Tobacco Dependence, Attitudes and Treatment Strategies Dr. Vajer Péter Department of Family Medicine Semmelweis University Section 1: Burden of Disease Smoking is highly prevalent worldwide Smoking increases morbidity and mortality The benefits of quitting have been demonstrated Gender-Specific Smoking Prevalence Across the World 1. Mackay J, et al. The Tobacco Atlas. Second Ed. American Cancer Society Myriad Editions Limited, Atlanta, Georgia, 2006. Also available online at: http://www.myriadeditions.com/statmap/. US 24% 19% Men Women Australia 19% 16% Belarus 53% 7% Brazil 22% 14% Canada 22% 17% Chile 48% 37% China 67% 2% Egypt 45% 12% France 30% 21% Iceland 25% 20% Mexico 13% 5% Iran 22% 2% Kenya 21% 1% Sweden 17% 18% Philippines 41% 8% Portugal 33% 10% South Africa 23% 8% India 47% 17% Russian Fed 60% 16% Italy 33% 17% Spain 39% 25% Germany 37% 28% Smoking Prevalence of Adults vs Youths: Young People Are Also at Risk *Young men/women = 15-year-old students who smoke cigarettes. 1. Shafey O, et al (eds). Tobacco Control Country Profiles 2003, American Cancer Society, Atlanta, Georgia, 2003. Available at: http://www.who.int/tobacco/globaldata/countryprofiles/en/. 2. Mackay J, et al. The Tobacco Atlas. Second Edition. American Cancer Society Myriad Editions Limited. Atlanta, Georgia, 2006. Also available online at: http://www.myriadeditions.com/statmap/. Adults 2 Young Men 2 Young Women 2 1.25 billion smokers worldwide 1-2 US 22% 18% 12% Australia 17% 24% 23% Belarus 27% 36% 28% Argentina 29% 16% 28% Canada 20% 16% 14% Egypt 29% 6% 3% France 25% 26% 27% Ireland 27% 20% 21% Venezuela 29% 5% 6% Iran 11% 2% N/A Kenya 11% 8% 4% Sweden 18% 11% 19% Philippines 24% 10% 3% Portugal 21% 18% 26% South Africa 16% 15% 8% Russian Fed 35% 27% 19% Spain 32% 24% 32% Italy 24% 22% 25% Germany 33% 32% 34% Smoking: Leading Preventable Cause of Disease and Death 1 Top 3 Smoking-Attributable Causes of Death in US #1 Lung cancer #2 Ischemic heart disease #3 COPD Cancer Lung (#1)* Leukemia (AML, ALL, CLL) 2-4 Oral cavity/pharynx Laryngeal Esophageal Stomach Pancreatic Kidney Bladder Cervical Cardiovascular Ischemic heart disease (#2)* Stroke – Vascular dementia 5 Peripheral vascular disease 6 Abdominal aortic aneurysm Respiratory COPD (#3)* Pneumonia Poor asthma control Reproductive Low-birth weight Pregnancy complications Reduced fertility Sudden Infant Death Syndrome Other Adverse surgical outcomes/wound healing Hip fractures Low-bone density Cataract Peptic ulcer disease † *Top 3 smoking-attributable causes of death. † In patients who are Helicobacter pylori positive. AML = Acute myeloid leukemia; ALL = acute lymphocytic leukemia; CLL = chronic lymphocytic leukemia; COPD = chronic obstructive pulmonary disease; SIDS = sudden infant death syndrome. 1. Surgeon General’s Report. The Health Consequences of Smoking; 2004. 2. Sandler DP, et al. J Natl Cancer Inst. 1993;85(24):1994-2003. 3. Crane MM, et al. Cancer Epidemiol Biomarkers Prev. 1996;5(8):639- 644. 4. Miligi L, et al. Am J Ind Med. 1999;36(1):60-69. 5. Roman GC. Cerebrovasc Dis. 2005;20(Suppl 2):91-100. 6. Willigendael EM, et al. J Vasc Surg. 2004;40:1158-1165. 29% 28% 23% 4% 8% 8% Lung, Trachea, Bronchus Cancer Ischemic Heart Disease Respiratory Diseases Cerebrovascular Disease Other Cancers Other Causes US Mortality From Smoking-Related Disease* Approximately 438,000 annual US deaths attributable to cigarette smoking between 1997 and 2001 † † *Percentage of deaths attributable to specific smoking-related diseases, 1997–2001. † Includes secondhand smoke deaths. 1. CDC. MMWR. 2005;54:625–628.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Tobacco Dependence, Attitudes
and Treatment Strategies
Dr. Vajer Péter
Department of Family Medicine
Semmelweis University
Section 1: Burden of Disease
� Smoking is highly prevalent worldwide
� Smoking increases morbidity and mortality
� The benefits of quitting have been
demonstrated
Gender-Specific Smoking
Prevalence Across the World
1. Mackay J, et al. The Tobacco Atlas. Second Ed. American Cancer Society Myriad Editions Limited, Atlanta,
Georgia, 2006. Also available online at: http://www.myriadeditions.com/statmap/.
US
24%
19%
Men
Women Australia
19%
16%
Belarus
53%
7%
Brazil
22%
14%
Canada
22%
17%
Chile
48%
37%
China
67%
2%
Egypt
45%
12%
France
30%
21%
Iceland
25%
20%
Mexico
13%
5%
Iran
22%
2%
Kenya
21%
1%
Sweden
17%
18%
Philippines
41%
8%
Portugal
33%
10%
South Africa
23%
8%
India
47%
17%
Russian Fed
60%
16%
Italy
33%
17%
Spain
39%
25%
Germany
37%
28%
Smoking Prevalence of Adults vs
Youths: Young People Are Also at Risk
*Young men/women = 15-year-old students who smoke cigarettes.
1. Shafey O, et al (eds). Tobacco Control Country Profiles 2003, American Cancer Society, Atlanta, Georgia, 2003.
Available at: http://www.who.int/tobacco/globaldata/countryprofiles/en/. 2. Mackay J, et al. The Tobacco Atlas. Second
Edition. American Cancer Society Myriad Editions Limited. Atlanta, Georgia, 2006. Also available online at:
http://www.myriadeditions.com/statmap/.
Adults2
Young Men2
Young Women2
1.25 billion smokers worldwide1-2
US
22%
18%
12%
Australia
17%
24%
23%
Belarus
27%
36%
28%
Argentina
29%
16%
28%
Canada
20%
16%
14%
Egypt
29%
6%
3%
France
25%
26%
27%
Ireland
27%
20%
21%
Venezuela
29%
5%
6%
Iran
11%
2%
N/AKenya
11%
8%
4%
Sweden
18%
11%
19%
Philippines
24%
10%
3%
Portugal
21%
18%
26%
South Africa
16%
15%
8%
Russian Fed
35%
27%
19%Spain
32%
24%
32%
Italy
24%
22%
25%
Germany
33%
32%
34%
Smoking: Leading Preventable
Cause of Disease and Death1
Top 3 Smoking-Attributable Causes of Death in US#1 Lung cancer
#2 Ischemic heart disease#3 COPD
Cancer
Lung (#1)* Leukemia
(AML, ALL, CLL)2-4
Oral cavity/pharynx Laryngeal
Esophageal Stomach
Pancreatic Kidney
Bladder Cervical
Cardiovascular
Ischemic heart disease (#2)*
Stroke – Vascular dementia5
Peripheral vascular disease6
Abdominal aortic aneurysm
Respiratory
COPD (#3)*
Pneumonia
Poor asthma control
Reproductive
Low-birth weight
Pregnancy complications
Reduced fertility
Sudden Infant Death Syndrome
Other
Adverse surgical outcomes/wound healing
Hip fractures
Low-bone density
Cataract
Peptic ulcer disease†
*Top 3 smoking-attributable causes of death. †In patients who are Helicobacter pylori positive.
AML = Acute myeloid leukemia; ALL = acute lymphocytic leukemia; CLL = chronic lymphocytic leukemia; COPD =
chronic obstructive pulmonary disease; SIDS = sudden infant death syndrome.
1. Surgeon General’s Report. The Health Consequences of Smoking; 2004. 2. Sandler DP, et al.
J Natl Cancer Inst. 1993;85(24):1994-2003. 3. Crane MM, et al. Cancer Epidemiol Biomarkers Prev. 1996;5(8):639-
644. 4. Miligi L, et al. Am J Ind Med. 1999;36(1):60-69. 5. Roman GC. Cerebrovasc Dis. 2005;20(Suppl 2):91-100. 6.
Willigendael EM, et al. J Vasc Surg. 2004;40:1158-1165.
29%
28%
23%4%
8%
8%
Lung, Trachea, Bronchus Cancer
Ischemic Heart Disease
Respiratory Diseases
Cerebrovascular Disease
Other Cancers
Other Causes
US Mortality From Smoking-Related
Disease*
Approximately 438,000 annual US deaths attributable to cigarette smoking
between 1997 and 2001
†
†
*Percentage of deaths attributable to specific smoking-related diseases, 1997–2001.†Includes secondhand smoke deaths.
1. CDC. MMWR. 2005;54:625–628.

Annual Deaths Attributable to
Tobacco: Worldwide Estimates
Canada
>25%
Australia
20%-24%
UK
>25%
Germany
>25%China & Taiwan
10%-14%
Brazil
15%-19%
% of Total Deaths Attributable to Tobacco*
*Regional estimates in 2000 in men aged >35 years.
1. Mackay J, Eriksen M. The Tobacco Atlas. Second Ed. World Health Organization; 2006.
US
>25%
Mexico
15%-19%
Argentina
15%-19%
Spain
>25%
Russian Federation
>25%Sweden
>25%
Turkey
>25%
% female
deaths
0
• Sub-Saharan
Africa
Four Stages of the Tobacco Epidemic:
Mortality Is Increasing in Many Countries1
If current smoking patterns continue, deaths from smoking in Asia—home to a third of
the world’s population—are expected to increase by 2020 to 4.9 million annually.2
Percentage
of smokers
among adults
Percentage
of deaths
caused by
smoking
• China
• Japan
• Southeast Asia
• Latin America
• North Africa
• Eastern Europe
• Southern Europe
• Western Europe,
UK
• USA
• Canada
• Australia
STAGE 1 STAGE 2 STAGE 3 STAGE 4
70
60
50
40
30
20
10
0
706050403020100 80 90 100
40
30
20
10% male
deaths
% male
smokers% female
smokers
Years
1. Lopez AD, et al. Tobacco Control. 1994;3:242-247. 2. Shafey O, et al (eds). Tobacco Control Country Profiles 2003,
American Cancer Society; 2003; Atlanta, Georgia. Available at:
http://www.who.int/tobacco/global_data/country_profiles/en/. Accessed June 2006.
Results From a Study of Male Physician Smokers in the United Kingdom
1. Doll R, et al. BMJ. 2004;328:1519–1527.
Smoking Reduces Survival an
Average of 10 Years
10 years
24
4
26
59
81
94
100
80
60
40
20
0
40 50 60 70 80 90 100
9791
81
59
2
Age (Years)
Survival At
Each Age
Point (%)
Physician Smokers
Physician Nonsmokers
What’s in a Cigarette?
� Tobacco smoke: ≥4000 chemicals, ≥250 toxic or carcinogenic1
� Nicotine is addictive, but not carcinogenic3
� Smoking cigarettes with lower tar and nicotine provides no health benefit4
Chemical in Tobacco Smoke2 Also Found In…
Acetone Paint stripper
Butane Lighter fluid
Arsenic Ant poison
Cadmium Car batteries
Carbon monoxide Car exhaust fumes
Toluene Industrial solvent
1. National Toxicology Program. 11th Report on Carcinogens; 2005. Available at: http://ntp-server.niehs.nih.gov. 2.
Mackay J, Eriksen M. The Tobacco Atlas. World Health Organization; 2006. 3. Harvard Health Letter. May 2005. 4.
Surgeon General’s Report. The Health Consequences of Smoking; 2004.
Mechanisms of Action:
How Smoking Causes Disease
� Lung cancer
– Direct respiratory cell exposure to potent mutagens
and carcinogens in tobacco smoke
� Ischemic heart disease
– Toxic products in the bloodstream create a
pro-atherogenic environment
– Leads to endothelial injury and dysfunction,
thrombosis, inflammation, and adverse lipid profiles
� Chronic Obstructive Pulmonary Disease (COPD)
– Accelerated decline in respiratory function
1. Surgeon General’s Report. The Health Consequences of Smoking; 2004.
What Does Secondhand Smoke Do?
� Estimated lung cancer risk increased by
20%–30%1
� Believed to cause and worsen diseases such as
asthma, COPD, and emphysema2
� Increases risk for developing heart disease by
25%–30%1
� Increases risk of nonfatal acute myocardial
infarction in a graded manner3
1. News release, June 27, 2006; US Department of Health & Human Services. Available at:
http://www.hhs.gov/news/press/2006pres/20060627.html. 2. Mackay J, et al. The Tobacco Atlas. World Health
Organization; 2002. 3. Teo KK, et al. Lancet. 2006;368:647-658.

What Does Secondhand Smoke Do
to Infants and Children?
� Almost 60% of US children are exposed to secondhand smoke1
� In some countries, ≥80% of youth live in homes where others smoke in their presence2
� Secondhand smoke increases disease burden and hospitalisation in
infants and children. For example:
– UK - 17,000 children under the age of 5 years hospitalised annually3
– Australia - 56% higher risk for hospitalisation if mother smoked in same
room as infant, 73% if smoked while holding infant, and 95% if smoked
while feeding infant (N = 4486)4
– Hong Kong - higher likelihood for hospitalisation for infants living with
any smoker at home with poor smoking hygiene (<3 metres away)5
1. Secondhand smoke; Fact sheet, June 2006. Available at:
http://www.cdc.gov/tobacco/factsheets/secondhand_smoke_factsheet.htm. 2. Mackay J, Eriksen M. The Tobacco
Atlas. World Health Organization; 2006. 3. Fagerstrom K. Drugs. 2002;62(suppl 2):1-9. 4. Blizzard L, et al. Arch
Pediatr Adolesc Med. 2004;158:687-693. 5. Leung GM, et al. Arch Pediatr Adolesc Med. 2004;158:687-693.
Smoking During Pregnancy
Harms Infants
� Exposure during pregnancy associated with1–3
– Increased risk of miscarriage, stillbirth, sudden infant
death syndrome (SIDS); eg
– Low-birth weight
• 4-fold risk1: eg, 9700–18,600 cases related to secondhand
smoke annually in US*3
– Impaired infant lung function2
– Possible association with cognitive and
developmental syndromes1,4
*1990s.
1. Fagerström K. Drugs. 2002;62(Suppl 2):1–9. 2. Le Souef PN. Thorax. 2000;55:1063–1067.
3. Mackay J, et al. The Tobacco Atlas. World Health Organization; 2002. 4. Hellstrom-Lindahl E,
et al. Respiration. 2002;69:289-293.
Importance of NOT Smoking
During Pregnancy
Rate of Infants with Low-Birth Weight
in Taiwanese Infants by Smoking Status of the Mother (N=9499)
†P<0.05 vs never smoked. ‡Before or during first trimester.
1. Wen CP, et al. Tob Control. 2005;14(Suppl 1):i56–i61.
†
†
4.8
5.8
8.2
0
2
4
6
8
10
Rate of Infants With
Low Birth Weight
(%)
Never Smoked Quit Smoking‡ Continued
Smoking
Why Quit? Potential Lifetime Health
Benefits of Quitting Smoking
1. CDC. Surgeon General Report 2004: http://www.cdc.gov/tobacco/sgr/sgr_2004/sgranimation/flash/index.html.
American Cancer Society. Guide to Quitting Smoking. Available at: http://www.cancer.org. Accessed June 2006.
2. American Cancer Society. Guide to Quitting Smoking. Available at: http://www.cancer.org. Accessed June 2006.
3.US Department of Health & Human Services. The Health Benefits of Smoking Cessation: A Report of the Surgeon
General. Centers for Disease Control and Prevention (CDC), Office on Smoking and Health. 1990. Available at:
http://profiles.nlm.nih.gov/NN/B/B/C/T/. Accessed July 2006.
Lung function may start to improve
with decreased cough, sinus
congestion, fatigue, and shortness of
breath
3 months
Lung cancer risk is 30-50% that of continuing smokers
Cessation
CHD: excess risk is reduced by 50% among ex-smokers
Cardiovascular heart disease (CHD) risk is similar to never smokers
Stroke risk returns to the level of people who have never
smoked at 5-15 years post-cessation
1 year
5 years
10 years
15 years
55-64
0
10
20
30
40
50
60
70
80
90
100
40 50 60 70 80 90 100
Age (Years)
1. Doll R, et al. BMJ. 2004;328:1519–1527.
Quitting at Any Age May Increase
Life Expectancy
Stopped Age
Results From a Study of Male Physician Smokers in the United Kingdom
Survival At
Each Age
Point (%)
60
Nonsmokers
Cigarette Smokers
0
10
20
30
40
50
60
70
80
90
100
40 50 60 70 80 90 100
1. Doll R, et al. BMJ. 2004;328:1519–1527.
Quitting at Any Age May Increase
Life Expectancy
Age (Years)
45-54Stopped Age
Nonsmokers
Cigarette Smokers
Results From a Study of Male Physician Smokers in the United Kingdom
Survival At
Each Age
Point (%)
50

0
10
20
30
40
50
60
70
80
90
100
40 50 60 70 80 90 100
Age (Years)
1. Doll R, et al. BMJ. 2004;328:1519–1527.
Quitting at Any Age May Increase
Life Expectancy
� Quitting sooner appears most beneficial
Survival At
Each Age
Point (%)
40
35-44Stopped Age
Results From a Study of Male Physician Smokers in the United Kingdom
Nonsmokers
Cigarette Smokers
Risk of Cardiovascular Disease
(CVD) Reduced By Quitting Smoking
� Quitting associated with
– 36% reduction in odds of all-cause mortality among patients with
coronary heart disease (CHD)1
– Decreases in CVD events in cardiac patients, even in those who
recently quit2
*Defined as self-reported smokers who were cotinine negative.
1. Critchley JA, Capewell S. JAMA. 2003;290:86-97. 2. Twardella D et al. Eur Heart J. 2004;25:2101–2108.
0.710.64
0.44
1.00
0.00
0.20
0.40
0.60
0.80
1.00
1.20
Currently Smokes Recently Quit* Formerly
Smoked
Never Smoked
Odds Ratio
Tobacco Dependence
and Treatment Strategies
Mechanism of Action of Nicotine in
the Central Nervous System
� Nicotine binds preferentially to nicotinic acetylcholinergic (nACh) receptors in
the central nervous system; the primary is the αααα4ββββ2 nicotinic receptor in the
Ventral Tegmental Area (VTA)
� After nicotine binds to the αααα4ββββ2 nicotinic receptor in the VTA, it results in a
release of dopamine in the Nucleus Accumbens (nAcc) which is believed to be
linked to reward
αααα4 ββββ2ββββ2ββββ2αααα4
αααα4ββββ2Nicotinic
Receptor
Nicotine Stimulates Dopamine
Release
� Nicotine activates α4β2 nicotinic receptors in the ventral tegmental area resulting in dopamine release at the
nucleus accumbens. This may result in the short-term
reward/satisfaction associated with cigarette smoking.
D
Ventral
Tegmental
Area
Nucleus
Accumbens
Adapted from Picciotto MR, et al. Nicotine and Tob Res. 1999: Suppl 2:S121-S125.
D − α4β2 Nicotinic Receptor− Nicotine − Dopamine
Reward
D
D
D
Axon
1. Schroeder SA. JAMA. 2005;294:482-487. 2. Jarvis MJ. BMJ. 2004; 328:277-279.
Nicotine May Cause Up-Regulation and
Desensitization of Receptors Resulting in
Tolerance
� Tolerance typically develops after long-term nicotine use1
� Tolerance is related to both the up-regulation (increased number)
and the desensitization of nicotine receptors in the VTA1
� A drop in nicotine level, in combination with the up-regulation and
decreased sensitivity of the nicotinic receptor, can result in
withdrawal symptoms and cravings1
� Smokers have the ability to self regulate nicotine intake by the
frequency of cigarette consumption and the intensity of inhalation1
� In order to maintain a steady nicotine level, smokers generally titrate
their smoking to achieve maximal stimulation and avoid symptoms
of withdrawal and craving2

The Cycle of Nicotine Addiction
� Nicotine binding causes an increase in
release of Dopamine1,2
� Dopamine gives feelings of pleasure
and calmness1
� The Dopamine decrease between
cigarettes leads to withdrawal
symptoms of irritability and stress1
� The smoker craves Nicotine to release
more Dopamine to restore pleasure
and calmness1
� Competitive binding of Nicotine to
nicotinic acetylcholinergic receptors
causes prolonged activation,
desensitization, and upregulation2
� As Nicotine levels decrease, receptors
revert to an open state causing
hyperexcitability leading to cravings1,2
1. Jarvis MJ. BMJ. 2004; 328:277-279. 2. Picciotto MR, et al. Nicotine and Tob Res. 1999: Suppl 2:S121-S125.
DopamineDopamine
NicotineNicotine
So Why Do People Smoke?
� Since at least the 1988 Surgeon General’s Report1
– Addiction defined as compulsive use despite damage to the individual or society and drug-seeking behavior can take precedence over important priorities
– Addiction persists despite a desire to quit or even repeated attempts to quit
� Most people smoke primarily because they are addicted to nicotine2
� There is a clear link between smoking, nicotinic receptors, and addiction21. Centers for Disease Control and Prevention. The Health Consequences of Smoking: Nicotine Addiction; A
Report of the Surgeon General. Washington DC: US Department of Health and Human Services; 1988.
2. Jarvis MJ. BMJ. 2004;328:277-279.
AddictionAddiction –– Habitual psychological and physiological dependence Habitual psychological and physiological dependence
on substance or practice which is beyond voluntary controlon substance or practice which is beyond voluntary control
–– StedmanStedman’’s Medical Dictionarys Medical Dictionary
Nicotine Addiction: A Chronic
Relapsing Medical Condition
� True drug addiction1
� Requires long-term clinical intervention, as do other addictive
disorders
– Failure to appreciate the chronic nature of nicotine addiction
may2
• Impair clinicians’ motivation to treat tobacco dependence long-term
• Impede acceptance that condition is comparable to diabetes,
hypertension, or hyperlipidemia, and requires counseling, support, and
appropriate pharmacotherapy
� Relapse is
– Common1,2
– The nature of addiction, not the failure of the individual3
• Long-term smoking abstinence in those who try to quit unaided† = 3%–5%
• Most relapse within the first 8 days
1. Fiore MC, Bailey WC, Cohen SJ, et al. Clinical Practice Guideline: Treating Tobacco Use and Dependence. US
Department of Health and Human Services. Public Health Service; June 2000. Available at:
www.surgeongeneral.gov/tobacco/default.htm. 2. Jarvis MJ. Why people smoke. BMJ. 2004;328:277-279.
Tobacco Dependence and Environmental
Behavior Reinforcement
� Pharmacologic effects
– Nicotine is a primary reinforcer
� Non-pharmacologic effects
– Environmental/social stimuli associated with smoking
play a role in reinforcing nicotine dependence
– Environmental/social stimuli enhance the reinforcing
effects of nicotine
Direct pharmacologic effects of nicotine are necessary but not
sufficient to explain tobacco dependence; these effects
must take into account the environmental/social context
in which the behavior occurs
1. Caggiula AR et al. Psychol Behavior. 2002;77:683–687.
Withdrawal Syndrome: a Combination of Physical and Psychological Conditions, Making
Smoking Hard to Treat1,2
Restlessness or impatience
(<4 weeks)2
Increased appetite or weight gain(>10 weeks)2
Withdrawal Syndrome
Anxiety(may increase or
decrease with quitting)1,2
Dysphoric or depressed mood
(<4 weeks)2
Irritability, frustration, or anger
(<4 weeks)2
Difficulty concentrating(<4 weeks)2
Insomnia/sleep disturbance(<4 weeks)2
1. Diagnostic and Statistical Manual of Mental Disorders, IV-TR. Washington, DC: APA; 2006: Available at
http://psychiatryonline.com. Accessed November 7, 2006. 2. West RW, et al. Fast Facts: Smoking Cessation. 1st ed.
Oxford, United Kingdom. Health Press Limited. 2004.
Why Some Smokers May Need More
Help to Quit
� Studies show some groups may be less
likely to quit:
– Higher level of dependence1
• Cigarettes per day
• Time to first cigarette upon awakening
– Living with a current smoker1
– Fewer educational qualifications2
– Lower socioeconomic class2
– Co-morbid psychiatric disorders3
1. Hyland A et al. Nicotine Tob Res. 2004;6(Suppl 3):S363-S369. 2. Chandola T et al. Addiction. 2004;99:770-777.
3. Kalman D et al. Am J Addict. 2005;14:106–123.

Multiple Quit Attempts
May Be Necessary
� More than 70% of US smokers have attempted to quit1
– Approximately 46% try to quit each year
– Less than 5% who try to quit are abstinent 1 year later
– Similar percentages in countries with established tobacco control
programs (eg, Australia, Canada, UK)2
• 30% to 50% try to quit; <5% achieve long-term abstinence
� Some smokers succeed after making several attempts3
– Past failure does not prevent future success
– Length of prior abstinence is related to quitting success
1. Fiore MC, et al. US Department of Health and Human Services. Public Health Service. June 2000. 2. Foulds J, et
al. Expert Opin Emerg Drugs. 2004;9:39–53. 3. Grandes G, et al. Br J Gen Pract. 2003;53:101–107.
Most Smokers Are Willing to
Try Again
� Of smokers who relapsed following a quit
attempt:
– 98% were willing to try again
– 50% immediately
– 28% within 1 month
� Of those willing to try again immediately
– Percentage did not differ based on time since
previous attempt
� Some smokers may prefer a waiting period
before attempting to quit again
1. Joseph A, et al. Nicotine Tob Res. 2004;6:1075–1077.
Length of Prior Abstinence Is
Related to Quitting Success
� Previous quit attempts of ≥3 months
positively predicted sustained,
biochemically confirmed abstinence1
– N = 1768; OR* = 1.8; 95% CI = 1.1–2.7
� Duration of previous quit attempts
influenced continuous abstinence at 6
months2
– N = 509; OR* = 1.73; 95% CI = 1.09–2.75
*OR = odds ratio.
1. Grandes G et al. Br J Gen Pract. 2003;53:101–107. 2. Aubin HJ et al. Addiction. 2004;99:1206-1218.
Non-pharmacologic Therapies:
Advice and Support
� All smokers should be1
– Advised to quit (the “5As”)
– Offered assistance irrespective of motivation
� Three types of non-pharmacologic therapies are
effective1
– Practical counseling (problem solving/skills training)
– Social support as part of treatment
– Securing social support outside of treatment
� Effectiveness increases with treatment intensity1,2
1. Fiore MC, et al. Clinical Practice Guideline: Treating Tobacco Use and Dependence. US Department of Health
and Human Services. Public Health Service; June 2000. Available at:
www.surgeongeneral.gov/tobacco/default.htm.
2. National Institute for Health and Clinical Excellence. Brief interventions and referral for smoking cessation in
primary care. Available at: www.nice.org.uk/page.aspx?o=299611. Accessed September 2006.
Tobacco Dependence Support:
The “5As”
� Ask about tobacco use
� Advise to quit
� Assess willingness to make a quit attempt
� Assist in quit attempt
� Arrange follow-up
1. Fiore MC, et al. US Department of Health and Human Services. Public Health Service. June 2000.
The “5As”: Ask About Tobacco Use
� Identify and document tobacco use status for
every patient at every visit
� Implement an office-wide system that ensures
tobacco-use status is queried and documented
– Expand vital sign documentation to include tobacco
use
– Tobacco-use stickers on charts
– Computer reminder systems for electronic medical
records
1. Fiore MC, et al. US Department of Health and Human Services. Public Health Service. June 2000.
The “5As”: Advise to Quit
� In a clear, strong, and personalized manner, urge every
tobacco user to quit at least once per year
– CLEAR
• “I think it is important for you to quit smoking now, and I can help
you.”
– STRONG
• “As your clinician, I need you to know that quitting smoking is very
important to protecting your health now and in the future.”
– PERSONALIZED
• Tie tobacco use to health/illness (reason for office visit),
social/economic costs, motivation level, and impact on others
(children)
1. Fiore MC, et al. US Department of Health and Human Services. Public Health Service. June 2000.
The “5As”: Assess Willingness to
Make a Quit Attempt
� Is the tobacco user willing to make a quit attempt
at this time?
– If patient is willing to attempt quitting, offer assistance
– If patient is unwilling to quit now, provide motivational
intervention
1. Fiore MC, et al. US Department of Health and Human Services. Public Health Service. June 2000.
The “5As”: Assist in Quit Attempt
� For the patient willing to make a quit attempt, use
counseling and pharmacotherapy
– Provide practical counseling (problem solving and skills training)
– Provide social support
– Offer pharmacotherapy as appropriate
– Provide supplementary materials
• World Health Organization: www.who.int
• Centers for Disease Control and Prevention: www.cdc.gov/tobacco
• Society for Research on Nicotine and Tobacco: www.srnt.org
– Consider need for referral to formal program
• In person
• Telephone or internet-based
1. Fiore MC, et al. US Department of Health and Human Services. Public Health Service. June 2000.
The “5As”: Arrange Follow-up
� Schedule follow-up contact, preferably within the first
week after the quit date
� Follow-up can occur either in person or via telephone
� Follow-up actions
– Congratulate success
– Review circumstances of lapse – elicit recommitment to
abstinence
– Identify and anticipate challenges
– Assess pharmacotherapy use
– Consider referral for more intensive treatment
1. Fiore MC, et al. US Department of Health and Human Services. Public Health Service. June 2000.
Patient Satisfaction Linked With
“5A” Interventions
� Regardless of readiness to quit, smokers receiving 5A
interventions were more satisfied with their health care
N=1160.
*P<0.0001; †P= 0.0014.
1. Conroy MB, et al. Nicotine Tob Research 2005;7(Suppl 1):S29–S34.
*
†
†
†
†
0 20 40 60 80 100
Arranged
Assisted
Assessed
Advised
Asked
Very Satisfied (%)
Received 5As
No 5As
Effectiveness Increases with
Treatment Intensity
Level of Contact
Estimated Odds
Ratio
(95% CI)
Estimated
Abstinence Rate
(95% CI)
No Contact 1.0 10.9
Minimal Counseling
(less than 3 minutes)1.3 (1.01, 1.6) 13.4 (10.9, 16.1)
Low Intensity Counseling
(3 to 10 minutes)1.6 (1.2, 2.0) 16.0 (12.8, 19.2)
Higher Intensity Counseling
(more than 10 minutes)2.3 (2.0, 2.7) 22.1 (19.4, 24.7)
1. Fiore MC, et al. Clinical Practice Guideline: Treating Tobacco Use and Dependence. US Department of Health and
Human Services. Public Health Service; June 2000. Available at: www.surgeongeneral.gov/tobacco/default.htm.
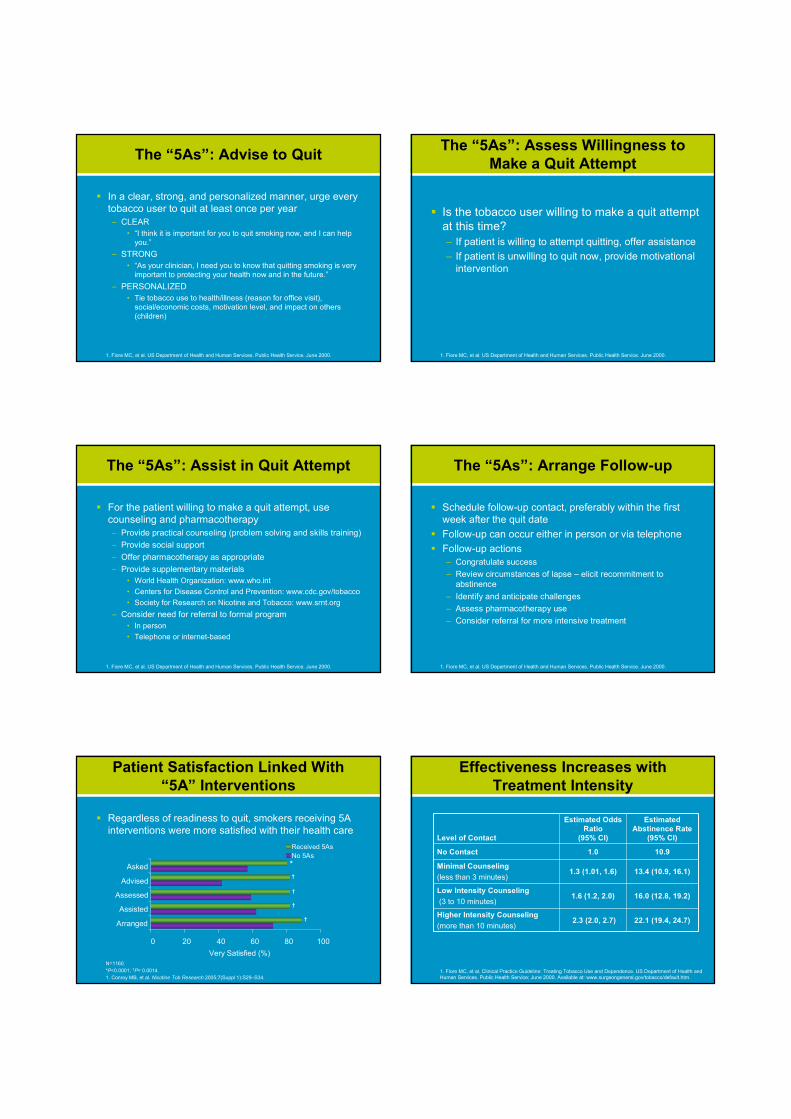
Non-Pharmacologic Treatment
for Smoking Cessation
Comparison
N
Trials
N
Participants
Pooled OR*
(95% CI)
Physician advice1
Brief vs no advice (usual care)
Intensive vs minimal advice
17
15
>13,000
>9,000
1.74 (1.48–2.05)
1.44 (1.24–1.67)
Individual counseling2
Vs minimal behavior intervention 17 >6,000 1.56 (1.32–1.84)
Group counseling3
Vs self-help
Vs no intervention
16
7
>4,000
815
2.04 (1.60–2.60)
2.17 (1.37–3.45)
Proactive Telephone counseling4
Vs less intensive interventions 13 >16,000 1.56 (1.38–1.77)
Self-help5
Vs no intervention 11 >13,000 1.24 (1.07–1.45)
*Abstinence assessed at least 6-months following intervention.
1. Lancaster T, Stead LF. Cochrane Database Syst Rev. 2004;(4):CD000165. 2. Lancaster T, Stead LF. Cochrane
Database Syst Rev. 2005;(2):CD001292. 3. Stead LF, Lancaster T. Cochrane Database Syst Rev. 2005;(4):
CD001007. 4. Stead LF et al. Cochrane Database Syst Rev. 2005;(4):CD002850. 5. Lancaster T, Stead LF. Cochrane
Database Syst Rev. 2005;(3):CD001118.
Pharmacotherapy for Tobacco
Dependence
� Nicotine replacement therapy (NRT)1
– Long acting1-3
• Patch
– Short acting1-3
• Gum
• Inhaler
• Nasal spray
• Sublingual tablets/lozenges
� Antidepressants4
– Bupropion SR4
– Nortriptyline3 (not approved for smoking cessation)
� Varenicline
1. Silagy C, et al. Cochrane Database Syst Rev. 2004;(3):CD000146. 2. Stead L, et al. Int J Epidemiol.
2005;34:1001–1003. 3. Henningfield JE, et al. CA Cancer J Clin. 2005;55:281-299.
4. Hughes JR et al. Cochrane Database Syst Rev. 2004;(4):CD000031.
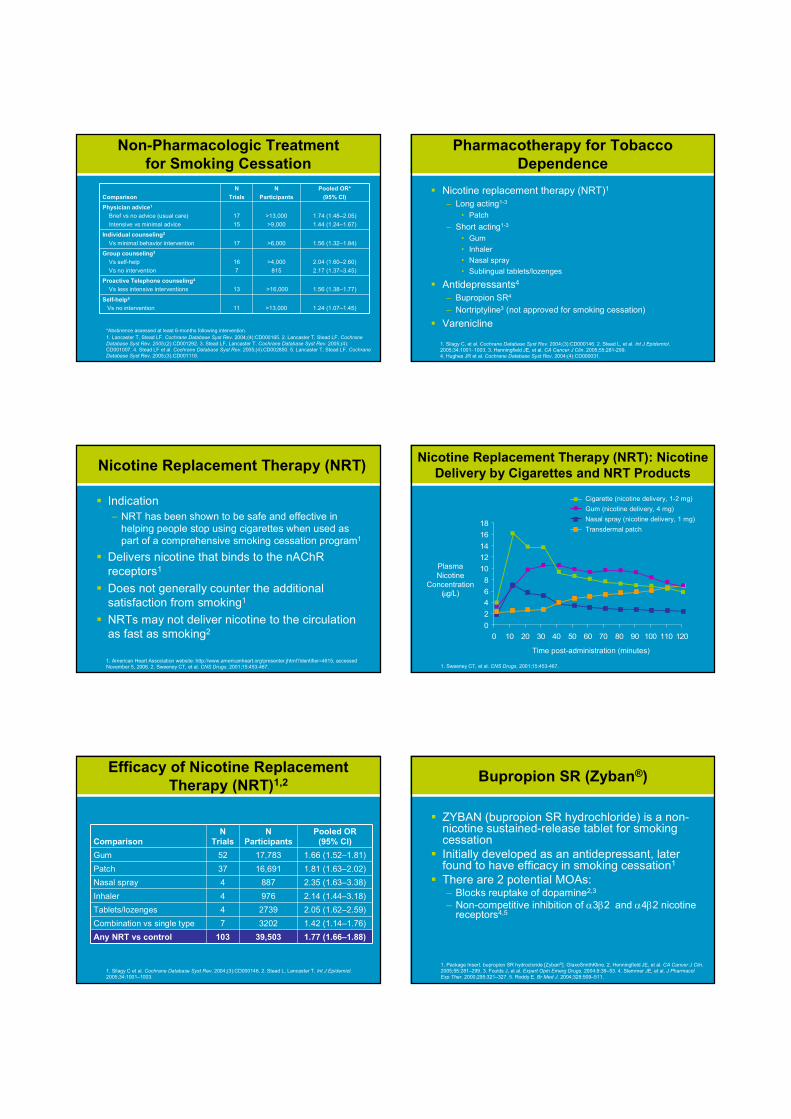
Nicotine Replacement Therapy (NRT)
� Indication
– NRT has been shown to be safe and effective in
helping people stop using cigarettes when used as
part of a comprehensive smoking cessation program1
� Delivers nicotine that binds to the nAChR
receptors1
� Does not generally counter the additional
satisfaction from smoking1
� NRTs may not deliver nicotine to the circulation
as fast as smoking2
1. American Heart Association website: http://www.americanheart.org/presenter.jhtml?identifier=4615, accessed
November 5, 2006. 2. Sweeney CT, et al. CNS Drugs. 2001;15:453-467.
0
2
4
6
8
10
12
14
16
18
0 10 20 30 40 50 60 70 80 90 100 110 120
Nicotine Replacement Therapy (NRT): Nicotine
Delivery by Cigarettes and NRT Products
Cigarette (nicotine delivery, 1-2 mg)
Gum (nicotine delivery, 4 mg)
Nasal spray (nicotine delivery, 1 mg)
Transdermal patch
Time post-administration (minutes)
Plasma
Nicotine
Concentration (µg/L)
1. Sweeney CT, et al. CNS Drugs. 2001;15:453-467.
Efficacy of Nicotine Replacement
Therapy (NRT)1,2
Comparison
N
Trials
N
Participants
Pooled OR
(95% CI)
Gum 52 17,783 1.66 (1.52–1.81)
Patch 37 16,691 1.81 (1.63–2.02)
Nasal spray 4 887 2.35 (1.63–3.38)
Inhaler 4 976 2.14 (1.44–3.18)
Tablets/lozenges 4 2739 2.05 (1.62–2.59)
Combination vs single type 7 3202 1.42 (1.14–1.76)
Any NRT vs control 103 39,503 1.77 (1.66–1.88)
1. Silagy C et al. Cochrane Database Syst Rev. 2004;(3):CD000146. 2. Stead L, Lancaster T. Int J Epidemiol.
2005;34:1001–1003.
Bupropion SR (Zyban®)
� ZYBAN (bupropion SR hydrochloride) is a non-nicotine sustained-release tablet for smoking cessation
� Initially developed as an antidepressant, later found to have efficacy in smoking cessation1
� There are 2 potential MOAs:– Blocks reuptake of dopamine2,3
– Non-competitive inhibition of α3β2 and α4β2 nicotine receptors4,5
1. Package Insert. bupropion SR hydrocloride [Zyban®]. GlaxoSmithKline. 2. Henningfield JE, et al. CA Cancer J Clin.
2005;55:281–299. 3. Foulds J, et al. Expert Opin Emerg Drugs. 2004;9:39–53. 4. Slemmer JE, et al. J Pharmacol
Exp Ther. 2000;295:321–327. 5. Roddy E. Br Med J. 2004;328:509–511.

Comparison of Nicotine Replacement Therapy (NRT)
and Bupropion SR Therapy for Quitting Smoking1
� Only study comparing NRT and antidepressant
therapy for quitting smoking2
*P≤ 0.001 vs placebo and patch alone.
1. Jorenby DE, et al. N Engl J Med. 1999;340:685–691. 2. Talwar A et al. Med Clin North Am. 2004;88:1517–1534.
5.69.8
18.4*22.5*
0
10
20
30
40
50
1 Year Continuous Abstinence(Week 2 to Week 52)
Abstinence
Rate (%)
Placebo (n = 160) Nicotine Patch (n = 244)
Bupropion SR (n = 244) Bupropion SR + Patch (n = 245)
Champix (varenicline): A Highly
Selective αααα4ββββ2 Receptor Partial Agonist
1. Coe JW et al. Presented at the 11th Annual Meeting and 7th European Conference of the Society for Research on
Nicotine and Tobacco. 2005. Prague, Czech Republic. 2. Picciotto MR et al. Nicotine Tob Res. 1999; Suppl 2:S121-
S125.
Binding of nicotine at the α4β2 nicotinic receptor in the VTA is believed to cause release of dopamine at the nAcc
Champix is an α4β2 nicotinic receptor partial agonist, a compound with dual agonist and antagonist activities. This is believed to result in both a lesser amount of dopamine release from the VTA at the nAcc as well as the prevention of nicotine binding at the α4β2 receptors.
Nicotine Chantix
Varenicline Mechanism of Action:
Efficacy for Tobacco Dependence
� Efficacy of varenicline in tobacco dependence – Believed to result from partial agonist activity at the α4β2
nicotinic receptor
� By preventing binding of nicotine, varenicline– Reduces craving and withdrawal symptoms (agonist activity)
– Produces a reduction of the rewarding and reinforcing effects ofsmoking (antagonist activity)
� The most frequently reported adverse events (>10%) with varenicline were nausea, headache, insomnia, and abnormal dreams.
1. Champix Summary of Product Characteristics. Pfizer Ltd, Sandwich, UK. 2006.
1: Findings from the STOP survey
69
81
97
92
87
53
0 20 40 60 80 100
Smoking is a lifestyle choice
Smoking is a medical condition
Smoking is addictive
Stopping is primarily down to willpower
Helping patient stop is part of job
Other things have higher priority
Percent
Pfizer-sponsored survey: Interviews with 2836 smoking and non-smoking
general practitioners in 16 countries
1: Apparent paradoxes
Smoking is an addiction stopping is a matter of
willpower
Smoking should be
regarded as a medical
condition
is primarily a lifestyle
choice
Helping patients to stop
is part of the job
other things have a
higher priority
but
1: What does this mean?
Need a message that recognises the
duality of beliefs about smoking
“Smokers must take responsibility for
stopping smoking, and they will need
determination to succeed; but when
determination is not enough, the
physician has effective tools to help the
smoker succeed.”

2: A simple model of nicotine
dependence
Chronic intake of
nicotine from
cigarettes
Changes to the
neural circuits
controlling
motivation
Nicotine hunger Nicotine habit False beliefs
A biologically driven
“need” to smoke
when nicotine levels
in the brain are low
Cues associated with
smoking trigger
nicotine-driven
reward seeking
Experience of relief
of nicotine withdrawal
symptoms leads to
expectations of more
general mood
enhancement
2: The process of stopping
Motivational tension
Triggers
Treatment
When smokers think about their smoking
most, they are unhappy about it, but many
of them:
Something needs to prompt them to make a
quit attempt using a method that maximises
their chances of success
The treatment needs to be of a type and
intensity that meets the individual smoker’s
needs, and available whenever and for as
long as the smoker needs it
1. Think it meets certain needs
2. Is a source of enjoyment
3. Think stopping will be difficult
3: The physician’s role
The
physician’s
role is:
Patients will
often respond
to a clear, firm
message from
their doctor
that:
• To give professional, expert
advice on health matters
• To provide treatment to those
who want and need it
• Now is a good time to stop
• It is always worth having
another attempt
• There are things available that
will make it easier
3: A simple consultation model
Yes, I know I should
stop, but...
I enjoy smoking
too much
Every month you put off
stopping, you may lose another
week off your life
Now is not a good time Now is always a good time for
stopping, smoking doesn’t really
help with stress
I am worried that
I will fail
Most smokers make many
attempts before they succeed
I am addicted Addictions can be conquered,
especially when you get help
We now
have
effective
treatments
available
that will
make it a lot
easier for
you to
succeed
Are you
smoking
at the
moment?
You have to question whether it is
worth the pain and suffering
you will endure later
It’s never too late…
Related Documents