Version 2 June 2018 Rapid Tranquillisation Target Audience Who Should Read This Policy All Inpatient Staff

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Version 2 June 2018
Rapid Tranquillisation
Target Audience
Who Should Read This Policy
All Inpatient Staff

Rapid Tranquillisation Policy
Version 2.0 January 2019 2
Ref. Contents Page
Explanation of terms used in this policy 4
1.0 Introduction 5
1.1 Rapid Tranquillisation Definition 5
2.0 Purpose 5
3.0 Objectives 6
4.0 Principle and Practise of Rapid Tranquillisation 6
4.1 De-escalation Techniques 6
4.2 Choice of Intervention 6
4.3 Use of oral p.r.n medication 7
4.4 Rapid Tranquillisation and Physical Intervention 7
4.5 Rapid Tranquillisation and Seclusion 8
4.6 Care Planning/Reviews 8
4.7 Risk Assessment 9
4.8 Advance Statements 9
4.9 Legal Issues and the Mental Health Act (MHA) 9
4.10 Physical monitoring/review of history Before Rapid Tranquillisation 9
5.0 Rapid Tranquillisation 10
5.1 Medical Staff Availability 10
5.2 Medical Equipment 10
5.3 Rapid Tranquillisation treatment aims 10
5.4 Rapid Tranquillisation Prescribing 11
5.5 Choice of Medication in Rapid Tranquillisation 12
5.6 Algorithm 1: BCPFT Algorithm for Rapid Tranquillisation / oral p.r.n prescribing for Working Age Adults/Older Adults
13
5.7 Table 1: Rapid Tranquillisation / oral p.r.n notes for Working Age Adults
14
5.8 Table 2: Rapid Tranquillisation / oral p.r.n notes for Older Adults 16
5.9 General Prescribing Notes 18
5.10 Table 3: Drug information for oral p.r.n and IM Rapid Tranquillisation medication to be used with guideline
19
5.11 Prescribing in complex cases 20
5.12 Guidelines for the use of Zuclopenthixol Acetate injection (Clopixol Acuphase®)
21
5.13 Zuclopenthixol Acetate (Clopixol Acuphase®) Post-Administration Physical Observations Record Chart
23

Rapid Tranquillisation Policy
Version 2.0 January 2019 3
6.0 Risks and Complications associated with Rapid Tranquillisation 24
6.1 Circumstances for special care 24
6.2 Observations 24
6.3 Remedial Measures 25
6.4 Table 3: Managing the Complications and Side Effects of Medication 26
7.0 Algorithm 2: Rapid Tranquillisation of the Acutely Disturbed / Violent Patient - Adolescents Aged > 12 Years
27
7.1 Notes for prescribing Rapid Tranquillisation / oral p.r.n for adolescents
28
8.0 Documentation 28
9.0 Post Incident Support and Debrief 29
10.0 Procedures connected to this policy 29
11.0 Links to Relevant Legislation 29
11.1 Links to Relevant National Standards 30
11.2 Links to other Key Policies 30
12.0 Best Practice - Dissemination, Implementation and Monitoring of NICE Quality Standards and Guidance
31
13.0 References 31
14.0 Roles and Responsibilities for this policy 32
15.0 Training 33
16.0 Equality Impact Assessment 34
17.0 Data Protection Act and Freedom of Information Act 34
18.0 Monitoring policy’s effectiveness 35
Appendix
NEWS Observation Chart 37
Medical Emergency Flowchart 41

Rapid Tranquillisation Policy
Version 2.0 January 2019 4
Explanation of terms used in this policy Rapid Tranquillisation (RT) - NICE defines Rapid Tranquilisation (RT) as ‘use of medication by
the parenteral route (usually intramuscular) if oral medication is not possible or appropriate
and urgent sedation with medication is needed’. The aim of treatment is to use medication to calm or lightly sedate the patient and reduce the risk to themselves and/or others. The desired outcome is to
achieve an optimal reduction in agitation and aggression, thereby allowing a thorough psychiatric evaluation to take place.
Violence - any incident where staff, patients or others are abused, threatened or assaulted in circumstances related to their work, involving an explicit or implicit challenge to their safety, wellbeing or
health
Aggression - this may be of a verbal nature or a physical act, whereby intentional behaviour leads to
harm to the individual, to another person or to the damage of property
Seclusion - supervised confinement of a patient in a room, which may be locked. Its sole aim is to contain severely disturbed behaviour that is likely to cause harm to others
Calming - reduction of anxiety
Advance Statements - preferred treatment choices expressed by the patient when well and are likely to be documented in care records. An advance statement is not legally binding
Light Sedation - state of rest and reduction of psychological activity, but verbal contact is maintained
QTc prolongation - QTc is a measurement obtained from an ECG. If this is above normal limits (440ms for men and 470ms for women) it may predict a risk factor for the ventricular arrhythmia Torsade de
Pointes, which is occasionally fatal (sudden cardiac death). Psychotropic agents such as haloperidol have been associated with QTc prolongation. Above 500ms there is strong evidence for increased risk of
arrhythmias. QTc prolongation may occur more frequently with higher doses, combinations of psychotropic medication, intravenous administration and in predisposed patients. Check Maudsley
guidelines for risk of QTc prolongation.
Parenteral - administration of medicine usually via intramuscular route or, exceptionally, intravenous
National Early Warning Scoring (NEWS) - single standardised early warning system which has been
developed by the Royal College of Physicians and has been adopted nationally by the NHS to enable
consistency across both acute and community hospital settings
p.r.n (pro re nata) - when required. In this guideline, p.r.n. refers to the use of oral medication as part of a strategy to de-escalate or prevent situations that may lead to violence or aggression; it does not refer
to p.r.n. medication used on its own for Rapid Tranquillisation during an episode of violence or aggression

Rapid Tranquillisation Policy
Version 2.0 January 2019 5
1.0 Introduction
Black Country Partnership NHS Foundation Trust recognises that it is sometimes necessary to use pharmacological intervention to maintain the safety and physical health of some patients who are acutely unwell. It is accepted that certain situations may arise in psychiatric in-patient environments or S136 suite that can lead to potential or actual harm of the patient or those around them as a result of their extremely disturbed or challenging behaviour. This could arise due to psychotic or non-psychotic illness and may need to be brought rapidly under control with the appropriate use of medication in order to avoid prolonged use of physical interventions. Rapid tranquillisation is not a first line therapy for managing violence and aggression. The underlying condition does not necessarily predict response to rapid tranquillisation nor preclude rapid tranquillisation. Other approaches to manage imminent violence include de-escalation techniques, consideration of placement, physical interventions and seclusion but when used, management strategies to reduce the level of risk should be recorded in care plans. The aim of treatment is to use medication to calm or lightly sedate the patient and reduce the risk to themselves and/or others. The desired outcome is to achieve an optimal reduction in agitation and aggression, thereby allowing a thorough psychiatric evaluation to take place. This policy should be read in conjunction with the Prevention and Management of Violence and Aggression including NHS Sanctions Policy. 1.1 Rapid Tranquillisation Definition CQC guidance BG0401 and NICE guidance NG10 defines Rapid Tranquillisation (RT) as ‘use of medication by the parenteral route (usually intramuscular) if oral medication is not possible or appropriate and urgent sedation with medication is needed’. RT includes all medication administered whilst the patient is restrained to control behaviour. Administration of oral medication is not considered to be RT, however due to the potential agitated state, it is good practice to closely monitor the patient following administration of combinations of oral medication and repeated doses of oral medication given within the same episode to control behaviour. 2.0 Purpose
The purpose of this policy is to provide staff with clear direction in regard to the use of Rapid Tranquillisation (RT) when faced with incidents of acutely disturbed behaviour and extreme aggression.

Rapid Tranquillisation Policy
Version 2.0 January 2019 6
3.0 Objectives
To define and explain the use of Rapid Tranquillisation in inpatient settings or the S136 Suite.
To provide a standardised approach to physical monitoring and nursing care before, during and following Rapid Tranquillisation.
To provide a framework for ensuring:
The decision to use Rapid Tranquillisation is made with due consideration.
Rapid tranquillisation is used safely and effectively.
The use of Rapid Tranquillisation (RT) is reflected upon and care plans reviewed appropriately.
4.0 Principles and Practice of Rapid Tranquillisation (RT)
In certain situations within psychiatric in-patient environments or the S136 suite, potential or actual harm of a patient or those around them can arise as a result of their extremely disturbed or challenging behaviour. Initial approaches to manage imminent violence can include de-escalation techniques, oral p.r.n medication, consideration of placement, physical interventions and seclusion. 4.1 De-escalation Techniques
Maintain adequate distance.
Ensure environment is conducive to calmness (e.g. low stimulation levels, noise and other patients).
Move to a safe place. Use a designated area or room to reduce emotional arousal or agitation and support the service user to become calm practised. Do not routinely use the seclusion room (if available) for this purpose because the service user may perceive this as threatening (NICE NG10 8.3.2.9).
Explain intentions and be calm and self-assured.
Use non-threatening non-verbal communication.
Converse and try to develop therapeutic relationship throughout.
Use of sensory resources i.e. weighted blanket, games consoles. 4.2 Choice of Intervention Where de-escalation techniques have failed to calm a patient, it may be necessary to make use of additional interventions, such as oral p.r.n medication, physical intervention, Rapid Tranquillisation (RT) and seclusion to manage the incident. All such interventions should only be considered once de-escalation techniques have been tried and have not succeeded in calming the patient. The choice of intervention(s) will depend on a number of factors, but should be guided primarily by:
Patient preference (if known).
The clinical needs of, and risks to, the patient.
Obligations to other patients affected by the disturbed/ violent behaviour.
The protection of staff, patients and visitors.
The facilities available within the particular setting.
Rapid Tranquillisation Policy
Version 2.0 January 2019 7
4.3 Use of oral p.r.n medication When prescribing oral p.r.n. medication as part of a strategy to de-escalate or prevent situations that may lead to violence and aggression, consider the following;
p.r.n should be offered first line.
do not prescribe p.r.n. medication routinely or automatically on admission
tailor p.r.n. medication to individual need and include discussion with the service user if possible
ensure there is clarity about the rationale and circumstances in which p.r.n. medication may be used and that these are included in the care plan
ensure that the maximum daily dose is specified and does not inadvertently exceed the maximum daily dose stated in the British national formulary (BNF) when combined with the person’s standard dose or their dose for RT
only exceed the BNF maximum daily dose (including p.r.n dose, the standard dose and dose for rapid tranquillisation) if this is planned to achieve an agreed therapeutic goal, documented, and carried out under the direction of a senior doctor
ensure that the interval between p.r.n doses is specified.
The multidisciplinary team should review oral p.r.n medication at least once a week and, if p.r.n medication is to be continued, the rationale for its continuation should be included in the review. If p.r.n medication has not been used since the last review, consider stopping it.
If more than one medication is prescribed, the care plan should include the preferred order of administration of medicines and time interval between the medicines.
If two medications are intended to be given at the same time this should be clearly stated.
It should be noted that a single p.r.n antipsychotic dose does not have an antipsychotic action, as onset of its antipsychotic effect will require regular dosing over days and weeks.
When deciding which medication to use take into account any contra-indications, special warnings or precautions required. Also consider;
the service user's preferences or advance statements and decisions pre-existing physical health problems or pregnancy possible intoxication (alcohol or psychoactive drugs) previous response to these medications, including adverse effects potential for interactions with other medications total daily dose of medications prescribed and administered.
For full details of contra-indications, special warnings and precautions for all medicines can be found on http://www.medicines.org.uk/emc
4.4 Rapid Tranquillisation and Physical Intervention In certain situations, the multidisciplinary team may agree use of medication as the most appropriate method of managing extreme behaviour. Where this is likely to require the use of physical intervention in order to safely administer the medication - the force used to administer medication must be reasonable. Current physical intervention skills do not allow for the complete immobilisation of a patient. Movement will be generated by an agitated patient thus making it difficult to safely

Rapid Tranquillisation Policy
Version 2.0 January 2019 8
administer RT. In order to reduce the injection risks staff should wait until movement is at a minimum and/or the patient is ready to cooperate with the injection. Consider RT or seclusion as alternatives to prolonged manual restraint (longer than 10 minutes) [NICE NG10 8.4.5.8]. 4.5 Rapid Tranquillisation and Seclusion The combined use of seclusion and RT should be avoided wherever possible, however, if seclusion is judged necessary to manage the serious risk of violence the following should be considered and the potential complications of RT should be taken seriously;
Continuous observation through the observation window by a delegated nurse
Terminating seclusion once RT has taken effect
The patient’s respiration and where possible all other vital signs should be monitored
Once seclusion is instigated refer to Seclusion Policy for further guidance 4.6 Care Planning/Reviews Ensure that patients who might be subject to RT have an individual care plan. The multidisciplinary team should develop and document an individualised pharmacological strategy for using routine and p.r.n. medication to calm, relax, tranquillise or sedate service users who are at risk of violence and aggression as soon as possible after admission to the ward or S136 suite. Where possible care plans for the management of individual service users should be made in advance of the episode of acutely disturbed behaviour. These care plans should indicate:
At what stage medicines should be used
If more than one medicine is prescribed in what order they should be administered
At what stage medical involvement is required.
clarification of target symptoms
the likely timescale for response to medication The plans should be developed on the basis of past experience of the response of the service user to the medicines used and should include any advance statements agreed with the service user. The multidisciplinary team should review the pharmacological strategy and the use of medication at least once a week and more frequently if events are escalating and restrictive interventions are being planned or used. The review should be recorded and include:
the total daily dose of medication, prescribed and administered, including p.r.n medication
the number of and reason for any missed doses
therapeutic response
the emergence of unwanted effects. If RT is being used, a senior doctor should review all medication at least once a day.

Rapid Tranquillisation Policy
Version 2.0 January 2019 9
4.7 Risk Assessment The decision to use RT should be made after clinical assessment of need and risk to the patient and/or others. All patients should have a regular and comprehensive risk assessment to ensure the safety of the patient and the clinical environment. Risk assessments should be ongoing as risks may change according to circumstances. The risks associated with RT are to be explored by the team prior to the administration of medication to determine safety and appropriateness. RT is potentially hazardous and the risk of adverse effects is higher if the patient has taken illicit drugs or alcohol. 4.8 Advance Statements Patients identified to be at risk of disturbed or violent behaviour should be given the opportunity to have their needs and wishes recorded in the form of an advance directive and within a care plan. 4.9 Legal Issues and the Mental Health Act (MHA) If a patient refuses or lacks capacity to give valid consent to treatment, ensure there is appropriate legal authority in place prior for prescribing/administering RT e.g. if detained over 3 months, a section 62 or T3 is in place to cover prescribed medication. The enforced administration of medication by injection to an informal patient may necessitate use of the Mental Health Act. If treatment is to continue against the patient’s wishes then a MHA assessment must be undertaken to ensure continued administration is lawful. 4.10 Physical monitoring/review of history Before Rapid Tranquillisation (RT) In anticipation of the likelihood of prescribing medication for RT, the prescribing doctor should:
Ensure baseline measurements are taken and recorded i.e. blood pressure, temperature, pulse, respiration, weight
Review the patient’s clinical record with regard to his/her general medical history and consider the possibility of a physical examination
Previous response to RT or other methods of managing imminent violence
Be aware of any previous drug sensitivity / allergies and communicate this information to all members of the MDT through normal communication channels Check for recent ECG, blood and urine drug screen results, a previous history of severe extrapyramidal side effects
Review current prescribed medication (including regular and p.r.n) and any recently administered depots/LAI’s. Also take note of recent administration of p.r.n medication

Rapid Tranquillisation Policy
Version 2.0 January 2019 10
5.0 Rapid Tranquillisation Rapid tranquillisation (RT) is used in situations requiring the rapid control of agitation, aggression or excitement when other less coercive techniques of calming a patient, such as verbal de-escalation or intensive nursing techniques have failed and the patient is refusing oral p.r.n medication. RT involves the administration of parenteral medication in order to produce a state of calm/light sedation. The medications used for RT should ideally have a low level of side effects and rapid onset of action. For the purpose of this policy, RT describes the use of parenteral medication to control severe mental and behavioural disturbance, including:
Aggression associated with the mental illness of schizophrenia, mania and other psychiatric conditions
Organic disorders, including dementia from a variety of causes
5.1 Medical Staff Availability
A doctor should be quickly available at all times to attend to an alert by ward staff or S136 suite staff when RT is implemented. NICE Clinical Guideline on Violence and Aggression (NG10) recommends that a doctor should aim to be at the scene within 30 minutes. Medical support must be available in case of adverse reactions, over sedation or the need to administer IV Flumazenil (to reverse sedation, drowsiness). If RT is to be considered out of hours the duty doctor should be contacted and requested to attend. 5.2 Medical Equipment
The blue emergency ILS bag should be available within 3 minutes in inpatient settings where RT might be used. The bag should be maintained and checked routinely. 5.3 Rapid Tranquillisation treatment aims
To reduce suffering for the patient: psychological or physical (through self-harm or accidents).
To reduce risk of harm to others by maintaining a safe environment.
To do no harm (by prescribing safe regimes and monitoring physical health).
Rapid Tranquillisation Policy
Version 2.0 January 2019 11
5.4 Rapid Tranquillisation Prescribing
RT as parenteral injection (usually IM) should only be considered when de-escalation techniques and oral p.r.n have been less effective or refused. The use of IM medication for RT must be reported externally and for this reason the use of IM medication must be reported via the Physical Intervention Monitoring Form and a Datix incident report completed. 5.4.1 The reason for prescribing should be documented in the clinical record, including the care plan. 5.4.2 Do not prescribe RT medication routinely or automatically on admission on the when required section of the drug chart. NICE guidance states that RT should initially only be prescribed as a single dose. Additional doses of RT should not be administered for the service user until the full effect of the first dose has been assessed and found to be physically tolerated. In exceptional circumstances, for example when the service user has a known relapse presentation requiring repeated episodes of RT, it may be prescribed with a specified number of doses for administration. Prescriptions for multiple doses of RT should be agreed by the multidisciplinary team or authorised by a Consultant Psychiatrist. 5.4.3 Only when RT continues to be required should it be prescribed on the ‘as required medicines’ section of the chart including indication, maximum dose, interval and maximum daily dose. This should be reviewed at least once weekly. 5.4.4 If more than one medication is prescribed, the care plan should include the preferred order of administration of medicines and time interval between the medicines. 5.4.5 When deciding which medication to use take into account any contra-indications, warning or precautions required.
the service user's preferences or advance statements and decisions
pre-existing physical health problems or pregnancy
possible intoxication (alcohol or psychoactive drugs) or delirium
previous response to these medications, including adverse effects
potential for interactions with other medications
the total daily dose of medications prescribed and administered. Full details of contra-indications, special warnings and precautions for all medicines can be found on http://www.medicines.org.uk/emc
5.4.6 Care must be taken when giving IM injections particularly to highly aroused and/or violent individuals. The provision of adequate staff trained in approved care and techniques should always be on standby even when patients agree to IM treatment, as there are the inadvertent risks of intra-arterial injection, bolus dosing, nerve damage, bruising, needle breakage in patients who may struggle or are resistive, and also a higher than expected absorption rate due to the increased blood flow to the muscles in a highly aroused individual.

Rapid Tranquillisation Policy
Version 2.0 January 2019 12
5.5 Choice of Medication in Rapid Tranquillisation NICE NG10 states the following;
Use either IM lorazepam on its own or IM haloperidol combined with intramuscular promethazine (due to its antimuscarinic properties) for RT in adults.
If there is insufficient information to guide the choice of medication for RT, or the service user has not taken antipsychotic medication before, use IM lorazepam.
If there is evidence of cardiovascular disease, including a prolonged QTc, or no ECG has been carried out, avoid intramuscular haloperidol combined with IM promethazine and use IM lorazepam instead.
If there is a partial response to intramuscular lorazepam, consider a further dose.
If there is no response to intramuscular lorazepam, consider IM haloperidol combined with IM promethazine.
If there is a partial response to IM haloperidol combined with IM promethazine, consider a further dose. If there is no response to intramuscular haloperidol combined with intramuscular promethazine, consider intramuscular lorazepam if this hasn't been used already during this episode.
If intramuscular lorazepam has already been used, arrange an urgent team meeting to carry out a review and seek a second opinion if needed.
Alternatives which may be considered are;
Aripiprazole IM (alone or in combination with Lorazepam IM). Although not considered by NICE NG10 due to insufficient evidence, it is may be prescribed on inpatient wards if it is considered to be the safest and most appropriate treatment option for the service user.
Olanzapine IM alone. Not considered by NICE NG10 because the manufacturer of IM olanzapine has withdrawn the product from the UK market. As a result they were unable to make recommendations regarding its use. However, it remains a licensed product in the European Union (EU) and may be prescribed, if following a multidisciplinary review it is considered to be the most appropriate treatment option for a service user. IM olanzapine MUST NOT be co-administered with IM lorazepam, hypnotics (e.g. promethazine) or other antipsychotics. These medicines must not be given within 60 minutes of IM olanzapine (pre or post dose). This is due to the increased risk of respiratory depression, hypotension and bradycardia; on rare occasions fatalities have occurred.
The use of two medicines of the same class for the purpose of RT or p.r.n should not occur.
Rapid Tranquillisation Policy
Version 2.0 January 2019 13
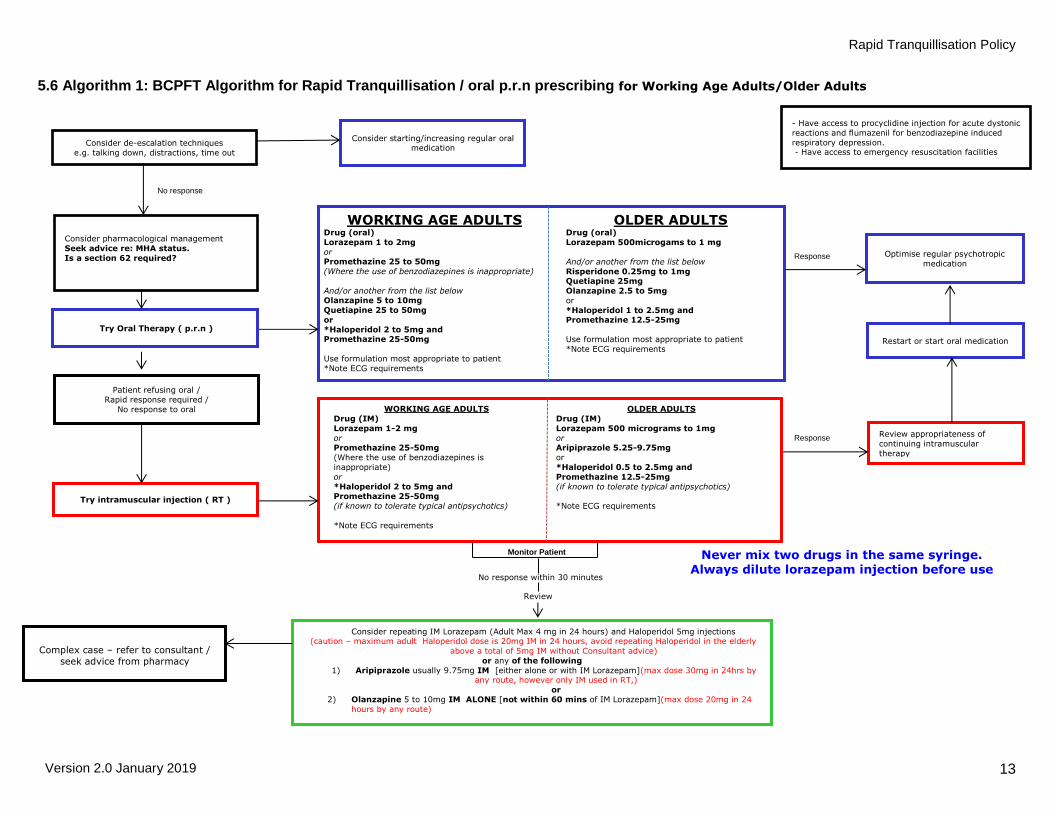
5.6 Algorithm 1: BCPFT Algorithm for Rapid Tranquillisation / oral p.r.n prescribing for Working Age Adults/Older Adults
- Have access to procyclidine injection for acute dystonic
reactions and flumazenil for benzodiazepine induced
respiratory depression. - Have access to emergency resuscitation facilities
Consider de-escalation techniques
e.g. talking down, distractions, time out
Consider starting/increasing regular oral medication
Consider pharmacological management
Seek advice re: MHA status.
Is a section 62 required?
Try Oral Therapy ( p.r.n )
Patient refusing oral /
Rapid response required /
No response to oral
Try intramuscular injection ( RT )
WORKING AGE ADULTS Drug (oral)
Lorazepam 1 to 2mg
or Promethazine 25 to 50mg
(Where the use of benzodiazepines is inappropriate)
And/or another from the list below Olanzapine 5 to 10mg
Quetiapine 25 to 50mg
or
*Haloperidol 2 to 5mg and Promethazine 25-50mg
Use formulation most appropriate to patient
*Note ECG requirements
OLDER ADULTS Drug (oral)
Lorazepam 500microgams to 1 mg
And/or another from the list below
Risperidone 0.25mg to 1mg Quetiapine 25mg
Olanzapine 2.5 to 5mg
or
*Haloperidol 1 to 2.5mg and Promethazine 12.5-25mg
Use formulation most appropriate to patient
*Note ECG requirements
WORKING AGE ADULTS
Drug (IM)
Lorazepam 1-2 mg
or Promethazine 25-50mg
(Where the use of benzodiazepines is
inappropriate)
or
*Haloperidol 2 to 5mg and Promethazine 25-50mg
(if known to tolerate typical antipsychotics)
*Note ECG requirements
OLDER ADULTS
Drug (IM)
Lorazepam 500 micrograms to 1mg
or Aripiprazole 5.25-9.75mg
or
*Haloperidol 0.5 to 2.5mg and
Promethazine 12.5-25mg
(if known to tolerate typical antipsychotics)
*Note ECG requirements
Optimise regular psychotropic
medication
Restart or start oral medication
Review appropriateness of
continuing intramuscular
therapy
Monitor Patient
No response within 30 minutes
Review
Consider repeating IM Lorazepam (Adult Max 4 mg in 24 hours) and Haloperidol 5mg injections (caution – maximum adult Haloperidol dose is 20mg IM in 24 hours, avoid repeating Haloperidol in the elderly
above a total of 5mg IM without Consultant advice)
or any of the following
1) Aripiprazole usually 9.75mg IM [either alone or with IM Lorazepam](max dose 30mg in 24hrs by any route, however only IM used in RT,)
or
2) Olanzapine 5 to 10mg IM ALONE [not within 60 mins of IM Lorazepam](max dose 20mg in 24
hours by any route)
Complex case – refer to consultant /
seek advice from pharmacy
Never mix two drugs in the same syringe. Always dilute lorazepam injection before use
No response
Response
Response

Rapid Tranquillisation Policy
Version 2.0 January 2019 14
5.7 Table 1: Rapid Tranquillisation / oral p.r.n notes for Working Age Adults
1 Review the use of non-pharmacological strategies for managing an imminent risk of violence
Review the patient’s consent to treatment. Is it necessary to use section 62?
Review the patient’s clinical record for previous medical history and recent investigations
Note total medication in last 24 hours and response
Consider physical examination
Consult with a more senior doctor at any stage if unsure
Flumazenil must be available in case of Benzodiazepine-induced respiratory depression
2 ORAL p.r.n medication.
LORAZEPAM oral 1-2mg
(May repeat after 45-60 minutes)
[Max. 4mg/24 hours]
PROMETHAZINE oral 25-50mg
(May repeat after 1-2 hours)
[Max. 100mg/24 hours]
OLANZAPINE oral 10mg
(May repeat after 4 hours.)
[Max. 20mg/24 hours)
HALOPERIDOL oral 5mg
(with Promethazine)
(May repeat after 4 hours.)
[Max. 20mg/24 hours]
QUETIAPINE oral 25-50MG
(may repeat after 4 hrs.)
[Max. 750-800mg/24hrs]
If the patient is prescribed a regular oral or depot antipsychotic or has
cardiovascular disease, consider using Lorazepam alone.
Consider using promethazine if the patient is benzodiazepine tolerant.
If not already taking a regular oral or depot/LAI antipsychotic, has respiratory
disease or a doctor is not present out of hours, consider using an antipsychotic
alone.
Avoid using Haloperidol in antipsychotic naïve patients or those with prolonged
QTc. The SPC for Haloperidol recommends avoiding concomitant antipsychotics
and having a pre-treatment ECG.
Haloperidol should be combined with promethazine to minimise EPSE as per
NICE NG10.
Ensure Procyclidine is available for extra pyramidal side-effects (EPSE).
Allow sufficient time for clinical response between doses.

Rapid Tranquillisation Policy
Version 2.0 January 2019 15
3 No response or patient refuses oral consider using INTRAMUSCULAR medication. The options for RT include:
LORAZEPAM IM 1-2 mg
(May repeat after 30-60 minutes.)
[Max. 4mg/24 hours]
PROMETHAZINE IM 25-50mg
(May repeat after 1-2 hours.)
[Max. 100mg/24 hours]
ARIPIPRAZOLE IM 5.25–9.75mg
Usual dose 9.75mg.
(May repeat after 2 hours.)
[Max. 30mg/24 hours]
HALOPERIDOL IM 2-5mg
(May repeat after 4-8 hours)
[Max.20mg/24 hours]
OLANZAPINE IM 5-10mg
(may repeat after 2 hours)
[Max. 20mg/24 hours]
If the patient is prescribed a regular oral or depot Antipsychotic or has
cardiovascular disease, consider using Lorazepam alone.
Promethazine may be used as an alternative and is a useful option in a
Benzodiazepine-tolerant patient.
If the patient is not already taking a regular oral or depot Antipsychotic, is
Benzodiazepine tolerant, has respiratory disease or a doctor is not present out of
hours, consider using an Antipsychotic alone.
Allow sufficient time for clinical response between doses. Transfer to oral route at
earliest opportunity.
Avoid using Haloperidol in Antipsychotic naïve patients. Maudsley suggests that
Haloperidol should be the last drug considered. The SPC recommends a pre-
treatment ECG. The incidence of acute dystonia is high – combine with IM
Promethazine and ensure oral/IM Procyclidine is available.
Allow sufficient time for clinical response between doses. Transfer to oral route at
earliest opportunity.
IM olanzapine MUST NOT be co-administered with IM lorazepam, Promethazine
or other antipsychotics.
4 If unsuccessful seek advice from consultant psychiatrist on duty. Consider alternatives.

Rapid Tranquillisation Policy
Version 2.0 January 2019 16
5.8 Table 2: Rapid Tranquillisation / oral p.r.n notes for Older Adults
1 Review the use of non-pharmacological strategies for managing an imminent risk of violence
Review the patient’s consent to treatment. Is it necessary to use section 62?
Review the patient’s clinical record for previous medical history and recent investigations
Note total medication in last 24 hours and response
Consider physical examination
Consult with a more senior doctor at any stage if unsure
Flumazenil must be available in case of benzodiazepine-induced respiratory depression
2 ORAL p.r.n medication should be first choice where possible
2.1 Patient with known diagnosis of schizophrenia, mania or
other functional disease
Have longer times between doses.
Consider half adult doses. Caution: renal or hepatic
impairment, cardiovascular disease. Monitor B.P.
2.2 Dementia with Lewy Bodies (DLB) present or cannot be
excluded
Avoid Antipsychotic medication as it can cause sudden
deterioration, side effects and even death.
Consider oral Lorazepam 0.5mg-1mg every 4 hours
[Max. 2mg/24 hours].
2.3
Dementia other than DLB
If the patient is established on a regular Antipsychotic or has
cardiovascular disease, consider using Lorazepam alone.
If the patient is benzodiazepine tolerant or has respiratory
disease or a doctor is not present out of hours, consider using
an antipsychotic alone.
Caution – antipsychotic drugs are associated with an
increased risk of mortality, stroke and transient ischaemic
attack.
Consider oral Lorazepam 0.5mg-1mg every 4 hours [Max.
2mg/24 hours].
Consider oral Haloperidol 1-2.5mg [Max.5mg/24 hours]
or Quetiapine 25mg or Risperidone 0.25mg.
(Avoid using haloperidol in Antipsychotic naïve patients. The
SPC recommends avoiding concomitant Antipsychotics and
having a pre-treatment ECG. Ensure Procyclidine is available
for EPSEs).
Promethazine in the elderly - caution should be exercised in
patients with a diagnosis of dementia.
Olanzapine – do not use in dementia.
3
Monitor status and continue oral. If no response or patient refuses oral medication seek advice from duty consultant
psychiatrist. In cases of emergency consider using INTRAMUSCULAR medication.

Rapid Tranquillisation Policy
Version 2.0 January 2019 17
3.1 Dementia with Lewy Bodies (DLB) present or cannot be
excluded
Consider IM Lorazepam 0.5mg-1mg only [Max. 2mg/24
hours.
3.2
Dementia other than DLB
If the patient is established on a regular antipsychotic or has
cardiovascular disease, consider using Lorazepam alone.
If the patient is benzodiazepine tolerant or has respiratory
disease or a doctor is not present out of hours, consider using
an antipsychotic alone.
Caution – antipsychotic drugs are associated with an
increased risk of mortality, stroke and transient ischaemic
attack.
Consider IM Lorazepam 0.5mg-1mg only (Max. 2mg/24
hours).
Consider IM Haloperidol 0.5-2.5mg (Max. 5mg in 24 hours).
(Avoid using Haloperidol in Antipsychotic naïve patients.
SPC recommends pre-treatment ECG. Ensure Procyclidine is
available for side-effects).
Consider IM Aripiprazole 5.25-9.75mg [max 30mg in
24hrs]. May be used in combination with IM Lorazepam.
Promethazine in the elderly - caution should be exercised in
patients with a diagnosis of dementia.
Olanzapine – do not use in dementia.
4 If unsuccessful seek advice from consultant psychiatrist on duty. Consider alternatives.

Rapid Tranquillisation Policy
Version 2.0 January 2019 18
5.9 General Prescribing Notes
1. Previous medication taken by the patient must be considered. 2. Care must be taken to ensure that High dose prescribing does not inadvertently occur through the
use of p.r.n medication given in combination with regular medication. 3. Two drugs of the same class should not be used for RT. 4. The BNF maximum doses include both oral and IM formulations. 5. Oral and intramuscular medications should be prescribed separately on the treatment chart. 6. Drugs should never be mixed in the same syringe prior to administration. 7. A baseline ECG is recommended prior to treatment in all patients prescribed Haloperidol. If it has
been refused or not taken for any other reason, this should be documented in the patient’s notes clearly with the reasons why stated.
8. Despite the need for rapid and effective treatment, the use of two or more antipsychotics (antipsychotic polypharmacy) should be avoided on the basis of risk associated with QTc prolongation. Other drugs may also affect the QT interval e.g. Citalopram, Escitalopram, Macrolide and Fluoroquinolone antibiotics, Amiodarone, Hydroxyzine. Contact pharmacy for further information.
9. Elderly: in patients with dementia, antipsychotic drugs are associated with a small increased risk of mortality, stroke and transient ischaemic attack. Risperidone should only be used for the short-term treatment (up to 6 weeks) of persistent aggression in patients with moderate to severe Alzheimer's dementia unresponsive to non-pharmacological approaches and when there is a risk of harm to self or others.
10. Ensure Procyclidine is available to manage acute dystonic reactions or other extrapyramidal side-effects of antipsychotic medication especially Haloperidol.
11. Risperidone and Olanzapine are available as oro-dispersible tablets. 12. Benzodiazepines side effects: loss of consciousness, respiratory depression or arrest, risk
cardiovascular collapse when receiving both Clozapine and benzodiazepines. 13. Antipsychotics side effects: loss of consciousness, cardiovascular/respiratory complications and
collapse, seizures, akathisia, dystonia, dyskinesia, neuroleptic malignant syndrome, excessive sedation.
14. Antihistamines side effects: excessive sedation, painful injection, additional anti-muscarinic effects.
15. Simultaneous administration of injectable antipsychotics and parenteral Benzodiazepines may be associated with excessive sedation and cardio-respiratory depression. Patients should be monitored for excessive sedation and orthostatic hypotension.
16. A resuscitation bag should be available within 3 minutes in healthcare settings where rapid tranquillisation might be used. The equipment should include an automatic external defibrillator, a bag valve mask, oxygen, cannulas, fluids, and suction and first-line resuscitation medications.
17. It is recognised that clinicians may decide that the use of medication outside the Summary of Product Characteristics (SPCs) is occasionally justified, bearing in mind the overall risks. However, where the regulatory authorities or manufacturer issues a specific warning that this may result in an increased risk of mortality, the medication should only be used strictly in accordance with the current marketing authorisation.

Rapid Tranquillisation Policy
Version 2.0 January 2019 19
5.10 Table 3: Drug information for oral p.r.n and IM Rapid Tranquillisation medication to be used with guideline
Drug
Route Onset of Action
Time to Reach Maximum Conc / Half life
BNF Maximum Dose in 24 hours
Other e.g. monitoring, licensing, administration
QT c rating
Aripiprazole IM NR Peak 1-3 hrs. t1/2 75 hrs
30mg May be repeated after 2 hrs. Half-life extends to 146 hrs in poor metabolisers of CYP2D6
Low
Haloperidol Oral 1-2 hrs. Peak 4 hrs. t1/2 20 hrs
20mg ECG requirement – QTc prolongation Note the change in maximum dose of IM haloperidol, as result of harmonisation by the
High
Haloperidol IM 20 mins Peak 60-90 mins. t1/2 20 hrs
20mg European Medicines Agency. See BNF. High
Lorazepam Oral 20-30 mins.
Peak 2hrs t1/2 12 hrs
4mg Oral has similar onset of action to IM Risk of paradoxical disinhibition
NR
Lorazepam IM <20-30 mins.
Peak 60-90 mins. t1/2 12 hrs
4mg IV Flumazenil must be available NR
Clonazepam PO 20-60 mins
Peak 1-4 hrs t1/2 20-60 hrs
8mg Caution: high relative maximum BNF dose. Risk of accumulation, due to long half-life.
NR
Olanzapine Oral 1 hr. Peak 5-8 hrs. t1/2 31-52 hrs
20mg Do not use Olanzapine in Dementia Time to peak is longer.
Low
Olanzapine IM 15-30 mins
Peak 15-45 mins t1/2 31-52 hrs
20mg Do not use within 1 hr of IM Lorazepam IM results in peak 5x higher than oral dose.
Low
Promethazine Oral 20 mins Peak 2-3 hrs. t1/2 7-15 hrs
100mg Suitable for benzodiazepine tolerant pts. NR
Promethazine IM 20 mins Peak 2-3 hrs t1/2 7-15 hrs
100mg Can be combined with Haloperidol due to its anti-cholinergic properties.
NR
Quetiapine IR Oral NR Peak 1.5-1.8 hrs. t1/2 hrs 7-12 hrs
750/800mg Limited clinical experience Moderate
Risperidone Oral NR Peak 1-2 hrs.
16mg Limited clinical experience or trial data Low
Zuclopenthixol ACETATE
IM 2-8 hrs. Peak 12-36 hrs. Duration of action 48-72 hours
150mg See separate guidelines NR
NR=Not Recorded

Rapid Tranquillisation Policy
Version 2.0 January 2019 20
5.11 Prescribing in complex cases After discussion with consultant only: not for routine use in Rapid Tranquillisation. If a patient is on maximum dose of oral antipsychotic, consider using above BNF maximum doses or alternative antipsychotic short-term only. In certain circumstance, current BNF limits and the manufacturer’s SPC may be knowingly exceeded. This decision should not be taken lightly or the risks underestimated. Record a risk-benefit analysis in the case notes and a rationale in the care plan. Undertake frequent and intensive monitoring of a calmed service user. Zuclopenthixol acetate injection (Clopixol Acuphase®) [See 5.12 on following page for further guidance] Caution in elderly. It is not recommended for RT due to its significantly delayed onset and relatively long duration of action. Benzodiazepines Consider Lorazepam: High dose. Use with caution and document in patients clinical notes reason for prescribing high dose. Undertake frequent and intensive monitoring. A doctor must be present to administer Flumazenil if needed.

Rapid Tranquillisation Policy
Version 2.0 January 2019 21
5.12 Guidelines for the use of Zuclopenthixol Acetate injection (Clopixol Acuphase®) N.B. For use following approval from consultant only
BNF Indication
Short-term management of acute psychosis, mania or exacerbations of chronic psychoses.
Dosage 50-150mg (1-3ml). Elderly: 50-100mg
Frequency
If necessary repeat after 2-3 days. One additional dose may be given 1-2 days after the first injection. Maximum cumulative dose 400mg over 14 days. Maximum duration of treatment of 2 weeks. Not for long-term treatment.
Route Deep intramuscular injection into the upper outer buttock or lateral thigh. Injection volumes greater than 2ml should be distributed between 2 sites.
Onset, duration of action
Sedative effects usually begin to be seen between 2-8 hours after injection and peak between 12-36 hours. The effects can last for up to 72 hours.
Other
If resisting injection i.e. struggling, use appropriate MAPA techniques to decrease risk of injection into vein. If maintenance treatment is necessary change to an oral Antipsychotic 2-3 days after last injection or to a longer acting Antipsychotic depot injection given concomitantly with last injection of Zuclopenthixol Acetate.
Clopixol Acuphase® injection should be considered only;
following consultant approval.
after an acutely psychotic patient has required repeated injections of short-acting Antipsychotic drugs such as Haloperidol, or sedative drugs such as Lorazepam.
for patients known to respond to it.
in physically violent patients for who repeated attempts at injection would be dangerous for all parties.
be given only when enough time has elapsed to assess the full response to previously injected drugs. Allow at least 60 minutes after IM injection.
if cited in an advance directive. Clopixol Acuphase® injection should never be administered;
in an attempt to ‘hasten’ the antipsychotic effect of other Antipsychotic Therapy for Rapid Tranquillisation (onset of effect is too slow) at the same time as other parenteral antipsychotics or benzodiazepines (may
lead to over sedation which is difficult to reverse) as a ‘test dose’ for Zuclopenthixol Decanoate depot injection to a patient who is physically resistant (risk of intravasation and oil embolus)

Rapid Tranquillisation Policy
Version 2.0 January 2019 22
Clopixol Acuphase® injection should never be used for, or in, the following:
Patients who accept oral medication
Patients who are antipsychotic naïve
Patients who are sensitive to extrapyramidal side effects (dystonia, laryngeal spasm, oculogyric crisis or previous neuroleptic malignant syndrome)
Patients who are unconscious
Patients who are pregnant
Patients with convulsive disorders or Parkinson’s disease
Those with hepatic or renal impairment
Those with cardiac disease
Those with a depressed level of consciousness due to any cause (e.g. intoxication with alcohol, illicit drugs, barbiturates or opiates), coma
Those resisting injection i.e. struggling. Use appropriate physical intervention techniques to decrease risk of injection into vein
Patients that are not detained under the Mental Health Act Caution should be exercised in patients who have recently received a dose of depot/LAI antipsychotic which has not yet reached peak levels. ECG monitoring is strongly recommended. Prolonged QTc related to antipsychotic treatment may also be exacerbated by the co- administration of other drugs known to significantly prolong QTc. NICE suggests that Clopixol Acuphase® injection may be considered an option when:
service user will be disturbed/violent over an extended time period
past history of good/timely response
past history of repeated parenteral administration
cited in an advance directive Never administer to those without previous antipsychotic exposure. There is no such thing as ‘a course of Acuphase’. Once a first dose has been prescribed the treatment plan should clearly document the circumstances when further doses may be administered. Subsequent doses should not be written up on the drug chart until patient has been reassessed by the doctor. Physical Monitoring Use Chart 1 overleaf to record physical monitoring following administration of zuclopenthixol acetate (Clopixol Acuphase®)

Rapid Tranquillisation Policy
Version 2.0 January 2019 23
5.13 Zuclopenthixol Acetate (Clopixol Acuphase®)
Post-Administration Physical Observations Record Chart
Name: Ward:
Date and time administered: Dose:
Time since
administration
Time
24hr
Level of
Alertness
(AVPU)
Respiratory
Rate
BP
Pulse
NEWS
Score
Signs of
EPSEs
(Yes/No)
Hydrated
(Yes/No)
Sign
Baseline
2 hours
4 hours
6 hours
8 hours
12 hours
16 hours
20 hours
24 hours
28 hours
32 hours
36 hours
40 hours
44 hours
48 hours
Codes: - Level of Alertness (AVPU)
A Alert: Eyes open with normal verbal response.
V Voice: Eyes closed but will open eyes on command, and with normal verbal response.
P Pain: Eyes closed, responds to painful stimuli (nail bed depression – finger or toe nail).
U Unresponsive: Does not respond to ANY of the above. Completely unconscious

Rapid Tranquillisation Policy
Version 2.0 January 2019 24
6.0 Risks and Complications associated with Rapid Tranquillisation There are specific risks associated with the different classes of medications that are used in RT. The specific properties of the individual drugs should be taken into consideration. When combinations are used, risks may be compounded. Staffs need to be aware of the following: For benzodiazepines:
Loss of consciousness
Respiratory depression or arrest
Cardiovascular collapse (in patients receiving both Clozapine and Benzodiazepines)
For antipsychotics:
Loss of consciousness
Cardiovascular and respiratory complications and collapse
Seizures
Subjective experience of restlessness (akathisia)
Acute muscular rigidity (dystonia)
Involuntary movements (dyskinesia)
Neuroleptic malignant syndrome (NMS)
Excessive sedation 6.1 Circumstances for special care Extra care should be taken when implementing RT in the following circumstances:
The presence of congenital prolonged QTc syndromes
The concurrent prescription or use of other medication that lengthens QTc intervals both directly and indirectly
The presence of certain disorders affecting metabolism, such as hypo-and hyperthermia, stress and extreme emotions and extreme physical exertion
6.2 Observations After RT is administered, the following should be monitored:
Results of vital signs must be recorded on the NEWS Observation Chart (see appendix 1), nursing and medical notes
Scheduled observation and engagement levels should be assessed by a doctor, with nursing staff, and the frequency of observations following RT recorded in case notes. However it is recommended that;
Side effects, blood pressure, pulse, temperature, respiratory rate, level of hydration and level of consciousness should be monitored every 15 minutes for 1 hour after IM injections
After the first hour continue to monitor every 30 minutes until the patient becomes ambulatory and there are no further concerns.
If the patient is asleep the use of pulse oximetry to continuously monitor oxygen saturation is recommended
If the patient becomes unconscious or if there is an increase in NEWS score, care should be escalated following the clinical response table in Appendix 1. Refer to the Medical Emergency Flowchart (Appendix 2)

Rapid Tranquillisation Policy
Version 2.0 January 2019 25
Some observations may be difficult if a patient remains agitated or aggressive. Problems in this regard should be clearly documented and discussed with the prescriber or the clinical team
For further information regarding this please see the Management of Deteriorating Patient Policy
6.3 Remedial Measures
Monitoring by nursing staff is necessary to ensure complications and side effects are recognised
The NEWS observation chart is to be completed following Rapid Tranquillisation (appendix 1)
Where possible, baseline measurements should be recorded.
After any parenteral drug administration, you should monitor: temperature; pulse; blood pressure, respiratory rate, level of consciousness, level of hydration and side effects.
Every 15 minutes for 1 hour and then half hourly until patient is ambulatory. Record in notes.
Patients who refuse to have their vital signs monitored or who remain too behaviourally disturbed to be approached should have respiration and level of consciousness recorded and refused documented for other vitals. Also be vigilant for signs/symptoms of pyrexia, hypotension, over sedation and general physical well-being.
If the patient is asleep, the continuous use of pulse oximetry to measure oxygen saturation is desirable. A nurse should remain with the patient until ambulatory
Seek urgent medical advice if the patient deteriorates or is unconscious.
ECG and haematological monitoring are also strongly recommended when parenteral antipsychotics are given, especially when higher doses are used. Hypokalaemia, stress, and agitation place the patient at risk of cardiac arrhythmias. ECG monitoring is formally recommended for all patients receiving Haloperidol in any formulation
Please refer to table 3 on the following page for more guidance

Rapid Tranquillisation Policy
Version 2.0 January 2019 26
6.4 Table 3: Managing the Complications and Side Effects of Medication
Complication Symptom Management
Acute Dystonia / EPSE
Muscle spasms especially in the head and neck and can result in a forced sideways twisting of the neck. Laryngeal spasm, which leads to difficulty in swallowing and breathing. Oculogyric crisis is forced movement of the eyes usually upwards which the patient can’t reverse
Procyclidine 5-10mgs IM immediately Repeat if necessary after 20 minutes Max 20 mg in 24 hours (If not severe oral may be given)
Fall in blood pressure
(>30 mmHg orthostatic drop or <50 mmHg diastolic) characterised by light-headedness and dizziness
Give oxygen, lay patient flat, raise legs, and ensure patient is not lying face down monitor blood pressure
Irregular or slow pulse
Slow (<50/minute) or irregular pulse Refer to specialist medical care immediately
Increased temperature
Neuroleptic Malignant Syndrome (NMS) include fever, rigidity, confusion, fluctuating consciousness, fluctuating blood pressure, and tachycardia
Check creatinine kinase urgently Risk of NMS and perhaps arrhythmias – monitor closely, cool patient, and refer to ITU if continued or any other signs of NMS Withhold antipsychotics and seek urgent medical advice
Reduced respiratory rate
(< 10/minute) or oxygen saturation (< 90%) (Respiratory depression) (Flumazenil – to treat benzodiazepine induced respiratory depression – patients may become agitated, anxious or fearful on awakening. Seizures may occur in regular benzodiazepine users)
Seek urgent medical advice
Give oxygen, raise legs and ensure patient is not lying face down
Nurses in BCPFT are not IV trained, so Flumazenil will need to be administered by a doctor
If respiratory rate drops below 10/minute in a patient who has received Benzodiazepines, give Flumazenil (Stock in the emergency cupboard at Penn Hospital and the ‘out of hours’ cupboard at Edward Street Hospital, Hallam Street Hospital and Heath Lane Hospital) 1. 200mcg I.V. over 15 seconds 2. If consciousness not resumed within 60 seconds give 100mcg
over 10 seconds 3. Repeat at 60 second intervals. Maximum dose 1mg/24 hours
Continue to monitor after respiratory rate returns to normal
Flumazenil has a short duration of action so further doses may be required
Do not use in pts with epilepsy on long term benzodiazepines
Dose should be carefully titrated in hepatic impairment
If induced by other agent – mechanical ventilation will be required
Arrange transfer to ITU at Acute Hospital immediately

Rapid Tranquillisation Policy
Version 2.0 January 2019 27
7.0 Algorithm 2: Rapid Tranquillisation of the Acutely Disturbed / Violent Patient - Adolescents Aged > 12y Years
Developed in consultation with BCPFT CAMHS Consultants
Consider de-escalation techniques e.g. talking down, distractions, time out
Consult any Advance Decisions
Check Consent has been given
Try Oral Therapy (oral p.r.n)
Patient refusing oral / Rapid response required /
No response to oral
Try intramuscular injection (RT)
Oral p.r.n
Lorazepam 1 to 2mg
or Promethazine 12.5mg to 25mg
(Where the use of benzodiazepines is inappropriate)
And/or another from the list below Olanzapine 5mg
Risperidone 0.25mg to 1mg
* Haloperidol 1 to 5mg and Promethazine 12.5-25mg
(if known to tolerate typical antipsychotics)
Use formulation most appropriate to patient *Note ECG requirements
Rapid Tranquillisation (IM)
Drug (IM)
Lorazepam 500 micrograms to 1mg or
Promethazine 25-50mg
(Where the use of benzodiazepines is inappropriate)
/or * Haloperidol 1 to 5mg and Promethazine 12.5-25mg
(if known to tolerate typical antipsychotics, however avoid if antipsychotics are co-administered)
*Note ECG requirements
Monitor Patient
No response within 30 minutes
Review
ALLOW AT LEAST 30 MINUTES FOR I/M LORAZEPAM TO WORK.
If ineffective, repeat at same doses and allow a further 30 mins for effect.
Complex case – seek specialist advice from consultant for further options
Never mix two drugs in the same syringe. Always dilute lorazepam injection before use
No response
Rapid Tranquillisation Policy
Version 2.0 January 2019 28
7.1 Notes for prescribing Rapid Tranquillisation / oral p.r.n for adolescents
Evidence The best evidence for benefit over risk of harm is for IM lorazepam used alone and the
combination of IM haloperidol plus an IM promethazine. When IM haloperidol is combined with IM promethazine there is some suggestion that
risk of movement-related side effects may be reduced. In contrast, the combination of an IM benzodiazepine plus IM haloperidol does not
appear to be more effective than an IM lorazepam used alone. While IM haloperidol used alone is more effective than placebo, it clearly carries greater
risk of extrapyramidal and other side effects when compared with placebo or an IM lorazepam.
Choice depends on current treatment. If patient is established on antipsychotics, lorazepam may be used alone. If the patient uses ‘street drugs’ or already receives regular benzodiazepines, an
antipsychotic may be used alone.
Ensure procyclidine injection is available. Antipsychotics may cause acute dystonic reaction/EPSE.
Ensure flumazenil IV injection is available to reverse effects of lorazepam injection.
The maximum daily dose of haloperidol is either 10mg orally or 5mg by IM injection.
In adolescents, older than 12 years of age the recommended dose of promethazine 10-25mg (max 50mg/day).
There is a higher incidence of paradoxical disinhibition with benzodiazepines compared to adults.
Caution if using haloperidol if young person is unknown to services, or antipsychotic naive adolescent, as EPSE may be more common than in adults. Baseline ECG is strongly recommended.
In young people who are not Gillick competent, parents/carers should be informed of the situation and consent sought for such treatment. It is good practice to inform both the young person and their parents/carers. The use of many of these medicines in under 18 years is outside of their UK license and is therefore ‘off’ label prescribing. As such the prescriber responsibility and potential liability are increased. The young person and their patient/carer should be informed of the ‘off label’ use of medicines, and this should be documented in the patient’s notes. Refer to the trusts Unlicensed Medicines Policy.
8.0 Documentation Record any incident requiring rapid tranquillisation:
Documenting all care or treatment given clearly in the patients records and DATIX
Rapid tranquillisation physical observation chart is to be used to monitor vital signs
Where an incident has required the use of a physical intervention, a physical intervention monitoring form should be completed
Where an incident has required the use of seclusion, a seclusion monitoring form should be completed

Rapid Tranquillisation Policy
Version 2.0 January 2019 29
9.0 Post Incident Support and Debrief Following the use of RT, a debrief should be completed soon afterwards. Patients should be offered the opportunity to discuss their experiences to reduce the incidence and severity of trauma. The patient should be provided with a clear explanation of; the decision to use RT, the medication and its effects and a discussion of their experiences. The patient’s care plan should acknowledge his/her preferences and wishes should they become behaviourally disturbed again. The patient should also be offered the opportunity to write about their experience and be supported to do this. Where the patient would like the involvement of an independent body the nurse in-charge should ensure that advocacy services are contacted. A post-incident staff debrief should take place immediately or as soon as possible and at least within 72 hours of an episode of RT. A person not directly involved in the incident (such as staff from a different ward) should ideally lead the debrief, which should include a minimum of a nurse and a doctor. This meeting should be used to ensure that the appropriate documentation has been completed and to identify and address physical harm to patients or staff, ongoing risks and the emotional impact on patients and staff, including witnesses, with issues relating to the use of RT discussed and lessons incorporated into practice. Prescriptions for RT should be reviewed by the multidisciplinary team and, especially if used repeatedly, with appropriate changes made to regularly prescribed medication.
10.0 Procedures connected to this Policy There are no procedures connected to this policy.
11.0 Links to Relevant Legislation
Mental Health Act 1983 The Mental Health Act 1983 (which was substantially amended in 2007) is the law in England and Wales that allows people with a ‘mental disorder’ to be admitted to hospital, detained and treated without their consent – either for their own health and safety, or for the protection of other people. Mental Capacity Act 2005 Mental Capacity Act 2005, covering England and Wales, provides a statutory framework for people who lack capacity to make decisions for themselves, or who have capacity and want to make preparations for a time when they may lack capacity in the future. The Act
sets out who can take decisions, in which situations, and how they should go about this.
In addition - in some cases, people lack the capacity to consent to particular treatment or care that is recognised by others as being in their best interests, or which will protect them from harm. Where this care might involve depriving adults at risk of their liberty in either a hospital or a care home, extra safeguards have been introduced in law – Deprivation of Liberty Safeguards, to protect their rights and ensure that the care or treatment they receive is in their best interests. 11.1 Links to Relevant National Standards
Nice Guidelines Violence and Aggression NG10 (2015) This guideline has been developed to advise on the short-term management of violence and aggression in mental health, health and community settings in adults, children (aged 12 years or under) and young people (aged 13 to 17 years). This guideline updates and replaces NICE guideline CG25 (published February 2005).

Rapid Tranquillisation Policy
Version 2.0 January 2019 30
Nice Guidelines Psychosis and Schizophrenia CG178 (2014) This guideline has been developed to advise on the treatment and management of psychosis and schizophrenia in adults. The guideline recommendations have been developed by a multidisciplinary team of healthcare professionals, people with psychosis and schizophrenia, their carers and guideline methodologists after careful consideration of the best available evidence. It is intended that the guideline will be useful to clinicians and service commissioners in providing and planning high quality care for people with psychosis and schizophrenia while also emphasising the importance of the experience of care for people with psychosis and schizophrenia and their carers Nice Guidelines Bipolar Disorder CG185 (2014) This guideline, which updates the 2006 National Institute for Health and Care Excellence (NICE) guideline (NCCMH, 2006; NICE, 2006), has been developed to advise on the assessment and management of bipolar disorder in adults, children (aged under 13 years) and young people (aged 13 to 18 years) in primary and secondary care. It applies to people with bipolar I, bipolar II, mixed affective and rapid cycling disorders. Non-bipolar affective disorders are not covered because these are addressed by other guidelines.
11.2 Links to other key policies
Management of the Deteriorating Patient Policy The purpose of this policy is to ensure that clinical staffs working within the trust have a standardised approach to recognising changes in the patient’s normal physiology and responding quickly by alerting experienced help. Prevention and Management of Violence and Aggression including NHS sanctions The purpose of this policy is to detail the Trust’s strategy and legislative compliance in tackling violence and aggression against patients and staff. Seclusion Policy The purpose of this policy is to ensure that employees of the Trust have clear Directions related to the use of seclusion. The policy will also ensure that staffs work within the Mental Health Act 1983 Code of Practice. Clinical Observation Policy The purpose of this policy is to make clear the arrangements in place for the observation of patients and to provide direction and guidance to clinical staff in order to ensure safe levels of observation in clinical areas.
Rapid Tranquillisation Policy
Version 2.0 January 2019 31
12.0 Best Practice - Dissemination, Implementation and Monitoring of NICE Quality Standards and Guidance The purpose of these guidelines is to provide a clear process for responding effectively to the publication of NICE quality standards and national guidance, to ensure current practice reflects the best possible evidence and it is both clinically and cost effective.
13.0 References
Care Quality Commission Brief Guide BG040: Rapid Tranquillisation (by the parenteral route) in Mental Health March 2018
Patel M, Sethi F et al. Joint BAP NAPICU evidence-based consensus guidelines for the clinical management of acute disturbance: De-escalation and rapid tranquillisation. 2018. Journal of Psychopharmacology,1-40.
European Medicines Agency. 28th April 2017. Questions and answers on Haldol and associated names (haloperidol, oral solutions and injectable solution). Outcome of a procedure under Article 30 of Directive 2001/83/EC.
Mental Health Policy Implementation Guide: Developing Positive Practice to Support the Safe and Therapeutic Management of Aggression and Violence in Mental Health In-Patient Settings Department of Health (2004)
Taylor D, Barnes T, Young A. The Maudsley Prescribing Guidelines in Psychiatry. 13th Edition. 2018. Wiley-Blackwell.
British National Formulary. Accessed via https://www.medicinescomplete.com on 1st Sept 2018.
Mental Health Act Manual, 8th edition. Jones R. (2003)
Good Practice Guide for the management of Violence. Royal College of Psychiatrists. Maden & Ashead (2006)
Mental Health Act (1983) Code of Practice (1999)
Nice Guidelines Violence and Aggression: Short-Term Management in Mental health, Health and Community Settings NG10 (2015)
Nice Guidelines Psychosis and Schizophrenia in Adults: Treatment and Management CG178 (2014)
Nice Guidelines Bipolar Disorder: The Assessment and Management of Bipolar Disorder in Adults, Children and Young People in Primary and Secondary Care CG185 (2014)
National Early Warning Score (2012) – Royal College of Physicians
BSMHFT Rapid Tranquillisation Policy V10 2017
Sussex Partnership NHS Foundation Trust The Rapid Tranquillization Policy. (including the use of oral PRN medication) 2016

Rapid Tranquillisation Policy
Version 2.0 January 2019 32
14.0 Roles and Responsibilities for this Policy
Title Role Responsibilities
Executive Director of
Nursing, AHPs and Governance
Executive Lead
- Ensure the Trust’s management and use of rapid tranquillisation is discharged appropriately and has lead responsibility for the implementation of this policy
- Ensure a systematic and consistent approach to the use of rapid tranquillisation within inpatient areas - Bring any serious concerns regarding the implementation of this policy to the attention of the Board
Trust Board Strategic - Strategic overview and final responsibility for overseeing the use of rapid tranquillisation within inpatient areas across the
Trust
Executive Committee Accountable - Responsible for ensuring that the use of rapid tranquillisation is managed efficiently and effectively in accordance with the
Board’s Assurance Framework and strategic priorities
Quality & Safety Steering Group
Responsible - Responsible for overseeing the implementation of a systematic and consistent approach to the use of rapid tranquillisation - Provide exception and progress reports to the Executive Committee
Clinical Directors Lead
- Responsible for the use of rapid tranquillisation within their Group
- Lead discussions on the use of rapid tranquillisation at Group Quality & Safety Steering Group meetings - Oversee the completion of audits and subsequent action plans in respect of rapid tranquillisation
- Provide updates on the use of rapid tranquillisation within their Group to the Quality & Safety Steering Group
Group Quality &safety
steering groups Implementation
- Responsible for monitoring the use of rapid tranquillisation within their Group - Ensure all incidents of rapid tranquillisation are reported via Datix, the trust’s incident reporting procedure
- Monitor use of rapid tranquillisation on a case by case basis within each Group
- Report and discuss all incidents at monthly meetings of each Quality & Safety Steering Group - Receive results and recommendations of all related clinical audits
- Responsible for monitoring action plans to implement changes to current practice until completion
Medicines Management
Committee
Scrutiny and
Performance
- Monitor the frequency and any trends regarding the use of rapid tranquillisation and liaising with Group Quality & Safety
Steering Groups
Pharmacy Staff Monitor - Responsible for monitoring the safe and appropriate prescribing of medication
Group Directors and
Group Managers Operational Lead
- Responsible for ensuring that all managers are aware of the policy and promote good practice - Provide support and guidance regarding resources to enable this policy to be implemented
- Ensure nursing staff implement safe systems of work in accordance with the procedures referred to in the policy
Service Managers and
Ward Managers Operational
- Ensure they are familiar with this policy and be responsible for adhering to the procedures referred to - Ensure staff attend training applicable to their role and for implementing the guidance across their areas of responsibility
- Ensure aggressive/violent patients have primary and secondary behavioural management plans in place
- Ensure risk assessments of environmental health and safety factors that can reduce the likelihood of violence/aggression are carried out and plans are put in place to minimise them
- Ensure all incidents of rapid tranquillisation are reported

Rapid Tranquillisation Policy
Version 2.0 January 2019 33
Title Role Responsibilities
Nurses in Charge Operational - Responsible for safe administration of prescribed rapid tranquillisation medication and subsequent observations
- Report incidents associated with the use of rapid tranquillisation
Nursing Staff Adherence
- Ensure they use de-escalation skills and promote the well-being and dignity of the patient at all times
- Ensure they are familiar with the policy and be responsible for adhering to the procedures referred to within the policy - Ensure Advance Statements are considered and documented in CPA and Early Warning Signs care plans
- Provide support and information to patients and carers regarding the application of guidelines implemented to address
aggressive/violent incidents - Undertake risk assessments with patients where there is deemed a potential for aggressive/violent behaviour
- Develop primary and secondary behavioural management plans - Attend training applicable to their role
- Ensure they are aware of signs and symptoms of adverse reaction to medication to ensure patient safety is maintained
- Any delegated observation task remains the responsibility of the delegating nurse
Medical Staff Adherence
- Adhere to the prescribing requirements identified in the guidelines and the actions to take in the event of an adverse drug
reaction
- Always refer to the most up to date British National Formulary (BNF) to check recommended drugs and dosage - Consider any advanced directives
- Be available at the time of administration but no longer than 30 minutes after being requested - Be available to administer Flumazenil if needed
- Be part of a multi-disciplinary team (MDT), ensuring risk assessments are conducted with the patient where there is a potential for aggressive/violent behaviour
- Support the implementation and monitoring of this policy
- Be aware of any previous adverse reactions to medication - Advise on the levels of scheduled observation and engagement levels required following rapid tranquillisation
Practice Development
Team - Responsible for collating monthly incidents of the use of rapid tranquillisation and feeding back to service leads

Rapid Tranquillisation Policy
Version 2.0 January 2019 34
15.0 Training
16.0 Equality Impact Assessment The following statement should always be included Black Country Partnership NHS Foundation Trust is committed to ensuring that the way we provide services and the way we recruit and treat staff reflects individual needs, promotes equality and does not discriminate unfairly against any particular individual or group. The Equality Impact Assessment for this policy has been completed and is readily available on the Intranet. If you require this in a different format e.g. larger print, Braille, different languages or audio tape, please contact the Equality & Diversity Team on Ext. 8067 or email [email protected]
17.0 Data Protection and Freedom of Information Data Protection Act provides controls for the way information is handled and to gives legal rights to individuals in relation to the use of their data. It sets out strict rules for people who use or store data about individuals and gives rights to those people whose data has been collected. The law applies to all personal data held including electronic and manual records. The Information Commissioner’s Office has powers to enforce the Data Protection Act and can do this through the use of compulsory audits, warrants, notices and monetary penalties which can be up to €20million or 4% of the Trusts annual turnover for serious breaches of the Data Protection Act. In addition to this the Information Commissioner can limit or stop data processing activities where there has been a serious breach of the Act and there remains a risk to the data.
What aspect(s) of this policy will
require staff training?
Which staff groups require this
training?
Is this training covered in the Trust’s Mandatory and Risk
Management Training Needs Analysis document?
If no, how will the training be delivered?
Who will deliver the training?
How often will staff require
training
Who will ensure and monitor that staff have
this training?
Rapid
Tranquillisation
All inpatient
qualified nurses and Healthcare
Support Workers in
MH and LD
Yes Learning and
Development Team
Annually Workforce Development
Group
Observation of
patients
Inpatient Nurses
and Healthcare Support
Workers
Yes Learning and
Development Team
3 yearly Workforce Development
Group
Medicines Management
Inpatient Nurses & Medical
staff
Yes Learning and Development Team
2 yearly Workforce Development Group

Rapid Tranquillisation Policy
Version 2.0 January 2019 35
The Freedom of Information Act provides public access to information held by public authorities. The main principle behind freedom of information legislation is that people have a right to know about the activities of public authorities; unless there is a good reason for them not to. The Freedom of Information Act applies to corporate data and personal data generally cannot be released under this Act. All staffs have a responsibility to ensure that they do not disclose information about the Trust’s activities; this includes information about service users in its care, staff members and corporate documentation to unauthorised individuals. This responsibility applies whether you are currently employed or after your employment ends and in certain aspects of your personal life e.g. use of social networking sites etc. The Trust seeks to ensure a high level of transparency in all its business activities but reserves the right not to disclose information where relevant legislation applies. The Information Governance Team provides a central point for release of information under Data Protection and Freedom of Information following formal requests for information; any queries about the disclosure of information can be forwarded to the Information Governance Team. 18.0 Monitoring this policy is working in practice
What key elements will be monitored?
(measurable policy objectives)
Where described in
policy?
How will they be monitored?
(method + sample size)
Who will undertake this
monitoring?
How Frequently?
Group/Committee that will receive and
review results
Group/Committee to ensure actions are completed
Evidence this has happened
Rapid Tranquillisation is used in line with national guidance
and to meet our legal obligations
4.0 Process New NICE or national guidance/legislation,
reports of best practice or recommendations from an
external agency in respect
of rapid tranquillisation will be identified and
implemented in accordance with the Trust’s Best
Practice NICE and Dealing
with External Recommendations policies
Quality & Safety Steering Group
Monthly Group Quality & Safety Steering
Groups
Group Quality & Safety Steering
Groups
Reports and minutes of the
meetings
Clinical Directors, Group Quality & Safety Steering
Groups, nursing and medical
staff are discharging their responsibilities for rapid
Tranquillisation
7.0 Roles and Responsibiliti
es for this
Policy
Monitoring of all incidents of rapid tranquillisation
Quality & Safety Steering Group
Monthly Group Quality & Safety Steering
Groups
Group Quality & Safety Steering
Groups
Minutes of meetings and
monitoring
templates
Group Annual Audit Programmes and the
implementation of action plans
Quality & Safety Steering Group
Annually
Group Quality & Safety Steering
Groups
Group Quality & Safety Steering
Groups
Minutes of meetings and
monitoring templates

Rapid Tranquillisation Policy
Version 2.0 January 2019 36
What key elements will be
monitored? (measurable policy objectives)
Where
described in policy?
How will they be
monitored? (method + sample size)
Who will
undertake this monitoring?
How
Frequently?
Group/Committee
that will receive and review results
Group/Committee to ensure
actions are completed
Evidence this
has happened
Prescribing guidelines for rapid Tranquillisation
4.4 Prescribing
Guidelines
All incidents of rapid tranquillisation must be
reported via Datix, the trust’s incident reporting
procedure
Group Pharmacist monitors the
medication used for Rapid
Tranquillisation on
a case by case basis within each
Group
Monthly Medicines Management
Committee
Medicines Management
Committee
Reports and minutes of the
meetings
How observations are recorded, including
timeframes when patients have received rapid
Tranquillisation
4.6 Observations
4.7 Remedial Measures
Appendix 1
NEWS Observation
Chart
A detailed review of practice will be audited
Quality & Safety Steering Group
Monthly Group Quality & Safety Steering
Group and Medicines Management
Committee
Quality & Safety Steering Group
Sign off of action
plans/minutes of meetings
Arrangements for monitoring
service users who have
received rapid tranquillisation
4.6
Observations
4.7 Remedial Measures
Appendix 1 NEWS
Observation
Chart
A detailed review of
practice will be audited
Quality & Safety
Steering Group
Monthly Group Quality &
Safety Steering
Group and Medicines Management
Committee
Quality & Safety
Steering Group
Sign off of
action plans/
minutes of meetings
How the organisation trains
staff, in line with the training needs analysis
8.0 Training Report on percentage of
staff trained in all mandatory topics
Workforce
Development Group
Quarterly Group Management
Boards for Group compliance and
Workforce
Development Group for Trust compliance
Group
Management Boards for Group
compliance and
Workforce Development
Group for Trust compliance
Reports and
minutes of the meetings
8.0 Training Reports on identified ward/
departmental compliance, where performance falls
below 95% compliance
Workforce
Development Group
Quarterly Group Management
Boards for Group compliance and
Workforce Development Group
for Trust compliance
Group
Management Boards
Reports and
minutes of the meetings

Rapid Tranquillisation Policy
Version 2.0 January 2019 37
Appendix 1 Based on the observation chart for the National Early Warning Score (NEWS)
Note: Where observations are Refused, record as ‘R’
RAPID TRANQUILLISATION PHYSICAL OBSERVATION CHART Patient name Ward Date of birth
DATE Time monitoring initiated: Time monitoring stopped: TIME(24 hour)
CO
NTI
NU
E TO
MO
NIT
OR
UN
TIL
AM
BU
LATO
RY
Observations (minutes) 0 15 30 45 60 90 120 150 180 210 240 270 300 NEWS
TEM
P ≥39 c 2
TEM
P
38.1-39. c 1 36.1 - 38 c 35.1 - 36 c 1
≤35 c 3
BLO
OD
PR
ESSU
RE
(SY
STO
LIC
)
≥220 3 3
BLO
OD
PR
ESSU
RE
(SY
STO
LIC
)
211-219 201-210 191-200 181-190 171-180 161-170 151-160 141-150 131-140 121-130 111-120 101-110 1 1 91-100 2 2 81-90 3 3 71-80 3 3 61-70 3 3 51-60 3 3 ≤50 3 3
PU
LSE
≥131 3
PU
LSE
121-130 2 111-120 2 101-110 1 91-100 1 81-90 71-80 61-70 51-60 41-50 1 ≤40 3
RESP RATE
≥ 25
3
RES
P R
ATE
21-24 2 12-20 9-11 1 ≤ 8 3
SpO2
≥96 94-95 1 92-93 2 ≤91 3
Inspired O2 % Oxygen Saturation Oxygen
Saturation Conscious Level = Alert Conscious Level V/P/U=3 V/P/U=3
Hydrated (Y/N) Hydrated TOTAL NEW SCORE TOTAL
NEWS Escalation plan Y / N / n/a Escalation plan Sign/Initials Sign/Initials

Rapid Tranquillisation Policy
Version 2.0 January 2019 38
The National Early Warning Score (NEWS) and Triggers
Scores
Clinical Risk
0
Low Aggregate 1 – 4
RED score*
(Individual parameter scoring 3)
Medium
Aggregate 5 – 6
Aggregate 7
or more
High

Rapid Tranquillisation Policy
Version 2.0 January 2019 39
Outline Clinical Response to NEWS Triggers
NEWS SCORE
FREQUENCY OF MONITORING
CLINICAL RESPONSE
0 Minimum 12 hourly Continue routine NEWS monitoring with every set of observations
Total:
1-4
Minimum 4-6 hourly
Inform registered nurse who must assess the patient
Registered nurse to decide if increased frequency of monitoring and / or escalation of clinical care is required
Total:
5 or more or
3 in one parameter
Increased frequency to a minimum
of 1 hourly
Registered nurse to urgently inform the medical team caring for the patient; (within 1hour)
Urgent assessment by a clinician with core competencies to assess acutely ill patients
Clinical care in an environment with monitoring facilities; Consider transfer to acute hospital
Total: 7
or more
Continuous monitoring of vital signs
Registered nurse to immediately inform the medical team caring for the patient – this should be at least at Specialist Registrar level;
A HIGH NEWS SCORE OF 7 OR MORE REQUIRES URGENT TRANSFER TO AN ACUTE HOSPITAL (9-999)

Rapid Tranquillisation Policy
Version 2.0 January 2019 40
CLINICAL PRACTICE STANDARDS: Rapid Tranquillisation (RT) Checklist
(Based on POMH audit)
Checklist Questions Yes No Sign Date Comments
Has oral medication been offered before administering IM medication for behavioural disturbance?
Has physical monitoring post RT been recorded adequately on the physical observation chart?
Has a debrief been completed promptly post RT? This as a minimum should include a nurse and a doctor and address physical harms to patients or staff, ongoing risks and the emotional impact on patients and staff, including witnesses.
Has the patient’s written care plan addressed the management of future episodes of disturbed behaviour. This should be completed within a week.
Has the patient’s care plan acknowledged his/her preferences and wishes should they become behaviourally disturbed again? This should be completed within a week
If Haloperidol has been used as part of RT, has a recent ECG been completed.
QTc =______ms Date of ECG:________

Rapid Tranquillisation Policy
Version 2.0 January 2019 41
Appendix 2
MEDICAL EMERGENCY
NURSE DISCOVERING EMERGENCY TO SHOUT FOR HELP/ACTIVATE
ALARM
BREATHING?
YES NO
GIVE 100% OXYGEN VIA NON RE-
BREATHE O₂ MASK. USING
ABCDE APPROACH RECORD OBSERVATIONS RECORD NEWS SCORE
1 MEMBER OF STAFF TO CALL 9-999 1 MEMBER OF STAFF TO COLLECT
EMERGENCY BAG AND SUCTION UNIT IMMEDIATELY
ILS TRAINED MEMBER OF
STAFF TO LEAD TEAM
ARRIVAL OF AMBULANCE
LEAD NURSE TO HANDOVER TO
AMBULANCE CREW
CALL
MEDICAL STAFF
TREATMENT GIVEN
AMBULANCE REQUIRED CALL 9-999
POST INCIDENT
CLEAN AREA, REPLENISH EMERGENCY BAG
COMPLETE DATIX AND MED EMERGENCY FORM
DEBRIEF STAFF (Resus Officer to attend debrief)
START 30 CHEST COMPRESSIONS FOLLOWED BY 2
RESCUE BREATHS
ASSESS RESPONSE, AIRWAY
AND BREATHING

Rapid Tranquillisation Policy
Version 2.0 January 2019 42
Policy Details Corporate Governance only
* For more information on the consultation process, implementation plan, equality impact
assessment, or archiving arrangements, please contact Corporate Governance
Review and Amendment History
Version Date Details of Change
V2.0 Jan 2019 Reviewed in light of CQC guidance BG040; Update to physical monitoring proforma
V1.1
Aug 2015 New policy format and minor amendments- maximum daily doses for Haloperidol (oral and IM) amended and National Early warning scoring system added
V1.0 Nov 2012 Alignment of policies following TCS
Title of Policy Rapid Tranquillisation Policy
Unique Identifier for this policy BCPFT-CB-POL-09
State if policy is New or Revised Revised
Previous Policy Title where applicable N/A
Policy Category Clinical, HR, H&S, Infection Control etc.
Challenging Behaviour Policy
Executive Director whose portfolio this policy comes under
Executive Director of Nursing, AHPs and Governance
Policy Lead/Author Job titles only
Deputy Chief Pharmacist / Chief Pharmacist
Committee/Group responsible for the approval of this policy
Medicines Management Committee
Month/year consultation process completed *
n/a
Month/year policy approved January 2019
Month/year policy ratified and issued March 2019
Next review date January 2022
Implementation Plan completed * Yes
Equality Impact Assessment completed * Yes
Previous version(s) archived * Yes
Disclosure status ‘B’ can be disclosed to patients and the public
Key Words for this policy
‘National Early Warning Score’, ‘NEWS’, ‘Lorazepam’, ‘Haloperidol’, ‘Olanzapine’, ‘Promethazine’, ‘Zuclopenthixol Acetate’, ‘Oral’, ‘IM’, ‘advance statement’, ‘seclusion’, ‘light sedation’
Related Documents











