ROLE OF CELL BLOCK IN ASCITIC FLUID CYTOLOGY IN THE EVALUATION & GRADING OF MALIGNANCY. DISSERTATION SUBMITTED TO THE TAMILNADU DR.M.G.R. MEDICAL UNIVERSITY CHENNAI in partial fulfilment of the requirements for the degree of M.D. (PATHOLOGY) BRANCH – III TIRUNELVELI MEDICAL COLLEGE TIRUNELVELI APRIL-2017

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ROLE OF CELL BLOCK IN ASCITIC FLUID CYTOLOGY IN THE
EVALUATION & GRADING OF MALIGNANCY.
DISSERTATION SUBMITTED TO
THE TAMILNADU DR.M.G.R. MEDICAL UNIVERSITY
CHENNAI
in partial fulfilment of
the requirements for the degree of
M.D. (PATHOLOGY)
BRANCH – III
TIRUNELVELI MEDICAL COLLEGE
TIRUNELVELI
APRIL-2017

CERTIFICATE
This is to certify that this Dissertation entitled “ROLE OF CELL BLOCK IN
ASCITIC FLUID CYTOLOGY IN THE EVALUATION & GRADING OF
MALIGNANCY” is the bonafide original work of Dr.K.SUMATHI, during
the period of her Post graduate study from 2014 –2017, under my guidance and
supervision, in the Department of Pathology Tirunelveli Medical College &
Hospital, Tirunelveli, in partial fulfilment of the requirement for M.D., (Branch
III) in Pathology examination of the Tamilnadu Dr.M.G.R Medical University
will be held in April 2017.
The DEAN
Tirunelveli Medical College,
Tirunelveli - 627011.
CERTIFICATE
This is to certify that this Dissertation entitled “ROLE OF CELL BLOCK IN
ASCITIC FLUID CYTOLOGY IN THE EVALUATION & GRADING OF
MALIGNANCY” is the bonafide original work of Dr.K.SUMATHI, during the
period of her Post graduate study from 2014 –2017, under my guidance and
supervision, in the Department of Pathology Tirunelveli Medical College &
Hospital, Tirunelveli, in partial fulfilment of the requirement for M.D., (Branch
III) in Pathology examination of the Tamilnadu Dr.M.G.R Medical University
will be held in April 2017.
Dr.K.Shantaraman,M.D Dr.Arasi Rajesh,M.D
Professor and HOD of Pathology, Department of Pathology
Professor of Pathology, Tirunelveli Medical college
Tirunelveli -11. Tirunelveli-11.

DECLARATION
I solemnly declare that this dissertation titled “ROLE OF CELL BLOCK
IN ASCITIC FLUID CYTOLOGY IN THE EVALUATION & GRADING
OF MALIGNANCY.” submitted by me for the degree of M.D, is the record
work carried out by me during the period of 2014-2017 under the guidance of
Prof. Dr.Arasi Rajesh,M.D Professor of Pathology, Department of Pathology,
Tirunelveli Medical College, Tirunelveli. The dissertation is submitted to The
Tamilnadu Dr.M.G.R. Medical University, Chennai, towards the partial
fulfilment of requirements for the award of M.D. Degree (Branch III) Pathology
examination to be held in April 2017.
Place: Tirunelveli DR.K.SUMATHI,Date: Department of Pathology,
Tirunelveli Medical College,Tirunelveli-11

ACKNOWLEDGEMENT
I take immense pleasure at this opportunity to acknowledge all those who
have helped me to make this dissertation possible. I express my heartfelt thanks
to the Dean, Tirunelveli Medical College, for permitting me to undertake this
study. I express my profound sense of gratitude to Dr.K.Shantaraman, MD.,
respected Professor and Head of Department of Pathology, Tirunelveli Medical
College, Tirunelveli, for his valuable advice, constant guidance and motivation
in the preparation of this work.
I consider it my privilege and honour to have worked under the unstinted
encouragement, and supervision of Dr.Arasi Rajesh,M.D., Professor of
Pathology.
I thank Dr.J.SureshDurai, MD., Dr.K.Swaminathan,MD., Dr.Vasuki,
MD., Professors of Pathology, for their constant support. I also thank the
Assistant Professors, for their encouragement. I take this opportunity to thank all
my postgraduate colleagues and all the technicians and other members of the
Department of Pathology for their constant help and support throughout the
tenure of this work.
K.SUMATHI

ABBREVIATION
CS - CONVENTIONAL SMEAR
CB - CELL BLOCK
FNAC - FINE NEEDLE ASPIRATION CYTOLOGY
IHC - IMMUNOHISTOCHEMISTRY
ER - ESTROGEN RECEPTOR
TTF-1 - THYROID TRANSCRIPTION FACTOR-1
CK - CYTOKERATIN
HCC - HEPATOCELLULAR CARCINOMA
MM - MALIGNANT MESOTHELIOMA
LA - LUNG ADENOCARCINOMA
CEA - CARCINO EMBRYONIC ANTIGEN
RCC - RENAL CELL CARCINOMA
SYN - SYNAPTOPHYSIN
CHR - CHROMOGRANIN
EMM - EPITHELOID MALIGNANT MESOTHELIOMA

TABLE OF CONTENTS
S.NO TITLES PAGE NO
1 INTRODUCTION 1
2 AIMS AND OBJECTIVES 4
3 REVIEW OF LITERATURE 5
4 MATERIALS AND METHODS 49
5 OBSERVATION AND RESULTS 56
6 DISCUSSION 69
7 SUMMARY 78
8 CONCLUSION 79
BIBLIOGRAPHY
APPENDIX
MASTER CHART

1
INTRODUCTION
Cell block technique was first described by Bahrenberg in 1896. This is
an old method for evaluation of body cavity fluids. The cell block technique
employs the retrieval of cells or small tissue fragments from any body fluid
including ascitic fluid, pleural fluid, bronchial wash and imaging guided fine
needle aspiration cytology specimens.
The cytodiagnosis by conventional smears have got some drawbacks due
to overcrowding of cells and cell loss leading to less cellularity1. To
overcome these drawbacks cell block technique was employed. Cell blocks
from fluid specimens can be prepared by using plasmathrombin or agar method.
The cell button formed is formalin fixed and processed routinely like
histopathological specimens.
The main advantage of cell block technique are possibility to obtain
multiple number of sections and the architecture of tissue were preserved and to
get from the same material for special stains and immunohistochemistry2,
The material preserved by cell block also improves the diagnostic accuracy
due to better architecture preservation and better nuclear and cytoplasmic
details. There is an increasing need for additional diagnostic technique
such as immunohistochemistry, to define a specific cell lineage on
cytology and FNAC specimens3,4. Immunohistochemistry is a highly
effective ancillary tool that can be used on cell block to distinguish sub
classify malignancies. Cell block increases accuracy, reproducibility and
minimizes the rate of unclassified carcinomas.

2
Aspiration biopsy material (FNA), sputum, effusions, urine sediment
and material from the gastrointestinal tract are all suitable for cell block
processing.
ADVANTAGES OF CELL BLOCK5:
In routine hospital laboratory this cell block method is a very simple and
readily adaptable&easily reproducible.
1. Cell block can bridges the gap between cytology and histology.
2. Preservation of architectural patterns like cell balls, papillae and
three dimentional clusters.
3. There is adequate cellularity, cell aggregates and also microscopic
fragments of tissue.
4. There is demarcation between the cells nuclear and also the
cytoplasmic details.
5. The crisp chromatin and the intact cell membrane details were
obtained.
6. In the same focal plane of microscopic examination the concentration of
one small area of cellular material can be evaluated.
7. The concentration of cellular elements in one small area that could
be evaluated at a glance with all cells were lying in the same focal
plane of microscope.
8. Cell block sections are suitable for histochemical stains and IHC.

3
Hence the present study was taken to assess the utility of cell block
technique in the diagnosis and grading of abdominal visceral malignancy in
ascitic fluid.

4
AIMS
1. Preparation of cell blocks of ascitic fluid in suspicious or confirmed cases
of visceral malignancy.
2. To compare the diagnostic accuracy of cell block technique with
conventional cytology smears.
3. To use immunohistochemistry on cell block for grading of tumour.
4. Evaluation and grading of visceral malignancy in cell block by applying
Ki67 marker by MIB index scoring system.

5
REVIEW OF LITERATURE:
In 1848 Bennethave an account on tumour cells in effusion fluids in his
publication that led to the development of cytopathological diagnosis of body
cavity fluids6. In 1867, Luke and Klebs gave a description of malignant cells in
effusion7. And Kanhouwa et al, correlated cytopathology and histopathology in
the typing of malignancy. And he showed a correlation of cytopathology and
histopathology of 77.5%8 in his study.
In clinical medicine the cytological evaluation of the fluids and effusions
has most acceptance value and with the surge of minimally invasive procedures,
a positive diagnosis is considered the definitive test and it will prevent
explorative surgery. It will be help in the diagnosis of malignant leisons, also
in grading, staging and prognosis. In conventional smears lack of morphological
details of the representative cells contributes to possibility of difficulties found
in making the definitive diagnosis.In the presence of resource limiting settings,
The Cell block technique is very safe and, simple and had cost
effectiveness9. The use of cell blocks is being increasingly advocated in the
diagnostic work up of patients. The routine use of this technique remains
confined to a number of centers.
CELL BLOCK TECHNIQUE:
By the historic evolution of this cell block techniques have been in use
for over a century. In 1896 Bahrenburg and Mandlebaum explained their

6
technique of embedding and sectioning the cellular sediments, and there have
been a number of reports concerning the formed elements in serous effusions6.
In 1917 the malignant tumors were diagnosed in paraffin sections of
centrifuged exudates to make specimens more readily interpretable even by
histopathologists10.
In 1928 Zemansky established the definitive arrangement of the cells as
acini and papilla or of aggregates of abnormal cells to be of malignant nature11.
THE MAIN ADVANTAGES OF CELL BLOCK:
- Even if there is less cellular disposal,this technique can allows better
and easier on microscopic observation than comparing the traditional
smears12.
- In interpretation there is less difficulty even if the background shows
excess blood during microscopic observation.
- Well recognition of the histological patterns of diseases which cannot be
identified correctly in conventional smears12.
- Possibility of obtaining multiple sections to study on routine and special
staining method.
- In the evaluation of ancillary studies like immunocytochemistry, in- situ
hybridization tests (FISH/ CISH), and in-situ polymerase chain
reaction(PCR)13 they will help.
- For retrospective study purpose storing of slides were possible .

7
ANATOMY:
The peritoneum is a serous membrane which lines the abdominal cavity.
It covers the anterior and posterior abdominal wall, the under surface of
diaphragm and pelvic cavity. All this is the parietal peritoneum.
In places it leaves the posterior abdominal wall or diaphragm to form a
partial or complete investment for viscera, this is visceral peritoneum, which
forms the serous covering for many viscera14.
Peritoneum consists of a single layer of flattened mesothelial, cells overlying
areolar tissue which varies in both thickness and density in different places.
PERITONIAL CAVITY:
The serous coated organs fill the abdominal cavity so that visceral
surfaces are in contact with one another or with the parietal peritoneum. The
space between them is only potential, not actual, and it contains only a few ml
of tissue fluid which lubricates adjacent surfaces so they glide over one
another.
ASCITES:
Ascites refer to the accumulation of free fluid in the peritoneal cavity
and is usually due to malignant disease, cirrhosis or heart failure15.However
many primary disorders of the peritoneum and visceral organs can produce
ascites and they needs to be consider even in a patient with chronic liver
disease.

8
ASCITES COMPLICATIONS
Infections – Occur in invasive investigations and treatment.
Renal failure
Hepato renal Syndrome
Spontaneous bacterial peritonitis.
DIFFERNCES BETWEEN TRANSUDATE & EXUDATE
FEATURE TRANSUDATE EXUDATE
Appearance Clear-thin Turbid, Hemorrhagic, Thick
Specific gravity less than 1.016 more than 1.016
Protein less than 2.5 g/dl more than 2.5g/dl
Total cell count <250/ml >250/ml
Differential
count
mesothelial cells or
lymphocytes
polymorphs, lymphocyte or RBC
PATHOGENESIS OF ASCITES:
In liver disease the pathogenesis of ascites occur due to secondary cause
of renal sodium and water retention. So many factors are involved in this
mechanism. Because of peripheral arterial dilatation will cause sodium & water
retention and also results in reduction in the effective blood volume.
Natriureteric peptide , prostaglandins , and nitric oxide were act as
vasodilators .
Subsequent reduction in effective blood volume will activates
neurohumoral pressure systems like the sympathetic nervous system & the

9
rennin angiotensin system . That will cause salt and water retention. Portal
hypertension exerts a local hydrostatic pressure and leads to increased
hepatic and splanchnic production of lymph and transudation of fluid into
the peritoneal cavity .
THE SERUM – ASCITES ALBUMIN GRADIENT
High serum – ascites albumin gradient > 11 g/ l
Portal HT , e.g hepatic cirrhosis
Buddchiari syndrome
Hepatic veno-occlusive disease
Cardiac ascites
Tricuspid regurgitation
Constrictive pericarditis
Right sided heart failure.
Low serum – ascites albumen gradiant ,<11g/l
Peritonial carcinomatosis
Pancreatitis
Pertoneal tuberculosis
Nephrotic syndrome
Low serum albumin may further contributes by a reduction in plasma
oncotic pressure. In ascetic patient in some cases the urine sodium excretion
will rarely goes beyond 5 mmol in 24 hrs .The sodium loss from extra
renal sites accounts 30mml in 24hrs.In general the dietary normal intake of
10
sodium may vary between 120 &200mmol, so it will cause positive sodium
balance of approximately 90 – 170 mmol in 24hrs.
Clinical features;
Within few days or so many weeks the with ascites with abdominal
swelling can occur. The most common precipitating factors were a high
sodium diet or the development of HCC (Hepato Cellular Carcinoma) or
thrombosis of splanchnic vein.In mild to moderate ascites there is presence of
mild discomfort and abdominal pain but if more severe and in massive
ascites there is suspicious of spontaneous bacterial peritonitis, and
accompanied by respiratory distress tense and also causes difficulty
during eating.
By demonstration of shifting dullness the presence of fluid is
confirmed.Many patients also have associate with peripheral edema.
INVESTIGATIONS:
10-20 ml ascitic of fluid received and the following diagnostic test
were performed.
1. Look for cell count : In Bacterial peritonitis the neutrophil count were
above 250 cells/mm.
2. For identification of pathogenic bacteria & acid fast bacilli we can do
the Grams stain& culture and sensitivity test.
3. Protein – A high SAAG of >11g/l suggests portal hypertension and a
low gradient <11g/l is associates with abnormalities of the
peritoneum e.g inflammation , infections and neoplasia.

11
4. For identification of malignant cells,the cytological smear study can
helpful.
5. To exclude the ascites caused by pancreatic cause we should perform
Amylase test.
CAUSES OF ASCITES DIVIDED BY TYPES OF ASCITIC FLUID:
Straw coloured
Malignancy
Cirrhosis
Infective
Tuberculosis
Following intra-abdominal perforation- any bacteria
may be found (e.g E.coli)
Spontaneous in cirrhosis
Hepatic vein obstructions
Chronic pancreatitis
Congestive cardiac failure
Constrictive pericarditis
Meig”syndrome
Hypoproteinemia (e.g nephrotic syndrome)
Chylous:
Obstruction of main lymphatic duct (e.g carcinoma)
Cirrhosis

12
Haemorrhagic:
Malignancy
Rupture of ectopic pregnancy
Abdominal trauma
Acute appendicitis
Ascitic fluid-cytomorphological useful findings:
1 Tight clusters with smooth borders
2 Large papillary groups
3 Signet ring cells in groups
4 Two cell types
5 Abnormal cell morphology
6 Cellular and nuclear molding
Ascitic fluid –Cytomorphalogical less significant findings:
1 Signet ring cells – individual
2 Mitoses, multinucleation
3 Cytoplasmic vacuoles
4 Psammoma bodies
Malignant ascitic fluid
Cellular pattern 1- cells in clusters
2-isolated cells
1-Tight & compact
Smooth borders

13
DD
Carcinoma
Malignant mesothelioma
2-Isolated cells-abnormal single cell , look for small clusters
Abnormal cell morphology:
1 Pleomorphism
2 Hyperchromasia
3 High N/C ratio
4 Clumped irregular chromatin
5 Abnormal nucleoli
6 Intraluminal mucin
Site of origin of tumour by cytomorphology:
1 Signet ring cells in breast , gastric & ovarian carcinoma
2 Indian filing in breast , gastric & pancreatic carcinoma
3 Tight cell balls in breast carcinoma
4 Keratin pearls in squamous cell carcinoma
5 Psammoma bodies in serous papillary carcinoma
6 Melanin in malignant melanoma
7 Intra nuclear inclusions in Adenocarcinoma of lung lipidic, papillary
thyroid carcinoma and Melanomas

14
8 Knobby clusters in mesothelioma, the reactive mesothelial cells may
group. If so the grouping usually presents as loose clusters , without
nuclear overlapping.
Immunohistochemistry is a technique commonly used to identify a tissue
component or an ultrastructure of a cell by means of antigen antibody reaction
tagged by a visible label.
In ascitic cell block preparations by applying IHC malignant mesothelioma
was differentiated from lung adenocarcinoma, MM shows positivity for
calretinin and negative for TTF-1. Whereas in adenocarcinoma it shows
positivity for TTF-1 and negative for calretinin.
MALIGNANTMESOTHELIOMA VS LUNG
ADENOCARCINOMA
Calretinin TTF -1 CEA D2-40
MM + - - +
LA - + + -

15
Adenocarcinoma in ascitic fluid found in males had the commonest
primary site of GIT-Pancreas , and next is GU , and followed by Lung .
Adenocarcinoma in ascitic fluid:
Primary sites in male Primary sites in female
GIT –Pancreas Ovary
GU Breast
Lung GIT- Pancreas
Lung
In female the most common primary sites are ovary , followed by breast
and next is GIT- Pancreas and Lung.
Colonic carcinoma was differentiated by adenocarcinoma of lung in IHC
marker, whereas colonic adenocarcinoma shows positivity for ck-20 and
negative for TTF-1 & ck7. In lung carcinoma TTF-1 is positive and ck-20 is
negative.
Adenocarcinoma of lung Vs Colonic carcinoma:
TTF1 CK20 CK7
Ad.ca.lung + - +
Col.ca - + -
Metastatic adenocarcinoma is differentiated from hepatocellular
carcinoma by shows positivity for ck-7 and negative for HCA. In HCC it
shows positivity for HCA and negative for ck-7.

16
In HCC the IHC marker shows positivity for HCA and shows negative
for RCA&EMA, whereas in RCC positive for RCA&EMA and shows
negative for HCA.
Hepatocellular ca Vs Metast .ade
CK7 HCA
HCC - +
Adeno.ca(Met) + -
Hepatocellular carcinoma Vs Renal cell carcinoma
HCA RCA EMA
HCC + - -
RCC - + +
Small cell carcinoma in ascitic fluid
Low power High power
Tight cell balls Nuclear molding
Indian file/chain Coarse chromatin
Isolated cells may be overlooked Wrinkled nuclear membrane
Occasional cells with nucleoli
In small cell lung carcinoma shows positivity for CK , SYN and CHR
whereas Non small cell lung carcinoma shows positive for CK & NEGATIVE
for CHR.

17
Lung carcinoma:
Non-small cell Vs Small cell
CK SYN CHR TTF-1
Non-small cell + -/+ - +/-
Small cell + + +/- +
Small cell carcinoma in ascitic fluid –DD:
1. Malignant lymphoma
2. Small blue cell tumours
Malignant lymphoma in ascitic fluid:
Low power –Isolated cells
High power- Nuclear variation in size and shape
-Nuclear indendations/convolutions
-Vesicular nuclei with prominent nucleoli
-Individual cell necrosis
-Scant basophilic cytoplasm rarely well preserved
Lymphocytes in effusion:
Effusion type CD45 CD20 CD3
Malignant + + -
Benign + - +
Squamous cell carcinoma are rare in effusions

18
Site of origin Diagnostic difficulties
1.Lung 1.Tumour cells do not shed.
2.Cx 2.May be mistaken for poorly differentiated
3.Skin adenocarcinoma or mesothelioma.
4.Esophagus
Squamous cell carcinoma cells are usually overlooked in body cavity
fluid cytology-only few cells shed. They might be confused with necrosis /
degenerative mesothelial cells.P63 & P40 are helpful to detect squamous
cells16.
In Melanoma differentiated from carcinoma by shows positivity for
S100&HMB-45,and shows negative for CK. Carcinoma shows positivity for
CK and negative for HMB-45.
Carcinoma Vs Melanoma
CK S100 HMB45
Carcinoma + -/+ -
Melanoma - + +
ICC In diagnostic cytology application:
Tumour diagnosis / classification
Prognostic / predictor markers
Target therapy

19
CELL BLOCK TECHNIQUE:
Cell block technique or paraffin embedding of sediments of fluids is
among the oldest methods of preparing material for microscopic examination.
The method uses histologic techniques for processing and thus multiple number
of sections of the material are available for hematoxylin and eosin like the
routine stain and for special stains. It also can used for identification of mucin,
melanin, or other cell products, and identification of many pathogenic bacteria
and fungi or IHC.
The residual material remaining after cytologic preparations can be
subjected to cell block technique. The residual material contains valuable
evidence of tissue fragments for processing by histotechniques. Richardson et
al (1955) have shown that additional diagnoses of cancer can be obtained in 5%
of fluid specimens by cell block sections of residual material, supplementing
the smear technique17. The most appreciable benefit of cell block technique is
to identify the histologic patterns of disease which cannot be correctly
identified in smears .
The best cellular details in cell blocks are obtained with Bouin's fixative
or picric acid fixative. However, a more practical fixative is buffered formalin
that allows a wide range of additional procedures.
Methods:
1.Bacterial Agar Method (3% Agar):
1. Mix sediment or tissue fragments with the fixative along with Fibrin clots
if present. Centrifuge this mixture.
20
2. Pour off supernatant and drain tube well by inverting the tube on a
paper towel.
3. Carefully remove the packed sediment or fibrin clot from the test tube
by means of a spatula and wrap it in lens paper. Place wrapped sediment in
a carefully labelled tissue cassette.
4. If sediment becomes hard and packs well with spatula gently remove it
from the test tube and place it on a paper towel with the conical side up.
5. Afterwards slice the sediment in half from the top to the bottom of the
conical clot with a scalpel.
6. Then place the cut side of the packed sediment in a small pool of
melted agar that has been spread on a glass slide or in a Petri dish. Cover all
exposed areas of the sediment with melted agar and let stand a few minutes
to harden. Care must be taken to avoid bubbles in the agar.
7. Then trim the excess agar from the sediment and slice the sediment in
half from the top to the bottom of the conical clot with a scalpel and place it
in a tissue cassette.
8. Even if the sediment does not pack well or if only a small amount is
available after completion of steps I through 3, a few drops of melted agar
should be added to the test tube and mixed thoroughly with sediment. After
the agar hardens, remove the agar button from gently the test tube and kept
it in a tissue cassette.

21
Method of Preparation of Agar:
The 3% agar is prepared by dissolving 3 g of bacterial agar in 100 ml of
boiling water. The melted agar may be coloured with a small amount of food
coloring to ensure contrast with the paraffin. Then the dissolved agar should be
poured into individual sterile glass tubes with a screw cap. Cap the tubes loosely
until the agar cools and hardens. When the agar has cooled, tighten the caps and
kept the tubes in a refrigerator until ready for use. If it is needed, melt the agar in
a 600C water bath. Then discard unused agar at the end of the day.
2.Fixed Sediment Method18
1. First Mix sediment or tissue fragments with the fixative along with
fibrin clots if present. Centrifuge this mixture.
2. Then pour off supernatant and drain tube well by inverting the tube on a
paper towel.
3. Afterwards carefully remove the packed sediment or fibrin clot from
the test tube by means of a spatula and wrap it in lens paper. Then place
wrapped sediment carefully in a labelled tissue cassette.
4. Finally put tissue cassette into a jar of the same type of fixative used
before. Then process as tissue biopsy.

22
3.Plasma-Thrombin Clot Method:
Thoroughly mix a few drops of blood plasma obtained from blood bank
with the fresh unfixed sediment. After that the plasma may be colored
with a small amount of food coloring to obtain contrast with the
paraffin. If the sample was prefixed with alcohol, the sediment must be
washed several times with a balanced salt solution, because alcohol
inhibits the clotting action of plasma and thrombin.
Then add the same few drops of thrombin solution as of the pooled
plasma and mix well. Thrombin is prepared by adding 5000
units(topical, 1 vial) with 10 ml of distilled water.
This mixture will form a clot in 1 to 2 minutes if the reagents are fresh
and not too cold. Then kept resulting clot in a cassette that has been
lined with lens paper to prevent the clot from oozing through the holes.
Since this clot is very soft instead of a forceps, a spatula, is recommended
for transfer to the embedding mold.
4.Simplified Cell Block Technique:
In 1988, Krogerus and Anderson19introduced a simple technique of cell
block preparation from materials obtained from effusions, fine-needle
aspiration and brushings. The technique is unique in that, the procedure is and
carried out in the sample tube, ensuring minimal cell loss. There is no transfer
of cells to a cassette is necessary, eliminating the need for wrapping paper,
agar, or thrombin. The procedure is as follows:

23
In a 50-ml plastic, conical centrifuge tube, fix the cell sample with 50%
alcohol for I hour.
Then spin sample at 300 g for totally 7 minutes and pour off supernatant.
After that re-suspend cell pellet in 3 ml of acetone for 10 minutes.
Then spin sample at 300 g for 10 minutes. Pour off acetone.
Place tubes for 1 hour on a warm plate (not more than 600C).
Then add melted paraffin to the dry, warm pellet.
After paraffin has solidified, to remove block tap the bottom of the tube.
Cut and process the conical end of the paraffin block as you would any
tissue section.
5.Microwave Technique for Rapid Processing of Cell Block:
Since in the early 1970s, microwaves have been used by histopathology
laboratories to shorten fixation and processing times of tissue samples. Kok et
a121in 1988 described a method in which cell blocks from fresh sputum can be
prepared in 35 minutes. The method can be adapted for use with other types of
specimens. Best results were obtained with a fixative consisting of 500 ml of
96% ethyl alcohol, 430 ml of distilled water, and 70 ml of polyethylene glycol.
Place sputum in 40 ml of fixative in a microwave-safe jar.
Microwave sample at 450 watts with the temperature set at 700C. This
usually takes 5 minutes.
Place the sputum, which has become condensed and rubbery, into a tissue
cassette. Then put the cassette into 40 ml of absolute ethyl alcohol and
microwave at 450 watts and 700C. This usually takes 3 minutes;
24
however, let the cassette sit in the microwave for another 2 minutes.
Transfer cassette to 40 ml of Histoclear. Microwave at 450 watts or 800C
for 7 minutes.
Then embed the material, cool blocks, cut and mount sections.
The sections can be de-paraffinized by kept them in Histoclear and
microwaving them for 5 minutes at 700 watts and then stained by the method
of choice.
6.Compact Cell Block Technique:
By Yang et al (1998)20described a technique that produces a compact cell
block about 10% to 20% the size of conventional cell blocks. Here cells are
packed into a small area free of extracellular protein and erythrocytes, thereby
reducing the overall time for screening and often the need for deeper cuts are
eliminated.
Pour off the supernatant after centrifugation of 40 cc of a well mixed
aliquot of the sample.
Then mix the sediment with an equal volume of Cyto Rich Red.
After 2 minutes, add 4 drops of plasma and 3 drops of thrombin (5,000
PI/ 10 ml).
Afterwards gently agitate the mixture. When the clotting stops, the clot
is slided onto the lens paper placed on top of paper towels.
The lens paper is folded over the clot. Press and mold the clot flat and
compact with a gloved fingertip. Wrap the compact clot tightly in lens
paper and place in fixative.

25
7.Modified cell block technique:
Nathan et al in 2000 suggested a modified cell block technique by using
Nathan alcohol formalin substitute (NAFS)29. After preparing smears, the
needles and syringes utilized for fine-needle aspirates were rinsed in 10 mL of
50% ethanol in a specimen container. Any residual clot or tissue in the hub of
needles was removed carefully in the laboratory with the aid of another needle
and rinsed in 50% ethanol. Then at 4,000 rpm for 6 minutes, the material was
centrifuged in a 10-mL centrifuge tube to create one or more cell pellets. The
supernatant fluid is decanted and the deposit fixed in freshly prepared Nathan
alcohol formalin substitute (NAFS) consisting of 9 parts oi- 100% ethanol and
1 part of 40% formaldehyde. Since formalin oxidises to formic acid on
exposure to air, forming acid hematin pigment artifacts a fresh working
solution is desired.
Centrifuged deposits of effusions, clots, washings, and other fluids,
following smear preparations, were fixed similarly for cell blocking. When
centrifuged deposits were more than 0.2 ml-J thick, to facilitate adequate
fixation, the deposit was detached carefully from the bottom of the centrifuge
tube with the aid of a sharp-edged dipstick. If the centrifuged deposits were too
thick, the material was divided into several tubes for multiple cell blocks
before fixing in NAFS solution. The fixed cell pellets, at the end of fixation for
45 minutes, were re-centrifuged for 6 minutes at 4,000 rpm. These pellets
should detach themselves or can be removed easily with a disposable Pasteur
pipette following centrifugation. After wrapping the cell pellets in crayon

26
paper and placing in a cassette it is stored in 80% ethanol until ready for
processing in the automatic tissue processor.
8.Cell blocks from Millipore Filters:
By Baloch et al (1999)22described a technique by which a portion of a
Papanicolaou stained Millipore filter is converted to a cell block for other stains
or immunocytochemical analysis for specimens of limited cellularity. This
technique produces hematoxylin and eosin (H&E) preparations with excellent
morphology and antibody test results. In most cases, routine cell blocks with
adequate background staining is not seen. The original cytologic preparation is
preserved as only half of the filter is used.
9.Thromboplastin Plasma Cell Block (TP-CB) technique:
Kulkarni et al in 2009 used plasma thromboplastin for preparing cell
block30.After preparing conventional smears, the remaining fluid were
centrifuged. In the case of aspirations, rinses of syringes and needles were
centrifuged by collecting it in normal saline. The supernatant was carefully
removed and the sediment was mixed with two drops of pooled plasma that
was kept frozen and brought to room temperature before use. Subsequently,
four drops of thromboplastin were added and mixed again. The thromboplastin
used for the TP-CB was the same as the one used for the thromboplastin test
and it should be stored in the refrigerator between 2-8 C o and brought to room
temperature before use. The tube was allowed to stand for 5 min. and the
resultant clot was slid into a filter paper pre-moistened with formalin, wrapped
and put in a cassette. The tissue cassette was then fixed in buffered formalin for

27
at least 4 hrs. After-wards, the sample was processed as usual for histological
techniques.
10. Shidhams protocol:
For evaluation of non-gynecologic cytology, cell block technique is a
most acceptable tool. It can help the cytopathologist to the morphologic
specimen detail like the architecture of the lesion. They can also allow for the
evaluation of ancillary studies like immunocytochemistry, in-situ hybridization
tests (FISH/CISH) and in-situ polymerase chain reaction (PCR). Cell blocks
have traditionally been applied to cytology of non-gynecologic specimens like
fine needle aspiration biopsies and body fluid effusions.
Liquid based non-gynecologic specimens have many individual scattered
cells When the cellularity is less, the cell block sections are difficult to
achieve. The histotechnologist making sections of the block cannot identify the
level of highest concentration of cells for sectioning and transferring it to the
glass slides for analysis. So the cell block area have maximum cells will be
missed, either by cutting past the region or not cutting deep enough. Current
Shidham protocol eliminates these drawbacks. This protocol is standardized
and reported for non-gynecologic specimens like FNA, brushings, effusion
fluids, cyst contents etc., for improving the quality of material in cell blocks.
The following are the two critical features for preparing cell blocks from
hypocellular specimens with scattered single loose cells by this protocol23-26

28
1. Step to concentrate the cells along a parallel plane to the cutting surface
of the cell block.
2. Dark inclusion as AV-marker, serving like a beacon for two purposes:
i.To visualize the site of cellular concentration, as dark colored beacon,
exposed during cutting. The ability to identify a dark coloured beacon
prevents from cutting through the+ 8 level with most cells or not
cutting too superficial into the level of highest concentration of cells.
ii. With the SCIP approach for assessment of coordinate immunoreactivity
the beacon will help to locate group of cells or particular cells27,28
Protocol-
Sample Preparation:
l) The residual liquid based cytology (LBC) specimen is transferred to a flat
bottomed glass tube (15mm diameter x 45mm).The (28 x 85mm) sized
plastic carrier tube for centrifugation is used. Afterwards the tube with
glass bottom is removed from the carrier tube then the supernatant is
poured off.
2) To prevent the spillage of heating water , the glass tube is capped and kept
inside a larger &flat bottom carrier plastic tube.
3) Then for centrifugation , the carrier plastic tube carrier with the glass
tube is capped and placed for centrifugation (with swiveling cups and not
fixed angle cups so that the cells fall perpendicularly to the flat bottom of
the glass tube) at 1805 G (3000 rpms, rotor radius- 17cm) for totally five
minutes.
29
4) Then the tubes were removed vertically from the centrifuge followed by
the removal of the smaller glass tube with forceps from the larger carrier
plastic tube avoiding any disturbance to the sedimented pellet of cells.
5) Afterwards the glass tube with specimen is uncapped then the supernatant
is poured off without disturbing the layer of cells, which were flat.
Inclusion of the reference coordinates, A V-marker and addition of gel:
1. A dark beacon AV-marker (about 2 mm X 2 mm size, flat surfaced,
fragment of dark colored, sectionable material) which is added, acts as a
sign post in the glass tube.
2. Afterwards an aliquot of histogel (HG) is liquefied by melting it in a
microwave at medium power for totally 10 seconds.
3. Then 0.5 ml of molten HG is added to the tube and mixed with the
sediment quickly and recapped (Proceed to the next step quickly without
allowing the HG to begin solidifying).
4. Then in the carrier plastic tube 2.5 ml of warm (45 0 C) water is added .
5. The next step is to kept the smaller glass tube capped is placed inside
the plastic tube which contains warm water. This step is essential to
keep the HG from solidification. Because the next step will need this.
6. The carrier plastic tube is placed for centrifugation (with swiveling cups
and not fixed angle cups so that the cells fall perpendicularly to the flat
bottom of the glass tube), for five minutes at 1805 G (3000 rpms, rotor
radius- 17cm). The centrifugation pushes the AV-marker and
30
concentrates the cells of the final paraffin embedded cell block into a
layer closer to the cutting surface.
7. The tubes were removed vertically and gently from the centrifuge
avoiding disturbance to the sedimented thin layer of cells at the bottom.
8. Uncapped the larger plastic tube followed by removal of the smaller
glass tube is removed vertically with a forceps and the sedimented layer
of cells should not be disturbed.
9. To cool and solidify the HG the small glass tube is kept in vertical
position& refrigerated for 15 mnts.
Removal of the cell block as a button of gel with specimen for final
processing:
1. The solidified HG disk, with the layer of concentrated/sediment
specimen at the bottom is dislodged from the flat bottom glass tube by
squirting 10% formalin through a 23-gauge needle with the syringe.
2. Then at the periphery of the HG disc with specimen the needle is
inserted along the side of the tube .
3. After that the formalin is being slowly pushed in through the syringe.
This will make in the separation of the HG button along with dark colored
beacon AV-marker and the concentrated specimen in it, from the flat bottom
of the glass tube.
4. Afterwards cell block (gel button with specimen cells) is then kept in a
cassette which is labelled. Then tissue processing done to prepare paraffin
embedded cell blocks.

31
Embedding and cutting of the specimen:
1. The dark beacon marker side facing down as cutting surface, the disc is
embedded in the paraffin.
2. Untill the dark colored A V-marker as a beacon is clearly visible
&exposed the cell block is sectioned.
3Three to four micron sections are cut from this level which should contain
most of the singly scattered cells from the specimen.
4The sections are collected on the glass slide for further staining,
immunohistochemical staining or other tests as indicated. Generally for
immunostaining, to prevent loss of sections and floating from the slides
during the immunostaining steps , coated slides were used.
IMMUNOHISTOCHEMISTRY
IHC is one of the most powerful and widely used ancillary methods in
surgical pathology31.This technique makes it possible to both visualize cell and
differentiation markers in standard tissue sections by light microscopy and also
has revolutionized diagnostic surgical pathology.
The utilization of IHC requires test selection, specimen acquisition and
management, methodology , validation, reporting and interpretation.
Test selection:
Usually IHC stains are ordered after examination of H&E stained
sections. The common indications for IHC are the diagnosis and
characterization of neoplasms and other indications such as detection of
infectious organisms and evaluation of prognostic and or predictive factors32.
32
Use of specific immunostain is driven by the clinical and morphological
context of each individual case. For this panel of antibodies are used. These
panels should be devised on the basis of the anticipated value added to the
clinical and radiographic and also the pathological differential diagnosis33.
Specimen type & Tissue management:
Immunostain also performed on cytological specimens although they
usually performed on standard histological tissue sections. Here this
discussion focuses on tissues fixed in 10% neutral buffered formalin, since the
tissue type commonly available in routine clinical practice.
Immediate fixation in neutral formalin for 12-48 hrs at room temperature
is needed. Formalin induces cross links that will mask some epitopes results in
loss of immune reactivity. And also decalcification of bone samples can also
will cause loss of immune reactivity. The unmasking of some epitopes from
FFPE tissue will be accompanied by antigen retrieval techniques. The
immunostaining must be done on freshly cut sections from the paraffin
block34. Since unstained sections exposed to air will lose antigen
immunoreactivity over the course of days to weeks
METHODOLOGY:
1. The primary antibody:-It is an immunoglobulin that binds to target antigen
in the tissue sections. The primary antibody is either a monoclonal
antibody derived from hybridoma technique or a polyclonal antibody from
an antiserum35.Every antibody whether it is monoclonal or polyclonal in
33
origin needs to be tested for sensitivity and specificity in target antigen
detection.
2. Background staining: It results from nonspecific antibody binding and
from endogenous enzymes that will non-specifically interact with
chromogenic substrate. The nonspecific antibody binding is more likely to
occur with polyclonal antibodies. The endogenous enzymes that cause
background staining were found in normal cells including neutrophils,
eosinophil, erythrocytes, plasma cells and neoplastic cells36.
3. Detection systems:
a. Direct conjugate labelled antibody method.
By this method the label such as peroxidase or fluorescein is
directly chemically linked to the primary antibody.
b. Indirect or sandwich method-
The primary antibody is unlabeled and a secondary antibody that
reactive against the primary antibody carries the label.
c. Unlabeled antibody method:
This method is also known as the PAP method, the bridge antibody,
directed against both the primary antibody and the antiperoxidase
antibody it links the primary antibody tissue antigen reaction to the signal
generated by the peroxidase.
d. Avidin – biotin conjugate method:
Here biotinylated secondary antibody is used to recognize the
primary antibody37.Avidin complexed with biotinylated peroxidase is

34
then bind with secondary antibody. So these reactions deliver several
peroxidase molecules to the primary antibody binding site and so boost
sensitivity.
e. Tyramine amplification method:
As there is major accumulation of biotin at the antigen – primary
antibody reaction site as a result of the catalytic activity of peroxidase on
biotinylated tyramine there is increased sensitivity.
f. Polymer – based labels:
This approach use dextran chain polymers to localize numerous
enzymes molecules to the antigens site by linking multiple antibody and
enzymes molecules together along the polymer chain.
g. Alkaline phosphatase:
It can be used instead of peroxidase when the target antigen is in
tissues rich in myeloid cells that contain high levels of endogenous
peroxidases, such as bone marrow.
h. Chromogens:
these are the colour producing reactants in the detection system.
DAB –produces brown colour, AEC- produces red colour.
i. Counter staining:
It is mostly accomplished using the nuclear stain hematoxylin.
Avoid overstaining.
j. Antibody cocktails
It can be used to detect two or more antigen s at the same time.
35
k. Automatation:
Here automated immunostaining devices are in routine use in many
labs and will improve standardization throughput, and reproducibility of
immunohistochemical procedures.
VALIDATION:
Here positive and negative controls should be included in every sample
and reviewed along with the test immunohistochemical reaction43. Some
laboratory place a positive control tissue section on the same slide as the test
tissue section for some immunostain, there may be an internal positive control
in the test tissue. A negative control may be generated using a tissue known to
lack the antigen of interest.
REPORTING43:
1- All immunostains must be reported if it is positive, negative or non-
contributory.
2- Differential diagnosis justifying immunostain selection should be given.
3- The report should include the nature of specimen tested, the paraffin
block number used to obtain sections for immunostain, the antibodies
used and the result of staining for each antibody including cellular
localization when relevant.
4- Interpretation of the findings in the context of the diagnosis, with
reference to the associated surgical pathology report if
immunohistochemical results are reported separately.

36
5- The exact protocols, antigen retrieval methods and reaction conditions
need not be part of the report but must be available in laboratory manuals
and records.
INTERPRETATION43:
Including their significance, it will be integrated with the interpretation
of the clinical, radiographic, gross and histopathologic findings of the case as
well as the results of any additional ancillary tests. Then following evaluation
of positive and negative controls the tissue section should be assessed for the
presence of the areas of interest localization of immunohistochemical signal
and intensity of signals and number of immune reactive cells or foci. Finally a
comment in the report should be indicate that immunostains were used to
establish , confirm or support a diagnosis or that they were non-contributory.
Ki67 marker44:
It is an antigen that corresponds to a nuclear non histone protein
expressed by cells in the proliferative phase G1, G2 , M&S.
Here the original antibody against the marker worked only in fresh
frozen sections, but monoclonal antibodies have been developed that detect
formalin resistant epitopes (MIB-1&MIB-3). In general, there is a good
correlation between ki67 staining & mitotic count.
Positive nuclei stain brown and percentage of positive nuclei divided by
total nuclei can be counted and calculated. This is called labelling index (LI)
or proliferation index(PI).

37
The ki67 protein was defined by the prototype monoclonal antibody ki67
that was generated by immunizing mice with nuclei of the Hodgkin lymphoma
cell line L42844. The name was derived from the city of origin –Kiel, Germany
and the number of the original clone in the 96 well plate45.
The MIB antibody was the first to detect ki67 epitopes in paraffin
sections of formalin fixed tissue. Antibodies that detect ki67 in paraffin
sections are preferred because they cover all proliferative phase of the cell
cycle and they provide crisp distinction between positive and negative cells.
Now there are antibodies other than MIB 1 that detected ki67 in paraffin
and ki67 is a more common term. This PI is usually sampled in regions of
highest proliferation called Hot spots.
A simple way to do this is to dot hot spot s with a pen under a 40x
objective.
Antibodies to ki67 have greater potential in diagnostic pathology than
this for delivered largely due to wide variations in sampling and counting
techniques46. Even when hot spots are counted, the pathologist may count,
each hot spots in a field of 100 cells , 1000 cells or the number of cells seen in
a given objective lens. Standardization of the method of counting is needed..
A standard number of 100 cells is better than large numbers for brain
tumour because the smaller denominator around hot spots accentuates
difference in proliferation among low grade tumors. Low grade tumors have
few or inconspicuous mitoses, and this where the ki67 is most useful. Most
high grade tumors show enough mitoses to estimates proliferation. However in

38
low grade tumors a spectrum of proliferative capacity can be exposed with
ki67. If we look for hot spots with ki67 like we look for single or multiple
mitoses in tumors a demonstration of 1000 cells diminishes the impact of the
hot spot in judging proliferation. Infact, the argument could be made to count
only the number of cells within the periphery of the hot spot. That ratio of
positive nuclei to all nuclei would maximize distinction between high and low
proliferative capacities.
There are rare situations where a uniquely large series of patients tumors
have been processed and counted in a specific manner. There PI correlated
with outcome, and PI of a certain percentage separated most good from bad
outcomes. In such cases reproducing the counting method on your own case
makes sense. Distinguising between central neurocytes may be one examples
that applies.
Here we have sufficient tumors of many kinds to establish our own
baseline. Ki67 predicts survival among fibrillary astrocytic neoplasm. These
PIs augment prognostication by standard histopathologic criteria.
Studies have revealed the prognostic value of MIB 1 labelling indices. In
one analysis , MIB 1 PI was the only independent predictor of survival among
only grade II astrocytes patients, MIB1 distinguishes tumors with good
prognosis by their low labelling indices. Lower MIB1 PI are found in younger
patients with glioblastomas , and they have a significantly better prognosis
than to older patients.

39
As valuable as it is to assessment of proliferative capacity, the ki67 PI is
a semi quantitative assay based on a qualitative staining method. Thus ki67
staining methods and counting criteria vary among laboratories.
A published value of PIs may not be relevant to a different laboratory.
This means that individual laboratories should set their own standards for PIs
based on their previous cases. Organisations that standardize assays worldwide
might contribute to standardisation of ki67 staining method and counting
criteria.
Basic points of information about ki67 include the ability of reactive and
inflammatory changes to produce conspicuous PIs easily as high as most
gliomas of low or intermediate grade47. (upto 20%). Thus a good pathologist
and H&E stain is essential for setting the context for interpretation of the ki67
PI. A check on nuclear features of ki67 positive cells can reveal very
important data, rounded nuclei of reactive cells or leucocytes elongated nuclei
in astrocytoma cells mixed with other glioma cells and more mitoses than seen
on other stains(they look like dark granule). Always consider structure and
contetxt when interpreting this and other stains.
Ki67 is an s – phase fraction related antigen which is a proliferative
marker. This can be detected by monoclonal antibodies and do not require
flow cytometry: technique as is required for s- phase related antigen44. This is
used to establish growth fraction of tumor cells determined by the number of
the positive tumor cells among the total number of cells and calculated as
index.

40
The index correlates well with the histological grading of the neoplasms.
Low grade lymphomas will show KI67 INDEX OF >20-25% will have a
more aggressive course and among intermediate and high grade lymphomas
ki67 index of >60% indicates poorer survival.
Ki67 used as a prognostic marker for some tumors. It detects number of
cycling cells in Burkitt lymphoma and large B cell lymphoma .
Aberrent membrane and cytoplasmic immunoreactivity is present in
trabecular hyalinising adenoma of thyroid and sclerosing hemangioma of the
lung.
METHODS:
There are many methods for scoring. Among the manual methods the
most reliable one is camera / printed images is widely used48. And it needs
counting 500 to 2000 cells to determine the K I67 scoring. But this method is
time and energy consuming.
Another method is after counting Ki67 positive tumor cells in the whole
image within the one tenth of the same image. The tumor cells were counted
with the aid of a previously prepared grid on an acetate sheet. Then the cell
counted was multiplied by 10 to calculate the total count and the ki67 score
was obtained. Then the agreement between the results of conventional whole
image counting method and results of acetate grid method was assessed.
Totally nearly perfect agreement was achieved regarding the total count
& ki67 score. The agreement on tumour grade between two methods was
perfect.

41
The total time spent on the process was significantly less than that spent
on the conventional method.
The acetate grid method might be considered an alternative method for
KI67 scoring in neuroendocrine tumors49.
In general ki67 levels over 15% or 25% are considered very high . The
high ki67 has been linked to unfavourable breast cancer outcomes in numerous
breast cancer studies50. And also ki67 provides information beyond that given
by other prognostic indicators., like that given by tumour size, grade ,
hormone receptor status and number of positive lymph node. The tumours of
the given size and ki67 have a better prognosis than tumors of the same size
and high ki67.s
Measurement of the Ki-S2 labelling index of a tumour sample also may
improve a clinician’s ability to make an accurate prognosis and not need
adjuvant therapy.
Scoring :
<10% score 0
1-20% score 1
21-50% score 2
>50% score 3

42
MESOTHELIAL MARKERS
The immunohistochemical marker that is both sensitive and specific for
malignant mesothelioma were found elusive. A pattern based approach to the
diagnosis of mesothelial lesions and their mimics and it shows the role of
immunohistochemistry and other ancillary techniques+61.When evaluating
suspected mesothelial lesions the morphological pattern most commonly
presented were spindle cell epitheloid pattern, or sarcomatoid pattern, biphasic
pattern , fibrotic pattern or pauci cellular .
Epithelioid Pattern of MM:
It has an epitheloid morphology consist of bland cells with eosinophilic
cytoplasm some cells have more anaplastic features. Epitheloid variant is the
most common type of MM.
Sarcomatoid mesothelioma:
It composed of spindle cells arranged in haphazard distribution.
Immunohistochemically this type less likely express CK5/6 and areas of
chondrosarcomatous or osteosarcomatous differentiation will show desmin,
actin, vimentin and s100 positive staining.
Cytokeratin 5/6 :
Cytokeratin 5/6 are high molecular weight, basic cytokeratins which
corresponds to keratins 58 and 56 kDa respectively. Cytokeratin 5/6 is most
commonly used in the diagnosis of mesothelioma, where it stains tumour cells
and reactive mesothelium in a diffuse cytoplasmic fashion68. Most pulmonary
adeno carcinomas do not express CK 5/6 , although one study showed that 19%
43
of them had weak or focal positive staining . Antibodies to CH 5/6 are best used
in a panel of antibodies for the differential diagnosis of mesothelioma and
pulmonary adeno carcinoma.
In more than 95% of EMM diffuse staining with pan CK 5/6 will useful
to confirms an epithelial process CK5/6. In a variety of adenocarcinomas
Cytokeratin 5/6 expression has been reported occasionally. In cases with a
squamoid morphology, the CK5/6 expression should be interpreted with caution
since most of the squamous cell carcinomas were positive.
Calretinin:
Calretinin is a calcium binding protein with a molecular weight of 29kDa
. Calretinin is constantly expressed in the normal and reactive mesothelial cell
lining of serosal membranes. It stains in diffuse nuclear/ cytoplasmic pattern in
formalin fixed paraffin embedded tissue sections. It is probably the most
specific marker for mesothelial cells. The presence of calretinin is also a
sensitive and specific indicator of normal and reactive mesothelial cells in
effusion cytology. And calretinin antibody is auseful marker to distinguish
mesothelioma from adenocarcinoma.
Depending on the clone used, the sensitivity of calretinin was varied and
it is in the range of 73-100%. Malignant mesothelioma commonly stain with
calretinin in the nuclear and cytoplasmic area even though the nuclear staining
is considered specific.
Monoclonal CEA is a positive marker in most of the pulmonary
adenocarcinomas and it also a reliable negative marker for EMM.
44
Thyroid transcription factor- 1(TTF)
Human TTF is a single polypeptide of 371 aminoacids. It is expressed at
the onset of lung and thyroid organogenesis and is essential for the normal
development of these organs65. It is expressed in thyroid follicular epithelial
cells, pulmonary type 11 cells and clara cells which makes it a useful diagnostic
epitope to identify adnocarcnomas. It is a useful marker in differential diagnosis
of primary tumours of lung and thyroid versus metastases from other organs. It
shows a nuclear staining pattern . TTF-1 is expressed in 90% of small cell
carcinomas of the lung , 80-90% of pulmonary carcinoids and 70-100% of
adenocarcinomas of lung.
Thyroid transcription factor -1 shows nuclear staining in more than75%
of pulmonary adenocarcinomas and is commonly negative in EMM.
HBME 1:
HBME 1 was derived from human malignant epithelioid mesothelioma
cells. It consist of antigens on the cell membrane of mesothelial cells, both
benign and malignant. So it shows membranous cell surface pattern in
epithelioid mesotheliomas , while it is negative or shows cytoplasmic staining in
adenocarcinoma. Its usefulness is limited by its low specificity.
B72.3:
The mouse monoclonal antibody to B72.3 RECOGNIZES A HIGH
MOLECULAR WEIGHT GLYCOPROTEIN COMPLEX , TAG 72 (tumor
associated glycoprotein- 72). This antibody works on formalin fixed , paraffin
embedded tissues and cell blocks prepared from body fluids. It can be used in an

45
antibody panel to distinguish adenocarcinomas from mesotheliomas. It has
been shown to be positive in about 90% of pulmonary adenocarcinomas and in
0-14% of mesotheliomas54.
In peritoneal biopsies the B72.3, is a suitable choice which diffusely
stains around 70-80% of adenocarcinomas, including ovarian carcinoma, and is
negative in most the EMMs. As thyroid transcription factor -1 –positive
tumours do not generally enter the differential diagnosis of peritoneal tumours,
Ber – EP4:
Antibody to Ber –EP4 shows a broad pattern of reactivity with human
epithelial tissues , from simple epithelia to basal layers of stratified , non-
keratinized squamous epithelium and epidermis. The staining pattern is
membranous and used to distinguish adenocarcinoma from from mesothelioma.
It has very high sensitivity(94- 100%) for lung adenocarcinoma, it also stains 9-
18% of epithelioid mesotheliomas60. So the interpretation of staining result
should always be done in combination with other antibodies. In peritoneal
biopsies Ber EP4 could be substituted as a second carcinoma .Like the B72.3,
Ber –EP4 is positive diffusely in a high proportion of adenocarcinomas. In a
minority of malignant mesotheliomas Ber EP4 staining is typically restricted to
a few cells.
In case of tumours that are positive for only one of the two mesothelial –
associated or carcinoma – associated markers, only pan – cytokeratin – positive,
or show doubtful results, additional markers can be helpful. The newly

46
developed markers like D2-40 and anti – podoplanin show membranous
staining in 86-96% of EMMs56.
Wilms tumour gene product (WT -1) is a nuclear protein expressed in the
mesothelial cells . Nuclear staining is seen in 71-95 % of malignant
mesotheliomas and 0-22% in adenocarcinoma.
Thrombomodulin (CD 141) is less sensitive and specific than other
markers . It shows membranous staining in 30-100 % of the epithelial
masothelioma and in 5-77% of adenocarcinoma.
Squamous cell carcinoma:
Squamous cell carcinomas are immunoreactive to most epithelial
markers such as pancytokeratin , high molecular weight keratins , low molecular
weight keratins and focally epithelial membrane antigen. Staining with p63 and
TTF-1 was known to be useful in differentiating small cell carcinoma from
poorly differentiated squamous cell carcinoma. Small cell carcinoma were
negative for p63 and 85% of them were positive for TTF-1, whereas in all
poorly differentiated squamous cell carcinoma were positive for p63 and
negative for TTF-1.
Carcinoembryonic antigen:
It is a glycoprotein of heterogenous composition with molecular weight
of 2000000 and normally detected in the glycocalyx of fetal epithelial cells ,
particularly of mucin secreting glandular nature.Present in large quantities in
carcinomas particularly seen in adenocarcinomas of the GIT –includes pancreas,

47
lung and in thyroid medullary carcinoma. Since it is primarily expressed by fetal
tissues and malignant tumours , it is refered to as an oncofetal antigen.
Betacatenin:
It is a widely expressed 90kDa protein with a major role in cell adhesion
and Wingless- type (Wnt) signalling. At the cell membrane site , Beta –catenin
is complexed with E-cadherin to generate cell adhesion complexes that assure
the structural integrity of many epithelial tissues. Immunohistochemical
demonstration of nuclear staining for Beta catenin is mainly used in the
differential diagnosis between fibromatosis and other spindle cell mesenchymal
neoplasms. Beta catenin is also useful in the diagnosis of colorectal
adenocarcinoma, craniopharyngioma , solid and pseudopapillary tumor of the
pancreas and other neoplasms.
CA19-9:
It is a carbohydrate antigen recognized by a monoclonal antibody
produced by a hybridoma raised against a human colonic carcinoma cell line .
Immunohistochemically positive reactions are obtained in most pancreatobiliary
adenocarcinomas and urothelial carcinomas. Adenocarcinoma of other sites can
also positive but with a lower frequency.
CA-125:
It is a cell surface glycoprotein originally identified in mucinous
epithelial ovarian tumors and recognized by the monoclonal antibody OC 125.
It is also expressed by adenocarcinomas of other sites including cervix,
endometrium, gastrointestinal tract , thyroid, and breast.
48
Alpha-fetoprotein:
It is a major plasma component of the fetus, the main sources being the
liver and the visceral endoderm of the yolk sac. It is one of the major oncofetal
antigens.It is invariably present in yolk sac tumors and in high proportion of
other germ cell tumours. It is also present in hepatocytic and hepatoid
neoplasms, in pancreatic tumors with acinar cell differentiation and in a variety
of carcinomas with germ cell like features.
49
METHODOLOGY
MATERIALS AND METHODS
MATERIAL:
During the period from December 2014 to May 2016, 100 samples of
ascitic fluid that were received in the cytology section of Department of
pathology, Tirunelveli Medical College and Hospital were studied by cell block
technique.
The clinical details of patients like name, age, sex and diagnosis were
recorded. After reporting the conventional cytological smear the representative
received samples were processed for cell block preparations immediately. Some
samples were stored in the refrigerator and processed on next day.
From the sample, one part was taken and centrifuged at 2500 Rpm for
totally 15 minutes, then the sediment was smeared on glass slide.
The smears were fixed in 99.9% isopropyl alcohol for totally 20 minutes,
then stained with Haematoxylin & Eosin. Afterwards the remaining other part
were used for cell block preparation by plasma thromboplastin method.
Plasma thromboplastin method:
By this method cell blocks were prepared. Ascitic fluid samples were
centrifuged at 2500 rpm for 15 minutes. Then followed by centrifuging,
supernatant was removed and discarded. Then the remaining sediment was
mixed with 4 drops of plasma that was kept frozen. This plasma was brought to
room temperature before use. Followed by few drops of thromboplastin (4-6
drops) were added and mixed. Thromboplastin which was stored at 20C and 80C
50
was brought to the room temperature before use. The tube containing the above
mixture was kept undisturbed for few minutes until clot was formed. If there
was no clot formation found 4 more extra drops of thromboplastin was added
until clot appeared. Then the formed clot was scooped out and placed into a
filter paper and kept in cassette. The tissue cassette was then fixed in 10%
neutral buffered formalin for at least 4 hrs. Then it was processed along with
routine histopathological specimens. Cell blocks were made and tissue section
of 4-5micron thickness were taken and stained with H &E. Then blocks were
used for IHC whenever need.
Immunohistochemistry Procedure:
1. 3 – 4 µm thickness section where taken from the cell block in a poly
lysine coated adhesive slides and then slides are incubated 450c for one
hour.
2. Then slides were subjected to two changes of xylene for 5 minutes each
for deparaffinization. Afterward the slides were shifted to absolute
alcohol for 5 minutes then followed by 80% and 70% alcohol for 5
minutes each to rehydrate the sections.
3. Afterward section were placed in running tap water for 5 minutes and
washed in distilled water.
4. Then antigen retrieval was performed by using pressure cooker in TRIS
EDTA buffer. Then sections were cooled and slides were washed in
distilled water.
51
5. The endogenous peroxidase activity was removed by incubating the
section with few drops of 3% peroxide block in a humidity chamber.
After the sections are washed in washed buffer, next protein block was
added for 20 minutes.
6. Afterwards primary antibody was added to the section and incubated for
30 minutes followed by primary amplifier was added for 20 minutes and
sections are washed in wash buffer.
7. Then DAB chromogen was added over the section and incubated for 4
minutes and washed with two changes of distilled water.
8. The next step was counterstaining with Mayer’s hematoxylin for 30
seconds and washed in running tap water.
9. Then dehydration was done in few changes of 100% alcohol. Afterwards
mounting was done by DPX mounting and observed under microscope.

52
Preparation of Buffer:
TRIS _ EDTA buffer (pH 9.0)
TRIS - 6.05gm
EDTA - 0.744gm
Distilled water - 1000ml
TRIS wash buffer:
Sodium chloride - 8gm
1N Hcl - 4ml
Distilled water - 1000ml
Interpretation of conventional smears and cell block:
A comparison between the cellularity, morphological preservation,
architectural preservation and background was performed on both conventional
smear and cell block based on the point scoring system described by Mair et
al68 .
53
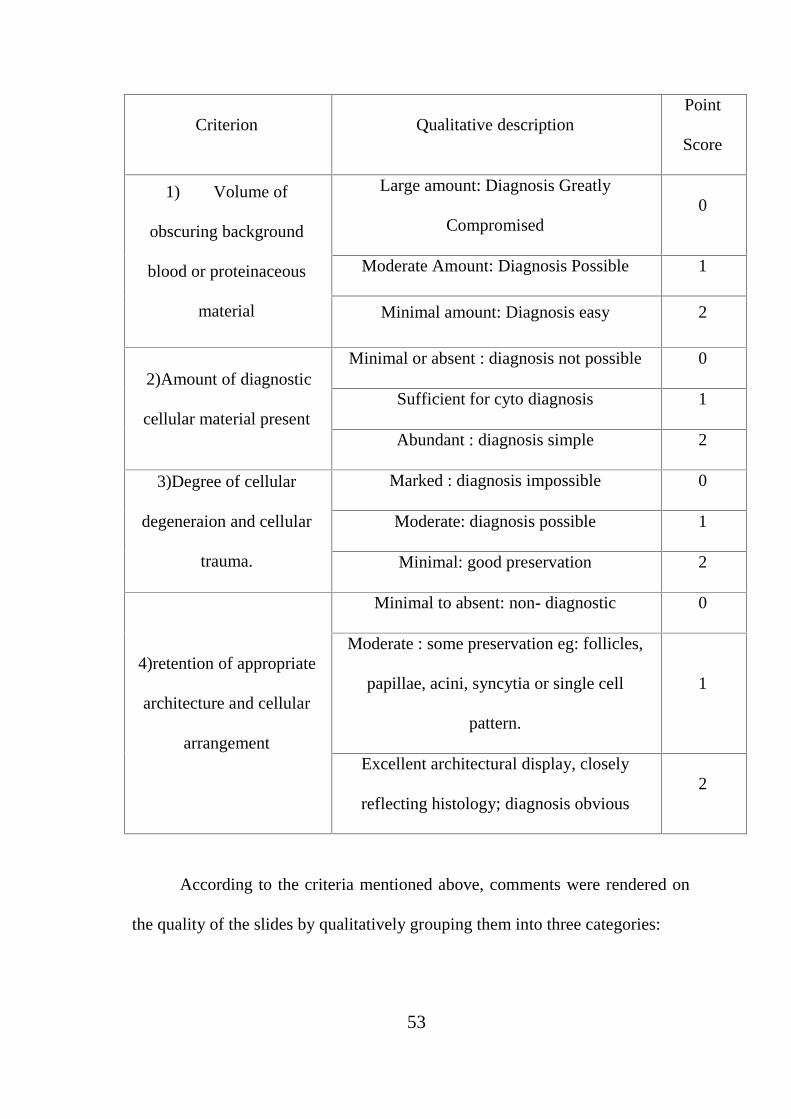
Criterion Qualitative descriptionPoint
Score
1) Volume of
obscuring background
blood or proteinaceous
material
Large amount: Diagnosis Greatly
Compromised0
Moderate Amount: Diagnosis Possible 1
Minimal amount: Diagnosis easy 2
2)Amount of diagnostic
cellular material present
Minimal or absent : diagnosis not possible 0
Sufficient for cyto diagnosis 1
Abundant : diagnosis simple 2
3)Degree of cellular
degeneraion and cellular
trauma.
Marked : diagnosis impossible 0
Moderate: diagnosis possible 1
Minimal: good preservation 2
4)retention of appropriate
architecture and cellular
arrangement
Minimal to absent: non- diagnostic 0
Moderate : some preservation eg: follicles,
papillae, acini, syncytia or single cell
pattern.
1
Excellent architectural display, closely
reflecting histology; diagnosis obvious2
According to the criteria mentioned above, comments were rendered on
the quality of the slides by qualitatively grouping them into three categories:
54
1) Diagnostically unsuitable (score 0-2)
2) Diagnostically adequate (score 3-6)
3) Diagnostically superior (score 7-8)
The conventional smears and cell block were reported under the diagnostic
category as benign, suspicious, malignant and non- diagnostic. Combined
evaluation of conventional smear and cell block was done and tabulation of
cytomorphological characters was analysed.
In this study Ki67 proliferation marker was applied and malignant cases
were graded into low grade or high grade by applying MIB index scoring
system.
MIB index
Number of positive cells
MIB index = X 100
Total number of cells counted
Scoring:
<10% score 0
1-20% score 1
21-50% score 2
>50% score 3

55
INCLUSION CRITERIA
100 ascitic fluid samples in suspicious or confirmed cases of
malignancies received in clinical pathology.
EXCLUSION CRITERIA
All other fluid specimen of body cavity except ascitic fluid.
The sample processed after 48 hours of collection.

56
RESULTS & OBSERVATION
In this prospective study of 100 cases of Ascitic Fluid, 48 cases were
male and 52 cases were female.
FIG 1:SAMPLE DISTRIBUTION OF THE STUDY
52
48
100FEMALE
MALE
TOTAL

57
TABLE 1: AGE DISTRIBUTION OF SAMPLES
AGE ASCITIC FLUID TOTAL
MALE FEMALE
<20 1 1 2
21-30 3 4 7
31-40 6 9 15
41-50 15 13 28
51-60 13 15 28
61-70 9 10 19
>70 1 - 1
Total 48 52 100
Of these 100 Sample maximum number of samples were in the age group
of 51-60 year (28%). Males were predominantly from the age group of 51-60
years (13%). Female were predominantly from the age group of 51-60 years
(15%). (TABLE 1)

58
FIG :2 AGE DISTRIBUTION IN THE SAMPLE ASCITIC FLUID

59
TABLE 2: COMPARISON OF QUALITY OF SMEAR AND CELL
BLOCK IN ASCITIC EFFUSION
QUALITY CONVENTIONAL
SMEAR
CELL
BLOCK
INFERENCE
Unsuitable 15 6 Pearson chi
square
0.001
Adequate 80 66
Adequate &
Superior
5 28
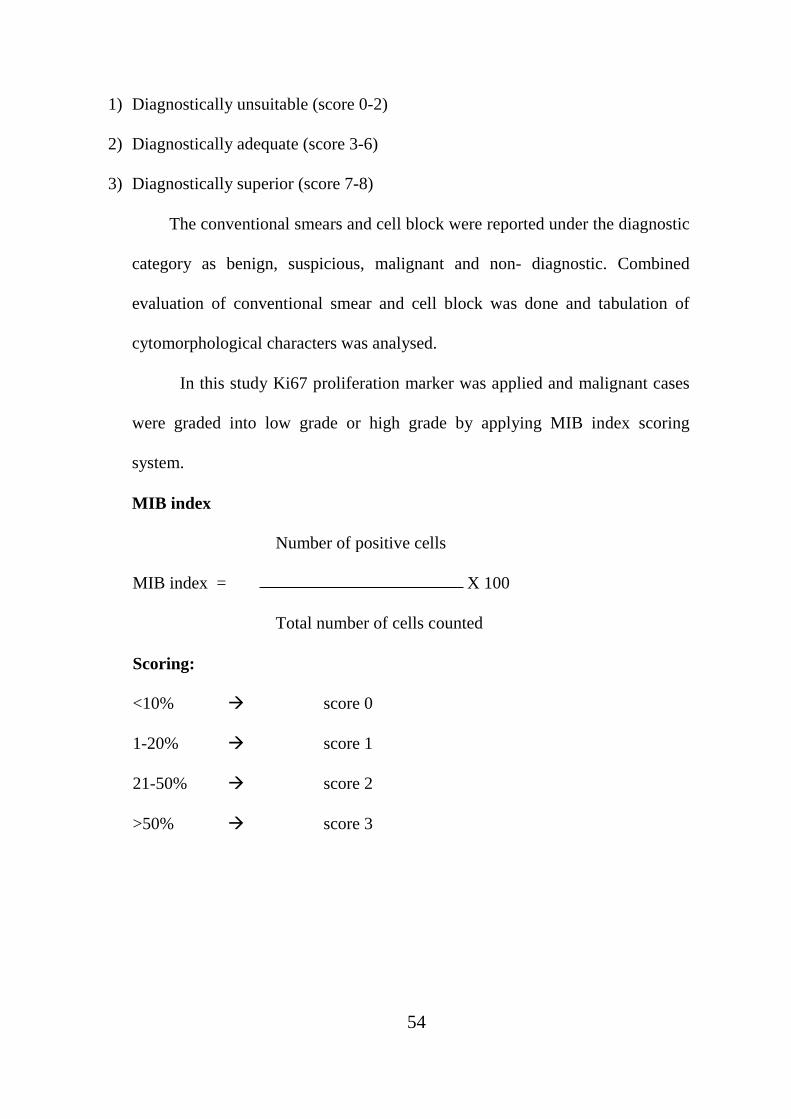
The Quality of smear analysed conventionally was unsuitable in 15
Cases (15%), adequate in 80 cases (80%),adequate and superior in 5cases (5%).
In cell block, 6 cases (6%) were unsuitable, 66 cases (66%) were
adequate and 28 (28%) cases were adequate & superior in cellularity and
cytomorphological preservation (FROM TABLE 2 & FIG3)
60
FIG 3 COMPARISON OF QUALITY OF CS AND CB IN ASCITIC
EFFUSION
0 20 40 60 80 100
CONVENTIONAL SMEAR
CELL BLOCK
Unsuitable Adequate Adequate &Superior

61
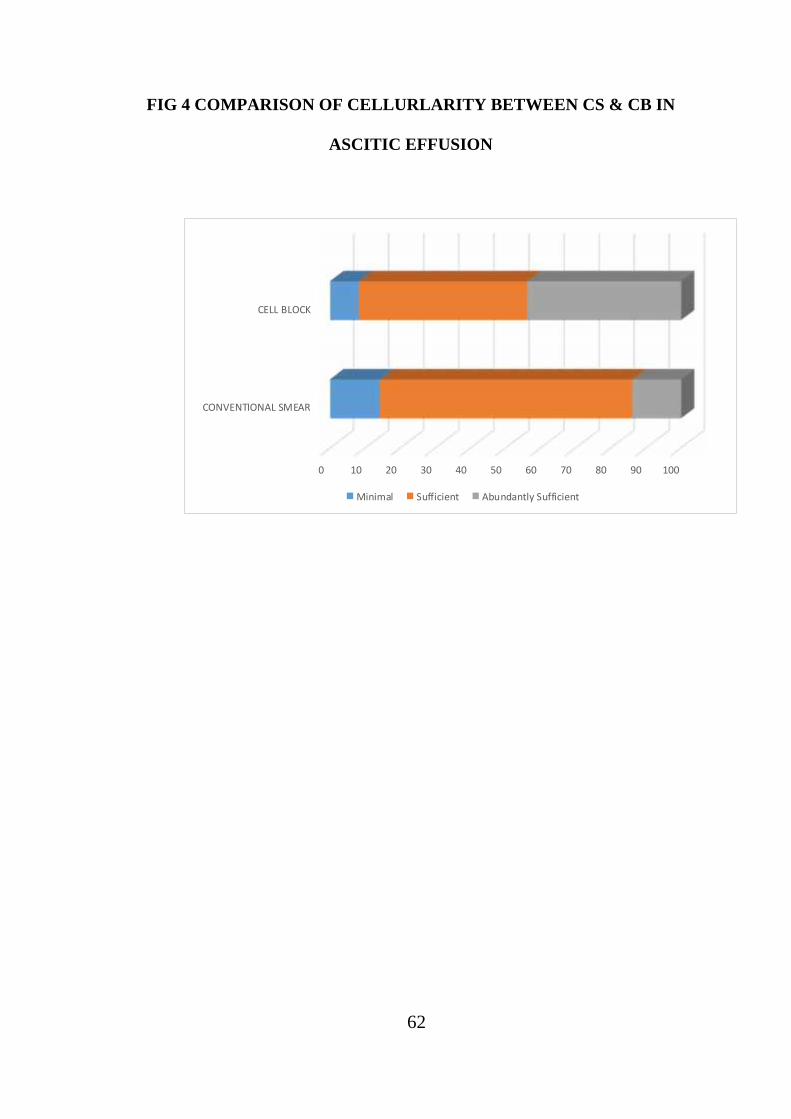
TABLE 3: COMPARISON OF CELLULARITY IN ASCITIC
EFFUSION:
CELLULARITY CONVENTIONAL
SMEAR
CELL
BLOCK
INFERENCE
Minimal 14 8 Pearson chi
square
0.006
Sufficient 72 48
Abundant 14 44
The Cellularity in conventional smear showed minimal cellularity in 14
Cases (14%), Sufficient Cellularity in 72 cases (72%) and abundant cellularity
in 14 Cases (14)
The cellularity in cell block were minimal in 8 Cases (8%) , Sufficient in
48 cases (48%) and abundant in 44 Cases (44%) ( FROM TABLE 3 & FIG 4).
62
FIG 4 COMPARISON OF CELLURLARITY BETWEEN CS & CB IN
ASCITIC EFFUSION
0 10 20 30 40 50 60 70 80 90 100
CONVENTIONAL SMEAR
CELL BLOCK
Minimal Sufficient Abundantly Sufficient

63
TABLE 4: COMPARISON OF ARCHITECTURE IN ASCITICEFFUSION:
ARCHITECTURE CONVENTIONAL
SMEAR
CELL
BLOCK
INFERENCE
Minimal 18 14 Pearson Chi-
square
<0.001
Moderate 82 78
Excellent 0 8
Whereas, the architecture analysis in cell block showed scattered/scant
cells in 14 cases (14%), cellular arrangement (acini, papillae, cell balls, clusters)
in 78 cases (78%) and excellent resemblance to histology in 8 cases (8%) from
TABLE 4 & FIG 5.
FIG:5 COMPARISON OF ARCHITECTURE BETWEEN CS & CB IN
ASCITIC EFFUSION:

64
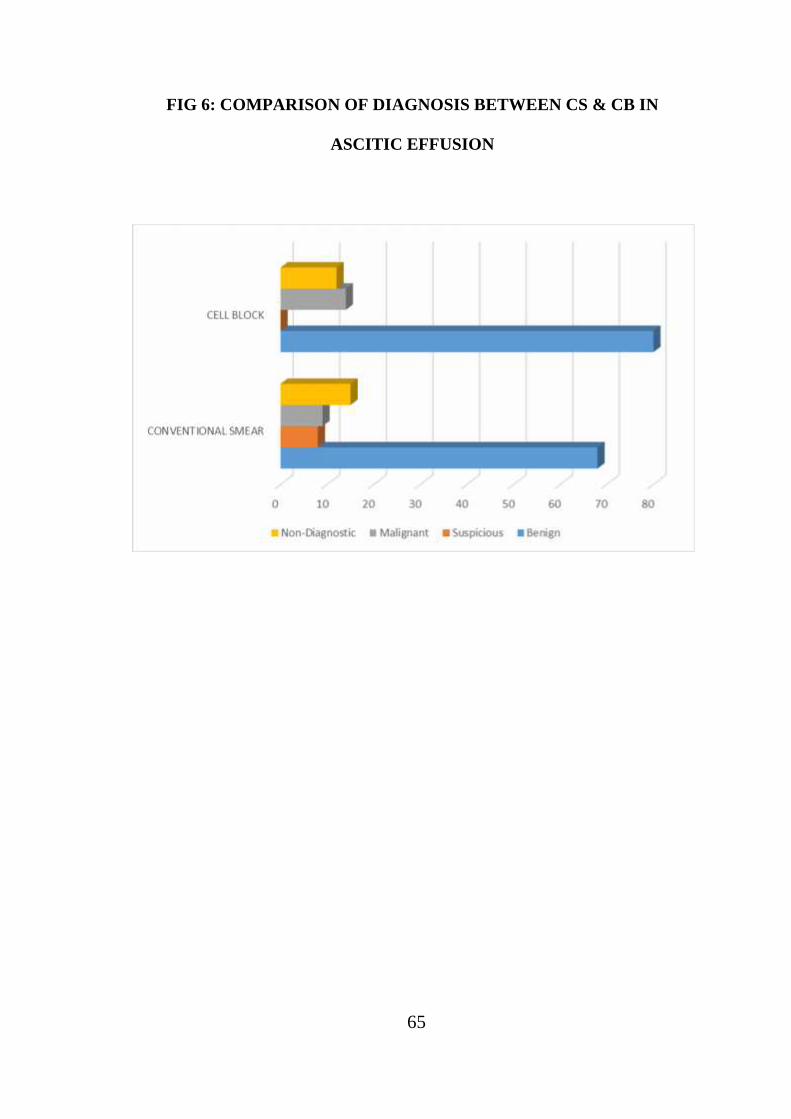
TABLE 5: COMPARISON OF DIAGNOSIS IN ASCITIC EFFUSION
DIAGNOSIS CONVENTIONAL
SMEAR
CELL
BLOCK
INFERENCE
Benign 68 80 Pearson Chi-
square
<0.001
Suspicious 8 0
Malignant 9 14
Non- diagnostic 15 6
By conventional smear the definite diagnosis of benign nature of ascitic
effusion was made in 68 cases (68%), malignant nature was made in 9 cases
(9%). Suspicious of malignancy in effusion was made out in 8 cases (8%) and
smear was non-diagnostic in 15 cases (15%).
In cell block, the benign nature was well defined in 80 cases (80%),
malignant in 14 cases (6%), non-diagnostic in 6 cases (6%) and none was still
suspicious (FROM TABLE 5& FIG 6)
65
FIG 6: COMPARISON OF DIAGNOSIS BETWEEN CS & CB IN
ASCITIC EFFUSION

66
TABLE: 6: PRIMARY SITES OF MALIGNANT ASCETIC EFFUSION
S. NO PRIMARY SITE NO: OF CASES PERCENTAGE
1 Breast 1 7.14%
2 Ovary 12 85.71%
3 Stomach 1 7.14%
Of the 14 cases of malignant effusion (Ascitic) the primary site was ovary
in 12 cases. And 1 case of primary from stomach and one case from breast
metastatic deposits confirmed by applying IHC – ER & PR for the breast cases
which showed positivity
Breast malignancy shows 7.14%, Ovary malignancy shows 78.57%, and
stomach malignancy shows 7.14% .(TABLE 6)
67
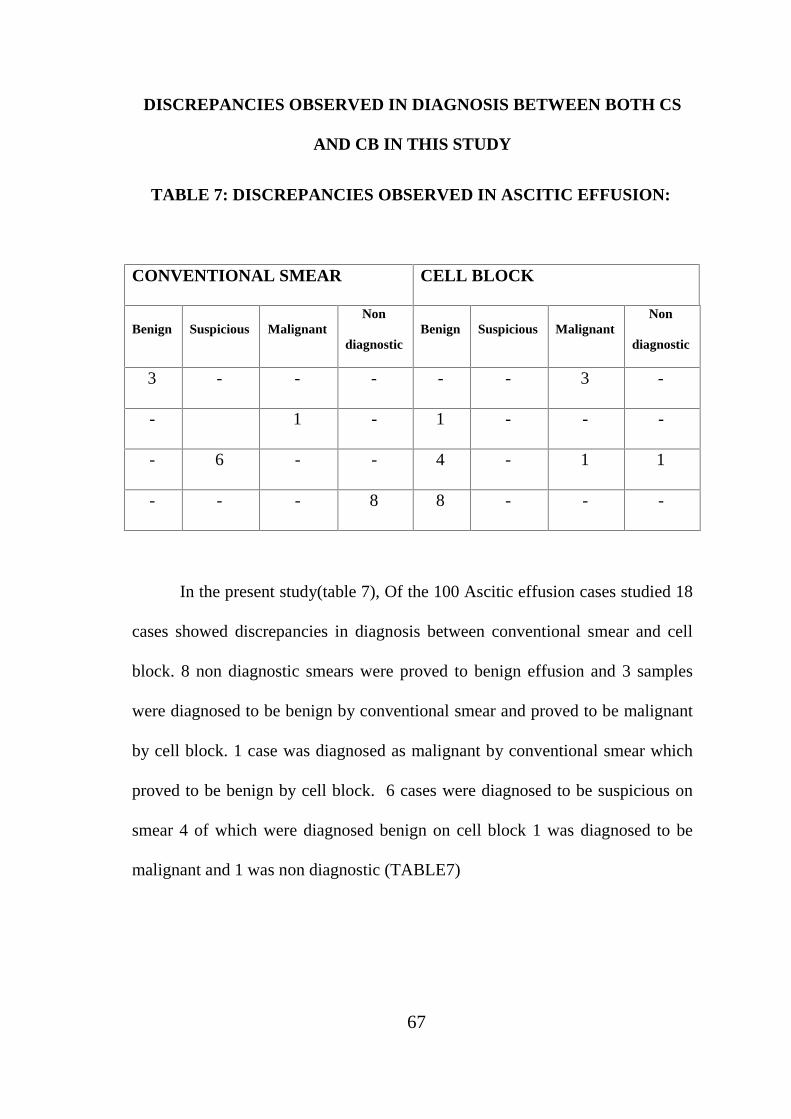
DISCREPANCIES OBSERVED IN DIAGNOSIS BETWEEN BOTH CS
AND CB IN THIS STUDY
TABLE 7: DISCREPANCIES OBSERVED IN ASCITIC EFFUSION:
CONVENTIONAL SMEAR CELL BLOCK
Benign Suspicious MalignantNon
diagnosticBenign Suspicious Malignant
Non
diagnostic
3 - - - - - 3 -
- 1 - 1 - - -
- 6 - - 4 - 1 1
- - - 8 8 - - -
In the present study(table 7), Of the 100 Ascitic effusion cases studied 18
cases showed discrepancies in diagnosis between conventional smear and cell
block. 8 non diagnostic smears were proved to benign effusion and 3 samples
were diagnosed to be benign by conventional smear and proved to be malignant
by cell block. 1 case was diagnosed as malignant by conventional smear which
proved to be benign by cell block. 6 cases were diagnosed to be suspicious on
smear 4 of which were diagnosed benign on cell block 1 was diagnosed to be
malignant and 1 was non diagnostic (TABLE7)

68
IMMUNO TYPING OF MALIGNANCY CASES IN ASCITIC FLUID.
Out of 100 cases of cell blocks of Ascitic fluid specimens, 14 cases were
diagnosed to be malignant effusion. Immunohistochemistry was done in these
14 cases.
In this study Ki67 proliferating marker was applied and cases were
graded into low grade and high grade by MIB index scoring system.
In this study we found 6 cases were high grade and 7 cases were low
grade and one case was negative. (TABLE:8)
IHC:
TABLE 8: Ki67 MARKER
S.NO SCORE GRADE
HIGH LOW NEGATIVE
1 0 Negative
2 2 High
3 2 High
4 1 Low
5 1 Low
6 2 High
7 2 High
8 1 Low
9 2 High
10 1 Low
11 1 Low
12 1 Low
13 1 Low
14 2 High
69
DISCUSSION
The cytodiagnosis by conventional smears have got some draw backs like
less cellularity due to cell loss & overcrowding of cells. To overcome these
drawbacks cell block technique was first employed. The cell block technique
works as an adjunct tool to conventional smear for establishing a definitive
cytopathological diagnosis. Many authors have reported good morphological
details in cell blocks that cannot be observed in cytology smears.
In this study, routine conventional smears and cell block from ascitic fluid
were studied for cellularity, cytological preservation of architecture and its
diagnostic utility and grading of malignancy.
The objective of this study is to evaluate the utility of routine use of cell
block to assess the concordance in diagnosis between conventional smear and
cell block, to perform IHC studies in cell block and grading of malignancy by
applying IHC markers.
In this study plasma thromboplastin method of cell block preparations is
used on ascitic fluid samples. This is similar to study done by Castro-villebon”
D et al and Kulkarni et al which also used this plasma thromboplastin method
for cell block preparation.
ASCITIC FLUID:
Of the 100 samples of ascitic effusion the maximum number of the sample
are in the age group of 41-50 yrs and accounting for 28% of age distribution.
Good cellularity is seen in 14% in cases of smear, while by cell block it was
44%.

70
The quality of smear & cell block was assessed by Mair et al point scoring
system. One study by Bista et al has 56.8% of the cases with abundant
cellularity by cell block which is slightly higher than the present study.
In this study cytology smear shows 80% of adequate smear of which 5%
were diagnostically superior. Whereas by cell block method the adequacy of
66% was observed and 28% were diagnostically superior. By cell block 8% of
our cases showed papillary, glandular and signet ring cells.
One study done by Bhanvadia et al also states that the benefit of cell block
technique is the recognition of histologic patterns in cell block method.
The ‘p’ value of cellularity, background and architectural difference
between CS&CB is <0.001. the ‘p’ value of morphology is 0.001. therefore
statistically there is highly significant difference in overall quality between
CS&CB.
TABLE 9: COMPARISON OF OVERALL CELLULARITY BY CELL
BLOCK IN THE PRESENT STUDY WITH OTHER STUDIES
CELLUARITY
IN CELL
BLOCK
ABUNDANT % SUFFICIENT % MINIMAL %
Castro-Villabon D
et al
29.6% 33% 37.4%
PRESENT
STUDY
44% 48% 8%

71
In the present study of 100 cases cell block showed abundant cellularity
in 44% of the cases which is higher than that of smear which shows abundant
cellularity in only 14% of the cases. In the study by Castro villebon D et al
abundant cellularity in cell block was seen in 29.6% of cases. In the present
study cases with minimal cellularity were 8%.Castrovillebon D et al had 37.4%
which is higher than that of the present study. (Table 9)
The quality of smear & cell block was assessed by using the point
scoring system by Mair et al. In this study the conventional smear showed 80%
of adequate smear of which 5% were diagnostically superior. Whereas by cell
block method the adequacy of 66% was observed of which 28% were
diagnostically superior. The ‘p’ value of cellularity, background & architectural
difference between CS&CB IS 0.000. The ‘p’ value of morphology is 0.001.
Therefore, statistically there is highly significant difference in overall quality
between CS&CB.
In the present study of 100 cases 80% were benign and 14% were malignant,
77% of the cases had similar diagnosis both in conventional smear and cell
block and discrepencies were seen in 18% of the cases.
72
TABLE 10: COMPARISON OF QUALITY OF CELL BLOCK WITH
OTHER STUDIES
QUALITY IN
CELL BLOCK
ADEQUATE
&
SUPERIOR%
ADEQUATE% UNSUITABLE%
THAPAR ET
AL (2009)
67 21 12
NATHANI ET
AL (2014)
25 55 20
PRESENT
STUDY
28 66 6
In a study by Richanathanni et al ,25% cases were adequate and
diagnostically superior and study by Thapar et al had higher number of
adequate diagnostically superior cases accounting for 67%.The percentage of
diagnostically unsuitable cases by cell block is 6% which is very less when
compared to the study by Richa Nathani et al which had 20% and Thapar et al
which had 12% of diagnostically unsuitable cases. (Table 10)

73
TABLE 11: COMPARISON OF DIAGNOSIS BY CELL BLOCK WITH
OTHER STUDIES
DIAGNOSISBY CELLBLOCK
BENIGN%
SUSPICIOUS%
MALIGNANT%
NONDIAGNOSTIC%
Bhanvadia et
al
78 0 22 0
RichaNathani
et al
85 0 15 0
PRESENT
STUDY
80 0 14 6
In the present study of 100 cases, 80% were benign and 14% were
malignant, 77% of the cases had similar diagnosis both in conventional smear
and cell block and discrepancies were seen in 18% of the cases. (Table 11)
The cell block yields higher diagnosis of malignancies which were missed
by conventional smears. The ‘p’ value is <0.001 which shows a very significant
difference between the two methods.

74
TABLE 12: COMPARISON OF INCREASE IN YIELD OF
MALIGNANCY WITH OTHER STUDIES
Flint et al
(1993)95
Calabretto et at
(1996)96
Present study
Increase in
Malignancy yield
9% 6.5% 5%
In this study among malignant ascitic effusion diagnosed by cell
block, the ovarian carcinoma were commonest accounting for 12 cases(78.5%)
followed by carcinoma stomach of 1case (7.14.%) and from breast carcinoma of
1 case (7.14%)
Malignancy was diagnosed in 9% of the cases by CS and in 14% cases
by cell block. Thus cell block has increased the diagnostic yield of malignancy
by 5%. In study by flint et al al increase in malignancy yield was 9% & in study
by calabretto et al was 6.5 %. The ‘p’ value is <0.001 which shows a very
significant difference between the two methods. (Table 12)

75
TABLE 13: COMPARISON OF DIAGNOSTIC CONCORDANCE
STUDY DIAGNOSTIC CONCORDANCE
(%)
Castro-Villabon D et al, 2014 81.6
Kulkarni et al, 2009 94
Present Study 86
Comparison of diagnostic concordance:
The diagnosis of malignancy by CS was 9% which increased into 14%
with the cell block method .The additional yield of malignancy by this study is
5%. Thus cell block yields higher malignancies which were missed by
conventional smear. The ‘p’ value by Pearson Chi square test is 0.000.
Therefore there is highly significant difference in diagnosis between CS& CB.
In this study diagnostic concordance was 86% where in study by castro –
Villabon D et al, it was 81.6% and in Kulkarni et al, it was 94% (Table 13)
There were 18 cases with discordant diagnosis both CS & CB benign
by CS were of the 18% of the cases with discrepancies includes 3 cases
considered as benign by CS were confirmed to be malignant by cell block. 6
cases suspicious of malignancy were diagnosed to be benign by cell block. And
1 case reported as malignant by smear was negative by CB. 6 cases of
suspicious of malignancy on CS 4 of which were diagnosed benign on cell

76
block 1 was diagnosed to be malignant and 1 was non diagnostic were
diagnosed as malignant by cell block is one.
Immunohistochemistry studies were done in 14 cases of malignancy, in
all these 14 cases ki67 proliferation marker was applied and MIB index scoring
was done and showed high grade of 7 cases, moderate grade 6 cases and low to
negative grade 1 cases.
In Hasteh et al study of ki67 proliferative index shows High grade 9% ,
Moderate 34% negative to low 56%. This study shows high grade 42.85%
Moderate 15% and Negative 7.14%. (Table 14)
TABLE 14: COMPARISON OF GRADING OF MALIGNANCY BY MIB
SCORING WITH PRESENT STUDY AND WITH OTHER STUDY
StudyHIGH MODERATE
NEGATIVE
TO LOW
% % %
Hasteh et al study 9 34 56
Our Study 42.85 50 7.14
This study shows increased percentage of high grade Ki 67 Expression
(42.8%).This is significant when compared to Hasth et al study which shows
only 7.3% of high grade Ki 67 expression (Table 14) . Hasteh et al concluded
that the cause of high labeling index in their benign cases might be due to the
presence of lymphocytes in the effusions which were frequently positive and

77
could cause difficulty in estimation of labeling index by immunostaining. In the
present study some benign cases show presence of inflammatory cells,
including lymphocytes in the background.Ki67 interpretation was estimated
only among the epithelial cells excluding the inflammatory cells.

78
SUMMARY
In this prospective study 100 samples of ascitic fluid were studied.
These cases were evaluated simultaneously by conventional smear and cell
block technique. Cell blocks were prepared by plasma thromboplastin method .
Immunohistochemistry for ki67 marker was done on cell blocks in all cases of
malignancy..Ki67 proliferation marker was applied and evaluated by MIB
index scoring system. By this marker the malignant cells were graded into low,
moderate , and high grade.
The smear and cell blocks were evaluated on the basis of cellularity,
architecture morphology and diagnosis .It was observed that the excellent
architecture equivalent to histology was seen in 8% of the cases by cell block.
With cell block the diagnostic yield of malignancy was increased by 5%.

79
CONCLUSION
The cell block technique by plasma thromboplastin method is a simple and
cost effective technique. It doesn’t require any special training and there is no
need of any special instrument. This technique can be used in routine practice
for cytological diagnosis. The main advantage of cell block is better cellularity
& morphology & grading. Multiple sections can be obtained for
immunohistochemistry . Grading of malignancy was done by the application of
proliferation marker ki67.The accuracy of the diagnosis and yield of malignancy
was increased in cell block & by IHC on these cell blocks. So cell block should
be routinely done as an adjuvant in all ascitic fluid samples to increase the
sensitivity of diagnosis of malignancy.

Fig: 7 Cell block showing “Signet rings cells’’ in a case of
carcinoma stomach (H&E, 40X)
Fig: 8 Cell block shows Glandular pattern in case of
Adenocarcinoma of Breast (H&E, 40X)

Fig:9 Cell block shows “Signet ring cells” in a case of
carcinoma ovary (H&E, 10X)
Fig:10 Ki67 marker shows positivity (IHC, 10X)
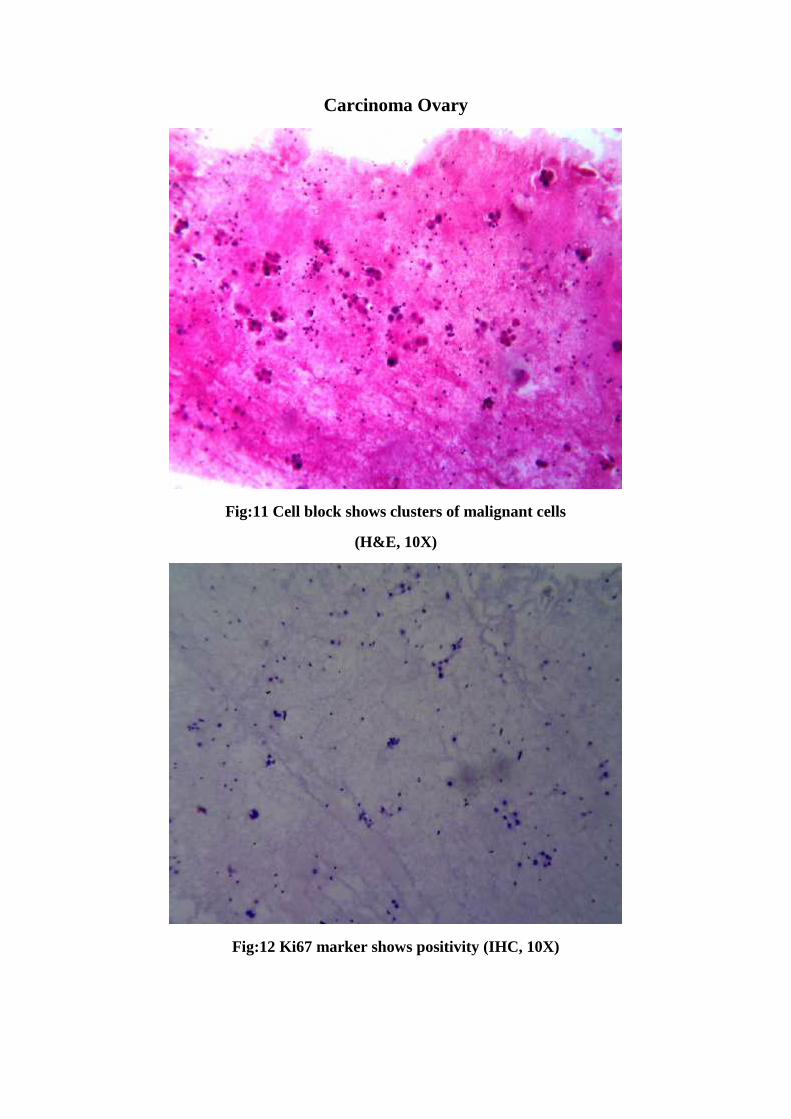
Carcinoma Ovary
Fig:11 Cell block shows clusters of malignant cells
(H&E, 10X)
Fig:12 Ki67 marker shows positivity (IHC, 10X)
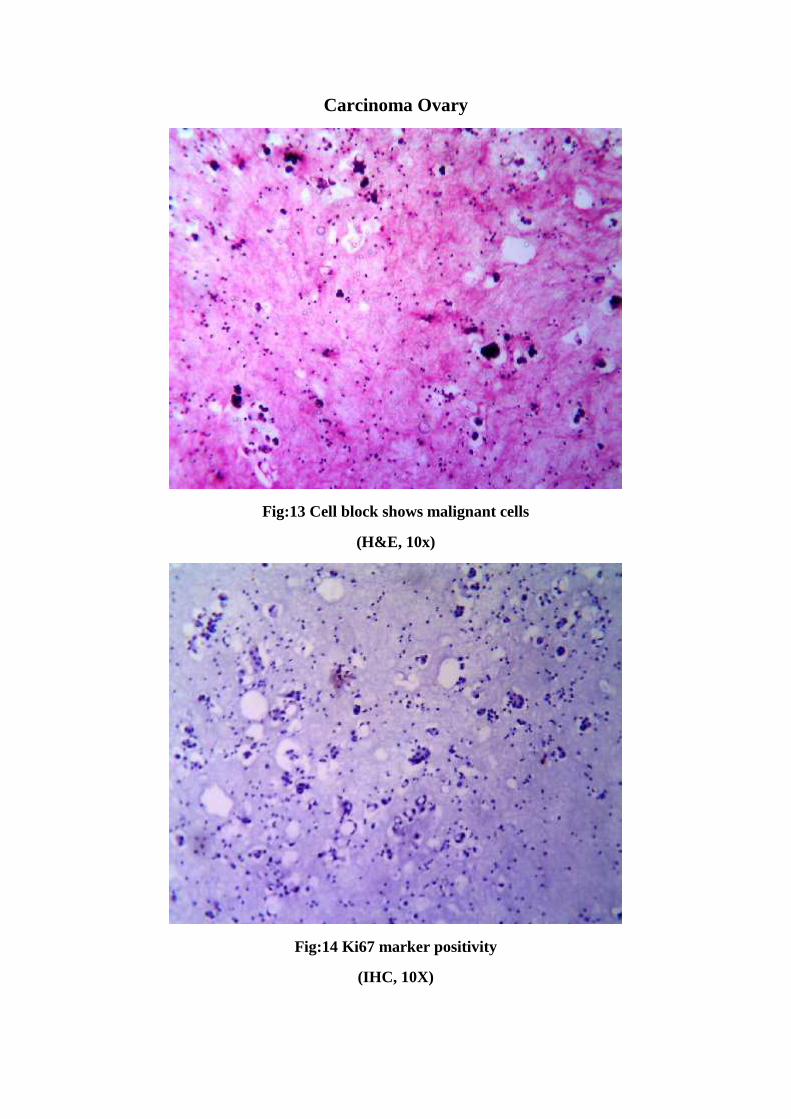
Carcinoma Ovary
Fig:13 Cell block shows malignant cells
(H&E, 10x)
Fig:14 Ki67 marker positivity
(IHC, 10X)
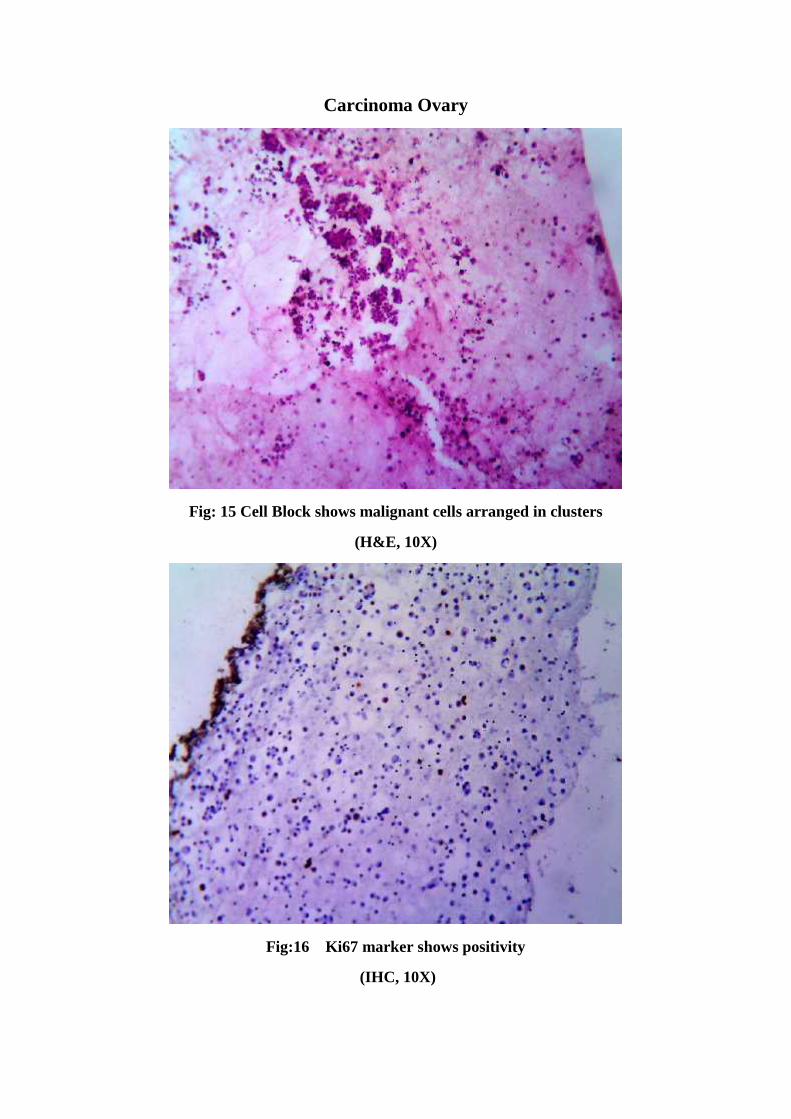
Carcinoma Ovary
Fig: 15 Cell Block shows malignant cells arranged in clusters
(H&E, 10X)
Fig:16 Ki67 marker shows positivity
(IHC, 10X)
BILIOGRAPHY
1) Bodele AK, Parate SN, Wadadekar AA, Bobhate SK, Munshi MM.
Diagnosticutility of cell block preparation in reporting of fluid cytology. Journal
of Cytology 2003;20(3 ): 133-135.
2) Dahlgren S, Nordenstrom B: Transthoracic Needle Biopsy.Chicago: Year
Book Medical Publishers, 1966.
3) Sujathan K, Pillai KR, Chandralekha B, Kannan S, Mathew A Nair
MK.Cytodiagnosis of serous effusions: A combined approach to
morphological features in Papanicolaou and May-Grunwald Giemsa
stained smears and modified cell block technique. Journal of Cytology
2000;17(2):89-95.
4) Dekker A, Bupp PA. Cytology of serous effusions. An investigation into
theusefulness of cellblocks versus smears. Am J Clin Pathol 1978;70
(6):855 860.
5) Rosai J. Why microscopy will remam a cornerstone of surgical
pathology.Lablnvest.2007;87:403-408.
6) Kim DH, Kwon MS. Role of fine needle aspiration cytology, cell blocl:
preparation and CD63, P63 and CD56.
7) Shobha SN, Kodandaswamy CR.Utility of modified cell block technique
in cases of pleural effusion suspected of malignancy.Int J Health Sci Res.
2013;3(1):33-38.
8) Velios F, Griffin J. Examination of body fluids for tumor cells. Am J Clin
Pathol.1954;24:676-81.
9) Sears D, Hajdu SI. The cytologic diagnosis of malignant neoplasm's in pleural
and peritoneal effusions. Acta Cytol.1987 ;31 (2):85-97.
10) Kanhouwa S B, Mary M. Reliability of Cytologic Typing of Lung Cancer.
Acta cytol.1975;20(3):229-32
11) Bousfield LR, Greenberg ML. cytogenetic diagnosis of cancer from body
fluids. Acta cytol 1985; 29(5): 768-773.
12) Karnanchow PN, Bouin RE. "Cell-block" technique for fine needle
aspiration biopsy. J Clin Pathol 1982;35:688.
13) Grahamg, . S.: The cancer cells of serous effusions. Am. J. Path. 9: 701-
710. Pl. 115-116, 1933.
14) Fetsch PA, Simsir A, Brosky K, Abati A: Comparison ofthree
commonly used cytologic preparations in effusion immunochemistry. Diagn
Cytopathol 2002, 26:61-66.
15) George M. Varsegi and Vinod Shidham .Cell Block Preparation from
Cytology Specimen with Predominance of Individually Scattered Cells. j vis
exp.2009; (29):1316.
16) Frost JK. The cell in health and disease. In: Weid GL (ed) Monographs
in Clinical Cytology. vol 2. Basel: Karger, 1986.
17) Farber SM, Wood DA, Pharr SL, et al.Significant cytologic findings in
nonmalignant pulmonary disease, Dis Chest 1957 ;3 l : l -13.
18) Y.S. Erozan, I. Ramzy, Pulmonary Cytopathology,Essentials m
Cytopathology 6, Springer Science+Business Media, LLC 2009.p.9-73.
19) Krogerus LA, Anderson LC. A simple method for the preparation of
paraffin-embedded cell blocks from fine needle aspirates, effusions, and
brushings. Acta Cytol 32:585-587, 1988.
20) Yang GC, Wan LW, Papellas J, Waisman J. Compact cell blocks.
Use for body fluids, fine needle aspirations and endometrial brush biopsies.
Acta Cytol 42:703- 706, 1998.
21) Kok LP, Visser PE, Boon ME. Histoprocessing with the microwave
oven: an update. Histochem J 20:323-328, 1988.
22) Baloch ZW, Lee A, Cobbs C, et al. Millipore filter cell block
preparation: an alternative to cell block in nongynecologic specimens of
limited cellularity. Diagn Cytopathol 20:389-392, 1999.
23) Shidham VB, Epple J. Chapter 14, Appendix I: Collection and
processing of effusion fluids for cytopathologic evaluation. In: Shidham
VB, Atkinson BF. 2007.
24) Varsegi G, D'Amore K, Shidham V. pl6INK.4a
Immunocytochemistry as an Adjunct to Cervical Cytology - Potential
Reflex Testing on Specially Prepared Cellblocks from Residual Liquid
Based Cytology (LBC) Specimens· Modem Pathology 22: 98th Annual
Meeting of United States and Canadian Academy of Pathology; 2009 Mar
7-13; Boston, Ma. 2009.

25) Nigro K, Tynski Z, Wasman J, Abdul-Karim F, Wang N.
Comparison of cell block preparation methods for nongynecologic
ThinPrep specimens. Diagn Cytopathol. 2007;35:640-643.
26) Saleh HA, Hammoud J, Zakaria R, Khan AZ. Comparison of Thin-
Prep and cell block preparation for the evaluation of Thyroid epithelial
lesions on fine needle aspiration biopsy. CytoJournal. 2008;5:3-3.
27) Kyroudi A, Paefthimiou M, Symiakaki H, Mentzelopoulou P,
Voulgaris Z, Karakitsos P. Increasing diagnostic accuracy with a cell block
preparation from thin-layer endometrial cytology: a feasibility study. Acta
Cytol. 2006;50:63-69
28) Atkinson BF. Chapter 5: Immunocytochemistry of effusion fluids:
introduction to SCIP approach (Chapter 5. In: Shidham VB, Atkinson BF,
editors. Cytopathologic Diagnosis of Serous Fluids. Elsevier;
29) Mair, Dunbar F, Becker PJ, Du Plessis W. Fine Needle cytology: Is
aspiration suction necessary? A study of 100 masses in various sites. Acta
Cytol 1989; 33:809-13.
30) Nathan HA, Narayan E,-Smith MM, Horn MJ. Cell Block Cytology.
Improved Preparation and its Efficacy in Diagnostic Cytology. Am J Clin
Pathol.2000; 114:599-606.
31) Kulkarni, SB Desai, RF Chinoy.Utility of thromboplastin-plasma
cell block technique for fine needle aspiration and serous effusions. Diag
Cytopathol. 2009;37(2):86-90.

32) Koss LG. Diagnostic Cytology and Its Histopathologicliases, 3rd edn.
Philadelphia:JB Lipincott, 1979.
33) Churg A, Cagle PT, Roggli VL (eds): Tumors of the Serosal
Membranes. Silver Spring, Md, ARP Press, 2006.
34) Koss LG, Melamed MR. Effusions in presence and absence of
cancer. In: Koss' Diagnostic cytology and its histopathologic bases.15th ed.
New York: Lippincott Williams and Wilkins; 2006. p. 919-49.
35) Staff of The Vincent memorial laboratoryof theVincent memorial
hospital The Cytologic Diagnosis of Cancer. Philadelphia. W. B. Saunders
Co. 1950.
36) Richardson HL, Koss LG, Simon TR. Evaluation of concomitant use
of cytological and histological technique in recognition of cancer in
exfoliated material from various sources. Cancer, 1955;8:948-50.
37) Hammar SP. Common neoplasms. In: Dail DH, Hammar SP, eds.
Pulmonary Pathology. 2nd ed. New York: Springer-Verlag; 1994:1487-
1579.
38) Chu P, Arber d. paraffin section detection of CDlO in 505
nonhemopoetic neoplasms. Amj clin pathology 2000; 113: 3740-82.
39) Chu PG, Weiss LM. Expression of cytokeratin 5/6 in epithelial
neoplasms: an immunohistochemical study of 509 cases 2002.
40) Clover j, oates j. anti cytokeratin 5/6: a positive marker for epitheliod
mesotheliomas. Histopathology 1997; 31: 140-3.
41) Ordonez NG. the immunohistochemical diagnosis of
mesotheliomas: a comparative study of epithelioid mesotheliomas and lung
adenocarcinoma. Amj surg pathol 2003; 27: 1031.
42) Comin CE, Novelli L. calretinin, Thrombomodulin, CEA and CD15:
a useful combination of immunohistochemical markers for differentiating
pleural epithelial mesotheliomas and periphery pulmonary
adenocarcinoma. Hum pathology 2001; 32: 529.
43) Ghaffari M, Zeng X et al. Nuclear localization domain of thyroid
transcription factor-I in respiratory epithelial cells. Biochem j 1997; 328: 757.
44) Bejarano PA, Baughman RP et al. surfactant proteins and thyroid
transcription factor-I in pulmonary and breast carcinomas. Mod pathol 1996; 9:
445.
45) Bishop JA, Sharma R, Illei PB: Napsin A and thyroid transcription factor-
I expression in carcinomas of the lung, breast, pancreas, colon, kidney, thyroid,
andmalignantmesothelioma. Hum Pathol 2010; 41:20-25.
46) Nakamura N, Miyagi E, et al. expression of thyroid transcription factor-I
in normal and neoplastic lung tissues. Mod pathol 2002b; 15:1058.
47) Pelosi G, Fraggetta F, et al. immunoreactivity for thyroid transcription
factor-1 in stage 1 non small cell carcinomas of the lung. Am J Surg Pathol 2001;
25: 363.
48) Khan N, Sherwani K R, Afroz N, Kapoor S. Usefulness of Cell Blocks
versus Smears in Malignant Effusion Cases. Journal of Cytology.2006; 23(3):
129-32.

49) Thapar M, Mishra RK, Sharma A, Goyal V.Critical analysis of cell block
versus smear examinations m Effusions.Journal of Cytology.2010;26(2):60-4.
50) Khan N, Sherwani R K, Afroz N, Kapoor S. Cytodiagnosis of Malignant
Effusion and Determination of Primary Site. Journal of Cytology.2005;22:107-
10.
51) Murphy WM, Alan BP. Determination of primary site by examination of
cancer cells in body fluids. Am J Clin Pathol 1972; 18: 479-488.
52) Diana Castro-Villabon, Yubelly Avello, Nathalie Ruiz, Paula A.
Rodriguez-Urrego. Implementation of routine thromboplastin-plasma cell block
technique in the evaluation of non-gynecologic specimens: A methodologic
comparison with conventional cytology. J Microsc Ultrastruct (2014)
53) Richa Nathani, Rakesh Singh Hazari, Yogesh G. Patle, Santosh Gupta
Comparative analyses of cavity effusions by cell blocks and smear examination.
International journal of recent trends in science and technology July 2014; 12(1):
69-72
54) Flint, Andrew. Detection of pulmonary neoplasms by bronchial washings
Are cell blocks a diagnostic aid?. Acta Cytologica. 1993; 37(1): 21-23
55) Bhanvadia Viral M., Santwani P.M., Vachhani J.H. Analysis of
diagnostic value of cytological smear method versus cell block method in body
fluid cytology: study of 150 cases. Ethiop J Health Sci. 2014; 24(2).
56) A. Churg, T.V. Colby, P. Cagle, J. Corson, A.R. Gibbs, B. Gilk, et al. The
separation of benign and malignant mesothelial proliferation Am J Surg Pathol,
24 (9) (2000), pp. 1183-1200 View Record in Scopus I Citing articles (186}

57) E. Cakir, F. Demirag, M. Aydin, E. Unsal Diagnosis of malignant
mesothelioma, adenocarcinoma, and reactive mesothelial cells: a logistic
regression analysis Diagn Cytopathol, 37 (2009}, pp. 4-10 Full Text via
CrossRef I View Record in Scopus I Citing articles (25}
58) L.A. Palaora, A.E. Rocher, J. Rofrano, S. Mercedes, V. Penzutil Utility
of Ag NOR, ICC for CEA, and tumor markers for the diagnosis in serous
effusions Revista Brasilleira de Cancerologia, 54 (4) (2008), pp. 317-323
59) K. Mohanty, P. Dey Serous effusions: diagnosis of malignancy beyond
cytomorphology. An analytic review Postgrad Med J, 79 (2003), pp. 569-574
60) M. Lozano, A. Panizo, G.R, Toledo, J.J. Sola lmmunocytochemistry in
the differential diagnosis of serous effusions: a comparative evaluation of eight
monoclonal antibodies in Papanicolaou stained smears Cancer, 93 (1) (2001 ),
pp. 68-72 Full Text via CrossRef I View Record in Scopus I Citing articles (54)
61) R.L. Attanoose, A. Griffin, A.R. Gibbs The use of immunohistochemistry
in distinguishing reactive from neoplastic mesothelium: a noveluse for desmin
and comparative evaluation with EMA, p53, PDGFR, p-glycoprotein, and Bcl-2
Histopathology, 43 (2003), pp. 231-238
62) A.E. Walts, J.W Said, H.P. Koeffler Is immunoreactivity for p53 useful
in distinguishing benign from malignant effusions? Localization of p53 gene
product in benign mesothelial and adenocarcinoma cells Mod Pathol, 7 (4)
(1994), pp. 462-468 View Record in Scopus I Citing articles (17)
63) J.D. Sington, L.S. Morris, A.G. Nicholson, N. Coleman Assessment of
cell cycle state may facilitate the histopathological diagnosis of malignant

mesothelioma · Histopathology, 42 (5) (2003), pp. 498-502 Full Text via
CrossRef I View Record in Scopus I Citing articles (15)
64) C. Cakir, M.G. Gulluoglu, D. Yilmazbayhan Cell proliferation rate and
telomerase activity in the differential diagnosis between benign and malignant
mesothelial proliferations · Pathology, 38 (2006), pp. 10-15 Article I PDF (261
K) I Full Text via CrossRef I View Record in Scopus I Citing articles (16)
65) G. Kafiri, D.M. Thomas, N.A. Shepherd, T. Krausz, D.P. Lane, P.A. Hall
p53 expression is common in malignant mesothelioma Histopathology, 21 (4)
(1992), pp. 331-334 Full Text via CrossRef I View Record in Scopus I Citing
articles (56)
66) H.J. Heidebrecht, F. Buck, E. Endl, M.L. Kruse, K. Adam, K. Andresen
Ki67-Mcm6, a new MoAb specific to Mcm6: comparison of the disbit, ution
profile ofMcm6 and ki67 antigen Lab Invest, 81 (8) (2001), pp. 1163-1165 Full
Text via CrossRef I View Record in Scopus I Citing articles (16)
67) LG. Koss, M.R. Melamed Effusions in the absence and the presence of
cancer Koss' diagnostic cytology & its histopathologic bases (5th ed.), Lippincott
Williams &Wilkins. Philadelphia(2006), pp. 919-1021 View Record in Scopus
I Citing articles (2)
68) R.T. Miller, P. Kubier lmmunohistochemisby on cytologic specimens and
previously stained slides (when no paraffinblock is available) J Histotechnol, 25
(2002), pp. 251-257Full Text via CrossRef I View Record in Scopus I Citing
articles (15)
69) F.G. Mayall, A. Heryet, D. Manga, A. Kriegeskotten p53 immunostalning
is a highly specific and moderately sensitive marker of maligniilncy in serous
fluid cytology Cytopathology, 8 (1) (1997), pp. 9-12 View Record in Scopus I
Citing articles (18)
70) P.A. Hall, A. Ray, N.R. Lemoine, C.A. Midgley, T.L. Krausz p53
immunostaining as a marker of malignant disease in diagnostic cytopathology
[Letter] Lancet, 338 (8765) (1991 ), p. 513 Article I PDF (178 K) I View Record
in Scopus I Citing articles (92)
71) G.N. Akhtar, M. Rahman,, S.A. Khan, N.A. Chaudrhy p53
immunostaining In benign and malignant effusions Pak J Med Sci, 19 (1) (2003),
pp. 33-35 View Record in Scopus I Citing articles (1)
72) F. Hasteh, Y. Lin, N. Weidner, C.W. Michael The use of
immunohistochemisby to distinguish reactive mesothelial cells from malignant
mesothelioma In cytologlc efflu;lons CancerCytopathol, 118 (2)(2010), pp. 90-
96 Full Text via CrossRef I View Record in Scopus I Citing articles (62)
73) P.T. Cagle, R.W. Brown, R.M. Lebovitz p53 immunostaining in
differentiation of reactive process from malignancy Hum Pathol, 25 (1994), pp.
443-448 Article I PDF (5191 K) I View Record in Scopus I Citing articles (61)
74) O.J. Stoetzer, R·. Munker, M. Darsow, W. Wilmanns p53-
immunoreactive cells in benign and malignant effusions: diagnostic value using
a panel of monoclonal antibodies and comparison with CEA-staining Oneal Rep,
6 (20) (1999), pp. 455-458 View Record in Scopus I Citing articles (9)

75) R. Stuart-Harris, C. Caldas. S.E. Pinder Proliferation markers and
survival in early breast cancer: a systematic meta-analysis of 85 studies in 32,
825 patients Breast, 17 (2008), pp. 323-334 Article I PDF (336 K) I View Record
in Scopus I Citing articles (183)
76) A.L. Johannessen, S.H. Trop The clinical value ofki67/MIB-1 index in
human astrocytoma Pathol Oncol Res, 12 (3) (2006), pp. 143-147 Full Text via
CrossRef I View Record in Scopus I Citing articles (80)
77) Z.M. Taheri, M. Mehrafza, F. Mohammad, M. Khoddami, M. Bahadori,
M.R. Masjedi The diagnostic value of ki67 and repp86 in distinguishing between
benign and malignant mesothelial proliferations : Arch Pathol Lab Med, 132 (4)
(2008), pp. 334-339
78) A.SchOnherr, M. Bayer, A. Bocking Dagnostic and prognostic value of
Ki-67 proliferation fraction in serous effusions Cell Oncol, 26 (2004), pp. 57-
62View Record in Scopus I Citing articles (13)
79) H. Saleh, M.T. Paula Bober, M.T. Pamela Tabaczka Value of ki67
immunostain in identification of malignancy in serous effusions Diagn
Cytopathol, 20 (1999), pp. 24-28 Full Text via CrossRef I View Record in
Scopus I Citing articles (13)
80) Q.J. Khan, B.T. Kimler, J. Clark, C. Zalles Kl67 expression in benign
breastductal cells obtained by Random periareolar FNA Cancer Epidemiol
Biomarkers Prev, 14 (2005), pp. 786-790
81) C.U. Kohler, A. Kreuter, T. Rahmel Replication markers for detection of
beta-cell proliferation in human pancreatic tissue Regul Pept, 162 (3) (2010), pp.
115-121 Article IPDF (1129 K) I View Record in Scopus I Citing articles (12)
82) F. Kimura, B.S. Kawamura, J. Watanabe, S. Kuwao Significance of cell
proliferation markers (MCM 7, topo Ila, and ki67) in cavital fluid cytology:
can w.e differentiate reactive mesothelial cells from malignant cells? Diagn
Cytopathol, 38 (3) (2010), pp. 161-167 View Record in Scopus I Citing articles
(7)
83) Z.M. Taheri, M .. Mehrafza, F. Mohammadi, M. Khoddami, M. Bahadori
Proliferative marker in distinction between benign and malignant
mesothelial proliferation Tanaffos, 5 (2) (2006), pp. 9-12 Corresponding
author. Tel.: + 20 0222607376/0104959148. Copyright© 2011 Production and
hosting by Elsevier B.V.

ANNEXURE - I
PROFORMA
S.No:
Patient Name: Age: Sex:
Hospital Ip/Op no:
Address of the Patient:
Contact phone no:
Clinical details:
Investigations:
Invasive:
Non-invasive:
Clinical Diagnosis:
Type of Sample: Ascitic Fluid
Cytology no:
Convectional smear findings: Cellularity / Architectural pattern/
Cytomorphology / Background.
Cell block findings: Cellularity / Architectural pattern / Cytomorphology
/ Background.
Immunohistochemistry (If needed):
Impression:

ANNEXURE-II
CONSENT FORM
I have been informed in detail (verbal and written) form the doctor in out
own language regarding the study. I hereby give consent to use the sample
material for Dr. K.Sumathi’s thesis as part of the MD degree curriculum. I have
no objection to her publishing details of this study in medical journal after its
completion. I understand that I have the liberty to withdraw from this study at any
stage.
Date: Signature:
Cytology No: Name of the patient:
Address:
Muha;r;rp jfty; jhs;
jpUney;Ntyp muR nghJ kUj;Jtkidf;F tUk; NehahspfSf;F
_______________________________________________ gw;wpa Muha;r;rp
eilngw;WtUfpw ________________________________ vt;tsT gutyhf
,Uf;fpwJ vd;gJ gw;wpAk; mjw;fhd fhuzq;fs; gw;wpAk; mwpe;J
nfhs;;tNj ,e;j Muha;r;rpapd; Nehf;fkhFk;.
ePq;fSk; ,e;j Muha;r;rpapy; gq;Nfw;f ehq;fs; tpUk;GfpNwhk;. KbTfis
my;yJ fUj;jf;fis ntspapLk; NghNjh my;yJ Muha;rpapd; NghNjh
jq;fsJ ngaiuNah my;yJ milahsq;fisNah ntspaplkhl;Nlhk;.
Vd;gijAk; njhptpj;J nfhs;fpNwhk;.
,e;j Muha;r;rpapy; gq;Nfw;gJ jq;fSila tpUg;gj;jpd; Nghpy; jhd;
,Ue;f;fpwJ NkYk; ePq;fs; ve;NeuKk; ,e;j Muha;r;rpapypUe;J
gpd;thq;fyhk; vd;gijAk; njhptpj;Jf;nfhs;fpNwhk;.
,e;j rpwg;G ghpNrhjidfspd; KbTfis Muha;r;rpapd; NghNjh my;yJ
Muha;r;rpapd; KbtpNyh jq;fSf;F mwptpg;Nghk; vd;gijAk; njhptpj;Jf;
nfhs;fpNwhk;.
Muha;r;rpahsH ifnahg;gk; gq;Nfw;ghsH ifnahg;gk;
Njjp:
Muha;r;rp xg;Gjy; fbjk;
Muha;r;rp jiyg;G :
ngaH:
taJ :
ghy; :
Njjp :
cs;Nehahsp vz; :
Muha;r;rp NrHf;if vz; :
,e;;j Muha;r;rpapd; tptuq;fSk; mjd; Nehf;fq;fSk; KOikahf
vdf;F njspthf tpsf;fg;gl;lJ vdf;F tpsf;fg;gl;l tp\aq;fis ehd;
Ghpe;J nfhz;L vdJ rk;kjj;ij njhptpf;fpNwd;.
,jw;F Njitahd ghpNrhjidfSf;F ehd; kdkhu rk;kjpf;fpNwd;.
ifnahg;gk;

MASTER CHART KEY WORDS
C – CELLULARITY
B - BACK GROUND
M - MORPHOLOGY
A - ARCHITECTURE
S - SCORE
C - CELLULARITY
0 - Minimal or absent: Diagnosis not possible
1 - Sufficient for cytodiagnosis
2 - Abundant : Diagnosis simple
B - BACK GROUND OBSCURED BY BLOOD AND PROTEINACEOUS
MATERIAL
0 - Large amount: Diagnosis greatly compromised
1 - Moderate amount: Diagnosis possible
2 - Minimal amount: Diagnosis easy
M - MORPHOLOGY cellular degeneration and cellular trauma.
0 - Marked: Diagnosis impossible
1- Moderate: Diagnosis possible
2 - Minimal: good preservation
A - ARCHITECTURE appropriate architecture and cellular arrangement
0 - Minimal to absent: non diagnostic
1 - Moderate: some preservation eg: follicles, papillae, acini, synctia or
single cell pattern
2 - Excellent architectural display, closely reflecting histology:
diagnosis obvious
QUALITY
Diagnostically unsuitable (score 0-2)
Diagnostically adequate (score 3-6)
Diagnostically superior (score 7-8)

QUALITY DIAGNOSIS
C B M A S C B M A S1 F3294 60 F 56040 1 1 2 1 5 adeq benign 1 0 1 2 4 adeq benign ?Ca ovary - - -2 F3876 20 F 65612 1 1 1 1 4 adeq benign 1 1 1 1 4 adeq benign Rt ovary cyst - - -3 F3939 56 M 69667 0 1 2 1 4 adeq benign 0 1 2 1 4 adeq benign DCLD - - -4 F 3906 50 F 67556 1 0 2 1 4 adeq benign 2 1 2 1 6 superior malignant Ca ovary done 0 neg5 F 3926 67 F 62987 0 1 1 0 2 unsuita non diag 1 1 0 0 2 unsuit non diag Pelvic mass - - -6 F 4093 45 F 69607 1 1 1 1 4 adeq suspicious 1 1 2 1 5 superior benign ?Ca ovary - - -7 F 3864 60 F 63867 2 1 2 1 6 adeq benign 2 1 2 1 6 superior benign Liver-mets - - -8 F3855 57 F 68267 1 1 2 1 5 adeq suspicious 1 1 2 2 6 superior malignant Ca ovary done 2 High9 F3964 60 M 64282 2 1 2 1 6 superior malignant 2 1 2 1 6 superior malignant Ca ovary done 2 High
10 F3848 41 F 65498 2 1 2 1 6 superior malignant 2 1 2 1 6 superior malignant Ca ovary done 1 Low11 F3892 28 M 69228 0 1 0 1 2 unsuita non diagn 1 1 0 0 2 unsuit non diag DCLD - - -12 F3729 65 M 17462 1 1 1 1 4 adeq benign 1 1 1 0 3 adeq benign Ca stomach - - -13 F3768 40 F 57142 0 1 1 0 2 unsuita nondiagn 0 1 1 0 2 unsuit nondia DCLD - - -14 F 3961 37 M 70665 1 1 2 1 5 adeq benign 1 1 1 1 4 adeq benign PHT - - -15 F 3927 49 F 66743 0 1 1 0 2 unsuita non diag 1 0 0 1 2 unsuit non dia ?Ca ovary - - -16 F3592 44 M 60709 1 1 1 1 4 adeq benign 1 1 1 1 4 adeq benign PHT - - -17 F3952 60 F 48755 2 1 1 2 6 superior malignant 2 1 1 2 6 superior malignant Ca ovary done 1 Low18 F3533 60 M 51468 1 1 1 1 4 adeq benign 1 1 0 1 3 adeq benign DCLD - - -19 F3642 55 F 64972 1 1 0 0 2 unsuita non diag 1 0 1 1 3 adeq benign Ileocec-TB - - -20 F4254 60 F 65743 1 1 1 1 4 adeq benign 1 1 2 0 4 adeq benign ?Ca ovary - - -21 F24/16 60 M 291 1 0 2 1 4 adeq benign 1 1 1 1 4 adeq benign D CLD/PHT - - -22 F47/16 47 M 722 1 0 1 0 2 unsuia non diag 1 0 1 0 2 unsuit nondia DCLD - - -23 F61 66 M 72659 2 1 1 1 5 adeq benign 1 1 1 1 4 adeq benign DCLD - - -24 F73 70 F 732 1 1 1 1 4 adeq benign 1 1 1 1 4 adeq benign PHT - - -25 F95 60 F 1902 1 2 1 1 5 adeq benign 1 1 1 0 3 adeq benign Chr.liver-dis - - -26 F96 50 M 1877 1 1 0 0 2 unsuita non diag 1 0 1 0 2 unsuit non diag ?TB-abdo - - -27 F102 45 M 1929 1 1 1 1 4 adeq benign 1 1 1 0 3 adeq benign CLD/MRD - - -28 F115 45 M 2415 1 1 2 1 5 superior benign 1 1 1 1 4 adeq benign DCLD - - -29 F127 37 M 2235 0 1 1 0 2 unsuita non diag 1 2 1 0 4 adeq benign DCLD - - -30 F129 25 F 2126 1 1 1 1 4 adeq benign 1 1 1 0 3 adeq benign ?Ca ovary - - -31 F134 45 F 2652 1 1 1 1 4 adeq benign 1 0 1 1 3 adeq benign TB/CLD - - -32 F135 40 F 70289 0 1 0 0 1 un suit non dia 1 1 1 1 4 adeq benign ?Ca ovary - - -33 F137 45 M 2526 0 0 1 0 1 unsuita non diag 0 1 2 0 3 adeq benign DCLD - - -34 F138 58 F 2382 1 1 1 1 4 adeq benign 1 1 1 1 4 adeq benign TB/CLD - - -35 F140 42 M 2598 1 1 1 1 4 adeq benign 0 1 2 1 4 adeq benign DCLD - - -36 F192 19 M 2608 1 0 1 1 3 adeq benign 1 1 1 1 4 adeq benign Pseudocyst pan - - -37 F832 45 F 7627 2 1 1 2 6 adeq suspicious 0 1 2 0 3 adeq benign ?Ca ovary - - -38 F3784 65 F 62097 2 2 1 2 7 superior suspicious 1 1 1 1 4 adeq benign ?Ca ovary - - -39 F881 32 F 16072 1 1 0 1 3 adeq benign 0 1 2 0 3 adeq benign ?Benign cyst - - -40 F927 55 F 14001 1 1 1 1 4 adeq benign 2 0 1 0 3 adeq benign HSM/Chr.chol - - -41 F932 52 M 16998 1 2 1 1 5 adeq benign 1 0 1 1 3 adeq benign DCLD - - -42 F938 62 F 859 1 1 1 1 4 adeq benign 1 1 1 1 4 adeq benign Recur-Ca cx - - -43 F939/16 59 F 15204 2 1 2 1 6 superior suspicious 1 0 1 2 4 adeq benign Ca ovary - - -44 F948 65 F 16432 1 1 1 1 4 adeq benign 1 0 1 1 3 adeq benign TB/CLD - - -45 F960 32 M 17506 1 1 2 1 5 adeq benign 1 1 1 1 4 superior benign DCLD - - -
CONVENTIONALSMEAR
CELL BLOCKS.No
PATHNO
AGE SEX IP/OP NO GRADEQUALITY DIAGNOSIS CLINICAL DIAGNOSISKi67
MARKERSCORE

QUALITY DIAGNOSIS
C B M A S C B M A S
CONVENTIONALSMEAR
CELL BLOCKS.No
PATHNO
AGE SEX IP/OP NO GRADEQUALITY DIAGNOSIS CLINICAL DIAGNOSISKi67
MARKERSCORE
46 F968 31 G 17902 1 1 1 1 4 adeq benign 0 1 1 2 4 adeq benign Beni ova cyst - - -47 F969 62 M 17105 1 0 2 1 3 adeq benign 1 1 1 1 4 adeq benign ?Ca stomach - - -48 F970 40 M 17747 1 1 1 1 4 adeq benign 1 0 1 1 3 adeq benign DCLD - - -49 F973 68 M 3333 1 1 0 0 2 un suitab non diag 0 1 1 2 4 adeq benign DCLD/ascit/ple - - -50 F982 52 F 874 1 1 1 1 4 adeq benign 1 1 1 1 4 adeq benign ?Ca stomach - - -51 F984 57 F 56757 2 1 2 1 6 superior malignant 2 1 2 2 7 superior malignant Ca ovary done 2 High52 F1026 70 M 19178 1 1 0 0 2 unsuita non diag 1 0 1 1 3 adeq benign DCLD /asci - - -53 F1059 76 M 16818 1 1 1 1 4 adeq benign 1 1 0 1 3 adeq benign B/L pneumo.co - - -54 F1073 36 M 20421 1 1 1 1 4 adeq benign 2 0 1 0 3 adeq benign ?Liver secon - - -55 F1083 32 M 19471 0 1 0 0 1 unsuita non diagn 1 1 1 1 4 adeq benign TB/CLD - - -56 F1021 62 F 16223 1 1 1 1 4 adeq benign 2 0 1 0 3 adeq benign ?Ca ovary - - -57 F1059 28 F 19639 1 1 1 1 4 adeq benign 1 1 1 1 4 adeq benign TB/CLD - - -58 F1060 50 F 18435 2 1 2 2 7 superior malignant 1 1 2 2 6 superior malignant Ca breast-met done 2 High59 F1091 47 F 21520 1 0 2 1 4 adeq benign 1 1 0 1 3 adeq benign Rt ovary cyst - - -60 F1065 23 M 3570 1 1 1 1 4 adeq benign 1 0 1 1 3 adeq benign TB/CLD - - -61 F1506 48 M 2736 1 0 1 1 3 adeq benign 1 1 1 1 4 adeq benign DCLD - - -62 F1507 57 M 27246 2 1 1 1 5 adeq benign 1 0 1 1 3 adeq benign DCLD - - -63 F1509 65 M 27182 1 1 1 1 4 adeq benign 2 0 1 0 3 adeq benign DCLD - - -64 F1526 15 F 27567 1 1 1 1 4 adeq benign 1 1 1 1 4 adeq benign ?TB-abdo - - -65 F1543 40 F 23772 1 0 1 1 3 adeq benign 1 0 1 1 3 adeq benign ?Ca ovary - - -66 F2959 45 M 18257 1 1 1 1 4 adeq benign 1 1 0 1 3 adeq benign DCLD - - -67 F3046 57 F 53966 1 1 1 1 4 adeq benign 1 1 1 1 4 adeq benign DM/Hypothy/as - - -68 F3814 60 F 62116 1 1 1 1 4 adeq benign 2 0 1 0 3 adeq benign Grade 1 MRD - - -69 F973 60 M 18912 1 0 0 1 2 unsuita non diag 1 1 0 1 3 adeq benign DCLD - - -70 F2971 42 M 53507 1 0 2 2 5 adeq benign 1 0 1 1 3 adeq benign CVA/DCLD - - -71 F3234 50 M 57972 1 1 1 1 4 adeq benign 2 0 1 0 3 adeq benign DCLD/PHT - - -72 F3140 43 M 56247 1 1 1 1 4 adeq benign 1 1 1 1 4 adeq benign DCLD - - -73 F2995 50 M 53654 1 0 0 1 2 unsuita non diag 1 1 0 1 3 adeq benign HSM /DCLD - - -74 F3213 41 M 57835 1 1 1 1 4 adeq benign 2 0 1 0 3 adeq benign DCLD - - -75 F3141 49 M 56933 1 0 1 2 4 adeq benign 1 1 1 0 3 adeq benign DCLD/Asciies - - -76 F3199 54 M 56713 1 1 1 1 4 adeq benign 1 0 1 1 3 adeq benign CAD/ Ascities - - -77 F3163 34 F 51836 2 1 1 1 5 adeq benign 1 1 2 2 6 superior malignant Ca ovary done 1 Low78 F1686 63 M 30379 1 1 1 1 4 adeq benign 1 0 1 1 3 adeq benign Chro.liver-dis - - -79 F1685 53 M 30284 1 0 1 1 3 adeq benign 1 1 0 1 3 adeq benign DCLD - - -80 F1946 46 F 25758 1 1 1 1 4 adeq benign 1 1 1 1 4 adeq benign ?Ca ovary - - -81 F1908 22 F 33611 1 0 2 1 4 adeq benign 2 0 1 0 3 adeq benign ?TB-abdo - - -82 F1959 29 F 35318 1 0 0 1 2 unsuita non diag 1 1 1 1 4 adeq benign ?TB-abdo - - -83 F1246 59 M 21548 2 1 2 1 6 superior malignant 2 1 2 1 6 superior malignant Ca stomach done 2 High84 F1385 62 F 24304 1 1 1 1 4 adeq suspicious 1 1 0 0 2 unsuit non diag ?Ca ovary - - -85 F1754 47 F 25254 2 1 1 1 5 adeq benign 1 0 0 1 2 unsuit non diag ?Lympho-stom - - -86 F1762 48 F 26612 1 1 1 1 4 adeq benign 1 1 1 1 4 adeq benign Lt ova cyst - - -87 F1765 30 M 26674 1 1 2 1 5 adeq benign 1 0 2 1 4 adeq benign Pseudocyst pan - - -88 F1767 55 F 32381 2 1 2 2 7 superior malignant 1 0 0 1 2 unsuit non diagn ?Ca ovary - - -89 F2230 31 F 30818 2 1 1 1 5 adeq suspicious 1 0 0 0 1 unsuit non diagn Rt adnex mass - - -90 F2832 57 F 46083 1 1 2 2 6 adeq suspicious 1 1 0 0 2 unsuit non diagn ?Ca ovary - - -

QUALITY DIAGNOSIS
C B M A S C B M A S
CONVENTIONALSMEAR
CELL BLOCKS.No
PATHNO
AGE SEX IP/OP NO GRADEQUALITY DIAGNOSIS CLINICAL DIAGNOSISKi67
MARKERSCORE
91 F3491 48 F 10714 1 1 2 1 5 adeq malignant 2 1 2 2 7 superior malignant Ca ovary done 1 Low92 F3784 48 F 21447 1 0 1 1 3 adeq benign 1 1 1 0 3 adeq benign ?Ca ovary - - -93 F2791 55 F 18172 1 1 2 1 5 adeq malignant 0 1 0 0 1 unsuit non diagno Liver sec - - -94 F3958 65 F 1580 1 2 2 1 6 superior malignant 2 0 2 2 6 superior malignant ?Ca ovary done 1 Low95 F1468 62 M 10456 1 1 1 1 4 adeq benign 1 1 1 1 4 adeq benign ?Ca stomach - - -96 F4256 60 F 74767 1 2 2 1 6 superior suspicious 1 2 2 1 6 superior malignant Ca ovary done 1 Low97 F3879 64 F 65922 1 1 1 1 4 superior suspicious 2 1 2 2 7 superior malignant Ca ovary done 1 Low98 F3187 63 M 57101 1 2 1 1 4 adeq benign 2 1 2 1 6 superior malignant Ca stomach done 2 High99 F3876 57 F 14102 1 0 1 1 3 adeq benign 1 1 1 1 4 adeq benign ?Ca ovary - - -
100 F3293 61 F 48041 1 1 1 1 4 adeq suspicious 1 0 1 1 3 adeq benign ?Ca ovary - - -



Related Documents





![IT 16 - Cytology of Body Fluid - HHH [Patologi Klinik]](https://static.cupdf.com/doc/110x72/577cc3a91a28aba71196c1a7/it-16-cytology-of-body-fluid-hhh-patologi-klinik.jpg)





