Radiographic evaluation CT scan : Advantage Suggest the histologic type of the tumor • The presence of fat and calcification within a tracheal mass : pathognomonic of a hamartoma • Marked enhancement of a tracheal lesion after IV contrast : suggests carcinoid tumor Provide clues to the benign or malignant nature of a tracheal

Radiographic evaluation CT scan : Advantage Suggest the histologic type of the tumor The presence of fat and calcification within a tracheal mass : pathognomonic.
Dec 24, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Radiographic evaluationRadiographic evaluation
CT scan : Advantage
Suggest the histologic type of the tumor• The presence of fat and calcification within a tracheal
mass : pathognomonic of a hamartoma• Marked enhancement of a tracheal lesion after IV contrast
: suggests carcinoid tumor
Provide clues to the benign or malignant nature of a tracheal tumor
Radiographic evaluationRadiographic evaluation
Features suggest : Benign lesion includeintraluminal tumor with limited spread along the tracheal wallwell-circumscribed lesion, smooth or lobulated appearancesize usually < 2 cm
Features suggest : Malignant tracheal lesion includeirregular surface, extension over variable lengths of tracheaextramural extension into the mediastinumlesions > 2 cmcircumferential tracheal involvementenlarged mediastinal lymph nodes

Radiographic evaluationRadiographic evaluation
CT scans : Disadvantage
Unreliable for submucosal spread of diseaseAdenoid cystic carcinoma submucosal spread tend to grow slowly and push mediastinal structures away
rather than invade them loss of fat planes between the tumor and mediastinal
structures

Radiographic evaluationRadiographic evaluation
MRI
• MRI offers some advantage over CT when
• vascular or cardiac invasion is suspected and to
• determine whether a lesion has a pedicle or broad-based
attachment
Pulmonary Function TestingPulmonary Function TestingPFT
Can suggest upper airway obstruction
Findings • Severe reduction in PEFR and FEV1

BronchoscopyBronchoscopy
Bronchoscopy represents the mainstay of diagnosis for tracheal tumors
Rigid bronchoscopyFlexible bronchoscopy
potentially hazardous for biopsy and manipulation of a tracheal tumorprecipitate bleeding or total obstruction

BronchoscopyBronchoscopy
Rigid bronchoscope
Pts with large proximal tracheal tumors
Subtotal obstruction Ventilation can be maintained Used to dilate and core-out the malignant lesion
providing stabilization of the airway
Tumor bleeding : rarely a problem Bronchoscope used to apply pressure to the site Cautery or laser treatment

TreatmentTreatment

Careful assessment of the overall situationCoexistent medical disorders, esp. cardiopulmonary diseasePneumonia should be cleared Stabilized the airway
rigid and flexible bronchoscopic techniques
Important tracheal tumors once symptomatic can rapidly progress to critical airway obstruction
TreatmentTreatment

Tracheal lumen ~ 8 mm Exertional dyspnea Worsens rapidly with any further decrease in diameter
Tracheal lumen ≤ 5 mm Stridor present at rest
Tracheal lumen > 10 mm : typically asymptomatic, even with activities
TreatmentTreatment

Primary Malignant tracheal tumors

Primary Malignant Tracheal Tumor
Primary Malignant Tracheal Tumor
The majority of adult tracheal tumors are malignant
The best therapy -> surgical excision with circumferential tracheal resection and primary end-to-end reconstruction
Limitations to resectability include invasion of critical mediastinal structures involvement of such an extensive length of trachea that reconstruction would be impossible
If metastatic is detected in superior mediastinal nodes -> combination chemoradiotherapy

Anesthetic ManagmentAnesthetic Managment
Before surgical resection of tracheal tumors
Flexible and rigid bronchoscope techniques are used to
stabilize the airway
Tracheostomy is unwarranted Stomal placement may interfere subsequently with ideal
positioning of the tracheal anastomosis
Intubation
Anesthetic ManagmentAnesthetic Managment
Surgical ManagementSurgical Management

Tracheal resection and primary reconstructionRelease maneuversSubglottal resectionsCarinal resections
Surgical ManagementSurgical Management
Tracheal Resection and Primary ReconstructionTracheal Resection and Primary Reconstruction
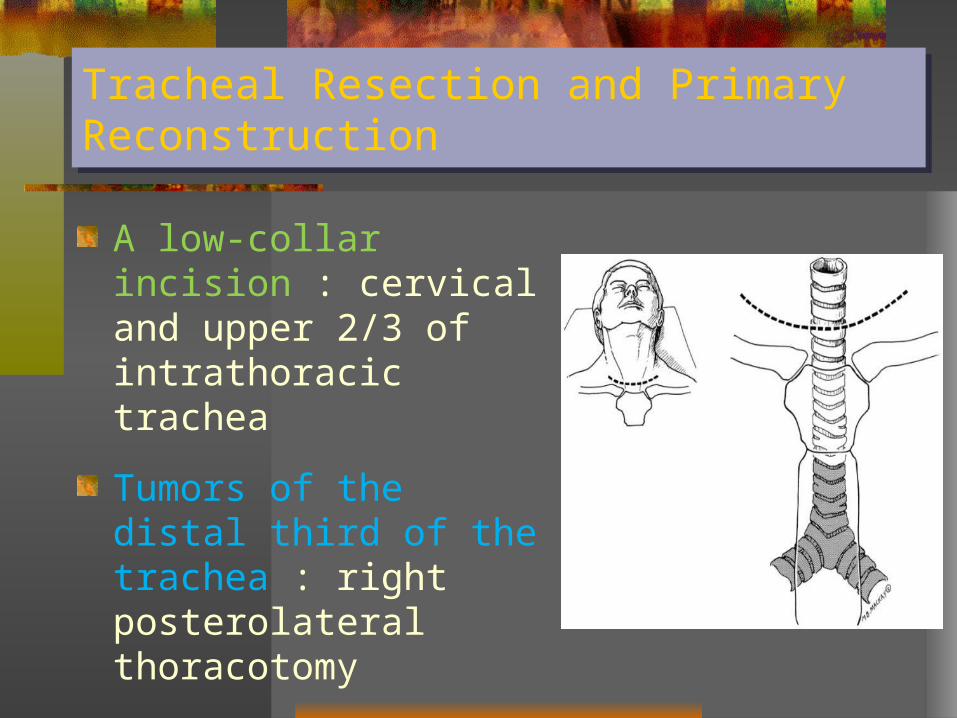
A low-collar incision : cervical and upper 2/3 of intrathoracic trachea
Tumors of the distal third of the trachea : right posterolateral thoracotomy
Carina is involved : a median sternotomy
Tracheal Resection and Primary ReconstructionTracheal Resection and Primary Reconstruction
Benign tumors the dissection is kept immediately adjacent to the trachea no attempt to identify the RLNs
Malignant tumorsidentification and preservation of the RLN if one RLN is involved with tumor sacrificedif sacrifice of both RLN requiresconcomitant tracheostomy subsequent vocal cord-lateralizing procedure
paratracheal nodes are excised

Tracheal Resection and Primary ReconstructionTracheal Resection and Primary Reconstruction
Resection margins should be assessed by intraoperative frozen section
During resection -> prevent anastomotic tension
~ ½ of the trachea can be resected : primary anastomosis
(but advanced patient age and prior mediastinal radiation)
Before complete division and resection stay sutures at proximal and distal ends to assist alignment and gauge tension

A, A tumor of the upper trachea has been excised, and the proximal and distal ends of the trachea are mobilized. Interrupted simple sutures are placed with the knots on the outside. Ventilation is accomplished initially across the field with intubation of the distal airway. Subsequently, as the anastomosis nears completion, the endotracheal tube is advanced across the anastomosis
B, A tumor of the distal trachea is excised, and ventilation is maintained by selective intubation of the left mainstem bronchus across the field. After suture placement, the endotracheal tube is advanced across the anastomosis and into the left mainstem bronchus. The completed anastomosis is wrapped with a pleural flap.

Tracheal Resection and Primary ReconstructionTracheal Resection and Primary Reconstruction
To reduce tension on the anastomosisCervical flexion is maintained with a heavy (No. 2) monofilament"guardian" stitch between the chin and the anterior chest wallPlace for ~ 7 days usually removed after confirmation of anastomotic healing by bronchoscopy
Tracheal resection and primary reconstructionRelease maneuversSubglottal resectionsCarinal resections
Surgical ManagementSurgical Management

Release ManeuversRelease Maneuvers
For resections involving the cervical tracheaNeck flexion and dissection along the anterior trachea in the neck and mediastinumAn additional 2 - 3 cm of tracheal length • Suprathyroid laryngeal release • Suprahyoid laryngeal release preferred
– lower incidence of swallowing complications postoperatively

Tracheal resection and primary reconstructionRelease maneuversSubglottal resectionsCarinal resections
Surgical ManagementSurgical Management

Tumors involve the subglottal region require Prevent permanent RLN damage and vocal cord injuryExcision of the anterior cricoid arch and the posterior cricoid plate leaving its perichondrium Primary thyrotracheal anastomosis
usually within 1 cm of the inferior border of the vocal cords
Subglottal ResectionsSubglottal Resections

Tracheal resection and primary reconstructionRelease maneuversSubglottal resectionsCarinal resections
Surgical ManagementSurgical Management
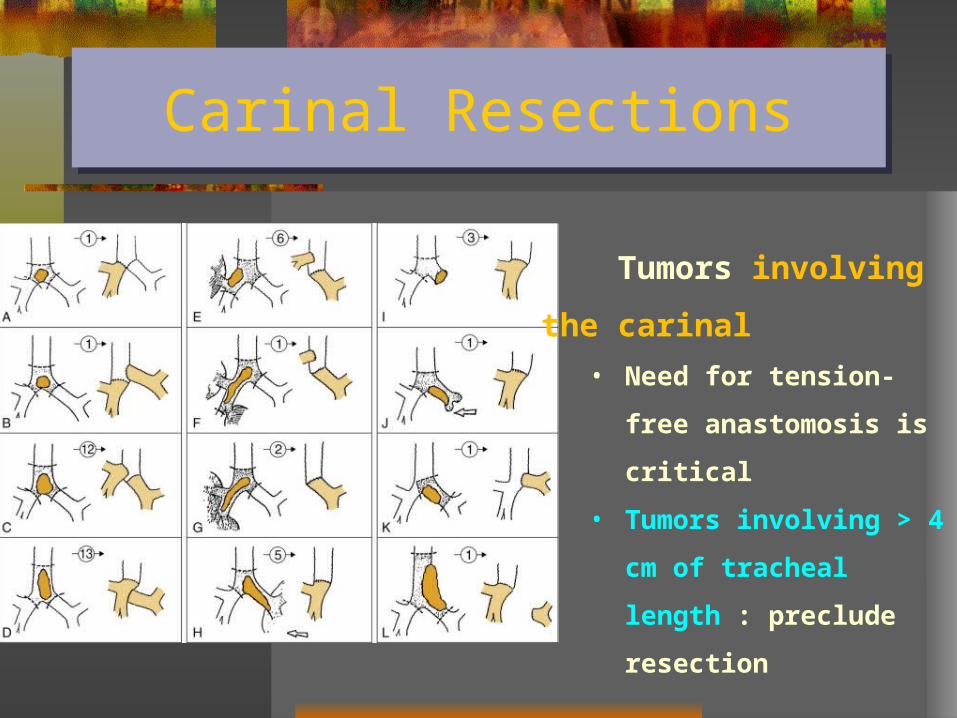
Carinal ResectionsCarinal Resections
Tumors involving the carinal
• Need for tension-free
anastomosis is critical
• Tumors involving > 4 cm of
tracheal length : preclude
resection

Carinal ResectionsCarinal Resections
The simplest technique for reconstruction Involves approximating the medial walls of the right and left mainstem bronchi to fashion a new carina and then anastomosing to distal tracheaOnly with small tumors

Carinal ResectionsCarinal Resections
More commonly
the trachea is anastomosed end-
to-end to one of the mainstem
bronchi
the other mainstem bronchus is
sutured into the lateral wall of the
trachea above the first
anastomosis

Adjuvant radiotherapyAdjuvant radiotherapy

Adjuvant radiotherapyAdjuvant radiotherapy
Recommended for both SCCA and adenoid cystic CAAdenoid cystic CA are especially sensitive to radiation therapyRadiation therapy is usually commenced ~ 4 weeks after surgical resectionuse at least 60 Gy of radiationmedian survival was 24 months, and 5-year survival was 27%

Palliative Treatment of Unresectable Malignant Tracheal Tumors

Therapeutic BronchoscopyTherapeutic Bronchoscopy
Endoscopic procedures including DilatationMechanical débridementLaser vaporizationPDTCryotherapyBrachytherapyStenting

Therapeutic BronchoscopyTherapeutic Bronchoscopy
Extrinsic compressionOnly stenting can provide palliation Mechanical débridement, laser vaporization, PDT, cryotherapy, and brachytherapy are contraindicated
For endotracheal lesionsThe optimal choice : depends on the individual tumor's characteristicsRigid bronchoscope can remove large tumor that obstruction• by running the scope against the wall of the trachea and
slicing off the tumor “coring-out” or mechanical débridement

Endoscopic techniqueEndoscopic technique

Bleeding controlled
compression by the rigid bronchoscope
• (+/- epinephrine-soaked sponges)
Laser vaporization
• performed through a flexible bronchoscope
• combination with rigid bronchoscope
• the most frequently used laser Nd:YAG
Therapeutic BronchoscopyTherapeutic Bronchoscopy

ComplicationsComplications

ComplicationsComplications
Regnard and colleagues : 4 factors that were significantly
associated with the development of postoperative complications
1. Increasing length of resection
2. The need for laryngeal release
3. Laryngotracheal or carinal resection
4. Squamous cell histology
Common problems after tracheal surgery includeAtelectasisRetained secretionsPneumoniaSwallowing dysfunction with aspirationWound infectionsAnastomotic dehiscenceTracheal-innominate or tracheal-pulmonary artery fistula
ComplicationsComplications
Late complications include
Granulation tissue or stenosis at the anastomosis
• often be extracted endoscopic with a bx forcep
Stenosis at the anastomosis
• Endoscopic techniques including dilation and T-tube
placement
ComplicationsComplications

SummarySummary
SummarySummary
Primary tracheal tumors are rareIn adults, most tumors are malignantMore than 80% of malignant tracheal tumors are either SCCA or adenoid cystic CA Tracheal tumors are best managed by resection with end-to-end anastomosisGreat care should be taken to avoid excessive tension on the anastomosis by
limiting the extent of the resection cervical flexionappropriate release procedures

Adjuvant radiotherapy is probably of benefit after resection of SCCA and adenoid cystic CA
Particularly in those with positive resection margins
Primary management for malignant tracheal tumorsMedically unfit for an operationUnresectable tumors Metastatic disease
SummarySummary

Overall, the 5-year survival rate adenoid cystic CA 73% is much greater than for those with SCCA 47%
Management for tumors involving the trachea secondarily is general palliative
Aggressive tracheal resection for invasive thyroid carcinoma and bronchogenic carcinoma offers a chance for cure
SummarySummary

Tumors of the EsophagusTumors of the Esophagus
Benign Esophageal Tumors and CystsBenign Esophageal Tumors and Cysts
Benign tumors are rare (< 1 %)Classified in two groups
MucosalExtramucosal (intramural)
More useful classification:60% of benign neoplasms are leiomyomas20% are cysts5% are polypsOthers (< 2%)

LeiomyomasLeiomyomas
Most common benign tumor of the esophagusIntramuralAge 20-50 years Male ~ Female80% occur in the middle and lower third of the esophagus, they are rare in the cervical regionObstruction and regurgitation may occur in large lesionsBleeding is a more common symptom of the malignant form of the tumor : leiomyosarcoma

Esophageal CystsEsophageal Cysts
Arise as diverticula of the embryonic foregut¾ of this cyst present in childhoodOver 60% are located along the right side of the esophagusAre often associated with vertebral anomalies (ex: spina bifida)60% present in the first year of life with either respiratory or esophageal symptomsCyst found in the upper third of the esophagus present in infancy while lower third lesions present later in childhood

Pedunculated Intraluminal Tumors (Polyps)Pedunculated Intraluminal Tumors (Polyps)
Benign polyps are rare
Usually occur in older men and may cause intermittent
dysphagia
Are sometimes easily missed with barium swallow and
esophagoscopy

Malignant Tumors of the EsophagusMalignant Tumors of the Esophagus
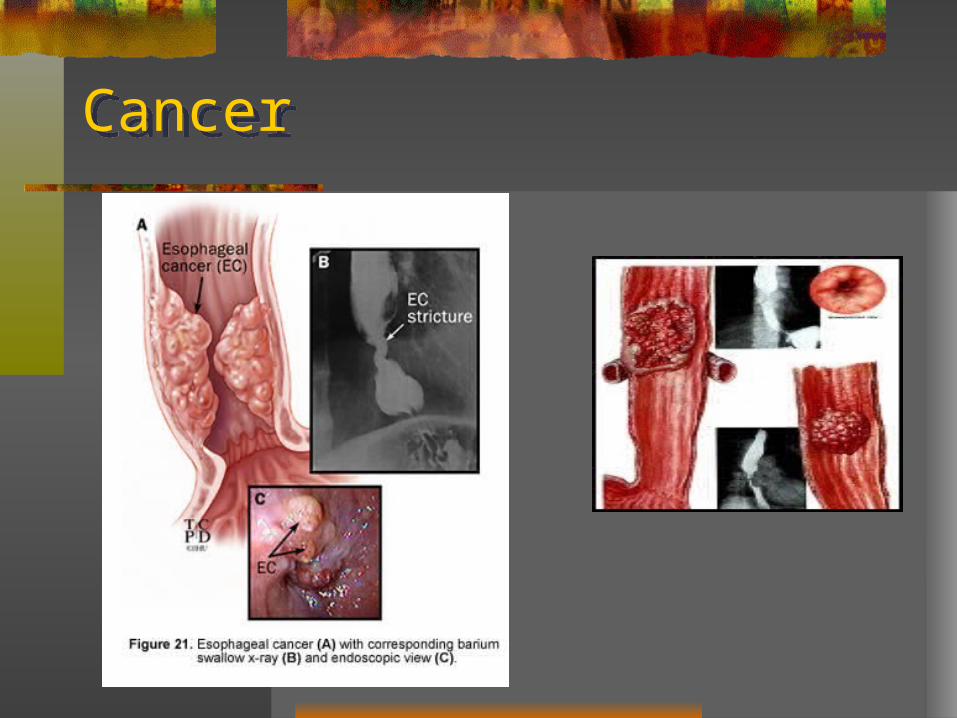
CancerCancer

Malignant Tumors of the EsophagusMalignant Tumors of the Esophagus
Usually are in advanced stages at the time of diagnosis
(involving the muscular wall and extending into adjacent
tissues)
Alcohol consumption and cigarette smoking seem to be
the most consistent risk factors

95% of all esophageal cancers is esophageal squamous cell carcinoma Male : female = 5:1
Squamous cell esophageal cancer occurs most often in the upper and midthoracic segments
Squamous cell esophageal cancer occurs least frequently in the cervical esophagus and
Malignant Tumors of the EsophagusMalignant Tumors of the Esophagus

Adenocarcinoma constitute approximate 8% of primary esophageal cancers
Most often occur in the distal third of the esophagus in the 6th decade of life.
Male to female ratio is 3:1
Patients with Barrett’s metaplasia are 40 times more likely to develop adenocarcinoma
These tumors are aggressive as well
Malignant Tumors of the EsophagusMalignant Tumors of the Esophagus

Clinical PresentationClinical Presentation
Dysphagia is the presenting complaint in 80-90% of patients with esophageal carcinoma
Early symptoms are sometimes nonspecific retrosternal discomfort or indigestion
As the tumor enlarges, dysphagia becomes more progressive
Later symptoms include weight loss, odynophagia, chest pain and hematemesis

DiagnosisDiagnosis
Barium swallow
Esophagoscopy
Esophageal biopsy
Brushings for cytologic evaluation

BariumBarium
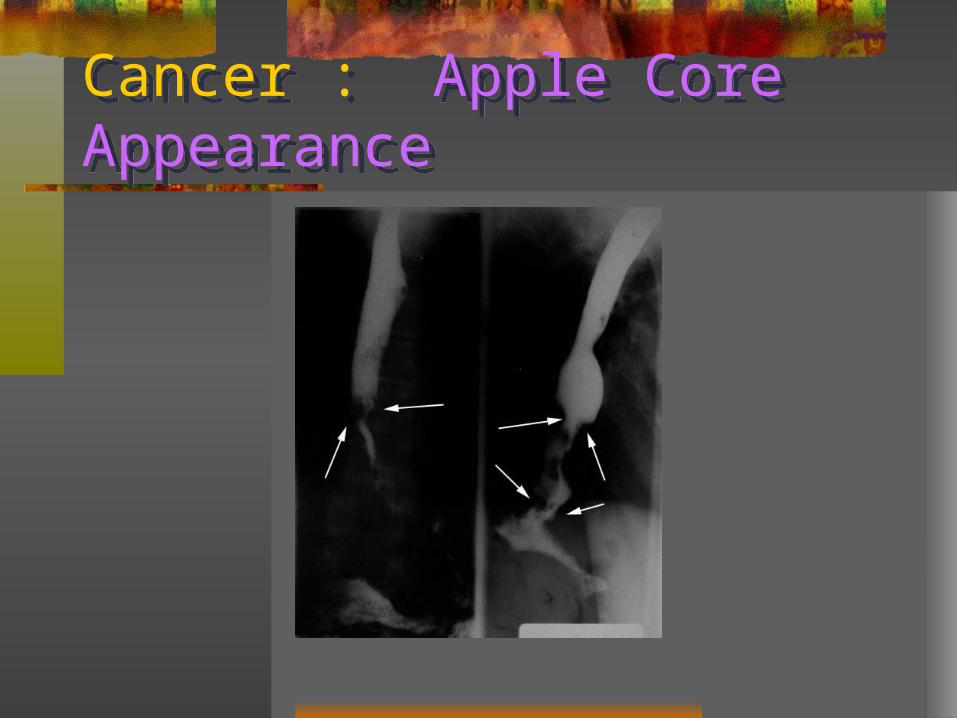
Cancer : Apple Core AppearanceCancer : Apple Core Appearance

CT scanCT scan

Staging of Tumors Staging of Tumors
Endoscopic ultrasound-to define the depth of invasion and presence of paraesophageal lymph nodes
Chest x-ray ± abnormal findings
CT scan (most widely used and now standard radiographic means of staging)
Bronchoscopy for tumors which are proximal to the trachea
TMN Classification for StagingTMN Classification for Staging
The esophagus is first divided into four segments
Cervical
Upper thoracic
Middle thoracic
Lower

Current AJCC 2002 stagingCurrent AJCC 2002 staging

TreatmentTreatment
Surgical resection is the standard treatment for early esophageal cancer ie Stages I, II and most cases of III
5-years survival rate30 - 50 % - stage I 15 - 30 % - stage IIA 5 - 15 % - stage IIB

Systemic Disorders that Cause DysphagiaSystemic Disorders that Cause Dysphagia
Stroke – present in up to 47%
Amyotrophic Lateral Sclerosis
Parkinson’s Disease
Multiple Sclerosis
Muscular Dystrophy
Myasthenia Gravis

Autoimmune DisordersAutoimmune Disorders
Systemic SclerosisSystemic Lupus ErythematosisDermatomyositsMixed Connective Tissue DiseaseMucosal Pemphigoid, Epidermolysis BulosaSjogren’s Syndrome (xerostomia)Rheumatoid Arthritis (cricoarytenoid joint fixation)

AgingAging
Dysphagia is present in 2% in age > 65 yr.Poor dentitionLoss of tongue connective tissueIncreased pharyngeal transit time

THANK YOU FOR YOUR ATTENTION
Related Documents











