European Journal of Radiology 51 (2004) 139–149 Radiological manifestations of pulmonary tuberculosis J. Andreu ∗ , J. Cáceres, E. Pallisa, M. Martinez-Rodriguez Department of Radiology, HGU Vall d’Hebron, Universitat Autónoma de Barcelona, Paseo Vall d’Hebron 116, Barcelona 08032, Spain Received 23 February 2004; received in revised form 26 February 2004; accepted 1 March 2004 Abstract Pulmonary tuberculosis (TB) is a common worldwide lung infection. The radiological features show considerable variation, but in most cases they are characteristic enough to suggest the diagnosis. Classically, tuberculosis is divided into primary, common in childhood, and postprimary, usually presenting in adults. The most characteristic radiological feature in primary tuberculosis is lymphadenopathy. On enhanced CT, hilar and mediastinal nodes with a central hypodense area suggest the diagnosis. Cavitation is the hallmark of postprimary tuberculosis and appears in around half of patients. Patchy, poorly defined consolidation in the apical and posterior segments of the upper lobes, and in the superior segment of the lower lobe is also commonly observed. Several complications are associated with tuberculous infection, such as hematogenous dissemination (miliary tuberculosis) or extension to the pleura, resulting in pleural effusion. Late complications of tuberculosis comprise a heterogeneous group of processes including tuberculoma, bronchial stenosis bronchiectasis, broncholithiasis, aspergilloma, bronchoesophageal fistula and fibrosing mediastinitis. Radiology provides essential information for the management and follow up of these patients and is extremely valuable for monitoring complications. © 2004 Elsevier Ireland Ltd. All rights reserved. Keywords: Lung diseases; Lung infection; Pulmonary tuberculosis 1. Introduction Pulmonary tuberculosis (TB) is a common lung infection worldwide, presenting characteristics that make the specific diagnosis important. It has a long, well-defined treatment that is different from those applied in other bacterial infec- tions. Its clinical form of presentation is insidious and early diagnosis is often difficult if the process is not suspected on radiological findings. Early treatment is important to reduce the morbidity and mortality associated with the process. The incidence of TB is quite heterogeneous geographi- cally. A slow reduction was seen in developed countries un- til the mid-1980s when the AIDS epidemic caused a marked increase in the disease. Despite the current control of AIDS, this infection has not decreased, a fact that has been related to high worldwide immigration. Clinically, TB presents with systemic manifestations, including fever, malaise and weight loss, which are often attributed to concomitant processes such as HIV infection, alcoholism or malnutrition. The fever is not very high and ∗ Corresponding author. E-mail address: [email protected] (J. Andreu). is usually well tolerated. Other common clinical features are cough, hemoptoic expectoration or hemoptisis [1]. The radiological features show considerable variation, but in most cases they are characteristic enough to suggest the diagnosis. Definite diagnosis is based on isolation or culture of the bacillus, usually in sputum samples [2]. Chest radio- graphy is the most useful tool for managing lung infections and plain film results are sufficient for tuberculosis in most cases. Nevertheless, CT has an increasingly clearer role: to provide diagnostic findings in cases where the chest radio- graph is normal or inconclusive [3], to control the activity and evolution of the pulmonary process, and to detection complications. Classically, tuberculosis is divided in two forms: primary and postprimary. These groups not only represent clinically different processes, but also different radiological presenta- tions [2]. 2. Primary tuberculosis Primary TB is common in the pediatric age group, but in areas where the disease is not prevalent, the primary form 0720-048X/$ – see front matter © 2004 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.ejrad.2004.03.009

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

European Journal of Radiology 51 (2004) 139–149
Radiological manifestations of pulmonary tuberculosis
J. Andreu∗, J. Cáceres, E. Pallisa, M. Martinez-Rodriguez
Department of Radiology, HGU Vall d’Hebron, Universitat Autónoma de Barcelona, Paseo Vall d’Hebron 116, Barcelona 08032, Spain
Received 23 February 2004; received in revised form 26 February 2004; accepted 1 March 2004
Abstract
Pulmonary tuberculosis (TB) is a common worldwide lung infection. The radiological features show considerable variation, but in mostcases they are characteristic enough to suggest the diagnosis. Classically, tuberculosis is divided intoprimary, common in childhood, andpostprimary,usually presenting in adults. The most characteristic radiological feature in primary tuberculosis is lymphadenopathy. Onenhanced CT, hilar and mediastinal nodes with a central hypodense area suggest the diagnosis. Cavitation is the hallmark of postprimarytuberculosis and appears in around half of patients. Patchy, poorly defined consolidation in the apical and posterior segments of the upperlobes, and in the superior segment of the lower lobe is also commonly observed.
Several complications are associated with tuberculous infection, such as hematogenous dissemination (miliary tuberculosis) or extension tothe pleura, resulting in pleural effusion. Late complications of tuberculosis comprise a heterogeneous group of processes including tuberculoma,bronchial stenosis bronchiectasis, broncholithiasis, aspergilloma, bronchoesophageal fistula and fibrosing mediastinitis.
Radiology provides essential information for the management and follow up of these patients and is extremely valuable for monitoringcomplications.© 2004 Elsevier Ireland Ltd. All rights reserved.
Keywords:Lung diseases; Lung infection; Pulmonary tuberculosis
1. Introduction
Pulmonary tuberculosis (TB) is a common lung infectionworldwide, presenting characteristics that make the specificdiagnosis important. It has a long, well-defined treatmentthat is different from those applied in other bacterial infec-tions. Its clinical form of presentation is insidious and earlydiagnosis is often difficult if the process is not suspected onradiological findings. Early treatment is important to reducethe morbidity and mortality associated with the process.
The incidence of TB is quite heterogeneous geographi-cally. A slow reduction was seen in developed countries un-til the mid-1980s when the AIDS epidemic caused a markedincrease in the disease. Despite the current control of AIDS,this infection has not decreased, a fact that has been relatedto high worldwide immigration.
Clinically, TB presents with systemic manifestations,including fever, malaise and weight loss, which are oftenattributed to concomitant processes such as HIV infection,alcoholism or malnutrition. The fever is not very high and
∗ Corresponding author.E-mail address:[email protected] (J. Andreu).
is usually well tolerated. Other common clinical featuresare cough, hemoptoic expectoration or hemoptisis[1].
The radiological features show considerable variation, butin most cases they are characteristic enough to suggest thediagnosis. Definite diagnosis is based on isolation or cultureof the bacillus, usually in sputum samples[2]. Chest radio-graphy is the most useful tool for managing lung infectionsand plain film results are sufficient for tuberculosis in mostcases. Nevertheless, CT has an increasingly clearer role: toprovide diagnostic findings in cases where the chest radio-graph is normal or inconclusive[3], to control the activityand evolution of the pulmonary process, and to detectioncomplications.
Classically, tuberculosis is divided in two forms: primaryand postprimary. These groups not only represent clinicallydifferent processes, but also different radiological presenta-tions [2].
2. Primary tuberculosis
Primary TB is common in the pediatric age group, but inareas where the disease is not prevalent, the primary form
0720-048X/$ – see front matter © 2004 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.ejrad.2004.03.009
140 J. Andreu et al. / European Journal of Radiology 51 (2004) 139–149
may represent up to a quarter of adult TB cases[4], and sinceit is not expected, it is often misdiagnosed[5]. Few clini-cal symptoms are present and the disease is often asymp-tomatic. In HIV-infected patients with fewer than 200 CD4cells/mm3, tuberculosis develops along a primary pattern[6].
In primary tuberculosis, the histologic features are notspecific because there has been no previous contact withthe tuberculosis bacillus. The bacillus enters the airwaysand reaches the alveoli where a usually small lung infil-trate is produced. Subsequently, the bacilli disseminate alongthe lymphatic system to the hilar and mediastinal nodes.The parenchyma presents infiltrates or consolidations that
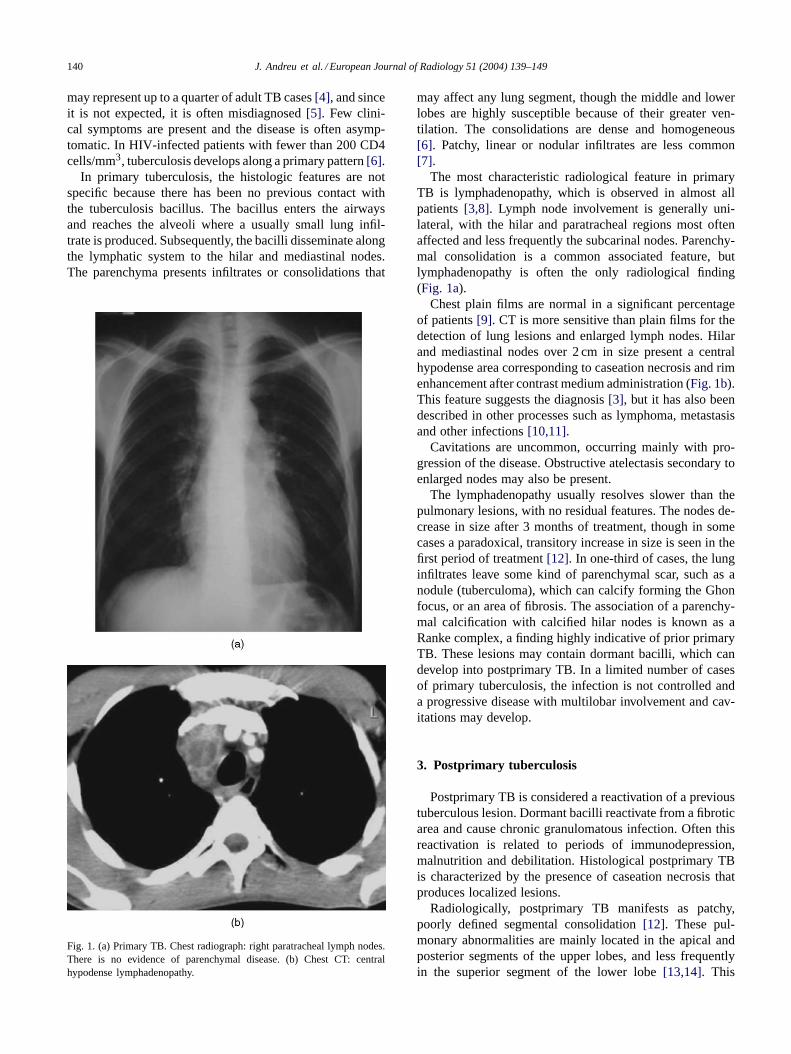
Fig. 1. (a) Primary TB. Chest radiograph: right paratracheal lymph nodes.There is no evidence of parenchymal disease. (b) Chest CT: centralhypodense lymphadenopathy.
may affect any lung segment, though the middle and lowerlobes are highly susceptible because of their greater ven-tilation. The consolidations are dense and homogeneous[6]. Patchy, linear or nodular infiltrates are less common[7].
The most characteristic radiological feature in primaryTB is lymphadenopathy, which is observed in almost allpatients[3,8]. Lymph node involvement is generally uni-lateral, with the hilar and paratracheal regions most oftenaffected and less frequently the subcarinal nodes. Parenchy-mal consolidation is a common associated feature, butlymphadenopathy is often the only radiological finding(Fig. 1a).
Chest plain films are normal in a significant percentageof patients[9]. CT is more sensitive than plain films for thedetection of lung lesions and enlarged lymph nodes. Hilarand mediastinal nodes over 2 cm in size present a centralhypodense area corresponding to caseation necrosis and rimenhancement after contrast medium administration (Fig. 1b).This feature suggests the diagnosis[3], but it has also beendescribed in other processes such as lymphoma, metastasisand other infections[10,11].
Cavitations are uncommon, occurring mainly with pro-gression of the disease. Obstructive atelectasis secondary toenlarged nodes may also be present.
The lymphadenopathy usually resolves slower than thepulmonary lesions, with no residual features. The nodes de-crease in size after 3 months of treatment, though in somecases a paradoxical, transitory increase in size is seen in thefirst period of treatment[12]. In one-third of cases, the lunginfiltrates leave some kind of parenchymal scar, such as anodule (tuberculoma), which can calcify forming the Ghonfocus, or an area of fibrosis. The association of a parenchy-mal calcification with calcified hilar nodes is known as aRanke complex, a finding highly indicative of prior primaryTB. These lesions may contain dormant bacilli, which candevelop into postprimary TB. In a limited number of casesof primary tuberculosis, the infection is not controlled anda progressive disease with multilobar involvement and cav-itations may develop.
3. Postprimary tuberculosis
Postprimary TB is considered a reactivation of a previoustuberculous lesion. Dormant bacilli reactivate from a fibroticarea and cause chronic granulomatous infection. Often thisreactivation is related to periods of immunodepression,malnutrition and debilitation. Histological postprimary TBis characterized by the presence of caseation necrosis thatproduces localized lesions.
Radiologically, postprimary TB manifests as patchy,poorly defined segmental consolidation[12]. These pul-monary abnormalities are mainly located in the apical andposterior segments of the upper lobes, and less frequentlyin the superior segment of the lower lobe[13,14]. This
J. Andreu et al. / European Journal of Radiology 51 (2004) 139–149 141
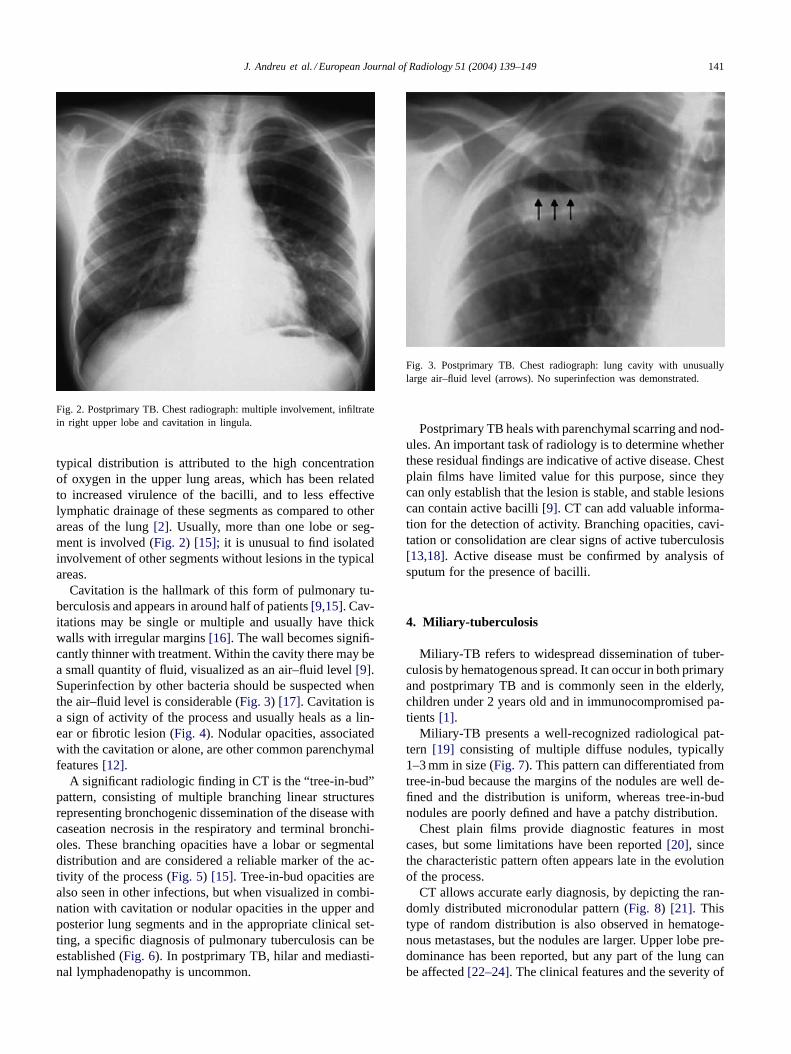
Fig. 2. Postprimary TB. Chest radiograph: multiple involvement, infiltratein right upper lobe and cavitation in lingula.
typical distribution is attributed to the high concentrationof oxygen in the upper lung areas, which has been relatedto increased virulence of the bacilli, and to less effectivelymphatic drainage of these segments as compared to otherareas of the lung[2]. Usually, more than one lobe or seg-ment is involved (Fig. 2) [15]; it is unusual to find isolatedinvolvement of other segments without lesions in the typicalareas.
Cavitation is the hallmark of this form of pulmonary tu-berculosis and appears in around half of patients[9,15]. Cav-itations may be single or multiple and usually have thickwalls with irregular margins[16]. The wall becomes signifi-cantly thinner with treatment. Within the cavity there may bea small quantity of fluid, visualized as an air–fluid level[9].Superinfection by other bacteria should be suspected whenthe air–fluid level is considerable (Fig. 3) [17]. Cavitation isa sign of activity of the process and usually heals as a lin-ear or fibrotic lesion (Fig. 4). Nodular opacities, associatedwith the cavitation or alone, are other common parenchymalfeatures[12].
A significant radiologic finding in CT is the “tree-in-bud”pattern, consisting of multiple branching linear structuresrepresenting bronchogenic dissemination of the disease withcaseation necrosis in the respiratory and terminal bronchi-oles. These branching opacities have a lobar or segmentaldistribution and are considered a reliable marker of the ac-tivity of the process (Fig. 5) [15]. Tree-in-bud opacities arealso seen in other infections, but when visualized in combi-nation with cavitation or nodular opacities in the upper andposterior lung segments and in the appropriate clinical set-ting, a specific diagnosis of pulmonary tuberculosis can beestablished (Fig. 6). In postprimary TB, hilar and mediasti-nal lymphadenopathy is uncommon.
Fig. 3. Postprimary TB. Chest radiograph: lung cavity with unusuallylarge air–fluid level (arrows). No superinfection was demonstrated.
Postprimary TB heals with parenchymal scarring and nod-ules. An important task of radiology is to determine whetherthese residual findings are indicative of active disease. Chestplain films have limited value for this purpose, since theycan only establish that the lesion is stable, and stable lesionscan contain active bacilli[9]. CT can add valuable informa-tion for the detection of activity. Branching opacities, cavi-tation or consolidation are clear signs of active tuberculosis[13,18]. Active disease must be confirmed by analysis ofsputum for the presence of bacilli.
4. Miliary-tuberculosis
Miliary-TB refers to widespread dissemination of tuber-culosis by hematogenous spread. It can occur in both primaryand postprimary TB and is commonly seen in the elderly,children under 2 years old and in immunocompromised pa-tients[1].
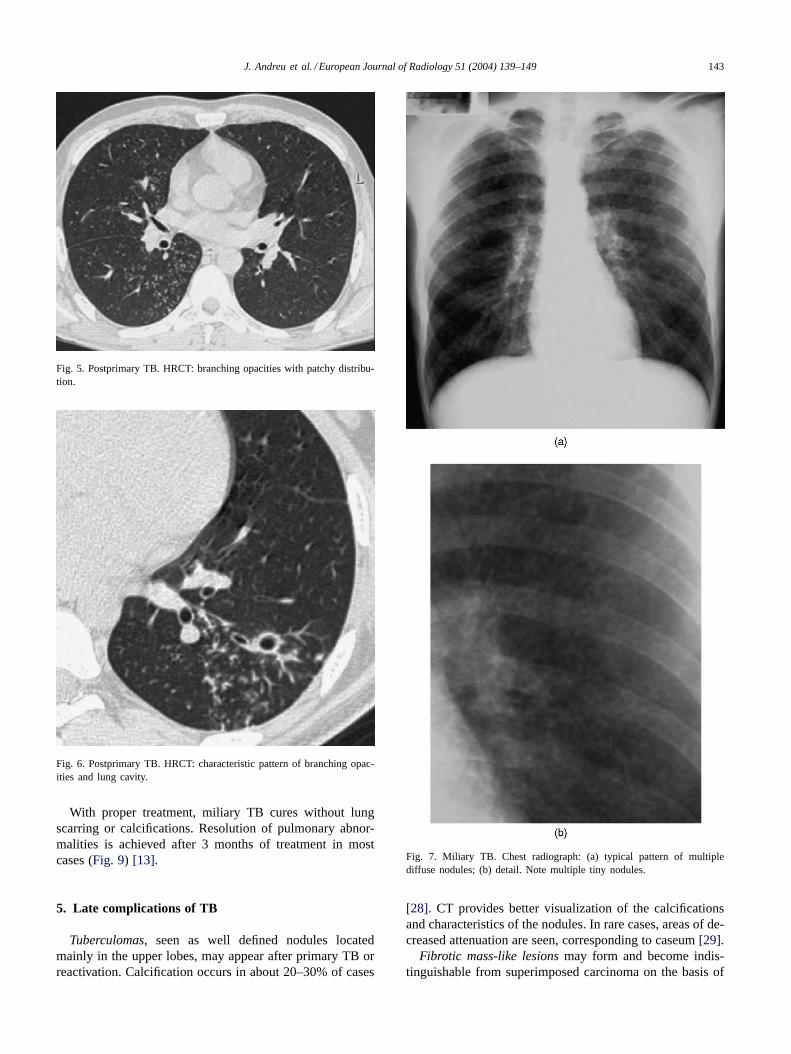
Miliary-TB presents a well-recognized radiological pat-tern [19] consisting of multiple diffuse nodules, typically1–3 mm in size (Fig. 7). This pattern can differentiated fromtree-in-bud because the margins of the nodules are well de-fined and the distribution is uniform, whereas tree-in-budnodules are poorly defined and have a patchy distribution.
Chest plain films provide diagnostic features in mostcases, but some limitations have been reported[20], sincethe characteristic pattern often appears late in the evolutionof the process.
CT allows accurate early diagnosis, by depicting the ran-domly distributed micronodular pattern (Fig. 8) [21]. Thistype of random distribution is also observed in hematoge-nous metastases, but the nodules are larger. Upper lobe pre-dominance has been reported, but any part of the lung canbe affected[22–24]. The clinical features and the severity of
142 J. Andreu et al. / European Journal of Radiology 51 (2004) 139–149
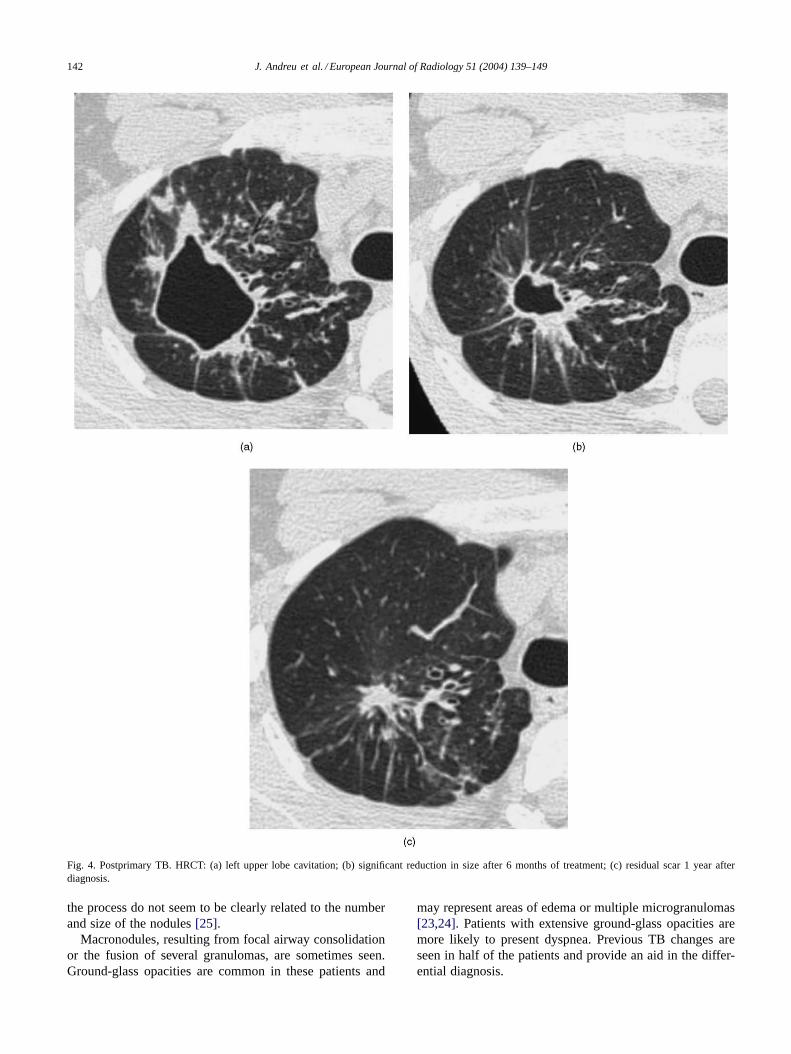
Fig. 4. Postprimary TB. HRCT: (a) left upper lobe cavitation; (b) significant reduction in size after 6 months of treatment; (c) residual scar 1 year afterdiagnosis.
the process do not seem to be clearly related to the numberand size of the nodules[25].
Macronodules, resulting from focal airway consolidationor the fusion of several granulomas, are sometimes seen.Ground-glass opacities are common in these patients and
may represent areas of edema or multiple microgranulomas[23,24]. Patients with extensive ground-glass opacities aremore likely to present dyspnea. Previous TB changes areseen in half of the patients and provide an aid in the differ-ential diagnosis.
J. Andreu et al. / European Journal of Radiology 51 (2004) 139–149 143
Fig. 5. Postprimary TB. HRCT: branching opacities with patchy distribu-tion.
Fig. 6. Postprimary TB. HRCT: characteristic pattern of branching opac-ities and lung cavity.
With proper treatment, miliary TB cures without lungscarring or calcifications. Resolution of pulmonary abnor-malities is achieved after 3 months of treatment in mostcases (Fig. 9) [13].
5. Late complications of TB
Tuberculomas, seen as well defined nodules locatedmainly in the upper lobes, may appear after primary TB orreactivation. Calcification occurs in about 20–30% of cases
Fig. 7. Miliary TB. Chest radiograph: (a) typical pattern of multiplediffuse nodules; (b) detail. Note multiple tiny nodules.
[28]. CT provides better visualization of the calcificationsand characteristics of the nodules. In rare cases, areas of de-creased attenuation are seen, corresponding to caseum[29].
Fibrotic mass-like lesionsmay form and become indis-tinguishable from superimposed carcinoma on the basis of
144 J. Andreu et al. / European Journal of Radiology 51 (2004) 139–149
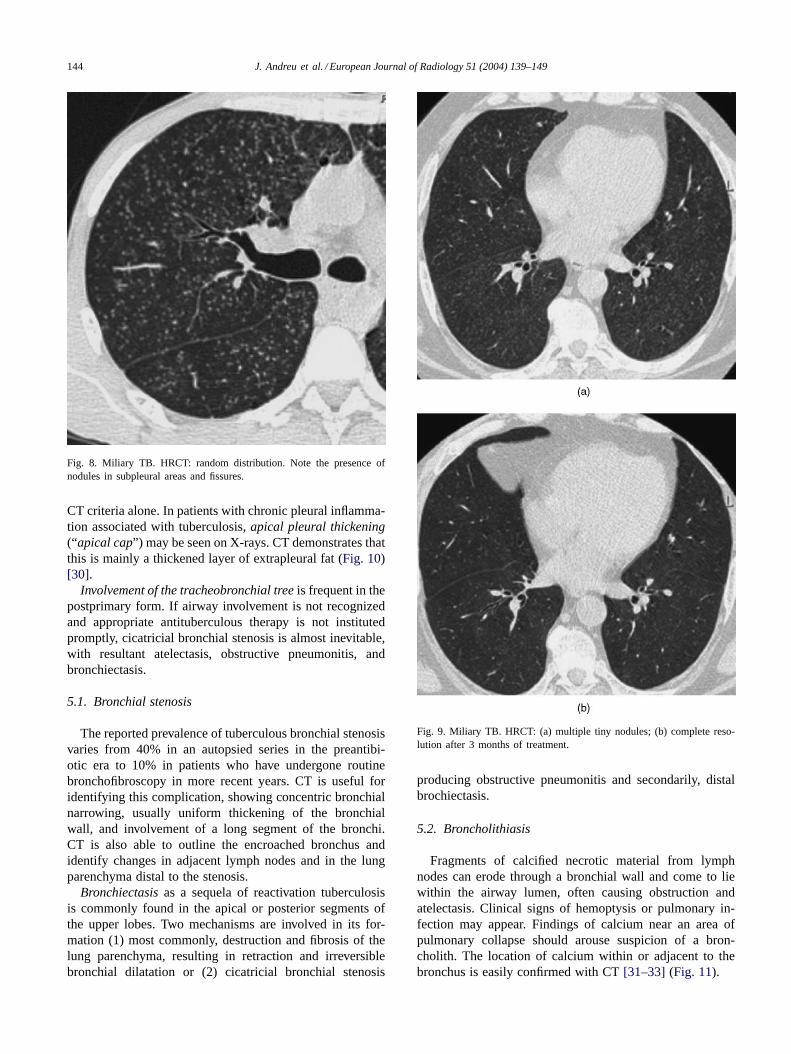
Fig. 8. Miliary TB. HRCT: random distribution. Note the presence ofnodules in subpleural areas and fissures.
CT criteria alone. In patients with chronic pleural inflamma-tion associated with tuberculosis,apical pleural thickening(“apical cap”) may be seen on X-rays. CT demonstrates thatthis is mainly a thickened layer of extrapleural fat (Fig. 10)[30].
Involvement of the tracheobronchial treeis frequent in thepostprimary form. If airway involvement is not recognizedand appropriate antituberculous therapy is not institutedpromptly, cicatricial bronchial stenosis is almost inevitable,with resultant atelectasis, obstructive pneumonitis, andbronchiectasis.
5.1. Bronchial stenosis
The reported prevalence of tuberculous bronchial stenosisvaries from 40% in an autopsied series in the preantibi-otic era to 10% in patients who have undergone routinebronchofibroscopy in more recent years. CT is useful foridentifying this complication, showing concentric bronchialnarrowing, usually uniform thickening of the bronchialwall, and involvement of a long segment of the bronchi.CT is also able to outline the encroached bronchus andidentify changes in adjacent lymph nodes and in the lungparenchyma distal to the stenosis.
Bronchiectasisas a sequela of reactivation tuberculosisis commonly found in the apical or posterior segments ofthe upper lobes. Two mechanisms are involved in its for-mation (1) most commonly, destruction and fibrosis of thelung parenchyma, resulting in retraction and irreversiblebronchial dilatation or (2) cicatricial bronchial stenosis
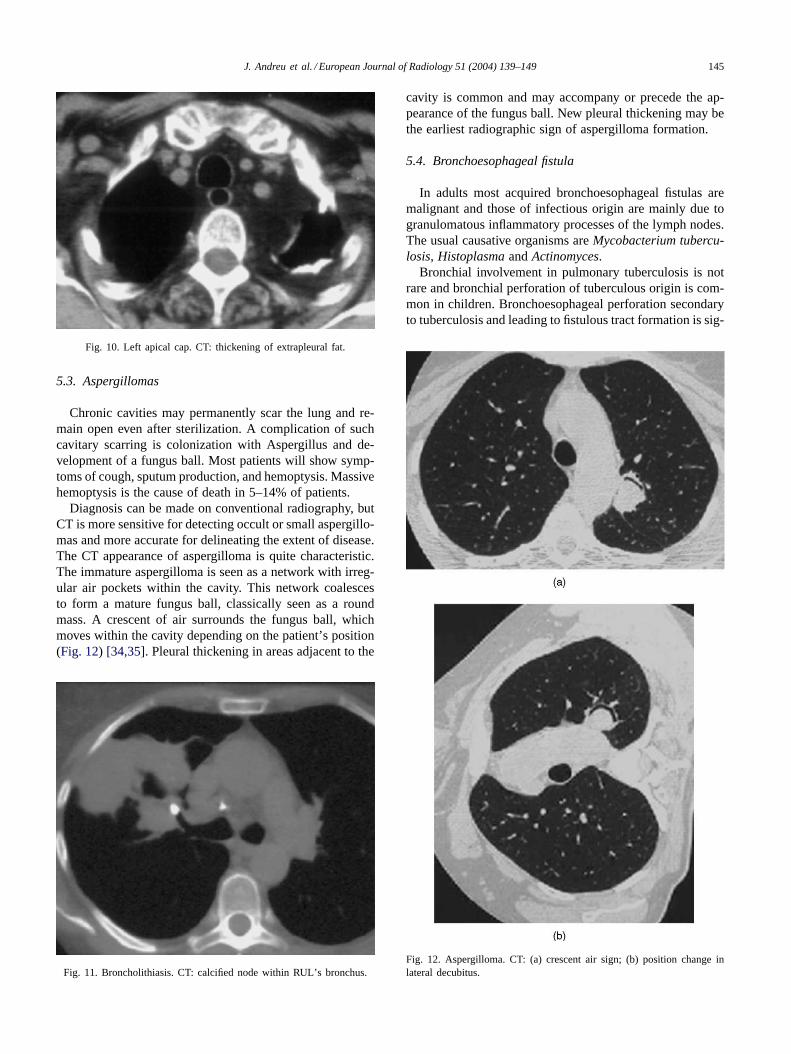
Fig. 9. Miliary TB. HRCT: (a) multiple tiny nodules; (b) complete reso-lution after 3 months of treatment.
producing obstructive pneumonitis and secondarily, distalbrochiectasis.
5.2. Broncholithiasis
Fragments of calcified necrotic material from lymphnodes can erode through a bronchial wall and come to liewithin the airway lumen, often causing obstruction andatelectasis. Clinical signs of hemoptysis or pulmonary in-fection may appear. Findings of calcium near an area ofpulmonary collapse should arouse suspicion of a bron-cholith. The location of calcium within or adjacent to thebronchus is easily confirmed with CT[31–33] (Fig. 11).
J. Andreu et al. / European Journal of Radiology 51 (2004) 139–149 145
Fig. 10. Left apical cap. CT: thickening of extrapleural fat.
5.3. Aspergillomas
Chronic cavities may permanently scar the lung and re-main open even after sterilization. A complication of suchcavitary scarring is colonization with Aspergillus and de-velopment of a fungus ball. Most patients will show symp-toms of cough, sputum production, and hemoptysis. Massivehemoptysis is the cause of death in 5–14% of patients.
Diagnosis can be made on conventional radiography, butCT is more sensitive for detecting occult or small aspergillo-mas and more accurate for delineating the extent of disease.The CT appearance of aspergilloma is quite characteristic.The immature aspergilloma is seen as a network with irreg-ular air pockets within the cavity. This network coalescesto form a mature fungus ball, classically seen as a roundmass. A crescent of air surrounds the fungus ball, whichmoves within the cavity depending on the patient’s position(Fig. 12) [34,35]. Pleural thickening in areas adjacent to the
Fig. 11. Broncholithiasis. CT: calcified node within RUL’s bronchus.
cavity is common and may accompany or precede the ap-pearance of the fungus ball. New pleural thickening may bethe earliest radiographic sign of aspergilloma formation.
5.4. Bronchoesophageal fistula
In adults most acquired bronchoesophageal fistulas aremalignant and those of infectious origin are mainly due togranulomatous inflammatory processes of the lymph nodes.The usual causative organisms areMycobacterium tubercu-losis, HistoplasmaandActinomyces.
Bronchial involvement in pulmonary tuberculosis is notrare and bronchial perforation of tuberculous origin is com-mon in children. Bronchoesophageal perforation secondaryto tuberculosis and leading to fistulous tract formation is sig-
Fig. 12. Aspergilloma. CT: (a) crescent air sign; (b) position change inlateral decubitus.
146 J. Andreu et al. / European Journal of Radiology 51 (2004) 139–149
nificantly rarer. The diagnosis of bronchoesophageal fistulais usually made with a barium esophagogram, which showsthe fistulous communication between the esophagus and thebronchi.
5.5. Fibrosing mediastinitis
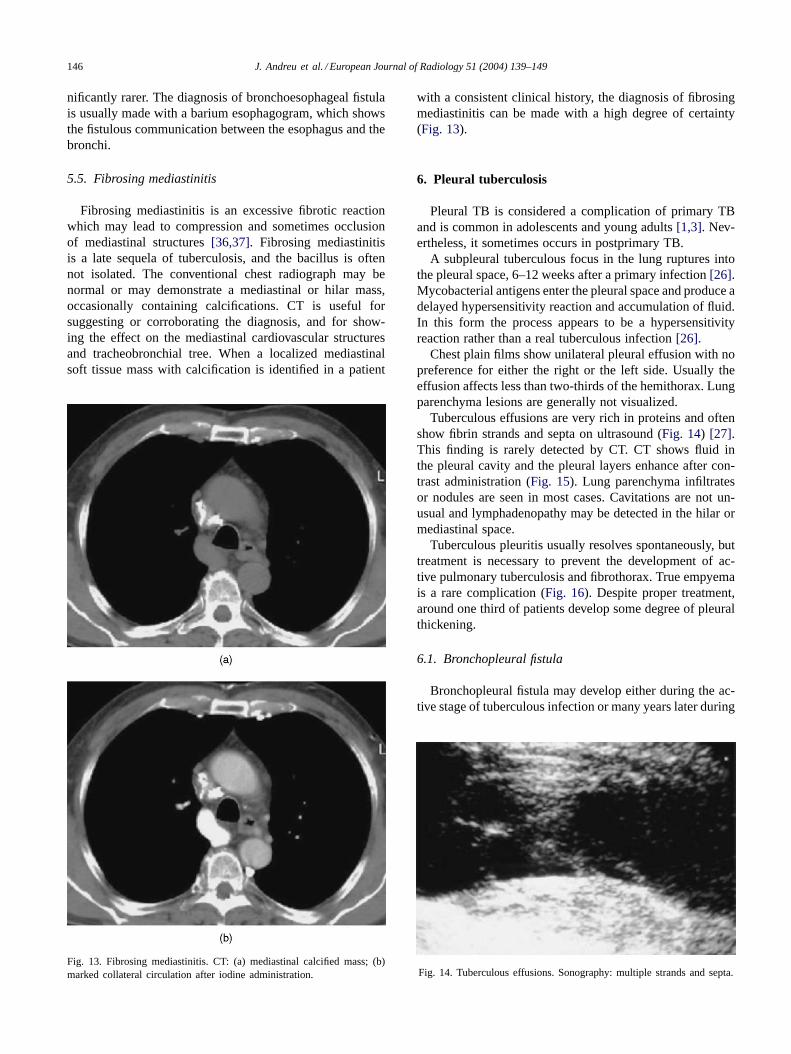
Fibrosing mediastinitis is an excessive fibrotic reactionwhich may lead to compression and sometimes occlusionof mediastinal structures[36,37]. Fibrosing mediastinitisis a late sequela of tuberculosis, and the bacillus is oftennot isolated. The conventional chest radiograph may benormal or may demonstrate a mediastinal or hilar mass,occasionally containing calcifications. CT is useful forsuggesting or corroborating the diagnosis, and for show-ing the effect on the mediastinal cardiovascular structuresand tracheobronchial tree. When a localized mediastinalsoft tissue mass with calcification is identified in a patient
Fig. 13. Fibrosing mediastinitis. CT: (a) mediastinal calcified mass; (b)marked collateral circulation after iodine administration.
with a consistent clinical history, the diagnosis of fibrosingmediastinitis can be made with a high degree of certainty(Fig. 13).
6. Pleural tuberculosis
Pleural TB is considered a complication of primary TBand is common in adolescents and young adults[1,3]. Nev-ertheless, it sometimes occurs in postprimary TB.
A subpleural tuberculous focus in the lung ruptures intothe pleural space, 6–12 weeks after a primary infection[26].Mycobacterial antigens enter the pleural space and produce adelayed hypersensitivity reaction and accumulation of fluid.In this form the process appears to be a hypersensitivityreaction rather than a real tuberculous infection[26].
Chest plain films show unilateral pleural effusion with nopreference for either the right or the left side. Usually theeffusion affects less than two-thirds of the hemithorax. Lungparenchyma lesions are generally not visualized.
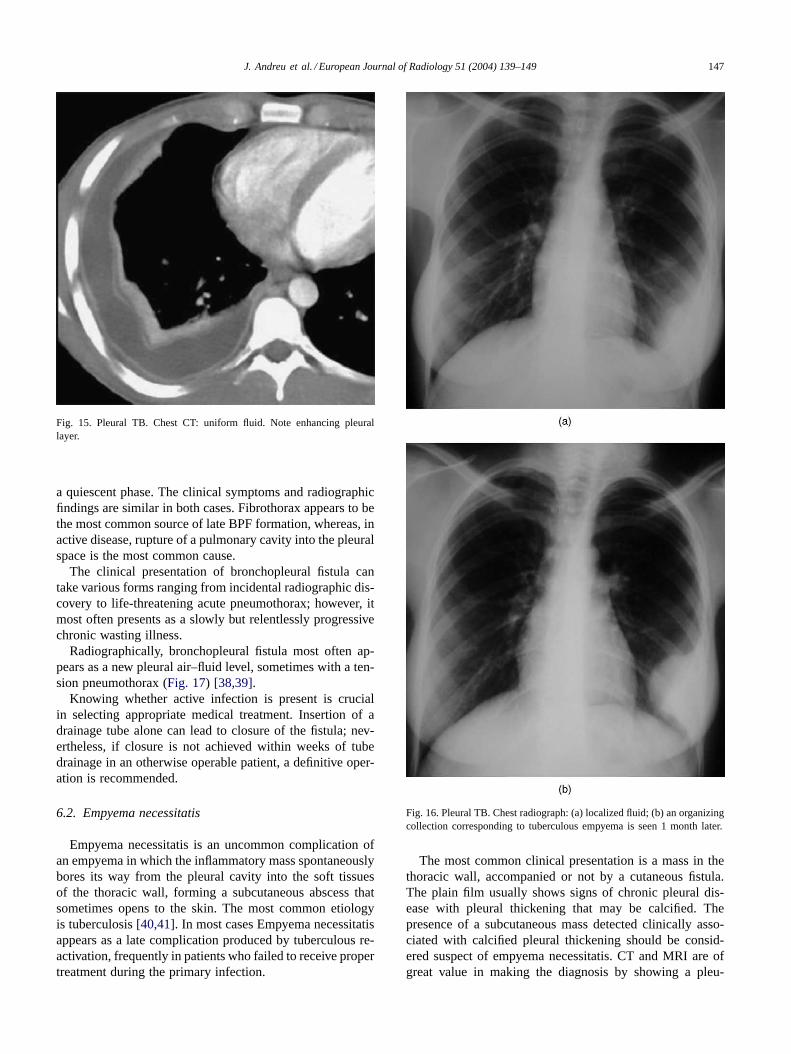
Tuberculous effusions are very rich in proteins and oftenshow fibrin strands and septa on ultrasound (Fig. 14) [27].This finding is rarely detected by CT. CT shows fluid inthe pleural cavity and the pleural layers enhance after con-trast administration (Fig. 15). Lung parenchyma infiltratesor nodules are seen in most cases. Cavitations are not un-usual and lymphadenopathy may be detected in the hilar ormediastinal space.
Tuberculous pleuritis usually resolves spontaneously, buttreatment is necessary to prevent the development of ac-tive pulmonary tuberculosis and fibrothorax. True empyemais a rare complication (Fig. 16). Despite proper treatment,around one third of patients develop some degree of pleuralthickening.
6.1. Bronchopleural fistula
Bronchopleural fistula may develop either during the ac-tive stage of tuberculous infection or many years later during
Fig. 14. Tuberculous effusions. Sonography: multiple strands and septa.
J. Andreu et al. / European Journal of Radiology 51 (2004) 139–149 147
Fig. 15. Pleural TB. Chest CT: uniform fluid. Note enhancing pleurallayer.
a quiescent phase. The clinical symptoms and radiographicfindings are similar in both cases. Fibrothorax appears to bethe most common source of late BPF formation, whereas, inactive disease, rupture of a pulmonary cavity into the pleuralspace is the most common cause.
The clinical presentation of bronchopleural fistula cantake various forms ranging from incidental radiographic dis-covery to life-threatening acute pneumothorax; however, itmost often presents as a slowly but relentlessly progressivechronic wasting illness.
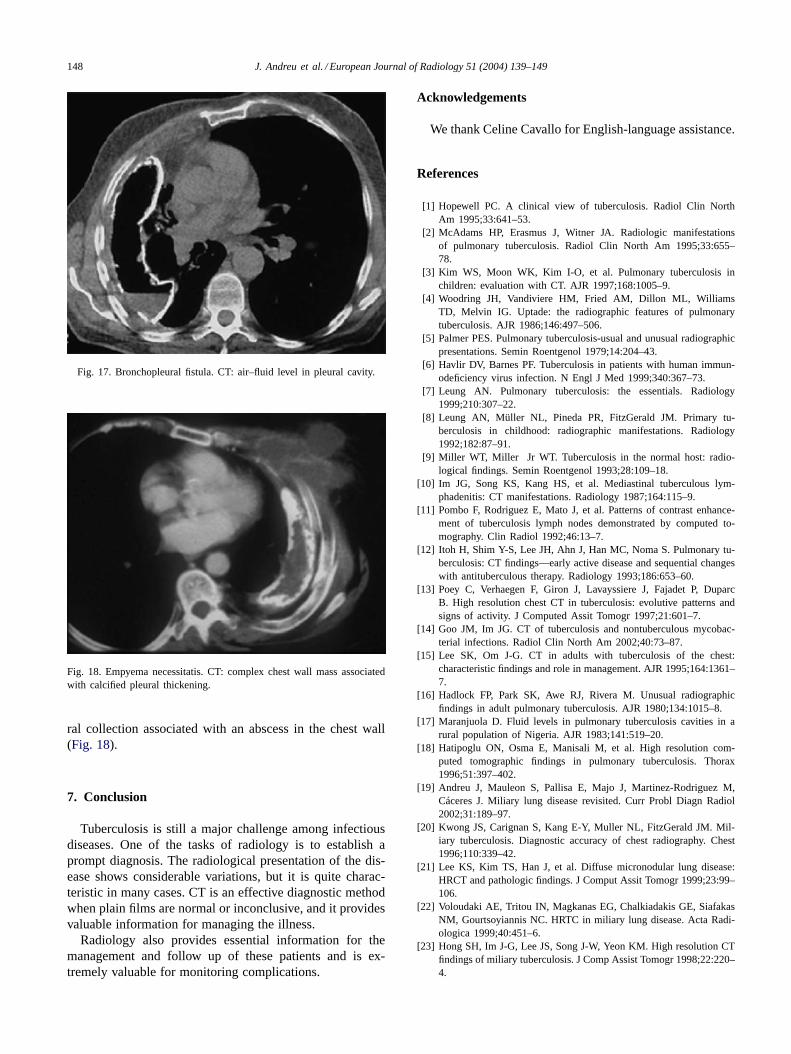
Radiographically, bronchopleural fistula most often ap-pears as a new pleural air–fluid level, sometimes with a ten-sion pneumothorax (Fig. 17) [38,39].
Knowing whether active infection is present is crucialin selecting appropriate medical treatment. Insertion of adrainage tube alone can lead to closure of the fistula; nev-ertheless, if closure is not achieved within weeks of tubedrainage in an otherwise operable patient, a definitive oper-ation is recommended.
6.2. Empyema necessitatis
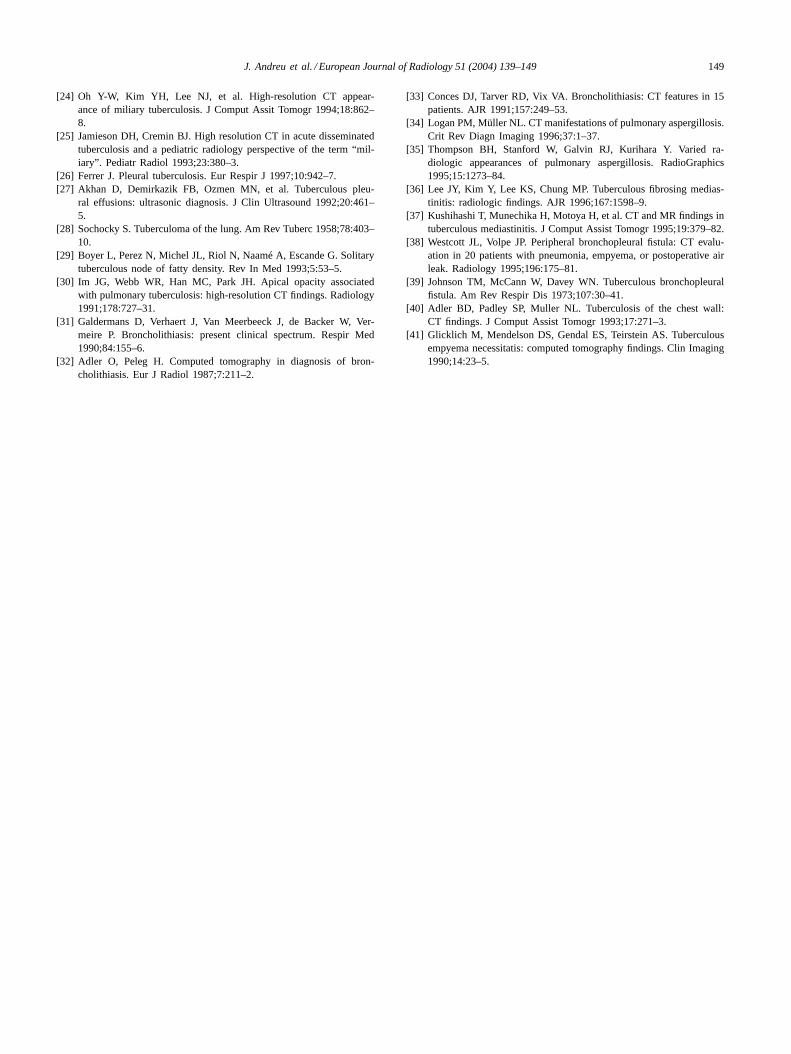
Empyema necessitatis is an uncommon complication ofan empyema in which the inflammatory mass spontaneouslybores its way from the pleural cavity into the soft tissuesof the thoracic wall, forming a subcutaneous abscess thatsometimes opens to the skin. The most common etiologyis tuberculosis[40,41]. In most cases Empyema necessitatisappears as a late complication produced by tuberculous re-activation, frequently in patients who failed to receive propertreatment during the primary infection.
Fig. 16. Pleural TB. Chest radiograph: (a) localized fluid; (b) an organizingcollection corresponding to tuberculous empyema is seen 1 month later.
The most common clinical presentation is a mass in thethoracic wall, accompanied or not by a cutaneous fistula.The plain film usually shows signs of chronic pleural dis-ease with pleural thickening that may be calcified. Thepresence of a subcutaneous mass detected clinically asso-ciated with calcified pleural thickening should be consid-ered suspect of empyema necessitatis. CT and MRI are ofgreat value in making the diagnosis by showing a pleu-
148 J. Andreu et al. / European Journal of Radiology 51 (2004) 139–149
Fig. 17. Bronchopleural fistula. CT: air–fluid level in pleural cavity.
Fig. 18. Empyema necessitatis. CT: complex chest wall mass associatedwith calcified pleural thickening.
ral collection associated with an abscess in the chest wall(Fig. 18).
7. Conclusion
Tuberculosis is still a major challenge among infectiousdiseases. One of the tasks of radiology is to establish aprompt diagnosis. The radiological presentation of the dis-ease shows considerable variations, but it is quite charac-teristic in many cases. CT is an effective diagnostic methodwhen plain films are normal or inconclusive, and it providesvaluable information for managing the illness.
Radiology also provides essential information for themanagement and follow up of these patients and is ex-tremely valuable for monitoring complications.
Acknowledgements
We thank Celine Cavallo for English-language assistance.
References
[1] Hopewell PC. A clinical view of tuberculosis. Radiol Clin NorthAm 1995;33:641–53.
[2] McAdams HP, Erasmus J, Witner JA. Radiologic manifestationsof pulmonary tuberculosis. Radiol Clin North Am 1995;33:655–78.
[3] Kim WS, Moon WK, Kim I-O, et al. Pulmonary tuberculosis inchildren: evaluation with CT. AJR 1997;168:1005–9.
[4] Woodring JH, Vandiviere HM, Fried AM, Dillon ML, WilliamsTD, Melvin IG. Uptade: the radiographic features of pulmonarytuberculosis. AJR 1986;146:497–506.
[5] Palmer PES. Pulmonary tuberculosis-usual and unusual radiographicpresentations. Semin Roentgenol 1979;14:204–43.
[6] Havlir DV, Barnes PF. Tuberculosis in patients with human immun-odeficiency virus infection. N Engl J Med 1999;340:367–73.
[7] Leung AN. Pulmonary tuberculosis: the essentials. Radiology1999;210:307–22.
[8] Leung AN, Müller NL, Pineda PR, FitzGerald JM. Primary tu-berculosis in childhood: radiographic manifestations. Radiology1992;182:87–91.
[9] Miller WT, Miller Jr WT. Tuberculosis in the normal host: radio-logical findings. Semin Roentgenol 1993;28:109–18.
[10] Im JG, Song KS, Kang HS, et al. Mediastinal tuberculous lym-phadenitis: CT manifestations. Radiology 1987;164:115–9.
[11] Pombo F, Rodriguez E, Mato J, et al. Patterns of contrast enhance-ment of tuberculosis lymph nodes demonstrated by computed to-mography. Clin Radiol 1992;46:13–7.
[12] Itoh H, Shim Y-S, Lee JH, Ahn J, Han MC, Noma S. Pulmonary tu-berculosis: CT findings—early active disease and sequential changeswith antituberculous therapy. Radiology 1993;186:653–60.
[13] Poey C, Verhaegen F, Giron J, Lavayssiere J, Fajadet P, DuparcB. High resolution chest CT in tuberculosis: evolutive patterns andsigns of activity. J Computed Assit Tomogr 1997;21:601–7.
[14] Goo JM, Im JG. CT of tuberculosis and nontuberculous mycobac-terial infections. Radiol Clin North Am 2002;40:73–87.
[15] Lee SK, Om J-G. CT in adults with tuberculosis of the chest:characteristic findings and role in management. AJR 1995;164:1361–7.
[16] Hadlock FP, Park SK, Awe RJ, Rivera M. Unusual radiographicfindings in adult pulmonary tuberculosis. AJR 1980;134:1015–8.
[17] Maranjuola D. Fluid levels in pulmonary tuberculosis cavities in arural population of Nigeria. AJR 1983;141:519–20.
[18] Hatipoglu ON, Osma E, Manisali M, et al. High resolution com-puted tomographic findings in pulmonary tuberculosis. Thorax1996;51:397–402.
[19] Andreu J, Mauleon S, Pallisa E, Majo J, Martinez-Rodriguez M,Cáceres J. Miliary lung disease revisited. Curr Probl Diagn Radiol2002;31:189–97.
[20] Kwong JS, Carignan S, Kang E-Y, Muller NL, FitzGerald JM. Mil-iary tuberculosis. Diagnostic accuracy of chest radiography. Chest1996;110:339–42.
[21] Lee KS, Kim TS, Han J, et al. Diffuse micronodular lung disease:HRCT and pathologic findings. J Comput Assit Tomogr 1999;23:99–106.
[22] Voloudaki AE, Tritou IN, Magkanas EG, Chalkiadakis GE, SiafakasNM, Gourtsoyiannis NC. HRTC in miliary lung disease. Acta Radi-ologica 1999;40:451–6.
[23] Hong SH, Im J-G, Lee JS, Song J-W, Yeon KM. High resolution CTfindings of miliary tuberculosis. J Comp Assist Tomogr 1998;22:220–4.
J. Andreu et al. / European Journal of Radiology 51 (2004) 139–149 149
[24] Oh Y-W, Kim YH, Lee NJ, et al. High-resolution CT appear-ance of miliary tuberculosis. J Comput Assit Tomogr 1994;18:862–8.
[25] Jamieson DH, Cremin BJ. High resolution CT in acute disseminatedtuberculosis and a pediatric radiology perspective of the term “mil-iary”. Pediatr Radiol 1993;23:380–3.
[26] Ferrer J. Pleural tuberculosis. Eur Respir J 1997;10:942–7.[27] Akhan D, Demirkazik FB, Ozmen MN, et al. Tuberculous pleu-
ral effusions: ultrasonic diagnosis. J Clin Ultrasound 1992;20:461–5.
[28] Sochocky S. Tuberculoma of the lung. Am Rev Tuberc 1958;78:403–10.
[29] Boyer L, Perez N, Michel JL, Riol N, Naamé A, Escande G. Solitarytuberculous node of fatty density. Rev In Med 1993;5:53–5.
[30] Im JG, Webb WR, Han MC, Park JH. Apical opacity associatedwith pulmonary tuberculosis: high-resolution CT findings. Radiology1991;178:727–31.
[31] Galdermans D, Verhaert J, Van Meerbeeck J, de Backer W, Ver-meire P. Broncholithiasis: present clinical spectrum. Respir Med1990;84:155–6.
[32] Adler O, Peleg H. Computed tomography in diagnosis of bron-cholithiasis. Eur J Radiol 1987;7:211–2.
[33] Conces DJ, Tarver RD, Vix VA. Broncholithiasis: CT features in 15patients. AJR 1991;157:249–53.
[34] Logan PM, Müller NL. CT manifestations of pulmonary aspergillosis.Crit Rev Diagn Imaging 1996;37:1–37.
[35] Thompson BH, Stanford W, Galvin RJ, Kurihara Y. Varied ra-diologic appearances of pulmonary aspergillosis. RadioGraphics1995;15:1273–84.
[36] Lee JY, Kim Y, Lee KS, Chung MP. Tuberculous fibrosing medias-tinitis: radiologic findings. AJR 1996;167:1598–9.
[37] Kushihashi T, Munechika H, Motoya H, et al. CT and MR findings intuberculous mediastinitis. J Comput Assist Tomogr 1995;19:379–82.
[38] Westcott JL, Volpe JP. Peripheral bronchopleural fistula: CT evalu-ation in 20 patients with pneumonia, empyema, or postoperative airleak. Radiology 1995;196:175–81.
[39] Johnson TM, McCann W, Davey WN. Tuberculous bronchopleuralfistula. Am Rev Respir Dis 1973;107:30–41.
[40] Adler BD, Padley SP, Muller NL. Tuberculosis of the chest wall:CT findings. J Comput Assist Tomogr 1993;17:271–3.
[41] Glicklich M, Mendelson DS, Gendal ES, Teirstein AS. Tuberculousempyema necessitatis: computed tomography findings. Clin Imaging1990;14:23–5.
Related Documents











