70% of the nuclei with a rate of co-local-ization >90% [30]. The disproportion is therefore difficultto explain: one possibility is a different proliferation rate.
els)
700
els) 350
400
ze o
f CC
UG
exp
foci
(in
pixe
100
200
300
400
500
600
ze o
f CC
UG
exp
foci
(in
pixe
50
100
150
200
250
300
350
Siz 0Siz
0<=50 50-100 >100
Size of MBNL1 foci (in pixels)
A B
Fig. 5. Correlation between the sizes of the CCUGexp and co-localizing MBN(epidermis, hair sheath, sweat gland) and (B) soft DM2 tissues (skeletal musc
Please cite this article in press as: Lukas Z et al., Sequestration of MBNL1 in(2012), http://dx.doi.org/10.1016/j.nmd.2012.03.004
A normal consequence of mitosis in eukaryotes is transitoryrepression of the transcription [44]. Epidermal (and hair fol-licle) cells are characterized by a relatively high proliferationrate compared to that in a differentiated skeletal muscle (per-manently in the G0 phase) or in other tissues examined(entering the cell cycle only on activation signal). Alterna-tively, the regulation of the ZNF9 (CCUGexp) expressionin ectodermal tissues may be differently regulated.
Question two: Is the sequestration of the MBNL1 pro-tein into the ribonuclear foci sufficient enough to depleteits activity from the nucleoplasm? Nucleoplasmic MBNL1is only partially sequestered into the ribonuclear foci ofexpanded repeats in the skeletal muscle (reviewed in [34]).Our results (Fig. 3) demonstrate that the MBNL1 proteinremains unsequestered in about 23–33% of the MBNL1-containing myonuclei and yet the DM2 pathological phe-notype develops. We also demonstrate aberrant splicingof the insulin receptor in the human adipose tissue despiteonly a partial sequestration of MBNL1.
Question three: Are there any specific target genes orpre-mRNAs for MBNL1 in other tissues examined? Dothese targets correspond to those in the skeletal muscle(or heart and brain) in patients with DM2? How aboutthe tissues examined in this study?
Previous studies suggested that insulin response defectsmight play a key role in the metabolic manifestations ofDM1 potentially leading to type 2 diabetes [45–47]. The
p<0 001
Median
25%-75%
Min-max
p<0.001
<=50 50-100 >100Size of MBNL1 foci (in pixels)
L1 foci. Results are displayed separately for (A) ectodermal DM2 tissuesle, vascular media and endothelium, adipocytes and Schwann cells).
tissues of patients with myotonic dystrophy type 2, Neuromuscul Disord

Fig. 6. Nuclear distribution of MBNL1 protein in skeletal muscle and epidermis of non-DM controls and DM2 patients. The level of MBNL1sequestration by CCUGexp foci in DM2 skeletal muscle and epidermis is visually compared in the main images (MBNL1: green, CCUGexp: red, nuclearchromatin: TOPRO-3, artificially blue). Quantification of MBNL1 sequestration by CCUGexp foci is provided as histograms showing distributionsof pixels according to their intensity in the green channel (from 0 [black] to 255 [green]). Histograms were made separately for CCUGexp foci andextrafocal nuclear area. The maximal images, composed from 20 optical confocal slices with a z-step of 0.2 lm, were used for demarcation of the foci areaand signal quantification in the Adobe Photoshop CS5 software.
Fig. 7. An aberrant splicing of the insulin receptor in DM2 skeletal muscleand adipose tissue. Insulin receptor splicing is compared for skeletalmuscles and adipose tissue of non-DM controls and DM2 patients, as theexpression levels of insulin receptor splicing variants IR-A and IR-BmRNAs. The ratios of IR-A to IR-B were determined by semiquantitativePCR. Figure shows IR-A (131 kb) and IR-B (167 kb) PCR ampliconsseparated on 10% PAGE gel (acrylamide:bis-acrylamide 29:1) in TBEbuffer. Lines A–E: skeletal muscle of DM2 patients P3, P9, P7, P6, and P1;Line F: adipocytes of a DM2 patient P3 (the same patient as in the LineA); Line C1: adipocytes from the DM1/DM2 negative control (taken fromsurgery); Lines C2–C4: DM1/DM2 negative skeletal muscles; Line C�:non-cDNA control (non-template PCR control). Size marker: 1 kb DNAladder.
10 Z. Lukas et al. / Neuromuscular Disorders xxx (2012) xxx–xxx
ARTICLE IN PRESS
muscles of DM1 patients contain lower than normal levels ofinsulin receptor RNA and protein [48] and display an abnor-mal regulation of insulin receptor mRNA splicing, resultingin a predominant expression of the lower-signalling non-mus-cle IR-A isoform associated with a weaker metabolic responsein skeletal muscle tissue and cultured skeletal muscle cells fromDM1 [14,15]. Importantly, MBNL1 was found to be the pri-mary determinant of CUGexp foci formation and aberrantinsulin receptor splicing in the myoblasts of patients with myo-tonic dystrophy [49].
Please cite this article in press as: Lukas Z et al., Sequestration of MBNL1 in(2012), http://dx.doi.org/10.1016/j.nmd.2012.03.004
Insulin receptor splicing in insulin-responsive tissues(skeletal muscle, liver and adipose tissue) was also studiedin transgenic mice carrying the human genomic DM1 regionwith expanded (>350 CTG) repeats [50]. The mice displayeda tissue-specific and age-dependent abnormal regulation ofinsulin receptor mRNA splicing in all the tissues studied.Splicing abnormalities of insulin receptors prior to thedevelopment of muscle pathology were also reported inDM2 muscle [16]. Recently, Sen et al. established thatMBNL1 binds specifically to the IR RNA [51] and overex-pression or knockdown of MBNL1 altered the levels of exon11 inclusion. The present finding of nuclear CCUGexp foci infat cells and sequestration of MBNL1 protein in these foci inDM2 patients therefore suggest a role of the MBNL1 pro-tein in abnormal splicing of the insulin receptor. Ourdemonstration of the shift in the proportion of IR-B/IR-Ain human DM2 adipocytes is in accordance with this idea.
The peripheral nerve expresses predominantly thehigh-affinity insulin receptor lacking exon 11. The insulinreceptor was localized to paranodal terminal Schwann cellloops and microvilli and to the paranodal axolemma, whilethe mRNA was found in Schwann cells, endothelial cells,and pericytes [52]. If the splicing of the receptor in Schw-ann cells is controlled by MBNL1, its sequestration maycontribute to an increased insulin resistance of DM2patients. Studies carried out to verify the involvement ofthe peripheral nervous system (PNS) concerned onlyDM1 patients [53–57].
There are also only few reports that concern thepresence of RNA foci or aberrant alternative splicingcontrolled by MBNL1 in vascular smooth muscle cells.Co-localization of ribonuclear inclusions and MBNL1 fociwas reported in the gallbladder smooth muscle of a DM1patient [25]. However, we do not know whether the
tissues of patients with myotonic dystrophy type 2, Neuromuscul Disord

Z. Lukas et al. / Neuromuscular Disorders xxx (2012) xxx–xxx 11
ARTICLE IN PRESS
sequestration of MBNL1 in the vascular smooth muscledemonstrated in this report is related to any specific targetgene or exon.
Thus, what could be the possible molecular pathwaysthat lead to an altered smooth muscle function or contractil-ity in DM1/DM2 patients? Contrary to the cell typesdiscussed above, there are no indications on the MBNL1-dependent alternative splicing of insulin receptors invascular smooth muscles. Other possible candidates for analtered alternative splicing controlled by MBNL1, describedfor DM1, could be represented by a-actinin [58] and theryanodine receptor [59].
Human endothelial cells possess insulin receptor mRNAand specific receptor proteins whose physicochemical prop-erties are similar to those of insulin receptors in other tis-sues [60–62]. If the splicing of the IR were regulated byMBNL1 protein, similarly to the skeletal muscle, then itsdisturbance could contribute to the insulin resistance inhuman tissues.
To date, there is no literature on MBNL-regulated splic-ing of insulin receptor mRNA in epidermal or adnexalcells. In fact, these tissues provided unique results concern-ing the MBNL1 protein distribution in the nucleus and itsco-localization with CUG/CCUG expanded repeat foci,showing a low rate of sequestration of the protein in thecells while intranuclear MBNL1 signals were present inthe majority of epidermal and adnexal cells. Nevertheless,age-dependent hyperhidrosis was reported in 20–30% ofDM2 patients and early-onset male frontal bolding wasobserved in approximately 20% of German and 50% ofAmerican men aged 21–34 years [63]. Mueller et al. [64]hypothesize that an association between myotonic dystro-phy and pilomatricomas (as well as other tumours reportedin DM patients) involves up-regulation of beta-catenin,possibly via the actions of CUGBP and MBNL1 proteins.
5. Conclusions
The present results show that the MBNL1 protein isexpressed and more or less sequestered into the CCUGexp
nuclear foci also in analyzed non-muscle tissues of DM2patients. Since the process of sequestration of MBNL1 inskeletal muscles is involved in the pathogenesis of DM1/DM2, the sequestration of the protein in soft and other tis-sues may represent a potential source of pathology andcontribute to the pathological phenotype in DM1/DM2patients.
The degree of ZNF9 RNA expression and MBNL1 co-localization differs among individual tissues. The level ofMBNL1 protein expression has been found to be relativelyhigh in all tissues. On the other hand, the level of theCCUGexp transcript differs. In the skeletal muscle, soft tis-sues and sweat glands, more than 50% of the cells expressthe CCUGexp transcript of ZNF9 protein, while a lowerpercentage of epidermal and hair sheath cells express this
Please cite this article in press as: Lukas Z et al., Sequestration of MBNL1 in(2012), http://dx.doi.org/10.1016/j.nmd.2012.03.004
transcript. Therefore, it seems that different tissues showdifferent levels of MBNL1 sequestration in DM1/2patients. However, Ho et al. [65] showed that formationof RNA foci and disruption of MBNL1-regulated splicingare separable events. Recent reports also suggest that theDM2 phenotype may not depend solely on the expressionof toxic mutant CCUGexp transcripts, but may also bedue to alterations of ZNF9 expression [41–43]. Chenet al. [66] demonstrated in animal models that haploinsuf-ficiency of ZNF9 contributes to the DM2 phenotype.Therefore, other factors contributing to the DM1/DM2pathogenesis must also be taken into consideration.
Acknowledgements
This work was supported by the grants NS/9877-4/2008of the Ministry of Health of CR, LD12039 of the Ministryof Education, IAA500040802 of the Grant Agency of theAS CR and the P302/10/1022 and P302/12/G157 grantsof the Grant Agency of CR.
Monoclonal antibody MB1a was supplied by ProfessorGlenn Morris, MDA Monoclonal antibody resource,Wolfson CIND, RJAH Orthopaedic Hospital, Oswestry,UK.
Appendix A. Supplementary data
Supplementary data associated with this article can befound, in the online version, at http://dx.doi.org/10.1016/j.nmd.2012.03.004.
References
[1] Taneja KL, McCurrach M, Schalling M, Housman D, Singer RH.Foci of trinucleotide repeat transcripts in nuclei of myotonicdystrophy cells and tissues. J Cell Biol 1995;128:995–1002.
[2] Davis BM, McCurrach ME, Taneja KL, Singer RH, Housman DE.Expansion of a CUG trinucleotide repeat in the 30 untranslated regionof myotonic dystrophy protein kinase transcripts results in nuclearretention of transcripts. Proc Natl Acad Sci USA 1997;94:7388–93.
[3] Miller JW, Urbinati CR, Teng-Umnuay P, et al. Recruitment ofhuman muscleblind proteins to (CUG)n expansions associated withmyotonic dystrophy. EMBO J 2000;19:4439–48.
[4] Liquori CL, Ricker K, Moseley ML, et al. Myotonic dystrophy type 2caused by a CCTG expansion in intron 1 of ZNF9. Science2001;293:864–7.
[5] Fardaei M, Rogers MT, Thorpe HM, et al. Three proteins MBNL,MBLL and MBXL, co-localize in vivo with nuclear foci of expanded-repeat transcripts in DM1 and DM2 cells. Hum Mol Genet2002;11:805–14.
[6] Pascual M, Vicente M, Monferrer L, Artero R. The muscleblindfamily of proteins: an emerging class of regulators of developmentallyprogrammed alternative splicing. Differentiation 2006;74:65–80.
[7] Timchenko NA, Welm AL, Lu X, Timchenko LT. CUG repeatbinding protein (CUGBP1) interacts with the 50 region of C/EBPbetamRNA and regulates translation of C/EBPbeta isoforms. NAR1999;27:4517–25.
[8] Ho TH, Charlet-B N, Poulos MG, Singh G, Swanson MS, CooperTA. Muscleblind proteins regulate alternative splicing. EMBO J2004;23:3103–12.
tissues of patients with myotonic dystrophy type 2, Neuromuscul Disord

12 Z. Lukas et al. / Neuromuscular Disorders xxx (2012) xxx–xxx
ARTICLE IN PRESS
[9] Osborne RJ, Thornton CA. RNA-dominant diseases. Hum MolGenet 2006;15:R162–9.
[10] Lin X, Miller JW, Mankodi A, et al. Failure of MBNL1-dependentpost-natal splicing transitions in myotonic dystrophy. Hum MolGenet 2006;15:2087–97.
[11] Lee JE, Cooper TA. Pathogenic mechanisms of myotonic dystrophy.Biochem Soc Trans 2009;37:1281–6.
[12] Botta A, Vallo L, Rinaldi F, et al. Gene expression analysis inmyotonic dystrophy: indications for a common molecular pathogenicpathway in DM1 and DM2. Gene Expr 2007;13:339–51.
[13] Charlet-B N, Savkur RS, Singh G, Philips AV, Grice EA, Cooper TA.Loss of the muscle-specific chloride channel in type 1 myotonic dystrophydue to misregulated alternative splicing. Mol Cell 2002;10(1):45–53.
[14] Osborne RJ, Lin X, Welle S, et al. Transcriptional and post-transcriptional impact of toxic RNA im myotonic dystrophy. HumMol Genet 2009;18:1471–81.
[15] Savkur RS, Phillips AV, Cooper TA. Aberrant regulation of insulinreceptor alternative splicing is associated with insulin resistance inmyotonic dystrophy. Nat Genet 2001;29:40–7.
[16] Savkur RS, Philips AV, Cooper TA, et al. Insulin receptor splicingalteration in myotonic dystrophy type 2. Am J Hum Genet2004;74:1309–13.
[17] Cardani R, Baldassa S, Botta A, et al. Ribonuclear inclusions andMBNL1 nuclear sequesteration do not affect myovlast differentiationbut alter gene splicing in myotonic dystrophy type 2. NeuromusculDisord 2009;19:335–43.
[18] Warf MB, Nakamori M, Matthys CM, et al. Pentamidine reverses thesplicing defects associated with myotonic dystrophy. Proc Natl AcadSci USA 2009;106:18551–6.
[19] Holt I, Mittal S, Furling D, Butler-Browne GS, Brook JD, MorrisGE. Effective mRNA in myotonic dystrophy accumulates at theperiphery of nuclear splicing speckles. Genes Cells 2007;12:1035–48.
[20] Perdoni K, Malatesta M, Cardani R, et al. RNA/MBNL1-comtaitingfoci in myoblast nuclei from patients affected by myotonic dystrophytype 2: an immunocytochemical study. Eur J Histochem 2009;53:151–8.
[21] Sarkar PS, Han J, Reddy S. In situ hybridization analysis of DmpkmRNA in adult mouse tissues. Neuromuscul Disord 2004;14:497–506.
[22] Winchester CL, Ferrieer RK, Sermoni A, Clark BJ, Johnson KJ.Characterization of the expression of DMPK and SIX5 in the humaneye and implications for pathogenesis in myotonic dystrophy. HumMol Genet 1998;8:481–92.
[23] Mankodi A, Urbinati CR, Yuan QP, et al. Muscleblind localizes tonuclear foci of aberrant RNA in myotonic dystrophy types 1 and 2.Hum Mol Genet 2001;10:2165–70.
[24] Jiang H, Mankodi A, Swanson MS, et al. Myotonic dystrophy type 1is associated with nuclear foci of mutant RNA, sequestration ofmuscleblind proteins and deregulated alternative splicing in neurons.Hum Mol Genet 2004;13:3079–88.
[25] Mankodi A, Lin X, Blaxall BC, Swanson MS, Thhornton CA.Nuclear RNA foci in the heart in myotonic dystrophy. Circ Res2005;97:1152–5.
[26] Wheeler TM, Krym MC, Thornton CA. Ribonuclear foci at theneuromuscular junction in myotonic dystrophy type 1. NeuromusculDisord 2007;17:242–7.
[27] Cardani R, Mancinelli E, Saino G, Bonavina L, Meola G. A putativerole of ribonuclear inclusions and MBNL1 in the impairment ofgallbladder smooth muscle contractility with cholelithiasis in myo-tonic dystrophy type 1. Neuromuscul Disord 2008;18:634–40.
[28] Bonifazi E, Gullotta F, Vallo L, et al. Use of RNA fluorescence in situhybridization in the prenatal molecular diagnosis of myotonicdystrophy type 1. Clin Chem 2006;52:319–22.
[29] Mankodi A, Teng-Umnuay P, Krym M, Henderson D, Swanson M,Thornton CA. Ribonuclear inclusions in skeletal muscle in myotonicdystrophy types 1 and 2. Ann Neurol 2003;54:760–8.
[30] Lucchiari S, Pagliarani S, Corti S, et al. Colocalization of ribonuclearinclusions with muscle blind like-proteins in a family with myotonicdystrophy type 2 associated with a short CCTG expansion. J NeurolSci 2008;275:159–63.
Please cite this article in press as: Lukas Z et al., Sequestration of MBNL1 in(2012), http://dx.doi.org/10.1016/j.nmd.2012.03.004
[31] Dubowitz V, Sewry CA. Muscle biopsy. A practical approach. 3rded. London: Elsevier Saunders; 2007.
[32] Warner JP, Barron LH, Goudie D, et al. A general method for thedetection of large CAG repeat expansions by fluorescent PCR. J MedGenet 1996;33(12):1022–6.
[33] Falk M, Vojtıskova M, Lukas Z, Kroupova I, Froster U. Simpleprocedure for automatic detection of unstable alleles in the myotonicdystrophy and Huntington’s disease loci. Genet Test 2006;10:85–97.
[34] Holt I, Jacquemin V, Fardaei M, et al. Muscleblind-like proteins:similarities and differences in normal and myotonic dystrophy muscle.Am J Pathol 2009;174:216–27.
[35] Kozubek M, Kozubek S, Lukasova E, et al. High-resolution cytometry ofFISH dots in interphase cell nuclei. Cytometry 1999;36:279–93.
[36] Kozubek M, Kozubek S, Lukasova E, et al. Combined confocal andwide-field high resolution cytometry of fluorescent in situ hybridiza-tion-stained cells. Cytometry 2001;45:1–12.
[37] Vihola A, Bassez G, Meola G, et al. Histopathological differences ofmyotonic dystrophy type 1 (DM1) and PROMM/DM2. Neurology2003;60:1854–7.
[38] Day JW, Ranum LP. RNA pathogenesis of the myotonic dystrophies.Neuromuscul Disord 2005;15:5–16.
[39] Lukas Z, Kroupova I, Bednarık J, et al. The muscle biopsy inmyotonic dystrophy in the era of molecular genetics (article in Czech).Cesk Slov Neurol N 2007;70:395–401.
[40] Harper PS. Myotonic dystrophy. 3rd ed. London: W.B. Saunders; 2004.[41] Salisbury E, Schloser B, Schneider-Gold C, et al. Expression of RNA
CCUG repeats dysregulates translation and degradation of proteinsin myotonic dystrophy 2 patients. Am J Pathol 2009;175:748–62.
[42] Huichalaf C, Schoser B, Schneider-Gold C, Jin B, Sarkar P,Timchenko LT. Reduction of the rate of protein translation inpatients with myotonic dystrophy 2. J Neurosci 2009;29:9042–9.
[43] Raheem O, Olufemi SE, Bachinski LL, et al. Mutant (CCTG)n
expansion causes abnormal expression of zinc finger protein 9 (ZNF9)in myotonic dystrophy type 2. Am J Pathol 2010;177:3025–36.
[44] Hartl P, Gottesfeld J, Forbes DJ. Mitotic repression of transcriptionin vitro. J Cell Biol 1993;120:613–24.
[45] Frasca F, Pandini G, Scalia P, et al. Insulin receptor isoform A, anewly recognized, high-affinity insulin-like growth factor II receptorin fetal and cancer cells. Mol Cell Biol 1999;19:3278–88.
[46] Sesti G, Marini MA, Tullio AN, et al. Altered expression of the twonaturally occurring human insulin receptor variants in isolatedadipocytes of non-insulin-dependent diabetes mellitus patients. Bio-chem Biophys Res Commun 1991;181:1419–24.
[47] Moxley RT, Kingston WJ, Minaker KL, Corbett AJ, Rowe JW.Insulin resistance and regulation of serum amino acid levels inmyotonic dystrophy. Clin Sci (Lond) 1986;71:429–36.
[48] Morrone A, Pegoraro E, Angellini C, Zammarchi E, Marconi G,Hoffman EP. RNA metabolism in myotonic dystrophy: patientmuscle shows decreases insulin receptor RNA and protein consistentwith abnormal insulin resistance. J Clin Invest 1997;99:1691–8.
[49] Dansithong W, Paul S, Comai L, Reddy S. MBNL1 is the primarydeterminant of focus formation and aberrant insulin receptor splicingin DM1. J Biol Chem 2005;280:5773–80.
[50] Guiraud-Dogan C, Huguet A, Gomes-Pereira M, et al. DM1 CTGexpansions affect insulin receptor isoforms expression in varioustissues of transgenic mice. Biochim Biophys Acta 2007;1772:1183–91.
[51] Sen S, Talukdar I, Liu Y, Tam J, Reddy S, Webster NJG.Muscleblind-like 1 (Mbnl1) promote insulin receptor exon 11inclusion via binding to a downstream evolutionarily conserved intronic enhancer. J Biol Chem 2010;285(33):25426–37.
[52] Sugimoto K, Marakawa Y, Zhang X, Xu G, Sima AA. Insulinreceptor in rat peripheral nerve: its localization and alternativelyspliced isoforms. Diabetes Metab Res Rev 2000;16(5):354–63.
[53] Panayiotopoulos CP, Scarpalezos S. Dystrophia myotonica. Peripheralnerve involvement and pathogenetic implications. J Neurol Sci 1976;27:1–16.
[54] Borenstein S, Noel P, Jacquy J, Flamentdurand J. Myotonicdystrophy with nerve hypertrophy. Report of a case with electro-
tissues of patients with myotonic dystrophy type 2, Neuromuscul Disord

Z. Lukas et al. / Neuromuscular Disorders xxx (2012) xxx–xxx 13
ARTICLE IN PRESS
physiological and ultrastructural study of the sural nerve. J NeurolSci 1977;34(1):87–99.
[55] Schroder JM, Himmelmann F. Fine structural evaluation of alteredSchmidt–Laterman incisures in human sural nerve biopsie. ActaNeuropathol 1992;83:120–33.
[56] Kurt S, Karaer H, Kaplan Y, et al. Combination of myotonicdystrophy and hereditary motor and sensory neuropathy. J NeurolSci 2010;288:197–9.
[57] Gantelet J, Kraftsik R, Delaloye S, Gourdon G, Kuntzer T, Barakat-Walter I. The expansion of 300 CTG repeats in myotonic dystrophytransgenic mice does not induce sensory or motor neuropathy. ActaNeuropathol 2007;114:175–85.
[58] Vicente M, Monferrer L, Poulos MG, et al. Muscleblind isoforms arefunctionally distinct and regulate alpha-actinin splicing. Differentia-tion 2007;7:427–40.
[59] Kimura T, Nakamori M, Lueck JD, et al. Altered mRNA splicing ofthe skeletal muscle ryanodine receptor and sarcoplasmic/endoplasmicreticulum Ca2+-ATPase in myotonic dystrophy type 1. Hum MolGenet 2005;14:2189–200.
[60] Sugimoto K, Marakawa Y, Zhang X, Xu G, Sima AA. Insulinreceptor in rat peripheral nerve: its localization and alternativelyspliced isoforms. Diabetes Metab Res Rev 2000;16:354–63.
Please cite this article in press as: Lukas Z et al., Sequestration of MBNL1 in(2012), http://dx.doi.org/10.1016/j.nmd.2012.03.004
[61] Cerosimo E, DeFronzo RA. Insulin resistance and endothelialdysfunction: the road map to cardiovascular diseases. DiabetesMetab Res Rev 2006;22:423–36.
[62] Finol H, Torres S, Rabucha A, Saenz H. Intramuscular capillaryabnormalities in a case of myotonic dystrophy (Steinert’s disease).Acta Cient Venez 1992;43:284–9.
[63] Day JW, Ricker K, Jacobsen JF, et al. Myotonic dystrophy type 2:molecular, diagnostic and clinical spectrum. Neurology 2003;60:657–64.
[64] Mueller CM, Hilbert JE, Martens W, Thornton CA, Moxley RT,Greene MH. Hypothesis: neoplasms in myotonic dystrophy. CancerCauses Control 2009;20(10):2009–20.
[65] Ho TH, Savkur RS, Poulos MG, Mancini MA, Swanson MS, CooperTA. Colocalization of muscleblind with RNA foci is separable frommis-regulation of alternative splicing in myotonic dystrophy. J CellSci 2005;118:2923–33.
[66] Chen W, Wang Y, Abe Y, Cheney L, Udd B, Li YP. Haploinsuffi-ciency for ZNF9 in ZNF9+/� mice is associated with multiorganabnormalities resembling myotonic dystrophy. J Mol Biol 2007;368:8–17.
tissues of patients with myotonic dystrophy type 2, Neuromuscul Disord
Related Documents











