INTRODUCTION The symptoms shown by people with dystrophia myotonica or myotonic dystrophy include myotonia and progressive weakness, and atrophy of skeletal muscle 228 Physiotherapy Research International, 7(4) 228–238, 2002 © Whurr Publishers Ltd A study of the facilitation of respiration in myotonic dystrophy JENNIFER NITZ Department of Physiotherapy, School of Health and Rehabilitation Sciences, The University of Queensland, Australia BRANDON BURKE Toowoomba General Hospital, Toowoomba, Australia ABSTRACT Background and Purpose. Dystrophia myotonica or myotonic dystrophy is a progressive neuromuscular disorder in which patients demonstrate an irregular respiratory pattern and are particularly subject to cardiopulmonary compromise. The aim of the present study was to investigate the effects of both proprioceptive neuromuscular facili- tation (PNF) and staged basal expansion (SBE) breathing exercises in subjects with myotonic dystrophy in two different positions: high support sitting and left side-lying. Method. A randomized, double-blind study design was used. Seven non-congenital myotonic dystrophy subjects took part in the study. Six ‘treatment’ levels were applied to each subject: resting in high support sitting; resting in left side-lying; PNF of deep breathing in high support sitting; PNF of deep breathing in left side-lying; SBE in high support sitting and SBE in left side-lying. The outcome measures employed were arterial oxygen saturation (SpO 2 ) and heart rate, as measured by oximetry and thoraco-abdominal motion (TAM), and respiratory rate, as measured by a pneumograph. Results. The PNF technique was found to be the main contributor to improvement in SpO 2 for subjects with myotonic dystrophy, where a 2.2% increase was found in the high support sitting position and a 2.6% increase was found in the left side-lying position. There was an increase of between 377% and 556% in TAM during application of both treatment techniques, in either the high support sitting or left side-lying positions. Respiratory rate declined between 15% and 30% immediately after treatment application and heart rate dropped slightly by between 0.2% and 4.1%. Conclusion. The present study provides objective evidence that application of these respiratory physiotherapy interventions elicits an improvement in respiratory function in subjects with myotonic dystrophy. Further research into the physio- logical effects of these techniques could explore the mechanisms responsible for improvement in respiratory indices. Key words: myotonic dystrophy, proprioceptive neuromuscular facilitation (PNF), respi- ratory physiotherapy, staged basal expansion (SBE)

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
INTRODUCTION
The symptoms shown by people with
dystrophia myotonica or myotonicdystrophy include myotonia and progressiveweakness, and atrophy of skeletal muscle
228 Physiotherapy Research International, 7(4) 228–238, 2002 © Whurr Publishers Ltd
A study of the facilitation of respirationin myotonic dystrophy
JENNIFER NITZ Department of Physiotherapy, School of Health and RehabilitationSciences, The University of Queensland, Australia
BRANDON BURKE Toowoomba General Hospital, Toowoomba, Australia
ABSTRACT Background and Purpose. Dystrophia myotonica or myotonic dystrophy is aprogressive neuromuscular disorder in which patients demonstrate an irregular respiratorypattern and are particularly subject to cardiopulmonary compromise. The aim of thepresent study was to investigate the effects of both proprioceptive neuromuscular facili-tation (PNF) and staged basal expansion (SBE) breathing exercises in subjects withmyotonic dystrophy in two different positions: high support sitting and left side-lying.Method. A randomized, double-blind study design was used. Seven non-congenitalmyotonic dystrophy subjects took part in the study. Six ‘treatment’ levels were applied toeach subject: resting in high support sitting; resting in left side-lying; PNF of deepbreathing in high support sitting; PNF of deep breathing in left side-lying; SBE in highsupport sitting and SBE in left side-lying. The outcome measures employed were arterialoxygen saturation (SpO
2) and heart rate, as measured by oximetry and thoraco-abdominal
motion (TAM), and respiratory rate, as measured by a pneumograph. Results. The PNFtechnique was found to be the main contributor to improvement in SpO
2for subjects with
myotonic dystrophy, where a 2.2% increase was found in the high support sitting positionand a 2.6% increase was found in the left side-lying position. There was an increase ofbetween 377% and 556% in TAM during application of both treatment techniques, in eitherthe high support sitting or left side-lying positions. Respiratory rate declined between 15%and 30% immediately after treatment application and heart rate dropped slightly bybetween 0.2% and 4.1%. Conclusion. The present study provides objective evidence thatapplication of these respiratory physiotherapy interventions elicits an improvement inrespiratory function in subjects with myotonic dystrophy. Further research into the physio-logical effects of these techniques could explore the mechanisms responsible forimprovement in respiratory indices.
Key words: myotonic dystrophy, proprioceptive neuromuscular facilitation (PNF), respi-ratory physiotherapy, staged basal expansion (SBE)
PRI 7(4)_crc 21/11/02 2:15 PM Page 228
Respiratory facilitation in myotonic dystrophy 229
involving the diaphragm, facial and limbmuscles (Harper, 1989). Myotonia is thepersistence of muscular contraction presentafter the cessation of applied mechanicalstimulus or voluntary contraction (Kimura,1983). Myotonic dystrophy affects skeletal,smooth and cardiac muscle function(Harper, 1989). In the adult onset form,pneumonia and cardiac arrhythmias accountfor the largest cause of death in myotonicdystrophy (de Die-Smulders et al., 1998).Patients with myotonic dystrophy also havean unusually high incidence of adversereactions to anaesthesia, which includeprofound respiratory depression and death(Mathieu et al., 1997). Spontaneous periodicdeep breaths that stimulate surfactantrelease are lost (Schmidt-Nowara andAltman, 1991). Progressive respiratorymuscle weakness leads to impairment ofairway clearance, inadequate ventilation andrespiratory failure (Berry et al., 1996).Restrictive lung disease, without airwayobstruction has been reported frequently inpeople with myotonic dystrophy (Jammes etal., 1985; Bogaard et al., 1992; Johnson etal., 1995). There is a high incidence ofdecreased forced vital capacity, total lungcapacity, maximum static respiratorypressures and alveolar hypoventilation(Bogaard et al., 1992; Johnson et al., 1995).Factors thought to contribute to therestrictive presentation include limited chestexpansion secondary to myotonia, respi-ratory muscle atrophy and weakness (Béginet al., 1982; Jammes et al., 1985; Mathieu etal., 1997) and reduced inspiratory muscleforce (Bogaard et al., 1992). Irregularities ofthe resting ventilation pattern have beenreported to include shallower tidal volume,elevated respiratory rate, smaller restingminute volume and prolonged apnoeicperiods (Caroll et al., 1977; Serisier et al.,1980; Jammes et al., 1985; Bogaard et al.,1992). Consequently, after surgery situa-tions arise when individuals with myotonic
dystrophy would benefit from assistance toimprove air entry to enhance lung venti-lation. Conditions that often require surgicalintervention and that present in people withmyotonic dystrophy include gynaecologicaldysfunction, volvulus and gallstones(Harper, 1989). Owing to the incidence ofsurgical interventions in people withmyotonic dystrophy, and gastrointestinaland uterine surgery in particular, physiother-apists are often called upon to instigatepreventive treatment interventions or to treatpost-operative cardiopulmonary complica-tions in patients with myotonic dystrophy(Nitz, 1999). These complications mayinclude acute respiratory failure, bronchop-neumonia, atelectasis and retainedsecretions.
A number of physiotherapy techniquesmay be employed to augment air entry post-operatively in an individual with respiratorycomplications. These include breathing andpositioning techniques. Staged basalexpansion (SBE) is one such technique,involving verbal and tactile facilitation(Webber, 1988). It is based on the obser-vation that by inflating slowly over severalinspirations, collapsed alveoli expandprogressively (Menkes and Traystman,1977). Proprioceptive neuromuscular facili-tation (PNF) is another acute respiratoryphysiotherapy treatment option. For respi-ration, it involves the application of stretchfacilitation to the chest wall at endexpiration to elicit a reflex enhanced respi-ratory muscle contraction (Adler et al.,1993). This stretch may assist initiation ofinspiration, increase volume and chest wallrange of motion and strengthen respiratorymuscles (Voss et al., 1985; Adler et al.,1993). Mechanical stimulation of the chestwall proprioceptors during PNF of deepbreathing may enhance the activity ofunderlying intercostal muscles. It isconsidered that the stretch to the intercostalmuscles during PNF of deep breathing in
PRI 7(4)_crc 21/11/02 2:15 PM Page 229

230 Nitz and Burke
myotonic dystrophy may serve to provide amore normal afferent input in the diseasedmuscle and possibly act concomitantly viahomogenous facilitation and reciprocalinhibition.
Ventilation and perfusion distributionthroughout the lung is influenced by gravity(West, 1977) and so is determined by bodypositioning. The negative influences of thesupine position have been well documentedand include a reduction in the functionalresidual capacity and decreased arterialoxygenation (Dean and Ross, 1992).Upright positioning is preferred over therecumbent position to enhance lungvolumes and flow rates (Dean, 1985). Druzand Sharp (1981) and De Troyer (1993)found that greater excursion of the lowerribcage was facilitated in the upright posturedue to a reduced compliance in theabdominal wall and improved tonic activityin abdominal muscles. Although not statisti-cally signif icant, Calabrese et al. (2000)reported more frequent breathing patternanomalies in the supine position comparedto the seated position in nine subjects withmyotonic dystrophy.
The side-lying position is useful inoptimizing pulmonary function for patientswith unilateral lung pathology (Remolina etal., 1981). In this position, the dependentlung receives greater ventilation andperfusion and an increased arterial partialpressure of oxygen (Clauss et al., 1968;Martin et al., 1976; Amis et al., 1984a). Intheir study on ventilation per unit alveolarvolume, Amis et al. (1984a) showed that thesuperior lung achieved more air entry thanthe dependent lung, which in the case ofatelectasis or unilateral lung pathology,might be the desired effect of treatment.
As people with myotonic dystrophy areat high risk of developing respiratorydysfunction at any stage in the progressionof the condition, and especially after
surgery, determination of the most appro-priate treatment technique for improving airentry and oxygen saturation is important forphysiotherapy practice. The purpose of thepresent study was to investigate the effectsof both PNF of deep breathing and SBE insubjects with myotonic dystrophy in twodifferent positions: high support sitting, aposition equivalent to upright positioning,and left side-lying. The high support sittingposition entailed subjects lying on a couchwith the backrest at an angle of 75˚ from thehorizontal. Subjects rested the head on apillow and a pillow was placed under theknees to slightly flex the hips and knees toallow relaxation of abdominal andhamstring muscle groups. A pillow undereach elbow supported the weight of theupper limbs. It was hypothesized that PNFof deep breathing and SBE would increasearterial oxygen saturation (SpO
2) and
thoraco-abdominal motion (TAM), decreaserespiratory rate and cause no change inheart rate compared to resting measure-ments in high support sitting and leftside-lying in the subject group.
METHOD
Subjects
A randomized double-blind study designwas used.
Seven non-congenital subjects withmyotonic dystrophy, whose characteristicsare presented in Table 1, participated in thestudy. The diagnosis of myotonic dystrophyhad been conf irmed by DNA analysis.Subjects were excluded on the basis of:
• History of long-term steroid use.• Thoracic/spinal abnormality.• Any respiratory condition that would
influence chest wall mechanics.• Long-term lung medications.• Known cardiac disease.
PRI 7(4)_crc 21/11/02 2:15 PM Page 230

Respiratory facilitation in myotonic dystrophy 231
• Recent myocardial infarction or otherischaemic disease.
• Recent chest infection.• Inability to comply with instructions.
No subject had previous experience withphysiotherapy respiratory techniques beforethe experiment and the subjects thereforehad no knowledge of its effects.
Procedure
Informed consent was gained from subjectsbefore participation in the study and thestudy was approved by the MedicalResearch Ethics Committees of TheUniversity of Queensland and GreenslopesPrivate Hospital. A randomized, double-blind study design was used for the sixtreatment levels:
• Resting in high support sitting.• Resting in left side-lying.• PNF of deep breathing in high support
sitting.• PNF of deep breathing in left side-lying.• SBE in high support sitting.• SBE in left side-lying.
Subjects acted as their own controls in arepeated-measures study design. Two inves-tigators conducted the study. Anexperienced physiotherapist performed thetechniques and randomized the order of test
conditions. A second investigator, who wasblinded to the position and order oftreatment by being separated from thetreatment area by a screen, prepared theequipment and recorded the measurements:SpO
2, heart rate, TAM and respiratory rate.
PNF was applied in high support sittingby the physiotherapist placing her hands onthe lateral aspect of the chest wall, with thebases of the palms near the apices of thelower ribs and with the fingers in an upwardand lateral direction. The physiotherapistthen instructed the subject to exhalecompletely and applied downward andmedial pressure to quickly stretch the inter-costal muscles. Subjects were theninstructed to breathe in. As subjectsinspired, the physiotherapist applied suffi-cient resistance through her hands to chestexpansion not to overcome the movementcapability of the subject, but so as toencourage range of motion response (Vosset al., 1985). The SBE technique involvedthe physiotherapist placing her hands in thesame location as for PNF and verballyencouraging the subject to take threesuccessively deeper breaths, inflating thechest under her hands so that a staged highvolume was achieved. In left side-lying thephysiotherapist applied PNF by placing herhands obliquely with the fingers followingthe line of the ribs on the lateral aspect ofthe lower ribcage on the right side. Pressurewas applied diagonally in a caudal and
TABLE 1: Subject characteristics
Number Age (years) Gender Mobility Sleep apnoea
1 38 M Independent No2 64 M Independent Yes3 61 F Electric wheelchair No4 45 M Independent Yes5 56 M Cane No6 53 F Four-point stick No7 40 M Independent Yes (CPAP)
PRI 7(4)_crc 21/11/02 2:15 PM Page 231

232 Nitz and Burke
medial direction with the plinth resisting themotion of the other side of the chest (Adleret al., 1993). SBE used a similar handplacement. Sleep apnoeic disturbances, aswell as the use of continuous positiveairways pressure (CPAP) for managing thisdisability, and any history of lung diseasewere recorded.
The protocol commenced with thecollection of five minutes’ baseline restingdata with subjects in either high supportsitting or left side-lying positions breathingat a self-selected volume and rate. The firsttreatment intervention (PNF or SBE) wasapplied for three breaths, three times, with ashort period between sets to prevent hyper-ventilation (so that a total of nine treatmentbreaths was recorded). The treatment wasapplied over a period of 60–90 s. Post-treatment recordings of the measuredvariables continued for approximately fiveminutes, as subjects breathed normally.Preliminary investigations had indicatedthat measurements returned to restingbaseline within five minutes of treatment orposition change. Therefore it wasconsidered suitable to wait for five minutesbetween treatment applications and for fiveminutes after position shift.
The second treatment intervention (PNFor SBE) was then immediately applied forthree sets of three breaths, followed by fiveminutes’ normal breathing. Subjects thenmoved to the second test position and thesame protocol followed, starting with thebaseline measurement that was taken afterfive minutes’ rest.
TAM and respiratory rate measurementswere recorded continually during restingbaseline data collection and throughouttreatment application. SpO
2and heart rate
were recorded every 30 s.
Measurements
SpO2
was monitored by a pulse oximeter
(Model 512, Novametrix Medical SystemsInc., CT, USA) placed on subjects’ rightindex f inger. Heart rate was monitoredconcomitantly by the pulse oximeter toassess when subjects had returned to restingbaseline between treatment applications.
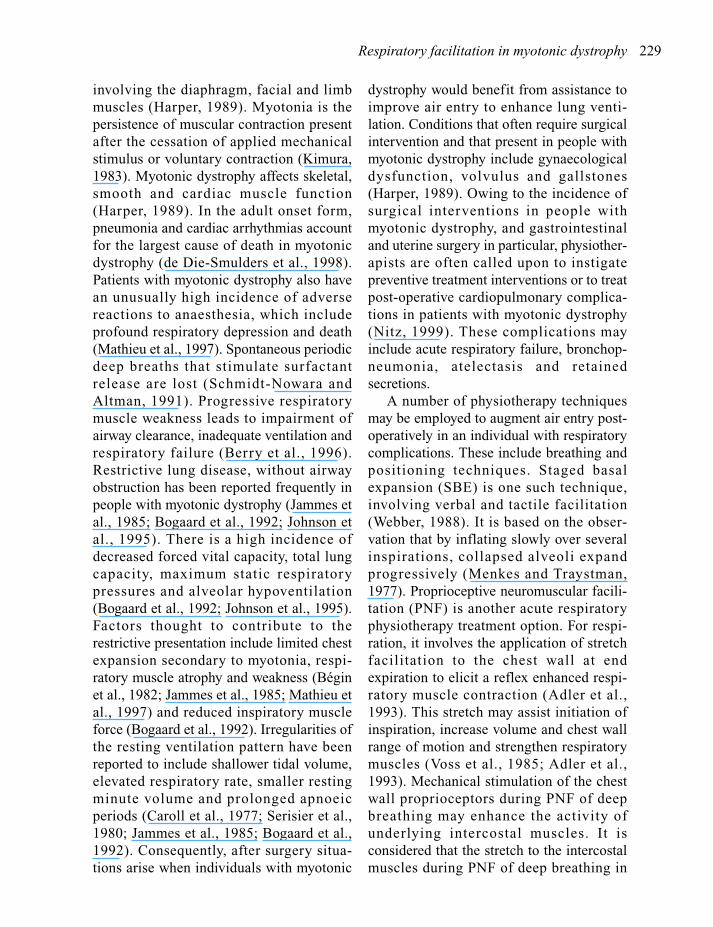
TAM and respiratory rate were measuredwith a pneumograph. A modified pressurebiofeedback unit (PBU) (Stabilizer™,Chattanooga Australia Pty) has previouslybeen used and shown to be reliable as apneumograph to monitor respiratory rateand ribcage movement (Hodges et al., 1997;McGuiness et al., 1997). A PBU wasinflated to 20 mmHg pressure and placedanteriorly on the lower chest wall at the levelof the xiphisternum and held in place by aninextensible strap. It was checked regularlyto ensure a minimum pressure of 20 mmHgwas maintained at all times. The pneumo-graph was attached to an X–Y plotter (YEWType 3033 X–Y recorder. Yokogawa ElectricWorks Ltd., Tokyo, Japan), which recordedalterations in pressure during respiration,giving a continuous indication of TAM andrespiratory rate. The TAM was displayedgraphically where inspiration resulted in anupward movement of the trace (Figure 1).The resting breathing pattern was acquiredby self-selected breathing rate for f ivecontinuous minutes and analysed withrespect to inspiratory TAM and respiratoryrate.
Data management
The TAM and respiratory rate traces fromthe X–Y plotter were scanned as input to acomputer (Canon, Model FB 330F) to allowaccurate TAM analysis. The inspiratoryTAM was obtained by connecting the pointat the start of inspiration with the point atthe end of inspiration, for each breath. Thelength of this curve was measured and themean calculated from all baseline measure-ments. The mean inspiratory TAM for the
PRI 7(4)_crc 21/11/02 2:15 PM Page 232
Respiratory facilitation in myotonic dystrophy 233
nine breaths from each treatment conditionwas calculated in the same manner forcomparison to the resting mean. Respiratoryrate was calculated by counting the upwarddisplaced peaks recorded in each 60-speriod.
Because of the small subject numbers,descriptive statistics (mean and standarddeviation (SD)) were calculated for SpO
2,
heart rate and respiratory rate during thefive-minute post-treatment period, and forTAM during treatment application, and foreach treatment position. The effect induced
by treatment and position was determinedby calculating the percentage change foreach measurement.
RESULTS
Three (43%) subjects with myotonicdystrophy reported sleep apnoea, one wasbeing managed during sleep by CPAP (seeTable 1).
There was an increase of between377.9% and 556.2% in TAM induced by thetreatment applications in high support
FIGURE 1: Thoraco-abdominal motion (TAM) trace: (a) at rest; (b) during proprioceptive neuromuscular facil-itation (PNF) application; (c) during staged basal expansion (SBE) in high support sitting.
PRI 7(4)_crc 21/11/02 2:15 PM Page 233
234 Nitz and Burke
sitting and left side-lying. This was reflectedin an increase in SpO
2of 2.2% and 2.6% for
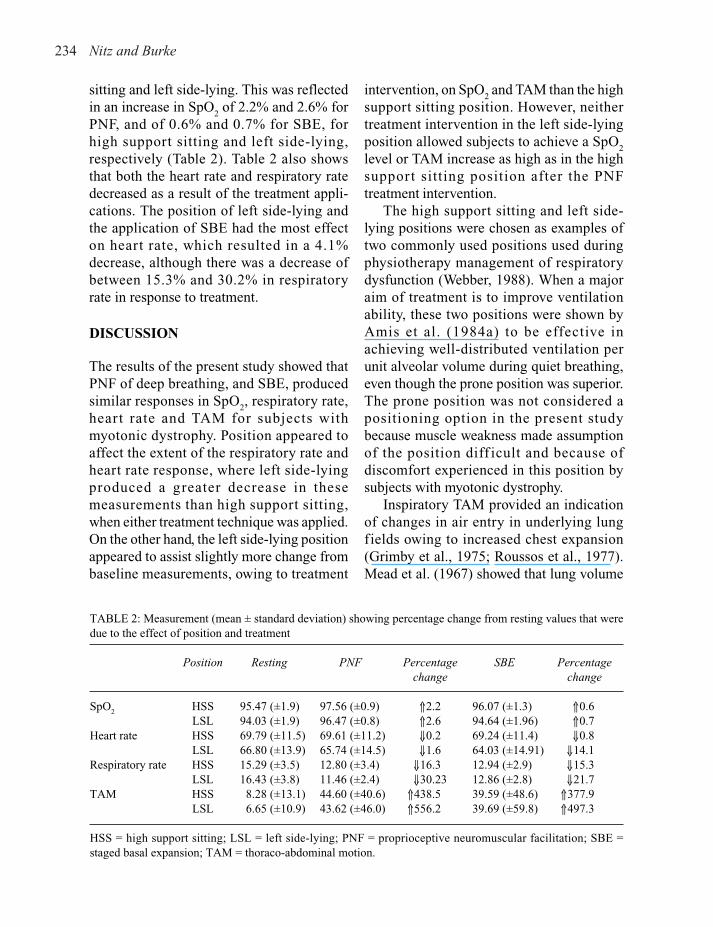
PNF, and of 0.6% and 0.7% for SBE, forhigh support sitting and left side-lying,respectively (Table 2). Table 2 also showsthat both the heart rate and respiratory ratedecreased as a result of the treatment appli-cations. The position of left side-lying andthe application of SBE had the most effecton heart rate, which resulted in a 4.1%decrease, although there was a decrease ofbetween 15.3% and 30.2% in respiratoryrate in response to treatment.
DISCUSSION
The results of the present study showed thatPNF of deep breathing, and SBE, producedsimilar responses in SpO
2, respiratory rate,
heart rate and TAM for subjects withmyotonic dystrophy. Position appeared toaffect the extent of the respiratory rate andheart rate response, where left side-lyingproduced a greater decrease in thesemeasurements than high support sitting,when either treatment technique was applied.On the other hand, the left side-lying positionappeared to assist slightly more change frombaseline measurements, owing to treatment
intervention, on SpO2and TAM than the high
support sitting position. However, neithertreatment intervention in the left side-lyingposition allowed subjects to achieve a SpO
2
level or TAM increase as high as in the highsupport sitting position after the PNFtreatment intervention.
The high support sitting and left side-lying positions were chosen as examples oftwo commonly used positions used duringphysiotherapy management of respiratorydysfunction (Webber, 1988). When a majoraim of treatment is to improve ventilationability, these two positions were shown byAmis et al. (1984a) to be effective inachieving well-distributed ventilation perunit alveolar volume during quiet breathing,even though the prone position was superior.The prone position was not considered apositioning option in the present studybecause muscle weakness made assumptionof the position diff icult and because ofdiscomfort experienced in this position bysubjects with myotonic dystrophy.
Inspiratory TAM provided an indicationof changes in air entry in underlying lungfields owing to increased chest expansion(Grimby et al., 1975; Roussos et al., 1977).Mead et al. (1967) showed that lung volume
TABLE 2: Measurement (mean ± standard deviation) showing percentage change from resting values that weredue to the effect of position and treatment
Position Resting PNF Percentage SBE Percentage change change
SpO2
HSS 95.47 (±1.9) 97.56 (±0.9) ⇑2.2 96.07 (±1.3) ⇑0.6LSL 94.03 (±1.9) 96.47 (±0.8) ⇑2.6 94.64 (±1.96) ⇑0.7
Heart rate HSS 69.79 (±11.5) 69.61 (±11.2) ⇓0.2 69.24 (±11.4) ⇓0.8LSL 66.80 (±13.9) 65.74 (±14.5) ⇓1.6 64.03 (±14.91) ⇓14.1
Respiratory rate HSS 15.29 (±3.5) 12.80 (±3.4) ⇓16.3 12.94 (±2.9) ⇓15.3LSL 16.43 (±3.8) 11.46 (±2.4) ⇓30.23 12.86 (±2.8) ⇓21.7
TAM HSS 8.28 (±13.1) 44.60 (±40.6) ⇑438.5 39.59 (±48.6) ⇑377.9LSL 6.65 (±10.9) 43.62 (±46.0) ⇑556.2 39.69 (±59.8) ⇑497.3
HSS = high support sitting; LSL = left side-lying; PNF = proprioceptive neuromuscular facilitation; SBE =staged basal expansion; TAM = thoraco-abdominal motion.
PRI 7(4)_crc 21/11/02 2:15 PM Page 234

Respiratory facilitation in myotonic dystrophy 235
was proportional to antero-posterior ribcagediameter. The pneumograph was designedto avoid the use of a mouthpiece or mask asthese devices may increase tidal volume anddecrease respiratory rate (Askanazi et al.,1980). Furthermore, patients with a neuro-muscular disease, such as myotonicdystrophy, have diff iculty forming a sealaround mouthpieces because of orofacialmuscle weakness (Harper, 1989). Highresting respiratory rate has been reportedpreviously in subjects with myotonicdystrophy (Caroll et al., 1977; Serisier et al.,1980; Jammes et al., 1985; Bogaard et al.,1992). Thus, it was useful to know ifposition or treatment conditions increasedTAM and lowered respiratory rate toproduce a more efficient ventilation pattern.Interestingly, Amis et al. (1984a) indicatedthat, in normal subjects, the air entry couldbe enhanced by facilitation of greater inspi-ratory muscle activity in any position andthis was demonstrated for the high supportsitting and left side-lying positions in thepresent study of subjects with myotonicdystrophy. The most obvious changeinduced by either treatment was on TAM,thereby concurring with Amis et al. (1984a)that with enhanced motion of the diaphragmand abdomen the dependent part of thelungs is better ventilated. The TAMmeasurements provided a means ofcomparing depth of inspiration occurringduring a facilitated deep breath to restingmeasurements. A signif icant effect wasshown for TAM on treatment applicationwith the left side-lying position showing agreater percentage response than highsupport sitting. Respiratory tidal volume isrelated to chest expansion or TAM, withincreased inspired volumes that, in theabsence of lung pathology, will increase theventilation:perfusion ratio and subsequentincrease in SpO
2(Amis et al., 1984b).
Respiratory drive is decreased by an
increase in SpO2and this would account for
the decrease in respiratory rate aftertreatment application.
There was no effect on heart rate from‘treatment’ application or ‘position’ of thepatient. This f inding supports the use ofthese respiratory treatment techniques forindividuals with myotonic dystrophy. Inspi-ratory holds that are often used to augmentthe PNF and SBE techniques were notevaluated in the present study and should beused with caution considering the potentialcardiac effect in subjects with myotonicdystrophy who have conduction irregular-ities (Nitz, 1999).
The observed changes to SpO2induced
by treatment application were small, but theresponse from PNF was around four timesthat for SBE. This small increase wasbecause at high levels of SpO
2(more than
90%) substantial change in the arterialpartial pressure of oxygen results in only asmall shift in SpO
2as measured by pulse
oximetry (Mengelkoch et al., 1994). Ugaldeet al. (2000) reported a similar increase inSpO
2in subjects with myotonic dystrophy
during pursed-lips breathing and matchedvolume breathing compared to resting tidalbreathing. Redirection of air to basal lungf ields and enhanced inspiratory musclerecruitment were likely to be responsible forthe improvements in the present study,especially for the PNF technique.
The benefits of breathing exercises facil-itated by verbal and tactile stimulation havebeen reported previously (Bethune, 1975;Morran et al., 1983; Jenkins et al., 1988).Slow staged inspiration facilitates alveolarexpansion and stability via collateral venti-lation channels reduced airways resistanceand stimulation of surfactant secretion(Menkes and Traystman, 1977). Excitatorycutaneous afferents stimulated by touch arelikely to have contributed to movementresponse in both treatment conditions as
PRI 7(4)_crc 21/11/02 2:15 PM Page 235
236 Nitz and Burke
stimulation of cutaneous nerves overlyingthe chest wall have been shown to causereflex intercostal muscle contraction(Grimby et al., 1975). Application of astretch to the lateral chest wall just prior toinspiration, increases the gammamotoneuron discharge and alphamotoneuron activity is enhanced (Sears andNewsom Davis, 1968). Because reflexneural interconnections exist between theintercostal muscles and the diaphragm(Downmann, 1955) this may facilitatediaphragmatic contraction (De Troyer andEstenne, 1984). Furthermore, externallyapplied compression to the chest wall mayresult in optimal setting of the resting lengthof respiratory muscles to augment theircontraction. Myotonia has been proposed asa mechanism of respiratory muscledysfunction for patients with myotonicdystrophy (Bégin et al., 1982; Jammes et al.,1985; Rimmer et al., 1993). The myotonicresponse demonstrated by electromyog-raphy (EMG) indicates repeated dischargesof single muscle fibres owing to membraneinstability initiated by voluntary contractionor externally applied mechanical stimuli(Kimura, 1983). Myotonia may hinderrespiratory muscle action by prolonginginspiratory muscle action during expirationand vice versa (Rimmer et al., 1993).Although myotonia has been noted in theintercostal muscles, it does not occur to asignificant degree during quiet breathing(Rimmer et al., 1993). This may be becausemyotonia tends to decrease with repeated,rapid contractions, such as in respiration(Harper, 1989). PNF during deep breathingconstituted both an externally appliedmechanical stimulus concomitant with avoluntary increase in muscle contraction,both of which may be expected to causemyotonia of the chest wall muscles.However, application of a stretch to theintercostal muscles prior to their
contraction, with resistance to movementduring inspiration appeared to diminishmyotonic events since there was an increasein TAM and subsequent increase in SpO
2
that was greater than that for SBE. Tofurther investigate this result, it would bebeneficial to study the effect of PNF anddeep breathing exercises using EMG insubjects with myotonic dystrophy.
Subjects with myotonic dystrophyfrequently suffer sleep-related breathingdisturbances (sleep apnoea); however, thecause of this has not been clearly established(Guilleminault et al., 1978; Cirignotta et al.,1987; Ververs et al., 1996). Three of theseven subjects presented with sleep apnoea.Studies have shown that the most likelyposition for a person to suffer obstructivesleep apnoea is lying supine (Kilkenny andGrenard, 1999). This was one reason thesupine lying position was avoided during thepresent study so situations that couldconfound the responses to the interventionsbeing evaluated were removed.
A major limitation of the present studywas the small number of subjects willingand able to travel to the hospital in order toparticipate in it. More information relatingto the effect of the treatment techniquesmight have been obtained had the interven-tions been repeated on the same day as wellas repeating them on another day.
Further research into the physiologicaleffects of these techniques could explore theproposed mechanisms responsible forimprovement in respiratory indices. Thepresent study has provided some objectiveevidence to support the use of PNF, and to alesser extent SBE, to facilitate deepbreathing and to raise SpO
2in individuals
with myotonic dystrophy. Such animprovement in ventilation is indicated inpeople with myotonic dystrophy during thepost-operative period, when they are atgreater risk of developing respiratory
PRI 7(4)_crc 21/11/02 2:15 PM Page 236

Respiratory facilitation in myotonic dystrophy 237
complications owing to their condition thanunaffected people. The treatment techniqueswould be indicated also in subjects withmyotonic dystrophy with other lungpathologies where ventilation was decreased.This is the first study to provide objectiveevidence that application of facilitatoryrespiratory physiotherapy interventions(PNF and SBE) elicit an improvement inrespiratory function in otherwise healthysubjects with myotonic dystrophy. Furtherstudy of the effect of these treatment appli-cations is indicated in people with myotonicdystrophy both post-operatively and whensuffering other lung pathology.
REFERENCES
Adler SS, Beckers D, Buck M. PNF in Practice: AnIllustrated Guide. Berlin: Springer-Verlag,1993.
Amis TC, Jones HA, Hughes JMB. Effect of postureon inter-regional distribution of pulmonary venti-lation in man. Respiration Physiology 1984a; 56:145–167.
Amis TC, Jones HA, Hughes JMB. Effect of postureon inter-regional distribution of pulmonaryperfusion and VA/Q ratios in man. RespirationPhysiology 1984b; 56: 169–182.
Askanazi J, Silverberg P, Foster RJ, Hijman AI,Milic-Emili J, Kinney JM. Effects of respiratoryapparatus on breathing pattern. Journal of AppliedPhysiology: Respiratory, Environmental andExercise Physiology 1980; 48: 577–580.
Bégin R, Bureau MA, Lupien L, Bernier JP, LemieuxB. Pathogenesis of respiratory insufficiency inmyotonic dystrophy. The mechanical factors.American Review of Respiratory Disease 1982;125: 312–318.
Berry JK, Vitalo CA, Larso JL, Patel M, Kim MJ.Respiratory muscle strength in older adults.Nursing Research 1996; 45: 154–159.
Bethune D. Neurophysiological facilitation of respi-ration in the unconscious adult patient.Physiotherapy Canada 1975; 27: 241–245.
Bogaard JM, van der Meché FGA, Hendriks I,Ververs C. Pulmonary function and restingbreathing pattern in myotonic dystrophy. Lung1992; 170: 143–153.
Calabrese P, Gryspeert N, Auriant I, Fromageot C,
Raphël J-C, Lofaso F et al. Postural breathingpattern changes in patients with myotonicdystrophy. Respiration Physiology 2000; 122:1–13.
Caroll JE, Zwillich CW, Weil JV. Ventilatoryresponse in myotonic dystrophy. Neurology 1977;27: 1125–1128.
Cirignotta F, Mondini S, Zucconi M, Barrot-Cortes E,Sturani C, Schiavina M et al. Sleep-relatedbreathing impairment in myotonic dystrophy.Journal of Neurology 1987; 235: 80–85.
Clauss RH, Scalabrini BY, Ray JF. Effects ofchanging body position upon improved venti-lation–perfusion relationships. Circulation 1968;37 (Suppl. 2): 214–217.
Dean E. Effect of body position on pulmonaryfunction. Physical Therapy 1985; 65: 613–618.
Dean E, Ross J. Discordance between cardiopul-monary physiology and physical therapy: towardsa rational basis for practice. Chest 1992; 101:1694–1698.
De Die-Smulders CEM, Howeler CJ, Thijs C, Miran-dolle JF, Anten HB, Smeets HJM et al. Age andcauses of death in adult-onset myotonicdystrophy. Brain 1998; 121: 1557–1563.
De Troyer A. Mechanical role of the abdominalmuscles in relation to posture. Respiration Physi-ology 1993; 53: 341–353.
De Troyer A, Estenne M. Coordination between ribcage muscles and diaphragm during quietbreathing. Journal of Applied Physiology: Respi-ratory, Environmental and Exercise Physiology1984; 57: 899–906.
Downmann CBB. Skeletal muscle reflexes ofsplancnic and intercostal nerve in acute spinal andcerebrated cats. Journal of Neurophysiology1955; 18: 217–235.
Druz WS, Sharp JT. Activity of respiratory muscles inupright and recumbent humans. Journal ofApplied Physiology 1981; 51: 1552–1561.
Grimby G, Oxhoj H, Bake B. Effects of abdominalbreathing on distribution of ventilation inobstructive lung disease. Clinical Science andMolecular Medicine 1975; 48: 193–199.
Guilleminault C, Cummiskey J, Motta J, Lynne-Davies P. Respiratory and haemodynamic studyduring wakefulness and sleep in myotonicdystrophy. Sleep 1978; 1: 19–31.
Harper PS. Myotonic Dystrophy. London: WBSaunders, 1989.
Hodges PW, Gandevia SC, Richhardson CA.Contractions of specific abdominal muscles inpostural tasks are affected by respiratory
PRI 7(4)_crc 21/11/02 2:15 PM Page 237
238 Nitz and Burke
manoeuvres. Journal of Applied Physiology 1997;83: 753–760.
Jammes Y, Pouget J, Grimaud C, Serratrice G.Pulmonary function and electromyographic studyof respiratory muscles in myotonic dystrophy.Muscle and Nerve 1985; 8: 586–594.
Jenkins S, Soutar S, Gray B, Evans J, Moxham J. Theacute effects of respiratory manoeuvres in post-operative patients. Physiotherapy Theory andPractice 1988; 4: 63–68.
Johnson ER, Abrasch RT, Carter GT, Kilmer DD,Fowler WMJ, Sigford BJ et al. Profiles of neuro-muscular diseases: myotonic dystrophy.American Journal of Physical Medicine andRehabilitation 1995; 74 (Suppl.): S104–S116.
Kilkenny TM, Grenard S. Body position andobstructive sleep apnoea. Journal of RespiratoryCare Practitioners 1999; 15: 59–64.
Kimura J. Electrodiagnosis in Disease of Nerve andMuscle, Principles and Practice. Philadelphia, PA:FA Davis, 1983.
Martin CJ, Ripley H, Reynolds J, Best F. Chestphysiotherapy and the distribution of ventilation.Chest 1976; 69: 174–178.
Mathieu J, Allard P, Gobeil G, Girard M, DeBraekeleer M, Bégin P. Anaesthetic and surgicalcomplications in 219 cases of myotonicdystrophy. Neurology 1997; 49: 1646–1650.
McGuiness J, Vicenzino B, Wright A. Influence of acervical mobilisation technique on respiratory andcardiovascular function. Manual Therapy 1997; 2:216–220.
Mead J, Peterson N, Grimby G, Mead J. Pulmonaryventilation measured from body surfacemovements. Science 1967; 156: 1383–1384.
Mengelkoch LJ, Martin D, Lawler J. A review of theprinciples of pulse oximetry and accuracy of pulseoximeter estimates during exercise. PhysicalTherapy 1994; 74: 40–49.
Menkes HA, Traystman RJ. Collateral ventilation.American Review of Respiratory Disease 1977;116: 287–309.
Morran CG, Finlay IG, Mathieson M, McKay AJ,Wilson N, McArdle CS. Randomised controlledtrial of physiotherapy for post-operativepulmonary complications. British Journal ofAnaesthesia 1983; 55: 1113–1116.
Nitz JC. Physiotherapy for myotonic dystrophy.Physiotherapy 1999; 85: 597–602.
Remolina C, Khan AV, Santiage TV, Edelman NH.Positional hypoxemia in unilateral lung disease.New England Journal of Medicine 1981; 304:523–525.
Rimmer KP, Golar SD, Lee MA, Whitelaw WA.Myotonia of the respiratory muscles in myotonicdystrophy. American Review of RespiratoryDisease 1993; 148: 1018–1022.
Roussos CS, Fixley M, Genest J, Cosio M, Kelly S,Martin RR, Engel LA. Voluntary factors influ-encing the distribution of inspired gas. AmericanReview of Respiratory Disease 1977; 116:457–467.
Schmidt-Nowara WW, Altman AR. Atelectasis andneuromuscular respiratory failure. Chest 1991;85: 792–795.
Sears TA, Newsom Davis J. The control of respiratorymuscles during voluntary breathing. Annals of theNew York Academy of Science 1968; 155:183–190.
Serisier DE, Mastaglia FL, Gibson GJ. Respiratorymuscle weakness and ventilatory control inmyotonic dystrophy. Thorax 1980; 35: 710.
Swash M, Fox KP. Abnormal intrafusal muscle fibres inmyotonic dystrophy: a study using serial sections.Journal of Neurology, Neurosurgery and Psychiatry1975; 38: 91–99.
Ugalde V, Breslin EH, Walsh SA, Bonekat HW,Abresch RT, Carteg GT. Pursed lips breathingimproves ventilation in myotonic musculardystrophy. Archives of Physical Medicine andRehabilitation 2000; 81: 472–478.
Ververs CCM, Van der Meché FGA, Verbraak AFM,van der Sluys HCM, Bogaard JM. Breathingpattern awake and asleep in myotonic dystrophy.Respiration 1996; 63: 1–7.
Voss DE, Ionta MK, Meyers BJ. ProprioceptiveNeuromuscular Facilitation Patterns andTechniques (third edition). Philadelphia, PA:Harper & Row, 1985.
Webber BA. The Brompton Hospital Guide to ChestPhysiotherapy (fifth edition). Oxford: BlackwellScientific Publications, 1988.
West JB. Ventilation and perfusion relationships.American Review of Respiratory Disease 1977;116: 919–943.
Address for correspondence: Dr Jennifer CNitz PhD M Phty B Phty, Lecturer,Department of Physiotherapy, School ofHealth and Rehabilitation Sciences, TheUniversity of Queensland, St Lucia 4072,Australia.
(Submitted August 2001; accepted June 2002)
PRI 7(4)_crc 21/11/02 2:15 PM Page 238
Related Documents