Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review) Teixeira DM, Barbosa MAP, Ferriani RA, Navarro PA, Raine-Fenning N, Nastri CO, Martins WP This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library 2013, Issue 7 http://www.thecochranelibrary.com Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review) Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Regular (ICSI) versus ultra-high magnification (IMSI) sperm
selection for assisted reproduction (Review)
Teixeira DM, Barbosa MAP, Ferriani RA, Navarro PA, Raine-Fenning N, Nastri CO, Martins
WP
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library2013, Issue 7
http://www.thecochranelibrary.com
Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

T A B L E O F C O N T E N T S
1HEADER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3SUMMARY OF FINDINGS FOR THE MAIN COMPARISON . . . . . . . . . . . . . . . . . . .
5BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
5OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
5METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
8RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Figure 1. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Figure 2. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Figure 3. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
Figure 4. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Figure 5. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Figure 6. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
14DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
15AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
15ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
15REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
17CHARACTERISTICS OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
32DATA AND ANALYSES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Analysis 1.1. Comparison 1 Ultra high (IMSI) versus regular magnification (ICSI), Outcome 1 Live birth per allocated
couple. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
Analysis 1.2. Comparison 1 Ultra high (IMSI) versus regular magnification (ICSI), Outcome 2 Clinical pregnancy per
allocated couple. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
Analysis 1.3. Comparison 1 Ultra high (IMSI) versus regular magnification (ICSI), Outcome 3 Miscarriage per clinical
pregnancy. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
Analysis 2.1. Comparison 2 IMSI versus ICSI: subgroup analysis by sperm quality, Outcome 1 Clinical pregnancy. . 35
35APPENDICES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
39CONTRIBUTIONS OF AUTHORS . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
39DECLARATIONS OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
40SOURCES OF SUPPORT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
40DIFFERENCES BETWEEN PROTOCOL AND REVIEW . . . . . . . . . . . . . . . . . . . . .
iRegular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
[Intervention Review]
Regular (ICSI) versus ultra-high magnification (IMSI) spermselection for assisted reproduction
Danielle M Teixeira1, Mariana AP Barbosa1 , Rui A Ferriani1, Paula A Navarro1, Nick Raine-Fenning2 , Carolina O Nastri1, Wellington
P Martins1
1Department of Obstetrics and Gynecology, Medical School of Ribeirao Preto, University of Sao Paulo, Ribeirao Preto, Brazil. 2Division
of Obstetrics and Gynaecology, School of Clinical Sciences, University of Nottingham, Nottingham, UK
Contact address: Wellington P Martins, Department of Obstetrics and Gynecology, Medical School of Ribeirao Preto, University of
Sao Paulo, Hospital das Clínicas da FMRP-USP, 8 andar, Campus Universitário, Campus Universitario da USP, Ribeirao Preto, Sao
Paulo, 14048-900, Brazil. [email protected].
Editorial group: Cochrane Menstrual Disorders and Subfertility Group.
Publication status and date: New, published in Issue 7, 2013.
Review content assessed as up-to-date: 8 May 2013.
Citation: Teixeira DM, Barbosa MAP, Ferriani RA, Navarro PA, Raine-Fenning N, Nastri CO, Martins WP. Regular (ICSI) versus
ultra-high magnification (IMSI) sperm selection for assisted reproduction. Cochrane Database of Systematic Reviews 2013, Issue 7. Art.
No.: CD010167. DOI: 10.1002/14651858.CD010167.pub2.
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
A B S T R A C T
Background
Subfertility is a condition found in up to 15% of couples of reproductive age. Gamete micromanipulation, such as intracytoplasmic
sperm injection (ICSI), is very useful for treating couples with compromised sperm parameters. Recently a new method of sperm
selection named ’motile sperm organelle morphology examination’ (MSOME) has been described and the spermatozoa selected under
high magnification (over 6000x) used for ICSI. This new technique, named intracytoplasmic morphologically selected sperm injection
(IMSI), has a theoretical potential to improve reproductive outcomes among couples undergoing assisted reproduction techniques
(ART).
Objectives
To compare the effectiveness and safety of IMSI and ICSI in couples undergoing ART.
Search methods
We searched for randomised controlled trials (RCT) in electronic databases (Cochrane Menstrual Disorders and Subfertility Group
Specialized Register, the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, EMBASE, PsycINFO, CINAHL,
LILACS), trials registers (ClinicalTrials.gov, Current Controlled Trials, World Health Organization International Clinical Trials Registry
Platform), conference abstracts (ISI Web of knowledge), and grey literature (OpenGrey); in addition, we handsearched the reference
lists of included studies and similar reviews. We performed the last electronic search on 8 May 2013.
Selection criteria
We considered only truly randomised controlled trials comparing ICSI and IMSI to be eligible; we did not include quasi or pseudo-
randomised trials. We included studies that permitted the inclusion of the same participant more than once (cross-over or ’per cycle’
trials) only if data regarding the first treatment of each participant were available.
1Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Data collection and analysis
Two review authors independently performed study selection, data extraction, and assessment of the risk of bias and we solved
disagreements by consulting a third review author. We corresponded with study investigators in order to resolve any queries, as required.
Main results
The search retrieved 294 records; from those, nine parallel design studies were included, comprising 2014 couples (IMSI = 1002; ICSI
= 1012). Live birth was evaluated by only one trial and there was no significant evidence of a difference between IMSI and ICSI (risk
ratio (RR) 1.14, 95% confidence interval (CI) 0.79 to 1.64, 1 RCT, 168 women, I2 = not applicable, low-quality evidence). IMSI was
associated with a significant improvement in clinical pregnancy rate (RR 1.29, 95% CI 1.07 to 1.56, 9 RCTs, 2014 women, I2 = 57%,
very-low-quality evidence). We downgraded the quality of this evidence because of imprecision, inconsistency, and strong indication
of publication bias. We found no significant difference in miscarriage rate between IMSI and ICSI (RR 0.82, 95% CI 0.59 to 1.14, 6
RCTs, 552 clinical pregnancies, I2 = 17%, very-low-quality evidence). None of the included studies reported congenital abnormalities.
Authors’ conclusions
Results from RCTs do not support the clinical use of IMSI. There is no evidence of effect on live birth or miscarriage and the evidence
that IMSI improves clinical pregnancy is of very low quality. There is no indication that IMSI increases congenital abnormalities.
Further trials are necessary to improve the evidence quality before recommending IMSI in clinical practice.
P L A I N L A N G U A G E S U M M A R Y
Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction
Background: sperm micromanipulation, such as intracytoplasmic sperm injection (ICSI), is very useful for treating couples in which
the male partner has a reduced sperm concentration or motility, or both. Recently, a new method of sperm selection named ’motile
sperm organelle morphology examination’ (MSOME) has been described, which analyses sperm under ultra-high powered (6000x)
magnification. Initial studies have shown that intracytoplasmic morphologically selected sperm injection (IMSI), using spermatozoa
selected under high magnification, is associated with higher pregnancy rates in couples with repeated implantation failures.
Search date: we searched the medical literature in May 2013 for studies that evaluated the effectiveness and safety of using ultra-high
magnification (over 6000x) for sperm selection prior to ICSI, compared with the use of a conventional ICSI procedure, with a 200-
400x magnification.
Study characteristics: we found nine randomised controlled trials, evaluating 2014 couples, that had compared regular ICSI with IMSI
for assisted reproduction. These studies were funded by fertility centres and universities.
Key results and quality of the evidence: for live birth, there was low-quality evidence compatible with either benefit or harm: for women
with a 38% chance of achieving live birth using regular ICSI, the chance of achieving live birth using ultra-high magnification (IMSI)
would be between 30% and 63%. For clinical pregnancy, there was very-low-quality evidence compatible with benefit: for women
with a 33% chance of achieving pregnancy using regular ICSI, the chance of achieving pregnancy using IMSI would be between 36%
and 52%; the quality of this evidence was downgraded because of imprecision, inconsistency of the observed effect across studies,
and high risk of publication bias. For miscarriage, there was very-low-quality evidence compatible with either benefit or harm: for
pregnant women with an 22% risk of miscarriage using regular ICSI, the risk using IMSI would be between 13% and 25%. There was
no evidence concerning congenital abnormalities. We concluded that the current evidence does not support using IMSI: there is no
evidence of benefit for live birth and miscarriage, we are very uncertain of the beneficial effect of IMSI in clinical pregnancy, and there
is no evidence of the effect of this intervention on congenital abnormalities. More studies to improve the evidence quality are necessary
before recommending IMSI in clinical practice.
2Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
S U M M A R Y O F F I N D I N G S F O R T H E M A I N C O M P A R I S O N [Explanation]
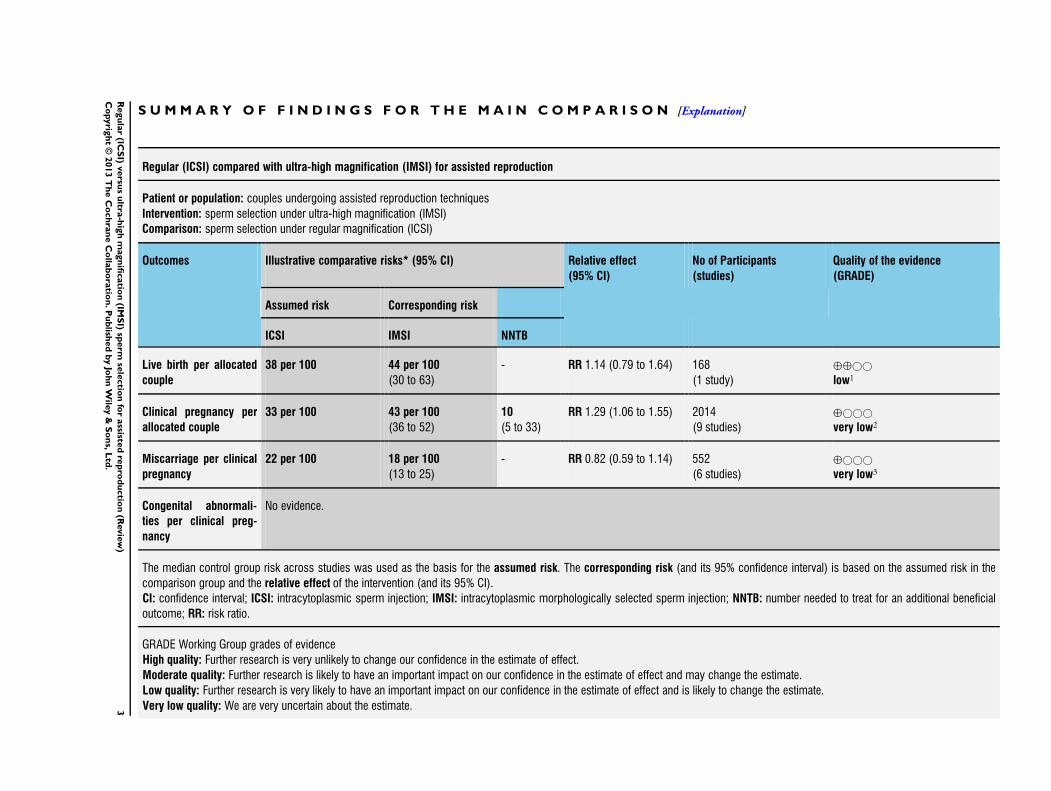
Regular (ICSI) compared with ultra-high magnification (IMSI) for assisted reproduction
Patient or population: couples undergoing assisted reproduction techniques
Intervention: sperm selection under ultra-high magnification (IMSI)
Comparison: sperm selection under regular magnification (ICSI)
Outcomes Illustrative comparative risks* (95% CI) Relative effect
(95% CI)
No of Participants
(studies)
Quality of the evidence
(GRADE)
Assumed risk Corresponding risk
ICSI IMSI NNTB
Live birth per allocated
couple
38 per 100 44 per 100
(30 to 63)
- RR 1.14 (0.79 to 1.64) 168
(1 study)
⊕⊕©©
low1
Clinical pregnancy per
allocated couple
33 per 100 43 per 100
(36 to 52)
10
(5 to 33)
RR 1.29 (1.06 to 1.55) 2014
(9 studies)
⊕©©©
very low2
Miscarriage per clinical
pregnancy
22 per 100 18 per 100
(13 to 25)
- RR 0.82 (0.59 to 1.14) 552
(6 studies)
⊕©©©
very low3
Congenital abnormali-
ties per clinical preg-
nancy
No evidence.
The median control group risk across studies was used as the basis for the assumed risk. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the
comparison group and the relative effect of the intervention (and its 95% CI).
CI: confidence interval; ICSI: intracytoplasmic sperm injection; IMSI: intracytoplasmic morphologically selected sperm injection; NNTB: number needed to treat for an additional beneficial
outcome; RR: risk ratio.
GRADE Working Group grades of evidence
High quality: Further research is very unlikely to change our confidence in the estimate of effect.
Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
Very low quality: We are very uncertain about the estimate.3R
egu
lar
(ICS
I)versu
su
ltra-h
igh
magn
ificatio
n(IM
SI)
sperm
sele
ctio
nfo
rassiste
dre
pro
du
ctio
n(R
evie
w)
Co
pyrig
ht
©2013
Th
eC
och
ran
eC
olla
bo
ratio
n.P
ub
lished
by
Joh
nW
iley
&S
on
s,L
td.
1. The quality of the evidence was downgraded two levels due to very serious imprecision.
2. The quality of the evidence was downgraded one level due to the high risk of bias in the included studies; another level due to
inconsistency across studies; and one further level because publication bias was strongly suspected.
3. The quality of the evidence was downgraded two levels due to very serious imprecision; and another level due to the high risk of bias
in the included studies.
xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx
4R
egu
lar
(ICS
I)versu
su
ltra-h
igh
magn
ificatio
n(IM
SI)
sperm
sele
ctio
nfo
rassiste
dre
pro
du
ctio
n(R
evie
w)
Co
pyrig
ht
©2013
Th
eC
och
ran
eC
olla
bo
ratio
n.P
ub
lished
by
Joh
nW
iley
&S
on
s,L
td.

B A C K G R O U N D
Description of the condition
Subfertility is a condition found in up to 15% of couples of re-
productive age and until the late 1970s, there were few options
for treating these couples. Since the first successful in vitro fer-
tilisation (IVF) was described, the efficacy of subfertility treat-
ment has greatly improved. However, it was soon realised that the
technique had great limitations in achieving pregnancy in couples
with compromised semen parameters. During the 1980s, some
other assisted reproductive technology techniques (ART) were de-
veloped focusing on gamete micromanipulation. However, for all
these techniques, spermatozoa had to be progressively motile and
needed to have the potential for an acrosome reaction, leaving in-
fertility due to severe male factors inadequately treated. Then, in
1992, the first successful intracytoplasmic sperm injection (ICSI)
was reported (Palermo 1992). For ICSI, after sperm preparation
an optical magnification of 200x to 400x is used to examine the
sample. The best ’normal looking’ motile spermatozoa are selected
based on their major morphology and then injected into oocytes
retrieved after ovarian stimulation. With ICSI, even men with se-
vere male factor infertility could possibly achieve pregnancy. How-
ever, despite 20 years of technological improvements, both clini-
cal pregnancy and live birth rates remain relatively low at approx-
imately 35% and 25% per started cycle, respectively (Jungheim
2010).
Description of the intervention
In the early 2000s, a new method of sperm selection named ’motile
sperm organelle morphology examination’ (MSOME) was de-
scribed (Bartoov 2002). This technique requires the analysis of
minor morphological criteria using ultra-high magnification (≥
6000x) microscopy. The ART using MSOME to select the sperm
was named intracytoplasmic morphologically selected sperm in-
jection (IMSI) (Bartoov 2003). When using this technique, the
motile sperm fraction is examined based on six subcellular or-
ganelles: acrosome, postacrosomal lamina, neck, mitochondria,
tail, and nucleus.
How the intervention might work
By using MSOME, some organelle malformations that are not
detectable using magnifications of 200x to 400x can be detected.
Sperm selection based on these small details is thought to improve
reproductive outcomes (Berkovitz 2006).
Why it is important to do this review
Initial reports have shown that IMSI is associated with higher
pregnancy rates in couples with repeated implantation failures (
Bartoov 2002; Bartoov 2003). However, both the effectiveness
and safety of IMSI in clinical practice remain unclear. Since there
are no large published studies, a systematic review of the best
available evidence is needed to facilitate a more robust conclusion.
Although a systematic review and meta-analysis on this issue has
been published (Setti 2010), the authors of that review evaluated a
single database (MEDLINE) and supplemented the evidence from
a single randomised controlled trial (RCT) with non-randomised
studies to improve precision, which is poorly justifiable, as this
decision increases the risk of obtaining a biased estimate (Higgins
2011). The present review aims to perform a wider and updated
search, considering only the evidence from RCTs .
O B J E C T I V E S
To compare the effectiveness and safety of IMSI and ICSI in cou-
ples undergoing ART.
M E T H O D S
Criteria for considering studies for this review
Types of studies
We considered only RCTs for inclusion; we excluded quasi- or
pseudo-randomised trials. We included studies that allowed the
inclusion of the same participant more than once (cross-over or
’per cycle’ trials) only if we could obtain the data regarding the
first inclusion of each participant.
Types of participants
Couples undergoing ART.
Types of interventions
Intracytoplasmic injection of sperm selected under high magnifi-
cation (≥ 6000x = IMSI) compared to intracytoplasmic injection
of sperm selected under regular magnification (200x to 400x =
ICSI).
Types of outcome measures
Primary outcomes
Effectiveness: live birth per allocated couple.
5Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Secondary outcomes
Effectiveness: clinical pregnancy per allocated couple.
Adverse events: miscarriage per clinical pregnancy; congenital ab-
normalities per live birth.
Although fertilisation and implantation rates were important out-
comes for this review, we did not include them in the quantita-
tive meta-analysis due to use of differing denominators (injected
oocytes for fertilisation rate and transferred embryos for implan-
tation rate). However, we included implantation and fertilisation
rates in the review for completeness, and describe them in the
Characteristics of included studies table.
Search methods for identification of studies
We developed the search strategy in consultation with the Men-
strual Disorders and Subfertility Group (MDSG) Trials Search
Co-ordinator. We did not limit searches by language or publica-
tion status.
Electronic searches
We performed the electronic searches on 31 August 2012 and
updated them on 8 May 2013.
We searched for RCTs in the following electronic databases:
• MDSG Specialised Register (Appendix 1; inception to 8
May 2013);
• Cochrane Central Register of Controlled Trials
(CENTRAL) (Appendix 2; 2013, Issue 2);
• MEDLINE (Appendix 3; 1946 to 8 May 2013), this search
was combined with the Cochrane highly sensitive search strategy
for identifying randomised trials (Higgins 2011);
• EMBASE (Appendix 4; 1980 to 8 May 2013), this search
was combined with trial filters developed by the Scottish
Intercollegiate Guidelines Network (SIGN) (www.sign.ac.uk);
• CINAHL (www.ebscohost.com/cinahl/) (Appendix 5;
inception to 7 May 2013);
• LILACS (regional.bvsalud.org) (Appendix 6; inception to 7
May 2013);
• PsycINFO (Appendix 7; inception to 8 May 2013).
We searched for study protocols and ongoing trials in the following
trials registers (Appendix 8):
• ClinicalTrials.gov (clinicaltrials.gov);
• Current Controlled Trials (www.controlled-trials.com);
• World Health Organization (WHO) International Clinical
Trials Registry Platform search portal (apps.who.int/trialsearch/
Default.aspx).
We searched for conference abstracts in the Web of Knowledge
(http://wokinfo.com; Appendix 9).
We searched for grey literature in Open Grey (www.opengrey.eu/)
(Appendix 10).
We searched for similar reviews in the Database of Abstracts of
Reviews of Effects (DARE) (Appendix 11).
Searching other resources
We handsearched the reference lists of included articles and related
reviews.
Data collection and analysis
We conducted data collection and analyses in accordance with the
Cochrane Handbook for Systematic Reviews of Interventions (Higgins
2011).
Selection of studies
Two review authors (DMT and MAPB) independently reviewed
titles and abstracts, and checked for duplicates using the pre-es-
tablished criteria for inclusion. We resolved disagreements by con-
sulting a third review author (WPM). We retrieved the full-text
manuscripts of trials considered potentially eligible for inclusion
and two review authors (DMT and MAPB) independently evalu-
ated eligibility of these trials. We resolved disagreements by con-
sulting a third review author (WPM). We corresponded with study
investigators as required to clarify study eligibility. We placed no
limitations regarding language, publication date or publication
status.
Data extraction and management
We extracted data from eligible studies using a data extraction form
designed and pilot-tested by the review authors. Where studies
had multiple publications, we used the main trial report as the
reference and obtained additional details from secondary papers.
We contacted study authors in order to resolve any data queries, as
required. Two review authors (DMT and WPM) independently
extracted the data and any disagreements between these review
authors were resolved by consulting a third review author (CON).
Assessment of risk of bias in included studies
Two review authors (DMT and WPM) independently assessed
the risk of selection bias (random sequence generation and allo-
cation concealment); performance bias (blinding of participants
and personnel); detection bias (blinding of outcome assessors); at-
trition bias (incomplete outcome data); reporting bias (selective
outcome reporting); and other potential sources of bias (e.g. a dif-
ference in the number of embryos transferred, age of participants,
co-interventions). We resolved any disagreements by consulting a
third review author (CON). To judge the risk of bias, we used The
Cochrane Collaboration’s criteria for judging risk of bias (Higgins
2011): we classified the trials as being at ’low’, ’high’, or ’unclear’
risk of bias.
6Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Measures of treatment effect
For dichotomous data (e.g. live birth rates), we used the numbers
of events in the control and intervention groups of each study to
calculate the Mantel-Haenszel risk ratio (RR). We prefer to use
RR because odds ratio (OR) is harder to understand and apply
in practice. Misinterpretation of the OR as if it equated to the
RR will tend to overestimate the intervention effect, especially
when events are common, and there is concern that this occurs
quite frequently in published reports of individual studies and
systematic reviews (Higgins 2011). However, if we had observed a
zero cell count or prevalence less than 1%, the Peto fixed-effect OR
would have been used because this method is found to be the least
biased and most powerful, providing the best confidence interval
(CI) coverage in these situations (Higgins 2011); in additional
the OR value in such situations is very similar to RR, avoiding
misinterpretations. We calculated the 95% CI to determine the
precision of the estimates. We considered the clinical relevance of
any statistically significant findings; in these situations, we also
determined the number needed to treat for an additional beneficial
outcome (NNTB) or an additional harmful outcome (NNTH).
Unit of analysis issues
The primary analysis was per couple randomised. Exceptions were
miscarriage, where we considered the number of clinical pregnan-
cies in each group as the denominator, because miscarriage is a
harm that can only occur in pregnant women; and congenital ab-
normalities, which would be analysed per live birth (but this out-
come was not reported by any study). We did not find any studies
that permitted the participant to be included more than once, as
cross-over or ’per cycle’ trials. We counted the delivery of a mul-
tiple pregnancy (e.g. twins or triplets) as one live birth event.
Dealing with missing data
We analysed the results on an intention-to-treat (ITT) basis, as far
as possible, and we contacted most of the original investigators to
obtain missing data. We planned that where these data were unob-
tainable, clinical pregnancy (and subsequent live birth or miscar-
riage) would be assumed not to have occurred in participants with
unreported outcomes. This was not necessary, because all studies
reported the occurrence of clinical pregnancy after embryo trans-
fer for all participants.
Assessment of heterogeneity
We assessed heterogeneity using the I2 statistic and addressed sub-
stantial heterogeneity (I2 > 50%) by: checking again that the data
were correct; performing the planned subgroup analysis; excluding
studies with high risk of bias; and, if it could not be explained, we
incorporated the heterogeneity by using a random-effects model.
Assessment of reporting biases
In view of the difficulty of detecting and correcting for publica-
tion bias and other reporting biases, we aimed to minimise their
potential impact by ensuring a comprehensive search for eligible
studies and by being alert for duplication of data. Even though
only nine studies were included, a funnel plot was used to explore
the possibility of small studies effect (a tendency for estimates of
the intervention effect to be more beneficial in smaller studies) for
clinical pregnancy.
Data synthesis
We combined the data from primary studies to compare IMSI
versus ICSI. An increased risk of a particular outcome associated
with IMSI, which may be beneficial (e.g. live birth) or detrimental
(e.g. miscarriage), was displayed graphically in the meta-analysis
to the right of the centre line and a decreased risk to the left of the
centre line.
Subgroup analysis and investigation of heterogeneity
We planned to perform the following subgroup analyses if sub-
stantial heterogeneity (I2 > 50%) was observed.
• Sperm quality: studies including only couples where the
male partner had poor sperm quality, or partners with good or
unselected sperm quality.
• Sperm source: ejaculate or surgical.
• Previous unsuccessful embryo transfers: studies including
only women with repeated previous unsuccessful embryo
transfers, or any women.
However, we could only perform the first subgroup analysis as no
studies evaluated only sperm obtained from surgical procedures or
only women with repeated previous unsuccessful embryo transfers.
Sensitivity analysis
We performed sensitivity analyses to verify whether the conclu-
sions about live birth and clinical pregnancy would differ if eligi-
bility was restricted to studies without high risk of bias.
Overall quality of the body of evidence: ’Summary of
findings’ table
We generated a ’Summary of findings’ table using GRADEpro
software. This table evaluated the overall quality of the body of evi-
dence for the main review outcomes, using the following GRADE
criteria: study limitations (i.e. risk of bias), consistency of effect,
imprecision, indirectness, and publication bias. Judgements about
evidence quality (high, moderate, low, or very low) were justified,
documented and incorporated into the reporting of results for
each outcome.
7Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
R E S U L T S
Description of studies
See: Characteristics of included studies; Characteristics of excluded
studies.
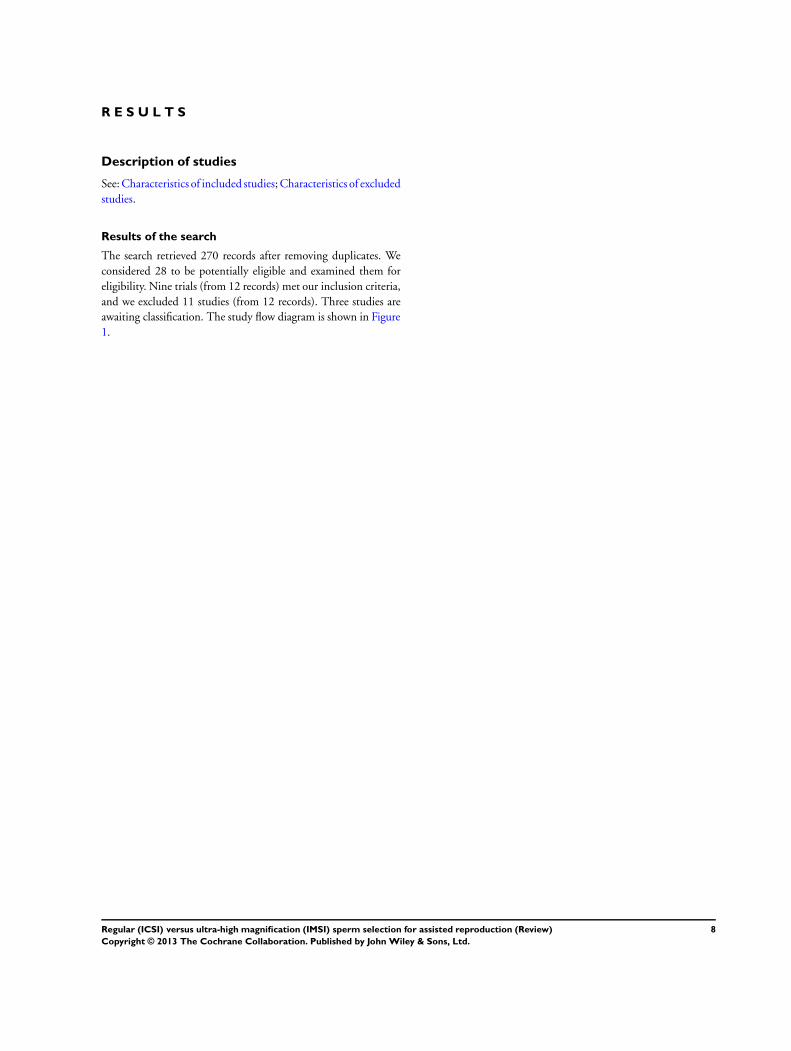
Results of the search
The search retrieved 270 records after removing duplicates. We
considered 28 to be potentially eligible and examined them for
eligibility. Nine trials (from 12 records) met our inclusion criteria,
and we excluded 11 studies (from 12 records). Three studies are
awaiting classification. The study flow diagram is shown in Figure
1.
8Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
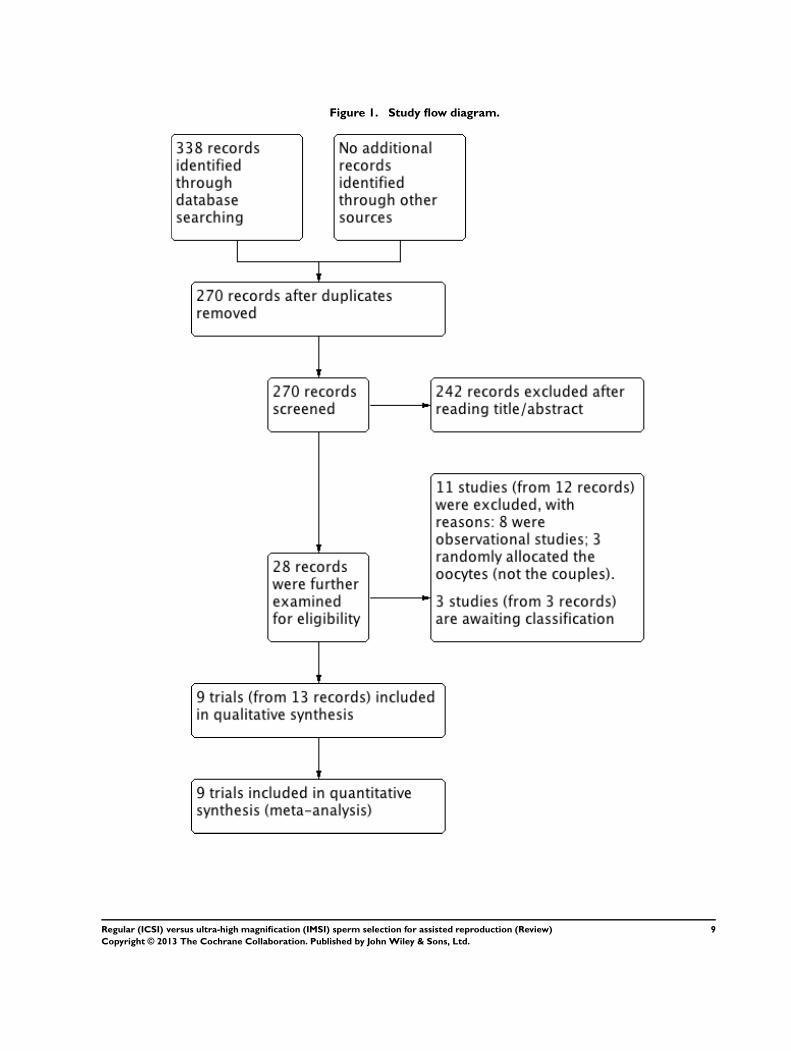
Figure 1. Study flow diagram.
9Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Included studies
Study design and setting
We included nine RCTs in the review. All were single-centre studies
conducted in academic centres from Italy (Antinori 2008), Turkey
(Balaban 2011), Brazil (Figueira 2011; Setti 2011; Setti 2012a;
Setti 2012b), Slovenia (Knez 2011; Knez 2012), and Tunisia (
Mahmoud 2011).
Participants
The studies included 1002 women in the intervention groups
(IMSI) and 1012 women in the control groups (ICSI). Five studies
included only couples in which the male partner had poor sperm
quality (Antinori 2008; Knez 2011; Knez 2012; Mahmoud 2011;
Setti 2011); three included women with advanced maternal age
(Figueira 2011; Setti 2012a; Setti 2012b); and one study included
couples who underwent ART without specifying further details
(Balaban 2011). One of the nine trials excluded couples with fe-
male factor infertility (Antinori 2008), and three excluded women
with polycystic ovaries syndrome (PCOS) or endometriosis (Knez
2011; Knez 2012; Setti 2012b).
Interventions
All studies compared regular (ICSI) versus ultra-high magnifica-
tion (IMSI).
Outcomes
• One study reported live birth.
• Nine studies reported clinical pregnancy.
• Six studies reported miscarriage.
• No studies reported congenital abnormalities.
Excluded studies
We excluded 11 studies from the review, for the following reasons:
• eight were not RCTs (observational studies);
• three randomly allocated the oocytes, not the couples.
Risk of bias in included studies
See table Characteristics of included studies; Figure 2; and Figure
3 for detailed information.
Figure 2. Risk of bias graph: review authors’ judgements about each risk of bias item presented as
percentages across all included studies.
10Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
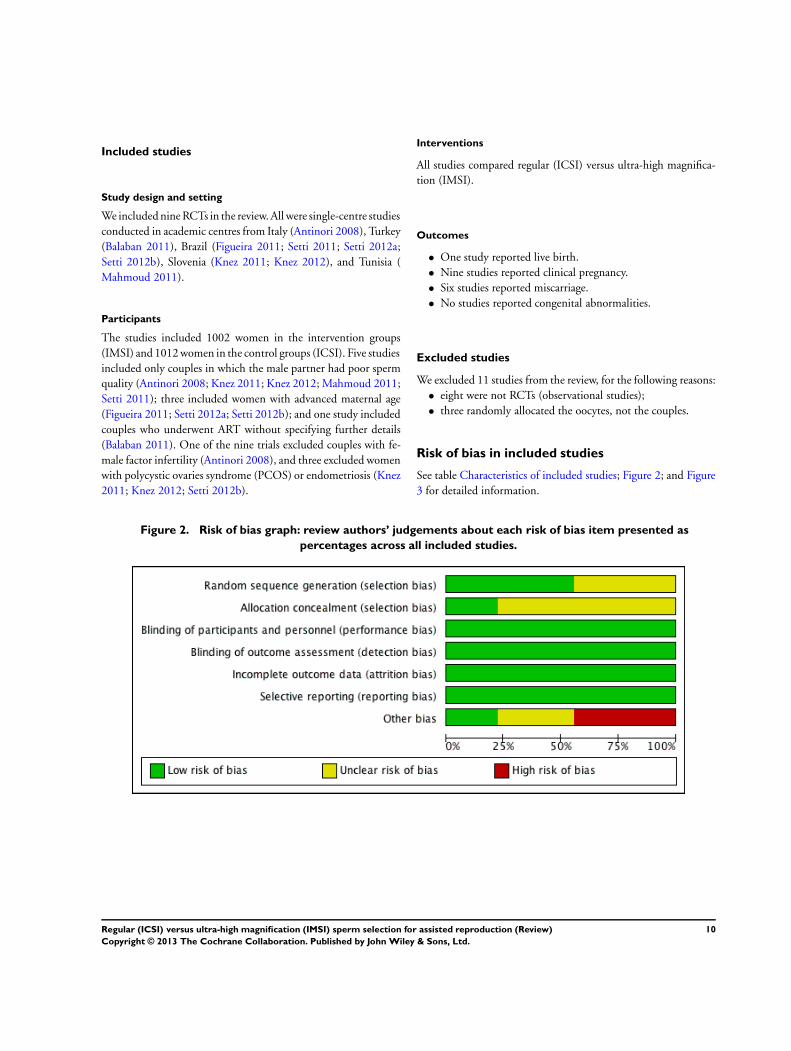
Figure 3. Risk of bias summary: review authors’ judgements about each risk of bias item for each included
study.
11Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Allocation
Five of the nine studies were at low risk of selection bias related
to sequence generation, as they used computer randomisation or
a random numbers table. The other four studies did not describe
the method used and were at unclear risk of this bias. Two studies
were at low risk of selection bias related to allocation concealment,
as they used sealed opaque envelopes prepared by research nurses
(Antinori 2008; Knez 2011). The other seven studies did not
describe the method for allocation concealment and we classified
them to be at unclear risk of bias.
Blinding
We did not consider that blinding of participants, personnel, and
outcome assessors was likely to influence findings for any of the
outcomes evaluated by this review (live birth, pregnancy rates,
miscarriage and congenital malformations). We judged all studies
to be at low risk of bias in this domain.
Incomplete outcome data
We considered all nine studies to be at low risk of bias in this
domain, as they stated that all allocated women were analysed.
Selective reporting
We considered all nine studies to be at low risk of selective report-
ing bias, because clinical pregnancy was reported by all included
studies. Although eight studies did not report live birth and nine
studies did not report congenital malformations, we believe these
studies might not be designed to evaluate these outcomes, as they
take longer to be assessed.
Other potential sources of bias
We deemed four studies to be at high risk of other bias, because
there were substantial differences regarding the mean number of
oocytes retrieved or embryos transferred between groups, or both
(Figueira 2011; Setti 2011; Setti 2012a; Setti 2012b). We con-
sidered three studies to be at unclear risk of bias, because there
was insufficient information to compare the number of oocytes
retrieved or embryos transferred, or both, per participant (Knez
2011; Knez 2012; Mahmoud 2011). We judged two studies to
be at low risk of other potential sources of bias (Antinori 2008;
Balaban 2011).
Effects of interventions
See: Summary of findings for the main comparison
1. Ultra-high magnification (IMSI) versus regular
(ICSI) sperm selection for assisted reproduction
Primary outcomes
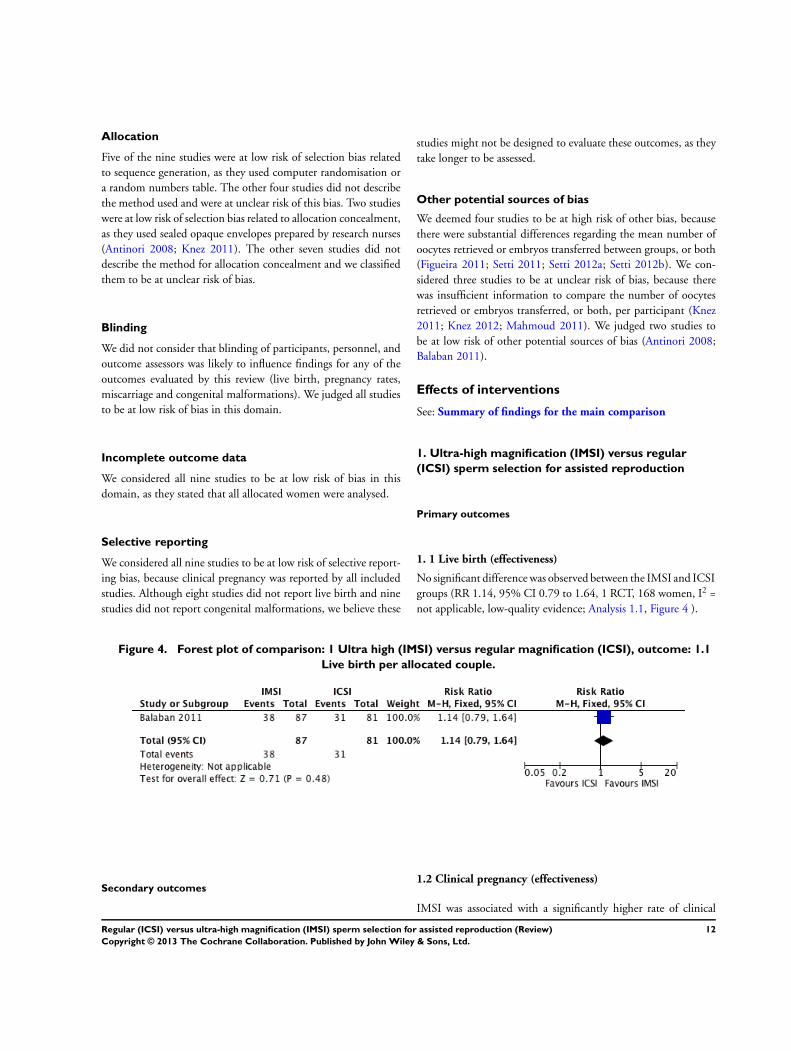
1. 1 Live birth (effectiveness)
No significant difference was observed between the IMSI and ICSI
groups (RR 1.14, 95% CI 0.79 to 1.64, 1 RCT, 168 women, I2 =
not applicable, low-quality evidence; Analysis 1.1, Figure 4 ).
Figure 4. Forest plot of comparison: 1 Ultra high (IMSI) versus regular magnification (ICSI), outcome: 1.1
Live birth per allocated couple.
Secondary outcomes1.2 Clinical pregnancy (effectiveness)
IMSI was associated with a significantly higher rate of clinical
12Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
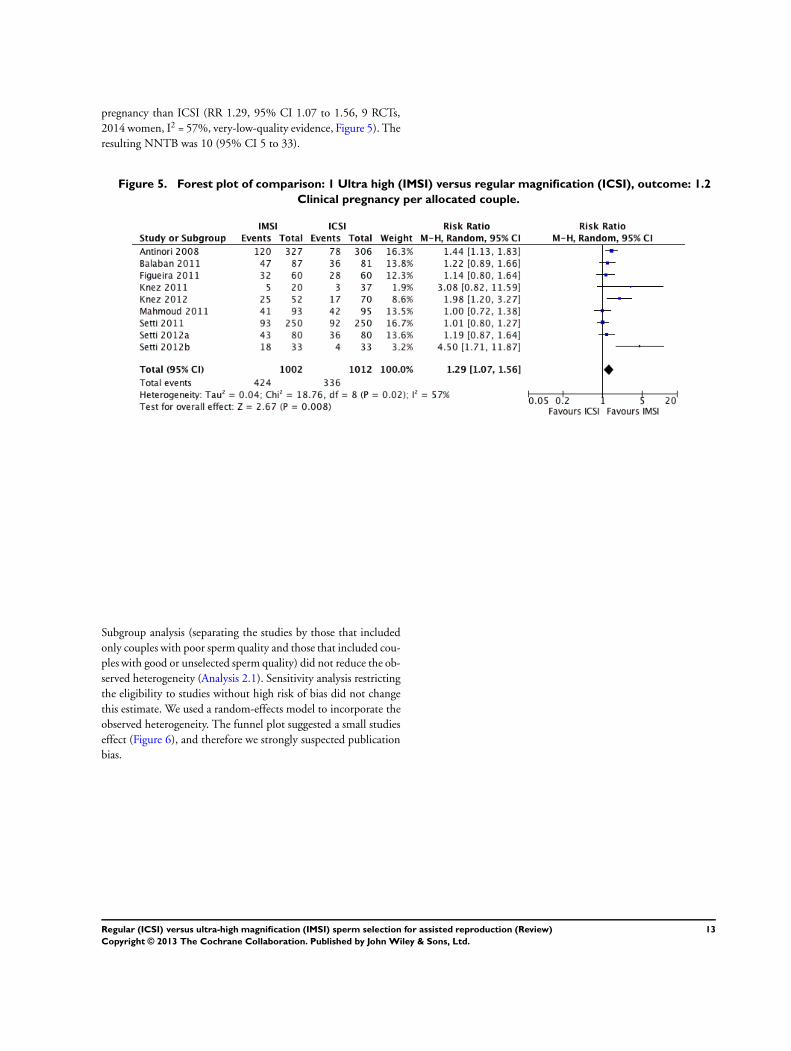
pregnancy than ICSI (RR 1.29, 95% CI 1.07 to 1.56, 9 RCTs,
2014 women, I2 = 57%, very-low-quality evidence, Figure 5). The
resulting NNTB was 10 (95% CI 5 to 33).
Figure 5. Forest plot of comparison: 1 Ultra high (IMSI) versus regular magnification (ICSI), outcome: 1.2
Clinical pregnancy per allocated couple.
Subgroup analysis (separating the studies by those that included
only couples with poor sperm quality and those that included cou-
ples with good or unselected sperm quality) did not reduce the ob-
served heterogeneity (Analysis 2.1). Sensitivity analysis restricting
the eligibility to studies without high risk of bias did not change
this estimate. We used a random-effects model to incorporate the
observed heterogeneity. The funnel plot suggested a small studies
effect (Figure 6), and therefore we strongly suspected publication
bias.
13Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
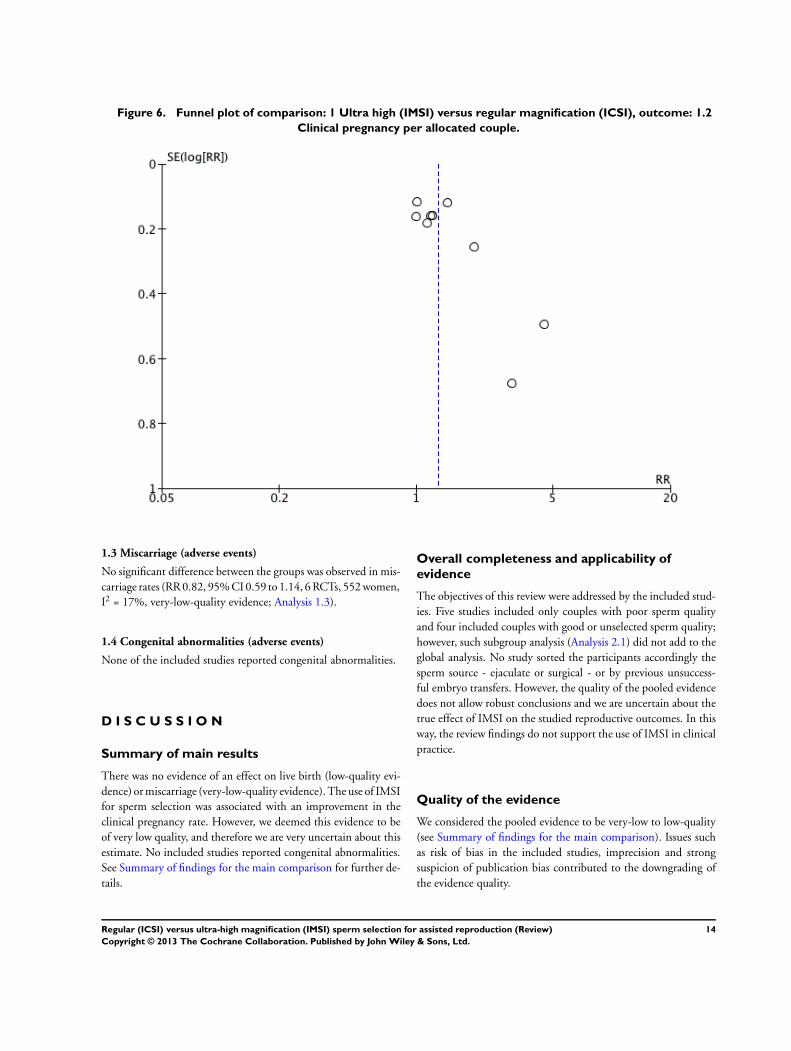
Figure 6. Funnel plot of comparison: 1 Ultra high (IMSI) versus regular magnification (ICSI), outcome: 1.2
Clinical pregnancy per allocated couple.
1.3 Miscarriage (adverse events)
No significant difference between the groups was observed in mis-
carriage rates (RR 0.82, 95% CI 0.59 to 1.14, 6 RCTs, 552 women,
I2 = 17%, very-low-quality evidence; Analysis 1.3).
1.4 Congenital abnormalities (adverse events)
None of the included studies reported congenital abnormalities.
D I S C U S S I O N
Summary of main results
There was no evidence of an effect on live birth (low-quality evi-
dence) or miscarriage (very-low-quality evidence). The use of IMSI
for sperm selection was associated with an improvement in the
clinical pregnancy rate. However, we deemed this evidence to be
of very low quality, and therefore we are very uncertain about this
estimate. No included studies reported congenital abnormalities.
See Summary of findings for the main comparison for further de-
tails.
Overall completeness and applicability ofevidence
The objectives of this review were addressed by the included stud-
ies. Five studies included only couples with poor sperm quality
and four included couples with good or unselected sperm quality;
however, such subgroup analysis (Analysis 2.1) did not add to the
global analysis. No study sorted the participants accordingly the
sperm source - ejaculate or surgical - or by previous unsuccess-
ful embryo transfers. However, the quality of the pooled evidence
does not allow robust conclusions and we are uncertain about the
true effect of IMSI on the studied reproductive outcomes. In this
way, the review findings do not support the use of IMSI in clinical
practice.
Quality of the evidence
We considered the pooled evidence to be very-low to low-quality
(see Summary of findings for the main comparison). Issues such
as risk of bias in the included studies, imprecision and strong
suspicion of publication bias contributed to the downgrading of
the evidence quality.
14Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
The evidence of effect on live birth was deemed low-quality be-
cause only one study reported this outcome, with very serious
imprecision in the estimate (Balaban 2011). There were only 69
events, and the 95% CI included appreciable harm, no effect, and
appreciable benefit.
We considered the evidence of effect on clinical pregnancy to be
of very-low-quality. We considered four out of the nine included
studies to be at high risk of potential bias, regarding differences
in the mean number of oocytes retrieved or embryos transferred
between groups, or both (see Assessment of risk of bias in included
studies; Figure 3). In addition, there was inconsistency across the
included studies; and publication bias was strongly suspected, as
funnel plot analysis (Figure 6) suggested a small studies effect.
Regarding miscarriage, we considered the evidence to be of very-
low-quality. This occurred because the four out of six studies that
reported this outcome were considered to be at high risk of bias
related to differences in the mean number of oocytes retrieved or
embryos transferred between groups, and there was also very seri-
ous imprecision in the estimate. There were only 107 miscarriages
across both groups, and the 95% CI was compatible with both
appreciable harm and no effect.
There was no evidence from RCTs on the effect of IMSI on con-
genital abnormalities.
Potential biases in the review process
We did not identify potential biases in the review process.
Agreements and disagreements with otherstudies or reviews
Another review evaluated the effect of IMSI (Setti 2010). It in-
cluded studies recovered from a single database (MEDLINE) and
supplemented evidence from a single RCT with non-RCT stud-
ies. In accordance to our review, they reported a significant im-
provement in clinical pregnancy rates. However, they observed a
beneficial effect of IMSI decreasing the risk of miscarriage while
we observed no evidence of such effect.
A U T H O R S ’ C O N C L U S I O N S
Implications for practice
The current evidence from randomised controlled trials does not
support the clinical use of intracytoplasmic sperm injection (in-
tracytoplasmic morphologically selected sperm injection (IMSI)):
there is no evidence of effect on live birth or miscarriage and the
evidence that IMSI improves clinical pregnancy is of very low qual-
ity. There is no evidence regarding the effect of this intervention
on the risk of congenital abnormalities. Further trials are neces-
sary to improve the quality of the evidence before recommending
IMSI in clinical practice.
Implications for research
More studies are needed to evaluate the effect of IMSI on live birth,
clinical pregnancy, miscarriage, and congenital abnormalities.
A C K N O W L E D G E M E N T S
We acknowledge the important help provided by Helen Nagels,
Managing Editor from the Cochrane Menstrual Disorders and
Subfertility Group, and by Marian Showell, Trials Search Co-or-
dinator for the Cochrane Menstrual Disorders and Subfertility
Group.
R E F E R E N C E S
References to studies included in this review
Antinori 2008 {published data only}
Antinori M, Licata E, Dani G, Cerusico F, Versaci C,
d’Angelo D, et al.Intracytoplasmic morphologically
selected sperm injection: a prospective randomized trial.
Reproductive BioMedicine Online 2008;16(6):835–41.
[PUBMED: 18549694]∗ Antinori S, Licata E, Dani G, Cerusico F, Versaci C,
Antinori M. A prospective randomized trial to verify the
efficacy of IMSI procedure in daily IVF routine. Human
Reproduction 2008;23 Suppl 1:i165.
Balaban 2011 {published data only}
Balaban B, Yakin K, Alatas C, Oktem O, Isiklar
A, Urman B. Clinical outcome of intracytoplasmic
injection of spermatozoa morphologically selected under
high magnification: a prospective randomized study.
Reproductive Biomedicine Online 2011;22(5):472–6.
[PUBMED: 21324747]
Figueira 2011 {published data only}
Figueira RCS, Braga DPAF, Pasqualotto EB, Pasqualotto
FF, Iaconelli A, Borges E. The role of morphological
nuclear integrity of the sperm cells in preimplantation
genetic aneuploidy screening cycles outcome. Journal fur
Reproduktionsmedizin und Endokrinologie 2010;7:250–1.∗ Figueira RDC, Braga DP, Setti AS, Iaconelli A Jr,
Borges E Jr. Morphological nuclear integrity of sperm
cells is associated with preimplantation genetic aneuploidy
screening cycle outcomes. Fertility and Sterility 2011;95(3):
15Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
990–3. [PUBMED: 21130987]
Knez 2011 {published data only}
Knez K, Zorn B, Tomazevic T, Vrtacnik-Bokal E, Virant-
Klun I. The IMSI procedure improves poor embryo
development in the same infertile couples with poor
semen quality: a comparative prospective randomized
study. Reproductive Biology and Endocrinology 2011;9:123.
[PUBMED: 21875440]
Knez 2012 {published data only}
Knez K, Tomazevic T, Zorn B, Vrtacnik-Bokal E,
Virant-Klun I. Intracytoplasmic morphologically selected
sperm injection improves development and quality of
preimplantation embryos in teratozoospermia patients.
Reproductive Biomedicine Online 2012;25(2):168–79.
[PUBMED: 22717245]
Mahmoud 2011 {published data only}
Mahmoud K, Triki-Hmam C, Terras K, Zhioua F, Hfaiedh
T, Ben Aribia MH. How and in which indication the IMSI
could improve outcomes?. Human Reproduction 2011;26
Suppl 1:i181.
Setti 2011 {published data only}
Setti AS, Figueira Rde C, Braga DP, Iaconelli A Jr, Borges
E Jr. Intracytoplasmic morphologically selected sperm
injection benefits for patients with oligoasthenozoospermia
according to the 2010 World Health Organization
reference values. Fertility and Sterility 2011;95(8):2711–4.
[PUBMED: 21458802]
Setti 2012a {published data only}
Iaconelli JA, Figueira RCS, Setti AS, Braga DPAF,
Pasqualotto EE, Borges E Jr. Gender incidence on
intracytoplasmic morphologically selected sperm injection
approach: a prospective randomized study. Human
Reproduction 2011;26 Suppl 1:i71.∗ Setti AS, Figueira RC, Braga DP, Iaconelli A Jr, Borges E
Jr. Gender incidence of intracytoplasmic morphologically
selected sperm injection-derived embryos: a prospective
randomized study. Reproductive BioMedicine Online 2012;
24(4):420–3. [PUBMED: 22377154]
Setti 2012b {published data only}
Setti AS, Figueira, RDC, de Almeida Ferreira Braga DP,
Iaconelli A, Borges E. IMSI is beneficial in cases of advanced
maternal age: a prospective randomized study. Reproductive
BioMedicine Online 2012;Withdrawn. [DOI: 10.1016/
j.rbmo.2012.10.020]
References to studies excluded from this review
Apryshko 2010 {published data only}
Apryshko VP, Yakovenko SA, Sivozhelezov VS, Yutkin EV,
Rutman BK, Troshina MN, et al.IMSI based on Hoffman
modulation contrast: 5 years experience. Reproductive
BioMedicine Online 2010;20:S25.
Bartoov 2003 {published data only}
Bartoov B, Berkovitz A, Eltes F, Kogosovsky A, Yagoda
A, Lederman H, et al.Pregnancy rates are higher with
intracytoplasmic morphologically selected sperm injection
than with conventional intracytoplasmic injection. Fertility
and Sterility 2003;80(6):1413–9. [PUBMED: 14667877]
Berkovitz 2005 {published data only}
Berkovitz A, Eltes F, Yaari S, Katz N, Barr I, Fishman A,
et al.The morphological normalcy of the sperm nucleus
and pregnancy rate of intracytoplasmic injection with
morphologically selected sperm. Human Reproduction
2005;20(1):185–90. [PUBMED: 15471930]
Berkovitz 2006 {published data only}
Berkovitz A, Eltes F, Lederman H, Peer S, Ellenbogen A,
Feldberg B, et al.How to improve IVF-ICSI outcome by
sperm selection. Reproductive Biomedicine Online 2006;12
(5):634–8. [PUBMED: 16790113]
Braga 2011 {published data only}
Braga DPAF, Setti AS, Figueira RC, Nichi M, Martinhago
CD, Iaconelli A Jr, et al.Sperm organelle morphologic
abnormalities: contributing factors and effects on
intracytoplasmic sperm injection cycles outcomes. Urology
2011;78(4):786–91. [PUBMED: 21820702]
Cassuto 2011 {published data only}
Cassuto NG, Hazout A, Benifla JL, Balet R, Larue L,
Viot G. Decreasing birth defect in children by using high
magnification selected spermatozoon injection. Fertility and
Sterility 2011;1:S85.
De Vos 2013 {published data only}
De Vos A, Van de Velde H, Bocken G, Eylenbosch G,
Franceus N, Meersdom G, et al.Does intracytoplasmic
morphologically selected sperm injection improve embryo
development? A randomized sibling-oocyte study. Human
Reproduction 2013;28:617–26.
Hazout 2005 {published data only}
Hazout A, Dumont-Hassan M, Junca AM, Cohen
Bacrie P, Tesarik J. High-magnification ICSI overcomes
paternal effect resistant to conventional ICSI. Reproductive
Biomedicine Online 2005;12(1):19–24. [PUBMED:
16454928]
Mauri 2011 {published data only}
Mauri AL, Petersen CG, Oliveira JB, Massaro FC, Baruffi
RL, Franco JG Jr. Comparison of day 2 embryo quality after
conventional ICSI versus intracytoplasmic morphologically
selected sperm injection (IMSI) using sibling oocytes.
European Journal of Obstetrics, Gynecology, and Reproductive
Biology 2011;150(1):42–6. [PUBMED: 20171776]
Oliveira 2011 {published data only}∗ Oliveira JBA, Cavagna M, Petersen CG, Mauri
AL, Massaro FC, Silva LFI, et al.Pregnancy outcomes
in women with repeated implantation failures after
intracytoplasmic morphologically selected sperm injection
(IMSI). Reproductive Biology and Endocrinology 2011;9:99.
[PUBMED: 21781299]
Oliveira JBA, Petersen CG, Mauri AL, Massaro FC, Baruffi
RLR, Franco JG Jr. Clinical outcomes of IMSI in previous
ICSI failures. Fertility and Sterility 2010;1:S55.
16Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Wilding 2011 {published data only}
Wilding M, Coppola G, di Matteo L, Palagiano A, Fusco
E, Dale B. Intracytoplasmic injection of morphologically
selected spermatozoa (IMSI) improves outcome after
assisted reproduction by deselecting physiologically poor
quality spermatozoa. Journal of Assisted Reproduction and
Genetics 2011;28(3):253–62. [PUBMED: 21072684]
References to studies awaiting assessment
Check 2013 {published data only}
Check JH, Bollendorf A, Summers-Chase D, Yuan W,
Horwath D. Isolating sperm by selecting those with normal
nuclear morphology prior to intracytoplasmic sperm
injection (ICSI) does not provide better pregnancy rates
compared to conventional ICSI in women with repeated
conception failure with in vitro fertilization. Clinical and
Experimental Obstetrics & Gynecology 2013;40:15–7.
Parinaud 2013 {unpublished data only}
Setti 2012c {published data only}
Setti AS, Braga DPAF, Figueira RCS, Colturato SS,
Iaconelli A, Borges E. Intracytoplasmic morphologically
selected sperm injection (IMSI) benefits in the presence of
unexplained infertility: a prospective randomized study.
Fertility and Sterility 2012; Vol. 98 Suppl 1, issue 3:S80.
Additional references
Bartoov 2002
Bartoov B, Berkovitz A, Eltes F, Kogosowski A, Menezo
Y, Barak Y. Real-time fine morphology of motile human
sperm cells is associated with IVF-ICSI outcome. Journal of
Andrology 2002;23(1):1–8. [PUBMED: 11780915]
Higgins 2011
Higgins JPT, Green S (editors). Cochrane Handbook
for Systematic Reviews of Interventions Version 5.1.0
[updated March 2011]. The Cochrane Collaboration,
2011. Available from www.cochrane-handbook.org.
Jungheim 2010
Jungheim ES, Ryan GL, Levens ED, Cunningham AF,
Macones GA, Carson KR, et al.Embryo transfer practices
in the United States: a survey of clinics registered with the
Society for Assisted Reproductive Technology. Fertility and
Sterility 2010;94(4):1432–6. [PUBMED: 19748089]
Palermo 1992
Palermo G, Joris H, Devroey P, Van Steirteghem AC.
Pregnancies after intracytoplasmic injection of single
spermatozoon into an oocyte. Lancet 1992;340(8810):
17–8. [PUBMED: 1351601]
Setti 2010
Setti AS, Ferreira RC, Braga DPAF, Figueira RCS, Iaconelli
A Jr, Borges E Jr. Intracytoplasmic sperm injection
outcome versus intracytoplasmic morphologically selected
sperm injection outcome: a meta-analysis. Reproductive
Biomedicine Online 2010;21(4):450–5. [PUBMED:
20800549]∗ Indicates the major publication for the study
17Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Antinori 2008
Methods Randomised controlled trial conducted in a private assisted reproduction centre (Italy).
Period of enrolment not reported
Participants Inclusion criteria: at least 2 previous diagnoses of severe oligoasthenospermia; 3 years
of primary infertility; absence of female factor
Interventions Couples were randomised into 2 groups:
Intervention: oocytes injected with spermatozoon selected under ultra-high magnifica-
tion (IMSI): on the basis of MSOME criteria, the examination and spermatozoa selec-
tion for IMSI procedure was performed in real time using an inverted light microscope
equipped with high-power Nomarski optics, enhanced by digital imaging to achieve
a magnification up to 6300x, and the Eppendorf Micromanipulation System (Trans-
fer-Man NK2, Eppendorf, Germany). Only spermatozoa with normal head dimension
(length 4.75 ± 0.28 µm; width 3.28 ± 0.20 µm) and shape, with no or maximum 1 vac-
uole (0.78 ± 0.18 µm) were microinjected; spermatozoa with abnormal head size were
excluded (such spermatozoa were identified by superimposing a transparent celluloid
form representing the correct spermatozoon size on the examined gametes). 2 sperma-
tozoa for each oocyte were selected to be inseminated using the classical ICSI technique
Control: oocytes injected with spermatozoon selected under regular magnification
(ICSI): no further details
Outcomes Clinical pregnancy, miscarriage, and implantation rates.
Notes We considered 2 publications to be related to the same study although the numbers of
participants were not the same, because the only difference we observed was that the
newer publication had evaluated more participants; the authors did not answer our e-
mails to resolve these data queries
Live birth and congenital abnormalities not reported.
Implantation rate: 23.0% (IMSI) vs. 16.6% (ICSI); P value not reported.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Not reported.
Allocation concealment (selection bias) Low risk Sealed, opaque envelopes prepared by a re-
search nurse.
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk Blinding of participants and personnel was
not considered as a potential source of bias
18Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Antinori 2008 (Continued)
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk Blinding of outcome assessment was not
considered as a potential source of bias
Incomplete outcome data (attrition bias)
All outcomes
Low risk No loss to follow-up.
Selective reporting (reporting bias) Low risk Not suspected.
Other bias Low risk None.
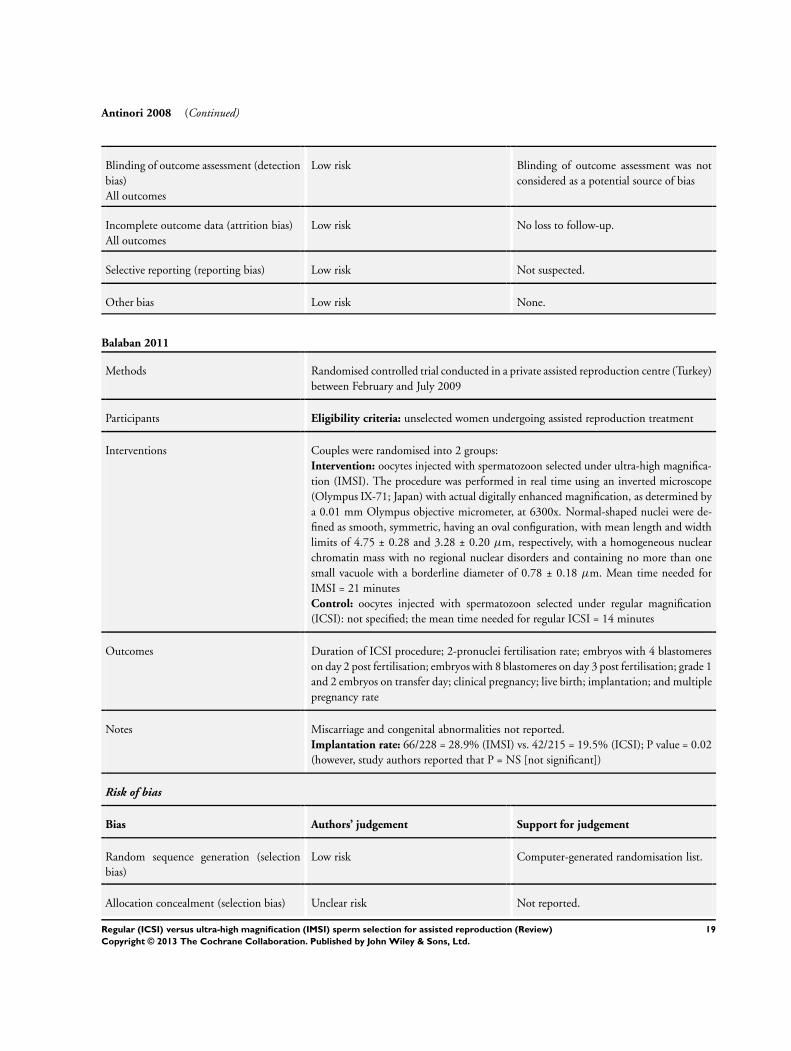
Balaban 2011
Methods Randomised controlled trial conducted in a private assisted reproduction centre (Turkey)
between February and July 2009
Participants Eligibility criteria: unselected women undergoing assisted reproduction treatment
Interventions Couples were randomised into 2 groups:
Intervention: oocytes injected with spermatozoon selected under ultra-high magnifica-
tion (IMSI). The procedure was performed in real time using an inverted microscope
(Olympus IX-71; Japan) with actual digitally enhanced magnification, as determined by
a 0.01 mm Olympus objective micrometer, at 6300x. Normal-shaped nuclei were de-
fined as smooth, symmetric, having an oval configuration, with mean length and width
limits of 4.75 ± 0.28 and 3.28 ± 0.20 µm, respectively, with a homogeneous nuclear
chromatin mass with no regional nuclear disorders and containing no more than one
small vacuole with a borderline diameter of 0.78 ± 0.18 µm. Mean time needed for
IMSI = 21 minutes
Control: oocytes injected with spermatozoon selected under regular magnification
(ICSI): not specified; the mean time needed for regular ICSI = 14 minutes
Outcomes Duration of ICSI procedure; 2-pronuclei fertilisation rate; embryos with 4 blastomeres
on day 2 post fertilisation; embryos with 8 blastomeres on day 3 post fertilisation; grade 1
and 2 embryos on transfer day; clinical pregnancy; live birth; implantation; and multiple
pregnancy rate
Notes Miscarriage and congenital abnormalities not reported.
Implantation rate: 66/228 = 28.9% (IMSI) vs. 42/215 = 19.5% (ICSI); P value = 0.02
(however, study authors reported that P = NS [not significant])
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk Computer-generated randomisation list.
Allocation concealment (selection bias) Unclear risk Not reported.
19Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Balaban 2011 (Continued)
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk Blinding of participants and personnel was
not considered as a potential source of bias
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk Blinding of outcome assessment was not
considered as a potential source of bias
Incomplete outcome data (attrition bias)
All outcomes
Low risk No loss to follow-up.
Selective reporting (reporting bias) Low risk Not suspected.
Other bias Low risk None.
Figueira 2011
Methods Randomised controlled trial conducted in a private assisted reproduction centre (Brazil)
between May and December 2009
Participants Eligibility criteria: women undergoing assisted reproduction treatment in conjunction
with pre-implantation genetic screening for aneuploidy, as a result of advanced maternal
age; sperm concentration > 1,000,000/mL and sperm motility > 20%; at least 6 oocytes
available on oocyte retrieval
Interventions Couples were randomised into 2 groups:
Intervention: oocytes injected with spermatozoon selected under ultra-high magnifi-
cation (IMSI): sperm morphology selection was assessed using an inverted Nikon Di-
aphot microscope (Eclipse TE 300; Nikon, Tokyo) equipped with high-power DIC
(Nomarski). The total calculated magnification was 6600x. The sperm cells exhibiting
normally shaped nuclei (smooth, symmetric, and oval configuration) and normal nuclear
chromatin content (if it contained no more than 1 vacuole, which occupies < 4% of the
nuclear area) were selected for injection
Control: oocytes injected with spermatozoon selected under regular magnification
(ICSI): sperm morphology selection was assessed using an inverted Nikon Diaphot mi-
croscope (Eclipse TE 300; Nikon, Tokyo) with a Hoffmann modulation contrast system
under 400x magnification
Outcomes Sperm nuclear morphology at high-magnification ICSI; incidence of aneuploidy in de-
rived embryos; clinical pregnancy rate
Notes All embryos were submitted to pre-implantation genetic diagnosis and aneuploidy screen-
ing. On the morning of day 3 of embryo development, 1 cell per embryo was biopsied
by laser zona drilling using a 1.48 mm infrared diode laser (Octax Laser Shot System,
MTG, Bruckberg, Germany). After the biopsies, the embryos were returned to the cul-
ture medium. The removed blastomere nuclei were spread using 0.1 N HCl and 0.01%
Tween 20 (Sigma, Dorset, UK). Briefly, the individual nuclei were placed on a slide in 1
drop of HCl-Tween spreading solution and observed until the cell had lysed. The slides
20Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figueira 2011 (Continued)
were then air dried and dehydrated before FISH analysis was performed. All embryos
were analysed for chromosomes X, Y, 13, 16, 18, 21, and 22. For the purpose of this
study, the blastomeres were classified as normal when 2 sexual and 2 of each tested auto-
somal chromosomes were present. Blastomeres with 2 or more chromosomal numerical
abnormalities were classified as chaotic. Embryos with abnormal findings in biopsied
nuclei were not submitted for re-analysis. Embryo transfer was performed on day 4 using
a soft catheter with transabdominal ultrasound guidance. Only the embryos found to
be chromosomally normal were considered for embryo transfer, and a maximum of 3
embryos were transferred. The cycle was cancelled if normal embryos were absent after
FISH
Live birth and congenital abnormalities not reported.
Implantation rate: 55.6% (IMSI) vs. 40.9% (ICSI); P value = 0.59.
Study authors were contacted to clarify information about the 4 different included
studies, from the same groups of authors (Figueira 2011; Setti 2011; Setti 2012a; Setti
2012b). All questions on methods of randomisation, patient overlapping, and data “per
woman” were clarified
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk Computer-generated balanced table in sets
of 10.
Allocation concealment (selection bias) Unclear risk Not reported.
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk Blinding of participants and personnel was
not considered as a potential source of bias
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk Blinding of outcome assessment was not
considered as a potential source of bias
Incomplete outcome data (attrition bias)
All outcomes
Low risk No loss to follow-up.
Selective reporting (reporting bias) Low risk Not suspected.
Other bias High risk The number of oocytes retrieved and em-
bryos transferred were significantly differ-
ent between groups (P value < 0.01). In the
article, study authors reported that differ-
ences were not significant (P value = 0.20
and P value = 0.17, oocytes retrieved and
embryos transferred, respectively)
21Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Knez 2011
Methods Randomised controlled trial conducted in an academic setting (Slovenia) between Oc-
tober 2009 and June 2010
Participants Eligibility criteria: all embryos arrested after prolonged 5-day embryo culture to the
blastocyst stage in their previous conventional ICSI attempts; poor semen quality charac-
terised by the incidence of teratozoospermia by less than 14% of morphologically normal
sperm according to the Strict Kruger Criteria, oligozoospermia by a sperm concentration
of < 20 million/mL and asthenozoospermia by < 50% of motile sperm according the
WHO criteria; women without PCOS or endometriosis and age < 42 years
Interventions Couples were randomised into 2 groups:
Intervention: oocytes injected with spermatozoon selected under ultra-high magnifica-
tion (IMSI): sperm were selected in dishes with a glass bottom (GWSt 1000; Will Co.,
Wells BV, Amsterdam, The Netherlands) and monitored under an inverted microscope
with a heated stage equipped with DIC (Nikon ECLIPSE TE2000-S, Japan). Approxi-
mately 5 elongated droplets of SpermSlow medium (Origio, Denmark) were placed on
the bottom of a glass dish to immobilise the sperm. A smaller droplet of prepared sperm
was placed near each SpermSlow droplet. Then the connections were made between
the sperm and the SpermSlow droplets for sperm to swim into the SpermSlow droplets
and to bind to the HA. All droplets were covered with paraffin oil (Origio, Denmark)
. For observation under 6000x magnification, a droplet of immersion oil was inserted
underneath the glass dish (under the SpermSlow droplet). One droplet of SpermSlow
with bound sperm was monitored by the immersion objective, DIC, and Nikon Digital
Sight DS-Ri1 camera. The single (mature) sperm that was bound to the HA and had
the best morphology was chosen, aspirated in the microinjection pipette, scored in 3-
dimensions, and evaluated according to the morphology and head vacuoles at 6000x
magnification
Control: oocytes injected with spermatozoon selected under regular magnification
(ICSI): the sperm selection for microinjection was performed at a magnification of 200x
to 400x. Sperm with severe head-shape defects clearly seen under the magnification (pin,
amorphous, tapered, round, and multinucleated head) were excluded from microinjec-
tion into the oocyte
Outcomes Fertilisation, blastocyst, implantation, and pregnancy rates
Notes Live birth and congenital abnormalities not reported.
Implantation rate: 6/35 = 17.1% (IMSI) vs. 3/44 = 6.8% (ICSI); P = 0.17.
Study author was contacted to clarify information about the 2 different included studies
(Knez 2011 and Knez 2012). All questions on methods of randomisation, patient over-
lapping, and data “per woman” were clarified
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk Computer-generated random numbers
(unrestricted randomisation list)
22Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Knez 2011 (Continued)
Allocation concealment (selection bias) Low risk Sealed, opaque envelopes prepared by a re-
search nurse.
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk Blinding of participants and personnel was
not considered as a potential source of bias
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk Blinding of outcome assessment was not
considered as a potential source of bias
Incomplete outcome data (attrition bias)
All outcomes
Low risk No loss to follow-up.
Selective reporting (reporting bias) Low risk Not suspected.
Other bias Unclear risk Study authors did not report the num-
ber of oocytes retrieved in the groups. The
number of transferred embryos per partici-
pant was not significantly different between
groups
Knez 2012
Methods Randomised controlled trial conducted in an academic setting (Slovenia) between Jan-
uary and October 2011
Participants Eligibility criteria: at least 6 mature oocytes available upon oocyte retrieval; isolated
teratozoospermia, which was determined as having < 14% of morphologically normal
spermatozoa according to the Kruger strict criteria, > 15 million spermatozoa per millilitre
and at least 40% motile spermatozoa; women without PCOS or endometriosis
Interventions Couples were randomised into 2 groups:
Intervention: oocytes injected with spermatozoon selected under ultra-high magnifica-
tion (IMSI): a single spermatozoon bound to the HA and with the best morphology was
chosen, aspirated in the microinjection pipette, scored in 3-dimensions and evaluated
according to the morphology and head vacuoles at 6000x magnification
Control: oocytes injected with spermatozoon selected under regular magnification
(ICSI): spermatozoa without severe head shape defects clearly seen under the microscope
(pin, amorphous, tapered, round, and multinucleated head) were selected at magnifica-
tion 200x to 400x
Outcomes Fertilisation, blastocyst, implantation, and pregnancy rates
Notes Live birth, miscarriage, and congenital abnormalities not reported
Implantation rate not reported.
Study author was contacted to clarify information about the 2 different included studies
(Knez 2011; Knez 2012). All questions on methods of randomisation, patient overlap-
23Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
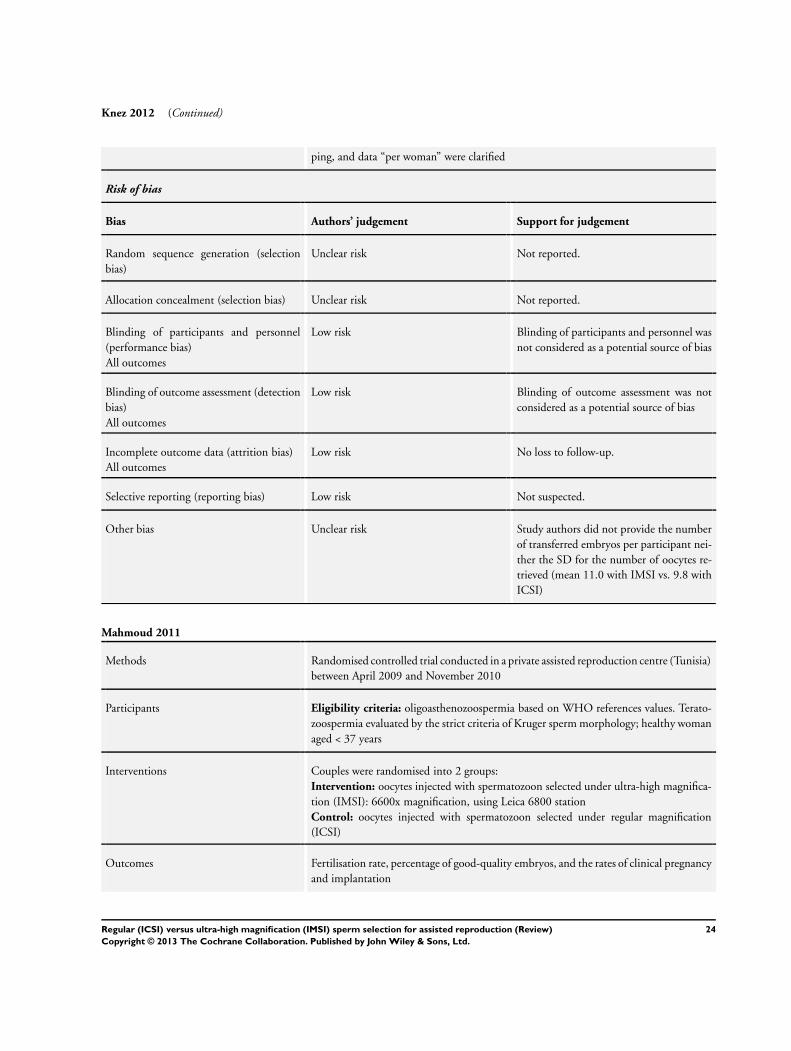
Knez 2012 (Continued)
ping, and data “per woman” were clarified
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Not reported.
Allocation concealment (selection bias) Unclear risk Not reported.
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk Blinding of participants and personnel was
not considered as a potential source of bias
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk Blinding of outcome assessment was not
considered as a potential source of bias
Incomplete outcome data (attrition bias)
All outcomes
Low risk No loss to follow-up.
Selective reporting (reporting bias) Low risk Not suspected.
Other bias Unclear risk Study authors did not provide the number
of transferred embryos per participant nei-
ther the SD for the number of oocytes re-
trieved (mean 11.0 with IMSI vs. 9.8 with
ICSI)
Mahmoud 2011
Methods Randomised controlled trial conducted in a private assisted reproduction centre (Tunisia)
between April 2009 and November 2010
Participants Eligibility criteria: oligoasthenozoospermia based on WHO references values. Terato-
zoospermia evaluated by the strict criteria of Kruger sperm morphology; healthy woman
aged < 37 years
Interventions Couples were randomised into 2 groups:
Intervention: oocytes injected with spermatozoon selected under ultra-high magnifica-
tion (IMSI): 6600x magnification, using Leica 6800 station
Control: oocytes injected with spermatozoon selected under regular magnification
(ICSI)
Outcomes Fertilisation rate, percentage of good-quality embryos, and the rates of clinical pregnancy
and implantation
24Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Mahmoud 2011 (Continued)
Notes Live birth, miscarriage, and congenital abnormalities not reported
Implantation rate: 19.2% (IMSI) vs. 17.2% (ICSI); P value = not significant.
Study authors were not contacted because we were unable to obtain their contact details
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Not reported.
Allocation concealment (selection bias) Unclear risk Not reported.
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk Blinding of participants and personnel was
not considered as a potential source of bias
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk Blinding of outcome assessment was not
considered as a potential source of bias
Incomplete outcome data (attrition bias)
All outcomes
Low risk No loss to follow-up.
Selective reporting (reporting bias) Low risk Not suspected.
Other bias Unclear risk Study authors did not report the number of
oocytes retrieved and embryos transferred
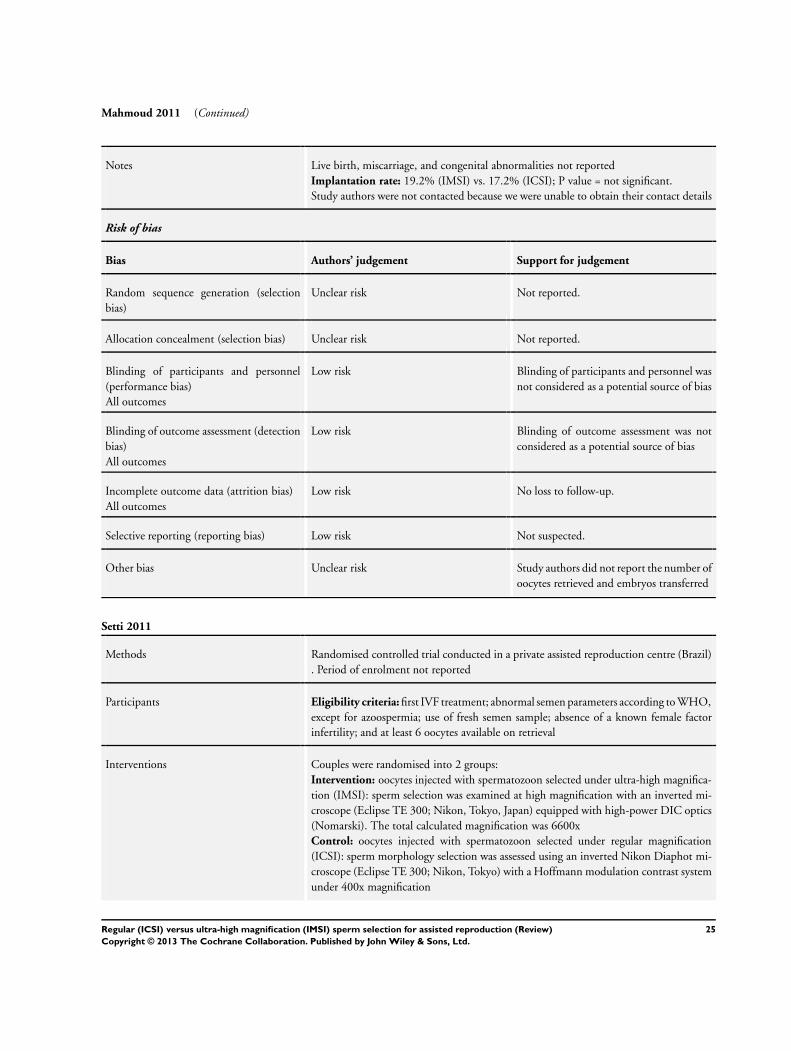
Setti 2011
Methods Randomised controlled trial conducted in a private assisted reproduction centre (Brazil)
. Period of enrolment not reported
Participants Eligibility criteria: first IVF treatment; abnormal semen parameters according to WHO,
except for azoospermia; use of fresh semen sample; absence of a known female factor
infertility; and at least 6 oocytes available on retrieval
Interventions Couples were randomised into 2 groups:
Intervention: oocytes injected with spermatozoon selected under ultra-high magnifica-
tion (IMSI): sperm selection was examined at high magnification with an inverted mi-
croscope (Eclipse TE 300; Nikon, Tokyo, Japan) equipped with high-power DIC optics
(Nomarski). The total calculated magnification was 6600x
Control: oocytes injected with spermatozoon selected under regular magnification
(ICSI): sperm morphology selection was assessed using an inverted Nikon Diaphot mi-
croscope (Eclipse TE 300; Nikon, Tokyo) with a Hoffmann modulation contrast system
under 400x magnification
25Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Setti 2011 (Continued)
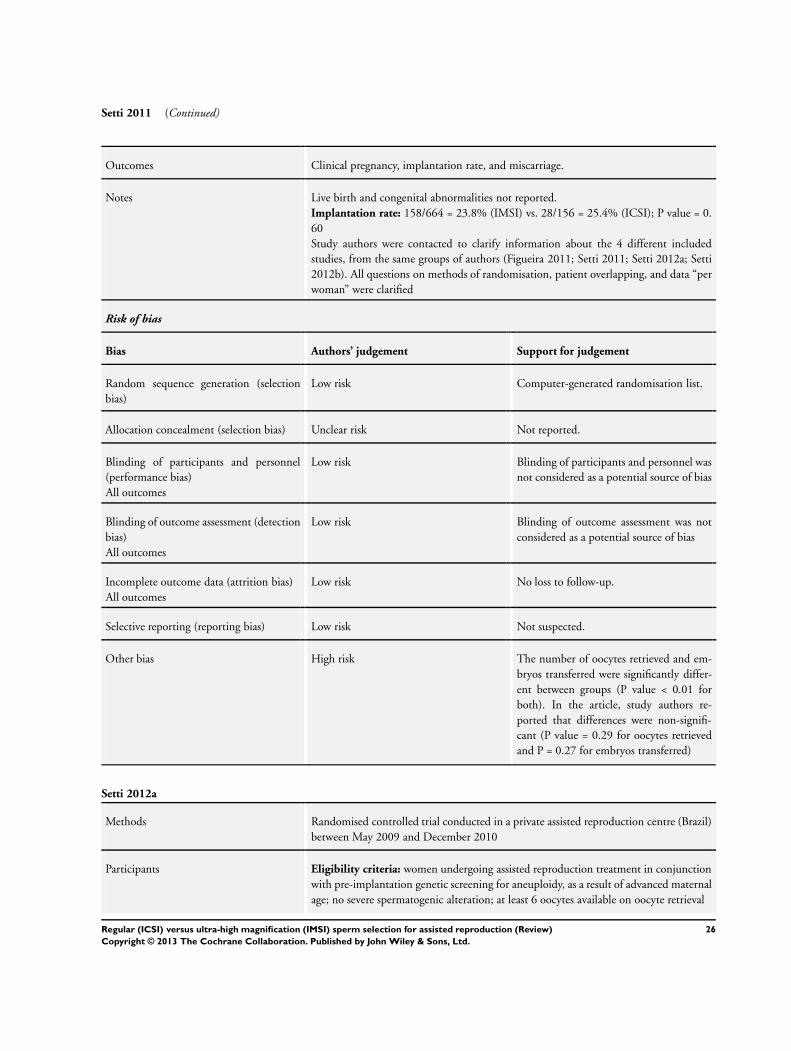
Outcomes Clinical pregnancy, implantation rate, and miscarriage.
Notes Live birth and congenital abnormalities not reported.
Implantation rate: 158/664 = 23.8% (IMSI) vs. 28/156 = 25.4% (ICSI); P value = 0.
60
Study authors were contacted to clarify information about the 4 different included
studies, from the same groups of authors (Figueira 2011; Setti 2011; Setti 2012a; Setti
2012b). All questions on methods of randomisation, patient overlapping, and data “per
woman” were clarified
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk Computer-generated randomisation list.
Allocation concealment (selection bias) Unclear risk Not reported.
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk Blinding of participants and personnel was
not considered as a potential source of bias
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk Blinding of outcome assessment was not
considered as a potential source of bias
Incomplete outcome data (attrition bias)
All outcomes
Low risk No loss to follow-up.
Selective reporting (reporting bias) Low risk Not suspected.
Other bias High risk The number of oocytes retrieved and em-
bryos transferred were significantly differ-
ent between groups (P value < 0.01 for
both). In the article, study authors re-
ported that differences were non-signifi-
cant (P value = 0.29 for oocytes retrieved
and P = 0.27 for embryos transferred)
Setti 2012a
Methods Randomised controlled trial conducted in a private assisted reproduction centre (Brazil)
between May 2009 and December 2010
Participants Eligibility criteria: women undergoing assisted reproduction treatment in conjunction
with pre-implantation genetic screening for aneuploidy, as a result of advanced maternal
age; no severe spermatogenic alteration; at least 6 oocytes available on oocyte retrieval
26Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Setti 2012a (Continued)
Interventions Couples were randomised into 2 groups:
Intervention: oocytes injected with spermatozoon selected under ultra-high magnifi-
cation (IMSI): sperm selection was examined at high magnification using a similar in-
verted microscope equipped with high-power DIC optics (Nomarski). The total cal-
culated magnification was 6600x. The sperm cells exhibiting normally shaped nuclei
(smooth, symmetric, and oval configuration) and normal nuclear chromatin content (if
it contained no more than 1 vacuole, which occupied < 4% of the nuclear area) were
selected for injection
Control: oocytes injected with spermatozoon selected under regular magnification
(ICSI): sperm morphology selection was assessed using an inverted Nikon Diaphot mi-
croscope (Eclipse TE 300; Nikon, Tokyo, Japan) with a Hoffmann modulation contrast
system under 400x magnification
Outcomes Clinical pregnancy, implantation rate, miscarriage, and gender incidence
Notes All embryos were submitted to pre-implantation genetic diagnosis and aneuploidy screen-
ing. On the morning of day 3 of embryo development, 1 cell per embryo was biopsied
by laser zona drilling using a 1.48 mm infrared diode laser (Octax Laser Shot System,
MTG, Bruckberg, Germany). Following the biopsies, the embryos were returned to the
culture medium. The removed blastomere nuclei were spread using 0.1 mol/L HCl and
0.01% Tween 20 (Sigma, Dorset, UK). Briefly, the blastomeres were placed on a slide
in a drop of HCl-Tween spreading solution and observed until the cell had lysed. The
slides were then air-dried and dehydrated before FISH analysis was performed. All em-
bryos were analysed for chromosomes X, Y, 13, 16, 18, 21, and 22. For the purpose of
this study, the blastomeres were classified as normal when 2 sexual and 2 of each tested
autosomal chromosomes were present. Embryo transfer was performed on day 5 using a
soft catheter with transabdominal ultrasound guidance. Only the embryos found to be
chromosomally normal were considered for embryo transfer, and up to a maximum of
3 embryos were transferred
Live birth and congenital abnormalities not reported.
Implantation rate: 46.1% (IMSI) vs. 41.6% (ICSI); P value = 0.59.
Study authors were contacted to clarify information about the 4 different included
studies, from the same groups of authors (Figueira 2011; Setti 2011; Setti 2012a; Setti
2012b). All questions on methods of randomisation, patient overlapping, and data “per
woman” were clarified
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Not reported.
Allocation concealment (selection bias) Unclear risk Not reported.
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk Blinding of participants and personnel was
not considered as a potential source of bias
27Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Setti 2012a (Continued)
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk Blinding of outcome assessment was not
considered as a potential source of bias
Incomplete outcome data (attrition bias)
All outcomes
Low risk No loss to follow-up.
Selective reporting (reporting bias) Low risk Not suspected.
Other bias High risk The number of oocytes retrieved and em-
bryos transferred were significantly differ-
ent between groups (P value = 0.01). In the
article, study authors reported these differ-
ences as not significant
Setti 2012b
Methods Prospective randomised clinical trial performed in a private fertility centre (Brazil). Period
of enrolment not reported
Participants Eligibility criteria: women of good physical and mental health; undergoing ICSI as a
result of advanced maternal age (≥ 37 years old); with regular menstrual cycles of 25-35
days; normal basal FSH and LH concentrations; body mass index < 30 kg/m2; presence
of both ovaries and intact uterus; absence of PCOS, endometriosis and gynaecological/
medical disorders; and a negative result in a screening for sexually transmitted diseases. All
male partners were normozoospermic, according to the WHO reference values (2010).
No woman had received any hormone therapy for at least 60 days preceding the study
Interventions Couples were randomised into 2 groups:
Intervention: sperm selection in the IMSI group was analysed under high magnification
using an inverted Nikon Diaphot microscope equipped with high-power DIC optics.
The total calculated magnification was 6600x. An aliquot of the sperm cell suspension
was transferred to a microdroplet of modified human tubal fluid medium containing
8% polyvinyl pyrrolidone (Irvine Scientific, Santa Ana, CA, USA) in a sterile glass dish
(FluoroDish; World Precision Instrument, Sarasota, FL, USA). The dish was placed on
a microscope stage above an Uplan Apo 100 oil/1.35 objective lens previously covered
by a droplet of immersion oil. The sperm cells that were selected for injection exhibited
normally shaped nuclei (smooth, symmetric and oval configuration) and normal nuclear
chromatin content (if it contained no more than 1 vacuole that occupied < 4% of the
nuclear area)
Control: sperm selection in the ICSI group was analysed under 400x magnification
using an inverted Nikon Eclipse TE 300 microscope
Outcomes Fertilisation rate, high-quality embryo rate on day 3, blastocyst formation rate, number
of transferred embryos, implantation rate, miscarriage rate and pregnancy rate
28Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Setti 2012b (Continued)
Notes Live birth and congenital abnormalities not reported.
Implantation rate: 38.3% (IMSI) vs. 12.1% (ICSI). P value = 0.03.
This article has been withdrawn. Authors were contacted for more information regarding
the reasons why this happened. Authors had also been contacted to clarify information
about the 4 different included studies, from the same groups of authors (Figueira 2011;
Setti 2011; Setti 2012a; Setti 2012b). All questions on methods of randomisation, patient
overlapping and data “per woman” were clarified
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk Computer-generated randomisation table.
Allocation concealment (selection bias) Unclear risk Not reported.
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk Blinding of participants and personnel was
not considered as a potential source of bias
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk Blinding of outcome assessment was not
considered as a potential source of bias
Incomplete outcome data (attrition bias)
All outcomes
Low risk No loss of follow-up.
Selective reporting (reporting bias) Low risk Not suspected.
Other bias High risk Although there was no significant differ-
ence in the number of oocytes retrieved,
and despite the total number of embryos
being higher in the ICSI group, more em-
bryos per woman were transferred in the
IMSI group
This article has been withdrawn.
DIC: differential interference contrast; FISH: fluorescent in situ hybridisation; FSH: follicle-stimulating hormone; HA: hyaluronate;
HCl: hydrochloric acid; ICSI: intracytoplasmic sperm injection; IMSI: intracytoplasmic morphologically selected sperm injection;
IVF: in vitro fertilisation; LH: luteinising hormone; MSOME: motile sperm organella morphology examination; PCOS: polycystic
ovaries syndrome; SD: standard deviation; WHO: World Health Organization.
29Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
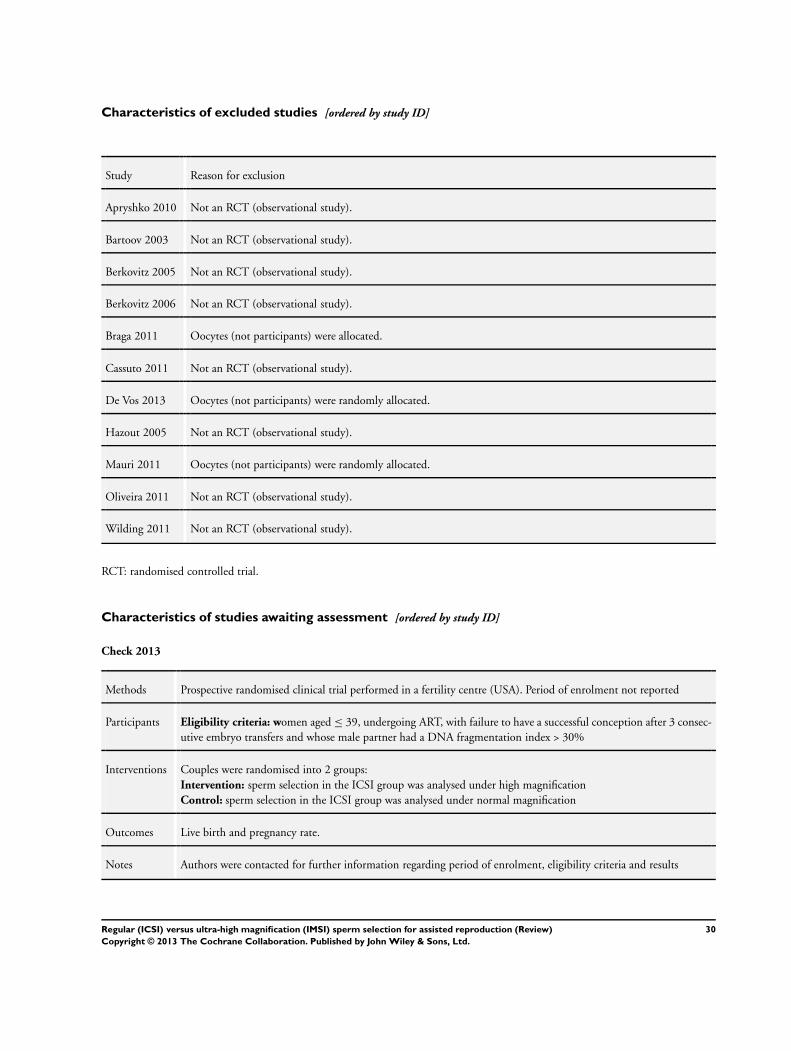
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Apryshko 2010 Not an RCT (observational study).
Bartoov 2003 Not an RCT (observational study).
Berkovitz 2005 Not an RCT (observational study).
Berkovitz 2006 Not an RCT (observational study).
Braga 2011 Oocytes (not participants) were allocated.
Cassuto 2011 Not an RCT (observational study).
De Vos 2013 Oocytes (not participants) were randomly allocated.
Hazout 2005 Not an RCT (observational study).
Mauri 2011 Oocytes (not participants) were randomly allocated.
Oliveira 2011 Not an RCT (observational study).
Wilding 2011 Not an RCT (observational study).
RCT: randomised controlled trial.
Characteristics of studies awaiting assessment [ordered by study ID]
Check 2013
Methods Prospective randomised clinical trial performed in a fertility centre (USA). Period of enrolment not reported
Participants Eligibility criteria: women aged ≤ 39, undergoing ART, with failure to have a successful conception after 3 consec-
utive embryo transfers and whose male partner had a DNA fragmentation index > 30%
Interventions Couples were randomised into 2 groups:
Intervention: sperm selection in the ICSI group was analysed under high magnification
Control: sperm selection in the ICSI group was analysed under normal magnification
Outcomes Live birth and pregnancy rate.
Notes Authors were contacted for further information regarding period of enrolment, eligibility criteria and results
30Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
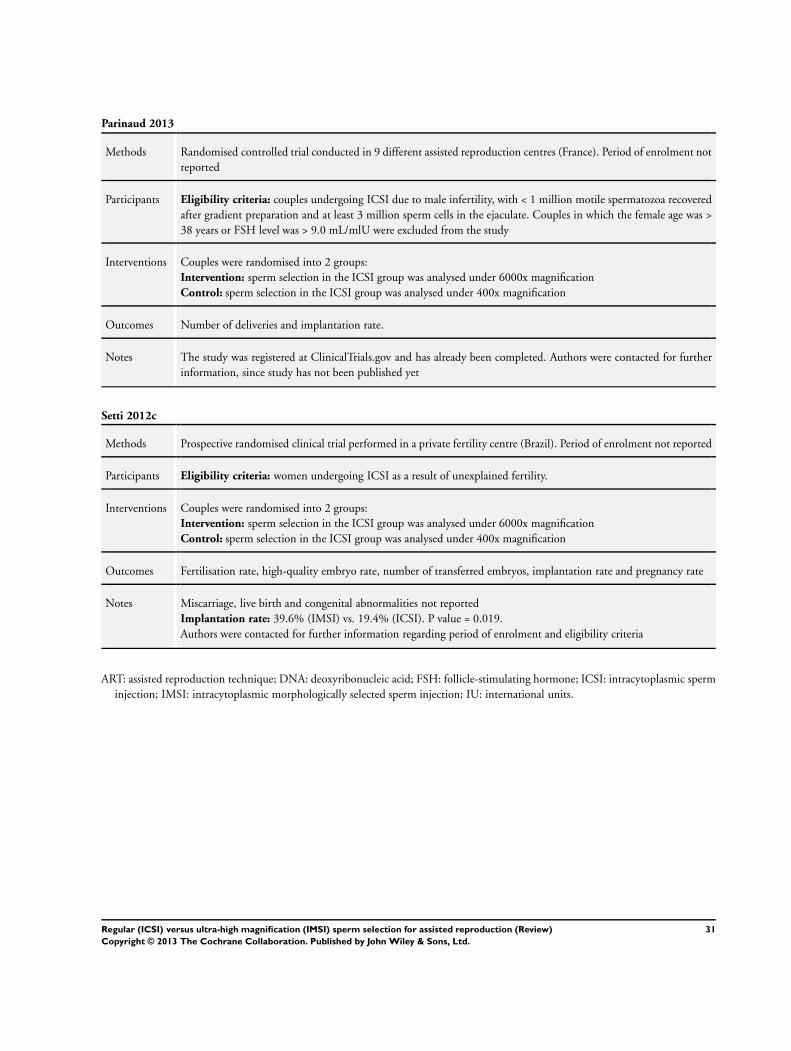
Parinaud 2013
Methods Randomised controlled trial conducted in 9 different assisted reproduction centres (France). Period of enrolment not
reported
Participants Eligibility criteria: couples undergoing ICSI due to male infertility, with < 1 million motile spermatozoa recovered
after gradient preparation and at least 3 million sperm cells in the ejaculate. Couples in which the female age was >
38 years or FSH level was > 9.0 mL/mlU were excluded from the study
Interventions Couples were randomised into 2 groups:
Intervention: sperm selection in the ICSI group was analysed under 6000x magnification
Control: sperm selection in the ICSI group was analysed under 400x magnification
Outcomes Number of deliveries and implantation rate.
Notes The study was registered at ClinicalTrials.gov and has already been completed. Authors were contacted for further
information, since study has not been published yet
Setti 2012c
Methods Prospective randomised clinical trial performed in a private fertility centre (Brazil). Period of enrolment not reported
Participants Eligibility criteria: women undergoing ICSI as a result of unexplained fertility.
Interventions Couples were randomised into 2 groups:
Intervention: sperm selection in the ICSI group was analysed under 6000x magnification
Control: sperm selection in the ICSI group was analysed under 400x magnification
Outcomes Fertilisation rate, high-quality embryo rate, number of transferred embryos, implantation rate and pregnancy rate
Notes Miscarriage, live birth and congenital abnormalities not reported
Implantation rate: 39.6% (IMSI) vs. 19.4% (ICSI). P value = 0.019.
Authors were contacted for further information regarding period of enrolment and eligibility criteria
ART: assisted reproduction technique; DNA: deoxyribonucleic acid; FSH: follicle-stimulating hormone; ICSI: intracytoplasmic sperm
injection; IMSI: intracytoplasmic morphologically selected sperm injection; IU: international units.
31Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
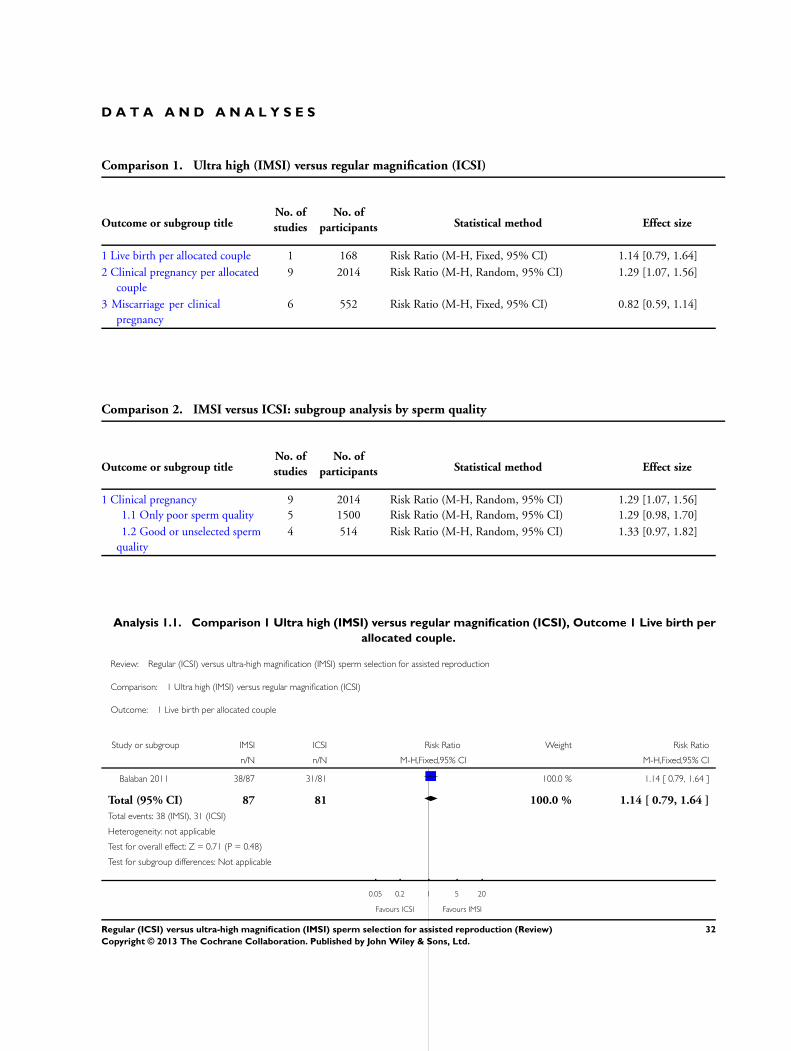
D A T A A N D A N A L Y S E S
Comparison 1. Ultra high (IMSI) versus regular magnification (ICSI)
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Live birth per allocated couple 1 168 Risk Ratio (M-H, Fixed, 95% CI) 1.14 [0.79, 1.64]
2 Clinical pregnancy per allocated
couple
9 2014 Risk Ratio (M-H, Random, 95% CI) 1.29 [1.07, 1.56]
3 Miscarriage per clinical
pregnancy
6 552 Risk Ratio (M-H, Fixed, 95% CI) 0.82 [0.59, 1.14]
Comparison 2. IMSI versus ICSI: subgroup analysis by sperm quality
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Clinical pregnancy 9 2014 Risk Ratio (M-H, Random, 95% CI) 1.29 [1.07, 1.56]
1.1 Only poor sperm quality 5 1500 Risk Ratio (M-H, Random, 95% CI) 1.29 [0.98, 1.70]
1.2 Good or unselected sperm
quality
4 514 Risk Ratio (M-H, Random, 95% CI) 1.33 [0.97, 1.82]
Analysis 1.1. Comparison 1 Ultra high (IMSI) versus regular magnification (ICSI), Outcome 1 Live birth per
allocated couple.
Review: Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction
Comparison: 1 Ultra high (IMSI) versus regular magnification (ICSI)
Outcome: 1 Live birth per allocated couple
Study or subgroup IMSI ICSI Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Balaban 2011 38/87 31/81 100.0 % 1.14 [ 0.79, 1.64 ]
Total (95% CI) 87 81 100.0 % 1.14 [ 0.79, 1.64 ]
Total events: 38 (IMSI), 31 (ICSI)
Heterogeneity: not applicable
Test for overall effect: Z = 0.71 (P = 0.48)
Test for subgroup differences: Not applicable
0.05 0.2 1 5 20
Favours ICSI Favours IMSI
32Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
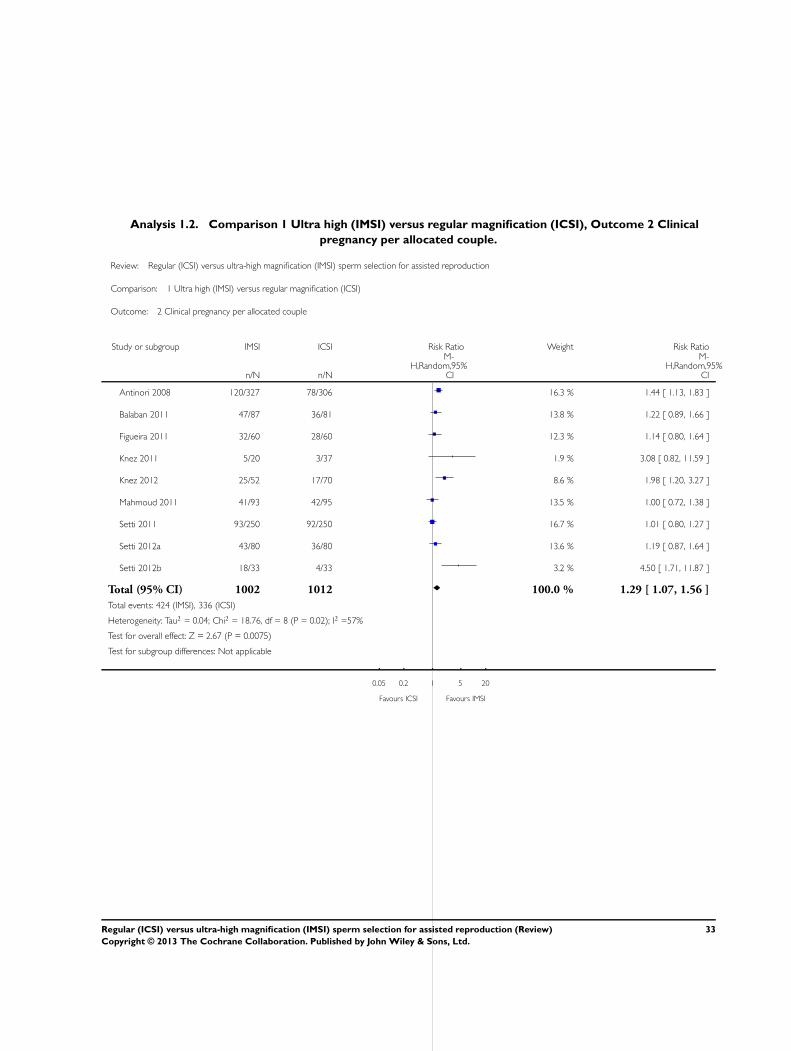
Analysis 1.2. Comparison 1 Ultra high (IMSI) versus regular magnification (ICSI), Outcome 2 Clinical
pregnancy per allocated couple.
Review: Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction
Comparison: 1 Ultra high (IMSI) versus regular magnification (ICSI)
Outcome: 2 Clinical pregnancy per allocated couple
Study or subgroup IMSI ICSI Risk Ratio Weight Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
Antinori 2008 120/327 78/306 16.3 % 1.44 [ 1.13, 1.83 ]
Balaban 2011 47/87 36/81 13.8 % 1.22 [ 0.89, 1.66 ]
Figueira 2011 32/60 28/60 12.3 % 1.14 [ 0.80, 1.64 ]
Knez 2011 5/20 3/37 1.9 % 3.08 [ 0.82, 11.59 ]
Knez 2012 25/52 17/70 8.6 % 1.98 [ 1.20, 3.27 ]
Mahmoud 2011 41/93 42/95 13.5 % 1.00 [ 0.72, 1.38 ]
Setti 2011 93/250 92/250 16.7 % 1.01 [ 0.80, 1.27 ]
Setti 2012a 43/80 36/80 13.6 % 1.19 [ 0.87, 1.64 ]
Setti 2012b 18/33 4/33 3.2 % 4.50 [ 1.71, 11.87 ]
Total (95% CI) 1002 1012 100.0 % 1.29 [ 1.07, 1.56 ]
Total events: 424 (IMSI), 336 (ICSI)
Heterogeneity: Tau2 = 0.04; Chi2 = 18.76, df = 8 (P = 0.02); I2 =57%
Test for overall effect: Z = 2.67 (P = 0.0075)
Test for subgroup differences: Not applicable
0.05 0.2 1 5 20
Favours ICSI Favours IMSI
33Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
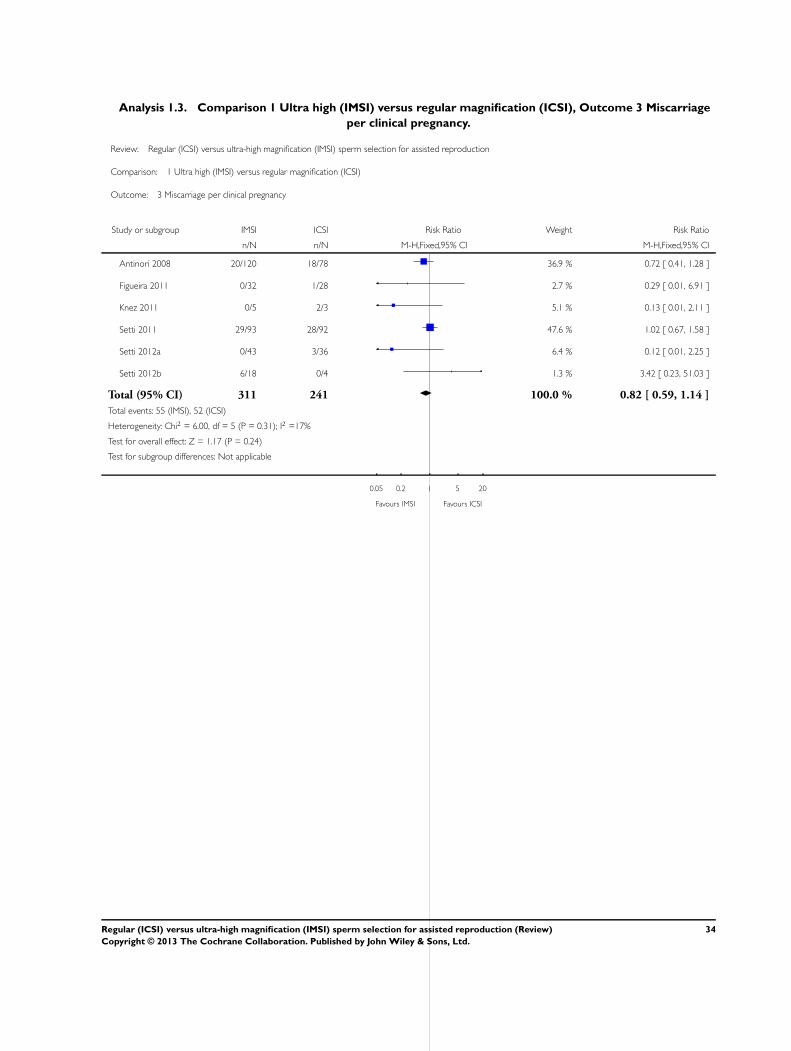
Analysis 1.3. Comparison 1 Ultra high (IMSI) versus regular magnification (ICSI), Outcome 3 Miscarriage
per clinical pregnancy.
Review: Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction
Comparison: 1 Ultra high (IMSI) versus regular magnification (ICSI)
Outcome: 3 Miscarriage per clinical pregnancy
Study or subgroup IMSI ICSI Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Antinori 2008 20/120 18/78 36.9 % 0.72 [ 0.41, 1.28 ]
Figueira 2011 0/32 1/28 2.7 % 0.29 [ 0.01, 6.91 ]
Knez 2011 0/5 2/3 5.1 % 0.13 [ 0.01, 2.11 ]
Setti 2011 29/93 28/92 47.6 % 1.02 [ 0.67, 1.58 ]
Setti 2012a 0/43 3/36 6.4 % 0.12 [ 0.01, 2.25 ]
Setti 2012b 6/18 0/4 1.3 % 3.42 [ 0.23, 51.03 ]
Total (95% CI) 311 241 100.0 % 0.82 [ 0.59, 1.14 ]
Total events: 55 (IMSI), 52 (ICSI)
Heterogeneity: Chi2 = 6.00, df = 5 (P = 0.31); I2 =17%
Test for overall effect: Z = 1.17 (P = 0.24)
Test for subgroup differences: Not applicable
0.05 0.2 1 5 20
Favours IMSI Favours ICSI
34Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
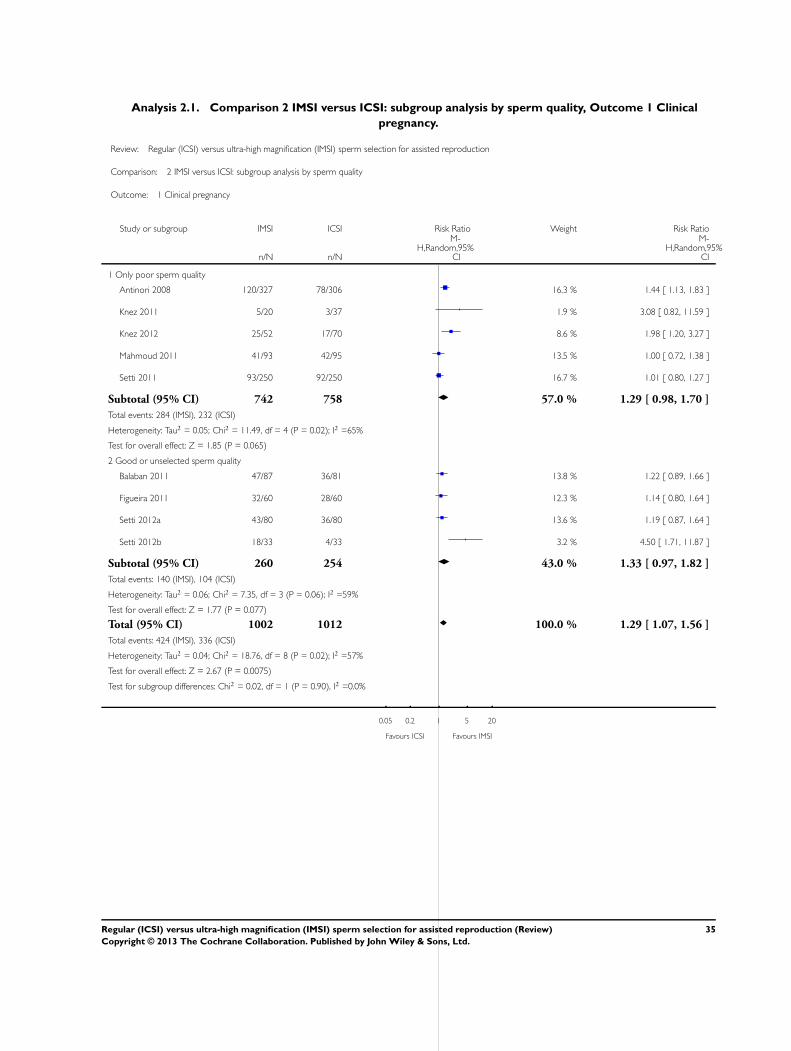
Analysis 2.1. Comparison 2 IMSI versus ICSI: subgroup analysis by sperm quality, Outcome 1 Clinical
pregnancy.
Review: Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction
Comparison: 2 IMSI versus ICSI: subgroup analysis by sperm quality
Outcome: 1 Clinical pregnancy
Study or subgroup IMSI ICSI Risk Ratio Weight Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
1 Only poor sperm quality
Antinori 2008 120/327 78/306 16.3 % 1.44 [ 1.13, 1.83 ]
Knez 2011 5/20 3/37 1.9 % 3.08 [ 0.82, 11.59 ]
Knez 2012 25/52 17/70 8.6 % 1.98 [ 1.20, 3.27 ]
Mahmoud 2011 41/93 42/95 13.5 % 1.00 [ 0.72, 1.38 ]
Setti 2011 93/250 92/250 16.7 % 1.01 [ 0.80, 1.27 ]
Subtotal (95% CI) 742 758 57.0 % 1.29 [ 0.98, 1.70 ]
Total events: 284 (IMSI), 232 (ICSI)
Heterogeneity: Tau2 = 0.05; Chi2 = 11.49, df = 4 (P = 0.02); I2 =65%
Test for overall effect: Z = 1.85 (P = 0.065)
2 Good or unselected sperm quality
Balaban 2011 47/87 36/81 13.8 % 1.22 [ 0.89, 1.66 ]
Figueira 2011 32/60 28/60 12.3 % 1.14 [ 0.80, 1.64 ]
Setti 2012a 43/80 36/80 13.6 % 1.19 [ 0.87, 1.64 ]
Setti 2012b 18/33 4/33 3.2 % 4.50 [ 1.71, 11.87 ]
Subtotal (95% CI) 260 254 43.0 % 1.33 [ 0.97, 1.82 ]
Total events: 140 (IMSI), 104 (ICSI)
Heterogeneity: Tau2 = 0.06; Chi2 = 7.35, df = 3 (P = 0.06); I2 =59%
Test for overall effect: Z = 1.77 (P = 0.077)
Total (95% CI) 1002 1012 100.0 % 1.29 [ 1.07, 1.56 ]
Total events: 424 (IMSI), 336 (ICSI)
Heterogeneity: Tau2 = 0.04; Chi2 = 18.76, df = 8 (P = 0.02); I2 =57%
Test for overall effect: Z = 2.67 (P = 0.0075)
Test for subgroup differences: Chi2 = 0.02, df = 1 (P = 0.90), I2 =0.0%
0.05 0.2 1 5 20
Favours ICSI Favours IMSI
35Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
A P P E N D I C E S
Appendix 1. Menstrual Disorders and Subfertility Group search strategy
Search results for Menstrual Disorders and Subfertility Group (MDSG) database, 8 May 2013:
Keywords CONTAINS “icsi”or “ICSI failure”or “ICSI injection site”or“intracytoplasmic sperm injection”or“intracytoplasmic sperm
injection cycle”or “intracytoplasmic sperm injection techniques”or Title CONTAINS “icsi”or “ICSI failure”or “ICSI injection
site”or“intracytoplasmic sperm injection”or“intracytoplasmic sperm injection cycle”or “intracytoplasmic sperm injection techniques”
AND
Keywords CONTAINS “IMSI” or “intracytoplasmic morphologically selected sperm injection” or Title CONTAINS “IMSI” or
“intracytoplasmic morphologically selected sperm injection”
22 records
Appendix 2. CENTRAL search strategy
Database: EBM Reviews - Cochrane Central Register of Controlled Trials, 2013, Issue 2
Search strategy:
--------------------------------------------------------------------------------
1 icsi.tw. (684)
2 intracytoplasmic sperm injection$.tw. (417)
3 exp Sperm Injections, Intracytoplasmic/ (334)
4 conventional intracytoplasmic injection$.tw. (1)
5 regular magnification.tw. (0)
6 or/1-5 (886)
7 intracytoplasmic morphologically selected sperm injection$.tw. (11)
8 IMSI.tw. (11)
9 MSOME.tw. (0)
10 motile sperm organelle morphology examination$.tw. (0)
11 high magnification.tw. (18)
12 or/7-11 (27)
13 6 and 12 (10)
Appendix 3. MEDLINE search strategy
Search results for Ovid MEDLINE(R) In-Process & Other Non-Indexed Citations, Ovid MEDLINE(R) Daily and Ovid MEDLINE(R)
<1946 to Present>, 8 May 2013:
1 icsi.tw. (5253)
2 intracytoplasmic sperm injection$.tw. (4724)
3 exp Sperm Injections, Intracytoplasmic/ (4426)
4 conventional intracytoplasmic injection$.tw. (1)
5 regular magnification.tw. (1)
6 or/1-5 (7703)
7 intracytoplasmic morphologically selected sperm injection$.tw. (36)
8 IMSI.tw. (40)
9 MSOME.tw. (29)
10 motile sperm organelle morphology examination$.tw. (22)
11 high magnification.tw. (1058)
12 or/7-11 (1101)
13 6 and 12 (62)
14 randomized controlled trial.pt. (348,486)
15 controlled clinical trial.pt. (85,883)
16 randomized.ab. (266,743)
36Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
17 placebo.tw. (147,938)
18 clinical trials as topic.sh. (164,266)
19 randomly.ab. (194,103)
20 trial.ti. (113,955)
21 (crossover or cross-over or cross over).tw. (56,715)
22 or/14-21 (857,284)
23 exp animals/ not humans.sh. (3,809,801)
24 22 not 23 (790,248)
25 13 and 24 (14)
Appendix 4. EMBASE search strategy
Database: EMBASE <1980 to 8 May 2013>
Search strategy:
--------------------------------------------------------------------------------
1 exp intracytoplasmic sperm injection/ (11,216)
2 icsi.tw. (8334)
3 intracytoplasmic sperm injection$.tw. (5798)
4 conventional intracytoplasmic injection$.tw. (1)
5 regular magnification.tw. (2)
6 or/1-5 (13,225)
7 intracytoplasmic morphologically selected sperm injection$.tw. (75)
8 IMSI.tw. (111)
9 MSOME.tw. (59)
10 motile sperm organelle morphology examination$.tw. (41)
11 high magnification.tw. (1291)
12 or/7-11 (1374)
13 6 and 12 (142)
14 Clinical Trial/ (877227)
15 Randomized Controlled Trial/ (341,619)
16 exp randomization/ (61290)
17 Single Blind Procedure/ (17,333)
18 Double Blind Procedure/ (114,409)
19 Crossover Procedure/ (36,788)
20 Placebo/ (217,264)
21 Randomi?ed controlled trial$.tw. (86,231)
22 Rct.tw. (11,331)
23 random allocation.tw. (1232)
24 randomly allocated.tw. (18,653)
25 allocated randomly.tw. (1878)
26 (allocated adj2 random).tw. (718)
27 Single blind$.tw. (13,248)
28 Double blind$.tw. (135,874)
29 ((treble or triple) adj blind$).tw. (312)
30 placebo$.tw. (187828)
31 prospective study/ (231,998)
32 or/14-31 (1,324,701)
33 case study/ (19,500)
34 case report.tw. (242,862)
35 abstract report/ or letter/ (866,817)
36 or/33-35 (1,124,107)
37 32 not 36 (1,288,419)
37Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
38 13 and 37 (34)
Appendix 5. CINAHL search strategy
Search results for Cumulative Index to Nursing and Allied Health Literature (CINAHL), 7 May 2013:
((intracytoplasmic sperm injection*) OR (icsi) OR (conventional intracytoplasmic injection*) OR (regular magnification)) AND
((intracytoplasmic morphologically selected sperm injection*) OR (IMSI) OR (MSOME) OR (motile sperm organelle morphology
examination*) OR (high magnification))
0 records
Appendix 6. LILACS search strategy
Search results for Literatura Latino-Americana e do Caribe em Ciências da Saúde (LILACS), 7 May 2013:
((intracytoplasmic sperm injection$) OR (icsi) OR (conventional intracytoplasmic injection$) OR (regular magnification)) AND
((intracytoplasmic morphologically selected sperm injection$) OR (IMSI) OR (MSOME) OR (motile sperm organelle morphology
examination$) OR (high magnification))
1 record
Appendix 7. PsycINFO search strategy
Search results for PsycINFO, 8 May 2013:
1 intracytoplasmic sperm injection$.tw. (33)
2 icsi.tw. (38)
3 conventional intracytoplasmic injection$.tw. (0)
4 regular magnification.tw. (0)
5 or/1-4 (50)
6 intracytoplasmic morphologically selected sperm injection$.tw. (0)
7 IMSI.tw. (1)
8 MSOME.tw. (0)
9 motile sperm organelle morphology examination$.tw. (0)
10 high magnification.tw. (20)
11 or/6-10 (21)
12 5 and 11 (0)
Appendix 8. Trials registers search strategy
Search results for ClinicalTrial.gov, 7 May 2013:
(imsi) OR (msome) OR (motile sperm organelle morphology examination) OR ((high magnification) AND (sperm))
6 records
Search results for Current Controlled Trials, 7 May 2013:
(imsi) OR (msome) OR (motile sperm organelle morphology examination) OR ((high magnification) AND (sperm))
0 records
Search results for World Health Organization International Clinical Trials Registry Platform, 7 May 2013:
IMSI OR MSOME
6 records
38Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Appendix 9. Web of Knowledge search strategy
Search results for Web of Knowledge, 7 May 2013:
(((intracytoplasmic sperm injection*) OR (icsi) OR (conventional intracytoplasmic injection*) OR (regular magnification)) AND
((intracytoplasmic morphologically selected sperm injection*) OR (IMSI) OR (MSOME) OR (motile sperm organelle morphology
examination*) OR (high magnification)))
240 records
Appendix 10. OpenGrey search strategy
Search results for OpenGrey, 7 May 2013:
((intracytoplasmic sperm injection*) OR (icsi) OR (conventional intracytoplasmic injection*) OR (regular magnification)) AND
((intracytoplasmic morphologically selected sperm injection*) OR (IMSI) OR (MSOME) OR (motile sperm organelle morphology
examination*) OR (high magnification))
0 records
Appendix 11. DARE search strategy
Search results for Database of Abstracts of Reviews of Effects (DARE), 7 May 2013:
((intracytoplasmic sperm injection$) OR (icsi) OR (conventional intracytoplasmic injection$) OR (regular magnification)) AND
((intracytoplasmic morphologically selected sperm injection$) OR (IMSI) OR (MSOME) OR (motile sperm organelle morphology
examination$) OR (high magnification))
5 records
C O N T R I B U T I O N S O F A U T H O R S
Drafting the protocol: Danielle M Teixeira, Mariana AP Barbosa, Rui A Ferriani, Paula A Navarro, Nick Raine-Fenning, Carolina O
Nastri, Wellington P Martins.
Development of search strategy: Danielle M Teixeira, Wellington P Martins.
Search for trials: Danielle M Teixeira, Mariana AP Barbosa, Wellington P Martins.
Obtaining copies of trials: Danielle M Teixeira, Wellington P Martins.
Selection of which trials to include: Danielle M Teixeira, Mariana AP Barbosa, Wellington P Martins.
Extraction of data from trials: Danielle M Teixeira, Mariana AP Barbosa, Wellington P Martins.
Assessment of risk of bias in included studies: Danielle M Teixeira, Mariana AP Barbosa, Carolina O Nastri.
Entry of data into RevMan: Danielle M Teixeira, Carolina O Nastri, Wellington P Martins.
Drafting the review: Danielle M Teixeira, Mariana AP Barbosa, Rui A Ferriani, Paula A Navarro, Nick Raine-Fenning, Carolina O
Nastri, Wellington P Martins.
39Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

D E C L A R A T I O N S O F I N T E R E S T
The authors declare no conflicts of interest.
S O U R C E S O F S U P P O R T
Internal sources
• Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), Brazil.
Scholarship
• Hospital das Clínicas FMRP-USP, Brazil.
Salary
• Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), Brazil.
Scholarship
• Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP), Brazil.
Scholarship
External sources
• No sources of support supplied
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
None.
40Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for assisted reproduction (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Related Documents











