Regulation of endothelial cell permeability by platelet-derived extracellular vesicles Byron Miyazawa, BS, Alpa Trivedi, PhD, Padma Priya Togarrati, PhD, Daniel Potter, PhD, Gyulnar Baimukanova, MD, PhD, Lindsay Vivona, BS, Maximillian Lin, BS, Ernesto Lopez, MD, PhD, Rachael Callcut, MD, Amit K. Srivastava, PhD, Lucy Z. Kornblith, MD, Alexander T. Fields, PhD, Martin A. Schreiber, MD, Charles E. Wade, PhD, John B. Holcomb, MD, and Shibani Pati, MD, PhD, San Francisco, California BACKGROUND: Platelet (Plt)-derived extracellular vesicles (Plt-EVs) have hemostatic properties similar to Plts. In addition to hemostasis, Plts also function to stabilize the vasculature and maintain endothelial cell (EC) barrier integrity. We hypothesized that Plt-EVs would inhibit vascular EC permeability, similar to fresh Plts. To investigate this hypothesis, we used in vitro and in vivo models of vascular endothelial compromise and bleeding. METHODS: In the vitro model, Plt-EVs were isolated by ultracentrifugation and characterized for Plt markers and particle size distribution. Effects of Plts and Plt-EVs on endothelial barrier function were assessed by transendothelial electrical resistance measurements and histological analysis of endo- thelial junction proteins. Hemostatic potential of Plt-EVs and Plts was assessed by multiple electrode Plt aggregometry. Using an in vivo model, the effects of Plts and Plt-EVs on vascular permeability and bleeding were assessed in non-obese diabetic-severe combined immunodeficient (NOD-SCID) mice by an established Miles assay of vascular permeability and a tail snip bleeding assay. RESULTS: In the in vitro model, Plt-EVs displayed exosomal size distribution and expressed Plt-specific surface markers. Platelets and Plt-EVs decreased EC permeability and restored EC junctions after thrombin challenge. Multiplate aggregometry revealed that Plt-EVs en- hanced thrombin receptor–activating peptide-mediated aggregation of whole blood, whereas Plts enhanced thrombin receptor–activat- ing peptide–, arachidonic acid–, collagen-, and adenosine diphosphate–mediated aggregation. In the in vivo model, Plt-EVs are equivalent to Plts in attenuating vascular endothelial growth factor (VEGF)-A–induced vascular permeability and uncontrolled blood loss in a tail snip hemorrhage model. CONCLUSION: Our study is the first to report that Plt-EVs might provide a feasible product for transfusion in trauma patients to attenuate bleeding, inhibit vascular permeability, and mitigate the endotheliopathy of trauma. (J Trauma Acute Care Surg. 2019;86: 931–942. Copyright © 2019 American Association for the Surgery of Trauma.) KEY WORDS: Vascular instability; trauma; barrier disruption; hemostasis. T raumatic injury is the leading cause of death worldwide in individuals between the ages of 1 and 44 years. 1–5 Hemor- rhage is responsible for the majority of preventable trauma- related deaths, 80% in the military, and 40% under the age of 65 years in the civilian population. 3–6 Goals for resuscitation and blood product transfusion in bleeding patients have been defined by landmark retrospective and prospective studies in which balanced ratios of blood products in a 1:1:1 ratio of red blood cells-plasma-platelets (Plts) are shown to improve survival and outcomes. 6,7 Findings from the Pragmatic, Randomized Op- timal Platelet and Plasma Ratios (PROPPR) trial also revealed that early Plt administration is associated with improved hemosta- sis and reduced mortality in severely injured bleeding patients. 8 Logistically, in austere settings or settings that require prolonged field care of bleeding patients, there are challenges in obtaining, storing, and administering blood products. Platelets in particular generate a greater logistical challenge than red blood cells and plasma since current blood banking practice in the United States allows Plts to be stored for a total of only 5 day at 22°C, which leads to increased risk of infections, decreased or wasted inven- tory of Plts, and a demonstrable storage lesion or decline in function of the Plts with storage at 22°C. 9–11 There are currently a number of preclinical and clinical endeavors to evaluate alternative Plt-derived hemostatic agents such as cold-stored Plts and freeze-dried Plts. 12,13 Platelet-derived hemostatic products can circumvent some of the logistical and practical challenges of Plt transfusion and with fewer infectious risks associated with standard apheresis or whole blood–derived Plt units. 14 Platelet-derived extracellular vesicles (EVs) are parti- cles secreted from Plts that express surface receptors and contain From the Department of Laboratory Medicine (B.M., A.T., D.P., L.V., M.L., S.P.), Uni- versity of California; Blood Systems Research Institute (P.P.T., G.B.), San Francisco, California; Department of Surgery (EL., C.E.W.), University of Texas Health Science Center at Houston; Department of Pediatric Surgery (A.K.S., J.B.H.), McGovern Medical School, University of Texas Health Science Center at Houston, Houston, Texas; Department of Surgery (R.C., L.Z.K., A.T.F.), Uni- versity of California San Francisco, San Francisco, California; Department of Surgery (M.A.S.), Oregon Health Science and University, Portland, Oregon. This study was presented at 77th Annual Meeting of AAST, 4th World Trauma Con- gress, September 28, 2018, in San Diego, California. Address for reprints: Shibani Pati, MD, PhD, Department of Laboratory Medicine, University of California, San Francisco, 513 Parnassus Ave, HSE 715, San Francisco, CA 94143; email: [email protected]. Supplemental digital content is available for this article. Direct URL citations appear in the printed text, and links to the digital files are provided in the HTML text of this article on the journal’s Web site (www.jtrauma.com). DOI: 10.1097/TA.0000000000002230 AAST 2018 PODIUM P APER J Trauma Acute Care Surg Volume 86, Number 6 931 Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

AAST 2018 PODIUM PAPER
Regulation of endothelial cell permeability byplatelet-derived extracellular vesicles
Byron Miyazawa, BS, Alpa Trivedi, PhD, Padma Priya Togarrati, PhD, Daniel Potter, PhD,Gyulnar Baimukanova, MD, PhD, Lindsay Vivona, BS, Maximillian Lin, BS, Ernesto Lopez, MD, PhD,Rachael Callcut, MD, Amit K. Srivastava, PhD, Lucy Z. Kornblith, MD, Alexander T. Fields, PhD,
Martin A. Schreiber, MD, Charles E. Wade, PhD, John B. Holcomb, MD,and Shibani Pati, MD, PhD, San Francisco, California
Fro
Thi
Ad
Sup
DO
J TrVol
BACKGROUND: P
m the Department of Lversity of CaliforniaFrancisco, California;Health Science CenteJ.B.H.), McGovern Mat Houston, Houston,versity of CaliforniaSurgery (M.A.S.), Ors study was presentedgress, September 28, 2dress for reprints: ShibUniversity of CaliforFrancisco, CA 94143;plemental digital contethe printed text, and linarticle on the journal’s
I: 10.1097/TA.000000
auma Acute Care Suume 86, Number 6
latelet (Plt)-derived extracellular vesicles (Plt-EVs) have hemostatic properties similar to Plts. In addition to hemostasis, Plts also functionto stabilize the vasculature and maintain endothelial cell (EC) barrier integrity. We hypothesized that Plt-EVs would inhibit vascular ECpermeability, similar to fresh Plts. To investigate this hypothesis, we used in vitro and in vivo models of vascular endothelial compromiseand bleeding.
METHODS: I
n the vitro model, Plt-EVswere isolated by ultracentrifugation and characterized for Plt markers and particle size distribution. Effects of Plts andPlt-EVs on endothelial barrier function were assessed by transendothelial electrical resistance measurements and histological analysis of endo-thelial junction proteins. Hemostatic potential of Plt-EVs and Plts was assessed by multiple electrode Plt aggregometry. Using an in vivo model,the effects of Plts and Plt-EVs on vascular permeability and bleeding were assessed in non-obese diabetic-severe combined immunodeficient(NOD-SCID) mice by an established Miles assay of vascular permeability and a tail snip bleeding assay.RESULTS: I
n the in vitro model, Plt-EVs displayed exosomal size distribution and expressed Plt-specific surface markers. Platelets and Plt-EVsdecreased EC permeability and restored EC junctions after thrombin challenge. Multiplate aggregometry revealed that Plt-EVs en-hanced thrombin receptor–activating peptide-mediated aggregation of whole blood, whereas Plts enhanced thrombin receptor–activat-ing peptide–, arachidonic acid–, collagen-, and adenosine diphosphate–mediated aggregation. In the in vivo model, Plt-EVs are equivalentto Plts in attenuating vascular endothelial growth factor (VEGF)-A–induced vascular permeability and uncontrolled blood loss in a tail sniphemorrhage model.CONCLUSION: O
ur study is the first to report that Plt-EVs might provide a feasible product for transfusion in trauma patients to attenuate bleeding, inhibitvascular permeability, and mitigate the endotheliopathy of trauma. (J Trauma Acute Care Surg. 2019;86: 931–942. Copyright © 2019American Association for the Surgery of Trauma.)KEYWORDS: V
ascular instability; trauma; barrier disruption; hemostasis.T raumatic injury is the leading cause of death worldwide inindividuals between the ages of 1 and 44 years.1–5 Hemor-
rhage is responsible for the majority of preventable trauma-related deaths, 80% in the military, and 40% under the age of65 years in the civilian population.3–6 Goals for resuscitationand blood product transfusion in bleeding patients have beendefined by landmark retrospective and prospective studies in
aboratory Medicine (B.M., A.T., D.P., L.V., M.L., S.P.), Uni-; Blood Systems Research Institute (P.P.T., G.B.), SanDepartment of Surgery (EL., C.E.W.), University of Texasr at Houston; Department of Pediatric Surgery (A.K.S.,edical School, University of Texas Health Science CenterTexas; Department of Surgery (R.C., L.Z.K., A.T.F.), Uni-San Francisco, San Francisco, California; Department ofegon Health Science and University, Portland, Oregon.at 77th Annual Meeting of AAST, 4th World Trauma Con-018, in San Diego, California.ani Pati, MD, PhD, Department of Laboratory Medicine,nia, San Francisco, 513 Parnassus Ave, HSE 715, Sanemail: [email protected] is available for this article. Direct URL citations appear inks to the digital files are provided in the HTML text of thisWeb site (www.jtrauma.com).
0000002230
rg
Copyright © 2019 Wolters Kluwer H
which balanced ratios of blood products in a 1:1:1 ratio of redblood cells-plasma-platelets (Plts) are shown to improve survivaland outcomes.6,7 Findings from the Pragmatic, Randomized Op-timal Platelet and Plasma Ratios (PROPPR) trial also revealedthat early Plt administration is associated with improved hemosta-sis and reduced mortality in severely injured bleeding patients.8
Logistically, in austere settings or settings that require prolongedfield care of bleeding patients, there are challenges in obtaining,storing, and administering blood products. Platelets in particulargenerate a greater logistical challenge than red blood cells andplasma since current blood banking practice in the United Statesallows Plts to be stored for a total of only 5 day at 22°C, whichleads to increased risk of infections, decreased or wasted inven-tory of Plts, and a demonstrable storage lesion or decline infunction of the Plts with storage at 22°C.9–11
There are currently a number of preclinical and clinicalendeavors to evaluate alternative Plt-derived hemostatic agentssuch as cold-stored Plts and freeze-dried Plts.12,13 Platelet-derivedhemostatic products can circumvent some of the logistical andpractical challenges of Plt transfusion and with fewer infectiousrisks associated with standard apheresis or whole blood–derivedPlt units.14 Platelet-derived extracellular vesicles (EVs) are parti-cles secreted from Plts that express surface receptors and contain
931
ealth, Inc. All rights reserved.

Miyazawa et al.J Trauma Acute Care Surg
Volume 86, Number 6
multiple types of RNA, proteins, lipids, and DNA. Extracellularvesicles range in size from 10 nm to 1,000 nm in diameter.Extracellular vesicles in the range of 50 mm to 100 nm in sizeare nanoparticles called exosomes, and particles in the size rangeof 100 nm to 1,000 nm are called microvesicles (MVs).15–22
Extracellular vesicles mediate cell-cell communication bytransferring their cargo from one cell to another.18,23 Extracellu-lar vesicles can bind and fuse with the plasma membrane of thetarget cell, or alternatively, are engulfed by the target cell,through which they can alter the biological function of the re-cipient cell.18 These nanometer sized particles are shown tocirculate systemically in the blood, in both health and disease,and are derived from a number of cellular sources includingmonocytes, macrophages, endothelial cells (ECs), and neutro-phils.19,23,24 Over the past decade, the role and biological func-tions of EVs have been the focus of scientific research inmultiples fields, with demonstrated diagnostic and therapeuticpotential of EVs, in cancer, hemostasis, autoimmune disease, andangiogenesis.19 Platelet-derived EVs are procoagulant and canenhance induced hemostasis through EV surface receptors,which include GPIIb/IIIa, tissue factor, and phosphatidylserine.16
Phosphatidylserine can activate coagulation factors II and X,hence triggering the coagulation cascade.25 Aside from surfacereceptors, there are only a few studies that have aimed to charac-terize the proteomic content of Plt-EVs. These reports have dem-onstrated that, regardless of the methods of stimulation of thePlts, there are a number of proteins packaged consistently withinthe EVs, including thrombospondin-1, fibrinogen, integrin IIb,and platelet factor 4, to name a few.26–28
We have previously demonstrated the ability of standardapheresis Plts to attenuate vascular endothelial permeability inboth in vitro and in vivo models in mice.29,30 In this article,we sought to determine if Plt-EVs could mediate hemostasissimilar to apheresis Plts and also modulate vascular endothelialprotection in our defined murine model of endothelial barrierdysfunction and permeability. We hypothesized that Plt-EVswould have similar therapeutic potential to Plts in vitro and invivo and may provide an alternative hemostatic and vasculo-protective option to bleeding patients when access to Plts orblood products are limited.
MATERIALS AND METHODS
Isolation of Plt-EVs From Apheresis PltsLeukoreduced apheresis Plts stored in plasma were ob-
tained from Bonfils Blood Bank, Denver, Colorado. All Pltswere tested for bacterial infection by the blood bank (BloodCenters of the Pacific) and found to be negative. To generateEVs from Plts, we first stored the Plts at 22°C for 3 days withgentle rocking. The Plts were spun at 1,000g for 30 minutes toobtain a cell-free supernatant. This supernatant was subse-quently spun at 13,000g at 4°C for 15 minutes, from whichthe resulting supernatant was collected, and spun at 100,000g(Beckman Coulter Optima LE-80 K ultracentrifuge and aSW-28 T rotor) at 4°C for 1 hour. The resulting pellet was resus-pended in a small volume of phosphate buffered saline (PBS)(approximately 200 μL), and the amount of protein was quantifiedon NanoDrop 2000 (Thermo Scientific, Waltham, MA) and thensubsequently aliquoted and stored at −80°C.
932
Copyright © 2019 Wolters Kluwer H
Flow Cytometry Characterization of EVsExtracellular vesicles collected from apheresis platelets
were characterized for the expression of Plt-specific markerssuch as CD31, CD41, and CD63 using fluorescently conjugatedantibodies (BioLegend, San Diego, CA). Extracellular vesicleswere further tested for the expression of tetraspanin markersusing CD9 and CD81 antibodies (BioLegend, San Diego, CA).
Before staining the EVs, antibodies were filtered using theUltrafree-MC/Durapore-PVDF centrifugal filter tubes (Millipore,Hayward, CA). After 30 minutes of staining at 4°C, EVs werespun in the Ultrafree-MC/Durapore-PVDF centrifugal filtertubes. Extracellular vesicles were collected by flushing the filtermembrane with 200 μL of PBS. Samples were analyzed by run-ning on an LSR II benchtop flow cytometer (BD Biosciences,San Jose, CA). For the size determination of EVs, 0.16, 0.2,0.24, and 0.5 μm Biocytex Megamix Plus-SSC reference beadswere used (Thermo Fisher Scientific, Waltham, MA). Data wereanalyzed using FlowJo software (Tree Star, Inc., Ashland, OR),as described previously.21
Characterization of Plt-EVs by NanoSightParticle size distribution of Plt-EVs was determined by
nanoparticle tracking analysis using a NanoSight NS300 system(Malvern Panalytical, Westborough, MA) as previously de-scribed.22 Samples were diluted 1:400 in particle-free PBS ac-cording to the manufacturer's recommendations. Data wereanalyzed using NTA 3.2 Dev Build 3.2.16 software (MalvernPanalytical, Westborough, MA).
Effects of Plt-EVs on EC PermeabilityHuman pulmonary microvascular endothelial cells (PECs)
were obtained from Promocell (Germany) and maintained usingGrowth Medium MVS (Promocell, Germany). The integrity ofPEC monolayers was measured using an electric cell-substrateimpedance sensing system (ECIS 1600, Applied BioPhysics,Troy, NY). An increase or decline in transendothelial electricalresistance across the cell monolayers indicated accordingly de-creased or increased endothelial paracellular permeability. Pulmo-nary microvascular endothelial cells were grown to confluenceon L-cysteine reduced, 96-well plates containing electrodes ineach well. Cells were treated with Plts (10 � 106/mL, 25 �106/mL, and 50 � 10/mL) or Plt-EVs (15 μg/mL, 30 μg/mL,and 60 μg/mL) and challenged after 30 minutes with Thrombin(Sigma, St. Louis, MO) at a concentration of 0.2 U/mL. Mono-layer resistance at 4/16/64 kHz was analyzed in 8-minute inter-vals. Data were normalized to the mean resistance of cellmonolayers before the treatments.
Effect of Plt-EVs on Cytoskeletal, Tight, andAdherens Junction Protein Expression on PECs
Pulmonary microvascular endothelial cells were grown toconfluence on collagen-coated cover slips before treatment.Platelets (50 � 106/mL) or Plt-EVs (30 μg/mL) were added tothe PEC monolayer for 30 minutes, followed by a 0.2 U/mL ofthrombin challenge for 5 minutes at 37°C. Cells were then fixedwith 4% paraformaldehyde and stained with antibodies againstVE-cadherin (Cell Signaling), zonula occludens-1 (ZO-1)(Invitrogen), and phalloidin (Cell Signaling) and then imaged
© 2019 American Association for the Surgery of Trauma.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 6 Miyazawa et al.
at 20 times magnification using the Revolve microscopy system(Echo) or Nikon Eclipse 80i microscope with RT-scmos camera.
To quantify junctional proteins, five nonoverlapping im-ages per treatment conditionwere captured at same exposure set-tings at 20 times magnification on Nikon Eclipse 80i microscopewith RT-scmos camera. Images were exported into MetaMorphsoftware (Molecular Devices, Inc.) and thresholded at similarsettings between all images and treatment groups. The numberof DAPI-positive nuclei was manually counted, and integratedintensity measurements of junctional proteins and F-actin thatincluded both cytoplasmic and membrane bound expressionwere measured using Measure Colocalization module. On anaverage, 70 cells were counted per image.
Multiple Electrode Plt Aggregometry of Plt-EVsBlood samples were obtained from healthy volunteers as
approved by the University of California Committee on HumanResearch as part of longitudinal study examining perturbationsin coagulation and inflammation after trauma (IRB number10-04417). Standard laboratory vacuum-sealed tubes containing3.2% (0.109 M) sodium citrate were used for all draws. Usingmultiple electrolyte Plt aggregometry (Multiplate) (Roche, Basel,Switzerland), we examined Plt aggregation of whole bloodtreated with EVs, in response to stimulation by the agonistsadenosine diphosphate (ADP), collagen, thrombin receptor–activating peptide-6 (TRAP-6), and arachidonic acid (ASPI).Briefly, 0.3 mL of whole blood was diluted in warmed normalsaline containing 3 mM of CaCl2 and incubated for 3 minutesat 37°C with continuous stirring in a Multiplate test cell. Eachtest cell contains two sets of 3 mm silver-coated copper wires,across which electrical resistance is measured at 0.57-secondintervals. Platelet activation was induced by ADP (final concen-tration, 6.5 μM; via P2 receptors), TRAP-6 (final concentration,32 μM; via PAR receptors), ASPI (final concentration, 0.5 mM;via the cyclooxygenase pathway), and collagen (final concentra-tion, 3.2 μg/mL; via GpIa/IIa and GpVI receptors). Platelet ad-hesion to the electrodes was detected as increasing electricalimpedance, measured by duplicate sets of sensor wires in eachtest cell. Whole blood samples were treated with apheresis Pltsor EVs for 5 minutes before agonist stimulation, and theresulting aggregation units were normalized to untreated wholeblood samples.
Tail Snip Bleeding Model in MiceAll animal protocols were performed with approval of
the Institutional Animal Care and use Committee at PMI Pre-clinical (San Carlos, CA). The tail snip bleeding model was per-formed in 8- to 10-week-old NOD.Cg-Prkdcscid Il2rgtm1Wjl/SzJ(NSG) mice (Jackson Laboratories, Sacramento, CA). Isoflurane-anesthetized mice were injected with vehicle (PBS), Plts (3 �108), Plt-EVs (35 μg), or fresh frozen plasma (FFP) (200 μL),through the tail vein. After 30 minutes, the distal portion ofthe tails (~5 mm segment) were amputated and immediately im-mersed in 10 mL of 37°C PBS. Once bleeding ceased, theresulting blood samples were centrifuged at 500g for 10 minutesto collect a pellet. The pellet was then resuspended in 300 μL ofred blood lysis buffer (Sigma, St. Louis, MO) and incubated at22°C for 10 minutes. To quantify blood loss, the absorbance
© 2019 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer H
of the samplewasmeasured using the SoftMax Pro 5MicroplateReader at 550 nm.
Miles Assay in MiceThe modified Miles assay (Miles AA, 1952) was per-
formed in 8- to 10-week old NSG mice (Jackson Laboratories,Sacramento, CA). Isoflurane-anesthetized mice were injectedwith vehicle (PBS), Plts (2 � 108) Plt-EVs (35 μg), or FFP(200 μL) via their tail veins. To stimulate permeability, 50 μLof vascular endothelial growth factor (VEGF)-A (2 ng/μL) andan equal volume of PBS were administered 30 minutes later in-tradermally to opposite sides of the dorsal skin. One hundredmi-croliters of a 0.5% Evans blue dye (Sigma, St. Louis, MO) wasadministered in the retro-orbital sinus. After 2 hours posttreat-ment, mice were photographed (�200, 1 NIKKOR, Nikon, Melville,NY) and euthanized. Barrier permeability was analyzed by re-moving the stimulated area via biopsy punch and extractingthe Evans blue dye with formamide at 37°C for 48 hours, andthe amount of leakage was quantitated by measuring absorbanceat 620 nm on a SoftMax Pro 5 Microplate Reader.
Statistical AnalysisMeasures of transendothelial electrical resistance (TEER),
junctional protein expression, vascular permeability, and bloodloss were analyzed by one-way analysis of variance (ANOVA),followed by Tukey's post hoc tests (GraphPad Prism 7 software,GraphPad Software, La Jolla, CA). Impedance aggregometryunderwent multiple group comparisons that were analyzed bytwo-way ANOVA and Tukey's multiple comparisons post hoctest to perform between group comparisons. Differences be-tween groups were considered significant with p ≤ 0.05.
RESULTS
EVs Express Intrinsic Plt-Specific and EV-SpecificCell Surface Markers
Extracellular vesicles were isolated from the stored Pltsusing differential ultracentrifugation procedure as described pre-viously.31 This method can result in isolation of EVs from neu-trophils, macrophages, or ECs. To confirm that the EVs arepredominantly of Plt origin, they were analyzed for the Plt-and EV-specific cell surface marker expression (Fig. 1). Fluores-cently labeled Megamix beads containing a mixture of variousreference size beads (Figs. S1 (1) and (2), http://links.lww.com/TA/B301) were used to determine the relative particle sizeof Plt-EVs (Fig. S1 (3), http://links.lww.com/TA/B301). It wasobserved that the Plt-EVs expressed high levels of Plt-specificmarkers such as CD31 (45%) and CD41 (58%) (Fig. 1A (1)).Expression of tetraspanin protein CD63, also known as the lyso-some-associated membrane protein-3 (lamp3), has been re-ported to be present on the activated Plts as well as Plt-derivedexosomes.32,33 Our results also revealed that CD63 was highlyexpressed (66%) on the Plt-EVs (Fig. 1A (1)). The representativeisotype controls have been shown in Figure 1A (2). In addition,other tetraspanin proteins, such as CD9 and CD81, that are knownto be present on exosomes, were also found to be expressed onPlt-EVs34 (Fig. 1B).
The NanoSight system was used to determine the particlesize distribution of the isolate. This assay revealed the mean
933
ealth, Inc. All rights reserved.
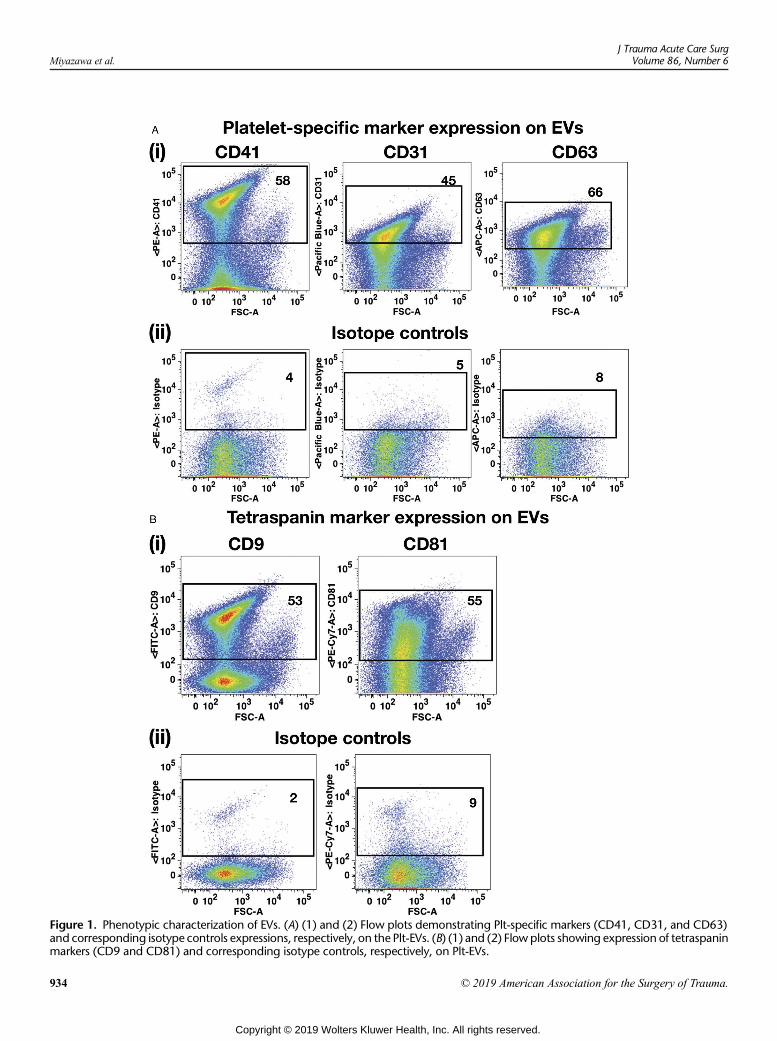
Figure 1. Phenotypic characterization of EVs. (A) (1) and (2) Flow plots demonstrating Plt-specific markers (CD41, CD31, and CD63)and corresponding isotype controls expressions, respectively, on the Plt-EVs. (B) (1) and (2) Flow plots showing expression of tetraspaninmarkers (CD9 and CD81) and corresponding isotype controls, respectively, on Plt-EVs.
Miyazawa et al.J Trauma Acute Care Surg
Volume 86, Number 6
934 © 2019 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
J Trauma Acute Care SurgVolume 86, Number 6 Miyazawa et al.
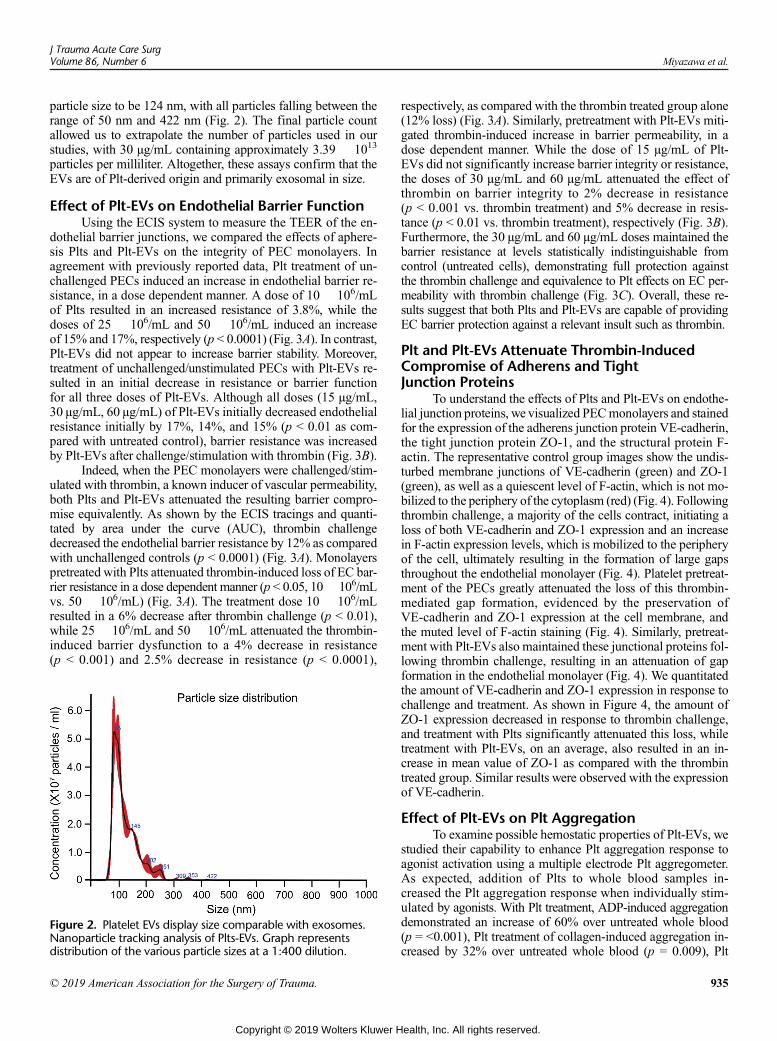
particle size to be 124 nm, with all particles falling between therange of 50 nm and 422 nm (Fig. 2). The final particle countallowed us to extrapolate the number of particles used in ourstudies, with 30 μg/mL containing approximately 3.39 � 1013
particles per milliliter. Altogether, these assays confirm that theEVs are of Plt-derived origin and primarily exosomal in size.
Effect of Plt-EVs on Endothelial Barrier FunctionUsing the ECIS system to measure the TEER of the en-
dothelial barrier junctions, we compared the effects of aphere-sis Plts and Plt-EVs on the integrity of PEC monolayers. Inagreement with previously reported data, Plt treatment of un-challenged PECs induced an increase in endothelial barrier re-sistance, in a dose dependent manner. A dose of 10 � 106/mLof Plts resulted in an increased resistance of 3.8%, while thedoses of 25 � 106/mL and 50 � 106/mL induced an increaseof 15% and 17%, respectively (p < 0.0001) (Fig. 3A). In contrast,Plt-EVs did not appear to increase barrier stability. Moreover,treatment of unchallenged/unstimulated PECs with Plt-EVs re-sulted in an initial decrease in resistance or barrier functionfor all three doses of Plt-EVs. Although all doses (15 μg/mL,30 μg/mL, 60 μg/mL) of Plt-EVs initially decreased endothelialresistance initially by 17%, 14%, and 15% (p < 0.01 as com-pared with untreated control), barrier resistance was increasedby Plt-EVs after challenge/stimulation with thrombin (Fig. 3B).
Indeed, when the PEC monolayers were challenged/stim-ulated with thrombin, a known inducer of vascular permeability,both Plts and Plt-EVs attenuated the resulting barrier compro-mise equivalently. As shown by the ECIS tracings and quanti-tated by area under the curve (AUC), thrombin challengedecreased the endothelial barrier resistance by 12% as comparedwith unchallenged controls (p < 0.0001) (Fig. 3A). Monolayerspretreated with Plts attenuated thrombin-induced loss of EC bar-rier resistance in a dose dependent manner (p < 0.05, 10� 106/mLvs. 50 � 106/mL) (Fig. 3A). The treatment dose 10 � 106/mLresulted in a 6% decrease after thrombin challenge (p < 0.01),while 25 � 106/mL and 50 � 106/mL attenuated the thrombin-induced barrier dysfunction to a 4% decrease in resistance(p < 0.001) and 2.5% decrease in resistance (p < 0.0001),
Figure 2. Platelet EVs display size comparable with exosomes.Nanoparticle tracking analysis of Plts-EVs. Graph representsdistribution of the various particle sizes at a 1:400 dilution.
© 2019 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer H
respectively, as compared with the thrombin treated group alone(12% loss) (Fig. 3A). Similarly, pretreatment with Plt-EVs miti-gated thrombin-induced increase in barrier permeability, in adose dependent manner. While the dose of 15 μg/mL of Plt-EVs did not significantly increase barrier integrity or resistance,the doses of 30 μg/mL and 60 μg/mL attenuated the effect ofthrombin on barrier integrity to 2% decrease in resistance(p < 0.001 vs. thrombin treatment) and 5% decrease in resis-tance (p < 0.01 vs. thrombin treatment), respectively (Fig. 3B).Furthermore, the 30 μg/mL and 60 μg/mL doses maintained thebarrier resistance at levels statistically indistinguishable fromcontrol (untreated cells), demonstrating full protection againstthe thrombin challenge and equivalence to Plt effects on EC per-meability with thrombin challenge (Fig. 3C). Overall, these re-sults suggest that both Plts and Plt-EVs are capable of providingEC barrier protection against a relevant insult such as thrombin.
Plt and Plt-EVs Attenuate Thrombin-InducedCompromise of Adherens and TightJunction Proteins
To understand the effects of Plts and Plt-EVs on endothe-lial junction proteins, we visualized PECmonolayers and stainedfor the expression of the adherens junction protein VE-cadherin,the tight junction protein ZO-1, and the structural protein F-actin. The representative control group images show the undis-turbed membrane junctions of VE-cadherin (green) and ZO-1(green), as well as a quiescent level of F-actin, which is not mo-bilized to the periphery of the cytoplasm (red) (Fig. 4). Followingthrombin challenge, a majority of the cells contract, initiating aloss of both VE-cadherin and ZO-1 expression and an increasein F-actin expression levels, which is mobilized to the peripheryof the cell, ultimately resulting in the formation of large gapsthroughout the endothelial monolayer (Fig. 4). Platelet pretreat-ment of the PECs greatly attenuated the loss of this thrombin-mediated gap formation, evidenced by the preservation ofVE-cadherin and ZO-1 expression at the cell membrane, andthe muted level of F-actin staining (Fig. 4). Similarly, pretreat-ment with Plt-EVs also maintained these junctional proteins fol-lowing thrombin challenge, resulting in an attenuation of gapformation in the endothelial monolayer (Fig. 4). We quantitatedthe amount of VE-cadherin and ZO-1 expression in response tochallenge and treatment. As shown in Figure 4, the amount ofZO-1 expression decreased in response to thrombin challenge,and treatment with Plts significantly attenuated this loss, whiletreatment with Plt-EVs, on an average, also resulted in an in-crease in mean value of ZO-1 as compared with the thrombintreated group. Similar results were observed with the expressionof VE-cadherin.
Effect of Plt-EVs on Plt AggregationTo examine possible hemostatic properties of Plt-EVs, we
studied their capability to enhance Plt aggregation response toagonist activation using a multiple electrode Plt aggregometer.As expected, addition of Plts to whole blood samples in-creased the Plt aggregation response when individually stim-ulated by agonists. With Plt treatment, ADP-induced aggregationdemonstrated an increase of 60% over untreated whole blood(p = <0.001), Plt treatment of collagen-induced aggregation in-creased by 32% over untreated whole blood (p = 0.009), Plt
935
ealth, Inc. All rights reserved.
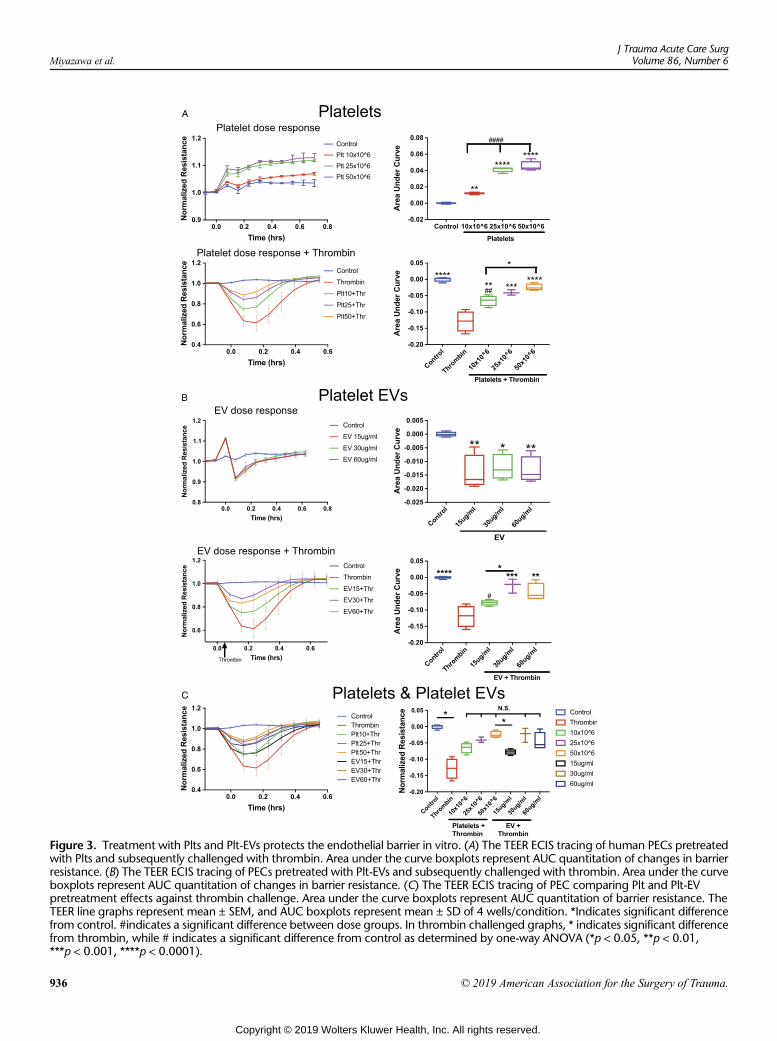
Figure 3. Treatment with Plts and Plt-EVs protects the endothelial barrier in vitro. (A) The TEER ECIS tracing of human PECs pretreatedwith Plts and subsequently challenged with thrombin. Area under the curve boxplots represent AUC quantitation of changes in barrierresistance. (B) The TEER ECIS tracing of PECs pretreated with Plt-EVs and subsequently challenged with thrombin. Area under the curveboxplots represent AUC quantitation of changes in barrier resistance. (C) The TEER ECIS tracing of PEC comparing Plt and Plt-EVpretreatment effects against thrombin challenge. Area under the curve boxplots represent AUC quantitation of barrier resistance. TheTEER line graphs represent mean ± SEM, and AUC boxplots represent mean ± SD of 4 wells/condition. *Indicates significant differencefrom control. #indicates a significant difference between dose groups. In thrombin challenged graphs, * indicates significant differencefrom thrombin, while # indicates a significant difference from control as determined by one-way ANOVA (*p < 0.05, **p < 0.01,***p < 0.001, ****p < 0.0001).
Miyazawa et al.J Trauma Acute Care Surg
Volume 86, Number 6
936 © 2019 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
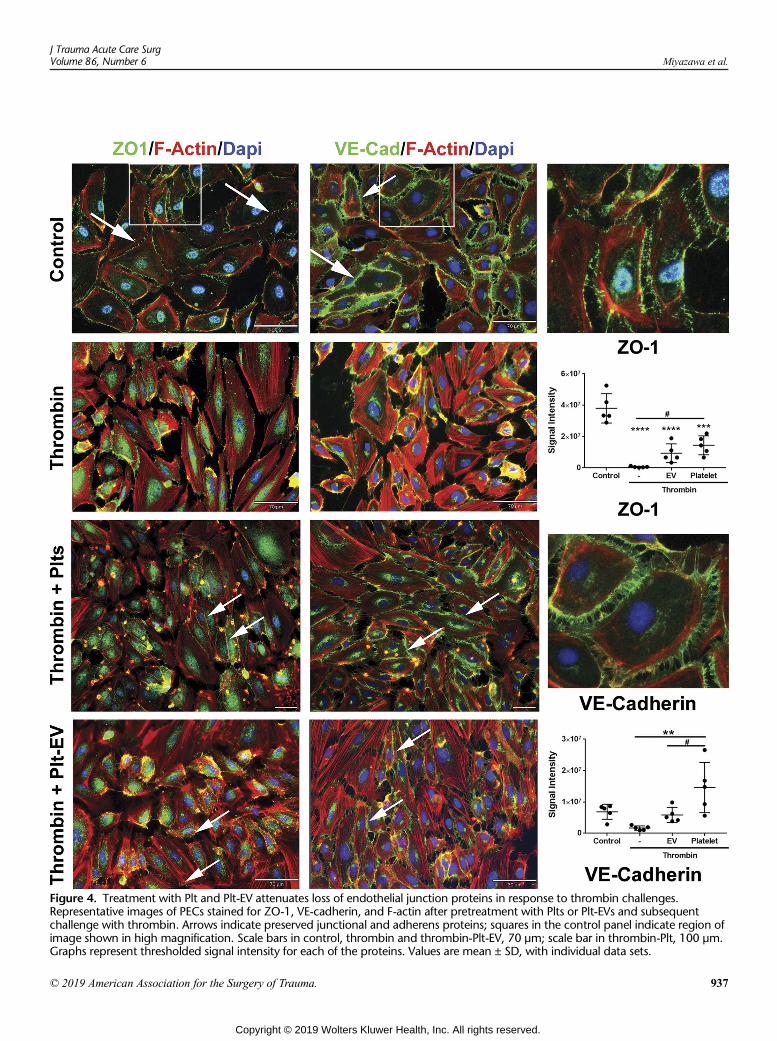
Figure 4. Treatment with Plt and Plt-EV attenuates loss of endothelial junction proteins in response to thrombin challenges.Representative images of PECs stained for ZO-1, VE-cadherin, and F-actin after pretreatment with Plts or Plt-EVs and subsequentchallenge with thrombin. Arrows indicate preserved junctional and adherens proteins; squares in the control panel indicate region ofimage shown in high magnification. Scale bars in control, thrombin and thrombin-Plt-EV, 70 μm; scale bar in thrombin-Plt, 100 μm.Graphs represent thresholded signal intensity for each of the proteins. Values are mean ± SD, with individual data sets.
J Trauma Acute Care SurgVolume 86, Number 6 Miyazawa et al.
© 2019 American Association for the Surgery of Trauma. 937
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
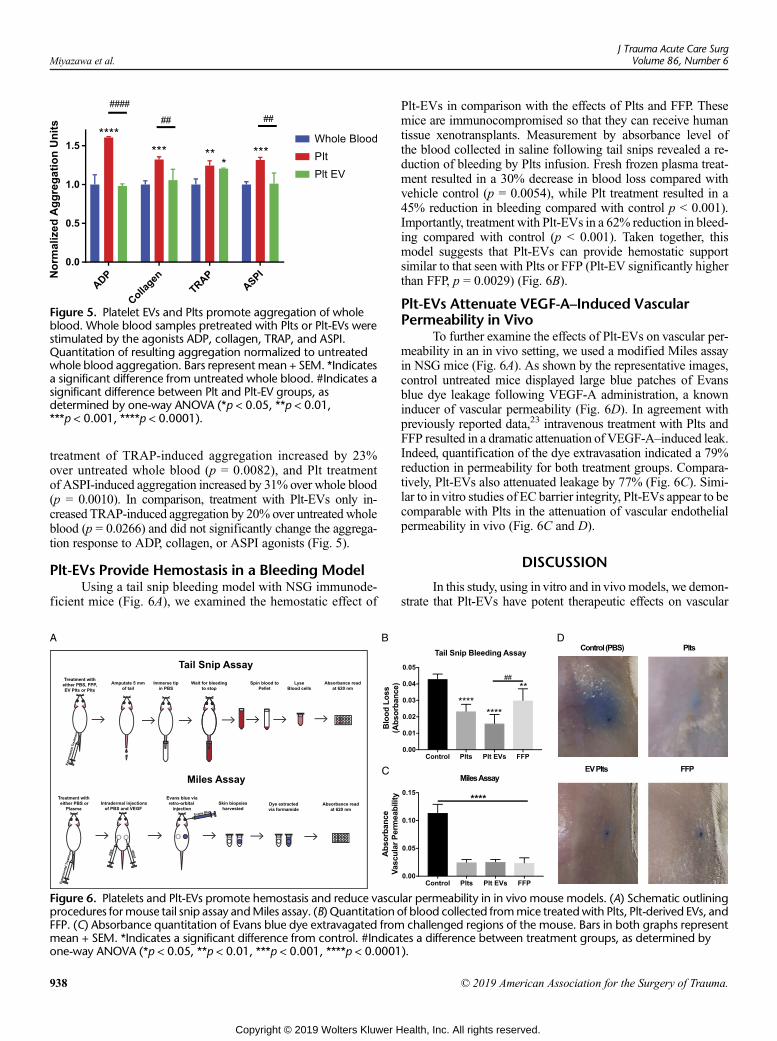
Figure 5. Platelet EVs and Plts promote aggregation of wholeblood. Whole blood samples pretreated with Plts or Plt-EVs werestimulated by the agonists ADP, collagen, TRAP, and ASPI.Quantitation of resulting aggregation normalized to untreatedwhole blood aggregation. Bars represent mean + SEM. *Indicatesa significant difference from untreated whole blood. #Indicates asignificant difference between Plt and Plt-EV groups, asdetermined by one-way ANOVA (*p < 0.05, **p < 0.01,***p < 0.001, ****p < 0.0001).
Miyazawa et al.J Trauma Acute Care Surg
Volume 86, Number 6
treatment of TRAP-induced aggregation increased by 23%over untreated whole blood (p = 0.0082), and Plt treatmentof ASPI-induced aggregation increased by 31% over whole blood(p = 0.0010). In comparison, treatment with Plt-EVs only in-creased TRAP-induced aggregation by 20% over untreated wholeblood (p = 0.0266) and did not significantly change the aggrega-tion response to ADP, collagen, or ASPI agonists (Fig. 5).
Plt-EVs Provide Hemostasis in a Bleeding ModelUsing a tail snip bleeding model with NSG immunode-
ficient mice (Fig. 6A), we examined the hemostatic effect of
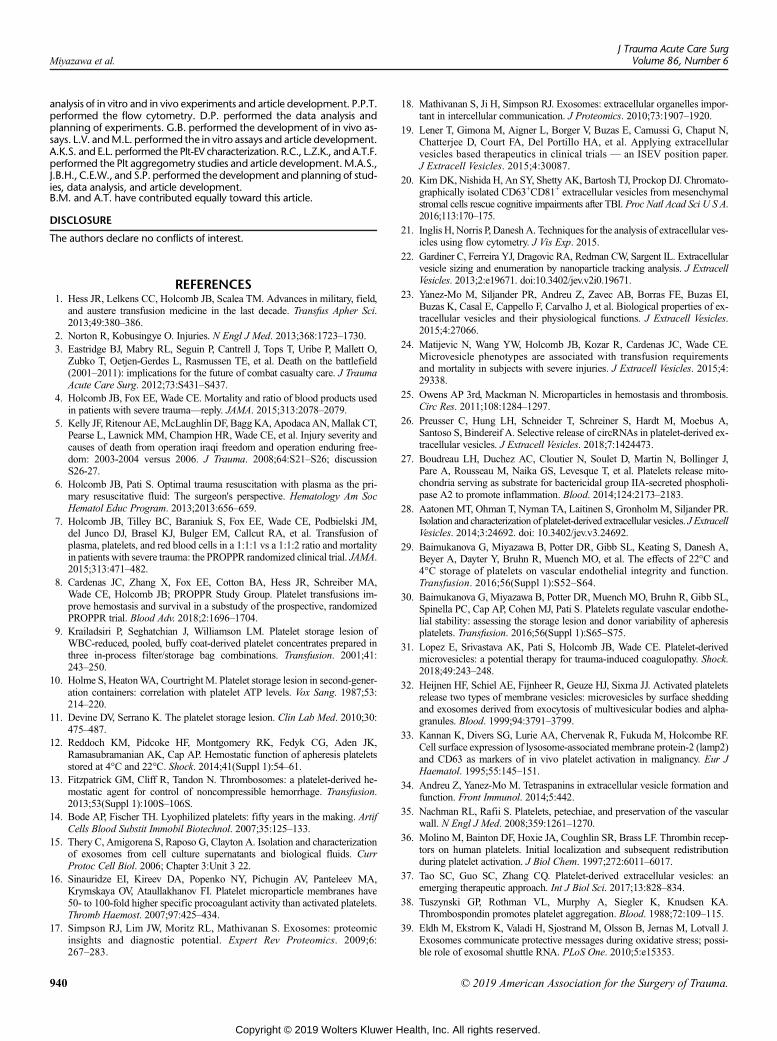
Figure 6. Platelets and Plt-EVs promote hemostasis and reduce vascuprocedures formouse tail snip assay andMiles assay. (B) Quantitation oFFP. (C) Absorbance quantitation of Evans blue dye extravagated frommean + SEM. *Indicates a significant difference from control. #Indicaone-way ANOVA (*p < 0.05, **p < 0.01, ***p < 0.001, ****p < 0.0001
938
Copyright © 2019 Wolters Kluwer H
Plt-EVs in comparison with the effects of Plts and FFP. Thesemice are immunocompromised so that they can receive humantissue xenotransplants. Measurement by absorbance level ofthe blood collected in saline following tail snips revealed a re-duction of bleeding by Plts infusion. Fresh frozen plasma treat-ment resulted in a 30% decrease in blood loss compared withvehicle control (p = 0.0054), while Plt treatment resulted in a45% reduction in bleeding compared with control p < 0.001).Importantly, treatment with Plt-EVs in a 62% reduction in bleed-ing compared with control (p < 0.001). Taken together, thismodel suggests that Plt-EVs can provide hemostatic supportsimilar to that seen with Plts or FFP (Plt-EV significantly higherthan FFP, p = 0.0029) (Fig. 6B).
Plt-EVs Attenuate VEGF-A–Induced VascularPermeability in Vivo
To further examine the effects of Plt-EVs on vascular per-meability in an in vivo setting, we used a modified Miles assayin NSG mice (Fig. 6A). As shown by the representative images,control untreated mice displayed large blue patches of Evansblue dye leakage following VEGF-A administration, a knowninducer of vascular permeability (Fig. 6D). In agreement withpreviously reported data,23 intravenous treatment with Plts andFFP resulted in a dramatic attenuation of VEGF-A–induced leak.Indeed, quantification of the dye extravasation indicated a 79%reduction in permeability for both treatment groups. Compara-tively, Plt-EVs also attenuated leakage by 77% (Fig. 6C). Simi-lar to in vitro studies of EC barrier integrity, Plt-EVs appear to becomparable with Plts in the attenuation of vascular endothelialpermeability in vivo (Fig. 6C and D).
DISCUSSION
In this study, using in vitro and in vivo models, we demon-strate that Plt-EVs have potent therapeutic effects on vascular
lar permeability in in vivo mouse models. (A) Schematic outliningf blood collected frommice treatedwith Plts, Plt-derived EVs, andchallenged regions of the mouse. Bars in both graphs represent
tes a difference between treatment groups, as determined by).
© 2019 American Association for the Surgery of Trauma.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 6 Miyazawa et al.
permeability and hemostasis. These particles, derived fromapheresis Plts, were confirmed to be the size of EVs,31 andexpressedmarker proteinswere known to be associatedwith Pltsand Plt-EV's (Figs. 1 and 2). In addition, they demonstrated anability, in vitro, to maintain endothelial junction protein expres-sion and functionally protect the endothelium from barrier dis-ruption (Figs. 3 and 4). It is of interest to note that the potencyand protective effects of Plt-EVs in vitro on endothelial barrierfunction are diminished when unchallenged by thrombin, indi-cating the necessity of Plts in the protection of an unstimulatedendothelium (compare Fig. 3B top and bottom panels). How-ever, after thrombin challenge, the Plt-EVs are equally protectiveof barrier integrity comparedwith Plts (Fig. 3C). Consistent withthese in vitro results with challenge, the in vivo data in the Milesassay and tail snip bleeding model suggest that Plt-EVs areequivalent to Plts in attenuating vascular permeability and pro-moting hemostasis. These results may suggest that some formof activation of the Plt-EVs, possibly by a stimulated endothe-lium, is required to initiate their EC barrier protective effects.This may be due to the release of Plt trophogens within the Plt-EVs that are known to regulate barrier stability.35
The Multiplate Plt aggregometry assays showed that Plt-EVs potentiate TRAP-induced Plt aggregation in healthy humanwhole blood but did not potentiate ASPI-, ADP-, or collagen-induced Plt aggregation. However, not surprisingly, the additionof Plts to healthy human whole blood potentiated all tested in-ducers of Plt aggregation. This observation may suggest thatPlt-EVs are indeed capable of providing a hemostatic functionbut may not be to the extent found with Plts. It is known thatthe Plt response to thrombin activation potentiates further ex-pression of surface thrombin receptors36 and that thrombin is avery potent Plt activator.28 It may be that the threshold for acti-vation is much lower for thrombin than other agonists, and thismechanism could be a potential explanation for the potentiationof thrombin response over the other agonists with the tested dos-ages of Plt-EVs. Further investigations with increasing dosagesof Plt-EVs may elucidate whether there is a dose-dependentresponse that potentiates ASPI-, ADP-, or collagen-inducedPlt aggregation.
Furthermore, Plt-EVs are known to have heterogeneousand highly diverse cargo, and studies have identified the pres-ence of both prothrombin and thrombospondin, a dominantprocoagulant α granule protein, in Plt-EVs.28,37,38 Given this,it may be that the Plt-EVs potentiation of the Plt aggregation re-sponse to thrombin can be explained by differential contents ofthrombin pathway-specific procoagulant proteins comparedwith the other Plt aggregation pathways tested in this study. Inaddition, proteomic studies have demonstrated differences inthe content of Plt MVs by size distribution, with smaller MVsenriched for increased procoagulant content than larger MVs.This association should also be considered as potential mechanis-tic support that there may be a variation in procoagulant contentsin the even smaller Plt-EVs, differentially potentiating the Plt re-sponse to thrombin-induced aggregation over others by contentsbeyond prothrombin and thrombospondin. In the future, it willbe critical to identify the array of contents within these Plt-EVs.
Limitations of this study are that Plt-EVs were tested froma single donor. In our past studies, we have demonstrated thatthere is considerable donor dependent variability in Plts and their
© 2019 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer H
effects on endothelial integrity.29,30 It has been shown that EVs,primarily of exosomal origin from a particular cell type, consis-tently have about 50% of their “cargo” in common,17–19,39,40
hence indicating that there is a cellular program mediated bythe particular cell type that packages specific proteins andothers such as RNA into EVs. Plasma from trauma patientslacking Plt-EVs demonstrates a decreased response to Lipo-polysaccharide (LBS),41 and trauma patients with acute trau-matic coagulopathy have reduced concentration of Plt-EVs.24
Taken together, these studies on Plt-EVs indicate that they playa role in trauma-induced inflammation and coagulation; hence,the delicate balance and interaction between the patient andthe effects of Plt-EVs on inflammation, coagulation, and vascu-lar function will likely determine outcomes. It is possible thatPlt-EVs as a therapeutic could result in different clinical out-comes depending on the patient, timing of delivery, and dosegiven in trauma. Indeed, the freeze-thaw nature of Plt-EV dosestorage could very likely affect the outcomes of their therapeuticeffects. Examination of any changes to the Plt-EV morphology,content, and function by long-term storage is warranted. Alto-gether, the role and therapeutic potential of Plt-EVs in traumacould potentially be mixed and requires further investigation.31
Future studies into donor dependent variability in EVs are war-ranted as well.
Another limitation of this study is that the Plt-EVs weretested in vivo by pretreating animals, which is not clinically rel-evant to the treatment of bleeding patients. The Plt-EVs werealso not tested in models of traumatic injury for their therapeuticpotential, for example, in models of hemorrhagic shock andhemorrhage-induced lung vascular permeability.42,43 This willbe the focus of future studies where Plt-EVswill be administeredafter traumatic injury in rodent models. It would be of interest aswell in future studies to distinguish between the contribution ofPlts and Plt-EVs in the regulation of hemostasis and vascularstability. One potential method to investigate this questionwould be to study Plts and the lack of Plt-EVs in a Rab27aand Rab27b double-knockout (Rab27DKO) mice that are defi-cient in exosome secretion.44 One can hypothesize that the ef-fects of Plts on both endpoints would be attenuated.
Treating uncontrolled hemorrhage is challenging in aus-tere environments such as remote rural areas of the United Statesand military Role 2 facilities or during prehospital transport.1 Inthe military, apheresis Plts can only be stored for up to 5 days atroom temperature (22°C), which makes transportation from theUnited States to the battlefield generally impossible. The mili-tary has moved to using cold-stored Plts or collecting Plts andPlt-containing products such as low-titer whole blood in the bat-tlefield, but these are more difficult to use under challengingconditions.1 Platelet EVs are a potential novel hemostatic agentthat could possibly be stored for extended periods at room tem-perature or dried, warranting further investigation. The availabil-ity of a dried hemostatic agent (i.e., dried Plt-EVs) that can bridgebleeding patients and attenuate the endotheliopathy of trauma,until patients can receive blood products, would provide severaltherapeutic advantages in both civilian and military settings.
AUTHORSHIP
B.M. performed the planning and execution of all assays as well as writingand editing of the article. A.T. performed the planning, execution, and
939
ealth, Inc. All rights reserved.
Miyazawa et al.J Trauma Acute Care Surg
Volume 86, Number 6
analysis of in vitro and in vivo experiments and article development. P.P.T.performed the flow cytometry. D.P. performed the data analysis andplanning of experiments. G.B. performed the development of in vivo as-says. L.V. andM.L. performed the in vitro assays and article development.A.K.S. and E.L. performed the Plt-EV characterization. R.C., L.Z.K., and A.T.F.performed the Plt aggregometry studies and article development.M.A.S.,J.B.H., C.E.W., and S.P. performed the development and planning of stud-ies, data analysis, and article development.B.M. and A.T. have contributed equally toward this article.
DISCLOSURE
The authors declare no conflicts of interest.
REFERENCES1. Hess JR, Lelkens CC, Holcomb JB, Scalea TM. Advances in military, field,
and austere transfusion medicine in the last decade. Transfus Apher Sci.2013;49:380–386.
2. Norton R, Kobusingye O. Injuries. N Engl J Med. 2013;368:1723–1730.3. Eastridge BJ, Mabry RL, Seguin P, Cantrell J, Tops T, Uribe P, Mallett O,
Zubko T, Oetjen-Gerdes L, Rasmussen TE, et al. Death on the battlefield(2001–2011): implications for the future of combat casualty care. J TraumaAcute Care Surg. 2012;73:S431–S437.
4. Holcomb JB, Fox EE, Wade CE. Mortality and ratio of blood products usedin patients with severe trauma—reply. JAMA. 2015;313:2078–2079.
5. Kelly JF, Ritenour AE,McLaughlin DF, BaggKA, ApodacaAN,Mallak CT,Pearse L, Lawnick MM, Champion HR, Wade CE, et al. Injury severity andcauses of death from operation iraqi freedom and operation enduring free-dom: 2003-2004 versus 2006. J Trauma. 2008;64:S21–S26; discussionS26-27.
6. Holcomb JB, Pati S. Optimal trauma resuscitation with plasma as the pri-mary resuscitative fluid: The surgeon's perspective. Hematology Am SocHematol Educ Program. 2013;2013:656–659.
7. Holcomb JB, Tilley BC, Baraniuk S, Fox EE, Wade CE, Podbielski JM,del Junco DJ, Brasel KJ, Bulger EM, Callcut RA, et al. Transfusion ofplasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortalityin patientswith severe trauma: the PROPPR randomized clinical trial. JAMA.2015;313:471–482.
8. Cardenas JC, Zhang X, Fox EE, Cotton BA, Hess JR, Schreiber MA,Wade CE, Holcomb JB; PROPPR Study Group. Platelet transfusions im-prove hemostasis and survival in a substudy of the prospective, randomizedPROPPR trial. Blood Adv. 2018;2:1696–1704.
9. Krailadsiri P, Seghatchian J, Williamson LM. Platelet storage lesion ofWBC-reduced, pooled, buffy coat-derived platelet concentrates prepared inthree in-process filter/storage bag combinations. Transfusion. 2001;41:243–250.
10. Holme S, HeatonWA, CourtrightM. Platelet storage lesion in second-gener-ation containers: correlation with platelet ATP levels. Vox Sang. 1987;53:214–220.
11. Devine DV, Serrano K. The platelet storage lesion. Clin Lab Med. 2010;30:475–487.
12. Reddoch KM, Pidcoke HF, Montgomery RK, Fedyk CG, Aden JK,Ramasubramanian AK, Cap AP. Hemostatic function of apheresis plateletsstored at 4°C and 22°C. Shock. 2014;41(Suppl 1):54–61.
13. Fitzpatrick GM, Cliff R, Tandon N. Thrombosomes: a platelet-derived he-mostatic agent for control of noncompressible hemorrhage. Transfusion.2013;53(Suppl 1):100S–106S.
14. Bode AP, Fischer TH. Lyophilized platelets: fifty years in the making. ArtifCells Blood Substit Immobil Biotechnol. 2007;35:125–133.
15. Thery C, Amigorena S, Raposo G, Clayton A. Isolation and characterizationof exosomes from cell culture supernatants and biological fluids. CurrProtoc Cell Biol. 2006; Chapter 3:Unit 3 22.
16. Sinauridze EI, Kireev DA, Popenko NY, Pichugin AV, Panteleev MA,Krymskaya OV, Ataullakhanov FI. Platelet microparticle membranes have50- to 100-fold higher specific procoagulant activity than activated platelets.Thromb Haemost. 2007;97:425–434.
17. Simpson RJ, Lim JW, Moritz RL, Mathivanan S. Exosomes: proteomicinsights and diagnostic potential. Expert Rev Proteomics. 2009;6:267–283.
940
Copyright © 2019 Wolters Kluwer H
18. Mathivanan S, Ji H, Simpson RJ. Exosomes: extracellular organelles impor-tant in intercellular communication. J Proteomics. 2010;73:1907–1920.
19. Lener T, Gimona M, Aigner L, Borger V, Buzas E, Camussi G, Chaput N,Chatterjee D, Court FA, Del Portillo HA, et al. Applying extracellularvesicles based therapeutics in clinical trials — an ISEV position paper.J Extracell Vesicles. 2015;4:30087.
20. KimDK, Nishida H, An SY, Shetty AK, Bartosh TJ, Prockop DJ. Chromato-graphically isolated CD63+CD81+ extracellular vesicles from mesenchymalstromal cells rescue cognitive impairments after TBI. Proc Natl Acad Sci U S A.2016;113:170–175.
21. Inglis H, Norris P, Danesh A. Techniques for the analysis of extracellular ves-icles using flow cytometry. J Vis Exp. 2015.
22. Gardiner C, Ferreira YJ, Dragovic RA, Redman CW, Sargent IL. Extracellularvesicle sizing and enumeration by nanoparticle tracking analysis. J ExtracellVesicles. 2013;2:e19671. doi:10.3402/jev.v2i0.19671.
23. Yanez-Mo M, Siljander PR, Andreu Z, Zavec AB, Borras FE, Buzas EI,Buzas K, Casal E, Cappello F, Carvalho J, et al. Biological properties of ex-tracellular vesicles and their physiological functions. J Extracell Vesicles.2015;4:27066.
24. Matijevic N, Wang YW, Holcomb JB, Kozar R, Cardenas JC, Wade CE.Microvesicle phenotypes are associated with transfusion requirementsand mortality in subjects with severe injuries. J Extracell Vesicles. 2015;4:29338.
25. Owens AP 3rd, Mackman N. Microparticles in hemostasis and thrombosis.Circ Res. 2011;108:1284–1297.
26. Preusser C, Hung LH, Schneider T, Schreiner S, Hardt M, Moebus A,Santoso S, Bindereif A. Selective release of circRNAs in platelet-derived ex-tracellular vesicles. J Extracell Vesicles. 2018;7:1424473.
27. Boudreau LH, Duchez AC, Cloutier N, Soulet D, Martin N, Bollinger J,Pare A, Rousseau M, Naika GS, Levesque T, et al. Platelets release mito-chondria serving as substrate for bactericidal group IIA-secreted phospholi-pase A2 to promote inflammation. Blood. 2014;124:2173–2183.
28. AatonenMT, Ohman T, Nyman TA, Laitinen S, GronholmM, Siljander PR.Isolation and characterization of platelet-derived extracellular vesicles. J ExtracellVesicles. 2014;3:24692. doi: 10.3402/jev.v3.24692.
29. Baimukanova G, Miyazawa B, Potter DR, Gibb SL, Keating S, Danesh A,Beyer A, Dayter Y, Bruhn R, Muench MO, et al. The effects of 22°C and4°C storage of platelets on vascular endothelial integrity and function.Transfusion. 2016;56(Suppl 1):S52–S64.
30. Baimukanova G, Miyazawa B, Potter DR, Muench MO, Bruhn R, Gibb SL,Spinella PC, Cap AP, Cohen MJ, Pati S. Platelets regulate vascular endothe-lial stability: assessing the storage lesion and donor variability of apheresisplatelets. Transfusion. 2016;56(Suppl 1):S65–S75.
31. Lopez E, Srivastava AK, Pati S, Holcomb JB, Wade CE. Platelet-derivedmicrovesicles: a potential therapy for trauma-induced coagulopathy. Shock.2018;49:243–248.
32. Heijnen HF, Schiel AE, Fijnheer R, Geuze HJ, Sixma JJ. Activated plateletsrelease two types of membrane vesicles: microvesicles by surface sheddingand exosomes derived from exocytosis of multivesicular bodies and alpha-granules. Blood. 1999;94:3791–3799.
33. Kannan K, Divers SG, Lurie AA, Chervenak R, Fukuda M, Holcombe RF.Cell surface expression of lysosome-associated membrane protein-2 (lamp2)and CD63 as markers of in vivo platelet activation in malignancy. Eur JHaematol. 1995;55:145–151.
34. Andreu Z, Yanez-Mo M. Tetraspanins in extracellular vesicle formation andfunction. Front Immunol. 2014;5:442.
35. Nachman RL, Rafii S. Platelets, petechiae, and preservation of the vascularwall. N Engl J Med. 2008;359:1261–1270.
36. Molino M, Bainton DF, Hoxie JA, Coughlin SR, Brass LF. Thrombin recep-tors on human platelets. Initial localization and subsequent redistributionduring platelet activation. J Biol Chem. 1997;272:6011–6017.
37. Tao SC, Guo SC, Zhang CQ. Platelet-derived extracellular vesicles: anemerging therapeutic approach. Int J Biol Sci. 2017;13:828–834.
38. Tuszynski GP, Rothman VL, Murphy A, Siegler K, Knudsen KA.Thrombospondin promotes platelet aggregation. Blood. 1988;72:109–115.
39. Eldh M, Ekstrom K, Valadi H, Sjostrand M, Olsson B, Jernas M, Lotvall J.Exosomes communicate protective messages during oxidative stress; possi-ble role of exosomal shuttle RNA. PLoS One. 2010;5:e15353.
© 2019 American Association for the Surgery of Trauma.
ealth, Inc. All rights reserved.
J Trauma Acute Care SurgVolume 86, Number 6 Miyazawa et al.
40. Thery C, Ostrowski M, Segura E. Membrane vesicles as conveyors of im-mune responses. Nat Rev Immunol. 2009;9:581–593.
41. Balvers K, Curry N, Kleinveld DJ, Boing AN, Nieuwland R, Goslings JC,Juffermans NP. Endogenous microparticles drive the proinflammatory hostimmune response in severely injured trauma patients. Shock. 2015;43:317–321.
42. Pati S, Potter DR, Baikamunova G, Farrell DH, Holcomb JB, Schreiber MA.Modulating the endotheliopathy of trauma: factor concentrate vs. fresh fro-zen plasma. J Trauma Acute Care Surg. 2016.
43. Potter DR, Baimukanova G, Keating SM, Deng X, Chu JA, Gibb SL,Peng Z, Muench MO, Fomin ME, Spinella PC, et al. Fresh frozen plasmaand spray-dried plasma mitigate pulmonary vascular permeability and in-flammation in hemorrhagic shock. J Trauma Acute Care Surg. 2015;78:S7–S17.
44. Alexander M, Ramstead AG, Bauer KM, Lee SH, Runtsch MC, Wallace J,Huffaker TB, Larsen DK, Tolmachova T, Seabra MC, et al. Rab27-dependentexosome production inhibits chronic inflammation and enables acute re-sponses to inflammatory stimuli. J Immunol. 2017;199:3559–3570.
DISCUSSIONSUSAN EVANS, M.D. (Charlotte, North Carolina):
Thank you, Dr. Schreiber, Dr. Henry, members and guests.Platelets are well recognized as crucial to controlling hemor-rhage. However, the availability of platelets remains limiteddue to insufficient supply and short storage life.
Dr. Pati and colleagues have attempted to address thiscrucial problem with a unique utilization of bloodstream con-stituents which, until now, have generally been considered dys-functional byproducts of physiologic stress.
Extracellular vesicles, sometimes called microparticles,are cell fragments released by exocytosis, often following cellactivation, and occur in the bloodstream in substantially in-creased concentration following injury or stress.
Because they carry only portions of cells, their signaling isaltered from their parent cell and they have been shown to con-tribute to inflammation. However, Dr. Pati and her colleagueshave identified a molecular response to extracellular vesicleswhich could be beneficial rather than detrimental.
They evaluated the impact of platelet extracellular vesicleson limiting vascular permeability and hemostasis.
In a very elegantly designed study they demonstrated thatextracellular vesicles have a generally similar efficacy to plate-lets in preventing vascular permeability.
At the very least, these findings help our understanding ofclotting and hemostasis to pursue further investigation into themechanisms of both platelets and extracellular vesicles.
At best, they provide an intervention which can improvehemorrhage control, despite our limited supply of platelets.
Dr. Pati, I have four questions.Number 1. At this World Trauma Conference we should
recognize the contributions of our Chinese colleagues who dem-onstrate an upregulation of CRP and IL6 in platelet extracellularvesicles.
Furthermore, non-platelet-derived extracellular vesicles,which are most certainly included in your concentrates, havebeen demonstrated to enhance inflammation, as well.
How could you exclude non-platelet-derived extracellularvesicles or mitigate the inflammatory effects of the platelet-derived extracellular vesicles?
Number 2. Our Canadian colleagues have identified thatonly a fraction of platelet extracellular vesicles actually contain
© 2019 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer H
the phosphatidylserine from the lipid bilayer integral to plateletaggregation.
Additionally, you demonstrate that platelet extracellularvesicles actually decrease endothelial barrier resistance withoutthe thrombin activation.
This is not equivalent to the platelet response, as you sug-gest in your title. Given these findings, could platelet extracel-lular vesicles lead to increased bleeding, perhaps?
Number 3. On the contrary, understanding that withoutthe entire cell for regulation is it possible these vesicles couldcreate upregulated thrombosis?
And, finally, coming from one of the labs that hasattempted to extend access to stored platelets I appreciate yourefforts to spare this precious resource.
However, your technique to harvest these fragments stillrequires platelet concentrates. Doesn’t that defeat the purposeof providing a treatment which, ideally, spares our limited plate-let supply?
Thank you to the AAST for the opportunity to review thisimportant manuscript. Dr. Pati, I look forward to your re-sponses. Thank you.
HASAN B. ALAM, M.D. (Ann Arbor, Michigan):Very nicely presented work. And every time I listen to oneof your talks I learn something, and this was no exception.Excellent job.
So, I have two quick questions. The first one is about thesevesicles from the platelets. Are these specific to the platelets, orwould you see the same effect if you have non-platelet vesiclesfrom a variety of different sources? Is it possible that other cel-lular products, such as exosomes, may be at play? As you know,you can drive exosomes frommultiple cellular sources. You canalso scale up the production, and generate exosomes in verylarge quantities, which has obvious commercial implications.There is a lot of research going on showing that exosomes canstabilize the endothelium, and promote healing. So how muchof the effect that you have observed is specific to platelet-derivedvesicles, versus a generalized response to various cellular prod-ucts that are shed in response to different stimuli?
And the second question is about finding the right bal-ance. We know that a lot of these cellular particles act asDAMPs and can create an exaggerated inflammatory response.And here you are showing data that they are beneficial. So,how do you sort out the good versus the bad?
MICHAEL GOODMAN, M.D. (Cincinnati, Ohio):More of a technical question for you. What are your EVs re-suspended in? And is this a dose-dependent response with theEVs, one, depending on the amount of EVs you use; and two,the size of the EVs that are applied?
SHIBANI PATI,M.D. Ph.D. (San Francisco, California):Thankyou verymuch,Dr. Evans, for your comments and questions.
So I wanted to address one of the questions you had aboutthe issue of thrombosis and also this addresses Dr. Alam’s ques-tion of whether or not there are potentially deleterious and alsobeneficial effects of these platelet EVs.
So I think that this is very context dependent. And if weare aiming as using this as a therapeutic we have to be mindfulof the fact that they do have pro-thrombotic effects.
They have phosphatidylserine on the surface. They acti-vate Factors II and X. They have tissue factor, also, on the
941
ealth, Inc. All rights reserved.

Miyazawa et al.J Trauma Acute Care Surg
Volume 86, Number 6
surface, GB2B and 3A. All of these taken together do, indeed,indicate that they have the capacity to be thrombotic.
In cancer research it has been shown really clearly thatthey are indicative of thrombotic events within cancer patientswith increased platelet EVs in their circulation.
So with that in mind I think that this is where – this is thenext step in our endeavors to understand this as a therapeutic in,for example, in ARDS or hemorrhagic shock-induced ARDS.Do we see microthrombi in the lung?
So to date, I think, I bet you, I’m sure that there is someissue with context and dose. And so that’s really what this re-quires is to understand therapeutic window, dose, and timingof delivery to really tease out whether there are deleterious ef-fects so we should be mindful of that.
Another question that was brought up by Dr. Evans relatedto the variability in extracellular vesicles and also the ones thatare not platelet-derived. Dr. Alam, you also alluded to this, too.
So in plasma, if you look at plasma it really actually de-pends on which donor you analyze the EV content from. Somedonors have very high amounts, numbers of endothelial-derived
942
Copyright © 2019 Wolters Kluwer H
microvesicles. Some donors have actually low EVs from endo-thelial cells and much higher from platelets.
Generally speaking, we’ve analyzed about ten donorsacross the board, what we’ve found is about 80 percent of themicrovesicles are EVs in plasma are derived from platelets.
And so you know that’s actually a thought is can we actu-ally start to sort out specific types of EVs. As you know, thereare other EVs, for example from mesenchymal stem cells, thatalso circulate and these have very potent effects.
So, no, I actually do not think that the effects we are seeingare completely just derived from platelet EVs, Dr. Alam. But Iactually think that there are other cell types that are in there.And that would be really a great interest in our future studies.
Another question that was asked was about what dowe re-suspend the EVs in, we spin them down and we re-suspend themin buffer, basically a phosphate buffered saline. We don’t putthem into plasma. And then they’re directly transfused or in-fused intravascular.
I think that – yes. So I think that basically sums up. I hopeI answered all the questions that were asked.
© 2019 American Association for the Surgery of Trauma.
ealth, Inc. All rights reserved.

AAST 2018 PODIUM PAPER
Red blood cell storage and adhesion to vascular endotheliumunder normal or stress conditions: An in vitro microfluidic study
Lawrence N. Diebel, MD and David M. Liberati, MS, Detroit, Michigan
Sub
Fro
Thi
Ad
DO
J TrVol
BACKGROUND: O
mitted: November 9,2019, Published onlinm the Michael and MaState University, Detros study was presentedthe Surgery of Traumadress for reprints: Lawrof Surgery, 6C Univeemail: [email protected]
I: 10.1097/TA.000000
auma Acute Care Suume 86, Number 6
bservational studies have identified an association between duration of red blood cell (RBC) storage and adverse outcomes in trauma.Hemorrhagic shock (HS) leads to impaired tissue perfusion which is associated with endothelial cell glycocalyx (eGC) shedding. Adhesionof stored RBC to the vascular endothelium has been shown to lead to impaired perfusion in the microcirculation and contribute to organfailure and poor outcome. The role of either or both of the EC and RBC glycocalyx in this process is unknown and was studied in an invitro model.
METHODS: H
uman umbilical vein endothelial cells were perfused in a microfluidic device with RBC solutions from fresh, less than 14-day or longerthan 21-day storage. In some experiments, the HSmicroenvironment was simulated by hypoxia-reoxygenation (H/R) and epinephrine (Epi)in the perfusion experiments. Measurements obtained included endothelial cell (EC) and RBC glycocalyx and RBC adherence to humanumbilical vein endothelial cell monolayers at variable shear rates.RESULTS: E
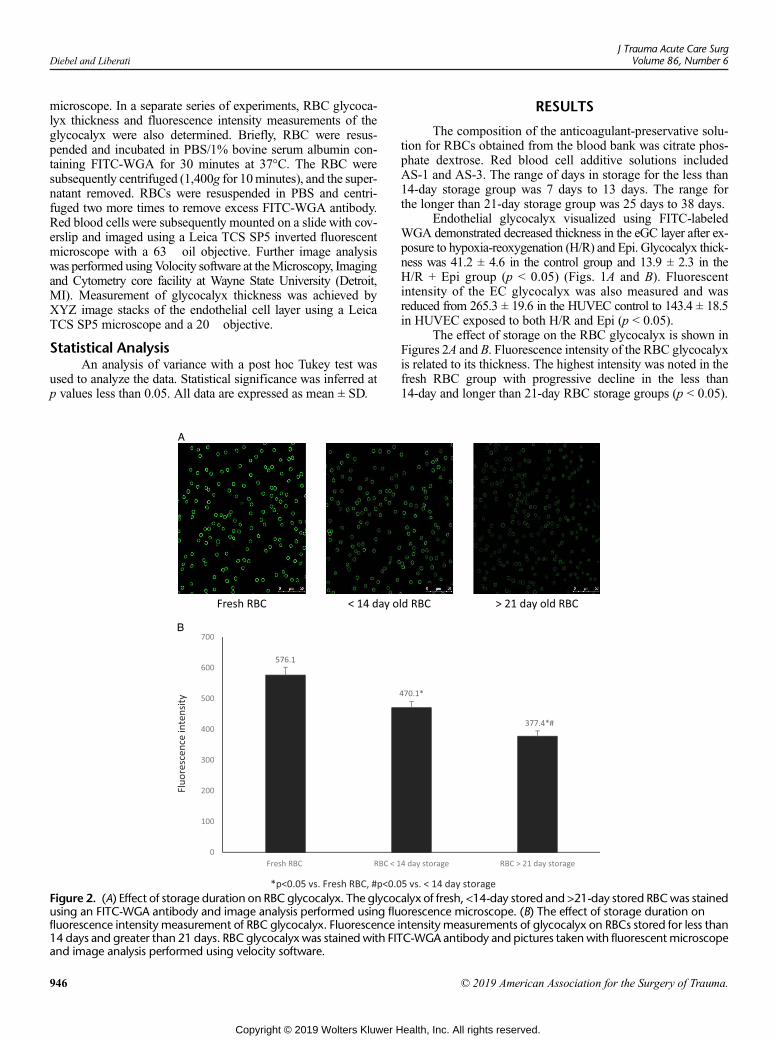
ndothelial cell glycocalyx and RBC glycocalyx dimensionswere reduced byH/R and Epi and storage duration respectively. Red blood celladherence to the endothelium was increased by H/R + Epi treatment and duration of RBC storage.CONCLUSION: O
ur data may help explain some of the remaining discrepancies regarding the impact of RBC storage duration on outcomes in the traumapopulation. Consideration of the integrity of the EC and RBC glycocalyx may guide future transfusion strategies in the trauma population.The microfluidic device system platform may offer a high throughput modality to study emerging therapies to mitigate adverse conse-quence of RBC storage duration on the perfused endothelium in the trauma setting. (J Trauma Acute Care Surg. 2019;86: 943–951. Copy-right © 2019 American Association for the Surgery of Trauma.)KEYWORDS: M
icrofluidic device; red blood cell glycocalyx; red blood cell storage lesion.T rauma patients are frequently given blood transfusions ei-ther during the resuscitation phase or within the first few
days following injury. A number of reviews have addressed theimpact of stored blood in the trauma population.1–3 The effectof the age of stored blood used has been carefully analyzed ina number of large studies and meta analyses. These studies sug-gest that red blood cell (RBC) storage time does not affect mor-tality.4,5 However, there is continued debate regarding otheroutcomes, including organ failure and infectious complications.Moreover, the trauma population has been underrepresented inrecent randomized trials that attempted to study the effect ofthe duration of blood storage on outcome.2,6 There are also anumber of confounding variables in the trauma populationwhich complicates analysis of the age of transfused allogeneicRBCs. These include number of units of blood transfused andthe timing of transfusion in relation to initial injury and themixing of old and relatively “fresh” units of packed RBCs(PRBC) administered.7,8
2018, Revised: January 29, 2019, Accepted: February 14,e: March 1, 2019.rian Ilitch Department of Surgery (L.N.D., D.M.L.), Wayneit, Michigan.at the 77th annual meeting of the American Association for, San Diego, CA September 26-29, 2018.ence N. Diebel, MD, Michael andMarian Ilitch Departmentrsity Health Center, 4201 St. Antoine, Detroit, MI 48201;ayne.edu.
0000002239
rg
Copyright © 2019 Wolters Kluwer H
Disturbances in the microcirculation have been describedin trauma and other critically ill patients. This is relevant becauseimpaired perfusion in the microvasculature has been shown toimpact the response to RBC transfusion.9 In addition, the endo-thelial glycocalyx (eGC) is now recognized for its importance inthe vascular barrier and promoting homogeneous blood flowdistribution in the microcirculation.10–13 The eGC regulates vas-cular permeability, coagulation, and interactions between the en-dothelial cells and the blood and acts as a mechanotransducer offluid shear stress on vascular tone via endothelial nitric oxide(NO) activity. As such, the eGC has been referred to as the “hel-met” of the microcirculation in trauma.14
Hemorrhagic shock (HS) has been shown to cause glycoca-lyx degradation and vascular barrier injury, and their magnitude isrelated to the severity of the insult.15–17 Because the eGC is thefirst layer of the vascular endothelium to come in contact withblood cells, it is likely that damage to the eGC would impact theflow properties of blood cells, especially RBCs. Red blood cell-vascular endothelial interactions have a causal relationship to thepathology of several disease states including sickle cell anemia,malaria and diabetes. A previous study by Chin-Lee and col-leagues18 demonstrated that stored RBCs showed increased ad-herence of stored RBCs compared with fresh RBCs in the ratmicrovasculature. Anniss et al.19 demonstrated that storage du-ration increases adhesion of stored RBC to the vascular endothe-lium in an in vitro model. In another study by this group, avariable effect on RBC adhesion to activated vascular endothe-lium was noted.20 However, the role of the eGC in effectingRBC adhesion was not addressed in these studies.
943
ealth, Inc. All rights reserved.

Diebel and LiberatiJ Trauma Acute Care Surg
Volume 86, Number 6
Red blood cells are also covered by a glycocalyx. Aging ofRBCs in circulation is associated with a decrease in thickness ofits glycocalyx. The thickness of the RBC glycocalyx is alsodiminished in certain forms of hypertension, obesity, and di-abetes.21 Oxidative stress is common in clinical conditionsassociated with glycocalyx degradation.22,23 Because oxida-tive stress may occur during RBC storage, we postulated thatstorage duration would impact the integrity of the RBC glyco-calyx. The importance of both the RBC glycocalyx and theeGC in promoting blood flow in the microcirculation has beenrecognized.24 Under normal circumstances, the eGC with itsnegatively charged components (especially heparin sulfate)prevents RBCs (also negatively charged) from becoming at-tached to the endothelial surface which may have importantconsequences. Loss of the glycocalyx layer from either the en-dothelium or the RBC surface could increase the interaction ofRBC with the endothelial surface of blood cells. Although theprimary objective of RBC transfusion is the restoration ofoxygen-carrying capacity, it is now apparent that RBC transfu-sion has an important role in the restoration of microvascularfunction. Loss or damage to either glycocalyx layer may impairmicrovascular perfusion due to adhesion of RBCs to the vascu-lar endothelium. This may be more likely if there are perturba-tions in both glycocalyx layers. We, therefore, postulated thattrauma/HS (T/HS) with subsequent eGC degradation and“older” RBC with a diminished glycocalyx layer would havethe most adverse effect on blood flow in the microcirculation.
Microfluidics is a technology that has been used to studyendothelial cell biology and stored RBC under in vitro flowconditions. This high throughput system allows study of theendothelial-RBC interaction under tightly controlled conditionsand was used to evaluate the impact of eGC and RBC glycoca-lyx on RBC-endothelial interaction in vitro.
METHODS
Human Umbilical Vein Endothelial Cell CultureHuman umbilical vein endothelial cells (HUVEC) were
purchased fromLonzaWalkersville, Inc. (Walkersville,MD). Cellswere grown in a 75-cm2 flask using complete media (EGM-2BulletKit; Lonza). Time to subculture is 5 days to 9 days, with me-dia changes every 2 days. Cells are subcultured at 85% confluenceusing 2 mL of 0.5% trypsin-ethylenediaminetetraacetic acid (LifeTechnologies, Carlsbad, CA). A new culture flask is preparedand the remaining cells are used to seed the microfluidic chan-nels of a BioFlux 48-well plate (Fluxion Bio) that has beenprimed and coated with 100 μg/mL fibronectin (Fisher Scien-tific) for 1 hour at room temperature. Monolayers were formedwithin the microfluidic channels after overnight perfusion ofthe cells with complete media at a shear force of 1 dyne/cm2.Human umbilical vein endothelial cell at passages 4 to 7 wereused for all experiments.
Well Plate Microfluidic Device SystemThe main components of the microfluidic device system
(MDS) include BioFlux plates, a pressure interface device, acontroller instrument, and software for the instrument controland image analysis. The BioFlux plates contain an array ofmicrofluidic flow channels on a well plate format which are
944
Copyright © 2019 Wolters Kluwer H
connected to inlet and outlet wells. The pressure interface devicecovers the top of the well plate and applies a controlled pneu-matic pressure from the control instrument. This serves todrive the fluid or perfusate through the microfluidic channelsat a user-defined flow rate. An observation window in the bot-tom of the microfluidic channels allows imaging by micros-copy. The MDS software allows control of the flow settings,as well as other parameters including image analysis. Thus,the microfluidic device allows the study of the glycocalyx bar-rier function under flow-induced shear stress under controlledexperimental conditions.
Blood PreparationBlood was collected from healthy volunteer donors
(N = 4) in citrated vacuum tubes containing ethylenediaminetet-raacetic acid present in the collection tubes. The blood sampleswere centrifuged for 10 minutes at 1,400g. After the first centri-fugation, the buffy coat is removed and the plasma layer leavingthe RBC in the bottom of the tube. Add 3 mL of phosphate-buffered saline (PBS) (no calcium or magnesium) to the tubecontaining the RBC and centrifuge for a second time for10 minutes at 1,400g. Discard the PBS and repeat above a thirdtime to yield clean RBCs.25 The RBC segments (<14-day stor-age [N = 6] and >21-day storage [N = 6]) were also obtainedfrom the blood bank at Harper University Hospital Detroit,MI. The blood bank samples were obtained from saved seg-ments of blood tubes which are routinely attached to the bloodunit in blood banks. All RBC samples were diluted in PBS at1.5% or 23%.
Experimental DesignOnce confluent HUVEC monolayers are formed, RBC
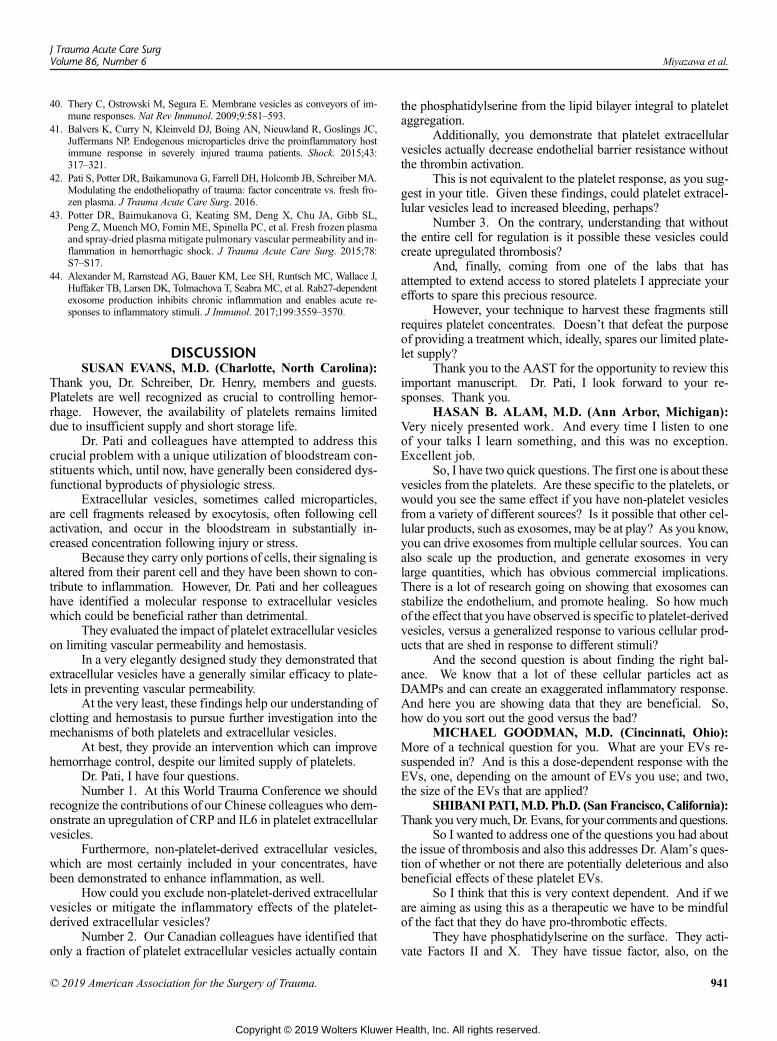
obtained from volunteers (fresh) or from the blood bank (<14-day storage or >21-day storage) at 1.5% and 23% cell suspen-sion were added to the perfusate at different flow rates. In someexperiments, HUVEC are exposed to 10−3 μM epinephrine (epi)and/or hypoxia for 60 minutes at 37°C and 95% N2/5% O2. Fol-lowing this, standard culture conditions are reinstated (37°Cwith 5% CO2; reoxygenation). The RBC adhesion to the endo-thelial cell monolayer under the microfluidic device under con-stant flow conditions was determined by light microscopy. TheRBC adherence strength was determined by progressively in-creasing the shear rate from 0.5 dyne/cm2 to 5 dyne/cm2. Glyco-calyx shedding in the endothelial monolayer and in fresh RBCsor those stored less than 14 days and greater than 21 days wasassessed by measuring both syndecan-1 (Syn-1) release andhyaluronic acid (HLA) present in cell supernatants. Glycocalyxinjury was also assessed in HUVEC and RBC by staining withFluorescein isothiocyante conjugated wheat germ agglutinin(FITC-WGA; Sigma Aldrich, St. Louis, MO) antibody whichbinds to N-acetyl neuraminic acid and N-acetyl glucosamineresidues of proteoglycans and glycoproteins present in theglycocalyx and visualizing the glycocalyx using a fluorescentmicroscope. Image analysis for quantification of glycocalyxthickness was accomplished using Volocity software.
RBC AdhesionFresh RBC, less than 14-day stored and longer than
21-day stored RBC were added to the perfusate and allowed to
© 2019 American Association for the Surgery of Trauma.
ealth, Inc. All rights reserved.
J Trauma Acute Care SurgVolume 86, Number 6 Diebel and Liberati
flow through the microfluidic device at sequentially increas-ing shear rates of 0.5 dyne/cm2 to 5 dyne/cm2. Flow of theRBC through the microfluidic device at each increasing shearrate was stopped after 5 minutes, and adherent cells werephotographed and counted using the Zeiss Observer SpinningDisk Confocal Microscope (Microscopy, Imaging and Cytometrycore facility atWayne State University, Detroit, MI). NonadherentRBCs were removed by washing the monolayer with PBS 2�(shear rate of 0.5 dyne/cm2 for 1 minute to wash).
Syn-1 and HLA AnalysisQuantitative measurement of syndecan protein and
HLA shed by HUVEC into the supernatants was accomplishedusing the Syn-1 human ELISA kit (Abcam, Cambridge, MA)and the hyaluronic immunoassay kit (from R & D Systems,Inc., Minneapolis, MN), respectively. Standards and unknownsamples are added to the microplate wells, and assay procedureswere followed. The optical density is determined using a micro-plate reader set to 450 nm, and the concentration of Syn-1 andHLA in the supernatants is calculated using a standard curve.
Figure 1. (A) Effect of HR and Epi on HUVEC glycocalyx layer. HUVECHR and Epi. Pictures were taken with a Leica TCS SP5 inverted fluoresthickness. (B) Effect of HR and Epi on HUVEC glycocalyx thickness. Thand analyzed using Volocity cellular imaging and analysis software to
© 2019 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer H
The sensitivity of the Syn-1 and HLA ELISAs are 5 pg/mLand 10 pg/mL, respectively.
Fluorescent Imaging and Thickness of GlycocalyxHuman umbilical vein endothelial cells were cultured in
endothelial cell growth medium supplemented by growth factors(EGM-2 BulletKit) Lonza. Before cell seeding, micro channelswere coated with human fibronectin (100 μg/mL; Fisher Scien-tific) for 1 hour at room temperature. The HUVEC suspensionswere seeded into the outlet wells of a 48-well BioFlux plate andinfused into the microchannel network using the BioFlux 200system (Fluxion Biosciences, Inc.). Cells were cultured for72 hours with complete media under flow conditions (shearforce of 1 dyne/cm2) or static conditions. Live cell stainingwas performed inside the microfluidic channels using WGAconjugated with FITC (Sigma). Briefly, endothelial cell culturestreated with epinephrine + HR or standard media had FITC-WGA infused into the microchannel network using the BioFlux200 system, and cells were allowed to incubate for 30 minutes.The cells were washed two times, and fresh culture mediumwas added, and cells were examined under a fluorescent
glycocalyx was stained with FITC-WGA antibody after exposure tocent microscope and xyz image stacks analyzed to calculateree-dimensional XYZ image stacks were acquired and processedassess glycocalyx thickness by measuring fluorescent intensity.
945
ealth, Inc. All rights reserved.
Diebel and LiberatiJ Trauma Acute Care Surg
Volume 86, Number 6
microscope. In a separate series of experiments, RBC glycoca-lyx thickness and fluorescence intensity measurements of theglycocalyx were also determined. Briefly, RBC were resus-pended and incubated in PBS/1% bovine serum albumin con-taining FITC-WGA for 30 minutes at 37°C. The RBC weresubsequently centrifuged (1,400g for 10minutes), and the super-natant removed. RBCs were resuspended in PBS and centri-fuged two more times to remove excess FITC-WGA antibody.Red blood cells were subsequently mounted on a slide with cov-erslip and imaged using a Leica TCS SP5 inverted fluorescentmicroscope with a 63� oil objective. Further image analysiswas performed usingVolocity software at theMicroscopy, Imagingand Cytometry core facility at Wayne State University (Detroit,MI). Measurement of glycocalyx thickness was achieved byXYZ image stacks of the endothelial cell layer using a LeicaTCS SP5 microscope and a 20� objective.
Statistical AnalysisAn analysis of variance with a post hoc Tukey test was
used to analyze the data. Statistical significance was inferred atp values less than 0.05. All data are expressed as mean ± SD.
Figure 2. (A) Effect of storage duration on RBC glycocalyx. The glycocusing an FITC-WGA antibody and image analysis performed using flufluorescence intensity measurement of RBC glycocalyx. Fluorescence i14 days and greater than 21 days. RBC glycocalyx was stained with FITand image analysis performed using velocity software.
946
Copyright © 2019 Wolters Kluwer H
RESULTS
The composition of the anticoagulant-preservative solu-tion for RBCs obtained from the blood bank was citrate phos-phate dextrose. Red blood cell additive solutions includedAS-1 and AS-3. The range of days in storage for the less than14-day storage group was 7 days to 13 days. The range forthe longer than 21-day storage group was 25 days to 38 days.
Endothelial glycocalyx visualized using FITC-labeledWGA demonstrated decreased thickness in the eGC layer after ex-posure to hypoxia-reoxygenation (H/R) and Epi. Glycocalyx thick-ness was 41.2 ± 4.6 in the control group and 13.9 ± 2.3 in theH/R + Epi group (p < 0.05) (Figs. 1A and B). Fluorescentintensity of the EC glycocalyx was also measured and wasreduced from 265.3 ± 19.6 in the HUVEC control to 143.4 ± 18.5in HUVEC exposed to both H/R and Epi (p < 0.05).
The effect of storage on the RBC glycocalyx is shown inFigures 2A and B. Fluorescence intensity of the RBC glycocalyxis related to its thickness. The highest intensity was noted in thefresh RBC group with progressive decline in the less than14-day and longer than 21-day RBC storage groups (p < 0.05).
alyx of fresh, <14-day stored and >21-day stored RBCwas stainedorescence microscope. (B) The effect of storage duration onntensity measurements of glycocalyx on RBCs stored for less thanC-WGA antibody and pictures takenwith fluorescent microscope
© 2019 American Association for the Surgery of Trauma.
ealth, Inc. All rights reserved.
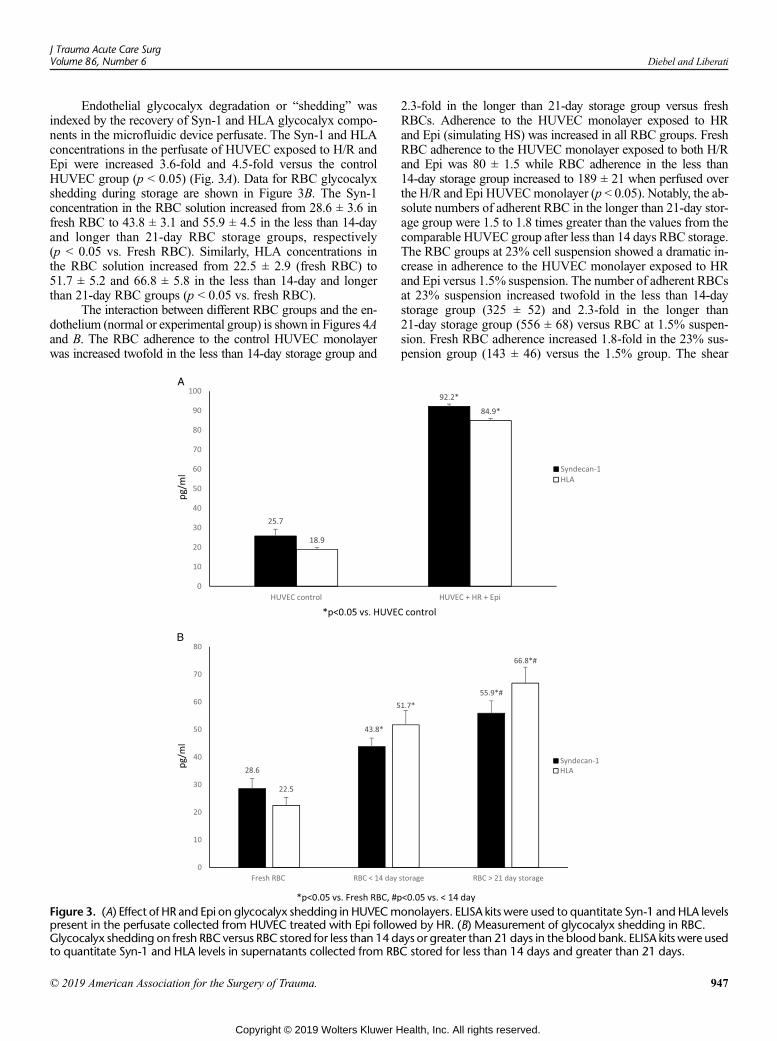
J Trauma Acute Care SurgVolume 86, Number 6 Diebel and Liberati
Endothelial glycocalyx degradation or “shedding” wasindexed by the recovery of Syn-1 and HLA glycocalyx compo-nents in the microfluidic device perfusate. The Syn-1 and HLAconcentrations in the perfusate of HUVEC exposed to H/R andEpi were increased 3.6-fold and 4.5-fold versus the controlHUVEC group (p < 0.05) (Fig. 3A). Data for RBC glycocalyxshedding during storage are shown in Figure 3B. The Syn-1concentration in the RBC solution increased from 28.6 ± 3.6 infresh RBC to 43.8 ± 3.1 and 55.9 ± 4.5 in the less than 14-dayand longer than 21-day RBC storage groups, respectively(p < 0.05 vs. Fresh RBC). Similarly, HLA concentrations inthe RBC solution increased from 22.5 ± 2.9 (fresh RBC) to51.7 ± 5.2 and 66.8 ± 5.8 in the less than 14-day and longerthan 21-day RBC groups (p < 0.05 vs. fresh RBC).
The interaction between different RBC groups and the en-dothelium (normal or experimental group) is shown in Figures 4Aand B. The RBC adherence to the control HUVEC monolayerwas increased twofold in the less than 14-day storage group and
Figure 3. (A) Effect of HR and Epi on glycocalyx shedding in HUVECmpresent in the perfusate collected from HUVEC treated with Epi followGlycocalyx shedding on fresh RBC versus RBC stored for less than 14 dto quantitate Syn-1 and HLA levels in supernatants collected from RB
© 2019 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer H
2.3-fold in the longer than 21-day storage group versus freshRBCs. Adherence to the HUVEC monolayer exposed to HRand Epi (simulating HS) was increased in all RBC groups. FreshRBC adherence to the HUVEC monolayer exposed to both H/Rand Epi was 80 ± 1.5 while RBC adherence in the less than14-day storage group increased to 189 ± 21 when perfused overthe H/R and Epi HUVECmonolayer (p < 0.05). Notably, the ab-solute numbers of adherent RBC in the longer than 21-day stor-age group were 1.5 to 1.8 times greater than the values from thecomparable HUVEC group after less than 14 days RBC storage.The RBC groups at 23% cell suspension showed a dramatic in-crease in adherence to the HUVEC monolayer exposed to HRand Epi versus 1.5% suspension. The number of adherent RBCsat 23% suspension increased twofold in the less than 14-daystorage group (325 ± 52) and 2.3-fold in the longer than21-day storage group (556 ± 68) versus RBC at 1.5% suspen-sion. Fresh RBC adherence increased 1.8-fold in the 23% sus-pension group (143 ± 46) versus the 1.5% group. The shear
onolayers. ELISA kits were used to quantitate Syn-1 and HLA levelsed by HR. (B) Measurement of glycocalyx shedding in RBC.ays or greater than 21 days in the blood bank. ELISA kits were usedC stored for less than 14 days and greater than 21 days.
947
ealth, Inc. All rights reserved.
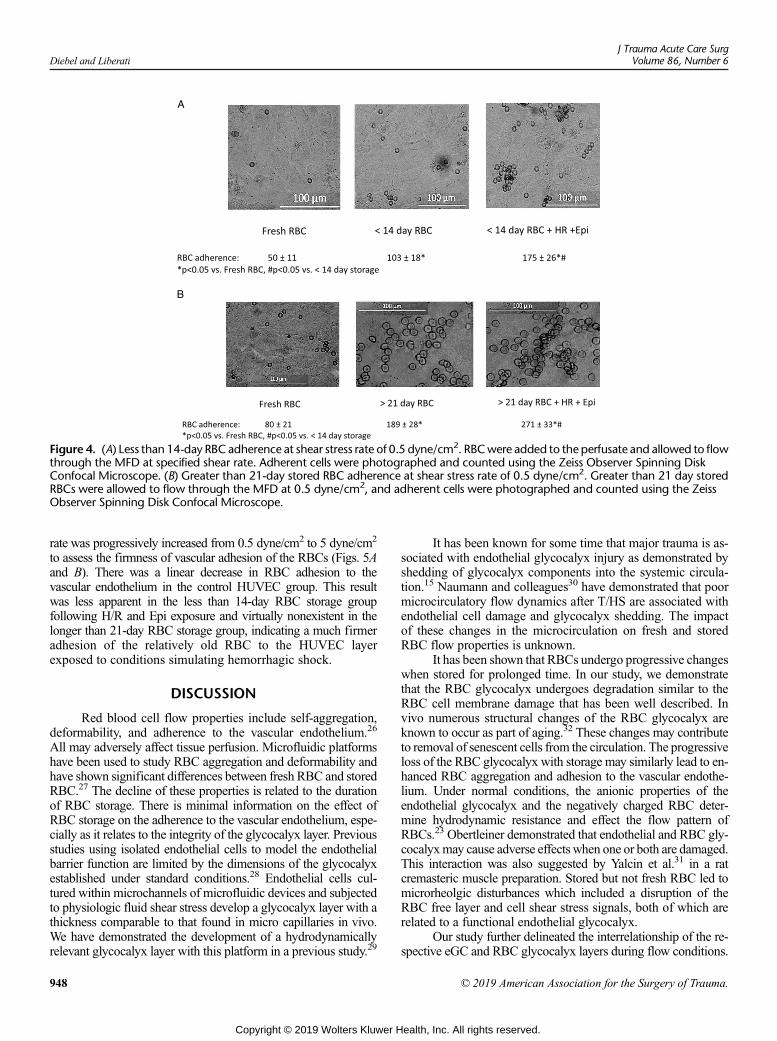
Figure 4. (A) Less than 14-day RBC adherence at shear stress rate of 0.5 dyne/cm2. RBCwere added to the perfusate and allowed to flowthrough the MFD at specified shear rate. Adherent cells were photographed and counted using the Zeiss Observer Spinning DiskConfocal Microscope. (B) Greater than 21-day stored RBC adherence at shear stress rate of 0.5 dyne/cm2. Greater than 21 day storedRBCs were allowed to flow through the MFD at 0.5 dyne/cm2, and adherent cells were photographed and counted using the ZeissObserver Spinning Disk Confocal Microscope.
Diebel and LiberatiJ Trauma Acute Care Surg
Volume 86, Number 6
rate was progressively increased from 0.5 dyne/cm2 to 5 dyne/cm2
to assess the firmness of vascular adhesion of the RBCs (Figs. 5Aand B). There was a linear decrease in RBC adhesion to thevascular endothelium in the control HUVEC group. This resultwas less apparent in the less than 14-day RBC storage groupfollowing H/R and Epi exposure and virtually nonexistent in thelonger than 21-day RBC storage group, indicating a much firmeradhesion of the relatively old RBC to the HUVEC layerexposed to conditions simulating hemorrhagic shock.
DISCUSSION
Red blood cell flow properties include self-aggregation,deformability, and adherence to the vascular endothelium.26
All may adversely affect tissue perfusion. Microfluidic platformshave been used to study RBC aggregation and deformability andhave shown significant differences between fresh RBC and storedRBC.27 The decline of these properties is related to the durationof RBC storage. There is minimal information on the effect ofRBC storage on the adherence to the vascular endothelium, espe-cially as it relates to the integrity of the glycocalyx layer. Previousstudies using isolated endothelial cells to model the endothelialbarrier function are limited by the dimensions of the glycocalyxestablished under standard conditions.28 Endothelial cells cul-tured within microchannels of microfluidic devices and subjectedto physiologic fluid shear stress develop a glycocalyx layer with athickness comparable to that found in micro capillaries in vivo.We have demonstrated the development of a hydrodynamicallyrelevant glycocalyx layer with this platform in a previous study.29
948
Copyright © 2019 Wolters Kluwer H
It has been known for some time that major trauma is as-sociated with endothelial glycocalyx injury as demonstrated byshedding of glycocalyx components into the systemic circula-tion.15 Naumann and colleagues30 have demonstrated that poormicrocirculatory flow dynamics after T/HS are associated withendothelial cell damage and glycocalyx shedding. The impactof these changes in the microcirculation on fresh and storedRBC flow properties is unknown.
It has been shown that RBCs undergo progressive changeswhen stored for prolonged time. In our study, we demonstratethat the RBC glycocalyx undergoes degradation similar to theRBC cell membrane damage that has been well described. Invivo numerous structural changes of the RBC glycocalyx areknown to occur as part of aging.32 These changes may contributeto removal of senescent cells from the circulation. The progressiveloss of the RBC glycocalyx with storage may similarly lead to en-hanced RBC aggregation and adhesion to the vascular endothe-lium. Under normal conditions, the anionic properties of theendothelial glycocalyx and the negatively charged RBC deter-mine hydrodynamic resistance and effect the flow pattern ofRBCs.23 Obertleiner demonstrated that endothelial and RBC gly-cocalyxmay cause adverse effectswhen one or both are damaged.This interaction was also suggested by Yalcin et al.31 in a ratcremasteric muscle preparation. Stored but not fresh RBC led tomicrorheolgic disturbances which included a disruption of theRBC free layer and cell shear stress signals, both of which arerelated to a functional endothelial glycocalyx.
Our study further delineated the interrelationship of the re-spective eGC and RBC glycocalyx layers during flow conditions.
© 2019 American Association for the Surgery of Trauma.
ealth, Inc. All rights reserved.
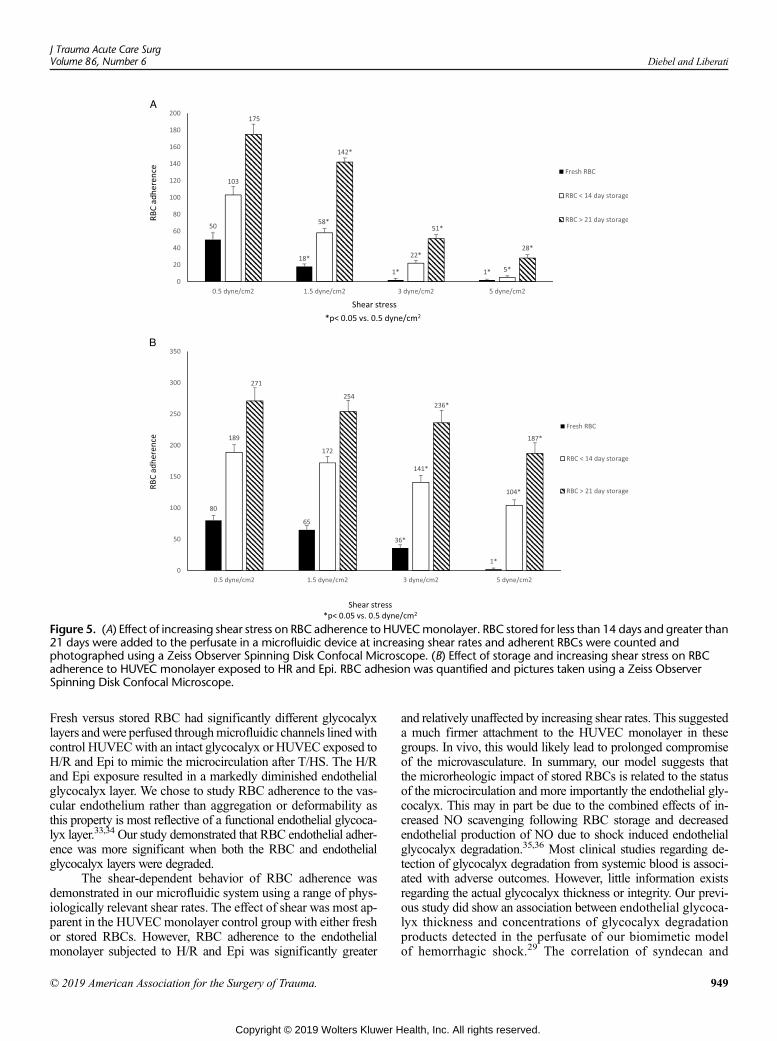
Figure 5. (A) Effect of increasing shear stress on RBC adherence to HUVECmonolayer. RBC stored for less than 14 days and greater than21 days were added to the perfusate in a microfluidic device at increasing shear rates and adherent RBCs were counted andphotographed using a Zeiss Observer Spinning Disk Confocal Microscope. (B) Effect of storage and increasing shear stress on RBCadherence to HUVEC monolayer exposed to HR and Epi. RBC adhesion was quantified and pictures taken using a Zeiss ObserverSpinning Disk Confocal Microscope.
J Trauma Acute Care SurgVolume 86, Number 6 Diebel and Liberati
Fresh versus stored RBC had significantly different glycocalyxlayers andwere perfused throughmicrofluidic channels linedwithcontrol HUVECwith an intact glycocalyx or HUVEC exposed toH/R and Epi to mimic the microcirculation after T/HS. The H/Rand Epi exposure resulted in a markedly diminished endothelialglycocalyx layer. We chose to study RBC adherence to the vas-cular endothelium rather than aggregation or deformability asthis property is most reflective of a functional endothelial glycoca-lyx layer.33,34 Our study demonstrated that RBC endothelial adher-ence was more significant when both the RBC and endothelialglycocalyx layers were degraded.
The shear-dependent behavior of RBC adherence wasdemonstrated in our microfluidic system using a range of phys-iologically relevant shear rates. The effect of shear was most ap-parent in the HUVECmonolayer control group with either freshor stored RBCs. However, RBC adherence to the endothelialmonolayer subjected to H/R and Epi was significantly greater
© 2019 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer H
and relatively unaffected by increasing shear rates. This suggesteda much firmer attachment to the HUVEC monolayer in thesegroups. In vivo, this would likely lead to prolonged compromiseof the microvasculature. In summary, our model suggests thatthe microrheologic impact of stored RBCs is related to the statusof the microcirculation and more importantly the endothelial gly-cocalyx. This may in part be due to the combined effects of in-creased NO scavenging following RBC storage and decreasedendothelial production of NO due to shock induced endothelialglycocalyx degradation.35,36 Most clinical studies regarding de-tection of glycocalyx degradation from systemic blood is associ-ated with adverse outcomes. However, little information existsregarding the actual glycocalyx thickness or integrity. Our previ-ous study did show an association between endothelial glycoca-lyx thickness and concentrations of glycocalyx degradationproducts detected in the perfusate of our biomimetic modelof hemorrhagic shock.29 The correlation of syndecan and
949
ealth, Inc. All rights reserved.

Diebel and LiberatiJ Trauma Acute Care Surg
Volume 86, Number 6
other glycocalyx degradation products with microvascularglycocalyx thickness was also shown in a rodent model per-formed by Torres Filho and colleagues.37
There are several limitations to our study. Two diluteRBC solutions were used to quantitate RBC adherence to theendothelium. Viscosity has been shown to effect RBC flowproperties which may not be significant when using diluteRBC solutions. Second, other blood elements, including leuko-cytes, platelets, and plasma, may impact RBC vascular adher-ence and were not included in the current study. Finally, therectangular geometric design of the microchannels in ourmicrofluidic plates do not recapitulate the complex branchingpattern of vessels in the microcirculation, which may also effectRBC flow properties.
There are a number of other potential uses of ourmicrofluidic system to study RBC-endothelial interactions un-der flow conditions. These include assessment of the efficacyof current and future RBC storage solutions and RBC rejuvena-tion strategies.38,39 In addition, it may provide useful informa-tion regarding the flow properties of cryopreserved RBC whenexposed to both normal and perturbed endothelial surfaces.40
The potential role of RBC microparticles in our study is un-known. Although microparticles including those from RBCsare normally continuously shed into the circulation, they are alsoproduced during processing and storage of blood for transfusion.Because they may adhere to vascular endothelium, the impact ofRBC microparticles in normal and perturbed microvasculature isunder investigation in our laboratory.41,42
Trauma-related injury to the glycocalyx and endothelialvascular barrier occurs early after injury and is related to shockseverity.17,43 The duration of the vascular barrier dysfunction isunknown. In vivo data suggest that recovery time of the glycoca-lyx endothelial barrier may require 5 days to 7 days.44 Spinellaet al.45 have shown that use of fresh whole blood may be optimalfor the early resuscitation of the patient with significant hemor-rhage. This may in part be due to the improved perfusion offeredby fresh RBCs as opposed to standard issue PRBC. Measure-ment of glycocalyx and endothelial parameters may help guidethe use of “young” versus “old” banked blood during this vul-nerable period.30
The microfluidic platform used in our in vitro study of theinteraction of the vascular endothelium with RBCs from freshand blood bank sources suggest that both entities are importantin assessing the impact of the age of stored blood in the abilityto restore microvascular perfusion in the transfusion therapy fol-lowing severe trauma.
AUTHORSHIP
L.N.D. and D.L. made substantial contributions to the conception ordesign of the work; they also conceived and designed the experi-ments. L.N.D. and D.L. analyzed the data. D.L. and L.N.D. drafted the ar-ticle. L.N.D. andD.L. critically revised the article for intellectual content. Allauthors provided final approval of the version to be published.
DISCLOSURE
The authors declare no conflicts of interest.
REFERENCES1. Sparrow RL. Red blood cell storage duration and trauma. Transfus Med Rev.
2015;29(2):120–126.
950
Copyright © 2019 Wolters Kluwer H
2. Spieth PM, Zhang H. Storage injury and blood transfusions in trauma pa-tients. Curr Opin Anaesthesiol. 2018;31(2):234–237.
3. Sowers N, Froese PC, Erdogan M, Green RS. Impact of the age of storedblood on trauma patient mortality: a systematic review. Can J Surg. 2015;58(5):335–342.
4. Garcia-Roa M, Del Carmen Vicente-Ayuso M, Bobes AM, Pedraza AC,Gonzalez-Fernandez A, Martin MP, Saez I, Seghatchian J, Gutierrez L.Red blood cell storage time and transfusion: current practice, concerns andfuture perspectives. Blood Transfus. 2017;15(3):222–231.
5. Rygard SL, Jonsson AB, Madsen MB, Perner A, Holst LB, Johansson PI,Wetterslev J. Effects of shorter versus longer storage time of transfused redblood cells in adult ICU patients: a systematic review with meta-analysisand Trial sequential analysis. Intensive Care Med. 2018;44(2):204–217.
6. Putter JS, Seghatchian J. Cumulative erythrocyte damage in blood storageand relevance to massive transfusions: selective insights into serial morpho-logical and biochemical findings. Blood Transfus. 2017;15(4):348–356.
7. Weinberg JA, McGwin G Jr., VandrommeMJ, Marques MB,Melton SM,Reiff DA, Kerby JD, Rue LW 3rd. Duration of red cell storage influencesmortality after trauma. J Trauma. 2010;69(6):1427–1431; discussion1431-1422.
8. van de Watering LM. Effects of red blood cell storage in heavily transfusedpatients. Curr Opin Anaesthesiol. 2013;26(2):204–207.
9. Barshtein G, Pries AR, Goldschmidt N, Zukerman A, Orbach A, Zelig O,Arbell D, Yedgar S. Deformability of transfused red blood cells is a potentdeterminant of transfusion-induced change in recipient's blood flow. Micro-circulation. 2016;23(7):479–486.
10. McClatchey PM, Schafer M, Hunter KS, Reusch JE. The endothelial glyco-calyx promotes homogenous blood flow distribution within the microvascu-lature. Am J Physiol Heart Circ Physiol. 2016;311(1):H168–H176.
11. Cabrales P, Vázquez BY, Tsai AG, IntagliettaM.Microvascular and capillaryperfusion following glycocalyx degradation. J Appl Physiol (1985). 2007;102(6):2251–2259.
12. Yao Y, Rabodzey A, Dewey CF Jr. Glycocalyx modulates the motility andproliferative response of vascular endothelium to fluid shear stress. Am JPhysiol Heart Circ Physiol. 2007;293(2):H1023–H1030.
13. Yalcin O, Ortiz D, Tsai AG, Johnson PC, Cabrales P.Microhemodynamic ab-errations created by transfusion of stored blood. Transfusion. 2014;54(4):1015–1027.
14. Tuma M, Canestrini S, Alwahab Z, Marshall J. Trauma and endothelial gly-cocalyx: the microcirculation helmet? Shock. 2016;46(4):352–357.
15. Rahbar E, Cardenas JC, Baimukanova G, et al. Endothelial glycocalyx shed-ding and vascular permeability in severely injured trauma patients. J TranslMed. 2015;13:117.
16. Halbgebauer R, Braun CK, Denk S, et al. Hemorrhagic shock drives glyco-calyx, barrier and organ dysfunction early after polytrauma. J Crit Care.2018;44:229–237.
17. Johansson PI, Stensballe J, Ostrowski SR. Shock induced endotheliopathy(SHINE) in acute critical illness—a unifying pathophysiologic mechanism.Crit Care. 2017;21(1):25.
18. Chin-Yee IH, Gray-Statchuk L,Milkovich S, Ellis CG. Transfusion of storedred blood cells adhere in the rat microvasculature. Transfusion. 2009;49(11):2304–2310.
19. Anniss AM, Sparrow RL. Storage duration and white blood cell content ofred blood cell (RBC) products increases adhesion of stored RBCs to endo-thelium under flow conditions. Transfusion. 2006;46(9):1561–1567.
20. Anniss AM, Sparrow RL. Variable adhesion of different red blood cell prod-ucts to activated vascular endothelium under flow conditions. Am J Hematol.2007;82(6):439–445.
21. Mazor R, Schmid-Schönbein GW. Proteolytic receptor cleavage in the path-ogenesis of blood rheology and co-morbidities in metabolic syndrome. Earlyforms of autodigestion. Biorheology. 2015;52(5–6):337–352.
22. Mohanty JG, Nagababu E, Rifkind JM. Red blood cell oxidative stress im-pairs oxygen delivery and induces red blood cell aging. Front Physiol.2014;5:84.
23. Oberleithner H. Vascular endothelium leaves fingerprints on the surface oferythrocytes. Pflugers Arch. 2013;465(10):1451–1458.
24. Relevy H, Koshkaryev A, Manny N, Yedgar S, Barshtein G. Blood banking-induced alteration of red blood cell flow properties. Transfusion. 2008;48(1):136–146.
© 2019 American Association for the Surgery of Trauma.
ealth, Inc. All rights reserved.
J Trauma Acute Care SurgVolume 86, Number 6 Diebel and Liberati
25. Mehri R, Mavriplis C, Fenech M. Controlled microfluidic environment for dy-namic investigation of red blood cell aggregation. J Vis Exp. 2015;(100):e52719.
26. Guo Q, Duffy SP, Matthews K, Santoso AT, Scott MD, Ma H. Microfluidicanalysis of red blood cell deformability. J Biomech. 2014;47(8):1767–1776.
27. KaulDK, Koshkaryev A, Artmann G, Barshtein G, Yedgar S. Additive ef-fect of red blood cell rigidity and adherence to endothelial cells in inducing vas-cular resistance. Am J Physiol Heart Circ Physiol. 2008;295(4):H1788–H1793.
28. Potter DR,Damiano ER. The hydrodynamically relevant endothelial cell gly-cocalyx observed in vivo is absent in vitro. Circ Res. 2008;102(7):770–776.
29. Diebel LN,Martin JV, Liberati DM.Microfluidics: a high-throughput systemfor the assessment of the endotheliopathy of trauma and the effect of timingof plasma administration on ameliorating shock-associated endothelial dys-function. J Trauma Acute Care Surg. 2018;84(4):575–582.
30. Naumann DN, Hazeldine J, Midwinter MJ, Hutchings SD, Harrison P. Poormicrocirculatory flow dynamics are associated with endothelial cell damageand glycocalyx shedding after traumatic hemorrhagic shock. J Trauma AcuteCare Surg. 2018;84(1):81–88.
31. Yalcin O, Jani VP, Johnson PC, Cabrales P. Implications enzymatic degradationof the endothelial glycocalyx on the microvascular hemodynamics and the arte-riolar red cell free layer of the rat cremaster muscle. Front Physiol. 2018;9:168.
32. Neu B, Sowemimo-Coker SO, Meiselman HJ. Cell-cell affinity of senescenthuman erythrocytes. Biophys J. 2003;85:75–84.
33. Yedgar S, Kaul DK, Barshtein G. RBC adhesion tovascular endothelial cells:more potent than RBC aggregation in inducing circulatory disorders.Micro-circulation. 2008;15(7):581–583.
34. Sherwood JM, Dusting J, Kaliviotis E, Balabani S. The effect of red bloodcell aggregation on velocity and cell-depleted layer characteristics of bloodin a bifurcating microchannel. Biomicrofluidics. 2012;6(2):24119.
35. Stapley R, Owusu BY, Brandon A, et al. Erythrocyte storage increases ratesof NO and nitrite scavenging: implications for transfusion-related toxicity.Biochem J. 2012;446(3):499–508.
36. Yen W, Cai B, Yang J, Zhang L, Zeng M, Tarbell JM, Fu BM. Endothelialsurface glycocalyx can regulate flow-induced nitric oxide production inmicrovessels in vivo. PLoS One. 2015;10(1):e0117133.
37. Torres Filho IP, Torres LN, Salgado C, Dubick MA. Plasma syndecan-1 andheparan sulfate correlate with microvascular glycocalyx degradation inhemorrhaged rats after different resuscitation fluids. Am J Physiol Heart CircPhysiol. 2016;310:H1468–H1478.
38. SparrowRL. Time to revisit red blood cell additive solutions and storage con-ditions: a role for “omics” analyses. Blood Transfus. 2012;10(Suppl 2):s7–s11.
39. Koshkaryev A, Zelig O, Manny N, Yedgar S, Barshtein G. Rejuvenationtreatment of stored red blood cells reverses storage-induced adhesion to vas-cular endothelial cells. Transfusion. 2009;49(10):2136–2143.
40. Chang A, Kim Y, Hoehn R, Jernigan P, Pritts T. Cryopreserved packed redblood cells in surgical patients: past, present, and future. Blood Transfus.2017;15(4):341–347.
41. Said AS, Rogers SC, Doctor A. Physiologic impact of circulating RBC mi-croparticles upon blood-vascular interactions. Front Physiol. 2018;8:1120.
42. Burnouf T, Chou ML, Goubran H, Cognasse F, Garraud O, Seghatchian J.An overview of the role of microparticles/microvesicles in blood components:are they clinically beneficial or harmful? Transfus Apher Sci. 2015;53:137–145.
43. Naumann DN, Hazeldine J, Davies DJ, Bishop J, Midwinter MJ, Belli A,Harrison P, Lord JM. Endotheliopathy of trauma is an on-scene phenome-non, and is associated with multiple organ dysfunction syndrome: a prospec-tive observational study. Shock. 2018;49(4):420–428.
44. Potter DR, Jiang J, Damiano ER. The recovery time course of the endothelialcell glycocalyx in vivo and its implications in vitro.Circ Res. 2009;104(11):1318–1325.
45. Spinella PC, Doctor A. Role of transfused red blood cells for shock andcoagulopathy within remote damage control resuscitation. Shock. 2014;41(Suppl 1):30–34.
DISCUSSIONROSEMARY A. KOZAR, M.D., Ph.D. (Baltimore,
Maryland): Good afternoon. The authors have continued theirinvestigations into the endothelial cell glycocalyx using theirin-vitro microfluidic system.
© 2019 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer H
In the current study the authors examined the interactionsof endothelial cells and red blood cells under stress conditionswith the hypotheses that older red cells would adversely affectthis interaction.
The authors confirmed changes in glycocalyx thickness aswell as syndecan-1 and hyaluronic acid shedding in activated en-dothelial cells and, interestingly, demonstrated changes in redblood cell glycocalyx with age of red cells.
They then examined red cell adherence in their activatedendothelial cells and found there to be an increase in RBC adher-ence as age of the red cells increased.
I must admit I was not aware that therewas a glycocalyx inred blood cells. I was wondering how the glycocalyx in red cellsdiffered from that of the endothelial cell? What is the function ofthe red cell glycocalyx?
Second, the authors demonstrated changes in endothelialcell glycocalyx when the cells were activated and in red cell gly-cocalyx with duration of storage. But do you have evidence thatthe increased adherence of the red cells is causally related to thechanges in the glycocalyx?
Third, as a control, did you look at the red cell adherencewhen cells were stimulated with the fresh red blood cells?
You showed us data for the 14 days and the 21 days but asa control did you look at how the fresh red blood cells were af-fected in the stimulated endothelial cells?
Lastly, could you hypothesize if the degree of red cell ad-herence that you demonstrate is sufficient to cause microvascu-lar thromboses and subsequent organ damage that we see insome of these clinical studies?
Thank you. I appreciate the privilege of the presentation.Lawrence Diebel M.D. (Detroit, Michigan): The Gly-
cocalyx is a part of the red blood cell membrane. Storage of redblood cells is known to cause compositional changes of the redblood cell membrane which increase with time in storage.
Thus the results of this experiment add new information tothe existing data regarding the effects of storage on red bloodcells. Also the loss of the red blood cell glycocalyx does occurwith senescence in vivo, and contributes to capture and removalin the splenic vasculature.
Regarding metabolic effects of storage, this is an entirelydifferent storys. What I can tell you in studies we are doing com-paring red blood cells in the obese with the metabolic syndromethat there are differences compared to red blood cells from non-obese patients. So this is something wewill look at in the future.
The three different blood groups, fresh blood, bankedblood with storage less than 14 days, or greater than 21 dayswere all perfused with normal endothelium and endotheliumsubjected to biomimetic conditions of shock...so all group var-iations were performed.
We use a hematocrit of 1.5% in these studies and have re-cently completed studies at a hematocrit of 21%. The lower he-matocrit makes it easier to accurately count individual red bloodcells. The studies with the higher hematocrit lead to signifi-cantly higher number of red blood cells adherent to the endothe-lium. And each microfluidic channel may be thought of asrepresenting a single microcirculatory unit in vivo, I believethese results would be clinically relevant.
951
ealth, Inc. All rights reserved.

AAST 2018 PODIUM PAPER
Should they stay or should they go? Who benefits from interfacilitytransfer to a higher-level trauma center following initial
presentation at a lower-level trauma center
Tessa Adzemovic, Thomas Murray, PhD, Peter Jenkins, MD, Julie Ottosen, MD, Uroghupatei Iyegha, MD,Krishnan Raghavendran, MD, Lena M. Napolitano, MD, Mark R. Hemmila, MD, Jonathan Gipson, MD,
Pauline Park, MD, and Christopher J. Tignanelli, MD, Minneapolis, Minnesota
Sub
Fro
Thi
Ad
DO
95
BACKGROUND: I
mitted: September 7, 2018, Re2019, Published online: Marchm the University ofMichiganMeof Biostatistics (T.M.), UnivDepartment of Surgery (P.J.), Inof Surgery (J.O., C.J.T.), UniDepartment of Surgery (J.O.,Robbinsdale, Minnesota, DeparMinnesota; Department of SurMichigan, Ann Arbor, MichigaUniversity of Minnesota, Mins study was presented as a pleAmerican Association for the2018, in San Diego, Californiadress for reprints: Christopher J.of Minnesota, 420 Delaware [email protected].
I: 10.1097/TA.00000000000022
2
nterfacility transfer of patients from Level III/IV to Level I/II (tertiary) trauma centers has been associated with improved out-comes. However, little data are available classifying the specific subsets of patients that derive maximal benefit from transfer toa tertiary trauma center. Drawbacks to transfer include increased secondary overtriage. Here, we ask which injury patterns are as-sociated with improved survival following interfacility transfer.
METHODS: D
ata from the National Trauma Data Bank was utilized. Inclusion criteria were adults (≥16 years). Patients with Injury SeverityScore of 10 or less or thosewho arrived with no signs of life were excluded. Patients were divided into two cohorts: those admittedto a Level III/IV trauma center versus those transferred into a tertiary trauma center. Multiple imputation was performed for miss-ing values, and propensity scores were generated based on demographics, injury patterns, and disease severity. Using propensityscore–stratified Cox proportional hazards regression, the hazard ratio for time to death was estimated.RESULTS: T
welve thousand five hundred thirty-four (5.2%) were admitted to Level III/IV trauma centers, and 227,315 (94.8%) were trans-ferred to a tertiary trauma center. Patients transferred to a tertiary trauma center had reduced mortality (hazard ratio, 0.69;p < 0.001). We identified that patients with traumatic brain injury with Glasgow Coma Scale score less than 13, pelvic fracture,penetrating mechanism, solid organ injury, great vessel injury, respiratory distress, and tachycardia benefited from interfacilitytransfer to a tertiary trauma center. In this sample, 56.8% of the patients benefitted from transfer. Among those not transferred,49.5% would have benefited from being transferred.CONCLUSION: I
nterfacility transfer is associated with a survival benefit for specific patients. These data support implementation of minimumevidence-based criteria for interfacility transfer. (J Trauma Acute Care Surg. 2019;86: 952–960. Copyright © 2019 American As-sociation for the Surgery of Trauma.)LEVEL OF EVIDENCE: T
herapeutic/Care Management, Level IV. KEYWORDS: I nterfacility transfer; triage; secondary overtriage; undertriage; trauma systems.T he goal of interfacility transfer of severely injured traumapatients is to ensure that patients are at the right place at the
right time to receive safe, reliable, high-quality care. AmericanCollege of Surgeons (ACS)-verified trauma centers voluntarilymaintain four categories (I–IV) of readiness based on the quan-tity of human and material resources at the respective centers.1
vised: December 19, 2018, Accepted: January 2,1, 2019.dical School (T.A.), AnnArbor, Michigan; Divisionersity of Minnesota, Minneapolis, Minnesota;diana University, Indianapolis, Indiana; Departmentversity of Minnesota, Minneapolis, Minnesota;J.G.P., C.J.T.), North Memorial Health Hospital,tment of Surgery (U.I.), Regions Hospital, St. Paul,gery (K.R., L.M.N., M.R.H., P.P.), University ofn; and Institute for Health Informatics (C.J.T.),neapolis, Minnesota.nary presentation at the 77th annual meeting ofSurgery of Trauma Meeting, September 26–29,.Tignanelli,MD, Department of Surgery, Universityt SE, MMC 195, Minneapolis, MN 55455; email:
48
Copyright © 2019 Wolters Kluwer H
Level I and II centers are considered tertiary trauma centersand are expected to have similar clinical outcomes.2 Currentevidence suggests that interfacility transfer of some injuredpatients from Level III/IV trauma centers to Level I/II centersis associated with improved outcomes, including reduction inmortality.3,4
Currently, it is agreed that the decision to transfer shouldbe made based on the patient's clinical status and the facility'savailable resources.1 The advantages are presumed to vary de-pending with the mechanism and severity of injury sustainedby the patient; however, there are limited data regarding whichspecific patients actually derive a mortality benefit frominterfacility transfer.5
In addition, secondary overtriage—patient transfers froma nontertiary trauma center to a tertiary trauma center with alength of stay shorter than 48 hours and not requiring operativeintervention—poses a burden to already saturated tertiary traumacenters and can potentially jeopardize the care of severely injuredpatients at these centers. Studies suggest secondary overtriage oc-curs in approximately 7% to 38% of tertiary trauma transfers,with the majority being patients with head and neck injuries.6–8
The overall lack of benefit data renders clinical practice ambigu-ous, and it continues to vary from center to center.
J Trauma Acute Care SurgVolume 86, Number 6
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 6 Adzemovic et al.
Reliable transfer criteria are essential. Ideal criteria wouldbe sensitive enough to identify all patients who could benefit fromtransfer while simultaneously limiting secondary overtriage. Theobjective of this study was to identify patient-level characteristicsassociated with mortality benefit from transfer from a Level III orIV trauma center to a Level I or II trauma center and to estimatemortality benefit of transfer in a national trauma cohort.
METHODS
Data CollectionThe data source for this study was the ACS National
Trauma Data Bank (NTDB), which is the largest trauma reg-istry in the United States. It includes patient and hospital dataon traumatic injuries and clinical outcomes for more than 700trauma centers.
This study was approved by the University of Minnesotainstitutional review board (STUDY00001489). The need for in-dividual patient consent waswaived, because all data used in thisstudy were already deidentified in the NTDB.
ParticipantsPatient-level data were obtained from the NTDB from
January 1, 2007, through December 31, 2014. The inclusioncriteria were as follows:
– Patients who were initially evaluated at a Level III or IVtrauma center and subsequently admitted to a Level III or IVtrauma center or those who were transferred from a priorhospital's emergency department (ED) to the ED of a LevelI or II trauma center for evaluation and treatment.– Age ≥ 16– At least 1 valid International Classification of Diseases,Ninth Revision, Clinical Modification (ICD-9-CM) traumacode (range, 800–959.9)– Admission to a US trauma center for definitive care– Injury Severity Score (ISS) greater than 10 or missing
Exclusion criteria included patients with no signs of life at initialevaluation ED systolic blood pressure (SBP) = 0, pulse = 0,Glasgow Coma Scale (GCS) score = 3).
AnalysisPatients were divided into two cohorts for subsequent
analysis: those who were initially evaluated at and subsequentlyadmitted to a Level III/IV trauma center versus those who weretransferred from a prior hospital's ED to a Level I/II trauma cen-ter for evaluation and treatment. The amount of missing data forclinically relevant variables was relatively low (mean, 4.1%;range, 0%–28.1%). Multiple Imputation by Chained Equationswas used to impute missing variables.9 Each missing variablewas imputed once following five iterations using predictivemean matching based on full conditional regression modeling.Imputation included patients who were missing ISS (19,466 pa-tients). After imputation, we analyzed the subset with an ISSgreater than 10. There were 6,288 observations with missingISS that received an imputed ISS greater than 10 and were in-cluded in the final analysis.
Injury types of interest included: any traumatic brain injury(TBI, ICD-9: 800.0–804.9, 850.0–854.1, 959.01), severe TBI
© 2019 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer H
(TBI with GCS score < 9), TBI with intracranial bleed (ICD-9:852.0–853.9), TBI with no bleed and GCS score greater than13, any cervical spine (C-spine) injury (ICD-9: 805.0–805.19,806.0–806.19, 839, 952), C-spine injury with spinal cord injury(ICD-9: 806.0–806.19, 839, 952), all solid organ injuries(ICD-9: 864.0–866.9), grade 3 or higher solid organ injury(ICD-9: 864.03, 864.13, 864.04, 864.14, 865.03, 865.13,865.04, 864.14, 866.03, 866.13, 866.04, 866.14), bowel orpancreas injury (ICD-9: 863.0–863.9), femur fracture (ICD-9:820.0–821.9), all pelvis fractures (ICD-9: 808.0–808.9), com-plex pelvic fracture (ICD-9: 808.43, 808.53), rib fractures(ICD-9: 807.0–807.4), hemothorax or pneumothorax (ICD-9:860.0–806.9), penetrating thoracic (ICD-9: 861.0–862.9 withpenetrating mechanism), sternum fracture (ICD-9: 807.2–807.39),thoracic aorta injury (ICD-9: 901.0), subclavian artery injury(ICD-9: 901.1), carotid artery injury (ICD-9: 900–900.03),and major venous injury (ICD-9: 900.1–900.3, 900.81, 902.1).Additional physiologic and demographic parameters were alsoevaluated. Physiologic criteria were evaluated as physiologicthresholds have already been identified for a minimum fulltrauma activation (e.g., GCS score < 9 and SBP < 90) and arehighly associated with poor clinical outcomes.10We specificallyevaluated: age, ED respiratory rate, ED pulse, ED SBP, total GCSscore, and ISS. The physiologic criteria analyzed were based onthe most aberrant recorded value during ED resuscitation.
Our primary outcome was time from admission to deathwith censoring at hospital discharge.
Statistical MethodsA causal analysis for the survival benefit of interfacility
transfer was performed using the imputed data set.11 This anal-ysis consisted of three aspects: (i) fitting a propensity scoremodel, (ii) constructing propensity score strata, and (iii) fittingoutcome models using propensity score–stratified Cox propor-tional hazards regression wherein each stratum is allowed itsown nonparametric baseline hazard function.
A logistic additive model was used to estimate the propen-sity score (i.e., the probability of being transferred given patientcharacteristics). This model included the following variables:demographic (age, race, and sex), injury severity, ED SBP, EDpulse, ED respiratory rate, ED oxygen saturation, ED temper-ature, ISS, predicted mortality (using the Trauma MortalityPrediction Model ICD-912), ED-assisted respirations, EDsupplemental oxygen requirements, preinjury drug or alcoholuse, mechanism of injury, GCS score, injury type, and work-related injury. The effect of each continuous variable on thepropensity was modeled with a penalized spline term, whichfacilitates capturing a nonlinear association between the con-tinuous covariate and the propensity score while guardingagainst overfitting by penalizing nonlinear curvature in theresulting estimate, whereas the effect of binary and categori-cal variables were modeled with standard linear terms.13 Al-though the propensity score model included a large numberof covariates, overfitting was not a concern because the num-ber of nontransferred and transferred observations both are farmore than 20 times larger than the number of covariates.14
The propensity score model provided 72% concordanceand 0.048 Brier score.15 Based on the estimated propensityscores, 78 strata were constructed by iteratively grouping
953
ealth, Inc. All rights reserved.
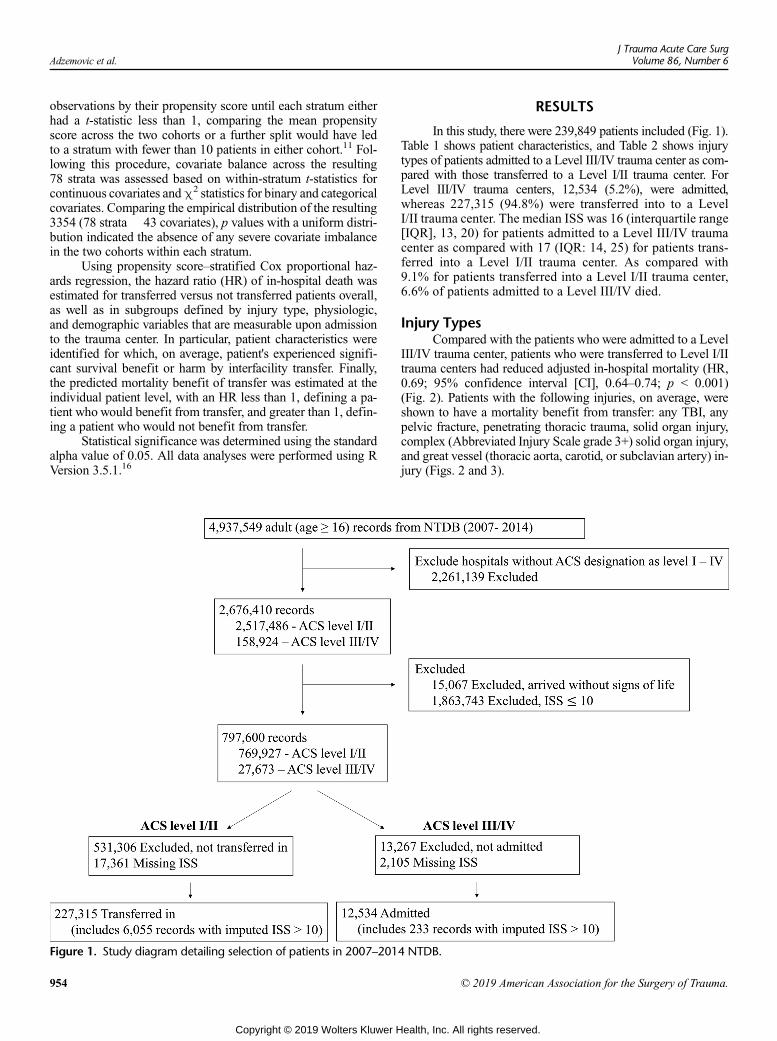
Adzemovic et al.J Trauma Acute Care Surg
Volume 86, Number 6
observations by their propensity score until each stratum eitherhad a t-statistic less than 1, comparing the mean propensityscore across the two cohorts or a further split would have ledto a stratum with fewer than 10 patients in either cohort.11 Fol-lowing this procedure, covariate balance across the resulting78 strata was assessed based on within-stratum t-statistics forcontinuous covariates andχ2 statistics for binary and categoricalcovariates. Comparing the empirical distribution of the resulting3354 (78 strata� 43 covariates), p values with a uniform distri-bution indicated the absence of any severe covariate imbalancein the two cohorts within each stratum.
Using propensity score–stratified Cox proportional haz-ards regression, the hazard ratio (HR) of in-hospital death wasestimated for transferred versus not transferred patients overall,as well as in subgroups defined by injury type, physiologic,and demographic variables that are measurable upon admissionto the trauma center. In particular, patient characteristics wereidentified for which, on average, patient's experienced signifi-cant survival benefit or harm by interfacility transfer. Finally,the predicted mortality benefit of transfer was estimated at theindividual patient level, with an HR less than 1, defining a pa-tient who would benefit from transfer, and greater than 1, defin-ing a patient who would not benefit from transfer.
Statistical significance was determined using the standardalpha value of 0.05. All data analyses were performed using RVersion 3.5.1.16
Figure 1. Study diagram detailing selection of patients in 2007–201
954
Copyright © 2019 Wolters Kluwer H
RESULTS
In this study, there were 239,849 patients included (Fig. 1).Table 1 shows patient characteristics, and Table 2 shows injurytypes of patients admitted to a Level III/IV trauma center as com-pared with those transferred to a Level I/II trauma center. ForLevel III/IV trauma centers, 12,534 (5.2%), were admitted,whereas 227,315 (94.8%) were transferred into to a LevelI/II trauma center. The median ISS was 16 (interquartile range[IQR], 13, 20) for patients admitted to a Level III/IV traumacenter as compared with 17 (IQR: 14, 25) for patients trans-ferred into a Level I/II trauma center. As compared with9.1% for patients transferred into a Level I/II trauma center,6.6% of patients admitted to a Level III/IV died.
Injury TypesCompared with the patients who were admitted to a Level
III/IV trauma center, patients who were transferred to Level I/IItrauma centers had reduced adjusted in-hospital mortality (HR,0.69; 95% confidence interval [CI], 0.64–0.74; p < 0.001)(Fig. 2). Patients with the following injuries, on average, wereshown to have a mortality benefit from transfer: any TBI, anypelvic fracture, penetrating thoracic trauma, solid organ injury,complex (Abbreviated Injury Scale grade 3+) solid organ injury,and great vessel (thoracic aorta, carotid, or subclavian artery) in-jury (Figs. 2 and 3).
4 NTDB.
© 2019 American Association for the Surgery of Trauma.
ealth, Inc. All rights reserved.
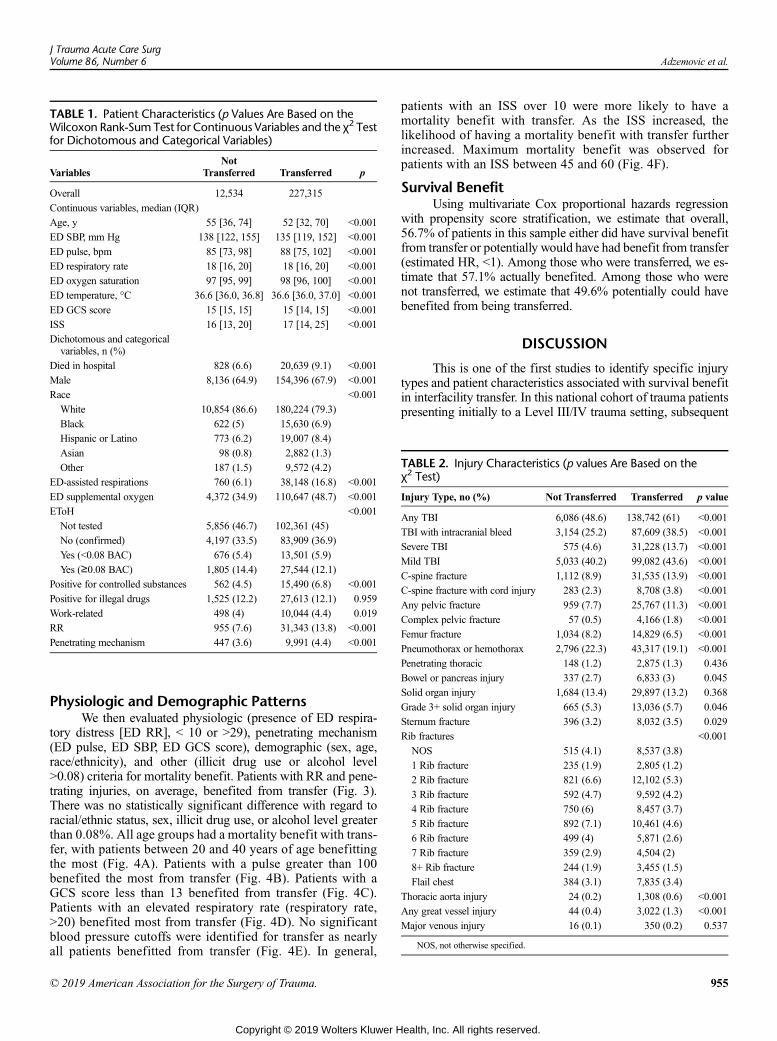
TABLE 1. Patient Characteristics (p Values Are Based on theWilcoxon Rank-Sum Test for Continuous Variables and the χ2 Testfor Dichotomous and Categorical Variables)
VariablesNot
Transferred Transferred p
Overall 12,534 227,315
Continuous variables, median (IQR)
Age, y 55 [36, 74] 52 [32, 70] <0.001
ED SBP, mm Hg 138 [122, 155] 135 [119, 152] <0.001
ED pulse, bpm 85 [73, 98] 88 [75, 102] <0.001
ED respiratory rate 18 [16, 20] 18 [16, 20] <0.001
ED oxygen saturation 97 [95, 99] 98 [96, 100] <0.001
ED temperature, °C 36.6 [36.0, 36.8] 36.6 [36.0, 37.0] <0.001
ED GCS score 15 [15, 15] 15 [14, 15] <0.001
ISS 16 [13, 20] 17 [14, 25] <0.001
Dichotomous and categoricalvariables, n (%)
Died in hospital 828 (6.6) 20,639 (9.1) <0.001
Male 8,136 (64.9) 154,396 (67.9) <0.001
Race <0.001
White 10,854 (86.6) 180,224 (79.3)
Black 622 (5) 15,630 (6.9)
Hispanic or Latino 773 (6.2) 19,007 (8.4)
Asian 98 (0.8) 2,882 (1.3)
Other 187 (1.5) 9,572 (4.2)
ED-assisted respirations 760 (6.1) 38,148 (16.8) <0.001
ED supplemental oxygen 4,372 (34.9) 110,647 (48.7) <0.001
EToH <0.001
Not tested 5,856 (46.7) 102,361 (45)
No (confirmed) 4,197 (33.5) 83,909 (36.9)
Yes (<0.08 BAC) 676 (5.4) 13,501 (5.9)
Yes (≥0.08 BAC) 1,805 (14.4) 27,544 (12.1)
Positive for controlled substances 562 (4.5) 15,490 (6.8) <0.001
Positive for illegal drugs 1,525 (12.2) 27,613 (12.1) 0.959
Work-related 498 (4) 10,044 (4.4) 0.019
RR 955 (7.6) 31,343 (13.8) <0.001
Penetrating mechanism 447 (3.6) 9,991 (4.4) <0.001
TABLE 2. Injury Characteristics (p values Are Based on theχ2 Test)
Injury Type, no (%) Not Transferred Transferred p value
Any TBI 6,086 (48.6) 138,742 (61) <0.001
TBI with intracranial bleed 3,154 (25.2) 87,609 (38.5) <0.001
Severe TBI 575 (4.6) 31,228 (13.7) <0.001
Mild TBI 5,033 (40.2) 99,082 (43.6) <0.001
C-spine fracture 1,112 (8.9) 31,535 (13.9) <0.001
C-spine fracture with cord injury 283 (2.3) 8,708 (3.8) <0.001
Any pelvic fracture 959 (7.7) 25,767 (11.3) <0.001
Complex pelvic fracture 57 (0.5) 4,166 (1.8) <0.001
Femur fracture 1,034 (8.2) 14,829 (6.5) <0.001
Pneumothorax or hemothorax 2,796 (22.3) 43,317 (19.1) <0.001
Penetrating thoracic 148 (1.2) 2,875 (1.3) 0.436
Bowel or pancreas injury 337 (2.7) 6,833 (3) 0.045
Solid organ injury 1,684 (13.4) 29,897 (13.2) 0.368
Grade 3+ solid organ injury 665 (5.3) 13,036 (5.7) 0.046
Sternum fracture 396 (3.2) 8,032 (3.5) 0.029
Rib fractures <0.001
NOS 515 (4.1) 8,537 (3.8)
1 Rib fracture 235 (1.9) 2,805 (1.2)
2 Rib fracture 821 (6.6) 12,102 (5.3)
3 Rib fracture 592 (4.7) 9,592 (4.2)
4 Rib fracture 750 (6) 8,457 (3.7)
5 Rib fracture 892 (7.1) 10,461 (4.6)
6 Rib fracture 499 (4) 5,871 (2.6)
7 Rib fracture 359 (2.9) 4,504 (2)
8+ Rib fracture 244 (1.9) 3,455 (1.5)
Flail chest 384 (3.1) 7,835 (3.4)
Thoracic aorta injury 24 (0.2) 1,308 (0.6) <0.001
Any great vessel injury 44 (0.4) 3,022 (1.3) <0.001
Major venous injury 16 (0.1) 350 (0.2) 0.537
NOS, not otherwise specified.
J Trauma Acute Care SurgVolume 86, Number 6 Adzemovic et al.
Physiologic and Demographic PatternsWe then evaluated physiologic (presence of ED respira-
tory distress [ED RR], < 10 or >29), penetrating mechanism(ED pulse, ED SBP, ED GCS score), demographic (sex, age,race/ethnicity), and other (illicit drug use or alcohol level>0.08) criteria for mortality benefit. Patients with RR and pene-trating injuries, on average, benefited from transfer (Fig. 3).There was no statistically significant difference with regard toracial/ethnic status, sex, illicit drug use, or alcohol level greaterthan 0.08%. All age groups had a mortality benefit with trans-fer, with patients between 20 and 40 years of age benefittingthe most (Fig. 4A). Patients with a pulse greater than 100benefited the most from transfer (Fig. 4B). Patients with aGCS score less than 13 benefited from transfer (Fig. 4C).Patients with an elevated respiratory rate (respiratory rate,>20) benefited most from transfer (Fig. 4D). No significantblood pressure cutoffs were identified for transfer as nearlyall patients benefitted from transfer (Fig. 4E). In general,
© 2019 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer H
patients with an ISS over 10 were more likely to have amortality benefit with transfer. As the ISS increased, thelikelihood of having a mortality benefit with transfer furtherincreased. Maximum mortality benefit was observed forpatients with an ISS between 45 and 60 (Fig. 4F).
Survival BenefitUsing multivariate Cox proportional hazards regression
with propensity score stratification, we estimate that overall,56.7% of patients in this sample either did have survival benefitfrom transfer or potentially would have had benefit from transfer(estimated HR, <1). Among those who were transferred, we es-timate that 57.1% actually benefited. Among those who werenot transferred, we estimate that 49.6% potentially could havebenefited from being transferred.
DISCUSSION
This is one of the first studies to identify specific injurytypes and patient characteristics associated with survival benefitin interfacility transfer. In this national cohort of trauma patientspresenting initially to a Level III/IV trauma setting, subsequent
955
ealth, Inc. All rights reserved.
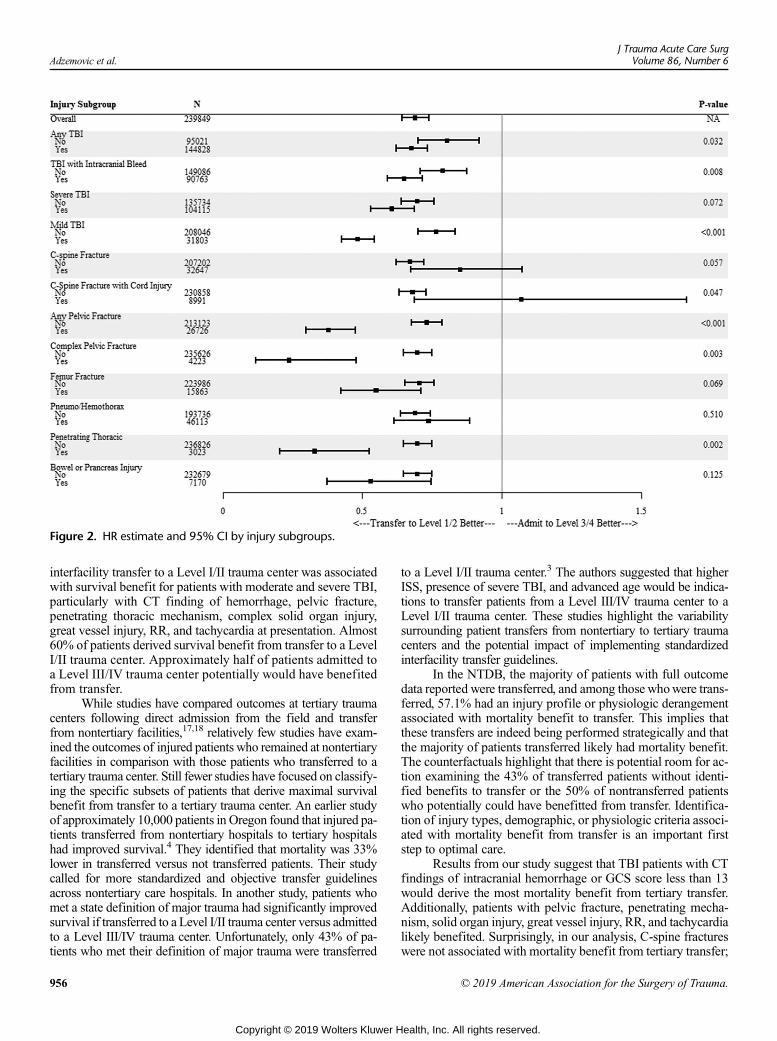
Figure 2. HR estimate and 95% CI by injury subgroups.
Adzemovic et al.J Trauma Acute Care Surg
Volume 86, Number 6
interfacility transfer to a Level I/II trauma center was associatedwith survival benefit for patients with moderate and severe TBI,particularly with CT finding of hemorrhage, pelvic fracture,penetrating thoracic mechanism, complex solid organ injury,great vessel injury, RR, and tachycardia at presentation. Almost60% of patients derived survival benefit from transfer to a LevelI/II trauma center. Approximately half of patients admitted toa Level III/IV trauma center potentially would have benefitedfrom transfer.
While studies have compared outcomes at tertiary traumacenters following direct admission from the field and transferfrom nontertiary facilities,17,18 relatively few studies have exam-ined the outcomes of injured patients who remained at nontertiaryfacilities in comparison with those patients who transferred to atertiary trauma center. Still fewer studies have focused on classify-ing the specific subsets of patients that derive maximal survivalbenefit from transfer to a tertiary trauma center. An earlier studyof approximately 10,000 patients in Oregon found that injured pa-tients transferred from nontertiary hospitals to tertiary hospitalshad improved survival.4 They identified that mortality was 33%lower in transferred versus not transferred patients. Their studycalled for more standardized and objective transfer guidelinesacross nontertiary care hospitals. In another study, patients whomet a state definition of major trauma had significantly improvedsurvival if transferred to a Level I/II trauma center versus admittedto a Level III/IV trauma center. Unfortunately, only 43% of pa-tients who met their definition of major trauma were transferred
956
Copyright © 2019 Wolters Kluwer H
to a Level I/II trauma center.3 The authors suggested that higherISS, presence of severe TBI, and advanced age would be indica-tions to transfer patients from a Level III/IV trauma center to aLevel I/II trauma center. These studies highlight the variabilitysurrounding patient transfers from nontertiary to tertiary traumacenters and the potential impact of implementing standardizedinterfacility transfer guidelines.
In the NTDB, the majority of patients with full outcomedata reported were transferred, and among those whowere trans-ferred, 57.1% had an injury profile or physiologic derangementassociated with mortality benefit to transfer. This implies thatthese transfers are indeed being performed strategically and thatthe majority of patients transferred likely had mortality benefit.The counterfactuals highlight that there is potential room for ac-tion examining the 43% of transferred patients without identi-fied benefits to transfer or the 50% of nontransferred patientswho potentially could have benefitted from transfer. Identifica-tion of injury types, demographic, or physiologic criteria associ-ated with mortality benefit from transfer is an important firststep to optimal care.
Results from our study suggest that TBI patients with CTfindings of intracranial hemorrhage or GCS score less than 13would derive the most mortality benefit from tertiary transfer.Additionally, patients with pelvic fracture, penetrating mecha-nism, solid organ injury, great vessel injury, RR, and tachycardialikely benefited. Surprisingly, in our analysis, C-spine fractureswere not associated with mortality benefit from tertiary transfer;
© 2019 American Association for the Surgery of Trauma.
ealth, Inc. All rights reserved.
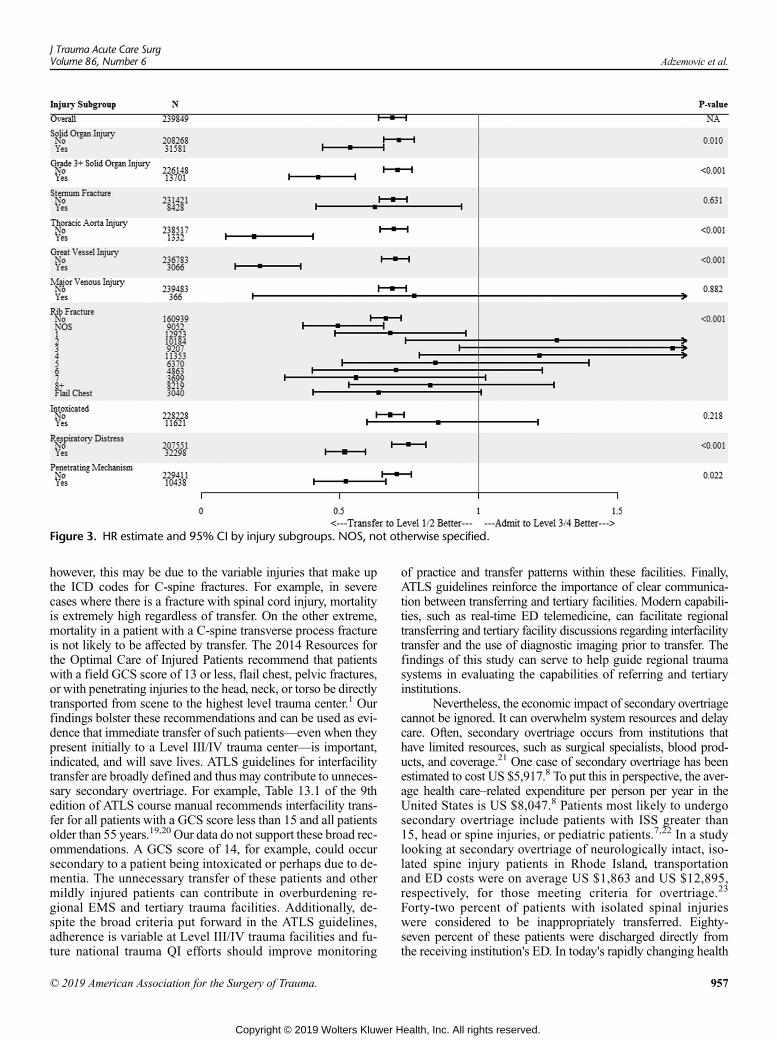
Figure 3. HR estimate and 95% CI by injury subgroups. NOS, not otherwise specified.
J Trauma Acute Care SurgVolume 86, Number 6 Adzemovic et al.
however, this may be due to the variable injuries that make upthe ICD codes for C-spine fractures. For example, in severecases where there is a fracture with spinal cord injury, mortalityis extremely high regardless of transfer. On the other extreme,mortality in a patient with a C-spine transverse process fractureis not likely to be affected by transfer. The 2014 Resources forthe Optimal Care of Injured Patients recommend that patientswith a field GCS score of 13 or less, flail chest, pelvic fractures,or with penetrating injuries to the head, neck, or torso be directlytransported from scene to the highest level trauma center.1 Ourfindings bolster these recommendations and can be used as evi-dence that immediate transfer of such patients—even when theypresent initially to a Level III/IV trauma center—is important,indicated, and will save lives. ATLS guidelines for interfacilitytransfer are broadly defined and thus may contribute to unneces-sary secondary overtriage. For example, Table 13.1 of the 9thedition of ATLS course manual recommends interfacility trans-fer for all patients with a GCS score less than 15 and all patientsolder than 55 years.19,20 Our data do not support these broad rec-ommendations. A GCS score of 14, for example, could occursecondary to a patient being intoxicated or perhaps due to de-mentia. The unnecessary transfer of these patients and othermildly injured patients can contribute in overburdening re-gional EMS and tertiary trauma facilities. Additionally, de-spite the broad criteria put forward in the ATLS guidelines,adherence is variable at Level III/IV trauma facilities and fu-ture national trauma QI efforts should improve monitoring
© 2019 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer H
of practice and transfer patterns within these facilities. Finally,ATLS guidelines reinforce the importance of clear communica-tion between transferring and tertiary facilities. Modern capabili-ties, such as real-time ED telemedicine, can facilitate regionaltransferring and tertiary facility discussions regarding interfacilitytransfer and the use of diagnostic imaging prior to transfer. Thefindings of this study can serve to help guide regional traumasystems in evaluating the capabilities of referring and tertiaryinstitutions.
Nevertheless, the economic impact of secondary overtriagecannot be ignored. It can overwhelm system resources and delaycare. Often, secondary overtriage occurs from institutions thathave limited resources, such as surgical specialists, blood prod-ucts, and coverage.21 One case of secondary overtriage has beenestimated to cost US $5,917.8 To put this in perspective, the aver-age health care–related expenditure per person per year in theUnited States is US $8,047.8 Patients most likely to undergosecondary overtriage include patients with ISS greater than15, head or spine injuries, or pediatric patients.7,22 In a studylooking at secondary overtriage of neurologically intact, iso-lated spine injury patients in Rhode Island, transportationand ED costs were on average US $1,863 and US $12,895,respectively, for those meeting criteria for overtriage.23
Forty-two percent of patients with isolated spinal injurieswere considered to be inappropriately transferred. Eighty-seven percent of these patients were discharged directly fromthe receiving institution's ED. In today's rapidly changing health
957
ealth, Inc. All rights reserved.
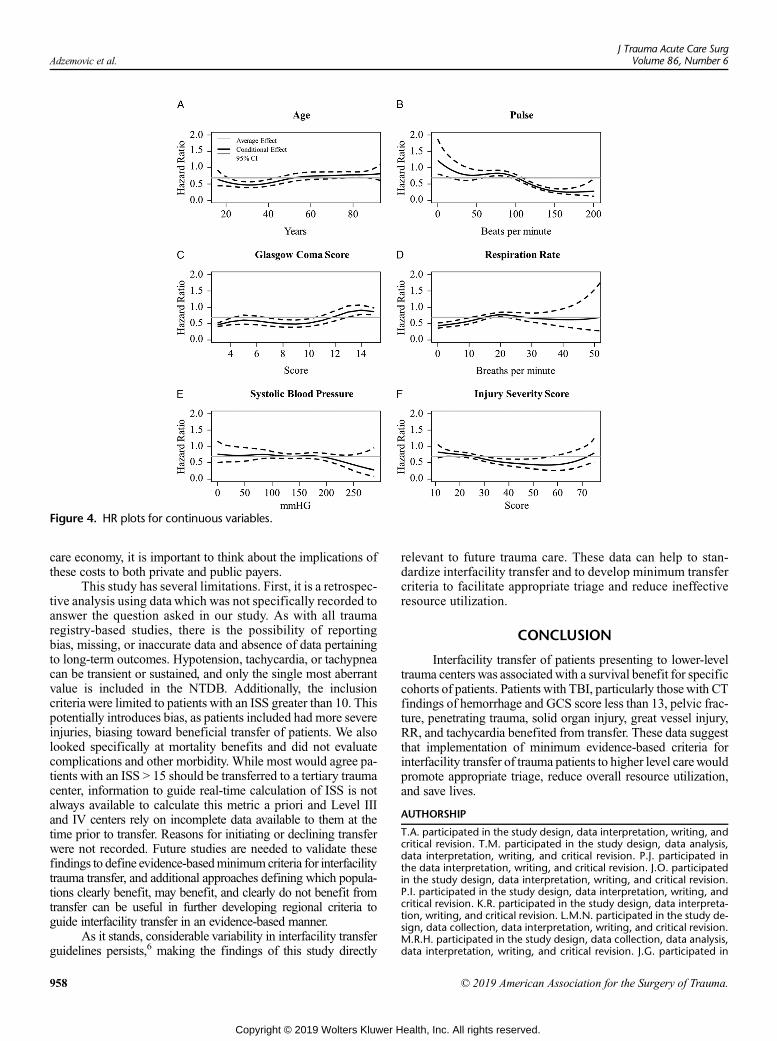
Figure 4. HR plots for continuous variables.
Adzemovic et al.J Trauma Acute Care Surg
Volume 86, Number 6
care economy, it is important to think about the implications ofthese costs to both private and public payers.
This study has several limitations. First, it is a retrospec-tive analysis using data which was not specifically recorded toanswer the question asked in our study. As with all traumaregistry-based studies, there is the possibility of reportingbias, missing, or inaccurate data and absence of data pertainingto long-term outcomes. Hypotension, tachycardia, or tachypneacan be transient or sustained, and only the single most aberrantvalue is included in the NTDB. Additionally, the inclusioncriteria were limited to patients with an ISS greater than 10. Thispotentially introduces bias, as patients included had more severeinjuries, biasing toward beneficial transfer of patients. We alsolooked specifically at mortality benefits and did not evaluatecomplications and other morbidity. While most would agree pa-tients with an ISS > 15 should be transferred to a tertiary traumacenter, information to guide real-time calculation of ISS is notalways available to calculate this metric a priori and Level IIIand IV centers rely on incomplete data available to them at thetime prior to transfer. Reasons for initiating or declining transferwere not recorded. Future studies are needed to validate thesefindings to define evidence-basedminimumcriteria for interfacilitytrauma transfer, and additional approaches defining which popula-tions clearly benefit, may benefit, and clearly do not benefit fromtransfer can be useful in further developing regional criteria toguide interfacility transfer in an evidence-based manner.
As it stands, considerable variability in interfacility transferguidelines persists,6 making the findings of this study directly
958
Copyright © 2019 Wolters Kluwer H
relevant to future trauma care. These data can help to stan-dardize interfacility transfer and to develop minimum transfercriteria to facilitate appropriate triage and reduce ineffectiveresource utilization.
CONCLUSION
Interfacility transfer of patients presenting to lower-leveltrauma centers was associatedwith a survival benefit for specificcohorts of patients. Patients with TBI, particularly thosewith CTfindings of hemorrhage and GCS score less than 13, pelvic frac-ture, penetrating trauma, solid organ injury, great vessel injury,RR, and tachycardia benefited from transfer. These data suggestthat implementation of minimum evidence-based criteria forinterfacility transfer of trauma patients to higher level carewouldpromote appropriate triage, reduce overall resource utilization,and save lives.
AUTHORSHIP
T.A. participated in the study design, data interpretation, writing, andcritical revision. T.M. participated in the study design, data analysis,data interpretation, writing, and critical revision. P.J. participated inthe data interpretation, writing, and critical revision. J.O. participatedin the study design, data interpretation, writing, and critical revision.P.I. participated in the study design, data interpretation, writing, andcritical revision. K.R. participated in the study design, data interpreta-tion, writing, and critical revision. L.M.N. participated in the study de-sign, data collection, data interpretation, writing, and critical revision.M.R.H. participated in the study design, data collection, data analysis,data interpretation, writing, and critical revision. J.G. participated in
© 2019 American Association for the Surgery of Trauma.
ealth, Inc. All rights reserved.
J Trauma Acute Care SurgVolume 86, Number 6 Adzemovic et al.
the study design, data interpretation, writing, and critical revision. P.K.P. participated in the study design, data interpretation, writing, andcritical revision. C.J.T. participated in the study design, data collection,data analysis, data interpretation, writing, and critical revision.
DISCLOSURE
Mark R. Hemmila receives support from Blue Cross Blue Shield ofMichigan and Blue Care Network (a nonprofit mutual company) forconduct of The Michigan Trauma Quality Improvement Program witha Collaborative Quality Initiatives grant. For the remaining authors, noconflicts were declared.
REFERENCES1. American College of Surgeons Committee on Trauma. Resources for opti-
mal care of the injuried patient. Chicago (IL): The Committee; 2014.2. Tignanelli CJ, Joseph B, Jakubus JL, Iskander GA, Napolitano LM,
Hemmila MR. Variability in management of blunt liver trauma and contribu-tion of level of American College of Surgeons Committee on Trauma verifi-cation status on mortality. J Trauma Acute Care Surg. 2018;84:273–279.
3. Garwe T, Cowan LD, Neas B, Cathey T, Danford BC, Greenawalt P. Survivalbenefit of transfer to tertiary trauma centers for major trauma patients ini-tially presenting to nontertiary trauma centers. Acad Emerg Med. 2010;17:1223–1232.
4. Newgard CD, McConnell KJ, Hedges JR, Mullins RJ. The benefit of higherlevel of care transfer of injured patients from nontertiary hospital emergencydepartments. J Trauma. 2007;63:965–971.
5. Pickering A, Cooper K, Harnan S, Sutton A, Mason S, Nicholl J. Impact ofprehospital transfer strategies in major trauma and head injury: systematic re-view, meta-analysis, and recommendations for study design. J Trauma AcuteCare Surg. 2015;78:164–177.
6. Ciesla DJ, Sava JA, Street JH 3rd, Jordan MH. Secondary overtriage: aconsequence of an immature trauma system. J Am Coll Surg. 2008;206:131–137.
7. Sorensen MJ, von Recklinghausen FM, Fulton G, Burchard KW. Secondaryovertriage: the burden of unnecessary interfacility transfers in a rural traumasystem. JAMA Surg. 2013;148:763–768.
8. Osen HB, Bass RR, Abdullah F, Chang DC. Rapid discharge after transfer:risk factors, incidence, and implications for trauma systems. J Trauma.2010;69:602–606.
9. van Buuren Stef, Groothuis-Oudshoorn Karin. MICE: Multivariate Imputa-tion by Chained Equations in R. J Stat Softw. 2011;45(3):1–67. URLhttps://www.jstatsoft.org/v45/i03/. Accessed on February 23, 2018.
10. Tignanelli CJ, Vander Kolk WE, Mikhail JN, Delano MJ, Hemmila MR.Non-compliance with ACS-COT recommended criteria for full trauma teamactivation is associated with undertriage deaths. J Trauma Acute Care Surg.2018;84:287–294.
11. Imbens G, Rubin D. Causal Inference for Statistics, Social, and BiomedicalSciences: An Introduction. Cambridge: Cambridge University Press; 2015.
12. Glance LG, Osler TM, Mukamel DB, Meredith W, Wagner J, Dick AW.TMPM-ICD9: a trauma mortality prediction model based on ICD-9-CMcodes. Ann Surg. 2009;249:1032–1039.
13. Ruppert D, Wand M, Carroll R. Semiparametric Regression (Cambridge Se-ries in Statistical and Probabilistic Mathematics). Cambridge: CambridgeUniversity Press; 2003.
14. Schuster T, Lowe WK, Platt RW. Propensity score model overfitting led toinflated variance of estimated odds ratios. J Clin Epidemiol. 2016;80:97–106.
15. Brier. Verification of forecasts expressed in terms of probability. MonWeather Rev. 1950;78:1–3.
16. R Core Team (2013). R: A language and environment for statistical comput-ing. R Foundation for Statistical Computing, Vienna, Austria. URL http://www.R-project.org/. Accessed on March 1, 2018.
17. Haas B, Stukel TA, Gomez D, Zagorski B, De Mestral C, Sharma SV. Themortality benefit of direct trauma center transport in a regional trauma sys-tem: a population-based analysis. J Trauma Acute Care Surg. 2012;72:1510–5; discussion 5–7.
18. Hill AD, Fowler RA, Nathens AB. Impact of interhospital transfer on out-comes for trauma patients: a systematic review. J Trauma. 2011;71:1885–1900; discussion 901.
© 2019 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer H
19. Subcommittee A, American College of Surgeons' Committee on T, Inter-national Awg. Advanced trauma life support (ATLS(R)): the ninth edition.J Trauma Acute Care Surg. 2013;74:1363–1366.
20. Advanced Trauma Life Support Student Course Manual. Ninth Edition.American College of Surgeons, 2012 .
21. Con J, Long D, Sasala E, Khan U, Knight J, Schaefer G, et al. Secondaryovertriage in a statewide rural trauma system. J Surg Res. 2015;198:462–467.
22. Lynch KT, Essig RM, Long DM, Wilson A, Con J. Nationwide secondaryovertriage in level 3 and level 4 trauma centers: are these transfers necessary?J Surg Res. 2016;204:460–466.
23. Bible JE, Kadakia RJ, Kay HF, Zhang CE, Casimir GE, Devin CJ. Howoftenare interfacility transfers of spine injury patients truly necessary? Spine J.2014;14:2877–2884.
DISCUSSIONJASONSPERRY,M.D.,M.P.H. (Pittsburgh,Pennsylvania):
I'd like to thank the AAST and the Program Committee for theprivilege to discuss this manuscript, and to the authors for get-ting the manuscript to the Program Committee and myself ontime, and for a very nice presentation.
So, the authors have presented a nicely written manuscriptrobustly characterizing the NTDB, which has its own limita-tions, regarding the transfer of patients from Level 3 and 4 cen-ters to Level 1 and 2 centers.
They use high-level statistical propensity score modeling,and the results suggest a large proportion of moderately injuredpatients would benefit from transport. I agree with their results.
Their methods and results could be used to improve theappropriate transfer of patients and demonstrate those injurieswhere transfer may not be beneficial. I do have some questionsfor the authors.
First, as stated in the manuscript and the discussion, theauthors utilized Injury Severity Score (ISS) in their model, andthis variable is not typically available in the pre-hospital or inthe Emergency Department setting at the time of transfer.
They also include specific injury types, which I agree with,in their methods. Are the authors able to do the same modelingwith and without Injury Severity Score being included, and if so,do those results change?
Number two, does the NTDB database allow the authors tocharacterize those patients who underwent imaging and then trans-fer, and if imaging itself, such as headCTresults, affects the results,and whether the authors recommend radiographic workup priorto transfer, which can sometimes delay definitive management.
Finally, the authors used a study cohort with an Injury Se-verity Score of greater than 10 as their inclusion criteria. If theywere to look at lower ISS scores, or injury characteristics, therewould likely be at an even higher rate of over-triage transfers.
The method is, thus, bias towards beneficial transfers ofthese patients. Do the authors have any recommendations forpatients with an estimated ISS less than 10?
Thank you for the privilege of the podium to discuss thismanuscript.
CHRISTOPHERJ. TIGNANELLI,M.D. (Minneapolis,Minnesota): Thank you, Dr. Sperry. The first question was, canwe do modeling with and without the Injury Severity Score.Yes, we can. We only used the Injury Severity Score in the gener-ation of the propensity score.
My thoughts would be if we did pull it out, I don't thinkthere would be a huge change, because in addition to the Injury
959
ealth, Inc. All rights reserved.

Adzemovic et al.J Trauma Acute Care Surg
Volume 86, Number 6
Severity Score, we also adjusted patients based onEDvitals, demo-graphics, and their injury characteristics; but we could definitelytake out Injury Severity Score and see how much that changes.
The next question is if the NTDB allows us to characterizepatients that underwent imaging. That's a really good thought;we can definitely do that. We can use the ICD-9 procedurecodes and use that to look at imaging the patients got beforeand after transfer.
And then, do we recommend imaging prior to transfer?That really depends on the comfort of the Level 3 and 4 centers,that they can do an accurate imaging study.
It needs to be decided on a region-to-region basis, and in-cludes the development of regional protocols for transfer.
One potential way that I see applying these findings toLevel 3 and 4 trauma centers would be, in the first phase, if a pa-tient comes in, they have a GCS less than 13 or a penetratingmechanism of injury or sustained tachycardia, then, stabilizethat patient, get your chest x-ray, FAST, pelvis x-ray, and thentransfer them to a Level 1 or 2 center.
Alternatively, it gets a little more tricky if the patient is sta-ble. If they can get an appropriate imaging study, and you have aregional protocol in place with tertiary trauma centers, then itwould be ideal to image them at the Level 3 or 4 centers. If
960
Copyright © 2019 Wolters Kluwer H
you identify a solid organ injury or a traumatic brain injury witha bleed, then transfer those patients to a Level 1 or 2 center.
Potentially a more sophisticated way to do it would actuallybe to leverage tele-medicine and actually call in to the Level 1 or 2centers and, review the patient, discuss imaging decisions, andmake sure that imaging actually gets to the tertiary trauma center.
And then the last question was thoughts on patients withan Injury Severity Score of less than 10. One of our figures,did look at the Injury Severity Score as a continuous variable,we saw that oncewe got below an Injury Severity Score of about11 or 12, there was not a benefit for survival for transfer to a 1 or2 center.
I think that it would be similar to, if you remember whenwe looked at the Grade 3 or above solid organ injuries, there's apretty wide gap for benefit, with the patients with higher gradeinjuries having more benefit, and then we just looked at the pa-tients who had just solid organ injuries, including the 1 and 2s,that benefit decreased some.
There would be a decreased benefit if we included all thepatients with Injury Severity Score less than 10, but for the onesthat were strongly statistically significant, that would hold, butwe'd have to look at it.
Thank you very much.
© 2019 American Association for the Surgery of Trauma.
ealth, Inc. All rights reserved.
ORIGINAL ARTICLE
Right hospital, right patients: Penetrating injury patients treated athigh-volume penetrating trauma centers have lower mortality
Chih-Yuan Fu, MD, Francesco Bajani, MD, Leah Tatebe, MD, Caroline Butler, MD, Frederic Starr, MD,Andrew Dennis, DO, Matthew Kaminsky, MD, Thomas Messer, MD, Victoria Schlanser, Kristina Kramer, MD,
Stathis Poulakidas, MD, Chi-Tung Cheng, MD, Justin Mis, RN, and Faran Bokhari, MD, Chicago, Illinois
Sub
Fro
Ad
The
DO
J TrVol
BACKGROUND: T
mitted: August 9, 2018, RevisePublished online: March 1, 201m the Department of Trauma anM.K., T.M., V.S., K.K., S.P. C-TRush University, Chicago, IllinSurgery (C-Y.F., C-T.C.), Chansity, Taoyuan City, Taiwan.dress for reprints: Faran BokharStroger Hospital of Cook CounIL, 60612; email: fbokhari@coabstract has been accepted for aHealth Association, November
I: 10.1097/TA.00000000000022
auma Acute Care Surgume 86, Number 6
he recognition of the relationship between volume and outcomes led to the regionalization of trauma care. The relationship be-tween trauma mechanism-subtype and outcomes has yet to be explored. We hypothesized that trauma centers with a high volumeof penetrating trauma patients might be associated with a higher survival rate for penetrating trauma patients.
METHODS: A
retrospective cohort analysis of penetrating trauma patients presenting between 2011 and 2015was conducted using the NationalTrauma Database and the trauma registry at the Stroger Cook County Hospital. Linear regression was used to determine the rela-tionship between mortality and the annual volume of penetrating trauma seen by the treating hospital.RESULTS: N
ationally, penetrating injuries account for 9.5% of the trauma cases treated. Patients treated within the top quartile penetrating-volume hospitals (≥167 penetrating cases per annum) are more severely injured (Injury Severity Score: 8.9 vs. 7.7) than thosetreated at the lowest quartile penetrating volume centers (<36.6 patients per annum). Therewas a lower mortality rate at institutionsthat treated high numbers of penetrating trauma patients per annum. A penetrating trauma mortality risk adjustment model showedthat the volume of penetrating trauma patients was an independent factor associated with survival rate.CONCLUSION: T
rauma centers with high penetrating trauma patient volumes are associated with improved survival of these patients. This associationwith improved survival does not hold true for the total traumavolume at a center but is specific to the volume of the penetrating traumasubtype. (J Trauma Acute Care Surg. 2019;86: 961–966. Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.)LEVEL OF EVIDENCE: P
rognostic/Epidemiology Study, Level-III; Therapeutic/Care Management, Level IV. KEYWORDS: P enetrating trauma; trauma center; high volume.T he centralization of complex health care services, such astransplant and oncology, improves outcomes.1–3 Several stud-
ies have demonstrated a similar association between the creationof trauma care and outcomes.4–7 In a landmark article, Mackenzieet al.8 demonstrated that adjusted-mortality rates are significantlylower when care is provided in a trauma center compared withwhen it is provided in a nontrauma center.
Mechanisms of traumatic injury can be diverse. Penetrating,blunt, and burn injuries require different skill sets from the treatingtrauma team. Geographic patterns of injury can result in somecenters receiving high volumes of specific subtypes of injury.To the best of our knowledge, the association between treatmentat a trauma center receiving a high-volume of a certain type ofinjury and outcomes has not been explored. We sought to definethe current volume and nature of penetrating trauma treatedwithin Level I/II trauma centers in the United States, and to
d: January 15, 2019, Accepted: January 30, 2019,9.d Burn Surgery (C-Y.F., F.B., L.T., C.B., F.S., A.D.,.C., J.M., F.B.), Stroger Hospital of Cook County,ois; and Department of Trauma and Emergencyg Gung Memorial Hospital, Chang Gung Univer-
i, MD, Department of Trauma and Burn Surgery,ty, Rush University, 1950 West Polk St, Chicago,okcountyhhs.org.poster at the Annual Meeting of American Public10–14, 2018 in San Diego, CA. (ID 2064.0).
45
Copyright © 2019 Wolters Kluwer H
explore the association between the volume of penetrating traumacared for at a center and outcomes. The data from our own center,the John H Stroger Jr. Hospital of Cook County (CCH), which isthe largest Level I trauma center in Cook County, Illinois wasalso analyzed. We hypothesized that trauma centers with a highvolume of penetrating trauma patients might be associated witha higher survival rate for penetrating trauma patients.
MATERIALS AND METHODS
A retrospective cohort analysis of penetrating injury patientsin our registry at the CCH and the National Trauma Data Bank(NTDB) for Level I/II trauma centers was undertaken for the years2011 to 2015. TheNTDB is largest data bank of collected informa-tion about traumatic injuries and outcomes in the United States.9
The CCH serves as the largest combined Level I adult and LevelI pediatric trauma center for Cook County. This institution issurrounded by West/East Garfield Park and the South Side ofChicago, both of which have high violent crime rates.10,11
The inclusion criteria for the current study were penetratinginjuries (origin file: RDS_ECODE and RDS_ECODEDES) treatedin Level I/II trauma centers either accredited by the American Col-lege of Surgery or state law (origin file: RDS_FACILITY). Patientswhowere dead on arrival or those with missing key values wereexcluded. Patients with missing records of age, vital signs, InjurySeverity Score (ISS), and trauma mechanisms were excluded(N = 154,567 within 5 years, 5.0%).
Systolic blood pressure/pulse in the emergency department(origin file: RDS_VITALS), age (origin file: RDS_DEMO),
961
ealth, Inc. All rights reserved.
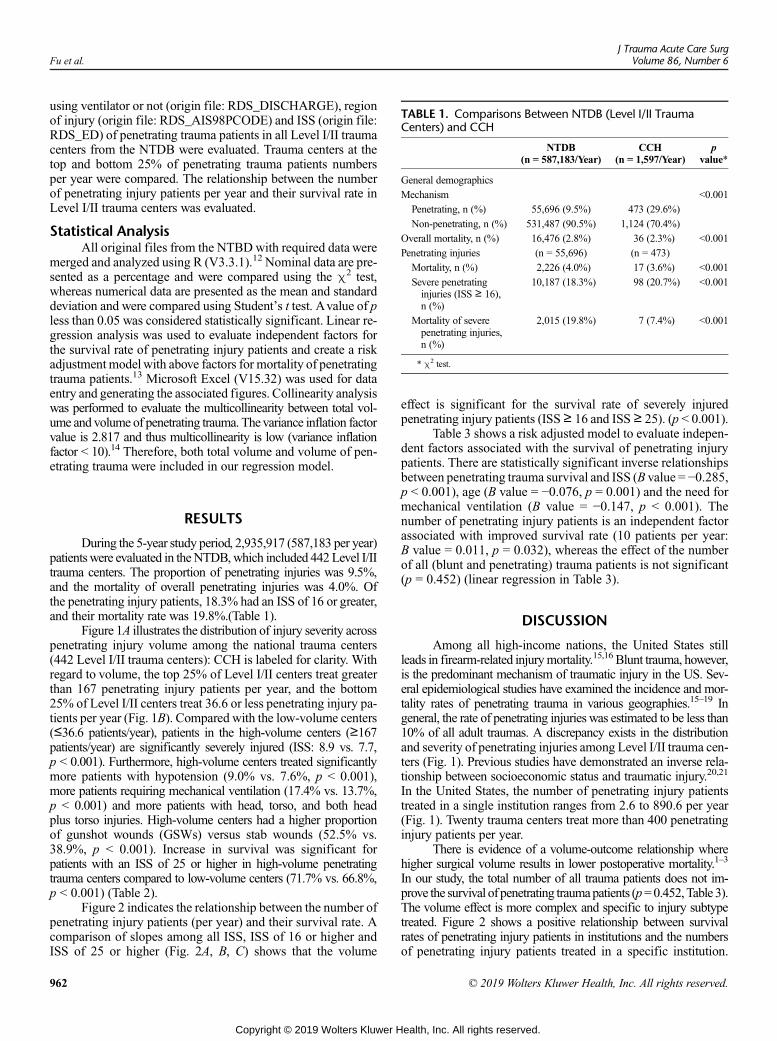
TABLE 1. Comparisons Between NTDB (Level I/II TraumaCenters) and CCH
NTDB(n = 587,183/Year)
CCH(n = 1,597/Year)
pvalue*
General demographics
Mechanism <0.001
Penetrating, n (%) 55,696 (9.5%) 473 (29.6%)
Non-penetrating, n (%) 531,487 (90.5%) 1,124 (70.4%)
Overall mortality, n (%) 16,476 (2.8%) 36 (2.3%) <0.001
Penetrating injuries (n = 55,696) (n = 473)
Mortality, n (%) 2,226 (4.0%) 17 (3.6%) <0.001
Severe penetratinginjuries (ISS ≥ 16),n (%)
10,187 (18.3%) 98 (20.7%) <0.001
Mortality of severepenetrating injuries,n (%)
2,015 (19.8%) 7 (7.4%) <0.001
* χ2 test.
Fu et al.J Trauma Acute Care Surg
Volume 86, Number 6
using ventilator or not (origin file: RDS_DISCHARGE), regionof injury (origin file: RDS_AIS98PCODE) and ISS (origin file:RDS_ED) of penetrating trauma patients in all Level I/II traumacenters from the NTDB were evaluated. Trauma centers at thetop and bottom 25% of penetrating trauma patients numbersper year were compared. The relationship between the numberof penetrating injury patients per year and their survival rate inLevel I/II trauma centers was evaluated.
Statistical AnalysisAll original files from the NTBDwith required data were
merged and analyzed using R (V3.3.1).12 Nominal data are pre-sented as a percentage and were compared using the χ2 test,whereas numerical data are presented as the mean and standarddeviation and were compared using Student’s t test. Avalue of pless than 0.05 was considered statistically significant. Linear re-gression analysis was used to evaluate independent factors forthe survival rate of penetrating injury patients and create a riskadjustment modelwith above factors for mortality of penetratingtrauma patients.13 Microsoft Excel (V15.32) was used for dataentry and generating the associated figures. Collinearity analysiswas performed to evaluate the multicollinearity between total vol-ume and volume of penetrating trauma. Thevariance inflation factorvalue is 2.817 and thus multicollinearity is low (variance inflationfactor < 10).14 Therefore, both total volume and volume of pen-etrating trauma were included in our regression model.
RESULTS
During the 5-year study period, 2,935,917 (587,183 per year)patientswere evaluated in theNTDB,which included 442 Level I/IItrauma centers. The proportion of penetrating injuries was 9.5%,and the mortality of overall penetrating injuries was 4.0%. Ofthe penetrating injury patients, 18.3% had an ISS of 16 or greater,and their mortality rate was 19.8%.(Table 1).
Figure 1A illustrates the distribution of injury severity acrosspenetrating injury volume among the national trauma centers(442 Level I/II trauma centers): CCH is labeled for clarity. Withregard to volume, the top 25% of Level I/II centers treat greaterthan 167 penetrating injury patients per year, and the bottom25% of Level I/II centers treat 36.6 or less penetrating injury pa-tients per year (Fig. 1B). Compared with the low-volume centers(≤36.6 patients/year), patients in the high-volume centers (≥167patients/year) are significantly severely injured (ISS: 8.9 vs. 7.7,p < 0.001). Furthermore, high-volume centers treated significantlymore patients with hypotension (9.0% vs. 7.6%, p < 0.001),more patients requiring mechanical ventilation (17.4% vs. 13.7%,p < 0.001) and more patients with head, torso, and both headplus torso injuries. High-volume centers had a higher proportionof gunshot wounds (GSWs) versus stab wounds (52.5% vs.38.9%, p < 0.001). Increase in survival was significant forpatients with an ISS of 25 or higher in high-volume penetratingtrauma centers compared to low-volume centers (71.7% vs. 66.8%,p < 0.001) (Table 2).
Figure 2 indicates the relationship between the number ofpenetrating injury patients (per year) and their survival rate. Acomparison of slopes among all ISS, ISS of 16 or higher andISS of 25 or higher (Fig. 2A, B, C) shows that the volume
962
Copyright © 2019 Wolters Kluwer H
effect is significant for the survival rate of severely injuredpenetrating injury patients (ISS≥ 16 and ISS ≥ 25). (p < 0.001).
Table 3 shows a risk adjusted model to evaluate indepen-dent factors associated with the survival of penetrating injurypatients. There are statistically significant inverse relationshipsbetween penetrating trauma survival and ISS (B value = −0.285,p < 0.001), age (B value = −0.076, p = 0.001) and the need formechanical ventilation (B value = −0.147, p < 0.001). Thenumber of penetrating injury patients is an independent factorassociated with improved survival rate (10 patients per year:B value = 0.011, p = 0.032), whereas the effect of the numberof all (blunt and penetrating) trauma patients is not significant(p = 0.452) (linear regression in Table 3).
DISCUSSION
Among all high-income nations, the United States stillleads in firearm-related injurymortality.15,16 Blunt trauma, however,is the predominant mechanism of traumatic injury in the US. Sev-eral epidemiological studies have examined the incidence and mor-tality rates of penetrating trauma in various geographies.15–19 Ingeneral, the rate of penetrating injuries was estimated to be less than10% of all adult traumas. A discrepancy exists in the distributionand severity of penetrating injuries among Level I/II trauma cen-ters (Fig. 1). Previous studies have demonstrated an inverse rela-tionship between socioeconomic status and traumatic injury.20,21
In the United States, the number of penetrating injury patientstreated in a single institution ranges from 2.6 to 890.6 per year(Fig. 1). Twenty trauma centers treat more than 400 penetratinginjury patients per year.
There is evidence of a volume-outcome relationship wherehigher surgical volume results in lower postoperative mortality.1–3
In our study, the total number of all trauma patients does not im-prove the survival of penetrating traumapatients (p=0.452,Table 3).The volume effect is more complex and specific to injury subtypetreated. Figure 2 shows a positive relationship between survivalrates of penetrating injury patients in institutions and the numbersof penetrating injury patients treated in a specific institution.
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
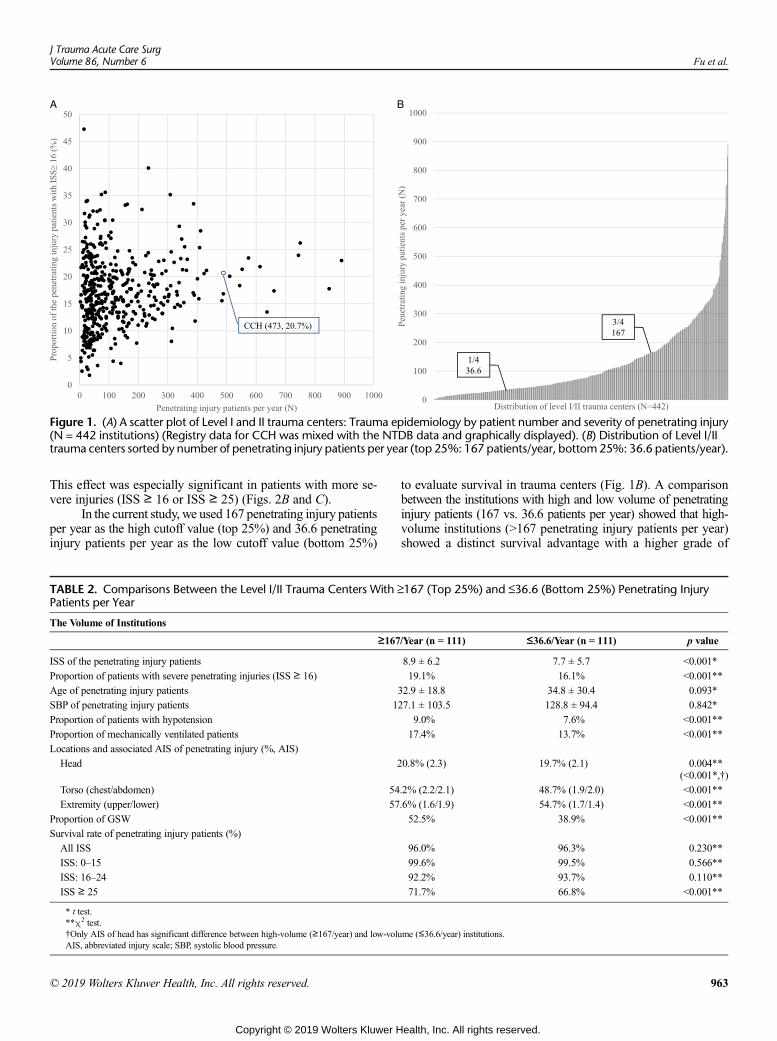
Figure 1. (A) A scatter plot of Level I and II trauma centers: Trauma epidemiology by patient number and severity of penetrating injury(N = 442 institutions) (Registry data for CCH was mixed with the NTDB data and graphically displayed). (B) Distribution of Level I/IItrauma centers sorted by number of penetrating injury patients per year (top 25%: 167 patients/year, bottom25%: 36.6 patients/year).
J Trauma Acute Care SurgVolume 86, Number 6 Fu et al.
This effect was especially significant in patients with more se-vere injuries (ISS ≥ 16 or ISS ≥ 25) (Figs. 2B and C).
In the current study, we used 167 penetrating injury patientsper year as the high cutoff value (top 25%) and 36.6 penetratinginjury patients per year as the low cutoff value (bottom 25%)
TABLE 2. Comparisons Between the Level I/II Trauma Centers With ≥Patients per Year
The Volume of Institutions
≥167
ISS of the penetrating injury patients
Proportion of patients with severe penetrating injuries (ISS ≥ 16)
Age of penetrating injury patients
SBP of penetrating injury patients 1
Proportion of patients with hypotension
Proportion of mechanically ventilated patients
Locations and associated AIS of penetrating injury (%, AIS)
Head 2
Torso (chest/abdomen) 54
Extremity (upper/lower) 57
Proportion of GSW
Survival rate of penetrating injury patients (%)
All ISS
ISS: 0–15
ISS: 16–24
ISS ≥ 25
* t test.**χ2 test.†Only AIS of head has significant difference between high-volume (≥167/year) and low-voluAIS, abbreviated injury scale; SBP, systolic blood pressure.
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
to evaluate survival in trauma centers (Fig. 1B). A comparisonbetween the institutions with high and low volume of penetratinginjury patients (167 vs. 36.6 patients per year) showed that high-volume institutions (>167 penetrating injury patients per year)showed a distinct survival advantage with a higher grade of
167 (Top 25%) and ≤36.6 (Bottom 25%) Penetrating Injury
/Year (n = 111) ≤36.6/Year (n = 111) p value
8.9 ± 6.2 7.7 ± 5.7 <0.001*
19.1% 16.1% <0.001**
32.9 ± 18.8 34.8 ± 30.4 0.093*
27.1 ± 103.5 128.8 ± 94.4 0.842*
9.0% 7.6% <0.001**
17.4% 13.7% <0.001**
0.8% (2.3) 19.7% (2.1) 0.004**(<0.001*,†)
.2% (2.2/2.1) 48.7% (1.9/2.0) <0.001**
.6% (1.6/1.9) 54.7% (1.7/1.4) <0.001**
52.5% 38.9% <0.001**
96.0% 96.3% 0.230**
99.6% 99.5% 0.566**
92.2% 93.7% 0.110**
71.7% 66.8% <0.001**
me (≤36.6/year) institutions.
963
ealth, Inc. All rights reserved.
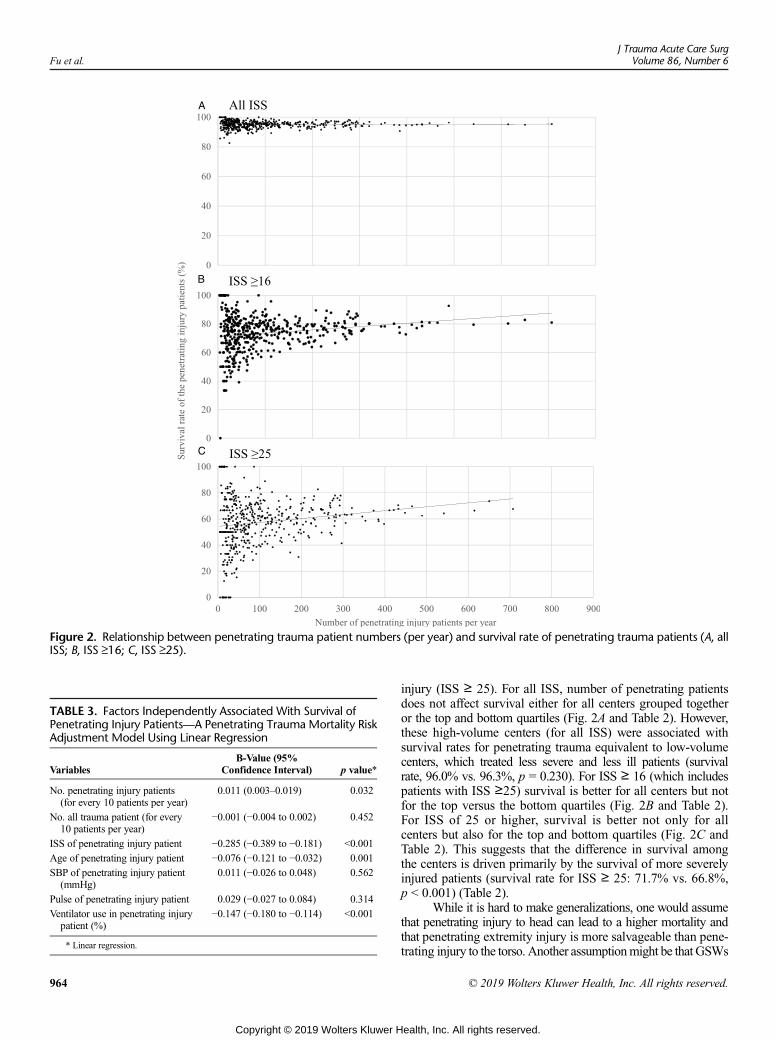
Figure 2. Relationship between penetrating trauma patient numbers (per year) and survival rate of penetrating trauma patients (A, allISS; B, ISS ≥16; C, ISS ≥25).
TABLE 3. Factors Independently Associated With Survival ofPenetrating Injury Patients—A Penetrating Trauma Mortality RiskAdjustment Model Using Linear Regression
VariablesB-Value (95%
Confidence Interval) p value*
No. penetrating injury patients(for every 10 patients per year)
0.011 (0.003–0.019) 0.032
No. all trauma patient (for every10 patients per year)
−0.001 (−0.004 to 0.002) 0.452
ISS of penetrating injury patient −0.285 (−0.389 to −0.181) <0.001
Age of penetrating injury patient −0.076 (−0.121 to −0.032) 0.001
SBP of penetrating injury patient(mmHg)
0.011 (−0.026 to 0.048) 0.562
Pulse of penetrating injury patient 0.029 (−0.027 to 0.084) 0.314
Ventilator use in penetrating injurypatient (%)
−0.147 (−0.180 to −0.114) <0.001
* Linear regression.
Fu et al.J Trauma Acute Care Surg
Volume 86, Number 6
964
Copyright © 2019 Wolters Kluwer H
injury (ISS ≥ 25). For all ISS, number of penetrating patientsdoes not affect survival either for all centers grouped togetheror the top and bottom quartiles (Fig. 2A and Table 2). However,these high-volume centers (for all ISS) were associated withsurvival rates for penetrating trauma equivalent to low-volumecenters, which treated less severe and less ill patients (survivalrate, 96.0% vs. 96.3%, p = 0.230). For ISS ≥ 16 (which includespatients with ISS ≥25) survival is better for all centers but notfor the top versus the bottom quartiles (Fig. 2B and Table 2).For ISS of 25 or higher, survival is better not only for allcenters but also for the top and bottom quartiles (Fig. 2C andTable 2). This suggests that the difference in survival amongthe centers is driven primarily by the survival of more severelyinjured patients (survival rate for ISS ≥ 25: 71.7% vs. 66.8%,p < 0.001) (Table 2).
While it is hard to make generalizations, one would assumethat penetrating injury to head can lead to a higher mortality andthat penetrating extremity injury is more salvageable than pene-trating injury to the torso. Another assumptionmight be that GSWs
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 6 Fu et al.
are more lethal than stab wounds. Our data found that the higher-volume centers treat more penetrating injuries to the head, torsoand extremities and more GSWs in general than low volume centers(52.5% vs. 38.9%, p < 0.001). The AIS scores of the head, andnot torso or extremities, were significantly higher in the high-volume centers.
Gunshot wounds usually occur in populations with lowersocioeconomic status, and most violence occurs in neighborhoodswith concentrated poverty and housing.22–25 In addition to increasedlaw enforcement efforts against gun violence, equal attentionshould be paid to improvingmedical survival fromGSWs.Delayedsurgical intervention for significant injuries, such as torso pene-trating injuries, can increase trauma-related morbidity and mor-tality rates.26,27 Therefore, a trauma center that provides rapidtransportation and timely treatment is necessary for people whoare victims of GSWs. Furthermore, while the trauma centers ana-lyzed havevery similar expert personnel, in a high-volume penetrat-ing center the personnel are exposed to more penetrating trauma.The results of the current study suggest that increased penetrat-ing volume is associated with better survival.
Improved outcomes of trauma patients whowere treated attrauma centers have been previously reported. However, volumeeffect has not been evaluated based onmechanism of injury. Themanagement of a non-penetrating injury can be as complicatedas the management of penetrating injury.28,29 Therefore, volume-related improved outcomes may exist not only for penetrating in-jury patients. We evaluated whether the salutary patient volumeeffect is specific to penetrating injuries. A risk adjustment modelusing linear regression analysis was created to evaluate indepen-dent risk factors that were related to the survival rate of penetrat-ing trauma patients. Older age, using ventilator, and higher ISSshow significantly negative effects on the survival of penetratingtrauma patients. Trauma centers show improved survival ratesof penetrating trauma patients associated with increased num-ber of penetrating injury patients treated per year (p = 0.032).Although it is difficult for emergency medical service personnelto evaluate injury severity at the scene, penetrating injury pa-tients is more easily identified. Triage of the right severity pen-etrating injury to the correct regional trauma center is morecomplex. The a priori assessment of a higher ISS injury and tri-age to a “high-volume penetrating trauma center” would need adiscussion, evaluation, and consensus within each region.
A nationwide data bank with a large sample size was eval-uated in the current study, but the conclusions are limited due tothe retrospective nature of the data and some missing elementsin the NTDB. In addition, the functional outcome of penetratinginjury patients and the cost-effectiveness of subspecialized traumacenters were not evaluated. Wewere not able to evaluate if concen-trating penetrating trauma in a few centers would actually improveoverall survival in a local trauma system. This would depend on thelocation of penetrating hotbeds and the deleterious effect of furtherdecreasing penetrating trauma patients going to already lowpenetrating trauma centers. Further studies with a prospectivedesign and long-term follow-up are needed.
CONCLUSION
Severely injured penetrating trauma patients have a highersurvival when treated at high-volume penetrating trauma centers.
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
The reason for improved survival in a penetrating injury traumacenter is more complex than a simple overall volume effect.
DISCLOSURE
The authors have no commercial associations or sources of support fromany grant, funding source or commercial interest including pharmaceuti-cal or device companies that might pose a conflict of interest.
REFERENCES1. Jonker FHW, Hagemans JAW, Verhoef C, Burger JWA. The impact of hos-
pital volume on perioperative outcomes of rectal cancer. Eur J Surg Oncol.2017;43:1894–1900.
2. de Wilde RF, Besselink MG, van der Tweel I, de Hingh IH, van Eijck CH,Dejong CH, Porte RJ, Gouma DJ, BuschOR,Molenaar IQ. Dutch pancreaticcancer group. Impact of nationwide centralization of pancreaticoduodenectomyon hospital mortality. Br J Surg. 2012;99:404–410.
3. Kopp W, van Meel M, Putter H, Samuel U, Arbogast H, Schareck W,Ringers J, Braat A. Center volume is associated with outcome after pancreastransplantation within the Eurotransplant region. Transplantation. 2017;101:1247–1253.
4. Hoff WS, Schwab CW. Trauma system development in North America. ClinOrthop. 2004;422:17–22.
5. Champion HR, Copes RH, SaccoWJ, LawnickMM, Keast SL, Bain LW Jr.,Flanagan ME, Frey CF. The major trauma outcome study: establishing na-tional norms for trauma care. J Trauma. 1990;30:1356–1365.
6. Mullins RJ, Mann NC. Population-based research assessing the effectivenessof trauma systems. J Trauma. 1999;47:S59–S66.
7. Bazzoli GJ, Madura KJ, Cooper GF, MacKenzie EJ, Maier RV. Progress inthe development of trauma systems in the United States. Results of a nationalsurvey. JAMA. 1995;273:395–401.
8. MacKenzie EJ, Rivara FP, Jurkovich GJ, Nathens AB, Frey KP, Egleston BL,Salkever DS, Scharfstein DO. A national evaluation of the effect of trauma-center care on mortality. N Engl J Med. 2006;26;354:366–78.
9. https://www.facs.org/quality-programs/trauma/ntdbAccessed January 15, 2019.10. http://crime.chicagotribune.com/ Accessed January 15, 2019.11. https://home.chicagopolice.org/online-services/crime-statistics/ Accessed January
15, 2019.12. R Core Team. R: A language and environment for statistical computing. Vi-
enna, Austria: R Foundation for Statistical Computing; 2014. URL http://www.R-project.org/ Accessed January 15, 2019.
13. Haider AH, Hashmi ZG, Zafar SN, et al. Developing best practices to studytrauma outcomes in large databases: an evidence-based approach to deter-mine the best mortality risk adjustment model. J Trauma Acute Care Surg.2014;76:1061–1069.
14. Kutner MH, Nachtsheim CJ, Neter J. Applied Linear Regression Models. 4th ed.New York, NY: McGraw-Hill Irwin; 2004.
15. Richardson EG, Homicide Hemenway D. Homicide, suicide, and uninten-tional firearm fatality: comparing the United States with other high-incomecountries, 2003. J Trauma. 2011;70:238–243.
16. Lee J, Quraishi SA, Bhatnagar S, Zafonte RD, Masiakos PT. The economiccost of firearm-related injuries in theUnited States from2006 to 2010. Surgery.2014;155:894–898.
17. Whittaker G, Norton J, Densley J, Bew D. Epidemiology of penetrating inju-ries in the United Kingdom: a systematic review. Int J Surg. 2017;41:65–69.
18. Zebib L, Stoler J, Zakrison TL. Geo-demographics of gunshot wound inju-ries in Miami-Dade county, 2002–2012. BMC Public Health. 2017;17:174.
19. Demetriades D, Velmahos GC. Penetrating injuries of the chest: indicationsfor operation. Scand J Surg. 2002;91:41–45.
20. Kacker S, Bishai D, Mballa GA, Monono ME, Schneider EB, NgambyMK,Hyder AA, Juillard CJ. Socioeconomic correlates of trauma: an analysis ofemergency ward patients in Yaoundé, Cameroon. Injury. 2016;47:658–664.
21. Nantulya VM, Reich MR. Equity dimensions of road traffic injuries in low-and middle-income countries. Inj Control Saf Promot. 2003;10:13–20.
22. Livingston DH, Lavery RF, Lopreiato MC, Lavery DF, Passannante MR.Unrelenting violence: an analysis of 6,322 gunshot wound patients at a levelI trauma center. J Trauma Acute Care Surg. 2014;76:2–9.
965
ealth, Inc. All rights reserved.

Fu et al.J Trauma Acute Care Surg
Volume 86, Number 6
23. KyriacouDN, Hutson HR,Anglin D, Peek-Asa C, Kraus JF. The relationshipbetween socioeconomic factors and gang violence in the City of LosAngeles. J Trauma. 1999;46:334–339.
24. Sampson RJ, Rauenbush SW, Earls F. Neighborhoods and violentcrime: a multilevel study of collective efficacy. Science. 1997;277:918–924.
25. Nance ML, Carr BG, Kallan MJ, Branas CC, Wiebe DJ. Variation in pedi-atric and adolescent firearm mortality rates in rural and urban US counties.Pediatrics. 2010;125:1112–1118.
966
Copyright © 2019 Wolters Kluwer H
26. Anderson IA,Woodford M, de Dombal FT, IrvingM. Retrospective study of1000 deaths from injury in England and Wales. BMJ. 1988;296:1305–1308.
27. Kreis DJ Jr., Plasencia G, Augenstein D, Davis JH, Echenique M, Vopal J,Byers P, Gomez G. Preventable trauma deaths: Dade County, Florida. J Trauma.1986;26:649–654.
28. Blank-Reid C. A historical review of penetrating abdominal trauma. CritCare Nurs Clin North Am. 2006;18:387–401.
29. Isenhour JL,Marx J. Advances in abdominal trauma. EmergMed Clin NorthAm. 2007;25:713–733.
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
ORIGINAL ARTICLE
Assessment of safety and bleeding risk in the use ofextracorporeal membrane oxygenation for multitrauma patients:
A multicenter review
Natalie Kruit, MBBS, Michal Prusak, MUDr, Matthew Miller, MBBS,Nicholas Barrett, MBBS, Carla Richardson, MBChB, andAlain Vuylsteke, MD, Kogarah, New South Wales, Australia
Sub
Fro
Ad
Sup
DO
J TrVol
BACKGROUND: R
mitted: August 29, 2018, RevisPublished online: March 6, 201m Royal Papworth Hospital (NUnited Kingdom; UNSW St GKogarah, New South Wales, AuLambeth, London, United Kingddress for reprints: Natalie KruiAustralia 2031; email: nattiejpkplemental digital content is avaithe printed text, and links to thearticle on the journal’s Web sit
I: 10.1097/TA.00000000000022
auma Acute Care Surgume 86, Number 6
espiratory failure is the most common form of organ failure following traumatic injury. Previously, there have been concerns re-garding extracorporeal membrane oxygenation (ECMO) use in the trauma setting because of the increased risk of bleeding andthrombotic complications. We sought to examine the management of trauma patients with ECMO and to assess the safety and out-come of its use.
METHODS: D
ata of all patients who experienced a traumatic injury and were supported with ECMOwere collected from the five National Re-spiratory ECMO centers in the United Kingdom over the period from December 2011 to May 2017. Primary outcome variablesincluded 30-day and 6-month mortality and exacerbation of underlying traumatic injury after ECMO commencement. Secondaryoutcome variables included duration of ECMO support, thrombotic complications, and worsening of intracranial injury.RESULTS: F
ifty-two patients were identified. The overall hospital mortality was 15%. The incidence of bleeding complications was 50%, themajority of these not requiring intervention. Forty patients underwent surgical management prior to ECMO commencement; onlyfour patients required take-back to the operating theater. Therewas no significant difference between the bleeding and nonbleedinggroups in time of injury to ECMO commencement (median difference, 4.5 days; 95% CI, −3 to 3 days; p = 0.75). There was nostatistically significant difference between the bleeding and nonbleeding groups in regard to time to anticoagulation commence-ment after starting ECMO (median difference, − 1 hour; 95% CI, −48 to 2 hours; p = 0.29) or after trauma (median difference,− 1 day; 95% CI, −4 to 2 days; p = 0.41). Nineteen patients were diagnosed with significant neurological injury. Twelve of thesepatients were anticoagulated. Two patients died as a direct result of worsening neurological injury.CONCLUSIONS: O
ur findings suggest that the use of ECMO in trauma patients does not exacerbate primary traumatic injury regardless of antico-agulation commencement andmay confer a survival benefit. Neurological injury should not be seen as an absolute contraindication toECMO. (J Trauma Acute Care Surg. 2019;86: 967–973. Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.)LEVEL OF EVIDENCE: T
herapeutic/Care Management, Level V. KEYWORDS: A nticoagulation; bleeding; ECMO; mortality; trauma.R espiratory failure is the most frequent form of organ failurefollowing major trauma, occurring in 10% to 20% of pa-
tients.1–4 Reasons for respiratory failure in this population aremultifactorial and include transfusion-related lung injury,transfusion-associated circulatory overload, the concomitantpresence of chest injury, severe pulmonary contusion, andthrombotic and/or fat embolism from pelvic or long bone frac-tures.3,5,6 When lung injury occurs in the setting of majortrauma, it is associated with a mortality as high as 50% to80%.3,7 Deaths occur from the primary lung injury as well asthe secondary effects of hypoxemia, respiratory acidosis, and
ed: January 24, 2019, Accepted: February 7, 2019,9..K., M.P., A.V.), Papworth Everard, Cambridge,eorge Hospital & Sutherland Hospitals (M.M.),stralia; Guy's and St Thomas' Hospital (N.B., C.R.),om.t, MBBS (Hons), FANZCA, New South Wales,@gmail.com.lable for this article. Direct URL citations appear indigital files are provided in the HTML text of thise (www.jtrauma.com).
42
Copyright © 2019 Wolters Kluwer H
raised mean intrathoracic pressures on other organs, includingthe traumatically injured brain.
Support with extracorporeal membrane oxygenation(ECMO) offers potential benefits in trauma patients.8–14 Extra-corporeal membrane oxygenation is able to provide respiratoryand cardiovascular support for patients. Provided bleeding isrelatively well controlled, ECMO affords the ability to warmpatients in hemorrhagic shock and control acid-base balance,potentially avoiding the lethal triad of metabolic acidosis, co-agulopathy, and hypothermia that is the main challenge in themanagement of these patients.15 Systemic heparinization is akey issue for ECMO as ECMO can carry up to a 40% risk ofintracranial and surgical site bleeding with or withoutheparinization.16 Increasingly, evidence supports the use ofheparin-free ECMO runs1,4 potentially allowing multitraumapatients to be stabilized on ECMO while their primary injuryis definitively treated.17
We undertook a retrospective observational study to definethe outcomes of patients whowere referred for ECMOwith a pri-mary diagnosis of trauma.We aim to examine the management oftrauma patients with venovenous (VV) and venoarterial (VA)ECMO and assess the feasibility, safety, and outcome of its use.
967
ealth, Inc. All rights reserved.
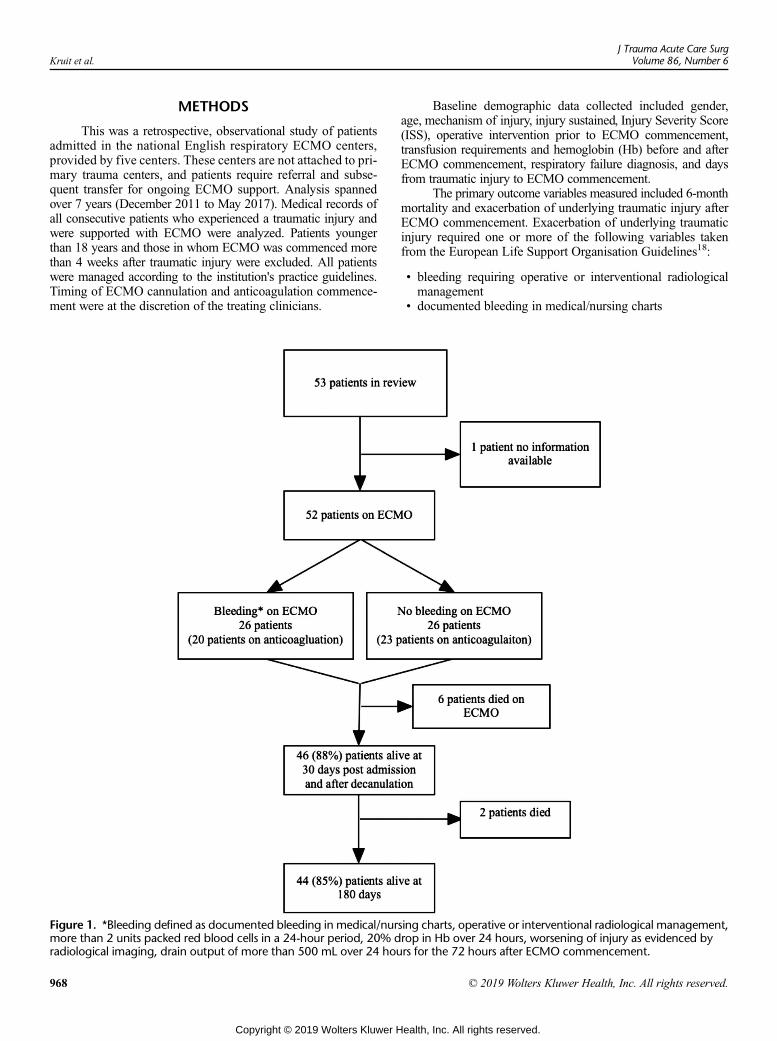
Kruit et al.J Trauma Acute Care Surg
Volume 86, Number 6
METHODS
This was a retrospective, observational study of patientsadmitted in the national English respiratory ECMO centers,provided by five centers. These centers are not attached to pri-mary trauma centers, and patients require referral and subse-quent transfer for ongoing ECMO support. Analysis spannedover 7 years (December 2011 to May 2017). Medical records ofall consecutive patients who experienced a traumatic injury andwere supported with ECMO were analyzed. Patients youngerthan 18 years and those in whom ECMO was commenced morethan 4 weeks after traumatic injury were excluded. All patientswere managed according to the institution's practice guidelines.Timing of ECMO cannulation and anticoagulation commence-ment were at the discretion of the treating clinicians.
Figure 1. *Bleeding defined as documented bleeding in medical/nurmore than 2 units packed red blood cells in a 24-hour period, 20% dradiological imaging, drain output of more than 500 mL over 24 hou
968
Copyright © 2019 Wolters Kluwer H
Baseline demographic data collected included gender,age, mechanism of injury, injury sustained, Injury Severity Score(ISS), operative intervention prior to ECMO commencement,transfusion requirements and hemoglobin (Hb) before and afterECMO commencement, respiratory failure diagnosis, and daysfrom traumatic injury to ECMO commencement.
The primary outcome variables measured included 6-monthmortality and exacerbation of underlying traumatic injury afterECMO commencement. Exacerbation of underlying traumaticinjury required one or more of the following variables takenfrom the European Life Support Organisation Guidelines18:
• bleeding requiring operative or interventional radiologicalmanagement
• documented bleeding in medical/nursing charts
sing charts, operative or interventional radiological management,rop in Hb over 24 hours, worsening of injury as evidenced byrs for the 72 hours after ECMO commencement.
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
J Trauma Acute Care SurgVolume 86, Number 6 Kruit et al.
• transfusion requirements of more than 2 units of packed redblood cells in a 24-hour period
• 20% drop in Hb over 24 hours• worsening of injury as evidenced by radiological imaging(ultrasound/computed tomography/magnetic resonance im-aging) and reported by the radiologist
• drain output of more than 500 mL over 24 hours for the72 hours after ECMO commencement
The secondary outcome variables included the following:• duration of ECMO support• thrombotic complications (patient thrombosis and circuitthrombosis)
• radiological evidence of worsening of head injury or new in-tracranial bleed after ECMO commencement
Statistical AnalysisAll analyses were performed with R statistical software
(version 3.4.3) (R Core Team, Vienna, Austria). Data were ex-amined for normality using the histograms and Shapiro test.Parametric and nonparametric descriptive statistics were pro-duced as appropriate. Where significance tests were performed,nonparametric tests were used. Categorical data were examinedusing the χ2 or Fisher exact test when expected cell outcomeswere less than 5. For all statistical tests, p = 0.05 was consideredsignificant. Logistic regression was performed with bleeding asthe outcome and ISS as the only predictor given our small sam-ple size.
TABLE 1. Demographic Data and Differences Between Survivors and
Demographic All Patients (n
Sex (male) 42 (81%)
Age, median (25th–75th percentile [range]), y 33 (25–45 [18–
Mechanism of injury
Road traffic collision (car) 18 (35%)
Road traffic collision (pedestrian) 8 (15%)
Fall 8 (15%)
Road traffic collision (motorbike) 7 (14%)
Road traffic collision (cyclist) 3 (6%)
Assault 4 (8%)
Helicopter crash 1 (2%)
Speedboat crash 1 (2%)
Missing data 1
Type of before ECMO surgery 40 (77%)
Orthopedic surgery only 11 (28%)
Neurosurgery only 7 (18%)
Laparotomy 5 (13%)
Laparotomy + orthopedic surgery 4 (10%)
Intercostal catheter only 3 (8%)
Cardiothoracic surgery only 3 (8%)
Orthopedic + intercostal catheter + neurosurgery 2 (5%)
Intercostal catheter + neurosurgery 1 (3%)
Orthopedic + intercostal catheter 1 (3%)
Laparotomy + neurosurgery 1 (3%)
Orthopedic + neurosurgery 1 (3%)
Laparotomy + thoracotomy 1 (3%)
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
RESULTS
Demographic DataFifty-two trauma patients requiring ECMO were identi-
fied from prospectively recorded databases held by the five Na-tional Respiratory ECMO centers in the United Kingdom duringthe 7-year study period (Fig. 1). There was a wide difference insample size between the sites ranging from 3 patients to18 patients (Supplemental digital content 1, Table 1, http://links.lww.com/TA/B303). The majority of patients were male(81%) and had a median age of 33 years (interquartile range[IQR], 25–45 years; range, 17–72 years; Table 1). The mostcommon mechanism of injury was road traffic collisions(35%). Venovenous ECMO support was used in 50 patientsand VA ECMO in 2 patients. Pulmonary contusions and acuterespiratory distress syndrome (ARDS) resulting in a lung injuryscore of 3 or more or pH of less than 7.20 due to respiratory ac-idosis were the main indications for ECMO support (Table 2).The median ISS was 35 (IQR, 25–56; range, 6–75). The medianduration of ECMO support was 7 days (IQR, 4–12 days; range,1–114 days).
The overall hospital mortality was 15% (n = 8). The over-all 180-day mortality was 15% (n = 8). Six deaths occurredwhile the patient was supported with ECMO, and two more oc-curred within 180 days (mean duration ECMO support in de-ceased patients, 2.6 days [range, 1–114 days]).
The leading cause of death, although infrequent, was cere-bral herniation (n = 2). One patient suffered cardiac arrest duringECMO cannulation and was placed onto VA ECMO support;
Nonsurvivors
= 52) Survivors (n = 44) Deaths (n = 8)
37 (84%) 5 (63%)
72]) 33 (23–45 [18–72]) 32 (26–37 [25–55])
16 (34%) 2 (25%)
6 (14%) 2 (25%)
7 (16%) 1 (13%)
7 (16%)
2 (5%) 1 (13%)
4 (7%) 1 (13%)
1 (2%)
1 (2%)
1 (13%)
33 (75%) 7 (88%)
9 (3%) 2 (29%)
5 (15%) 2 (29%)
4 (12%) 1 (14%)
4 (12%)
3 (9%)
2 (6%) 1 (14%)
2 (6%)
1 (3%)
1 (3%)
1 (3%)
1 (14%)
1 (3%)
969
ealth, Inc. All rights reserved.
TABLE 2. Respiratory Failure Diagnosis
Respiratory Failure DiagnosisAll Patients(n = 52)
Survivors(n = 44)
Nonsurvivors(n = 8)
Single respiratory problem (n = 30)
Contusion only 18 16 2
ARDS only 3 3
Fat embolism 3 2 1
Aspiration 2 1 1
Pneumonia 2 2
PE 1 1
Bronchial rupture 1 1
Two respiratory problems (n = 13)
Contusion, ARDS 6 5 1
ARDS, aspiration 1 1
Contusion, aspiration 1 1
Contusion, PE 1 1
Contusion, laceration 2 2
Contusion, VAP 1 1
Contusion, tracheal injury 1 1
>2 Respiratory problems (n = 8)
Contusion, ARDS, air embolism 1 1
Contusion, ARDS, aspiration, PE 2 1 1
Contusion, pneumonectomy, PE 1 1
Contusion, pneumonia, PE, air leak 1 1
Contusion, ARDS, aspiration 2 2
Aspiration, pneumonia, ARDS 1 1
PE indicates pulmonary embolism; VAP, ventilator-acquired pneumonia.
Kruit et al.J Trauma Acute Care Surg
Volume 86, Number 6
one death was secondary to mesenteric ischemia, and onedeath secondary to massive hemorrhage during lung trans-plant. The cause of death was unknown in three patients(Table 3). One patient required operative reintervention onECMO prior to succumbing to injury. Five patients experi-enced thrombosis on ECMO; however, this was not cited asthe primary cause of death in all but one case. The medianISS score among patients who died was 31 (range, 18–66).Survival at 30 days was 88% (n = 46), and survival at 180 dayswas 85% (n = 44).
TABLE 3. Characteristics of Nonsurvivors
Age, yMechanismOf Injury ISS
Pre-ECMOSurgery
RespiratoryFailure Diagnosis
On ECThrom
55 RTA: cyclist 66 EVD Aspiration No
33 RTA: pedestrian 41 Orthopedic EVD Contusion, aspiration,ARDS
PE
25 Unknown 41 No Contusion, ARDS DVT/PE
31 RTA: car 27 Thoracic Contusion, PE Oxygenator
26 RTA: car 30 Laparotomy Contusion Oxygenator
45 RTA: pedestrian 34 Orthopedic Contusion Oxygenatormesenteric
26 Assault 25 SDH evacuation Aspiration, ARDS No
34 Fall 18 Orthopedic Fat embolism No
DVT indicates deep vein thrombosis; OT, operating theater; PE, pulmonary embolism; RTA,
970
Copyright © 2019 Wolters Kluwer H
There was no association between ISS and 180-day sur-vival (median difference, 9; 95% CI, −7 to 27; p = 0.33). Mediantime from injury to commencement of ECMOwas 6 days (IQR,3–111 days; range, 1–24 days) (Table 4). There was no signifi-cant difference between survivors and nonsurvivors in time frominjury to ECMO commencement (median difference, 1 day;95% CI, −3 to 5; p = 0.65) and time from injury to anticoagula-tion commencement (median difference, 1 day; 95%CI, −4 to 7;p = 0.81).
Exacerbation of Primary Traumatic InjuryThe incidence of bleeding complications was 50%, the
majority of these not requiring intervention. Forty patients(77%) underwent surgical management prior to ECMO com-mencement. Four patients (7%) required repeat surgical interven-tion for worsening of liver laceration, worsening of hemothorax,development of compartment syndrome, and complications afterintercostal catheter insertion. One patient required operative inter-ventionwithin the first 72 hours of ECMOcommencement. Radio-logical evidence of worsening bleeding occurred in four patients(7%), with three occurring in the first 72 hours after ECMO com-mencement. Three patients experienced worsening of neurologicalinjury. Clinically reported bleeding not requiring intervention oc-curred in eight patients (15%), drain output greater than 500 mLover 24 hours occurred in 10 patients (20%), and a 20% drop inHb over 24 hours occurred in three patients (5%). Blood productusage did not differ before or after ECMO commencement (Sup-plemental digital content 2, Fig 1, http://links.lww.com/TA/B332).
The median ISS difference between the bleeding andnonbleeding groups was 9. Logistic regression analysis demon-strated ISS as a weak predictor for bleeding (odds ratio, 1.033;95%CI, 1.002–1.069; p = 0.04). Therewas no significant differ-ence between the bleeding and nonbleeding groups in time frominjury to commencement of ECMO (median difference,4.5 days; 95% CI, −3 to 3 days; p = 0.748) (Table 5).
AnticoagulationAnticoagulation was commenced in 43 patients (84%);
for 36 patients (65%), this was in the first 72 hours after ECMOcommencement. The median time from injury to anticoagulation
MObosis
On ECMOReturn to OT On ECMO ICH
ECMORun, d Cause of Death
No No 3 Cerebral herniation
No Yes 2 Cerebral herniation
No No 1 Unknown
failure No No 114 Massive hemorrhageduring lung transplant
failure Liver packing No 12 Unknown
failure,ischemia
No No 8 Mesenteric ischemia
No No 1 Cardiac arrest duringcannulation
No No 1 Unknown
road traffic accident; SDH, subdural hematoma.
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
TABLE 4. Measures of Illness Severity and Differences Between Survivors and Nonsurvivors
Variable All Patients (n = 52) Survivors (n = 44) Deaths (n = 8) p
Days from injury to ECMO, median (IQR [range]) 6 (3–11 [1–24]) 6 (3–11 [1–24]) 7 (3–8 [1–24]) 0.65
ISS, median (25–75 centile [range]) 35 (25–56 [6–75]) 36 (24–57 [6–75]) 2 9 (26–33 [18–41]) 0.33
SOFA score, median (25th–75th centile [range])(n = 48 [missing = 4])
12 (5–13 [3–19]) 12 (4–14 [3–19]) 12 (12–13 [3–13]) 0.84
Pre-ECMO FIO2, median (25th–75th centile [range]),mmHg (n = 35 [missing = 6])
100 (95–100 [40–100]) 100 (100–100 [40–100]) 100 (95–100 [70–100]) 0.58
Pre-ECMO PaO2, median (25th–75th centile [range]),mmHg (n = 36 [missing = 5])
62.2 (54.7–73.3 [31.5–120]) 63 (54–73.5 [31.5–120]) 60.8 (54.8–69.8 [48–90]) 0.86
Pre-ECMO PaCO2, median (25th–75th centile [range]),mmHg (n = 36 [missing = 5])
63.8 (52.5–72 [20.3–157.5]) 63.8 (52.5–71.3 [20.3–157.5]) 63.8 (55.5–74.3 [38.3–81.8]) 0.94
SOFA indicates Sepsis-related Organ Failure Assessment.
J Trauma Acute Care SurgVolume 86, Number 6 Kruit et al.
commencement was 7 days (IQR, 5–13 days; range, 1–26 days).Median time fromECMO to anticoagulation commencement was3 hours (IQR, 0–72 hours; range, 0–204 hours). In the 26 patientswho experienced bleeding complications, 20 (77%) had receivedanticoagulation. There was no statistically significant differencebetween the bleeding and nonbleeding groups in regard to timeto anticoagulation commencement after starting ECMO (mediandifference, − 1 hour; 95% CI, −48 to 2 hours; p = 0.29) or aftertrauma (median difference, − 1 day; 95% CI, −4 to 2 days;p = 0.41) (Table 5).
In the group of patients who bled and were anticoagulated,14 of those patients experienced drain output of greater than500mL in the 72-hour period. Two patients experienced surgicalsite bleeding but did not require take-back to theater; nine pa-tients required more than 2 units of packed red blood cells in a24-hour period, and this was mostly associated with increaseddrain output.
Thrombotic ComplicationsThrombotic complications occurred in 21 patients (39%),
16 (76%) of whom were anticoagulated at the time thrombosisoccurred. The main thrombotic complication was oxygenatorfailure (n = 8) and deep vein thrombosis (n = 8), followed by pul-monary embolism (n = 3). There was no significant differencebetween the anticoagulated and nonanticoagulated groups in re-gard to thrombosis rate (odds ratio, 1.7; 95% CI, 0.45–6.11;p = 0.48).
Worsening of Neurological InjurySignificant neurological injury was diagnosed in
19 patients prior to ECMO commencement. Three patients with
TABLE 5. Differences in Predictors of Bleeding Between the Bleeding
VariableHem
Age, median (25th–75th centile)
ISS, median (25th–75th centile)
Injury to ECMO time, median days (25th–75th centile)
Injury to anticoagulation time, median days (25th–75th centile)
Anticoagulation commencement in 1st 72 h after ECMO initiation (no. patients)
Trauma to anticoagulation time is time interval between traumatic injury and commencement omencement on ECMO.
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
traumatic brain injury (TBI) died (16%): two died of cerebralherniation (mean ECMO duration, 2 days) and the other onedied of cardiac arrest secondary to hypovolemia during cannula-tion. Twelve patients with TBI (63%) were anticoagulated. Neu-rosurgical intervention occurred in 12 patients prior to ECMO;the majority of these interventions were for intracranial pressuremonitoring and/or external ventricular drain (EVD) insertion.There was radiological evidence of further cerebral hemorrhagein three patients while on ECMO; two of these patients had neu-rosurgical procedures prior to ECMO, and none of these patientsreceived anticoagulation while on ECMO.
DISCUSSION
We describe the experience of the UK national severe re-spiratory failure network supporting 52 patientswith ECMO fol-lowing traumatic injury over a 7-year period. The populationhad a median age of 33 years and a median ISS of 35. Despitethis, the 6-month survival was 85%, suggesting that ECMO isboth feasible and safe in a carefully selected trauma population.The current findings do not support neurological injury as an ab-solute contraindication to ECMO.
The 6-month survival rate of 85% compares to a reportedsurvival rate of 55% to 76% in the general ARDS populationsupported with VV ECMO.16,19–21 However, the cohort in thisstudy is likely younger (median age, 33 years) than the generalARDS population, which may have influenced the results. Oursurvival rate is in keeping with previous reports describing themanagement of trauma patients with ECMO.4,8,9,22–24 One re-cent systematic review combining 215 trauma patients supported
Group and Nonbleeding Group
orrhagic Complication(n = 26 [50%])
No Hemorrhagic Complication(n = 26 [50%])
Median Differenceand (p)
30 (24–37) 36 (27–50) −7 (0.05)
39 (28–57) 27 (21–51) 9 (0.04)
7 (3.0–12) 6 (4–10) 4.5 (0.75)
7 (4–14) 8 (6–13) −1 (0.4)
17 (65%) 9 (35%) χ2 = 0.76
f anticoagulation. Trauma to ECMO time is time interval between traumatic injury and com-
971
ealth, Inc. All rights reserved.

Kruit et al.J Trauma Acute Care Surg
Volume 86, Number 6
with ECMO reported a survival to discharge after VV ECMOranging from 56% to 89% and 42% to 63% in VA ECMO.4
Our study demonstrated no difference in characteristics or treat-ment times between survivors and nonsurvivors, making it diffi-cult to predict the subset of trauma patients who would benefitfrom ECMO.
There was an overall incidence of bleeding complicationsof 50% in this series. A total of 77% of patients had surgicalmanagement prior to ECMO commencement, and the cohorthad a median ISS of 35, both of which are established risk fac-tors for bleeding. Extracorporeal membrane oxygenation isknown to exacerbate bleeding risk with an established incidenceof bleeding of 33% while on ECMO described in a meta-analysis of 2,070 patients25 and correlates with the evidence todate.4,13,23 Despite this increased risk, most bleeding complica-tions were managed conservatively, with only 7% of all patientsrequiring surgical intervention.
There was a weak correlation between ISS score andbleeding. The median ISS difference between the bleeding andnonbleeding groups was 9. An ISS difference of 9 may indicateserious injury to one of six body systems and is not clinically in-significant. The weak correlation may be underestimated be-cause of the small study sample size.
The low incidence of major hemorrhage could be attrib-uted to the median injury to ECMO time of 6 days. Delay incommencement of ECMO after injury may have allowed timefor the trauma-induced coagulopathy that is often present in thispopulation to settle26 and may allow primary hemostasis to oc-cur. The hypothesis that the fewer bleeding complications occur,the greater the time from injury to ECMO commencement issupported by previous research. Comparatively, Ried et al.10 de-scribe a major hemorrhage incidence of 4% with a median timefrom trauma to commencement of ECMO 4.5 days, whereasWuet al.11 found a 35% incidence of major hemorrhage when themedian time from trauma to commencement of ECMO was10 hours.
The majority of patients enrolled in this study (65%) re-ceived anticoagulation within the first 72 hours of ECMO, witha median time from trauma to commencement of anticoagula-tion of 7 days. This included 63% of patients with a TBI. Hepa-rin was commenced earlier in the nonbleeding group and islikely due to patients at risk of bleeding having heparin withheld.
There was no significant difference in bleeding incidencebetween the anticoagulated and nonanticoagulated groups. Theabsence of difference may be attributed to the multifactorial na-ture of bleeding in both the trauma and ECMO populations.Platelet activation, inflammation, and consumption of clottingfactors all occur in response to the contact activation of bloodwith the artificial membrane and contribute to the risk of bleed-ing associated with ECMO.27
Thrombotic complications occurred in 39% of patients inthis study, nearly half of which were circuit-related thrombosis,with the remainder as deep vein thrombosis. This compares toa reported 20% thrombosis rate described in the 2014 ESLO reg-istry data28 and similar to the incidence of deep vein thrombosispreviously reported following decannulation fromVVECMO.29
Seventy-six percent of patients with evidence of thrombosis inour study were anticoagulated at the time. Given that ECMOcan be run safely for prolonged periods of time without
972
Copyright © 2019 Wolters Kluwer H
anticoagulation4,8 and the complex disruption of the clottingequilibrium that can occur in response to both trauma andECMO,26 the need for anticoagulation should be consideredon an individual patient basis.
Acute respiratory distress syndrome can occur in up to20% to 30% of patients with TBI,4 and spontaneous intracranialhemorrhage (ICH) is known to occur in patients receivingECMO for severe respiratory failure.30 Until recently, TBI hasbeen considered a relative contraindication to ECMO becauseof the risk of worsening ICH associated with anticoagulation.31
Anticoagulation was commenced in the majority of patients inthis study with known TBI and was not associated with worsen-ing ICH.
Our findings are in keeping with the results from a sys-tematic review conducted by Bedeir et al.,4 who reported that19 of 23 patients with traumatic ICH supported with ECMO sur-vived, and the other four mortalities were not attributed to in-creasing ICH. The main tenet of TBI management is to reducesecondary brain injury by maintaining adequate oxygenation,normocarbia, and cerebral perfusion32; this strategy can oftenbe at odds with lung protective ventilation strategies. It seemsreasonable that ECMO can assist in reducing secondary brain in-jury and improve outcome. Although anticoagulation commence-ment does not appear to be associated with worsening ICH, thenumbers in this study are small. Anticoagulation regimens in thispopulation of patients should be individually tailored, taking intoaccount timing and severity of neurological injury.
This study has several limitations. The retrospective de-sign and small sample size make it difficult to adequately assesspredictors of survival or draw conclusions with certainty. Selec-tion bias may have contributed to the favorable survival ratesdemonstrated. All clinical decisions were at the discretion ofthe treating clinician spanning multiple institutions, making thecare patients received nonstandardized. Significant data weremissing on clotting function, making it difficult to assesstargeted anticoagulation therapy and the risk of bleeding. Posthoc power calculations demonstrated the power of this studywas low (0.05). This is because of the small effect sizes foundbetween groups when the sample size was divided into bleedingand nonbleeding patients. We consider this to be an importantfinding as it demonstrates that in order to truly understand therisks for bleeding, correctly powered prospective studies or acentralized registry is needed.
CONCLUSIONS
The use of ECMO in trauma patients does not exacerbateprimary traumatic injury regardless of anticoagulation commence-ment and is not associated with aworsening survival rate. The cur-rent findings do not support neurological injury as an absolutecontraindication to ECMO; however, the current evidence is insuf-ficient to conclude that it is safe. The favorable outcomes seen inthis study may be attributed to the delayed timing in ECMO com-mencement after injury and the identification of patients at highrisk of bleeding resulting in anticoagulation omission.
AUTHORSHIP
N.K. is the lead investigator, collected the data, designed the study, andperformed literature search. M.P. collected the data, designed the study,
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
J Trauma Acute Care SurgVolume 86, Number 6 Kruit et al.
and revised the manuscript. M.M. performed the statistical analysis. N.B.and A.V. designed the study and revised the manuscript. C.R. collectedthe data and revised the manuscript.
ACKNOWLEDGMENTS
The authors thank Chris Harvey, MBChB,MRCS, clinical director of ECMOservices, Glenfield Hospital, Leicester, United Kingdom; Alan Ashworth,MBChB, FCICM/FRCA, and Chinmay Patvardhan, MBChB, FRCA, con-sultants, Anaesthesia and Intensive Care, University Hospital of SouthManchester, Wythenshawe, Manchester, United Kingdom; and BrijishPatel, PhD, FRCA, consultant anesthetist, Royal BromptonHospital, Chelsea,London, United Kingdom.
DISCLOSURE
The authors declare no conflicts of interest.
REFERENCES1. Huang YK, Liu KS, Lu MS, Wu MY, Tsai FC, Lin PJ. Extracorporeal life
support in post-traumatic respiratory distress patients. Resuscitation. 2009;80(5):535–539.
2. Treggiari MM, Hudson LD,Martin DP,Weiss NS, Caldwell E, Rubenfeld G.Effect of acute lung injury and acute respiratory distress syndrome on out-come in critically ill trauma patients. Crit Care Med. 2004;32(2):327–331.
3. Watkins TR, Nathens AB, Cooke CR, Psaty BM, Maier RV, Cuschieri J,Rubenfeld GD. Acute respiratory distress syndrome after trauma: develop-ment and validation of a predictive model. Crit Care Med. 2012;40(8):2295–2303.
4. Bedeir K, Seethala R, Kelly E. Extracorporeal life support in trauma: Worththe risks? A systematic review of published series. J Trauma Acute CareSurg. 2017;82(2):400–406.
5. Durham RM, Moran JJ, Mazuski JE, Shapiro MJ, Baue AE, Flint LM. Mul-tiple organ failure in trauma patients. J Trauma. 2003;55(4):608–616.
6. Silverboard H, Aisiku I, Martin GS, Adams M, Rozycki G, Moss M. Therole of acute blood transfusion in the development of acute respiratory distresssyndrome in patients with severe trauma. J Trauma. 2005;59(3):717–723.
7. Navarrete-Navarro P, Ruiz-Bailen M, Rivera-Fernandez R, Guerrero-Lopez F,Pola-Gallego-de-Guzman MD, Vazquez-Mata G. Acute respiratory distresssyndrome in trauma patients: ICU mortality and prediction factors. IntensiveCare Med. 2000;26(11):1624–1629.
8. Arlt M, Philipp A, Voelkel S, Rupprecht L, Mueller T, Hilker M, Graf BM,Schmid C. Extracorporeal membrane oxygenation in severe trauma patientswith bleeding shock. Resuscitation. 2010;81(7):804–809.
9. Cordell-Smith JA, Roberts N, Peek GJ, Firmin RK. Traumatic lung injurytreated by extracorporeal membrane oxygenation (ECMO). Injury. 2006;37(1):29–32.
10. Ried M, Bein T, Philipp A, Müller T, Graf B, Schmid C, Zonies D, Diez C,Hofmann HS. Extracorporeal lung support in trauma patients with severechest injury and acute lung failure: a 10-year institutional experience. CritCare. 2013;17(3):R110.
11. Wu MY, Lin PJ, Tseng YH, Kao KC, Hsiao HL, Huang CC. Venovenousextracorporeal life support for posttraumatic respiratory distress syn-drome in adults: the risk of major hemorrhages. Scand J Trauma ResuscEmerg Med. 2014;22:56.
12. Gothner M, Buchwald D, Strauch JT, Schildhauer TA, Swol J. The use ofdouble lumen cannula for veno-venous ECMO in trauma patients withARDS. Scand J Trauma Resusc Emerg Med. 2015;23:30.
13. Bosarge PL, Raff LA,McGwin G Jr., Carroll SL, Bellot SC, Diaz-Guzman E,Kerby JD. Early initiation of extracorporeal membrane oxygenation im-proves survival in adult trauma patients with severe adult respiratory distresssyndrome. J Trauma Acute Care Surg. 2016;81(2):236–243.
14. MadershahianN,Wittwer T, Strauch J, FrankeUF,Wippermann J, KaluzaM,Wahlers T. Application of ECMO inmultitrauma patients with ARDS as res-cue therapy. J Card Surg. 2007;22(3):180–184.
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
15. Dreizin D, Menaker J, Scalea TM. Extracorporeal membranous oxygenation(ECMO) in polytrauma: what the radiologist needs to know. Emerg Radiol.2015;22(5):565–576.
16. Paden ML, Conrad SA, Rycus PT, Thiagarajan RR; ELSO Registry. Extra-corporeal Life Support Organization Registry Report 2012. ASAIO J.2013;59(3):202–210.
17. Perchinsky MJ, Long WB, Hill JG, Parsons JA, Bennett JB. Extracorporealcardiopulmonary life support with heparin-bonded circuitry in the resuscita-tion of massively injured trauma patients. Am J Surg. 1995;169(5):488–491.
18. ELSO. ELSOAnticoagulation Guideline. 2014.19. ARDS Definition Task Force, Ranieri VM, Rubenfeld GD, Thompson BT,
Ferguson ND, Caldwell E, Fan E, Camporota L, Slutsky AS. Acute respira-tory distress syndrome: the Berlin Definition. JAMA. 2012;307(23):2526–2533.
20. Noah MA, Peek GJ, Finney SJ, Griffiths MJ, Harrison DA, Grieve R,Sadique MZ, Sekhon JS, McAuley DF, Firmin RK, et al. Referral to an ex-tracorporeal membrane oxygenation center and mortality among patientswith severe 2009 influenza A(H1N1). JAMA. 2011;306(15):1659–1668.
21. Extracorporeal Life Support Organisation. Extracorporeal Life Support Or-ganisation data registry. 2018.
22. Michaels AJ, Schriener RJ, Kolla S, Awad SS, Rich PB, Reickert C,Younger J, Hirschl RB, Bartlett RH. Extracorporeal life support in pulmo-nary failure after trauma. J Trauma. 1999;46(4):638–645.
23. Jacobs JV, Hooft NM, Robinson BR, Todd E, Bremner RM, Petersen SR,SmithMA. The use of extracorporeal membrane oxygenation in blunt thoracictrauma: A study of the Extracorporeal Life Support Organization database. JTrauma Acute Care Surg. 2015;79(6):1049–1053; discussion 1053–54.
24. Guirand DM, Okoye OT, Schmidt BS, Mansfield NJ, Aden JK, Martin RS,Cestero RF, Hines MH, Pranikoff T, Inaba K, et al. Venovenous extracorpo-real life support improves survival in adult trauma patients with acute hypox-emic respiratory failure: a multicenter retrospective cohort study. J TraumaAcute Care Surg. 2014;76(5):1275–1281.
25. Zangrillo A, Landoni G, Biondi-Zoccai G, Greco M, Greco T, Frati G,Patroniti N, Antonelli M, Pesenti A, Pappalardo F. A meta-analysis of com-plications and mortality of extracorporeal membrane oxygenation. Crit CareResusc. 2013;15(3):172–178.
26. Frith D, Brohi K. The pathophysiology of trauma-induced coagulopathy.Curr Opin Crit Care. 2012;18(6):631–636.
27. Murphy DA, Hockings LE, Andrews RK, Aubron C, Gardiner EE,Pellegrino VA, Davis AK. Extracorporeal membrane oxygenation-hemostatic complications. Transfus Med Rev. 2015;29(2):90–101.
28. ESLO. ELSO Anticoagulation Guideline. 2014 accessed 01/02/2018 [Avail-able from: https://www.elso.org/portals/0/files/elsoanticoagulationguideline8-2014-table-contents.pdf.
29. Cooper E, Burns J, Retter A, Salt G, Camporota L, Meadows CI,Langrish CC, Wyncoll D, Glover G, Ioannou N, et al. Prevalence of VenousThrombosis Following Venovenous Extracorporeal Membrane Oxygenationin Patients With Severe Respiratory Failure. Crit Care Med. 2015;43(12):e581–e584.
30. Lockie CJA, Gillon SA, Barrett NA, Taylor D, Mazumder A, Paramesh K,Rowland K, Daly K, Camporota L, Meadows CIS, et al. Severe RespiratoryFailure, Extracorporeal Membrane Oxygenation, and Intracranial Hemor-rhage. Crit Care Med. 2017;45(10):1642–1649.
31. Peek GJ, Elbourne D, Mugford M, Tiruvoipati R, Wilson A, Allen E,Clemens F, Firmin R, Hardy P, Hibbert C, et al. Randomised controlled trialand parallel economic evaluation of conventional ventilatory support versusextracorporeal membrane oxygenation for severe adult respiratory failure(CESAR). Health Technol Assess. 2010;14(35):1–46.
32. C. CNTAOR. Guidelines for the management of severe Traumatic Brain In-jury. 2016 [4th accessed 16/03/2018:[Available from: https://www.braintrauma.org/uploads/13/06/Guidelines_for_Management_of_Severe_TBI_4th_Edition.pdf.
973
ealth, Inc. All rights reserved.
ORIGINAL ARTICLE
The associations between initial radiographic findingsand interventions for renal hemorrhage after high-grade
renal trauma: Results from the Multi-InstitutionalGenitourinary Trauma Study
Sorena Keihani, MD, Bryn E. Putbrese, MD, Douglas M. Rogers, MD, Chong Zhang, MS, Raminder Nirula, MD,Xian Luo-Owen, PhD, Kaushik Mukherjee, MD, Bradley J. Morris, RN, Sarah Majercik, MD, MBA,
Joshua Piotrowski, MD, PhD, Christopher M. Dodgion, MD, MSPH, Ian Schwartz, MD, Sean P. Elliott, MD, MS,Erik S. DeSoucy, DO, Scott Zakaluzny, MD, Brenton G. Sherwood, MD, Bradley A. Erickson, MD, MS,Nima Baradaran, MD, Benjamin N. Breyer, MD, MAS, Cameron N. Fick, MS, Brian P. Smith, MD,
BarbaraU.Okafor,MBA,RezaAskari,MD, BrandiMiller, DO,RichardA. Santucci,MD,MatthewM.Carrick,MD,Jurek F. Kocik, MD, Timothy Hewitt, MD, Frank N. Burks, MD, Marta E. Heilbrun, MD, Jeremy B. Myers, MD,
and in conjunction with the Trauma and Urologic Reconstruction Network of Surgeons, Salt Lake City
AAST Continuing Medical Education Article
Accreditation StatementThis activity has been planned and implemented in accordance with the Es-sential Areas and Policies of the Accreditation Council for Continuing MedicalEducation through the joint providership of the American College of Surgeonsand the American Association for the Surgery of Trauma. The AmericanCollege Surgeons is accredited by the ACCME to provide continuing medicaleducation for physicians.
AMA PRA Category 1 Credits™The American College of Surgeons designates this journal-based CME activity fora maximum of 1 AMA PRA Category 1 Credit™. Physicians should claim only thecredit commensurate with the extent of their participation in the activity.
Of the AMA PRA Category 1 Credit™ listed above, a maximum of 1 creditmeets the requirements for self-assessment.
Credits can only be claimed online
ObjectivesAfter reading the featured articles published in the Journal of Trauma and AcuteCare Surgery, participants should be able to demonstrate increased understandingof the material specific to the article. Objectives for each article are featured at thebeginning of each article and online. Test questions are at the end of the article,with a critique and specific location in the article referencing the question topic.
Claiming CreditTo claim credit, please visit the AAST website at http://www.aast.org/ and click onthe “e-Learning/MOC” tab. You must read the article, successfully complete thepost-test and evaluation. Your CME certificate will be available immediately uponreceiving a passing score of 75% or higher on the post-test. Post-tests receiving ascore of below 75% will require a retake of the test to receive credit.
System RequirementsThe system requirements are as follows: Adobe® Reader 7.0 or above installed; Internet Explorer® 7 and above; Firefox® 3.0 and above, Chrome® 8.0 and above, or
Safari™ 4.0 and above.
QuestionsIf you have any questions, please contact AAST at 800-789-4006. Paper test and evaluations will not be accepted.
Disclosure InformationIn accordance with the ACCME Accreditation Criteria, the American College of
Surgeons, as the accredited provider of this journal activity, must ensure that anyone
in a position to control the content of J Trauma Acute Care Surg articles selected for
CME credit has disclosed all relevant financial relationships with any commercial
interest. Disclosure forms are completed by the editorial staff, associate editors,
reviewers, and all authors. The ACCME defines a `commercial interest' as “any
entity producing, marketing, re-selling, or distributing health care goods or services
consumed by, or used on, patients.” “Relevant” financial relationships are those (in
any amount) that may create a conflict of interest and occur within the 12’months
preceding and during the time that the individual is engaged in writing the article. All
reported conflicts are thoroughly managed in order to ensure any potential bias
within the content is eliminated. However, if you’perceive a bias within the article,
please report the circumstances on the evaluation form.
Please note we have advised the authors that it is their responsibility to disclose within
the article if they are describing the use of a device, product, or drug that is not FDA
approved or the off-label use of an approved device, product, or drug or unapproved usage.
Disclosures of Significant Relationships withRelevant Commercial Companies/Organizationsby the Editorial StaffErnest E. Moore, Editor: PI, research support and shared U.S. patents Haemonetics;
PI, research support, Instrumentation Laboratory, Inc.; Co-founder, Thrombo Thera-
peutics. Associate Editors David Hoyt, Ronald V. Maier and Steven Shackford have
nothing to disclose. Editorial staff and Angela Sauaia have nothing to disclose.
Author DisclosuresSean P. Elliot, Co-author – Urotronic, Percuvision; Boston Scientific – Money/Grant.
Reviewer DisclosuresThe reviewers have nothing to disclose.
CostFor AAST members and Journal of Trauma and Acute Care Surgery subscribersthere is no charge to participate in this activity. For those who are not a memberorsubscriber, the cost for each credit is $25.
974J Trauma Acute Care Surg
Volume 86, Number 6
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 6 Keihani et al.
BACKGROUND: Indications for intervention after high-grade renal trauma (HGRT) remain poorly defined. Certain radiographic findings can be
Sub
Fro
©
mitted: January 24, 2019, Acce11, 2019.m the Division of Urology, DepRadiology (B.E.P., D.M.R.), DMedicine (C.Z.), DepartmentCity, Utah; Division of Acute Csity Medical Center, Loma LinCritical Care (B.J.M., S.M), Intement of Urology (J.P.), DepartmMilwaukee, Wisconsin; DepartMedical Center, University ofof Surgery (E.S.D.); Division ofCare, Department of Surgery (Ster, Sacramento, California; DeIowa, IowaCity, Iowa; DepartmenSanFrancisco, SanFrancisco,Ca(C.N.F., B.P.S), Hospital of the U
2019 Wolters Kluwer Heal
used to guide the management of HGRT. We aimed to assess the associations between initial radiographic findings and interven-tions for hemorrhage after HGRT and to determine hematoma and laceration sizes predicting interventions.
METHODS: T
he Genitourinary Trauma Study is a multicenter study including HGRT patients from 14 Level I trauma centers from 2014 to 2017.Admission computed tomography scans were categorized based on multiple variables, including vascular contrast extravasation(VCE), hematoma rim distance (HRD), and size of the deepest laceration. Renal bleeding interventions included angioembolization,surgical packing, renorrhaphy, partial nephrectomy, and nephrectomy. Mixed-effect Poisson regression was used to assess theassociations. Receiver operating characteristic analysis was used to define optimal cutoffs for HRD and laceration size.RESULTS: I
n the 326 patients, injury mechanism was blunt in 81%. Forty-seven (14%) patients underwent 51 bleeding interventions, includ-ing 19 renal angioembolizations, 16 nephrectomies, and 16 other procedures. In univariable analysis, presence of VCE was asso-ciated with a 5.9-fold increase in risk of interventions, and each centimeter increase in HRD was associated with 30% increase inrisk of bleeding interventions. An HRD of 3.5 cm or greater and renal laceration depth of 2.5 cm or greater were most predictive ofinterventions. In multivariable models, VCE and HRD were significantly associated with bleeding interventions.CONCLUSION: O
ur findings support the importance of certain radiographic findings in prediction of bleeding interventions after HGRT. Thesefactors can be used as adjuncts to renal injury grading to guide clinical decision making. (J Trauma Acute Care Surg. 2019;86:974–982. Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.)LEVEL OF EVIDENCE: P
rognostic and Epidemiological Study, Level III and Therapeutic/Care Management, Level IV. KEYWORDS: R enal trauma; nephrectomy; conservative treatment; computed tomography; wounds and injuries; trauma centers; multicenter study.M anagement of renal trauma has changed dramatically dur-ing the past two decades, and the majority of injuries are
now managed nonoperatively.1,2 This paradigm shift, and thewidespread use of computed tomography (CT) scans for traumaevaluation, has led to investigation of radiographic findings thatcan guide decisions for management of severe injuries. Currentevidence suggests that some CT findings, such as hematomaand laceration characteristics, are associated with bleeding con-trol interventions.2,3 For example, vascular contrast extravasa-tion (VCE) and large perirenal hematomas have been shown tobe highly associated with the need for endovascular or openprocedures.4–10 However, most data are from single-center studieswith a small number of interventions. Validation of these findingsin a multicenter setting with a larger cohort is needed.
The 1989 American Association for the Surgery ofTrauma (AAST) organ injury scale is commonly used to graderenal injuries. However, it was initially developed based uponsurgical findings in an era when open exploration was the stan-dard of care for renal trauma management.11 This grading sys-tem does not incorporate some important CT findings such asVCE and hematoma size and was not designed to predict therisk of bleeding control interventions. For instance, a lacerationdepth of 1 cm is used as a criterion in the AAST grading to sep-arate grade II and III injuries, which has not been validated in
pted: February 20, 2019, Published online: March
artment of Surgery (S.K., J.B.M.), Department ofivision of Epidemiology, Department of Internalof Surgery (R.N.), University of Utah, Salt Lakeare Surgery (X. L-O, K.M), Loma Linda Univer-da, California; Division of Trauma and Surgicalrmountain Medical Center, Murray, Utah; Depart-ent of Surgery (C.M.D.), University ofWisconsin,ment of Urology (I.S., S.P.E.), Hennepin CountyMinnesota, Minneapolis, Minnesota; DepartmentTrauma,Acute Care Surgery, and Surgical Critical.Z.), University of California Davis Medical Cen-partment of Urology (B.G.S., BA.E), University oft of Urology (N.B., B.N.B.), University of California-lifornia;Division of Trauma andSurgicalCriticalCareniversity of Pennsylvania, Philadelphia, Pennsylvania;
th, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
studies as having prognostic importance.11 Additionally, varioushematoma size cutoffs from 2 cm to 6 cm4–6,10 have been sug-gested to predict the need for bleeding intervention, but the op-timal cutoff point remains unknown.
We hypothesize that specific radiographic findings, be-yond the AAST renal injury grading system, are associated withbleeding interventions after high-grade renal trauma (HGRT).We aimed to use a multi-institutional database of HGRT to ex-plore the associations between these CT findings and interven-tions. To improve the clinical application, we also aim to findthe cutoff points for hematoma and laceration size that optimizeprediction of undergoing bleeding control interventions.
PATIENTS AND METHODS
Study DesignFrom 2014 to 2017, data were collected from adult pa-
tients with HGRT as part of the Multi-institutional Genitouri-nary Trauma Study (MiGUTS, http://www.turnsresearch.org/page/aast-gu-trauma-study-group-author-list-renal-trauma). Detailson the renal trauma study protocol and data collection havebeen previously published.12 In brief, the study is a multi-institutional, prospective, collaborative effort supported by theAAST multi-institutional trials committee, in conjunction with
Division of Trauma, Department of Surgery (B.U.O., R.A.), Brigham and Women'sHospital, Boston, Massachusetts; Department of Urology (B.M., R.A.S), DetroitMedical Center, Detroit, Michigan; Medical City Plano (M.M.C.), Plano; Depart-ment of Surgery (J.F.K.), East Texas Medical Center, Tyler, Texas; Department ofUrology (T.H., F.N.B.), Oakland University William Beaumont School of Medi-cine, Royal Oak, Michigan; Department of Radiology and Imaging Sciences(M.E.H.), Emory University Hospital, Atlanta, Georgia.
Address for reprints: Sorena Keihani, MD, Division of Urology, Department ofSurgery University of Utah School of Medicine 30 North 1900 East, Salt LakeCity, UT 84132; email: [email protected].
This abstract of this work is accepted for presentation at the 114th Annual Meeting ofthe American Urological Association (AUA), 3–6 May 2019, Chicago, IL.
Supplemental digital content is available for this article. Direct URL citations appear inthe printed text, and links to the digital files are provided in the HTML text of thisarticle on the journal’s Web site (www.jtrauma.com).
DOI: 10.1097/TA.0000000000002254
975
ealth, Inc. All rights reserved.
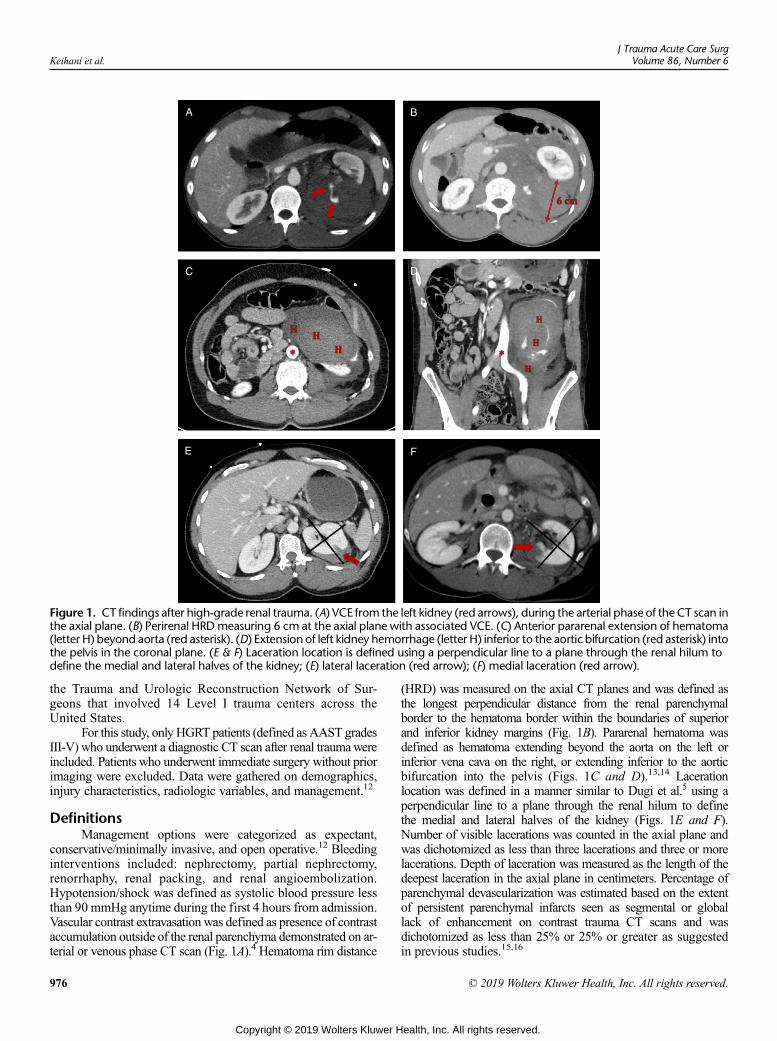
Figure 1. CT findings after high-grade renal trauma. (A) VCE from the left kidney (red arrows), during the arterial phase of the CT scan inthe axial plane. (B) Perirenal HRDmeasuring 6 cm at the axial plane with associated VCE. (C) Anterior pararenal extension of hematoma(letter H) beyond aorta (red asterisk). (D) Extension of left kidney hemorrhage (letter H) inferior to the aortic bifurcation (red asterisk) intothe pelvis in the coronal plane. (E & F) Laceration location is defined using a perpendicular line to a plane through the renal hilum todefine the medial and lateral halves of the kidney; (E) lateral laceration (red arrow); (F) medial laceration (red arrow).
Keihani et al.J Trauma Acute Care Surg
Volume 86, Number 6
the Trauma and Urologic Reconstruction Network of Sur-geons that involved 14 Level I trauma centers across theUnited States.
For this study, only HGRT patients (defined as AAST gradesIII-V) who underwent a diagnostic CT scan after renal traumawereincluded. Patients who underwent immediate surgery without priorimaging were excluded. Data were gathered on demographics,injury characteristics, radiologic variables, and management.12
DefinitionsManagement options were categorized as expectant,
conservative/minimally invasive, and open operative.12 Bleedinginterventions included: nephrectomy, partial nephrectomy,renorrhaphy, renal packing, and renal angioembolization.Hypotension/shock was defined as systolic blood pressure lessthan 90 mmHg anytime during the first 4 hours from admission.Vascular contrast extravasation was defined as presence of contrastaccumulation outside of the renal parenchyma demonstrated on ar-terial or venous phase CT scan (Fig. 1A).4 Hematoma rim distance
976
Copyright © 2019 Wolters Kluwer H
(HRD) was measured on the axial CT planes and was defined asthe longest perpendicular distance from the renal parenchymalborder to the hematoma border within the boundaries of superiorand inferior kidney margins (Fig. 1B). Pararenal hematoma wasdefined as hematoma extending beyond the aorta on the left orinferior vena cava on the right, or extending inferior to the aorticbifurcation into the pelvis (Figs. 1C and D).13,14 Lacerationlocation was defined in a manner similar to Dugi et al.5 using aperpendicular line to a plane through the renal hilum to definethe medial and lateral halves of the kidney (Figs. 1E and F).Number of visible lacerations was counted in the axial plane andwas dichotomized as less than three lacerations and three or morelacerations. Depth of laceration was measured as the length of thedeepest laceration in the axial plane in centimeters. Percentage ofparenchymal devascularization was estimated based on the extentof persistent parenchymal infarcts seen as segmental or globallack of enhancement on contrast trauma CT scans and wasdichotomized as less than 25% or 25% or greater as suggestedin previous studies.15,16
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 6 Keihani et al.
Radiologic Data ExtractionAll deidentified CT scans were uploaded to a secureWeb-
based Orthanc17 server for central review. Imaging data werecollected and managed using Research Electronic Data Capture(REDCap) electronic database.18 Radiographic variables included:VCE, HRD, hematoma extension (none/subcapsular; perirenal;pararenal), laceration location (lateral, medial, complex [both]),number of lacerations, depth of laceration, and parenchymaldevascularization. For bilateral injuries, injury specifics fromthe side with higher injury grade were considered.
Two radiologists, blinded to the intervention data and pa-tient outcomes, independently reviewed the CT scans to extractinjury specifics. An initial training set of 20 CT scans from renaltrauma patients was used to assure a common understanding ofthe study terminology and achieve substantial agreement be-tween reviewers in test cases (kappa>0.6). Interrater reliabilityanalyses were used to assess the agreement on radiologic mea-surements between the readers (Supplemental Digital Content,Table 1, http://links.lww.com/TA/B311). After measuring initialinterradiologist agreements, the scans were rereviewed to reacha consensus on discordant findings. For continuous variables(e.g., HRD and laceration depth), the average of the two mea-surements was used. Input from a third reviewer was used to re-solve the disagreements when needed.
Statistical AnalysisValues are reported as percentages for categorical vari-
ables and mean (standard deviation) or median (25th to 75th in-terquartile ranges [IQR]) for continuous variables as appropriate.Independent t test, χ2 test, and Wilcoxon rank sum test wereused to compare variables. Mixed-effect univariable Poisson re-gression models, with clustering by facility and robust estimatorfor error, were developed to assess the associations between ra-diologic variables and the outcome. Results from regressionmodels are reported as risk ratios (RR) with 95% confidenceintervals (CIs). Mixed effect Poisson regression was used todevelop the multivariable model, which included HRD, lacer-ation depth, VCE, and ≥3 lacerations. The AAST grade wasnot included as the radiographic appearance of the injurieswas characterized in detail and the intent of this study wasto characterize these risk factors separately; there is also sig-nificant variability and some ambiguity about the grading ofHGRT.5,19 For HRD and laceration depth, diagnostic accu-racy was measured using the receiver operating characteristic(ROC) analysis, and the optimal cutoffs were chosen based onthe F-1 score maximizing sensitivity and positive predictivevalue (PPV) simultaneously.20 A second multivariable modelwas developed using the dichotomized values of HRD andlaceration size based upon the cutoffs from the ROC analysis.Statistical analyses were conducted using STATA 15 (Stata Corp,College Station, TX).
RESULTS
From 431 patients with HGRT, 326 (76%) had CT scans onpresentation and were included. Excluded patients (n = 105) hadhigher rates of shock, as well as penetrating and concomitant in-juries, leading directly to surgical exploration. As expected, mostthese patients underwent immediate surgery without imaging
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
studies and the rates of bleeding interventions were significantlyhigher for these patients compared to those who were includedin the study (54% vs. 14%, p < 0.001).
Among the 326 patients with initial imaging, 47 (14.4%)underwent a total of 51 bleeding interventions including 19 renalangioembolization, 16 nephrectomies, 3 partial nephrectomies,7 renorrhaphies, and 6 renal packings. Patient demographics, in-jury characteristics, radiographic variables, and injury manage-ment are summarized in Table 1.
Overall, 73 patients (22%) hadVCE. In 123 patients (38%),the hematoma from renal injury expanded beyond the midline orinto the pelvis (pararenal hematoma). Median HRD was 1.8 cm(IQR, 0.8–2.9) and was higher in those who underwent bleedinginterventions compared to those who did not (3.8 cm; IQR,2.1–5.0 vs. 1.4 cm; IQR, 0.8–2.3, p < 0.001). Median lacerationdepth was 1.9 (IQR, 1.4–2.5) and was also higher in patientswho underwent bleeding interventions (2.8 cm, IQR, 2.3–3.5vs. 1.8 cm, IQR, 1.4–2.3, p < 0.001).
In the univariable analyses, VCE, larger HRD, deeper lac-erations, pararenal extent of hematoma, and three or more paren-chymal lacerations were all associated with increased risk ofbleeding interventions (Table 2). The rate of intervention wassignificantly higher for those with VCE compared to those with-out VCE (40% vs. 7%, p < 0.001).
In the multivariable regression (variables: HRD, lacerationdepth, VCE, and ≥3 lacerations), the presence of VCE was as-sociated with a threefold increase in risk of interventions (RR,3.03; 95%CI, 1.48–6.21; p = 0.002) and each centimeter increasein HRD was associated with a 15% increase in risk of bleedinginterventions (RR, 1.15; 95% CI, 1.01–1.31; p = 0.03)(Table 3, model 1).
An HRD cutoff of 3.5 cm provided the best predictiveaccuracy for undergoing bleeding interventions (sensitivity,0.62; specificity, 0.87; PPV, 0.44; F1 score, 0.51) (Fig. 2A).The intervention rate was higher for those with an HRD of 3.5or greater compared to those with an HRD less than 3.5 cm(44% vs. 7%, p < 0.001). This cutoff (HRD ≥ 3.5 cm) wasassociated with a 6.3-fold increase in the risk of undergoingbleeding interventions in the univariable analysis (RR, 6.3; 95%CI, 3.5–11.4). For laceration depth, a cutoff of 2.5 cmprovided the best predictive accuracy for undergoing bleedinginterventions (sensitivity, 0.62; specificity, 0.80; PPV, 0.36; F1score, 0.44) (Fig. 2B). The intervention rate was higher forthose with laceration depth of 2.5 cm or greater compared withthose with laceration depth less than 2.5 cm (34% vs. 7%,p < 0.001). A laceration depth of 2.5 cm or greater was associatedwith 4.4-fold increased risk of bleeding interventions in theunivariable analysis (RR, 4.4; 95% CI, 2.5–8.0). In themultivariable regression model using the cutoffs from theROC analysis, an HRD of 3.5 cm or greater was associatedwith 2.5-fold increased risk of bleeding interventions whencontrolling for laceration depth, VCE, and number of lacerations(Table 3, model 2).
DISCUSSION
This study confirms the critical associations of radio-graphic findings with bleeding control interventions afterHGRT. Our results show that the presence of VCE and size of
977
ealth, Inc. All rights reserved.
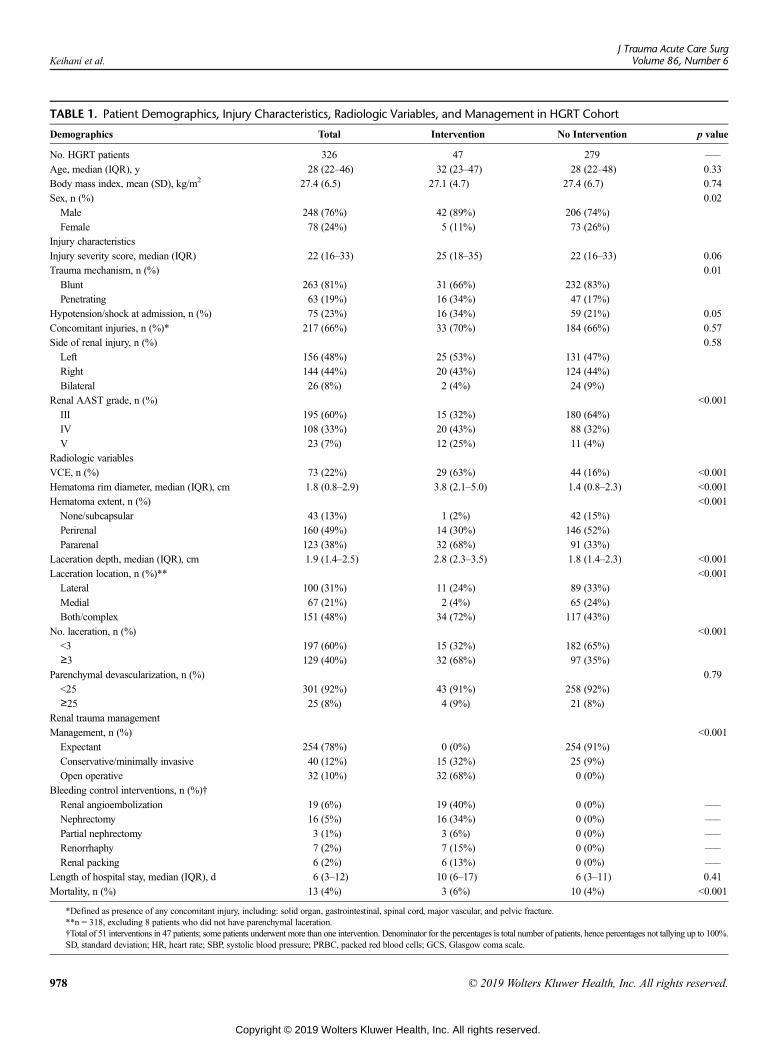
TABLE 1. Patient Demographics, Injury Characteristics, Radiologic Variables, and Management in HGRT Cohort
Demographics Total Intervention No Intervention p value
No. HGRT patients 326 47 279 –––
Age, median (IQR), y 28 (22–46) 32 (23–47) 28 (22–48) 0.33Body mass index, mean (SD), kg/m2 27.4 (6.5) 27.1 (4.7) 27.4 (6.7) 0.74Sex, n (%) 0.02Male 248 (76%) 42 (89%) 206 (74%)Female 78 (24%) 5 (11%) 73 (26%)
Injury characteristicsInjury severity score, median (IQR) 22 (16–33) 25 (18–35) 22 (16–33) 0.06Trauma mechanism, n (%) 0.01Blunt 263 (81%) 31 (66%) 232 (83%)Penetrating 63 (19%) 16 (34%) 47 (17%)
Hypotension/shock at admission, n (%) 75 (23%) 16 (34%) 59 (21%) 0.05Concomitant injuries, n (%)* 217 (66%) 33 (70%) 184 (66%) 0.57Side of renal injury, n (%) 0.58Left 156 (48%) 25 (53%) 131 (47%)Right 144 (44%) 20 (43%) 124 (44%)Bilateral 26 (8%) 2 (4%) 24 (9%)
Renal AAST grade, n (%) <0.001III 195 (60%) 15 (32%) 180 (64%)IV 108 (33%) 20 (43%) 88 (32%)V 23 (7%) 12 (25%) 11 (4%)
Radiologic variablesVCE, n (%) 73 (22%) 29 (63%) 44 (16%) <0.001Hematoma rim diameter, median (IQR), cm 1.8 (0.8–2.9) 3.8 (2.1–5.0) 1.4 (0.8–2.3) <0.001Hematoma extent, n (%) <0.001None/subcapsular 43 (13%) 1 (2%) 42 (15%)Perirenal 160 (49%) 14 (30%) 146 (52%)Pararenal 123 (38%) 32 (68%) 91 (33%)
Laceration depth, median (IQR), cm 1.9 (1.4–2.5) 2.8 (2.3–3.5) 1.8 (1.4–2.3) <0.001Laceration location, n (%)** <0.001Lateral 100 (31%) 11 (24%) 89 (33%)Medial 67 (21%) 2 (4%) 65 (24%)Both/complex 151 (48%) 34 (72%) 117 (43%)
No. laceration, n (%) <0.001<3 197 (60%) 15 (32%) 182 (65%)≥3 129 (40%) 32 (68%) 97 (35%)
Parenchymal devascularization, n (%) 0.79<25 301 (92%) 43 (91%) 258 (92%)≥25 25 (8%) 4 (9%) 21 (8%)
Renal trauma managementManagement, n (%) <0.001Expectant 254 (78%) 0 (0%) 254 (91%)Conservative/minimally invasive 40 (12%) 15 (32%) 25 (9%)Open operative 32 (10%) 32 (68%) 0 (0%)
Bleeding control interventions, n (%)†Renal angioembolization 19 (6%) 19 (40%) 0 (0%) –––
Nephrectomy 16 (5%) 16 (34%) 0 (0%) –––
Partial nephrectomy 3 (1%) 3 (6%) 0 (0%) –––
Renorrhaphy 7 (2%) 7 (15%) 0 (0%) –––
Renal packing 6 (2%) 6 (13%) 0 (0%) –––
Length of hospital stay, median (IQR), d 6 (3–12) 10 (6–17) 6 (3–11) 0.41Mortality, n (%) 13 (4%) 3 (6%) 10 (4%) <0.001
*Defined as presence of any concomitant injury, including: solid organ, gastrointestinal, spinal cord, major vascular, and pelvic fracture.**n = 318, excluding 8 patients who did not have parenchymal laceration.†Total of 51 interventions in 47 patients; some patients underwent more than one intervention. Denominator for the percentages is total number of patients, hence percentages not tallying up to 100%.SD, standard deviation; HR, heart rate; SBP, systolic blood pressure; PRBC, packed red blood cells; GCS, Glasgow coma scale.
Keihani et al.J Trauma Acute Care Surg
Volume 86, Number 6
978 © 2019 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
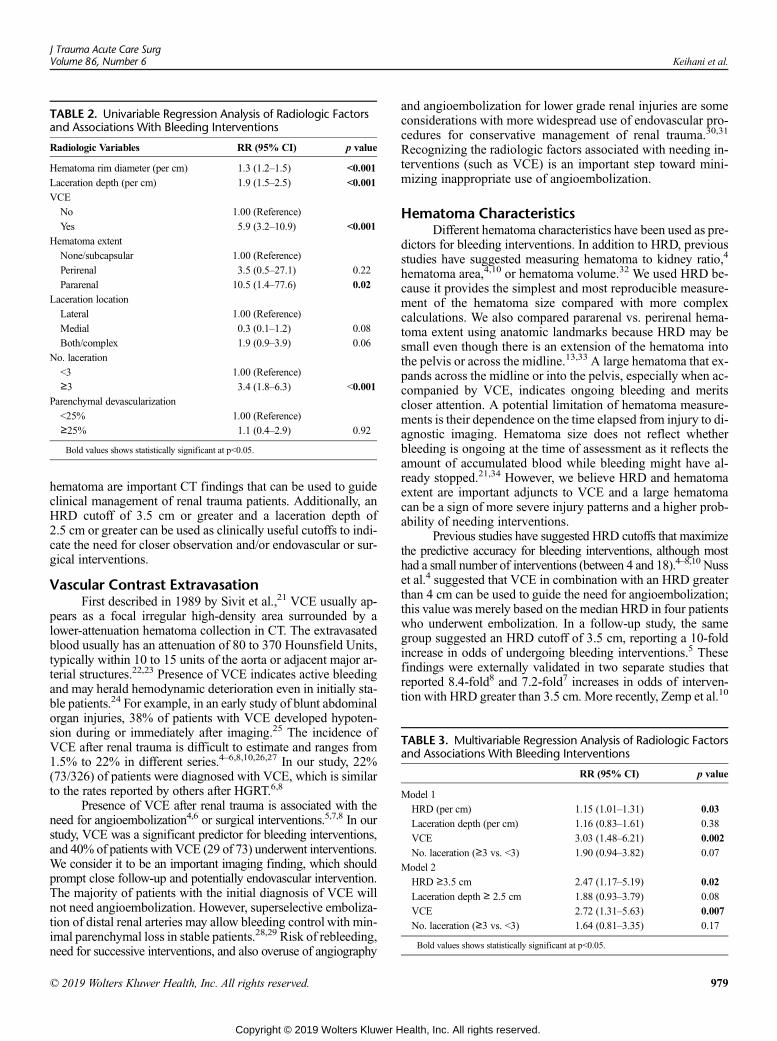
TABLE 2. Univariable Regression Analysis of Radiologic Factorsand Associations With Bleeding Interventions
Radiologic Variables RR (95% CI) p value
Hematoma rim diameter (per cm) 1.3 (1.2–1.5) <0.001
Laceration depth (per cm) 1.9 (1.5–2.5) <0.001
VCE
No 1.00 (Reference)
Yes 5.9 (3.2–10.9) <0.001
Hematoma extent
None/subcapsular 1.00 (Reference)
Perirenal 3.5 (0.5–27.1) 0.22
Pararenal 10.5 (1.4–77.6) 0.02
Laceration location
Lateral 1.00 (Reference)
Medial 0.3 (0.1–1.2) 0.08
Both/complex 1.9 (0.9–3.9) 0.06
No. laceration
<3 1.00 (Reference)
≥3 3.4 (1.8–6.3) <0.001
Parenchymal devascularization
<25% 1.00 (Reference)
≥25% 1.1 (0.4–2.9) 0.92
Bold values shows statistically significant at p<0.05.
TABLE 3. Multivariable Regression Analysis of Radiologic Factorsand Associations With Bleeding Interventions
RR (95% CI) p value
Model 1
HRD (per cm) 1.15 (1.01–1.31) 0.03
Laceration depth (per cm) 1.16 (0.83–1.61) 0.38
VCE 3.03 (1.48–6.21) 0.002
No. laceration (≥3 vs. <3) 1.90 (0.94–3.82) 0.07
Model 2
HRD ≥3.5 cm 2.47 (1.17–5.19) 0.02
Laceration depth ≥ 2.5 cm 1.88 (0.93–3.79) 0.08
VCE 2.72 (1.31–5.63) 0.007
No. laceration (≥3 vs. <3) 1.64 (0.81–3.35) 0.17
Bold values shows statistically significant at p<0.05.
J Trauma Acute Care SurgVolume 86, Number 6 Keihani et al.
hematoma are important CT findings that can be used to guideclinical management of renal trauma patients. Additionally, anHRD cutoff of 3.5 cm or greater and a laceration depth of2.5 cm or greater can be used as clinically useful cutoffs to indi-cate the need for closer observation and/or endovascular or sur-gical interventions.
Vascular Contrast ExtravasationFirst described in 1989 by Sivit et al.,21 VCE usually ap-
pears as a focal irregular high-density area surrounded by alower-attenuation hematoma collection in CT. The extravasatedblood usually has an attenuation of 80 to 370 Hounsfield Units,typically within 10 to 15 units of the aorta or adjacent major ar-terial structures.22,23 Presence of VCE indicates active bleedingand may herald hemodynamic deterioration even in initially sta-ble patients.24 For example, in an early study of blunt abdominalorgan injuries, 38% of patients with VCE developed hypoten-sion during or immediately after imaging.25 The incidence ofVCE after renal trauma is difficult to estimate and ranges from1.5% to 22% in different series.4–6,8,10,26,27 In our study, 22%(73/326) of patients were diagnosed with VCE, which is similarto the rates reported by others after HGRT.6,8
Presence of VCE after renal trauma is associated with theneed for angioembolization4,6 or surgical interventions.5,7,8 In ourstudy, VCE was a significant predictor for bleeding interventions,and 40% of patients with VCE (29 of 73) underwent interventions.We consider it to be an important imaging finding, which shouldprompt close follow-up and potentially endovascular intervention.The majority of patients with the initial diagnosis of VCE willnot need angioembolization. However, superselective emboliza-tion of distal renal arteries may allow bleeding control with min-imal parenchymal loss in stable patients.28,29 Risk of rebleeding,need for successive interventions, and also overuse of angiography
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
and angioembolization for lower grade renal injuries are someconsiderations with more widespread use of endovascular pro-cedures for conservative management of renal trauma.30,31
Recognizing the radiologic factors associated with needing in-terventions (such as VCE) is an important step toward mini-mizing inappropriate use of angioembolization.
Hematoma CharacteristicsDifferent hematoma characteristics have been used as pre-
dictors for bleeding interventions. In addition to HRD, previousstudies have suggested measuring hematoma to kidney ratio,4
hematoma area,4,10 or hematoma volume.32 We used HRD be-cause it provides the simplest and most reproducible measure-ment of the hematoma size compared with more complexcalculations. We also compared pararenal vs. perirenal hema-toma extent using anatomic landmarks because HRD may besmall even though there is an extension of the hematoma intothe pelvis or across the midline.13,33 A large hematoma that ex-pands across the midline or into the pelvis, especially when ac-companied by VCE, indicates ongoing bleeding and meritscloser attention. A potential limitation of hematoma measure-ments is their dependence on the time elapsed from injury to di-agnostic imaging. Hematoma size does not reflect whetherbleeding is ongoing at the time of assessment as it reflects theamount of accumulated blood while bleeding might have al-ready stopped.21,34 However, we believe HRD and hematomaextent are important adjuncts to VCE and a large hematomacan be a sign of more severe injury patterns and a higher prob-ability of needing interventions.
Previous studies have suggested HRD cutoffs that maximizethe predictive accuracy for bleeding interventions, although mosthad a small number of interventions (between 4 and 18).4–8,10 Nusset al.4 suggested that VCE in combination with an HRD greaterthan 4 cm can be used to guide the need for angioembolization;this value was merely based on the median HRD in four patientswho underwent embolization. In a follow-up study, the samegroup suggested an HRD cutoff of 3.5 cm, reporting a 10-foldincrease in odds of undergoing bleeding interventions.5 Thesefindings were externally validated in two separate studies thatreported 8.4-fold8 and 7.2-fold7 increases in odds of interven-tion with HRD greater than 3.5 cm. More recently, Zemp et al.10
979
ealth, Inc. All rights reserved.
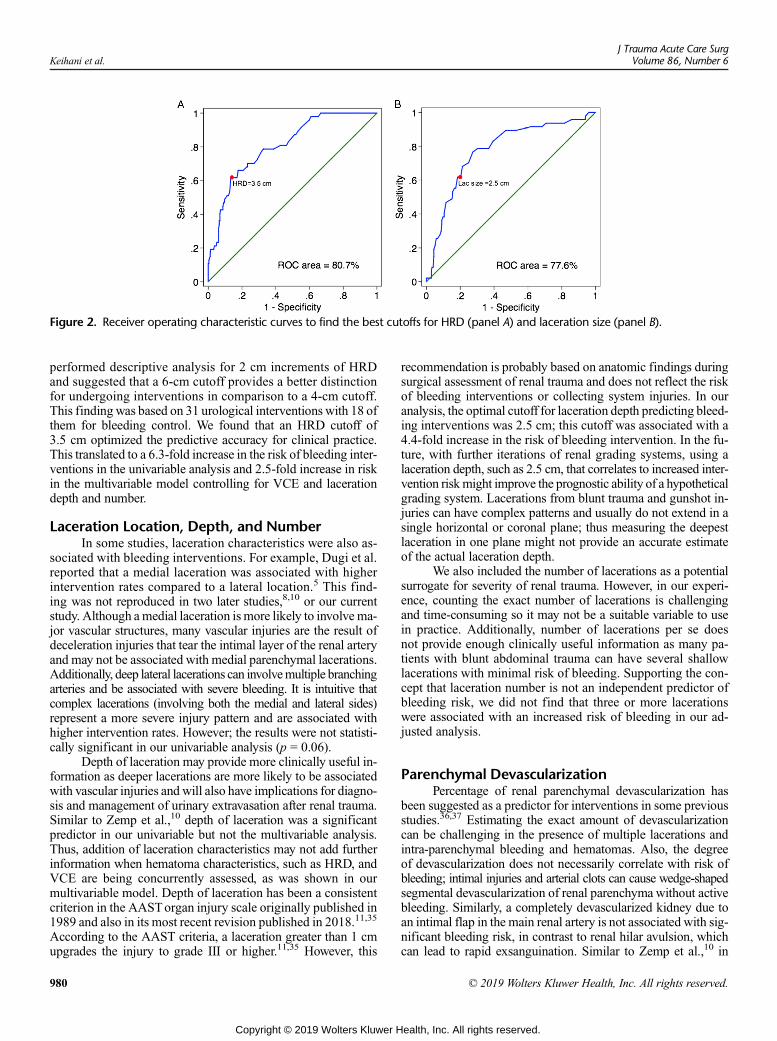
Figure 2. Receiver operating characteristic curves to find the best cutoffs for HRD (panel A) and laceration size (panel B).
Keihani et al.J Trauma Acute Care Surg
Volume 86, Number 6
performed descriptive analysis for 2 cm increments of HRDand suggested that a 6-cm cutoff provides a better distinctionfor undergoing interventions in comparison to a 4-cm cutoff.This finding was based on 31 urological interventions with 18 ofthem for bleeding control. We found that an HRD cutoff of3.5 cm optimized the predictive accuracy for clinical practice.This translated to a 6.3-fold increase in the risk of bleeding inter-ventions in the univariable analysis and 2.5-fold increase in riskin the multivariable model controlling for VCE and lacerationdepth and number.
Laceration Location, Depth, and NumberIn some studies, laceration characteristics were also as-
sociated with bleeding interventions. For example, Dugi et al.reported that a medial laceration was associated with higherintervention rates compared to a lateral location.5 This find-ing was not reproduced in two later studies,8,10 or our currentstudy. Although amedial laceration is more likely to involve ma-jor vascular structures, many vascular injuries are the result ofdeceleration injuries that tear the intimal layer of the renal arteryand may not be associated with medial parenchymal lacerations.Additionally, deep lateral lacerations can involvemultiple branchingarteries and be associated with severe bleeding. It is intuitive thatcomplex lacerations (involving both the medial and lateral sides)represent a more severe injury pattern and are associated withhigher intervention rates. However; the results were not statisti-cally significant in our univariable analysis (p = 0.06).
Depth of laceration may provide more clinically useful in-formation as deeper lacerations are more likely to be associatedwith vascular injuries and will also have implications for diagno-sis and management of urinary extravasation after renal trauma.Similar to Zemp et al.,10 depth of laceration was a significantpredictor in our univariable but not the multivariable analysis.Thus, addition of laceration characteristics may not add furtherinformation when hematoma characteristics, such as HRD, andVCE are being concurrently assessed, as was shown in ourmultivariable model. Depth of laceration has been a consistentcriterion in the AASTorgan injury scale originally published in1989 and also in its most recent revision published in 2018.11,35
According to the AAST criteria, a laceration greater than 1 cmupgrades the injury to grade III or higher.11,35 However, this
980
Copyright © 2019 Wolters Kluwer H
recommendation is probably based on anatomic findings duringsurgical assessment of renal trauma and does not reflect the riskof bleeding interventions or collecting system injuries. In ouranalysis, the optimal cutoff for laceration depth predicting bleed-ing interventions was 2.5 cm; this cutoff was associated with a4.4-fold increase in the risk of bleeding intervention. In the fu-ture, with further iterations of renal grading systems, using alaceration depth, such as 2.5 cm, that correlates to increased inter-vention riskmight improve the prognostic ability of a hypotheticalgrading system. Lacerations from blunt trauma and gunshot in-juries can have complex patterns and usually do not extend in asingle horizontal or coronal plane; thus measuring the deepestlaceration in one plane might not provide an accurate estimateof the actual laceration depth.
We also included the number of lacerations as a potentialsurrogate for severity of renal trauma. However, in our experi-ence, counting the exact number of lacerations is challengingand time-consuming so it may not be a suitable variable to usein practice. Additionally, number of lacerations per se doesnot provide enough clinically useful information as many pa-tients with blunt abdominal trauma can have several shallowlacerations with minimal risk of bleeding. Supporting the con-cept that laceration number is not an independent predictor ofbleeding risk, we did not find that three or more lacerationswere associated with an increased risk of bleeding in our ad-justed analysis.
Parenchymal DevascularizationPercentage of renal parenchymal devascularization has
been suggested as a predictor for interventions in some previousstudies.36,37 Estimating the exact amount of devascularizationcan be challenging in the presence of multiple lacerations andintra-parenchymal bleeding and hematomas. Also, the degreeof devascularization does not necessarily correlate with risk ofbleeding; intimal injuries and arterial clots can cause wedge-shapedsegmental devascularization of renal parenchyma without activebleeding. Similarly, a completely devascularized kidney due toan intimal flap in the main renal artery is not associated with sig-nificant bleeding risk, in contrast to renal hilar avulsion, whichcan lead to rapid exsanguination. Similar to Zemp et al.,10 in
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 6 Keihani et al.
our study, the degree of devitalized segment (≥25%) was notassociated with increased interventions for renal bleeding.
Our study has some limitations. Given the lack of clearguidelines for intervention after HGRT, management was notstandardized in our multicenter study setting, and thresholdsfor intervention and overall care among these centers are likelydifferent. However, our data reflect the real-world managementfrom Level I trauma centers across the country, which have themost experience in the management of HGRT. Lack of follow-up after patient discharge is another weakness of the study,which limits the discussion of our findings to the acute traumaperiod. In addition, these radiologic parameters only apply to pa-tients who are stable enough to undergo a CT scan, and many in-terventions were performed on patients who were taken directlyto the operating room for management of their injuries. How-ever, the patients that are stable enough to get a CT scan arethe population that would benefit the most from clinical toolspredicting the need to intervene for hemorrhage. There is alsoa potential for bias as the presence of these radiographic find-ings could have impacted the decision for intervention in theclinical setting but not necessarily reflect the need for interven-tion or collate with outcomes. Despite these limitations, this isthe first study that validates these radiologic findings and as-sesses the cutoffs in a multi-institutional setting and with a largeenough sample size allowing for multivariable analysis. Also,all the images were reviewed by two radiologists, blinded to theoutcomes, which increases the validity and reproducibility ofour results.
CONCLUSION
Presence of VCE and the size of hematoma around thekidney are two important radiologic findings that can be usedto guide the need for bleeding control interventions after HGRT.An HRD of 3.5 cm or greater and a laceration depth of 2.5 cm orgreater can be used as surrogates for severity of injury and riskof bleeding and patients with these characteristics may needcloser observation or early endovascular and/or surgical inter-ventions. These radiologic factors can be used as adjuncts tothe AAST renal grading to guide clinical decision making andcould be incorporated in future predictive tools and renal traumamanagement algorithms.
AUTHORSHIP
J.B.M. and S.K. designed the study. B.E.P., D.M.R., M.E.H., and S.K. re-viewed the imaging data and interpreted the results. C.Z., S. K., and J. B. M.participated in data analysis and interpretation. J.B.M. and S.K. draftedthe article. X.L., K.M., B.J.M., S.M., J.P., C.M.D., I.S., S.P.E., E.S.D., S.Z.,B.G.S., B.A.E., N.B., B.N.B., C.N.F., B.P.S., B.U.O., R.A., B.M., R.A.S., M.M.C.,J.F.K., T.H., F.N.B., S. K., and J. B. M. participated in the data collectionand revisions for this article. J. B. M., D.M.R., B.N.B., B.A.E., S.Z., and R.N.provided critical revisions for this article. All the authors read and approvedthe final submission.
ACKNOWLEDGMENT
We thank the staff and contributors from the Trauma and Urologic Re-construction Network of Surgeons (http://www.turnsresearch.org/page/aast-gu-trauma- study-group-author-list-renal-trauma) and all theparticipating centers for sharing their data and supporting the study, aswell as the American Association for the Surgery of Trauma and theMulti-Institutional Trials Committee for providing continuous supportfor the project.
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
DISCLOSURE
The authors declare no conflicts of interest.This study was not directly supported by any industrial or federal funds.
FUNDING
The investigation was in part supported by the University of UtahStudy Design and Biostatistics Center, with funding in part from theNational Center for Research Resources and the National Center for Ad-vancing Translational Sciences, National Institutes of Health, throughGrant 5UL1TR001067–05 (formerly 8UL1TR000105 and UL1RR025764).
REFERENCES1. Sujenthiran A, Elshout PJ, Veskimae E, Mac Lennan S, Yuan Y,
Serafetinidis E, Sharma DM, Kitrey ND, Djakovic N, Lumen N, et al.Is nonoperative management the best first-line option for high-grade renaltrauma? A systematic review. Eur Urol Focus. 2017.
2. Johnsen NV, Betzold RD, Guillamondegui OD, Dennis BM, Stassen NA,Bhullar I, Ibrahim JA. Surgical management of solid organ injuries. SurgClin North Am. 2017;97(5):1077–1105.
3. Myers JB, Brant WO, Broghammer JA. High-grade renal injuries: radiographicfindings correlated with intervention for renal hemorrhage. Urol Clin North Am.2013;40(3):335–341.
4. Nuss GR, Morey AF, Jenkins AC, Pruitt JH, Dugi DD 3rd, Morse B,Shariat SF. Radiographic predictors of need for angiographic embolizationafter traumatic renal injury. J Trauma. 2009;67(3):578–582; discussion 82.
5. Dugi DD 3rd, Morey AF, Gupta A, Nuss GR, Sheu GL, Pruitt JH. AmericanAssociation for the Surgery of Trauma grade 4 renal injury substratificationinto grades 4a (low risk) and 4b (high risk). J Urol. 2010;183(2):592–597.
6. Charbit J, Manzanera J, Millet I, Roustan JP, Chardon P, Taourel P,Capdevila X. What are the specific computed tomography scan criteria thatcan predict or exclude the need for renal angioembolization after high-graderenal trauma in a conservative management strategy? J Trauma. 2011;70(5):1219–1128.
7. Figler BD, Malaeb BS, Voelzke B, Smith T, Wessells H. External validationof a substratification of the American Association for the Surgery of Traumarenal injury scale for grade 4 injuries. J AmColl Surg. 2013;217(5):924–928.
8. Hardee MJ, Lowrance W, Brant WO, Presson AP, Stevens MH, Myers JB.High grade renal injuries: application of Parkland Hospital predictors of in-tervention for renal hemorrhage. J Urol. 2013;189(5):1771–1776.
9. Chong ST, Cherry-Bukowiec JR, Willatt JM, Kielar AZ. Renal trauma: im-aging evaluation and implications for clinical management. Abdom Radiol(NY). 2016;41(8):1565–1579.
10. Zemp L, Mann U, Rourke KF. Perinephric hematoma size is independentlyassociated with the need for urological intervention in multisystem blunt re-nal trauma. J Urol. 2018;199(5):1283–1288.
11. Moore EE, Shackford SR, Pachter HL, McAninch JW, Browner BD,Champion HR, Flint LM, Gennarelli TA, Malangoni MA, Ramenofsky ML,et al. Organ injury scaling: spleen, liver, and kidney. J Trauma. 1989;29(12):1664–1666.
12. Keihani S, Xu Y, Presson AP, Hotaling JM, Nirula R, Piotrowski J,Dodgion CM, Black CM, Mukherjee K, Morris BJ, et al. Contemporarymanagement of high-grade renal trauma: results from the American Associ-ation for the Surgery of Trauma Genitourinary Trauma study. J TraumaAcute Care Surg. 2018;84(3):418–425.
13. Lee YJ, Oh SN, Rha SE, Byun JY. Renal trauma. Radiol Clin N Am. 2007;45(3):581–592, ix.
14. Kneeland JB, AuhYH, RubensteinWA, Zirinsky K,MorrisonH,Whalen JP,Kazam E. Perirenal spaces: CTevidence for communication across the mid-line. Radiology. 1987;164(3):657–664.
15. Chiron P, Hornez E, Boddaert G, Dusaud M, Bayoud Y, Molimard B,Desfemmes FR, Durand X. Grade IV renal trauma management. A revisionof the AAST renal injury grading scale is mandatory. EuroIntervention.2016;42(2):237–241.
16. Au JK, Tan X, Sidani M, Stanasel I, Roth DR, Koh CJ, Seth A, Gargollo PC,Tu D, Gonzales ET, et al. Imaging characteristics associated with failure ofnonoperative management in high-grade pediatric blunt renal trauma.J Pediatr Urol. 2016;12(5):294.e1–e6.
981
ealth, Inc. All rights reserved.

Keihani et al.J Trauma Acute Care Surg
Volume 86, Number 6
17. Jodogne S. The Orthanc Ecosystem for Medical Imaging. J Digit Imaging.2018.
18. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Researchelectronic data capture (REDCap)—a metadata-driven methodology andworkflow process for providing translational research informatics support.J Biomed Inform. 2009;42(2):377–381.
19. Buckley JC, McAninch JW. Revision of current American Association forthe Surgery of Trauma Renal Injury grading system. J Trauma. 2011;70(1):35–37.
20. Powers DM. Evaluation: from precision, recall and F-measure to ROC,informedness, markedness and correlation. Adelaide, Australia: School ofInformatics and Engineering Flinders University; 2007.
21. Sivit CJ, Peclet MH, Taylor GA. Life-threatening intraperitoneal bleeding:demonstration with CT. Radiology. 1989;171(2):430.
22. Harris AC, Zwirewich CV, Lyburn ID, Torreggiani WC, Marchinkow LO. CTfindings in blunt renal trauma. Radiographics. 2001;21 Spec No:S201–S214.
23. Lane MJ, Katz DS, Shah RA, Rubin GD, Jeffrey RB Jr. Active arterial con-trast extravasation on helical CTof the abdomen, pelvis, and chest. AJR Am JRoentgenol. 1998;171(3):679–685.
24. Broghammer JA, Fisher MB, Santucci RA. Conservative management of re-nal trauma: a review. Urology. 2007;70(4):623–629.
25. Jeffrey RB Jr., Cardoza JD, Olcott EW.Detection of active intraabdominal ar-terial hemorrhage: value of dynamic contrast-enhanced CT. AJR Am JRoentgenol. 1991;156(4):725–729.
26. Yao DC, Jeffrey RB Jr., Mirvis SE,Weekes A, Federle MP, Kim C, Lane MJ,Prabhakar P, Radin R, Ralls PW. Using contrast-enhanced helical CT to visu-alize arterial extravasation after blunt abdominal trauma: incidence and organdistribution. AJR Am J Roentgenol. 2002;178(1):17–20.
27. Baghdanian AH, Baghdanian AA, Armetta A, Babayan RK, LeBedis CA,Soto JA, Anderson SW. Utility of MDCT findings in predicting patient man-agement outcomes in renal trauma. Emerg Radiol. 2017;24(3):263–272.
28. Bauer JR, Ray CE. Transcatheter arterial embolization in the trauma patient:a review. Semin Interv Radiol. 2004;21(1):11–22.
982
Copyright © 2019 Wolters Kluwer H
29. Chatziioannou A, Brountzos E, Primetis E, Malagari K, Sofocleous C,Mourikis D, Kelekis D. Effects of superselective embolization for renal vas-cular injuries on renal parenchyma and function. Eur J Vasc Endovasc Surg.2004;28(2):201–206.
30. Hotaling JM, Sorensen MD, Smith TG 3rd, Rivara FP, Wessells H,Voelzke BB. Analysis of diagnostic angiography and angioembolizationin the acute management of renal trauma using a national data set. J Urol.2011;185(4):1316–1320.
31. Gor RA, Styskel BA, Li T, Canter DJ, Simhan J. Unexpected high rates ofangiography and angioembolization for isolated low-grade renal trauma: re-sults from a large, statewide, trauma database. Urology. 2016;97:92–97.
32. Rezai P, Tochetto S, Galizia M, Yaghmai V. Perinephric hematoma: semi-automated quantification of volume on MDCT: a feasibility study. AbdomImaging. 2011;36(2):222–227.
33. Keihani S, Myers JB. Re: Perinephric hematoma size is independently asso-ciated with the need for urological intervention in multisystem blunt renaltrauma: L. Zemp, U. Mann and K. F. Rourke J Urol 2018;199:1283–1288.J Urol. 2018;200(3):656–657.
34. Brick SH, Taylor GA, Potter BM, Eichelberger MR. Hepatic and splenic in-jury in children: role of CT in the decision for laparotomy. Radiology. 1987;165(3):643–646.
35. Kozar RA, Crandall M, Shanmuganathan K, Zarzaur BL, Coburn M,Cribari C, Kaup K, Schuster K, Tominaga GT, , AAST Patient AssessmentCommittee. Organ injury scaling 2018 update: spleen, liver, and kidney.J Trauma Acute Care Surg. 2018;85(6):1119–1122.
36. Long JA, Fiard G, Descotes JL, Arnoux V, Arvin-Berod A, Terrier N,Boillot B, Skowron O, Thuillier C, Rambeaud JJ. High-grade renal injury:non-operative management of urinary extravasation and prediction of long-term outcomes. BJU Int. 2013;111(4 Pt B):E249–E255.
37. Santucci RA, Wessells H, Bartsch G, Descotes J, Heyns CF, McAninch JW,Nash P, Schmidlin F. Evaluation and management of renal injuries: con-sensus statement of the renal trauma subcommittee. BJU Int. 2004;93(7):937–954.
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

ORIGINAL ARTICLE
Low-value clinical practices in injury care: A scopingreview and expert consultation survey
Lynne Moore, PhD, François Lauzier, MD, MSc, Pier-Alexandre Tardif, MA, MSc,Khadidja Malloum Boukar, MSc, Imen Farhat, MSc, Patrick Archambault, MD, MSc, Éric Mercier, MD, MSc,
François Lamontagne, MD, MSc, Michael Chassé, MD, PhD, Henry T. Stelfox, MD, PhD,Simon Berthelot, MD, MSc, Belinda Gabbe, PhD, Fiona Lecky, MD, MSc, Natalie Yanchar, MD, MSc,
Howard Champion, MD, John Kortbeek, MD, Peter Cameron, MD, Paule Lessard Bonaventure, MD, MSc,Jérôme Paquet, MD, Catherine Truchon, PhD, Alexis F. Turgeon, MD, MSc,
and on behalf of the Canadian Traumatic brain injury Research Consortium, Québec, Canada
AAST Continuing Medical Education Article
Accreditation StatementThis activity has been planned and implemented in accordance with the Es-sential Areas and Policies of the Accreditation Council for Continuing MedicalEducation through the joint providership of the American College of Surgeonsand the American Association for the Surgery of Trauma. The AmericanCollege Surgeons is accredited by the ACCME to provide continuing medicaleducation for physicians.
AMA PRA Category 1 Credits™The American College of Surgeons designates this journal-based CME activity fora maximum of 1 AMA PRACategory 1 Credit™. Physicians should claim only the creditcommensurate with the extent of their participation in the activity.
Of the AMA PRACategory 1 Credit™ listed above, a maximum of 1 credit meetsthe requirements for self-assessment.
Credits can only be claimed online
ObjectivesAfter reading the featured articles published in the Journal of Trauma and AcuteCare Surgery, participants should be able to demonstrate increased understandingof the material specific to the article. Objectives for each article are featured atthe beginning of each article and online. Test questions are at the end of the article,with a critique and specific location in the article referencing the question topic.
Claiming CreditTo claim credit, please visit the AAST website at http://www.aast.org/ and click onthe “e-Learning/MOC” tab. You must read the article, successfully complete thepost-test and evaluation. Your CME certificate will be available immediately uponreceiving a passing score of 75% or higher on the post-test. Post-tests receiving a scoreof below 75% will require a retake of the test to receive credit.
System RequirementsThe system requirements are as follows: Adobe® Reader 7.0 or above installed; Internet Explorer® 7 and above; Firefox® 3.0 and above, Chrome® 8.0 and above, or
Safari™ 4.0 and above.
QuestionsIf you have any questions, please contact AAST at 800-789-4006. Paper test and evaluations will not be accepted.
Disclosure InformationIn accordance with the ACCME Accreditation Criteria, the American College of Surgeons, as
the accredited provider of this journal activity, must ensure that anyone in a position to control
the content of J Trauma Acute Care Surg articles selected for CME credit has disclosed
all relevant financial relationships with any commercial interest. Disclosure forms
are completed by the editorial staff, associate editors, reviewers, and all authors. The
ACCME defines a `commercial interest' as “any entity producing, marketing, re-selling,
or distributing health care goods or services consumed by, or used on, patients.” “Rele-
vant” financial relationships are those (in any amount) that may create a conflict of in-
terest and occur within the 12’months preceding and during the time that the individual
is engaged in writing the article. All reported conflicts are thoroughly managed in order
to ensure any potential bias within the content is eliminated. However, if you’perceive a
bias within the article, please report the circumstances on the evaluation form.
Please note we have advised the authors that it is their responsibility to disclose within
the article if they are describing the use of a device, product, or drug that is not FDA
approved or the off-label use of an approved device, product, or drug or unapproved usage.
Disclosures of Significant Relationships withRelevant Commercial Companies/Organizationsby the Editorial StaffErnest E. Moore, Editor: PI, research support and shared U.S. patents Haemonetics;
PI, research support, Instrumentation Laboratory, Inc.; Co-founder, Thrombo Thera-
peutics. Associate Editors David Hoyt, Ronald V. Maier and Steven Shackford have
nothing to disclose. Editorial staff and Angela Sauaia have nothing to disclose.
Author DisclosuresJohn Kortbeek, Co-author – Employed by AHS & the University of Calgary as a medical
leader and professor of surgery; Shock Trauma Air Rescue Society –Money/Grant; Jerome
Paquet, Co-author –Medtronic of Canada –Money/Grant
Reviewer DisclosuresThe reviewers have nothing to disclose.
CostFor AAST members and Journal of Trauma and Acute Care Surgery subscribersthere is no charge to participate in this activity. For those who are not a memberor subscriber, the cost for each credit is $25.
J Trauma Acute Care SurgVolume 86, Number 6 983
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.

Fro
Moore et al.J Trauma Acute Care Surg
Volume 86, Number 6
98
BACKGROUND: T
m the Department of Social andulation Health and Optimal HeCritical Care Medicine (L.M., FA.F.T.), Centre de Recherche dl'Enfant-Jésus), Department of AA.F.T.), Population Health andTransfert des Connaissances et Éen Santé, Centre de RechercheFrançois d'Assise), UniversitéUniversité de Sherbrooke, Sherbde Montréal, Montréal, QuébecMedicine andCommunity Healtversity of Calgary, Calgary, Albtive Medicine (B.G.), MonasMedicine (F.Lecky), UniversityNetwork, United Kingdom; DeHalifax, Nova Scotia; Depar
4
ests and treatments that are not supported by evidence and could expose patients to unnecessary harm, referred to here as low-value clinical practices, consume up to 30% of health care resources. ChoosingWisely and other organizations have published listsof clinical practices to be avoided. However, few apply to injury and most are based uniquely on expert consensus. We aimed toidentify low-value clinical practices in acute injury care.
METHODS: W
e conducted a scoping review targeting articles, reviews and guidelines that identified low-value clinical practices specific to in-jury populations. Thirty-six experts rated clinical practices on a five-point Likert scale from clearly low value to clearly beneficial.Clinical practices reported as low value by at least one level I, II, or III study and considered clearly or potentially low-value by atleast 75% of experts were retained as candidates for low-value injury care.RESULTS: O
f 50,695 citations, 815 studies were included and led to the identification of 150 clinical practices. Of these, 63 were consideredcandidates for low-value injury care; 33 in the emergency room, 9 in trauma surgery, 15 in the intensive care unit, and 5 in ortho-pedics. We also identified 87 “gray zone” practices, which did not meet our criteria for low-value care.CONCLUSION: W
e identified 63 low-value clinical practices in acute injury care that are supported by empirical evidence and expert opinion. Con-ditional on future research, they represent potential targets for guidelines, overuse metrics and de-implementation interventions.We also identified 87 “gray zone” practices, which may be interesting targets for value-based decision-making. Our study repre-sents an important step toward the deimplementation of low-value clinical practices in injury care. (J Trauma Acute Care Surg.2019;86: 983–993. Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.)LEVEL OF EVIDENCE: S
ystematic Review, Level IV. KEYWORDS: L ow-value care; trauma systems; scoping review; expert survey.I njuries led to 192,000 deaths, 3 million hospitalizations and 27million emergency department visits in the USA in 2013 and
generated medical and work loss costs of US $671 billion.1 InCanada, injury deaths increased by 23% from 13,000 in 2004to 16,000 in 2010 while costs increased by 35% and areprojected to reach $75 billion CAN by 2035.2 Given the hugeburden of injury and evidence of unwarranted variation in injuryoutcomes across health care providers,3–5 efforts to optimizecare has the potential to yield major dividends.
Rapid innovation in imaging and therapeutic techniqueshas led to an exponential rise in the use of tests and treatmentsthat are not supported by evidence and could expose patientsto unnecessary harm,6,7 referred to here as low-value clinicalpractices.8–15 Low-value clinical practices have been estimatedto consume up to 30% of health care resources10,12,14,16 but littleis known about this issue in the context of injury care. Low-value clinical practices have multiple negative consequences.From a health care system perspective, they strain health carebudgets and decrease the availability of resources. From a pa-tient and caregiver perspective, they expose patients to physi-cal and psychological harm, delay effective treatment, andincrease direct and indirect expenses.8–10,12,14 Finally, from asocietal perspective, low-value clinical practices threaten thesustainability of affordable, accessible health care. Interventionstargeting the de-implementation of low-value clinical practices
Preventative Medicine (L.M., K.M.B., I.F.), Pop-alth Practices Research Unit, Trauma, Emergency,.Lauzier, P.-A.T., K.M.B., I.M., E.M., S.B., P.L.B.,u CHU de Québec, Université Laval (Hôpital denesthesiology and Critical CareMedicine (F.Lauzier,Optimal Health Practices Research Unit (P.A.),valuation des Technologies etModes d'Interventiondu CHU de Québec, Université Laval (Hôpital StLaval; Department of Medicine (F.Lamontagne),rooke; Department of Medicine (M.C.), Université; Departments of Critical Care Medicine (H.T.S.),h Sciences, O'Brien Institute for Public Health, Uni-erta, Canada; School of Public Health and Preven-h University, Melbourne, Australia; Emergencyof Sheffield, Sheffield; Trauma Audit and Researchpartment of Surgery (N.Y.), Dalhousie University,tment of Surgery (H.C.), Uniformed Services
Copyright © 2019 Wolters Kluwer H
therefore have the potential to reduce waste and improve patientoutcomes.15,17
Physicians report overusing resources for fear of legal ac-tions but also because of lack of guidelines on low-value clini-cal practices.12–14,18 Choosing Wisely has developed lists ofcommonly used tests or procedures whose necessity shouldbe questioned including top five lists for emergency medicine,radiology, pediatric orthopedics, neurology, and surgery.11
However, few apply to injury care and most are based solelyon expert consensus. Previous systematic reviews aiming toidentify low-value clinical practices have not been specific to in-jury but have underlined the importance of targeting diagnosticgroups to improve feasibility and subsequent knowledgetransfer.15,19–22We aimed to identify low-value clinical practicesin acute, intrahospital injury care.
METHODS
Our study was conducted in six stages following pub-lished guidelines for scoping reviews and comprised a literaturereview followed by a Web-based survey consultation with clini-cal experts.23,24 The protocol has been published previously.25
Ethics approval was obtained from the institutional researchethics committee.
University of the Health Sciences, Bethesda, Maryland; Department of Surgery(J.K.), University of Calgary, Calgary, Alberta, Canada; The Alfred Hospital (P.C.),Monash University, Melbourne, Australia; Division of Neurosurgery, Departmentof Surgery (P.L.B., J.P.), Université Laval; Institut National D'Excellence en Santéet en Services Sociaux (C.T.), Québec, Canada.
Address for reprints: Lynne Moore, CHU de Québec Research Center (Enfant-JésusHospital), Population Health and Optimal Health Practices Research Unit,Trauma, Emergency, Critical Care Medicine, 1401, 18e rue, local H-012a, Québec,Canada G1J 1Z4; email: lynne.moore @fmed.ulaval.ca.
The results of this study were presented at the 77th Annual Meeting of AAST andClinical Congress of Acute Care Surgery and 4th World Trauma Congress,September 26th-29th, 2018 in San Diego, California.
Supplemental digital content is available for this article. Direct URL citations appear inthe printed text, and links to the digital files are provided in the HTML text of thisarticle on the journal’s Web site (www.jtrauma.com).
DOI: 10.1097/TA.0000000000002246
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 6 Moore et al.
Identify Research Questions and DevelopDefinitions
First, using an iterative approach, the interdisciplinary andintersectorial project steering committee comprising clinicians,allied health professionals and policy and decision-makers iden-tified the following research question for our review: Whichclinical practices are considered low-value in acute injury care?Second, the committee used highly-cited literature on health careoveruse7,13,14,17 to establish the following working definition oflow-value clinical practices: A test or treatment (i.e., admission,monitoring, diagnostic interventions, therapeutic interventions,consultation) that is used in practice but is ineffective or itsharm/cost outweighs its benefits. Third, the committee consultedUniversity of California at Los Angeles (UCLA) / Research andDevelopment (RAND) corporation recommendations to estab-lish the following criteria for identifying candidates for low-value injury care: clinical practices identified as low-value in atleast one Level I, II, or III study AND considered to be clearly/potentially low-value by at least 75% of experts and not consid-ered clearly beneficial by any expert.
Identify Relevant StudiesEligibility Criteria
We included original research, literature reviews, recom-mendations and guidelines that identified at least one low-valueclinical practice specific to injury populations according to thedefinition given above.11 We included studies on clinical prac-tices specific to intrahospital acute care (in the emergency de-partment or following hospital admission). We excluded: (i)studies with no clear indication for the low-value practice (e.g.,based on physician gestalt); (ii) studies based exclusively on pop-ulationswith combat injuries, osteoporotic fractures, burns, bites,or foreign bodies; (iii) case reports, animal and cadaver studies;(iv) studies on prehospital or postacute clinical practices.
Information SourcesWe systematically searched MEDLINE, EMBASE,
Cochrane CENTRAL, BIOSIS/Web of Science, ClinicalTrialsand ISRCTN; Thesis repositories (Thesis portal Canada,EtHOS, DART-Europe E-Theses Portal, the National Libraryof Australia's Trove and ProQuest Dissertations & ThesesGlobal); Websites of health care quality organizations (Agencyfor Healthcare Research and Quality, Australasian Associationfor Quality in Healthcare, Canadian Institutes for Health Infor-mation, Choosing Wisely, Lown Institute, National Associationfor Healthcare Quality, National Institute of Health and CareExcellence, National Quality Forum, andWorld Health Organi-zation) and injury organizations (American Association for theSurgery of Trauma, American Association of Orthopedic Sur-geons, American College of Surgeons, American Trauma Soci-ety, Australasian Trauma Society, Brain Trauma Foundation,British Trauma Society, Eastern Association for the Surgeryof Trauma, International Association for Trauma Surgery andIntensive Care, International Trauma Anesthesia and CriticalCare Society, Orthopedic Trauma Association, The Societyof Trauma Nurses, Trauma Association of Canada, TraumaAudit Research Network, Trauma.org, and Western Trauma
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
Association.); and patient advocacy organizations includingSafer Healthcare Now!
Search StrategyWe developed a systematic search strategy with an infor-
mation specialist.26 The strategy was developed for MEDLINEand EMBASE using keywords covering combinations of searchterms under the themes injury and low-value clinical practices(Supplemental Digital Content 3, Table 1, http://links.lww.com/TA/B326). This search strategy was then adapted for theother databases.
Select StudiesData Management
Citations were managed using EndNote software (versionX7.0.1, New York City: Thomson Reuters, 2011). Duplicateswere identified and eliminated using electronic and manualscreening.Multiple publications based on the same data set wereidentified by crosschecking authors, dates and settings. In thecase of replication, we identified only one publication for analy-ses using criteria based on study dates (most recent) and samplesize (largest).
Selection ProcessPairs of reviewers with methodological and content exper-
tise (two of four reviewers, L.M., K.M.B., P.A.T., I.F.) indepen-dently evaluated all citations for eligibility. Consecutive samplesof 500 citations were independently assessed by each revieweruntil high agreement was achieved on study inclusion (threesamples for kappa > 0.8). Any further disagreement on study el-igibility was resolved by consensus and a fifth reviewer adjudi-cated when necessary (F.L.).
Chart MaterialA standard electronic data abstraction form and a detailed
instruction manualwere developed and piloted independently byall reviewers on a representative sample of five publications.Pairs of reviewers (L.M., K.M.B., P.A.T., I.F.) independently ex-tracted information on the study design, setting (country, year,language, funding), study objective, study population, low-valueclinical practices, and primary outcomes when appropriate. Anydiscrepancies between reviewers was resolved by consensus anda fifth reviewer adjudicated when necessary (F.L.).
Collate, Summarize, and Report on ResultsClinical practices were classified according to the type of
practice and the clinical speciality.19 Classifications were con-ducted independently by two reviewers (K.M.B., P.A.T.) andthen checked independently by a third reviewer (L.M.- Lauzier).Any disagreements were adjudicated by a fourth reviewer (F.L.).As is common in scoping reviews, the methodological quality ofincluded studies was not evaluated.27 We summarized the levelof evidence for each practice by calculating the number of stud-ies by type using an adaptation of Oxford Center for Evidence-based Medicine classifications28: randomized-controlled trials(RCTs) or systematic review of RCTs (I), prospective cohortstudies or systematic review of RCTs and prospective cohortstudies (II), retrospective cohort, case-control, cross sectional
985
ealth, Inc. All rights reserved.
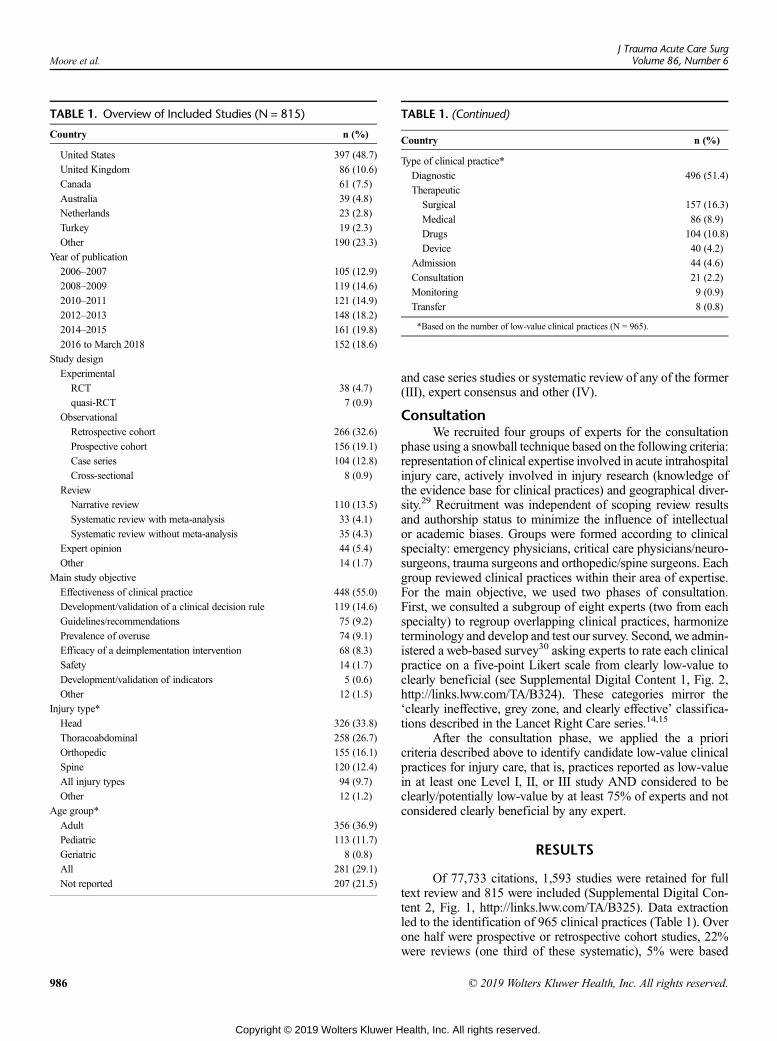
TABLE 1. Overview of Included Studies (N = 815)
Country n (%)
United States 397 (48.7)
United Kingdom 86 (10.6)
Canada 61 (7.5)
Australia 39 (4.8)
Netherlands 23 (2.8)
Turkey 19 (2.3)
Other 190 (23.3)
Year of publication
2006–2007 105 (12.9)
2008–2009 119 (14.6)
2010–2011 121 (14.9)
2012–2013 148 (18.2)
2014–2015 161 (19.8)
2016 to March 2018 152 (18.6)
Study design
Experimental
RCT 38 (4.7)
quasi-RCT 7 (0.9)
Observational
Retrospective cohort 266 (32.6)
Prospective cohort 156 (19.1)
Case series 104 (12.8)
Cross-sectional 8 (0.9)
Review
Narrative review 110 (13.5)
Systematic review with meta-analysis 33 (4.1)
Systematic review without meta-analysis 35 (4.3)
Expert opinion 44 (5.4)
Other 14 (1.7)
Main study objective
Effectiveness of clinical practice 448 (55.0)
Development/validation of a clinical decision rule 119 (14.6)
Guidelines/recommendations 75 (9.2)
Prevalence of overuse 74 (9.1)
Efficacy of a deimplementation intervention 68 (8.3)
Safety 14 (1.7)
Development/validation of indicators 5 (0.6)
Other 12 (1.5)
Injury type*
Head 326 (33.8)
Thoracoabdominal 258 (26.7)
Orthopedic 155 (16.1)
Spine 120 (12.4)
All injury types 94 (9.7)
Other 12 (1.2)
Age group*
Adult 356 (36.9)
Pediatric 113 (11.7)
Geriatric 8 (0.8)
All 281 (29.1)
Not reported 207 (21.5)
TABLE 1. (Continued)
Country n (%)
Type of clinical practice*
Diagnostic 496 (51.4)
Therapeutic
Surgical 157 (16.3)
Medical 86 (8.9)
Drugs 104 (10.8)
Device 40 (4.2)
Admission 44 (4.6)
Consultation 21 (2.2)
Monitoring 9 (0.9)
Transfer 8 (0.8)
*Based on the number of low-value clinical practices (N = 965).
Moore et al.J Trauma Acute Care Surg
Volume 86, Number 6
986
Copyright © 2019 Wolters Kluwer H
and case series studies or systematic review of any of the former(III), expert consensus and other (IV).
ConsultationWe recruited four groups of experts for the consultation
phase using a snowball technique based on the following criteria:representation of clinical expertise involved in acute intrahospitalinjury care, actively involved in injury research (knowledge ofthe evidence base for clinical practices) and geographical diver-sity.29 Recruitment was independent of scoping review resultsand authorship status to minimize the influence of intellectualor academic biases. Groups were formed according to clinicalspecialty: emergency physicians, critical care physicians/neuro-surgeons, trauma surgeons and orthopedic/spine surgeons. Eachgroup reviewed clinical practices within their area of expertise.For the main objective, we used two phases of consultation.First, we consulted a subgroup of eight experts (two from eachspecialty) to regroup overlapping clinical practices, harmonizeterminology and develop and test our survey. Second, we admin-istered a web-based survey30 asking experts to rate each clinicalpractice on a five-point Likert scale from clearly low-value toclearly beneficial (see Supplemental Digital Content 1, Fig. 2,http://links.lww.com/TA/B324). These categories mirror the‘clearly ineffective, grey zone, and clearly effective’ classifica-tions described in the Lancet Right Care series.14,15
After the consultation phase, we applied the a prioricriteria described above to identify candidate low-value clinicalpractices for injury care, that is, practices reported as low-valuein at least one Level I, II, or III study AND considered to beclearly/potentially low-value by at least 75% of experts and notconsidered clearly beneficial by any expert.
RESULTS
Of 77,733 citations, 1,593 studies were retained for fulltext review and 815 were included (Supplemental Digital Con-tent 2, Fig. 1, http://links.lww.com/TA/B325). Data extractionled to the identification of 965 clinical practices (Table 1). Overone half were prospective or retrospective cohort studies, 22%were reviews (one third of these systematic), 5% were based
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
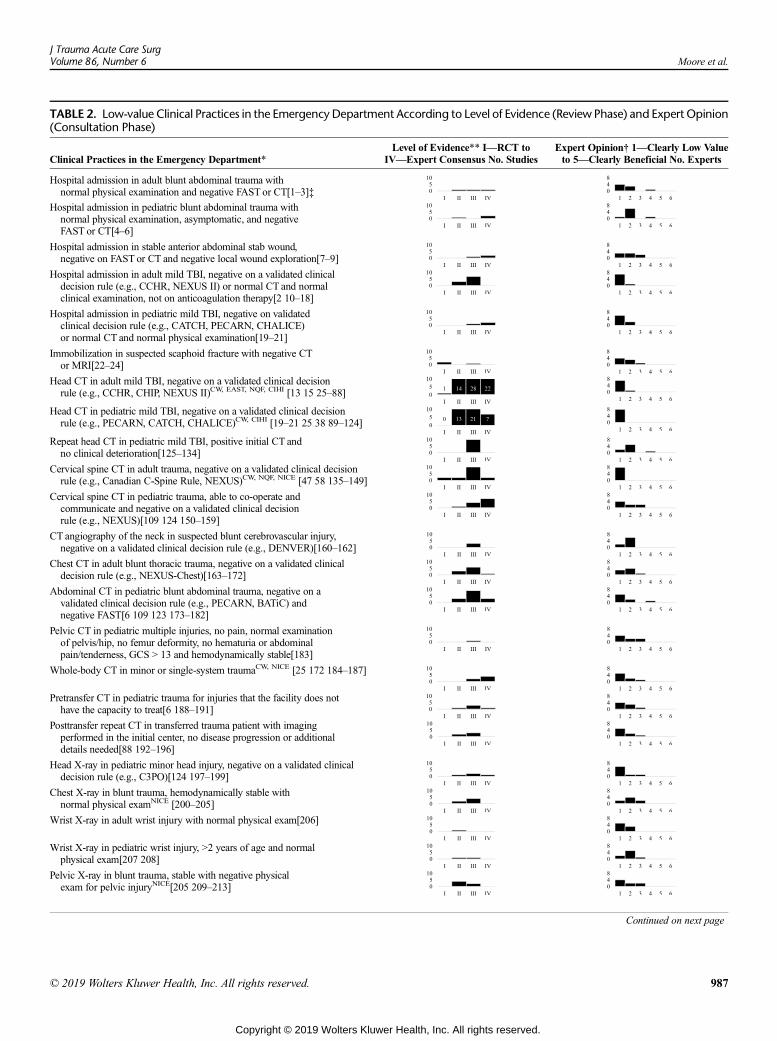
TABLE 2. Low-value Clinical Practices in the Emergency Department According to Level of Evidence (Review Phase) and Expert Opinion(Consultation Phase)
Clinical Practices in the Emergency Department*Level of Evidence** I—RCT to
IV—Expert Consensus No. StudiesExpert Opinion† 1—Clearly Low Valueto 5—Clearly Beneficial No. Experts
Hospital admission in adult blunt abdominal trauma withnormal physical examination and negative FAST or CT[1–3]‡
Hospital admission in pediatric blunt abdominal trauma withnormal physical examination, asymptomatic, and negativeFAST or CT[4–6]
Hospital admission in stable anterior abdominal stab wound,negative on FAST or CT and negative local wound exploration[7–9]
Hospital admission in adult mild TBI, negative on a validated clinicaldecision rule (e.g., CCHR, NEXUS II) or normal CT and normalclinical examination, not on anticoagulation therapy[2 10–18]
Hospital admission in pediatric mild TBI, negative on validatedclinical decision rule (e.g., CATCH, PECARN, CHALICE)or normal CT and normal physical examination[19–21]
Immobilization in suspected scaphoid fracture with negative CTor MRI[22–24]
Head CT in adult mild TBI, negative on a validated clinical decisionrule (e.g., CCHR, CHIP, NEXUS II)CW, EAST, NQF, CIHI [13 15 25–88]
Head CT in pediatric mild TBI, negative on a validated clinical decisionrule (e.g., PECARN, CATCH, CHALICE)CW, CIHI [19–21 25 38 89–124]
Repeat head CT in pediatric mild TBI, positive initial CT andno clinical deterioration[125–134]
Cervical spine CT in adult trauma, negative on a validated clinical decisionrule (e.g., Canadian C-Spine Rule, NEXUS)CW, NQF, NICE [47 58 135–149]
Cervical spine CT in pediatric trauma, able to co-operate andcommunicate and negative on a validated clinical decisionrule (e.g., NEXUS)[109 124 150–159]
CT angiography of the neck in suspected blunt cerebrovascular injury,negative on a validated clinical decision rule (e.g., DENVER)[160–162]
Chest CT in adult blunt thoracic trauma, negative on a validated clinicaldecision rule (e.g., NEXUS-Chest)[163–172]
Abdominal CT in pediatric blunt abdominal trauma, negative on avalidated clinical decision rule (e.g., PECARN, BATiC) andnegative FAST[6 109 123 173–182]
Pelvic CT in pediatric multiple injuries, no pain, normal examinationof pelvis/hip, no femur deformity, no hematuria or abdominalpain/tenderness, GCS > 13 and hemodynamically stable[183]
Whole-body CT in minor or single-system traumaCW, NICE [25 172 184–187]
Pretransfer CT in pediatric trauma for injuries that the facility does nothave the capacity to treat[6 188–191]
Posttransfer repeat CT in transferred trauma patient with imagingperformed in the initial center, no disease progression or additionaldetails needed[88 192–196]
Head X-ray in pediatric minor head injury, negative on a validated clinicaldecision rule (e.g., C3PO)[124 197–199]
Chest X-ray in blunt trauma, hemodynamically stable withnormal physical examNICE [200–205]
Wrist X-ray in adult wrist injury with normal physical exam[206]
Wrist X-ray in pediatric wrist injury, >2 years of age and normalphysical exam[207 208]
Pelvic X-ray in blunt trauma, stable with negative physicalexam for pelvic injuryNICE[205 209–213]
Continued on next page
J Trauma Acute Care SurgVolume 86, Number 6 Moore et al.
© 2019 Wolters Kluwer Health, Inc. All rights reserved. 987
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.

TABLE 2. (Continued)
Clinical Practices in the Emergency Department*Level of Evidence** I—RCT to
IV—Expert Consensus No. StudiesExpert Opinion† 1—Clearly Low Valueto 5—Clearly Beneficial No. Experts
Knee X-ray in adult trauma, negative on a validated clinicaldecision rule (e.g., Ottawa Knee Rule, Pittsburgh)[214–217]
Ankle X-ray in adult trauma, negative on a validated clinicaldecision rule (e.g., Ottawa Ankle Rule)[218–239]
Ankle X-ray in pediatric trauma, >2 years of age and negative on avalidated clinical decision rule (e.g., Ottawa Ankle Rule)[240–248]
Routine blood tests in trauma, <60 years old, no regular medications,isolated peripheral or low-energy injury and no significantmedical history[249]
Cardiac enzymes in sternal fractures[250]
Tube thoracostomy in pediatric blunt trauma with small hemothoraxor occult pneumothorax[251]
Tranexamic acid >3 h in traumaNICE [172 252 253]
Recombinant factor VIIa (rFVIIa) in isolated TBI with intracerebralhemorrhage[254 255]
Thoracotomy in penetrating trauma with CPR >15 minutes and no signsof life (pupillary response, respiratory effort, or motor activity)[256–259]
Thoracotomy in blunt trauma with CPR > 10 minutes, no signs of life orasystole is the presenting rhythm and no pericardial tamponade[257–259]
*Review phase: at least one Level I, II, or III study (review phase) AND Consultation phase:≥75% of experts who responded to the question classified the practice as clearly or potentiallylow value and no experts classified it as clearly beneficial.
**Level of evidence of clinical practices based on study design, I, RCTor SR of RCT; II, prospective studies, quasi-randomized studies, SR of level II studies; III, case–control, case series,cross-sectional, retrospective, SR of level III studies; IV, expert consensus, narrative review, other.
†Level of agreement of consulted experts on the value of clinical practices, 1, clearly low-value; 2, possibly low-value; 3, controversial; 4, possibly beneficial; 5, clearly beneficial; 6,undecided.
‡See Supplemental Digital Content 1, eReferences, http://links.lww.com/TA/B327, for table's references.BATIC, blunt abdominal trauma in children; CATCH, Canadian Assessment of Tomography for Childhood Head injury; CCHR, Canadian CT Head Rule; CHALICE, Children's Head
Injury Algorithm for the prediction of Important Clinical Events; CHIP, CT in head injury patients; CIHI, Canadian Institute for Health Information; CPR, cardiopulmonary resuscitation;CW, Choosing Wisely; EAST, Eastern Association for the Surgery of Trauma; FAST, Focused Assessment with Sonography in Trauma; GCS, Glasgow Coma Scale; MRI, magnetic resonanceimaging; NEXUS, National Emergency X-ray Utilization; NICE, National Institute for Health and Care Excellence; NQF, National Quality Forum; PECARN, Pediatric Emergency Care Ap-plied Research Network; SR, systematic review.
Moore et al.J Trauma Acute Care Surg
Volume 86, Number 6
on expert opinion, and less than 5%were RCTs. The majority ofstudies aimed to evaluate the effectiveness of the clinical prac-tice (55%), whereas one quarter aimed to develop guidelinesor derive/validate a clinical decision rule. Seventeen percentaimed to evaluate the prevalence of overuse or the efficacy of ade-implementation intervention. Less than 1% aimed to deriveor validate quality indicators. More than one third of low-valuepractices pertained to the treatment of head injury, and mostwere specific to adult (37%) or pediatric (12%) populations.One half of clinical practices targeted diagnostic interventions,40% targeted therapeutic interventions and 5% targeted ICUor hospital admission.
We approached 39 experts of whom 36 (92%) agreed toparticipate and completed the survey including 8 of 9 emergencyphysicians, 9 of 9 critical care physicians, 1 of 1 neurosurgeon,10 of 12 trauma surgeons, and 8 of 8 orthopedic/spine surgeonsfrom Canada, United States, Australia and the United Kingdom.After the first consultation phase, we identified 150 clinical prac-tices (Tables 2–5 and Supplemental Digital Content 4, Table 2,http://links.lww.com/TA/B327). In the Web-based survey, 66clinical practices were considered clearly or potentially low-value
988
Copyright © 2019 Wolters Kluwer H
by at least 75% of respondents. Thereafter, we identified 63clinical practices that met our criteria as candidates for low-value injury care, that is, they were reported as low value in atleast one Level I, II, or III study, considered clearly or potentiallylow value by at least 75% of respondents and not consideredclearly beneficial by any of the experts (Tables 2–5). Amongthese clinical practices, 13 were supported by do-not-do recom-mendations in internationally recognized clinical practice guide-lines (i.e., indications were the same or very similar). Ninepractices included as do-not-do recommendations in clinicalguidelines were not selected by our criteria (Supplemental Dig-ital Content 4, Table 2, http://links.lww.com/TA/B327).
We identified 33 candidates for low-value injury care inthe emergency room of which five were related to hospital ad-mission for abdominal trauma or mild traumatic brain injury(TBI) and 20 were related to imaging including computed to-mography (CT) or X-ray for mild TBI, ankle, knee, chest andcervical spine injuries (Table 2). We also identified 15 ED prac-tices in the gray zone including repeat head CT in adult mildcomplicated TBI and hospital admission in pediatric isolatedskull fracture (Supplemental Digital Content 4, Table 2, http://
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

TABLE 3. Low-value Clinical Practices in General Trauma Surgery According to Level of Evidence (Review Phase) and Expert Opinion(Consultation Phase)
Clinical Practices in Surgery*Level of Evidence** I—RCT to
IV—Expert Consensus No. StudiesExpert Opinion† 1—Clearly Low Value to
5—Clearly Beneficial No. Experts
Prolonged bedrest for pediatric blunt splenic or liver injury; >1 night forgrade I-II and >2 nights for grade III[1 2]‡
Angioembolization for grade I-III renal injuries[3]
Damage control laparotomy for resuscitated trauma patients whoare physiologically restored and not massively transfused[4]
Surgical management of grade IV-V liver injury in patients whoare hemodynamically stable with no indication for surgicaltreatment of associated injuriesEAST [5–9]
Surgical management of pediatric liver injury[10 11]
Surgical management of penetrating neck injury with soft signs onclinical examination and negative on multidetector CT angiography[12–16]
Surgical management of penetrating renal injury in patients who arehemodynamically stable, have no contrast blush indicating arterialhemorrhage, have a viable kidney and have no gross extravasation[17 18]
Surgical management of blunt isolated splenic injury in patients who arehemodynamically stableEAST[19–24]
Surgical management of pediatric splenic injury in children who aremonitored and hemodynamically stable[25–28]
*Review phase: at least one Level I, II or III study (review phase) AND Consultation phase: ≥75% of experts who responded to the question classified the practice as clearly or potentiallylow value and no experts classified it as clearly beneficial.
**Level of evidence of clinical practices based on study design, I, RCTor SR of RCT; II, prospective studies, quasi-randomized studies, SR of level II studies; III, case–control, case series,cross-sectional, retrospective, SR of level III studies; IV, expert consensus, narrative review, other.
†Level of agreement of consulted experts on the value of clinical practices, 1, clearly low-value; 2, possibly low-value; 3, controversial; 4, possibly beneficial; 5, clearly beneficial; 6,undecided.
‡See eReferences for table's references.EAST, Eastern Association for the Surgery of Trauma; SR, systematic review.
J Trauma Acute Care SurgVolume 86, Number 6 Moore et al.
links.lww.com/TA/B327). Nine low-value practices were se-lected for general trauma surgery, six of which were related tooperative management of liver, renal, splenic, and neck injuries(Table 3). In addition, we identified 15 practices in the gray zoneincluding follow-up imaging for nonoperative blunt renal injuryand surgical management of high-grade pancreatic or renal inju-ries (Supplemental Digital Content 4, Table 2, http://links.lww.com/TA/B327). We identified 15 low-value practices in the in-tensive care unit of which eight targeted TBI (Table 4). Fourwere related to medications (corticosteroids, antibiotics and an-tiseizure prophylaxis) and four were related to fluids and bloodproducts (albumin, colloids, platelet and red blood cell transfu-sion). Twenty-six (63%) of ICU clinical practices were in thegray zone (Supplemental Digital Content 4, Table 2, http://links.lww.com/TA/B327) including neurosurgical consultationin acute mild complicated TBI, decompressive craniotomy andhourly neurological assessments >24 hours for stable TBI. Fivelow-value practices were identified in orthopedics targeting fol-low-up consultation, spine service consultation, repeat X-ray, or-thosis for thoracolumbar burst fractures and preoperative bloodtests (Table 5). Thirty-one (86%) orthopedic practices in acuteinjury care were classed in the gray zone of which six targetedfollow-up consultation, nine imaging, and five immobilization(Supplemental Digital Content 4, Table 2, http://links.lww.com/TA/B327).
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
DISCUSSION
We identified 63 clinical practices that met criteria forlow-value intrahospital injury care. These potential low-valuepractices are supported by empirical evidence and expert opin-ion. Conditional on the results of future research, they representpotential targets for guidelines, overuse metrics and de-imple-mentation interventions. We also identified 87 clinical practicesin the gray zone, which are not consistently supported by empir-ical studies and expert opinion. While these practices requiremore evidence before being labeled low-value, they may be in-teresting targets for value-based decision-making.
The literature on low-value clinical practices in injury careis scarce. Internationally recognized medical associations pub-lish guidelines on injury care.31–34 However, few pertain to clin-ical practices that should be avoided. Health care qualityorganizations including ChoosingWisely and the National Insti-tute for Health and Care Excellence publish recommendationsspecific to low-value practices but few target injury care.35,36
In addition, these recommendations are often based only on ex-pert consensus.20 Three previous literature reviews on low-valuecare across a range of diagnostic groups identified nine low-value practices specific to injury care.14,19,20,37 We were ableto identify many more practices because targeting a specificdiagnostic group allows for a much more sensitive review
989
ealth, Inc. All rights reserved.

TABLE 4. Low-value Clinical Practices in the Intensive Care Unit According to Level of Evidence (Review Phase) and Expert Opinion(Consultation Phase)
Clinical Practices in the Intensive Care Unit*Level of Evidence** I—RCT to
IV—Expert Consensus No. StudiesExpert Opinion† 1—Clearly Low Value to
5—Clearly Beneficial No. Experts
ICU admission in adults with acute mild complicated TBI whoare not on irreversible anticoagulation[1–5]‡
Neurosurgical consultation in adults with acute mild TBI anda negative CT[6 7]
Inferior vena cava filter for prevention of PE in acute spinal cord injurywithout DVT and no contraindications for low-molecular weight heparin[8 9]
Intermittent pneumatic devices for thrombophrophylaxis in nonambulatoryadults admitted to the trauma service with no contraindicationsfor low-molecular-weight heparin[10]
Chest X-ray after chest tube removal in patients with thoracic trauma whoare not mechanically ventilated and have appropriate mental status tocommunicate new symptoms[11]
Antibiotic prophylaxis in basal skull fractures without evidenceof CSF leakage[12–14]
High-dose corticosteroids in spinal cord injury[15–20]
High-dose corticosteroids in adults with TBIBTF, CW, NICE[21–32]
Antiseizure prophylaxis >1 week in adults with severe TBIBTF [32–36]
Albumin in severe TBI[37–39]
Synthetic colloids (dextran, gelatin, hydroxyethyl starch) in traumapatients[40–46]
Platelet transfusion in adults with TBI on antiplatelet therapy[47–51]
RBC transfusion in adult trauma patients above the transfusionthreshold (Hemoglobin >7 g/dL) with no ongoing or suspecteduncontrolled bleeding, no TBI and no coronary heart disease[52–66]
Therapeutic hypothermia in adults with TBI and ICP responding to otherstage 2 treatmentsACS, BTF [32 67–74]
Prophylactic hyperventilation in adults with severe TBIBTF [22 28 32 67 75 76]
*Review phase: at least one Level I, II or III study (review phase) AND consultation phase: ≥75% of experts who responded to the question classified the practice as clearly or potentiallylow value and no experts classified it as clearly beneficial.
**Level of evidence of clinical practices based on study design, I, RCTor SR of RCT; II, prospective studies, quasi-randomized studies, SR of level II studies; III, case–control, case series,cross-sectional, retrospective, SR of level III studies; IV, expert consensus, narrative review, other.
†Level of agreement of consulted experts on the value of clinical practices, 1, clearly low-value; 2, possibly low-value; 3, controversial; 4, possibly beneficial; 5, clearly beneficial; 6,undecided.
‡See eReferences for table's references.ACS, American College of Surgeons; BTF, Brain Trauma Foundation; CSF, cerebrospinal fluid; ICP, intracranial pressure; SR, systematic review; RBC: red blood cell.
Moore et al.J Trauma Acute Care Surg
Volume 86, Number 6
strategy.15 With over 50,000 citations to screen and more than1,400 documents to extract in our study, a similar search strategywith no restrictions on diagnosis would have been unfeasible.
Twenty-six percent of low-value practices identified in ourreview were related to imaging. This is consistent with a previ-ous review of low-value care measures20 and may be becausethe value of imaging is relatively easy to evaluate retrospectively.Unnecessary imaging generates important costs14,38 and mayexpose patients to high doses of radiation with non-negligiblelong-term risks of cancer.39–41 We retained 12 low-value prac-tices on imaging which are already supported by guidelinesand/or widely used clinical decision rules and eight additionalclinical practices which are potential targets for low-value imag-ing. We identified 21 low-value practices related to operative
990
Copyright © 2019 Wolters Kluwer H
(versus nonoperative) management of which two are includedin EAST guidelines.31 A recent review found 71 low-value prac-tices in general surgery representing an estimated annual cost of153 million euros per year in the United Kingdom.42 However,none of these practices pertained to injury. Seventeen prac-tices identified in our review pertained to medications of whichfive were supported by do-not-do recommendations in clinicalguidelines.31,33,35,36 There is a large body of literature onoverprescribing in primary care.14,43–45 However, an importantknowledge gap on in-hospital medication exists, probably inpart due to the fact that hospital prescriptions are not recordedin administrative databases. Other low-value practices identifiedin our review were hospital and ICU admission (n = 11) and fol-low-up consultation (n = 7). Literature on overuse in these areas
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

TABLE 5. Low-value Clinical Practices in Orthopedics According to Level of Evidence (Review Phase) and Expert Opinion(Consultation Phase)
Clinical Practices in Orthopedics*Level of Evidence** I—RCT to
IV—Expert Consensus Number of StudiesExpert Opinion† 1—Clearly Low Value to5—Clearly Beneficial NUMBER of Experts
Follow-up consultation for pediatric closed isolateduncomplicated zone 2 clavicle fracture[1]‡
Spine service consultation for isolated thoracolumbartransverse process fracture[2]
Repeat X-ray for isolated closed Mason-Johnson type-I radialhead/neck fracture with no clinical complaints[3]
Orthosis for A0-A3 thoracolumbar burst fracture with kyphoticdeformity <35 degrees, no associated posterior ligamentouscomplex injury and no neurologic symptoms[4–7]
Preoperative blood tests for ASA grade I orthopedic injuryrequiring minor surgery[8]
*Review phase: at least one Level I, II or III study (review phase) AND Consultation phase: ≥75% of experts who responded to the question classified the practice as clearly or potentiallylow value and no experts classified it as clearly beneficial.
**Level of evidence of clinical practices based on study design, I, RCTor SR of RCT; II, prospective studies, quasi-randomized studies, SR of level II studies; III, case–control, case series,cross-sectional, retrospective, SR of level III studies; IV, expert consensus, narrative review, other.
†Level of agreement of consulted experts on the value of clinical practices, 1, clearly low-value; 2, possibly low-value; 3, controversial; 4, possibly beneficial; 5, clearly beneficial; 6,undecided.
‡See eReferences for table's references.ASA, American Society of Anesthesiologists.
J Trauma Acute Care SurgVolume 86, Number 6 Moore et al.
is sparse, possibly because they are very context-specific. Ninepractices included in internationally recognized guidelines aspractices to avoid were not retained in our study, all because lessthan 75% of experts identified them as clearly or potentiallylow-value. This discordance could be due to our strict selectioncriteria based on literature evidence and agreement of more than75% of experts. Guidelines are often based on few, low-qualitystudies or expert consensus, but rarely both.46 It may also be ex-plained by differing influences of local context, industry pres-sure or single highly-mediatized studies.13,15,21,47,48 It doessuggest that moving forward, guidelines/metrics on low-valueinjury care should be based both on evidence from high-qualityexperimental or observational studies AND expert opinion andshould account for the possible influence of local context. Also,the consensus process should strive to minimize intellectual, ac-ademic and financial biases.
Strengths and LimitationsThis study represents a rigorous, exhaustive review of the
literature on low-value clinical practices in injury care. Resultsfrom our scoping review are supported by a consultation studywith 36 experts representing the clinical specialties involved intrauma care on three continents. The participation rate of over90% demonstrates the high level of knowledge-user interest inthis topic. In addition, experts are all involved in clinical re-search in acute injury care so are likely to have good knowledgeof the evidence-base on clinical practices for injury admissions.
This study does have limitations that should be consideredin the interpretation of results. First, for feasibility reasons, oursearch strategywas based on key words related to low-value careand was therefore dependent on authors' judgment of the valueof clinical practices. This may have led us to miss some low-value practices. For example, authors of the Randomized Evalu-ation of Surgery with Craniectomy of Uncontrollable Elevation
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
of Intracranial Pressure (RESCUEicp) trial that observed lowermortality but worse functional outcomes in the interventiongroup did not clearly identify decompressive craniectomy as alow-value practice.49 However, by thoroughly screening articlereferences, gray literature including injury organizations andhealth care quality websites, and consulting experts for furtherreferences, we are confident that we captured a large propor-tion of potentially low-value clinical practices that have beenreported in the literature. Second, for feasibility reasons, werestricted the review to studies published since 2006. Wemay therefore have missed some important RCTs publishedearlier, for example, the National Acute Spinal Cord InjuryStudies I on high-dose steroids for spinal cord injury50 and theHarborview trial on antiseizure prophylaxis in traumatic braininjury.51 However, both these practices were captured throughreviewof guidelines. Fourth, due to the scoping design of our re-view, we did not evaluate methodological quality. Strength ofevidence was only based on study design. Fifth, the last phaseof the review was based on a single web survey therefore rep-resents the results of a consultation rather than expert consen-sus. In addition, we used a convenience sample and only oneneurosurgeon was surveyed. Finally, to identify targets for de-implementation we will need data on frequency (how frequentlyis the clinical practice actually used?), inter-provider variations(is there evidence of practice variation?) and economic impact(would deadoption lead to important savings?).52,53 These as-pects will be incorporated into the following subsequent phasesof the Canadian Program for Monitoring Overuse in InjuryCare; a systematic review to GRADE evidence for low-valueclinical practices identified in this review,54 a RAND-UCLA ex-pert consensus study to develop a set of quality indicatorstargeting low-value practices, a multicenter retrospective cohortstudy to derive and validate metrics for the quality indicatorsand a cluster RCT to evaluate the effectiveness of quality
991
ealth, Inc. All rights reserved.

Moore et al.J Trauma Acute Care Surg
Volume 86, Number 6
indicators in an audit-feedback intervention. The research pro-gram will also allow us to take into account the specificitiesof low-frequency, high-risk injuries.
CONCLUSION
This study fills a major knowledge gap on medical proce-dure overuse in acute injury care. Results will inform researchpriorities and the development of metrics to measure overuse.This knowledge will provide a solid basis for the developmentof interventions targeting deimplementation, such as clinicaldecision rules and shared decision making tools. This has thepotential to decrease costs, increase resource availability, andreduce mortality and morbidity due to unnecessary tests andtreatments and reduce patient stress and physicians' workload.
AUTHORSHIP
L.M. led the conception and design of the study, acquisition of data, anal-ysis and interpretation of data, and drafted the article. F.Lauzier made sub-stantial contributions to the conception and design, the acquisition ofthe data, the analysis and the interpretation of data. He revised the articlecritically for important intellectual content and gave final approval of theversion to be published. P.-A.T. made substantial contributions to the ac-quisition of the data, the analysis and the interpretation of data. He partic-ipated in drafting the article and gave final approval of the version to bepublished. K.M.B. made substantial contributions to the acquisition ofthe data. She revised the article critically for important intellectual contentand gave final approval of the version to be published. I.made substantialcontributions to the acquisition of the data. She revised the article criticallyfor important intellectual content and gave final approval of the version tobe published. P.A. made substantial contributions to the conception anddesign, the acquisition of the data, the analysis and the interpretation ofdata. He revised the article critically for important intellectual contentand gave final approval of the version to be published. É.M. made sub-stantial contributions to the conception and design and the acquisitionof the data. He revised the article critically for important intellectual con-tent and gave final approval of the version to be published. F.Lamontagnemade substantial contributions to the acquisition of the data. He revisedthe article critically for important intellectual content and gave final ap-proval of the version to be published. M.C. made substantial contribu-tions to the acquisition of the data. He revised the article critically forimportant intellectual content and gave final approval of the version tobe published. H.T.S. made substantial contributions to the conceptionand design and the acquisition of the data. He revised the article criticallyfor important intellectual content and gave final approval of the version tobe published. S.B. made substantial contributions to the conception anddesign and the acquisition of the data. He revised the article critically forimportant intellectual content and gave final approval of the version tobe published. B.G. made substantial contributions to conception and de-sign. She revised the article critically for important intellectual content andgave final approval of the version to be published. F.L. made substantialcontributions to the acquisition of the data. She revised the article criticallyfor important intellectual content and gave final approval of the version tobe published. N.Y. made substantial contributions to the acquisition ofthe data. He revised the article critically for important intellectual contentand gave final approval of the version to be published. H.C. made sub-stantial contributions to the acquisition of the data. He revised the articlecritically for important intellectual content and gave final approval of theversion to be published. J.K. made substantial contributions to the acqui-sition of the data. He revised the article critically for important intellectualcontent and gave final approval of the version to be published. P.C. madesubstantial contributions to the acquisition of the data. He revised the ar-ticle critically for important intellectual content and gave final approval ofthe version to be published. P.L.B. made substantial contributions to theacquisition of the data and the analysis and the interpretation of data.She revised the article critically for important intellectual content and gavefinal approval of the version to be published. J.P. made substantial contri-butions to the acquisition of the data and the analysis and the
992
Copyright © 2019 Wolters Kluwer H
interpretation of data. He revised the article critically for important intel-lectual content and gave final approval of the version to be published.C.T. made substantial contributions to the acquisition of the data. She re-vised the article critically for important intellectual content and gave finalapproval of the version to be published. A.F.T. made substantial contribu-tions to the conception and design, the acquisition of the data, the anal-ysis and the interpretation of data. He revised the article critically forimportant intellectual content and gave final approval of the version tobe published.
DISCLOSURE
Conflict of interest and source of funding: This research is funded by theCanadian Institutes of Health Research (Foundation grant, 353374) and theFonds de Recherche du Québec – Santé (career award, L.M., F.Lau, F.Lam,M.C.). Patrick Archambault is supported by a Clinical-Embedded ScientistAward from the CIHR. Dr Turgeon is the Canada Research Chair in Criti-cal Care Neurology and Trauma. For the remaining authors, no conflictswere declared.
REFERENCES1. Centers for Disease Control and Prevention. Injury Prevention&Control 2018.
Available at: https://www.cdc.gov/injury/index.html. Accessed Mai 14, 2018.2. Egi M, Bellomo R, Stachowski E, French CJ, Hart G, Stow P, Li WQ,
Bates S. Intensive insulin therapy in postoperative intensive care unitpatients—a decision analysis. Am J Respir Crit Care Med. 2006;173(4):407–413.
3. Birkmeyer JD, Reames BN, McCulloch P, Carr AJ, Campbell WB,Wennberg JE. Understanding of regional variation in the use of surgery.Lancet. 2013;382(9898):1121–1129.
4. Fisher ES, Wennberg DE, Stukel TA, Gottlieb DJ, Lucas FL, Pinder EL. Theimplications of regional variations in Medicare spending. Part 2: health out-comes and satisfaction with care. Ann Intern Med. 2003;138(4):288–298.
5. Moore L, Evans D, Hameed SM, Yanchar NL, Stelfox HT, Simons R,Kortbeek J, Bourgeois G, Clément J, Lauzier F, et al. Mortality in Canadiantrauma systems: a multicenter cohort study. Ann Surg. 2017;265(1):212–217.
6. Barker P, Buchanan-Barker P. More harm than good. Nursing standard(Royal College of Nursing (Great Britain) : 1987). 2006;20(30):28–29.
7. Institute of Medicine Committee on Quality of Health Care in A. Crossingthe Quality Chasm: A New Health System for the 21st Century. Washington,DC: National Academies Press (US); 2001.
8. Berwick DM, Hackbarth AD. Eliminating waste in US health care. JAMA.2012;307(14):1513–1516.
9. Boat TF, Chao SM, O'Neill PH. From waste to value in health care. JAMA.2008;299(5):568–571.
10. Reilly BM, Evans AT. Much ado about (doing) nothing. Ann Intern Med.2009;150(4):270–271.
11. Morgan DJ, Dhruva SS, Wright SM, Korenstein D. 2016 update on medicaloveruse: a systematic review. JAMA Intern Med. 2016;176(11):1687–1692.
12. Hauser CJ, Adams CA Jr., Eachempati SR; Council of the Surgical InfectionS. Surgical infection society guideline: prophylactic antibiotic use in openfractures: an evidence-based guideline. Surg Infect. 2006;7(4):379–405.
13. Berwick DM. Avoiding overuse—the next quality frontier. Lancet. 2017.14. Brownlee S, Chalkidou K, Doust J, Elshaug AG, Glasziou P, Heath I,
Nagpal S, Saini V, Srivastava D, Chalmers K, et al. Evidence for overuseof medical services around the world. Lancet. 2017;390:156–168.
15. Saini V, Brownlee S, Elshaug AG, Glasziou P, Heath I. Addressing overuseand underuse around the world. Lancet. 2017;390:105–107.
16. Bennett MH, Trytko BE, Jonker B. A systematic review of the use of hyper-baric oxygen therapy in the treatment of acute traumatic brain injury. DivingHyperb Med. 2006;36(1):39–46.
17. Niven DJ, Mrklas KJ, Holodinsky JK, Straus SE, Hemmelgarn BR, Jeffs LP,Stelfox HT. Towards understanding the de-adoption of low-value clinicalpractices: a scoping review. BMC Med. 2015;13:255.
18. Emanuel EJ, Fuchs VR. The perfect storm of overutilization. JAMA. 2008;299(23):2789–2791.
19. Chan KS, Chang E, Nassery N, Chang HY, Segal JB. The state of overusemeasurement: a critical review. Medical care research and review : MCRR.2013;70(5):473–496.
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
J Trauma Acute Care SurgVolume 86, Number 6 Moore et al.
20. de Vries EF, Struijs JN, Heijink R, Hendrikx RJ, Baan CA. Are low-valuecare measures up to the task? A systematic review of the literature. BMCHealth Serv Res. 2016;16(1):405.
21. Elshaug AG, Rosenthal MB, Lavis JN, Brownlee S, Schmidt H, Nagpal S,Littlejohns P, Srivastava D, Tunis S, Saini V. Levers for addressing medicalunderuse and overuse: achieving high-value health care. Lancet. 2017.
22. Segal JB, Bridges JF, Chang HY, Chang E, Nassery N, Weiner J, Chan KS.Identifying possible indicators of systematic overuse of health care proce-dures with claims data.Med Care. 2014;52(2):157–163.
23. Arksey H, O'Malley L. Scoping studies: towards a methodological frame-work. Int J Soc Res Methodol. 2005;8:19–32.
24. Tricco AC, Lillie E, ZarinW, O'Brien K, Colquhoun H, KastnerM, Levac D,Ng C, Sharpe JP, Wilson K, et al. A scoping review on the conduct andreporting of scoping reviews. BMC Med Res Methodol. 2016;16:15.
25. Moore L, Boukar KM, Tardif PA, Stelfox HT, Champion H, Cameron P,Gabbe B, Yanchar N, Kortbeek J, Lauzier F, et al. Low-value clinical prac-tices in injury care: a scoping review protocol. BMJ Open. 2017;7(7):e016024.
26. Dretzke J, Burls A, Bayliss S, Sandercock J. The clinical effectiveness of pre-hospital intravenous fluid replacement in trauma patients without head in-jury: a systematic review. Dent Traumatol. 2006;8(3):131–141.
27. GuttmannA, RazzaqA, Lindsay P, Zagorski B, AndersonGM.Developmentof measures of the quality of emergency department care for children using astructured panel process. Pediatrics. 2006;118(1):114–123.
28. OCEBM Levels of Evidence Working Group. The Oxford 2011 levels ofevidence: Oxford Centre for Evidence-Based Medicine; 2011. Availableat: http://www.cebm.net/index.aspx?o=5653. Accessed January 25, 2019.
29. Morgan D. Snowball sampling. In: Given L, ed. The SAGE Encyclopedia ofQualitative Research Methods. Thousand Oaks: SAGE Publications Inc.;2008:816–817.
30. Limesurvey GmbH. LimeSurvey: an open source survey tool LimeSurveyGmbH, Hamburg, Germany. Available at: http://www.limesurvey.org. AccessedJanuary 25, 2019.
31. Eastern Association for the Surgery of Trauma. EAST Practice ManagementGuidelines 2018. Available at: https://www.east.org/education/practice-management-guidelines. Accessed Mai 3, 2018.
32. Carney N, Ghajar J, Jagoda A, Bedrick S, Davis-OʼReilly C, du Coudray H,Hack D, Helfand N, Huddleston A, Nettleton T, et al. Concussion guide-lines step 1: systematic review of prevalent indicators. Neurosurgery.2014;75(Suppl 1):S3–S15.
33. Carney N, Totten AM, O'Reilly C, Ullman JS, Hawryluk GW, Bell MJ,Bratton SL, Chesnut R, Harris OA, Kissoon N, et al. Guidelines for the man-agement of severe traumatic brain injury, fourth edition.Neurosurgery. 2017;80(1):6–15.
34. American College of Surgeons. Resources for optimal care of the injured pa-tient 2014/resources repository 2018. Available at: https://www.facs.org/quality-programs/trauma/vrc/resources. Accessed May 4, 2018.
35. Choosing Wisely. Clinician lists: ABIM foundation. Available at: http://www.choosingwisely.org/clinician-lists/. Accessed May 4, 2018.
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
36. National Institute for Health and Care Excellence (NICE). Trauma qualitystandard 2018.Available at: https://www.nice.org.uk/guidance/qs166.AccessedMay 4, 2018.
37. Elshaug AG. Over 150 potentially low-value health care practices: anAustralian study. Med J Aust. 2013;198(2):85.
38. Schoen C, Osborn R, Doty MM, Bishop M, Peugh J, Murukutla N. Towardhigher-performance health systems: adults' health care experiences in sevencountries, 2007. Health Aff (Millwood). 2007;26(6):w717–w734.
39. Brenner DJ, Hricak H. Radiation exposure from medical imaging: time toregulate? JAMA. 2010;304(2):208–209.
40. Hendee WR, O'Connor MK. Radiation risks of medical imaging: separatingfact from fantasy. Radiology. 2012;264(2):312–321.
41. Royal HD. Effects of low level radiation—what's new? Semin Nucl Med.2008;38(5):392–402.
42. Malik HT, Marti J, Darzi A, Mossialos E. Savings from reducing low-valuegeneral surgical interventions. Br J Surg. 2018;105(1):13–25.
43. Morgan SG, Hunt J, Rioux J, Proulx J, Weymann D, Tannenbaum C. Fre-quency and cost of potentially inappropriate prescribing for older adults: across-sectional study. CMAJ open. 2016;4(2):E346–E351.
44. Makary MA, Overton HN, Wang P. Overprescribing is major contributor toopioid crisis. BMJ. 2017;359:j4792.
45. Bentley TG, Effros RM, Palar K, Keeler EB. Waste in the U.S. health caresystem: a conceptual framework.Milbank Q. 2008;86(4):629–659.
46. Chen Y, Yang K, Marušic A, Qaseem A, Meerpohl JJ, Flottorp S, Akl EA,Schünemann HJ, Chan ES, Falck-Ytter Y, et al. A reporting tool for practiceguidelines in health care: the RIGHT statement. Ann Intern Med. 2017;166(2):128–132.
47. Kleinert S, Horton R. From universal health coverage to right care for health.Lancet. 2017;390(10090):101–102.
48. Saini V, Garcia-Armesto S, Klemperer D, Paris V, Elshaug AG, Brownlee S,Ioannidis JPA, Fisher ES. Drivers of poor medical care. Lancet. 2017;390(10090):178–190.
49. Hutchinson PJ, Kolias AG, Timofeev IS, Corteen EA, Czosnyka M,Timothy J, Anderson I, Bulters DO, Belli A, EynonCA, et al. Trial of decom-pressive craniectomy for traumatic intracranial hypertension. N Engl J Med.2016;375(12):1119–1130.
50. Bracken MB, Shepard MJ, Hellenbrand KG, Collins WF, Leo LS,Freeman DF, Wagner FC, Flamm ES, Eisenberg HM, Goodman JH, et al.Methylprednisolone and neurological function 1 year after spinal cord injury.Results of the National Acute Spinal Cord Injury Study. J Neurosurg. 1985;63(5):704–713.
51. Temkin NR, Dikmen SS,Wilensky AJ, Keihm J, Chabal S, WinnHR. A ran-domized, double-blind study of phenytoin for the prevention of post-traumatic seizures. N Engl J Med. 1990;323(8):497–502.
52. Pandya A. Adding cost-effectiveness to define low-value care. JAMA. 2018.53. Ryan AM, Tompkins CP. Efficiency and value in healthcare: linking cost and
quality measures. National Quality Forum. 2014.54. Atkins D, Best D, Briss PA, Eccles M, Falck-Ytter Y, Flottorp S, Guyatt GH,
Harbour RT, Haugh MC, Henry D, et al. Grading quality of evidence andstrength of recommendations.BMJ (Clinical research ed). 2004;328(7454):1490.
993
ealth, Inc. All rights reserved.
ORIGINAL ARTICLE
Gamma probe-guided confirmation of balloon placement inendovascular procedures
Yunchul Park, MD, Young Goun Jo, MD, Kang-Ho Choi, MD, PhD,Munki Kim, DVM, PhD, and Jahae Kim, MD, PhD, Gwangju, Korea
Sub
Fro
Ad
DO
99
BACKGROUND: G
mitted: November 9,2019, Published onlinm the Division of Trational University Hostional University HwChonnam National UWelfare and Family AK.), Chonnam Nationdress for reprints: JahChonnam National UKorea; email: jhbt060
I: 10.1097/TA.000000
4
amma probes can provide real-time information on lesion location and allow radioguided surgery in many diseases. The purpose of thisstudy was to determine whether a gamma probe could be used to confirm balloon location in resuscitative endovascular balloon occlusionof the aorta and to determine the ease-of-use of the gamma probe localization method using human vasculature phantom and large animal.
METHODS: T
his investigation comprised a proof-of-concept study using human vasculature phantom and feasibility study using large animal. An as-sistant and two general surgeonswith no prior experience in handling a gamma probe participated in both studies. A gamma probewas usedby each surgeon to explore the location of a catheter balloon filled with 8 mL of normal saline containing 37 MBq of 99mTechnetium. Thedifferences between predicted and actual balloon locations and the times taken to perform the trials were recorded. Balloon locations wereconfirmed by planar gamma camera images. The results were analyzed and compared according to the operators and experiments.RESULTS: O
verall sensitivity and specificity for the localization of the catheter balloon were 100% and 91% in phantom study, respectively, and 100%and 100% in animal study, respectively. The performance of the two operators for exploring the balloon location was similar in both thephantom and the animal studies. The mean time taken to explore the balloon locations with the aid of the gamma probe was only 2.36 mi-nutes in phantom study and 2.65 minutes in the animal study.CONCLUSION: T
he gamma probe method was accurate and rapid for confirming balloon location. We suggest that the gamma probe has potential for con-firming balloon placement in endovascular procedures without the need for fluoroscopy. (J Trauma Acute Care Surg. 2019;86: 994–1000.Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.)KEYWORDS: G
amma probe; balloon; location; resuscitative endovascular balloon occlusion of the aorta.R esuscitative endovascular balloon occlusion of the aorta(REBOA) is a technique used to temporarily occlude large
vessels for controlling non-compressible truncal hemorrhage.The lower invasiveness and significant reductions in equipmentand experience compared with thoracotomy make REBOA ap-propriate for managing central circulation in patients at immi-nent risk of cardiovascular collapse.1,2 Fluoroscopic guidanceis generally required to confirm balloon location after blind in-sertion,2,3 but it is limited to the hospital setting.
A gamma probe is a handheld intraoperative radiation de-tector of photons, such as gamma rays. Radiation detectionprobe systems allow radioguided surgery for localization of thesentinel lymph node and occult lesions, as well as evaluationof intraoperative margins according to their radioactivity.4 Itcan provide vital and real-time information to the surgeon, notonly in malignancies, such as breast cancer,5 melanoma,6 and
2018, Revised: February 9, 2019, Accepted: February 14,e: March 1, 2019.uma, Department of Surgery (Y.P., Y.G.J.), Chonnam Na-pital; Department of Neurology (K.-H.C.), Chonnam Na-asun Hospital; The Heart Research Center (M.K.),niversity Hospital Designated by the Ministry of Health,ffairs of Korea; and Department of Nuclear Medicine (J.al University Hospital, Donggu, Gwangju, Korea.ae Kim, MD, PhD, Department of Nuclear Medicine,niversity Hospital, Jebongro 42, Donggu, Gwangju 61469,[email protected].
0000002238
Copyright © 2019 Wolters Kluwer H
colorectal cancer,7 but also in the surgical management ofparathyroid disease.8 These characteristics have resulted inconsideration expansion of gamma detection probe applica-tions.4 However, to our knowledge, the application of a gammaprobe to guide and confirm balloon location in catheter proce-dures has not yet been investigated.
The purpose of this experimental study was to determinewhether a gamma probe can be used to confirm balloon locationin REBOA in a human vasculature phantom. A further objectivewas to compare the performance of gamma-probe guided bal-loon exploration by two surgeons who had no previous experi-ence with gamma probes to determine whether the gammaprobe-guided method is easy to use. Finally, we performed anexperiment using a large animal to assess the feasibility of thisnovel approach for determining the balloon position in humantissue in REBOA.
METHODS
PhantomThe inner part of the human vasculature phantom was
purchased from Invasive Models LLC (Plymouth, MN). Thiseducational simulator (Bilateral Bob Plus, BB-6050) featuresthe arterial and venous structure of an average-sized adultmale and is intended to improve invasive transluminal tech-nique with regard to the setup, insertion, and managementof catheters, guidewires, and balloon catheters. The outershell of the phantom consists of a 5-mm thick, skin-colored
J Trauma Acute Care SurgVolume 86, Number 6
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 6 Park et al.
box, measuring 300 (W) � 600 (L) � 300 mm (H). When thelid is covered, all sides of the rectangular parallelepiped areenclosed, except a small gap for the approach to the bilateraliliac sheath port in the bottom of the outer shell (Fig. 1A).
AnimalA Yorkshire male swine (75 kg) was provided and ob-
served in the animal breeding house of our center designatedby the Ministry of Health, Welfare and Family Affairs ofKorea, for 2 months prior to the experiment. The experimentwas performed under anesthesia with zolazepam (2.5 mg/kg, in-tramuscular), tiletamine (2.5 mg/kg, intramuscular), xylazine(3 mg/kg, intramuscular), and azaperone (6 mg/kg, intramuscu-lar). After infusion of 10,000 units of heparin, in the supine po-sition, the left external iliac artery was exposed, and a 7F arterialsheath was placed using a modified Seldinger technique. A 7Fartery guiding catheter was inserted along the abdominal aortathrough the opening of the left external iliac artery, and the bal-loon catheter (REBOA RB-167080-E; Tokai Medical, Aichi,Japan) was then inserted.
Study DesignThis investigation consisted of two studies; a proof-
of-concept study using human vasculature phantom and a feasi-bility study using large animal. First, the phantom study wasperformed to validate the gamma probe-guided balloon localiza-tionmethod. An assistant and two general surgeons acting as op-erators participated. The assistant prepared the study equipment
Figure 1. Phantom study (A, B): schematic of the phantom (A) and timaging room (B). Animal study (C, D): the animal on the table of SPgamma probe for localization of the balloon catheter (D).
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
in the nuclear medicine imaging room before each surgeon en-tered the room, with this involving preparation of the balloon cath-eter (REBOA RB-167080-E; Tokai Medical, Aichi, Japan) andthen advancing it to an arbitrary location in aortic zone I or III.2
An 8-mL volume of normal saline containing 37 MBq oftechnetium-99m (99mTc) pertechnetate was then pushed into theballoon to inflate it with the outer shell of the phantom covered sothat the operators were blinded to the catheter placement (Fig. 1B).
After preparation of the inflated catheter, each operatorentered the nuclear medicine imaging room and used a gammaprobe with a setting for 99mTc energy to determine the balloonlocation (Neoprobe 2000; Neoprobe Corp, Dublin, OH). Thesystem console-emitted audible beeps and showed count persecond (cps) as a numeric value on the monitor when the probeneared the balloon. Stronger detector beeps and higher countsmeant that the position of the probe was closer to the ballooncontaining 99mTc-pertechnetate. Each operator marked the loca-tion of the inflated balloon according to the position where thebeeps and counts were the highest by putting a gamma-ray pointsource with a diameter of 3 mm on the outer shell of the phan-tom. The assistant recorded the count and the time taken to per-form the study. This defined one location trial, and 20 trials weremade by each operator in both zones I and III.
Second, animal study was performed to evaluate the feasi-bility of applying the gamma probe method for balloon localiza-tion to translate to human tissue (Fig. 1C). The same assistantand surgeons participated. The assistant entered the nuclearmedicine imaging room and randomly positioned the balloon
he experiment setting of gamma probe in the nuclear medicineECT/CT imaging machine (C) and the experiment picture using
995
ealth, Inc. All rights reserved.

Park et al.J Trauma Acute Care Surg
Volume 86, Number 6
catheter within the abdominal aorta of the swine. Then, theassistant pushed the same volume of normal saline containing99mTc-pertechnetate into the balloon to inflate it and fixed itslocation. After preparation of the inflated catheter, each operatorfollowed the same experimental method as described above tolocate the balloon (Fig. 1D). Once an operator predicted theballoon location, he placed a gamma-ray point source on theabdominal skin of the swine. Each operator performed 10 trialsin the animal study. Moreover, to determine whether the soundsemitted by the system console are audible in a noisy prehospitalenvironment, the maximum level of console-emitted noisedetected at the operator's location was measured. To evaluatethe safety of the swine, the skin color was examined before andafter the experiment. To estimate the operator's effective dosewhen using 37 MBq of 99mTc-pertechnetate, each operator worean electronic personal dosimeter (model EPD Mk2.3; Thermo)inside their surgical gown. The minimum detectable dose of thisdosimeter is 10 μSv, and this instrument is approved by theregulatory authority.
Balloon Location ConfirmationThe predicted and actual balloon locations were confirmed
using a hybrid Single Photon Emission Computed Tomography/Computed Tomography (SPECT/CT) imaging system (DiscoveryNM/CT 670; GE Healthcare). A 10-second lateral planar imagewas acquired for each trial using a 256 � 256 matrix and a 20%window centered around the 140 keV photopeak with a low-energy high-resolution parallel collimator. Additional SPECT/CTwas performed once every 10 trials (Fig. 2). A step-and-shootprotocol of 5 seconds/30° for 12 views per camera head wasused. CTwas performed immediately after SPECT. The currentwas 40mA, the voltage 140 kV, and 3.75-mm slices reconstructedin a 512 � 512 matrix.
All planar images were reviewed on a Xeleris workstation(GE Healthcare). The vertical distance from the inferior borderto the center of either gamma-ray point source or the catheterballoon was measured on each image. The predicted distancewas defined as the distance from the inferior border of the planarimage to the center of the gamma-ray point source, while the ac-tual distancewas defined as the distance from the inferior borderof the planar image to the center of catheter balloon (Fig. 3). Thedifference between the predicted and actual location was calcu-lated by subtracting the predicted location from the actual bal-loon location and taking the absolute value. The result of eachtrial was classified as a success if the gamma-ray point sourcewas located within the length of the inflated balloon, and as fail-ure if the gamma-ray point source did not fall within the lengthof the inflated balloon. Sensitivity was defined as the detectionof a signal during each trial, and specificity was defined as theratio of the number of successes to the number of trials.
Statistical AnalysisContinuous variables are expressed as mean ± standard
deviation (SD), and categorical variables as frequencies and per-centages. Student’s t-tests, Mann-Whitney U tests and Fisher'sexact tests were used to compare data between the two groups.With the significance level at 5% and the power at 80%, the ef-fect size of 2 was chosen on the basis of previous REBOA stud-ies,9,10 and the SD was calculated from the pilot experiments for
996
Copyright © 2019 Wolters Kluwer H
the calculation of the sample size in both the phantom and theanimal studies. From these data, the minimum number of trialsrequired to reach statistical significance was calculated byPS-Power and Sample Size Calculation Software (http:biostat.mc.vanderbilt.edu). Statistical analyses were performed usingSPSS version 21.0 (IBM Corp., Armonk, NY), with a p valueless than 0.05 being considered as statistically significant.
RESULTS
Phantom Study Results According to Aortic Zonesand Operator
A total of 20 balloon location prediction trials were per-formed by each operator in zones I and III (Table 1). All trialsdetected the signal from the balloon containing the radioactivematerial, and 37 of 40 trials were successful in locating the bal-loon in zone I and 36 in zone III. Therefore, sensitivity was100%, and specificity was 92.5% in zone I and 90% in zone III.Overall, sensitivity and specificity for balloon localization were100% and 91%. The predicted distance was 29.57 ± 5.37 cm,and the actual distance was 30.03 ± 5.30 cm in zone I, whilethe predicted distance was 23.18 ± 5.91 cm and the actual dis-tance was 24.61 ± 5.78 cm in zone III.
When the two operators were compared, both operatorshad 100% sensitivity, while operator 1 had 90% specificity (36successes in 40 trials) and operator 2 had 92.5% specificity(37 successes in 40 trials) for correct balloon localization. Therewas no significant difference in locating the balloon between thetwo operators (Table 2). For operator 1, the predicted distancewas25.43 ± 6.32 cm and the actual distance was 26.32 ± 5.55 cm;thus, the difference between predicted and actual balloon locationwas 1.71 ± 1.43 cm. For operator 2, the predicted distance was27.32 ± 6.54 cm, and the actual distance was 28.32 ± 6.61 cm;thus, the difference between predicted and actual balloon locationwas 1.25 ± 1.06 cm. The difference between predicted and actualballoon location was higher for operator 1 than for operator 2,but there was no difference between the two operators for bothzones I and III. The time taken to explore the balloon locationwas longer for operator 1 than for operator 2 in both zones Iand III, but the differences did not reach statistical significance.
Animal Study ResultsEach operator performed 10 trials in the swine (Table 3).
Sensitivity and specificity for balloon localization in the swinewere 100% for both operators. The difference between the pre-dicted and actual locations, the time taken to perform the trials,and the gamma-ray counts did not significantly differ betweenthe two operators. The level of console-emitted noise at theoperator's location was 82.50 ± 4.54 dB, and did not signifi-cantly differ between the two operators. A skin color change, in-dicative of acute radiation toxicity, was not detected in the swine.The effective dose recorded by the electronic personal dosimeterafter 10 trials was 0 μSv in both operators.
DISCUSSION
The human vasculature phantom study demonstrated thatthe gamma probe-guided method may be useful for the explora-tion of balloon location of REBOA, and the large animal study
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
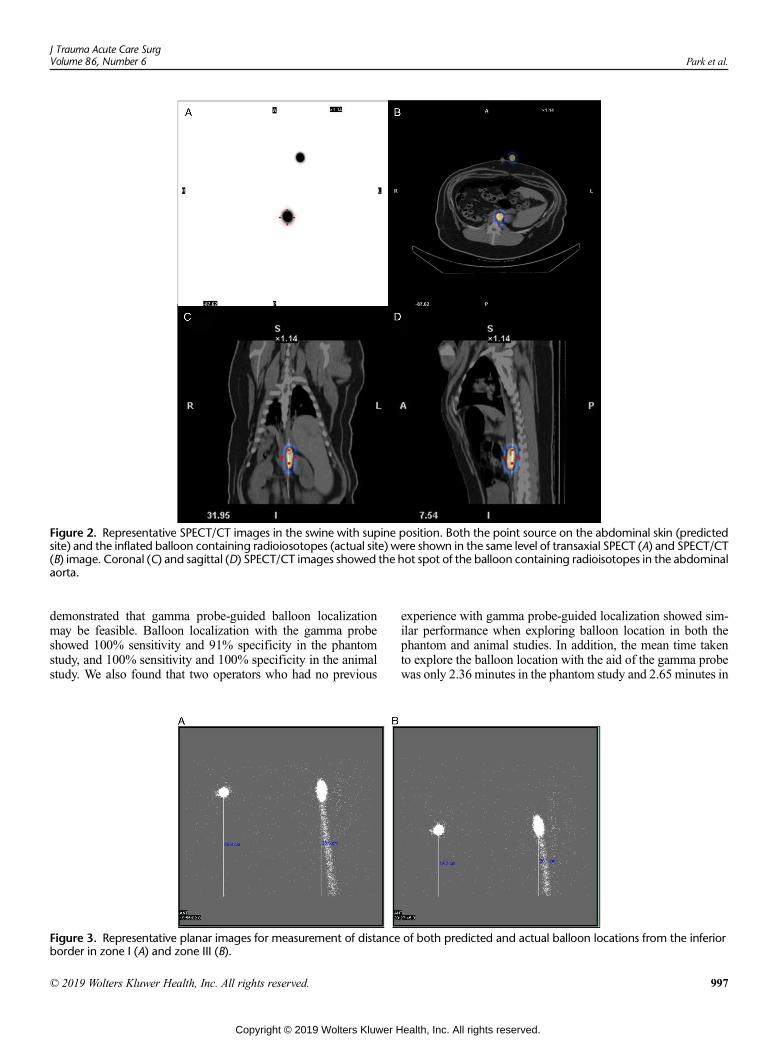
Figure 2. Representative SPECT/CT images in the swine with supine position. Both the point source on the abdominal skin (predictedsite) and the inflated balloon containing radioiosotopes (actual site) were shown in the same level of transaxial SPECT (A) and SPECT/CT(B) image. Coronal (C) and sagittal (D) SPECT/CT images showed the hot spot of the balloon containing radioisotopes in the abdominalaorta.
J Trauma Acute Care SurgVolume 86, Number 6 Park et al.
demonstrated that gamma probe-guided balloon localizationmay be feasible. Balloon localization with the gamma probeshowed 100% sensitivity and 91% specificity in the phantomstudy, and 100% sensitivity and 100% specificity in the animalstudy. We also found that two operators who had no previous
Figure 3. Representative planar images for measurement of distanceborder in zone I (A) and zone III (B).
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
experience with gamma probe-guided localization showed sim-ilar performance when exploring balloon location in both thephantom and animal studies. In addition, the mean time takento explore the balloon location with the aid of the gamma probewas only 2.36 minutes in the phantom study and 2.65 minutes in
of both predicted and actual balloon locations from the inferior
997
ealth, Inc. All rights reserved.
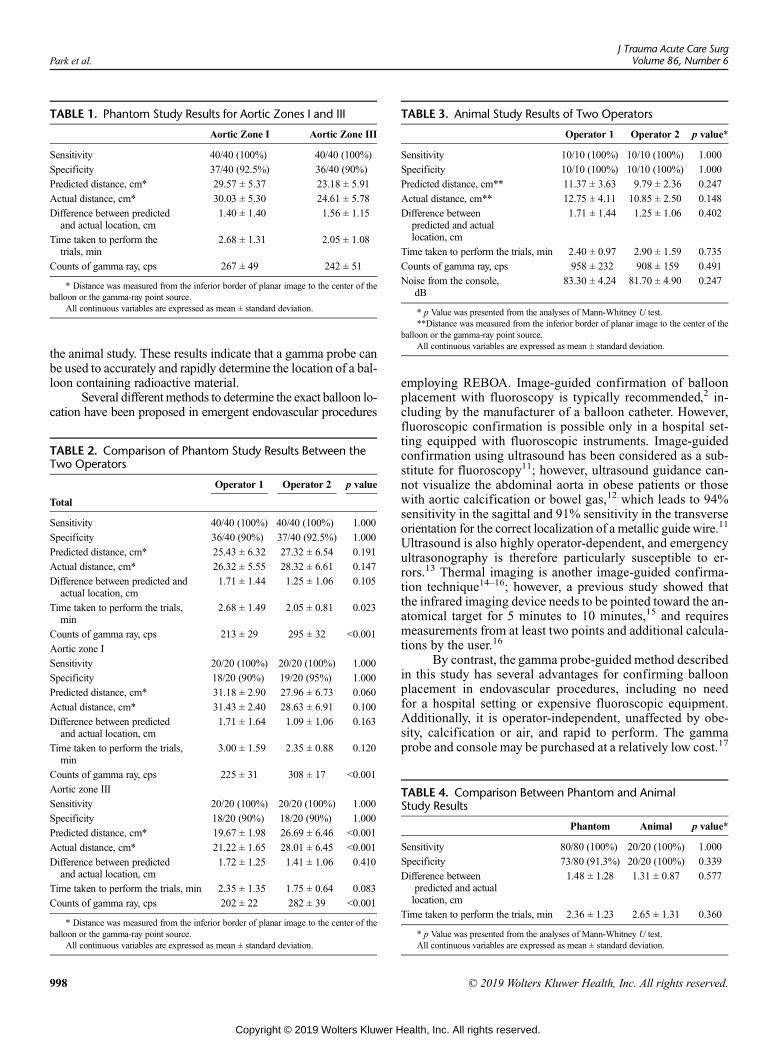
TABLE 1. Phantom Study Results for Aortic Zones I and III
Aortic Zone I Aortic Zone III
Sensitivity 40/40 (100%) 40/40 (100%)
Specificity 37/40 (92.5%) 36/40 (90%)
Predicted distance, cm* 29.57 ± 5.37 23.18 ± 5.91
Actual distance, cm* 30.03 ± 5.30 24.61 ± 5.78
Difference between predictedand actual location, cm
1.40 ± 1.40 1.56 ± 1.15
Time taken to perform thetrials, min
2.68 ± 1.31 2.05 ± 1.08
Counts of gamma ray, cps 267 ± 49 242 ± 51
* Distance was measured from the inferior border of planar image to the center of theballoon or the gamma-ray point source.
All continuous variables are expressed as mean ± standard deviation.
TABLE 3. Animal Study Results of Two Operators
Operator 1 Operator 2 p value*
Sensitivity 10/10 (100%) 10/10 (100%) 1.000
Specificity 10/10 (100%) 10/10 (100%) 1.000
Predicted distance, cm** 11.37 ± 3.63 9.79 ± 2.36 0.247
Actual distance, cm** 12.75 ± 4.11 10.85 ± 2.50 0.148
Difference betweenpredicted and actuallocation, cm
1.71 ± 1.44 1.25 ± 1.06 0.402
Time taken to perform the trials, min 2.40 ± 0.97 2.90 ± 1.59 0.735
Counts of gamma ray, cps 958 ± 232 908 ± 159 0.491
Noise from the console,dB
83.30 ± 4.24 81.70 ± 4.90 0.247
* p Value was presented from the analyses of Mann-Whitney U test.**Distance was measured from the inferior border of planar image to the center of the
balloon or the gamma-ray point source.All continuous variables are expressed as mean ± standard deviation.
Park et al.J Trauma Acute Care Surg
Volume 86, Number 6
the animal study. These results indicate that a gamma probe canbe used to accurately and rapidly determine the location of a bal-loon containing radioactive material.
Several different methods to determine the exact balloon lo-cation have been proposed in emergent endovascular procedures
TABLE 2. Comparison of Phantom Study Results Between theTwo Operators
Operator 1 Operator 2 p value
Total
Sensitivity 40/40 (100%) 40/40 (100%) 1.000
Specificity 36/40 (90%) 37/40 (92.5%) 1.000
Predicted distance, cm* 25.43 ± 6.32 27.32 ± 6.54 0.191
Actual distance, cm* 26.32 ± 5.55 28.32 ± 6.61 0.147
Difference between predicted andactual location, cm
1.71 ± 1.44 1.25 ± 1.06 0.105
Time taken to perform the trials,min
2.68 ± 1.49 2.05 ± 0.81 0.023
Counts of gamma ray, cps 213 ± 29 295 ± 32 <0.001
Aortic zone I
Sensitivity 20/20 (100%) 20/20 (100%) 1.000
Specificity 18/20 (90%) 19/20 (95%) 1.000
Predicted distance, cm* 31.18 ± 2.90 27.96 ± 6.73 0.060
Actual distance, cm* 31.43 ± 2.40 28.63 ± 6.91 0.100
Difference between predictedand actual location, cm
1.71 ± 1.64 1.09 ± 1.06 0.163
Time taken to perform the trials,min
3.00 ± 1.59 2.35 ± 0.88 0.120
Counts of gamma ray, cps 225 ± 31 308 ± 17 <0.001
Aortic zone III
Sensitivity 20/20 (100%) 20/20 (100%) 1.000
Specificity 18/20 (90%) 18/20 (90%) 1.000
Predicted distance, cm* 19.67 ± 1.98 26.69 ± 6.46 <0.001
Actual distance, cm* 21.22 ± 1.65 28.01 ± 6.45 <0.001
Difference between predictedand actual location, cm
1.72 ± 1.25 1.41 ± 1.06 0.410
Time taken to perform the trials, min 2.35 ± 1.35 1.75 ± 0.64 0.083
Counts of gamma ray, cps 202 ± 22 282 ± 39 <0.001
* Distance was measured from the inferior border of planar image to the center of theballoon or the gamma-ray point source.
All continuous variables are expressed as mean ± standard deviation.
998
Copyright © 2019 Wolters Kluwer H
employing REBOA. Image-guided confirmation of balloonplacement with fluoroscopy is typically recommended,2 in-cluding by the manufacturer of a balloon catheter. However,fluoroscopic confirmation is possible only in a hospital set-ting equipped with fluoroscopic instruments. Image-guidedconfirmation using ultrasound has been considered as a sub-stitute for fluoroscopy11; however, ultrasound guidance can-not visualize the abdominal aorta in obese patients or thosewith aortic calcification or bowel gas,12 which leads to 94%sensitivity in the sagittal and 91% sensitivity in the transverseorientation for the correct localization of a metallic guidewire.11
Ultrasound is also highly operator-dependent, and emergencyultrasonography is therefore particularly susceptible to er-rors.13 Thermal imaging is another image-guided confirma-tion technique14–16; however, a previous study showed thatthe infrared imaging device needs to be pointed toward the an-atomical target for 5 minutes to 10 minutes,15 and requiresmeasurements from at least two points and additional calcula-tions by the user.16
By contrast, the gamma probe-guided method describedin this study has several advantages for confirming balloonplacement in endovascular procedures, including no needfor a hospital setting or expensive fluoroscopic equipment.Additionally, it is operator-independent, unaffected by obe-sity, calcification or air, and rapid to perform. The gammaprobe and console may be purchased at a relatively low cost.17
TABLE 4. Comparison Between Phantom and AnimalStudy Results
Phantom Animal p value*
Sensitivity 80/80 (100%) 20/20 (100%) 1.000
Specificity 73/80 (91.3%) 20/20 (100%) 0.339
Difference betweenpredicted and actuallocation, cm
1.48 ± 1.28 1.31 ± 0.87 0.577
Time taken to perform the trials, min 2.36 ± 1.23 2.65 ± 1.31 0.360
* p Value was presented from the analyses of Mann-Whitney U test.All continuous variables are expressed as mean ± standard deviation.
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 6 Park et al.
The startup costs for a gamma probe system range from ap-proximately US $20,000 in 200918 to 50,000 Canadian dol-lars inn 2016.19 However, the price of a radiographic systemranges from US $415,000 to US $1,150,000 according tothe report for Core Medical Equipment of World Health Orga-nization 2011.20 Gamma probe systems are less expensivethan fluoroscopic systems. Moreover, a gamma probe systemis small and portable, and it may therefore also be used inprehospital settings where fluoroscopy is unavailable or inthe operating room to determine the balloon location whenthe balloon catheter is moved from the inflation site.
As shown in this study, this new method does not dependon the operator's technique or experience, because gammaprobes are easy to use,17 and no special technical skills are re-quired. The two operators who participated in this study eachhad 10 years' of experience as general surgeons, but had no ex-perience in handling a gamma probe. However, they quicklylearned how to use the probe, and the two operators showed nosignificant differences with respect to performance in locatingthe balloon or in the time taken to perform the trials in the phan-tom study. The animal study was performed after the phantomstudy. Therefore, both operators were already familiar with useof the gamma probe in the animal study and consequently bothhad an improved specificity of 100% (Table 4). This demon-strates that gamma probe-guidance is an easy-to-use methodand is unaffected by inter-operator variability. The gamma-probe guided technique is little influenced by the type ofREBOA, such as echogenic or radiopaque tip, unlike ultraso-nography, which is dependent on the REBOA catheter tip typeand is hampered by air and shrapnel.10
The gamma probe method also provides real-time infor-mation, unlike fluoroscopy or thermal imaging. An auditory sig-nal is emitted and a numerical value is displayed on the consolewhen the radioactive material in the balloon is detected, whichenables the balloon to be tracked in real time when the balloonis advanced into or withdrawn from the blood vessel. Thegamma probe console is sufficiently noisy and has the advantageof displaying the counts on the monitor, which means that sig-nals can still be detected in environments that are too noisy tohear console-emitted sounds. Although a radiofrequency devicecan track the balloon in real time, specificity to predict thelocation of the catheter tip ranges from 16% to 86% and a ra-diofrequency device only generates auditory signals withoutquantified numeric values.10 Moreover, if an imaging mo-dality, such as a handheld gamma camera, is combined withthe gamma probe, it would compensate for the lack of informa-tion on balloon shape, extent, and depth, as shown previously inthe case of the radiofrequency identification method.21 We planto study the use of imaging gamma probes in endovascularprocedures.
The novel gamma probe-guided localization method hassome limitations. First, the storage and preparation of radioiso-topes may be problematic. 99mTc has a short half-life of 6 hoursand therefore rapidly decays upon prolonged storage. However,the cost of 99mTc ranged from US $0.28 to US $0.45 per mCi(1 mCi is equivalent to about 37 MBq, which was the dose usedin this study) in 2008.22 Consequently, this radioisotope is af-fordable for use in ambulance and prehospital settings. 99mTccan be stored not only as the complete 99mTc form in individual
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
doses, but also as the incomplete 99Mo form, which is themother radionuclide of 99mTc in a technetium generator. Conver-sion of 99Mo, which has a half-life of 67 hours, to 99mTc whenrequired may be more economical if 99mTc is used infrequently.The process by which 99mTc is extracted from a commercialgenerator is simple and only takes about 1 minute. Therefore,even considering the decay of radioisotopes and inconvenienceof extracting 99mTc from a generator, the gamma probe-guidedmethod can be performed rapidly in a timeframe that may beapplicable to the trauma setting. Second, a gamma probe isan essential prerequisite for gamma probe-guided localization.Such probes are expensive, and there is an initial investment costfor installation of a gamma probe system in ambulance andprehospital settings. However, such systems are less expensivethan fluoroscopic equipment. Third, radiation exposure to med-ical staffs who handle radioactive materials should be consid-ered. Our results demonstrated that the effective dose of bothoperators after 10 trials was below the detection limit due tothe small dose of the radioisotope used and the short durationof exposure. Administration of 99mTc, which has a short half-life, in hospitals does not require isolation of patients.23 Expo-sure to this radioisotope is of less concern than exposure to otherradioisotopes. However, the very low level of radiation that med-ical staffs are exposed to is a potential limitation of gammaprobe systems in comparison with other methods that do notuse ionizing radiation. Some of these limitations are acceptableand surmountable; therefore, the novel gamma probe-guided lo-calization method is applicable in settings where minutes matter.Finally, the caution is needed for the applicability of this animalstudy to human tissue because the swine model is not the sameas the human anatomy, and the experimental animal has nointeracting factors that affect the cardiovascular system. Furtherhuman clinical trials are required to evaluate the performance ofthe gamma-probe guided localization method.
In conclusion, the gamma probe-guided balloon localiza-tion method showed excellent performance, operator indepen-dency, and rapidity, indicating that it could be a valid alternativeto existing image-based confirmation of catheter balloon place-ment, such as fluoroscopy. The results potentially open the pros-pect of fluoroscopy-free gamma probe-guided confirmation ofballoon location in the new age of catheter procedures.
AUTHORSHIP
Y.P. performed experiments, data interpretation, writing and criticalrevision. Y.G.J. performed experiments, data interpretation, and criti-cal revision. M.K. performed experiments and data interpretation.K.-H.C. performed literature searches, study design, data analysis, datainterpretation, critical revision. J.K. performed literature searches,study design, experiments, data analysis, data interpretation, writing,and critical revision.
ACKNOWLEDGMENT
We thank the animal studies for this article from professor Myung Ho Jeongand professor Doo Sun Sim (The Heart Research Center of Chonnam Na-tional University Hospital Designated by Korea Ministry of Health, Welfareand Family Affairs, Gwangju, Korea).
DISCLOSURE
This researchwas supported byNational Research Foundation of Korea (NRF)grants funded by the Korean government (NRF-2017M3A9E8023017) andby Chonnam National University Hospital Biomedical Research Institute
999
ealth, Inc. All rights reserved.

Park et al.J Trauma Acute Care Surg
Volume 86, Number 6
(BCRI18021). The funder had no role in study design, data collection or anal-ysis, decision to publish, or preparation of the article. Y.P. and J.K. declare acurrent patent related to the content of the article: Korean Patent ApplicationNo. 10-2018-0129274. And Y.G.J., M.K. and K.-H.C. declare no potentialconflict of interest.Ethical Approval: All animals received humane care. All procedures wereapproved by the Institutional Animal Care and Use Committee (IACUC)of Chonnam National University Hospital.Informed Consent: Requirement to obtain informed consent was waived.
REFERENCES1. Manzano-Nunez R, Orlas CP, Herrera-Escobar JP, Galvagno S, DuBose J,
Melendez JJ, Serna JJ, Salcedo A, Pena CA, Angamarca E, et al. A meta-analysis of the incidence of complications associated with groin access afterthe use of resuscitative endovascular balloon occlusion of the aorta in traumapatients. J Trauma Acute Care Surg. 2018;85(3):626–634.
2. Stannard A, Eliason JL, Rasmussen TE. Resuscitative endovascular balloonocclusion of the aorta (REBOA) as an adjunct for hemorrhagic shock. JTrauma. 2011;71(6):1869–1872.
3. Brenner ML, Moore LJ, DuBose JJ, Tyson GH, McNutt MK, Albarado RP,Holcomb JB, Scalea TM, Rasmussen TE. A clinical series of resuscitativeendovascular balloon occlusion of the aorta for hemorrhage control and re-suscitation. J Trauma Acute Care Surg. 2013;75(3):506–511.
4. Povoski SP, Neff RL, Mojzisik CM, O'Malley DM, Hinkle GH, Hall NC,Murrey DA Jr, Knopp MV, Martin EW Jr. A comprehensive overview ofradioguided surgery using gamma detection probe technology.World J SurgOncol. 2009;7:11.
5. Povoski SP, Young DC, Walker MJ, Carson WE, Yee LD, Agnese DM,Farrar WB. Re-emphasizing the concept of adequacy of intraoperative as-sessment of the axillary sentinel lymph nodes for identifying nodal positivityduring breast cancer surgery. World J Surg Oncol. 2007;5:18.
6. Kroon HM, Lowe L, Wong S, Fullen D, Su L, Cimmino V, Chang AE,Johnson T, Sabel MS. What is a sentinel node? Re-evaluating the 10% rulefor sentinel lymph node biopsy in melanoma. J Surg Oncol. 2007;95(8):623–628.
7. BilchikAJ, Nora DT, Sobin LH, Turner RR, Trocha S, Krasne D,Morton DL.Effect of lymphatic mapping on the new tumor-node-metastasis classifica-tion for colorectal cancer. J Clin Oncol. 2003;21(4):668–672.
8. RubelloD, PelizzoMR, Boni G, Schiavo R, Vaggelli L, Villa G, Sandrucci S,Piotto A, Manca G, Marini P, et al. Radioguided surgery of primary hyper-parathyroidism using the low-dose 99mTc-sestamibi protocol: multiinstitutionalexperience from the Italian study group on Radioguided surgery andImmunoscintigraphy (GISCRIS). J Nucl Med. 2005;46(2):220–226.
9. Pezy P, Flaris AN, Prat NJ, Cotton F, Lundberg PW, Caillot JL, David JS,Voiglio EJ. Fixed-distance model for balloon placement duringfluoroscopy-free resuscitative endovascular balloon occlusion of the aortain a civilian population. JAMA Surg. 2017;152(4):351–358.
10. Wessels LE, Wallace JD, Bowie J, Butler WJ, Spalding C, Krzyzaniak M.Radiofrequency identification of the ER-REBOA: confirmation of place-ment without fluoroscopy. Mil Med. 2018.
1000
Copyright © 2019 Wolters Kluwer H
11. Guliani S, Amendola M, Strife B, Morano G, Elbich J, Albuquerque F,Komorowski D, Sydnor M, Malhotra A, Levy M. Central aortic wire confir-mation for emergent endovascular procedures: as fast as surgeon-performedultrasound. J Trauma Acute Care Surg. 2015;79(4):549–554.
12. Chaudery M, Clark J, Morrison JJ, Wilson MH, Bew D, Darzi A. Cancontrast-enhanced ultrasonography improve zone III REBOA placementfor prehospital care? J Trauma Acute Care Surg. 2016;80(1):89–94.
13. Pinto A, Pinto F, Faggian A, Rubini G, Caranci F, Macarini L, Genovese EA,Brunese L. Sources of error in emergency ultrasonography. Crit UltrasoundJ. 2013;(5 Suppl 1):S1.
14. Barron MR, Kuckelman JP, McClellan JM, Derickson MJ, Phillips CJ,Marko ST, Smith JP, Eckert MJ, Martin MJ. Smartphone-based mobile ther-mal imaging technology to assess limb perfusion and tourniquet effective-ness under normal and blackout conditions. J Trauma Acute Care Surg.2017;83(6):1129–1135.
15. Barron MR, Kuckelman JP, McClellan JM, Derickson MJ, Phillips CJ,Marko ST, Sokol K, Eckert MJ, MartinMJ. Mobile forward-looking infraredtechnology allows rapid assessment of resuscitative endovascular balloon oc-clusion of the aorta in hemorrhage and blackout conditions. J Trauma AcuteCare Surg. 2018;85(1):25–32.
16. Sokol KK, Black GE, Willey SB, Kniery K, Marko ST, Eckert MJ,Martin MJ. There's an app for that: a handheld smartphone-based infraredimaging device to assess adequacy and level of aortic occlusion duringREBOA. J Trauma Acute Care Surg. 2017;82(1):102–108.
17. FujisawaY, Nakamura Y, Kawachi Y, Otsuka F. A custom-made, low-cost in-traoperative fluorescence navigation system with indocyanine green for sen-tinel lymph node biopsy in skin cancer.Dermatology. 2011;222(3):261–268.
18. Troyan SL, Kianzad V, Gibbs-Strauss SL, Gioux S, Matsui A, Oketokoun R,Ngo L, Khamene A, Azar F, Frangioni JV. The FLARE intraoperative near-infrared fluorescence imaging system: a first-in-human clinical trial in breastcancer sentinel lymph node mapping. Ann Surg Oncol. 2009;16(10):2943–2952.
19. Zhang Y, Seely J, Cordeiro E, Hefler J, Thavorn K, Mahajan M, Domina S,Aro J, Ibrahim AM, Arnaout A, et al. Radioactive seed localization versuswire-guided localization for nonpalpable breast cancer: a cost and operatingroom efficiency analysis. Ann Surg Oncol. 2017;24(12):3567–3573.
20. World Health Organization. Core medical equipment 2011. http://apps.who.int/iris/bitstream/handle/10665/95788/WHO_HSS_EHT_DIM_11.03_eng.pdf?sequence=1&isAllowed=y. Published 2011. Accessed Dec 21, 2018.
21. Bugby SL, Lees JE, Perkins AC. Hybrid intraoperative imaging techniquesin radioguided surgery: present clinical applications and future outlook. ClinTransl Imaging. 2017;5(4):323–341.
22. National Research Council (US) Committee on Medical Isotope ProductionWithout Highly Enriched Uranium. Medical Isotope Production withoutHighly Enriched Uranium. Washington (DC): National Academies Press(US); 2009: 6, Molybdenum-99/Technetium-99m Production Costs.Available from: https://www.ncbi.nlm.nih.gov/books/NBK215132/. AccessedDec 27, 2018.
23. International Commission on Radiological Protection. Release of patients af-ter therapy with unsealed radionuclides. Ann ICRP. 2004;34(2):v–vi, 1-79.
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
ORIGINAL ARTICLE
Obesity as protective against, rather than a risk factor for,postoperative Clostridium difficile infection: A nationwideretrospective analysis of 1,426,807 surgical patients
Karien Meier, MSc, Ask T. Nordestgaard, BSc, Ahmed I. Eid, MD, Napaporn Kongkaewpaisan, MD,Jae M. Lee, BA, Manansun Kongwibulwut, MD, Kelsey R. Han, AB, Nikolaos Kokoroskos, MD,
April E. Mendoza, MD, MPH, Noelle Saillant, MD, David R. King, MD, George C. Velmahos, MD, PhD,and Haytham M.A. Kaafarani, MD, MPH, Boston, Massachusetts
AAST Continuing Medical Education Article
Accreditation StatementThis activity has been planned and implemented in accordance with the Essential Areasand Policies of the Accreditation Council for Continuing Medical Education throughthe joint providership of the American College of Surgeons and the American Associationfor the Surgery of Trauma. The American College Surgeons is accredited by theACCME to provide continuing medical education for physicians.
AMA PRA Category 1 Credits™The American College of Surgeons designates this journal-based CME activity fora maximum of 1 AMA PRACategory 1 Credit™. Physicians should claim only the creditcommensurate with the extent of their participation in the activity.
Of the AMA PRACategory 1 Credit™ listed above, a maximum of 1 credit meetsthe requirements for self-assessment.
Credits can only be claimed online
ObjectivesAfter reading the featured articles published in the Journal of Trauma and AcuteCare Surgery, participants should be able to demonstrate increased understandingof the material specific to the article. Objectives for each article are featured atthe beginning of each article and online. Test questions are at the end of the article,with a critique and specific location in the article referencing the question topic.
Claiming CreditTo claim credit, please visit the AAST website at http://www.aast.org/ and click onthe “e-Learning/MOC” tab. You must read the article, successfully complete thepost-test and evaluation. Your CME certificate will be available immediately uponreceiving a passing score of 75% or higher on the post-test. Post-tests receiving a scoreof below 75% will require a retake of the test to receive credit.
System RequirementsThe system requirements are as follows: Adobe® Reader 7.0 or above installed; Internet Explorer® 7 and above; Firefox® 3.0 and above, Chrome® 8.0 and above, or
Safari™ 4.0 and above.
QuestionsIf you have any questions, please contact AAST at 800-789-4006. Paper test and evaluations will not be accepted.
Disclosure InformationIn accordance with the ACCME Accreditation Criteria, the American College of
Surgeons, as the accredited provider of this journal activity, must ensure that anyone
in a position to control the content of J Trauma Acute Care Surg articles selected for
CME credit has disclosed all relevant financial relationships with any commercial
interest. Disclosure forms are completed by the editorial staff, associate editors,
reviewers, and all authors. The ACCME defines a `commercial interest' as “any
entity producing, marketing, re-selling, or distributing health care goods or services
consumed by, or used on, patients.” “Relevant” financial relationships are those (in
any amount) that may create a conflict of interest and occur within the 12’months
preceding and during the time that the individual is engaged in writing the article. All
reported conflicts are thoroughly managed in order to ensure any potential bias
within the content is eliminated. However, if you’perceive a bias within the article,
please report the circumstances on the evaluation form.
Please note we have advised the authors that it is their responsibility to disclose within
the article if they are describing the use of a device, product, or drug that is not FDA
approved or the off-label use of an approved device, product, or drug or unapproved usage.
Disclosures of Significant Relationships withRelevant Commercial Companies/Organizationsby the Editorial StaffErnest E. Moore, Editor: PI, research support and shared U.S. patents Haemonetics;
PI, research support, Instrumentation Laboratory, Inc.; Co-founder, Thrombo Thera-
peutics. Associate Editors David Hoyt, Ronald V. Maier and Steven Shackford have
nothing to disclose. Editorial staff and Angela Sauaia have nothing to disclose.
Author DisclosuresThe authors have nothing to disclose.
Reviewer DisclosuresThe reviewers have nothing to disclose.
CostFor AAST members and Journal of Trauma and Acute Care Surgery subscribersthere is no charge to participate in this activity. For those who are not a memberor subscriber, the cost for each credit is $25.
J Trauma Acute Care SurgVolume 86, Number 6 1001
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.

Sub
Fro
Ad
Wi
Wi
Pos
Sup
DO
Meier et al.J Trauma Acute Care Surg
Volume 86, Number 6
10
BACKGROUND: R
mitted: January 17, 2019, RevisPublished online: March 11, 20m the Division of Trauma, Emerment of Surgery (K.M., A.T.N.,N.S., D.R.K., G.C.V., H.M.A.K.School, Boston,Massachusetts,versityMedical Center, Leiden Uaesthesia (A.T.N.), Centre of HeCopenhagen, Denmark.dress for reprints: Haytham M.ASurgery and Surgical Critical CaStreet, Suite 810, Boston, MA 0nner of the Massachusetts ComCompetition (oral presentation,nner of the Region 1 COT ResidDecember 2018).ter of Distinction at the 65th Anthe American College of Surgeplemental digital content is avaithe printed text, and links to thearticle on the journal’s Web sit
I: 10.1097/TA.00000000000022
02
ecent studies suggest that obesity is a risk factor for Clostridium difficile infection, possibly due to disruptions in the intestinalmicrobiome composition. We hypothesized that body mass index (BMI) is associated with increased incidence of C. difficile in-fection in surgical patients.
METHODS: I
n this nationwide retrospective cohort study in 680 American College of Surgeons National Surgical Quality Improvement Pro-gram participating sites across the United States, the occurrence of C. difficile infection within 30 days postoperatively betweendifferent BMI groups was compared. All American College of Surgeons National Surgical Quality Improvement Program patientsbetween 2015 and 2016 were classified as underweight, normal-weight, overweight, or obese class I-III if their BMI was less than18.5, 18.5 to 25, 25 to 30, 30 to 35, 35 to 40 or greater than 40, respectively.RESULTS: A
total of 1,426,807 patients were included; median agewas 58 years, 43.4%weremale, and 82.9%were white. The postoperativeincidence of C. difficile infection was 0.42% overall: 1.11%, 0.56%, 0.39%, 0.35%, 0.33% and 0.36% from the lowest to thehighest BMI group, respectively (p < 0.001 for trend). In univariate then multivariable logistic regression analyses, adjusting forpatient demographics (e.g., age, sex), comorbidities (e.g., diabetes, systemic sepsis, immunosuppression), preoperative laboratoryvalues (e.g., albumin, white blood cell count), procedure complexity (work relative unit as a proxy) and procedure characteristics(e.g., emergency, type of surgery [general, vascular, other]), compared with patientswith normal BMI, high BMI was inversely andincrementally correlated with the postoperative occurrence of C. difficile infection. The underweight were at increased risk (oddsratio, 1.15 [1.00–1.32]) while the class III obese were at the lowest risk (odds ratio, 0.73 [0.65–0.81]).CONCLUSION: I
n this nationwide retrospective cohort study, obesity is independently and in a stepwise fashion associated with a decreased risk ofpostoperative C. difficile infection. Further studies are warranted to explore the potential and unexpected association. (J TraumaAcute Care Surg. 2019;86: 1001–1009. Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.)LEVEL OF EVIDENCE: P
rognostic/Epidemiologic, Level IV. KEYWORDS: O besity; Clostridium difficile infection; ACS-NSQIP.T he incidence, severity, and lethality of Clostridium difficileinfection (CDI) continue to increase among hospitalized pa-
tients in developed nations.1–7 The incidence of CDI in theUnited States nearly doubled from 4.5 cases to 8.2 per 1000 patientsbetween 2001 and 2010, while its associated mortality increasedfrom 6.6% to 7.2% in the same time period.5 Patient risk factors(e.g., advanced age, comorbidities, immunosuppression), alter-ations in the intestinal microbiome (e.g., antibiotic use, surgery,chemotherapy) and exposure to bacterial spores (e.g., by hospi-talization) all increase the risk of intestinal CDI.8
Among patient risk factors, both obesity and underweightare often found to be risk factors for infections, mortality, andhospitalization.9–11 In surgical patients specifically, obesity isassociated with increased perioperative morbidity as well as in-fectious complications such as urinary tract infection and surgi-cal site infections.12,13 It is hypothesized that excess adiposetissue initiates and propagates a series of metabolic changes
ed: February 15, 2019, Accepted: March 2, 2019,19.gency Surgery, and Surgical Critical Care, Depart-A.I.E., N.K., J.M.L.,M.K., K.R.H., N.K., A.E.M.,), Massachusetts General Hospital, HarvardMedicalDepartment of Trauma Surgery (K.M.), LeidenUni-niversity, The Netherlands; and Department of An-ad and Orthopaedics, Rigshospitalet, University of
. Kaafarani, MD, Division of Trauma, Emergencyre,Massachusetts General Hospital, 165 Cambridge2114; email: [email protected] on Trauma (COT) Resident Trauma PaperNovember 2018).ent Trauma Paper Competition (oral presentation,
nual Meeting during the Massachusetts Chapter ofons (December 2018).lable for this article. Direct URL citations appear indigital files are provided in the HTML text of thise (www.jtrauma.com).
49
Copyright © 2019 Wolters Kluwer H
and hormonal alterations, increases production of inflammatorycytokines (e.g., leptin), leading to a chronic low-grade state ofinflammation as well as decreased immune cell function.14,15
In addition, obesity alters the composition of the intestinalmicrobiome, resulting in fewer bacteroidetes and potential path-ogenic firmicutes, proteobacteria, and actinobacteria.16,17
Currently, more than a third of the United States adult pop-ulation is obese.18 The United States surgical population reflectsthese biometric shifts, and the inherent risks of increased nosocomialinfections due to an altered immune response.More recently, obesitywas suggested as a potential risk factor for both community-acquiredand hospital-onset CDI. Three small retrospective studies have sug-gested that obesity is associatedwith an increased susceptibility toCDI.19–21 However, other similar studies have failed to demon-strate a relationship between obesity and CDI.22,23
In this study, we sought to test the relationship betweenbody mass index (BMI) and the incidence of postoperative CDIin surgical patients. We hypothesized that both the obese andthe underweight surgical patient is most susceptible to postsurgi-cal intestinal CDI.
METHODS
Design and SettingThis is a nationwide population-based cohort study, using
the American College of Surgeons National Surgical QualityImprovement Program (ACS-NSQIP) database that contains in-formation on surgical patients from up to 680 participating sitesacross the United States. The study was approved and granted“exempted” status by our institutional review board.
PatientsAll surgical cases from the ACS-NSQIP 2015 to 2016 da-
tabase with available information on age, sex, BMI, CDI status,and surgical specialty were included. The data on postoperativeCDI were not routinely collected by ACS-NSQIP prior to thethird quarter of 2015.
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
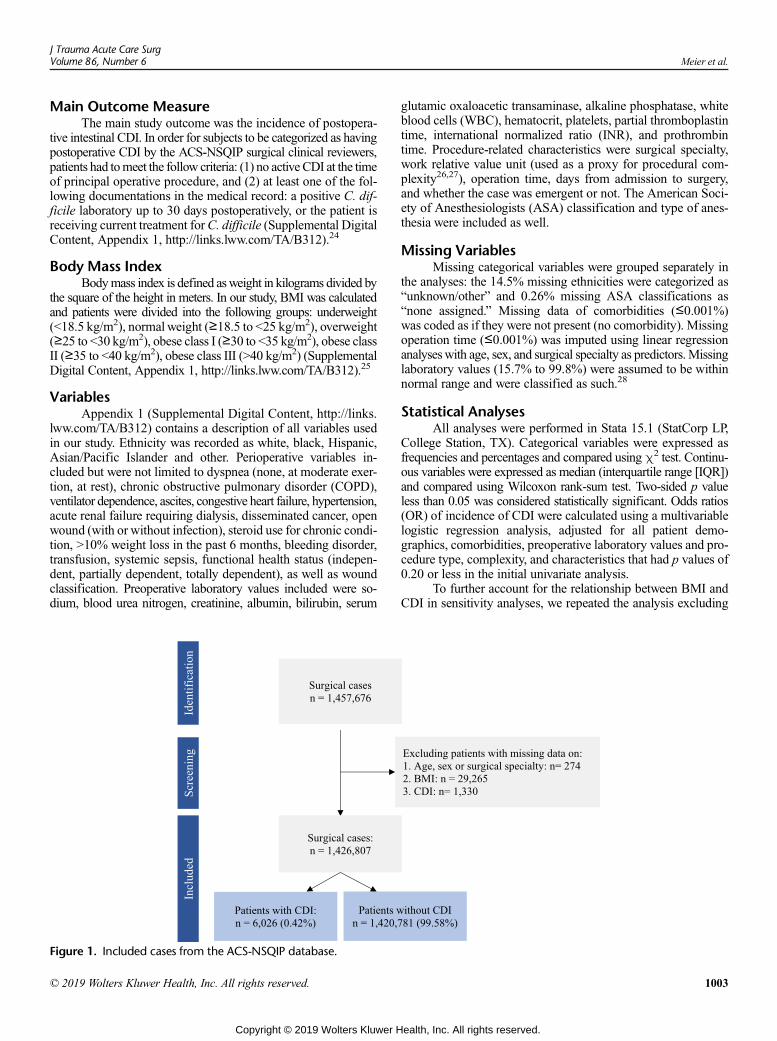
J Trauma Acute Care SurgVolume 86, Number 6 Meier et al.
Main Outcome MeasureThe main study outcome was the incidence of postopera-
tive intestinal CDI. In order for subjects to be categorized as havingpostoperative CDI by the ACS-NSQIP surgical clinical reviewers,patients had tomeet the follow criteria: (1) no active CDI at the timeof principal operative procedure, and (2) at least one of the fol-lowing documentations in the medical record: a positive C. dif-ficile laboratory up to 30 days postoperatively, or the patient isreceiving current treatment forC. difficile (Supplemental DigitalContent, Appendix 1, http://links.lww.com/TA/B312).24
Body Mass IndexBodymass index is defined asweight in kilograms divided by
the square of the height in meters. In our study, BMI was calculatedand patients were divided into the following groups: underweight(<18.5 kg/m2), normalweight (≥18.5 to <25 kg/m2), overweight(≥25 to <30 kg/m2), obese class I (≥30 to <35 kg/m2), obese classII (≥35 to <40 kg/m2), obese class III (>40 kg/m2) (SupplementalDigital Content, Appendix 1, http://links.lww.com/TA/B312).25
VariablesAppendix 1 (Supplemental Digital Content, http://links.
lww.com/TA/B312) contains a description of all variables usedin our study. Ethnicity was recorded as white, black, Hispanic,Asian/Pacific Islander and other. Perioperative variables in-cluded but were not limited to dyspnea (none, at moderate exer-tion, at rest), chronic obstructive pulmonary disorder (COPD),ventilator dependence, ascites, congestive heart failure, hypertension,acute renal failure requiring dialysis, disseminated cancer, openwound (with or without infection), steroid use for chronic condi-tion, >10% weight loss in the past 6 months, bleeding disorder,transfusion, systemic sepsis, functional health status (indepen-dent, partially dependent, totally dependent), as well as woundclassification. Preoperative laboratory values included were so-dium, blood urea nitrogen, creatinine, albumin, bilirubin, serum
Figure 1. Included cases from the ACS-NSQIP database.
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
glutamic oxaloacetic transaminase, alkaline phosphatase, whiteblood cells (WBC), hematocrit, platelets, partial thromboplastintime, international normalized ratio (INR), and prothrombintime. Procedure-related characteristics were surgical specialty,work relative value unit (used as a proxy for procedural com-plexity26,27), operation time, days from admission to surgery,and whether the case was emergent or not. The American Soci-ety of Anesthesiologists (ASA) classification and type of anes-thesia were included as well.
Missing VariablesMissing categorical variables were grouped separately in
the analyses: the 14.5% missing ethnicities were categorized as“unknown/other” and 0.26% missing ASA classifications as“none assigned.” Missing data of comorbidities (≤0.001%)was coded as if they were not present (no comorbidity). Missingoperation time (≤0.001%) was imputed using linear regressionanalyseswith age, sex, and surgical specialty as predictors.Missinglaboratory values (15.7% to 99.8%) were assumed to be withinnormal range and were classified as such.28
Statistical AnalysesAll analyses were performed in Stata 15.1 (StatCorp LP,
College Station, TX). Categorical variables were expressed asfrequencies and percentages and compared usingχ2 test. Continu-ous variables were expressed as median (interquartile range [IQR])and compared using Wilcoxon rank-sum test. Two-sided p valueless than 0.05 was considered statistically significant. Odds ratios(OR) of incidence of CDI were calculated using a multivariablelogistic regression analysis, adjusted for all patient demo-graphics, comorbidities, preoperative laboratory values and pro-cedure type, complexity, and characteristics that had p values of0.20 or less in the initial univariate analysis.
To further account for the relationship between BMI andCDI in sensitivity analyses, we repeated the analysis excluding
1003
ealth, Inc. All rights reserved.
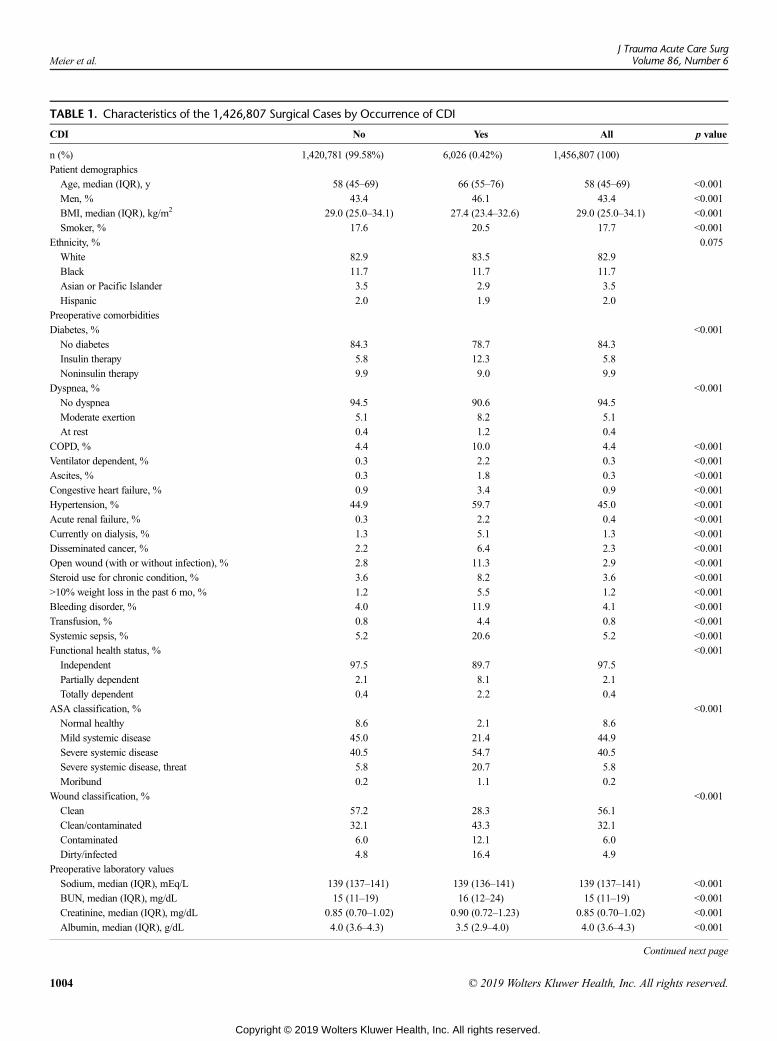
TABLE 1. Characteristics of the 1,426,807 Surgical Cases by Occurrence of CDI
CDI No Yes All p value
n (%) 1,420,781 (99.58%) 6,026 (0.42%) 1,456,807 (100)
Patient demographics
Age, median (IQR), y 58 (45–69) 66 (55–76) 58 (45–69) <0.001
Men, % 43.4 46.1 43.4 <0.001
BMI, median (IQR), kg/m2 29.0 (25.0–34.1) 27.4 (23.4–32.6) 29.0 (25.0–34.1) <0.001
Smoker, % 17.6 20.5 17.7 <0.001
Ethnicity, % 0.075
White 82.9 83.5 82.9
Black 11.7 11.7 11.7
Asian or Pacific Islander 3.5 2.9 3.5
Hispanic 2.0 1.9 2.0
Preoperative comorbidities
Diabetes, % <0.001
No diabetes 84.3 78.7 84.3
Insulin therapy 5.8 12.3 5.8
Noninsulin therapy 9.9 9.0 9.9
Dyspnea, % <0.001
No dyspnea 94.5 90.6 94.5
Moderate exertion 5.1 8.2 5.1
At rest 0.4 1.2 0.4
COPD, % 4.4 10.0 4.4 <0.001
Ventilator dependent, % 0.3 2.2 0.3 <0.001
Ascites, % 0.3 1.8 0.3 <0.001
Congestive heart failure, % 0.9 3.4 0.9 <0.001
Hypertension, % 44.9 59.7 45.0 <0.001
Acute renal failure, % 0.3 2.2 0.4 <0.001
Currently on dialysis, % 1.3 5.1 1.3 <0.001
Disseminated cancer, % 2.2 6.4 2.3 <0.001
Open wound (with or without infection), % 2.8 11.3 2.9 <0.001
Steroid use for chronic condition, % 3.6 8.2 3.6 <0.001
>10% weight loss in the past 6 mo, % 1.2 5.5 1.2 <0.001
Bleeding disorder, % 4.0 11.9 4.1 <0.001
Transfusion, % 0.8 4.4 0.8 <0.001
Systemic sepsis, % 5.2 20.6 5.2 <0.001
Functional health status, % <0.001
Independent 97.5 89.7 97.5
Partially dependent 2.1 8.1 2.1
Totally dependent 0.4 2.2 0.4
ASA classification, % <0.001
Normal healthy 8.6 2.1 8.6
Mild systemic disease 45.0 21.4 44.9
Severe systemic disease 40.5 54.7 40.5
Severe systemic disease, threat 5.8 20.7 5.8
Moribund 0.2 1.1 0.2
Wound classification, % <0.001
Clean 57.2 28.3 56.1
Clean/contaminated 32.1 43.3 32.1
Contaminated 6.0 12.1 6.0
Dirty/infected 4.8 16.4 4.9
Preoperative laboratory values
Sodium, median (IQR), mEq/L 139 (137–141) 139 (136–141) 139 (137–141) <0.001
BUN, median (IQR), mg/dL 15 (11–19) 16 (12–24) 15 (11–19) <0.001
Creatinine, median (IQR), mg/dL 0.85 (0.70–1.02) 0.90 (0.72–1.23) 0.85 (0.70–1.02) <0.001
Albumin, median (IQR), g/dL 4.0 (3.6–4.3) 3.5 (2.9–4.0) 4.0 (3.6–4.3) <0.001
Continued next page
Meier et al.J Trauma Acute Care Surg
Volume 86, Number 6
1004 © 2019 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
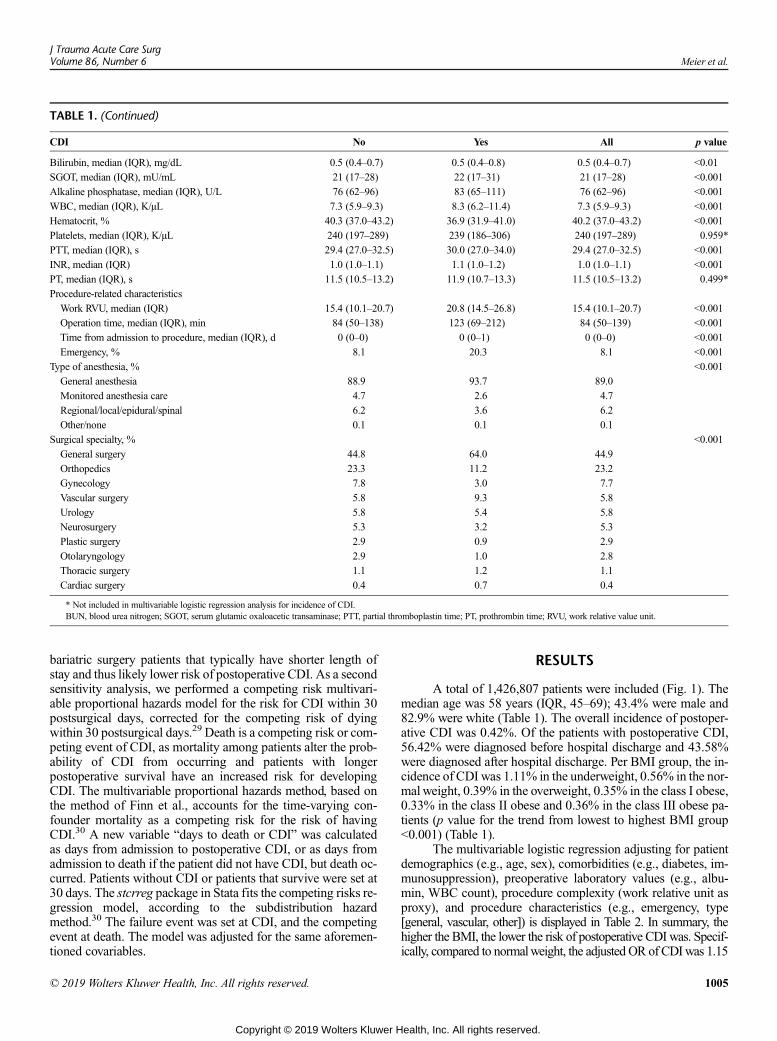
TABLE 1. (Continued)
CDI No Yes All p value
Bilirubin, median (IQR), mg/dL 0.5 (0.4–0.7) 0.5 (0.4–0.8) 0.5 (0.4–0.7) <0.01
SGOT, median (IQR), mU/mL 21 (17–28) 22 (17–31) 21 (17–28) <0.001
Alkaline phosphatase, median (IQR), U/L 76 (62–96) 83 (65–111) 76 (62–96) <0.001
WBC, median (IQR), K/μL 7.3 (5.9–9.3) 8.3 (6.2–11.4) 7.3 (5.9–9.3) <0.001
Hematocrit, % 40.3 (37.0–43.2) 36.9 (31.9–41.0) 40.2 (37.0–43.2) <0.001
Platelets, median (IQR), K/μL 240 (197–289) 239 (186–306) 240 (197–289) 0.959*
PTT, median (IQR), s 29.4 (27.0–32.5) 30.0 (27.0–34.0) 29.4 (27.0–32.5) <0.001
INR, median (IQR) 1.0 (1.0–1.1) 1.1 (1.0–1.2) 1.0 (1.0–1.1) <0.001
PT, median (IQR), s 11.5 (10.5–13.2) 11.9 (10.7–13.3) 11.5 (10.5–13.2) 0.499*
Procedure-related characteristics
Work RVU, median (IQR) 15.4 (10.1–20.7) 20.8 (14.5–26.8) 15.4 (10.1–20.7) <0.001
Operation time, median (IQR), min 84 (50–138) 123 (69–212) 84 (50–139) <0.001
Time from admission to procedure, median (IQR), d 0 (0–0) 0 (0–1) 0 (0–0) <0.001
Emergency, % 8.1 20.3 8.1 <0.001
Type of anesthesia, % <0.001
General anesthesia 88.9 93.7 89.0
Monitored anesthesia care 4.7 2.6 4.7
Regional/local/epidural/spinal 6.2 3.6 6.2
Other/none 0.1 0.1 0.1
Surgical specialty, % <0.001
General surgery 44.8 64.0 44.9
Orthopedics 23.3 11.2 23.2
Gynecology 7.8 3.0 7.7
Vascular surgery 5.8 9.3 5.8
Urology 5.8 5.4 5.8
Neurosurgery 5.3 3.2 5.3
Plastic surgery 2.9 0.9 2.9
Otolaryngology 2.9 1.0 2.8
Thoracic surgery 1.1 1.2 1.1
Cardiac surgery 0.4 0.7 0.4
* Not included in multivariable logistic regression analysis for incidence of CDI.BUN, blood urea nitrogen; SGOT, serum glutamic oxaloacetic transaminase; PTT, partial thromboplastin time; PT, prothrombin time; RVU, work relative value unit.
J Trauma Acute Care SurgVolume 86, Number 6 Meier et al.
bariatric surgery patients that typically have shorter length ofstay and thus likely lower risk of postoperative CDI. As a secondsensitivity analysis, we performed a competing risk multivari-able proportional hazards model for the risk for CDI within 30postsurgical days, corrected for the competing risk of dyingwithin 30 postsurgical days.29 Death is a competing risk or com-peting event of CDI, as mortality among patients alter the prob-ability of CDI from occurring and patients with longerpostoperative survival have an increased risk for developingCDI. The multivariable proportional hazards method, based onthe method of Finn et al., accounts for the time-varying con-founder mortality as a competing risk for the risk of havingCDI.30 A new variable “days to death or CDI” was calculatedas days from admission to postoperative CDI, or as days fromadmission to death if the patient did not have CDI, but death oc-curred. Patients without CDI or patients that survive were set at30 days. The stcrreg package in Stata fits the competing risks re-gression model, according to the subdistribution hazardmethod.30 The failure event was set at CDI, and the competingevent at death. The model was adjusted for the same aforemen-tioned covariables.
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
RESULTS
A total of 1,426,807 patients were included (Fig. 1). Themedian age was 58 years (IQR, 45–69); 43.4% were male and82.9% were white (Table 1). The overall incidence of postoper-ative CDI was 0.42%. Of the patients with postoperative CDI,56.42% were diagnosed before hospital discharge and 43.58%were diagnosed after hospital discharge. Per BMI group, the in-cidence of CDI was 1.11% in the underweight, 0.56% in the nor-mal weight, 0.39% in the overweight, 0.35% in the class I obese,0.33% in the class II obese and 0.36% in the class III obese pa-tients (p value for the trend from lowest to highest BMI group<0.001) (Table 1).
The multivariable logistic regression adjusting for patientdemographics (e.g., age, sex), comorbidities (e.g., diabetes, im-munosuppression), preoperative laboratory values (e.g., albu-min, WBC count), procedure complexity (work relative unit asproxy), and procedure characteristics (e.g., emergency, type[general, vascular, other]) is displayed in Table 2. In summary, thehigher the BMI, the lower the risk of postoperative CDI was. Specif-ically, compared to normalweight, the adjusted OR of CDIwas 1.15
1005
ealth, Inc. All rights reserved.
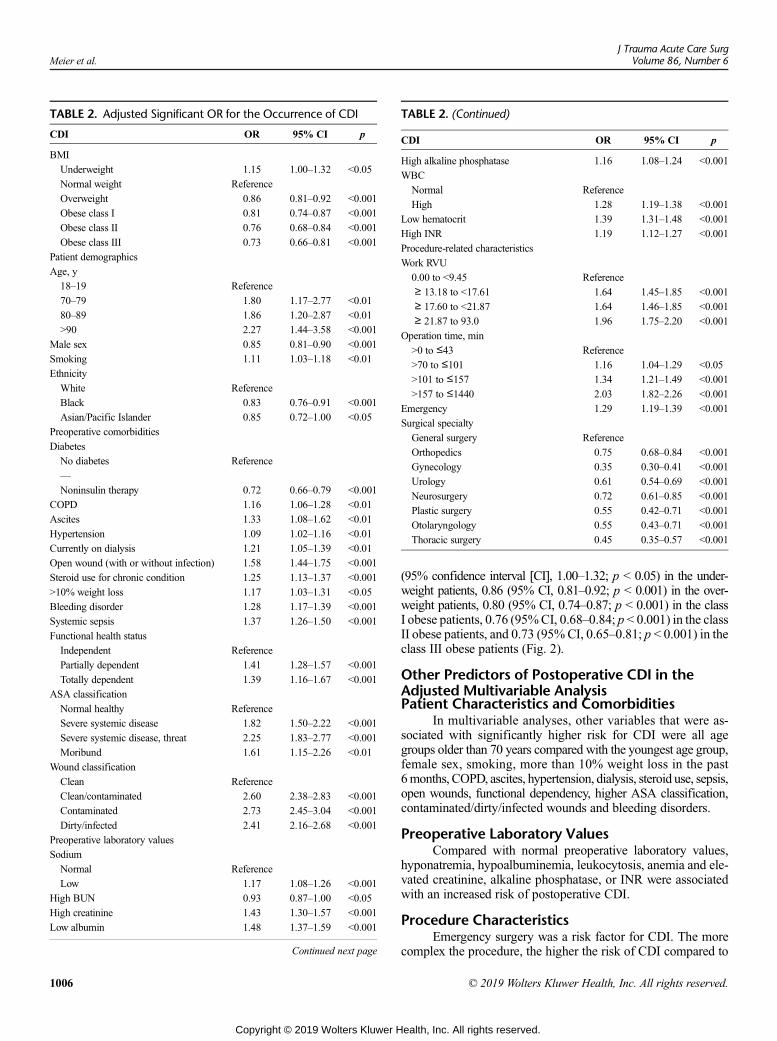
TABLE 2. Adjusted Significant OR for the Occurrence of CDI
CDI OR 95% CI p
BMI
Underweight 1.15 1.00–1.32 <0.05
Normal weight Reference
Overweight 0.86 0.81–0.92 <0.001
Obese class I 0.81 0.74–0.87 <0.001
Obese class II 0.76 0.68–0.84 <0.001
Obese class III 0.73 0.66–0.81 <0.001
Patient demographics
Age, y
18–19 Reference
70–79 1.80 1.17–2.77 <0.01
80–89 1.86 1.20–2.87 <0.01
>90 2.27 1.44–3.58 <0.001
Male sex 0.85 0.81–0.90 <0.001
Smoking 1.11 1.03–1.18 <0.01
Ethnicity
White Reference
Black 0.83 0.76–0.91 <0.001
Asian/Pacific Islander 0.85 0.72–1.00 <0.05
Preoperative comorbidities
Diabetes
No diabetes Reference
—
Noninsulin therapy 0.72 0.66–0.79 <0.001
COPD 1.16 1.06–1.28 <0.01
Ascites 1.33 1.08–1.62 <0.01
Hypertension 1.09 1.02–1.16 <0.01
Currently on dialysis 1.21 1.05–1.39 <0.01
Open wound (with or without infection) 1.58 1.44–1.75 <0.001
Steroid use for chronic condition 1.25 1.13–1.37 <0.001
>10% weight loss 1.17 1.03–1.31 <0.05
Bleeding disorder 1.28 1.17–1.39 <0.001
Systemic sepsis 1.37 1.26–1.50 <0.001
Functional health status
Independent Reference
Partially dependent 1.41 1.28–1.57 <0.001
Totally dependent 1.39 1.16–1.67 <0.001
ASA classification
Normal healthy Reference
Severe systemic disease 1.82 1.50–2.22 <0.001
Severe systemic disease, threat 2.25 1.83–2.77 <0.001
Moribund 1.61 1.15–2.26 <0.01
Wound classification
Clean Reference
Clean/contaminated 2.60 2.38–2.83 <0.001
Contaminated 2.73 2.45–3.04 <0.001
Dirty/infected 2.41 2.16–2.68 <0.001
Preoperative laboratory values
Sodium
Normal Reference
Low 1.17 1.08–1.26 <0.001
High BUN 0.93 0.87–1.00 <0.05
High creatinine 1.43 1.30–1.57 <0.001
Low albumin 1.48 1.37–1.59 <0.001
Continued next page
TABLE 2. (Continued)
CDI OR 95% CI p
High alkaline phosphatase 1.16 1.08–1.24 <0.001
WBC
Normal Reference
High 1.28 1.19–1.38 <0.001
Low hematocrit 1.39 1.31–1.48 <0.001
High INR 1.19 1.12–1.27 <0.001
Procedure-related characteristics
Work RVU
0.00 to <9.45 Reference
≥ 13.18 to <17.61 1.64 1.45–1.85 <0.001
≥ 17.60 to <21.87 1.64 1.46–1.85 <0.001
≥ 21.87 to 93.0 1.96 1.75–2.20 <0.001
Operation time, min
>0 to ≤43 Reference
>70 to ≤101 1.16 1.04–1.29 <0.05
>101 to ≤157 1.34 1.21–1.49 <0.001
>157 to ≤1440 2.03 1.82–2.26 <0.001
Emergency 1.29 1.19–1.39 <0.001
Surgical specialty
General surgery Reference
Orthopedics 0.75 0.68–0.84 <0.001
Gynecology 0.35 0.30–0.41 <0.001
Urology 0.61 0.54–0.69 <0.001
Neurosurgery 0.72 0.61–0.85 <0.001
Plastic surgery 0.55 0.42–0.71 <0.001
Otolaryngology 0.55 0.43–0.71 <0.001
Thoracic surgery 0.45 0.35–0.57 <0.001
Meier et al.J Trauma Acute Care Surg
Volume 86, Number 6
1006
Copyright © 2019 Wolters Kluwer H
(95% confidence interval [CI], 1.00–1.32; p < 0.05) in the under-weight patients, 0.86 (95% CI, 0.81–0.92; p < 0.001) in the over-weight patients, 0.80 (95% CI, 0.74–0.87; p < 0.001) in the classI obese patients, 0.76 (95%CI, 0.68–0.84; p < 0.001) in the classII obese patients, and 0.73 (95%CI, 0.65–0.81; p < 0.001) in theclass III obese patients (Fig. 2).
Other Predictors of Postoperative CDI in theAdjusted Multivariable AnalysisPatient Characteristics and Comorbidities
In multivariable analyses, other variables that were as-sociated with significantly higher risk for CDI were all agegroups older than 70 years compared with the youngest age group,female sex, smoking, more than 10% weight loss in the past6months, COPD, ascites, hypertension, dialysis, steroid use, sepsis,open wounds, functional dependency, higher ASA classification,contaminated/dirty/infected wounds and bleeding disorders.
Preoperative Laboratory ValuesCompared with normal preoperative laboratory values,
hyponatremia, hypoalbuminemia, leukocytosis, anemia and ele-vated creatinine, alkaline phosphatase, or INR were associatedwith an increased risk of postoperative CDI.
Procedure CharacteristicsEmergency surgery was a risk factor for CDI. The more
complex the procedure, the higher the risk of CDI compared to
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
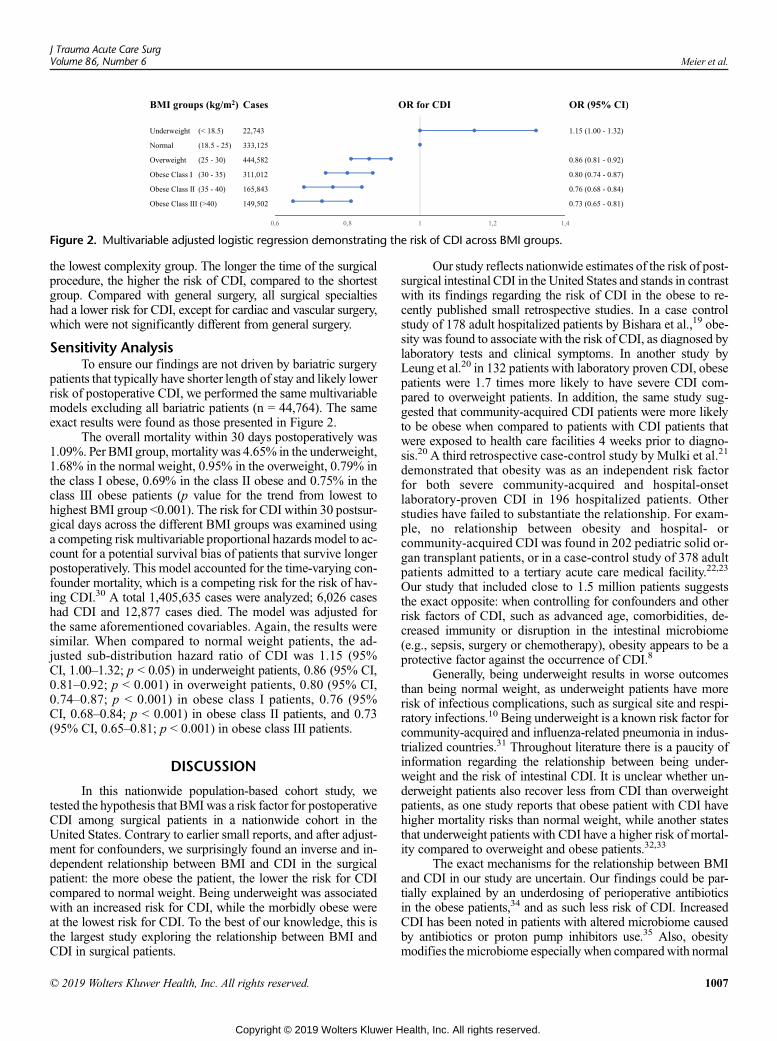
Figure 2. Multivariable adjusted logistic regression demonstrating the risk of CDI across BMI groups.
J Trauma Acute Care SurgVolume 86, Number 6 Meier et al.
the lowest complexity group. The longer the time of the surgicalprocedure, the higher the risk of CDI, compared to the shortestgroup. Compared with general surgery, all surgical specialtieshad a lower risk for CDI, except for cardiac and vascular surgery,which were not significantly different from general surgery.
Sensitivity AnalysisTo ensure our findings are not driven by bariatric surgery
patients that typically have shorter length of stay and likely lowerrisk of postoperative CDI, we performed the same multivariablemodels excluding all bariatric patients (n = 44,764). The sameexact results were found as those presented in Figure 2.
The overall mortality within 30 days postoperatively was1.09%. Per BMI group, mortality was 4.65% in the underweight,1.68% in the normal weight, 0.95% in the overweight, 0.79% inthe class I obese, 0.69% in the class II obese and 0.75% in theclass III obese patients (p value for the trend from lowest tohighest BMI group <0.001). The risk for CDI within 30 postsur-gical days across the different BMI groups was examined usinga competing riskmultivariable proportional hazards model to ac-count for a potential survival bias of patients that survive longerpostoperatively. This model accounted for the time-varying con-founder mortality, which is a competing risk for the risk of hav-ing CDI.30 A total 1,405,635 cases were analyzed; 6,026 caseshad CDI and 12,877 cases died. The model was adjusted forthe same aforementioned covariables. Again, the results weresimilar. When compared to normal weight patients, the ad-justed sub-distribution hazard ratio of CDI was 1.15 (95%CI, 1.00–1.32; p < 0.05) in underweight patients, 0.86 (95% CI,0.81–0.92; p < 0.001) in overweight patients, 0.80 (95% CI,0.74–0.87; p < 0.001) in obese class I patients, 0.76 (95%CI, 0.68–0.84; p < 0.001) in obese class II patients, and 0.73(95% CI, 0.65–0.81; p < 0.001) in obese class III patients.
DISCUSSION
In this nationwide population-based cohort study, wetested the hypothesis that BMI was a risk factor for postoperativeCDI among surgical patients in a nationwide cohort in theUnited States. Contrary to earlier small reports, and after adjust-ment for confounders, we surprisingly found an inverse and in-dependent relationship between BMI and CDI in the surgicalpatient: the more obese the patient, the lower the risk for CDIcompared to normal weight. Being underweight was associatedwith an increased risk for CDI, while the morbidly obese wereat the lowest risk for CDI. To the best of our knowledge, this isthe largest study exploring the relationship between BMI andCDI in surgical patients.
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
Our study reflects nationwide estimates of the risk of post-surgical intestinal CDI in the United States and stands in contrastwith its findings regarding the risk of CDI in the obese to re-cently published small retrospective studies. In a case controlstudy of 178 adult hospitalized patients by Bishara et al.,19 obe-sity was found to associate with the risk of CDI, as diagnosed bylaboratory tests and clinical symptoms. In another study byLeung et al.20 in 132 patients with laboratory proven CDI, obesepatients were 1.7 times more likely to have severe CDI com-pared to overweight patients. In addition, the same study sug-gested that community-acquired CDI patients were more likelyto be obese when compared to patients with CDI patients thatwere exposed to health care facilities 4 weeks prior to diagno-sis.20 A third retrospective case-control study by Mulki et al.21
demonstrated that obesity was as an independent risk factorfor both severe community-acquired and hospital-onsetlaboratory-proven CDI in 196 hospitalized patients. Otherstudies have failed to substantiate the relationship. For exam-ple, no relationship between obesity and hospital- orcommunity-acquired CDI was found in 202 pediatric solid or-gan transplant patients, or in a case-control study of 378 adultpatients admitted to a tertiary acute care medical facility.22,23
Our study that included close to 1.5 million patients suggeststhe exact opposite: when controlling for confounders and otherrisk factors of CDI, such as advanced age, comorbidities, de-creased immunity or disruption in the intestinal microbiome(e.g., sepsis, surgery or chemotherapy), obesity appears to be aprotective factor against the occurrence of CDI.8
Generally, being underweight results in worse outcomesthan being normal weight, as underweight patients have morerisk of infectious complications, such as surgical site and respi-ratory infections.10 Being underweight is a known risk factor forcommunity-acquired and influenza-related pneumonia in indus-trialized countries.31 Throughout literature there is a paucity ofinformation regarding the relationship between being under-weight and the risk of intestinal CDI. It is unclear whether un-derweight patients also recover less from CDI than overweightpatients, as one study reports that obese patient with CDI havehigher mortality risks than normal weight, while another statesthat underweight patients with CDI have a higher risk of mortal-ity compared to overweight and obese patients.32,33
The exact mechanisms for the relationship between BMIand CDI in our study are uncertain. Our findings could be par-tially explained by an underdosing of perioperative antibioticsin the obese patients,34 and as such less risk of CDI. IncreasedCDI has been noted in patients with altered microbiome causedby antibiotics or proton pump inhibitors use.35 Also, obesitymodifies the microbiome especially when comparedwith normal
1007
ealth, Inc. All rights reserved.

Meier et al.J Trauma Acute Care Surg
Volume 86, Number 6
weight individuals.16,17,36 Increased body fat and obesity-relatedmetabolic disorders are associated with having fewer microbialgenes in the colon.36 Causal relations between microbiome andweight regulation have also been suggested. Animal studies haveshown that mice receiving gut microbes from obese humans gainmore weight than mice receiving gut microbes from a lean hu-man donor.37 The mechanism of how C. difficile colonizes theintestinal microbiome in certain microbiomes remains unclear.
Another interesting finding was that surgical patients withdiabetes mellitus receiving noninsulin therapy had significantlyless risk of CDI compared with nondiabetics. The risk of surgi-cal patients with diabetes receiving insulin therapy was similarto nondiabetics. While the mechanism remains unclear, it couldbe related to the most commonly used oral hypoglycemic metfor-min. Metformin is believed to influence the function of and alterthe gut microbiome.38–40Metformin also has anti-inflammatory ef-fects.41,42 It has been shown to reduce intestinal inflammation andacute diverticulitis.38,39 Recently, Eliakim-Raz et al.43 have sug-gested a protective effect of metformin therapy in diabetic patientsagainst CDI. These pathways are poorly understood and future re-search is needed to examine the relationship between intestinalCDI, BMI, and other factors affecting the microbiome.
Our study has a number of limitations. First, despite ourmeticulous attempt at controlling for all existing patient and pro-cedure related factors, there likely exist confounders not recordedwith the ACS-NSQIP database. These include the duration andtype of antibiotic used, the use of proton pomp inhibitors, theuse of tube feedings, exposure to health care facilities prior to ad-mission, the geographic locations of the participating center, andwhether any unusual outbreaks of CDI impacted our results.However, there is no apparent nonrandom relationship betweenBMI and any of these confounders that we are aware of. Lastly,the association we found, does not prove causality.
CONCLUSION
Our data suggest that obesity is independently and in a step-wise fashion associated with a decreased risk of postoperativeCDI. Further studies are warranted to explore the potential asso-ciation and mitigate that risk.
AUTHORSHIP
K.M., A.T.N., A.I.E., N.K., J.M.L., M.K., K.R.H., N.K., A.E.M.,N.S., D.R.K., G.C.V., and H.M.A.K. contributed to the conception and design of the re-search. K.M., A.T.N., and J.M.L. contributed to the acquisition of data.K.M., A.T.N., A.I.E., J.M.L., M.K., K.R.H., and N.K., and H.M.A.K. contrib-uted to the data analysis. K.M., A.T.N., A.I.E., N.K., J.M.L., M.K., K.R.H.,N.K., A.E.M., N.S., D.R.K., G.C.V., and H.M.A.K. contributed to the datainterpretation. K.M. drafted the article. All authors critically revised the ar-ticle, read and approved the final article, and agree to be fully accountablefor ensuring the integrity and accuracy of the work. Each of the individualauthors has sufficiently participated in this study to be listed as author.
DISCLOSURE
The authors have no conflicts of interest.The authors have no sources of funding to disclose.
REFERENCES1. Banaei N, Anikst V, Schroeder LF. Burden of Clostridium difficile infection
in the United States. N Engl J Med. 2015;372(24):2368–2369.
1008
Copyright © 2019 Wolters Kluwer H
2. Chandler RE, Hedberg K, Cieslak PR. Clostridium difficile-associated dis-ease in Oregon: increasing incidence and hospital-level risk factors. InfectControl Hosp Epidemiol. 2007;28(2):116–122.
3. Dallal RM, Harbrecht BG, Boujoukas AJ, Sirio CA, Farkas LM, Lee KK,Simmons RL. Fulminant Clostridium difficile: an underappreciated and in-creasing cause of death and complications. Ann Surg. 2002;235(3):363–372.
4. Kazakova SV, Ware K, Baughman B, Bilukha O, Paradis A, Sears S,Thompson A, Jensen B, Wiggs L, Bessette J, et al. A hospital outbreak of di-arrhea due to an emerging epidemic strain of Clostridium difficile. ArchIntern Med. 2006;166(22):2518–2524.
5. Reveles KR, Lee GC, Boyd NK, Frei CR. The rise in Clostridium difficileinfection incidence among hospitalized adults in the United States: 2001–2010.Am J Infect Control. 2014;42(10):1028–1032.
6. Tan ET, Robertson CA, Brynildsen S, Bresnitz E, Tan C,McDonald C.Clos-tridium difficile-associated disease in New Jersey hospitals, 2000–2004.Emerg Infect Dis. 2007;13(3):498–500.
7. McDonald LC, Owings M, Jernigan DB. Clostridium difficile infection inpatients discharged from US short-stay hospitals, 1996–2003. Emerg InfectDis. 2006;12(3):409–415.
8. McFarland LV. Renewed interest in a difficult disease: Clostridium difficileinfections—epidemiology and current treatment strategies. Curr Opin Gastroenterol.2009;25(1):24–35.
9. Ringback Weitoft G, Eliasson M, Rosen M. Underweight, overweight andobesity as risk factors for mortality and hospitalization. Scand J PublicHealth. 2008;36(2):169–176.
10. Dobner J, Kaser S. Body mass index and the risk of infection—from under-weight to obesity. Clin Microbiol Infect. 2018;24(1):24–28.
11. Flegal KM, Graubard BI, Williamson DF, Gail MH. Excess deaths asso-ciated with underweight, overweight, and obesity. JAMA. 2005;293(15):1861–1867.
12. Hourigan JS. Impact of obesity on surgical site infection in colon and rectalsurgery. Clin Colon Rectal Surg. 2011;24(4):283–290.
13. Bamgbade OA, Rutter TW, Nafiu OO, Dorje P. Postoperative complications inobese and nonobese patients.World J Surg. 2007;31(3):556–560; discussion 561.
14. Cao H. Adipocytokines in obesity and metabolic disease. J Endocrinol.2014;220(2):T47–T59.
15. Madan R, Petri WA Jr. Role of obesity and adipose tissue-derived cytokineleptin during Clostridium difficile infection. Anaerobe. 2015;34:182–186.
16. Armougom F, Henry M, Vialettes B, Raccah D, Raoult D. Monitoring bacterialcommunity of human gut microbiota reveals an increase in lactobacillus in obesepatients and methanogens in anorexic patients. PLoS One. 2009;4(9):e7125.
17. Turnbaugh PJ, Ley RE, Mahowald MA, Magrini V, Mardis ER, Gordon JI.An obesity-associated gut microbiome with increased capacity for energyharvest. Nature. 2006;444(7122):1027–1031.
18. Hales CM, Carroll MD, Fryar CD, Ogden CL. Prevalence of obesity amongadults and youth: United States, 2015–2016.NCHSData Brief. 2017;(288):1–8.
19. Bishara J, Farah R, Mograbi J, Khalaila W, Abu-Elheja O, Mahamid M,Nseir W. Obesity as a risk factor for Clostridium difficile infection. Clin In-fect Dis. 2013;57(4):489–493.
20. Leung J, Burke B, Ford D, Garvin G, Korn C, Sulis C, Bhadelia N. Possibleassociation between obesity and Clostridium difficile infection. Emerg InfectDis. 2013;19(11):1791–1796.
21. Mulki R, Baumann AJ, Alnabelsi T, Sandhu N, Alhamshari Y, Wheeler DS,Perloff S, Katz PO. Body mass index greater than 35 is associated with severeClostridium difficile infection. Aliment Pharmacol Ther. 2017;45(1):75–81.
22. Ciricillo J, Haslam D, Blum S, Kim MO, Liu C, Paulsen G, Courter J,Danziger-Isakov L. Frequency and risks associated with Clostridiumdifficile-associated diarrhea after pediatric solid organ transplantation: asingle-center retrospective review. Transpl Infect Dis. 2016;18(5):706–713.
23. Punni E, Pula JL, Asslo F, Baddoura W, DeBari VA. Is obesity a risk factorfor Clostridium difficile infection? Obes Res Clin Pract. 2015;9(1):50–54.
24. ACS-NSQIP. User Guide for the 2016ACSNSQIP Participant Use Date File(PUF). 2016; [cited 2018 January]. Available from: https://www.facs.org/~/media/files/quality%20programs/nsqip/nsqip_puf_userguide_2016.ashx.
25. Romero-CorralA, SomersVK, Sierra-Johnson J, ThomasRJ, Collazo-ClavellML,Korinek J, Allison TG, Batsis JA, Sert-Kuniyoshi FH, Lopez-Jimenez F. Ac-curacy of body mass index in diagnosing obesity in the adult general popu-lation. Int J Obes. 2008;32(6):959–966.
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 6 Meier et al.
26. Bohnen JD, Mavros MN, Ramly EP, Chang Y, Yeh DD, Lee J, de Moya M,King DR, Fagenholz PJ, Butler K, et al. Intraoperative adverse events in ab-dominal surgery: what happens in the operating room does not stay in the op-erating room. Ann Surg. 2017;265(6):1119–1125.
27. Davenport DL, HendersonWG, Khuri SF, Mentzer RM Jr. Preoperative riskfactors and surgical complexity are more predictive of costs than postoperativecomplications: a case study using the National Surgical Quality ImprovementProgram (NSQIP) database. Ann Surg. 2005;242(4):463–468; discussion468-71.
28. Burns HJ. The metabolic and nutritional effects of injury and sepsis. BaillieresClin Gastroenterol. 1988;2(4):849–867.
29. Gooley TA, Leisenring W, Crowley J, Storer BE. Estimation of failure prob-abilities in the presence of competing risks: new representations of old esti-mators. Stat Med. 1999;18(6):695–706.
30. Fine JP, Gray RJ. A proportional hazards model for the subdistribution of acompeting risk. J Am Stat Assoc. 1999;94(446):496–509.
31. Phung DT, Wang Z, Rutherford S, Huang C, Chu C. Body mass index andrisk of pneumonia: a systematic review and meta-analysis. Obes Rev. 2013;14(10):839–857.
32. Mansoor MS, Feuerstadt P. Underweight patients with C. difficile infection(CDI) are at higher risk of poor outcome than normal, overweight and obesepatients. Gastroenterology. 2015;148(4):S-484.
33. Nathanson BH, Higgins TL,McGeeWT. The dangers of extreme bodymass in-dex values in patients with Clostridium difficile. Infection. 2017;45(6):787–793.
34. Tucker CE, Lockwood AM, Nguyen NH. Antibiotic dosing in obesity: thesearch for optimum dosing strategies. Clin Obes. 2014;4(6):287–295.
35. Lagier JC. Gut microbiota andClostridium difficile infections.HumMicrobiomeJ. 2016;2:10–14.
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
36. Le Chatelier E, Nielsen T, Qin J, Prifti E, Hildebrand F, Falony G, Almeida M,ArumugamM,Batto JM,Kennedy S, et al. Richness of human gutmicrobiomecorrelates with metabolic markers. Nature. 2013;500(7464):541–546.
37. Ridaura VK, Faith JJ, Rey FE, Cheng J, Duncan AE, Kau AL, Griffin NW,Lombard V, Henrissat B, Bain JR, et al. Cultured gut microbiota from twinsdiscordant for obesity modulate adiposity and metabolic phenotypes in mice.Science. 2013;341(6150):1241214.
38. Freckelton J, Evans JA, Croagh D, Moore GT. Metformin use in diabeticswith diverticular disease is associated with reduced incidence of diverticuli-tis. Scand J Gastroenterol. 2017;52(9):969–972.
39. Wu H, Esteve E, Tremaroli V, Khan MT, Caesar R, Manneras-Holm L,Stahlman M, Olsson LM, Serino M, Planas-Felix M, et al. Metformin altersthe gut microbiome of individuals with treatment-naive type 2 diabetes, con-tributing to the therapeutic effects of the drug. Nat Med. 2017;23(7):850–858.
40. de la Cuesta-Zuluaga J, Mueller NT, Corrales-Agudelo V, Velásquez-Mejía EP,Carmona JA, Abad JM, Escobar JS. Metformin is associated with higher rel-ative abundance of mucin-degrading Akkermansia muciniphila and severalshort-chain fatty acid–producing microbiota in the gut. Diabetes Care.2016;40(1):54–62.
41. Cameron AR, Morrison VL, Levin D, Mohan M, Forteath C, Beall C,McNeilly AD, Balfour DJ, Savinko T, Wong AK, et al. Anti-inflammatoryeffects of metformin irrespective of diabetes status. Circ Res. 2016;119(5):652–665.
42. Saisho Y. Metformin and inflammation: its potential beyond glucose-loweringeffect. Endocr Metab Immune Disord Drug Targets. 2015;15(3):196–205.
43. Eliakim-Raz N, Fishman G, Yahav D, Goldberg E, Stein GY, Zvi HB,Barsheshet A, Bishara J. PredictingClostridium difficile infection in diabeticpatients and the effect of metformin therapy: a retrospective, case–controlstudy. Eur J Clin Microbiol Infect Dis. 2015;34(6):1201–1205.
1009
ealth, Inc. All rights reserved.
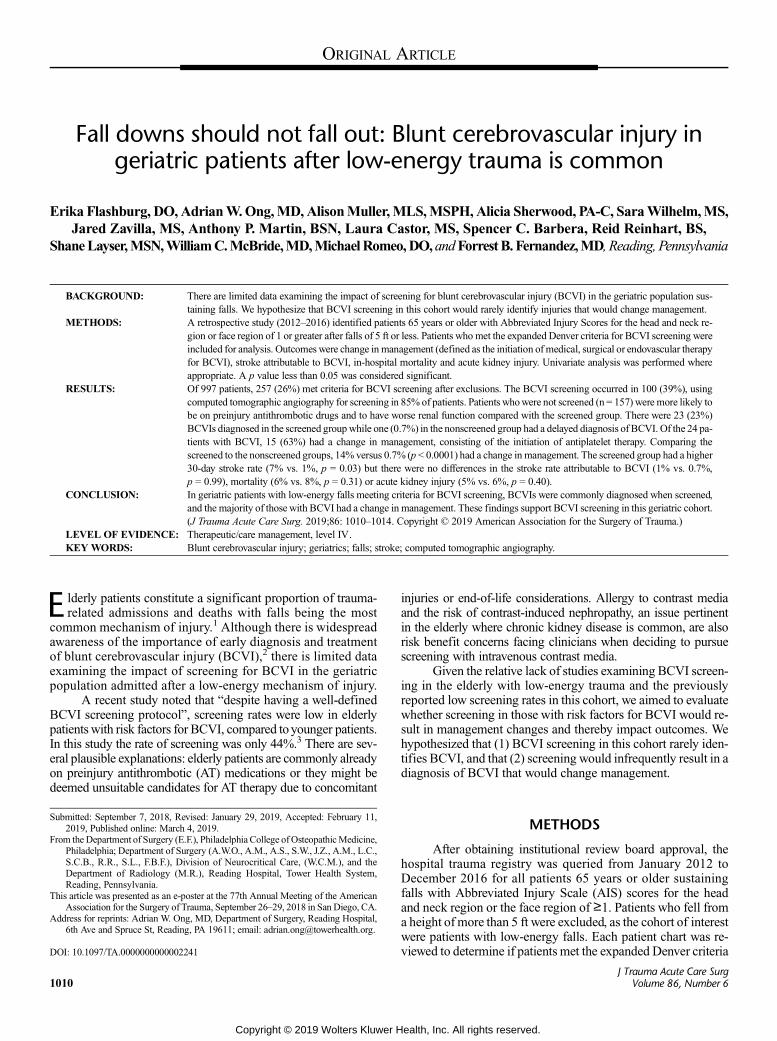
ORIGINAL ARTICLE
Fall downs should not fall out: Blunt cerebrovascular injury ingeriatric patients after low-energy trauma is common
Erika Flashburg, DO,AdrianW.Ong,MD,AlisonMuller,MLS,MSPH,Alicia Sherwood, PA-C, SaraWilhelm,MS,Jared Zavilla, MS, Anthony P. Martin, BSN, Laura Castor, MS, Spencer C. Barbera, Reid Reinhart, BS,
ShaneLayser,MSN,WilliamC.McBride,MD,MichaelRomeo,DO,andForrestB. Fernandez,MD, Reading, Pennsylvania
Sub
Fro
Thi
Ad
DO
10
BACKGROUND: T
mitted: September 7, 2018, Re2019, Published online: Marchm the Department of Surgery (EPhiladelphia; Department of SuS.C.B., R.R., S.L., F.B.F.), DiDepartment of Radiology (MReading, Pennsylvania.s article was presented as an e-pAssociation for the Surgery of Tdress for reprints: Adrian W. On6th Ave and Spruce St, Readin
I: 10.1097/TA.00000000000022
10
here are limited data examining the impact of screening for blunt cerebrovascular injury (BCVI) in the geriatric population sus-taining falls. We hypothesize that BCVI screening in this cohort would rarely identify injuries that would change management.
METHODS: A
retrospective study (2012–2016) identified patients 65 years or older with Abbreviated Injury Scores for the head and neck re-gion or face region of 1 or greater after falls of 5 ft or less. Patients who met the expanded Denver criteria for BCVI screening wereincluded for analysis. Outcomes were change in management (defined as the initiation of medical, surgical or endovascular therapyfor BCVI), stroke attributable to BCVI, in-hospital mortality and acute kidney injury. Univariate analysis was performed whereappropriate. A p value less than 0.05 was considered significant.RESULTS: O
f 997 patients, 257 (26%) met criteria for BCVI screening after exclusions. The BCVI screening occurred in 100 (39%), usingcomputed tomographic angiography for screening in 85% of patients. Patients whowere not screened (n = 157) were more likely tobe on preinjury antithrombotic drugs and to have worse renal function compared with the screened group. There were 23 (23%)BCVIs diagnosed in the screened groupwhile one (0.7%) in the nonscreened group had a delayed diagnosis of BCVI. Of the 24 pa-tients with BCVI, 15 (63%) had a change in management, consisting of the initiation of antiplatelet therapy. Comparing thescreened to the nonscreened groups, 14% versus 0.7% (p < 0.0001) had a change in management. The screened group had a higher30-day stroke rate (7% vs. 1%, p = 0.03) but there were no differences in the stroke rate attributable to BCVI (1% vs. 0.7%,p = 0.99), mortality (6% vs. 8%, p = 0.31) or acute kidney injury (5% vs. 6%, p = 0.40).CONCLUSION: I
n geriatric patients with low-energy falls meeting criteria for BCVI screening, BCVIs were commonly diagnosed when screened,and the majority of those with BCVI had a change in management. These findings support BCVI screening in this geriatric cohort.(J Trauma Acute Care Surg. 2019;86: 1010–1014. Copyright © 2019 American Association for the Surgery of Trauma.)LEVEL OF EVIDENCE: T
herapeutic/care management, level IV. KEYWORDS: B lunt cerebrovascular injury; geriatrics; falls; stroke; computed tomographic angiography.E lderly patients constitute a significant proportion of trauma-related admissions and deaths with falls being the most
common mechanism of injury.1 Although there is widespreadawareness of the importance of early diagnosis and treatmentof blunt cerebrovascular injury (BCVI),2 there is limited dataexamining the impact of screening for BCVI in the geriatricpopulation admitted after a low-energy mechanism of injury.
A recent study noted that “despite having a well-definedBCVI screening protocol”, screening rates were low in elderlypatients with risk factors for BCVI, compared toyounger patients.In this study the rate of screening was only 44%.3 There are sev-eral plausible explanations: elderly patients are commonly alreadyon preinjury antithrombotic (AT) medications or they might bedeemed unsuitable candidates for AT therapy due to concomitant
vised: January 29, 2019, Accepted: February 11,4, 2019..F.), Philadelphia College ofOsteopathicMedicine,rgery (A.W.O., A.M., A.S., S.W., J.Z., A.M., L.C.,vision of Neurocritical Care, (W.C.M.), and the.R.), Reading Hospital, Tower Health System,
oster at the 77th Annual Meeting of the Americanrauma, September 26–29, 2018 in San Diego, CA.g, MD, Department of Surgery, Reading Hospital,g, PA 19611; email: [email protected].
41
Copyright © 2019 Wolters Kluwer H
injuries or end-of-life considerations. Allergy to contrast mediaand the risk of contrast-induced nephropathy, an issue pertinentin the elderly where chronic kidney disease is common, are alsorisk benefit concerns facing clinicians when deciding to pursuescreening with intravenous contrast media.
Given the relative lack of studies examining BCVI screen-ing in the elderly with low-energy trauma and the previouslyreported low screening rates in this cohort, we aimed to evaluatewhether screening in those with risk factors for BCVI would re-sult in management changes and thereby impact outcomes. Wehypothesized that (1) BCVI screening in this cohort rarely iden-tifies BCVI, and that (2) screening would infrequently result in adiagnosis of BCVI that would change management.
METHODS
After obtaining institutional review board approval, thehospital trauma registry was queried from January 2012 toDecember 2016 for all patients 65 years or older sustainingfalls with Abbreviated Injury Scale (AIS) scores for the headand neck region or the face region of ≥1. Patients who fell froma height of more than 5 ft were excluded, as the cohort of interestwere patients with low-energy falls. Each patient chart was re-viewed to determine if patients met the expanded Denver criteria
J Trauma Acute Care SurgVolume 86, Number 6
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 6 Flashburg et al.
for BCVI screening.4 Patients who met the criteria formed thebasis group for the study.
The BCVI screening was mostly performed with com-puted tomography (CT) angiography (CTA) using a 128-sliceCT scanner throughout the study period. Ultimately, the decisionto proceed with BCVI screening and the choice of radiologicmodality was at the discretion of the admitting physician. Usingthe expanded Denver criteria, patients were categorized intothose who presented with signs and symptoms suggestive ofBCVI, and those with risk factors for BCVI.4 For each of thetwo categories, we compared outcomes for patients that receivedscreening on presentation with those that did not. Study out-comes were: change in management after BCVI screening, in-hospital mortality, acute kidney injury (AKI), and documentedstroke in the 30-day period following the index admissionafter trauma. The AT drugs were defined as antiplatelet drugs,vitamin K, or nonvitamin K antagonists. Change in manage-ment was defined as initiation of any new AT therapy not pres-ent before admission, any operative or endovascular treatmentof BCVI. Acute kidney injury was defined as that meetingat least stage 1 criteria based on the 2011 Kidney Disease:Improving Global Outcomes Clinical Practice Guideline for AcuteKidney Injury.5
We assumed that if 10% in the screened group had achange in management compared with 0% in the nonscreenedgroup, this would be clinically significant. Setting alpha = 0.05and power = 80%, 72 and 108 patients would be needed in thescreened and nonscreened groups, respectively, assuming a1:1.5 enrollment ratio of screened to nonscreened patients.
Univariate analysis was performed using the unpairedStudent’s t test, Mann-Whitney U test, χ2 test or Fisher's exacttest where appropriate. Means were expressed with standarddeviations and medians with interquartile ranges. Ninety-fivepercent confidence intervals were calculated for proportionsusing the exact (Clopper-Pearson) method. A p value less than0.05 indicated statistical significance. Statistical analysis wasperformed using StatsDirect version 3.1.8 (StatsDirect Ltd.,Cheshire, United Kingdom).
RESULTS
Of 1791 patients 65 years or older who fell with an AIS—head/neck or AIS—face score of ≥1, 997(56%) fell from aheight of ≤5 feet. Of these, 263 (26%) met criteria for screeningbased on the expanded Denver criteria (Fig. 1). After excludingsix patients who arrived in cardiac arrest, 257 patients formedthe basis group for further analysis.
Of these 257, 100 (39%) underwent screening for BCVIon arrival. CTA was used for screening, except in 15 (15%)where magnetic resonance angiography (MRA) was used andin one where four-vessel cerebral angiography was used for urgentcontrol of oropharyngeal and nasal bleeding. Patients that were notscreened were more likely to be on preinjury AT drugs and to haveworse renal function compared to the screened group, butwere sim-ilarwith respect to InjurySeverityScore,AIS—head/neck,AIS—face,Glasgow Coma Scale score and systolic blood pressure (Table 1).
In patients who presented with signs and symptoms sug-gestive of BCVI (n = 20), 12 (60%) underwent screening onadmission with none having a BCVI (Fig. 1 and Table 2). Three
© 2019 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer H
screened patients were ultimately diagnosed with strokes, all notattributable to BCVI: two had their home AT drugs continued,and one was started on aspirin. Of the nonscreened patients,one developed a stroke that could be attributable to a BCVI: thispatient presented with asymptomatic age-indeterminate parietaland basal ganglia infarcts on CT (thus was labeled as having apossible “stroke on imaging”). No screening was performedon admission but the development of hemiplegia prompted im-aging on day 2 that revealed cerebral infarction and an ipsilateralinternal carotid artery occlusion. It is difficult to ascertainwhether the stroke occurred prior to the fall or as a result ofthe injury, but it was noted that the patient was neurologically in-tact on admission. The patient was started on clopidogrel on thethird hospital day. In the nonscreened group, there also werethree other patients with focal neurologic deficits or stroke-likesymptoms (Fig. 1): one required urgent pacemaker placementcomplicated by a ventricular perforation and care was with-drawn, one had an MRI that ruled out an acute stroke and onerefused stroke workup. It is not clear from the patient recordsas to why four patients with “potential arterial hemorrhage” werenot screened, but these four presented with epistaxis that stoppedspontaneously or with nasal packing. Overall, in the 20 patientswith signs and symptoms suggestive of BCVI, there were four(20%) strokes, with one (5%) attributable to a BCVI.
In patients with risk factors for BCVI (n = 237), 88 (37%)underwent BCVI screening, of which 23 (26%) had BCVI(Table 2). In the nonscreened group (n = 149), none had a de-layed diagnosis of BCVI. Of the 23 patients with BCVI, all ofwhich were vertebral artery injuries, 14 (61%) had a changein management consisting of initiation of antiplatelet therapy.The rest were either already on AT medications prior to arrival(n = 5) or were felt to be unsuitable for initiation of AT therapydue to injuries at risk for hemorrhagic progression (n = 4). Bifflgrades for the 23 BCVIs were as follows: grade 1, n = 13; grade2, n = 7; grade 3, n = 2; grade 4, n = 1. Overall, in the 237 patientswith risk factors suggestive of BCVI, there were five (2%)strokes, with only one (0.7%) attributable to a vertebral artery in-jury. This stroke occurred 2 weeks in the screened group and af-ter initiation of antiplatelet therapy without delay. The otherstrokes were thought to be due to cardiac emboli (n = 1) orin the anterior circulation territory that did not correspondto vertebral artery injuries (n = 3).
Comparing the screened (n = 100) with the nonscreened(n = 157) groups, 14% versus 0.7% (p < 0.0001) had a changeof management respectively related to BCVI diagnosis. Thescreened group had a higher 30-day stroke rate (7% vs. 1%,p = 0.03), but there were no differences in the stroke rate attrib-utable to BCVI (1% vs. 0.7%, p = 0.99), mortality (6% vs. 8%,p = 0.31), or AKI (5% vs. 6%, p = 0.40).
Overall, the prevalence of BCVI in the screened group(n = 100) was 23% (95% confidence interval, 15%–32%) whileone (0.7%) of the nonscreened group had a BCVI that wasnot diagnosed on admission. In total, of the 24 BCVI patients,15 (63%) had a change in management (medical therapy).
DISCUSSION
Blunt cerebrovascular injury occurs in approximately0.1% to 0.2% of patients in large registry databases.6,7 Early
1011
ealth, Inc. All rights reserved.
Figure 1. Flow diagram of study groups. GCS, Glasgow Coma Scale.
Flashburg et al.J Trauma Acute Care Surg
Volume 86, Number 6
diagnosis through aggressive screening is important in reducingstroke risk.8,9 However, it is not clear whether current clinicalscreening practices are cost-effective or impact outcomes inthe geriatric population sustaining low-energy trauma.
The principal findings in our study were that: (1) BCVIwas common in geriatric patients sustaining falls who metscreening criteria; (2) the prevalence of stroke attributed toBCVI was low, regardless of BCVI screening; and that (3) themajority of patients (63%) diagnosed with BCVI had a changein management.
Only one other recent study had specifically analyzedBCVI in elderly patients with a low-energy mechanism of in-jury. Anto et al.3 found that with a screening rate of 44% in theirelderly patients sustaining ground level falls, the incidence ofBCVI was 2.9% in almost 2500 patients with at least one risk
1012
Copyright © 2019 Wolters Kluwer H
factor for BCVI. With a similar screening rate (39%), we founda much higher incidence where there were BCVI risk factors.However, the prevalence of stroke of 4.2% that was attributableto BCVI reported by Anto et al. was similar in absolute magni-tude to that of our study.
There were several possible reasons for the low screeningrate in our study: there could have been perceptions of a low riskfor BCVI given the low-energy mechanism, or of a low likeli-hood of change in therapy for abovementioned reasons (alreadyon AT therapy, contraindications to AT therapy, poor quality oflife due to comorbid conditions such as dementia). In thenonscreened group (n = 157), 108 (69%) were on preinjuryAT drugs. Of these, 32 (30%) had hemorrhagic risks resultingin cessation of the AT drugs on admission. Our study couldnot determine if screening would have changed management
© 2019 American Association for the Surgery of Trauma.
ealth, Inc. All rights reserved.
TABLE 1. Characteristics of Screened vs Nonscreened Patients
Screened on Admission (n = 100) Not Screened on Admission (n = 157) p
Median age, y 80 (73–87) 84 (75–88) 0.054
Male sex, % 46 (46%) 83 (53%) 0.28
Median admission SBP, mm Hg 153 (127–172) 147 (123–172) 0.45
Median admission GCS 15 (15–15) 15 (15–15) 0.18
Median admission serum creatinine, mg/dL 0.92 (0.80–1.29) 1.20 (0.93–1.51) 0.001
Preinjury AT drug use, % 49 (49%) 108 (69%) 0.0008
ICH on admission CT, % 23 (23%) 35 (22%) 0.89
Median AIS—head and neck 3 (2–3) 3 (2–3) 0.83
Median AIS—face 0 (0–0) 0 (0–1) 0.11
Median ISS 10 (9–14) 10 (5–14) 0.17
Median values expressed with interquartile ranges.GCS, Glasgow Coma Scale; ICH, intracranial hemorrhage; ISS, Injury Severity Score; SBP, systolic blood pressure.
J Trauma Acute Care SurgVolume 86, Number 6 Flashburg et al.
for patients already on AT therapy who were continued on theirAT drugs. On the other hand, restarting or initiation of AT drugsafter a diagnosis of BCVI in patients with relative bleedingcontraindications may be safe. Shahan et al.10 found that in119 patients with traumatic brain injury or solid organ injury,starting low-dose aspirin or low-intensity heparin infusion aftera BCVI diagnosis was not associated with hemorrhage progres-sion when compared with patients without BCVI.10 However,their study did not compare injury severity between the patientswith BCVI and those without BCVI. In another study of 212 pa-tients with BCVI with multisystem injuries and contraindica-tions to immediate AT therapy, 19% had no AT therapy initiatedfor various reasons. In the remainder, there were no recordedbleeding complications due to AT therapy.11 Although these stud-ies support the safety of initiation of AT therapy in patients withrelative contraindications, further studies are needed to assess riskof bleeding in relation to injury severity.
The stroke rates in both the screened and nonscreenedgroups were low. There are possible reasons: (1) a significantproportion of patients in both groups were already on preinjuryAT therapy, and most patients had AT drugs continued for treat-ment of BCVI or in the absence of any contraindications. There-fore, the “true” stroke rate is not known in untreated patients,which is a limitation of the study. (2) The low-grade vertebral ar-tery injuries diagnosed on CTA may in fact not be injuries. Tworecent studies found false positive rates of greater than 40%
TABLE 2. Outcomes of the Two Presentation Categories
Signs and Symptoms Suggestive of BCVI (n
Screened (n = 12) Not Screened (n = 8)
BCVI (%) 0 1 (13%)
Vertebral artery injury 0 0
ICA injury 0 1 (13%)
Change in management 0 1 (13%)
Stroke within 30 d (%) 3 (25%) 1 (13%)
Stroke attributable to BCVI 0 1 (13%)
AKI (%) 1 (8%) 2 (25%)
In-hospital mortality (%) 1 (8%) 1 (13%)
ICA, internal carotid artery; N/A, not applicable.
© 2019 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer H
when BCVIs were diagnosed by CTA compared with confir-matory digital subtraction angiography (DSA).12,13 We werenot able to verify these results as none of the BCVI patientsunderwent DSA. Although some studies have shown low strokerates with low-grade vertebral artery injuries,14–16 Biffl et al.17
found that a large proportion of patients (3 [12%] of 25) withgrade 1 vertebral artery injuries had posterior circulation strokesin their series. Given these conflicting findings, we think thatthat treatment of low-grade asymptomatic vertebral artery inju-ries when diagnosed by CTA is warranted unless there are otherimportant competing factors.
Other limitations of this study were as follows: (1) Screen-ing methods were not uniform. Comparison studies of the accu-racy of CTAversus MRA are few. While two studies more than15 years ago had noted similar sensitivities and specificities forMRA and CTA,9,17 a more recent study evaluating radiologists'preferences found that CTA was the preferred test especiallyfor vertebral artery injuries.18 Since our study was retrospec-tive in nature, physician preference for MRA instead of CTAwas difficult to elucidate. The risk of contrast nephropathy,history of allergy to iodinated contrast, or need to evaluate forcerebral ischemia may have been reasons for utilizing MRI. Al-though CTA remains our preferred modality, a recently usedMRI technique of high-resolution double inversion recoveryblack-blood imaging was found to compare favorably withCTA in patients with arterial dissection.19 A recent review also
= 20) Risk Factors for BCVI (n = 237)
p Screened (n = 88) Not Screened (n = 149) p
0.40 23 (26%) 0 <0.0001
23 (26%) 0
0 0
0.40 14 (16%) 0 <0.0001
0.61 4 (5%) 1 (0.7%) 0.06
0.40 1 (1%) 0 0.37
0.54 4 (5%) 7 (5%) 0.99
0.99 5 (6%) 11 (7%) 0.79
1013
ealth, Inc. All rights reserved.
Flashburg et al.J Trauma Acute Care Surg
Volume 86, Number 6
noted that while CTAwas usually used, “that choice is based onconsensus among the neuroradiologists at our institution ratherthan on evidence culled from the medical literature indicatinga clear superiority of CTA for diagnosis of dissection”.20 (3)Contraindications to initiation of AT therapy for BCVI treatmentcan be time-dependent and the risk benefit can change duringthe hospital course. The intentions of the treating physicianswere oftentimes unclear in this retrospective review as to treat-ment decisions with regard to screening. Therefore, the magni-tude of the “change in management” could have been greaterthan what we found, but this fundamentally would not alterour conclusion that identification of BCVI frequently resultedin management changes.
In summary, contrary to our hypothesis, BCVI was com-mon in geriatric patients with low-energy falls meeting criteriafor BCVI screening, and the majority of those with BCVI hada change in management. Our findings support BCVI screeningin the majority of geriatric patients with low-energy traumameeting screening criteria. Further studies are needed to exam-ine the impact of treatment of BCVI on long-term outcomes inthe geriatric population.
AUTHORSHIP
E.F., A.W.O., A.M., F.B.F. participated in the literature search. E.F., A.W.O.,A.M., F.B.F., A.P.M. participated in the study design. E.F., A.W.O., A.M.,A.P.M., A.S., S.W., J.Z., L.C., S.C.B., R.R., S.L. participated in data collec-tion, E.F., A.W.O., A.M., W.C.M. participated in data analysis. E.F., A.W.O.,W.C.M., F.B.F, M.R. participated in data interpretation. E.F., A.W.O., F.B.F.,W.C.M. participated in writing. E.F., A.W.O., A.M., A.S., S.W., J.Z., A.P.M.,L.C., S.C.B., R.R., S.L., F.B.F., W.C.M., M.R. participated in critical revision.
DISCLOSURE
Conflicts of interest and sources of funding: None declared.
REFERENCES1. Sterling DA, O'Connor JA, Bonadies J. Geriatric falls: injury severity is high
and disproportionate to mechanism. J Trauma. 2001;50(1):116–119.2. Bromberg WJ, Collier BC, Diebel LN, Dwyer KM, Holevar MR,
Jacobs DG, Kurek SJ, SchreiberMA, ShapiroML, Vogel TR. Blunt cerebro-vascular injury practice management guidelines: the Eastern Association forthe Surgery of trauma. J Trauma. 2010;68(2):471–477.
3. Anto VP, Brown JB, Peitzman AB, Zuckerbraun BS, Neal MD, Watson G,Forsythe R, Billiar TR, Sperry JL. Blunt cerebrovascular injury in elderly fallpatients: are we screening enough? World J Emerg Surg. 2018;13:30.
4. Burlew CC, Biffl WL, Moore EE, Barnett CC, Johnson JL, Bensard DD.Blunt cerebrovascular injuries: redefining screening criteria in the era of non-invasive diagnosis. J Trauma Acute Care Surg. 2012;72(2):330–335.
5. Kellum JA, Lameire N, , KDIGO AKI Guideline Work Group. Diagnosis,evaluation, and management of acute kidney injury: a KDIGO summary(part 1). Crit Care. 2013;17(1):204.
6. Grigorian A, Kabutey NK, Schubl S, de Virgilio C, Joe V, Dolich M,Elfenbein D, Nahmias J. Blunt cerebrovascular injury incidence, stroke-rate,
1014
Copyright © 2019 Wolters Kluwer H
and mortality with the expanded Denver criteria. Surgery. 2018;164(3):494–499.
7. Weber CD, Lefering R, Kobbe P, Horst K, Pishnamaz M, Sellei RM,Hildebrand F, Pape HC, TraumaRegister DGU. Blunt cerebrovascular arteryinjury and stroke in severely injured patients: an international multicenteranalysis. World J Surg. 2018;42(7):2043–2053.
8. Tso MK, Lee MM, Ball CG, Morrish WF, Mitha AP, Kirkpatrick AW,Wong JH. Clinical utility of a screening protocol for blunt cerebrovascular in-jury using computed tomography angiography. J Neurosurg. 2017;126(4):1033–1041.
9. Miller PR, Fabian TC, Croce MA, Cagiannos C, Williams JS, Vang M,QaisiWG, Felker RE, Timmons SD. Prospective screening for blunt cerebro-vascular injuries: analysis of diagnostic modalities and outcomes. Ann Surg.2002;236(3):386–393.
10. Shahan CP, Magnotti LJ, McBeth PB, Weinberg JA, Croce MA, Fabian TC.Early antithrombotic therapy is safe and effective in patients with blunt cere-brovascular injury and solid organ injury or traumatic brain injury. J TraumaAcute Care Surg. 2016;81:173–177.
11. McNutt MK, Kale AC, Kitagawa RS, Turkmani AH, Fields DW, Baraniuk S,Gill BS, Cotton BA,Moore LJ,Wade CE,DayA, Holcomb JB.Managementof blunt cerebrovascular injury (BCVI) in themultisystem injury patient withcontraindications to immediate anti-thrombotic therapy. Injury. 2018;49:67–74.
12. Shahan CP, Magnotti LJ, Stickley SM, Weinberg JA, Hendrick LE,Uhlmann RA, Schroeppel TJ, Hoit DA, Croce MA, Fabian TC. A safe andeffective management strategy for blunt cerebrovascular injury: avoiding un-necessary anticoagulation and eliminating stroke. J Trauma Acute CareSurg. 2016;80(6):915–922.
13. Grandhi R, Weiner GM, Agarwal N, Panczykowski DM, Ares WJ,Rodriguez JS, Gelfond JA, Myers JG, Alarcon LH, Okonkwo DO, et al.Limitations of multidetector computed tomography angiography for thediagnosis of blunt cerebrovascular injury. J Neurosurg. 2018;128(6):1642–1647.
14. Lytle ME, West J, Burkes JN, Beteck B, Fisher T, Daoud Y, Gable DR,Shutze WP. Limited clinical relevance of vertebral artery injury in blunttrauma. Ann Vasc Surg. 2018;53:53–62. Epub 2018 Jul 25.
15. Scott WW, Sharp S, Figueroa SA, Madden CJ, Rickert KL. Clinical andradiological outcomes following traumatic grade 1 and 2 vertebral arteryinjuries: a 10-year retrospective analysis from a level 1 trauma center.J Neurosurg. 2014;121(2):450–456.
16. Stein DM, Boswell S, Sliker CW, Lui FY, Scalea TM. Blunt cerebrovascularinjuries: does treatment always matter? J Trauma. 2009;66:132–144.
17. Biffl WL, Ray CE Jr, Moore EE, Mestek M, Johnson JL, Burch JM.Noninvasive diagnosis of blunt cerebrovascular injuries: a preliminaryreport. J Trauma. 2002;53(5):850–856.
18. Vertinsky AT, Schwartz NE, Fischbein NJ, Rosenberg J, Albers GW,Zaharchuk G. Comparison of multidetector CT angiography and MR im-aging of cervical artery dissection. AJNR Am J Neuroradiol. 2008;29(9):1753–1760.
19. Hunter MA, Santosh C, Teasdale E, Forbes KP. High-resolution double in-version recovery black-blood imaging of cervical artery dissection using3T MR imaging. AJNR Am J Neuroradiol. 2012;33:E133–E137.
20. Provenzale JM, Sarikaya B. Comparison of test performance characteristicsof MRI, MR angiography, and CT angiography in the diagnosis of carotidand vertebral artery dissection: a review of the medical literature. AJR AmJ Roentgenol. 2009;193(4):1167–1174.
© 2019 American Association for the Surgery of Trauma.
ealth, Inc. All rights reserved.

ORIGINAL ARTICLE
Identifying patients with time-sensitive injuries: Association ofmortality with increasing prehospital time
Xilin Chen, MPH, Francis X. Guyette, MD, MPH, Andrew B. Peitzman, MD, Timothy R. Billiar, MD,Jason L. Sperry, MD, MPH, and Joshua B. Brown, MD, MSc, Pittsburgh, Pennsylvania
Sub
Fro
The
Ad
Sup
DO
J TrVol
BACKGROUND: T
mitted: November 21, 2018, Re2019, Published online: Marchm the Division of General SurgeP., T.R.B., J.L.S., J.B.B.B), and Dversity of Pittsburgh Medical Cse data were presented as a posAmerican Association for theSan Diego, CA.dress for reprints: Joshua B. BroTrauma, Department of SurgeLothrop Street, Pittsburgh, PAplemental digital content is avaithe printed text, and links to thearticle on the journal’s Web sit
I: 10.1097/TA.00000000000022
auma Acute Care Surgume 86, Number 6
rauma is a time-sensitive disease. However, recognizingwhich patients have time-critical injuries in the field is challenging.Manystudies failed to identify an association between increasing prehospital time (PHT) andmortality due to evaluation of heterogenoustrauma patients, as well as inherent survival bias frommissed deaths in patients with long PHT. Our objective was to determine if asubset of existing trauma triage criteria can identify patients in whom mortality is associated with PHT.
METHODS: T
rauma patients 16 years or older transported from the scene in the National Trauma Databank 2007 to 2015 were included. Cubicspline analysis used to identify an inflection where mortality increases to identify a marginal population in which PHT is morelikely associatedwith mortality and exclude biased patients with long PHT. Logistic regression determined the association betweenmortality and PHT, adjusting for demographics, transport mode, vital signs, operative interventions, and complications. Interactionterms between existing trauma triage criteria and PHTwere tested, with model stratification across triage criteria with a significantinteraction to determine which criteria identify patients that have increased risk of mortality associated with increasing PHT.RESULTS: M
ortality risk increased in patients with total PHT of 30 minutes or less, comprising a study population of 517,863 patients. Me-dian total PHTwas 26 minutes (interquartile range, 22–28 minutes) with median Injury Severity Score of 9 (interquartile range,4–14) and 7.4%mortality. Overall, PHTwas not associated with mortality (adjusted odd ratio [AOR], 0.984 per 5-minute increase;95% confidence interval [CI], 0.960–1.009; p = 0.20). Interaction analysis demonstrated increased mortality associated with in-creasing PHT for patients with systolic blood pressure less than 90 mm Hg (AOR, 1.039; 95% CI, 1.003–1.078, p = 0.04), Glas-gow Coma Scale score of 8 or less (AOR, 1.047; 95% CI, 1.018–1.076; p < 0.01), or nonextremity firearm injury (AOR, 1.049;95% CI, 1.010–1.089; p < 0.01).CONCLUSION: P
atients with prehospital hypotension, Glasgow Coma Scale score of 8 or less, and nonextremity firearm injury have highermortality with increasing PHT. These patients may have time-sensitive injuries and benefit from rapid transport to definitive care.(J Trauma Acute Care Surg. 2019;86: 1015–1022. Copyright © 2019 American Association for the Surgery of Trauma.)LEVEL OF EVIDENCE: P
rognostic/Epidemiologic III; Therapeutic/Care Management IV. KEYWORDS: E mergency medical services; prehospital; transport; time; triage.T rauma is a time-sensitive disease. This has been embodiedby the “golden hour” concept.1 The underlying theory is that
minimizing the time from injury to definitive care at a traumacenter improves outcomes. This has led to the “scoop and run”approach to emergency medical services (EMS) in which rapidtransport is favored with few or no prehospital interventions.2
However, many studies have not identified an association be-tween increasing prehospital time and mortality, calling intoquestion this tenet of trauma care.3–8
This lack of relationship between prehospital time andoutcome may have been seen in prior studies for two reasons.
vised: February 13, 2019, Accepted: February 22,11, 2019.ry and Trauma, Department of Surgery (X.C., A.B.epartment of EmergencyMedicine (F.X.G.), Uni-enter, Pittsburgh, Pennsylvania.ter presentation at the 77th Annual Meeting of theSurgery of Trauma, September 26-29th, 2018 in
wn, MD, MSc, Division of General Surgery andry, University of Pittsburgh Medical Center, 20015213; email: [email protected] for this article. Direct URL citations appear indigital files are provided in the HTML text of thise (www.jtrauma.com).
51
Copyright © 2019 Wolters Kluwer H
First is the inherent survival bias in trauma registry data usedin prior studies. Registry data are collected from only patientsbrought to a participating trauma center. Thus, patients fartherfrom the trauma center with long prehospital times that survivelong enough to get to the trauma center are likely to survive theirinjuries. Patients far from the trauma center who die in the fieldor at a closer nontrauma center are not captured. Only patientsthat survive to arrive at the trauma center are included in registrydata and bias the true relationship between prehospital time andmortality for patients with longer prehospital times. This may re-sult in paradoxical findings in which longer prehospital time ap-pears to be associated with lower mortality.
Second, prior studies evaluate a heterogenous popula-tion of all trauma patients. Ultimately, many patients do nothave time-sensitive injuries. Absence of any selection criteriaproduces a heterogenous population in which prehospitaltime is unlikely to be associated with mortality. The key issuebecomes recognizing which patients have time critical inju-ries in the field. However, this remains challenging, as EMSproviders have few resources to identify these patients andact accordingly. To our knowledge, no prior studies have evalu-ated whether injured patients with time-sensitive injuries couldbe identified in the field. Triage criteria that identify time-sensitive trauma patients represent actionable information forEMS providers, allowing them to prioritize rapid transport with
1015
ealth, Inc. All rights reserved.

Chen et alJ Trauma Acute Care Surg
Volume 86, Number 6
scoop and run or activating helicopter EMS (HEMS) to mini-mize prehospital time.
Thus, it was our objective to determine if a subset ofexisting field trauma triage criteria can identify patients in whommortality is associated with increasing prehospital time after ac-counting for potential survival bias.
METHODS
Study PopulationAll patients 16 years or older transported by EMS from
the scene in the National Trauma Databank (NTDB) 2007 to2015 were included. Patients with burn injury, missing totalprehospital time, or total prehospital time greater than 3 hourswere excluded. Prehospital times longer than 3 hours were ex-cluded as this is greater than 90th percentile of total prehospitaltime in the data set and are not representative of typical EMStransports across the United States. A subset of these patientswas studied in further detail using the Pennsylvania TraumaOutcomes Study (PTOS) 2007–2015. The PTOS includes moredetailed prehospital data to allow further exploratory analysis offactors affecting prehospital time. The same inclusion/exclusioncriteria and definitions were applied to the PTOS subset.
Total prehospital time was defined as the time elapsedfrom dispatch of EMS by the 911-system to arrival of EMS withthe patient at the hospital. This incorporates three intervals ofprehospital time, including response (time from dispatch to ar-rival at the scene), scene (time from arrival at the scene to leavingthe scene), and transport time (time from leaving the scene tohospital arrival). Total prehospital time was chosen because it ac-counts for the entire prehospital care period and each time intervalcomponent may be modifiable through different strategies.
Missing DataMultiple imputation was performed to account for the
missing values. Imputed variables included sex, race, insurancestatus, Injury Severity Score (ISS), admission systolic bloodpressure (SBP), and mechanism of injury. Multiple imputationusing chained equations developed five imputed data sets. Out-come models combined coefficients and standard errors fromeach imputed data set while adjusting for the variability betweenimputed data sets.9 Missing data for imputed variables rangedfrom 0.1% (mechanism, PTOS) to 12.9% (insurance status,NTDB). Sensitivity analysis with complete cases was performedand similar results were seen, thus results from imputed data arepresented below. Imputation was not used for variables affectingtriage criteria (prehospitalGlasgowComaScale [GCS], SBP, respira-tory rate [RR]). These variables were not imputed as different valuescould be imputed for themissing observations in each of the five im-puted data sets. Thus, a patient might have a positive triage criterionin some but not all imputed data sets for criteria using thesevariables.This would make it impossible to analyze a stratified sample basedon interaction testing if the criterion was different within the samepatient across imputed data sets. Prehospital GCS, SBP, RR weremissing in 5.1%, 7.0%, and 5.2% of patients respectively.
Survival BiasSince the databases utilized suffer from the survival bias
noted above, we addressed this by excluding patients with long
1016
Copyright © 2019 Wolters Kluwer H
prehospital times which represent a biased group where only pa-tients surviving long enough to reach a trauma center were cap-tured in the data sets. We sought the prehospital timeframewheremortality drops off and remains relatively constant to identify thisbiased group. To determine the prehospital time threshold to ex-clude this biased group, we used restricted cubic spline analysiswhich evaluates the nonlinear relationship between mortalityand prehospital time. This allowed us to empirically select theprehospital time threshold to exclude patients with longer timesbased on data rather than using an arbitrary threshold.
Restricted cubic splines were created for total prehospitaltime with 3 knots. Logistic regression was then performed withmortality as the dependent variable and the cubic splines as theindependent variables. The adjusted odds ratio (AOR) and95% confidence interval (95% CI) were estimated for each min-ute of total prehospital time relative to 180 minutes. The AORand 95% CI were plotted across prehospital time. This identifieda marginal population with a shorter prehospital timeframe thatallowed patients to reach a trauma center regardless of injury se-verity and would be less likely to suffer from survival bias. Allfurther analyses were performed only on patients within thisprehospital timeframe.
Statistical AnalysisThe primary outcome was in-hospital mortality. Logistic
regression was used to determine the association between in-hospital mortality and total prehospital time. Total prehospitaltime was evaluated as a continuous variable. The model was ad-justed for age, sex, race, insurance status, transport mode, mech-anism of injury, ISS, prehospital SBP, admission SBP, need forurgent operation (emergency department disposition of operat-ing room), need for mechanical ventilation, in-hospital compli-cations, and trauma center level. Models were also adjusted forisolated severe (Abbreviated Injury Scale score ≥ 3) head, chest,or abdominal injury, as well as combinations of severe head,chest, or abdominal injury to account for differing anatomic pat-terns of injury. Interactions between prehospital time and ana-tomic injury pattern were tested to determine if prehospitaltime had a different effect onmortality based on the anatomic in-jury pattern. Robust variance estimatorswere used to account forclustering at the center level.
Existing triage criteria were evaluated to identify patentswith time-sensitive injuries, including SBP less than 90 mmHg, GCS score of 13 or less, GCS score of 8 or less, RR less than10 or greater than 29 bpm, penetrating injury, unstable chestwall, open skull fracture, two or more proximal long bone frac-tures, pelvic fracture, crush injury, amputation, paralysis, hemo-thorax or pneumothorax, multisystem trauma (≥3 body regionsinjured), and combination of physiologic plus anatomic triagecriteria from the national field triage guidelines.10 Penetratinginjury was further classified as firearm versus nonfirearm injurybased on external injury codes (e-codes), and nonextremity(head, face, neck, chest, abdomen, or spine) versus extremity lo-cation of penetrating injury based on Abbreviated Injury Scalebody regions. Interaction terms between these triage criteriaand total prehospital time were tested.
A significant interaction indicates prehospital time has adifferent effect on mortality based on the presence or absenceof the criterion. Models were stratified across triage criteria with
© 2019 American Association for the Surgery of Trauma.
ealth, Inc. All rights reserved.
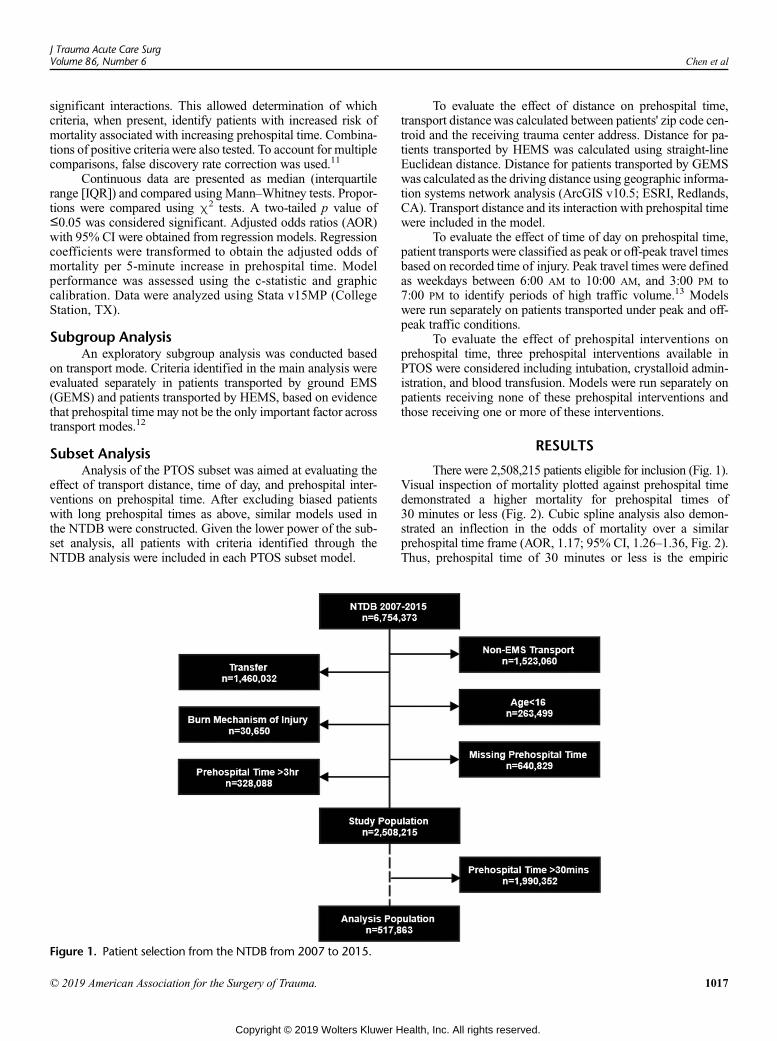
J Trauma Acute Care SurgVolume 86, Number 6 Chen et al
significant interactions. This allowed determination of whichcriteria, when present, identify patients with increased risk ofmortality associated with increasing prehospital time. Combina-tions of positive criteriawere also tested. To account for multiplecomparisons, false discovery rate correction was used.11
Continuous data are presented as median (interquartilerange [IQR]) and compared using Mann–Whitney tests. Propor-tions were compared using χ2 tests. A two-tailed p value of≤0.05 was considered significant. Adjusted odds ratios (AOR)with 95% CI were obtained from regression models. Regressioncoefficients were transformed to obtain the adjusted odds ofmortality per 5-minute increase in prehospital time. Modelperformance was assessed using the c-statistic and graphiccalibration. Data were analyzed using Stata v15MP (CollegeStation, TX).
Subgroup AnalysisAn exploratory subgroup analysis was conducted based
on transport mode. Criteria identified in the main analysis wereevaluated separately in patients transported by ground EMS(GEMS) and patients transported by HEMS, based on evidencethat prehospital time may not be the only important factor acrosstransport modes.12
Subset AnalysisAnalysis of the PTOS subset was aimed at evaluating the
effect of transport distance, time of day, and prehospital inter-ventions on prehospital time. After excluding biased patientswith long prehospital times as above, similar models used inthe NTDB were constructed. Given the lower power of the sub-set analysis, all patients with criteria identified through theNTDB analysis were included in each PTOS subset model.
Figure 1. Patient selection from the NTDB from 2007 to 2015.
© 2019 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer H
To evaluate the effect of distance on prehospital time,transport distancewas calculated between patients' zip code cen-troid and the receiving trauma center address. Distance for pa-tients transported by HEMS was calculated using straight-lineEuclidean distance. Distance for patients transported by GEMSwas calculated as the driving distance using geographic informa-tion systems network analysis (ArcGIS v10.5; ESRI, Redlands,CA). Transport distance and its interaction with prehospital timewere included in the model.
To evaluate the effect of time of day on prehospital time,patient transports were classified as peak or off-peak travel timesbased on recorded time of injury. Peak travel times were definedas weekdays between 6:00 AM to 10:00 AM, and 3:00 PM to7:00 PM to identify periods of high traffic volume.13 Modelswere run separately on patients transported under peak and off-peak traffic conditions.
To evaluate the effect of prehospital interventions onprehospital time, three prehospital interventions available inPTOS were considered including intubation, crystalloid admin-istration, and blood transfusion. Models were run separately onpatients receiving none of these prehospital interventions andthose receiving one or more of these interventions.
RESULTS
There were 2,508,215 patients eligible for inclusion (Fig. 1).Visual inspection of mortality plotted against prehospital timedemonstrated a higher mortality for prehospital times of30 minutes or less (Fig. 2). Cubic spline analysis also demon-strated an inflection in the odds of mortality over a similarprehospital time frame (AOR, 1.17; 95% CI, 1.26–1.36, Fig. 2).Thus, prehospital time of 30 minutes or less is the empiric
1017
ealth, Inc. All rights reserved.
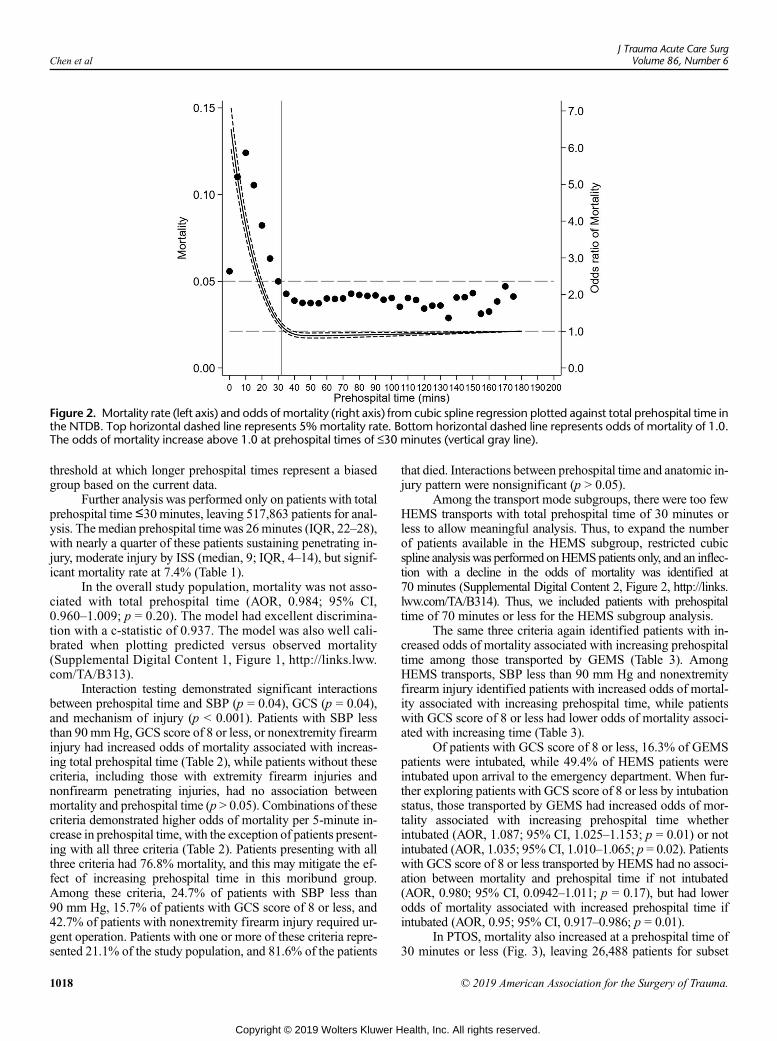
Figure 2. Mortality rate (left axis) and odds of mortality (right axis) from cubic spline regression plotted against total prehospital time inthe NTDB. Top horizontal dashed line represents 5% mortality rate. Bottom horizontal dashed line represents odds of mortality of 1.0.The odds of mortality increase above 1.0 at prehospital times of ≤30 minutes (vertical gray line).
Chen et alJ Trauma Acute Care Surg
Volume 86, Number 6
threshold at which longer prehospital times represent a biasedgroup based on the current data.
Further analysis was performed only on patients with totalprehospital time≤30minutes, leaving 517,863 patients for anal-ysis. Themedian prehospital timewas 26minutes (IQR, 22–28),with nearly a quarter of these patients sustaining penetrating in-jury, moderate injury by ISS (median, 9; IQR, 4–14), but signif-icant mortality rate at 7.4% (Table 1).
In the overall study population, mortality was not asso-ciated with total prehospital time (AOR, 0.984; 95% CI,0.960–1.009; p = 0.20). The model had excellent discrimina-tion with a c-statistic of 0.937. The model was also well cali-brated when plotting predicted versus observed mortality(Supplemental Digital Content 1, Figure 1, http://links.lww.com/TA/B313).
Interaction testing demonstrated significant interactionsbetween prehospital time and SBP (p = 0.04), GCS (p = 0.04),and mechanism of injury (p < 0.001). Patients with SBP lessthan 90 mmHg, GCS score of 8 or less, or nonextremity firearminjury had increased odds of mortality associated with increas-ing total prehospital time (Table 2), while patients without thesecriteria, including those with extremity firearm injuries andnonfirearm penetrating injuries, had no association betweenmortality and prehospital time (p > 0.05). Combinations of thesecriteria demonstrated higher odds of mortality per 5-minute in-crease in prehospital time, with the exception of patients present-ing with all three criteria (Table 2). Patients presenting with allthree criteria had 76.8% mortality, and this may mitigate the ef-fect of increasing prehospital time in this moribund group.Among these criteria, 24.7% of patients with SBP less than90 mm Hg, 15.7% of patients with GCS score of 8 or less, and42.7% of patients with nonextremity firearm injury required ur-gent operation. Patients with one or more of these criteria repre-sented 21.1% of the study population, and 81.6% of the patients
1018
Copyright © 2019 Wolters Kluwer H
that died. Interactions between prehospital time and anatomic in-jury pattern were nonsignificant (p > 0.05).
Among the transport mode subgroups, there were too fewHEMS transports with total prehospital time of 30 minutes orless to allow meaningful analysis. Thus, to expand the numberof patients available in the HEMS subgroup, restricted cubicspline analysiswas performed onHEMSpatients only, and an inflec-tion with a decline in the odds of mortality was identified at70 minutes (Supplemental Digital Content 2, Figure 2, http://links.lww.com/TA/B314). Thus, we included patients with prehospitaltime of 70 minutes or less for the HEMS subgroup analysis.
The same three criteria again identified patients with in-creased odds of mortality associated with increasing prehospitaltime among those transported by GEMS (Table 3). AmongHEMS transports, SBP less than 90 mm Hg and nonextremityfirearm injury identified patients with increased odds of mortal-ity associated with increasing prehospital time, while patientswith GCS score of 8 or less had lower odds of mortality associ-ated with increasing time (Table 3).
Of patients with GCS score of 8 or less, 16.3% of GEMSpatients were intubated, while 49.4% of HEMS patients wereintubated upon arrival to the emergency department. When fur-ther exploring patients with GCS score of 8 or less by intubationstatus, those transported by GEMS had increased odds of mor-tality associated with increasing prehospital time whetherintubated (AOR, 1.087; 95% CI, 1.025–1.153; p = 0.01) or notintubated (AOR, 1.035; 95% CI, 1.010–1.065; p = 0.02). Patientswith GCS score of 8 or less transported by HEMS had no associ-ation between mortality and prehospital time if not intubated(AOR, 0.980; 95% CI, 0.0942–1.011; p = 0.17), but had lowerodds of mortality associated with increased prehospital time ifintubated (AOR, 0.95; 95% CI, 0.917–0.986; p = 0.01).
In PTOS, mortality also increased at a prehospital time of30 minutes or less (Fig. 3), leaving 26,488 patients for subset
© 2019 American Association for the Surgery of Trauma.
ealth, Inc. All rights reserved.
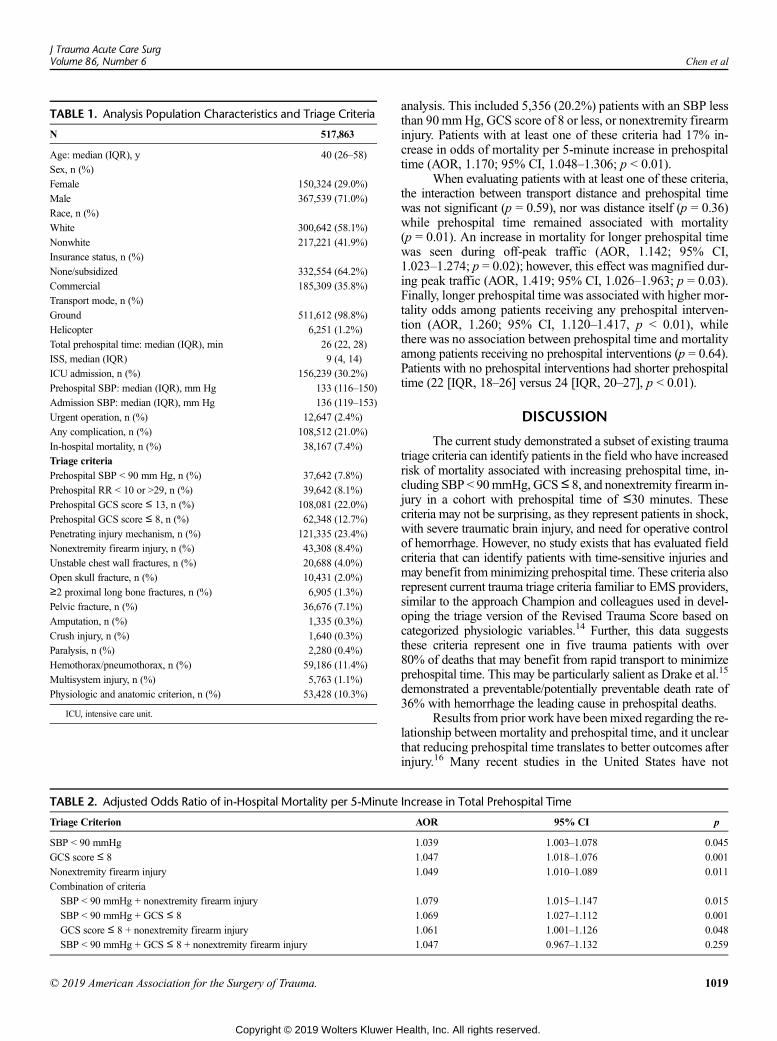
TABLE 2. Adjusted Odds Ratio of in-Hospital Mortality per 5-Minute
Triage Criterion
SBP < 90 mmHg
GCS score ≤ 8
Nonextremity firearm injury
Combination of criteria
SBP < 90 mmHg + nonextremity firearm injury
SBP < 90 mmHg + GCS ≤ 8
GCS score ≤ 8 + nonextremity firearm injury
SBP < 90 mmHg + GCS ≤ 8 + nonextremity firearm injury
TABLE 1. Analysis Population Characteristics and Triage Criteria
N 517,863
Age: median (IQR), y 40 (26–58)
Sex, n (%)
Female 150,324 (29.0%)
Male 367,539 (71.0%)
Race, n (%)
White 300,642 (58.1%)
Nonwhite 217,221 (41.9%)
Insurance status, n (%)
None/subsidized 332,554 (64.2%)
Commercial 185,309 (35.8%)
Transport mode, n (%)
Ground 511,612 (98.8%)
Helicopter 6,251 (1.2%)
Total prehospital time: median (IQR), min 26 (22, 28)
ISS, median (IQR) 9 (4, 14)
ICU admission, n (%) 156,239 (30.2%)
Prehospital SBP: median (IQR), mm Hg 133 (116–150)
Admission SBP: median (IQR), mm Hg 136 (119–153)
Urgent operation, n (%) 12,647 (2.4%)
Any complication, n (%) 108,512 (21.0%)
In-hospital mortality, n (%) 38,167 (7.4%)
Triage criteria
Prehospital SBP < 90 mm Hg, n (%) 37,642 (7.8%)
Prehospital RR < 10 or >29, n (%) 39,642 (8.1%)
Prehospital GCS score ≤ 13, n (%) 108,081 (22.0%)
Prehospital GCS score ≤ 8, n (%) 62,348 (12.7%)
Penetrating injury mechanism, n (%) 121,335 (23.4%)
Nonextremity firearm injury, n (%) 43,308 (8.4%)
Unstable chest wall fractures, n (%) 20,688 (4.0%)
Open skull fracture, n (%) 10,431 (2.0%)
≥2 proximal long bone fractures, n (%) 6,905 (1.3%)
Pelvic fracture, n (%) 36,676 (7.1%)
Amputation, n (%) 1,335 (0.3%)
Crush injury, n (%) 1,640 (0.3%)
Paralysis, n (%) 2,280 (0.4%)
Hemothorax/pneumothorax, n (%) 59,186 (11.4%)
Multisystem injury, n (%) 5,763 (1.1%)
Physiologic and anatomic criterion, n (%) 53,428 (10.3%)
ICU, intensive care unit.
J Trauma Acute Care SurgVolume 86, Number 6 Chen et al
© 2019 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer H
analysis. This included 5,356 (20.2%) patients with an SBP lessthan 90 mmHg, GCS score of 8 or less, or nonextremity firearminjury. Patients with at least one of these criteria had 17% in-crease in odds of mortality per 5-minute increase in prehospitaltime (AOR, 1.170; 95% CI, 1.048–1.306; p < 0.01).
When evaluating patients with at least one of these criteria,the interaction between transport distance and prehospital timewas not significant (p = 0.59), nor was distance itself (p = 0.36)while prehospital time remained associated with mortality(p = 0.01). An increase in mortality for longer prehospital timewas seen during off-peak traffic (AOR, 1.142; 95% CI,1.023–1.274; p = 0.02); however, this effect was magnified dur-ing peak traffic (AOR, 1.419; 95% CI, 1.026–1.963; p = 0.03).Finally, longer prehospital time was associated with higher mor-tality odds among patients receiving any prehospital interven-tion (AOR, 1.260; 95% CI, 1.120–1.417, p < 0.01), whilethere was no association between prehospital time and mortalityamong patients receiving no prehospital interventions (p = 0.64).Patients with no prehospital interventions had shorter prehospitaltime (22 [IQR, 18–26] versus 24 [IQR, 20–27], p < 0.01).
DISCUSSION
The current study demonstrated a subset of existing traumatriage criteria can identify patients in the field who have increasedrisk of mortality associated with increasing prehospital time, in-cluding SBP < 90mmHg, GCS≤ 8, and nonextremity firearm in-jury in a cohort with prehospital time of ≤30 minutes. Thesecriteria may not be surprising, as they represent patients in shock,with severe traumatic brain injury, and need for operative controlof hemorrhage. However, no study exists that has evaluated fieldcriteria that can identify patients with time-sensitive injuries andmay benefit fromminimizing prehospital time. These criteria alsorepresent current trauma triage criteria familiar to EMS providers,similar to the approach Champion and colleagues used in devel-oping the triage version of the Revised Trauma Score based oncategorized physiologic variables.14 Further, this data suggeststhese criteria represent one in five trauma patients with over80% of deaths that may benefit from rapid transport to minimizeprehospital time. This may be particularly salient as Drake et al.15
demonstrated a preventable/potentially preventable death rate of36% with hemorrhage the leading cause in prehospital deaths.
Results from prior work have beenmixed regarding the re-lationship between mortality and prehospital time, and it unclearthat reducing prehospital time translates to better outcomes afterinjury.16 Many recent studies in the United States have not
Increase in Total Prehospital Time
AOR 95% CI p
1.039 1.003–1.078 0.045
1.047 1.018–1.076 0.001
1.049 1.010–1.089 0.011
1.079 1.015–1.147 0.015
1.069 1.027–1.112 0.001
1.061 1.001–1.126 0.048
1.047 0.967–1.132 0.259
1019
ealth, Inc. All rights reserved.
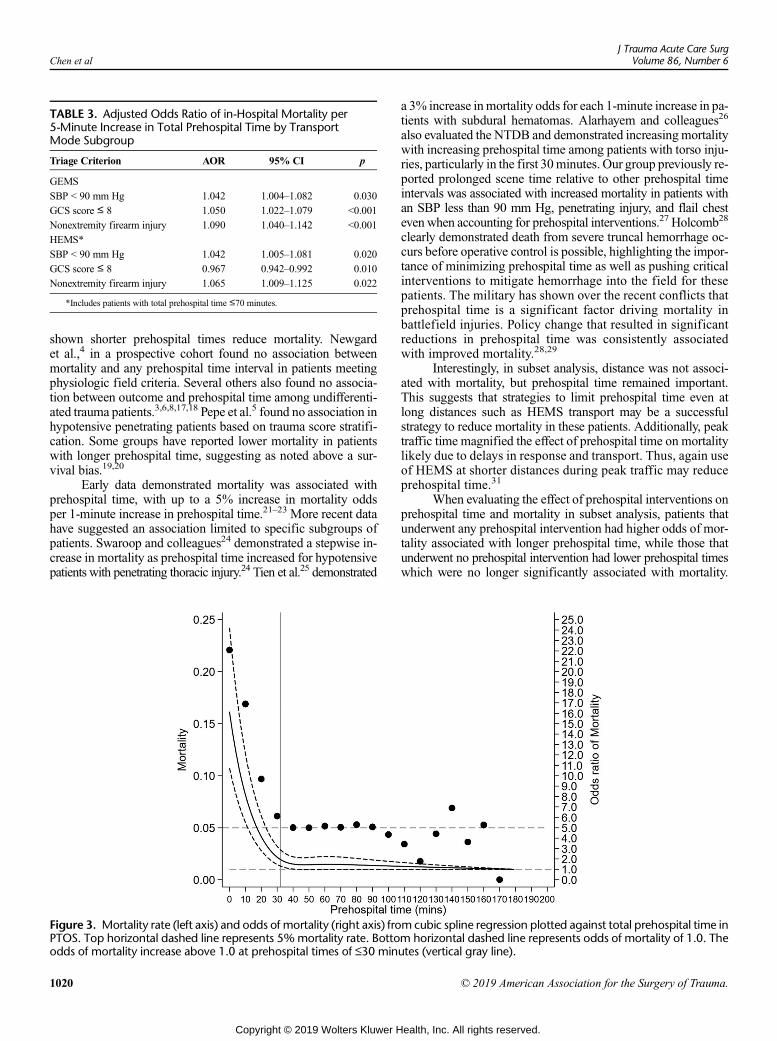
TABLE 3. Adjusted Odds Ratio of in-Hospital Mortality per5-Minute Increase in Total Prehospital Time by TransportMode Subgroup
Triage Criterion AOR 95% CI p
GEMS
SBP < 90 mm Hg 1.042 1.004–1.082 0.030
GCS score ≤ 8 1.050 1.022–1.079 <0.001
Nonextremity firearm injury 1.090 1.040–1.142 <0.001
HEMS*
SBP < 90 mm Hg 1.042 1.005–1.081 0.020
GCS score ≤ 8 0.967 0.942–0.992 0.010
Nonextremity firearm injury 1.065 1.009–1.125 0.022
*Includes patients with total prehospital time ≤70 minutes.
Chen et alJ Trauma Acute Care Surg
Volume 86, Number 6
shown shorter prehospital times reduce mortality. Newgardet al.,4 in a prospective cohort found no association betweenmortality and any prehospital time interval in patients meetingphysiologic field criteria. Several others also found no associa-tion between outcome and prehospital time among undifferenti-ated trauma patients.3,6,8,17,18 Pepe et al.5 found no association inhypotensive penetrating patients based on trauma score stratifi-cation. Some groups have reported lower mortality in patientswith longer prehospital time, suggesting as noted above a sur-vival bias.19,20
Early data demonstrated mortality was associated withprehospital time, with up to a 5% increase in mortality oddsper 1-minute increase in prehospital time.21–23 More recent datahave suggested an association limited to specific subgroups ofpatients. Swaroop and colleagues24 demonstrated a stepwise in-crease in mortality as prehospital time increased for hypotensivepatients with penetrating thoracic injury.24 Tien et al.25 demonstrated
Figure 3. Mortality rate (left axis) and odds of mortality (right axis) froPTOS. Top horizontal dashed line represents 5%mortality rate. Bottoodds of mortality increase above 1.0 at prehospital times of ≤30 min
1020
Copyright © 2019 Wolters Kluwer H
a 3% increase inmortality odds for each 1-minute increase in pa-tients with subdural hematomas. Alarhayem and colleagues26
also evaluated the NTDB and demonstrated increasingmortalitywith increasing prehospital time among patients with torso inju-ries, particularly in the first 30minutes. Our group previously re-ported prolonged scene time relative to other prehospital timeintervals was associated with increased mortality in patients withan SBP less than 90 mm Hg, penetrating injury, and flail chesteven when accounting for prehospital interventions.27 Holcomb28
clearly demonstrated death from severe truncal hemorrhage oc-curs before operative control is possible, highlighting the impor-tance of minimizing prehospital time as well as pushing criticalinterventions to mitigate hemorrhage into the field for thesepatients. The military has shown over the recent conflicts thatprehospital time is a significant factor driving mortality inbattlefield injuries. Policy change that resulted in significantreductions in prehospital time was consistently associatedwith improved mortality.28,29
Interestingly, in subset analysis, distance was not associ-ated with mortality, but prehospital time remained important.This suggests that strategies to limit prehospital time even atlong distances such as HEMS transport may be a successfulstrategy to reduce mortality in these patients. Additionally, peaktraffic time magnified the effect of prehospital time on mortalitylikely due to delays in response and transport. Thus, again useof HEMS at shorter distances during peak traffic may reduceprehospital time.31
When evaluating the effect of prehospital interventions onprehospital time and mortality in subset analysis, patients thatunderwent any prehospital intervention had higher odds of mor-tality associated with longer prehospital time, while those thatunderwent no prehospital intervention had lower prehospital timeswhich were no longer significantly associated with mortality.
mcubic spline regression plotted against total prehospital time inm horizontal dashed line represents odds of mortality of 1.0. Theutes (vertical gray line).
© 2019 American Association for the Surgery of Trauma.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 6 Chen et al
This suggests for patients meeting one of the time-sensitivecriteria, a scoop and run approach may be favored as the timeto perform field interventions results in an increase in mortalityas prehospital time increases.
These findings have several potential implications. At theindividual patient level, these criteria may help EMS providersmake decisions about if and when to provide prehospital inter-ventions based on the presence or absence of the criteria demon-strated here. These criteria allow EMS providers to take a moretailored approach to their patients, applying a scoop and run ap-proach in patients who may truly benefit from it. This also mayallow mitigation of risk to EMS providers and the public byinforming appropriate utilization strategies for HEMS or useof lights and sirens transport.31,32 At the system level, thesecriteria may be considered in triage protocols to encourage min-imization of scene time. They may facilitate performance im-provement review to identify opportunities to reduce delays inpatients meeting these criteria. These potential clinical and pol-icy implications require further targeted study prior to consider-ation of wide-spread application.
In our transport mode subgroup analysis, patients transportedby GEMS had increasing mortality associated with increasingprehospital time across all three criteria, while HEMS patientsonly had this relationship if they had an SBP less than 90mmHgor nonextremity firearm injury. However, HEMS patients hadlower mortality associated with increasing prehospital time ifthey had a GCS score of 8 or less. When investigating the poten-tial role of prehospital intubation in patients with a GCS score of8 or less, lower mortality was associated with longer prehospitaltime in patients intubated by HEMS crews, while increasedmor-tality was associated with increasing prehospital time in GEMSpatients regardless of intubation status. The point estimate formortality odds was more than double for patients who wereintubated compared with those not intubated by GEMS crews.
These finding suggest prehospital intubation significantlyaffects outcomes for injured patients with a GCS score of 8 orless. Further, that effect is different across transport modes,and the additional time to perform intubation in the fieldmay improve outcome in the hands of HEMS but not GEMSproviders, which has been supported by prior reports aswell.12,33–35 GEMS and HEMS differ with respect to training,experience, and regulatory requirements. Additionally, theremay be some selection bias as GEMS in some locations can-not perform medication assisted intubation. Mounting evi-dence suggests the speed of HEMS transport is not the onlyimportant factor, and the care received by HEMS crews influ-ences outcome.12,36,37 These findings may also have implica-tions for air medical triage policies in which HEMS may beconsidered if it would ultimately reduce prehospital time for patientswith these criteria, or prehospital intubation is indicated for a GCSscore of 8 or less.
Taking the subset and transport subgroup data together,our results suggest patients with SBP less than 90 mm Hg andnonextremity firearm injury should undergo few if any prehospitalinterventions with priority placed on rapid transport to minimizeprehospital time, while patients with a GCS score of 8 or lessbenefit from undergoing prehospital intubation by HEMS pro-viders when available even if this may not result in the shortestprehospital time possible.
© 2019 American Association for the Surgery of Trauma.
Copyright © 2019 Wolters Kluwer H
There are several limitations for consideration. First arethose inherent to a retrospective observational design. Secondare those documented for the NTDB.38 The advantage of theNTDB is a large national sample of patients; however, there arelimited outcomes and variables for analysis. We supplementedthis limitation by performing a subset analysis using the PTOSdata set which included more granular prehospital data. Missingdata are always a limitation of registry studies; however, we usedmultiple imputation to mitigate this. Despite our large sample inthe NTDB, cohorting based on triage criteria resulted in somesmall groups that limited our power to evaluate the relationshipof mortality and prehospital time. This is a particular limitationin the PTOS subset analysis, requiring evaluation of patientswith any one of the three criteria identified in NTDB tomaintainadequate power for regression modeling.
As noted above, we restricted analysis to prehospital timesof 30 minutes or less to address the survival bias inherent to longprehospital times in registry data based on empirical analysis ofthe data sets utilized. This represents a trade-off in which we didnot evaluate longer prehospital times where there may be evenmore opportunity to minimize prehospital time, and limits ourgeneralizability. Our data likely are more representative of urban/suburban environments relatively close to trauma centers. Thisis particularly important in potential urban-rural differences ofthe prehospital time and outcome relationship, where differentcriteria may be useful across different geographies. We also donot have the time from injury to 911-system notification whichmay be significant in some patients. A number of patients weremissing prehospital time and excluded; however, this repre-sented only 9% of eligible patients.
Our primary outcome was in-hospital mortality; however,longer-term outcomes and morbidity not available in the NTDB orPTOS are important outcomes for injured patients. Our subgroupand subset analyses are exploratory and should beviewed tomotivatefuture research. We included HEMS patients with a prehospital timeof 70 minutes or longer in subgroup analysis for power reasons;however, this cutoff was based on data from similar cubic splineanalysis used for the main analysis. We investigated prehospitalintubation as a potential mechanism of the differences seen be-tween HEMS and GEMS among patients with a GCS score of8 or less; however, there was limited data available regardingtiming or other prehospital interventions and again is exploratory.
CONCLUSION
In patients with short total prehospital time, prehospitalhypotension, a GCS score of 8 or less, and nonextremity firearminjury identify patients with increased risk of mortality associ-ated with increasing prehospital time. These patients may havetruly time-sensitive injuries and benefit from rapid transport todefinitive care with few or no prehospital interventions. An ex-ception is patients with a GCS score of 8 or less that may benefitfrom intubation by HEMS providers. Further prospective re-search is necessary to refine the identification of patients withtime-sensitive injuries in the field and overcome the survivalbias for patients with longer prehospital times.
ACKNOWLEDGMENTS
Committee on Trauma, American College of Surgeons. NTDB 2007–2015,Chicago, IL. The content reproduced from the NTDB remains the full and
1021
ealth, Inc. All rights reserved.
Chen et alJ Trauma Acute Care Surg
Volume 86, Number 6
exclusive copyrighted property of the American College of Surgeons. TheAmerican College of Surgeons is not responsible for any claims arisingfrom works based on the original data, text, tables, or figures.
AUTHORSHIP
X.C., F.X.G., and J.B.B. designed the study and performed the literaturesearch. X.C. and J.B.B. performed the data collection. X.C. and J.B.B. per-formed the data analysis. X.C., F.X.G, and J.B.B. participated in initial arti-cle preparation. All authors contributed to data interpretation and criticalrevision of the article.
DISCLOSURE
The authors declare no conflicts of interest.
REFERENCES1. Lerner EB, Moscati RM. The golden hour: scientific fact or medical “urban
legend”? Acad Emerg Med. 2001;8:758–760.2. Seamon MJ, Fisher CA, Gaughan J, Lloyd M, Bradley KM, Santora TA,
Pathak AS, Goldberg AJ. Prehospital procedures before emergency depart-ment thoracotomy: “scoop and run” saves lives. J Trauma. 2007;63:113–120.
3. Lerner EB, Billittier AJ, Dorn JM, Wu YW. Is Total out-of-hospital time asignificant predictor of trauma patient mortality? Acad Emerg Med. 2003;10:949–954.
4. Newgard CD, Schmicker RH, Hedges JR, Trickett JP, Davis DP, Bulger EM,Aufderheide TP,Minei JP, Hata JS, Gubler KD, et al. Emergencymedical ser-vices intervals and survival in trauma: assessment of the “golden hour” in anorth American prospective cohort. Ann Emerg Med. 2010;55:235–246 e234.
5. Pepe PE, Wyatt CH, Bickell WH, Bailey ML, Mattox KL. The relationshipbetween total prehospital time and outcome in hypotensive victims of pene-trating injuries. Ann Emerg Med. 1987;16:293–297.
6. Petri RW, Dyer A, Lumpkin J. The effect of prehospital transport time on themortality from traumatic injury. Prehosp Disaster Med. 1995;10:24–29.
7. Pons PT,Markovchick VJ. Eight minutes or less: does the ambulance responsetime guideline impact trauma patient outcome? J Emerg Med. 2002;23:43–48.
8. Stiell IG, Nesbitt LP, Pickett W, Munkley D, Spaite DW, Banek J, Field B,Luinstra-Toohey L, Maloney J, Dreyer J, et al. The OPALS major traumastudy: impact of advanced life-support on survival and morbidity. CMAJ.2008;178:1141–1152.
9. Rubin DB. Multiple Imputation for Nonresponse in Surveys. Hoboken, NJ:John Wiley & Sons; 1987.
10. Sasser SM, Hunt RC, Faul M, Sugerman D, Pearson WS, Dulski T,WaldMM, Jurkovich GJ, Newgard CD, Lerner EB, et al. Guidelines for fieldtriage of injured patients.MMWR. 2012;61:1–20.
11. Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practicaland powerful approach tomultiple testing. J R Statist Soc B. 1995;57:289–300.
12. Chen X, Gestring ML, Rosengart MR, Billiar TR, Peitzman AB, Sperry JL,Brown JB. Speed is not everything: identifying patients who may benefitfrom helicopter transport despite faster ground transport. J Trauma AcuteCare Surg. 2018;84:549–557.
13. Schrank D, Eisele B, Lomax T, Bak J. 2015 UrbanMobility Score Card. Col-lege Station, Tx: Texas A&M Transportation Institute; 2015.
14. Champion HR, Sacco WJ, Copes WS, Gann DS, Gennarelli TA,Flanagan ME. A revision of the trauma score. J Trauma Acute Care Surg.1989;29:623–629.
15. Drake SA, Holcomb JB, Yang Y, Thetford C, Myers L, Brock M, Wolf DA,Cron S, Persse D, McCarthy J, et al. Establishing a regional traumapreventable/potentially preventable death rate. Ann Surg. 2018.
16. Harmsen AM, Giannakopoulos GF, Moerbeek PR, Jansma EP, Bonjer HJ,Bloemers FW. The influence of prehospital time on trauma patients outcome:a systematic review. Injury. 2015;46:602–609.
17. Baez AA, Lane PL, Sorondo B, Giraldez EM. Predictive effect of out-of-hospital time in outcomes of severely injured young adult and elderly pa-tients. Prehosp Disaster Med. 2006;21:427–430.
18. McCoy CE, Menchine M, Sampson S, Anderson C, Kahn C. Emergencymedical services out-of-hospital scene and transport times and their association
1022
Copyright © 2019 Wolters Kluwer H
withmortality in trauma patients presenting to an urban level I trauma center.Ann Emerg Med. 2013;61:167–174.
19. Osterwalder JJ. Can the “golden hour of shock” safely be extended in bluntpolytrauma patients? Prospective cohort study at a level I hospital in easternSwitzerland. Prehosp Disaster Med. 2002;17:75–80.
20. Ryb GE, Dischinger P, Cooper C, Kufera JA. Does helicopter transport im-prove outcomes independently of emergencymedical system time? J TraumaAcute Care Surg. 2013;74:149–154; discussion 154–146.
21. Sampalis JS, Denis R, Lavoie A, Frechette P, Boukas S, Nikolis A, Benoit D,Fleiszer D, Brown R, Churchill-Smith M, et al. Trauma care regionalization: aprocess-outcome evaluation. J Trauma Acute Care Surg. 1999;46:565–581.
22. Sampalis JS, Lavoie A,Williams JI, Mulder DS, Kalina M. Impact of on-sitecare, prehospital time, and level of in-hospital care on survival in severely in-jured patients. J Trauma. 1993;34:252–261.
23. Feero S, Hedges JR, Simmons E, Irwin L. Does out-of-hospital EMS timeaffect trauma survival? Am J Emerg Med. 1995;13:133–135.
24. SwaroopM, Straus DC, AgubuzuO, Esposito TJ, Schermer CR, CrandallML.Pre-hospital transport times and survival for hypotensive patientswith penetrat-ing thoracic trauma. J Emerg Trauma Shock. 2013;6:16–20.
25. Tien HC, Jung V, Pinto R, Mainprize T, Scales DC, Rizoli SB. Reducingtime-to-treatment decreases mortality of trauma patients with acute subduralhematoma. Ann Surg. 2011;253:1178–1183.
26. AlarhayemAQ,Myers JG, Dent D, Liao L,Muir M,Mueller D, Nicholson S,Cestero R, Johnson MC, Stewart R, et al. Time is the enemy: mortality intrauma patients with hemorrhage from torso injury occurs long before the“golden hour”. Am J Surg. 2016;212:1101–1105.
27. Brown JB, Rosengart MR, Forsythe RM, Reynolds BR, Gestring ML,Hallinan WM, Peitzman AB, Billiar TR, Sperry JL. Not all prehospital timeis equal: influence of scene time on mortality. J Trauma Acute Care Surg.2016;81:93–100.
28. Holcomb JB. Transport time and preoperating room hemostatic interventionsare important: Improving outcomes after severe truncal injury. Crit CareMed. 2018;46:447–453.
29. Howard JT, Kotwal RS, Santos-Lazada AR, Martin MJ, Stockinger ZT. Re-examination of a battlefield trauma golden hour policy. J Trauma Acute CareSurg. 2018;84:11–18.
30. Kotwal RS, Howard JT, Orman JA, Tarpey BW, Bailey JA, Champion HR,Mabry RL, Holcomb JB, Gross KR. The effect of a golden hour policy onthe morbidity and mortality of combat casualties. JAMA Surg. 2016;151:15–24.
31. Chen X, Gestring ML, Rosengart MR, Peitzman AB, Billiar TR, Sperry JL,Brown JB. Logistics of air medical transport: when and where does helicop-ter transport reduce prehospital time for trauma? J Trauma Acute Care Surg.2018;85:174–181.
32. Kahn CA, Pirrallo RG, Kuhn EM. Characteristics of fatal ambulance crashesin the United States: an 11-year retrospective analysis. Prehosp Emerg Care.2001;5:261–269.
33. CudnikMT, Newgard CD,WangH, Bangs C,Herrington R4th. Distance im-pacts mortality in trauma patients with an intubation attempt. Prehosp EmergCare. 2008;12:459–466.
34. Davis DP, Stern J, Sise MJ, Hoyt DB. A follow-up analysis of factors asso-ciated with head-injury mortality after paramedic rapid sequence intubation.J Trauma. 2005;59:486–490.
35. Wang HE, Peitzman AB, Cassidy LD, Adelson PD, Yealy DM. Out-of-hospital endotracheal intubation and outcome after traumatic brain injury.Ann Emerg Med. 2004;44:439–450.
36. Brown JB, Gestring ML, Guyette FX, Rosengart MR, Stassen NA, Forsythe RM,Billiar TR, Peitzman AB, Sperry JL. Helicopter transport improves survivalfollowing injury in the absence of a time-saving advantage. Surgery. 2016;159:947–959.
37. Holcomb JB, Donathan DP, Cotton BA, Del Junco DJ, Brown G,Wenckstern TV, Podbielski JM, Camp EA, Hobbs R, Bai Y, et al. Prehospitaltransfusion of plasma and red blood cells in trauma patients. Prehosp EmergCare. 2014;19:1–9.
38. American College of Surgeons. NTDB Research Data Set User Manual andVariable Description List. American College of Surgeons; 2017.
© 2019 American Association for the Surgery of Trauma.
ealth, Inc. All rights reserved.

ORIGINAL ARTICLE
Establishing the first Hartford consensus-compliant medicalschool in the United States
Jeremy Fridling, BA, Christine Van Cott, MD,Pina Violano, PhD, MSPH, and Lenworth Jacobs, Jr, MD, MPH, North Haven, Connecticut
Sub
Fro
Ad
DO
J TrVol
BACKGROUND: F
mitted: August 23, 2012018, Published onlinm the FrankH. Netter,C.), Frank H. Netter Mvention, Community Opital, New Haven; DeJr.), University of Contute (L.J.Jr.), Hartforddress for reprints: JereHamden, CT 06518; em
I: 10.1097/TA.000000
auma Acute Care Suume 86, Number 6
ollowing the Hartford Consensus meetings, the Stop the Bleed Campaign was created to reduce the prevalence of death from exsan-guination in the case of traumatic hemorrhage. The campaign revolves around providing hemorrhage control training to members ofthe public and increasing public access to hemorrhage control equipment. To our knowledge, no medical school has established a self-sustaining Stop the Bleed program to train their students and faculty as well as made hemorrhage control equipment available for usein an emergency.
METHODS: B
leeding control classes were offered at the Frank H. Netter MD School of Medicine beginning in January 2018. A proposal was made tothe medical school's Council on Curriculum Oversight in May 2018 to incorporate the training as part of the required curriculum for first-year students. A second proposal was made to Quinnipiac University’s Emergency Management Team in June 2018 to purchase hemor-rhage control equipment.RESULTS: T
welve bleeding control courses were held between January and August 2018. Two hundred ten medical students, 19 faculty members, and36 public safety officers completed initial training. Thirty-four medical students, two faculty members, and two public safety officers be-came certified instructors. Training was incorporated into the first-year curriculum to be taught by certified second-year students under thedirection of the school’s Department of Surgery. The school purchased approved training equipment. A student-coordinator position wascreated in the Surgery Interest Group. Hemorrhage control equipment was purchased for each public safety officer, patrol vehicles, and forthe Central Dispatch headquarters. Public-access equipment has been purchased for each Automated External Defibrillator cabinet at themedical school.CONCLUSION: T
he School ofMedicine community has been empoweredwith the ability to save lives. Students and faculty have been trained in life-savingskills, a self-sustaining training process has been created, and equipment has been purchased for hemorrhage control efforts. (J TraumaAcute Care Surg. 2019;86: 1023–1026. Copyright © 2018 Wolters Kluwer Health, Inc. All rights reserved.)KEYWORDS: S
top the bleed; Hartford consensus; bleeding control; medical education; injury prevention.F ollowing the 2012 shooting at Sandy Hook ElementarySchool in Newtown, Connecticut, representatives from the
American College of Surgeons and members of organizationsof first responders and the federal government gathered in a se-ries of four meetings in Hartford, Connecticut. Deliberationsfrom the four meetings were published as the Hartford Consen-sus, with the goal of maximizing survival during mass-casualtyevents using the principles captured in the acronym THREAT:Threat suppression, Hemorrhage control, Rapid Extrication tosafety,Assessment by medical providers, and Transport to de-finitive care.1 The Hartford Consensus recognized that externalhemorrhage is the most significant preventable cause of death inthe prehospital environment2 and acknowledged that hemor-rhage control training is simple, effective, and easily retained.3
The consensus papers include recommendations to minimize
8, Revised: September 12, 2018, Accepted: September 18,e: October 2, 2018.MD, School ofMedicine (J.F.), Department of Surgery (C.V.D School of Medicine, Quinnipiac University, Injury Pre-utreach & Research Program (P.V.), Yale-New Haven Hos-partment of Emergency Medicine and Traumatology (L.J.necticut School ofMedicine, Farmington; and Trauma Insti-Hospital, Hartford, Connecticut.my Fridling, Quinnipiac University, 275 Mt. Carmel Ave,ail: [email protected].
0000002078
rg
Copyright © 2019 Wolters Kluwer H
these preventable deaths by empowering members of the publicto provide immediate care to the traumatically injured, maxi-mizing the ability of the immediate responder to provide careby making bleeding control equipment readily available to thepublic,4 and establishing a continuum of care for the treatmentof the injured.5
In 2015, the White House launched the Stop the BleedCampaign following President Barack Obama’s PresidentialPolicy Directive 8 to strengthen the security and resilience ofthe United States.6,7 The goal of the Stop the Bleed Campaignis to empower and prepare members of the public to act as “im-mediate responders,”who can start treatment to control bleedingof the traumatically injured before traditional first respondersarrive. The Hartford Consensus recommended that an educa-tional program be designed and implemented to train all peopleon hemorrhage control in a manner similar to cardiopulmonaryresuscitation (CPR) training. The American College of SurgeonsCommittee on Trauma worked with the National Association ofEmergency Medical Technicians to create the one-hour BleedingControl Basic course. As of March 2018, the Bleeding ControlBasic course has been taught by more than 28,500 instructors tomore than 350,000 participants in every state in the UnitedStates and multiple countries worldwide.8 In addition, the Bul-letin of the American College of Surgeons published a letter tothe editor in February 2018 from a medical student and ArmyRanger Physician Assistant from the Texas A&M College of
1023
ealth, Inc. All rights reserved.

Fridling et al.J Trauma Acute Care Surg
Volume 86, Number 6
Medicine calling for hemorrhage control training to be part ofthe education of all health care providers.9
At the Frank H. Netter School of Medicine at QuinnipiacUniversity in North Haven, Connecticut, we set out to meet theHartford Consensus recommendations and establish the firstHartford Consensus-Compliant Medical School in the UnitedStates. To do so, we first needed to inform the population of stu-dents, faculty, and staff at the medical school about the need forhemorrhage control training. Then, we educated the group byproviding them with the knowledge and skills necessary to treatlife-threatening bleeding. Finally, we empowered individuals byproviding them with a life-saving skill, generating an instructorpool, and using the trained population to teach future classes.To meet the Hartford Consensus recommendations for a resilientpopulation trained to minimize death from traumatic hemor-rhage, we established a set of objectives in the fall of 2017:
1. Teach bleeding control skills to more than 50% of first-yearmedical students, more than 25% of faculty members, andmore than 25% of public safety staff
2. Establish a process to continue course delivery following the2017–2018 academic year
3. Secure hemorrhage control equipment for the FrankH. NetterMD School of Medicine
METHODS
All bleeding control courses were delivered according tostandards set by the Bleeding Control Basic Course Guidelinesby instructors certified by the American College of SurgeonsCommittee on Trauma.10 The courses were held on each of thethree Quinnipiac University campuses beginning in January2018. Each class lasted between one and 2 hours divided intolecture and hands-on skills practice. The Bleeding Control Basicv. 1.0 slides were projected or shown on a screen to provide thelecture-based instruction of direct pressure, tourniquet applica-tion, and wound packing. The skills practice focused on the useof the 7th-Generation Combat Application Tourniquets (Compos-ite Resources, Rock Hill, SC) and QuikClot hemostatic dressing(Z-Medica, Wallingford, Connecticut). Approved training equip-ment was provided by Z-Medica. The initial courses were taughtby a first-year medical student certified as a paramedic. Subse-quently, other Frank H. Netter MD School of Medicine students,Quinnipiac University nursing students, and staff from theYale-NewHaven Hospital Injury Prevention Program, whowerealso certified as instructors, assisted with course instruction.Courses were advertised on social media and by word of mouth.
Process for Instituting Curriculum ChangesThe students responded to the initial wave of Bleeding
Control classes with positive feedback, and the Surgery Clerk-ship Director called a meeting with the medical student involvedin the project to discuss the idea of incorporating the traininginto the preclerkship curriculum at the School of Medicine.Changes to the curriculum for the Netter School of Medicineare approved by the Council on Curriculum Oversight. Thecouncil hosts monthly meetings, and proposed changes are ap-proved by a vote following a formal presentation on the pro-posal. After discussion with the chair of the Council and the
1024
Copyright © 2019 Wolters Kluwer H
Associate Dean for Student Affairs, a Stop the Bleed presenta-tion was prepared by the medical student involved in the projectand delivered by the School of Medicine Surgery ClerkshipCoordinator on May 31, 2018.
Process for Obtaining EquipmentThe Quinnipiac University Emergency Management
Team is composed of representatives from each of the three Uni-versity campuses, and it includes staff from the Departments ofFacilities, Public Safety and Student Health Services. The teammeets monthly and oversees the University’s crisis responsepreparation.11 The medical student involved in the projectprepared and delivered a proposal to the Emergency Manage-ment Team during their June 12, 2018 meeting for the purchaseof hemorrhage control equipment for the public safety officersand for public access. The proposal also included training equip-ment to be used for the future training of Quinnipiac Universitypublic safety officers.
RESULTS
Between January and May 2018, 11 noncompulsoryBleeding Control classes were held at the Frank H. Netter MDSchool of Medicine at Quinnipiac University. Training was pro-vided to 48 of the 95 medical students of the class of 2021 notinvolved in the project (51%), 13 medical students of the classof 2020, and one student of the class of 2018. Seventeen(34%) of the 50 School of Medicine faculty members completedthe training, and 36 of the 76 Quinnipiac University Public Safetyofficers completed the course (47%). In addition, 34 medicalstudents, two faculty members, and two Public Safety Officerswere certified as instructors. Moreover, 25 Quinnipiac Univer-sity nursing students also completed the training, and two werecertified as instructors.
The proposal to include the Bleeding Control class in themedical school curriculumwas approved by the Council on Cur-riculum Oversight in May 2018. The Netter School of MedicineDepartment of Surgery took ownership of the program and sup-ported a training session for the incoming students in the class of2022 and the remaining untrained students in the class of 2021during the first week of the 2018 to 2019 school year. Thistraining session, which was delivered by 25 certified student-instructors from the class of 2021, was attended by 97 of the 98members of the class of 2022, all 51 members of the remaininguntrained (now larger) class of 2021, and two faculty members.
Subsequent training will be conducted each fall for thefirst-year students, and it will be led by second-year studentsand supervised and supported by the School of Medicine De-partment of Surgery. A Stop the Bleed Student Coordinator po-sition was created in the Netter School of Medicine’s SurgeryInterest Group under direction of the Surgical Clerkship Directorto lead the school’s Stop the Bleed activities. The coordinatorwill be responsible for overseeing the training and certificationof instructors at the School of Medicine and conducting trainingin the community on behalf of the School of Medicine.
Approved training equipment was purchased by theSchool ofMedicine's Standardized Patient and Assessment Cen-ter. Hemorrhage control equipment was purchased for theQuinnipiac University Department of Public Safety through a
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 6 Fridling et al.
donation from the Yale New Haven Injury Prevention and Com-munity Outreach Program. A QuikClot Bleeding Control Bagand Public Access Bleeding Control Station Kit (Z-Medica,Wallingford, CT) containing 12 SOFTT-W tourniquets (TacticalMedical Solutions, Anderson, SC), QuikClot hemostatic dress-ings (Z-Medica), TacMed control wraps (Tactical Medical Solu-tions), EMS-style shears, and nitrile medical gloves was set upin the Public Safety headquarters office on the University’s maincampus. A QuikClot Bleeding Control Kit (Z-Medica) withthree SOFTT-W tourniquets, three QuikClot hemostatic dress-ings, three mini compression bandages (H&HMedical Corpora-tion, Williamsburg, Virginia), EMS-style shears, and nitrilemedical gloves were placed in each of the 12 public safety ve-hicles. A SOFTT-W tourniquet was given to each public safetyofficer for use while on duty. In addition, public-access hemor-rhage control equipment was purchased by the Netter School ofMedicine Department of Surgery. A Premium Personal Bleed-ing Control Kit (Z-Medica) with one 7th-generation CombatApplication Tourniquet, one QuikClot bleeding control dress-ing, one H&H compression bandage, pair of medical gloves,mini Sharpie marker (Sharpie, Oak Brook, IL), and instructionalbooklet will be placed in each of the eight Automated ExternalDefibrillator cabinets on the medical school campus. The cabi-nets will be marked with signage to alert the public to the pres-ence of hemorrhage control equipment.
DISCUSSION
Establishing a Hartford Consensus-compliant medicalschool is necessary not only as a preparation for a potentialschool shooting or other mass casualty event but because medi-cal students, as future leaders in the health care community,should be prepared to act to save lives in case of any emergency.Traumatic bleeding can occur from a spectrum of causes includ-ing natural disasters, motor vehicle collisions, and work, recrea-tional, or home-related accidents involving sharp tools or glass.Trained students will be empowered to act in case of such anevent and, more importantly, be able to advocate for or host sim-ilar training in the communities in which they will practice.
Bringing a Stop the Bleed program to the Netter School ofMedicine created several additional opportunities. The classestaught in the spring of 2018 were open to all students on theQuinnipiac University North Haven campus, which is also hometo schools of Nursing and Health Sciences. Twenty-five nursingstudents voluntarily attended the training, and the class becameapproved as a nursing elective. Two nursing students becamecertified as instructors of the course and assisted with the deliv-ery of subsequent classes. The involvement of medical studentsteaching nursing students and then nursing students teachingmedical students facilitated interaction and collaboration be-tween the programs and the development of interprofessionaleducation. The Netter Stop the Bleed core instructor team alsowent into the community to teach classes, interacting with localfire departments, police departments, ambulance companies,Community Emergency Response Teams, schools, hospitals, andthe general public, thus promoting community outreach oppor-tunities. In total, 11 classes were held with a total of 228 peopletrained. As a result, a new relationship was developed with theYale New Haven Hospital Center for Emergency Medical
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
Services and with St. Francis Hospital to collaborate on futureclasses. Moreover, there was an increase in public awarenessof the Stop the Bleed efforts of the University. The instructionalefforts and information about the Stop the Bleed campaign werecovered by three local television stations and featured in 11Connecticut newspapers following the shooting at StonemanDouglas High School. A class led by the Netter group onMarch 31, National Stop the Bleed Day, was also showcasedby more than 40 CBS affiliates nationwide including CBS2in New York, New York, CBS4 in Miami, Florida, and CBS8in Las Vegas, Nevada.
While the framework for Hartford Consensus-compliancehas been established and the Netter School of Medicine is betterprepared for hemorrhagic emergencies than it was 1 year ago,the efforts are still ongoing. Future classes will be held to trainthe remainder of the Public Safety staff, School of Medicine fac-ulty, and the current medical students who have yet to completethe training. An expansion of the training for the students of theschools of Nursing and Health Sciences will also be offered, andmeetings are underway to add the training to their curriculum.Such training further cultivates interprofessional education andcollaboration by facilitating the students working together andlearning from each other.
The Stop the Bleed program at the Frank H. Netter Schoolof Medicine at Quinnipiac University was a grassroots effort ledby a single first-year medical student certified as a paramedic.The program’s momentum grew as the number of people trainedincreased, and, once trained, key faculty members served as ad-vocates for future efforts including the incorporation of the train-ing into the School of Medicine curriculum. These efforts wereaided by the University's proximity to the Sandy Hook Elemen-tary School, Hartford Hospital—site of the Hartford Consensus,and the offices of Z-Medica, all located in Connecticut. How-ever, there is no doubt that this framework could serve as a tem-plate to assist other medical schools across the country inestablishing or expanding similar programs to Bleeding Controltraining in the education of their students.
AUTHORSHIP
J.F. conducted the majority of training, wrote the proposal to the NetterSchool ofMedicine Council onCurriculumOversight, wrote and deliveredthe proposal to theQuinnipiac University EmergencyManagement Team,and drafted the article. C.V.C. organized activities at the Netter School ofMedicine, delivered the proposal to the Council of Curriculum Oversight,assisted in the revision of the article to make important changes in con-tent, approved the final version of the article, and directed the purchaseof public-access equipment for the Frank H. Netter MD School of Medi-cine. P.V. conducted training, assisted in the revision of the article tomakeimportant changes in content and formatting, approved the final versionof the article, and provided equipment for the Quinnipiac University Pub-lic Safety Department. L.J.Jr. conceived and designed the project, oversawits execution, assisted in the writing of the article, and approved the finalversion of the article.
DISCLOSURE
The authors declare no funding or conflicts of interest.J.F. was provided a budget of $2500 by the Frank H. Netter MD School ofMedicine for research. Equipment for Quinnipiac University Departmentof Public Safety was funded by the Yale-New Haven Hospital Departmentof Injury Prevention & Community Outreach Program. Public-accessequipment for the Frank H. Netter MD School of Medicine was fundedby the Frank H. Netter MD School of Medicine Department of Surgery.Ethics approval: Quinnipiac University Institutional Review Board.
1025
ealth, Inc. All rights reserved.

Fridling et al.J Trauma Acute Care Surg
Volume 86, Number 6
REFERENCES1. Warshaw AL. A systematic response to mass trauma: the public, organized
first responders, and the American College of Surgeons. Bull Am Coll Surg.2015;100:14–15.
2. Jacobs LM, Carmona R, McSwain N, Butler FK, Elliot D, Warshaw AL,Woodson J, Hunt RC, Mitchell E, Eastman A, et al. The Hartford consensusIII: implementation of bleeding control: if you see something do something.Bull Am Coll Surg. 2015;100:40–46.
3. Jacobs LM, McSwain N, Rotondo M, Wade DS, Fabbri WP, Eastman A,Butler FK, Sinclair J. Joint Committee to Create a National Policy to En-hance Survivability from Mass Casualty Shooting Events. Improvingsurvival from active shooter events: the Hartford consensus. Bull AmColl Surg. 2013;98:14–16.
4. Jacobs LM, Carmona R, Butler F, Warshaw AL, Hoyt DB, Knudson M,Woodson J, Eastman A, Brinsfield K, Fabbri W, et al. The Hartford consen-sus IV: a call for increased national resilience. Bull Am Coll Surg. 2016;101(3):17–24.
5. Jacobs LM, Rotondo M, McSwain N, Wade DS, Fabbri WP, Eastman A,Butler FK, Sinclair J, Burns K, Brinsfield K, et al. Active shooter and inten-tional mass-casualty events: the Hartford consensus II. Bull Am Coll Surg.2013;98:18–22.
1026
Copyright © 2019 Wolters Kluwer H
6. Obama BH. Presidential policy directive: National Preparedness. Bull AmColl Surg. 2015;100:10–13.
7. Office of the Press Secretary. “Fact sheet: bystander: ‘stop the bleed’ broadprivate sector support for effort to save lives and build resilience.” the whitehouse: president Barack Obama, ObamaWhiteHouse. Archives.gov, 6 Oct.2015, obamawhitehouse archives.gov/the-press-office/2015/10/06/fact-sheet-bystander-stop-bleed-broad-private-sector-support-effort-save. Accessed22 Aug. 2018.
8. American College of Surgeons. Stop the bleed: 2018 Progress Report.https://www.bleedingcontrol.org/~/media/bleedingcontrol/files/2018_stb_progressreport.ashx. Accessed April 1, 2018.
9. Fisher AD. Hemorrhage control training should be mandatory for health careprofessionals [letter to the editor]. Bull Am Coll Surg. 2018.
10. American College of Surgeons. Bleeding control basic (BCon) course v. 1.0instructor information. https://www.bleedingcontrol.org/~/media/bleedingcontrol/files/private/bleeding%20control%20basic%20instructor%20guide.ashx. Accessed September 12, 2017.
11. Quinnipiac University. Health and campus safety at Quinnipiac Uni-versity: emergency preparedness. https://www.qu.edu/student-resources/health-campus-safety.html#emergencypreparedness. AccessedJuly 13, 2018.
© 2018 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
ORIGINAL ARTICLE
Psychiatric outcome at least 20 years after trauma: A survey on thestatus of subjective general health and psychiatric symptomswith a
focus on posttraumatic stress disorder
Sascha Halvachizadeh, MD, Henrik Teuber, DO, Florin Allemann, MD, Anna Theresa Luidl, MD,Roland von Känel, MD, Boris Zelle, MD, Simon Tiziani, MD, Katrin Rauen, MD,
Hans-Christoph Pape, MD, and Roman Pfeifer, MD, Zurich, Switzerland
Sub
Fro
Thi
Ad
DO
J TrVol
BACKGROUND: I
mitted: August 8, 2018, RevisePublished online: February 13,m the Department of Trauma (S.HZurich, University of Zurich, Zur(A.T.L.), Aachen, Germany; DePsychosomatic Medicine (R.v.KZurich, Zurich, Switzerland; anTexas Health Science Center ats study was presented at the 77thof Acute Care Surgery and 4thW26–29 2018; WTC Oral Presentadress for reprints: Sascha HalvaHospital Zurich, University of Zemail: Sascha.halvachizadeh@u
I: 10.1097/TA.00000000000022
auma Acute Care Surgume 86, Number 6
nformation on long-term psychiatric sequelae after severe trauma is sparse. We therefore performed a survey addressingseveral symptoms related to posttraumatic stress disorder (PTSD) in patients who sustained multiple injuries more than20 years after trauma.
METHODS: P
atients injured between January 1, 1973, and December 31, 1990, were contacted at least 20 years later. We included multiplyinjured patients aged between 3 and 60 years from a single level 1 trauma center. A questionnaire based on the Diagnostic andStatistical Manual of Mental Disorders, Fourth Edition, diagnostic criteria for PTSD, including individual symptoms related tointrusion, avoidance, and hyperarousal was sent to all patients.RESULTS: A
total of 359 patients (56.35%) received a questionnaire. Of these, 337 patients (93.87%) returned the questionnaire and wereincluded in the study (223 males [66.17%] and 114 females [33.82%]). Mean ± SD follow-up was 29.5 ± 8.5 years. Nearly halfthe study population (47.18%) experienced lasting psychiatric sequelae, such as intrusive recollection (n = 65, 19.28%), avoidance(n = 92, 27.29%), or hyperarousal (n = 95, 28.18%) at least monthly. Ten patients (2.96%) fulfilled all Diagnostic and StatisticalManual of Mental Disorders, Fourth Edition, diagnostic criteria for PTSD. A total of 131 patients (38.87%) reported fair or poorgeneral health status. There was no difference in injury severity in patients with or without PTSD (injury severity score, 8.33 vs.20.36, respectively; p = 0.52) or PTSD-related symptoms including intrusion (19.88 vs. 20.32, p = 0.74), avoidance (19.99 vs.20.3, p = 0.79), and hyperarousal (19.36 vs. 20.68, p = 0.26).CONCLUSION: A
t least 20 years after injury, no correlation was found between the development of psychiatric complications and the severity ofinjury. While the rate of full-blown PTSD was low, nearly half the study population regularly suffered from at least one psychiatricsymptom attributable to the initial trauma. Awareness for the development of psychiatric complications and early initiation of psy-chiatric counseling are advisable. (J Trauma Acute Care Surg. 2019;86: 1027–1032. Copyright © 2019 Wolters Kluwer Health,Inc. All rights reserved.)LEVEL OF EVIDENCE: P
rognostic and epidemiologic, level II. KEYWORDS: P TSD; long-term follow-up; severe injury; multiple trauma; psychiatric complication; intrusion; avoidance; arousal.A fter severe trauma, patients may suffer from psychological,psychiatric, cognitive, and/or behavioral disabilities.1 Se-
verely injured patients are prone to develop psychiatric diseasesand mental disorders with higher rates of suicide or additionaltraumatic events when compared with the general population.2,3
In addition, psychiatric disorders, such as depression, anxiety, or
d: January 8, 2019, Accepted: January 15, 2019,2019.., H.T., F.A., S.T., H.-C.P., R.P.), University Hospitalich, Switzerland;Medical University RWTHAachenpartment of Consultation-Liaison Psychiatry and., K.R.), University Hospital Zurich, University ofd Department of Orthopedic Surgery, University ofSan Antonio (B.Z.), San Antonio, Texas.Annual Meeting of AASTand Clinical Congressorld TraumaCongress, SanDiego, CA, September,tion for AAST20180021.chizadeh, MD, Department of Trauma, Universityurich, Rämistrasse 100 8091, Zurich, Switzerland;sz.ch.
32
Copyright © 2019 Wolters Kluwer H
posttraumatic stress disorder (PTSD) may interfere with thephysical rehabilitation process in these patient groups. Patientswho exhibited a higher sense of self-efficacy showed improvedoutcomes and rehabilitation results.4 Finally, family involvementin the rehabilitation process also appears to show positive effectson outcome.5 Our group has previously performed a 10-yearfollow-up survey to assess long-term psychological and generalquality of life.6 The survey confirmed that patients with injuriesto the lower extremities or intra-articular fractures were signifi-cantly more likely to experience poor outcomes.7,8 Moreover,traumatic brain injuries and spinal cord injuries were indepen-dent predictors of long-term disability.2,9,10
The aim of the current 20-year follow-up study was to an-swer the following questions:
1. Is the severity of multiple injured patients associated withthe development of PTSD or PTSD-related symptoms, suchas intrusion, avoidance, or arousal?
2. Are psychiatric problems and subjective perception ofgeneral health associated with injury distribution or injuryseverity?
1027
ealth, Inc. All rights reserved.

Halvachizadeh et al.J Trauma Acute Care Surg
Volume 86, Number 6
PATIENTS AND METHODS
Ethical ConsiderationsThis study was conducted according to the Declaration
of Helsinki.11 The local ethics committee approved this study(Ethical Committee Trial ID Number 2325-200/03/22). Partici-pants who consented to participate in this study were included.
Study PopulationIn our previous studies,12,13 a database was established to
allow for long-term follow-up. Using an exhaustive recruitmentprocess with multiple steps to find patients who had moved,6,14
patients treated between January 1, 1973, and December 31,1990, at a single level 1 trauma center were contacted. All pa-tients were contacted by phone or mail before sending out thequestionnaire. With a returned questionnaire, patients consentedto participate and were included in this study. This investigationwas designed as a prospective cohort study. All multiply injuredpatients between 3 and 60 years of age with a minimum follow-up of 20 years and a properly completed questionnaire fulfilledthe study inclusion criteria. Inability to fill out the questionnaireand incomplete data led to exclusion.
QuestionnaireThe self-administered questionnaire consisted of 118
questions. Questions assessing PTSD were strictly based on Di-agnostic and Statistical Manual of Mental Disorders, FourthEdition (DSM-IV), criteria for PTSD.15 The questionnaire inves-tigated psychiatric symptoms, the ability to complete activities ofdaily living, work status, and the degree of current psychotherapeu-tic treatment or rehabilitation. General health status was assessedthrough several self-ratings with scores ranging from 1 (poor)to 2 (excellent).
Definitions of PTSDQuestions (n = 33) assessing PTSD were based on the
American Psychiatric Association's DSM-IV criteria for PTSD.Most of the questions (n = 23) were adopted from the Impactof Event Scale (IES).16,17 According to DSM-IV, six categoriesof symptoms (A–F) must be evaluated to diagnose PTSD. Cate-gory A establishes the occurrence of a life-threatening traumaticevent. Categories B toDwere evaluated with the following num-ber of questions (n): Category B evaluates reexperiencing thetrauma, recurrent and stressful memories, flashbacks, night-mares, or intrusion (n = 8); Category C, the symptoms of avoid-ance (n = 9); and Category D evaluates the presence of arousal(n = 7). Specifically, the questionnaire evaluated trauma-related psychiatric complications on a 4-point numerical scaleassessing howoften patients experienced these symptomswithinthe last month:
1) Never: 1 point2) Seldom (once or twice per month): 2 points3) Occasionally (once or twice per week): 3 points4) Often (at least once per day): 4 points
The PTSD criteria for each category were fulfilled if ascore of greater than 3 points was tabulated. Criteria for Cate-gory E were fulfilled if the above symptoms were present for
1028
Copyright © 2019 Wolters Kluwer H
more than 1 month. Category F assessed whether the previouslymentioned disturbances have led to clinically significant distressor impairment in social or occupational situations. The PTSDportion of the questionnaire was based exclusively on these di-agnostic categories and therefore reliably suggests the presenceor absence of PTSD. Patients were then stratified into twogroups: those who fulfilled the previously mentioned diagnosticcriteria for PTSD as well as those experiencing at least one itemof the intrusion, avoidance, or arousal symptom cluster andthose who did not.
Statistical AnalysisStatistical analysis was performed using GraphPad Prism
statistical software (version 7.00 for Windows; GraphPad Soft-ware, La Jolla, CA; www.graphpad.com) and SPSS Statisticsprogram (IBM SPSS Statistics for Windows, version 25.0, re-leased 2017; IBM Corp., Armonk, NY). The data were testedfor normal distribution using the Kolmogorov-Smirnov test.The analysis of variance test was used to compare groups oncontinuously scaled variables with a normal distribution. TheKruskal-Wallis test was used for nonnormal distributed continu-ous variables with a skewed distribution. The Pearson χ2 testwas applied to compare groups on categorical variables. Signif-icance level was set at a p value of <0.05 (two-tailed).
RESULTS
Patient Selection and DemographicsFigure 1 shows the flow diagram of patient enrollment. Of
637 patients whowere initially enrolled,2 36 patients (5.6%) haddied and 242 (38.0%) were lost to follow-up. Of the 359 patientswho received the questionnaire, 337 (93.9%) responded, 21(5.8%) did not respond, and 1 patient (0.3%) returned an illegi-ble questionnaire. The demographics are summarized in Table 1.Patients who did not contribute to this study demonstrated a sim-ilar demographic distribution (78% male, mean ± SD age at thetime of injury of 26.6 ± 12.8 years and injury severity score[ISS] ± SD of 21 ± 10 points). We found no significant differ-ences between the population that was included in this studyand those who did not contribute regarding their demographics.
General OutcomeGeneral health was reported as excellent (n = 14, 4.1%),
very good (n = 43, 12.8%), good (n = 149, 44.2%), fair(n = 107, 31.8%), or poor (n = 24, 7.1%). More than one third(38.87%) of patients rated their current health status as fair orpoor, whereas 16.91% of patients reported excellent or verygood health.
With respect to physical activity, 10 patients (2.9%) re-ported no capability of being physically active, 118 patients(35.0%) claimed severe limitations, 111 (32.9%) had few limita-tions, 46 (13.6%) minimal, and 52 (15.4%) had no limitationsduring physical activity.
More than one in four patients (n = 88, 26.1%) experi-enced at least one additional psychiatric insult through furthertrauma or other traumatic events with 53 patients (15.7%) suffer-ing additional severe injuries or experiencing fires or explosions.
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
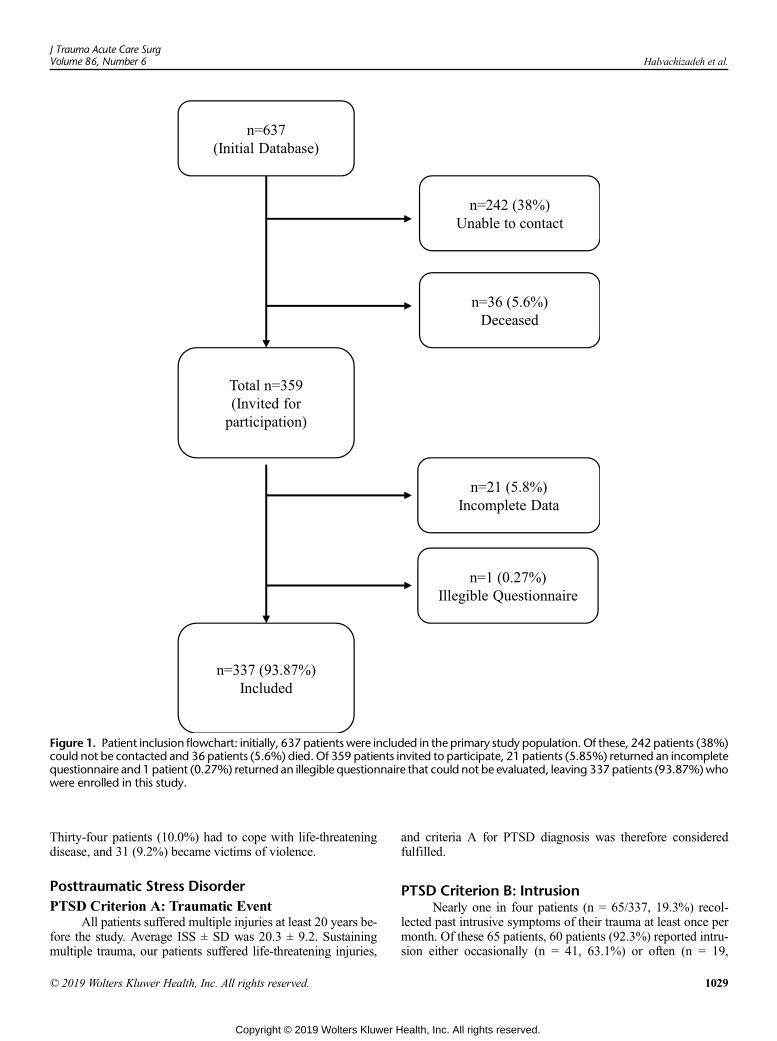
Figure 1. Patient inclusion flowchart: initially, 637 patients were included in the primary study population. Of these, 242 patients (38%)could not be contacted and 36 patients (5.6%) died. Of 359 patients invited to participate, 21 patients (5.85%) returned an incompletequestionnaire and 1 patient (0.27%) returned an illegible questionnaire that could not be evaluated, leaving 337 patients (93.87%)whowere enrolled in this study.
J Trauma Acute Care SurgVolume 86, Number 6 Halvachizadeh et al.
Thirty-four patients (10.0%) had to cope with life-threateningdisease, and 31 (9.2%) became victims of violence.
Posttraumatic Stress DisorderPTSD Criterion A: Traumatic Event
All patients suffered multiple injuries at least 20 years be-fore the study. Average ISS ± SD was 20.3 ± 9.2. Sustainingmultiple trauma, our patients suffered life-threatening injuries,
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
and criteria A for PTSD diagnosis was therefore consideredfulfilled.
PTSD Criterion B: IntrusionNearly one in four patients (n = 65/337, 19.3%) recol-
lected past intrusive symptoms of their trauma at least once permonth. Of these 65 patients, 60 patients (92.3%) reported intru-sion either occasionally (n = 41, 63.1%) or often (n = 19,
1029
ealth, Inc. All rights reserved.

TABLE 1. Demographics of Patients Who Were Included inThis Article
Demographic (N = 337)
Age (years) 25.44 (±11.69)
Gender (male) 223 (66.0%)
Married (yes) 107 (31.7%)
ISS 20.3 (±9.26)
MAIS 1 Head 2.68 (±0.77)
MAIS 2 Face 1.61 (±0.71)
MAIS 4 Thorax 3.23 (±1.17)
MAIS 5 Abdomen 2.58 (±0.72)
MAIS 6 Spine 2.54 (±1.14)
MAIS 7 UpperEx 2.13 (±0.56)
MAIS 8 LowerEx 2.77 (±0.46)
Mean (SD) for each demographic is shown.
Halvachizadeh et al.J Trauma Acute Care Surg
Volume 86, Number 6
29.2%). The remaining five patients (7.7%) rarely experiencedthese symptoms.
PTSD Criterion C: AvoidanceAvoidance was reported in 92 (27.4%) of 337 patients, of
which 21 patients (22.8%) frequently experienced symptomsof avoidance, 32 (34.8%) of them occasionally, and 39 (42.4%)of them rarely.
PTSD Criterion D: HyperarousalWith respect to criteria D, 95 (28.2%) of 337 patients suf-
fered from hyperarousal at least once per month. Of these,60 patients (63.2%) experienced symptoms of arousal eitherweekly (n = 40, 42.1%) or daily (n = 20, 21.1%). Thirty-five pa-tients (36.8%) reported to suffer rarely from hyperarousal.
PTSD Diagnosis (All Symptom Dimensions)In this study, 159 patients (47.2%) reported symptoms in
at least one item of the intrusion, avoidance, or arousal cluster.Ten patients (2.9%) reported suffering daily symptoms in allthree clusters and may therefore fulfill the DSM-IV diagnosticcriteria of PTSD. Patients with PTSD did not significantly differin age, sex, ISS, and Maximum Abbreviated Injury Scale(MAIS) from those not fulfilling PTSD criteria. Furthermore,patients suffering any PTSD-related symptoms at least onceper month also did not differ demographically to those with noPTSD-related symptoms in all categories. The development ofpsychiatric complications was significantly associated with psy-chiatric treatment (p < 0.01). Psychiatric treatment after traumawas common in all patient groups. Unemployment because ofthe initial trauma was significantly more likely in patients withPTSD (p = 0.009) and those reporting symptoms of hyperarousal(p = 0.04). Additional trauma or early retirement was not morecommonly seen in those patients with PTSD or PTSD-relatedsymptoms. These findings are summarized in Table 2.
DISCUSSION
Traumatic injuries continue to be among the leadingcauses of death and disability worldwide.18 In patients surviving
1030
Copyright © 2019 Wolters Kluwer H
severe trauma, psychiatric sequelae are frequent and may lead tolong-term disability unrelated to their medical condition.19
This study shows a low prevalence of full blown PTSD(3%), comparable with the life-time prevalence of PTSD in thegeneral population.20 In contrast, nearly half of the patients suf-fer at least one symptom of PTSD (i.e., intrusion, avoidance, orhyperarousal) after more than 20 years after their initial injury.No association with the development PTSD or PTSD-relatedsymptoms was observed, neither was there an associationwith their self-rated general health status and the injury sever-ity or distribution.
We feel that our study has both limitations and advan-tages. One might argue that the management of severely injuredpatients may differ from that of other institutions. However, asingle-center survey reduces the likelihood of interhospital dif-ferences in trauma management. The questionnaires were com-pleted by the patients and represent a subjective self-evaluation.Inability of some patients to successfully fill out the question-naire because of older age or long-term trauma sequelae maybe considered another confounding variable. However, since93% of patients returned a properly completed questionnaire,we feel that this did not negatively affect our results. In addition,questions in our questionnaire were derived exclusively fromvalidated questionnaires. Furthermore, the distinct possibilityexists that some patients who did not consent to participate, ordid not return the questionnaire, are unwilling to discuss and re-live the psychiatric stress of their respective trauma. This mayhave caused underreporting of a significant level of patients suf-fering from long-term psychiatric complications, which cannotbe completely ruled out. Moreover, when the complete syn-drome of PTSD is regarded as an isolated outcome measure,the statistical power may have been too low to identify signifi-cant differences (n = 10/337).
Finally, we could not evaluate the psychiatric influencethat subsequent traumatic events experienced by our patientpopulation had on study results.
In contrast, the questionnaire was designed, and patientswere specifically instructed to focus their assessment on the ini-tial traumatic event. We feel that further strengths of this studywere the high inclusion rate of greater than 90% and the largedegree of long-term follow-up data, with these data reflectingthe patients' current state of health and mind.
To our knowledge, this assessment of the psychiatric com-plications of multiply injured patients after more than 20 yearsrepresent the longest follow-up in the literature, thus justifyingour conclusions.
In this long-term follow-up study, a high percentage of pa-tients still reported unsatisfactory general health. This is in ac-cordance with previous studies that evaluated multiple factorsincluding inability to return to work and socioeconomic fac-tors.12,21 We concur with previous authors that these issues per-sist and do not appear to regress over time.22
Severe injury is not necessarily sufficient to explain thedevelopment of PTSD.23 Risk factors for developing PTSD in-clude the extent to which the traumatic event remains in thepatient's memory24; pretrauma vulnerability25; the magnitudeof the stressor, anticipation of the event, immediate reactionsto the trauma and posttrauma factors26; and peritraumatic dis-sociation.27 In the literature, PTSD, depression, and other
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
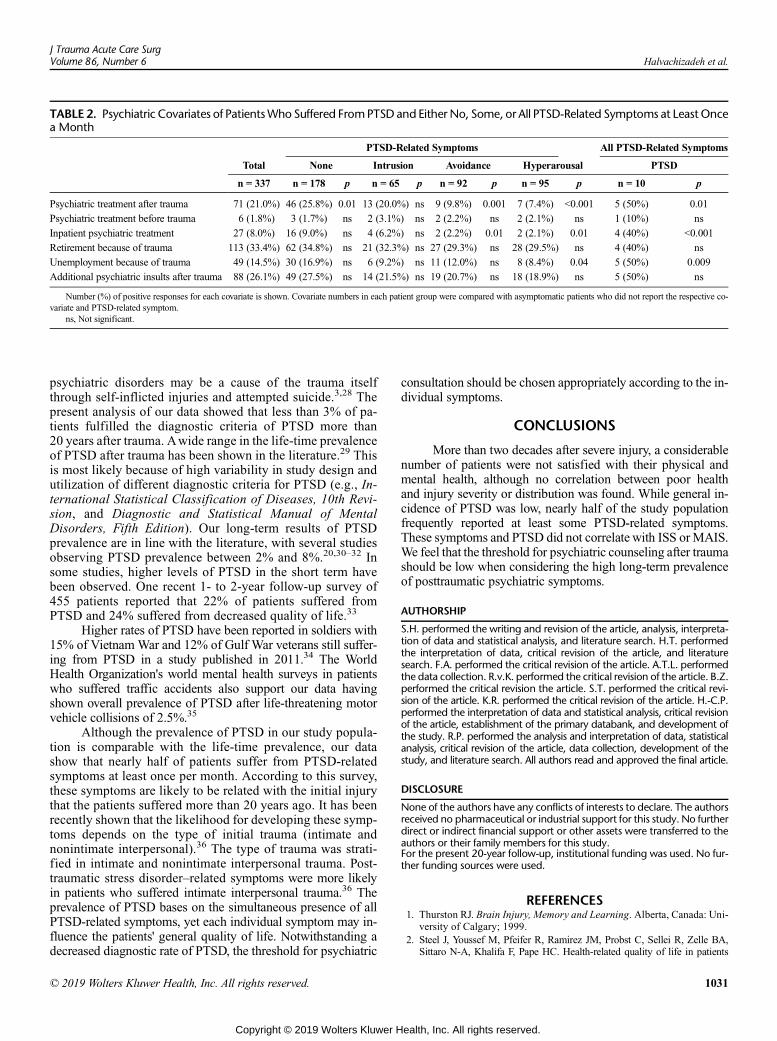
TABLE 2. Psychiatric Covariates of PatientsWho Suffered FromPTSD and Either No, Some, or All PTSD-Related Symptoms at LeastOncea Month
PTSD-Related Symptoms All PTSD-Related Symptoms
Total None Intrusion Avoidance Hyperarousal PTSD
n = 337 n = 178 p n = 65 p n = 92 p n = 95 p n = 10 p
Psychiatric treatment after trauma 71 (21.0%) 46 (25.8%) 0.01 13 (20.0%) ns 9 (9.8%) 0.001 7 (7.4%) <0.001 5 (50%) 0.01
Psychiatric treatment before trauma 6 (1.8%) 3 (1.7%) ns 2 (3.1%) ns 2 (2.2%) ns 2 (2.1%) ns 1 (10%) ns
Inpatient psychiatric treatment 27 (8.0%) 16 (9.0%) ns 4 (6.2%) ns 2 (2.2%) 0.01 2 (2.1%) 0.01 4 (40%) <0.001
Retirement because of trauma 113 (33.4%) 62 (34.8%) ns 21 (32.3%) ns 27 (29.3%) ns 28 (29.5%) ns 4 (40%) ns
Unemployment because of trauma 49 (14.5%) 30 (16.9%) ns 6 (9.2%) ns 11 (12.0%) ns 8 (8.4%) 0.04 5 (50%) 0.009
Additional psychiatric insults after trauma 88 (26.1%) 49 (27.5%) ns 14 (21.5%) ns 19 (20.7%) ns 18 (18.9%) ns 5 (50%) ns
Number (%) of positive responses for each covariate is shown. Covariate numbers in each patient group were compared with asymptomatic patients who did not report the respective co-variate and PTSD-related symptom.
ns, Not significant.
J Trauma Acute Care SurgVolume 86, Number 6 Halvachizadeh et al.
psychiatric disorders may be a cause of the trauma itselfthrough self-inflicted injuries and attempted suicide.3,28 Thepresent analysis of our data showed that less than 3% of pa-tients fulfilled the diagnostic criteria of PTSD more than20 years after trauma. Awide range in the life-time prevalenceof PTSD after trauma has been shown in the literature.29 Thisis most likely because of high variability in study design andutilization of different diagnostic criteria for PTSD (e.g., In-ternational Statistical Classification of Diseases, 10th Revi-sion, and Diagnostic and Statistical Manual of MentalDisorders, Fifth Edition). Our long-term results of PTSDprevalence are in line with the literature, with several studiesobserving PTSD prevalence between 2% and 8%.20,30–32 Insome studies, higher levels of PTSD in the short term havebeen observed. One recent 1- to 2-year follow-up survey of455 patients reported that 22% of patients suffered fromPTSD and 24% suffered from decreased quality of life.33
Higher rates of PTSD have been reported in soldiers with15% of VietnamWar and 12% of Gulf War veterans still suffer-ing from PTSD in a study published in 2011.34 The WorldHealth Organization's world mental health surveys in patientswho suffered traffic accidents also support our data havingshown overall prevalence of PTSD after life-threatening motorvehicle collisions of 2.5%.35
Although the prevalence of PTSD in our study popula-tion is comparable with the life-time prevalence, our datashow that nearly half of patients suffer from PTSD-relatedsymptoms at least once per month. According to this survey,these symptoms are likely to be related with the initial injurythat the patients suffered more than 20 years ago. It has beenrecently shown that the likelihood for developing these symp-toms depends on the type of initial trauma (intimate andnonintimate interpersonal).36 The type of trauma was strati-fied in intimate and nonintimate interpersonal trauma. Post-traumatic stress disorder–related symptoms were more likelyin patients who suffered intimate interpersonal trauma.36 Theprevalence of PTSD bases on the simultaneous presence of allPTSD-related symptoms, yet each individual symptom may in-fluence the patients' general quality of life. Notwithstanding adecreased diagnostic rate of PTSD, the threshold for psychiatric
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
consultation should be chosen appropriately according to the in-dividual symptoms.
CONCLUSIONS
More than two decades after severe injury, a considerablenumber of patients were not satisfied with their physical andmental health, although no correlation between poor healthand injury severity or distribution was found. While general in-cidence of PTSD was low, nearly half of the study populationfrequently reported at least some PTSD-related symptoms.These symptoms and PTSD did not correlate with ISS orMAIS.We feel that the threshold for psychiatric counseling after traumashould be low when considering the high long-term prevalenceof posttraumatic psychiatric symptoms.
AUTHORSHIP
S.H. performed the writing and revision of the article, analysis, interpreta-tion of data and statistical analysis, and literature search. H.T. performedthe interpretation of data, critical revision of the article, and literaturesearch. F.A. performed the critical revision of the article. A.T.L. performedthe data collection. R.v.K. performed the critical revision of the article. B.Z.performed the critical revision the article. S.T. performed the critical revi-sion of the article. K.R. performed the critical revision of the article. H.-C.P.performed the interpretation of data and statistical analysis, critical revisionof the article, establishment of the primary databank, and development ofthe study. R.P. performed the analysis and interpretation of data, statisticalanalysis, critical revision of the article, data collection, development of thestudy, and literature search. All authors read and approved the final article.
DISCLOSURE
None of the authors have any conflicts of interests to declare. The authorsreceived no pharmaceutical or industrial support for this study. No furtherdirect or indirect financial support or other assets were transferred to theauthors or their family members for this study.For the present 20-year follow-up, institutional funding was used. No fur-ther funding sources were used.
REFERENCES1. Thurston RJ. Brain Injury, Memory and Learning. Alberta, Canada: Uni-
versity of Calgary; 1999.2. Steel J, Youssef M, Pfeifer R, Ramirez JM, Probst C, Sellei R, Zelle BA,
Sittaro N-A, Khalifa F, Pape HC. Health-related quality of life in patients
1031
ealth, Inc. All rights reserved.
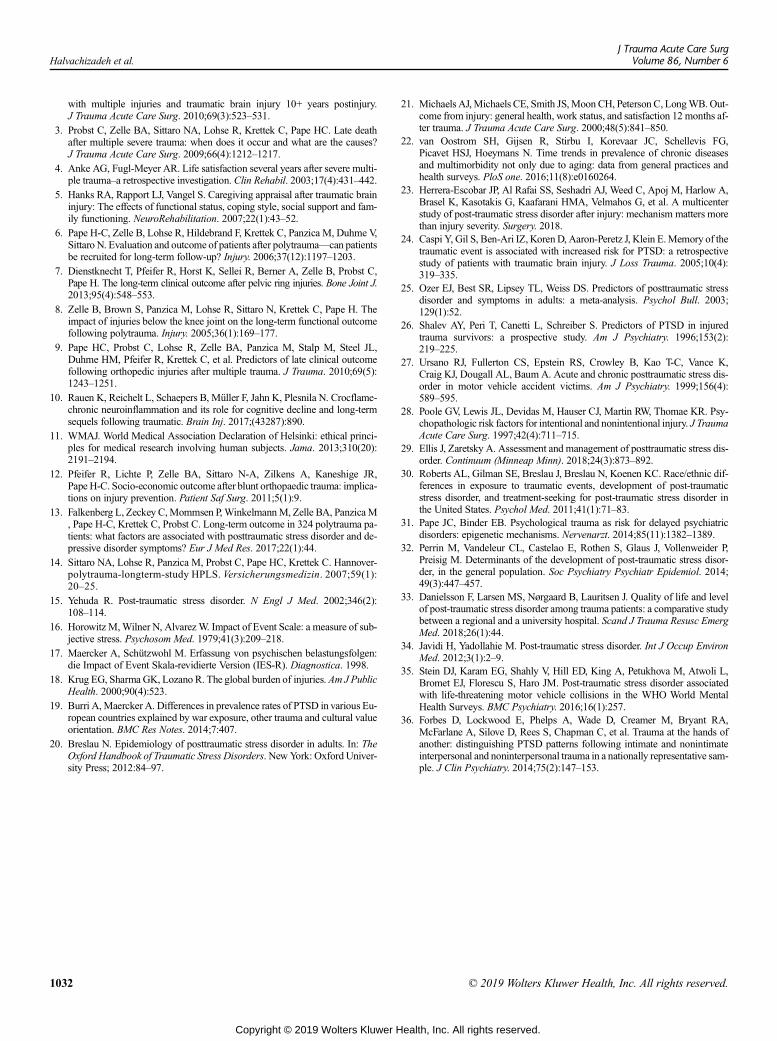
Halvachizadeh et al.J Trauma Acute Care Surg
Volume 86, Number 6
with multiple injuries and traumatic brain injury 10+ years postinjury.J Trauma Acute Care Surg. 2010;69(3):523–531.
3. Probst C, Zelle BA, Sittaro NA, Lohse R, Krettek C, Pape HC. Late deathafter multiple severe trauma: when does it occur and what are the causes?J Trauma Acute Care Surg. 2009;66(4):1212–1217.
4. Anke AG, Fugl-Meyer AR. Life satisfaction several years after severe multi-ple trauma–a retrospective investigation. Clin Rehabil. 2003;17(4):431–442.
5. Hanks RA, Rapport LJ, Vangel S. Caregiving appraisal after traumatic braininjury: The effects of functional status, coping style, social support and fam-ily functioning. NeuroRehabilitation. 2007;22(1):43–52.
6. Pape H-C, Zelle B, Lohse R, Hildebrand F, Krettek C, Panzica M, Duhme V,Sittaro N. Evaluation and outcome of patients after polytrauma—can patientsbe recruited for long-term follow-up? Injury. 2006;37(12):1197–1203.
7. Dienstknecht T, Pfeifer R, Horst K, Sellei R, Berner A, Zelle B, Probst C,Pape H. The long-term clinical outcome after pelvic ring injuries. Bone Joint J.2013;95(4):548–553.
8. Zelle B, Brown S, Panzica M, Lohse R, Sittaro N, Krettek C, Pape H. Theimpact of injuries below the knee joint on the long-term functional outcomefollowing polytrauma. Injury. 2005;36(1):169–177.
9. Pape HC, Probst C, Lohse R, Zelle BA, Panzica M, Stalp M, Steel JL,Duhme HM, Pfeifer R, Krettek C, et al. Predictors of late clinical outcomefollowing orthopedic injuries after multiple trauma. J Trauma. 2010;69(5):1243–1251.
10. Rauen K, Reichelt L, Schaepers B, Müller F, Jahn K, Plesnila N. Crocflame-chronic neuroinflammation and its role for cognitive decline and long-termsequels following traumatic. Brain Inj. 2017;(43287):890.
11. WMAJ. World Medical Association Declaration of Helsinki: ethical princi-ples for medical research involving human subjects. Jama. 2013;310(20):2191–2194.
12. Pfeifer R, Lichte P, Zelle BA, Sittaro N-A, Zilkens A, Kaneshige JR,Pape H-C. Socio-economic outcome after blunt orthopaedic trauma: implica-tions on injury prevention. Patient Saf Surg. 2011;5(1):9.
13. Falkenberg L, Zeckey C,Mommsen P,WinkelmannM, Zelle BA, PanzicaM, Pape H-C, Krettek C, Probst C. Long-term outcome in 324 polytrauma pa-tients: what factors are associated with posttraumatic stress disorder and de-pressive disorder symptoms? Eur J Med Res. 2017;22(1):44.
14. Sittaro NA, Lohse R, Panzica M, Probst C, Pape HC, Krettek C. Hannover-polytrauma-longterm-study HPLS. Versicherungsmedizin. 2007;59(1):20–25.
15. Yehuda R. Post-traumatic stress disorder. N Engl J Med. 2002;346(2):108–114.
16. Horowitz M,Wilner N, AlvarezW. Impact of Event Scale: a measure of sub-jective stress. Psychosom Med. 1979;41(3):209–218.
17. Maercker A, Schützwohl M. Erfassung von psychischen belastungsfolgen:die Impact of Event Skala-revidierte Version (IES-R). Diagnostica. 1998.
18. Krug EG, Sharma GK, Lozano R. The global burden of injuries. Am J PublicHealth. 2000;90(4):523.
19. Burri A, Maercker A. Differences in prevalence rates of PTSD in various Eu-ropean countries explained by war exposure, other trauma and cultural valueorientation. BMC Res Notes. 2014;7:407.
20. Breslau N. Epidemiology of posttraumatic stress disorder in adults. In: TheOxford Handbook of Traumatic Stress Disorders. NewYork: Oxford Univer-sity Press; 2012:84–97.
1032
Copyright © 2019 Wolters Kluwer H
21. Michaels AJ,Michaels CE, Smith JS,Moon CH, Peterson C, LongWB.Out-come from injury: general health, work status, and satisfaction 12 months af-ter trauma. J Trauma Acute Care Surg. 2000;48(5):841–850.
22. van Oostrom SH, Gijsen R, Stirbu I, Korevaar JC, Schellevis FG,Picavet HSJ, Hoeymans N. Time trends in prevalence of chronic diseasesand multimorbidity not only due to aging: data from general practices andhealth surveys. PloS one. 2016;11(8):e0160264.
23. Herrera-Escobar JP, Al Rafai SS, Seshadri AJ, Weed C, Apoj M, Harlow A,Brasel K, Kasotakis G, Kaafarani HMA, Velmahos G, et al. A multicenterstudy of post-traumatic stress disorder after injury: mechanism matters morethan injury severity. Surgery. 2018.
24. Caspi Y, Gil S, Ben-Ari IZ, KorenD, Aaron-Peretz J, Klein E.Memory of thetraumatic event is associated with increased risk for PTSD: a retrospectivestudy of patients with traumatic brain injury. J Loss Trauma. 2005;10(4):319–335.
25. Ozer EJ, Best SR, Lipsey TL, Weiss DS. Predictors of posttraumatic stressdisorder and symptoms in adults: a meta-analysis. Psychol Bull. 2003;129(1):52.
26. Shalev AY, Peri T, Canetti L, Schreiber S. Predictors of PTSD in injuredtrauma survivors: a prospective study. Am J Psychiatry. 1996;153(2):219–225.
27. Ursano RJ, Fullerton CS, Epstein RS, Crowley B, Kao T-C, Vance K,Craig KJ, Dougall AL, Baum A. Acute and chronic posttraumatic stress dis-order in motor vehicle accident victims. Am J Psychiatry. 1999;156(4):589–595.
28. Poole GV, Lewis JL, Devidas M, Hauser CJ, Martin RW, Thomae KR. Psy-chopathologic risk factors for intentional and nonintentional injury. J TraumaAcute Care Surg. 1997;42(4):711–715.
29. Ellis J, Zaretsky A. Assessment and management of posttraumatic stress dis-order. Continuum (Minneap Minn). 2018;24(3):873–892.
30. Roberts AL, Gilman SE, Breslau J, Breslau N, Koenen KC. Race/ethnic dif-ferences in exposure to traumatic events, development of post-traumaticstress disorder, and treatment-seeking for post-traumatic stress disorder inthe United States. Psychol Med. 2011;41(1):71–83.
31. Pape JC, Binder EB. Psychological trauma as risk for delayed psychiatricdisorders: epigenetic mechanisms. Nervenarzt. 2014;85(11):1382–1389.
32. Perrin M, Vandeleur CL, Castelao E, Rothen S, Glaus J, Vollenweider P,Preisig M. Determinants of the development of post-traumatic stress disor-der, in the general population. Soc Psychiatry Psychiatr Epidemiol. 2014;49(3):447–457.
33. Danielsson F, Larsen MS, Nørgaard B, Lauritsen J. Quality of life and levelof post-traumatic stress disorder among trauma patients: a comparative studybetween a regional and a university hospital. Scand J Trauma Resusc EmergMed. 2018;26(1):44.
34. Javidi H, Yadollahie M. Post-traumatic stress disorder. Int J Occup EnvironMed. 2012;3(1):2–9.
35. Stein DJ, Karam EG, Shahly V, Hill ED, King A, Petukhova M, Atwoli L,Bromet EJ, Florescu S, Haro JM. Post-traumatic stress disorder associatedwith life-threatening motor vehicle collisions in the WHO World MentalHealth Surveys. BMC Psychiatry. 2016;16(1):257.
36. Forbes D, Lockwood E, Phelps A, Wade D, Creamer M, Bryant RA,McFarlane A, Silove D, Rees S, Chapman C, et al. Trauma at the hands ofanother: distinguishing PTSD patterns following intimate and nonintimateinterpersonal and noninterpersonal trauma in a nationally representative sam-ple. J Clin Psychiatry. 2014;75(2):147–153.
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

CURRENT OPINION
Addressing posttraumatic amnesia—Recommendations forimproving patient lives after brain injury
Cathy Meng Fei Li, BSc, Lawrence Russell Robinson, MD,and Alan Ka Ho Tam, MD, Toronto, Ontario, Canada
B etween 2002 and 2006, approximately 1.7 million traumaticbrain injuries (TBIs) occurred annually in the United States.1
With an average increase in incidence of 29.7 per 100,000 annu-ally, the United States is expected to bear the burden of over2.8 million TBIs in 2018.2 While acute survival after TBI con-tinues to improve, advancements in optimizing long-term out-comes were less fruitful, and the average life expectancy forTBI survivors remains shortened by nearly a decade.3
The American College of Surgeons advocates that “acutecare should be consistent with preservation of optimal functionalrecovery” and recommends initiating physiatrist-directed reha-bilitation as soon as reasonably possible after injury.4 Physiat-rists are medical doctors who focus on increasing functionalcapacity of patients during recovery and are well positioned tolead early rehabilitative efforts of TBI patients who require acutemedical attention.5,6
Brain injuries are classified by severity. Patients withmoderate-to-severe TBI are at higher risk of morbidity and mor-tality, and exercising early prudence in managing these patientscan have profound effects on long-term outcomes. This commen-tary focuses on optimizing early management of moderate-to-severe TBI patients in Level I or II trauma centers, with theunderstanding that the heterogenous presentation and nature ofmoderate-to-severe TBIs, among other factors, severely limitthe availability of high-quality evidence.
When TBI patients are admitted to a trauma center, theprimary objective of the health care team is to hemodynamicallyand neurologically stabilize the patients. Once patients are med-ically stabilized, the priority shifts from survival to recovery.During this period, over 70% of TBI patients exhibit signs ofconfusion, agitation, amnesia, or impaired consciousness.7 Thistemporary state, during which the patient cannot form newmemories, is termed posttraumatic amnesia (PTA), and is recog-nized as one of the best indicators of injury severity and prog-nosticators of long-term outcomes.8–11
Studies demonstrated that PTA duration has greater prog-nostic value for predicting functional and cognitive outcomes
Submitted: October 5, 2018, Revised: December 6, 2018, Accepted: January 4, 2019,Published online: February 14, 2019.
From the University of Toronto (C.M.F.L.), Ontario, M5S1A8; Division of PhysicalMedicine and Rehabilitation (L.R.L.), Sunnybrook Health Sciences Centre,Ontario, M4N3M5; and Division of Physical Medicine & Rehabilitation, Depart-ment of Medicine (A.K.H.T.), University of Toronto, Ontario, M5S1A8.
Address for reprints: Alan Ka Ho Tam, MD, Toronto Rehabilitation Institute, Rm 10-107,550 University Ave, Toronto, Ontario, Canada M5G 2A2; email: [email protected].
DOI: 10.1097/TA.0000000000002233
J Trauma Acute Care SurgVolume 86, Number 6
Copyright © 2019 Wolters Kluwer H
than the Glasgow Coma Scale.8,9 In particular, PTA duration ishighly predictive of cognitive recovery, including executivefunctioning and processing speed, and return to work at 1-yearpostinjury.8,10 While Glasgow Coma Scale captures a momentin time, prospective PTA evaluations provide more informationabout the patient's course of recovery and has greater clinical utilitybecause PTA duration is amenable to intervention. The presence ofPTA is also a risk factor for disrupted sleep, posttraumatic epi-lepsy, and reduced effort in rehabilitation—all associated withpoor patient outcomes.12–14
Despite the importance of PTA, health care professionalsdo not always recognize the seriousness of prolonged PTA andclinical practices in this domain remain inconsistent. To improvethe management of TBI patients in PTA, this commentary willclarify the symptomatology of PTA for an accurate diagnosis,the use of pharmacological agents in minimizing PTA duration,and the role of early rehabilitation.
STANDARDIZING TERMINOLOGY
The terminology of “posttraumatic amnesia” is mislead-ing, as the name alludes to a single primary deficit in memory.While the inability to consolidate new memories or anterogradeamnesia is the hallmark of PTA, recent studies further character-ized PTA as impairments in attention, executive function, disin-hibition, orientation, and retrograde memory.7,15–17 The widearray of symptoms led to controversies around the primaryimpairment in PTA. Stuss et al.17 argued that attention deficitwas the predominant disorder, and proposed that “posttraumaticconfusion” was better suited to describe this state. Other terms,such as “posttraumatic delirium” and “posttraumatic agitation,”were also considered equivalents or substitutes of PTA.15
A literature review for PTA is difficult given the inconsis-tencies in basic terminology. Unsurprisingly, PTA is not a Med-ical Subject Heading in PubMed, which further supports thecompelling need to standardize the terminology for TBI patientsin this acute recovery period. In this commentary, the operationaldefinition of PTA is the transitional state of impaired conscious-ness between time of injury and the returned ability to form con-tinuous memories.
PTA ASSESSMENT TOOLS
Numerous tools are used for PTA assessments, includingthe Orientation Log,18 Westmead PTA Scale,19 ModifiedOxford PTA Scale,20 Galveston Orientation and Amnesia Test
1033
ealth, Inc. All rights reserved.
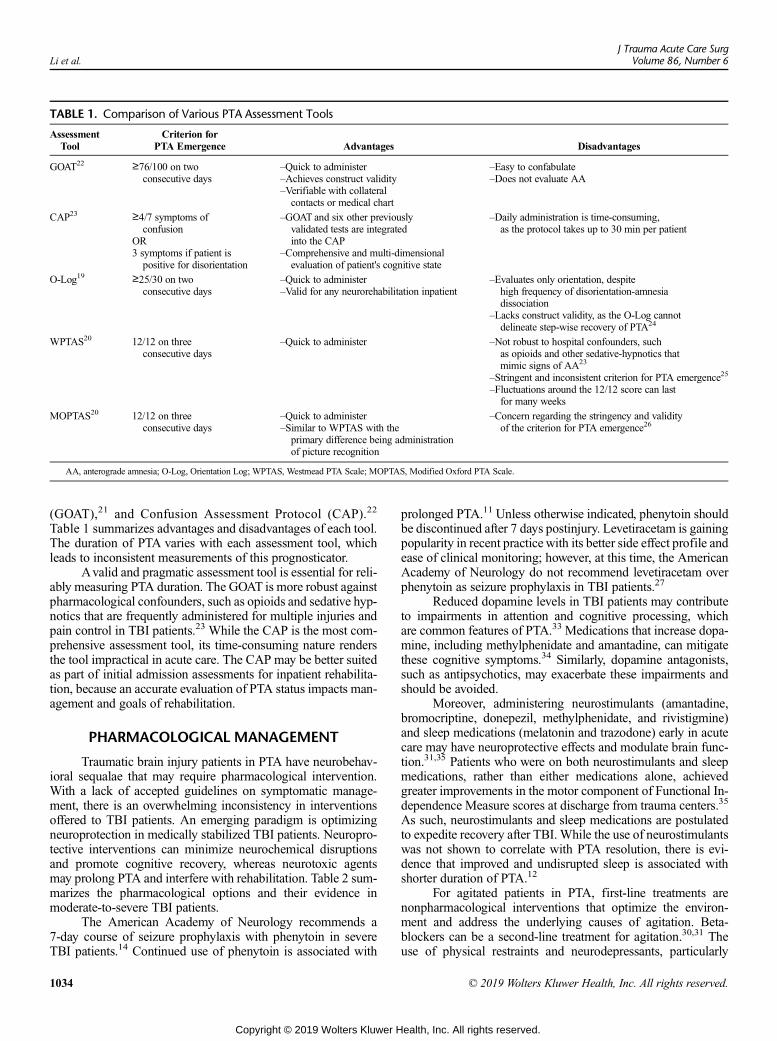
TABLE 1. Comparison of Various PTA Assessment Tools
AssessmentTool
Criterion forPTA Emergence Advantages Disadvantages
GOAT22 ≥76/100 on twoconsecutive days
–Quick to administer–Achieves construct validity–Verifiable with collateral
contacts or medical chart
–Easy to confabulate–Does not evaluate AA
CAP23 ≥4/7 symptoms ofconfusion
OR3 symptoms if patient ispositive for disorientation
–GOAT and six other previouslyvalidated tests are integratedinto the CAP
–Comprehensive and multi-dimensionalevaluation of patient's cognitive state
–Daily administration is time-consuming,as the protocol takes up to 30 min per patient
O-Log19 ≥25/30 on twoconsecutive days
–Quick to administer–Valid for any neurorehabilitation inpatient
–Evaluates only orientation, despitehigh frequency of disorientation-amnesiadissociation
–Lacks construct validity, as the O-Log cannotdelineate step-wise recovery of PTA24
WPTAS20 12/12 on threeconsecutive days
–Quick to administer –Not robust to hospital confounders, suchas opioids and other sedative-hypnotics thatmimic signs of AA23
–Stringent and inconsistent criterion for PTA emergence25
–Fluctuations around the 12/12 score can lastfor many weeks
MOPTAS20 12/12 on threeconsecutive days
–Quick to administer–Similar to WPTAS with the
primary difference being administrationof picture recognition
–Concern regarding the stringency and validityof the criterion for PTA emergence26
AA, anterograde amnesia; O-Log, Orientation Log; WPTAS, Westmead PTA Scale; MOPTAS, Modified Oxford PTA Scale.
Li et al.J Trauma Acute Care Surg
Volume 86, Number 6
(GOAT),21 and Confusion Assessment Protocol (CAP).22
Table 1 summarizes advantages and disadvantages of each tool.The duration of PTA varies with each assessment tool, whichleads to inconsistent measurements of this prognosticator.
Avalid and pragmatic assessment tool is essential for reli-ably measuring PTA duration. The GOAT is more robust againstpharmacological confounders, such as opioids and sedative hyp-notics that are frequently administered for multiple injuries andpain control in TBI patients.23 While the CAP is the most com-prehensive assessment tool, its time-consuming nature rendersthe tool impractical in acute care. The CAP may be better suitedas part of initial admission assessments for inpatient rehabilita-tion, because an accurate evaluation of PTA status impacts man-agement and goals of rehabilitation.
PHARMACOLOGICAL MANAGEMENT
Traumatic brain injury patients in PTA have neurobehav-ioral sequalae that may require pharmacological intervention.With a lack of accepted guidelines on symptomatic manage-ment, there is an overwhelming inconsistency in interventionsoffered to TBI patients. An emerging paradigm is optimizingneuroprotection in medically stabilized TBI patients. Neuropro-tective interventions can minimize neurochemical disruptionsand promote cognitive recovery, whereas neurotoxic agentsmay prolong PTA and interfere with rehabilitation. Table 2 sum-marizes the pharmacological options and their evidence inmoderate-to-severe TBI patients.
The American Academy of Neurology recommends a7-day course of seizure prophylaxis with phenytoin in severeTBI patients.14 Continued use of phenytoin is associated with
1034
Copyright © 2019 Wolters Kluwer H
prolonged PTA.11 Unless otherwise indicated, phenytoin shouldbe discontinued after 7 days postinjury. Levetiracetam is gainingpopularity in recent practicewith its better side effect profile andease of clinical monitoring; however, at this time, the AmericanAcademy of Neurology do not recommend levetiracetam overphenytoin as seizure prophylaxis in TBI patients.27
Reduced dopamine levels in TBI patients may contributeto impairments in attention and cognitive processing, whichare common features of PTA.33 Medications that increase dopa-mine, including methylphenidate and amantadine, can mitigatethese cognitive symptoms.34 Similarly, dopamine antagonists,such as antipsychotics, may exacerbate these impairments andshould be avoided.
Moreover, administering neurostimulants (amantadine,bromocriptine, donepezil, methylphenidate, and rivistigmine)and sleep medications (melatonin and trazodone) early in acutecare may have neuroprotective effects and modulate brain func-tion.31,35 Patients who were on both neurostimulants and sleepmedications, rather than either medications alone, achievedgreater improvements in the motor component of Functional In-dependence Measure scores at discharge from trauma centers.35
As such, neurostimulants and sleep medications are postulatedto expedite recovery after TBI. While the use of neurostimulantswas not shown to correlate with PTA resolution, there is evi-dence that improved and undisrupted sleep is associated withshorter duration of PTA.12
For agitated patients in PTA, first-line treatments arenonpharmacological interventions that optimize the environ-ment and address the underlying causes of agitation. Beta-blockers can be a second-line treatment for agitation.30,31 Theuse of physical restraints and neurodepressants, particularly
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
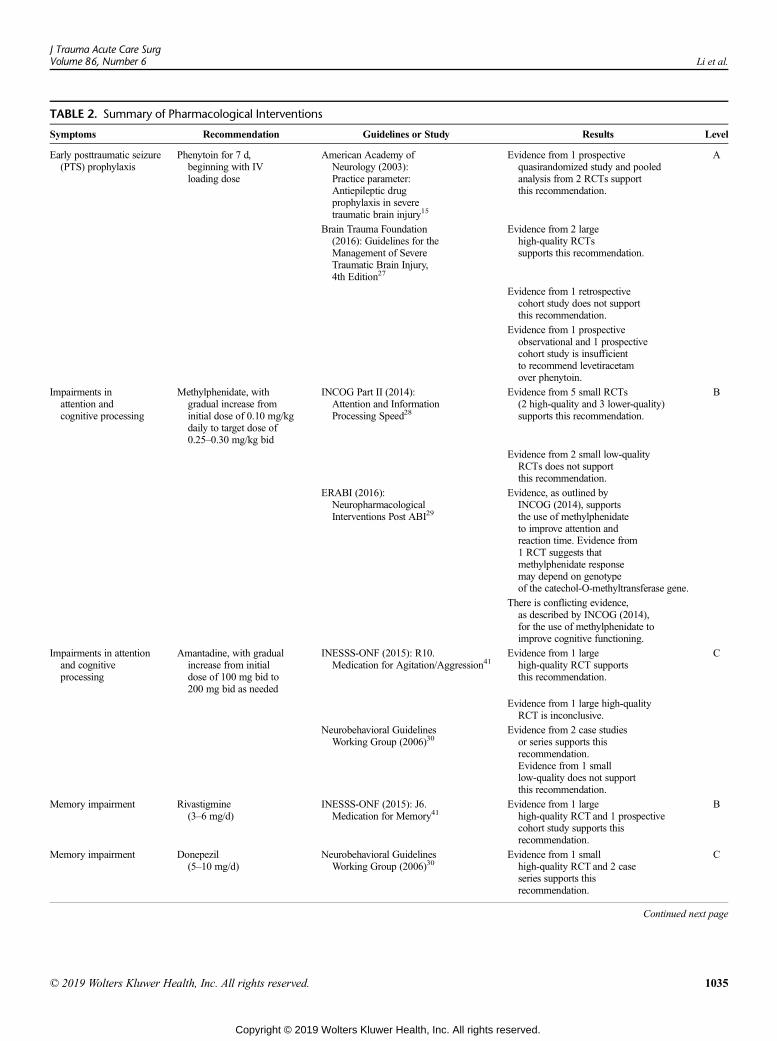
TABLE 2. Summary of Pharmacological Interventions
Symptoms Recommendation Guidelines or Study Results Level
Early posttraumatic seizure(PTS) prophylaxis
Phenytoin for 7 d,beginning with IVloading dose
American Academy ofNeurology (2003):Practice parameter:Antiepileptic drugprophylaxis in severetraumatic brain injury15
Evidence from 1 prospectivequasirandomized study and pooledanalysis from 2 RCTs supportthis recommendation.
A
Brain Trauma Foundation(2016): Guidelines for theManagement of SevereTraumatic Brain Injury,4th Edition27
Evidence from 2 largehigh-quality RCTssupports this recommendation.
Evidence from 1 retrospectivecohort study does not supportthis recommendation.
Evidence from 1 prospectiveobservational and 1 prospectivecohort study is insufficientto recommend levetiracetamover phenytoin.
Impairments inattention andcognitive processing
Methylphenidate, withgradual increase frominitial dose of 0.10 mg/kgdaily to target dose of0.25–0.30 mg/kg bid
INCOG Part II (2014):Attention and InformationProcessing Speed28
Evidence from 5 small RCTs(2 high-quality and 3 lower-quality)supports this recommendation.
B
Evidence from 2 small low-qualityRCTs does not supportthis recommendation.
ERABI (2016):NeuropharmacologicalInterventions Post ABI29
Evidence, as outlined byINCOG (2014), supportsthe use of methylphenidateto improve attention andreaction time. Evidence from1 RCT suggests thatmethylphenidate responsemay depend on genotypeof the catechol-O-methyltransferase gene.
There is conflicting evidence,as described by INCOG (2014),for the use of methylphenidate toimprove cognitive functioning.
Impairments in attentionand cognitiveprocessing
Amantadine, with gradualincrease from initialdose of 100 mg bid to200 mg bid as needed
INESSS-ONF (2015): R10.Medication for Agitation/Aggression41
Evidence from 1 largehigh-quality RCT supportsthis recommendation.
C
Evidence from 1 large high-qualityRCT is inconclusive.
Neurobehavioral GuidelinesWorking Group (2006)30
Evidence from 2 case studiesor series supports thisrecommendation.Evidence from 1 smalllow-quality does not supportthis recommendation.
Memory impairment Rivastigmine(3–6 mg/d)
INESSS-ONF (2015): J6.Medication for Memory41
Evidence from 1 largehigh-quality RCT and 1 prospectivecohort study supports thisrecommendation.
B
Memory impairment Donepezil(5–10 mg/d)
Neurobehavioral GuidelinesWorking Group (2006)30
Evidence from 1 smallhigh-quality RCT and 2 caseseries supports thisrecommendation.
C
Continued next page
J Trauma Acute Care SurgVolume 86, Number 6 Li et al.
© 2019 Wolters Kluwer Health, Inc. All rights reserved. 1035
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
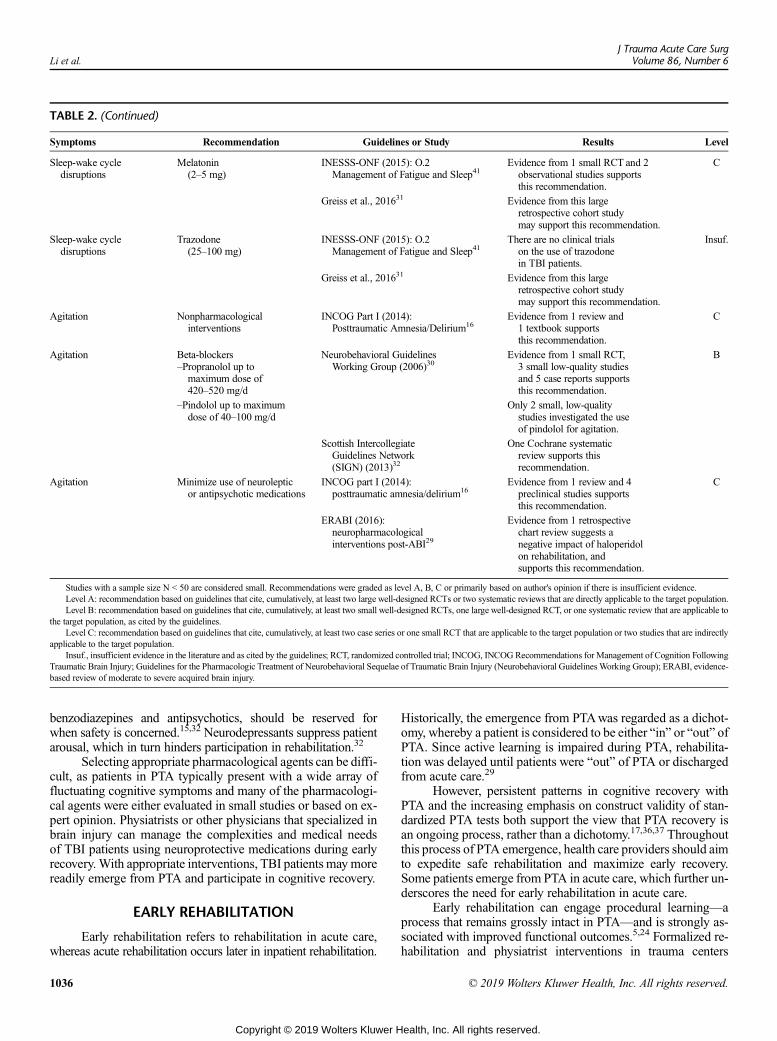
TABLE 2. (Continued)
Symptoms Recommendation Guidelines or Study Results Level
Sleep-wake cycledisruptions
Melatonin(2–5 mg)
INESSS-ONF (2015): O.2Management of Fatigue and Sleep41
Evidence from 1 small RCT and 2observational studies supportsthis recommendation.
C
Greiss et al., 201631 Evidence from this largeretrospective cohort studymay support this recommendation.
Sleep-wake cycledisruptions
Trazodone(25–100 mg)
INESSS-ONF (2015): O.2Management of Fatigue and Sleep41
There are no clinical trialson the use of trazodonein TBI patients.
Insuf.
Greiss et al., 201631 Evidence from this largeretrospective cohort studymay support this recommendation.
Agitation Nonpharmacologicalinterventions
INCOG Part I (2014):Posttraumatic Amnesia/Delirium16
Evidence from 1 review and1 textbook supportsthis recommendation.
C
Agitation Beta-blockers–Propranolol up to
maximum dose of420–520 mg/d
Neurobehavioral GuidelinesWorking Group (2006)30
Evidence from 1 small RCT,3 small low-quality studiesand 5 case reports supportsthis recommendation.
B
–Pindolol up to maximumdose of 40–100 mg/d
Only 2 small, low-qualitystudies investigated the useof pindolol for agitation.
Scottish IntercollegiateGuidelines Network(SIGN) (2013)32
One Cochrane systematicreview supports thisrecommendation.
Agitation Minimize use of neurolepticor antipsychotic medications
INCOG part I (2014):posttraumatic amnesia/delirium16
Evidence from 1 review and 4preclinical studies supportsthis recommendation.
C
ERABI (2016):neuropharmacologicalinterventions post-ABI29
Evidence from 1 retrospectivechart review suggests anegative impact of haloperidolon rehabilitation, andsupports this recommendation.
Studies with a sample size N < 50 are considered small. Recommendations were graded as level A, B, C or primarily based on author's opinion if there is insufficient evidence.Level A: recommendation based on guidelines that cite, cumulatively, at least two large well-designed RCTs or two systematic reviews that are directly applicable to the target population.Level B: recommendation based on guidelines that cite, cumulatively, at least two small well-designed RCTs, one large well-designed RCT, or one systematic review that are applicable to
the target population, as cited by the guidelines.Level C: recommendation based on guidelines that cite, cumulatively, at least two case series or one small RCT that are applicable to the target population or two studies that are indirectly
applicable to the target population.Insuf., insufficient evidence in the literature and as cited by the guidelines; RCT, randomized controlled trial; INCOG, INCOG Recommendations for Management of Cognition Following
Traumatic Brain Injury; Guidelines for the Pharmacologic Treatment of Neurobehavioral Sequelae of Traumatic Brain Injury (Neurobehavioral Guidelines Working Group); ERABI, evidence-based review of moderate to severe acquired brain injury.
Li et al.J Trauma Acute Care Surg
Volume 86, Number 6
benzodiazepines and antipsychotics, should be reserved forwhen safety is concerned.15,32 Neurodepressants suppress patientarousal, which in turn hinders participation in rehabilitation.32
Selecting appropriate pharmacological agents can be diffi-cult, as patients in PTA typically present with a wide array offluctuating cognitive symptoms and many of the pharmacologi-cal agents were either evaluated in small studies or based on ex-pert opinion. Physiatrists or other physicians that specialized inbrain injury can manage the complexities and medical needsof TBI patients using neuroprotective medications during earlyrecovery.With appropriate interventions, TBI patients maymorereadily emerge from PTA and participate in cognitive recovery.
EARLY REHABILITATION
Early rehabilitation refers to rehabilitation in acute care,whereas acute rehabilitation occurs later in inpatient rehabilitation.
1036
Copyright © 2019 Wolters Kluwer H
Historically, the emergence from PTAwas regarded as a dichot-omy, whereby a patient is considered to be either “in” or “out” ofPTA. Since active learning is impaired during PTA, rehabilita-tion was delayed until patients were “out” of PTA or dischargedfrom acute care.29
However, persistent patterns in cognitive recovery withPTA and the increasing emphasis on construct validity of stan-dardized PTA tests both support the view that PTA recovery isan ongoing process, rather than a dichotomy.17,36,37 Throughoutthis process of PTA emergence, health care providers should aimto expedite safe rehabilitation and maximize early recovery.Some patients emerge from PTA in acute care, which further un-derscores the need for early rehabilitation in acute care.
Early rehabilitation can engage procedural learning—aprocess that remains grossly intact in PTA—and is strongly as-sociated with improved functional outcomes.5,24 Formalized re-habilitation and physiatrist interventions in trauma centers
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.

J Trauma Acute Care SurgVolume 86, Number 6 Li et al.
correlate with shorter lengths of hospital stay and earlier dis-charge to inpatient rehabilitation.5,38 Trevena-Peters et al.39 re-ported that routine retraining activities of daily living duringPTA facilitated patients' functional recovery beyond the ex-pected natural recovery. These findings suggest that early reha-bilitation can and should capitalize on the functioning domainsof cognition.
The gradual emergence from PTA is a sensitive and op-portune stage of recovery that can benefit from personalized re-habilitation. Patients in PTA should be routinely screened forparticipation in therapies. Physicians are encouraged to collabo-rate with speech language pathologists, physiotherapists, oc-cupational therapists, and other members of the trauma teamto develop interprofessional care plans that support functionaland cognitive recovery in acute care. Personalizing early rehabil-itation to accommodate ongoing changes in patient cognitionand capability, accompanied by judicious use of neuroprotectivemedications, can strengthen patient readiness for rehabilitationand prevent overstimulation and its possible sequalae of agita-tion or delirium-like presentations.
Given the resources required and the high likelihood ofmultiple injuries, a formalized early rehabilitation program forTBI patients is best implemented in Levels I and II trauma cen-ters, which have more access to rehabilitation services thanLevels III or IV trauma centers. Integrating a formalized rehabil-itation program into acute care can ultimately improve patients'transition into the community and long-term functional out-comes while reducing their length of stay.
ACUTE REHABILITATION
Once sufficiently stabilized, TBI patients are typicallytransferred from acute care to an inpatient rehabilitation wardor a free-standing rehabilitation hospital for acute rehabilitation.Physiatrists or physicians who are familiar with a patient's func-tional status formulate a continued interprofessional rehabilita-tion plan and bridge the transition to acute rehabilitation.24
Oftentimes, patients have limited days in acute rehabilitation;thus, expediting PTA emergence in acute care can enable pa-tients to maximize their functional gains during their limitedtime in acute rehabilitation.
In addition to physical and cognitive recovery, psycholog-ical recovery plays an important role in continued rehabilitation,as posttraumatic stress disorder and anxiety-related symptomsincrease the risk of poor functional outcomes in TBI patients.37
Continued rehabilitation aims to mitigate complications associ-ated with prolonged bedrest and facilitate a holistic patient-centered recovery.
CONCLUSION
In the context of moderate-to-severe TBI, PTA durationcontinues to be a valuable prognosticator of long-term outcomes,and its susceptibility to intervention renders it as a unique tar-get for treatment. It is imperative that health care providersunderstand the complete symptomology of PTA, because thefluctuating symptoms cannot be attributed to amnesia alone.These symptoms include inattention, agitation, confusion, exec-utive dysfunction, and impaired self-awareness.
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer H
Personalized rehabilitation in acute care, coupled withneuroprotective interventions, can minimize PTA duration andoptimize patient engagement in therapies to improve functionaloutcomes. Trauma centers and rehabilitation hospitals are rec-ommended to institute the GOAT for routine evaluations ofTBI patients. Integrating the CAP into initial admission assess-ments for inpatient rehabilitation can play an influential role inmanagement planning. Beyond evaluating clinical utility, futureimplementation science studies examining the roll-out processesof these assessment tools, within an established organizationalworkflow, will be important to facilitate possible widespreadadoption of these recommendations.
A designated specialist should be responsible for leadingearly neuroprotective and rehabilitative interventions in acutecare. Physiatrists specialized in brain injuries are well equippedto undertake this role as part of the trauma team. This role in-cludes making clinical decisions based on the GOAT, managingneurobehavioral symptomswith minimal neurochemical disrup-tions, personalizing early rehabilitation in acute care, and devel-oping an interprofessional care plan that traverses subsequentstages of rehabilitation.
From assessment to intervention, managing TBI patientsin PTA can be a uniquely challenging experience that can makea lasting impact on patients' lives. An optimal functional andcognitive recovery is consistent with the fundamental goals ofacute care: after all, saving patient lives becomes more meaning-ful when the patient's abilities to experience life are simulta-neously preserved.
AUTHORSHIP
C.L., A.T., and L.R. conceived and shaped the idea of the article. C.L. andA.T. conducted the literature review and summarized the findings. C.L.wrote the article with input from all authors. A.T. and L.R. provided guid-ance and supervised the project. All authors discussed the recommenda-tions of the article and contributed to the final article.
DISCLOSURE
The authors declare no conflict of interest.
REFERENCES1. Faul M, Xu L, Wald MM, Coronado VG. Traumatic brain injury in the
united states: Emergency department visits, hospitalizations and deaths2002–2006. Atlanta, GA: Centers for Disease Control and Prevention, Na-tional Center for Injury Prevention and Control; 2010.
2. DiMaggio CJ, Avraham JB, Lee DC, Frangos SG, Wall SP. The epidemiol-ogy of emergency department trauma discharges in the United States. AcadEmerg Med. 2017;24(10):1244–1256.
3. Harrison-Felix C, Pretz C, Hammond FM, Cuthbert JP, Bell J, Corrigan J,Miller AC, Haarbauer-Krupa J. Life expectancy after inpatient rehabilitationfor traumatic brain injury in the United States. J Neurotrauma. 2015;32(23):1893–1901.
4. American College of Surgeons Committee on Trauma. Chapter 12: Rehabil-itation. In: Resources for optimal care of the injured patient. 6th ed. Chicago,IL: American College of Surgeons; 2014:88. https://www.facs.org/~/media/files/quality%20programs/trauma/vrc%20resources/resources%20for%20optimal%20care.ashx. Accessed 08-22-2018.
5. Wagner AK, Fabio T, Zafonte RD, Goldberg G, Marion DW, Peitzman AB.Physical medicine and rehabilitation consultation: relationships with acutefunctional outcome, length of stay, and discharge planning after traumaticbrain injury. Am J Phys Med Rehabil. 2003;82(7):526–536.
6. TamAK, Berbrayer D, Robinson LR. What should be the role of physiatristsin early acute care rehabilitation?: current literature, models of care, andthoughts for the future. Am J Phys Med Rehabil. 2016;95(3):225–229.
1037
ealth, Inc. All rights reserved.
Li et al.J Trauma Acute Care Surg
Volume 86, Number 6
7. Nakase-Thompson R, Sherer M, Yablon SA, Nick TG, Trzepacz PT. Acuteconfusion following traumatic brain injury. Brain Inj. 2004;18(2):131–142.
8. Sigurdardottir S, Andelic N, Wehling E, Roe C, Anke A, Skandsen T,Holthe OO, Jerstad T, Aslaksen PM, SchankeAK. Neuropsychological func-tioning in a national cohort of severe traumatic brain injury: demographicand acute injury-related predictors. J Head Trauma Rehabil. 2015;30(2):E1–E12.
9. Walker W, Stromberg KA, Marwitz JH, Sima AP, Agyemang AA,Graham KM, Harrison-Felix C, Hoffman JM, Brown AW, Kreutzer JS,et al. Predicting long-term global outcome after traumatic brain injury: devel-opment of a practical prognostic tool using the traumatic brain injury modelsystems national database. J Neurotrauma. 2018;35:1587–1595.
10. Nakase-Richardson R, Sherer M, Seel RT, Hart T, Hanks R,Arango-Lasprilla JC, Yablon SA, Sander AM, Barnett SD, Walker WC,et al. Utility of post-traumatic amnesia in predicting 1-year productivity follow-ing traumatic brain injury: comparison of the Russell and Mississippi PTAclassification intervals. J Neurol Neurosurg Psychiatry. 2011;82(5):494–499.
11. Ellenberg JH, Levin HS, Saydjari C. Posttraumatic amnesia as a predictor ofoutcome after severe closed head injury. Prospective assessment. ArchNeurol. 1996;53(8):782–791.
12. Makley MJ, Johnson-Greene L, Tarwater PM, Kreuz AJ, Spiro J, Rao V,Celnik PA. Return of memory and sleep efficiency following moderate to se-vere closed head injury. Neurorehabil Neural Repair. 2009;23(4):320–326.
13. Seel RT, Corrigan JD, Dijkers MP, Barrett RS, Bogner J, Smout RJ,Garmoe W, Horn SD. Patient effort in traumatic brain injury inpatient reha-bilitation: course and associations with age, brain injury severity, and timepostinjury. Arch Phys Med Rehabil. 2015;96(Suppl 8):S235–S244.
14. Chang BS, Lowenstein DH. Practice parameter: antiepileptic drug prophy-laxis in severe traumatic brain injury. Neurology. 2003;60(1):10–16. http://n.neurology.org/content/60/1/10.abstract. Accessed 08-22-2018.
15. Ponsford J, Janzen S, McIntyre A, Bayley M, Velikonja D, Tate R, , INCOGExpert Panel. INCOG recommendations for management of cognition fol-lowing traumatic brain injury, part I: posttraumatic amnesia/delirium. J HeadTrauma Rehabil. 2014;29(4):307–320.
16. Marshman LA, Jakabek D, HennessyM, Quirk F, Guazzo EP. Post-traumaticamnesia. J Clin Neurosci. 2013;20(11):1475–1481.
17. Stuss DT, Binns MA, Carruth FG, Levine B, Brandys CE, Moulton RJ,SnowWG, Schwartz ML. The acute period of recovery from traumatic braininjury: posttraumatic amnesia or posttraumatic confusional state? J Neurosurg.1999;90(4):635–643.
18. Novack TA, Dowler RN, Bush BA, Glen T, Schneider JJ. Validity of the ori-entation log, relative to the Galveston orientation and amnesia test. J HeadTrauma Rehabil. 2000;15(3):957–961.
19. Shores EA, Marosszeky JE, Sandanam J, Batchelor J. Preliminary validationof a clinical scale for measuring the duration of post-traumatic amnesia.MedJ Aust. 1986;144(11):569–572.
20. Fortuny LA, Briggs M, Newcombe F, Ratcliff G, Thomas C. Measuring theduration of post traumatic amnesia. J Neurol Neurosurg Psychiatry. 1980;43(5):377–379.
21. Levin HS, O'Donnell VM, Grossman RG. The Galveston orientation andamnesia test. A practical scale to assess cognition after head injury. J NervMent Dis. 1979;167(11):675–684.
22. Sherer M, Nakase-Thompson R, Yablon SA, Gontkovsky ST. Multidimen-sional assessment of acute confusion after traumatic brain injury. Arch PhysMed Rehabil. 2005;86(5):896–904.
23. McLellan J, Marshman LAG, HennessyM. Anterograde amnesia and disori-entation are associated with in-patients without traumatic brain injury taking
1038
Copyright © 2019 Wolters Kluwer H
opioids. Retrograde amnesia (RA) is absent. RA assessment should be inte-gral to post-traumatic amnesia testing. J Clin Neurosci. 2017;44:184–187.
24. Carney N, Totten AM, O'Reilly C, et al. Guidelines for the management ofsevere traumatic brain injury, fourth edition. Neurosurgery. 2017;80(1):6–15.
25. Stahl S. Stahl's Essential Pyschopharmacology. 4th ed. New York, NY:Cambridge University Press; 2013.
26. Willmott C, Ponsford J. Efficacy of methylphenidate in the rehabilitation ofattention following traumatic brain injury: A randomised, crossover, doubleblind, placebo controlled inpatient trial. J Neurol Neurosurg Psychiatry.2009;80(5):552–557.
27. Greiss C, Yonclas PP, Jasey N, et al. Presence of a dedicated trauma centerphysiatrist improves functional outcomes following traumatic brain injury.J Trauma Acute Care Surg. 2016;80(1):70–75.
28. Neurobehavioral Guidelines Working Group, Warden DL, Gordon B, et al.Guidelines for the pharmacologic treatment of neurobehavioral sequelae oftraumatic brain injury. J Neurotrauma. 2006;23(10):1468–1501.
29. Scottish Intercollegiate Guidelines Network (SIGN). Chapter 6: Rehabil-itation of behavioural and emotional disorders. In: Brain Injury Rehabil-itation in Adults. Edinburgh, Scotland: A national clinical guideline; 2013:23. https://www.sign.ac.uk/assets/sign130.pdf. Accessed October 31, 2018.
30. BayleyM, Janzen S, Anderson R, Aubut J, Lee A, Teasell R. Evidence-basedreview of moderate to severe acquired brain injury: Module 12 neurophar-macological interventions post ABI. https://www.abiebr.com/sites/default/files/modules/Module12_V12_final%20draft.pdf. Updated 2018. AccessedOctober 9, 2018.
31. Gasquoine PG. Learning in post-traumatic amnesia following extremelysevere closed head injury. Brain Inj. 1991;5(2):169–175.
32. Leach K, Kinsella G, Jackson M, Matyas T. Recovery of components ofmemory in post-traumatic amnesia. Brain Inj. 2006;20(12):1241–1249.
33. Kean J, Abell M, Malec JF, Trzepacz PT. Rasch analysis of the orientationlog and reconsideration of the latent construct during inpatient rehabilitation.J Head Trauma Rehabil. 2011;26(5):364–374.
34. Steiner E, Murg-Argeny M, Steltzer H. The severe traumatic brain injury inAustria: Early rehabilitative treatment and outcome. J Trauma Manag Out-comes. 2016;10:5.
35. Mackay LE, Bernstein BA, Chapman PE, Morgan AS, Milazzo LS. Earlyintervention in severe head injury: Long-term benefits of a formalized pro-gram. Arch Phys Med Rehabil. 1992;73(7):635–641.
36. Trevena-Peters J, McKay A, Spitz G, Suda R, Renison B, Ponsford J.Efficacy of activities of daily living retraining during posttraumatic amnesia:A randomized controlled trial. Arch Phys Med Rehabil. 2018;99(2):329–337.e2.
37. Zatzick DF, Rivara FP, Jurkovich GJ, et al. Multisite investigation of trau-matic brain injuries, posttraumatic stress disorder, and self-reported healthand cognitive impairments. Arch Gen Psychiatry. 2010;67(12):1291–1300.
38. Tate RL, Pfaff A, Baguley IJ, et al. A multicentre, randomised trial examin-ing the effect of test procedures measuring emergence from post-traumaticamnesia. J Neurol Neurosurg Psychiatry. 2006;77(7):841–849.
39. Ponsford J, Bayley M, Wiseman-Hakes C, et al. INCOG recommendationsfor management of cognition following traumatic brain injury, part II: Atten-tion and information processing speed. J Head Trauma Rehabil. 2014;29(4):321–337.
40. INESSS-ONF. Clinical practice guideline for the rehabilitation of adultswith moderate to severe TBI. https://braininjuryguidelines.org/modtosevere/.Updated 2015. Accessed October 9, 2018.
© 2019 Wolters Kluwer Health, Inc. All rights reserved.
ealth, Inc. All rights reserved.
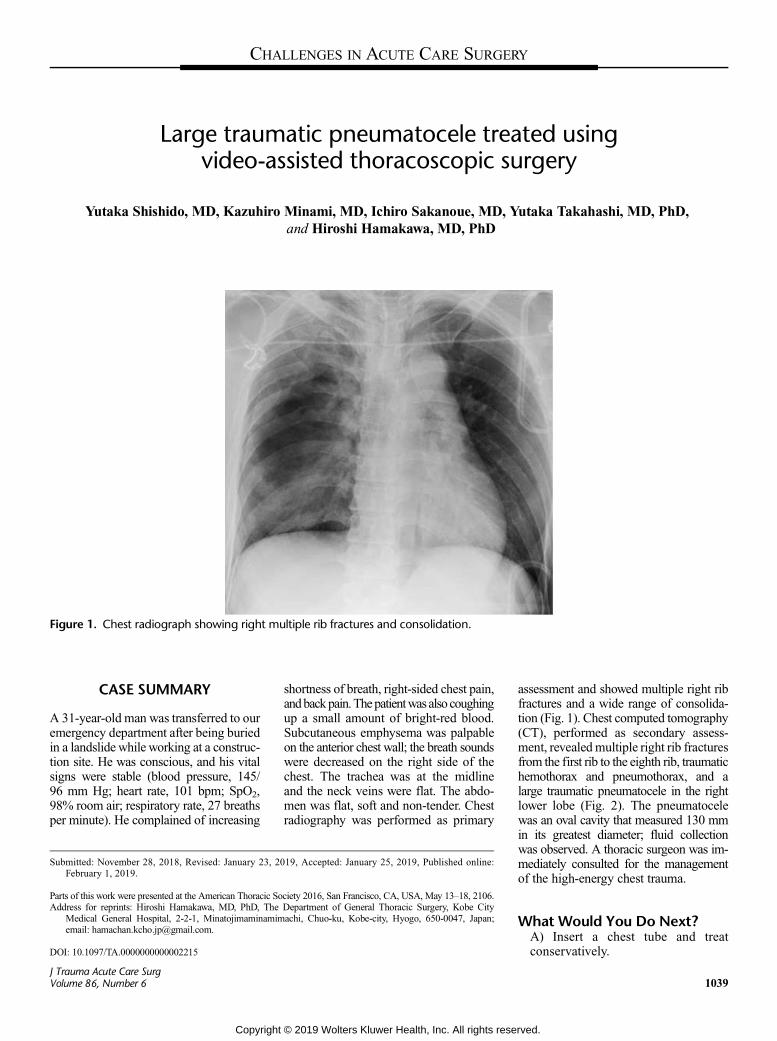
CHALLENGES IN ACUTE CARE SURGERY
Large traumatic pneumatocele treated usingvideo-assisted thoracoscopic surgery
Yutaka Shishido, MD, Kazuhiro Minami, MD, Ichiro Sakanoue, MD, Yutaka Takahashi, MD, PhD,and Hiroshi Hamakawa, MD, PhD
Figure 1. Chest radiograph showing right multiple rib fractures and consolidation.
CASE SUMMARY
A 31-year-old man was transferred to ouremergency department after being buriedin a landslide while working at a construc-tion site. He was conscious, and his vitalsigns were stable (blood pressure, 145/96 mm Hg; heart rate, 101 bpm; SpO2,98% room air; respiratory rate, 27 breathsper minute). He complained of increasing
Submitted: November 28, 2018, Revised: January 23, 20February 1, 2019.
Parts of this work were presented at the American Thoracic SoAddress for reprints: Hiroshi Hamakawa, MD, PhD, The
Medical General Hospital, 2-2-1, Minatojimaminamimemail: [email protected].
DOI: 10.1097/TA.0000000000002215
J Trauma Acute Care SurgVolume 86, Number 6
Copyright
shortness of breath, right-sided chest pain,andbackpain.Thepatientwas also coughingup a small amount of bright-red blood.Subcutaneous emphysema was palpableon the anterior chest wall; the breath soundswere decreased on the right side of thechest. The trachea was at the midlineand the neck veins were flat. The abdo-men was flat, soft and non-tender. Chestradiography was performed as primary
19, Accepted: January 25, 2019, Published online:
ciety 2016, San Francisco, CA, USA, May 13–18, 2106.Department of General Thoracic Surgery, Kobe Cityachi, Chuo-ku, Kobe-city, Hyogo, 650-0047, Japan;
© 2019 Wolters Kluwer Health, Inc. All rights rese
assessment and showed multiple right ribfractures and a wide range of consolida-tion (Fig. 1). Chest computed tomography(CT), performed as secondary assess-ment, revealed multiple right rib fracturesfrom the first rib to the eighth rib, traumatichemothorax and pneumothorax, and alarge traumatic pneumatocele in the rightlower lobe (Fig. 2). The pneumatocelewas an oval cavity that measured 130 mmin its greatest diameter; fluid collectionwas observed. A thoracic surgeon was im-mediately consulted for the managementof the high-energy chest trauma.
What Would You Do Next?A) Insert a chest tube and treatconservatively.
1039
rved.

Figure 2. Chest CT scan showing multiple right rib fractures, pneumothorax, and a large pneumatocele in the right lower lung lobe.
Shishido et al.J Trauma Acute Care Surg
Volume 86, Number 6
B) Insert a chest tube and intubateimmediately.C) Intubate immediately and performan emergency surgery.
What We Did and WhyC) Intubate immediately and performan emergency surgery.
The patient was taken to the oper-ating room and intubated immediatelyusing a double-lumen endotracheal tubeunder general anesthesia. We noted activebleeding flowing away from the endotra-cheal tube; thus, the anesthesiologistsneeded to suction continuously.We plannedfor an urgent right lower lobectomy fol-lowing thoracoscopic evaluation usingthe video-assisted thoracoscopic surgery(VATS) technique. First, we conducteda thoracoscopic evaluation via intercostalthoracic ports, 11.5 mm in diameter. Alarge volume of hemorrhagic fluid filled thepleural cavity, and the mediastinal pleurawas partly cracked; however, intrapleuralactive bleeding was not observed. Whilethe right upper and middle lobes were in-tact, the right lower lobe was congestedand markedly enlarged. The right lowerVATS lobectomy using two intercostal11.5-mm diameter thoracic ports and one45-mm-long utility port, was performed.Consequently, the active airway bleeding
1040
Copyright
immediately stopped, and neither thefractured rib protruding into the thoraciccavity nor the air leak was observed fol-lowing the lobectomy. The operationtime was 174 minutes, and the total vol-ume of hemorrhagic pleural fluid was200 mL. When the operation was com-pleted, the patient was extubated in goodrespiratory condition, with a SpO2 of95% to 99% room air, and no hemoptysiswas observed. He recovered uneventfullyand was discharged on postoperative day9. At 1 month after the injury, there wasneither any adverse event regarding theoperation nor major abnormalities onfollow-up chest radiography.
Traumatic pneumatocele typicallyresolves spontaneously; therefore, mostpatients are managed conservatively. How-ever, in complicated cases, surgery may berequired rather than conservative manage-ment. In this case, rapid induction and in-tubation for anesthesia was performed toprotect the airway, and we planned an ur-gent right lower lobectomy. This was be-cause the patient coughed up bright-redblood, and fluid collection into a largepneumatocele on the chest CT was ob-served. Both indicated that pneumatocelewas the source of the active airway bleed-ing. In emergency situations of high-energychest trauma, which could cause multiplerib fractures and lung injuries, conventional
© 2019 W
© 2019 Wolters Kluwer Health, Inc. All rights rese
thoracotomy might be recommended.However, we first conducted a thoracoscopicevaluation as a primary survey, becausethe vital signs of the patient were withinsafe limits, and it was necessary to decidewhether operation could be performed inthe VATS manner or not. There was nointrapleural active bleeding, and the dam-age was limited to the right lower lobe.Based on these observations, it was esti-mated that we could complete the VATSlobectomy, which had the advantage ofminimizing further deformation of thechest wall by the multiple rib fracturesand reducing the postoperative pain toavoid rib spreading and injury whichcould lead to further collapse of the tho-racic cage. Thus, the strategy of usingthe VATS technique might be beneficialfor postoperative respiratory functionthorough maintaining the elasticity ofthoracic cage within an adequate rangeand preventing the progression of restric-tive ventilatory impairment, which couldalso contribute to shorten hospital stays.
AUTHORSHIP
Y.S. and K.M. contributed equally to thewritingof this article.
DISCLOSURE
The authors declare no conflicts of interest.No funding has been received for this workfrom NIH, Wellcome Trust, or HHMI.
olters Kluwer Health, Inc. All rights reserved.
rved.

From the Divisions oAddress for reprints
Rkarmy-jones@
DOI: 10.1097/TA.00
J Trauma Acute CaVolume 86, Numb
Commentary on “Large traumaticpneumatocele treated using video-assisted
thoracoscopic surgery”
Riyad Karmy-Jones, MD, Vancouver, Washington
P osttraumatic pneumatoceles can result from a combination of crush and/or shear effect. Lowerlobe rents, such as described in this case, have been attributed to shearing of the lung where it
is fixed by the inferior pulmonary ligament. In general, the natural history is benign, but these cavitiescan be complicated by infection, and inmost cases, the management is similar to that of lung abscess.
In this case, the pneumatocele presented at the extreme of the presentation, really representinga massive parenchymal and possible second-order airway disruption, as manifested by the radio-graphic and clinical findings of significant air leak, shift, and hemoptysis. This, appropriately, wasmanaged by early surgery rather than expectant management.
The authors chose lobectomy, which in this setting was appropriate. Although tempting to per-form lesser resection, in this setting, there is evidence to suggest that lobectomy is associated withlower postsurgical risk of infection, parenchymal necrosis and need for further surgery.
VATS lobectomy in nontrauma setting has been demonstrated to have reduction of postopera-tive morbidity. In this case, it appears that despite multiple rib fractures, the ribs were not misaligned,and a major advantage of VATS is it avoids rib displacement. Had there been frank bony disruption,the utility port sometimes can be placed over the ribs involved, affording an opportunity to plan someform of fixation.
Of note, the patient was stable enough to tolerate a double lumen tube and video-assisted thoracicsurgery (VATS) exploration. In unstable patients, those with massive chest wall disruption, and/ormajor air loss and hemoptysis, a single lumen tube is preferred, and thoracotomy is more appropriate.
The authors were able to hit the “sweet spot,” use a double lumen tube permitting VATS, andperform the correct operation, avoiding a lesser resection which would have been associated with in-creased postoperative complications.
DISCLOSURE
The author declares no conflict of interest.
f Thoracic/Vascular and Trauma Surgery, PeaceHealth Southwest Washington Medical Center (R.K-J.), Vancouver, Washington.: Riyad Karmy-Jones, MD, Southwest Washington Medical Center, Suite 301, building B 505 NE 87th Ave, 98664 Vancouver, WA, 98664; email:peacehealth.org.
00000000002274
re Surger 6 1041
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
AAST
September 18Y21, 2019Join the American Association for the Surgeryof Trauma for the 78th AnnualMeetingof AAST& Clinical Congress of Acute Care SurgerySheraton Dallas, Dallas, TXhttp://www.aast.org/Meetings/AnnualMeeting/Default.aspx
PEDIATRIC TRAUMA SOCIETY (PTS)6TH ANNUAL MEETING
November 13Y16, 2019Sheraton San Diego Hotel and MarinaSan Diego, CAhttp://pediatrictraumasociety.org/
33RD EAST ANNUALSCIENTIFIC ASSEMBLY
January 14Y18, 2020Loews Sapphire Falls ResortOrlando, FLhttps://www.east.org/education/annual-scientific-assembly
TRAUMA CENTER ASSOCIATION OFAMERICA’S 22ND ANNUAL
CONFERENCE
April 28YMay 3, 2019Luxor Hotel 18, 2019 Luxor Hotel & Casino inLas Vegas, NVhttps://www.traumacenters.org
ENDOVASCULAR RESUSCITATIONAND TRAUMA MANAGEMENT
(EVTM) SYMPOSIUM
November 17Y18, 2019Pan-American EVTM Denver,Colorado (#panamevtm2019)http://www.jevtm.com/evtm-symposium/
Please send your meeting and course information to [email protected] to be included in the Meetings/Courses sectionof the journal. Please contact [email protected] if you would like to highlight your event in The Journal of Traumaand Acute Care Surgery with a paid advertising placement.
MEETINGS/COURSES
J Trauma Acute Care SurgVolume 86, Number 61042
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.

Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
Featured Articles for CME Credit June 2019
Obesity as Protective Against, Rather than a Risk Factor for PostoperativeClostridium Difficile Infection: A Nationwide Retrospective Analysis of1,426,807 Surgical PatientsKarien Meier, MSc, Ask T. Nordestgaard, BSc, Ahmed I. Eid, MD, MSc, Napaporn Kongkaewpaisan, MD, Jae Moo Lee, BA,Manansun Kongwibulwut, MD, Kelsey R. Han, Nikolaos Kokoroskos, MD, April E. Mendoza, MD, MPH, Noelle Saillant,MD, David R. King, MD, George C. Velmahos, MD, PhD, MSEd, Haytham M.A. Kaafarani, MD, MPH, FACS(J Trauma Acute Care Surg. 2019;86(6):1001Y1009)
The Associations Between Initial Radiographic Findings andInterventions for Renal Hemorrhage After High-Grade Renal Trauma:The Multi-Institutional Genito-Urinary Trauma StudySorena Keihani, M.D., Bryn E. Putbrese, Douglas M. Rogers, Chong Zhang Raminder, Nirula Xian, Luo-Owen, KaushikMukherjee, Bradley J. Morris, Sarah Majercik, Joshua Piotrowski, Christopher M. Dodgion, Ian Schwartz, Sean P. Elliott,Erik S. DeSoucy, Scott Zakaluzny, Brenton G. Sherwood, Bradley A. Erickson, Nima Baradaran, Benjamin N. Breyer,Cameron N. Fick, Brian P. Smith, Barbara U. Okafor, Reza Askari, Brandi Miller, Richard A. Santucci, Matthew M. Carrick,Jurek F. Kocik, Timothy Hewitt, Frank N. Burks, Marta E. Heilbrun, Jeremy B. Myers(J Trauma Acute Care Surg. 2019;86(6):974Y982)
Low-Value Clinical Practices in Injury Care: A Scoping Review and ExpertConsultation SurveyLynne Moore, PhD, Francois Lauzier, MD, MSc, Pier-Alexandre, Tardif Khadidja, Malloum Boukar, MSc, Imen Farhat,MSc, Patrick Archambault, MD, MSc, Eric Mercier, MD, MSc, Francois Lamontagne, MD, MSc, Michael Chasse, MD, PhD,Henry Thomas Stelfox, MD, PhD, Simon Berthelot, MD, MSc, Belinda Gabbe, PhD, Fiona Lecky, MD, MSc, NatalieYanchar, MD, MSc, Howard Champion, MD, John Kortbeek, MD, Peter Cameron, MD, Paule Lessard Bonaventure, MD,MSc, Jerome Paquet, MD, Catherine Truchon, PhD, Alexis Francois Turgeon, MD, MSc(J Trauma Acute Care Surg. 2019;86(6):983Y993)
CME ARTICLE 1
Obesity as protective against, rather than a risk factor forpostoperative Clostridium Difficile Infection: A nationwideretrospective analysis of 1,426,807 surgical patients
Karien Meier, MSc, Ask T. Nordestgaard, BSc, Ahmed I. Eid, MD,MSc,Napaporn Kongkaewpaisan, MD, Jae Moo Lee, BA, ManansunKongwibulwut,MD,KelseyR.Han,NikolaosKokoroskos,MD,April EMendoza,MD,MPH,Noelle Saillant,MD, DavidR. King,MD, GeorgeC. Velmahos, MD, PhD, MSEd, Haytham M.A. Kaafarani, MD, MPH,FACS(J Trauma Acute Care Surg. 2019;86(6):1001Y1009)
Impact Statement:Among patient risk factors, both obesity and underweight areoften found to be risk factors for infections, mortality, andhospitalization. In surgical patients specifically, obesity is as-sociated with increased perioperative morbidity as well as in-fectious complications such as urinary tract infection andsurgical site infections. Currently, more than a third of theUnited States adult population is obese. The United Statessurgical population reflect these biometric shifts, and the
inherent risks of increased nosocomial infections due to analtered immune response.More recently, obesity was suggestedas a potential risk factor for both community-acquired andhospital-onset Clostridium difficile infection (CDI). In thisnationwide population-based cohort study of 1,426,807 sur-gical patients, after adjustment for confounders, we surpris-ingly found an inverse and independent relationship betweenbody mass index (BMI) and CDI: the more obese the patient,the lower the risk for CDI compared to normal weight. Beingunderweight was associated with an increased risk for CDI,while the morbidly obese were at the lowest risk for CDI. Tothe best of our knowledge, this is the largest study exploringthe relationship between BMI and CDI in surgical patients.The exact mechanisms for the relationship between BMI andCDI in our study are uncertain, although it could be potentiallyexplained by the altered microbiome seen in obesity.
Article Objective:We sought to test the relationship between BMI and the inci-dence of postoperative CDI in surgical patients. We hypothe-sized that both the obese and the underweight surgical patient ismost susceptible to postsurgical intestinal CDI.
CONTINUING MEDICAL EDUCATION PROGRAM
J Trauma Acute Care SurgVolume 86, Number 6 e19
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
Learning Objective(s):- Analyze the relationship between being underweight or obesity, andClostridium difficile infection (CDI)- Evaluate risk factors for postoperative clostridium difficile infectionsin practice, given the risk factors identified by this paper- Differentiate between the obese and the underweight as patients thathave different risk profiles for infectious complications in general- Evaluate the effect of obesity and being underweight on the risk of CDI
QUESTION 1:For many reasons, the obese are generally considered at increased riskof postoperative infectious complications. Which answer is not one ofthose reasons?
A. Cardiometabolic risk profileB. Chronic pro-inflammatory state of the bodyC. Decreased immune cell functionD. Decreased mobilization after surgery
QUESTION 2:Why did the authors exclude bariatric surgery patients in additionalsensitivity analysis?
A. Bariatric surgery patients generally have a shorter hospitallength of stay.
B. Because of the extremely high incidence of CDI amongbariatric surgerypatients.
C. Because of the large proportion of obese patients amongbariatric surgerypatients.
D. Postoperative bowel function changes after bariatric surgery (e.g.,diarrhea), confound the association between obesity and CDI
QUESTION 3:
Which one of the following factors is not a significant risk factorfor postoperativeCDI in this nationwide retrospective analysis of1,426,807 surgical patients?
A. SmokingB. Steroid useC. Systemic sepsisD. Ventilator dependency
QUESTION 4:A 56-year old women, with a BMI of 41.2 kg/m 2 is admitted to thehospital for close monitoring after thoracic surgery. On the fourth dayof her hospital stay, she develops acute diarrhea (Q3 loose stools within24 hours). CDI is suspected, as there is no obvious alternative ex-planation for her acute diarrhea. Several diagnostic tests are availablefor the diagnosis of CDI, each with its advantages and limitations.Which of the following can be considered for the identification ofpathogenic CDI in this patient?
1. ELISA2. Fecal leukocyte testing3. Latex agglutination test4. Lower gastrointestinal endoscopy
5. Nucleic acid amplification testing (NAAT)6. PCR or EIA for glutamate dehydrogenase (GDH) antigen7. PCR or EIA for toxins A and B8. Rectal swab for toxin assay or anaerobic culture9. Radiographic imaging of the abdomen and pelvis
A. 1, 2, 4, 6, 9B. 3, 6C. 5, 6, 7D. 2, 7, 8
CME ARTICLE 2
The Associations Between Initial Radiographic Findings andInterventions for Renal Hemorrhage After High-Grade RenalTrauma: The Multi-Institutional Genito-Urinary Trauma Study
Sorena Keihani, M.D. Bryn E Putbrese Douglas M Rogers ChongZhang Raminder Nirula Xian Luo-Owen Kaushik Mukherjee BradleyJ Morris Sarah Majercik Joshua Piotrowski Christopher M DodgionIan Schwartz Sean P Elliott Erik S DeSoucy Scott Zakaluzny BrentonG Sherwood Bradley A Erickson Nima Baradaran Benjamin N BreyerCameron N Fick Brian P Smith Barbara U Okafor Reza Askari BrandiMiller Richard A Santucci MatthewMCarrick Jurek F Kocik TimothyHewitt Frank N Burks Marta E Heilbrun Jeremy B Myers
(J Trauma Acute Care Surg. 2019;86(6):974Y982)
Impact Statement:CT scans play a pivotal role in diagnosis and evaluation of renal trauma.Certain radiologic findings, such as hematoma characteristics and presenceof vascular contrast extravasation can be used to guide managementdecisions. This study confirms the important associations between anumber of radiologic findings and undergoing bleeding control inter-ventions after high-grade renal trauma. We also propose cut-offs forhematoma and laceration size that optimize prediction of bleedinginterventions for easier clinical use.
Article Objective:This study aims to explore the associations between different CTfindings and undergoing bleeding control interventions after high-graderenal trauma.
Learning Objective(s):- To recognize important CT findings in the evaluation of renal traumaand be able to identify or measure them- To be able to discuss the importance of vascular contrast extrava-sation after renal trauma- To assess hematoma rim distance in the axial plane- To use the proposed hematoma and laceration size cut-offs as sur-rogates for severity of renal injury and possible need for interventions
QUESTION 1:According to this study results, which of the following CT findings isassociated with a higher risk of undergoing bleeding interventions afterhigh-grade renal trauma?
A. Medical location of parenchymal lacerationB. Parenchymal devascularization Q25%C. Hematoma rim distance Q3.5 cmD. Presence of Q3 parenchymal lacerations
J Trauma Acute Care SurgVolume 86, Number 6Continuing Medical Education Program
e20 * 2019 Wolters Kluwer Health, Inc. All rights reserved.
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
QUESTION 2:According to the AAST organ injury scale for renal trauma, alaceration size Q1.0 cm is a criterion used to differentiate gradeII vs. III injuries. What laceration size cut-off was associatedwith bleeding interventions in the current study?
A. 0.5 cmB. 1.0 cmC. 2.5 cmD. 3.5 cm
QUESTION 3:What percentage of patients with vascular contrast extravasation un-derwent any bleeding control interventions in the current study?
A. 100% (all)B. 80%C. 40%D. 20%
QUESTION 4:A patient is transferred to the Emergency Department after hitting atreeonhis rightflankwhile skiing.Hehasabloodpressureof100/65mmHgand a heart rate of 95 and breathes normally. GCS is 15. A trauma CTscan with 10-min excretory phase is performed that shows 3 lacerationsthe deepest being 3 cm in size on the lateral aspect of the right kidney.Anassociated hematoma is measured 5 cm in the axial plane around thekidney. There is extravasation of contrastmaterial seen in the early phaseof theCT scan that is scattered and less prominent in the excretory phase.A wedged-shaped area of parenchymal devascularization is noticed onthe lower pole of the kidney approximately measuring about 1/4 of thetotal kidney volume.Combination ofwhich of the followingCTfindingswouldprovide a better estimationof theneed for bleeding interventions forthis patient?
A. Laceration depth + Parenchymal devascularizationB. Vascular contrast extravasation + Hematoma sizeC. Laceration location + Laceration depthD. Laceration location + Hematoma size
CME ARTICLE 3
Low-Value Clinical Practices in Injury Care: A Scoping Reviewand Expert Consultation Survey
Lynne Moore, PhD Francois Lauzier, MD, MSc Pier-AlexandreTardif Khadidja Malloum Boukar, MSc Imen Farhat, MSc PatrickArchambault, MD,MSc Eric Mercier, MD,MSc Francois Lamontagne,MD,MScMichael Chasse, MD, PhDHenry Thomas Stelfox, MD, PhDSimonBerthelot,MD,MScBelindaGabbe,PhDFionaLecky,MD,MScNatalie Yanchar, MD, MSc Howard Champion, MD John Kortbeek,MD Peter Cameron, MD Paule Lessard Bonaventure, MD, MScJerome Paquet, MD Catherine Truchon, PhD Alexis Francois Turgeon,MD, MSc
(J Trauma Acute Care Surg. 2019;86(6):983Y993)
Impact Statement:Tests and treatments that are not supported by evidence and could exposepatients to unnecessary harm, referred to here as low-value clinicalpractices, consume up to 30% of healthcare resources. ChoosingWiselyand other organisations have published lists of clinical practices to beavoided. However, few apply to injury and most are based uniquely onexpert consensus.
Article Objective:Identify low-value clinical practices in acute, intrahospital injury care
Learning Objective(s):
1. Define low-value care and describe its potential impact2. List three potentially low-value clinical practices in injury
care that may apply in your practice3. List three grey-zone clinical practices in injury care that
may apply in your practice4. Describe the research steps that must be completed after
this study to achieve the goal of reducing low-value carefor injury admissions
QUESTION 1:Which of the following is considered to be a level III study
A. Case-controlB. RetrospectiveC. Expert opinionD. Meta-analysis of randomized controlled trials
QUESTION 2:How many low-value practices are part of Brain TraumaFoundation guidelines?
A. FourB. ThreeC. NoneD. All practices
QUESTION 3:What percentage of experts considered ’ICU admission in adults withacute, mild complicated TBI not on irreversible anticoagulation’ to beclearly low- value?
A. 44%B. 33%C. 50%D. 22%
QUESTION 4:A child presents to the emergency department with mild TBI. Theinitial CT scan is positive. Under what circumstances may a repeat CTbe considered low- value for this patient?
A. If the child is over 9 years oldB. If there is no clinical deteriorationC. If the child is negative on the Canadian CT Head RuleD. If there is no high-impact injury mechanism
DISCLOSURESCME ARTICLE 1 NoneCME ARTICLE 2 Sean P. Elliot, Co-authorYUrotronic, Percuvision,Boston ScientificYMoney/GrantCME ARTICLE 3 John Kortbeek, Co-author - Employed by AHS &the University of Calgary as a medical leader and professor of Surgery,ShockTraumaAirRescueSocietyYMoney/Grant JeromePaquet,Co-author -Medtronic of CanadaYMoney/Grant
J Trauma Acute Care SurgVolume 86, Number 6 Continuing Medical Education Program
* 2019 Wolters Kluwer Health, Inc. All rights reserved. e21
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
Related Documents











