Prince of Wales clinical school and Lowy cancer research centre Decision making – square pegs in round holes: the Australian HTA experience Professor Robyn Ward Director POW Cancer centre, Clinical Associate Dean UNSW Chair of Medical Services Advisory Committee and Member PBAC

Robyn Ward - Dept of Health and Aging: Decision Making – Square Pegs In Round Holes: The Australian HTA Experience
Jul 30, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Prince of Wales clinical school and Lowy cancer research centre
Decision making – square pegs in round
holes: the Australian HTA experience
Professor Robyn Ward
Director POW Cancer centre, Clinical Associate Dean UNSW
Chair of Medical Services Advisory Committee and Member PBAC


Pharmaceuticals
$8 billion pa
Non-
pharmaceuticals
$16 billion pa
Reimbursement of health care through
the public purse
PBAC MSAC

“In theory there is no
difference between
theory and practice HTA of drugs and other
health interventions
In practice there is”
Yogi Berra

Overview of talk
The MSAC process
• review the steps
• coordination with TGA, PBAC, PLAC
Three case studies
• Prepare for the future
• Follow the money
• Exit strategy
The future

The MSAC process
• review the steps
• coordination with TGA, PBAC, PLAC

Overview of the reimbursement process
Positioning and dialogue
Preparing the submission
Appraisal of evidence
Implementation
Submission
lodgement

• Complete short application form
• Protocol advisory committee
Define the question for public subsidy Define the bellwether issue – evidence, economics, data Consultation – with HESP, public, competitors and allies
PASC is not compulsory but its functions are
Positioning and dialogue

Preparing the submission
• Contracted assessment
OR
• Prepare your own

Evidence should be fit for purpose
• RCT
• Observational studies
• MBS data
for utilisation
for patterns of care
• Grey literature
• Consumer voice
• TGA submissions
• PLAC evaluations
• Submissions to other HTA bodies

“Any belief that the controlled trial is the only
way … to generate evidence would mean
not that the pendulum had swung too far but
that it had come right off the hook”
Bradford Hill the architect of the RCT

Lodgement of the submission
• External critique of submission
• Review by evaluation subcommittee
• Policy input
• Opportunities for rebuttal
• MSAC consideration and
recommendations, outlining way forward
• Public summary documents
Appraisal of the evidence

Implementation - departmental work, government decision and
release to the wild
• Potential time savings because
policy input and MBS costing now
part of the MSAC process

The MSAC process
• review the steps
• coordination with TGA, PBAC, PLAC
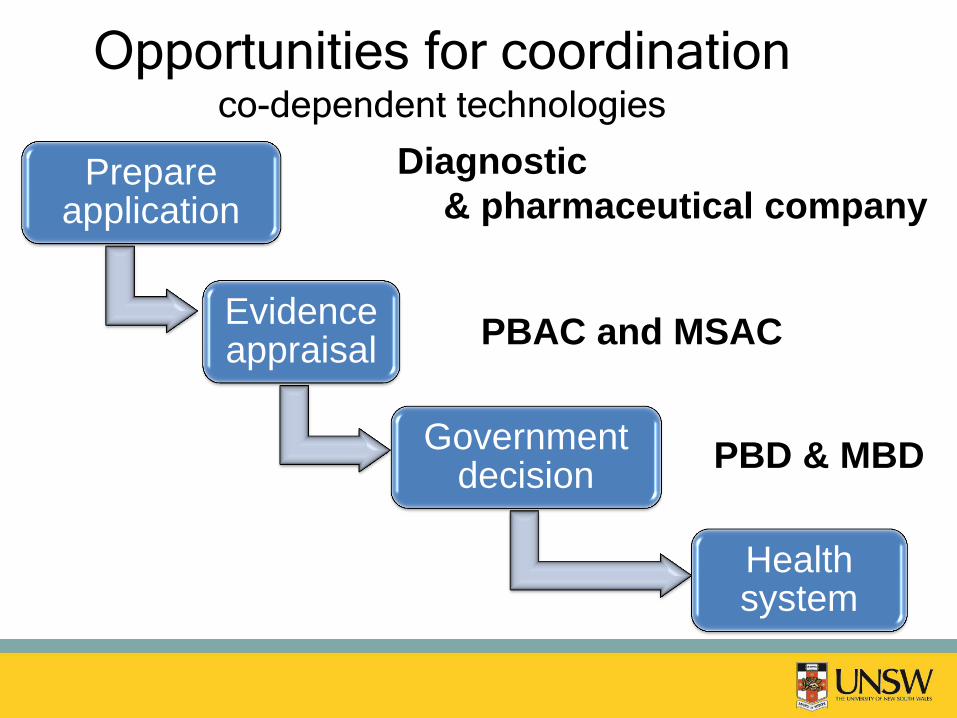
Prepare application
Evidence appraisal
Government decision
Health system
Diagnostic
& pharmaceutical company
PBAC and MSAC
PBD & MBD
Opportunities for coordination co-dependent technologies
Coordination is possible
test and drugs
• Melanoma - BRAF testing and dabrafenib
• Colorectal cancer - KRAS and anti-EGFR
antibodies
• Lung cancer – TKIs and EGFR testing

Egs
• Botox for bladder dysfunction
• Sculptra for lipoatrophy
Coordination is possible
drugs and services

Success factors
• Role (responsibility) delineation
• Taking genetic testing seriously
• Champions in government
• Commitment to making the system work

Case studies
1. Prepare for the future
esp. for co-dependent test/drug
2. Follow the money
3. Exit strategy

Case 1 – prepare for the future
The idea of a single target - single
treatment model (for cancer) is a
conceptual fallacy
Case 1 - Pre-existing state
EGFR antibodies and KRAS testing reimbursed for
patients with metastatic colorectal cancer
History
2004 - FDA approved companion diagnostic in
DakoCytomation EGFR pharmDx immunostaining
(detects overexpression of EGFR)
2008 – KRAS mutations a negative predicator of
response to anti-EGFR antibodies

Case 1 - The catalyst for change: Testing for KRAS status is not good enough
Other activating RAS mutations may
also be negative predictive biomarkers
for anti-EGFR therapy.
September 2013

Case 1 – Consequences, lessons learnt
• Yet again reinforces the conceptual fallacy of single target -
single treatment model
• Yet again shows that the net benefits of a co-dependent test
and drug are negated if incorrect test assignment exposes
patients to inferior treatments
• Yet again reinforces the importance of providing preclinical
data on drug/target interactions (biological plausibility)
• Yet again highlights the importance of including a plan for
updating evidence – esp. emerging molecular data and impact
on risk/benefit of treatment
Case 2 – follow the money

Case 2 – Pre-existing state
Unloved MBS item number (42740) for eye
injections - $295.15 - rarely used
Case 2 – The catalyst for change
• Ranibizumab (LUCENTIS®) listed on the
Pharmaceutical Benefits Scheme (PBS) on 1 August
2007 for the treatment of age related macular
degeneration.
BUT
• Costs of administration of Lucentis (using
previously unloved MBS item number 42740) was
not evaluated.

Case 2 - Consequences
0
10,000
20,000
30,000
40,000
50,000
60,000
70,000
80,000
Jan-03 Jan-04 Jan-05 Jan-06 Jan-07 Jan-08 Jan-09 Jan-10 Jan-11 Jan-12 Jan-13
Number of eye injection services - 2003 to 2013
LUCENTIS® listed on the PBS
Rebates for
Avastin®
restricted
Serv
ices p
er
quart
er

Benefits paid for out-of-hospital eye injection
services ($Million)
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
EMSN
Rebates

Response from government
• To address excessive fee charging by a
small number of providers
• Extended medicare safety net benefit
capped at equal to 80% of the MBS fee –
introduced on 1st November 2012 (2012-
2013 budget)

Average fees charged fell
$0
$200
$400
$600
$800
$1,000
$1,200
$1,400
Jan-Mar 2011 Jul-Sept 2011 Jan-Mar 2012 Jul-Sept 2012 Jan-Mar 2013
Average fees charged for eye injection services in postcodes with the highest average fees prior to
capping
Postcode A
Postcode B
Postcode C
Capping introduced (1 November 2012)
Avera
ge f
ee c
harg
ed (
$)

Case 2 – Consequences for
submissions
• Consider out of pocket patient expenses
• Consider incentives for health
practitioners in terms of MBS billing
• Consider the knock-on effects on the
health system of new technologies
Case 3 – Removal of an item from the schedule

Case 3 - Pre-existing state
Hyperbaric oxygen therapy funded
for non-diabetic wounds on the
MBS since 2003 on an “interim
basis”

Case 3 - The catalyst for change
Scheduled interim funding review in 2011
MSAC reviewed the evidence
MSAC advised the minister that it did not
support continuation of interim funding
(scientific judgement)
Minister discontinued public funding in 2012
Case 3 - Consequences
• Political interventions
• Multiple reconsiderations by MSAC
• Commonwealth Senate hearing
• Items not reinstated on schedule
The future
Lay bare the evidence gaps and describe if
and how they can be addressed
Live with the consequences of a changing
evidence base and disinvest if
drug/test/technology can’t be shown to work
Communicate intentions & progress to all
is it possible…..
Related Documents











