Risk Factors for Pulmonary Barotrauma in Divers* Kay Tetzloff, MD; Michael Renter, MD; Bernd Leplow, PhD; Martin Heller, MD; and Eyke Bettinghausen, MD Study objectives: Pulmonary barotrauma (PBT) of ascent is a feared complication in compressed air diving. Although certain respiratory conditions are thought to increase the risk of suffering PBT and thus should preclude diving, in most cases of PBT, risk factors are described as not being present. The purpose of our study was to evaluate factors that possibly cause PBT. Design: We analyzed 15 consecutive cases of PBT with respect to dive factors, clinical and radiologic features, and lung function. They were compared with 15 cases of decompression sickness without PBT, which appeared in the same period. Results: Clinical features of PBT were arterial gas embolism (n= 13), mediastinal emphysema (n=l), and pneumothorax (n=l). CT of the chest (performed in 12 cases) revealed subpleural emphysematous blebs in 5 cases that were not detected in preinjury and postinjury chest radiographs. A comparison of predive lung function between groups showed significantly lower midexpiratory flow rates at 50% and 25% of vital capacity in PBT patients (p<0.05 and p<0.02, respectively). Conclusions: These results indicate that divers with preexisting small lung cysts and/or end- expiratory flow limitation may be at risk of PBT. (CHEST 1997; 112:654-59) Key words: computed tomography; diving; lung function; pulmonary barotrauma Abbreviations: DCS = decompression sickness; IVC=inspiratory vital capacity; MEF255075=midexpiratory flow at 25%, 50%, and 75%, respectively, of vital capacity; PBT=pulmonary barotrauma; VC=vital capacity A lthough rare, pulmonary barotrauma (PBT) of -^ascent is a well-known complication of com¬ pressed air diving. Its clinical features are pulmonary tissue damage, pneumothorax, and mediastinal em- For editorial comment see page 576 physema. The most feared sequela, however, is arterial gas embolism, which is the second largest cause of death in underwater diving accidents after drowning.12 These manifestations may occur singly or in combination.34 One way of reducing diving fatalities is to identify those people who may be predisposed to an in¬ creased risk of death from PBT. Behavioral factors such as voluntary breath-holding during rapid ascent *From the Department of Diving and Hyperbaric Medicine (Drs. Tetzlaff and Bettinghausen), Naval Medical Institute, Kiel; and the Departments of Diagnostic Radiology (Drs. Reuter and Heller) and Psychology (Dr. Leplow), University Hospital, Keil, Germany. Manuscript received October 29, 1996; revision accepted April 16, 1997. Reprint requests: Kay Tetzlaff, MD, Schiffahrtmedizinisches In- stut der Marine, Kopperpahler Allee 19, d-24119 Kronshagen, Germany and predisposing pulmonary abnormalities have been identified as increasing mortality and thus are recommended to preclude diving.5 Nevertheless, in most cases of PBT reported in the literature, appro¬ priate exhalation techniques had been carried out and postinjury examination revealed no clinical evi¬ dence of lung damage.6-9 Progress in diagnostics encouraged us to evaluate risk factors of PBT in a retrospective survey of patients referred to our insti¬ tute during the past 6 years. Materials and Methods We studied 15 PBT patients, who had been referred to our department consecutively, and compared them with 15 patients who suffered neurologic decompression sickness (DCS type 2). There were 11 male and 4 female divers in both groups. Seven patients in the PBT group were current smokers vs nine in the DCS group (Table 1). Among the PBT patients, there were three military divers, one police diver, one commercial diver, seven sports divers, two submarine escape tank trainees, and one hyperbaric chamber attendant. Five divers had diving experience of >100 dives. Medical history revealed prior lung diseases in four patients: childhood asthma in two patients, pleuritis in one, and one patient had suffered a chest injury in early childhood. Four patients had performed rapid ascents (Table 2). In the DCS group, there were three military divers and 12 sports divers. 654 Clinical Investigations

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Risk Factors for Pulmonary Barotraumain Divers*
Kay Tetzloff, MD; Michael Renter, MD; Bernd Leplow, PhD; Martin Heller, MD;and Eyke Bettinghausen, MD
Study objectives: Pulmonary barotrauma (PBT) of ascent is a feared complication in compressedair diving. Although certain respiratory conditions are thought to increase the risk of sufferingPBT and thus should preclude diving, in most cases of PBT, risk factors are described as not beingpresent. The purpose of our study was to evaluate factors that possibly cause PBT.Design: We analyzed 15 consecutive cases of PBT with respect to dive factors, clinical andradiologic features, and lung function. They were compared with 15 cases of decompressionsickness without PBT, which appeared in the same period.Results: Clinical features of PBT were arterial gas embolism (n= 13), mediastinal emphysema(n=l), and pneumothorax (n=l). CT of the chest (performed in 12 cases) revealed subpleuralemphysematous blebs in 5 cases that were not detected in preinjury and postinjury chestradiographs. A comparison of predive lung function between groups showed significantly lowermidexpiratory flow rates at 50% and 25% of vital capacity in PBT patients (p<0.05 and p<0.02,respectively).Conclusions: These results indicate that divers with preexisting small lung cysts and/or end-expiratory flow limitation may be at risk ofPBT. (CHEST 1997; 112:654-59)
Key words: computed tomography; diving; lung function; pulmonary barotrauma
Abbreviations: DCS= decompression sickness; IVC=inspiratory vital capacity; MEF255075=midexpiratory flow at25%, 50%, and 75%, respectively, of vital capacity; PBT=pulmonary barotrauma; VC=vital capacity
A lthough rare, pulmonary barotrauma (PBT) of-^ascent is a well-known complication of com¬
pressed air diving. Its clinical features are pulmonarytissue damage, pneumothorax, and mediastinal em-
For editorial comment see page 576
physema. The most feared sequela, however, isarterial gas embolism, which is the second largestcause of death in underwater diving accidents afterdrowning.12 These manifestations may occur singlyor in combination.34One way of reducing diving fatalities is to identify
those people who may be predisposed to an in¬creased risk of death from PBT. Behavioral factorssuch as voluntary breath-holding during rapid ascent
*From the Department of Diving and Hyperbaric Medicine (Drs.Tetzlaff and Bettinghausen), Naval Medical Institute, Kiel; andthe Departments of Diagnostic Radiology (Drs. Reuter andHeller) and Psychology (Dr. Leplow), University Hospital, Keil,Germany.Manuscript received October 29, 1996; revision accepted April16, 1997.Reprint requests: Kay Tetzlaff, MD, Schiffahrtmedizinisches In-stut der Marine, Kopperpahler Allee 19, d-24119 Kronshagen,Germany
and predisposing pulmonary abnormalities havebeen identified as increasing mortality and thus are
recommended to preclude diving.5 Nevertheless, inmost cases of PBT reported in the literature, appro¬priate exhalation techniques had been carried outand postinjury examination revealed no clinical evi¬dence of lung damage.6-9 Progress in diagnosticsencouraged us to evaluate risk factors of PBT in a
retrospective survey of patients referred to our insti¬tute during the past 6 years.
Materials and Methods
We studied 15 PBT patients, who had been referred to our
department consecutively, and compared them with 15 patientswho suffered neurologic decompression sickness (DCS type 2).There were 11 male and 4 female divers in both groups. Sevenpatients in the PBT group were current smokers vs nine in theDCS group (Table 1). Among the PBT patients, there were threemilitary divers, one police diver, one commercial diver, seven
sports divers, two submarine escape tank trainees, and one
hyperbaric chamber attendant. Five divers had diving experienceof >100 dives. Medical history revealed prior lung diseases infour patients: childhood asthma in two patients, pleuritis in one,and one patient had suffered a chest injury in early childhood.Four patients had performed rapid ascents (Table 2). In the DCSgroup, there were three military divers and 12 sports divers.
654 Clinical Investigations

Table 1.Subject Characteristics*
PBT (n= 15) DCS (n=15) p Value
Age, yr
Height, cm
Weight, kgSmokersPrior lung disease
25.2±3.3177.9±7.474.1±12.8
74
27.9±4.6179.9±8.476.9+12.0
9None
NSNSNS
*Values are means±SDs (age, height,medical history). NS=not significant.
;ight) and totals (smoking,
Eight divers were experienced (>100 dives). None had prior lungdiseases. All patients had undergone a medical examination forfitness to dive. The military and commercial divers were found as
fit to dive in a German Navy diving medical examination thatdemands normal chest radiograph in two planes and normalspirometric values with respect to vital capacity (VC), FEVl5 andthe relation of FEVX in percent of VC (FEV^VC). Becausemedical examinations are not compulsory for recreational divers,chest radiographs were not available in all of our cases.
According to the common procedure,210 initial diagnosis was
made solely on the basis of history and clinical findings (Tables 3and 4).
All patients underwent postinjury chest radiograph in two
planes and lung function testing (Jaeger Master-Lab; Germany).In one patient, postinjury lung function was not available becauseof his worse clinical outcome (Table 3). Twelve PBT patients andfour DCS patients underwent additional CT of the chest fordiagnostic reasons. CT was performed using the conventionalmode (seven patients) on a scanner (Tomoscan LX scanner;
Philips; Hamburg, Germany) using contiguous slices 8 to 10 mmthick. In the remaining, more recent patients, the spiral mode(Somatom Plus-S; Siemens; Erlangen, Germany) was applied11with a table feed rate per second and a nominal section thicknessof 10 mm each, increment of 8 mm. Chest radiographs were
performed within several hours for the military divers and within2 to 8 days postinjury for the sports divers. Preinjury chestradiographs were available for 10 PBT patients (taken 5 to 12months before the accident) and revealed no abnormality.
Preinjury lung function tests were available for all patients.Static lung volumes (inspiratory VC [IVC], FVC), dynamicvolumes (FEV1), and expiratory flow rates (midexpiratory flow at75%, 50%, and 25% of vital capacity [MEF755025]) were allanalyzed.To avoid an observer bias, the clinical diagnosis and the results
of lung function were checked by two diving medical officers(K.T., E.B.) in turn. The consultant radiologist (M.R.) was notinformed of the clinical diagnosis.Data were analyzed by testing the differences between group
means of subject characteristics and spirometric values by t tests
Table 2.Dive Characteristics*
PBT (n-15) DCS (n=15)Scuba diveFree ascent
Buoyant asc
Emergency asc
Chamber dive
102111
15NoneNoneNoneNone
*Values are totals; scuba.self contained underwater breathing appa¬ratus; asc=ascent.
for independent samples. A p value <0.05 was consideredsignificant. All data are given as means±1 SD.
Results
PBT patients were younger than DCS patients(25.2 vs 27.9 years; p=0.07). No significant differ¬ences between groups were found with respect to
body height (p=0.51) or weight (p= 0.54) (Table 1).Among the patients who suffered PBT from div¬
ing, there were 13 cases of arterial gas embolism, 1case of pneumothorax, and 1 case of mediastinalemphysema. In 3 of 13 cases, arterial gas embolismwas accompanied by mediastinal emphysema andpneumothorax. All but one were first incidents; one
female sports diver suffered a recurrent arterial gasembolism.
Postinjury chest radiographs showed pneumotho¬rax in two cases, atelectasis in two cases, and a
discrete pneumomediastinum in one case. Plainradiographs were normal in the remaining 10 cases.
CT of the chest revealed positive findings in 13 cases:
pleural effusion (n=l), atelectasis (n=2), pneumo¬mediastinum (n=2) (Fig 1), pneumothorax (n=2),lung cysts (n=5) (Fig 2), and alveolar infiltrate(n=l). Two patients presented no abnormality on
CT. In two patients, a follow-up CT scan showed thatthe lung cysts were unchanged after 6 and after 15months. CT of the chest was normal in all four DCScases so evaluated.
All patients initially had normal lung functionvalues with respect to IVC, FVC, and FEV^ Themeans exceeded the predicted values.12 The means
of the expiratory flow rates MEF75_25 exceededpredicted values in the DCS group only. In the PBTgroup, MEF75 and MEF50 ranged within 80 to 100%of the predicted values, while mean MEF25 did notreach 80% of the predicted values. In 10 PBTpatients, MEF25 was below 80% of the predictedvalues, whereas only one DCS patient had a reducedMEF25.
Analysis of preinjury lung function parametersrevealed a significant difference between groupswith respect to MEF25 (p<0.02) and with respect to
MEF50 (p<0.05) (Table 5, top). Analysis of postin¬jury lung function was performed in only 14 cases
due to clinical deterioration in one patient despitetherapy, who was not able to perform voluntaryspirometric maneuvers (Table 3). The postinjuryvalues only differed significantly between groupswith respect to MEF25 (p<0.05) (Table 5, bottom).Comparison of preinjury and postinjury lung func¬tion showed lower postinjury values concerning allparameters. The difference in MEF50 reached sig¬nificance in the DCS group (p<0.05).
CHEST/112 73/SEPTEMBER, 1997 655
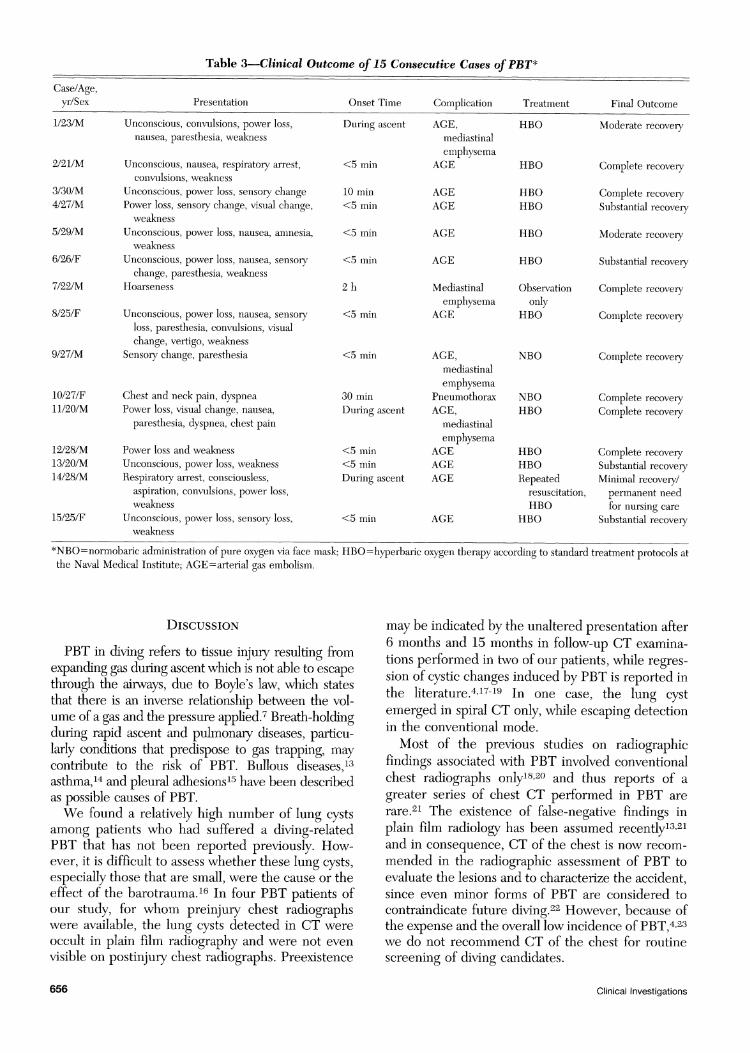
Table 3.Clinical Outcome of 15 Consecutive Cases ofPBT*Case/Age,yr/Sex Presentation Onset Time Complication Treatment Final Outcome
1/23/M Unconscious, convulsions, power loss, During ascentnausea, paresthesia, weakness
2/21/M Unconscious, nausea, respiratory arrest, <5 minconvulsions, weakness
3/30/M Unconscious, power loss, sensory change 10 min4/27/M Power loss, sensory change, visual change, <5 min
weakness5/29/M Unconscious, power loss, nausea, amnesia, <5 min
weakness6/26/F Unconscious, power loss, nausea, sensory <5 min
change, paresthesia, weakness7/22/M Hoarseness2 h
8/25/F Unconscious, power loss, nausea, sensory <5 minloss, paresthesia, convulsions, visualchange, vertigo, weakness
9/27/M Sensory change, paresthesia <5 min
10/27/F Chest and neck pain, dyspnea 30 min11/20/M Power loss, visual change, nausea, During ascent
paresthesia, dyspnea, chest pain
12/28/M Power loss and weakness <5 min13/20/M Unconscious, power loss, weakness <5 min14/28/M Respiratory arrest, consciousless, During ascent
aspiration, convulsions, power loss,weakness
15/25/F Unconscious, power loss, sensoiy loss, <5 minweakness
AGE,mediastinalemphysema
AGE
AGEAGE
AGE
AGE
Mediastinalemphysema
AGE
AGE,mediastinalemphysema
PneumothoraxAGE,
mediastinalemphysema
AGEAGEAGE
AGE
HBO
HBO
HBOHBO
HBO
HBO
Observationonly
HBO
NBO
NBOHBO
HBOHBO
Repeatedresuscitation,HBO
HBO
Moderate recovery
Complete recovery
Complete recoverySubstantial recovery
Moderate recovery
Substantial recovery
Complete recovery
Complete recovery
Complete recovery
Complete recoveryComplete recovery
Complete recoverySubstantial recoveryMinimal recovery/permanent needfor nursing care
Substantial recovery
*NBO=normobaric administration of pure oxygen via face mask; HBO=hyperbaric oxygen therapy according to standard treatment protocols atthe Naval Medical Institute; AGE=arterial gas embolism.
Discussion
PBT in diving refers to tissue injury resulting fromexpanding gas during ascent which is not able to escapethrough the airways, due to Boyle's law, which statesthat there is an inverse relationship between the vol¬ume of a gas and the pressure applied.7 Breath-holdingduring rapid ascent and pulmonary diseases, particu¬larly conditions that predispose to gas trapping, maycontribute to the risk of PBT. Bullous diseases,13asthma,14 and pleural adhesions15 have been describedas possible causes of PBT.We found a relatively high number of lung cysts
among patients who had suffered a diving-relatedPBT that has not been reported previously. How¬ever, it is difficult to assess whether these lung cysts,especially those that are small, were the cause or theeffect of the barotrauma.16 In four PBT patients ofour study, for whom preinjury chest radiographswere available, the lung cysts detected in CT were
occult in plain film radiography and were not even
visible on postinjury chest radiographs. Preexistence
may be indicated by the unaltered presentation after6 months and 15 months in follow-up CT examina¬tions performed in two of our patients, while regres¬sion of cystic changes induced by PBT is reported inthe literature.41719 In one case, the lung cystemerged in spiral CT only, while escaping detectionin the conventional mode.Most of the previous studies on radiographic
findings associated with PBT involved conventionalchest radiographs only1820 and thus reports of a
greater series of chest CT performed in PBT are
rare.21 The existence of false-negative findings inplain film radiology has been assumed recently13'21and in consequence, CT of the chest is now recom¬
mended in the radiographic assessment of PBT toevaluate the lesions and to characterize the accident,since even minor forms of PBT are considered tocontraindicate future diving.22 However, because ofthe expense and the overall low incidence of PBT,423we do not recommend CT of the chest for routinescreening of diving candidates.
656 Clinical Investigations
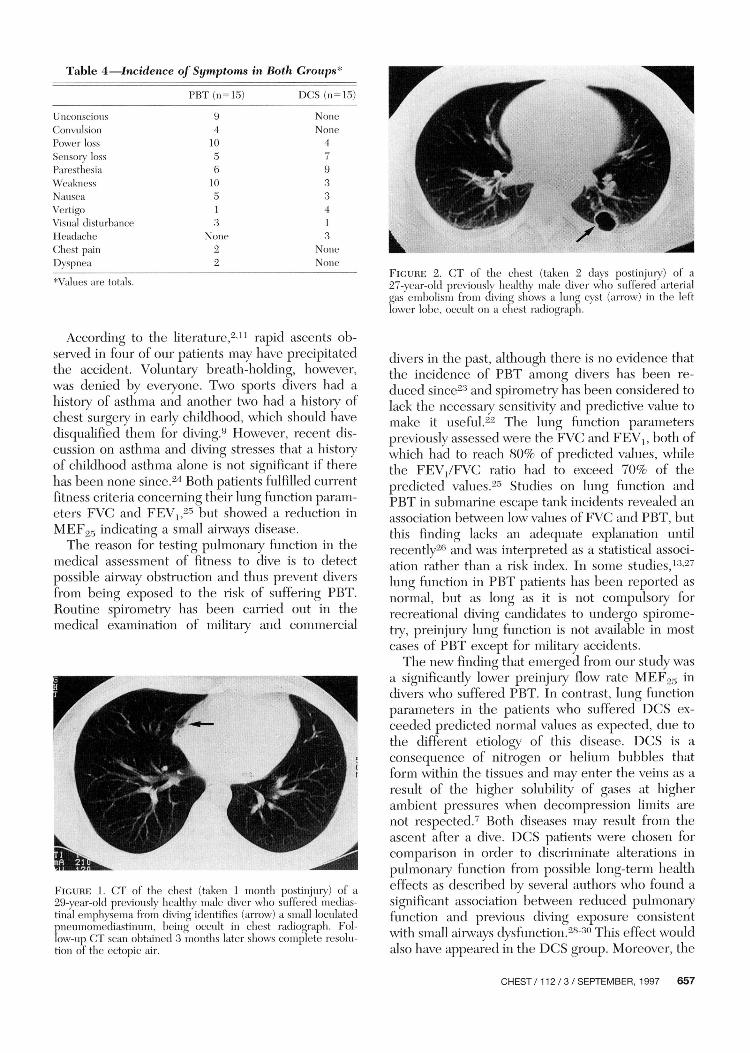
Table 4.Incidence of Symptoms in Both Groups*PBT(n=15) DCS (n=15)
UnconsciousConvulsionPower lossSensor)' lossParesthesiaWeaknessNauseaVertigoVisual disturbanceHeadacheChest painDyspnea
94105610513
None22
NoneNone4
33413
NoneNone
*Values are totals.
According to the literature,211 rapid ascents ob¬served in four of our patients may have precipitatedthe accident. Voluntary breath-holding, however,was denied by everyone. Two sports divers had a
history of asthma and another two had a history ofchest surgery in early childhood, which should havedisqualified them for diving.9 However, recent dis¬cussion on asthma and diving stresses that a historyof childhood asthma alone is not significant if therehas been none since.24 Both patients fulfilled currentfitness criteria concerning their lung function param¬eters FVC and FEVt,25 but showed a reduction in
MEF25 indicating a small airways disease.The reason for testing pulmonary function in the
medical assessment of fitness to dive is to detectpossible airway obstruction and thus prevent diversfrom being exposed to the risk of suffering PBT.Routine spirometry has been carried out in themedical examination of military and commercial
Figure 1. CT of the chest (taken 1 month postinjury) of a
29-year-old previously healthy male diver who suffered medias¬tinal emphysema from diving identifies (arrow) a small loculatedpneumomediastinum, being occult in chest radiograph. Fol¬low-up CT scan obtained 3 months later shows complete resolu¬tion of the ectopic air.
Figure 2. CT of the chest (taken 2 days postinjury) of a
27-year-old previously healthy male diver who suffered arterialgas embolism from diving shows a lung cyst (arrow) in the leftlower lobe, occult on a chest radiograph.
divers in the past, although there is no evidence thatthe incidence of PBT among divers has been re¬
duced since23 and spirometry has been considered tolack the necessary sensitivity and predictive value tomake it useful.22 The lung function parameterspreviously assessed were the FVC and FEV1? both ofwhich had to reach 80% of predicted values, whilethe FEV/FVC ratio had to exceed 70% of thepredicted values.25 Studies on lung function andPBT in submarine escape tank incidents revealed an
association between low values ofFVC and PBT, butthis finding lacks an adequate explanation untilrecently26 and was interpreted as a statistical associ¬ation rather than a risk index. In some studies,13-27lung function in PBT patients has been reported as
normal, but as long as it is not compulsory forrecreational diving candidates to undergo spirome¬try, preinjury lung function is not available in mostcases of PBT except for military accidents.The new finding that emerged from our study was
a significantly lower preinjury flow rate MEF25 indivers who suffered PBT. In contrast, lung functionparameters in the patients who suffered DCS ex¬
ceeded predicted normal values as expected, due tothe different etiology of this disease. DCS is a
consequence of nitrogen or helium bubbles thatform within the tissues and may enter the veins as a
result of the higher solubility of gases at higherambient pressures when decompression limits are
not respected.7 Both diseases may result from theascent after a dive. DCS patients were chosen forcomparison in order to discriminate alterations in
pulmonary function from possible long-term healtheffects as described by several authors who found a
significant association between reduced pulmonaryfunction and previous diving exposure consistentwith small airways dysfunction.2830 This effect wouldalso have appeared in the DCS group. Moreover, the
CHEST / 112 / 3 / SEPTEMBER, 1997 657

Table 5.Preinjury (Top) and Postinjury (Rottom) Lung Function*
PBT (n=15) % of Predicted DCS (n=15) of Predicted p Value
L/sL/sL/s
PreinjuryIVC, LFVC, LFEVjl, LMEF75:MEF50:MEF25:
PostinjuryIVC, LFVC, LFEVl5 LMEF75, L/sMEFsq, L/sMEF9. L/s
5.28+0.855.5±0.89
4.61±0.378.26±1.735.25±1.42.07±0.79PBT (n=14)5.16±1.045.25±1.034.25+0.698.14±2.244.82±1.262.12±0.75
102.0±11.0107.6±12.2101.5±11.097.3±21.687.5±23.378.5±28.5
7o of Predicted98.5+ 13.0104.9±13.0106.6±22.796.9±24.686.9±23.875.4 ±22.7
5.125.794.768.336.193.0
DCS5.195.474.558.365.372.56
1.111.82
±1.121.452.211.25
(n=15)±0.99±1.160.912.19
±1.420.93
105.0±20.2116.0±26.5111.5±18.7103.2±20.2113.1±36.7112.8±44.4
% of Predicted99.6±13.9108.1±17.8107.6±17.3101.1±19.999.2±24.2100.9±32.8
NSNSNSNS<0.05<0.02p ValueNSNSNSNSNS<0.05
^Values are given as means of spirometric values and as means of predicted (from 12) ±SDs; NS^not significant.
relatively low diving experience of our patientsmakes such exposure unlikely to confound the re¬
sults.The difference in age between groups amounted
to 2.7 years. Lung function results may not havebeen influenced by this, because the well-knownage-related decline in lung function develops in laterdecades in life.31
It has to be pointed out that the reduction ofMEF25 indicates a usually irreversible peripheralairway obstruction due to a small airways disease.Closure of small airways, in particular, is consideredto cause gas trapping in regions distal to the site ofobstruction32 and thus may contribute to PBT. Re¬cent discussion has stressed that the expiratory flowrates MEF255075 may be of value in the assessmentof fitness to dive3234 and there now is consensus thatan MEF limitation after effort should preclude a
subject from diving.32-34'35 Our results may supportthe need to measure and assess MEF rates even atrest in the diving medical examination.
In view of the evaluated risk factors, the analysis ofclinical and radiologic features and lung functionrevealed only one patient who presented none ofthese factors. This female sports diver suffered a
moderate pneumothorax from scuba diving and re¬
covered after normobaric oxygen therapy. Thus, wefound precipitating factors in 93% of our patientswho suffered PBT from diving.We conclude that a history of respiratory disease,
preexisting lung cysts, and a reduction in the MEF25of >20% of the predicted values may contribute tothe risk of suffering PBT. Thus, we recommend theassessment of expiratory flow rates in addition toconventional spirometry for screening diving candi¬dates. The MEF50 and MEF25 or MEF25_75 shouldat least reach 80% ofthe predicted values. Moreover,the CT scanning of the chest.preferably in the
spiral mode.should be performed in the routinediagnosis of diving-related PBT.
References1 Bradley ME. Pulmonary barotrauma. In: Davis JC, Bove AA,
eds. Diving medicine. Philadelphia: Saunders, 19902 Kizer KW. Dysbaric cerebral air embolism in Hawaii. AnnEmerg Med 1987; 16:535-41
3 Broome CR, Jarvis LJ, Clark RJ. Pulmonary barotrauma insubmarine escape training. Thorax 1994; 49:186-87
4 Edmonds C, Lowry C, Pennefather J. Diving and subaquaticmedicine. 3rd ed. Oxford: Butterworth & Heinemann, 1992
5 Jenkins C, Anderson SD, Wong R, et al. Compressed airdiving and respiratory disease: a discussion document of theThoracic Society of Australia and New Zealand. Med J Aust1993; 158:275-79
6 Francis TJR, Gorman DF. Pathogenesis of the decompres¬sion disorders. In: Bennett PB, Elliott DH, eds. The physi¬ology and medicine of diving. 4th. ed. London: Saunders,1993; 454-80
7 Melamed Y, Shupak A, Bitterman H. Medical problemsassociated with underwater diving. N Engl J Med 1992;326:30-35
8 Pearson R. Diagnosis and treatment of gas embolism. In:Shilling C, Carlston C, Mathias R, eds. The physicians guideto diving medicine. New York: Plenum Press, 1984
9 Strauss RH. Diving medicine: state of the art. Am Rev RespirDis 1979; 119:1001-23
10 Leitch DR, Green RD. Pulmonary barotrauma in divers andthe treatment of cerebral arterial gas embolism. Aviat SpaceEnviron Med 1986; 57:931-38
11 Kalender WA, Seissler W, Klotz E, et al. Spiral volumetric CTwith single-breath hold technique, continuous transport, andcontinuous scanner rotation. Radiology 1990; 176:181-83
12 Quanjer PH, ed. Standardized lung function testing. Bull EurPhysiopathol Respir 1983; 19(suppl 5):7-10
13 Mellem H, Emhjellen S, Horgen O. Pulmonary barotraumaand arterial gas embolism caused by an emphysematous bullain a SCUBA diver. Aviat Space Environ Med 1990; 61:559-62
14 Weiss LD, Van Meter KW. Cerebral air embolism in asth¬matic scuba divers in a swimming pool. Chest 1995; 107:1653-54
15 Calder IM. Autopsy and experimental observations on factors
658 Clinical Investigations

leading to barotrauma in man. Undersea Biomed Res 1985;12:165-82
16 Saywell WR. Submarine escape training, lung cysts andtension pneumothorax. Br J Radiol 1989; 62:276-78
17 Collins JJ. An unusual case of air embolism precipitated bydecompression. N Engl J Med 1962; 266:595-98
18 Elliott DH, Harrison JAB, Barnard EEP. Clinical and radio¬logical features of 88 cases of decompression barotrauma. In:
Shilling CW, Beckett MW, eds. Proceedings of the SixthSymposium on Underwater Physiology. Bethesda, Md: FedAm Soc Exp Biol, 1978; 527-35
19 Liebow AA, Stark JE, Vogel J, et al. Intrapulmonary air
trapping in submarine escape training casualties. US ArmedForces Med J 1959; 10:265-89
20 Harker CP, Neuman TS, Olson LK, et al. The roentgeno-graphic findings associated with air embolism in sport scubadivers. J Emerg Med 1993; 11:443-49
21 Le Vot J, Solacroup JC, Muyard B, et al. The thorax ofpatients in diving accidents: radiologic study. J Radiol 1989;70:357-63
22 Raymond LW. Pulmonary barotrauma and related events indivers. Chest 1995; 107:1648-52
23 Leitch DR, Green RD. Recurrent pulmonary barotrauma.Aviat Space Environ Med 1986; 57:1039-43
24 Elliott DH, ed. Are asthmatics fit to dive? ConcludingStatement. Kensington, Md: Undersea Hyperbaric MedicalSociety, 1996; 84
25 Linaweaver PG. Physical and psychological examination fordiving. In: Schilling CW, Carlston CB, Mathias RA, eds. Thephysicians guide to diving medicine. New York: PlenumPress, 1984; 489-530
26 Benton PJ, Woodfine JD, Francis TJR. A review of spirom¬
etry and submarine escape training tank incidents (1987-1993) using objective diagnostic criteria. In: Elliott DH, ed.Are asthmatics fit to dive? Kensington, Md: Undersea Hyper¬baric Medical Society, 1996; 17-25
27 Lindemark C, Adolfson J. Lung rupture as a complication infree escape. In: Ornhagen H, Carlsson AL, eds. Proceedingsof the 11th Annual Meeting of the European UnderseaBiomedical Society, held at Goteborg, Sweden, August 21-23,1985. Bromma, Sweden: Kugel Tryckeri AB, 1985
28 Thorsen E, Segadal K, Kambestad B, et al. Diver's lungfunction: small airways disease? Br J Ind Med 1990; 47:519-23
29 Thorsen E, Kambestad B. Persistent small airways dysfunc¬tion after exposure to hyperoxia. J Appl Physiol 1995; 78:1421-24
30 Watt S. Effect of commercial diving on ventilatory function.Br J Ind Med 1985; 42:59-62
31 Burrows B, Cline MG, Knudson RJ, et al. A descriptiveanalysis of the growth and decline of the FEV2 and FVC.Chest 1983; 83:717-24
32 Neuman TS, Bove AA, O'Connor RD, et al. Asthma anddiving. Ann Allergy 1994; 73:344-50
33 Denison DM. Lung function testing of divers. In: Elliott DH,ed. Medical assessment of fitness to dive. Flagstaff, Ariz: Best
Publishing, 1995; 123-3334 Harries M. Why asthmatics should be allowed to dive. In:
Elliott DH, ed. Are asthmatics fit to dive? Kensington, Md:Undersea Hyperbaric Medical Society, 1996; 7-12
35 Watt S. Current criteria of pulmonary fitness to dive. In:Elliott DH, ed. Medical assessment of fitness to dive. Flag¬staff, Ariz: Best Publishing, 1995; 114-15
CHEST/ 112/3 /SEPTEMBER, 1997 659
Related Documents











