Respiratory System Infections Chapter 24

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Respiratory System Infections
Chapter 24
Respiratory System InfectionsEncompass enormous variety of illnesses
Trivial to fatal
Divided into infections of
Upper respiratory
Head and neck
Uncomfortable but generally not life threatening
Lower respiratory
Chest
More serious
Can be life-threatening
Particularly in the immunocompromised

Normal Flora
Nasal cavity, nasopharynx and pharynx colonized by numerous bacteria
Other sites are sterile
Numerous classes of organisms are present from aerobes to anaerobes
Conjunctiva commonly have no bacteria
Organisms that do invade are swept into the nasolacrimal duct (tear duct) and nasopharynx

Symptoms
Characterized by
Difficulty swallowing
Fever
Red throat with pus patches
Enlarged tender lymph nodes
Localized to neck
Most patients recover uneventfully in approximately a week
Streptococcal Pharyngitis

Streptococcal Pharyngitis
Causative Agent
– Streptococcus pyogenes
Gram-positive
Coccus in chains
β hemolytic
Complete hemolysis of red blood cells
Commonly referred to as group A streptococcus
Due to group A carbohydrate in cell wall
Basis for identification from other organisms

Pathogenesis due to numerous virulence factors
Streptolysin
Protein G
Complications of infection can occur during acute illness
Scarlet fever
Acute glomerulonephritis
Acute rheumatic fever
Treatment
Penicillin is antibiotic of choice
Streptococcal Pharyngitis

Common ColdSymptoms
Malaise
Scratchy mild sore throat
Runny nose
Cough and hoarsness
Nasal secretion
Initially profuse and watery
Later, thick and purulent
No fever
Unless complicated with secondary infection
Symptoms disappear in about a week

Common Cold
Causative Agent
30% to 50% caused by rhinoviruses
More than 100 serotypes of rhinoviruses
Non-enveloped
Single-stranded RNA genome

Common ColdPathogenesis
Virus attach to specific receptors on respiratory epithelial cells and multiply in cells
Large number of viruses released from infected cells
Injured cells cause inflammation which stimulates profuse nasal secretion, sneezing and tissue swelling
Infection is halted by inflammatory response, interferon release, and immune response
Infection can extend to ears, sinuses and lower respiratory tract before stopping
Treatment is supportive with OTC medications

Aka: Pertussis
Symptoms
Runny nose followed by bouts of uncontrollable coughing
Termed paroxymal coughing
Severe cough can cause rupture of small blood vessels in the eyes
Coughing spasm followed by characteristic “whoop”
Sound made by the forceful inspiration of air
Vomiting and seizure may occur
Whooping Cough

Whooping Cough
Causative Agent
– Bordetella pertussis
Small
Encapsulated
Strictly aerobic
Gram-negative
Bacillus
Does not survive long periods outside the host

Pathogenesis
Enters respiratory tract with inspired air and attaches to ciliated cells
Organism colonizes structures of the upper and lower respiratory tract
Mucus secretion increases which causes ciliary action to decrease
Cough reflex is only mechanism for clearing secretions
Whooping Cough

Whooping Cough
Video on web page

Whooping CoughPathogenesis
– B. pertussis produces numerous toxic products
Pertussis toxin - A-B toxin
B portion attaches to cell surface
A portion enters cell and inactivates regulation of cAMP
Causes increased mucus formation
Decreases phagocytic killing
Invasive adenylate cyclase
Increases production of cAMP
Increased mucus formation

Epidemiology
Spreads via infected respiratory droplets
Most infectious during runny nose period
Number of organisms decrease with onset of cough
Classically disease of infants
Milder forms are seen in older children and adults
Often overlooked a persistent cold
Fosters transmission
Whooping Cough

Whooping Cough
Prevention
Vaccine directed at protection of infants
Prevents disease in 70% of individuals
Pertussis vaccine combined with diphtheria and tetanus toxoids (DPT)
Injections given at 6 weeks, 4, 6,and 18 months, 5 years, and now recommended for 12 year olds
Treatment
Erythromycin is effective at reducing symptoms if given early

TuberculosisSymptoms
Chronic illness
Symptoms include
Slight fever with night sweats
Progressive weight loss
Chronic productive cough
Sputum often blood streaked
Causative Agent
Mycobacterium tuberculosis (and M. bovis in AIDS)
Gram-positive cell wall
Slender bacillus
Acid fast due to mycolic acid in cell wall
Slow growing
Generation time 12 hours or more
Resists most prevention methods of control

Pathogenesis
Usually contracted by inhalation of airborne organisms
Bacteria are taken up by pulmonary macrophages in the lungs
Resists destruction within phagocyte
Organism prevents the fusion of phagosome with lysosomes; allows multiplication in protected vacuole
Tuberculosis

Pathogenesis
Organisms are carried to lymph nodes
About 2 weeks post infection intense immune reaction occurs
Macrophages fuse together to make large multinucleated cell
Macrophages and lymphocytes surround large cell and form a tubercle of connective tissue
This is an effort to wall off infected tissue
Activated macrophages release into infected tissue
• Causes death of tissue resulting in formation of “cheesy” material (biofilm)
Tuberculosis
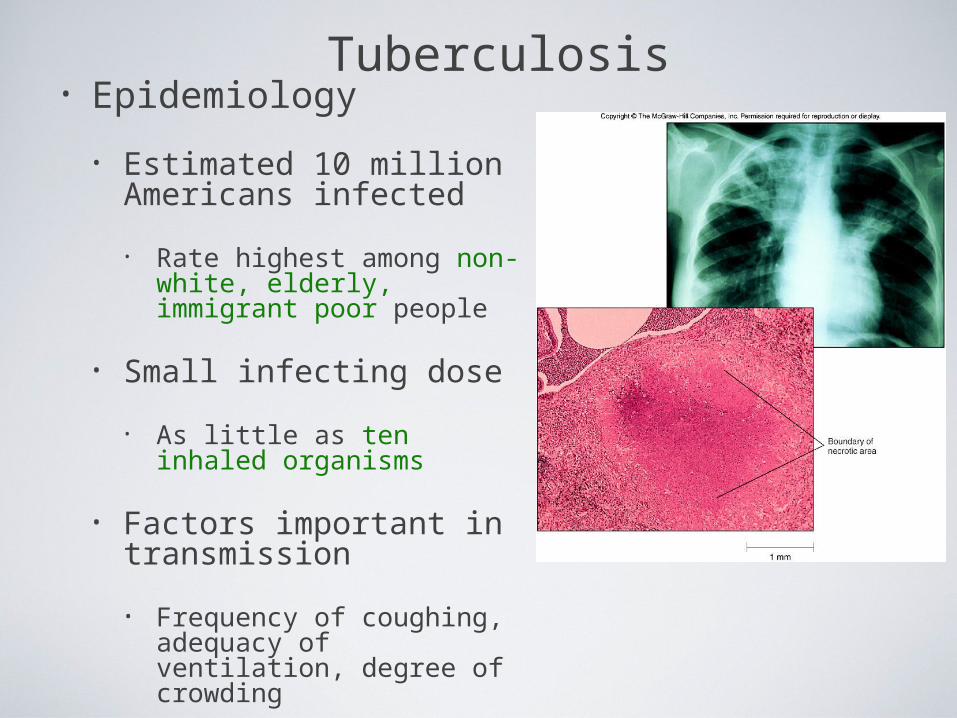
Tuberculosis• Epidemiology
• Estimated 10 million Americans infected
• Rate highest among non-white, elderly, immigrant poor people
• Small infecting dose
• As little as ten inhaled organisms
• Factors important in transmission
• Frequency of coughing, adequacy of ventilation, degree of crowding

Tuberculosis
• Epidemiology
• Tuberculin skin test used to detect those infected
• Small amount of tuberculosis antigen is injected under the skin
• Injection site becomes red and firm if infected
• Positive test does not indicate active disease

Tuberculosis• Prevention
• Vaccination for tuberculosis widely used in many parts of the world
• Vaccine known as Bacillus of Calmette and Guérin
• BCG derived from Mycobacterium bovis
• Gives weak, partial immunity against tuberculosis
• Vaccine not given in United States because it eliminates use of tuberculin test as diagnostic tool
•Treatment
Antibiotic treatment is given in cases of active tuberculosis
Two or more medications are given together to reduce potential antimicrobial resistance
Antimicrobials include Rifampin and Isoniazid (INH)
Both target actively growing organisms and metabolically inactive intracellular organisms
Therapy is pronged, lasting at least 6 months
•Multi-drug resistant strains have arisen in the U. S. and Russia that have spread to other countries

• Symptoms
• Influenza Type A
• Short incubation period
• Averaging 2 days
• Headache
• Fever
• Muscle pain
• Dry cough
• Acute symptoms abate within a week
• Cough, fatigue and generalized weakness may linger
Seasonal Influenza

• Causative Agents• Influenza A virus
• Belong to orthomyxovirus
• Single-stranded RNA genome
• Genome divided into 8 gene segments
• Spiked envelope
• H spike – hemagglutinin (subtypes H1-H16)• Aids in attachment
• Only H1, H2 and H3 viruses circulate in humans
• N spikes – neuraminidase (subtypes N1-N9)
• Cleaves H protein to allow fusion of viral and cellular membranes (i.e., entry into the cell)
• Requires cellular enzyme trypsin to facilitate infection
• Influenza B & C viruses only circulate in humans
Seasonal Influenza

Influenza A Transmission Cycle
Circulates withlimited pathology
Transmission todomestic fowl
Adaptation/reassortment
with swineinfluenza viruses
Transmissionto humans

• Pathogenesis• Acquired through inhalation of infected respiratory
secretions
• Virus attaches to host cells via hemagglutinin spikes
• Once attached viral envelope fuses with host membrane, leading to viral replication within the cell
• Mature viruses bud from host cell
• Budding allows mature virus to pick up envelope
• Infected cells die and slough off
• Host immunity quickly controls viral spread
• Anti-HA neutralizing IgG is protective
• Mortality rate is low
• However, hundreds of thousands or millions of people are infected each year in the U. S.
• On average, about 30,000 Americans, mostly elderly and very young children, die from influenza each year
Seasonal Influenza

• Epidemiology• Outbreaks occur in United States every year
• Vaccines are formulated months in advance using prominent circulating strains
• 2010-2011 vaccine strains
• A/California/7/2009 (H1N1)-like (the same strain as was used for 2009 H1N1 monovalent vaccines)
• A/Perth/16/2009 (H3N2)-like
• B/Brisbane/60/2008-like
• Pandemics occur periodically• Most famous pandemic of 1918 (Spanish flu)
• Spanned the globe in 9 months
• Pandemics have higher than normal morbidity
Seasonal Influenza
Type / Geographic origin / Strain/ Year isolated (H & N genes)

• Epidemiology
• Spread caused by major antigenic changes
• Antigenic drift
• Consists of amino acid changes in spikes (point mutations)
• Particularly hemagglutinin
• Changes minimize effectiveness of immunity to previous strains
• Ensures enough susceptible people are available for continued virus survival
•Antigenic shift
Represent more dramatic changes
Virus strains are drastically antigenically different from previous strains, importantly in the hemagglutinin
New virus comes from genetic re-assortment
Occurs when two different viruses infect a cell at the same time
Genetic mixing results in new virus that is often more virulent
Seasonal Influenza

Seasonal Influenza

• Prevention and Treatment
• Vaccine can be 80% to 90% effective
• New vaccine required every year
• Due to antigenic drift
• Antiviral medications are 70% to 90% effective
• Include amantadine, rimantadine, and Tamiflu
• Must be taken early
• Not a substitute for vaccine
Seasonal Influenza

• There are hundreds, if not thousands, of influenza A viruses circulating in nature
• Seasonal influenza occurs from mammalian viruses
• Pigs in SE Asia are frequently a source of these viruses
• New reassortants arise every year, but most are not pathogenic to humans
• Avian influenza viruses routinely circulate among wild birds
• Some species can be infected without conspicuous pathology
• These species often carry the viruses along migratory routes, exposing other birds
Avian Influenza

• Most avian influenza viruses are highly inefficient at infecting humans
• However, some cultures have domestic birds and pigs in close periodomestic proximity
• This practice increases the chance of
• Reassortment with mammalian influenza viruses
• 1957, 1967 pandemic strains were reasortant mammalian viruses with avian segments (antigenic shift)
• Emergence of mutant avian strains that can infect humans
• 1918 pandemic strain was an avian virus that adapted to efficient human to human transmission (antigenic drift)
Avian Influenza

• Rescue of the 1918 pandemic strain
• Virology did not exist in 1918
• The virus could not be isolated, thus went extinct when the pandemic ended
• In 2005 a group resurrected the 1918 strain from bodies buried in Alaskan permafrost
• Viral genome sequencing indicated it was an avian influenza A virus
• It was also infectious...
Avian Influenza

Avian InfluenzaLungs from Mice Infected with Rescued 1918 H1N1 Pandemic Virus
1918 Strain 1918 Strain
1918 Strain
1918 Strain(HN)/Texa
s 1991 Strain hybrid
1918 Strain with
Texas 1991 Hsegment
Texas 1991 strain
(control)
Tumpey et al., 310:77.
2005

Avian InfluenzaFeature SI1 H5N1 AI2 1918 H1N13
Transmission efficiency High Very low/none High
Replication siteUpper and lower respiratory tract
Lower RT onlyLikely upper &
lower RT
Viral CPE4 Limited Substantial Substantial
Immunopathology Limited Substantial Substantial
Kills embyronated chicken eggs?
No Yes Yes
Requires trypsin for infection of cell cultures?
Yes No No
Vaccine Yes No N/A
Fatality rate 0.03% (U.S.) 57% (global)About 1-2%
(U.S)
DemographicYoung children,
elderlyYoung adults Young adults
1 Seasonal influenza2 Currently circulating H5N1 avian influenza virus3 Rescued 1918 pandemic H1N1 avian influenza virus4 Cytopathic effect (damage directly caused by the virus)
Red - more pathogenic featureGreen - less pathogenic feature
Hantavirus (Cardio)Pulmonary Syndrome• Symptoms
• Early symptoms
• Fever
• Muscle ache
• Especially in the lower back
• Nausea and vomiting
• Diarrhea
• Later symptoms• Unproductive cough
• Increasing shortness of breath
• Capillary leak syndrome in lungs
• Shock and death
•Causative Agents
HantavirusesIncludes Sin Nombre virus found in initial outbreak
Belong to bunyavirus family
Single-stranded RNA genome
Divided into 3 segments
Enveloped
Causes apathogenic, lifetime infection in rodent hosts
Death in humans is caused by cardiac failure from severe hypotension

• Pathogenesis
• Enters body via inhalation of dust contaminated with urine, feces and saliva of infected rodents
• Viremia
• Mechanism unknown
• Carried throughout body
• Infects capillary endothelial cells
• Inflammation causes capillaries to leak fluid into lungs
• Causes hypoxia and hypotension
• Cardiac shock and death occurs in over 36% of patients
Hantavirus Pulmonary Syndrome

• Hantavirus disease is a T cell cytokine-mediated immunopathology
• TNF
• IFNγ
• Interleukin-1
• Interleukin-2
• Lymphotoxin
Hantavirus Pulmonary Syndrome
•Immune cell infiltrates•No viral damage to the lung epithelium
Normal Hantavirus Infection
Proinflammatorycytokines

• Epidemiology
• Emerging disease due to recent discovery
• Most cases in United States occur west of Mississippi River
• Principally caused by Sin Nombre virus
• Deer mice (Peromyscus maniculatus) are the reservoir
• Outbreaks causality with increase rodent populations
• Many, if not all, infected deer mice become persistently infected
• Person-to-person transmission does not occur
• Notable exception: Andes hantavirus in South America (Argentina, Chile)
Hantavirus Pulmonary Syndrome

• Prevention and Treatment
• Prevention is directed towards minimizing exposure
• Keep pet and human food in containers
• Maximal ventilation when cleaning mouse droppings
• Mop with disinfectant
• NEVER use brooms or vacuums
• Wear N-100 HEPA-filtered mask
• Lethal traps and poisons to decrease rodent population
• No effective antiviral treatment (nor would it work anyway)
• Treatment limited to supportive care
• Extracorporeal membrane oxygenation (ECMO)
Hantavirus Pulmonary Syndrome
Related Documents











