Retinopathy of prematurity Dr. Tareq rahman , Resident Phase B , Neonatology, Bangabandhu Sheikh Mujib Medical University( BSMMU).

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Retinopathy of prematurity
Dr. Tareq rahman ,
Resident Phase B , Neonatology,
Bangabandhu Sheikh Mujib Medical University( BSMMU).

Definition
Retinopathy of prematurity (ROP), formerly known as retrolental fibroplasia because of its end-stage appearance, is a developmental vascular proliferative disorder that occurs in the retina of preterm infants with incomplete retinal vascularization.

Epidemiology
• Most studies report ROP incidences that are about 60% for babies less than 1500 g (Zin and Gole, 2013)
• The worldwide prevalence of blindness due to ROP is approximately 50,000.
• In India the incidence of ROP is between 38 and 51.9% in low-birth-weight infants.

BSMMU experience :
- 1st case was reported in 2004
- Between 2013 to 2015 , 446 babies were screened where 82 ( 19%) were diagnosed as ROP and APROP 6% .

Embryology of retinal blood vessels
• Retinal vascularization begins at 15 to 18 weeks’ gestation.
• Retinal blood vessels extend out from the optic disc and grow peripherally.
• Vascularization in the nasal retina is complete at approximately 32 – 34 weeks and temporal retina by 40 weeks.
• Insulin-like growth factor-1 (IGF-1) supports normal retinal vascular growth and interacts with VEGF under influence of hypoxic state in utero.

Pathogenesis

• Premature delivery interrupts normal vascular growth• Phase 1 : delayed retinal vascularisation (birth-31/32
weeks)• Developing retina exposed to hyperoxic environment
(ambient andsupplemental)• Reduces angiogenic factors delaying retinal
vascularisation• Phase 2 : neovascularisation• Neuroretina continues to develop causing hypoxia
with overproduction of angiogenic factors especially VEGF causes uncontrolled retinal blood vessel growth.


Risk factors for ROP• Three crucial risk factors:
– Low Birth weight specially less than 1500 gm
– Prematurity specially 32 weeks of GA
– Unrestricted oxygen supplementation
– Other risk factors:
– Anemia
– Blood transfusions
– Intra Uterine Growth Retardation (IUGR)
– Failure of increase in weight
– Respiratory Distress Syndrome (RDS)
– Fluctuations in Sa O2
– Multiple apneic episodes
– Hypercarbia, Acidosis
– Sepsis
– Intra Ventricular Hemorrhage (IVH)
– Low level of the serum IGF-I in early postnatal period
– Raised level of erythropoietin.
– Necrotising enterocolitis.
– Bronchopulmonary dysplasia
• Our baby is preterm ( 30 weeks) and low birth weight ( 1500 gm)
• He got MV , CPAP support
• He had sepsis , acidosis and h/o multiple apneicepisodes.
• Had h/o blood transfusion due to anaemia.

International Classification for Retinopathy of Prematurity (ICROP)
• 5 parameters:
- Zone (1-3)
– Stage (1-5)
– Clock hours: The extent of the developing
vasculature that is involved quantified from 1-12 clock hours.
– Plus disease (Plus disease is a primary factor in treatment decision).
– Pre-plus disease

• Aggressive posterior ROP (AP-ROP) is a severe form of ROP that rapidly causes total retinal detachment without going through the normal stages of ROP

Anterior-posterior locationZone
• Zone I is the posterior retina within 60 degrees of the optic disc
• Zone II is a concentric circle extending from Zone 1 to the nasal oraserrata
• Zone III is the remaining temporal retina

Stage 1

Stage 2
Demarcation line with elevation between vascular and avascular area

Stage 3

Stage 4


STAGE 5 : TOTAL RETINAL DETACHMENT

Stage 5
Stage 5. Total retinal detachment
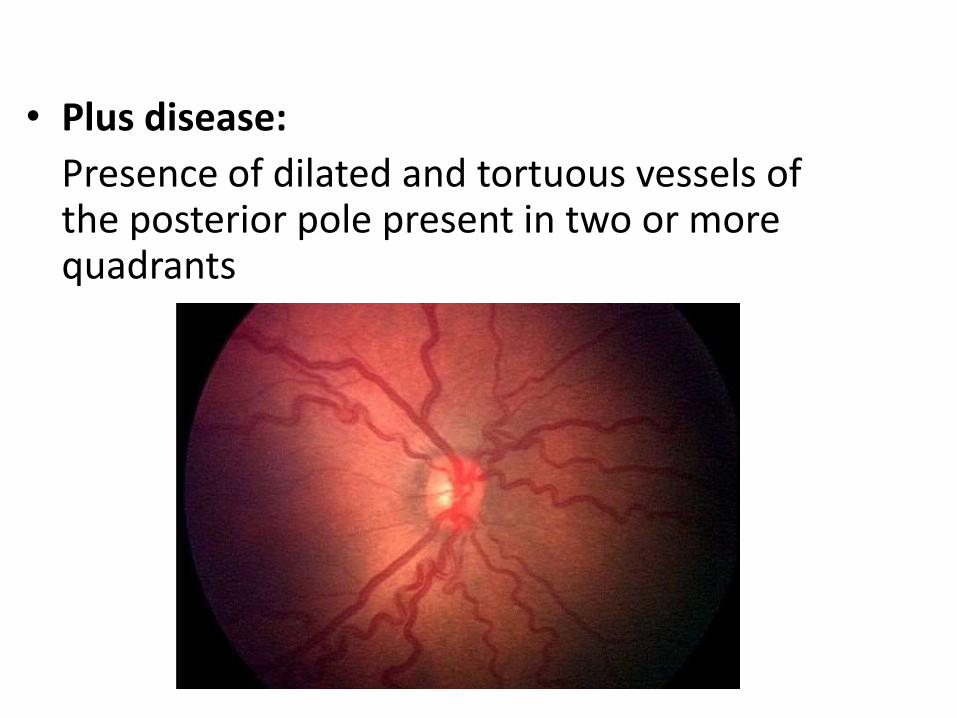
• Plus disease:
Presence of dilated and tortuous vessels of the posterior pole present in two or more quadrants

• Preplus disease:
Abnormal vascular dilation and tortuosity that is insufficient for diagnosis of plus disease present in two or more quadrants

Threshold ROP :
ROP is defined as five contiguous clock hours or eight total clock hours of stage 3 and plus disease in zone 1 or 2.

• Prethreshold ROP — Prethreshold ROP is defined as one of the following –
ROP at any stage less than threshold in zone I
Stage 2 and plus disease in zone II
Stage 3 without plus disease in zone II
Stage 3 with plus disease in zone II but with fewer clock hours of stage 3 than required to meet threshold

• High-risk prethreshold ROP includes –
Any stage ROP with plus disease in zone I
Stage 3 ROP without plus disease in zone I
Stage 2 or 3 ROP with plus disease in zone II

Long Term Complications of ROP
Retinal Dragging and Folds
Others:
Acute angle closure glaucoma
Late onset Retinal Detachment( 22%)
Significant myopia (80%)
Anisometropia
AmblyopiaStrabismus

Criteria for screening
• United States: infants with a gestational age of ≤30 weeks or birth weight of <1500 g and selected infants with a gestational age of >30 weeks and an unstable clinical course.
• United Kingdom: infants with a gestational age of ≤31 weeks or birth weight of ≤1500 g
• Canada: infants with a gestational age of ≤30 weeks, or birth weight of ≤1250 g
M. Elizabeth Hartnett et al , N Engl J Med 2012;367:2515-26.

ROP screening-current UK guideline
Which infant should be screened?
All infants born < 32 weeks of gestation or <1500g
When should the first screening examination be performed?
Gestational age at birth (weeks) Postnatal age at first ROP examination
(weeks)
23 7
24 6
25 5
26 4
27 4
28 4
29 4
30 4
31 4

ROP screening – in BSMMU
All neonates weighing <2000 g and/or with a gestation <35weeks admitted to the NICU are being routinely screened forROP.
Neonates with birth weight ≥ 2000 g or gestational age morethan 35 weeks are being screened if they have an unstableneonatal including those requiring cardiorespiratory support forprolonged period.

ROP screening – in BSMMU
At a 4 weeks of postnatal age for infants born ator more than 32 weeks of gestation or birthweight ≥1200 g and at a 3 weeks of postnatal agefor infants less than 32 weeks of gestation orbirth weight <1200 g.

Diagnosis
• Ophthalmologic examination by an expert examiner usually confirms the diagnosis.
• Binocular indirect ophthalmoscopy (BIO) is generally used.
• Newer digital camera technology demonstrated 100% sensitivity in detecting ROP requiring treatment. But it does not permit adequate assessment of retinal periphery.

Ophthalmoscopy
• Pupillary Dilation : 2.5% phenyl ephrine + 0.5% Tropicamide – 3 times , 10 mins apart 30 minsbefore exam
• Speculum
• INDIRECT ophthalmoscope
• PLUS DISEASE to be looked for before speculum and scleral depression

Treatment
• Indications for treatment - Retinal ablative therapy is indicatedfor eyes with threshold retinopathy of prematurity (ROP) andeyes with high-risk prethreshold retinopathy of prematurity(ROP) based on clinical findings.
• High-risk prethreshold ROP includes –
Zone I: any stage ROP with plus disease
Zone I: stage 3 ROP without plus disease
Zone II: stage 2 or 3 ROP with plus disease
• When treatment should start?
Once a treatment decision has been made, treatment should beperformed within 48-72 hours.

Treatment

• Treatment modalities –
Cryotherapy
Laser photocoagulation – Standard treatment
Antivascular endothelial growth factor (VEGF) monoclonal antibody (Bevacizumab)
- stage 3 and plus disease in zone I. Surgery - vitrectomy, Scleral buckling.
- Results are best when done before the fovea has detached.

Outcome of treatment
• Treatment of acute ROP generally results in normal or nearnormal anatomy of macula and posterior retina.
• Treatment fails in small proportion of cases and retinaldetachment ensues.
• Prompt vitreoretinal surgery may be needed to preservevision.
• Severe visual impairment continue to occur in some infants.
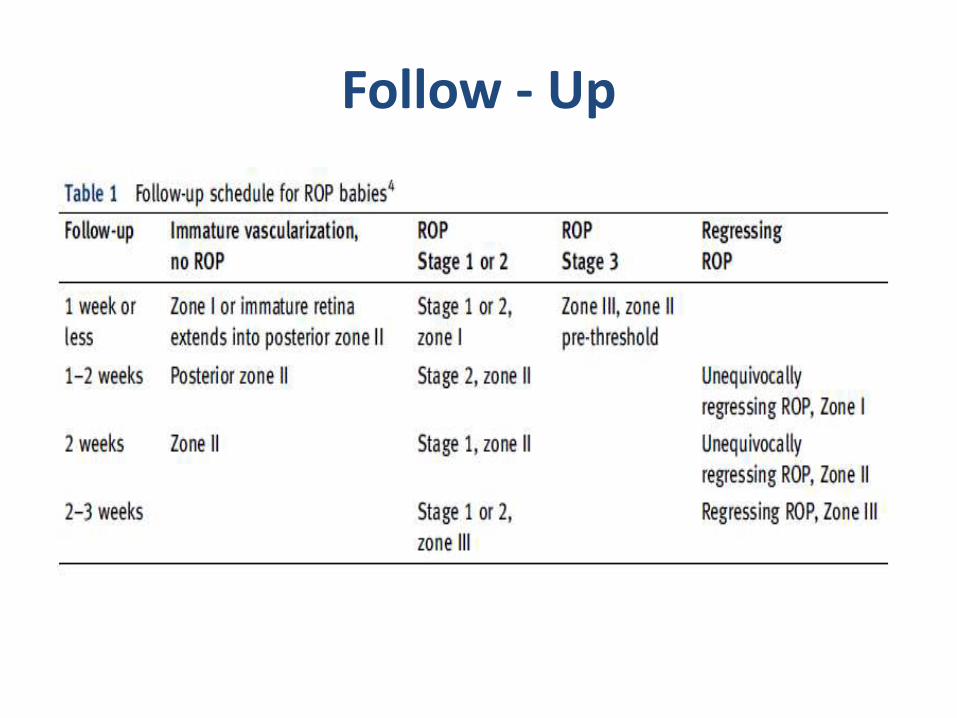
Follow - Up

Care in NICU
• Maintain SpO2 88 – 93 %
• Avoid flactuation of SpO2 while on O2 supplementation.
• Keep Hb level not less than 10 gm/dl
• Ensure adequate weight gain.

Prognosis
Spontaneous regression:
• Stage I - and stage-II: 90%.
• Stage III+ disease : 50%.

• PREVENTION - Interventions to prevent or limit the
progression of retinopathy of prematurity (ROP) have been unsuccessful, although further evaluation may be needed. Because oxidant injury contributes to ROP, antioxidant therapies, such as vitamin E, D-penicillamine, and limited exposure to light, have been tested.

Concerning matter ?
• Retinopathy of prematurity has become a leading but preventable cause of childhood blindness worldwide.(M. Elizabeth Hartnett et al, 2012)
• ROP occurs primarily in infants of low birth weight and low gestational age at birth.
• Infants with ROP having higher risk for developing certain eye problems later in life
- retinal detachment, myopia, strabismus, amblyopia, glaucoma.

Reference
• www.uptodate.com
• www.medscape.com
• American Academy of Ophthalmology

THANK YOU
Related Documents











