CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024 Page 1 of 34 Rapid Tranquillisation Protocol for the prescribing and administration of injectable drugs for rapid tranquillisation (RT), physical health assessment and monitoring, including prescribing guidelines on the drugs to be used for RT Clinical Protocol CP11 Protocol Summary Rapid Tranquillisation (RT) with injectable medication refers to the appropriate use of medication to manage violent behaviour safely and effectively. The aim of the intervention is an emergency measure to quickly calm a person down and reduce the risk of further violence and harm to themselves or others rather than treat any underlying mental illness. If an intramuscular (IM) antipsychotic or benzodiazepine is prescribed as an alternative route of administration where an individual is refusing the oral drug but they are otherwise not acutely disturbed then this is NOT rapid tranquillisation.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 1 of 34
Rapid Tranquillisation
Protocol for the prescribing and administration of injectable drugs for rapid tranquillisation (RT), physical health
assessment and monitoring, including prescribing guidelines on the drugs to be used for RT
Clinical Protocol CP11
Protocol Summary
Rapid Tranquillisation (RT) with injectable medication refers to the appropriate use of medication to manage violent behaviour safely and effectively. The aim of the intervention is an emergency measure to quickly calm a person down and reduce the risk of further violence and harm to themselves or others rather than treat any underlying mental illness. If an intramuscular (IM) antipsychotic or benzodiazepine is prescribed as an alternative route of administration where an individual is refusing the oral drug but they are otherwise not acutely disturbed then this is NOT rapid tranquillisation.

CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 2 of 34
Contents
Page
1. Introduction 4 2. Treatment Aims 4
3. Principle Considerations 4
4. Risks Associated with Rapid Tranquillisation 5
5. Circumstances where Special Caution is Required 5
6. Prescribing Rapid Tranquillisation 6
7. Administration of Rapid Tranquillisation 17
8. Post Incident review and Monitoring after Rapid Tranquillisation 19
Appendix 1 - Rapid Tranquillisation Administration Protocol 20
Appendix 2a - Rapid Tranquillisation Prescription and Administration Chart 21
Appendix 2b - Rapid Tranquillisation Monitoring Sheet 22
Appendix 3 - Management of Problems Occurring during Rapid Tranquillisation 23
Appendix 4 - How to use Flumazenil
Appendix 5 - Rapid Tranquillisation C36/CP11 – NICE Position Statement
References 30 Acknowledgements 31

CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 3 of 34
Document Control
Version Date Issued Author / Job Title / Email
1.0 Sept 2010 Samantha Churchward
Forensic services pharmacist
[email protected] 2.0 May 2012
3.0 October 2014
4.0 October 2015
5.0 March 2017
6.0 July 2017 James Lee, Clinical Pharmacist, [email protected]
7.0 October 2017 James Lee, Clinical Pharmacist, [email protected]
8.0 October 2018 Samantha Churchward, Forensic services pharmacist
9.0 September 2019 Samantha Churchward, Deputy Chief Pharmacist, Medicines Safety and Governance, [email protected]
10.0 December 2019 Emily Riddiford, Clinical Pharmacist
11.0 July 2020 Emily Riddiford, Clinical Pharmacist
12.0 July 2021 Samantha Churchward, Deputy Chief Pharmacist [email protected]
Thea Bull, Meds Opt Nurse Practitioner [email protected]
Target audience/ staff groups: Clinical staff: staff responsible for the prescribing, administration and monitoring of rapid tranquillisation therapy
Ratifying Group: Drug & Therapeutic Committee
Date ratified: July 2021
Implementation date: July 2021
Review date: July 2024

CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 4 of 34
Document History Version Start
date End date
Author History
1.0 Sep 10 SC New Protocol (incorporating C36 Rapid Tranquillisation Policy)
1.1 Mar 12 SC Amendments made to section 7. Changes made to appendices. New statement added to section 2.5.
1.2 May12 SC Updated following feedback from the Drugs and Therapeutics Committee.
2.0 May12 KS Version ratified.
2.0 Oct 13 KS Removed QT interval list (was appendix 3) and replaced with link to new QT doc.
2.0 Mar-14 KS Agreed to extend this guideline to November 2014. An audit is being completed in this area and a review later in the year will coincide with the results for this audit being available.
2.0 Jul14 SC/KS Maximum haloperidol dose changed from 18mg to 12mg.
2.1 Sep14 SC Protocol reviewed by the Safe and Therapeutic Management of Violence and Aggression Group – no changes made as evidence base is still current. Flumazenil Flow Chart added to appendix 4
3.0 Oct14 KS Document ratified at October DTC and signed off.
3.0 Jun15 SC/KS RT Chart updated to prompt physical health monitoring and highlight that a new prescription is required for each episode.
3.1 Sept 15 Oct 15 SC Protocol reviewed in light of the updated NICE guidelines NG10“Violence and aggression: short-term management in mental health, health and community settings” published in May 2015. Requirement for clinical review prior to giving a further dose added. Guidelines updated in line with NICE to include the combined use of Promethazine with Haloperidol.
3.2 Oct15 Oct15 LO Amendments made to appendix 1 , amendments made to appendix 2.b awaiting confirmation of approval from SC
3.3 Oct15 Oct15 LO Amendment made to appendix
4.0 Oct 15 JBS Document ratified at October DTC and signed off
4.1 Sep 16 SC Section 7.2 ammended
4.2 Mar 17 SC Section 6, 8 and appendix 2 changed to reference new form on CareNotes, plus physical monitoring form removed and replaced with observation table on the reverse of the form.
5.0 Mar 17 JBS Ratified by DTC and signed off
5.1 July 17 Aug 17 SC Treatment guidelines amended to remove 1st, 2nd, 3rd line and include notes on each choice. Table 2 amended to reflect relative risks.
6.0 Aug 17 JBS Ratified at July DTC and signed off
6.1 Sept 17 JL Updated NICE pregnancy advice and update addition info to include perinatal advice.
7.0 Oct 17 JBS Ratified at October DTC and signed off
7.1 Sep 18 SC Haloperidol doses updated in line with BNF changes from maximum 12mg to 20mg.
8.0 Oct 18 JBS Ratified at October DTC and signed off
8.1 Sept 19 Sept 19 SC Definition of Chemical Restraint added to p6 section 3 Principal considerations. How to RMS section added to p23 section 8.10
9.0 Sep 19 JBS Ratified at DTC and signed off
9.1 Nov 19 ER Clarified 1 hour gap between IM lorazepam and IM olanzapine as per discussion with SC.
10.0 Dec 19 JBS Ratified at DTC and signed off
10.1 Jul 20 ER Statement relating not prescribing dose ranges added to 6.1 as per MOGG and table 1 on page 12.
11.0 Jul 20 JBS Ratified at DTC and signed off
11.1 Jul 21 SC/TB Updated to include Nursing Associates
12.0 Jul 21 JBS Ratified at MSC and signed off

CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 5 of 34
1. Introduction
This protocol and accompanying notes must be read in conjunction with the ‘Policy for Rapid Tranquillisation with injectable drugs on Devon Partnership Trust Inpatient Units (C36)’, to support the safe and appropriate use of medication for Rapid Tranquillisation (RT).
The protocol should be followed where RT is considered a suitable clinical intervention,
although it is recognised that rigid adherence may not always be appropriate. If it is necessary to prescribe treatment outside these guidelines then this must first be discussed with “an appropriately experienced doctor” and the rationale for this must be clearly recorded in the clinical notes.
“An appropriately experienced doctor” is defined as a doctor who is in possession of
MRCPsych or appointment as Consultant, Associate Specialist or ST4-6 doctor within the Trust.
If an intramuscular (IM) antipsychotic or benzodiazepine is prescribed as an alternative
route of administration where an individual is refusing the oral drug but they are otherwise not acutely disturbed then this is NOT rapid tranquillisation. The drug in this case should be prescribed on the PRN section of the main drug chart and clearly marked that it is not to be used as part of rapid tranquillisation – there is no need for it to be prescribed on the RT chart or for a Incident report to be completed. It should be noted that for many drugs this would be an unlicensed indication. If there is any doubt whether the prescription falls within the criteria of rapid tranquillisation then it must be treated as rapid tranquillisation and this protocol followed fully.
2. Treatment Aims
The aim of the intervention is an emergency measure to quickly calm a person down and reduce the risk of further violence and harm to themselves or others rather than treat any underlying mental illness The objective is not to induce sleep or unconsciousness, but to promote a calmer state where the individual is still able to participate in further assessment and/ or treatment.
3. Principal Considerations
3.1 Rapid tranquillisation is only one management strategy in the control of
disturbed/violent behaviour. Non-drug approaches should be continued throughout rapid tranquillisation. RT should never be used as first line management for aggressive/violent behaviour.
3.2 All medication used in rapid tranquillisation must be given time to work before further
medication is administered. A minimum of 1 hour is recommended. Longer intervals are needed for IM olanzapine and Aripiprazole (2 hours).
3.3 Intravenous (IV) administration is likely to be extremely hazardous. It cannot be safely
administered within the Trust and therefore should not be used. 3.4 Violent behaviour can usually be controlled and managed without the need to use high
doses or ‘cocktails’ of medication. The aim of RT is to use the lowest effective dose to promote calmness and reduce the risk of further violence. It is recognised that it is

CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 6 of 34
sometimes necessary to exceed the BNF maximum recommended doses, and in situations where this is likely to occur the consultant or duty consultant must be contacted. The Trust protocol on High Dose Antipsychotics (CP10) should be followed.
3.5 Rapid Tranquillisation is defined as “chemical restraint” in guidance issued by the
Mental Health Services Data Set. Chemical restraint refers to: ‘the use of medication which is prescribed, and administered (whether orally or by injection) for the purpose of controlling or subduing disturbed/violent behaviour, where it is not prescribed for the treatment of a formally identified physical or mental illness’. Chemical restraint is a form of restrictive intervention and is required to be incident reported to the national Mental Health Services Data Set see section 8.10 p23.
4. Risks associated with Rapid Tranquillisation
There are specific risks associated with the different classes of medications and when
combinations are used the risks are compounded. Risks include:
Excessive sedation
Loss of consciousness
Respiratory depression or arrest
Cardiovascular complications and collapse
Seizures
Akathisia, dystonias and dyskinesias
Neuroleptic malignant syndrome
5. Circumstances where special caution is required
5.1 Separate Treatment Guidelines have been developed for physically frail adults and those with dementia. Physically frail adults are defined as older adults, those with a co-morbid medical condition or those who are underweight.
5.2 General considerations for those who are physically frail:
‘Start low & go slow’ with respect to doses of medication prescribed
Absorption and onset of action may be delayed- this must be taken into consideration before administering further doses if initial response to treatment poor
Older people may have a larger volume of distribution, leading to longer duration of action and possible accumulation of medication, therefore increasing risk and duration of adverse effects experienced.
5.3 General considerations for those with dementia:
The use of antipsychotics in people with a diagnosis of dementia is associated with an increased risk of cerebrovascular adverse events and an increased risk of all-cause mortality. For individuals with an organic illness (know or suspected Alzheimer’s dementia, lewy-body dementia ), the use of antipsychotics should generally be avoided, and should only be considered (by or on the recommendation of a consultant psychiatrist) where treatment with benzodiazepines alone have been ineffective and where risks associated with RT are considered less than no treatment.

CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 7 of 34
5.4 Concurrent physical illness and/ or conditions known to alter drug metabolism:
renal or hepatic impairment
organic disorder/ delirium
alcohol or drug intoxication Consult the current edition of the BNF and / Summary of Product Characteristics for
the product to obtain further information. 5.5 Extreme care is needed in the following circumstances:
congenital prolonged QTc syndromes present
concurrent prescription or use of other medication that lengthens QTc intervals both directly and indirectly (click here). Many psychotropic drugs affect the QTc interval, including antipsychotics, tricyclic antidepressants and lithium. This risk may be increased by the co-administration of other drugs also known to affect the QTc interval e.g. anti-arrhythmics, anti-histamines
the presence of disorders affecting metabolism e.g. hypo and hyperthermia, stress and extreme emotions and extreme physical exertion
5.6 Pregnancy: Rapid tranquillisation should be avoided if possible during pregnancy
where possible. NICE recommend pregnant woman requiring rapid tranquillisation should be treated according to the standard clinical guidelines on the short term management of violence and aggression (Antenatal and postnatal mental health CG192). NICE also recommend that:
individuals should not be secluded after rapid tranquillisation
restraint procedures should be adapted to avoid possible harm to the fetus
when choosing an agent for rapid tranquillisation in a pregnant woman, an antipsychotic or a benzodiazepine with a short half-life should be considered; if an antipsychotic is used, it should be at the minimum effective dose because of neonatal extrapyramidal symptoms; if a benzodiazepine is used, the risks of floppy baby syndrome should be taken into account (see Table 1 for more info)
during the perinatal period, the woman’s care should be managed in close collaboration with a paediatrician, an anaesthetist and obstetrician
6 Prescribing Rapid Tranquillisation
6.1 Medication for RT must be prescribed on form CP11a ‘Rapid Tranquillisation
Prescription and Administration chart’ (see Appendix 2a) AND must be cross referenced on the main ‘Inpatient Prescription and Administration Chart’ in the ‘As required prescriptions’ section, i.e.
Each new episode of rapid tranquillisation requires a new Rapid Tranquillisation

CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 8 of 34
Prescription and Administration chart. An episode is defined as the time from which RT is administered until the situation has resolved and the individual requires no further intervention at that time. If the individual at a later date requires further administration of RT then this constitutes another discrete episode of RT and a new RT chart is required. A medical review should take place prior to prescribing RT for a second episode. Only ONE RT chart may be written up for any individual at a time. The reason for prescribing any medication for an acutely disturbed individual must be documented in the individuals’ notes in the Rapid Tranquillisation form on the medication tab on CareNotes. Dose ranges are not appropriate for rapid tranquilisation. A single dose should be prescribed in accordance with the treatment guidelines in this document, taking into account the individual’s frailty and co-morbidities.
6.2 Situations under which a Prescription for RT may be written
Planned in anticipation of the individual requiring RT during their admission. This is the preferred way for RT to be prescribed allowing a full consideration of past response to RT and physical health assessment to be completed. The prescription of RT should be kept under regular review and if the individual is no longer likely to require RT then the prescription should be stopped.
Urgent where RT is required immediately. If an individual deteriorates suddenly or
has just been admitted a prescription may be required urgently. It is acknowledged that in this situation a full assessment may not be practical. However all available information should be considered prior to prescribing RT and any contraindications noted. The discretion of the prescribing doctor should be used to determine the safety of prescribing RT in light of the available information.
6.3 Assessment prior to prescribing RT
1. A physical examination should be conducted wherever possible, with particular reference to:
Parkinson’s Disease, Lewy body dementia, organic syndromes and acute confusional states
General condition and weight
Falls
State of hydration
Infection
Evidence of pre-existing cardiac or pulmonary conditions
Pregnancy
Baseline pulse, blood pressure, temperature and respiratory rate
Head injuries and seizures
Note any illicit drug intoxication, especially alcohol or benzodiazepines, and urine drug screen results where available; the risk of RT may be compounded in people who have recently abused illicit drugs or alcohol
Baseline electrolytes and ECG where recent test results available. ECG monitoring is advisable and wherever possible a baseline ECG should be done
2. Review the notes with regard to person’s medical and medication history
including:
Allergies/ sensitivities/ severity of EPSEs

CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 9 of 34
Review medication currently prescribed taking note of doses of antipsychotic and benzodiazepines received over the past 48 hours (including the administration of prn medication)
The benefits and adverse effects of previous medication, and previous history of severe extra-pyramidal side effects
Previous response to medication or RT and/or other methods of managing imminent violence
3. Authority under which RT is to be given/Advance directives
What legal authority is RT being given under? Consideration of the mental capacity act/mental health act must be taken. Further guidance on this can be found in the RT policy C36 (click here to access)
Are any advance directives available?
6.4 Choice of Medication
These treatment guidelines are intended to be used for the majority of people. If it is necessary to prescribe treatment not covered by these guidelines then this must first be discussed with an appropriately experienced doctor. If an advance directive has been made by the individual or a care plan covering rapid tranquillisation exists this should be considered and adhered to wherever clinically possible. The individuals’ previous response to medication should always be considered when deciding on the choice of drug or dose to use during rapid tranquillisation. There is a lack of high quality clinical trial evidence surrounding the drugs used for rapid tranquillisation and their safety. The guidelines were produced using the evidence which is available. Table 1 below gives a summary of key information for the drugs included in the treatment guidelines and table 2 outlines some of the alternative treatment options which may be considered by “an appropriately experienced doctor”. Please refer to the BNF and product data sheet for more detailed prescribing and administration advice.
CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 10 of 34
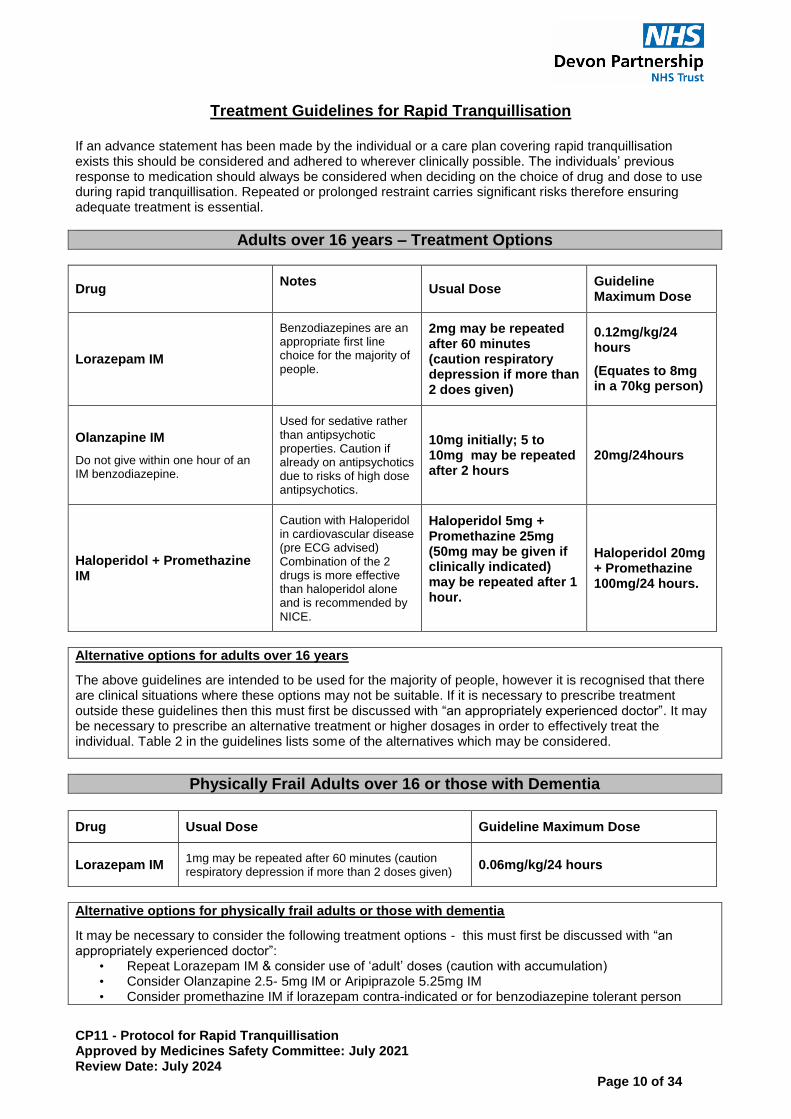
Treatment Guidelines for Rapid Tranquillisation
If an advance statement has been made by the individual or a care plan covering rapid tranquillisation exists this should be considered and adhered to wherever clinically possible. The individuals’ previous response to medication should always be considered when deciding on the choice of drug and dose to use during rapid tranquillisation. Repeated or prolonged restraint carries significant risks therefore ensuring adequate treatment is essential.
Adults over 16 years – Treatment Options
Drug Notes
Usual Dose Guideline Maximum Dose
Lorazepam IM
Benzodiazepines are an appropriate first line choice for the majority of people.
2mg may be repeated after 60 minutes (caution respiratory depression if more than 2 does given)
0.12mg/kg/24 hours
(Equates to 8mg in a 70kg person)
Olanzapine IM
Do not give within one hour of an IM benzodiazepine.
Used for sedative rather than antipsychotic properties. Caution if already on antipsychotics due to risks of high dose antipsychotics.
10mg initially; 5 to 10mg may be repeated after 2 hours
20mg/24hours
Haloperidol + Promethazine IM
Caution with Haloperidol in cardiovascular disease (pre ECG advised) Combination of the 2 drugs is more effective than haloperidol alone and is recommended by NICE.
Haloperidol 5mg + Promethazine 25mg (50mg may be given if clinically indicated) may be repeated after 1 hour.
Haloperidol 20mg + Promethazine 100mg/24 hours.
Alternative options for adults over 16 years
The above guidelines are intended to be used for the majority of people, however it is recognised that there are clinical situations where these options may not be suitable. If it is necessary to prescribe treatment outside these guidelines then this must first be discussed with “an appropriately experienced doctor”. It may be necessary to prescribe an alternative treatment or higher dosages in order to effectively treat the individual. Table 2 in the guidelines lists some of the alternatives which may be considered.
Physically Frail Adults over 16 or those with Dementia
Drug Usual Dose Guideline Maximum Dose
Lorazepam IM 1mg may be repeated after 60 minutes (caution respiratory depression if more than 2 doses given)
0.06mg/kg/24 hours
Alternative options for physically frail adults or those with dementia
It may be necessary to consider the following treatment options - this must first be discussed with “an appropriately experienced doctor”:
• Repeat Lorazepam IM & consider use of ‘adult’ doses (caution with accumulation) • Consider Olanzapine 2.5- 5mg IM or Aripiprazole 5.25mg IM • Consider promethazine IM if lorazepam contra-indicated or for benzodiazepine tolerant person

CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 11 of 34
Treatment Guidelines for Rapid Tranquillisation ONLY FOR USE WHEN LORAZEPAM IS UNAVAILABLE
If an advance statement has been made by the individual or a care plan covering RTexists this should be considered and adhered to wherever clinically possible. The individuals’ previous response to medication should always be considered when deciding on the choice of drug and dose to use during RT. Repeated or prolonged restraint carries significant risks, therefore ensuring adequate treatment is essential. CAUTION RESPIRATORY DEPRESSION: Midazolam is associated with a higher risk of respiratory depression than lorazepam. Given the risks a doctor must attend if a second dose of midazolam is required and stay on the ward for an hour after the second dose is given on a unit not co-located with a hospital with an A&E department, advance prescriptions for midazolam must be limited to one dose only before calling a doctor.
Adults over 16 years – Treatment Options
Drug Notes
Usual Dose Guideline Maximum Dose
Olanzapine IM
Do not give within one hour of an IM benzodiazepine.
Used for sedative rather than antipsychotic properties. Caution if already on antipsychotics due to risks of high dose antipsychotics.
10mg initially; 5 to 10mg may be repeated after 2 hours
20mg/24hours
Haloperidol + Promethazine IM
Caution with Haloperidol in cardiovascular disease (pre ECG advised) Combination of the 2 drugs is more effective than haloperidol alone and is recommended by NICE.
Haloperidol 5mg + Promethazine 25mg (50mg may be given if clinically indicated) may be repeated after 1 hour.
Haloperidol 20mg + Promethazine 100mg/24 hours.
Midazolam IM
2nd Line choice only when Lorazepam is unavailable.
5mg may be repeated after 1 hour (see respiratory depression caution above)
15mg/24 hours
Alternative options for adults over 16years The above guidelines are intended to be used for the majority of people, however it is recognised that there are clinical situations where these options may not be suitable. If it is necessary to prescribe treatment outside these guidelines then this must first be discussed with a doctor who is “an appropriately experienced doctor” It may be necessary to prescribe an alternative treatment or higher dosages in order to effectively treat the individual. Table 2 in the guidelines lists some of the alternatives which may be considered.
Physically Frail Adults over 16 or those with Dementia
Drug Usual Dose Guideline Maximum Dose
Midazolam IM 2.5mg may be repeated after 60 minutes 7.5mg/24 hours
Alternative options for Physically frail adults or those with dementia:
It may be necessary to consider the following treatment options - this must first be discussed with “an appropriately experienced doctor”:
• Repeat Midazolam IM & consider use of ‘adult’ doses (Caution with accumulation) • Consider Olanzapine 2.5- 5mg IM or Aripiprazole 5.25mg IM • Consider promethazine IM if lorazepam contra-indicated or for benzodiazepine tolerant person

CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 12 of 34
Table 1 - Key Drug Information for Drugs included in the RT Treatment Guidelines Please note that the dose ranges in these tables are only to illustrate the various doses available for use. When prescribing, do not use dose ranges. A single dose should be prescribed in accordance with the treatment guidelines in this document, taking into account the individual’s frailty and co-morbidities.
Drug Place in Treatment Administration Cautions and Additional Comments
IM Lorazepam Benzodiazepines are relatively safe and their effects can be reversed with the antagonist flumazenil.
Dose 1-2mg up to 120mcg/kg/24hrs Lorazepam injection (stored in the fridge) should be diluted 1:1 with Water for Injection immediately before IM use.
Risks with benzodiazepines include loss of consciousness and respiratory depression or arrest. Flumazenil injection (short acting benzodiazepine antagonist) must be available for benzodiazepine-induced respiratory depression. The pharmacokinetics of lorazepam are the same whether given orally or IM. The only reason to give IM lorazepam is if the person refuses oral. Concern is sometimes expressed about the possibility of disinhibition following the administration of benzodiazepines. There is conflicting evidence available about this. It is, however, a rare side effect. Disinhibition maybe more likely to occur in those with organic brain disease, including learning disabilities, the under 18s and the over 65s, and perhaps those with impulse control problems. Perinatal advice: Greatest risk with use is during first and third trimesters. Use in the first trimester may increase malformation risk in the unborn child and use during third trimester can lead to ‘floppy infant syndrome’ and neonatal withdrawal. General principles would favour shorter-acting preparations (such as lorazepam) and for exposure to be minimised by using the lowest effective dose for as short a time as necessary.
IM Olanzapine Where benzodiazepines are not considered to be appropriate, such as for individuals who are tolerant to benzodiazepines or where benzodiazepines have been ineffective in the past. It should be noted that antipsychotics used during
Dose: 5-10mg (usual dose 10mg) followed by 5-10mg after 2 hours if necessary up to 20mg in 24 hours (maximum combined oral and IM) Maximum 3 injections in
IM olanzapine has been shown in a number of studies to be at least as effective, and overall more effective than IM haloperidol with significantly less extrapyramidal side effects or risk of QT prolongation and may have a faster onset of action. If the person is considered to need IM benzodiazepine treatment, this should not be given until at least one hour after IM olanzapine

CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 13 of 34
Drug Place in Treatment Administration Cautions and Additional Comments
rapid tranquillisation are used for their sedative rather than antipsychotic properties.
24 hours for 3 days
administration. If the person has received IM benzodiazepine, IM olanzapine administration should only be considered after careful evaluation of clinical status, and the person should be closely monitored for excessive sedation and cardiorespiratory depression. IM olanzapine may produce a 5-fold increase in plasma concentration compared to the same dose given by the oral route. Olanzapine IM is a black triangle drug▼: Please report ALL adverse reactions observed using the Yellow card system or the MHRA website. Perinatal advice: If an atypical is preferred in a patient with a known predisposition to extra-pyramidal side-effects, or if there is previous evidence of treatment response to either olanzapine or risperidone, these may be suitable options instead. If an IM atypical is required, aripiprazole may be considered. Olanzapine may increase the risk of hyperglycaemia and fetal growth, although evidence for this is conflicting. Use of antipsychotics in pregnancy has been associated with neonatal withdrawal and EPSEs.
IM Haloperidol+ promethazine.
It is recommended that this is not used unless a pre-treatment ECG is available and the person has had a previous history of a good response to haloperidol and has tolerated it well. There may however be situations where other treatment options have failed and based on an assessment of the risks/benefits to the individual haloperidol IM is given despite these recommendations not being met – the reason for proceeding with haloperidol in these circumstances should be clearly
Dose: Haloperidol 5mg up to a maximum of 20mg in 24 hours. Promethazine 25 -50mg up to a maximum of 100mg/24 hours.
IM haloperidol is no longer recommended first line for rapid tranquillisation due to:
High incidence of acute dystonia
Requirement for a pre-treatment ECG Haloperidol and lorazepam IM should no longer be used routinely in combination. The data sheet for lorazepam IM states that there have been reports of apnoea, coma, bradycardia, heart arrest and death with the concomitant use of lorazepam injection solution and haloperidol. Procyclidine injection must be available. It is recommended that it is prescribed with IM haloperidol to reduce the risk of dystonia/other EPSEs. The bioavailability of IM haloperidol is 50% greater that oral haloperidol.

CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 14 of 34
Drug Place in Treatment Administration Cautions and Additional Comments
documented in the individual’s notes. NICE CG10 recommends the combination of haloperidol with promethazine – The Trust guidelines have been updated in accordance with this. When IM haloperidol is combined with IM promethazine there is some suggestion that risk of movement-related side effects may be reduced.
Prescriptions for oral and IM medication must be written separately (not PO/IM). Promethazine is contraindicated in people with central nervous system depression and those who have taken monoamine oxidase inhibitors within the past 14 days. Cautions include respiratory conditions, coronary artery disease, epilepsy and hepatic and renal insufficiency. Adverse effects include drowsiness, dizziness, restlessness, headaches, nightmares, tiredness, disorientation and anticholinergic effects. Promethazine and haloperidol must not be mixed in the same syringe but given as separate injections. Perinatal advice: Haloperidol is the antipsychotic of choice due to there being more experience of its use during pregnancy compared to the newer agents. If extra-pyramidal side-effects develop, switching to an atypical may be preferable to exposure to additional anti-muscarinic medicine. Use of antipsychotics in pregnancy has been associated with neonatal withdrawal and EPSEs.
Midazolam 2nd Line only when Lorazepam is unavailable.
In reported trials, the dose used has ranged from 2.5mg to 15mg, although it must be noted that the higher doses appear to induce sleep, whereas the aim of rapid tranquilisation is to promote a calmer state and not induce sleep/unconsciousness. The recommended dose in the Trust Guidelines is 5mg for adults over 16 years and 1 to 2.5mg for
Like other benzodiazepines midazolam has the potential to cause respiratory depression but this risk is thought to be greater than with lorazepam. Always ensure that emergency resuscitation equipment and medication (including flumazenil) is present before administration. Remember midazolam acts for a longer period than flumazanil - additional doses may be required. Following IM Midazolam, anterograde amnesia of short duration may occur with the individual not remembering events that occurred during the maximum activity of the compound. Midazolam is now a schedule 3 controlled drug, therefore must be ordered from the pharmacy department using the ward controlled drug requisition book in accordance with Trust standard operating procedure CD1. Once received, midazolam injection should be recorded in the controlled drugs register and stored in the controlled drugs cupboard.

CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 15 of 34
Drug Place in Treatment Administration Cautions and Additional Comments
physically frail adults. Only the 10mg/5ml strength should be stocked for rapid tranquillisation on inpatient wards:
The NPSA issued an alert on reducing risk of overdose with midazolam injection in adults. Link:http://www.nrls.npsa.nhs.uk/resources/?entryid45=59896. The strength of midazolam injection recommended in this Guidelines is classed by the NPSA as being high strength. However the volume required of the lower strength preparation to allow the doses needed for rapid tranquillisation would be too large. To minimise the risk of errors in dosing occurring only the 10mg/5ml strength should be stocked for rapid tranquillisation on inpatient wards. If in exceptional circumstances there is a clinical need for a different strength of midazolam injection to be kept on a ward then an individual risk assessment should be done and all possible steps taken to avoid any confusion between the different strengths. Please note Midazolam injection is in section 15.1.4 of the BNF rather than section 4 therefore existing T2/T3 forms will need to be updated to allow midazolam to be given instead of lorazepam.

CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 16 of 34
Table 2 - Other Treatment Options (must be discussed with “an appropriately experienced doctor” prior to prescribing)
Drug Place in Treatment Administration Cautions and Additional Comments
IM Haloperidol + IM Lorazepam
May be appropriate where an individual has responded well to this combination in the past or has failed to respond to the drugs given alone. The warning in the product data sheet regarding the potential risks of combing the 2 drugs must be taken into consideration.
See above under individual drugs for doses
See above under individual drugs for specific cautions. It has been common for combinations of benzodiazepines and antipsychotics to be used. Previous guidelines have advocated this approach. In people where antipsychotics are considered necessary this practice is thought to be beneficial because it reduces the dose of the antipsychotic that is required. It has been suggested that the two classes of drug have a synergistic action. Due to the risks of combining benzodiazepines and antipsychotics it is now recommended that this approach is avoided. The data sheet for lorazepam IM states that there have been reports of apnoea, coma, bradycardia, heart arrest and death with the concomitant use of lorazepam injection solution and haloperidol. The haloperidol warning was added following a review of adverse event reports worldwide by Wyeth Pharmaceuticals. It should be noted that the risk of this is low when considered in the context of the large number of people who have been treated with this combination. The individual should be monitored closely where this combination is given. Caution is required in the use of Haloperidol in Cardiovascular disease. It is recommended that a pre treatment ECG is done before the use of Haloperidol.
IM Aripiprazole
An alternative antipsychotic treatment option to olanzapine IM.
Dose: 5.25 -15mg (usual dose 9.75mg) followed by 5.25 -15mg after 2 hours if necessary up to 30mg in 24 hours (maximum combined oral and IM) Maximum 3 injections in 24 hours.
IM aripiprazole was licensed in the UK in 2008. It has been shown in some clinical trials to be as effective as haloperidol, but there are no head-to-head comparisons with olanzapine at present. Overall trial data suggests that it is less effective than olanzapine or haloperidol. Aripiprazole IM is a black triangle drug▼: Please report ALL adverse reactions observed using the Yellow card system or the MHRA website. Perinatal advice:

CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 17 of 34
Drug Place in Treatment Administration Cautions and Additional Comments
If an atypical is preferred in a patient with a known predisposition to extra-pyramidal side-effects, or if there is previous evidence of treatment response to either olanzapine or risperidone, these may be suitable options instead. If an IM atypical is required, aripiprazole may be considered. Use of antipsychotics in pregnancy has been associated with neonatal withdrawal and EPSEs.
IM Aripiprazole + IM Lorazepam
IM aripiprazole and IM lorazepam can be administered at the same time however the risk of orthostatic hypotension is increased.
See above under individual drugs for doses.
See above under individual drugs for specific cautions. If Aripiprazole and lorazepam are co-administered monitor blood pressure closely as the risk of orthostatic hypotension is increased.
IM Promethazine This is an antihistamine which may be used as an alternative to benzodiazepines or antipsychotics, although it has a slow onset of action.
Dose: 50mg may be repeated up to a maximum of 100mg in 24hours. Dilution is not required before IM administration.
This antihistamine has a slow onset of action, but is often an effective sedative especially when individuals are regularly prescribed or abuse benzodiazepines. Wait 1-2 hours after the injection to assess the response. Promethazine IM is NOT licensed for use in rapid tranquillisation. Perinatal advice: Studies do not suggest an association between in utero promethazine exposure and increased risks of congenital malformation, preterm delivery, low birth weight or adverse neurodevelopmental outcome. Neonatal monitoring may be necessary where antenatal exposure has occurred close to delivery due to possibility of side effects and neonatal withdrawal.

CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 18 of 34
Adjuncts to RT
Zuclopenthixol acetate (Clopixol Acuphase): Zuclopenthixol acetate is not considered as part of rapid tranquillisation due to its long onset and duration of action. However there are individual cases where its use may be considered as an adjunct to RT. See Prescribing Guideline (PG21) which contains information on the safe and appropriate use of this medicine. Please note Zuclopenthixol acetate should be prescribed on the main prescription chart NOT on an RT chart.
The following treatments are NOT recommended for rapid tranquillisation within the Trust:
1. IM/IV chlorpromazine: Chlorpromazine is particularly dangerous when administered IM. IM chlorpromazine should not be used under any circumstances.
2. IM Diazepam: Diazepam should not be administered intramuscularly due to slow and erratic absorption, leading to an unpredictable
response. 3. IV Diazepam: The IV administration of diazepam is extremely hazardous and given the lack of adequate medical support to give IV
diazepam safely within the Trust it should not be used.

CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 19 of 34
7. Administration of Rapid Tranquillisation Rapid Tranquilisation is not within the scope of practice of the Nursing Associate
7.1 Prior to administering RT consider:
Have alternative approaches to RT been considered such as verbal de-escalation? Continue to use non-drug approaches throughout rapid tranquillisation
Has oral medication been offered? If an individual will take oral medication this should be used instead of RT
Facilities for resuscitation must be available.
The following medication must be available in case of emergencies to treat complications:
o Procyclidine injection o Flumazenil injection (doctor only)
What other medication has the individual received in the past 24 hours? If they have already received benzodiazepines or antipsychotics via any route then will the administration of RT exceed the BNF maximum dose, if so than a doctor should be contacted prior to administration.
The individual’s physical state – There may be physical reasons for the individual’s distress such as infection which can be treated. If the individual is physically unwell or intoxicated it may be unsafe to administer RT therefore a doctor should be contacted prior to administration.
Consideration should be given to the risks of not proceeding with RT versus the risks of going ahead with RT.Clinical judgement is important in weighing up the decision to proceed with RT in any situations where there is a risk to the individual or others if RT isn’t given.
What legal authority is RT being given under? Consideration of the mental capacity act/mental health act must be taken. If RT is given without the appropriate legal authority then it will constitute an assault on the individual and legal action may be taken against the person administering the drug. Always check that you have the legal authority to administer the drug, if in doubt contact “an appropriately experienced doctor” prior to administering RT. Further guidance on this can be found in the RT policy C36
The Medusa website may be useful to obtain information and advice on administering injectable drugs. Click here to access (login details can be obtained by contacting the medicines optimisation team).
7.2 Administering RT
Once the decision has been made to proceed with RT, the RT administration protocol (Appendix 1) should be followed and administered as per the RT prescription. Use the rapid tranquillisation chart (Appendix 2) to record the administration and record all mandatory physical monitoring on the reverse. A record of the administration must also be made on the main drug chart in the PRN section as follows:

CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 20 of 34
Before giving further doses of rapid tranquillisation a clinical review is required to ensure the safety of proceeding. The nurse in charge should contact a member of the medical team prior to giving further doses of rapid tranquillisation. The medic must confirm that physical health monitoring/observation has been completed appropriately and that the results of this support further doses IM medication to be safely given – this does not necessitate a physical review in person but the medic must assure themselves that they have sufficient information to allow a further dose of IM medication to be given. If there are any concerns regarding the safety to precede a full medical review should be completed prior to administering further doses of IM medication. In certain situations the risk of provoking further violent behaviour/ assault by imposing physical observations will need to be balanced against the risks of not carrying out these checks. If it is not possible to carry out regular physical observations, due to the person’s level of disturbance, then 15 minute visual observations should be maintained and recorded, until physical observations become possible and a decision to proceed made on the basis of this.
CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 21 of 34
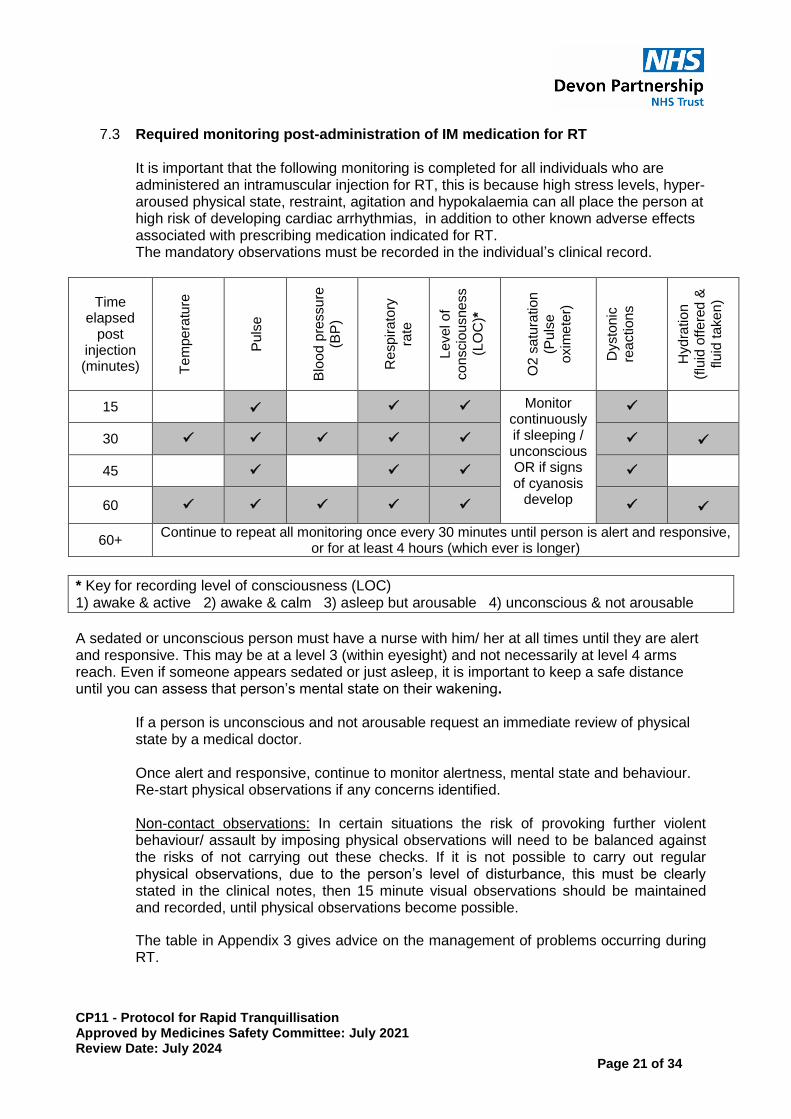
7.3 Required monitoring post-administration of IM medication for RT
It is important that the following monitoring is completed for all individuals who are administered an intramuscular injection for RT, this is because high stress levels, hyper-aroused physical state, restraint, agitation and hypokalaemia can all place the person at high risk of developing cardiac arrhythmias, in addition to other known adverse effects associated with prescribing medication indicated for RT. The mandatory observations must be recorded in the individual’s clinical record.
Time elapsed
post injection (minutes)
Te
mpe
ratu
re
Puls
e
B
loo
d p
ressu
re
(BP
)
R
esp
ira
tory
ra
te
Le
vel o
f co
nscio
usne
ss
(LO
C)*
O2
sa
tura
tion
(Pu
lse
o
xim
ete
r)
Dysto
nic
rea
ction
s
Hyd
ratio
n
(flu
id o
ffe
red
&
flu
id ta
ke
n)
15 Monitor continuously if sleeping / unconscious OR if signs of cyanosis
develop
30
45
60
60+ Continue to repeat all monitoring once every 30 minutes until person is alert and responsive,
or for at least 4 hours (which ever is longer)
* Key for recording level of consciousness (LOC) 1) awake & active 2) awake & calm 3) asleep but arousable 4) unconscious & not arousable
A sedated or unconscious person must have a nurse with him/ her at all times until they are alert and responsive. This may be at a level 3 (within eyesight) and not necessarily at level 4 arms reach. Even if someone appears sedated or just asleep, it is important to keep a safe distance until you can assess that person’s mental state on their wakening.
If a person is unconscious and not arousable request an immediate review of physical state by a medical doctor. Once alert and responsive, continue to monitor alertness, mental state and behaviour. Re-start physical observations if any concerns identified. Non-contact observations: In certain situations the risk of provoking further violent behaviour/ assault by imposing physical observations will need to be balanced against the risks of not carrying out these checks. If it is not possible to carry out regular physical observations, due to the person’s level of disturbance, this must be clearly stated in the clinical notes, then 15 minute visual observations should be maintained and recorded, until physical observations become possible.
The table in Appendix 3 gives advice on the management of problems occurring during RT.

CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 22 of 34
8. Post RT Debrief and Monitoring Required after Rapid Tranquillisation
8.1 An incident report must be completed for the RT episode. The Incident number must be recorded on the top of the completed RT prescription chart and this scanned onto Electronic Record System. See below 8.10 for how to record on RMS.
8.2 Once the episode has finished at the earliest opportunity a documented discussion of
the RT episode by the clinical team should take place including response to treatment and side effects, so that this can inform future treatment. This should involve the individual (and parents/ guardians/ carers) where possible. The discussion should be documented on the Rapid Tranquillisation form in the medication tab of CareNotes.
Care plans should be updated to reflect future plans for RT in light of response to current episode.
8.3 The individual should be reviewed by a doctor at the earliest opportunity, but within 24
hours of receiving RT. A new RT prescription chart should be written up if required and appropriate for the individual – this should be done taking into account their response to RT and side effects experienced. A new Rapid Tranquillisation form must be created on CareNotes in the medication tab –information on the debrief and outcomes will be pulled forward into the new form.
8.4 Regularly prescribed medication should be reviewed: start, restart or change medication
where clinically indicated. Review any ‘when required’ medication. A new RT prescription should be completed if clinically appropriate.
8.5 Consider conducting an ECG following the administration of antipsychotics if the
following apply:
high doses are used,
when used in combination with any other medication known to prolong the QTc interval (click here)
if the baseline ECG is abnormal or a baseline ECG wasn’t available
if there is any clinical indication to repeat the ECG. 8.6 Monitor electrolytes if not checked in the last 3-4 days. 8.7 Following any intervention for the acute management of disturbed behaviour, the
individual involved must be given the opportunity to talk to a member of staff about the incident. Every effort must be made to establish whether the individual understands why this happened. This must be documented in the individual’s notes on the Rapid Tranquillisation form in the medication tab.
8.8 The individual must be offered the opportunity to write an account of their experience
which should be uploaded onto the Electronic Record System. The individual may wish to dictate this to a member of staff to document if they are unable or unhappy to write it themselves. This is optional, but should be encouraged.
8.9 Any post incident learning and or follow up actions should be captured within ‘actions’ function of RMS and followed up via that route.

CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 23 of 34
8.10 How to Record on RMS The use of chemical restraint must be recorded as on RMS. This is done in the following way (see also screenshots)
1. Enter the details of the incident on the first page.
2. On the second page select the following in response to the questions.
3. Was Restraint/chemical restraint/segregation or seclusion used? Answer YES
4. Add Intervention? List All Used Select from the list: SELECT “Rapid
Tranquillisation IM”

CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 24 of 34
Appendix 1 RAPID TRANQUILLISATION ADMINISTRATION PROTOCOL
Check medication administered in previous 24 hours to ensure BNF limits not exceeded without advice from an appropriately
experienced doctor. Consider and appropriately treat other medical conditions such as acute infection, intoxication, delirium,
discomfort, pain, side effects from other medication (e.g. akathisia). Consider past response to Rapid Tranquillisation (RT).
Is oral medication
unsuccessful?
OR
Is medication refused?
OR
Is there a serious risk to person
from restraint?
Consider
alternative
intervention(s)
before proceeding
to RT
Complete ‘Before Administration’ section of prescription chart
Administer IM medication according to prescription chart
(see treatment guidelines for specific information, where 2
drugs are being given together they should not be mixed in the
same syringe).
Monitor for response and adverse side effects.
Nursing and medical team to review.
After a period of at least 60 minutes, is response to treatment
positive?
Repeat dose (A member of the
medical team must verbally confirm
that it is safe to give a further dose of
IM medication based on clinical
safety. - Olanzapine may only be
repeated after 2 hours).
Consider giving an alternative
medication (A member of the
medical team must verbally confirm
that it is safe to give a further dose of
IM medication based on clinical
safety).
Monitor for response and adverse side effects.
Nursing and medical team to review.
After a period of at least 60 minutes, is response to treatment
positive?
Have 3 separate doses of IM medication been administered?
AND / OR
Has maximum BNF recommended daily dose of medication(s)
been reached / exceeded?
Seek urgent advice from a doctor
who is a member of the Royal College of
Psychiatrists who may consider specialist
treatment options.
Contact a Medicines Management Pharmacist to
discuss treatment options where required.
Complete a Incident Report.
Plan for the 24 hours after
successful RT
Review physical health status and
continue physical monitoring.
Doctor to review person within
24hr and write new RT chart if
appropriate
Complete a Incident Report.
CO
NT
INU
E T
O U
SE
NO
N-D
RU
G A
PP
RO
AC
HE
S T
HR
OU
GH
OU
T T
HE
INC
IDE
NT
YES
NO
PARTIAL RESPONSE NO RESPONSE
NO
YES
YES
What is the type
of response?
NO
NO
YES
Required monitoring post-administration of IM medication for Rapid Tranquillisation
Time elapsed post injection
Temp Pulse Blood pressure
Resp. Rate
Level of consciousness
O2 saturation (Pulse oximeter)
Dystonic reactions
Hydration (fluid offered & taken)
15 mins Monitor continuously if
sleeping/ unconscious OR
if signs of cyanosis develop
30 mins
45 mins
60 mins
60 mins + Continue to repeat all monitoring once every 30 minutes until person is alert and responsive, or for at least 4 hours (which
ever is longer)
A sedated or unconscious person must have a nurse with him / her at all times until they are alert and responsive.

CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 25 of 34
Appendix 2a Rapid Tranquillisation Prescription and Administration Chart
A new chart must be written for each separate episode of rapid tranquillisation Prescriber must complete a rapid tranquillisation rationale form on CareNotes [Tick]
SURNAME: FIRST NAME:
NHS No. WARD DOB CONSULTANT
Physical health risk factors?
Allergies/sensitivities?
Must be completed before administering: (by nursing staff)
Other antipsychotics or benzodiazepines received in past 24 hrs? Please specify
Has oral medication been offered? Yes/No
Authority under which RT is being given? (e.g. Mental Capacity act, Mental Health Act: 3 month rule, T3,or section 62)
Prescription (for ONE episode of rapid tranquillisation ONLY)
Drug name: Route: IM
Dose: Min. Dose Interval:
Max dose in 24 hrs:
Additional instructions: (refer to guidelines)
Prescriber’s signature:
Date:
Prescriber’s name and contact number:
Pharmacy: Form completed on CareNotes Tick
Administration record:
Date Time Dose Given by
Prior to 2nd Dose: Has a member of the medical team confirmed that a further dose may be safely given? [Tick]
Drug name: Route: IM
Dose: Min. Dose Interval: Max dose in 24 hrs:
Additional instructions: (refer to guidelines)
Prescriber’s signature:
Date:
Prescriber’s name and contact number:
Pharmacy:
Administration record:
Date Time Dose Given by
Prior to 2nd Dose: Has a member of the medical team confirmed that a further dose may be safely given? [Tick]
Ensure physical health monitoring is completed as per the table on the reverse
Debrief /outcome of episode must be completed on CareNotes Rapid Tranquillisation form
THIS FORM IS INCLUDED IN THIS CLINICAL PROTOCOL FOR INFORMATION ONLY
TO OBTAIN A COPY OF THIS FORM, PLEASE
DOWNLOAD CP11a FROM THE MEDICINES
MANAGEMENT SECTION OF THE DEVON PARTNERSHIP TRUST INTRANET
CLICK HERE TO ACCESS

CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 26 of 34
Appendix 2b
Rapid Tranquillisation Physical Health Monitoring:
Time
elapsed post
injection (minutes)
Te
mpe
ratu
re
Puls
e
B
loo
d p
ressu
re
(BP
)
R
esp
ira
tory
ra
te
Le
vel o
f co
nscio
usne
ss
(LO
C)*
O2
sa
tura
tion
(Pu
lse
o
xim
ete
r)
Dysto
nic
rea
ction
s
Hyd
ratio
n
(flu
id o
ffe
red
&
flu
id ta
ke
n)
15 Monitor continuously if sleeping / unconscious OR if signs of cyanosis
develop
30
45
60
60+ Continue to repeat all monitoring once every 30 minutes until person is alert and responsive,
or for at least 4 hours (whichever is longer)
* Key for recording level of consciousness (LOC) 1) awake & active 2) awake & calm 3) asleep but arousable 4) unconscious & not arousable
Physical health monitoring has been recorded as part of the clinical records on the appropriate monitoring form. Tick Please document where physical monitoring has been recorded If it is NOT possible to safely monitor physical health following rapid tranquillisation due to the level of disturbance, confirm that the person is alert and responsive. (Non-contact Observations) Tick 15 minute visual observations must be maintained and recorded, until physical observations become possible.

CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 27 of 34
Appendix 3
Management of Problems Occurring During Rapid Tranquillisation
Problem Remedial Measures
Acute dystonias (including oculogyric crisis) and parkinsonism (see also below)
Procyclidine 5 – 10 mg IM (repeat after 20 minutes if necessary) or IV (repeat after 10 minutes if necessary) Older adults: 2.5 – 5mg
Increased temperature or marked muscular rigidity (risk of Neuroleptic Malignant Syndrome and perhaps arrhythmias)
Withhold antipsychotics
Monitor closely - send bloods for CPK level
Cool the person
Seek urgent medical advice immediately AND refer to ITU if continued or any other signs of NMS, such as sweating, hypertension or fluctuating BP, tachycardia, incontinence/retention/obstruction, muscular rigidity (may be confined to head and neck) or confusion, agitation/altered consciousness.
Respiratory depression:
respiratory rate <10/minute after lorazepam or if oxygen saturation <90%)
Oxygen and flumazenil (a benzodiazepine antagonist) may be given if benzodiazepine-induced respiratory depression. Flumazenil may only be administered by a DOCTOR only who, in their professional opinion are competent to use it safely. There is no expectation for other medical staff of any grade or any other clinician to use it. There are risks associated with the use of flumazenil it should only be used in life threatening situations. See flow chart below in Appendix 4 for how to give Flumazanil. If induced by other agent, person will require mechanical ventilation – arrange transfer to an ITU immediately.
Irregular/slow (<50/min) pulse Monitor closely and refer to specialist medical care immediately
Hypotension Fall in blood pressure (Orthostatic or <50mmHg diastolic)
Lie person flat, raise legs if possible Monitor closely

CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 28 of 34
Appendix 4
How to use Flumazenil Flowchart describing the use of i/v flumazenil in the event of respiratory depression associated with benzodiazepines given as part of the Rapid Tranquillisation Protocol:
To only be administered by a DOCTOR who, in their professional opinion, are competent to use it safely. There is no expectation for other medical staff of any
grade or any other clinician to use it. There are risks associated with the use of flumazenil it should only be used in life
threatening situations.
If, after the administration of benzodiazepines, the individual appears to go into respiratory depression and respiration falls below 10 /minute:
Call the emergency services.
Give Flumazenil 200micrograms I/V over 15 seconds
If required level of consciousness is not obtained, after 60 seconds, give another Flumazenil 100micrograms I/V over 10 seconds
Repeat process until consciousness is achieved (maximum of 7 further cycles, i.e. a maximum dose of flumazenil of 1mg/24 hours)
Notes

CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 29 of 34
This is only part of the initial stage of managing respiratory depression induced by benzodiazepines. The individual must be transferred immediately to an acute medical hospital for further treatment.
A pulse oximeter should be used to gauge whether Flumazenil should be used. Consider using oxygen and bagging the individual if required.
The duration of action of flumazenil (half-life 52 minutes, duration of action 1-2 hours) is much shorter than the benzodiazepines; therefore, the respiratory function may recover and then deteriorate again.
Flumazenil may precipitate:
o a withdrawal syndrome in benzodiazepine-dependent individuals
o convulsions in epileptics
o arrhythmias in people who have taken cardiotoxic drugs.
Do NOT give flumazenil for mixed overdoses particularly combined tricyclic antidepressant and benzodiazepine overdosage as convulsions and cardiac arrest may be precipitated.
Flumazenil should be used with caution in people with a history of seizures, head injury, hepatic impairment or chronic benzodiazepine use.
The aim of this sheet is to provide basic information to facilitate the safe use of flumazenil in an emergency situation. Please refer to the products SPC for more detailed information.

CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 30 of 34
Appendix 5
Rapid Tranquillisation C36/CP11 – NICE Position Statement September 2015
Situation
The Trust rapid tranquillisation policy and clinical protocol were reviewed in light of the updated NICE guidelines NG10“Violence and aggression: short-term management in mental health, health and community settings” published in May 2015.
Background
The following areas were identified in which our current guidelines varied from the updated NICE guidelines – these questions were sent out to all consultant psychiatrists via the Medical Advisory Committee (MAC) and to senior nurses throughout the Trust:
1. Choice of Medication: The new NICE guideline does not include Olanzapine IM which is the 2nd line choice in our current guidelines - this was excluded by NICE because Olanzapine IM does not have a UK marketing authorisation (for commercial reasons) however NICE does not take into account the fact that it does have a pan European licence and therefore is licensed for use in the UK and is still readily available to import and there have been no issues with supply. This does have an effect on the cost although owing to its infrequent use this does not have a major budgetary impact overall. There is a substantial amount of evidence to support the use of IM Olanzapine in rapid tranquillisation. Olanzapine does not have the requirement which haloperidol has for a baseline ECG to be done or the same risk as haloperidol of severe extra pyramidal side effects. Should we maintain our current position of including Olanzapine IM as a treatment option in our Rapid Tranquillisation guidelines?
2. Prescribing of a single dose only: The new NICE guideline states - When prescribing medication for use in rapid tranquillisation, write the initial prescription as a single dose, and do not repeat it until the effect of the initial dose has been reviewed. Our current guidelines/prescription charts allow the prescription of repeated doses for one "episode" of rapid tranquillisation. If we were to follow the NICE guidelines this may cause delays in the prescription of a second dose causing increased suffering or risk. Should we maintain our current position of allowing repeated doses to be prescribed for an episode of rapid tranquillisation?
3. Inclusion of Promethazine: The new NICE guideline recommends that Haloperidol is given with Promethazine. Promethazine does not have a licence for use in rapid tranquillisation however is supported by a number of international studies. Should we update our guidelines in line with NICE to include the combined use of Promethazine with Haloperidol?
Assessment:
13 email responses were received from 12 consultants and 1 pharmacist. All unanimously agreed to keep Olanzapine as an option in our guidelines. 12 out of the 13 agreed that we should maintain our current position of allowing repeated doses to be prescribed for an episode of rapid tranquillisation however a number commented about the need to strengthen the requirement for a clinical review between doses. 12 out of the 13 agreed that we should update our guidelines in line with NICE to include the combined use of Promethazine with Haloperidol. The attendees of the DTC meeting in September were also unanimously in agreement with this.

CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 31 of 34
Recommendation:
1. Our current position of including Olanzapine IM second line as a treatment option in our Rapid Tranquillisation guidelines should be maintained.
2. We should maintain our current position of allowing repeated doses to be prescribed for an episode of rapid tranquillisation, however a requirement to obtain a clinical review prior to giving a further dose will be added – this will involve the nurse contacting the medic who should ensure that all physical observations have been completed and that on the basis of this it is safe to proceed with a further dose.
3. We should update our guidelines in line with NICE to include the combined use of Promethazine with
Haloperidol.
Decision:
The September 15 meeting of the Drugs and Therapeutics committee supported the recommendations above.

CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 32 of 34
References Andrezina R, Josiassen R, Marcus R et al (2006). Intramuscular aripiprazole for the treatment of acute agitation in patients with schizophrenia or schizoaffective disorder: a double-blind, placebo controlled comparison with intramuscular haloperidol. Psychopharmacology (Berl) 188(3), 281-292 Battaglia J, Moss S, Rush J et al (1997) Haloperidol, Lorazepam or Both for Psychotic Agitation? A Multicenter, Prospective, Double-Blind, Emergency Department Study. American Journal of Emergency Medicine 15 3335-40 Bazire Stephen (2009) Psychotropic Drug Directory Bieniek S, Ownby R, Penalver A et al (1998) A Double-Blind Study of Lorazepam versus the Combination of Haloperidol and Lorazepam in Managing Agitation. Pharmacotherapy 18 57-62 Currier G and Simpson G (2001)Risperidone Liquid Concentrate and Oral Lorazepam Versus Intramuscular Haloperidol and Intramuscular Lorazepam for Treatment of Psychotic Agitation. Journal of Clinical Psychiatry 62 153-157 Dickinson T et al (2009) Managing aggression and violence using rapid tranquillisation. Nursing Standard. 24(7), 40-51 Dubin, W. R. (1988) Rapid Tranquillisation: antipsychotics or benzodiazepines? Journal of Clinical Psychiatry, 49, 5-11.
Holmes, C. L., Simmons, H., Pilowsky, L. S. (2001) Rapid tranquillisation. In Psychiatric intensive care (eds M. D. Beer, S. Pereira, & C. Paton), pp. 41-58. London. Huf, G., Coutinho, E.S.F. and Adams, C.E. 2002 TREC-Rio trial: a RCT for rapid tranquillisation for agitated patients in emergency psychiatric rooms. BMC Psychiatry 2:11 Huf G, Alexander J, Allen M, Raveendran N. 2009. Haloperidol plus promethazine for psychosis-induced aggression (review). The Cochrane Library 2009 Issue 3 Huf G TREC Collabrotive group. 2003 Rapid Tranquillisation for agitated patients in emergency psychiatric rooms: a randomised trial of midazolam versus haloperidol plus promethazine. BMJ 327(7417): 708- 13 Innes J and Iyeke L. 2011. A review of the practice and position of monitoring in today’s rapid tranquilisation protocols. Journal of Psychiatric Intensive Care. 8 (1), 15-24 Jones, B., Taylor, C. C., and Meehan, K. (2001) The efficacy of a rapid-acting intramuscular formulation of olanzapine for positive symptoms. Journal of Clinical Psychiatry, 62, 22-24.
Karagianis J, Dawe I, Thakur A et al (2001) Rapid Tranquillisation With Olanzapine in Acute Psychosis:A Case Series Journal of Clinical Psychiatry 12-16 Karagianis, J. L., Dawe, I. C., Thakur, A., et al (2001) Rapid tranquillisation with olanzapine in acute psychosis: a case series. Journal of Clinical Psychiatry, 6, 12-16.
Kerr, I. B. and Taylor, D. (1997) Acute disturbed or violent behaviour: principles of treatment. Journal of Psychopharmacology, 11, 271-277.

CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 33 of 34
Kinon B, Rotelli M, Gilmore J et al. (2003) The Efficacy of Olanzapine and Adjunctive Lorazepam to Treat Acute Behavioural Agitation in Schizophrenia Martel M, Sterzinger A, Miner J, Clinton J, Biros M. (2005). Management of acute undifferentiated agitation in the emergency department: A randomised double-blind trial of droperidol, zisprasidone, and midazolam. Academic Emergency Medicine. 12(12): 1167-1173. McAllister-Williams, R. H. and Ferrier, I. N. (2002) Rapid tranquillisation: time for a reappraisal of options for parenteral therapy. The British Journal of Psychiatry, 180, 485-489.
NICE (2005) Clinical Guidelines for the Short Term Management of Disturbed/ violent behaviour in psychiatric in-patient settings and accident and emergency settings. CG25 NICE (2007) Clinical Guidelines for antenatal and postnatal mental health. CG45 NICE (May 2015) Violence and aggression: short-term management in mental health, health and community settings. CG10 Nishiyama T, Matsukawa T, Hanaoka K. 1998. The Effects of age and gender on optimal premedication dose of intramuscular midazolam. 86: 1103-1108. Nobay, F., Simon, B., Levitt, A. and Dresden, G.M. 2004 A Prospective, DB, RCT of midazolam vs, Haloperidol vs. lorazepam in the chemical restraint of violent and severely agitated patients. Academic Emergency Medicine 11(7) 744-749 Paton, C (2002) Benzodiazepines and disinhibition: a review. Psychiatric Bulletin, 26, 460-462.
Pereira S et al (2006) Treatment of acute behavioural disturbance: a UK national survey of rapid tranquillisation. Journal of Psychiatric Intensive Care, 1, 84-88
Pratt P et al. (2008) Establishing gold standard approaches to rapid tranquillisation: A review and discussion of the evidence on the safety and efficacy of medications currently used. Journal of psychiatric intensive care, 4, 43-57
Taylor D, Paton C, Kapur S (2009) The Maudsley Prescribing Guidelines 10th Edition: Acutely disturbed or violent behaviour pg 417-422.
Taylor D, Paton C, Kapur S (2012) The Maudsley Prescribing Guidelines 11th Edition: Acutely disturbed or violent behaviour pg 531-538
The electronic Medicines Compendium (eMC)
Tran-Johnson T et al. (2007) Efficacy and Safety of intramuscular aripiprazole in patients with acute agitation: a randomised, double-blind, placebo-controlled trial. Journal clin Psychiatry 68(1), 111-119
TREC Collaborative Group 2003 Rapid tranquillisation for agitated patients in emergency psychiatric rooms: a randomised trial of midazolam vs. haloperidol plus promethazine. British Medical Journal 327 708-711
Wright, Padraig, Birkett, Martin, David, Stacy R., et al (2001) Double-Blind, Placebo-Controlled Comparison of Intramuscular Olanzapine and Intramuscular Haloperidol in the Treatment of Acute Agitation in Schizophrenia. American Journal of Psychiatry, 158, 1149-1151

CP11 - Protocol for Rapid Tranquillisation Approved by Medicines Safety Committee: July 2021 Review Date: July 2024
Page 34 of 34
Acknowledgements
Guidelines from other Trusts
Rapid Tranquillisation; South West Region Guidelines (2004)
Central and North West London Mental Health NHS Trust (2003)
Norfolk Mental Healthcare NHS Trust (2003)
North East London Mental Health Trust
South West Yorkshire Mental Health NHS Trust
Sussex Partnership NHS Foundation Trust The RT policy (2009)
Derbyshire Mental Health services NHS Trust Guidelines for the management of the acutely disturbed patient.
Coventry and Warwickshire Partnership Trust. Medication for RT and challenging behaviour.
Related Documents











