Red and Scaly Rashes Dr Ben CM Lee MB BS MRCP(UK) Speciality Doctor in Dermatology

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Red and Scaly RashesDr Ben CM Lee MB BS MRCP(UK)Speciality Doctor in Dermatology
Content (you should know. Keep it systematic!)• Acute (<6 weeks)• Localised
• Dermatophyte infections• Generalised
• With fever• Scarlet fever• Kawasaki syndrome• Erythroderma
• Without fever• Pityriasis rosea• Acute guttate psoriasis• Drug reactions: pityriasiform (lichenoid drug eruption)
Content (to talk about if we have time…)• Chronic (>6 weeks)
• Localised• Seborrhoeic dermatitis• Psoriasis• Discoid lupus erythematosus• Pityriasis versicolor• Keratosis pilaris• Annular erythema• Palmoplantar keratoderma
• Generalised• Chronic plaque psoriasis• Lichen planus• Pityriasis lichenoides• Pityriasis rubra pilaris• Cutaneous T cell lymphoma

Dermatophyte infections• Tineas
• Barbae (beard)• Capitis (head)• Corporis (body)• Cruris (groin)• Faciei (face)• Manuum (hands)• Pedis (feet)• Unquium (nail)
• 3 genera microsporum, Trichophyton, epidermophyton• Keratinolytic enzymes (e.g. keratinase)• Sebum has an inhibitory effect on dermatophytes

Clinical features: main points• Typically erythematous, sharply marginated, scaly plaque
• With raised, advancing border; typically with central clearing and annular or arcuate shape
• If inflammatory reaction robust – tinea profunda (aka kerion on H&N)• With prior treatment with topical corticosteroid – tinea incognito• Invasion of hair follicles – fungal folliculitis (Majocchi’s granuloma); granulomatous folliculitis
• Must treat with oral antifungal
• Onychomycosis• Leukonychia, dystrophic nail plate due to hyperkeratosis, onycholysis• Must treat with oral antifungal
• Tinea cruris• Scrotum rarely involved; if so, consider candidiasis
• Erythrasma, a bacterial infection by Corynebacterium minutissiumum
Investigation• Direct microscopy of affected tissue• Mycology culture• Screen for diabetes
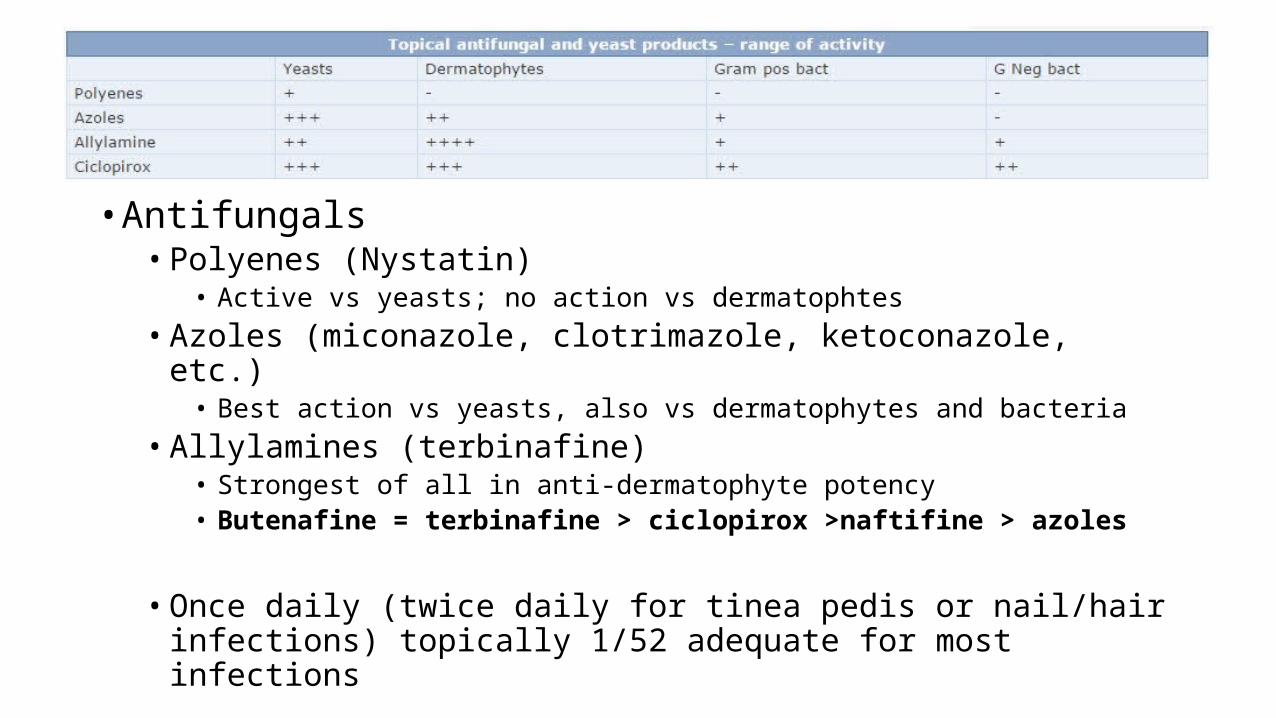
Treatment: you need to know• Antifungals• Polyenes (Nystatin)
• Active vs yeasts; no action vs dermatophtes• Azoles (miconazole, clotrimazole, ketoconazole, etc.)
• Best action vs yeasts, also vs dermatophytes and bacteria• Allylamines (terbinafine)
• Strongest of all in anti-dermatophyte potency• Butenafine = terbinafine > ciclopirox >naftifine > azoles
• Once daily (twice daily for tinea pedis or nail/hair infections) topically 1/52 adequate for most infections

Scarlet Fever• aetiology: group A strep (erythrogenic toxin A B and C – the primary
cause)• Children (aged 1-10 yrs)• Erythema of axilla, neck and chest -> pink papules with erythematous
back ground (sandpaper like) -> hand and foot desquamation (7-10 days)• Oral: “red strawberry” tongue• Pastia’s lines (linear petechial streaks in body folds)

Scarlet Fever• Treatment• PCN 7-10 days; erythromycin is PCN allergic

Kawasaki Disease• Aka mucocutaneous lymph node syndrome• Aetiology: unknown, ?infection• Children, <5 yrs• Systemic symptoms (dx criteria); cardiac aneurysm in 25% untreated and
therefore is important• 5/6 of: Rash; fever >5 days; conjunctivitis; palmoplantar erythema and
desquamation; swollen lips or red tongue; cervical LNs
• Polymorphous eruption +/- oedema and erythema of distal extremities• Oral: red swollen or dry fissured lips; strawberry tongue; pharyngeal
erythema

Erythroderma• Most common: 30% idiopathic• drug eruption• Atopic dermatitis• Psoriasis• Pityriasis rubra pilaris• Contact dermatitis• Sezary syndrome• Haematological malignancies• Other malignancies• Immunobullous disease• HIV infection
• Defined as generalised exfoliative dermatitis with 90% BSA involvement• DO NOT RX systemic steroid

Erythroderma• Clinical Features• History of pre-existing dermatosis• Skin feels warm to touch• Intolerable pruritis• Eye swelling -> ectropion• Scaling and varying degree of hair loss o scalp• Nail involvement• Keratoderma• Lymphadenopathy• Clues of underlying cause
Erythroderma• History and examination paramount• FBC: anaemia WCC abnormal (eosinophilia common, but if +++,
suspect lymphoma)• 20% sezary cells in sezary sx• CRP may be elevated• Raised IgE in idiopathic erythroderma• Skin biopsies from several sites inc. for IMF (immunobullous dx)
Erythroderma: General Management• Derm emergency• Immediate fluid resus ABCDE• Discontinue all unnecessary medications• Monitor fluid balance and body temperature• Restore skin barrier with wet wraps, emollients, mild topical steroids• Antibiotics if bacterial infection• Antihistamine to reduce severe itch and sedation• Systemic steroid only if certain NOT pustular psoriasis; suitable for atopic
dermatitis; acetretin or MTX for psoriasis.

Cutaneous T cell lymphoma• T cell neoplasm originating in skin• Patch stage
• Erythematous, violet or hyperpigmented patches in sun-protected areas such as buttocks, thighs, abdomen
• Plaque stage• Well-demarcated irregularly shaped erythematous to violaceous to red-brown plaques in sun-
protected areas; often pruritic and assymetric; may arise de novo or from existing patches
• Tumour stages• Enlarging dome-shaped smooth nodules; vertical growth
• Sezary syndrome• Triad of: generalised lymphadenopathy, pruritic erythroderma, and sezary cells• other sx: alopecia, nail dystrophy, scaling of palms/soles (keratoderma)
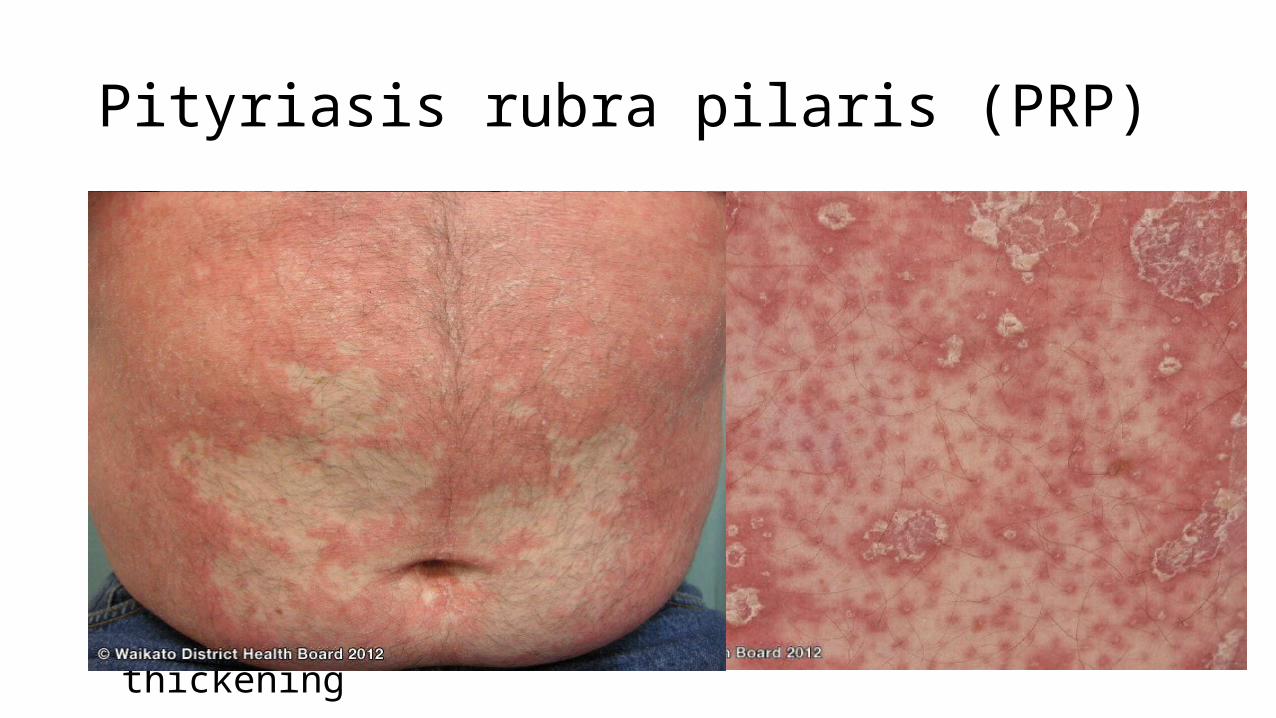
Pityriasis rubra pilaris (PRP)• Disorder of keratinisation • Bimodal distribution (type III-V in children and I-II in adults)• Acquired in most cases
• Hyperkeratotis follicular papules on erythematous base• Coalesce into large orange-red to red patches • Islands of sparing• Keratoderma• Nail: subungual hyperkeratosis and nail plate thickening

PRP: histology and treatment• Vertically and horizontally alternating parakeratosis and
orthokeratosis – checker board parakeratosis• Treatment• High potency topical corticosteroid• Systemic retinoid• MTX +/- phototherapy• Azathioprin• infliximab

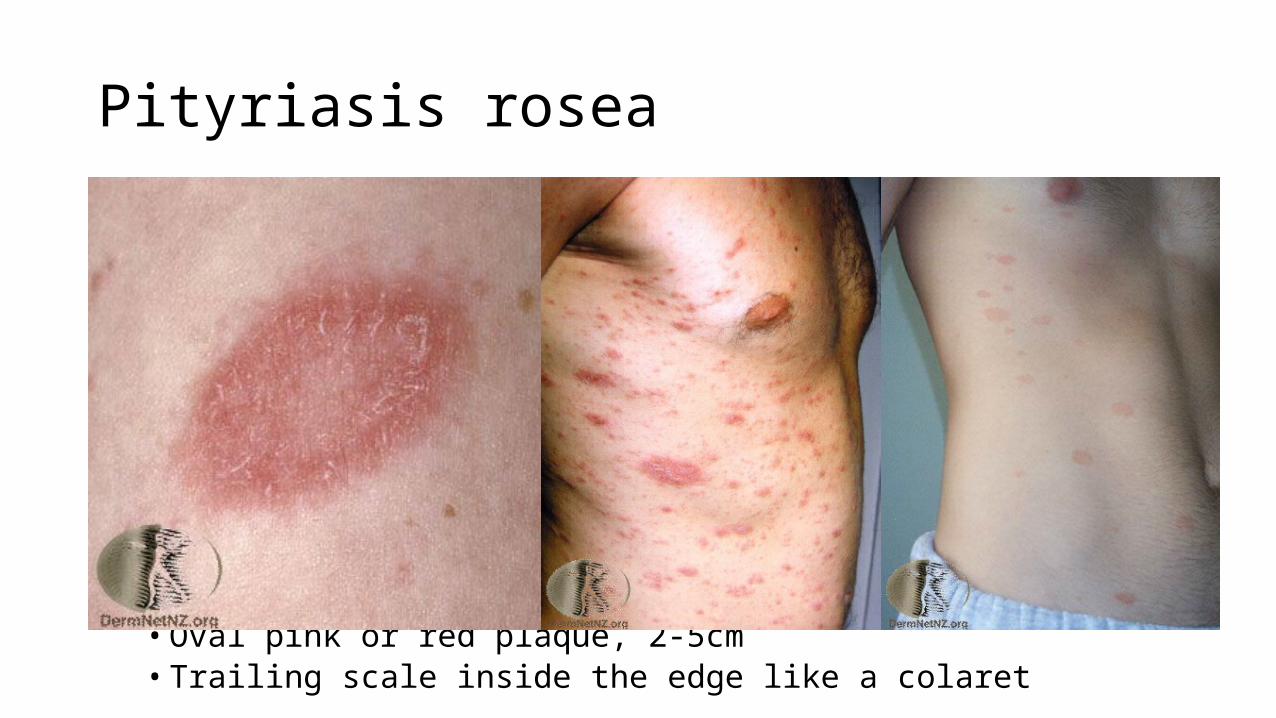
Pityriasis rosea• Pityriasis – oatmeal scaling; pityriasiform• Different to roseola infantum/6th disease (HHV6 or 7)• Can be associated
• Viral exanthem; can last for up to 12 weeks• Herald patch -> smaller, similar patches on chest and back• Herald patch• 1-20days before generalised eruption• Oval pink or red plaque, 2-5cm• Trailing scale inside the edge like a colaret
Psoriasis
• Chronic, recurrent disease affecting 2% population– Abnormal T cell activation: TH mediated autoimmunity towards ?antigens– Abnormal keratinocytes (3-5 days of migration from basal layer to surface vs
normal of 28 days); ↑antimicrobial peptides: human-beta-defensin-2, secretory leukocyte protease inhibitor, skin-derived anti-leukoproteinase (SKALP)
– Polygenic and multifactorial: HLA Cw6>B27 (seroneg spondylopathy)>B17, B57, DR7, B13>Cw2, HLA A2
– Associated with IHD, dyslipidemia, DM, IBD (B27+)– Parakeratotic scales; acanthosis, dilated vessels in superficial dermis, perivascular
lymphocytes– Microabscesses in SC (Munro microabscesses); in SS (Kogoj pustules)

Chronic Plaque Psoriasis

Guttate Psoriasis

Palmoplantar psoriasis

Pustular Psoriasis

Treatment• Topicals
– Fixed combination betamethasone diproprionate/calcipotriol (Dovibet®)– Calcineurin inhibitors (Protopic®) for intertriginous or sensitive areas– Coal tar messy
• Systemic– Methotrexate– Cyclosporin– Acetretin
• Apremilast (phosphodiesterase-4 inhibitor)– PDE4 degrades cAMP-AMP: proinflammatory
• Biologics • Phototherapy (PUVA, NB UVB)
Lichenoid Dermatoses
• A very important pattern of dermatitis• Centre of gravity is located at the DEJ– Lymphocytic inflammation at the DEJ– Vacuolar change in basal keratinocytes (“hydropic” degeneration)– Colloid bodies– A huge variety of clinical pictures, but typically 4 Ps:• Pruritic• Purple/violaceous• Polygonal• Papular (flat-topped)

Conditions with lichenoid pattern• Lichen Planus and its variants
– Hypertropic LP: hyperkeratotic, easily misdiagnosed as SCC• Lichen nitidus• Lupus erythematosus• Dermatomyositis• Lichen sclerosus• Erythema multiforme• Drug reactions• Fixed drug reaction• Viral exanthema• Mycosis fungoides• Lichenoid actinic keratosis• Lichenoid Keratosis (lichen planus like keratosis)


Thankyou
Related Documents











