Scientific Research Journal of India (SRJI) Dr. L. Sharma Campus, Muhammadabad Gohana Scientific Research Journal of India an open access journal SRJI Volume: 1 » No: 4 »Year: 2012 Mau, U.P., India. Pin- 276403 | +91-9320699167, 8822485959, 9305835734 [email protected] | http//www.srji.co.cc Cont: Email: Web: ISSN » 2277-1700

Scientific Research Journal of India SRJI Vol-1 No-4 October-December 2012
Mar 11, 2016
Scientific Research Journal of India SRJI Vol-1 No-4 October-December 2012
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Scientific Research Journal of India (SRJI)Dr. L. Sharma Campus, Muhammadabad Gohana
Scientific Research Journal of India
an open access journal
SRJI
Volume: 1 » No: 4 » Year: 2012
Mau, U.P., India. Pin- 276403 | +91-9320699167, 8822485959, [email protected] | http//www.srji.co.cc
Cont:
Email: Web:
ISSN » 2277-1700
Vol.1 No.4 2012
About Us: Scientific Research JournalCare and Educational Development Society.funded by the Dr. L. Sharma Medical Care and Educational Development Society.Multidisciplinary, Peer Reviewed,intended audiences of this journal are the professionals and students. The scope of journal is broad to cover the recent scientific research. The Journal publishes selebook reviews in the fields of Botany, Zoology,Environmental Sciences, Natural Sciences, Anthropology and any other branch of related sciences. Frequency: The issues will be regularly published Special Issue: Special issue based on specific themesexecutive committee of Society and the members of editorial of SRJI. Disclaimer:
• Information provided on the site is meant to complement and not replace any or information from a health professional.
• We do not make claims relating to the benefit or performance of a specific medical treatment, commercial product or service.
• All the papers published are claimed to be original by the authors. The editors, publisher, and reviewers will not be responsible for plagiarism.
Contact Us: Scientific Research Journal of India,Dr.L.Sharma Campus, Muhammadabad Gohana,Mau, U.P., India. Pin
Website: http://www.srji.co.ccEmail: [email protected]: +91-9320699167, 8822485959, 9305835734
Scientific Research Journal of India
http://www.srji.co.cc
Scientific Research Journal of India (SRJI) is the official organ of Dr.Care and Educational Development Society. It was founded by Dr. Krishna N. Sharma.
Sharma Medical Care and Educational Development Society.Peer Reviewed, Open Access Journal of science. The of this journal are the professionals and students. The scope of journal
recent inventions/discoveries in structural and functional principles of
The Journal publishes selected original research articles, reviews, short communication and book reviews in the fields of Botany, Zoology, Medical Sciences, Agricultural Sciences, Environmental Sciences, Natural Sciences, Anthropology and any other branch of related
The issues will be regularly published quarterly.
Special issue based on specific themes may be published at the suggestion of the Dr. L. Sharma Medical Care and Educational Development
members of editorial of SRJI.
Information provided on the site is meant to complement and not replace any or information from a health professional. We do not make claims relating to the benefit or performance of a specific medical treatment, commercial product or service. All the papers published are claimed to be original by the authors. The editors, publisher, and reviewers will not be responsible for plagiarism.
Scientific Research Journal of India, Dr.L.Sharma Campus, Muhammadabad Gohana, Mau, U.P., India. Pin- 276403
Website: http://www.srji.co.cc [email protected]
9320699167, 8822485959, 9305835734
1
http://www.srji.co.cc
(SRJI) is the official organ of Dr. L. Sharma Medical It was founded by Dr. Krishna N. Sharma. It is
Sharma Medical Care and Educational Development Society. It is a Journal of science. The
of this journal are the professionals and students. The scope of journal in structural and functional principles of
short communication and Medical Sciences, Agricultural Sciences,
Environmental Sciences, Natural Sciences, Anthropology and any other branch of related
published at the suggestion of the Sharma Medical Care and Educational Development
Information provided on the site is meant to complement and not replace any advice
We do not make claims relating to the benefit or performance of a specific medical
All the papers published are claimed to be original by the authors. The editors,

This page is intentionally left blank

Vol.1 No.4 2012 Scientific Research Journal of India 3
http://www.srji.co.cc
Index
Editorial
Dr. Krishna N. Sharma
5
Comparison of Clinic and Home Based
Exercise Programs after Total Knee Arthroplasty: A Pilot Study
Bijender Sindhu, Dr.Manoj Sharma, Dr.Raj K Biraynia
7
Electrical Muscle Stimulation (EMS) Improve Functional Independence in
Critically Ill Patients
Dharam Pani Pandey, Dr. Uday
Shankar Sharma, Dr. Ram Babu
19
A Comparative Study on Supervised Clinical Exercise versus Home Based Exercise in Primary Unilateral Total
Knee Arthroplasty
Bijender Sindhu, Dr.Manoj Sharma, Dr.Raj K Biraynia
Physiotherapy 27
Comparison of the Effect of Isometric
Exercise of Upper Limb on Vitals between Young Males and Females
Pranjal Parmar 37
Paraplegia with Sacral Pressure ulcer
treated by Ultrasound therapy- A Single Case Report
Shanmuga Raju P., Ramalingam P. 50
Arterio-Enteric Fistula: A Case Report Anil Degaonkar, Nikhil Bhamare,
Mandar Tilak Surgery 57
All-Oxide Solar Cells: The Way of the
Future
Akshay Vijay Dongarwar
Chemical Engineering 63

This page is intentionally left blank

Vol.1 No.4 2012 Scientific Research Journal of India 5
http://www.srji.co.cc
Editorial
Dear Readers,
I am very pleased to present the fourth issue of the Scientific Research
Journal of India (SRJI) as the next Editor in Chief. This multidisciplinary and
open access Journal of science is the official organ of Dr. L. Sharma Medical
Care and Educational Development Society. The previous issues had covered
three disciplines of science Physiotherapy, Agriculture, Anthropology and
Computer science. In this current issue we are covering two new branches of
science- Surgery, and Chemical Engineering. I would like to mention that this
journal is intended to publish selected original research articles, reviews, short
communications and book reviews etc. in the various fields of science like Botany,
Zoology, Medical Sciences, Agricultural Sciences, Environmental Sciences,
Natural Sciences, Anthropology and any other branch of related sciences and
we’ll be more than happy to recognize any of your works in these field too.
Your comments and suggestions are very valuable for us.
Happy Reading.
Regards,
Dr. Krishna N. Sharma
Editor in Chief

This page is intentionally left blank

Vol.1 No.4 2012 Scientific Research Journal of India 7
http://www.srji.co.cc
Comparison of Clinic and Home Based Exercise Programs after Total
Knee Arthroplasty: A Pilot Study
Bijender Sindhu PhD, PT*, Dr.Manoj Sharma, MBBS, MS(Ortho)**, Dr.Raj K Biraynia, MBBS,
D.Ortho***
Abstract: Sixteen patients (mean age, 68+-8 years) having primary total knee
arthroplasty were assigned randomly to two rehabilitation programs: (1) clinic-
based rehabilitation provided by outpatient physical therapists; or (2) home-
based rehabilitation monitored by periodic telephone calls from a physical
therapist. Both rehabilitation programs emphasized a common home exercise
program. Before surgery, and at discharge and follow up after surgery, no
statistically significant differences were observed between the clinic and the
home-based groups on any of the following measures: (1) total score on the Knee
Society clinical rating scale; (2) total score on the ILOA level of assistance (3)
total score on the Goniometry; (4) total score of VAScale. After primary total
knee arthroplasty, patients who completed a home exercise program (home-based
rehabilitation) performed similarly to patients who completed regular outpatient
clinic sessions in addition to the home exercises (clinic-based rehabilitation).
Additional studies need to determine which patients are likely to benefit most
from clinic-based rehabilitation programs.
Key Words: Total Knee Arthroplasty, Home Based Exercise Program, Clinic
Based Exercise Program
INTRODUCTION The aim of the arthroplasty is to resurface
the tibiofemoral joint to allow better
articulation and to reciprocate normal
kinematics of the knee (Palmer &
Cross,2004) Another aim of surgeons is to
correct valgus deformity through the
release of lateral structures (Elson &
Brenkel, 2006). The most common
approach is the medial parapatellar
approach. This has been shown to give
better radiological results, but more pain
in the short term than the minimally
invasive mid-vastus approach (Chen,
2006). Soft tissue and bony alignment can
be ensured using the Tensor/ Balancer
system (Winemaker, 2002). The Tensor/
Balancer system is important as
malalignment can lead to failure of the
operation (Winemaker,2002) Prostheses
consist of a femoral and tibial component.
The femoral or tibial component can be
cemented, hybrid (one component
cemented and the other uncemented) or
uncemented (Zavadak et al., 1995). The
type of prosthesis used depends on the
surgeons’ protocol.This question is
important because of time and cost
differences between these service delivery
settings. Clinic-based programs typically
are provided by outpatient physical
therapy clinics, and facilitate monitoring
the patient’s progress, modifying
individual programs, and providing patient
support and motivation. Home-based
programs, however, typically do not
require the patient to attend outpatient
clinic sessions or require attendance at a
minimum number of outpatient sessions,
and provide fewer opportunities for
monitoring or program modification.
Although usually developed by and taught
to patients by physical therapists, home-
based exercises typically are completed
independently by the patient at home.
The populations examined in those studies
have tended to be younger individuals
who otherwise were healthy, and with an
interest in returning to work or sporting
activities or both. The efficacy of clinic-
and home-based rehabilitation programs is
particularly important with respect to
elderly patients. Owing to the older age of
patients who have total knee arthroplasty,
the likelihood of complicating medical
conditions, the serious implications of
postoperative complications in this
population,and the medicolegal climate,
surgeons may be hesitant to prescribe non
clinically based rehabilitation programs
after hospital discharge. An often used
alternative to mandatory outpatient
physical therapy has been having all
patients complete a limited number of
clinic visits. Another alternative may be a
home-based program, monitored via
periodic telephone calls. Monthly phone

Vol.1 No.4 2012 Scientific Research Journal of India 9
http://www.srji.co.cc
calls by therapist individuals were
associated with increased function in
patients with osteoarthritis. Although
caution must be exercised in generalizing
the findings of their study, home exercise
programs developed and monitored by
physical therapists via periodic phone
calls may provide an alternative to
mandatory clinic-based programs and to
requiring a defined number of clinic visits,
and a means to provide some monitoring
of patients during the early rehabilitation
phase.
Objective of the Study: Objective of the Study:
The purpose of the current study was to
compare two rehabilitation programs after
total knee arthroplasty: (1) clinic-based
rehabilitation delivered in outpatient
physical therapy clinics; and (2) home-
based rehabilitation monitored by a
physical therapist via periodic telephone
calls, on disease-specific, joint-specific,
and functional outcome measures.
MATERIAL AND METHODS
Inclusion and Exclusion Criteria
Patients were selected using the following
criteria: patients having primary unilateral
total knee arthroplasty as a result of
osteoarthritis, both male and female who
had a primary unilateral TKA, age 50-85.
Able to give independent informed
consent. Patients with rheumatoid arthritis
or major neurologic conditions were
excluded.
Randomization to Groups
At the time of primary total knee
arthroplasty, 32 patients were assigned
randomly to two rehabilitation programs
(1) clinic-based rehabilitation provided by
outpatient physical therapy clinics; or (2)
home-based rehabilitation, monitored by a
physical therapist via periodic telephone
calls.
Inpatient and Home Exercise.
Familiarization Period
All patients received standard inpatient
physical therapy twice daily, for 20
minutes on each occasion. Inpatient
physical therapy also included instruction
in a series of home exercises to be
completed daily after discharge, regardless
of the patient’s group assignment.
Ambulatory status on the surgical side
was weight bearing as tolerated on
discharge after surgery, at which time the
patient progressed to walking with walker.
Discharge criteria included the ability to
transfer independently, ambulate more
than 30 m using walker/crutches, and
ascend and descend at least five steps.
Medication given at discharge was pain
killer, nutrition’s and antibiotics.
Common Home Exercises (for both
groups)

The common home exercise program was
that developed for routine total knee
arthroplasty rehabilitation at the authors’
institution, and consisted of basic (Stage 1)
and more advanced (Stage 2) ROM and
strengthening exercises. Each patient
received Stages 1 and 2 booklets, which
included written and pictorial descriptions
of each exercise and educational
information on using ice, controlling
swelling, walking, and ROM. They were
instructed to complete the common home
exercises three times daily until their 8-
week follow up, at which time they were
advised to continue the home exercises at
least once daily, indefinitely. Home-Based
Group A physical therapist familiar with
the common home exercises telephoned
each patient in the home-based group at
least two times ask whether the patient
was having any problems with the
exercises, to remind them of the
importance of completing the exercises,
and to provide advice on wound care, scar
treatment, and pain control. During each
telephone call, which lasted approximately
10 minutes, the patient was asked when
and how often he or she wished to be
telephoned in the future. Patients also
were provided with a contact telephone
number to call if additional questions
arose.
Table 1. Patient Baseline Characteristics for the Clinic- and Home-Based Groups
Clinic-Based Group In addition to the common home exercises,
patients in the clinic-based group were
Variable Clinic-Based (n=16)
Home-Based(n=16)
Continuous variables: mean (standard deviation) Age (years) 65.2 (6.9)* 64.6 (7.8) Height (cm) 160.2 (9.6) 162.3 (11.1) Mass (kg) 86.4 (15.6) 85.5 (15.9) Disease duration (years) 9.8 (6.4) 9.2 (7.3) Discrete variables: frequency and percent of group (percent)
Gender—female 9 (56.25%) 5 (31.25%) Left replacement 6 (37.5%) 3 (18.75%) Contralateral knee involvement 8 (50%) 6 (37.50%) Contralateral hip involvement 3 (18.75%) 1 (6.25%) Ipsilateral hip involvement 1 (6.25%) 0 (0%)

Vol.1 No.4 2012 Scientific Research Journal of India 11
http://www.srji.co.cc
required to attend outpatient physical
therapy after discharge to 8 weeks after
surgery, for as many as three sessions per
week, for approximately 1 hour per
session. Outpatient physical therapists
were provided with copies of the Stages 1
and 2 exercise booklets, and were asked to
use these exercises as the basic component
of their rehabilitation program. However,
they were not advised that the patient was
participating in a study comparing two
rehabilitation programs. Therapists were
permitted to modify or add exercises, use
therapeutic modalities (such as ice, heat,
and ultrasound), joint mobilizations, or
other measures as they deemed
appropriate. Patients in the clinic-based
group were requested to complete the
common home exercises at home only
twice on days that they attended clinic
sessions.
Fig 1. The study time-sequence flow chart is shown. Patients in both rehabilitation groups completed the common home exercises daily between Weeks 2 to 8.
Assessments and Measurements
In conjunction with routine orthopaedic
clinic evaluations pre surgically, and at
discharge, 8 weeks after surgery, patients
completed a series of questionnaires and
functional tests that required
approximately 1 hour. Throughout the
study, these tests were conducted by two
experienced testers who were blinded as
to the patient’s group assignment, and
gave the test results directly to the study
coordinator. The following tests were
completed: (1) total score on the Knee
Society clinical rating scale; (2) total score
on the ILOA level of assistance (3) total
score on the Gonioetry; (4) total score of
VAScale. From a position of maximum
extension, the patient slid the heel of the
test leg toward the buttocks to a position
of maximum knee flexion. The knee angle
was measured using a goniometer and
scored as the average of three repetitions.
Non directional, t tests, and tests of the
significance of the difference between two
percentages were used to compare the
clinic- and home-based groups on pre
surgical descriptive measures, and to
compare the patients who were lost to, or
dropped out of the study with those who
remained in the study, on baseline
Eligibility
Randomization
Clinic Based Rehabilitation
Home Based Rehabilitation
Total Knee Arthroplasty Inpatient Physical Therapy Common Home Exercise
Hospital Discharge at 5-7 days
OPD 3 session /week at 1
hour
Atleast 1 telephonic call
by therapist
Stage 2 4 week follow up
Instruction common home exrecise
OPD 2 session /week at 1
hour
Atleast 1 telephonic call
by therapist
Stage 3 8 week follow up
Instruction common home exrecise
measures. Four-way analysis of variance
(ANOVA) were used to examine the
following four criterion variables(1) total
score on the Knee Society clinical rating
scale; (2) total score on the ILOA level of
assistance (3) total score on the Gonioetry;
(4) total score of VAScale. After a
significant F-ratio, the Newman-Keuls
technique was used to compare selected
means.
Any patients who were removed from
their assigned group by the surgeons for
reasons related to the surgically treated
knee or medical conditions not related to
the surgically treated knee, or who
withdrew consent to participate, were
encouraged to continue with the home
exercises and any other therapies
prescribed, and to continue coming for
regular follow ups and testing. To take
into account that some patients were
removed or otherwise lost from their
group, but did continue to be tested at
their regular follow ups, two types of
analyses were completed: (1) a per
protocol analysis, which included all
patients who completed the study in their
assigned group; and (2) an intent to treat
analysis, in which all patients were
analyzed as having remained in their
assigned group, regardless of whether they
had completed the study in that group.
Analysis of variance tests were confined
to patients who had full data sets for the
three times of measurement (before
surgery, and discharge and 6 weeks after
surgery). In view of the number of
statistical tests computed and to minimize
the likelihood of Type 1 or alpha error, the
0.01 level was used to denote statistical
significance throughout analyses.
RESULT
Before surgery, no significant differences
were observed between the clinic- and the
home based groups on the demographic
variables shown in Table 1, or on any of
the nine criterion measures (p>0.01). No
statistically significant differences were
observed between the patients lost and
those who remained in the study (Table 2),
or between the patients lost to the two
groups on the baseline scores for any of
the four criterion measures, or for age,
height, and weight (p>0.01). Length of
stay in the hospital for the patients who
completed the study in their assigned
group was 5.1+-1.5 and 5.2+-1.7 days for
the home- and clinic-based groups,
respectively. On ANOVA tests, the per
protocol and the intent to treat analyses
produced identical results for all nine
criterion measures; no treatment, surgeon,
or prosthesis-related effects were observed
(p>0.01), and only the main effect for time
(averaged over treatment, surgeon) was
significant (p<0.01) (Figs 2, 3).
Subsequent analysis of the main effect for

Vol.1 No.4 2012 Scientific Research Journal of India 13
http://www.srji.co.cc
time indicated that the scores before
surgery, at discharge after surgery, and 6
weeks after surgery differed significantly
from one another (p<0.01); with one
minor exception. Pain before surgery,
measured via Visual analog score, was
significantly greater than that at discharge
and 8 weeks after surgery (p<0.01),
whereas there was no statistically
significant difference (p>0.01) between
the pain scores at discharge and 8 weeks,
on the per protocol and the intent to treat
analyses.
Table 2. Number of Patients Lost From Each Group and Reason for Loss
DISCUSSION
After primary total knee arthroplasty,
patients who completed home-based
rehabilitation performed similarly to
patients who completed clinic-based
rehabilitation during the first 4 weeks after
surgery. That all four criterion measures in
the current study produced similar results
for the per protocol and the intent-to-treat
analyses suggests that these findings apply
across a spectrum of disease-specific,
joint-specific, and functional variables.
Overall, the additional patient monitoring,
adjustment of program, and motivational
support available through clinic-based
rehabilitation was not advantageous for
the population studied. These findings
were not confounded by any interactions
with surgeon, type of prosthesis or time
since surgery. The current results extend
those of previous studies of meniscectomy
5,7,10 and anterior cruciate ligament
reconstruction1,3,4,11 populations, and
corroborate a previous retrospective study
using a total knee arthroplasty sample.
Patients who were lost to their assigned
group were not included in the per
protocol analysis, but did raise concerns
Patient Losses Clinic Based (n=16)
Home Based (n=16)
Patients lost during the inpatient period (before hospital discharge)
Medical issues related to the surgically treated knee 2 1 Withdrawal of consent by the patient 1 2 Other medical issues 2 1 Totals 5 4 Patients lost after hospital discharge (Weeks 2–52 after surgery)
Medical issues related to the surgically treated knee 0 1 Withdrawal of consent by the patient 0 0 Other medical issues 1 1 Total losses 1 2
that the group comparisons may have been
affected (Table 2). Comparisons within
and between groups indicated
differences between patients lost and
remaining. In addition, when patients
had been lost to their assigned group, but
continued being tested at their normal
follow-ups and had complete data sets,
were returned to their assigned group for
the intent to treat analysis, results were the
same as for the per protocol analysis. For
these reasons, patient losses were not
considered to have significantly
the overall results of the current study.
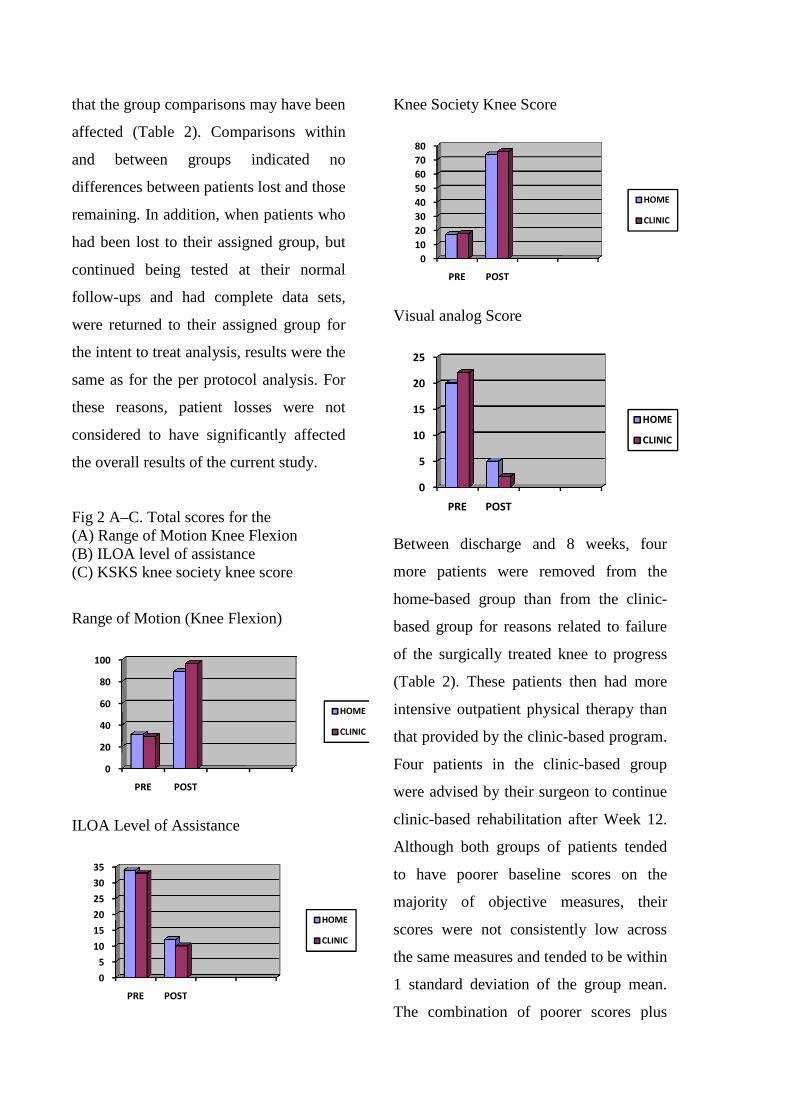
Fig 2 A–C. Total scores for the (A) Range of Motion Knee Flexion(B) ILOA level of assistance (C) KSKS knee society knee score
Range of Motion (Knee Flexion)
ILOA Level of Assistance
0
20
40
60
80
100
PRE POST
0
5
10
15
20
25
30
35
PRE POST
comparisons may have been
Comparisons within
and between groups indicated no
differences between patients lost and those
addition, when patients who
had been lost to their assigned group, but
continued being tested at their normal
and had complete data sets,
to their assigned group for
treat analysis, results were the
r protocol analysis. For
losses were not
considered to have significantly affected
the overall results of the current study.
Range of Motion Knee Flexion
nee society knee score
Knee Society Knee Score
Visual analog Score
Between discharge and 8 weeks
more patients were removed from the
home-based group than from the clinic
based group for reasons related
of the surgically treated knee to
(Table 2). These patients then had
intensive outpatient physical therapy than
that provided by the clinic-based program.
Four patients in the clinic
were advised by their surgeon to continue
clinic-based rehabilitation after Week 12.
Although both groups of patients tended
to have poorer baseline scores on the
majority of objective measures,
scores were not consistently low across
the same measures and tended to b
1 standard deviation of the group mean.
The combination of poorer scores plus
HOME
CLINIC
HOME
CLINIC
0
10
20
30
40
50
60
70
80
PRE POST
0
5
10
15
20
25
PRE POST
Between discharge and 8 weeks, four
were removed from the
from the clinic-
r reasons related to failure
of the surgically treated knee to progress
(Table 2). These patients then had more
intensive outpatient physical therapy than
based program.
patients in the clinic-based group
eir surgeon to continue
after Week 12.
of patients tended
scores on the
majority of objective measures, their
scores were not consistently low across
the same measures and tended to be within
standard deviation of the group mean.
combination of poorer scores plus
HOME
CLINIC
HOME
CLINIC

Vol.1 No.4 2012 Scientific Research Journal of India 15
http://www.srji.co.cc
subjective factors such as the patients’
attitudes, motivation, pain tolerance, and
home environment were considered in
making the decision to remove these
patients from their assigned group or to
continue clinic-based rehabilitation.
Additional studies are needed to document
psychosocial and demographic variables
to help identify patients who might derive
greatest benefit from clinic-based
rehabilitation programs.
The telephone calls to patients in the home
based group were completed by an
experienced physical therapist who had
been introduced to all of the patients
during their inpatient period. The
telephone calls focused on the home
exercises and did not introduce any new
exercises or provide unique treatment
guidance beyond that available from
similarly experienced therapists. Two
patients with potential major
problem ,such as unresolved swelling,
infection, and deep vein thrombosis, were
identified via the telephone calls and were
referred to the patient’s physician or
surgeon for treatment. Whether delayed
treatment of these conditions would have
resulted in major complications is unclear.
All of these patients completed the 8 week
study in their assigned group. As a result,
the telephone calls received by the home-
based group provided a form of minimally
supervised rehabilitation, which also
enabled some monitoring of the patient’s
medical status.
The major component of the current study
was the common home exercise program,
taught to all patients during their
hospitalization after surgery and at their 8
week follow up. Outpatient clinicians used
this program as the basis for their
treatments, and determined the number
and frequency of treatments, which
averaged 15+-20 sessions; whereas the
home-based group was monitored by
periodic telephone calls from a physical
therapist, which averaged 3+-1 calls
during the first 8 weeks after hospital
discharge. At hospital discharge, patients
in the home-based group indicated when
they wished to be telephoned, and again
did so during each telephone call. Pilot
study had indicated that virtually all
patients having primary total knee
arthroplasty had previous experience with
home exercise programs and that the
majority preferred to determine the
contact schedule themselves.
In addition to the phone calls, the follow-
ups at 4 and 8 weeks after surgery
included review of the home exercises.
That no patients in the home-based group
requested additional telephone calls after
4weeks and only three patients in the
clinic-based group phoned to ask
questions about the home exercises,
suggests all patients felt competent in
doing their home exercises. Although
passive ROM was examined by the
surgeons at each follow up, active ROM
was used to compare groups, to minimize
the extent to which pain tolerance and
motivation may have affected ROM.
Compliance with the home exercises was
considered high, with only two patients in
the home-based group and one patient in
the clinic-based group considered to have
been noncompliant at discharge and 4
after surgery (where compliance was
defined as completion of the home
exercises at least 90% of the time, as per
exercise log booklets). Exercise
compliance was discussed with the
patients before surgery and at each follow
up thereafter. The sample studied was
limited to elderly patients who agreed to
be assigned randomly to one of the two
rehabilitation programs. Approximately
10% of eligible patients refused to
participate for this reason. The extent to
which a home exercise program would be
effective for patients with a more
complicated history, more limited ROM,
or less motivation, needs to be determined.
CONCLUSION
The current study compared two
rehabilitation programs, where the basic
component of each program was a series
of common exercises to be completed
independently by all patients at home.
Because these exercises were developed
by and taught to the patients by physical
therapists, the current study might be
viewed as having compared two means of
providing physical therapy services; that is,
physical therapy monitored by telephone
calls (home-based) and physical therapy
monitored in person by outpatient physical
therapists (clinic-based). The current study
did not compare physical therapy versus
no physical therapy. There is no
significant difference in the data of study
but there is statistical difference in both
group. So this pilot studies shows that the
group of clinic based rehabilitation after
total knee arthroplasty having more better
prognosis than home based exercise group
ie. range of motion and functional ability
and pain.
REFERENCES:
1. Beard DJ, Dodd CAF: Home or
supervised rehabilitation following
anterior cruciate ligament
reconstruction: A randomized
controlled trial. J Orthop Sports
Phys Ther 27:134–143, 1998.
2. 2Bellamy N, Buchanan WW,
Goldsmith CH, Campbell J, Stitt
Vol.1 No.4 2012 Scientific Research Journal of India 17
http://www.srji.co.cc
LW: Validation study of WOMAC:
A health status instrument for
measuring clinically important
patient relevant outcomes to
antirheumatic drug therapy in
patients with osteoarthritis of hip
or knee. J Rheumatol 15:1833–
1840, 1988.
3. De Carlo MS, Sell KE: The effects
of the number and frequency of
physical therapy treatments on
selected outcomes of treatment in
patients with anterior cruciate
ligament reconstruction. J Orthop
Sports Phys Ther 26:332–339,
1997.
4. Fischer DA, Tewes DP, Boyd JL,
et al: Home based rehabilitation
for anterior cruciate ligament
reconstruction. Clin Orthop
347:194–199, 1998.
5. Forster DP, Frost CEB: Cost-
effectiveness of outpatient
physiotherapy after medial
menisectomy. BMJ 284:485–487,
1982.
6. Insall JN, Dorr L, Scott RD, Scott
WN: Rationale of the Knee
Society clinical rating system. Clin
Orthop 248:13–14, 1989.
7. Jokl P, Stull PA, Lynch JK,
Vaughan V: Independent home
exercise versus supervised
rehabilitation following
arthroscopic knee surgery: A
prospective randomized trial.
Arthroscopy 5:298–305, 1989.
8. Mahomed NN, Koo See Lin MJ,
Levesque L, Lan S, Bogoch ER:
Determinants and outcomes of
inpatient versus home-based
rehabilitation following elective
hip and knee replacement. J
Rheumatol 27:1753–1758,2000.
9. Rene J, Weinberge M, Mazzuca
SA, Brandt KD, Katz BP:
Reduction of joint pain in patients
with knee osteoarthritis who have
received monthly telephone calls
from lay personnel and whose
medical treatment regimens have
remained stable. Arthritis Rheum
35:511–515, 1992.
10. Seymour N: The effectiveness of
physiotherapy after medial
menisectomy. Br J Surg 56:518–
520, 1969.
11. Treacy SH, Baron OA, Brunet ME,
Barrack RL: Assessing the need

for extensive supervised
rehabilitation following
arthroscopic reconstruction. Am J
Orthop 26:25–29, 1997.
12. Ware JE, Sherbourne CD: The
Medical Outcomes Study Short
Form (SF-36). Med Care 3:473,
1992. Clinical Orthopaedics 234
Kramer et al and Related Research
ACKNOWLEDGMENT:
The authors thank Dharam Pandey (MPT-neuro), Deepa Dabas (MSc-psycho) for assistance
throughout the study.
CORRESPONDENCE:
*Bijender Sindhu PhD,PT Research Student**Dr.Manoj Sharma, MBBS, MS(ortho)***Dr.Raj k Biraynia,
MBBS, D.ortho *School of Physical Therapy, Faculty of Medical Science, Singhania University**Department
of orthopedic surgery, Jaipur Golden Hospital *** Department of orthopedic surgery, Sarvodaya
Multispeciality Hospital. This study was not funded through a grant from the any organization.

Vol.1 No.4 2012 Scientific Research Journal of India 19
http://www.srji.co.cc
Electrical Muscle Stimulation (EMS) Improve Functional Independence in
Critically Ill Patients
Dharam Pani Pandey PT*, Dr. Uday Shankar Sharma**,Dr. Ram Babu***
Abstract: Objective. This study was designed to investigate the effects of
electrical muscle stimulation (EMS) on strength of muscle groups stimulated and
improvement in functional independence in critically ill patients .Methods. 134
subjects were recruited among the patient admitted in multidisciplinary intensive
care units and randomly divided in to control and EMS group. Patients unable to
understand or speak English and or Hindi due to language barrier or cognitive
impairment prior to admission, unable to transfer from bed to chair at baseline
prior to hospital admission, Patient with known history of primary systemic
neuromuscular disease were excluded from study. Results. EMS group patients
achieved higher MRC scores than controls in knee extensors and ankle
dorsiflexors. Independence level was higher in EMS group Conclusions. EMS
application constitutes a promising means of muscle strength preservation and
early mobilization which can directly reflects the gain in functional independence
post ICU discharge in critically ill patients.
Key words: Electrical muscle stimulation, muscle strength, CIPNM, CIM,
functional independence
INTRODUCTION Weakness that is acquired during
hospitalization for critical illness is
increasingly recognized as common and
important clinical problem. Weakness
acquired in the intensive care unit (ICU)
and related acquired neuromuscular
dysfunction occur in a large percentage of
critically ill patients1–3 and are associated
with increased morbidity and mortality.4,5
Critical illness polyneuromyopathy
(CIPNM) is an acquired neuromuscular
disorder observed in survivors of acute
critical illness. It is characterized by
profound muscle weakness and
diminished or absent deep tendon
reflexes1 and is associated with delayed
weaning from mechanical ventilation
suggesting a possible relation between
limb and respiratory neuromuscular
involvement. In addition, the syndrome is
associated with prolonged hospitalization
and increased mortality.3 The diagnosis of
CIPNM requires a reliable bedside muscle
strength examination and depends on
patient's cooperation and maximal effort.
Several risk factors have been identified
including systemic inflammatory response
and sepsis5, medications such as
corticosteroids6 and neuromuscular
blocking agents7, inadequate glycemic
control8, protracted immobility
hypoalbuminemia9, Gram-
bacteremia9 and severity of organ
dysfunction.10 Thus, looking for the
potentially reversible risk factors and
subsequent adjustment of therapy are so
far advocated as preventive measures to
decrease the risk of CIPNM.
A very few of studies available suggesting
the treatment and prevention of critical
illness myopathy these includes intensive
insulin therapy, optimal gycemic control
and minimized use of neuromuscular
blocking agents, high dose and prolong
use of corticosteroids.
OBJECTIVE OF THE STUDY
diminished or absent deep tendon
and is associated with delayed
weaning from mechanical ventilation2
suggesting a possible relation between
limb and respiratory neuromuscular
involvement. In addition, the syndrome is
associated with prolonged hospitalization
The diagnosis of
eliable bedside muscle
strength examination and depends on
patient's cooperation and maximal effort.4
Several risk factors have been identified
including systemic inflammatory response
, medications such as
and neuromuscular
, inadequate glycemic
, protracted immobility4,
-negative
and severity of organ
Thus, looking for the
potentially reversible risk factors and
subsequent adjustment of therapy are so
advocated as preventive measures to
A very few of studies available suggesting
the treatment and prevention of critical
illness myopathy these includes intensive
insulin therapy, optimal gycemic control
uromuscular
blocking agents, high dose and prolong
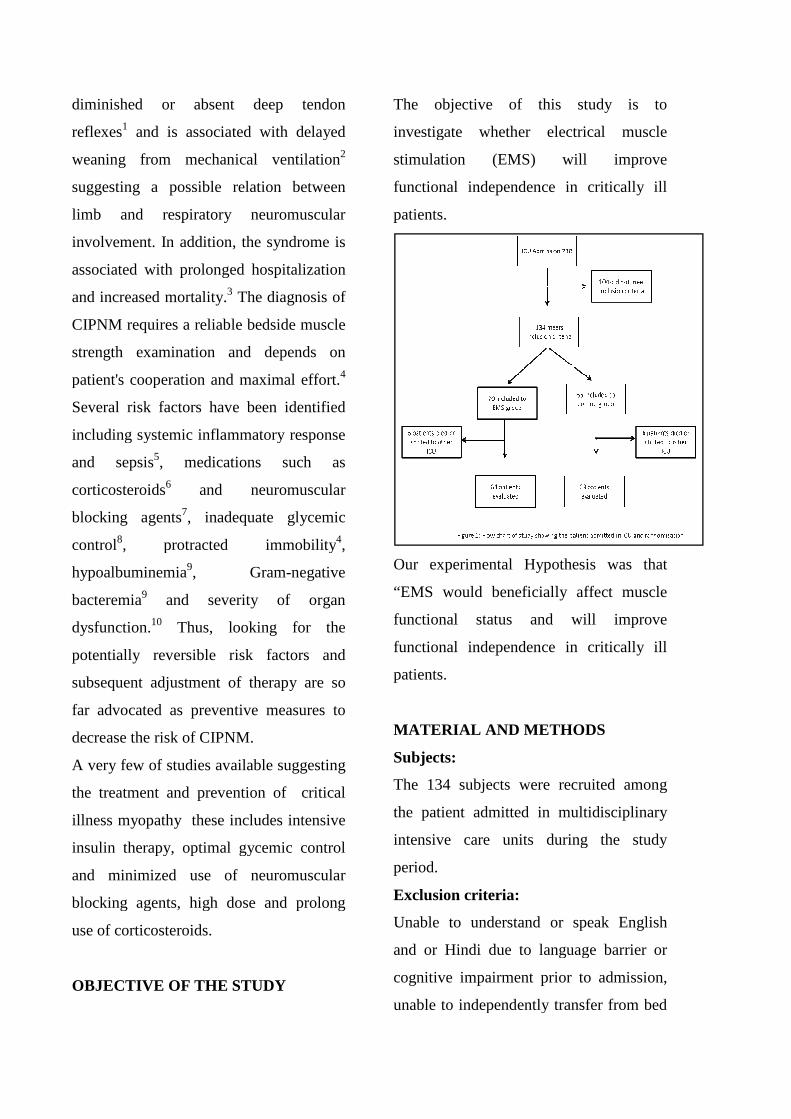
The objective of this study is to
investigate whether electrical muscle
stimulation (EMS) will improve
functional independence in critically ill
patients.
Our experimental Hypothesis was that
“EMS would beneficially affect muscle
functional status and will improve
functional independence in critically ill
patients.
MATERIAL AND METHODS
Subjects:
The 134 subjects were recruited among
the patient admitted in multidisciplinary
intensive care units during the study
period.
Exclusion criteria:
Unable to understand or speak English
and or Hindi due to language barrier or
cognitive impairment prior to admission,
unable to independently transfer from bed
The objective of this study is to
investigate whether electrical muscle
stimulation (EMS) will improve
functional independence in critically ill
Our experimental Hypothesis was that
“EMS would beneficially affect muscle
functional status and will improve
functional independence in critically ill
MATERIAL AND METHODS
The 134 subjects were recruited among
n multidisciplinary
intensive care units during the study
Unable to understand or speak English
and or Hindi due to language barrier or
cognitive impairment prior to admission,
unable to independently transfer from bed

Vol.1 No.4 2012 Scientific Research Journal of India 21
http://www.srji.co.cc
to chair at baseline prior to hospital
admission (based on detail history taken
from caregivers. Patient with known
history of primary systemic
neuromuscular disease, vascular events,
organ transplant, intracranial process that
is associated with localizing weakness,
transferred from another ICU after >2
consecutive days of mechanical
ventilation, amputation of lower
extremities, any limitation of life support,
pregnancy, age under 18 years, obesity,
technical obstacles that did not allow the
implementation of EMS such as bone
fractures, skin lesions and, end-stage
malignancy were excluded from our study
Design of study:
The study employed a randomized single
blind controlled experimental study design
consisting of two group experimental
group and control group, Subjects were
randomly assigned ether to experimental
group or to control group everyday the
ICU patient admission register were
observed and with in 24 hour the
assessment were done , each time when a
patient met the criteria for inclusion a
random number were picked up between 1
to 10 using sealed envelope method if it
were an odd number than the subject were
assigned to experimental group similarly
if it even number were obtained the
subjects were assigned to control group.
Intervention:
EMS was implemented on knee extensors,
tibialis anterior and of both lower
extremities. Patients received daily
sessions. After skin cleaning, rectangular
electrodes (90 × 50 mm) were placed on
motor point of targeted muscle. The
stimulator (Unistim, HMS medical system)
delivered biphasic, symmetric impulses of
50 Hz, 100 µsec pulse duration, 12
seconds at intensities able to cause visible
contractions. The duration of the session
was 30 minutes each muscle group. EMS
sessions were continued until ICU
discharge, both group were getting routine
physiotherapy included the passive
movements, active assisted movements
and chest physiotherapy.
Outcome Measures:
Primary Outcome Measures were the
score of barthel index, it is reliable and
valid outcome measure used to assess
functional independence.
Secondary Outcome Measures were lower
extremity strength, at ICU discharge, of 2
bilateral muscle groups which were
stimulated measured by MMT using a
composite Medical Research Council
(MRC) score.
DATA ANALYSIS AND RESULTS
All continuous variables were presented
by mean. The statistical significance of P
value was set at 0.05. One-way repeated
measures analysis of variance (ANOVA)

was made to compare MRC Grading and
barthel index score between-group. Two
hundred and thirty-eight patients were
admitted to our multidisciplinary ICU
during the eight-month study period and
104 patients fulfilled the exclusion criteria
or stayed in the ICU less than 48 hours.
The study population consisted of 134
patients of which of these patients, 70
were randomly assigned to the EMS group
and 64 to the control group. 6 patients
from EMS group and 1 patient from
control died or were discharged from the
ICU before the second measurement.
MRC muscle grading score of muscle
group being stimulated were for left knee
extensors were control group mean 3.49
and EMS group mean 3.91 (p = 0.0187),
right knee extensors control group mean
3.69 and EMS group mean 3.87 (p =
0.0387). left ankle dorsiflexors control
group mean 3.78 and EMS group m
3.91 (p = 0.04), right ankle dorsiflexors
were observed as follows mean control
group mean 3.37 and EMS group mean
3.3.46 (p = 0.0587) found.
Barthel index score of control group was
(mean) 68.6 and EMS group (mean) 71.9
and found significant between groups (p =
0.010).
was made to compare MRC Grading and
group. Two
eight patients were
admitted to our multidisciplinary ICU
month study period and
104 patients fulfilled the exclusion criteria
or stayed in the ICU less than 48 hours.
The study population consisted of 134
hese patients, 70
were randomly assigned to the EMS group
and 64 to the control group. 6 patients
from EMS group and 1 patient from
control died or were discharged from the
ICU before the second measurement.
MRC muscle grading score of muscle
stimulated were for left knee
extensors were control group mean 3.49
and EMS group mean 3.91 (p = 0.0187),
right knee extensors control group mean
3.69 and EMS group mean 3.87 (p =
0.0387). left ankle dorsiflexors control
group mean 3.78 and EMS group mean
3.91 (p = 0.04), right ankle dorsiflexors
were observed as follows mean control
group mean 3.37 and EMS group mean
Barthel index score of control group was
(mean) 68.6 and EMS group (mean) 71.9
een groups (p =
Graph 1: Showing the mean and significance level of two group of left and right knee extensor.
Graph 2: Showing the mean and significance level of two group of left and right ankle dorsiflexors.
Graph 3: Showing the mean andsignificance level functional independence level as assessed on barthel index.
DISCUSSION
The main finding of our randomized
controlled study is that EMS of lower
extremities seems to preserve the muscle
Graph 1: Showing the mean and significance level of two group of left and
Graph 2: Showing the mean and significance level of two group of left and
Graph 3: Showing the mean and significance level functional independence level as assessed on barthel index.
The main finding of our randomized
controlled study is that EMS of lower
extremities seems to preserve the muscle
Vol.1 No.4 2012 Scientific Research Journal of India 23
http://www.srji.co.cc
strength of critically ill patients as
assessed with MRC muscle strength
grading system. EMS of lower extremities
applied to critically ill patients upon
admission is associated with a lesser
degree of muscle strength loss of these
patients as assessed with MRC muscle
strength grading system. barthel index
score were higher in EMS group and the
patient of EMS group were more
independent.
Electrical stimulation has been used to
increase strength and endurance in
partially and fully paralyzed muscle. It has
been used for peroneal nerve stimulation10,
11 the restoration of shoulder movement12,
recovery of tendonesis grip13, and in the
use of an upper arm prosthesis.14
Electrical muscle stimulation (EMS) has
been used as an alternative to active
exercise in patients with chronic heart
failure (CHF)15 and chronic obstructive
pulmonary disease (COPD).16, 17 Many of
these patients, even those who are
clinically unstable, experience severe
dyspnea on exertion, which can prohibit
the regular application of conventional
exercise training, considered necessary for
an integrated therapeutic approach. In a
recent systematic review, EMS
implementation in most of the selected
controlled clinical trials produced
significant improvements in muscle
strength, exercise capacity and disease-
specific health status.18 Recently, an study
identified an acute systemic effect exerted
by EMS on peripheral microcirculation of
critically ill patients.19 Specifically, after
performing a 45-minute session of EMS
on the lower extremities, an improvement
in the microcirculation of the thenar
muscle as assessed by near infrared
spectroscopy technique was observed.
EMS, as a possible substitute to aerobic
and resistance exercise training in severe
CHF and COPD patients, has been shown
to improve muscle performance, aerobic
exercise capacity, and disease-specific
health status.9-11
CONCLUSIONS
EMS exercise induces beneficial effects in
muscle strength of ICU patients. These
effects mainly concern muscle groups
directly stimulated, but there is also
evidence of effects in muscle groups not
stimulated. EMS application constitutes a
promising means of muscle strength
preservation and early mobilization which
can directly reflects the gain in functional
independence post ICU discharge in
critically ill patients.
Clinical relevance & limitation
EMS is an alternative method of exercise
causing minimal discomfort to patients
who are not able to perform any form of
physical exercise, as is often the case in
critically ill patients. It is a limitation of
this study that it did not evaluated the
follow up stage and upper extremities
function. Further studies are needed to
explore the possible role of EMS as a tool
for preserving the muscle strength and
gain in functional independence post ICU
discharge with longer follow up
evaluation, the muscle properties and
preventing CIPNM in critically ill patients
and to define which patients would benefit
most from this intervention.
REFERENCES:
1. De Jonghe B, Sharshar T,
Lefaucheur JP, Authier FJ,
Durand-Zaleski I, Boussarsar M, et
al; Groupe de Reflexion et d’Etude
des Neuromyopathies en
Reanimation. Paresis acquired in
the intensive care unit: a
prospective multicenter study.
JAMA 2002;288(22):2859–2867.
2. De Letter MA, Schmitz PI, Visser
LH, Verheul FA, Schellens RL,
Op de Coul DA, van der Meche
FG. Risk factors for the
development of polyneuropathy
and myopathy in critically ill
patients. Crit Care Med
2001;29(12):2281–2286.
3. Coakley JH, Nagendran K,
Yarwood GD, Honavar M, Hinds
CJ. Patterns of neurophysiological
abnormality in prolonged critical
illness. Intensive Care Med
1998;24(8):801–807.
4. Garnacho-Montero J, Madrazo-
Osuna J, Garcia-Garmendia JL,
Ortiz- Leyba C, Jimenez-Jimenez
FJ, Barrero-Almodovar A, et al.
Critical illness polyneuropathy:
risk factors and clinical
consequences: a cohort study in
septic patients. Intensive Care Med
2001;27(8): 1288–1296.
5. Spitzer AR, Giancarlo T, Maher L,
Awerbuch G, Bowles A.
Neuromuscular causes of
prolonged ventilator dependency.
Muscle Nerve 1992;15(6):682–686.
6. Rudis MI, Guslits BJ, Peterson EL,
Hathaway SJ, Angus E, Beis S,
Zarowitz BJ. Economic impact of
prolonged motor weakness
complicating neuromuscular
blockade in the intensive care unit.
Crit Care Med 1996;24(10):1749–
1756.
Vol.1 No.4 2012 Scientific Research Journal of India 25
http://www.srji.co.cc
7. Latronico N, Peli E, Botteri M.
Critical illness myopathy and
neuropathy. Curr Opin Crit Care
2005;11(2):126–132.
8. Bednarik J, Lukas Z, Vondracek P.
Critical illness polyneuromyopathy:
the electrophysiological
components of a complex entity.
Intensive Care Med
2003;29(9):1505–1514.
9. Van den Berghe G, Wouters P,
Weekers F, Verwaest C,
Bruyninckx F, Schetz M, et al.
Intensive insulin therapy in the
critically ill patients. N Engl J Med
2001;345(19):1359–1367.
10. Tennila A, Salmi T, Pettila V,
Roine RO, Varpula T, Takkunen O.
Early signs of critical illness
polyneuropathy in ICU patients
with systemic inflammatory
response syndrome or sepsis.
Intensive Care Med
2000;26(9):1360–1363.
11. Rabuel C, Renaud E, Brealey D,
Ratajczak P, Damy T, Alves A, et
al. Human septic myopathy:
induction of cyclooxygenase,
heme oxygenase and activation of
the ubiquitin proteolytic pathway.
Anesthesiology 2004;101(3):583–
590.
12. MacFarlane IA, Rosenthal FD.
Severe myopathy after status
asthmaticus (letter). Lancet
1977;2(8038):615.
13. Witt NJ, Zochodne DW, Bolton
CF, Grand’Maison F, Wells G,
Young GB, Sibbald WJ. Peripheral
nerve function in sepsis and
multiple organ failure. Chest
1991;99(1):176–184.
14. Knox AJ, Mascie-Taylor BH,
Muers MF. Acute hydrocortisone
myopathy in acute severe asthma.
Thorax 1986;41(5):411–412.
15. Hund E, Genzwurker H, Bohrer H,
Jakob H, Thiele R, Hacke W.
Predominant involvement of motor
fibres in patients with critical
illness polyneuropathy. Br J
Anaesth 1997;78(3):274–278.
16. Thiele RI, Jakob H, Hund E,
Tantzky S, Keller S, Kamler M, et
al. Sepsis and catecholamine
support are the major risk factors
for critical illness polyneuropathy
after open heart surgery. Thorac

Cardiovasc Surg 2000;48(3):145–
150.
17. Garnacho-MonteroJ, Amaya-Villar
R, Garcia-Garmendia JL,Madrazo-
Osuna J, Ortiz-Leyba C. Effect of
critical illness polyneuropathy on
the withdrawal from mechanical
ventilation and the length of stay
in septic patients. Crit Care Med
2005;33(2):349–354.
18. Bolton CF. Sepsis and the
systemic inflammatory response
syndrome: neuromuscular
manifestations. Crit Care Med
1996;24(8): 1408–1416.
ACKNOWLEDGMENT:
We would like also to acknowledge the support of all intensive care unit staff, consultants
and all the patients caregivers.
CORRESPONDENCE:
*Department Of Physiotherapy & Rehabilitation,BLK Super Speciality Hospital, Pusa Road, New Delhi, India.
**Sr. Consultant Neurologist, Department of Neurology, Jaipur Golden Hospital,2 institutional area, sector 3,
Rohini, New Delhi, India. ***Sr. Consultant Physician, Department of Internal, Medicine, Jaipur Golden
Hospital,2 institutional area, sector 3, Rohini, New Delhi, India.

Vol.1 No.4 2012 Scientific Research Journal of India 27
http://www.srji.co.cc
A Comparative Study on Supervised Clinical Exercise versus Home Based
Exercise in Primary Unilateral Total Knee Arthroplasty
Bijender Sindhu PhD, PT*, Dr.Manoj Sharma, MBBS, MS(Ortho)**, Dr.Raj K Biraynia, MBBS,
D.Ortho***
Abstract: Objective. This study was designed to investigate the effects of
supervised clinical exercise and home Based Exercise in patient with unilateral
total knee arthroplasty in sub acute phase (after 5-6 weeks of discharge). To
assess the effect on function ability of patient after primary unilateral total knee
arthroplasty. To assess the effect on knee integrity (it include pain, ROM, knee
stability)of patient after primary unilateral total knee arthroplasty. Methods. 130
subjects were recruited from OPD physiotherapy among the patient discharge
from hospital and randomly divided into supervised clinic exercise and home
based exercise. Socio demographic and clinical data, pain, range of movement
(ROM) and function of TKA patients were collected on day of discharge (ie day 5
to 8 post operation). A self designed data capture sheet, the goniometer, VAS
(Visual Analogue Scale) and ILOA (Iowa Level of Assistance) KSKS (kne society
knee score)were used to measure data. Criteria for recruitment is patient having
primary unilateral total knee replacement, having a functional hip on operated
side, both male and female and age between 50 to 80 years. Able to follow simple
verbal commands. Patient excluded from study who are suffering from
Rheumatoid Arthritis, revision TKA, bilateral knee arthroplasty. Results. The
results indicate that there is significant difference between experimental group
(supervised clinical exercise) and Control group (home based exercise). For knee
integrity measured using the Knee Society Knee Score (p=0.017)and function
measured using the ILOA Scale (p= 0.018) and goniometry (p=>0.05). The
average age was 64 years in male and 66 years in females . There were 41%
males and 59% females. There is statistical difference between pain, range of
motion, Knee integrity, Knee functional outcomes of groups that receive post-

discharge outpatient physiotherapy as compared to those who do not attend
physiotherapy. Conclusions. After primary total knee arthroplasty, patients who
completed a home based exercise program (control group) performed similarly to
patients who completed regular outpatient clinic sessions in addition to the home
exercises (supervised clinic exercise ie. experimental group). Additional studies
need to determine which patients are likely to benefit most from clinic-based
rehabilitation programs. The overall aim of this study was to establish the early
post operative status of Total knee arthroplasty patient.
Key words: Supervised clinical exercise, Home based exercise, KSKS (knee
society knee score), ILOA (ILOA level of assistance)
INTRODUCTION Osteoarthritis is a leading cause of pain
and disability affecting joints (Marchet al
1999). Progressive loss of the articular
cartilage can result in joints that are
painful and inflamed. The joint becomes
stiffer and there is less stability in the joint
(Parmet et al 2003). These factors affect
the function of the joint which ultimately
impacts on patients’ functional ability and
their quality of life (March et al 1999).
Total knee arthroplasty has been found to
be effective in the management of pain
(Palmer & Cross, 2004), functional status
and quality of life in people suffering from
OA, rheumatoid arthritis (RA) and related
conditions (Zavadak et al., 1995).
Physiotherapists aim to prevent
contractures (Lenssen et al., 2006)
decrease pain and swelling and improve
knee and functional mobility in
preparation for discharge (Oldmeadow et
al.,2002. Post operative physiotherapy
aims to minimize the complications
following total knee replacements and to
rehabilitate the patient to full functional
recovery. Techniques such as cryotherapy,
strengthening and stretching exercises are
used (Zavadak et al 1995). Physiotherapy
in hospital also includes functional
techniques such as bed mobility, transfers,
ambulation and stair climbing. An
assumption can be made that if there is a
relationship between knee integrity and
function, physiotherapists may decide to
only work on improving function, or only
work on improving knee integrity
(improving knee range of motion,
reducing swelling, reducing pain and
improving muscle strength). Time could
then be better utilized on one aspect of
rehabilitation.
Early discharge can sometimes result in
transfer to an inpatient facility. A study by
Bozic et al. (2006), states that clinical,

Vol.1 No.4 2012 Scientific Research Journal of India 29
http://www.srji.co.cc
demographic and socioeconomic factors
all affect the decision to discharge a
patient to an inpatient rehabilitation centre.
Objective of the Study:
To assess the effect on knee integrity (it
include pain, ROM and knee stability) and
knee function ability. To establish
pain,ROM of the operated knee and
functional level of TKA patients. To
establish socio-demographic factors and
clinical data of TKA patients on first
follow up. To establish the relationship
amongst supervised clinical exercise as
well as home based exercise and
postoperative functional status of TKA
patients. To study this procedure can be
clinically implemented.
MATERIAL AND METHODS
Subjects: 130 subjects were recruited
from OPD physiotherapy among the
patient discharge from hospital and
randomly divided into supervised clinic
exercise and home based exercise.
Inclusion criteria:
Patient having primary unilateral total
knee replacement having a functional hip
on operated side .Both male and female
who had a primary unilateral TKA able to
give independent informed consent Patient
between the age of 50 to 80 years of age,
presented to the first follow-up session.
(This was around six to eight weeks post
operation who gave informed
constant).Able to follow simple verbal
commands
Exclusion criteria:
Any additional trauma to the lower limb,
inability to participate in the assessment
from a physical and cognitive point of
view such as dementia, confusion etc.
Inability of the patient to walk prior to the
TKA(with or without aid). Patient
suffering from Rheumatoid Arthritis.
Unwillingness to participate in the
assessments Revision TKA, Bilateral knee
arthroplasty. Inability of the patients to
walk prior to the total knee replacement
(with or without the aid of an assistive
device).
Design of study:
The study employed a randomized single
blind controlled experimental study design
consisting of two group experimental
group and control group, Subjects were
randomly assigned either to experimental
group or to control group everyday in
physiotherapy OPD before discharge ,
each time when a patient met the criteria
for inclusion a random number were
picked up between 1 to 10 using sealed
envelope method if it were an odd number
than the subject were assigned to
experimental group.

Intervention
Supervised clinical exercise: These are
exercise which are perfomed by patient
under the observation of a qualified
physiotherapist. Postoperative
rehabilitation usually consists of passive
and active knee mobilisation, quadriceps
strengthening and functional activities
(Lenssen et al., 2006). Hip and knee
flexion; hip and knee extension in neutral;
hip abduction; hip adduction to neutral;
ankle dorsi- and plantar flexion, static
quadriceps contraction and inner range
quadriceps contraction over a rolled up
towel. The physiotherapist performs anti-
inflammatory modalities on the patient
which include ultrasound, interferential
therapy, pulsed short wave diathermy,
transcutaneous electrical nerve stimulation
(TENS), laser, acutouch and heat or
cryotherapy. Myofascial release,
continuous passive mobilisation exercises,
stretching, strengthening exercises, gait
re-training, massage, patient education
and an exercise programme are also
prescribed.
Home based exercise: Home based
exercise group performed the exercise
which are explained and demonstrated by
physiotherapist in OPD at the time of
discharge to the patient for home, which
included isometric exercises for
quadriceps, knee range of motion,
strengthening exercise, effective use of
assistive devices and appliance, walking
pattern, safety & precaution, do’s and
dont’s.
Outcome Measures:
ILOA : The patients’ functional ability
was assessed using the Iowa Level of
Assistance (ILOA) Scale, which was first
described by Shields et al (1995). It was
shown to be reliable and valid.The best
overall result the patient is able to achieve
with this scale is zero. This indicates that
the patient was able to perform all five
tasks independently without the use of any
assistive device. The worst overall score
that could be achieved is fifty which
indicates that the patient was unable to
perform the tasks due to medical and
safety reasons and the assistive device
used for standing or mobilizing was a
walking frame.
KSKS: This rating system was developed
in 1989 by the American Knee Society to
provide an evaluation form for knee
integrity (Insall et al, 1989). The knee
assessment has three parameters which
measure pain, stability and range of
motion. The knee is given a score out of a
hundred. A well-aligned knee with no pain,
negligible instability and range of motion
of 125 degrees scores a hundred points
Goniometry: It is a measuring tool used to
assess the range of motion of a joint. It
can be used as an initial assessment and it

Vol.1 No.4 2012 Scientific Research Journal of India 31
http://www.srji.co.cc
evaluate the patient’s progress (Rothstein
et al 1983). Rothstein et al (1983) assessed
goniometric reliability and which
goniometer size was the most reliable in a
clinical setting.
DATA ANALYSIS AND RESULTS
All continuous variables were presented
by mean. The statistical significance of P
value was set at 0.05.
One-way repeated measures analysis of
variance (ANOVA) was made to compare
ILOA score, KSKS score, Goniometry
range between-groups.
130 subjects were recruited from OPD
physiotherapy among the patient
discharge from hospital and randomly
divided into supervised clinic exercise and
home based exercise. 19 patients not
fulfilled the inclusion criteria and four
patients due to prolonged hospital stay for
medical reasons, two patients for medical
conditions, two patient consented to the
socio demographic and clinical
questionnaire, but not to the goniometry
and Iowa Level of Assistance (ILOA)
testing, and therefore had to be excluded.
One patient refused to be tested · two
patient had been discharged before the
researcher had been able to collect data
(morning of day three).
The following results are presented:
Range of movement (ROM) of the
operated knee and functional level of
TKA patients, Knee integrity and Socio-
demographic factors and clinical data of
TKA patients, The relationship between
identified factors and postoperative
functional status of TKA patients in
relevance of level of assistance (ILOA) in
control group mean (home based exercise)
is11.94 and experimental group
(supervised clinical exercise) 10.01 (p=
0.018), KSKS in control group mean
(home based exercise) is74.72 and
experimental group (supervised clinical
exercise) 76.78 (p=0.017), goniometry in
control group mean (home based exercise)
is 88.06 and experimental group
(supervised clinical exercise) 95.52
(p=>0.05) found.
Graph 1: Showing the mean and significance level of range of motion of two group of supervised and home based exercise.
pre post
Home 30.46 88.06
Super 28.86 95.52
0.
50.
100.
150.
RO
M )
in d
eg
tre
e)
ROM Knee Flexion
pre post
Home 33.9 11.94
Super 32.9 10.1
0.
10.
20.
30.
40.
Lev
el
of
ass
iste
nce
ILOA

Graph 2: Showing the mean and significance level of IOLA(level of assistance) of two group of supervised and home based exercise.
Graph 3: Showing the mean and significance level of KSKS (knee society knee score) of two group of supervised and home based exercise.
DISCUSSION
KSKS: 1. Pain: Fifty percent of the
patients had virtually no pain at six weeks
post operation. The other fifty percent had
pain that ranged from occasional to severe
pain Two patients (4%) had severe pain.
This indicates that the patients’ pain is not
being managed well at home after
discharge. They are perhaps not given
physiotherapy modalities which are
healing in reducing pain. Cryotherapy and
simultaneous exercise is more effective in
reducing pain than icing alone. Icing and
compression also helps to reduce pain in
patients post surgery. Transcutaneous
Electrical Nerve Stimulation (TENS)
causes a reduction of pain in 93% of
patients who undergo surgery and the
TENS group of patients consumed less
pain medication. Interferential therapy has
been shown to reduce pain in patients at
intervals of 24-hours, 48-hours, 72- hours
and at one to eight weeks post operation
(Hubbard and Denegar 2004; Jensen et al
1985; Jarit et al 2003).
2: Range of motion: People normally
require knee flexion of 45º to 105º during
various activities of daily living. To
demonstrate a normal gait pattern, 65º of
flexion is required. To ascend and descend
stairs, 90º of flexion is needed and to go
from sitting to standing, 105º of flexion is
required (Miner et al 2003). From the
results of the range of movement shows
that experimental group (mean=95.52) and
control group (mean=88.06), one can
assume that 51% of the patients (twenty
six patients) would not be able to go from
sitting to standing as they only had knee
flexion of 80º. However, from our sample
of 50-patients, 24-patients (49%) who had
90º-100 of knee flexion were able to go
from sitting to standing independently
without any assistance or assistive devices.
Patients with less than 95º of knee flexion
had worse Goniometry scores (p<.0001).
Only patients with a very stiff knee will
have function that is really affected by
ROM. Their study identified 95º of knee
flexion as a clinically meaningful cut-off
point above which ROM does not limit a
patient’s normal activities after TKR.
However the long-term effects of this
limitation of ROM could be detrimental to
pre post
Home 18.16 74.72
Super 18.52 76.78
0.
50.
100.
Kn
ee
in
teg
rity
&
fun
ctio
n
KSKS

Vol.1 No.4 2012 Scientific Research Journal of India 33
http://www.srji.co.cc
the normal joints, because of the patients
over compensation when performing
activities of daily living.
3. Knee Stability and alignment: The
majority of the patients had normal
stability and alignment. This indicates that
the total score of the Knee Society Knee
Score in this sample is not really affected
by the components of stability and
alignment, but mainly by pain and ROM.
Malalignment of the prosthesis could
result in stiffness which although
uncommon is a disabling problem (Jerosh
and Aldawoudy 2007). Treatment of
malalignment could include manipulation
or revision arthroplasty (Bong and Di
Cesare 2004),which has been shown to be
successful in terms of post-operative
function(Miner et al 2003).
4. Knee Flexion contracture and extension
lag: A percentage of the patients in this
study had some degree of a flexion
contracture and some degree of an
extension lag at six weeks post operation.
This could indicate that attaining full knee
extension and flexion is not that important
when it comes to functional activities such
as going from sitting to standing, walking
and stair climbing, as these same patients
performed well when assessed using the
ILOA Scale. Functional range of motion is
between 45º and 105º (Miner et al 2003).
As long as the extension lag and the
flexion contracture do not interfere with
this range of motion, the patient should
manage functionally. Patients also
compensate when performing activities by
using the other leg or their arms to assist
with transfers. The quality of the
movement being performed is not
important to the patient, what is of
importance is completing the movement
by any means possible. The long term
effect of poor ROM and poor quality of
movement is that the normal joints take
excess strain and over a prolonged period,
there is an increased risk of developing
pain and discomfort in the normal joints
due to osteoarthritis.
ILOA Score:
Most of the patients were able to go from
lying to sitting, sitting to standing and
walking 4.57 meters independently, with
minimal assistance. The patients scored
very well in these three categories. This
indicates that the ILOA Scale is not a
sensitive enough functional measuring
tool when used at six weeks post operation.
It measures basic functional ability, not
higher function. It was developed to
determine whether patients who had had
total hip and knee replacements were
ready to be discharged from hospital
(Shield et al 1995). It is the role of
physiotherapists in the hospital to ensure
that patients are able to perform basic
transfers so that they will be independent
at home, after they are discharged from

hospital. Five patient did not use an
assistive device to perform the five
functional tasks. She did however require
nearby supervision for the walking, stairs
and the speed test. Two patients used a
walking frame at six weeks after the
operation. Only one patient was unable to
climb the stairs even with maximal
assistance
CONCLUSIONS
The goal of a TKA is to provide the
patient with a stable and painless knee
with sufficient ROM to perform ADL’s
(Gandhi et al., 2006). As many studies
only focused on the long-term status of
TKA patients (Aarons et al., 1996), this
study examined the short-term status. The
value of this is to furnish patients and the
therapist with knowledge of their acute
postoperative status and appropriate
rehabilitation programme that will
influence their prognosis. integrity which
was measured using the Knee Society
Knee Score and function as measured
using the ILOA Scale, six to eight weeks
post surgery on total knee replacement.
Research Recommendations:
A functional tool should be developed that
assesses the attainment of higher
functional milestones, as well as the
quality of the movement. If a more
sensitive functional assessment tool was
used, one that looked at higher functional
levels, a more accurate functional
evaluation of the knee replacement could
be determined.
REFERENCES:
1. De Jonghe B, Sharshar T,
Lefaucheur JP, Authier FJ, Durand-
Zaleski I, Boussarsar M, et al; Groupe
de Reflexion et d’Etude des
Neuromyopathies en Reanimation.
Paresis acquired in the intensive care
unit: a prospective multicenter study.
JAMA 2002;288(22):2859–2867.
2. de Letter MA, Schmitz PI, Visser
LH, Verheul FA, Schellens RL, Op de
Coul DA, van der Meche FG. Risk
factors for the development of
polyneuropathy and myopathy in
critically ill patients. Crit Care Med
2001;29(12):2281–2286.
3. Coakley JH, Nagendran K,
Yarwood GD, Honavar M, Hinds CJ.
Patterns of neurophysiological
abnormality in prolonged critical
illness. Intensive Care Med
1998;24(8):801–807.
4. Garnacho-Montero J, Madrazo-
Osuna J, Garcia-Garmendia JL, Ortiz-

Vol.1 No.4 2012 Scientific Research Journal of India 35
http://www.srji.co.cc
Leyba C, Jimenez-Jimenez FJ,
Barrero-Almodovar A, et al. Critical
illness polyneuropathy: risk factors
and clinical consequences: a cohort
study in septic patients. Intensive Care
Med 2001;27(8): 1288–1296.
5. Spitzer AR, Giancarlo T, Maher L,
Awerbuch G, Bowles A.
Neuromuscular causes of prolonged
ventilator dependency. Muscle Nerve
1992;15(6):682–686.
6. Rudis MI, Guslits BJ, Peterson EL,
Hathaway SJ, Angus E, Beis S,
Zarowitz BJ. Economic impact of
prolonged motor weakness
complicating
neuromuscular blockade in the
intensive care unit. Crit Care Med
1996;24(10):1749–1756.
7. Latronico N, Peli E, Botteri M.
Critical illness myopathy and
neuropathy. Curr Opin Crit Care
2005;11(2):126–132.
8. Bednarik J, Lukas Z, Vondracek P.
Critical illness polyneuromyopathy:
the electrophysiological components
of a complex entity. Intensive Care
Med 2003;29(9):1505–1514.
9. Van den Berghe G, Wouters P,
Weekers F, Verwaest C, Bruyninckx F,
Schetz M, et al. Intensive insulin
therapy in the critically ill patients. N
Engl J Med 2001;345(19):1359–1367.
10. Tennila A, Salmi T, Pettila V,
Roine RO, Varpula T, Takkunen O.
Early signs of critical illness
polyneuropathy in ICU patients with
systemic inflammatory response
syndrome or sepsis. Intensive Care
Med 2000;26(9):1360–1363.
11. Rabuel C, Renaud E, Brealey D,
Ratajczak P, Damy T, Alves A, et al.
Human septic myopathy: induction of
cyclooxygenase, heme oxygenase and
activation of the ubiquitin proteolytic
pathway. Anesthesiology
2004;101(3):583–590.
12. MacFarlane IA, Rosenthal FD.
Severe myopathy after status
asthmaticus (letter). Lancet
1977;2(8038):615.
13. Witt NJ, Zochodne DW, Bolton
CF, Grand’Maison F, Wells G, Young
GB, Sibbald WJ. Peripheral nerve
function in sepsis and multiple organ
failure. Chest 1991;99(1):176–184.

14. Knox AJ, Mascie-Taylor BH,
Muers MF. Acute hydrocortisone
myopathy in acute severe asthma.
Thorax 1986;41(5):411–412.
15. Hund E, Genzwurker H, Bohrer H,
Jakob H, Thiele R, Hacke W.
Predominant involvement of motor
fibres in patients with critical illness
polyneuropathy. Br J Anaesth
1997;78(3):274–278.
16. Thiele RI, Jakob H, Hund E,
Tantzky S, Keller S, Kamler M, et al.
Sepsis and catecholamine support are
the major risk factors for critical
illness polyneuropathy after open heart
surgery. Thorac Cardiovasc Surg
2000;48(3):145–150.
17. Garnacho-MonteroJ, Amaya-Villar
R, Garcia-Garmendia JL,Madrazo-
Osuna J, Ortiz-Leyba C. Effect of
critical illness polyneuropathy on the
withdrawal from mechanical
ventilation and the length of stay in
septic patients. Crit Care Med
2005;33(2):349–354.
18. Bolton CF. Sepsis and the
systemic inflammatory response
syndrome: neuromuscular
manifestations. Crit Care Med
1996;24(8): 1408–1416.
19. Latronico N, Fenzi F, Recupero D,
Guarneri B, Tomelleri G, Tonin P, et
al. Critical illness myopathy and
neuropathy. Lancet 1996;
347(9015):1579–1582.
ACKNOWLEDGMENT:
The authors thank Dharam Pandey (MPT-neuro), Deepa Dabas (MSc-psycho) for assistance
throughout the study.
CORRESPONDENCE:
*Bijender Sindhu PhD,PT Research Student**Dr.Manoj Sharma, MBBS, MS(ortho)***Dr.Raj k Biraynia,
MBBS, D.ortho *School of Physical Therapy, Faculty of Medical Science, Singhania University**Department
of orthopedic surgery, Jaipur Golden Hospital *** Department of orthopedic surgery, Sarvodaya
Multispeciality Hospital. This study was not funded through a grant from the any organization.

Vol.1 No.4 2012 Scientific Research Journal of India 37
http://www.srji.co.cc
Comparison of the Effect of Isometric Exercise of Upper Limb on Vitals
between Young Males and Females
Pranjal Parmar. BPT*
Abstract: Background and objective: studies on gender difference in
cardiovascular responses to isometric exercises have been numerous and
confliction the objective of this study was to determine if cardiovascular response
to upper extremities isometric exercises differ between apparently healthy male
and female subjects. Method: 60 young adults age between 18 to 22 years were
included in study. These consisted of 30 males and 30 females. The baseline
cardiovascular parameters (HR, SBP, DBP & MAP) were recorded. After two
sets of three isometric upper limbs for 3 minutes these parameters recorded at the
end of exercise and after recovery. Results:An increase in HR ,SBP , DBP&MAP
was seen in both groups after exercise .the result showed group B had more
increase in HR,SBP,DBP and MAP as compared to group A and significant rise
in MAP &SBP in group B. Conclusion: Isometric exercise of upper limb can lead
to increase in SBP, DBP, MAP &HR among apparently healthy males & females.
It is more proannounced in males as compared to females. SBP &MAP increased
in both but more in males as compared to females.
Keywords: Isometric Exercises, Cardiovascular Measures
INTRODUCTION Exercise, a common physiological stress,
can elicit cardiovascular abnormalities not
present at rest and can be used to
determine the adequacy of cardiac
function.1 The isometric contractions are
seen in various exercises like pushing or
lifting heavy load where net displacement
of load is not, but the rising tension can be
felt in contracting muscles.3 It imposes
greater pressure than volume load on left

ventricle in relation to the body ability to
supply oxygen.4 The metabolic demands
of the exercising muscles increases,
depending upon intensity of exercises and
are met with various changes in
circulatory and respiratory system.13
The effect of isometric exercises on vitals
in between males and females may vary
with substantial anatomical, physiological
and morphological differences that exist
between men and women which may
affect their exercise capacity and influence
magnitude of response to exercise.5
The average isometric strength estimate is
generally 30% greater in men than in
women in different muscle group. Gender
difference in cardiovascular response to
static exercise is believed to be due to
differences in sympathetic –
parasympathetic or adrenal interactions at
cardiac level.
The larger the muscle group that is
involved in isometric tension the greater
the cardiovascular response.6
Response To Exercise:7
When you exercise or take part in a
strenuous sport you will notice several
changes taking place in your body:
a. Your heart beats stronger and faster
b. Your breathing quickens and deepens
c. Your body temperature increases
d. You start to sweat
e. Your muscles begin to ache
1. Heart beats stronger and faster:
During exercise it is mainly adrenaline
that produces changes in the heartbeat.
Adrenaline is a hormone which causes the
heart rate to quicker.
2. Breathing quickens and deepens:
You breathe quicker so as to get more
oxygen into the lungs. An efficient heart
can then transport this to the working
muscles. Training can be of great benefit
to the Respiratory System. The capacity of
the lungs is increased, which allows more
oxygen to be taken in per breath.
3. Temperature rises:
When we exercise, our muscles are
working and they generate heat, so our
body temperature rises. Body temperature
is regulated by heat radiating from the
skin and water evaporating by sweating.
When we shiver, our muscles are working
to produce heat in order to raise our body
temperature.
4. Start to sweat:
As we have just seen, some of our energy
is turned into heat. The body will tolerate
a small rise in temperature, but very soon
we begin to sweat. If the conditions are
hot, we sweat more and produce less urine.
We also lose salt as well as body heat and
water. We have to replace the salt so that
the body stays the same, otherwise we will
get cramp.
5. Muscles begin to ache:
As we now know, in order to work,
muscles need energy. Energy comes from

Vol.1 No.4 2012 Scientific Research Journal of India 39
http://www.srji.co.cc
food, which is mainly converted to
glucose. To work more efficiently muscles
also need plenty of oxygen. Glucose and
oxygen are brought to the muscles in the
blood. Wastes such as carbon dioxide are
carried away in the blood. This process of
getting energy is called respiration.
Glucose + Oxygen = Energy + CO2 +
Water
When muscles do extra work more
Glucose and Oxygen are needed, so more
blood must flow to the muscles.
Eventually it becomes impossible to get
enough oxygen to the muscles, so they use
a different method of getting energy.
Glucose is still used, but now there is a
waste product called lactic acid, which
makes muscle ache, & muscles.
Acute Cardiovascular Response to
Exercise:
As exercise intensity increases, heart rate,
stroke volume, and cardiac output increase
to get more blood to the tissues. More
blood forced out of the heart during
exercise allows for more oxygen and
nutrients to get to the muscles and for
waste to be removed more quickly. Blood
flow distribution changes from rest to
exercise as blood is redirected to the
muscles and systems that need it.
CLINCAL SIGNIFICANCE
Vitals response to exercise has been used
as major criteria in exercise prescription
for both patient and healthy population.
Thus for prescribing isometric exercise,
repetitions and frequency it would be
helpful and prevent the adverse effect on
vitals. The study would also be helpful in
prescribing exercises for those with
cardiovascular compromise. It would help
to determine the safety limits of the
exercise.
OBJECTIVES:
1. To analyze if there is any change in
vitals as a result of isometric exercises of
upper limb
2. To compare the response of upper limb
isometric exercises in young male and
female.
METHODOLOGY
Research Design: An quasi-Experimental
(comparative) study. Sample Size: 60
normal individuals. Sample Population:
60 young adults between 18 to 22 yrs.
Group A: 30 normal individuals (females)
Group B: 30 normal individuals(males)
Type of Sampling: Convenient sampling
with random assignment. Duration of
Study: one month. Study Set Up:
Physiotherapy OPD of a tertiary care
hospital.
Inclusion Criteria:
• No previous history of known
cardiovascular condition.
• Normal values of vitals at rest.
• No neurological defecit in upper
limb.
• Sex – both male and female.
• Willingnessof patient.
Exclusion Criteria:
• Fracture of upper limb bones.
• Cervical vertebrae or scapula
fracture.
• Neurogenic deficit.
• Congenital anomalies.
• Previous exercise training
• Any disability limiting to upper
limb exercise.
• Psychiatric patients.
• Non-willing patients.
Outcome Measures:
• Heart rate of patient at rest,
immediately post exercise and 3
minutes after exercise
• Blood pressure i.e. systolic and
diastolic blood pressure at rest,
immediately postexercise and 3
minutes after exercise.
• Mean arterial pressure was
calculated from the above data.
PROCEDURE
60 individuals were selected according to
the inclusion and exclusion criteria. The
need of the study and treatment
intervention was explained to the
individuals and their written consent was
taken from them. 60 individuals were
assigned into two groups, group A and
group B, 30 patients in each group.
Procedure details of group A and group B:
Pre-measures: Heart rate and blood
pressure was measured using an electronic
sphygmomanometer in standing position.
Reading was noted.
Individual position: standing position.
Therapist position: on the individual side
in stride standing position.
Procedure: Participants in upstanding
position performed 3 upper extremities
isometric exercises i.e. 2 sets of each
exercise for each 30 second each thus total
duration of exercise for 3 minutes.
1. The exercise are pushing against the
wall with outstretched arms and were
instructed to exert maximal tension on
wall.8
2. Hands clasped together and brought to
manubrosternal level to chest while
shoulders are 60 70 degree abducted and
participants were instructed to maximally
generate tension by pressing opposite
hands against each other.8
3. Both palms on wall with participants
standing ahead arms extended and were
asked to push the wall without coming
behind and keeping elbow straight.8
Participants were instructed to avoid
valsalva maneuver by not holding breath
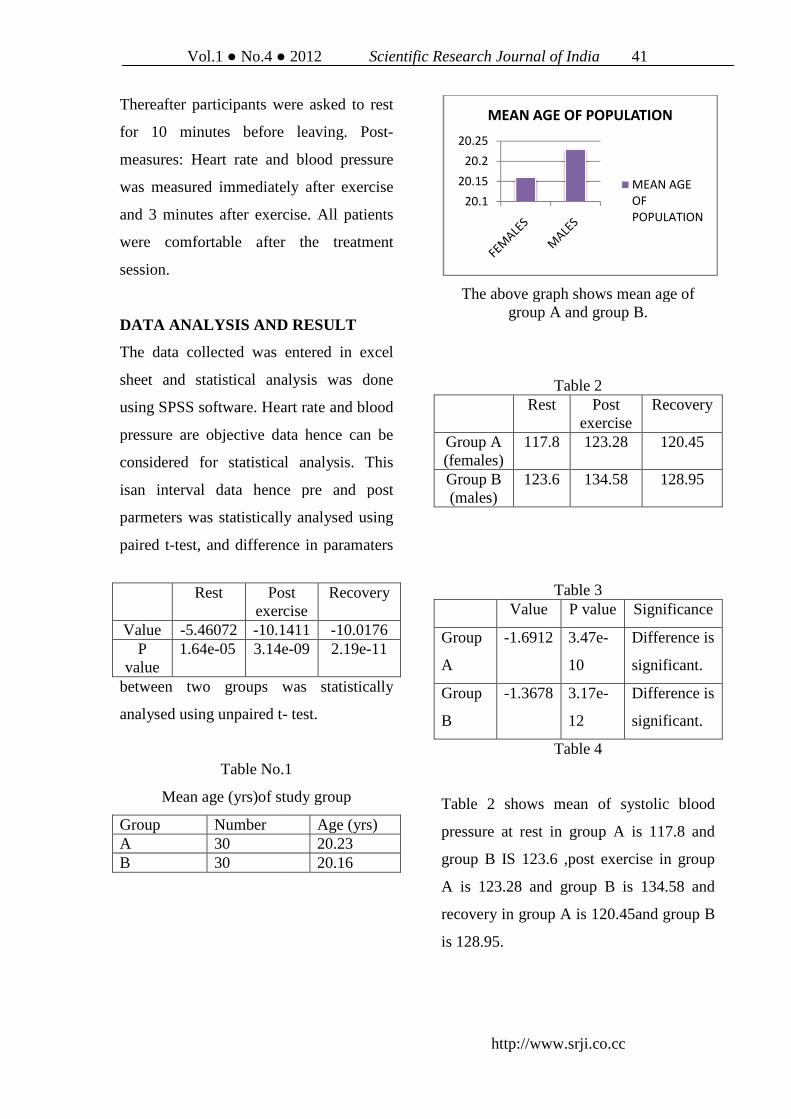
Vol.1 No.4
Thereafter participants were asked to rest
for 10 minutes before leaving.
measures: Heart rate and blood pressure
was measured immediately after exercise
and 3 minutes after exercise.
were comfortable after the treatment
session.
DATA ANALYSIS AND RESULT
The data collected was entered in excel
sheet and statistical analysis
using SPSS software. Heart rate and blood
pressure are objective data hence can be
considered for statistical analysis.
isan interval data hence pre and post
parmeters was statistically analysed using
paired t-test, and difference in paramate
between two groups was statistically
analysed using unpaired t-
Table No.1
Mean age (yrs)of study group
Group Number A 30 B 30
Rest Post exercise
Value -5.46072 -10.1411P
value 1.64e-05 3.14e
2012 Scientific Research Journal of India
http://www.srji.co.cc
Thereafter participants were asked to rest
for 10 minutes before leaving. Post-
Heart rate and blood pressure
was measured immediately after exercise
s after exercise. All patients
were comfortable after the treatment
DATA ANALYSIS AND RESULT
The data collected was entered in excel
sheet and statistical analysis was done
Heart rate and blood
pressure are objective data hence can be
considered for statistical analysis. This
isan interval data hence pre and post
parmeters was statistically analysed using
test, and difference in paramaters
between two groups was statistically
- test.
Table No.1
)of study group
Age (yrs) 20.23 20.16
The above graph shows mean age of group A and group B.
Table 2 Rest
Group A (females)
117.8
Group B (males)
123.6
Table 3 Value P
Group
A
-1.6912 3.47e
10
Group
B
-1.3678 3.17e
12
Table 4
Table 2 shows mean of systolic blood
pressure at rest in group A is 117.8 and
group B IS 123.6 ,post exercise in group
A is 123.28 and group B is 134.58 and
recovery in group A is 120.45and group B
is 128.95.
20.1
20.15
20.2
20.25
MEAN AGE OF POPULATION
Post exercise
Recovery
10.1411 -10.0176 3.14e-09 2.19e-11
Scientific Research Journal of India 41
http://www.srji.co.cc
The above graph shows mean age of group A and group B.
Table 2 Post
exercise Recovery
123.28 120.45
134.58 128.95
Table 3 P value Significance
3.47e-
10
Difference is
significant.
3.17e-
12
Difference is
significant.
Table 4
Table 2 shows mean of systolic blood
pressure at rest in group A is 117.8 and
group B IS 123.6 ,post exercise in group
A is 123.28 and group B is 134.58 and
in group A is 120.45and group B
MEAN AGE OF POPULATION
MEAN AGE
OF
POPULATION

Table 3 shows p value by paired t test in
group A and group B and difference is
statically significant.
Table 4 shows p value by unpaired t test in
group A and group B at rest, post exercise
and recovery and difference is statically
significant.
The graph shows mean of males and females of systolic blood pressure at rest ,
post exercise and recovery.
.
0
50
100
150
REST POST
EXERCISE
RECOVERY
SYSTOLIC BLOOD PRESSURE
0
0.05
0.1
0.15
0.2
102106110114118122126130
SYSTOLIC BLOOD PRESSURE
0
0.05
0.1
0.15
108112116120124128132136140
SYSTOLIC BLOOD PRESSURE - POST EXERCISE
Table 3 shows p value by paired t test in
group A and group B and difference is
Table 4 shows p value by unpaired t test in
group A and group B at rest, post exercise
difference is statically
The graph shows mean of males and females of systolic blood pressure at rest ,
post exercise and recovery.
The above graph shows distribution of
systolic blood pressure in males and
females at rest, post exercise and recovery.
Diastolic Blood Pressure
Table 5 Rest Post
exerciseGroup A (Females)
75.6 84.25
Group B (Males)
80 96.50
Table 6
Value P value Group
A -1.345 3.95e-
15 Group
B -1.236 3.21e-
08 Table 7
Rest Post exercise
Value -5.78263 -14.6703P
value 1.1e-06 3.14e-09
Table 5 shows mean of diastolic blood
pressure at rest in group A is 75.6 and
group B is 80, at post exercise in group A
is 84.25 and in group B is 96.50 and at
recovery in group A is 80.20 and group B
is 83.60.
RECOVERY
SYSTOLIC BLOOD PRESSURE
SYSTOLIC BLOOD PRESSURE - REST
Female
Male
POST EXERCISE
Female
Male
0
0.05
0.1
0.15
0.2
0.25
0.3
108110112114116118120122124126128
SYSTOLIC BLOOD PRESSURE
The above graph shows distribution of
systolic blood pressure in males and
exercise and recovery.
Diastolic Blood Pressure
Post exercise
Recovery
84.25 80.20
96.50 83.60
Significance Difference is significant.
Difference is significant.
Post exercise
Recovery
14.6703 -4.4098 09 1.58e-07
Table 5 shows mean of diastolic blood
pressure at rest in group A is 75.6 and
exercise in group A
is 84.25 and in group B is 96.50 and at
recovery in group A is 80.20 and group B
128130132
SYSTOLIC BLOOD PRESSURE - RECOVERY
Female
Male

Vol.1 No.4 2012 Scientific Research Journal of India 43
http://www.srji.co.cc
Table 6 shows p value by paired t test in
group A and group B and difference is
statistically significant.
Table 7 shows p value by unpaired t test at
rest, post exercise and recovery in group
A and group B and difference is
statistically significant
The above graph shows mean of males
and females of diastolic blood pressure at
rest, post exercise and recovery.
The above graph shows distribution of
diastollic blood pressure between males
and females at rest, post exercise and
recovery.
Mean Arterial Pressure
Table 8
Rest Post exercise
Recovery
Group A (Females)
89.66 97.26 93.61
Group B (Males)
94.53 109.19 98.71
Table 9 Value P value Significance
Group A
-1.327 5.78e-10
Difference is significant
Group B
-1.784 4.08e-12
Difference is significant.
Table 10
Table 8 shows mean of mean arterial
pressure at rest in group A is 89.66 and in
group B is 94.53,at post exercise in group
A is 97.26and in group B is 109.19 and at
recovery in group A is 93.61 and group B
is 98.71.
Table 9 shows p value by paired t test in
group A and group B difference is
statistically significant.
Table 10 shows p value by unpaired t test
at rest, post exercise and recovery in
group A and group and difference is
statistically significant.
020406080
100120
DIASTOLIC BLOOD PRESSURE
FEMALES
MALES
0
0.1
0.2
68 70 72 74 76 78 80 82 84 86 88
DIASTOLIC BLOOD PRESSURE - REST
Female
Male
0
0.1
0.2
74767880828486889092949698100102
DIASTOLIC BLOOD PRESSURE - POST EXERCISE
Female
Male
0
0.1
0.2
70 72 74 76 78 80 82 84 86 88 90 92
DIASTOLIC BLOOD PRESSURE - RECOVERY
Female
Male
Rest Post exercise
Recovery
Value -7.001 -9.57881 -7.17096 P value 1.16e-
09 1.91e-11 2.06e-09

The above graph shows mean of mean
arterial pressure at rest, post exercise and
recovery between group A and group B.
The above graph shows distribution of
mean arterial pressure between males and
females at rest, post exercise and recovery.
Heart Rate
Table 11 Rest Post
exercise Recovery
Group A (Females)
72.6 80.40 76.40
Group B (Males)
74.4 82.95 78.65
Table 12
Value P value Significance Group
A 0.00615 0.015E-
04 Difference is significant
Group B
0.00322 0.14E-05
Difference is significant
Table 13 Rest Post
exercise Recovery
Value 0.00123 0.00808 0.00055 P
value 0.012e-
06 0.080e-
05 0.055e-06
Table 11 shows mean of heart rate at rest
in group A is 72.6 and in group B is 74.4,
at post exercise in group A is 80.40 and in
group B is 82.95 and at recovery in group
A is 76.40 and in group B is 78.65.
Table 12 shows p value by paired t test in
group A and group B and difference is
statistically significant.
Table 13 shows p value by unpaired t test
at rest, post exercise and recovery in
group A and group B and difference is
statistically significant.
020406080
100120
MEAN ARTERIAL PRESSURE
FEMALES
MALES
0
0.05
0.1
0.15
0.2
80 90 100
MEAN ARTERIAL PRESSURE -REST
Female
Male
0
0.05
0.1
86889092949698100102104106108110112114116118
MEAN ARTERIAL PRESSURE - POST EXERCISE
Female
Male
0
0.05
0.1
0.15
0.2
82 84 86 88 90 92 94 96 98 100102104106
MEAN ARTERIAL PRESSURE - RECOVERY
Female
Male
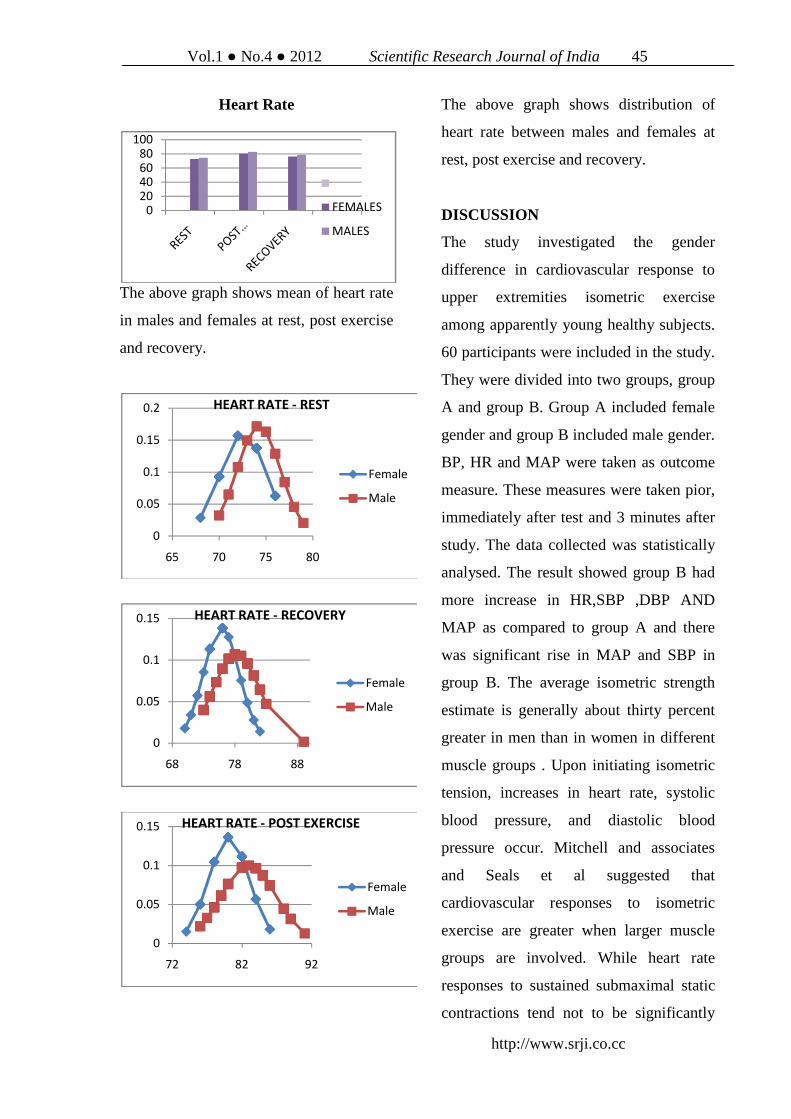
Vol.1 No.4 2012 Scientific Research Journal of India 45
http://www.srji.co.cc
Heart Rate
The above graph shows mean of heart rate
in males and females at rest, post exercise
and recovery.
The above graph shows distribution of
heart rate between males and females at
rest, post exercise and recovery.
DISCUSSION
The study investigated the gender
difference in cardiovascular response to
upper extremities isometric exercise
among apparently young healthy subjects.
60 participants were included in the study.
They were divided into two groups, group
A and group B. Group A included female
gender and group B included male gender.
BP, HR and MAP were taken as outcome
measure. These measures were taken pior,
immediately after test and 3 minutes after
study. The data collected was statistically
analysed. The result showed group B had
more increase in HR,SBP ,DBP AND
MAP as compared to group A and there
was significant rise in MAP and SBP in
group B. The average isometric strength
estimate is generally about thirty percent
greater in men than in women in different
muscle groups . Upon initiating isometric
tension, increases in heart rate, systolic
blood pressure, and diastolic blood
pressure occur. Mitchell and associates
and Seals et al suggested that
cardiovascular responses to isometric
exercise are greater when larger muscle
groups are involved. While heart rate
responses to sustained submaximal static
contractions tend not to be significantly
0
20
4060
80
100
FEMALES
MALES
0
0.05
0.1
0.15
0.2
65 70 75 80
HEART RATE - REST
Female
Male
0
0.05
0.1
0.15
68 78 88
HEART RATE - RECOVERY
Female
Male
0
0.05
0.1
0.15
72 82 92
HEART RATE - POST EXERCISE
Female
Male

different before, during, or after exercise,
blood pressure responses to this exercise
are significantly elevated before, during,
and after exercise Gender differences in
cardiovascular responses to static exercise
are believed to be due to differences in
sympathetic-parasympathetic or adrenal
interactions at the cardiac level. The
finding of this study revealed that there
was no significant gender difference in
vitals of participants at baseline which
was statistically significant. The data
collected reveals that post exercise heart
rate, systolic blood pressure ,diastolic
blood pressure and mean arterial pressure
were higher than pre exercise values and
was statistically significant in both groups
ie group A and group B.
When values of recovery i.e. 3 minutes
after exercise when compared it was
almost same in both groups but when
compared to values at rest it was much
greater than recovery values.
The result between the two was calculated
using unpaired t test. Therefore upper
extremities isometric exercise had
significant effect on heart rate, systolic
blood pressure, diastolic blood pressure
and mean arterial blood blood pressure.
When values of group A and group B at
post exercise were compared it was seen
that male participants (group B) had
higher post exercise MAP and SBP had
level than females (group A) (p<0.05)
These result indicate that more blood is
pumped by left ventricle into aorta in
response to upper extremities isometric
exercise among males than females; while
myocardial oxygen uptake & measure of
oxygen consumption of heart muscles of
female participants in response to upper
extremities isometric exercises is higher
than that of males.
The tissues working hard during exercise
and also after the completion of exercise
require more oxygen than normal to pay
off this oxygen debt incurred during the
exercise. These results in increase in blood
supply to active muscles to supply this
extra amount of blood. At rest, muscles
receive approximately 20% of total blood
flow but during exercise blood flow to
muscles increase to 80 -85% .
Generally ,longer the duration of exercise
greater the role the cardiovascular system
plays in metabolism and performance
during exercise bout.eg an 1T00 meter
walk (little or no cardiovascular
involvement) versus a marathon(maximal
involvement).9
It has reported that release of adrenaline
and lactic acid into the blood result
increase in a heart rate.
The isometric exercises does not increase
the oxygen demand to the extend raised by
isotonic exercise thus DBP does not rise
much in isometric exercise The isometric
exercise results in pressure overload on

Vol.1 No.4 2012 Scientific Research Journal of India 47
http://www.srji.co.cc
heart. The myocardial oxygen
consumption (mvo2) also increase due to
exercise . Higher ventricular contraction is
evoked among males leading to increase
in systolic blood pressure.
This indicates that the males have higher
myocardial oxygen demand during
isometric exercise predisposing them to
greater risk of ischemia if developing
cardiovascular risk, factor compromising
the coronary blood flow.10
It has been seen males have higher plasma
levels of all three catecholoamines out of
which plasma levels of epinephrine are
higher as compared to females .this results
in increase in MAP immediately at of
exercise.
The findings supports the results of
previous investigators than upon initiation
isometric tension increase heart rate,
systolic blood pressure and diastolic blood
pressure occur.12 The result of
investigations have been reported at best
inconsistent and do not follow definite
pattern.12
However during the recovery period the
vitals were decreased as compared to
immediately post exercise in both genders.
However the vitals were not the same as
they were at rest prior to commmencent of
exercise.
The result of study is supported by the
articles “Gender difference in
cardiovascular response to upper
extremities isometric exercise in
normotensive subjects.” By Cembada and
“Gender differences in cardiovascular
response to isometric in seated and supine
positions” by Don Melrose. The proposed
mechanisms attempting to explain gender
differences in cardiovascular responses to
isometric exercise have been numerous
and conflicting. Sanchez et al. found
differences in adrenergic patterns between
genders in response to isometric exercise
and support the study. Ettinger and
associates demonstrated attenuated
increases in blood pressure and muscle
sympathetic nerve activity compared with
men. In data also derived from static
exercise as well as temperature and
psychological stressors, Jones et al found
that gender did not influence sympathetic
neural reactivity to stressors such as
isometric handgrip exercise
Changes in posture often experienced
during exercise or sporting activities have
also been shown to elicit various
circulatory adaptations. Sagiv et al. and
Borst et al. both noted changes in
cardiovascular regulation as a result of
postural changes. Relatively fewer studies
have investigated the cardiovascular
adaptations to exercise performed when
posture does not change during the time
course of the positions.
A further study can be made:

• Comparison of vitals for larger
muscles groups to smaller muscles
group in upper limb isometric
exercises.
• Comparison of vitals in isometric
exercise for upper limb versus
lower limb.
The result can be used as
• It can be used for prescription of
exercise in those with
cardiovascular crompromise and
elderly patients.
• It can be used to determine the
safety limits during exercise
regimen.
CONCLUSION
The above study gives following
conclusion:
1. Isometric exercises of upper limb can
lead to increase in systolic blood
pressure ,diastolic blood pressure ,mean
arterial pressure and heart rate among
apparently healthly males and females.
2. This was more preannounced in males
than females .Systolic blood pressure
(SBP) and Mean arterial pressure (MAP)
increased in both but more males as
compared to females
LIMITATION
1. The participants in study were young
and elderly or middle aged participants
were not included in these study.
2. All the subjects who were included in
the study were students.
3. The participants nutritional status or
BMI were not considered while selection.
4. The occupation or lifestyle of
participants was not considered.
5. The muscle mass or bulk of upper limb
was not considered.
REFERENCES:
1. Journal of Exercise Physiology
Online. Volume 8, number 5,
august 2005.
2. Therapeutic Exercise, Carolyn
Kisner & Lynn Allen Collby.Pg
No 168,5th Edition
3. Sports Fitness Advisor, Fleck
st&kramerwj(2004).
4. Husketh Mount, pg no 92-96,lord
street,merseyside, england.
5. Effect of exercise .stending
lenderg 2004
6. Gender difference in
cardiovascular response to
isometric exercise.gatzke 2005
7. Circulation, amercian heart
association,2007pg no 3 &4
8. Clinical Orthopaedic
rehabilitation ,2nd editions brent
brotzman,pg no 138-142

Vol.1 No.4 2012 Scientific Research Journal of India 49
http://www.srji.co.cc
9. Cardiovascular system and
exercise physiology,aulter &amer
suleman
10. International journal of biomedical
reserach,srinath galag & ravipati
sarath volume 2,november 2011
11. Gender difference in
cardiovascular response to
isometric exercise of upper
limbs,howden et clf 2006.
12. Gender difference in
cardiovascular response to
isometric exercise,gatzke
13. The essential guide to building
muscles by phil daviee.
CORRESPONDENCE:
* Consultant Physiotherapist, Bhagwan Mahaveer Medical Centre, M.G. Road, Goregaon (W), Mumbai.
Email: [email protected]

Paraplegia with Sacral Pressure ulcer treated by Ultrasound therapy- A
Single Case Report
Shanmuga Raju P. MPT *, Ramalingam P. MS, FICA, MAMS
Abstract: Pressure ulcers are important and common complications after
paraplegia. The use of therapeutic ultrasound as an adjunct to wound healing has
gained interest in recent years. An twenty five year old male reported with a two
months history of a grade two, non healing, sacral pressure ulcer. Ultrasound
therapy (UST) is simple, safe, without side effects, bedside procedure, inexpensive
with positive wound healing results for difficult to treat non healing pressure sore.
I hope that this article will encourage other wound care specialists to engage in
further research in this area.
Key Words: Paraplegia, Sacral pressure ulcer; Continuous mode of ultrasound
therapy; wound healing.
INTRODUCTION Pressure Ulcer, also called as Decubitus
ulcers, was first seriously studied by
“Jean- Martin Charcot”, a clinician in the
19th Century (1-3). Pressure ulcer is a
serious health issue, very painful, a
significant physiological challenge, can
shorten the life of patient, an emotional
and financial burden to the patient.
Pressure sore are important and common
complications after paraplegia. An
estimated 50 – 80% of individuals
suffering from spinal cord injury develop
pressure ulcer at least once in their life
time (9). Pressure ulcer are treated by
using wound dressings, relieving pressure
on the wound, Water beds/ Alpha bed by
treating concurrent conditions which may
delay healing and by the use of physical
therapy such as electrical stimulation,
laser therapy and ultrasound (1).
Ultrasound is now the most frequently
used electrophysical agent worldwide,
used at least daily for patient treatment by
the majority of physiotherapists (4-5).The
aim of this study to investigate the effect
of ultrasound (US) therapy in sacral
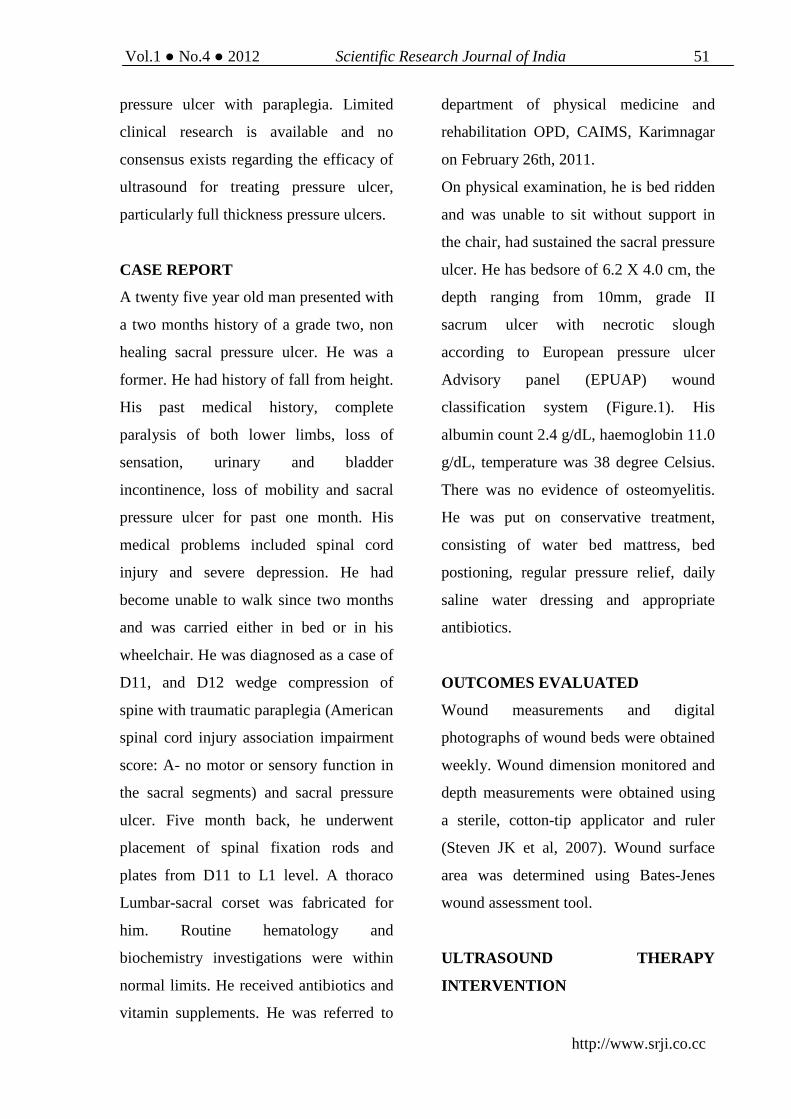
Vol.1 No.4 2012 Scientific Research Journal of India 51
http://www.srji.co.cc
pressure ulcer with paraplegia. Limited
clinical research is available and no
consensus exists regarding the efficacy of
ultrasound for treating pressure ulcer,
particularly full thickness pressure ulcers.
CASE REPORT
A twenty five year old man presented with
a two months history of a grade two, non
healing sacral pressure ulcer. He was a
former. He had history of fall from height.
His past medical history, complete
paralysis of both lower limbs, loss of
sensation, urinary and bladder
incontinence, loss of mobility and sacral
pressure ulcer for past one month. His
medical problems included spinal cord
injury and severe depression. He had
become unable to walk since two months
and was carried either in bed or in his
wheelchair. He was diagnosed as a case of
D11, and D12 wedge compression of
spine with traumatic paraplegia (American
spinal cord injury association impairment
score: A- no motor or sensory function in
the sacral segments) and sacral pressure
ulcer. Five month back, he underwent
placement of spinal fixation rods and
plates from D11 to L1 level. A thoraco
Lumbar-sacral corset was fabricated for
him. Routine hematology and
biochemistry investigations were within
normal limits. He received antibiotics and
vitamin supplements. He was referred to
department of physical medicine and
rehabilitation OPD, CAIMS, Karimnagar
on February 26th, 2011.
On physical examination, he is bed ridden
and was unable to sit without support in
the chair, had sustained the sacral pressure
ulcer. He has bedsore of 6.2 X 4.0 cm, the
depth ranging from 10mm, grade II
sacrum ulcer with necrotic slough
according to European pressure ulcer
Advisory panel (EPUAP) wound
classification system (Figure.1). His
albumin count 2.4 g/dL, haemoglobin 11.0
g/dL, temperature was 38 degree Celsius.
There was no evidence of osteomyelitis.
He was put on conservative treatment,
consisting of water bed mattress, bed
postioning, regular pressure relief, daily
saline water dressing and appropriate
antibiotics.
OUTCOMES EVALUATED
Wound measurements and digital
photographs of wound beds were obtained
weekly. Wound dimension monitored and
depth measurements were obtained using
a sterile, cotton-tip applicator and ruler
(Steven JK et al, 2007). Wound surface
area was determined using Bates-Jenes
wound assessment tool.
ULTRASOUND THERAPY
INTERVENTION
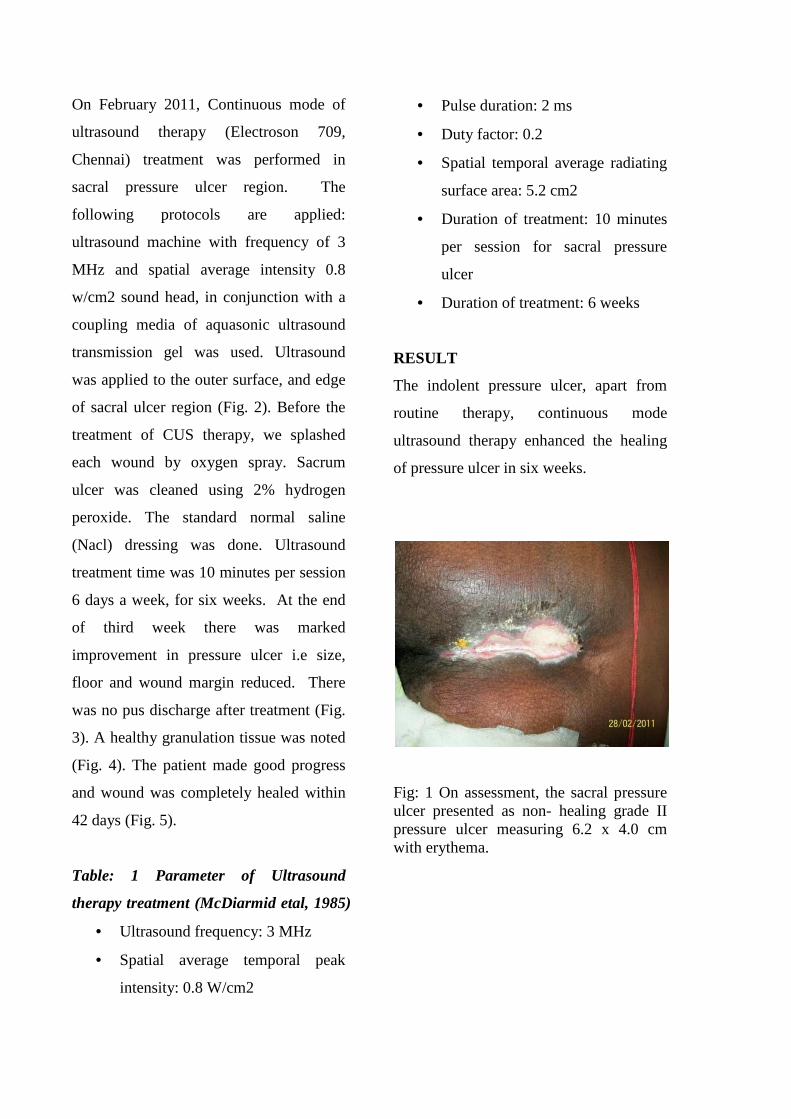
On February 2011, Continuous mode of
ultrasound therapy (Electroson 709,
Chennai) treatment was performed in
sacral pressure ulcer region. The
following protocols are applied:
ultrasound machine with frequency of 3
MHz and spatial average intensity 0.8
w/cm2 sound head, in conjunction with a
coupling media of aquasonic ultrasound
transmission gel was used. Ultrasound
was applied to the outer surface, and edge
of sacral ulcer region (Fig. 2). Before the
treatment of CUS therapy, we splashed
each wound by oxygen spray. Sacrum
ulcer was cleaned using 2% hydrogen
peroxide. The standard normal saline
(Nacl) dressing was done. Ultrasound
treatment time was 10 minutes per session
6 days a week, for six weeks. At the end
of third week there was marked
improvement in pressure ulcer i.e size,
floor and wound margin reduced. There
was no pus discharge after treatment (Fig.
3). A healthy granulation tissue was noted
(Fig. 4). The patient made good progress
and wound was completely healed within
42 days (Fig. 5).
Table: 1 Parameter of Ultrasound
therapy treatment (McDiarmid etal, 1985)
• Ultrasound frequency: 3 MHz
• Spatial average temporal peak
intensity: 0.8 W/cm2
• Pulse duration: 2 ms
• Duty factor: 0.2
• Spatial temporal average radiating
surface area: 5.2 cm2
• Duration of treatment: 10 minutes
per session for sacral pressure
ulcer
• Duration of treatment: 6 weeks
RESULT
The indolent pressure ulcer, apart from
routine therapy, continuous mode
ultrasound therapy enhanced the healing
of pressure ulcer in six weeks.
Fig: 1 On assessment, the sacral pressure ulcer presented as non- healing grade II pressure ulcer measuring 6.2 x 4.0 cm with erythema.

Vol.1 No.4 2012 Scientific Research Journal of India 53
http://www.srji.co.cc
Fig: 2 the full thickness of sacral ulcer was treated with continuous mode ultrasound therapy (CUST)
Fig: 3 three weeks after the treatment of CUST
Fig: 4 Fifth weeks after CUST, the wound size are decreased for sacral ulcer
Fig: 5 After six week of treatment, picture showing that sacral pressure ulcer are completely healed.
DISCUSSION
The purpose of the study was to assess the
effect of ultrasound therapy in healing of
sacrum pressure ulcer in patients with
paraplegia. Infected sores heal more
slowly than clean sores while no effect of
ultrasound clean sores were observed
ultrasound therapy appeared to improve
the rate of healing of infected sores. It is
non thermal effect produced by ultrasound
that are most significant in the stimulation
of tissue repair (Dyson, 1976). Paul et al
(1960) ultrasound was effective in
relieving congestion, cleansing necrotic
areas and promoting healing with healthy,
non-adherent skin approaching normal
thickness. Cyclic vibration effect of
ultrasound might induced a form of micro
massage which by reducing edema, might
facilitate repair, their requires further
investigations. It is also stimulate protein
synthesis infact ultrasound initiates two

processess which results in release of
energy tissue: Surface cavitation (creation
and dissipation of tiny bubbles in the
tissues) and acoustic microstreaming that
is movement of fluids along acoustic
boundaries, such as cell membrane. This
biophysical effect that are non-thermal
alternations in cellular protein synthesis
and release, blood flow and vascular
permeability, angiogenesis, and collagen
content and alignment by various workers
it as quoted as follows: 1. General protein
and collagen synthesis by fibroplasts
(Harvey etal, 1975, Webster etal. 1980). 2.
Fibroplast mobility (Miller etal, 1978). 3.
Fibroblast ultrastructure (Dyson and Pond,
1970). 4. Permeability of fibroblast
membrane (Harvey etal, 1975). 5.
Lysosomal fragilty (Tayor and Pond,
1972). 6. Tensile strength and elasticity of
scar tissue (Dyson et al, 1979). 7.
Modification of contraction in skin
wounds (Dyson et al, 1981).
With this parameters of ultrasound
treatment (frequency 3 MHz, Intensity 0.8
W/cm2, Pulse duration 2 ms, Duty cycle
0.2, effective radiating surface area 5.2
cm2, Duration of treatment 10 minute
per/session, Duration of frequency 6
weeks) pressure ulcer healed in time
without side effects. Our case study
showed that continuous mode of
ultrasound therapy treatment enhances
healing of sacral pressure ulcer. This case
study confirmed that continuous UST has
a positive effect on pressure ulcer with
paraplegia (Fig.5). No complications were
observed with application of the
continuous ultrasound. Further studies are
needed to evaluate the efficacy of
ultrasound therapy in pressure ulcers in
spinal cord injury in a large number of
patients.
CONCLUSION
Continuous mode of ultrasound therapy
was effective in the treatment of patient
with grade II pressure ulcer in young
paraplegic patient. Ultrasound therapy
treatment of pressure ulcer is less
expensive, more comfortable and can
enhance wound healing process without
side effects and complication.
REFERENCES:
1. Sella EJ, Barrette C. Staging of
charcot neuro arthropathy along
the medial column of the foot in
the diabetic patient. J. Foot Ankle
Surg. 1999, 38; 34-40.
2. Levine JM. Historical perspective
on pressure ulcers: The decubitus
ominosus of Jean- Martin Charcot.
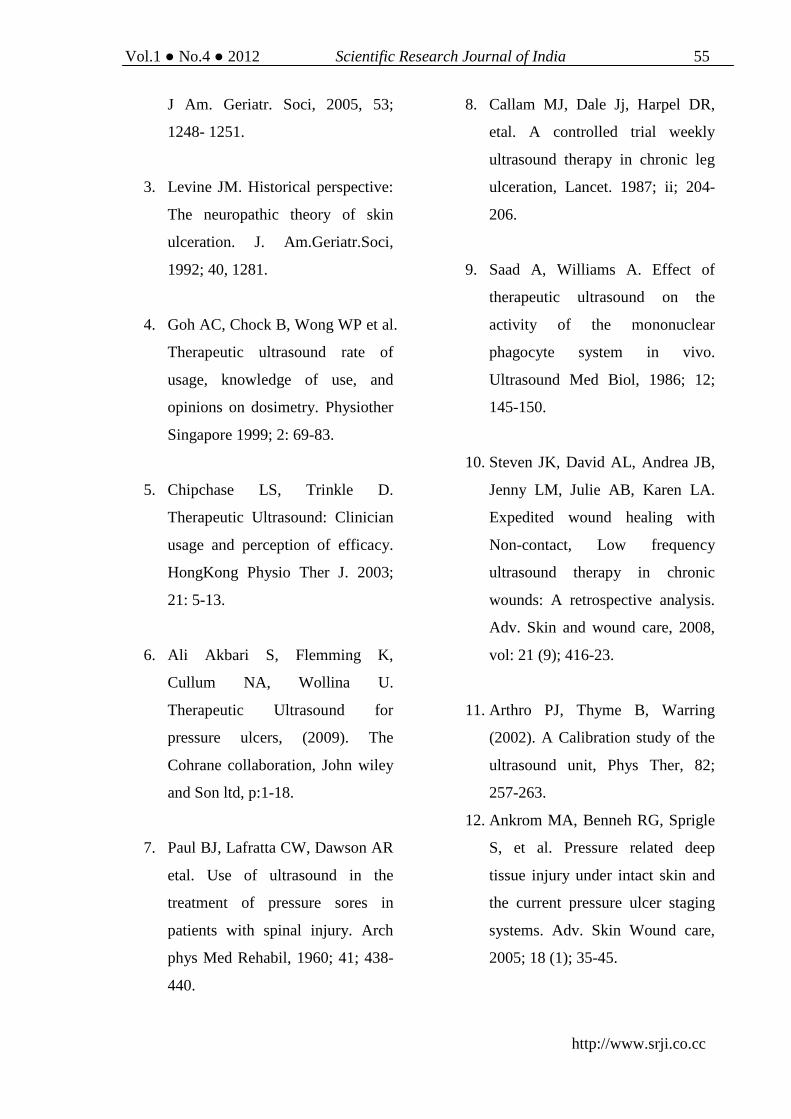
Vol.1 No.4 2012 Scientific Research Journal of India 55
http://www.srji.co.cc
J Am. Geriatr. Soci, 2005, 53;
1248- 1251.
3. Levine JM. Historical perspective:
The neuropathic theory of skin
ulceration. J. Am.Geriatr.Soci,
1992; 40, 1281.
4. Goh AC, Chock B, Wong WP et al.
Therapeutic ultrasound rate of
usage, knowledge of use, and
opinions on dosimetry. Physiother
Singapore 1999; 2: 69-83.
5. Chipchase LS, Trinkle D.
Therapeutic Ultrasound: Clinician
usage and perception of efficacy.
HongKong Physio Ther J. 2003;
21: 5-13.
6. Ali Akbari S, Flemming K,
Cullum NA, Wollina U.
Therapeutic Ultrasound for
pressure ulcers, (2009). The
Cohrane collaboration, John wiley
and Son ltd, p:1-18.
7. Paul BJ, Lafratta CW, Dawson AR
etal. Use of ultrasound in the
treatment of pressure sores in
patients with spinal injury. Arch
phys Med Rehabil, 1960; 41; 438-
440.
8. Callam MJ, Dale Jj, Harpel DR,
etal. A controlled trial weekly
ultrasound therapy in chronic leg
ulceration, Lancet. 1987; ii; 204-
206.
9. Saad A, Williams A. Effect of
therapeutic ultrasound on the
activity of the mononuclear
phagocyte system in vivo.
Ultrasound Med Biol, 1986; 12;
145-150.
10. Steven JK, David AL, Andrea JB,
Jenny LM, Julie AB, Karen LA.
Expedited wound healing with
Non-contact, Low frequency
ultrasound therapy in chronic
wounds: A retrospective analysis.
Adv. Skin and wound care, 2008,
vol: 21 (9); 416-23.
11. Arthro PJ, Thyme B, Warring
(2002). A Calibration study of the
ultrasound unit, Phys Ther, 82;
257-263.
12. Ankrom MA, Benneh RG, Sprigle
S, et al. Pressure related deep
tissue injury under intact skin and
the current pressure ulcer staging
systems. Adv. Skin Wound care,
2005; 18 (1); 35-45.

13. McDiarmid T, Burns PN, Lewith
GT, Machin D. Ultrasound and the
treatment of pressure sores,
Physiotherapy, 1985; 71; 66-70.
14. Dyson M. Role of ultrasound in
wound healing. In: Mcculloch JM.
Kloth LC, Feeder JA, eds. Wound
Healing. Alteratives in
Management, 2nd ed, Philadelphia
Pa: FA Davis co; 1995; 319-345.
15. Sari AA etal. Therapeutic
ultrasound for pressure ulcers.
Cochrane Database of systemic
reviews. 2009 (4).
16. TerRiet G, Kessels AG,
Knipschild P (1996). A
randomized clinical trial of
ultrasound in the treatment of
pressure sores. Phys Ther 76;
1301-1311.
17. Whatson GW, Milani JC, Dean LS.
Pressure sore profile: cost and
management, ASIA, Abstracts
Digest, 1987; 115-119.
18. Houghton PE, Kincaid CB,
Campell KE, et al. Photographic
assessment of the appearance of
chronic pressure and leg ulcers.
Ostomy / Wound Management.
2000; 46(4); 20-30.
ACKNOWLEDGMENT:
I thank the men who participated in this trial. I would also like to thank chairman Sri. C.
Lakshmi Narasimha Rao, Prof. V. Suryanarayana Reddy, Director, Chalmeda Anand Rao
Institute of Medical Sciences, Karimnagar for his support and encouragement of this study.
CORRESPONDENCE:
*Asst. Professor & I/C Head, Department of Physical Medicine and Rehabilitation Chalmeda Anand Rao
Institute of Medical Sciences Karimnagar -505001, Andhra Pradesh, INDIA. Mobile: 08790544270, Fax: 0878-
2285318. E-mail: [email protected]

Vol.1 No.4 2012 Scientific Research Journal of India 57
http://www.srji.co.cc
Arterio-Enteric Fistula: A Case Report
Anil Degaonkar*, Nikhil Bhamare**, Mandar Tilak***
Abstract: Gastro-intestinal (GI) bleeding may originate anywhere from oral
cavity to anus from the innocuous one like peptic ulcers to capricious lesion like
ca colon.Classically if the cause of bleeding is somewhere below the ligament of
Treitz, the stools are maroon or bright red in colour and it is described as lower
GI bleeding or hematochezia. Arterioenteric fistula signifies a rare but important
cause of massive lower GI bleeding .The vexing problem lies in proper and timely
diagnosis of this condition.A keen clinical acumen and proper use of tests lead to
accurate diagnosis and prompt treatment and can be lifesaving for the patient by
treating significant ongoing bloodloss. We wish to report such a case of an
arterio-enteric fistula between artery of broad ligament of uterus and terminal
ileum diagnosed and successfully treated at our institute .
Keywords: Arterioenteric fistula, massive GI bleed, rare cause
INTRODUCTION Arterioenteric fistula is a anomalous
communication between artery &
gastrointestinal tract. It is a rare cause of
massive lower GI bleeding with the
dreaded aortoenteric fistula leading to
massive and many times fatal GI bleed.
CASE REPORT
A 28 yr lady presented with complains
of recurrent per rectal bleeding and severe
anemia. She had undergone exploration
for ectopic pregnancy 1 month back at a
private hospital..On 8th post operative day
she had complained of three episodes of
per rectal bleeding which was associated
with giddiness and profound weakness.
Her sigmoidoscopy had been done and no
abnormality was detected.Patient had been
transfused, stabilised and subsequently
discharged .She whad been stable for the

next 20 days and now presented with
above complains of recurrent per rectal
bleeding and severe anemia. Patient was
investigated. Hematological investigations
showed low haemoglobin hb-5 gm% with
reticulocytosis. Platelets were adequate
and bleeding and clotting time was normal.
Serum Beta hCG was elevated .Upper GI
scopy showed no abnormality. O
colonoscopy only significant finding
observed was presence of blood clots near
caecum. USG was suggestive of
heterogeneous mass in right adnexa with
left ovarian cyst. CT confirmed the
ultrasound findings.
Pt was transfused with 3 pints of PCV.
Her condition improved and she remained
stable for next 8 days .On 9th day she
developed three episodes of massive per
rectal bleed and went into hypovolemic
shock. Her pulse rate was 146/min, BP
90/60 mm of hg. Patient was pale and
dehydrated. She did not have an
hematemesis and ryle’s tube aspirate was
clear. Due to absence of hematemesis and
pain in epigastrium upper GI bleeding was
less likely. Also patient had a history of
abdominal exploration. Thus an
arterioenteric fistula was suspected.
Advanced investigation modalities like
angiography and technicium99 labelled
rbc scan was unavailable at our institute.
Hence a decision for emergency
next 20 days and now presented with
above complains of recurrent per rectal
ere anemia. Patient was
investigated. Hematological investigations
5 gm% with
reticulocytosis. Platelets were adequate
and bleeding and clotting time was normal.
Serum Beta hCG was elevated .Upper GI
scopy showed no abnormality. On
colonoscopy only significant finding
observed was presence of blood clots near
caecum. USG was suggestive of
heterogeneous mass in right adnexa with
left ovarian cyst. CT confirmed the
Pt was transfused with 3 pints of PCV.
ition improved and she remained
stable for next 8 days .On 9th day she
developed three episodes of massive per
rectal bleed and went into hypovolemic
shock. Her pulse rate was 146/min, BP
90/60 mm of hg. Patient was pale and
dehydrated. She did not have any
hematemesis and ryle’s tube aspirate was
clear. Due to absence of hematemesis and
pain in epigastrium upper GI bleeding was
less likely. Also patient had a history of
abdominal exploration. Thus an
arterioenteric fistula was suspected.
tion modalities like
angiography and technicium99 labelled
rbc scan was unavailable at our institute.
Hence a decision for emergency
exploratory laparotomy after proper
resuscitation of the patient was taken.
On exploratory laparotomy there was
evidence of adherent ileum to the
posterior aspect of the broad lig. of
uterus (site at which the gestational sac
of previous ectopic was present.) Ileum
was separated from adhesion site. Erosion
of ileum wall with bleeder at site of
adhesion to broad ligament was found.
The site of adhesion on the broad ligament
showed necrosis.
Fig.1: Involved Ileal Segment
Thus this was a case of arterioenteric
fistula between the adherent ileum and a
branch of the ovarian artery supplying the
broad ligament. All bowel adhesions were
separated. The bleeder as ligated
hysterectomy was done. Adherent and
eroded segment of ileum was resected.
Intra-operative enteroscopy both
antegrade and retrograde was done in the
ileum to rule out any othe site of GI bleed.
Ileo-ileal anastomosis was done.
Postoperatively the patient was monitored
in surgical intensive care unit. Patient
exploratory laparotomy after proper
resuscitation of the patient was taken.
On exploratory laparotomy there was
f adherent ileum to the
posterior aspect of the broad lig. of
uterus (site at which the gestational sac
of previous ectopic was present.) Ileum
was separated from adhesion site. Erosion
of ileum wall with bleeder at site of
ad ligament was found.
The site of adhesion on the broad ligament
Involved Ileal Segment
Thus this was a case of arterioenteric
fistula between the adherent ileum and a
branch of the ovarian artery supplying the
ll bowel adhesions were
separated. The bleeder as ligated
hysterectomy was done. Adherent and
eroded segment of ileum was resected.
operative enteroscopy both
antegrade and retrograde was done in the
ileum to rule out any othe site of GI bleed.
ileal anastomosis was done.
Postoperatively the patient was monitored
in surgical intensive care unit. Patient
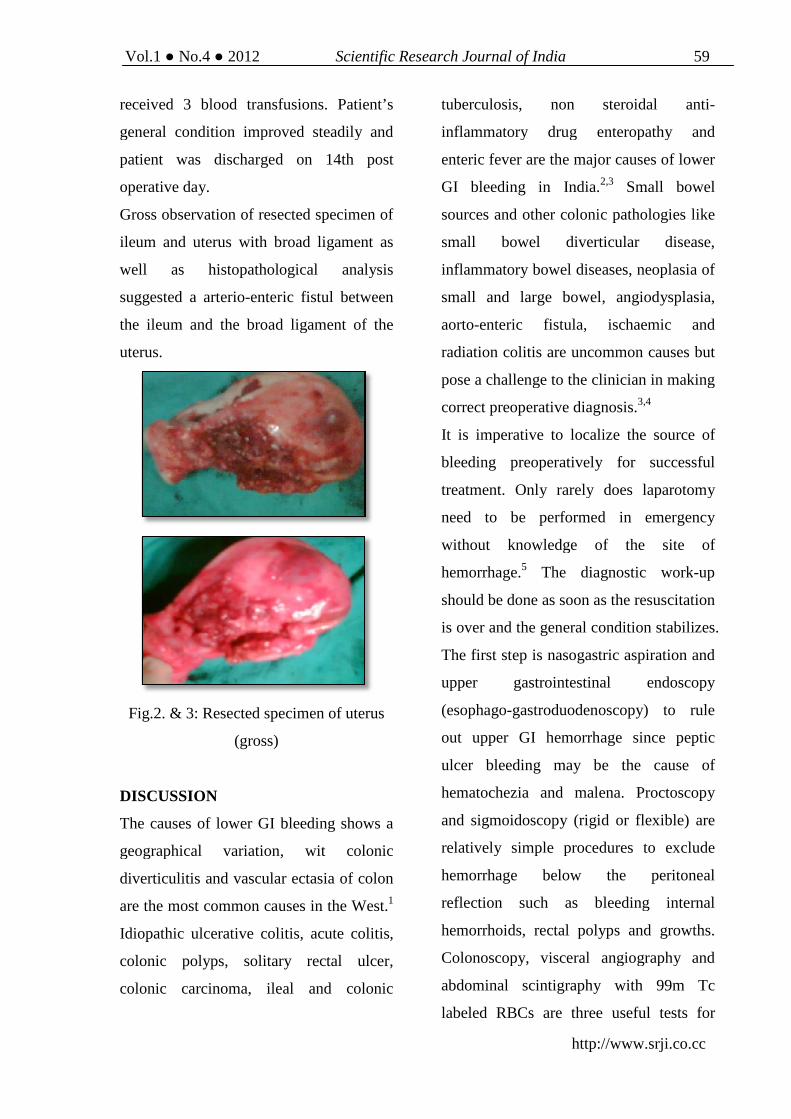
Vol.1 No.4 2012
received 3 blood transfusions. Patient’s
general condition improved steadily and
patient was discharged on 14th post
operative day.
Gross observation of resected specimen of
ileum and uterus with broad ligament as
well as histopathological analysis
suggested a arterio-enteric fistul between
the ileum and the broad ligament of the
uterus.
Fig.2. & 3: Resected specimen of uterus
(gross)
DISCUSSION
The causes of lower GI bleeding shows a
geographical variation, wit colonic
diverticulitis and vascular ectasia of colon
are the most common causes in the West.
Idiopathic ulcerative colitis, acute colitis,
colonic polyps, solitary rectal ulcer,
colonic carcinoma, ileal and colonic
Scientific Research Journal of India
http://www.srji.co.cc
received 3 blood transfusions. Patient’s
general condition improved steadily and
patient was discharged on 14th post
tion of resected specimen of
ileum and uterus with broad ligament as
well as histopathological analysis
enteric fistul between
the ileum and the broad ligament of the
esected specimen of uterus
The causes of lower GI bleeding shows a
geographical variation, wit colonic
diverticulitis and vascular ectasia of colon
are the most common causes in the West.1
Idiopathic ulcerative colitis, acute colitis,
colonic polyps, solitary rectal ulcer,
colonic carcinoma, ileal and colonic
tuberculosis, non steroidal anti
inflammatory drug enteropathy and
enteric fever are the major causes of lower
GI bleeding in India.
sources and other colonic pathologies like
small bowel diverticular disease,
inflammatory bowel diseases, neoplasia of
small and large bowel, angiodysplasia,
aorto-enteric fistula, ischaemic and
radiation colitis are uncommon causes but
pose a challenge to the clinician in making
correct preoperative diagnosis.
It is imperative to localize the source of
bleeding preoperatively for successful
treatment. Only rarely does laparotomy
need to be performed in emergency
without knowledge of the s
hemorrhage.5 The diagnostic work
should be done as soon as the resuscitation
is over and the general condition stabilizes.
The first step is nasogastric aspiration and
upper gastrointestinal endoscopy
(esophago-gastroduodenoscopy) to rule
out upper GI hemorrhage since peptic
ulcer bleeding may be the cause of
hematochezia and malena. Proctoscopy
and sigmoidoscopy (rigid or flexible) are
relatively simple procedures to exclude
hemorrhage below the peritoneal
reflection such as bleeding internal
hemorrhoids, rectal polyps and growths.
Colonoscopy, visceral angiography and
abdominal scintigraphy with 99m Tc
labeled RBCs are three useful tests for
59
http://www.srji.co.cc
tuberculosis, non steroidal anti-
inflammatory drug enteropathy and
enteric fever are the major causes of lower
GI bleeding in India.2,3 Small bowel
sources and other colonic pathologies like
small bowel diverticular disease,
inflammatory bowel diseases, neoplasia of
small and large bowel, angiodysplasia,
enteric fistula, ischaemic and
radiation colitis are uncommon causes but
a challenge to the clinician in making
correct preoperative diagnosis.3,4
It is imperative to localize the source of
bleeding preoperatively for successful
treatment. Only rarely does laparotomy
need to be performed in emergency
without knowledge of the site of
The diagnostic work-up
should be done as soon as the resuscitation
is over and the general condition stabilizes.
The first step is nasogastric aspiration and
upper gastrointestinal endoscopy
gastroduodenoscopy) to rule
er GI hemorrhage since peptic
ulcer bleeding may be the cause of
hematochezia and malena. Proctoscopy
and sigmoidoscopy (rigid or flexible) are
relatively simple procedures to exclude
hemorrhage below the peritoneal
reflection such as bleeding internal
orrhoids, rectal polyps and growths.
Colonoscopy, visceral angiography and
abdominal scintigraphy with 99m Tc
labeled RBCs are three useful tests for

localization.5 Colonoscopy may be most
useful if the bleeding has stopped or at
least slowed substantially.
Selective visceral angiography is very
useful if the patient is having active
bleeding to locate exact site of bleeding.
Abdominal scintigraphy with 99m Tc
labeled RBC infusion is helpful in
delineating the site of bleeding when
bleeding is intermittent and at a rate below
that which is detectable by angiography.
In case the above facilities are not at hand,
a combination of sigmoidoscopy and air
contrast barium enema may be tried if
patient’s general condition permits.6 We
have searched the literature on the subject
and have come across some pathological
conditions leading to fistula formation
between aorta and the intestine.7,8
Abdominal aortic aneurysm and infective
aortitis may lead to primary aorto-enteric
fistula but in most of the cases the
bleeding occurs due to erosion of aortic
vascular prosthesis through the wall of
distal duodenam due to prolonged contact
between prosthetic graft and a fixed
segment of intestine (secondary aorto-
enteric fistula). Bleeding may occur due
to dehiscence of the anastomosis with
bleeding into the bowel lumen from the
edges of the eroded intestine.7
The intestine may take blood supply from
the anterior abdominal wall due to
adhesion formation as seen sometimes as
a sequele of mesenteric venous thrombosis,
malignancies and fungal infection. A case
has been reported where mucomycosal
invasion took place into the iliac artery
causing severe haemorrhage, in a case of
non Hodgkin’s lymphoma receiving
chemotherapy.8 In this case, the cause of
arterio-enteric fistula formation was due to
continued trophoblastic activity of
incompletely removed gestational sac &
as the syncytiotrophoblast has invading
property.9 It has eroded the ileum &
fistula is formed between uterine artery of
broad ligament & terminal ileum.
Monitoring of trophoblastic activity can
be done by estimation of serum beta HCG
levels.10
In the above case report we have
presented a case of arterio-enteric fistula
between ileum and broad ligament of the
uterus. This is a very rare pathology and
has seldom been reported. We hypothesize
that the ectopic pregnancy and exploratory
laparotomy for the same probably created
a inflamed and eroded surface on the
broad ligament where ileum adhered. The
ileal wall was further eroded .The
inflammatory process exposed a artery on
the broad ligament and this adhered to the
ileum cresting the arterioenteric fistula.

Vol.1 No.4 2012 Scientific Research Journal of India 61
http://www.srji.co.cc
REFERENCES:
1. DeMarkles MP, Murphy JR. Acute
lower gastrointestinal bleeding.
Med Clin North Am 1993 Sep;
77(5):1085-100.
2. Goenka MK, Kochhar R, Mehata
SK. Spectrum of lower
gastrointestinal hemorrhage: an
endoscopic study of 166 patients.
Indian J Gastroenterology 1993
Oct; 12(4):129-31.
3. Anand AC, Patnaik PK, Bhalla VP,
Choudhary, et al. Massive lower
intestinal bleeding – a decade of
experience. Trop Gastroenterol
2001 Jul-Sep;22(3):131-4.
4. Miller LS, Barbarvech C,
Friedman LS. Less frequent causes
of lower gastrointestinal bleeding.
Gastroenterol Clin North Am
1994 Mar;23(1):21-52.
5. Gracia Osogobio S, Remes Troche
JM, et al. Surgical treatment of
lower digestive tract hemorrhage –
Experience at the Institute
Nacional de ciencias Medicas Y
Nutricion Salvador Zubiran.Rev
Invest Clin 2002 Mar-Apr;
52(2):119-24.
6. Mark HB, Robert B, Mark B.
Merk Manual Diagnosis and
Therapy. Seventeenth Edition Sec
– 3, Ch-22. Gastrointestinal
Bleeding.
7. Kahhlke V, Brossmanm J, Klomp
HJ. Lethal hemorrhage caused by
aortoenteric fistula following
endovascular stent implant.
Cardiovasc Intervent. Radiol 2002
May-Jun:25(3):205-7.
8. Mir N, Edmonson R, Yeghen T,
Rashid H. Gastrointestinal
mucormycosis complicated by
arterio-enteric fistula in a patient
with non-Hodgkin’s lymphoma.
Clin Lab Haematology 2000
Feb;22(1):441-4.
9. Datta; textbook of
gynaecology;6th edtn;chapter
2;page no.23
10. Datta; textbook of
gynaecology;6th edtn;chapter
15;page no.186.

CORRESPONDENCE:
*Assistant Professor Surgery, Dr. Shankarrao Chavan Govt Medical College, Nanded, Maharashtra;
**Resident 3rd yr General Surgery, Dr. Shankarrao Chavan Govt Medical College, Nanded, Maharashtra;
***Assistant Professor Surgery, Dr. Shankarrao Chavan Govt Medical College, Nanded, Maharashtra. E-mail
id: [email protected] Mob no: 09975033726

Vol.1 No.4 2012 Scientific Research Journal of India 63
http://www.srji.co.cc
All-Oxide Solar Cells: The Way of the Future
Akshay Vijay Dongarwar*
Abstract: We as a world are looking at our globe depleting of its natural
resources. The quantity of coal presently available can lead us through for twenty
more years at maximum considering the growing demand for high quality coal
and natural resources and to suffice the growing population and bettering
lifestyle. Again, on one side we have cut throat technological advancement in the
silicon valley and the mobile world and on other, we have fairly advanced
technologies for bringing in better, faster, more efficient and cheaper solutions to
the environmental concerns. The question is basically inspired from this ever
daunting situation. Can’t we have a cheap and highly effective solar energy
treatment plant which can actually reach poor countries and help them get over
their energy crisis without undergoing high-end processing in posh labs like is
done for silicon cells? Even in one of the fastest growing economies of world,
India, silicon processing is not done by any industry commercially to make solar
cells. All the pre-processed cells are imported and further distributed because of
the complexity in the process. Also, being cheap and easily available, it must have
a huge life like silicon cells have. So, it should possess the best of silicon while
eliminating the negatives. Can we find an alternative to conventional solar cells
that can reach out to everyone?
Keywords: All Oxide Solar Cell
THE QUESTION We as a world are looking at our globe
depleting of its natural resources. The
quantity of coal presently available can
lead us through for twenty more years at
maximum considering the growing
demand for high quality coal and natural
resources and to suffice the growing
population and bettering lifestyle. Again,
on one side we have cut throat
technological advancement in the silicon

valley and the mobile world and on other,
we have fairly advanced technologies for
bringing in better, faster, more efficient
and cheaper solutions to the
environmental concerns. The question is
basically inspired from this ever daunting
situation.
Can’t we have a cheap and highly
effective solar energy treatment plant
which can actually reach poor countries
and help them get over their energy crisis
without undergoing high-end processing
in posh labs like is done for silicon cells?
Even in one of the fastest growing
economies of world, India, silicon
processing is not done by any industry
commercially to make solar cells. All the
pre-processed cells are imported and
further distributed because of the
complexity in the process. Also, being
cheap and easily available, it must have a
huge life like silicon cells have. So, it
should possess the best of silicon while
eliminating the negatives. Can we find an
alternative to conventional solar cells that
can reach out to everyone?
HYPOTHESIS
A cavity of metal m2 (W2) with thin
polish of metal m1 (W1, W1<W2) on
inner surface, with a pin hole is kept at the
focus of the solar concentrator coinciding
the pinhole and focus. Pinhole is covered
with transparent glass to protect inner
polish of cavity from atmospheric reaction.
Such cavity behaves as metal-metal
junction solar cell (termed M-M cavity
solar cell).
But using nanowires and nanotubes
increases the functionality further as
diffraction light rays occurs. Again, using
metal oxide makes further sense as they
are chemically under thermodynamic
equilibrium. Another approach is used
which is of titanium dioxide for photo-
sensitization.
RESEARCH
The main challenge with producing a solar
cell with whole new materials is the
availability of photo sensitive materials
and their production. I had prepared a
project for the prestigious “KVPY”
scholarship, where I tried to theoretically
explain the use of metal-metal junction
cavity cell for emitting electrons. The
same research is used here, but with some
changes to make it further effective and to
eliminate short-comings. Here, I present
an all-oxide solar cell fabricated from
vertically oriented zinc oxide nanowires
and cuprous oxide nanoparticles. It
consists of vertically oriented n-type zinc
oxide nanowires, surrounded by a film
constructed from p-type cuprous oxide
nanoparticles. The idea behind using
metal oxides is to eliminate the effects of
atmosphere. Oxides being benign, are safe

Vol.1 No.4 2012 Scientific Research Journal of India 65
http://www.srji.co.cc
from environmental contamination. The
use of cuprous oxide as solar cells is a
very well studied since last 20 years.
Adding another metal-oxide film seemed
difficult at first as the oxides are already
in stable states and to make use of metal-
metal junction films, we had to change the
physical properties to excite them. But,
with the knowledge of photo-electricity
(diffusion) that I had acquired in the
recent months made me think a step
further and the idea of using nanowires
and nano-particles that respond better to
incident light seemed possible.
In the second part, I used titanium dioxide,
another successful oxide to take in the
solar light and convert them into
electricity (Research done by Dr. M.
Graetzel ). The cell was not taken as it
was. I just used pure titanium dioxide dust
here as polyphyrine derivatives. I did not
use dyes as is done in Graetzel cell but
instead let the oxide in white colour. Its
property of reflecting back visible range
light was later used and sorted out with
design. Being from an engineering
background, I designed a model, that
could make use of both these oxide films
efficiently and expected to get a desired
output of >12% efficiency.
EXPERIMENT
Zn oxide film preparation:
5 mM solution of zinc acetate dihydrate in
absolute ethanol was prepared. Two drops
of this solution were placed onto an
indium tin oxide (ITO) coated glass
substrate (Thin Film Devices, ~40-50
Ω/square). The substrate was then rinsed
with absolute ethanol and blown dry with
nitrogen. The dropcasting, rinsing and
drying was repeated four times per
substrate. The substrates were then
annealed in air at 350°C for 30 minutes,
converting the Zn(OAc)2 into ZnO, and
then cooled to room temperature. This
process was then repeated a second time
to ensure a conformal layer of ZnO.
The nanowires were then grown by
placing the seeded substrate in an aqueous
solution containing 25 mM zinc nitrate
hexahydrate, 25 mM
hexamethylenetetraamine, and 5 mM
polyethyleneimine at 90°C. The substrate
was suspended upside-down to prevent
any larger ZnO aggregates from
accumulating on the surface. Typical
growth times ranged from 30-60 minutes,
yielding wires that averaged from 400-
1000 nm in length and 30-50 nm in
diameter. After the growth, the nanowire
arrays were rinsed thoroughly with
deionized water, then annealed at 400°C
for 30 minutes to remove any residual
organics on the nano wire surface.

The Cu2O nanoparticles (NPs) were
prepared as follows:
A solution of copper (I) acetate (0.5 g),
trioctylamine (15 mL) and oleic acid (Alfa
Aesar, 99%, 4 mL) was flushed with
nitrogen, then rapidly heated to 180°C
under nitrogen flow. The solution was
maintained at this temperature for 1 hour,
then was quickly increased to 270°C and
held for one additional hour, ultimately
producing a burgundy colloidal solution,
which are metallic copper nanoparticles.
The solution was cooled to room
temperature, at which point absolute
ethanol was added to precipitate the
nanoparticles. The supernatant was
removed and the nanoparticles were
redispersed in hexane and then exposed to
air. After 12 hours, the burgundy solution
turned into deep green, indicating the
oxidation of the copper nanoparticles into
Cu2O. The Cu2O nanoparticles underwent
further cleaning by repeated precipitation
with ethanol. Finally, the nanoparticles
were dispersed in toluene for dropcasting
onto the ZnO nanowire arrays.
The processing required no posh research
labs and could be done without much
efforts.
The titanium oxide film is prepared the
usual Graetzel cell way. Except, we do not
use dye. The main motto was to simplify
the process. Dying induces lot of
complexity and we want the process to
remain easy.
DATA
The complete experiment was done by
using the available technologies at
disposal. Instead of using the paraboloid
sun-tracking reflector concentrator, a fine
beam of SODIUM VAPOUR LAMP was
used to create a similar effect. The metal-
metal oxide junction solar cell and the
titanium oxide cell were tested over a long
period of time to get accurate readings.
The cuprous oxide-zinc oxide junction
cells were studied first as they formed the
key research. A fine layer of the junction
nanoparticles was taken and placed in a
small glass box. The glass was designed in
such a way that it didnt let the incident
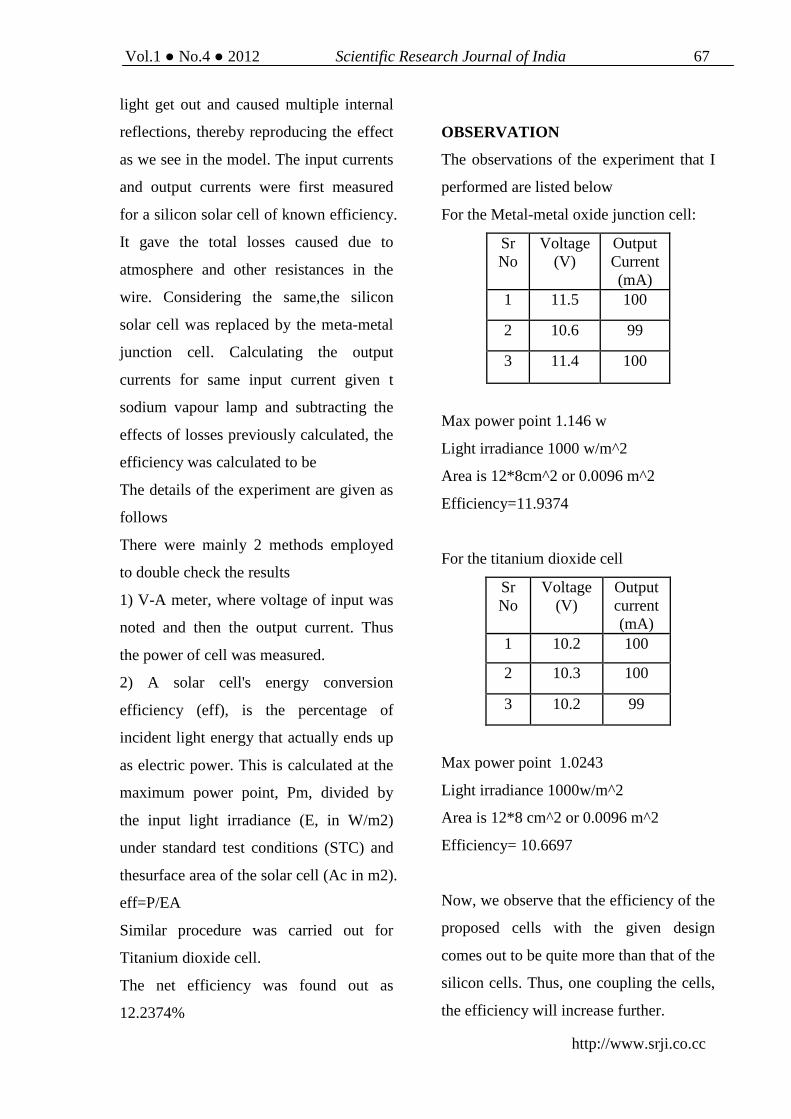
Vol.1 No.4 2012 Scientific Research Journal of India 67
http://www.srji.co.cc
light get out and caused multiple internal
reflections, thereby reproducing the effect
as we see in the model. The input currents
and output currents were first measured
for a silicon solar cell of known efficiency.
It gave the total losses caused due to
atmosphere and other resistances in the
wire. Considering the same,the silicon
solar cell was replaced by the meta-metal
junction cell. Calculating the output
currents for same input current given t
sodium vapour lamp and subtracting the
effects of losses previously calculated, the
efficiency was calculated to be
The details of the experiment are given as
follows
There were mainly 2 methods employed
to double check the results
1) V-A meter, where voltage of input was
noted and then the output current. Thus
the power of cell was measured.
2) A solar cell's energy conversion
efficiency (eff), is the percentage of
incident light energy that actually ends up
as electric power. This is calculated at the
maximum power point, Pm, divided by
the input light irradiance (E, in W/m2)
under standard test conditions (STC) and
thesurface area of the solar cell (Ac in m2).
eff=P/EA
Similar procedure was carried out for
Titanium dioxide cell.
The net efficiency was found out as
12.2374%
OBSERVATION
The observations of the experiment that I
performed are listed below
For the Metal-metal oxide junction cell:
Sr No
Voltage (V)
Output Current (mA)
1 11.5 100
2 10.6 99
3 11.4 100
Max power point 1.146 w
Light irradiance 1000 w/m^2
Area is 12*8cm^2 or 0.0096 m^2
Efficiency=11.9374
For the titanium dioxide cell
Sr No
Voltage (V)
Output current (mA)
1 10.2 100
2 10.3 100
3 10.2 99
Max power point 1.0243
Light irradiance 1000w/m^2
Area is 12*8 cm^2 or 0.0096 m^2
Efficiency= 10.6697
Now, we observe that the efficiency of the
proposed cells with the given design
comes out to be quite more than that of the
silicon cells. Thus, one coupling the cells,
the efficiency will increase further.

Here, an interesting trend observed is that
the maximum power point doesn't change
much for a considerable change of input
voltage in case of metal-metal oxide
junction cells. The reason is unknown.
CONCLUSION
Thus, as the results showcase, using some
of the most common oxides and some
simple primary treatment processes
coupled with engineering ideas, we were
able to increase the efficiency of solar
energy harnessing devices by an
outstanding ~6-7% (results show 4.3% but
that is under lab conditions).
Thus, the basic idea of trying to use the
metal oxides arising from a simple urge to
use environmentally inert materials turns
out to be a revolutionary alternative for
the conventional silicon solar cells. The
trait that make the idea highly successful
is that the processing is very easy and can
be done on a commercial level with some
material engineering guidance. Also, it
turns out to be a relief for countries like
India and other developing countries as
importing silicon cells was never cheap.
Hence, here, with technologically
advanced institutes in the nation like IITs
and NITs the implementation and
bettering the scope of the idea can be done.
A major issue was designing.
• How could we make most of the
sunlight. The answer came with
the paraboloid concentrator.
• How could we use it at all times
during the day? The secret lied
with the solar tracking device
which had become pretty common.
• How would we place the cells to
get output from both? The design
came to me by instincts. After a
host of designs, the most suitable
and easy to construct was used.
• Titanium di-oxide reflects back the
visible light. I offered a solution in
the design.
• At some places, the solar energy is
directly used for heating purposes.
Thus a band filter can be employed
to filter out the harmful ultraviolet
and infra-red light.
CORRESPONDENCE:
*29, Nelco Housing Society, Near Nagarjuna Trust Hospital, Khamla-Nagpur-440025. Contact- +91
9175017645, Email-id: [email protected]

Vol.1 No.4 2012 Scientific Research Journal of India 69
http://www.srji.co.cc
Call for Papers Scientific Research Journal of India (SRJI) globally welcomes research
scholars & scientists from different fields of science like Botany, Zoology, Medical
Sciences, Agricultural Sciences, Environmental Sciences, Natural
Sciences, Anthropology etc to contribute their researches in this Open Access
Publication.
::For full detail kindly visit:: http://www.srji.co.cc

This page is intentionally left blank
Related Documents











