REVIEW ARTICLE published: 04 February 2015 doi: 10.3389/fpsyg.2015.00039 Psychological effects of implantable cardioverter defibrillator shocks. A review of study methods Gian Mauro Manzoni 1,2 *, Gianluca Castelnuovo 1,2 , Angelo Compare 3 , Francesco Pagnini 2 , Vidal Essebag 4 and Riccardo Proietti 5 1 Psychology Research Laboratory, Istituto Auxologico Italiano IRCCS, Verbania, Italy 2 Department of Psychology, Catholic University of Milan, Milano, Italy 3 Department of Psychology, University of Bergamo, Bergamo, Italy 4 McGill University Health Center, Montreal, QC, Canada 5 Cardiology Department, Luigi Sacco Hospital, Milano, Italy Edited by: Sayyed Mohsen Fatemi, Harvard University, USA Reviewed by: Valentina Ieraci, University of Turin, Italy Mingna Liu, Northwestern University, USA *Correspondence: Gian Mauro Manzoni, Psychology Research Laboratory, Istituto Auxologico Italiano IRCCS, Via Cadorna 90, 28824 Piancavallo (Oggebbio), Verbania, Italy e-mail: [email protected] Background: The implantable cardioverter defibrillator (ICD) saves lives but clinical experience suggests that it may have detrimental effects on mental health. The ICD shock has been largely blamed as the main offender but empirical evidence is not consistent, perhaps because of methodological differences across studies. Objective: To appraise methodologies of studies that assessed the psychological effects of ICD shock and explore associations between methods and results. Data Sources: A comprehensive search of English articles that were published between 1980 and 30 June 2013 was applied to the following electronic databases: PubMed, EMBASE, NHS HTA database, PsycINFO, Sciencedirect and CINAHL. Review Methods: Only studies testing the effects of ICD shock on psychological and quality of life outcomes were included. Data were extracted according to a PICOS pre-defined sheet including methods and study quality indicators. Results: Fifty-four observational studies and six randomized controlled trials met the inclusion criteria. Multiple differences in methods that were used to test the psychological effects of ICD shock were found across them. No significant association with results was observed. Conclusions: Methodological heterogeneity of study methods is too wide and limits any quantitative attempt to account for the mixed findings. Well-built and standardized research is urgently needed. Keywords: implantable cardioverter defibrillator, ICD shock, quality of life, anxiety, depression, review INTRODUCTION The implantable cardioverter defibrillator (ICD) has become the treatment of choice for both primary and secondary prevention of sudden cardiac death (SCD) due to ventricular arrhythmias (VA). Major clinical trials have consistently shown the ICD to be superior to antiarrhythmic drugs in patients at high risk (Buxton et al., 1999; Kuck et al., 2000; Connolly et al., 2000a,b; Moss et al., 2002; Bardy et al., 2005). As ICDs can avoid SCD but can- not affect the underlying cardiac substrate, the prolonged lifespan enjoyed by patients with significant heart disease is thus shift- ing the clinical burden to the resulting increase in heart failure events (Sears et al., 2006; Mishkin et al., 2009) and to the pos- sibility of repeated shocks (Barnay et al., 2007). Reported rates of appropriate ICD shocks range from 60% in the 3-year sec- ondary prevention AVID study (Anderson et al., 1999) to 20% in the 2-year primary prevention MADIT II trial (Moss et al., 2002). As many patients who receive a shock develop some form of psychological distress in the aftermath (Sears and Kirian, 2010), the possible relation between ICD shocks and psychologi- cal distress/disorders or reduced QoL was assessed with particular attention. Investigations of such relationship were largely con- fined to descriptive or observational studies because of the clear impossibility to control the shock factor and thus to use ran- domized designs. Despite these limitations, an amount of studies attempted to test the hypothesis that ICD shocks are respon- sible for the occurrence of psychological distress/disorders and the reduction of QoL in ICD patients. However, findings were promptly discordant (Sears et al., 1999; Burke et al., 2003) and the supposed negative effect of ICD shock on patients’ QoL and psychological health is still an object of debate (Pedersen and Van Den Broek, 2008; Pedersen et al., 2010b). In order to examine whether such mixed findings might depend on design and methodological differences, we reviewed and critically appraised all quantitative studies that statistically assessed the effect of ICD shocks on psychological variables such as QoL, anxiety, depression, psychological stress or well-being and www.frontiersin.org February 2015 | Volume 6 | Article 39 | 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

REVIEW ARTICLEpublished: 04 February 2015
doi: 10.3389/fpsyg.2015.00039
Psychological effects of implantable cardioverterdefibrillator shocks. A review of study methodsGian Mauro Manzoni1,2*, Gianluca Castelnuovo1,2, Angelo Compare3, Francesco Pagnini2,
Vidal Essebag4 and Riccardo Proietti5
1 Psychology Research Laboratory, Istituto Auxologico Italiano IRCCS, Verbania, Italy2 Department of Psychology, Catholic University of Milan, Milano, Italy3 Department of Psychology, University of Bergamo, Bergamo, Italy4 McGill University Health Center, Montreal, QC, Canada5 Cardiology Department, Luigi Sacco Hospital, Milano, Italy
Edited by:
Sayyed Mohsen Fatemi, HarvardUniversity, USA
Reviewed by:
Valentina Ieraci, University of Turin,ItalyMingna Liu, NorthwesternUniversity, USA
*Correspondence:
Gian Mauro Manzoni, PsychologyResearch Laboratory, IstitutoAuxologico Italiano IRCCS, ViaCadorna 90, 28824 Piancavallo(Oggebbio), Verbania, Italye-mail: [email protected]
Background: The implantable cardioverter defibrillator (ICD) saves lives but clinicalexperience suggests that it may have detrimental effects on mental health. The ICD shockhas been largely blamed as the main offender but empirical evidence is not consistent,perhaps because of methodological differences across studies.
Objective: To appraise methodologies of studies that assessed the psychological effectsof ICD shock and explore associations between methods and results.
Data Sources: A comprehensive search of English articles that were published between1980 and 30 June 2013 was applied to the following electronic databases: PubMed,EMBASE, NHS HTA database, PsycINFO, Sciencedirect and CINAHL.
Review Methods: Only studies testing the effects of ICD shock on psychological andquality of life outcomes were included. Data were extracted according to a PICOSpre-defined sheet including methods and study quality indicators.
Results: Fifty-four observational studies and six randomized controlled trials met theinclusion criteria. Multiple differences in methods that were used to test the psychologicaleffects of ICD shock were found across them. No significant association with results wasobserved.
Conclusions: Methodological heterogeneity of study methods is too wide and limitsany quantitative attempt to account for the mixed findings. Well-built and standardizedresearch is urgently needed.
Keywords: implantable cardioverter defibrillator, ICD shock, quality of life, anxiety, depression, review
INTRODUCTIONThe implantable cardioverter defibrillator (ICD) has become thetreatment of choice for both primary and secondary preventionof sudden cardiac death (SCD) due to ventricular arrhythmias(VA). Major clinical trials have consistently shown the ICD to besuperior to antiarrhythmic drugs in patients at high risk (Buxtonet al., 1999; Kuck et al., 2000; Connolly et al., 2000a,b; Mosset al., 2002; Bardy et al., 2005). As ICDs can avoid SCD but can-not affect the underlying cardiac substrate, the prolonged lifespanenjoyed by patients with significant heart disease is thus shift-ing the clinical burden to the resulting increase in heart failureevents (Sears et al., 2006; Mishkin et al., 2009) and to the pos-sibility of repeated shocks (Barnay et al., 2007). Reported ratesof appropriate ICD shocks range from 60% in the 3-year sec-ondary prevention AVID study (Anderson et al., 1999) to 20% inthe 2-year primary prevention MADIT II trial (Moss et al., 2002).
As many patients who receive a shock develop some formof psychological distress in the aftermath (Sears and Kirian,
2010), the possible relation between ICD shocks and psychologi-cal distress/disorders or reduced QoL was assessed with particularattention. Investigations of such relationship were largely con-fined to descriptive or observational studies because of the clearimpossibility to control the shock factor and thus to use ran-domized designs. Despite these limitations, an amount of studiesattempted to test the hypothesis that ICD shocks are respon-sible for the occurrence of psychological distress/disorders andthe reduction of QoL in ICD patients. However, findings werepromptly discordant (Sears et al., 1999; Burke et al., 2003) andthe supposed negative effect of ICD shock on patients’ QoL andpsychological health is still an object of debate (Pedersen and VanDen Broek, 2008; Pedersen et al., 2010b).
In order to examine whether such mixed findings mightdepend on design and methodological differences, we reviewedand critically appraised all quantitative studies that statisticallyassessed the effect of ICD shocks on psychological variables suchas QoL, anxiety, depression, psychological stress or well-being and
www.frontiersin.org February 2015 | Volume 6 | Article 39 | 1
Manzoni et al. ICD shocks and psychological effect
post-traumatic stress disorder (PTSD) in patients implanted withan ICD for primary and secondary prevention.
METHODSSTUDY ELIGIBILITY CRITERIATypes of studiesQuantitative studies that statistically assessed the associationbetween ICD shock and psychological outcomes were included.Qualitative and single-case or case-series reports were not consid-ered. Studies were selected irrespective of designs, aims, hypothe-ses, time from ICD implantation and length of follow-up. Studiesthat explicitly assessed the causal effect of psychosocial factors onICD shock occurrence were not considered.
Types of participantsPatients of age ≥18 implanted with an ICD for primary orsecondary prevention of SCD were considered. No restrictionwas made on patients’ clinical and demographic characteristicswith the exception of age. Young patients of age <18 were notconsidered.
Types of interventionOnly automatic ICD shock therapy was considered. No restrictionwas made on appropriateness (both appropriate and misappro-priate shocks were considered), duration, electric power and theabsolute or relative number of delivered shocks (isolated shocks,electric storms and shock clusters were considered).
Types of outcome measuresOnly valid and reliable standardized measures of psychologicaland quality of life outcomes were considered. Anxiety, depression,PTSD and health-related quality of life measures were specifiedin advance and documented in the review protocol. However, norestriction was made on any other psychological outcomes thatwere measured in a valid and reliable manner.
REPORT ELIGIBILITY CRITERIAOnly English articles that were published in indexed journalswere considered. Abstracts, letters, unpublished data and grayliterature in general were not searched nor considered.
DATA SOURCESA comprehensive search of English articles that were publishedbetween 1980 and 30 June 2013 was applied to the followingelectronic databases: PubMed, EMBASE, NHS HTA database,PsycINFO, Sciencedirect and CINAHL. Since the first ICDimplantation took place in 1980, it was unnecessary to searchrecords predating that year. Bibliographies of included studieswere screened for further references.
LITERATURE SEARCHA two-step search strategy was used. We arbitrarily defined fourtime intervals (1980–1996, 1997–2003, 2004–2007, 2008–2011)and randomly assigned each of them to one of four indepen-dent reviewers who had been previously instructed about thesearch protocol. We first searched online databases for the fol-lowing terms in article titles or abstracts: ICD, implant∗, defib∗,cardiover∗, (internal near defib∗), (internal near cardiover∗),
(implant∗ near cardiover∗), (implant∗ or internal), (cardiac neardefib∗), (implant∗ and defib∗), (internal and defib∗), (cardiac anddefib∗). We recorded results in a reference database (EndNoteX2, the Thomson Corporation). The second step refined the firstsearch by filtering for the following terms: mood, quality of life,QOL, health, health-related quality of life, adjust∗, psych∗, anx∗,depress∗, stress, well-being.
STUDY SELECTIONStudies identified by the whole search strategy were assessed forinclusion through three stages. First, three independent review-ers (GMM, RP, and GC) screened titles and abstracts of papersto exclude irrelevant records. Full-texts of remaining papers wereobtained and assessed against eligibility criteria by the same inde-pendent reviewers at the second stage. Any differences in opin-ion were resolved through discussion with a forth independentreviewer at the third stage.
DATA COLLECTIONAll included studies were randomly and equally assigned to threereview authors (GMM, RP, SC) who independently extracted andcoded data in accordance to a refined sheet. Information wasextracted on: (1) design and aim of study, (2) ICD indication(primary, secondary or both) and programming (only shock orshock and pacing); (3) demographic characteristics of partici-pants implanted with an ICD (age and sex); (4) inclusion andexclusion criteria; (5) number of participants included in theanalysis and lost to follow-up; (6) shock therapy; (7) timing ofpsychological assessments and length of follow-up; (8) outcomemeasures; (9) statistical analysis; (10) results.
RISK OF BIAS ASSESSMENTThe Cochrane data collection form for non-randomized studiesand the Newcastle-Ottawa scale for assessing quality of cohortstudies were used to assess risk of bias and to ascertain the valid-ity of studies. Both templates were retrieved from the CochraneHandbook for Systematic Reviews of Interventions, Chapter13, Supplementary Material (retrieved at www.cochrane.org/training/cochrane-handbook). The same three review authors(GMM, RP, and GC) who extracted data determined also theadequacy of: (1) ascertainment of shock exposure; (2) demon-stration that outcomes of interest was not present before ICDimplantation; (3) control for confounding; (4) assessment of out-comes (self-report or interview); (5) validity and reliability ofoutcome measures; (6) completeness of data set. Furthermore,the review authors appraised the method used for identifying rel-evant confounders and the method used for controlling relevantconfounders.
DATA ANALYSISWide methodological differences were promptly observed acrossstudies during the review process. The feasibility of standardizingindividual study results and combining them in a meta-analysiswas thus discussed several times during the first intermediatemeetings and no consensus was established before the middle ofthe review process when we decided not to perform any meta-analysis. As reported extensively in the results section, includedstudies differ in many characteristics, in particular analytical and
Frontiers in Psychology | Psychology for Clinical Settings February 2015 | Volume 6 | Article 39 | 2
Manzoni et al. ICD shocks and psychological effect
operationalizing methods, and statistical combination of datafrom two or more similar studies in a meta-analysis may beneither necessary nor desirable (Liberati et al., 2009). Hence,the extracted data were only qualitatively analyzed and tabu-lated. Despite the danger of poor validity associated to quasi-quantitative methods such as vote counting, we decided alsoto perform subgroup analyses in order to explore if significantresults depend on the methodological factors we specified inadvance. Publication bias or selective reporting bias were not sys-tematically assessed because we did not specify this possibilitybefore starting the review and, even if we observed some cluesof selective reporting in a number of articles, we decided not toinvestigate further.
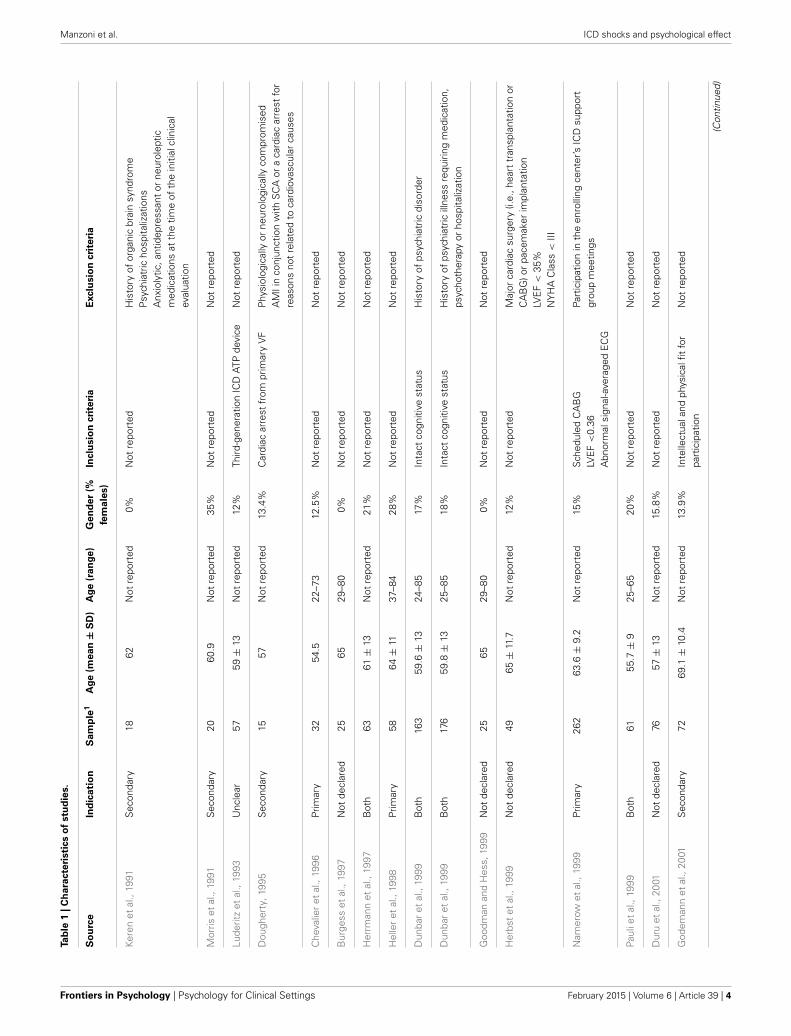
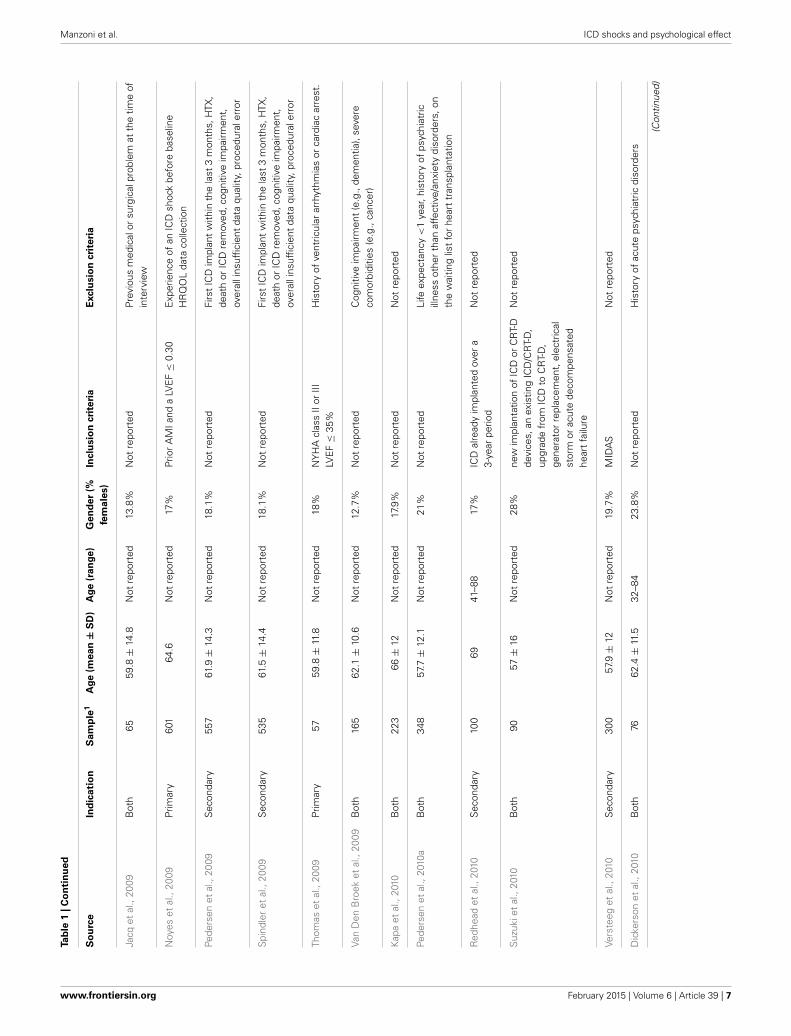
RESULTSSTUDY SELECTIONA total of 60 studies were identified for inclusion in the review(Table 1). The first-step search of electronic databases provided ahuge amount of records that were then drastically reduced withthe filtering for the second-step search terms. Of these records,a large part was discarded in accordance to the report eligibil-ity criteria and because, after screening the abstracts, it appearedthat these studies clearly did not assess a statistical associationbetween ICD shock and the outcomes of interest. No further arti-cle was discarded after examining the full text of the remaining60 records. No additional study was identified by checking the ref-erences of relevant papers, by searching for studies that have citedthese papers or by contacting the principal authors of the field.
CHARACTERISTICS OF INCLUDED STUDIESDesignsStudy designs were coded considering only the part of study inwhich an association between ICD shock and outcomes of inter-est was assessed. According to criterion, 32 studies out of 60 wereclassified as cross-sectional, 27 as prospective and 1 as random-ized controlled trial (RCT). Hence, prospective cohort studiesthat evaluated the effect of shock cross-sectionally (e.g., Market al., 2008) were coded as cross-sectional. Only cohort studiesthat assessed the effect of ICD shock on change in psychologicalvariables and quality of life along time were considered prospec-tive. Six of the included studies are randomized controlled trials(Namerow et al., 1999; Irvine et al., 2002; Schron et al., 2002;Strickberger et al., 2003; Wathen et al., 2004; Mark et al., 2008)but three out of them were classified as cross-sectional (Namerowet al., 1999; Strickberger et al., 2003; Mark et al., 2008) and twoas prospective (Irvine et al., 2002; Schron et al., 2002) becauseassessment of the shock effect was a sub-analysis performed onlyon patients randomized to the ICD condition. Only the PainFREERx II trial (Wathen et al., 2004) was coded as RCT because the ICDshock was partially manipulated. In fact, patients with ICDs wererandomized into two treatment conditions that differed only forthe delivering of shock therapy or anti-tachycardia pacing.
Participants with ICDsThe included studies vary a lot with respect to sample sizes. Thestudy with the smaller sample involved 15 ICD patients and hasa prospective design (Dougherty, 1995), while the study with the
larger sample included 816 ICD patients and was coded as cross-sectional although it is an RCT comparing amiodarone vs. ICDin heart failure patients (Mark et al., 2008). Considering onlypatients with an ICD whose data were included in statistical anal-yses and contributed to results, the whole number of participantsconsidered in this review is 10558. The average of the mean ages ofpatients across the included studies is 61.2 with a standard devia-tion (SD) of 3.6 (range: 53–69.1), while the average of the relativeSDs is 12.1 (range: 6.3–16). Patients included in the studies weremainly males. Percentages of females varied from 0% (Keren et al.,1991; Burgess et al., 1997; Goodman and Hess, 1999) to 81%(Pedersen et al., 2008b) with a mean of only 20% (SD 10.9%).
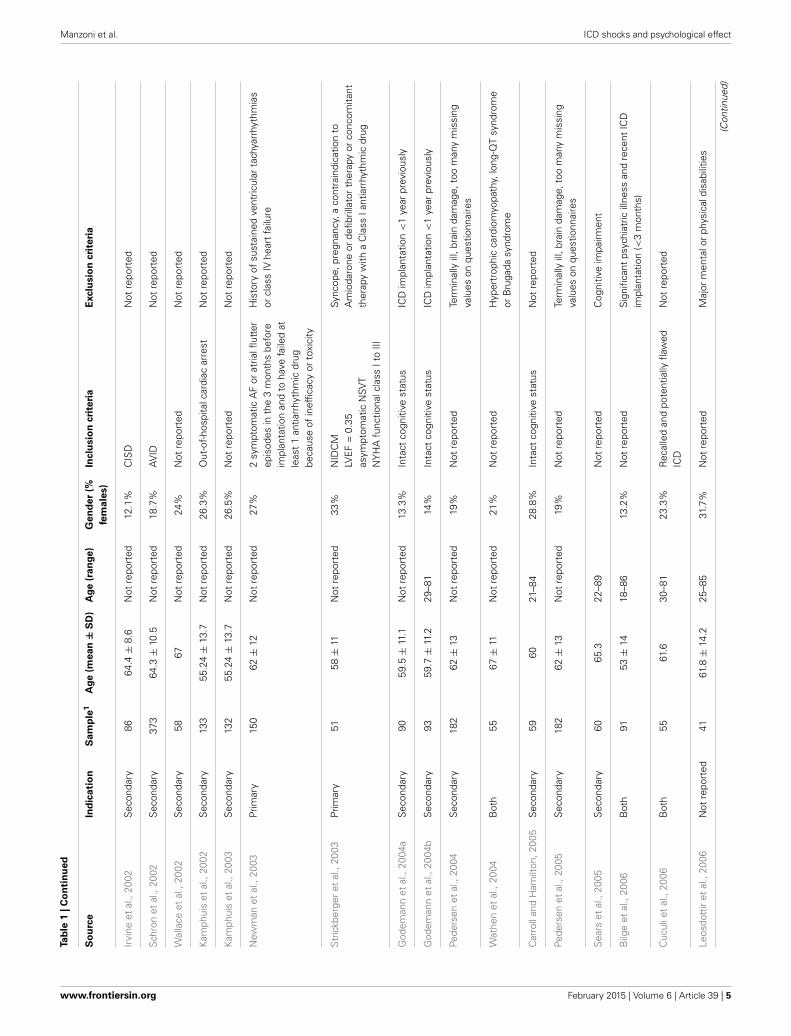
ICD indicationAs expected, studies that involved only patients with a secondaryICD indication are more frequent than studies that recruitedonly patients with a primary ICD indication (22 vs. 10). Sampleswere heterogeneous (both patients with a primary indication andpatients with a secondary prevention were recruited) in 22 stud-ies, while in 6 papers no information about ICD indication wasreported and relative studies were thus not classified (see Table 1for details).
ICD Shock therapyTwenty-seven studies operationalized number of ICD shocks ina dichotomized variable with patients who received 1 or moreshocks classified in one category and patients who did not receiveany shock assigned to the other one. Across 22 out of 27 studiesthat operationalized ICD shocks in this manner (no shock vs. ≥1shocks), 38.5% of patients received at least 1 shock on average.The smallest percentage of patients who received 1 or more shocks(4.2%) was found in the study of Van Den Broek et al. (2009),while the higher (64%) was found in the study of Crossmann et al.(2007), followed by Jacq et al. (2009) and Bilge et al. (2006) with61.5% shocked patients. In five of the articles describing the stud-ies that we classified in this category (no shock vs. ≥1 shocks),data about percentage of patients who received 1 or more shockfrom their ICD were lacking (Keren et al., 1991; Kamphuis et al.,2002; Wathen et al., 2004; Cuculi et al., 2006; Piotrowicz et al.,2007). Indeed, some articles reported only the number, the meanor the median of ICD shocks delivered during the study period.Furthermore, we found that two articles classified in this category(no shock vs. ≥1 shocks) described two studies whose aims andhypotheses were different but shared the same sample (Pedersenet al., 2004, 2005). Two studies operationalized number of ICDshocks in a dichotomized variable with patients who received 5 ormore shocks classified in one category and patients who receivedbetween 0 and 4 shocks assigned to the other one. In Luderitzet al.’s study (1993), 57.9% of ICD patients received 5 or moreshocks during a 12-month follow-up, while in the Von Känelet al.’s study (2011), 8.4% received 5 or more shocks before base-line assessment (24.4 ± 20.7 months post ICD-implantation) and19.3 % received 5 or more shocks between the baseline and theend of follow-up (65.5 ± 27.4 months post ICD-implantation).Nine studies categorized ICD shocks in multiple groups and eightdifferent categorizations were used. Three studies out of themcreated an extreme group of patients who had received ten or
www.frontiersin.org February 2015 | Volume 6 | Article 39 | 3
Manzoni et al. ICD shocks and psychological effect
Tab
le1
|C
ha
racte
risti
cs
of
stu
die
s.
So
urc
eIn
dic
ati
on
Sa
mp
le1
Ag
e(m
ean
±S
D)
Ag
e(r
an
ge)
Gen
der
(%
fem
ale
s)
Inclu
sio
ncri
teri
aE
xclu
sio
ncri
teri
a
Kere
net
al.,
1991
Sec
onda
ry18
62N
otre
port
ed0%
Not
repo
rted
His
tory
ofor
gani
cbr
ain
synd
rom
eP
sych
iatr
icho
spita
lizat
ions
Anx
ioly
tic,a
ntid
epre
ssan
tor
neur
olep
ticm
edic
atio
nsat
the
time
ofth
ein
itial
clin
ical
eval
uatio
n
Mor
riset
al.,
1991
Sec
onda
ry20
60.9
Not
repo
rted
35%
Not
repo
rted
Not
repo
rted
Lude
ritz
etal
.,19
93U
ncle
ar57
59±
13N
otre
port
ed12
%Th
ird-g
ener
atio
nIC
DAT
Pde
vice
Not
repo
rted
Dou
gher
ty,1
995
Sec
onda
ry15
57N
otre
port
ed13
.4%
Car
diac
arre
stfr
ompr
imar
yV
FP
hysi
olog
ical
lyor
neur
olog
ical
lyco
mpr
omis
edA
MIi
nco
njun
ctio
nw
ithS
CA
ora
card
iac
arre
stfo
rre
ason
sno
tre
late
dto
card
iova
scul
arca
uses
Che
valie
ret
al.,
1996
Prim
ary
3254
.522
–73
12.5
%N
otre
port
edN
otre
port
ed
Bur
gess
etal
.,19
97N
otde
clar
ed25
6529
–80
0%N
otre
port
edN
otre
port
ed
Her
rman
net
al.,
1997
Bot
h63
61±
13N
otre
port
ed21
%N
otre
port
edN
otre
port
ed
Hel
ler
etal
.,19
98Pr
imar
y58
64±
1137
–84
28%
Not
repo
rted
Not
repo
rted
Dun
bar
etal
.,19
99B
oth
163
59.6
±13
24–8
517
%In
tact
cogn
itive
stat
usH
isto
ryof
psyc
hiat
ricdi
sord
er
Dun
bar
etal
.,19
99B
oth
176
59.8
±13
25–8
518
%In
tact
cogn
itive
stat
usH
isto
ryof
psyc
hiat
ricill
ness
requ
iring
med
icat
ion,
psyc
hoth
erap
yor
hosp
italiz
atio
n
Goo
dman
and
Hes
s,19
99N
otde
clar
ed25
6529
–80
0%N
otre
port
edN
otre
port
ed
Her
bst
etal
.,19
99N
otde
clar
ed49
65±
11.7
Not
repo
rted
12%
Not
repo
rted
Maj
orca
rdia
csu
rger
y(i.
e.,h
eart
tran
spla
ntat
ion
orC
AB
G)o
rpa
cem
aker
impl
anta
tion
LVE
F<
35%
NY
HA
Cla
ss<
III
Nam
erow
etal
.,19
99Pr
imar
y26
263
.6±
9.2
Not
repo
rted
15%
Sch
edul
edC
AB
GLV
EF
<0.
36A
bnor
mal
sign
al-a
vera
ged
EC
G
Part
icip
atio
nin
the
enro
lling
cent
er’s
ICD
supp
ort
grou
pm
eetin
gs
Paul
iet
al.,
1999
Bot
h61
55.7
±9
25–6
520
%N
otre
port
edN
otre
port
ed
Dur
uet
al.,
2001
Not
decl
ared
7657
±13
Not
repo
rted
15.8
%N
otre
port
edN
otre
port
ed
God
eman
net
al.,
2001
Sec
onda
ry72
69.1
±10
.4N
otre
port
ed13
.9%
Inte
llect
uala
ndph
ysic
alfit
for
part
icip
atio
nN
otre
port
ed
(Con
tinue
d)
Frontiers in Psychology | Psychology for Clinical Settings February 2015 | Volume 6 | Article 39 | 4
Manzoni et al. ICD shocks and psychological effect
Tab
le1
|C
on
tin
ued
So
urc
eIn
dic
ati
on
Sa
mp
le1
Ag
e(m
ean
±S
D)
Ag
e(r
an
ge)
Gen
der
(%
fem
ale
s)
Inclu
sio
ncri
teri
aE
xclu
sio
ncri
teri
a
Irvi
neet
al.,
2002
Sec
onda
ry86
64.4
±8.
6N
otre
port
ed12
.1%
CIS
DN
otre
port
ed
Sch
ron
etal
.,20
02S
econ
dary
373
64.3
±10
.5N
otre
port
ed18
.7%
AV
IDN
otre
port
ed
Wal
lace
etal
.,20
02S
econ
dary
5867
Not
repo
rted
24%
Not
repo
rted
Not
repo
rted
Kam
phui
set
al.,
2002
Sec
onda
ry13
355
.24
±13
.7N
otre
port
ed26
.3%
Out
-of-
hosp
italc
ardi
acar
rest
Not
repo
rted
Kam
phui
set
al.,
2003
Sec
onda
ry13
255
.24
±13
.7N
otre
port
ed26
.5%
Not
repo
rted
Not
repo
rted
New
man
etal
.,20
03Pr
imar
y15
062
±12
Not
repo
rted
27%
2sy
mpt
omat
icA
For
atria
lflut
ter
epis
odes
inth
e3
mon
ths
befo
reim
plan
tatio
nan
dto
have
faile
dat
leas
t1
antia
rrhy
thm
icdr
ugbe
caus
eof
inef
ficac
yor
toxi
city
His
tory
ofsu
stai
ned
vent
ricul
arta
chya
rrhy
thm
ias
orcl
ass
IVhe
art
failu
re
Str
ickb
erge
ret
al.,
2003
Prim
ary
5158
±11
Not
repo
rted
33%
NID
CM
LVE
F=
0.35
asym
ptom
atic
NSV
TN
YH
Afu
nctio
nalc
lass
Ito
III
Sync
ope,
preg
nanc
y,a
cont
rain
dica
tion
toA
mio
daro
neor
defib
rilla
tor
ther
apy
orco
ncom
itant
ther
apy
with
aC
lass
Iant
iarr
hyth
mic
drug
God
eman
net
al.,
2004
aS
econ
dary
9059
.5±
11.1
Not
repo
rted
13.3
%In
tact
cogn
itive
stat
usIC
Dim
plan
tatio
n<
1ye
arpr
evio
usly
God
eman
net
al.,
2004
bS
econ
dary
9359
.7±
11.2
29–8
114
%In
tact
cogn
itive
stat
usIC
Dim
plan
tatio
n<
1ye
arpr
evio
usly
Pede
rsen
etal
.,20
04S
econ
dary
182
62±
13N
otre
port
ed19
%N
otre
port
edTe
rmin
ally
ill,b
rain
dam
age,
too
man
ym
issi
ngva
lues
onqu
estio
nnai
res
Wat
hen
etal
.,20
04B
oth
5567
±11
Not
repo
rted
21%
Not
repo
rted
Hyp
ertr
ophi
cca
rdio
myo
path
y,lo
ng-Q
Tsy
ndro
me
orB
ruga
dasy
ndro
me
Car
roll
and
Ham
ilton
,200
5S
econ
dary
5960
21–8
428
.8%
Inta
ctco
gniti
vest
atus
Not
repo
rted
Pede
rsen
etal
.,20
05S
econ
dary
182
62±
13N
otre
port
ed19
%N
otre
port
edTe
rmin
ally
ill,b
rain
dam
age,
too
man
ym
issi
ngva
lues
onqu
estio
nnai
res
Sea
rset
al.,
2005
Sec
onda
ry60
65.3
22–8
9N
otre
port
edC
ogni
tive
impa
irmen
t
Bilg
eet
al.,
2006
Bot
h91
53±
1418
–86
13.2
%N
otre
port
edS
igni
fican
tps
ychi
atric
illne
ssan
dre
cent
ICD
impl
anta
tion
(<3
mon
ths)
Cuc
ulie
tal
.,20
06B
oth
5561
.630
–81
23.3
%R
ecal
led
and
pote
ntia
llyfla
wed
ICD
Not
repo
rted
Leos
dott
iret
al.,
2006
Not
repo
rted
4161
.8±
14.2
25–8
531
.7%
Not
repo
rted
Maj
orm
enta
lor
phys
ical
disa
bilit
ies
(Con
tinue
d)
www.frontiersin.org February 2015 | Volume 6 | Article 39 | 5

Manzoni et al. ICD shocks and psychological effect
Tab
le1
|C
on
tin
ued
So
urc
eIn
dic
ati
on
Sa
mp
le1
Ag
e(m
ean
±S
D)
Ag
e(r
an
ge)
Gen
der
(%
fem
ale
s)
Inclu
sio
ncri
teri
aE
xclu
sio
ncri
teri
a
Luys
ter
etal
.,20
06B
oth
100
67.9
±11
.735
–85
19%
Not
repo
rted
Not
repo
rted
Cro
ssm
ann
etal
.,20
07B
oth
3557
±6.
335
–65
14%
LVE
F<
0.36
Abn
orm
alsi
gnal
-ave
rage
del
ectr
ocar
diog
ram
Part
icip
atio
nin
the
enro
lling
cent
er’s
ICD
supp
ort
grou
pm
eetin
gs
Pass
man
etal
.,20
07Pr
imar
y22
759
±14
Not
repo
rted
27%
LVE
F≤
35%
not
caus
edby
CA
DH
isto
ryof
sym
ptom
atic
hear
tfa
ilure
Eith
erno
n-su
stai
ned
vent
ricul
arta
chyc
ardi
aor
10or
mor
epr
emat
ure
vent
ricul
arde
pola
rizat
ions
per
hour
Not
repo
rted
Pede
rsen
etal
.,20
07S
econ
dary
154
58.5
±12
.5N
otre
port
ed18
.8%
Not
repo
rted
Life
expe
ctan
cy<
1ye
ar,h
isto
ryof
psyc
hiat
ricill
ness
othe
rth
anaf
fect
ive/
anxi
ety
diso
rder
s,on
the
wai
ting
list
for
hear
ttr
ansp
lant
atio
n
Pio
trow
icz
etal
.,20
07Pr
imar
y39
0U
ncle
arN
otre
port
edU
ncle
arM
AD
IT-II
Not
repo
rted
Sos
song
,200
7B
oth
9065
.4±
10.6
36–8
822
.2%
ICD
for
atle
ast
2m
onth
ssi
nce
impl
anta
tion
Inta
ctco
gniti
vest
atus
Not
repo
rted
Joha
nsen
etal
.,20
08S
econ
dary
610
62.4
18–8
518
%N
otre
port
edFi
rst
ICD
impl
ant
with
inth
ela
st3
mon
ths,
HTX
,de
ath
orIC
Dre
mov
ed,c
ogni
tive
impa
irmen
t,ov
eral
lins
uffic
ient
data
qual
ity,p
roce
dura
lerr
or
Ladw
iget
al.,
2008
Bot
h14
759
.9±
13N
otre
port
ed15
%Ti
me
sinc
eim
plan
tatio
nlo
nger
than
3m
onth
sR
apid
onse
tof
the
CH
Dco
nditi
on
Not
repo
rted
Mar
ket
al.,
2008
Prim
ary
816
59.9
±11
.9N
otre
port
ed22
.9%
NY
HA
chro
nic
and
stab
lecl
ass
IIor
IIIco
nges
tive
hear
tfa
ilure
LVE
F≤
35%
Not
repo
rted
Pede
rsen
etal
.,20
08a
Sec
onda
ry56
661
.9±
14.3
18–8
518
%N
otre
port
edFi
rst
ICD
impl
ant
with
inth
ela
st3
mon
ths,
HTX
,de
ath
orIC
Dre
mov
ed,c
ogni
tive
impa
irmen
t,ov
eral
lins
uffic
ient
data
qual
ity,p
roce
dura
lerr
or
Pede
rsen
etal
.,20
08b
Bot
h17
659
Not
repo
rted
80.7
%LV
EF
<0.
36A
bnor
mal
sign
al-a
vera
ged
elec
troc
ardi
ogra
m
Life
expe
ctan
cy<
1ye
ar,h
isto
ryof
psyc
hiat
ricill
ness
othe
rth
anaf
fect
ive/
anxi
ety
diso
rder
s,on
the
wai
ting
list
for
hear
ttr
ansp
lant
atio
n
Van
Den
Bro
eket
al.,
2008
Bot
h30
862
.6±
10.1
Not
repo
rted
18%
Not
repo
rted
Not
repo
rted
(Con
tinue
d)
Frontiers in Psychology | Psychology for Clinical Settings February 2015 | Volume 6 | Article 39 | 6
Manzoni et al. ICD shocks and psychological effect
Tab
le1
|C
on
tin
ued
So
urc
eIn
dic
ati
on
Sa
mp
le1
Ag
e(m
ean
±S
D)
Ag
e(r
an
ge)
Gen
der
(%
fem
ale
s)
Inclu
sio
ncri
teri
aE
xclu
sio
ncri
teri
a
Jacq
etal
.,20
09B
oth
6559
.8±
14.8
Not
repo
rted
13.8
%N
otre
port
edPr
evio
usm
edic
alor
surg
ical
prob
lem
atth
etim
eof
inte
rvie
w
Noy
eset
al.,
2009
Prim
ary
601
64.6
Not
repo
rted
17%
Prio
rA
MIa
nda
LVE
F≤
0.30
Exp
erie
nce
ofan
ICD
shoc
kbe
fore
base
line
HR
QO
Lda
taco
llect
ion
Pede
rsen
etal
.,20
09S
econ
dary
557
61.9
±14
.3N
otre
port
ed18
.1%
Not
repo
rted
Firs
tIC
Dim
plan
tw
ithin
the
last
3m
onth
s,H
TX,
deat
hor
ICD
rem
oved
,cog
nitiv
eim
pairm
ent,
over
alli
nsuf
ficie
ntda
taqu
ality
,pro
cedu
rale
rror
Spi
ndle
ret
al.,
2009
Sec
onda
ry53
561
.5±
14.4
Not
repo
rted
18.1
%N
otre
port
edFi
rst
ICD
impl
ant
with
inth
ela
st3
mon
ths,
HTX
,de
ath
orIC
Dre
mov
ed,c
ogni
tive
impa
irmen
t,ov
eral
lins
uffic
ient
data
qual
ity,p
roce
dura
lerr
or
Thom
aset
al.,
2009
Prim
ary
5759
.8±
11.8
Not
repo
rted
18%
NY
HA
clas
sII
orIII
LVE
F≤
35%
His
tory
ofve
ntric
ular
arrh
ythm
ias
orca
rdia
car
rest
.
Van
Den
Bro
eket
al.,
2009
Bot
h16
562
.1±
10.6
Not
repo
rted
12.7
%N
otre
port
edC
ogni
tive
impa
irmen
t(e
.g.,
dem
entia
),se
vere
com
orbi
ditie
s(e
.g.,
canc
er)
Kap
aet
al.,
2010
Bot
h22
366
±12
Not
repo
rted
17.9
%N
otre
port
edN
otre
port
ed
Pede
rsen
etal
.,20
10a
Bot
h34
857
.7±
12.1
Not
repo
rted
21%
Not
repo
rted
Life
expe
ctan
cy<
1ye
ar,h
isto
ryof
psyc
hiat
ricill
ness
othe
rth
anaf
fect
ive/
anxi
ety
diso
rder
s,on
the
wai
ting
list
for
hear
ttr
ansp
lant
atio
n
Red
head
etal
.,20
10S
econ
dary
100
6941
–88
17%
ICD
alre
ady
impl
ante
dov
era
3-ye
arpe
riod
Not
repo
rted
Suz
ukie
tal
.,20
10B
oth
9057
±16
Not
repo
rted
28%
new
impl
anta
tion
ofIC
Dor
CR
T-D
devi
ces,
anex
istin
gIC
D/C
RT-
D,
upgr
ade
from
ICD
toC
RT-
D,
gene
rato
rre
plac
emen
t,el
ectr
ical
stor
mor
acut
ede
com
pens
ated
hear
tfa
ilure
Not
repo
rted
Vers
teeg
etal
.,20
10S
econ
dary
300
57.9
±12
Not
repo
rted
19.7
%M
IDA
SN
otre
port
ed
Dic
kers
onet
al.,
2010
Bot
h76
62.4
±11
.532
–84
23.8
%N
otre
port
edH
isto
ryof
acut
eps
ychi
atric
diso
rder
s
(Con
tinue
d)
www.frontiersin.org February 2015 | Volume 6 | Article 39 | 7

Manzoni et al. ICD shocks and psychological effect
Tab
le1
|C
on
tin
ued
So
urc
eIn
dic
ati
on
Sa
mp
le1
Ag
e(m
ean
±S
D)
Ag
e(r
an
ge)
Gen
der
(%
fem
ale
s)
Inclu
sio
ncri
teri
aE
xclu
sio
ncri
teri
a
Hab
ibov
icet
al.,
2012
Bot
h39
562
.8±
10.3
Not
repo
rted
19%
Not
repo
rted
Cog
nitiv
eim
pairm
ents
(e.g
.,de
men
tia),
psyc
hiat
richi
stor
y(o
ther
than
affe
ctiv
edi
sord
ers)
,lif
e-th
reat
enin
gco
mor
bidi
ties
(e.g
.,ca
ncer
),lif
eex
pect
ancy
<1y
ear
Pede
rsen
etal
.,20
11B
oth
284
61.2
±10
.2N
otre
port
ed21
.1%
Not
repo
rted
Sig
nific
ant
cogn
itive
impa
irmen
ts(e
.g.,
dem
entia
),lif
e-th
reat
enin
gco
mor
bidi
ties
(e.g
.,ca
ncer
),hi
stor
yof
psyc
hiat
ricill
ness
othe
rth
anaf
fect
ive/
anxi
ety
diso
rder
s
Von
Kän
elet
al.,
2011
Bot
h10
757
.2±
14.2
Not
repo
rted
38.3
%Ti
me
sinc
eim
plan
tatio
nlo
nger
than
3m
onth
sN
otre
port
ed
1N
umbe
rof
ICD
patie
nts
who
seda
taw
ere
anal
yzed
.
more shocks (Herrmann et al., 1997; Ladwig et al., 2008; Suzukiet al., 2010), while three studies grouped also patients who hadreceived electrical storms (Kapa et al., 2010; Redhead et al., 2010;Suzuki et al., 2010). Three studies operationalized ICD shocks inunits of time. Morris et al. (1991) divided the number of delayedICD shocks by length of follow-up (in months) to generate a fre-quency rate per unit of time; Jacq et al. (2009) divided the numberof shocks received since implantation by the time elapsed sinceimplantation (ratio shock) in order to take into account the sig-nificant difference in time elapsed since implantation betweenparticipants who did or did not experience ICD shock; Pauli et al.(1999) calculated the relative number of ICD shocks per year.Finally, six studies calculated the number of ICD shocks that weredelivered within a fixed length of time or since last assessment(Kamphuis et al., 2003; Bilge et al., 2006; Mark et al., 2008; Noyeset al., 2009; Dickerson et al., 2010; Suzuki et al., 2010). In allthe other studies, the absolute number of ICD shocks that eachpatient received was considered for the analysis.
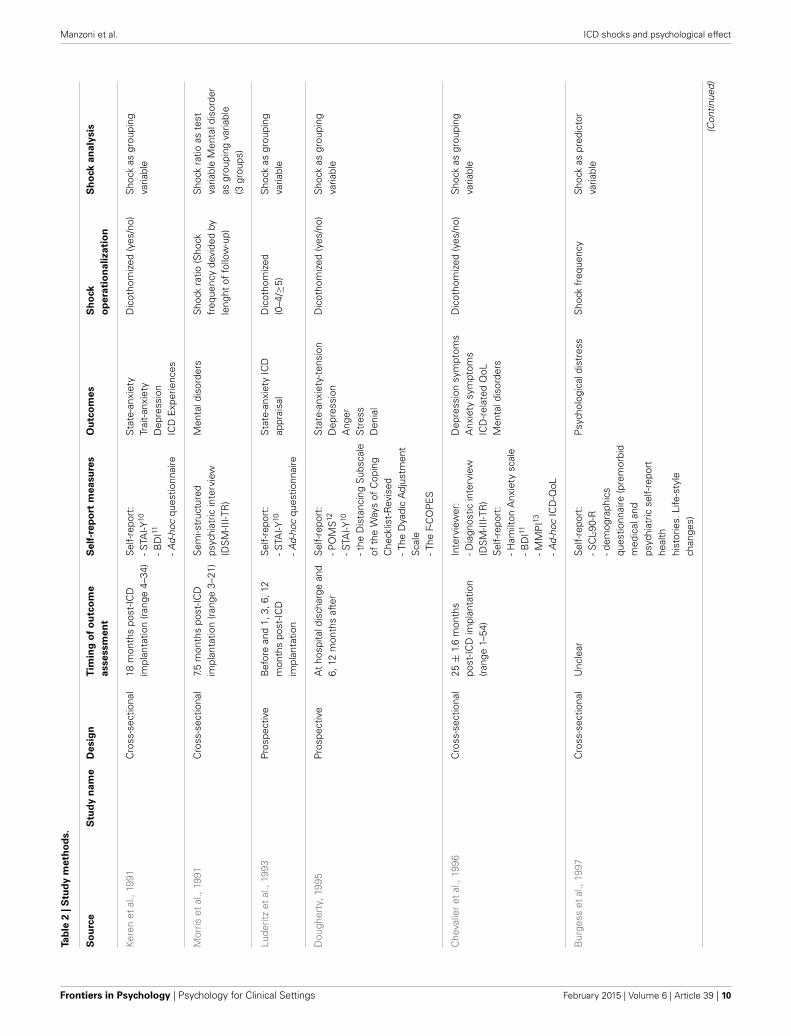
OutcomesThe most prevalent outcomes are measures of anxiety, depressionand health-related quality of life. In particular, anxiety wasmeasured in 36 studies, depression in 30 studies and health-related quality of life (both mental and physical) in 29 studies.Anxiety and depression were mostly measured with self-reportquestionnaires. In only three studies (two of them used also aself-report questionnaire) anxiety was assessed with a clinicalinterview (Van Den Broek et al., 2008, 2009; Jacq et al., 2009),while depression was evaluated with a diagnostic interview inonly one study (Jacq et al., 2009). With respect to the self-reportmeasure of anxiety as an outcome of ICD shocks, the HospitalAnxiety and Depression Scale (HADS) was the most usedpsychometric questionnaire (13 studies out of 35, i.e., the totalnumber of studies that used a self-report measure of anxiety, usedthe HADS). The second most used measure is the SpielbergerState-Trait Anxiety Inventory (STAI), which was used in tenstudies. The remaining self-report questionnaires that were usedto measure anxiety are the Hamilton Anxiety Scale (1 study),the Beck Anxiety Inventory (1 study) and the anxiety index ofthe Symptom Checklist 90 (1 study). The Hamilton Rating Scalefor Anxiety was used in two of the three studies that assessedanxiety with a clinical interview. Differently, Jacq et al. (2009)used the Mini International Neuropsychiatric Interview. Withrespect to the self-report measure of depression as an outcome ofICD shocks, the Hospital Anxiety and Depression Scale (HADS)was again the most used psychometric questionnaire (13 studiesout of 30, i.e., the total number of studies that used a self-reportmeasure of depression, used the HADS). The second most usedmeasure is the Beck Depression Inventory (version 1 or 2) whichwas used in 6 studies. The remaining self-report questionnairesthat were used to measure depression are the Zung Self-RatingDepression Scale (1 study), the Centre for Epidemiologic StudiesDepression Scale (1 study) and the depression index of theSymptom Checklist 90 (1 study). The only study that assesseddepression symptoms with a clinical interview used the MiniInternational Neuropsychiatric Interview (Jacq et al., 2009).General mental disorders were assessed in four studies (Morris
Frontiers in Psychology | Psychology for Clinical Settings February 2015 | Volume 6 | Article 39 | 8

Manzoni et al. ICD shocks and psychological effect
et al., 1991; Chevalier et al., 1996; Godemann et al., 2001,2004a). All of them used a semi-structured psychiatric interviewaccording to the DSM-III-R criteria. Health-related quality of lifewas mostly measured with the SF-36 (15 studies) and the SF-12(4 studies). Few other studies used the Health Utility Index 3(Noyes et al., 2009), the Health Complaints Scale (Van Den Broeket al., 2009), the RAND-36 Health Survey (Kamphuis et al., 2002,2003), the Ferrans and Powers Quality of Life Index (Carrolland Hamilton, 2005; Sossong, 2007; Dickerson et al., 2010), theGeneral Health Questionnaire and the Icelandic Quality of LifeQuestionnaire (Leosdottir et al., 2006), the RAND-38 MentalHealth Inventory and the Nottingham Health Profile (Irvineet al., 2002), and the Quality of Well Being Schedule (Strickbergeret al., 2003). Further psychological outcomes are Post-TraumaticStress Disorder (PTSD) or PTSD symptomatology, ICD accep-tance and ICD concerns. PTSD was evaluated in five studies.The Impact of Event Scale-R was used in three studies (Ladwiget al., 2008; Kapa et al., 2010; Von Känel et al., 2011), while thePosttraumatic Stress Diagnostic Scale was administered in theother ones (Versteeg et al., 2010; Habibovic et al., 2012). ICDacceptance was analyzed as an outcome of ICD shocks in threestudies (Pedersen et al., 2008a; Spindler et al., 2009; Keren et al.,2011). The Florida Patient Acceptance Survey was used in all ofthem. Finally, ICD concerns were assessed as an outcome of ICDshocks in two studies (Spindler et al., 2009; Van Den Broek et al.,2009). The ICD Concerns questionnaire was used in both ones.
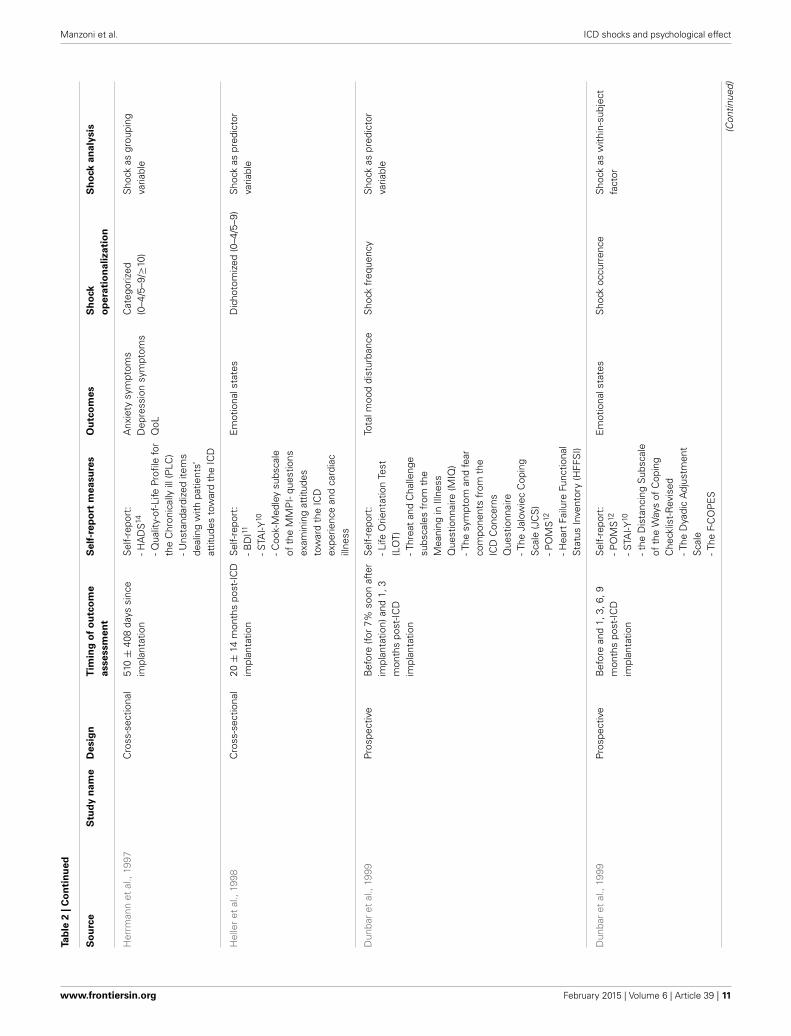
Timing of outcome assessment and follow-upIncluded studies vary a lot with respect to the timing of out-come assessment and follow-up. The first sharp distinction con-cerns study design. However, even considering cross-sectionaland prospective studies separately, a large amount of variabilityremains in each category. In real cross-sectional studies, in whichpatients were assessed only once, a great heterogeneity in timefrom ICD implantation was observed both within and betweenstudies. For example, the average of the mean times from ICDimplantation across the 19 cross-sectional studies that reportedtime data on a continuous scale is 32 months with a SD of18.2 (range: −60). The briefer mean time from ICD implanta-tion was found in Namerow et al.’ study (1999), while the longerone was found in Pedersen, Spindler, Johansen and Mortensenstudy (2009). In Jacq et al.’s study (2009), mean time from ICDimplantation was divided between patients who received 1 ormore shocks (37.4 months ±31.9) and patients who did notreceive any shock (17.9 months ±16), while in 2 studies (Bilgeet al., 2006; Redhead et al., 2010) patients were divided into mul-tiple sub-groups according to fixed time intervals. In prospectivestudies, in which patients were assessed at least twice along thefollow-up (repeated measures), differences and heterogeneitieswere observed in four factors: (1) baseline assessment (beforeICD implantation or after ICD implantation); (2) time beforeICD implantation; (3) timing of repeated measurements fromICD implantation; (4) length of follow-up. Baseline was clearlyassessed before ICD implantation in 14 studies, but in only 3 outof them the baseline time-point was explicitly reported, i.e., 1 daybefore ICD implantation (Pedersen et al., 2007, 2008a, 2010a).However, these 3 studies are not independent because patients
who comprised the three samples participated in the same study(MIDAS—Mood and personality as precipitants of arrhythmia inpatients with an ICD: A prospective Study). Baseline was assessedbefore ICD implantation also in other 3 studies but not for allparticipants, some of whom were evaluated just after the implan-tation before hospital discharge (Dunbar et al., 1999; Irvine et al.,2002; Suzuki et al., 2010). Baseline was clearly assessed afterICD implantation in 8 studies but the timing of first assess-ment was highly heterogeneous both between and within them.For example, in some studies patients were evaluated few daysafter ICD implantation or at hospital discharge, while in otherstudies patients were firstly assessed after months from surgery.Finally, if baseline assessment was performed before or after theICD implantation was impossible to establish in three studiesbecause the respective articles do not report sufficient informa-tion. Prospective studies are quite heterogeneous also with respectto the number and timing of repeated measurements from ICDimplantation and length of follow-up. For example, in only 19out of 28 studies patients were followed for at least 12 months(see Table 2 for details).
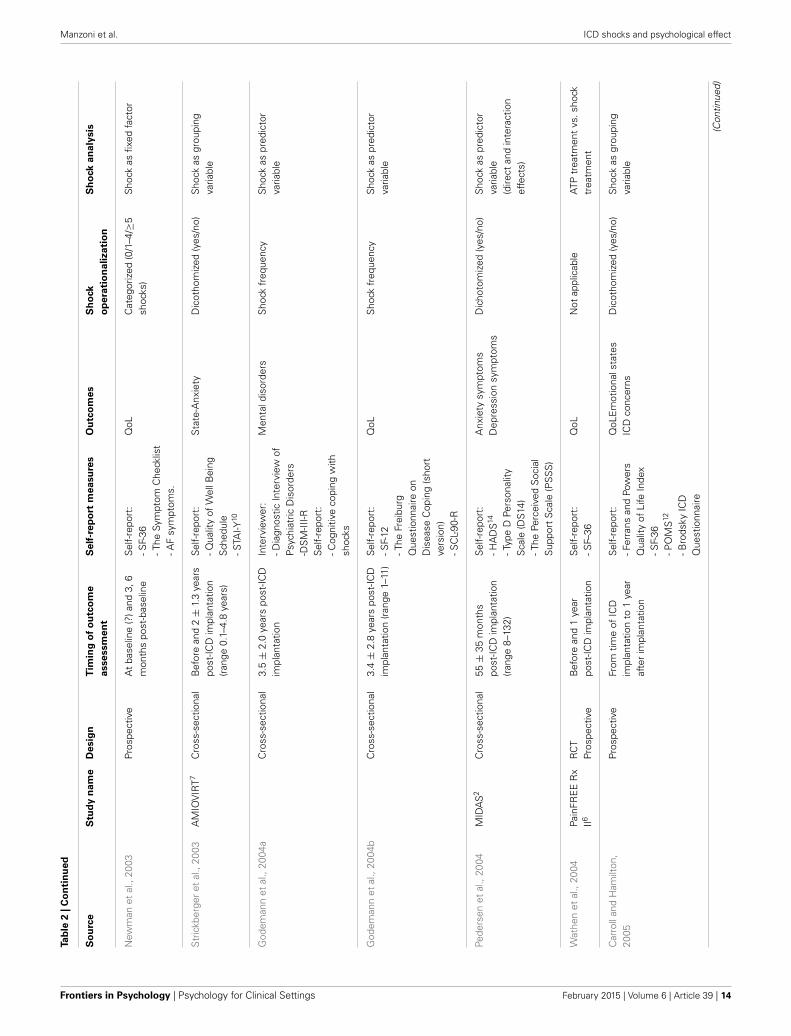
Statistical analysisLast but not least, studies vary quite a lot with respect to thestatistical analyses that were performed to test the effect ofICD shocks on patients’ psychological health and quality of life.Clearly, much of this heterogeneity is explained by the ways out-comes and ICD shocks were operationalized and also by studydesigns. However, two main analytical solutions were identified:(1) classifying patients in two or more shock-groups in accor-dance with different numerical criteria and testing the simpleor adjusted effect of such dichotomized or categorized shockvariable by univariate or multivariate analyses and (2) regress-ing outcome on number of shocks by multivariate regressionanalyses. Furthermore, in few studies patients were classified indifferent outcome-groups according to criteria such as psychi-atric diagnoses, outcome change patterns or outcome distributioncut-offs and then compared on number of shocks. Finally, inonly two studies intra-individual changes from pre-shock topost-shock assessments were analyzed by hierarchical regressionmodels.
The heterogeneity of analytical approaches can be furtherexplained by three factors: (1) the outcome variable scale(dichotomous, dichotomized or continuous); (2) the operational-ization of ICD shocks (see previous paragraph) and (3) thenumber and kind of covariates/predictors that were enteredinto the statistical models. A fourth factor that pertains onlyto multivariate regression models concerns the importance ofthe ICD shock variable within the analysis. In fact, some ofthe studies that were included in the review did not han-dle the ICD shock variable as the main explaining factor buttreated it as a potential covariate or controlling predictor. Inthese studies, the leading role was given to other psychologi-cal or medical factors (for example, type-D personality, con-cerns about the ICD, device acceptance and disease severity)and the ICD shock variable was mainly used as a competingpredictor in the statistical explanation of patients’ psychologicaldistress.
www.frontiersin.org February 2015 | Volume 6 | Article 39 | 9
Manzoni et al. ICD shocks and psychological effect
Tab
le2
|S
tud
ym
eth
od
s.
So
urc
eS
tud
yn
am
eD
esig
nT
imin
go
fo
utc
om
e
asse
ssm
en
t
Self
-rep
ort
measu
res
Ou
tco
mes
Sh
ock
op
era
tio
nalizati
on
Sh
ock
an
aly
sis
Kere
net
al.,
1991
Cro
ss-s
ectio
nal
18m
onth
spo
st-IC
Dim
plan
tatio
n(r
ange
4–34
)S
elf-
repo
rt:
-STA
I-Y10
-BD
I11
-Ad-
hoc
ques
tionn
aire
Sta
te-a
nxie
tyTr
ait-
anxi
ety
Dep
ress
ion
ICD
Exp
erie
nces
Dic
otho
miz
ed(y
es/n
o)S
hock
asgr
oupi
ngva
riabl
e
Mor
riset
al.,
1991
Cro
ss-s
ectio
nal
7.5
mon
ths
post
-ICD
impl
anta
tion
(ran
ge3–
21)
Sem
i-str
uctu
red
psyc
hiat
ricin
terv
iew
(DS
M-II
I-TR
)
Men
tald
isor
ders
Sho
ckra
tio(S
hock
freq
uenc
yde
vide
dby
leng
htof
follo
w-u
p)
Sho
ckra
tioas
test
varia
ble
Men
tald
isor
der
asgr
oupi
ngva
riabl
e(3
grou
ps)
Lude
ritz
etal
.,19
93Pr
ospe
ctiv
eB
efor
ean
d1,
3,6,
12m
onth
spo
st-IC
Dim
plan
tatio
n
Sel
f-re
port
:-S
TAI-Y
10
-Ad-
hoc
ques
tionn
aire
Sta
te-a
nxie
tyIC
Dap
prai
sal
Dic
otho
miz
ed(0
–4/≥
5)S
hock
asgr
oupi
ngva
riabl
e
Dou
gher
ty,1
995
Pros
pect
ive
At
hosp
itald
isch
arge
and
6,12
mon
ths
afte
rS
elf-
repo
rt:
-PO
MS
12
-STA
I-Y10
-the
Dis
tanc
ing
Sub
scal
eof
the
Way
sof
Cop
ing
Che
cklis
t-R
evis
ed-T
heD
yadi
cA
djus
tmen
tS
cale
-The
F-C
OP
ES
Sta
te-a
nxie
ty-t
ensi
onD
epre
ssio
nA
nger
Str
ess
Den
ial
Dic
otho
miz
ed(y
es/n
o)S
hock
asgr
oupi
ngva
riabl
e
Che
valie
ret
al.,
1996
Cro
ss-s
ectio
nal
25±
1.6
mon
ths
post
-ICD
impl
anta
tion
(ran
ge1–
54)
Inte
rvie
wer
:-D
iagn
ostic
inte
rvie
w(D
SM
-III-T
R)
Sel
f-re
port
:-H
amilt
onA
nxie
tysc
ale
-BD
I11
-MM
PI13
-Ad-
hoc
ICD
-QoL
Dep
ress
ion
sym
ptom
sA
nxie
tysy
mpt
oms
ICD
-rel
ated
QoL
Men
tald
isor
ders
Dic
otho
miz
ed(y
es/n
o)S
hock
asgr
oupi
ngva
riabl
e
Bur
gess
etal
.,19
97C
ross
-sec
tiona
lU
ncle
arS
elf-
repo
rt:
-SC
L-90
-R-d
emog
raph
ics
ques
tionn
aire
(pre
mor
bid
med
ical
and
psyc
hiat
ricse
lf-re
port
heal
thhi
stor
ies.
Life
-sty
lech
ange
s)
Psy
chol
ogic
aldi
stre
ssS
hock
freq
uenc
yS
hock
aspr
edic
tor
varia
ble
(Con
tinue
d)
Frontiers in Psychology | Psychology for Clinical Settings February 2015 | Volume 6 | Article 39 | 10
Manzoni et al. ICD shocks and psychological effect
Tab
le2
|C
on
tin
ued
So
urc
eS
tud
yn
am
eD
esig
nT
imin
go
fo
utc
om
e
asse
ssm
en
t
Self
-rep
ort
measu
res
Ou
tco
mes
Sh
ock
op
era
tio
nalizati
on
Sh
ock
an
aly
sis
Her
rman
net
al.,
1997
Cro
ss-s
ectio
nal
510
±40
8da
yssi
nce
impl
anta
tion
Sel
f-re
port
:-H
AD
S14
-Qua
lity-
of-L
ifePr
ofile
for
the
Chr
onic
ally
ill(P
LC)
-Uns
tand
ardi
zed
item
sde
alin
gw
ithpa
tient
s’at
titud
esto
war
dth
eIC
D
Anx
iety
sym
ptom
sD
epre
ssio
nsy
mpt
oms
QoL
Cat
egor
ized
(0–4
/5–9
/≥10
)S
hock
asgr
oupi
ngva
riabl
e
Hel
ler
etal
.,19
98C
ross
-sec
tiona
l20
±14
mon
ths
post
-ICD
impl
anta
tion
Sel
f-re
port
:-B
DI11
-STA
I-Y10
-Coo
k-M
edle
ysu
bsca
leof
the
MM
PI-
ques
tions
exam
inin
gat
titud
esto
war
dth
eIC
Dex
perie
nce
and
card
iac
illne
ss
Em
otio
nals
tate
sD
icho
tom
ized
(0–4
/5–9
)S
hock
aspr
edic
tor
varia
ble
Dun
bar
etal
.,19
99Pr
ospe
ctiv
eB
efor
e(fo
r7%
soon
afte
rim
plan
tatio
n)an
d1,
3m
onth
spo
st-IC
Dim
plan
tatio
n
Sel
f-re
port
:-L
ifeO
rient
atio
nTe
st(L
OT)
-Thr
eat
and
Cha
lleng
esu
bsca
les
from
the
Mea
ning
inIll
ness
Que
stio
nnai
re(M
IQ)
-The
sym
ptom
and
fear
com
pone
nts
from
the
ICD
Con
cern
sQ
uest
ionn
aire
-The
Jalo
wie
cC
opin
gS
cale
(JC
S)
-PO
MS
12
-Hea
rtFa
ilure
Func
tiona
lS
tatu
sIn
vent
ory
(HFF
SI)
Tota
lmoo
ddi
stur
banc
eS
hock
freq
uenc
yS
hock
aspr
edic
tor
varia
ble
Dun
bar
etal
.,19
99Pr
ospe
ctiv
eB
efor
ean
d1,
3,6,
9m
onth
spo
st-IC
Dim
plan
tatio
n
Sel
f-re
port
:-P
OM
S12
-STA
I-Y10
-the
Dis
tanc
ing
Sub
scal
eof
the
Way
sof
Cop
ing
Che
cklis
t-R
evis
ed-T
heD
yadi
cA
djus
tmen
tS
cale
-The
F-C
OP
ES
Em
otio
nals
tate
sS
hock
occu
rren
ceS
hock
asw
ithin
-sub
ject
fact
or
(Con
tinue
d)
www.frontiersin.org February 2015 | Volume 6 | Article 39 | 11

Manzoni et al. ICD shocks and psychological effect
Tab
le2
|C
on
tin
ued
So
urc
eS
tud
yn
am
eD
esig
nT
imin
go
fo
utc
om
e
asse
ssm
en
t
Self
-rep
ort
measu
res
Ou
tco
mes
Sh
ock
op
era
tio
nalizati
on
Sh
ock
an
aly
sis
Goo
dman
and
Hes
s,19
99C
ross
-sec
tiona
lU
ncle
arS
elf-
repo
rt:-
SC
L-90
-R-d
emog
raph
ics
ques
tionn
aire
(pre
mor
bid
med
ical
and
psyc
hiat
ricse
lf-re
port
heal
thhi
stor
ies)
Anx
iety
sym
ptom
sD
epre
ssio
nsy
mpt
oms
Sho
ckfr
eque
ncy
Sho
ckas
pred
icto
rva
riabl
e
Her
bst
etal
.,19
99C
ross
-sec
tiona
l31
.2±
16.8
mon
ths
post
-ICD
impl
anta
tion
Sel
f-re
port
:-S
F-36
-Brie
fSy
mpt
omIn
vent
ory
-dem
ogra
phic
squ
estio
nnai
re(p
rem
orbi
dm
edic
alan
dps
ychi
atric
self-
repo
rthe
alth
hist
orie
s)
QoL
Psy
chol
ogic
aldi
stre
ssD
icot
hom
ized
(yes
/no)
Sho
ckas
grou
ping
varia
ble
Nam
erow
etal
.,19
99C
AB
GPa
tch
Tria
lR
CT
Cro
ss-s
ectio
nal
6m
onth
saf
ter
CA
BG
surg
ery
Sel
f-re
port
:-S
F-36
-dem
ogra
phic
squ
estio
nnai
re(p
rem
orbi
dm
edic
alan
dps
ychi
atric
self-
repo
rthe
alth
)
QoL
Dic
otho
miz
ed(y
es/n
o)S
hock
asgr
oupi
ngva
riabl
e
Paul
iet
al.,
1999
Cro
ss-s
ectio
nal
22.8
±19
.2m
onth
spo
st-IC
Dim
plan
tatio
n(r
ange
2–89
)
Sel
f-re
port
:-A
ICD
-que
stio
nnai
re(a
nxie
tyre
late
dto
futu
resh
ocks
)-T
heA
CQ
(cat
astr
ophi
zing
cogn
ition
s)-T
heB
SQ
(anx
iety
ofbo
dily
sym
ptom
s)-S
TAI-Y
10
-BA
I15
-BD
I11
Sho
ck-r
elat
edan
xiet
yS
hock
sfr
eque
ncy
Sho
ckra
tio(S
hock
freq
uenc
yde
vide
dby
leng
htof
follo
w-u
p)D
icho
tom
ized
(yes
/no)
Sho
ckas
pred
icto
rva
riabl
eS
hock
asfix
edfa
ctor
Dur
uet
al.,
2001
Cro
ss-s
ectio
nal
≥6m
onth
spo
st-IC
Dim
plan
tatio
n(2
.3ye
ars
onav
erag
e)
Sel
f-re
port
:-S
F-36
-HA
DS
14
-Ad-
hoc
ques
tionn
aire
(per
cept
ions
ofIC
D)
Anx
iety
sym
ptom
sD
epre
ssio
nsy
mpt
oms
ICD
appr
aisa
l
Dic
otho
miz
ed(y
es/n
o)S
hock
asgr
oupi
ngva
riabl
e
(Con
tinue
d)
Frontiers in Psychology | Psychology for Clinical Settings February 2015 | Volume 6 | Article 39 | 12

Manzoni et al. ICD shocks and psychological effect
Tab
le2
|C
on
tin
ued
So
urc
eS
tud
yn
am
eD
esig
nT
imin
go
fo
utc
om
e
asse
ssm
en
t
Self
-rep
ort
measu
res
Ou
tco
mes
Sh
ock
op
era
tio
nalizati
on
Sh
ock
an
aly
sis
God
eman
net
al.,
2001
Cro
ss-s
ectio
nal
3.4
±1.
8ye
ars
post
-ICD
impl
anta
tion
Inte
rvie
wer
:-S
emi-s
truc
ture
din
terv
iew
(DIP
S)
Sel
f-re
port
:-S
CL-
90-R
Men
tald
isor
ders
Sho
ckfr
eque
ncy
Sho
ckas
pred
icto
rva
riabl
e
Irvi
neet
al.,
2002
CIS
D9
RC
TPr
ospe
ctiv
eB
efor
eor
soon
afte
rra
ndom
izat
ion
and
2,6,
12m
onth
spo
st-IC
Dim
plan
tatio
n
Sel
f-re
port
:-R
and
Cor
pora
tion’
s38
-item
Men
talH
ealth
Inve
ntor
y-N
ottin
gham
Hea
lthPr
ofile
QoL
Cat
egor
ized
(0/1
–4/≥
5)S
hock
asfix
edfa
ctor
Sch
ron
etal
.,20
02A
VID
8R
CT
Pros
pect
ive
Bef
ore
rand
omiz
atio
nan
d3,
6,12
mon
ths
afte
rra
ndom
izat
ion
Sel
f-re
port
:-S
F-36
-Pat
ient
conc
erns
chec
klis
t-T
heca
rdia
cve
rsio
nof
the
QoL
inde
x
QoL
Dic
hoto
miz
ed(y
es/n
oan
d<
3/≥3
)S
hock
asfix
edfa
ctor
Wal
lace
etal
.,20
02C
ross
-sec
tiona
l12
–24
(70.
6%),
25–3
6(2
7.4%
)and
37–4
8(2
%)
mon
ths
post
-ICD
impl
anta
tion
Sel
f-re
port
:-S
tate
Trai
tPe
rson
ality
Inve
ntor
y-I
nter
pers
onal
Sup
port
Eva
luat
ion
List
-Dis
ease
-spe
cific
QoL
AV
IDch
eckl
ist
-SF-
12
QoL
Sho
cks
freq
uenc
yS
hock
aspr
edic
tor
varia
ble
Kam
phui
set
al.,
2002
Pros
pect
ive
Few
days
befo
rean
d1,
6,12
mon
ths
post
-dis
char
ge
Sel
f-re
port
:-R
and
36-it
emH
ealth
Sur
vey
-The
Hea
rtPa
tient
sP
sych
olog
ical
Que
stio
nnai
re(H
PP
Q)
-CE
S-D
16
-STA
I-Y10
QoL
Sta
te-A
nxie
tyD
epre
ssio
nsy
mpt
oms
Psy
chol
ogic
alw
ell-b
eing
Dic
otho
miz
ed(y
es/n
o)S
hock
asfix
edfa
ctor
Kam
phui
set
al.,
2003
Pros
pect
ive
afte
rad
mis
sion
(bef
ore
card
iac
eval
uatio
n)an
d1,
6,12
mon
ths
afte
rdi
scha
rge
Sel
f-re
port
:-R
AN
D-3
6-H
eart
Patie
ntP
sych
olog
ical
Que
stio
nnai
re(H
PP
Q)
-STA
I-Y10
-CE
S-D
16
QoL
Sta
te-A
nxie
tyD
epre
ssio
nsy
mpt
oms
Psy
chol
ogic
alw
ell-b
eing
Cat
egor
ized
(Sho
cks
inbo
thtim
ein
terv
als/
Sho
cks
excl
usiv
ely
durin
gth
efir
st6
mon
ths/
Sho
cks
excl
usiv
ely
durin
gth
ela
st6
mon
ths/
No
shoc
ksdu
ring
first
year
)
Sho
ckas
fixed
fact
or
(Con
tinue
d)
www.frontiersin.org February 2015 | Volume 6 | Article 39 | 13
Manzoni et al. ICD shocks and psychological effect
Tab
le2
|C
on
tin
ued
So
urc
eS
tud
yn
am
eD
esig
nT
imin
go
fo
utc
om
e
asse
ssm
en
t
Self
-rep
ort
measu
res
Ou
tco
mes
Sh
ock
op
era
tio
nalizati
on
Sh
ock
an
aly
sis
New
man
etal
.,20
03Pr
ospe
ctiv
eA
tba
selin
e(?
)and
3,6
mon
ths
post
-bas
elin
eS
elf-
repo
rt:
-SF-
36-T
heSy
mpt
omC
heck
list
-AF
sym
ptom
s.
QoL
Cat
egor
ized
(0/1
–4/≥
5sh
ocks
)S
hock
asfix
edfa
ctor
Str
ickb
erge
ret
al.,
2003
AM
IOV
IRT7
Cro
ss-s
ectio
nal
Bef
ore
and
2±
1.3
year
spo
st-IC
Dim
plan
tatio
n(r
ange
0.1–
4.8
year
s)
Sel
f-re
port
:-Q
ualit
yof
Wel
lBei
ngS
ched
ule
-STA
I-Y10
Sta
te-A
nxie
tyD
icot
hom
ized
(yes
/no)
Sho
ckas
grou
ping
varia
ble
God
eman
net
al.,
2004
aC
ross
-sec
tiona
l3.
5±
2.0
year
spo
st-IC
Dim
plan
tatio
nIn
terv
iew
er:
-Dia
gnos
ticIn
terv
iew
ofP
sych
iatr
icD
isor
ders
-DS
M-II
I-RS
elf-
repo
rt:
-Cog
nitiv
eco
ping
with
shoc
ks
Men
tald
isor
ders
Sho
ckfr
eque
ncy
Sho
ckas
pred
icto
rva
riabl
e
God
eman
net
al.,
2004
bC
ross
-sec
tiona
l3.
4±
2.8
year
spo
st-IC
Dim
plan
tatio
n(r
ange
1–11
)S
elf-
repo
rt:
-SF-
12-T
heFr
eibu
rgQ
uest
ionn
aire
onD
isea
seC
opin
g(s
hort
vers
ion)
-SC
L-90
-R
QoL
Sho
ckfr
eque
ncy
Sho
ckas
pred
icto
rva
riabl
e
Pede
rsen
etal
.,20
04M
IDA
S2
Cro
ss-s
ectio
nal
55±
35m
onth
spo
st-IC
Dim
plan
tatio
n(r
ange
8–13
2)
Sel
f-re
port
:-H
AD
S14
-Typ
eD
Pers
onal
ityS
cale
(DS
14)
-The
Perc
eive
dS
ocia
lS
uppo
rtS
cale
(PS
SS
)
Anx
iety
sym
ptom
sD
epre
ssio
nsy
mpt
oms
Dic
hoto
miz
ed(y
es/n
o)S
hock
aspr
edic
tor
varia
ble
(dire
ctan
din
tera
ctio
nef
fect
s)
Wat
hen
etal
.,20
04Pa
inFR
EE
Rx
II6R
CT
Pros
pect
ive
Bef
ore
and
1ye
arpo
st-IC
Dim
plan
tatio
nS
elf-
repo
rt:
-SF–
36Q
oLN
otap
plic
able
ATP
trea
tmen
tvs
.sho
cktr
eatm
ent
Car
roll
and
Ham
ilton
,20
05Pr
ospe
ctiv
eFr
omtim
eof
ICD
impl
anta
tion
to1
year
afte
rim
plan
tatio
n
Sel
f-re
port
:-F
erra
nsan
dPo
wer
sQ
ualit
yof
Life
Inde
x-S
F-36
-PO
MS
12
-Bro
dsky
ICD
Que
stio
nnai
re
QoL
Em
otio
nals
tate
sIC
Dco
ncer
nsD
icot
hom
ized
(yes
/no)
Sho
ckas
grou
ping
varia
ble
(Con
tinue
d)
Frontiers in Psychology | Psychology for Clinical Settings February 2015 | Volume 6 | Article 39 | 14
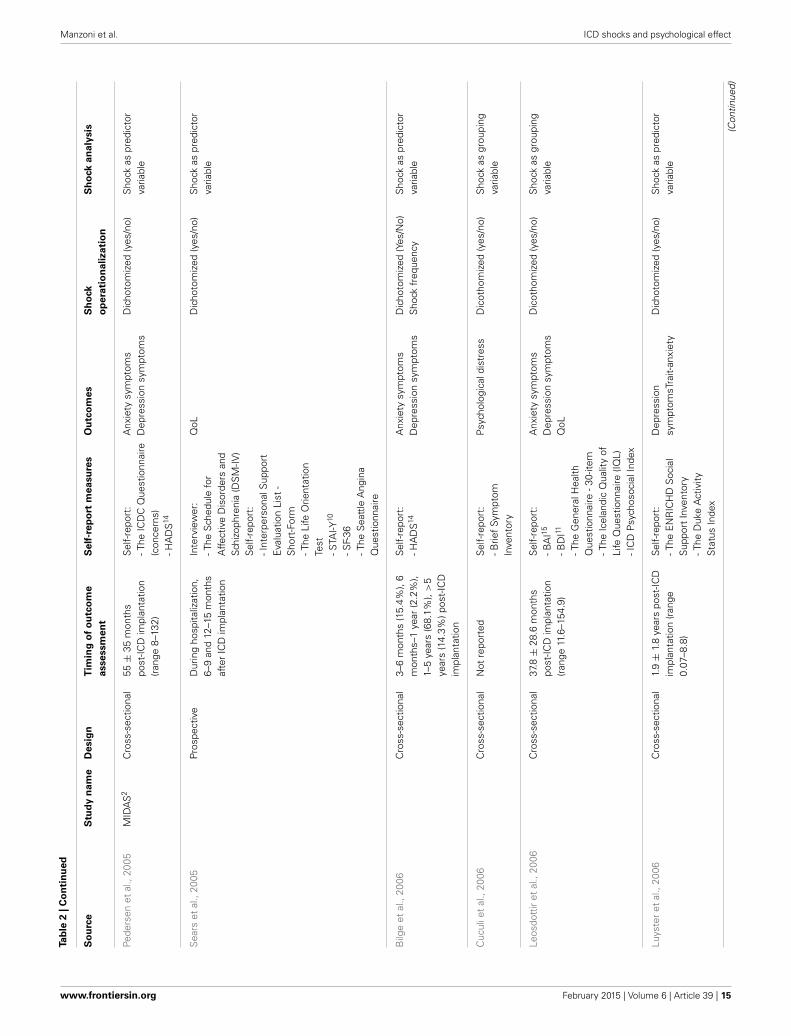
Manzoni et al. ICD shocks and psychological effect
Tab
le2
|C
on
tin
ued
So
urc
eS
tud
yn
am
eD
esig
nT
imin
go
fo
utc
om
e
asse
ssm
en
t
Self
-rep
ort
measu
res
Ou
tco
mes
Sh
ock
op
era
tio
nalizati
on
Sh
ock
an
aly
sis
Pede
rsen
etal
.,20
05M
IDA
S2
Cro
ss-s
ectio
nal
55±
35m
onth
spo
st-IC
Dim
plan
tatio
n(r
ange
8–13
2)
Sel
f-re
port
:-T
heIC
DC
Que
stio
nnai
re(c
once
rns)
-HA
DS
14
Anx
iety
sym
ptom
sD
epre
ssio
nsy
mpt
oms
Dic
hoto
miz
ed(y
es/n
o)S
hock
aspr
edic
tor
varia
ble
Sea
rset
al.,
2005
Pros
pect
ive
Dur
ing
hosp
italiz
atio
n,6–
9an
d12
–15
mon
ths
afte
rIC
Dim
plan
tatio
n
Inte
rvie
wer
:-T
heS
ched
ule
for
Affe
ctiv
eD
isor
ders
and
Sch
izop
hren
ia(D
SM
-IV)
Sel
f-re
port
:-I
nter
pers
onal
Sup
port
Eva
luat
ion
List
-S
hort
-For
m-T
heLi
feO
rient
atio
nTe
st-S
TAI-Y
10
-SF-
36-T
heS
eatt
leA
ngin
aQ
uest
ionn
aire
QoL
Dic
hoto
miz
ed(y
es/n
o)S
hock
aspr
edic
tor
varia
ble
Bilg
eet
al.,
2006
Cro
ss-s
ectio
nal
3–6
mon
ths
(15.
4%),
6m
onth
s–1
year
(2.2
%),
1–5
year
s(6
8.1%
),>
5ye
ars
(14.
3%)p
ost-
ICD
impl
anta
tion
Sel
f-re
port
:-H
AD
S14
Anx
iety
sym
ptom
sD
epre
ssio
nsy
mpt
oms
Dic
hoto
miz
ed(Y
es/N
o)S
hock
freq
uenc
yS
hock
aspr
edic
tor
varia
ble
Cuc
ulie
tal
.,20
06C
ross
-sec
tiona
lN
otre
port
edS
elf-
repo
rt:
-Brie
fSy
mpt
omIn
vent
ory
Psy
chol
ogic
aldi
stre
ssD
icot
hom
ized
(yes
/no)
Sho
ckas
grou
ping
varia
ble
Leos
dott
iret
al.,
2006
Cro
ss-s
ectio
nal
37.8
±28
.6m
onth
spo
st-IC
Dim
plan
tatio
n(r
ange
11.6
–154
.9)
Sel
f-re
port
:-B
AI15
-BD
I11
-The
Gen
eral
Hea
lthQ
uest
ionn
aire
-30-
item
-The
Icel
andi
cQ
ualit
yof
Life
Que
stio
nnai
re(IQ
L)-I
CD
Psy
chos
ocia
lInd
ex
Anx
iety
sym
ptom
sD
epre
ssio
nsy
mpt
oms
QoL
Dic
otho
miz
ed(y
es/n
o)S
hock
asgr
oupi
ngva
riabl
e
Luys
ter
etal
.,20
06C
ross
-sec
tiona
l1.
9±
1.8
year
spo
st-IC
Dim
plan
tatio
n(r
ange
0.07
–8.8
)
Sel
f-re
port
:-T
heE
NR
ICH
DS
ocia
lS
uppo
rtIn
vent
ory
-The
Duk
eA
ctiv
ityS
tatu
sIn
dex
Dep
ress
ion
sym
ptom
sTra
it-an
xiet
yD
icho
tom
ized
(yes
/no)
Sho
ckas
pred
icto
rva
riabl
e
(Con
tinue
d)
www.frontiersin.org February 2015 | Volume 6 | Article 39 | 15

Manzoni et al. ICD shocks and psychological effect
Tab
le2
|C
on
tin
ued
So
urc
eS
tud
yn
am
eD
esig
nT
imin
go
fo
utc
om
e
asse
ssm
en
t
Self
-rep
ort
measu
res
Ou
tco
mes
Sh
ock
op
era
tio
nalizati
on
Sh
ock
an
aly
sis
-The
Con
serv
atio
nof
Res
ourc
esE
valu
atio
n(C
OR
-E)
-BD
I11
-Brie
fPa
tient
Hea
lthQ
uest
ionn
aire
-STA
I-Y10
Cro
ssm
ann
etal
.,20
07Pr
ospe
ctiv
e25
.5±
19.2
mon
ths
post
-ICD
impl
anta
tion
(ran
ge1.
5–88
)and
30.3
mon
ths
afte
rfir
stas
sess
men
t(r
ange
29.6
–31.
2)
Sel
f-re
port
:-T
heA
CQ
(cat
astr
ophi
zing
cogn
ition
s)-T
heB
SQ
(anx
iety
ofbo
dily
sym
ptom
s)-S
TAI-Y
10
-BA
I15
-The
Mob
ility
Inve
ntor
y(a
void
ance
beha
vior
)
Trai
t-an
xiet
yA
nxie
tysy
mpt
oms
Anx
iety
rela
ted
tobo
dily
sym
ptom
s
Dic
otho
miz
ed(y
es/n
o)S
hock
asgr
oupi
ngva
riabl
e
Pass
man
etal
.,20
07Pr
ospe
ctiv
eB
asel
ine
(?),
1an
d3
mon
ths
afte
rra
ndom
izat
ion
and
ever
y3
mon
ths
ther
eaft
erup
to63
mon
ths
Sel
f-re
port
:-S
F-12
-the
Min
neso
taLi
ving
with
Hea
rtFa
ilure
Que
stio
nnai
re
QoL
Sho
ckoc
curr
ence
Sho
ckas
with
in-s
ubje
ctfa
ctor
Pede
rsen
etal
.,20
07M
IDA
S2
Pros
pect
ive
1da
ypr
ior
toim
plan
tatio
nan
d3
mon
ths
post
-ICD
impl
anta
tion
Sel
f-re
port
:-T
ype
DPe
rson
ality
Sca
le(D
S14
)-S
F-36
QoL
Sho
ckfr
eque
ncy
Sho
ckas
cova
riate
Pio
trow
icz
etal
.,20
07M
AD
IT-II
3Pr
ospe
ctiv
eA
tba
selin
e(b
efor
era
ndom
izat
ion)
and
at12
-mon
thfo
llow
-up
Sel
f-re
port
:-S
F-12
QoL
Dic
otho
miz
ed(y
es/n
o)S
hock
asgr
oupi
ngva
riabl
e
Sos
song
,200
7C
ross
-sec
tiona
l15
.9±
13m
onth
spo
st-IC
Dim
plan
tatio
n(r
ange
2.1–
56.1
)
Sel
f-re
port
:-T
heS
osso
ngIC
DK
now
ledg
eQ
uest
ionn
aire
-Mis
helU
ncer
tain
tyin
Illne
ssS
cale
(MU
IS-A
dult)
-Fer
rans
and
Pow
ers
Qua
lity
ofLi
feIn
dex
-C
ardi
acVe
rsio
nIV
QoL
Sho
ckfr
eque
ncy
Sho
ckas
pred
icto
rva
riabl
e
(Con
tinue
d)
Frontiers in Psychology | Psychology for Clinical Settings February 2015 | Volume 6 | Article 39 | 16
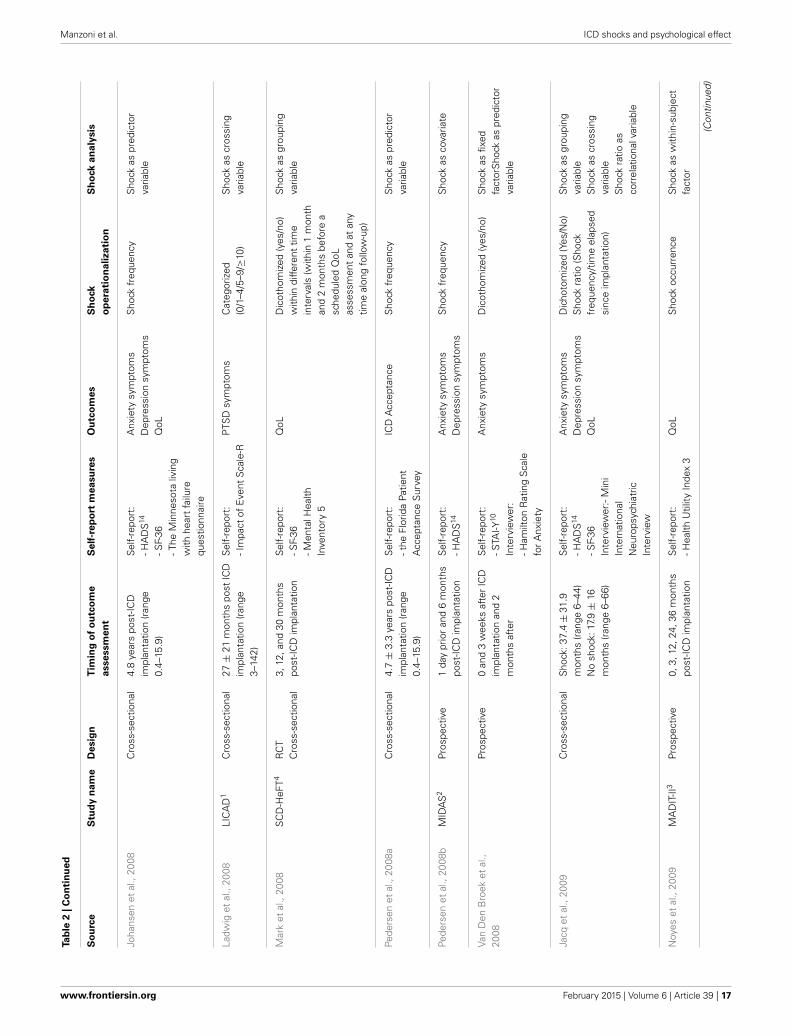
Manzoni et al. ICD shocks and psychological effect
Tab
le2
|C
on
tin
ued
So
urc
eS
tud
yn
am
eD
esig
nT
imin
go
fo
utc
om
e
asse
ssm
en
t
Self
-rep
ort
measu
res
Ou
tco
mes
Sh
ock
op
era
tio
nalizati
on
Sh
ock
an
aly
sis
Joha
nsen
etal
.,20
08C
ross
-sec
tiona
l4.
8ye
ars
post
-ICD
impl
anta
tion
(ran
ge0.
4–15
.9)
Sel
f-re
port
:-H
AD
S14
-SF-
36-T
heM
inne
sota
livin
gw
ithhe
art
failu
requ
estio
nnai
re
Anx
iety
sym
ptom
sD
epre
ssio
nsy
mpt
oms
QoL
Sho
ckfr
eque
ncy
Sho
ckas
pred
icto
rva
riabl
e
Ladw
iget
al.,
2008
LIC
AD
1C
ross
-sec
tiona
l27
±21
mon
ths
post
ICD
impl
anta
tion
(ran
ge3–
142)
Sel
f-re
port
:-I
mpa
ctof
Eve
ntS
cale
-RP
TSD
sym
ptom
sC
ateg
oriz
ed(0
/1–4
/5–9
/≥10
)S
hock
ascr
ossi
ngva
riabl
e
Mar
ket
al.,
2008
SC
D-H
eFT4
RC
TC
ross
-sec
tiona
l3,
12,a
nd30
mon
ths
post
-ICD
impl
anta
tion
Sel
f-re
port
:-S
F-36
-Men
talH
ealth
Inve
ntor
y5
QoL
Dic
otho
miz
ed(y
es/n
o)w
ithin
diffe
rent
time
inte
rval
s(w
ithin
1m
onth
and
2m
onth
sbe
fore
asc
hedu
led
QoL
asse
ssm
ent
and
atan
ytim
eal
ong
follo
w-u
p)
Sho
ckas
grou
ping
varia
ble
Pede
rsen
etal
.,20
08a
Cro
ss-s
ectio
nal
4.7
±3.
3ye
ars
post
-ICD
impl
anta
tion
(ran
ge0.
4–15
.9)
Sel
f-re
port
:-t
heFl
orid
aPa
tient
Acc
epta
nce
Sur
vey
ICD
Acc
epta
nce
Sho
ckfr
eque
ncy
Sho
ckas
pred
icto
rva
riabl
e
Pede
rsen
etal
.,20
08b
MID
AS
2Pr
ospe
ctiv
e1
day
prio
ran
d6
mon
ths
post
-ICD
impl
anta
tion
Sel
f-re
port
:-H
AD
S14
Anx
iety
sym
ptom
sD
epre
ssio
nsy
mpt
oms
Sho
ckfr
eque
ncy
Sho
ckas
cova
riate
Van
Den
Bro
eket
al.,
2008
Pros
pect
ive
0an
d3
wee
ksaf
ter
ICD
impl
anta
tion
and
2m
onth
saf
ter
Sel
f-re
port
:-S
TAI-Y
10
Inte
rvie
wer
:-H
amilt
onR
atin
gS
cale
for
Anx
iety
Anx
iety
sym
ptom
sD
icot
hom
ized
(yes
/no)
Sho
ckas
fixed
fact
orS
hock
aspr
edic
tor
varia
ble
Jacq
etal
.,20
09C
ross
-sec
tiona
lS
hock
:37.
4±
31.9
mon
ths
(ran
ge6–
44)
No
shoc
k:17
.9±
16m
onth
s(r
ange
6–66
)
Sel
f-re
port
:-H
AD
S14
-SF-
36In
terv
iew
er:-
Min
iIn
tern
atio
nal
Neu
rops
ychi
atric
Inte
rvie
w
Anx
iety
sym
ptom
sD
epre
ssio
nsy
mpt
oms
QoL
Dic
hoto
miz
ed(Y
es/N
o)S
hock
ratio
(Sho
ckfr
eque
ncy/
time
elap
sed
sinc
eim
plan
tatio
n)
Sho
ckas
grou
ping
varia
ble
Sho
ckas
cros
sing
varia
ble
Sho
ckra
tioas
corr
elat
iona
lvar
iabl
e
Noy
eset
al.,
2009
MA
DIT
-II3
Pros
pect
ive
0,3,
12,2
4,36
mon
ths
post
-ICD
impl
anta
tion
Sel
f-re
port
:-H
ealth
Util
ityIn
dex
3Q
oLS
hock
occu
rren
ceS
hock
asw
ithin
-sub
ject
fact
or
(Con
tinue
d)
www.frontiersin.org February 2015 | Volume 6 | Article 39 | 17
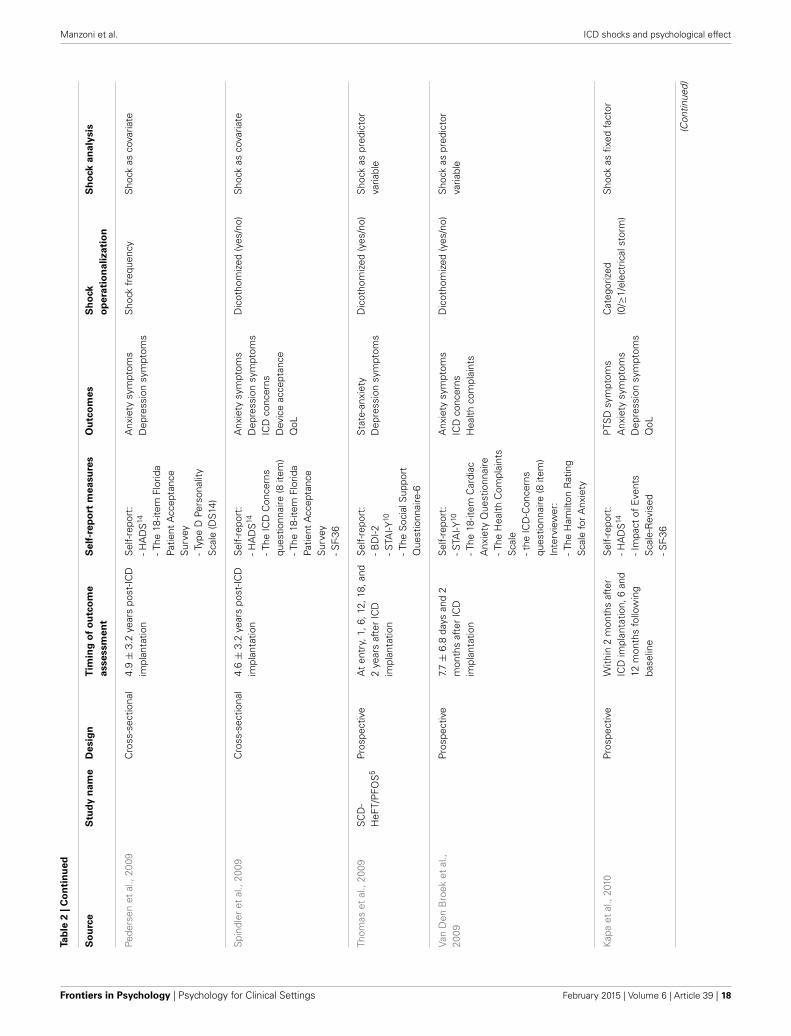
Manzoni et al. ICD shocks and psychological effect
Tab
le2
|C
on
tin
ued
So
urc
eS
tud
yn
am
eD
esig
nT
imin
go
fo
utc
om
e
asse
ssm
en
t
Self
-rep
ort
measu
res
Ou
tco
mes
Sh
ock
op
era
tio
nalizati
on
Sh
ock
an
aly
sis
Pede
rsen
etal
.,20
09C
ross
-sec
tiona
l4.
9±
3.2
year
spo
st-IC
Dim
plan
tatio
nS
elf-
repo
rt:
-HA
DS
14
-The
18-it
emFl
orid
aPa
tient
Acc
epta
nce
Sur
vey
-Typ
eD
Pers
onal
ityS
cale
(DS
14)
Anx
iety
sym
ptom
sD
epre
ssio
nsy
mpt
oms
Sho
ckfr
eque
ncy
Sho
ckas
cova
riate
Spi
ndle
ret
al.,
2009
Cro
ss-s
ectio
nal
4.6
±3.
2ye
ars
post
-ICD
impl
anta
tion
Sel
f-re
port
:-H
AD
S14
-The
ICD
Con
cern
squ
estio
nnai
re(8
item
)-T
he18
-item
Flor
ida
Patie
ntA
ccep
tanc
eS
urve
y-S
F-36
Anx
iety
sym
ptom
sD
epre
ssio
nsy
mpt
oms
ICD
conc
erns
Dev
ice
acce
ptan
ceQ
oL
Dic
otho
miz
ed(y
es/n
o)S
hock
asco
varia
te
Thom
aset
al.,
2009
SC
D-
HeF
T/P
FOS
5Pr
ospe
ctiv
eA
ten
try,
1,6,
12,1
8,an
d2
year
saf
ter
ICD
impl
anta
tion
Sel
f-re
port
:-B
DI-2
-STA
I-Y10
-The
Soc
ialS
uppo
rtQ
uest
ionn
aire
-6
Sta
te-a
nxie
tyD
epre
ssio
nsy
mpt
oms
Dic
otho
miz
ed(y
es/n
o)S
hock
aspr
edic
tor
varia
ble
Van
Den
Bro
eket
al.,
2009
Pros
pect
ive
7.7
±6.
8da
ysan
d2
mon
ths
afte
rIC
Dim
plan
tatio
n
Sel
f-re
port
:-S
TAI-Y
10
-The
18-it
emC
ardi
acA
nxie
tyQ
uest
ionn
aire
-The
Hea
lthC
ompl
aint
sS
cale
-the
ICD
-Con
cern
squ
estio
nnai
re(8
item
)In
terv
iew
er:
-The
Ham
ilton
Rat
ing
Sca
lefo
rA
nxie
ty
Anx
iety
sym
ptom
sIC
Dco
ncer
nsH
ealth
com
plai
nts
Dic
otho
miz
ed(y
es/n
o)S
hock
aspr
edic
tor
varia
ble
Kap
aet
al.,
2010
Pros
pect
ive
With
in2
mon
ths
afte
rIC
Dim
plan
tatio
n,6
and
12m
onth
sfo
llow
ing
base
line
Sel
f-re
port
:-H
AD
S14
-Im
pact
ofE
vent
sS
cale
-Rev
ised
-SF-
36
PTS
Dsy
mpt
oms
Anx
iety
sym
ptom
sD
epre
ssio
nsy
mpt
oms
QoL
Cat
egor
ized
(0/≥
1/el
ectr
ical
stor
m)
Sho
ckas
fixed
fact
or
(Con
tinue
d)
Frontiers in Psychology | Psychology for Clinical Settings February 2015 | Volume 6 | Article 39 | 18

Manzoni et al. ICD shocks and psychological effect
Tab
le2
|C
on
tin
ued
So
urc
eS
tud
yn
am
eD
esig
nT
imin
go
fo
utc
om
e
asse
ssm
en
t
Self
-rep
ort
measu
res
Ou
tco
mes
Sh
ock
op
era
tio
nalizati
on
Sh
ock
an
aly
sis
Pede
rsen
etal
.,20
10a
MID
AS
2Pr
ospe
ctiv
e1
day
prio
rto
ICD
impl
anta
tion
(bas
elin
e)an
d10
days
,3m
onth
s,6
mon
ths
and
1ye
arpo
st-IC
Dim
plan
tatio
n.
Sel
f-re
port
:-S
TAI-Y
10
-the
ICD
-Con
cern
squ
estio
nnai
re(8
item
)-T
ype
DPe
rson
ality
Sca
le(D
S14
)-M
ultid
imen
sion
alS
cale
ofPe
rcei
ved
Soc
ial
Sup
port
Sta
te-a
nxie
tyTr
ait-
anxi
ety
ICD
conc
erns
Sho
ckfr
eque
ncy
Sho
ckas
pred
icto
rva
riabl
e
Red
head
etal
.,20
10C
ross
-sec
tiona
l6-
mon
th“t
ime
win
dow
s”:6
–12,
12–1
8,18
–24,
24–3
0,an
d30
–36
mon
ths
post
-ICD
impl
anta
tion
Sel
f-re
port
:-H
AD
S14
-SF–
36
Anx
iety
sym
ptom
sD
epre
ssio
nsy
mpt
oms
QoL
Cat
egor
ized
(0/≥
1/st
orm
)S
hock
ascr
ossi
ngva
riabl
e
Suz
ukie
tal
.,20
10Pr
ospe
ctiv
eW
ithin
7da
ysbe
fore
impl
anta
tion
or8
±5
days
afte
rad
mis
sion
and
2ye
ars
late
r
Sel
f-re
port
:-Z
ung
Sel
f-R
atin
gD
epre
ssio
nS
cale
Dep
ress
ion
Dic
hoto
miz
ed(y
es/n
o)D
icho
tom
ized
(with
in6
mon
ths
/bey
ond
6m
onth
s)C
ateg
oriz
ed(0
,1–
9,≥1
0)
Sho
ckas
test
varia
ble
Dep
ress
edpa
tient
svs
.no
n-de
pres
sed
patie
nts
Vers
teeg
etal
.,20
10M
IDA
S2
Pros
pect
ive
3an
d6
mon
ths
post
-ICD
impl
anta
tion
Sel
f-re
port
:-T
hePo
sttr
aum
atic
Str
ess
Dia
gnos
ticS
cale
PTS
Dsy
mpt
oms
Sho
ckfr
eque
ncy
Sho
ckas
pred
icto
rva
riabl
e
Dic
kers
onet
al.,
2010
Pros
pect
ive
Bef
ore
and
1an
d3
mon
ths
afte
rIC
Dim
plan
tatio
n
Sel
f-re
port
:-S
TAI-Y
10
-the
Ferr
ans
and
Pow
ers
Qua
lity
ofLi
feIn
dex,
Car
diac
Vers
ion
Sta
te-a
nxie
tyS
hock
freq
uenc
yS
hock
aste
stva
riabl
eC
ompa
rison
ofQ
oL-c
hang
epa
tter
ns
Hab
ibov
icet
al.,
2012
Cro
ss-s
ectio
nal
0–3
wee
ksan
d18
mon
ths
post
-ICD
impl
anta
tion
Sel
f-re
port
:-S
TAI-Y
10
-the
Post
trau
mat
icS
tres
sD
iagn
ostic
Sca
le-T
ype
DPe
rson
ality
Sca
le(D
S14
)
PTS
Dsy
mpt
oms
Sho
ckfr
eque
ncy
Sho
ckas
pred
icto
rva
riabl
e
Pede
rsen
etal
.,20
11M
IDA
S2
Pros
pect
ive
0–3
wee
ksan
d12
mon
ths
post
-ICD
impl
anta
tion
Sel
f-re
port
:-S
TAI-Y
10
-Typ
eD
Pers
onal
ityS
cale
(DS
14)
Chr
onic
anxi
ety
Sho
ckfr
eque
ncy
Sho
ckas
pred
icto
rva
riabl
e
(Con
tinue
d)
www.frontiersin.org February 2015 | Volume 6 | Article 39 | 19
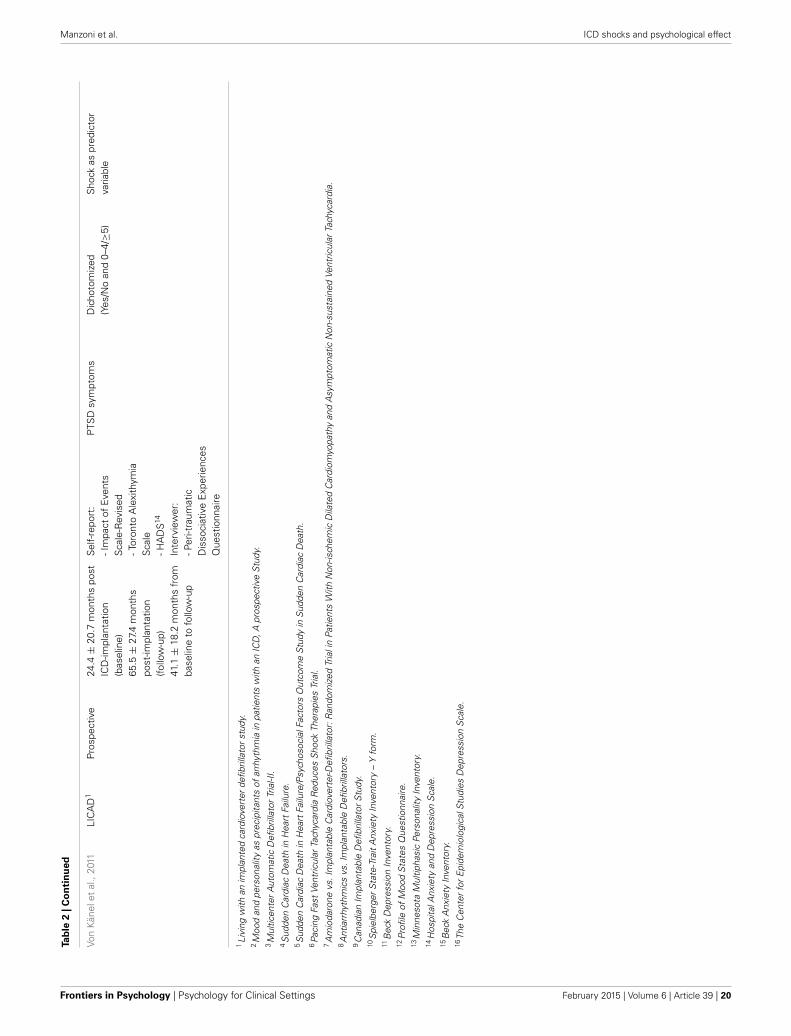
Manzoni et al. ICD shocks and psychological effect
Tab
le2
|C
on
tin
ued
Von
Kän
elet
al.,
2011
LIC
AD
1Pr
ospe
ctiv
e24
.4±
20.7
mon
ths
post
ICD
-impl
anta
tion
(bas
elin
e)65
.5±
27.4
mon
ths
post
-impl
anta
tion
(follo
w-u
p)41
.1±
18.2
mon
ths
from
base
line
tofo
llow
-up
Sel
f-re
port
:-I
mpa
ctof
Eve
nts
Sca
le-R
evis
ed-T
oron
toA
lexi
thym
iaS
cale
-HA
DS
14
Inte
rvie
wer
:-P
eri-t
raum
atic
Dis
soci
ativ
eE
xper
ienc
esQ
uest
ionn
aire
PTS
Dsy
mpt
oms
Dic
hoto
miz
ed(Y
es/N
oan
d0–
4/≥5
)S
hock
aspr
edic
tor
varia
ble
1Li
ving
with
anim
plan
ted
card
iove
rter
defib
rilla
tor
stud
y.2M
ood
and
pers
onal
ityas
prec
ipita
nts
ofar
rhyt
hmia
inpa
tient
sw
ithan
ICD
,Apr
ospe
ctiv
eS
tudy
.3M
ultic
ente
rA
utom
atic
Defi
brill
ator
Tria
l-II.
4S
udde
nC
ardi
acD
eath
inH
eart
Failu
re.
5S
udde
nC
ardi
acD
eath
inH
eart
Failu
re/P
sych
osoc
ialF
acto
rsO
utco
me
Stu
dyin
Sud
den
Car
diac
Dea
th.
6Pa
cing
Fast
Vent
ricul
arTa
chyc
ardi
aR
educ
esS
hock
Ther
apie
sTr
ial.
7A
mio
daro
nevs
.Im
plan
tabl
eC
ardi
over
ter-D
efibr
illat
or:R
ando
miz
edTr
iali
nPa
tient
sW
ithN
on-is
chem
icD
ilate
dC
ardi
omyo
path
yan
dA
sym
ptom
atic
Non
-sus
tain
edVe
ntric
ular
Tach
ycar
dia.
8A
ntia
rrhy
thm
ics
vs.I
mpl
anta
ble
Defi
brill
ator
s.9C
anad
ian
Impl
anta
ble
Defi
brill
ator
Stu
dy.
10S
piel
berg
erS
tate
-Tra
itA
nxie
tyIn
vent
ory
–Y
form
.11
Bec
kD
epre
ssio
nIn
vent
ory.
12Pr
ofile
ofM
ood
Sta
tes
Que
stio
nnai
re.
13M
inne
sota
Mul
tipha
sic
Pers
onal
ityIn
vent
ory.
14H
ospi
talA
nxie
tyan
dD
epre
ssio
nS
cale
.15
Bec
kA
nxie
tyIn
vent
ory.
16Th
eC
ente
rfo
rE
pide
mio
logi
calS
tudi
esD
epre
ssio
nS
cale
.
Frontiers in Psychology | Psychology for Clinical Settings February 2015 | Volume 6 | Article 39 | 20

Manzoni et al. ICD shocks and psychological effect
RISK OF BIAS WITHIN STUDIESAll papers that were included in the review were screened insearch of some potential biases that could affect the validity ofresults. In particular, we searched for the systematic biases thatcan affect the internal validity of cross-sectional and cohort stud-ies. In this kind of non-randomized studies, the major threatto internal validity concerns all the systematic differences thatmay exist between groups over and beyond the difference deter-mined by the factor of interest and that may confound its effect.One of the methods that can protect against this bias consistsin statistically controlling for the effects of all confounding vari-ables that are related to the outcome and/or to the factor. Afurther method consists in matching subjects between groupsaccording to some variables (for example, age, sex, type of heartdisease, LVEF, NYHA Functional Class, etc.) but this procedurewas used in only one study (Keren et al., 1991). All the otherstudies that attempted to reduce the risk of such a bias used themultiple regression method (35 out of 60). However, the num-ber and kind of confounding variables that were selected andcontrolled for vary significantly across studies. The effect of theICD shock was indeed adjusted for heterogeneous confoundersand this may partially explain why results are discordant. A fur-ther major threat to the internal validity of cross-sectional andcohort studies is the presence of the outcome of interest beforethe occurrence of the event that hypothetically causes it. Thisbias, when uncontrolled, may affect seriously the causal mean-ing of an association and, for example, may lead to the wrongconclusion that the ICD shock caused the development of psy-chological disorders when the reverse was true. The most robustmethod that may protect against this bias consists in starting theevaluation of patients quite before the ICD implantation and incollecting short-spaced repeated measures along the follow-up.This was fully accomplished in only 18 prospective studies, inwhich patients were evaluated for the first time few days beforesurgery. In all the other prospective studies, the baseline wasassessed after the ICD implantation. Anyway, for the issue of thereview, i.e., the critical appraisal of methods that were adoptedin studies on the psychological effect of ICD shock, the mostimportant part of the procedure is clearly the short-spaced timingof repeated measurements that, combined with the hierarchicalanalysis of intra-individual pre- to post-shock changes, repre-sents for us the best methodology for enhancing the internalvalidity of cohort studies whose aim is to evaluate the negativeeffect of ICD shock on patient’s health. Another method thatwas used in few studies consists in evaluating patients retrospec-tively. However, this approach is prone to biases (e.g., the recallbias and the response shift) that may affect seriously the validityand reliability of patients’ responses and that should be avoided.According to the Newcastle-Ottawa checklist, further threats tothe internal validity of cross-sectional and cohort studies are theself-reported exposure to the event, the self-reported assessmentof outcome, the low validity and reliability of outcome measuresand the incompleteness of data set. Except for this last bias, whichmay seriously affect the validity of results as much as the previ-ous major ones, all the other items were considered minor threatsbecause of their relative low and negligible impact on the validityof results.
RESULTS OF STUDIES AND SUBGROUP ANALYSISBecause of the great heterogeneity that was observed in methodsacross the included studies, a statistical meta-analysis of effectsand moderators was deemed unfeasible and was not performed.Further, no attempt was made to describe each study in a narrativemanner because of two reasons: (1) the large number of stud-ies that were included and (2) the review aim to focus mainly onmethods and to explore cross-sectionally their effects on results.Hence, key methodological features and results of each studywere only coded and tabulated (Tables 2, 3). For example, resultswere coded with 1 when a significant effect of ICD shock wasfound and with 0 otherwise. We established the statistical sig-nificance of effects only on the basis of final results (in studieswhere both bivariate and multivariate analyses were performed,we considered only the adjusted effects). A series of subgroupanalyses according to study design, shock operationalization,shock analysis and multivariate controlling was then performedonly on outcomes for which at least 20 studies were available(twenty units were deemed sufficient to test cross-sectional asso-ciations between methodological factors and results). Findingsare described in the following paragraphs for each outcome ofinterest.
AnxietyPatients’ anxiety was assessed as an outcome in 35 studies andit was mainly measured by self-report questionnaires. In RCTsthat were included in the review, anxiety was never measured. Astatistically significant effect of ICD shocks on self-reported anx-iety was found in 17 studies, while a significant effect of shockson interviewer-rated anxiety was found in only 1 study out of 3.Subgroup analyses (Fisher’s exact test) did not demonstrate anysignificant association between the methodological factors andthe statistical significance of the shock effect on anxiety.
DepressionPatients’ depression was assessed as an outcome in 29 studies and,as for anxiety, it was mainly measured by self-report question-naires. Even depression was never measured in the RCTs includedin the review. A statistically significant effect of ICD shocks onself-reported depression was detected in 10 studies, while a non-significant result was found in the only study in which depressionwas rated by a clinical interview. Subgroup analyses did notdemonstrate any significant association between the methodolog-ical factors and the statistical significance of the shock effect ondepression.
Health-related quality of lifePatients’ health-related quality of life was assessed as an outcomein 30 studies and was always measured with self-report question-naires. In most studies, both mental and physical componentswere evaluated, while in few studies only mental health (4 stud-ies) or physical health (3 studies) were evaluated. With respect tomental health or psychological well-being, a statistically signifi-cant effect of ICD shock was found in 12 studies out of 27, whilea statistically significant effect of ICD shock on physical healthwas detected in 11 studies out of 26. Subgroup analyses did not
www.frontiersin.org February 2015 | Volume 6 | Article 39 | 21
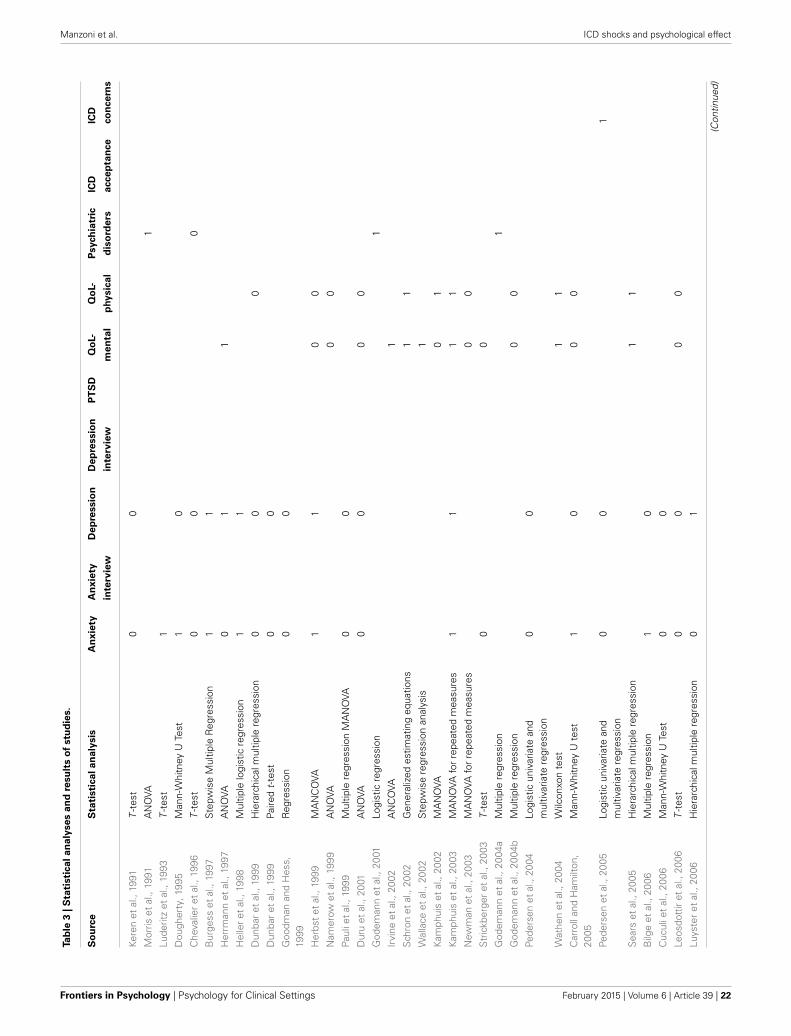
Manzoni et al. ICD shocks and psychological effect
Tab
le3
|S
tati
sti
ca
lan
aly
ses
an
dre
su
lts
of
stu
die
s.
So
urc
eS
tati
sti
calan
aly
sis
An
xie
tyA
nx
iety
De
pre
ssio
nD
ep
ressio
nP
TS
DQ
oL-
Qo
L-P
sych
iatr
icIC
DIC
D
inte
rvie
win
terv
iew
men
tal
ph
ysic
al
dis
ord
ers
accep
tan
ce
co
ncern
s
Kere
net
al.,
1991
T-t
est
00
Mor
riset
al.,
1991
AN
OVA
1
Lude
ritz
etal
.,19
93T
-tes
t1
Dou
gher
ty,1
995
Man
n-W
hitn
eyU
Test
10
Che
valie
ret
al.,
1996
T-t
est
00
0
Bur
gess
etal
.,19
97S
tepw
ise
Mul
tiple
Reg
ress
ion
11
Her
rman
net
al.,
1997
AN
OVA
01
1
Hel
ler
etal
.,19
98M
ultip
lelo
gist
icre
gres
sion
11
Dun
bar
etal
.,19
99H
iera
rchi
calm
ultip
lere
gres
sion
00
0
Dun
bar
etal
.,19
99Pa
ired
t-te
st0
0
Goo
dman
and
Hes
s,19
99R
egre
ssio
n0
0
Her
bst
etal
.,19
99M
AN
CO
VA1
10
0
Nam
erow
etal
.,19
99A
NO
VA0
0
Paul
iet
al.,
1999
Mul
tiple
regr
essi
onM
AN
OVA
00
Dur
uet
al.,
2001
AN
OVA
00
00
God
eman
net
al.,
2001
Logi
stic
regr
essi
on1
Irvi
neet
al.,
2002
AN
CO
VA1
Sch
ron
etal
.,20
02G
ener
aliz
edes
timat
ing
equa
tions
11
Wal
lace
etal
.,20
02S
tepw
ise
regr
essi
onan
alys
is1
Kam
phui
set
al.,
2002
MA
NO
VA0
1
Kam
phui
set
al.,
2003
MA
NO
VAfo
rre
peat
edm
easu
res
11
11
New
man
etal
.,20
03M
AN
OVA
for
repe
ated
mea
sure
s0
0
Str
ickb
erge
ret
al.,
2003
T-t
est
00
God
eman
net
al.,
2004
aM
ultip
lere
gres
sion
1
God
eman
net
al.,
2004
bM
ultip
lere
gres
sion
00
Pede
rsen
etal
.,20
04Lo
gist
icun
ivar
iate
and
mul
tivar
iate
regr
essi
on0
0
Wat
hen
etal
.,20
04W
ilcon
xon
test
11
Car
roll
and
Ham
ilton
,20
05M
ann-
Whi
tney
Ute
st1
00
0
Pede
rsen
etal
.,20
05Lo
gist
icun
ivar
iate
and
mul
tivar
iate
regr
essi
on0
01
Sea
rset
al.,
2005
Hie
rarc
hica
lmul
tiple
regr
essi
on1
1
Bilg
eet
al.,
2006
Mul
tiple
regr
essi
on1
0
Cuc
ulie
tal
.,20
06M
ann-
Whi
tney
UTe
st0
0
Leos
dott
iret
al.,
2006
T-t
est
00
00
Luys
ter
etal
.,20
06H
iera
rchi
calm
ultip
lere
gres
sion
01
(Con
tinue
d)
Frontiers in Psychology | Psychology for Clinical Settings February 2015 | Volume 6 | Article 39 | 22
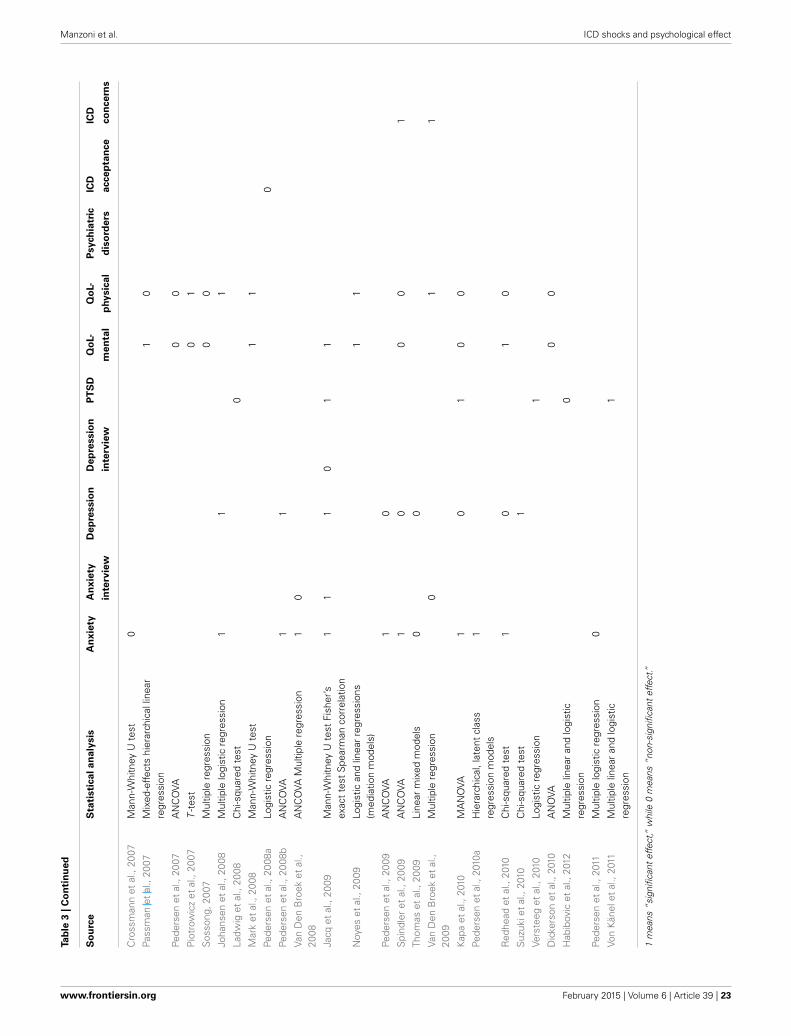
Manzoni et al. ICD shocks and psychological effect
Tab
le3
|C
on
tin
ued
So
urc
eS
tati
sti
calan
aly
sis
An
xie
tyA
nx
iety
De
pre
ssio
nD
ep
ressio
nP
TS
DQ
oL-
Qo
L-P
sych
iatr
icIC
DIC
D
inte
rvie
win
terv
iew
men
tal
ph
ysic
al
dis
ord
ers
accep
tan
ce
co
ncern
s
Cro
ssm
ann
etal
.,20
07M
ann-
Whi
tney
Ute
st0
Pass
man
etal
.,20
07M
ixed
-effe
cts
hier
arch
ical
linea
rre
gres
sion
10
Pede
rsen
etal
.,20
07A
NC
OVA
00
Pio
trow
icz
etal
.,20
07T
-tes
t0
1
Sos
song
,200
7M
ultip
lere
gres
sion
00
Joha
nsen
etal
.,20
08M
ultip
lelo
gist
icre
gres
sion
11
1
Ladw
iget
al.,
2008
Chi
-squ
ared
test
0
Mar
ket
al.,
2008
Man
n-W
hitn
eyU
test
11
Pede
rsen
etal
.,20
08a
Logi
stic
regr
essi
on0
Pede
rsen
etal
.,20
08b
AN
CO
VA1
1
Van
Den
Bro
eket
al.,
2008
AN
CO
VAM
ultip
lere
gres
sion
10
Jacq
etal
.,20
09M
ann-
Whi
tney
Ute
stFi
sher
’sex
act
test
Spe
arm
anco
rrel
atio
n1
11
01
1
Noy
eset
al.,
2009
Logi
stic
and
linea
rre
gres
sion
s(m
edia
tion
mod
els)
11
Pede
rsen
etal
.,20
09A
NC
OVA
10
Spi
ndle
ret
al.,
2009
AN
CO
VA1
00
01
Thom
aset
al.,
2009
Line
arm
ixed
mod
els
00
Van
Den
Bro
eket
al.,
2009
Mul
tiple
regr
essi
on0
11
Kap
aet
al.,
2010
MA
NO
VA1
01
00
Pede
rsen
etal
.,20
10a
Hie
rarc
hica
l,la
tent
clas
sre
gres
sion
mod
els
1
Red
head
etal
.,20
10C
hi-s
quar
edte
st1
01
0
Suz
ukie
tal
.,20
10C
hi-s
quar
edte
st1
Vers
teeg
etal
.,20
10Lo
gist
icre
gres
sion
1
Dic
kers
onet
al.,
2010
AN
OVA
00
Hab
ibov
icet
al.,
2012
Mul
tiple
linea
ran
dlo
gist
icre
gres
sion
0
Pede
rsen
etal
.,20
11M
ultip
lelo
gist
icre
gres
sion
0
Von
Kän
elet
al.,
2011
Mul
tiple
linea
ran
dlo
gist
icre
gres
sion
1
1m
eans
“sig
nific
ant
effe
ct,”
whi
le0
mea
ns“n
on-s
igni
fican
tef
fect
.”
www.frontiersin.org February 2015 | Volume 6 | Article 39 | 23

Manzoni et al. ICD shocks and psychological effect
demonstrate any significant association between the methodolog-ical factors and the statistical significance of the shock effect onquality of life.
Post-Traumatic Stress Disorder (PTSD)PTSD or PTSD symptoms were assessed as outcomes in five stud-ies and were always measured with self-report questionnaires. Astatistically significant effect of ICD shocks was found in 3 studies.
Psychiatric disordersIn four studies the effect of ICD shocks was assessed on psychi-atric diagnosis of mental disorders and in 3 out of them the effectwas statistically significant.
ICD acceptance and concernsICD acceptance was assessed as an outcome in 1 study but no sig-nificant effect of ICD shocks was found, while ICD concerns weremeasured in 3 studies and the effect of ICD shocks was statisticallysignificant in all of them.
DISCUSSIONThe critical appraisal of the mixed evidence concerning the rela-tionship between ICD shocks and patient-centered outcomes(mainly QoL, anxiety and depression) is the main content of threerecently published papers (Pedersen and Van Den Broek, 2008;Pedersen et al., 2010b; Sears and Kirian, 2010). Despite slightlydifferent paradigmatic views on the relative importance of ICDshocks within the group of the numerous factors that may neg-atively influence the psychological adaptation and well-being ofimplanted patients, the authors agree that the heterogeneity ofdesigns and methods across studies is most likely to account forthe mixed findings.
The quasi-quantitative results of our review do not sup-port this hypothesis. In particular, study design (cross-sectionalvs. prospective studies), shock operationalization (the way ICDshocks were operationalized/quantified), shock analysis (the waythe effect of ICD shocks was tested) and control for confound-ing (bivariate vs. multivariate analyses) were examined in vote-counting subgroup analysis, but statistical evidence was null foreach of them.
As already noted by Pedersen et al. in a recent viewpoint(2010b), results are mixed even in the subgroup of RCTs. Hence,it seems that the statistical significance of the ICD shock effecton patients’ QoL (anxiety and depression were not measured inRCTs) does not depend strictly on sample size. Furthermore, con-trary to the hypothesis that a dose-response relationship may existbetween the number of shocks and QoL, with only patients expe-riencing ≥5 shocks being at risk for impaired QoL (Irvine et al.,2002; Pedersen et al., 2010b), studies that categorized the shockvariable in classes of increasing shock incidence (e.g., 0–4 vs. 5–9vs. ≥10 shocks) did not show consistent significant results in anyof the outcomes of interest.
However, such null evidence is far from being conclusive. Thissystematic review shows clearly that methods are very hetero-geneous across studies and suggests that such methodologicaldifferences should be considered in a multivariate fashion ratherthan bivariately. However, subgrouping the included studies in
a multivariate manner is unfeasible because it would parcel outstudies in a number of cells that would be too small for validstatistical analysis.
Subgroup analyses were not performed on the few studies thatevaluated the effect of ICD shock on PTSD development or PTSDsymptoms, psychiatric disorders, ICD acceptance and ICD con-cerns. With the exception of the five studies that assessed PTSDand whose results are mixed as well, the evidences pertaining tothe psychiatric diagnosis of mental disorders (4 studies) and toICD concerns (3 studies) are consistently significant and sup-port the hypothesis that one or more ICD shocks may causethe development of a psychiatric disorder and the hypothesisthat shocked patients have significantly more concerns aboutthe ICD. However, the strength of the former evidences is lowbecause the very few studies that tested the effect of ICD shockon mental disorders used a cross-sectional approach. In none ofthem patients were actually administered the psychiatric inter-view before ICD implantation and the mental disorders thatwere diagnosed long after implantation might have been alreadypresent before or immediately after, even before the occurrence ofthe first shock. Despite the severe limitations of a vote-countingapproach, the attempt to explore whether methodological dif-ferences across studies account for the mixed findings of theliterature on the effect of ICD shocks on patients’ QoL, anxietyand depression was not vain because it allowed the full discov-ery of the wide and multiple heterogeneities that exist acrossstudies. Furthermore, it allowed the discovery of severe method-ological flaws, the most important of which are undoubtedly thecross-sectional design that was applied by the great part of stud-ies and the multiple wrong ways that were used to operationalizeshocks.
Our description is not comprehensive inasmuch as otherhypothetical accounting factors were intentionally overlooked.Some information on demographics (age and sex), ICD indi-cation (primary or secondary prevention) and both inclusionand exclusion criteria was extracted from studies and tabulated(Table 1), but any explorative attempt to meta-correlate themwith the significance of the shock effect failed. However, in manyof the studies that were included in this review, a variety ofpatient characteristics (demographic, clinical, psychological, etc.)was considered for explaining why, in some patients, QoL andpsychological health deteriorate after ICD implantation. Suchvariables were also entered in multivariate analyses together withICD shocks, but their effects on patient-centered outcomes weremainly examined as competitors of ICD shocks. Surprisingly, onlyone study tested the moderating effect of a patient characteristic(i.e., Type-D personality) on the relationship between shocks andpsychological distress (anxiety and depression) (Pedersen et al.,2004). A significant interaction (Type-D × Shocks ≥1) was foundonly for depression, i.e., ICD patients who received one or moreshocks and had a type D personality (negative affectivity andsocial inhibition) reported an higher mean level of depressionthan ICD patients who received one or more shocks and hadnot a type D personality. However, this interesting result receivedno consideration in the discussion, probably because the authorswere more concerned in looking beyond shocks toward otherdeterminants such as the type-D personality.
Frontiers in Psychology | Psychology for Clinical Settings February 2015 | Volume 6 | Article 39 | 24

Manzoni et al. ICD shocks and psychological effect
CONCLUSIONSClinical practice suggests that ICD shocks have a detrimentaleffect on patients’ QoL and account for the development of anx-iety and depression disorders. However, results of studies thathave investigated this issue are discordant. The heterogeneity ofdesigns and methods has been ascribed as the main reason for thediscrepancy but our findings do not support such hypothesis.
The attempt to solve the problem with a quasi-quantitativeapproach was daring due to its severe limitations but no othermeta-analytic approach was feasible. Regardless of this, the sys-tematic review allowed us to look more clearly at studies and topaint a partial picture of the current status of research on theimpact of ICD shocks on patient-centered outcomes.
We think that drawing firm statements about the short, midand long-term impact of ICD shocks on patients’ QoL and psy-chological well-being is an important matter both for the optimalclinical management of patients and for the adoption of new ICDprogramming strategies that eliminate or reduce ICD shocks. It isthus imperative that research on the psychological effects of ICDshocks goes further. Future studies should avoid the methodologi-cal flaws described in this review and should also consider that therelationship between ICD shocks and patient-centered outcomesmay not be as straightforward as expected. Some other putativevariables such as personality traits (e.g., Type D personality), cop-ing skills and social support play surely a role and their effects onICD patients’ psychological health should be investigated also ininteraction with the occurrence of shocks in order to know theprofile of patients who might respond badly and focus treatmentresources on them.
REFERENCESAnderson, J. L., Hallstrom, A. P., Epstein, A. E., Pinski, S. L., Rosenberg, Y., Nora, M.
O., et al. (1999). Design and results of the antiarrhythmics vs implantable defib-rillators (AVID) registry. The AVID Investigators. Circulation 99, 1692–1699.
Bardy, G. H., Lee, K. L., Mark, D. B., Poole, J. E., Packer, D. L., Boineau, R., et al.(2005). Amiodarone or an implantable cardioverter-defibrillator for congestiveheart failure. N. Engl. J. Med. 352, 225–237. doi: 10.1056/NEJMoa043399
Barnay, C., Taieb, J., and Morice, R. (2007). [Electrical storm]. Ann. Cardiol.Angeiol. 56, 183–187. doi: 10.1016/j.ancard.2007.08.003
Bilge, A. K., Ozben, B., Demircan, S., Cinar, M., Yilmaz, E., and Adalet, K. (2006).Depression and anxiety status of patients with implantable cardioverter defib-rillator and precipitating factors. Pacing Clin. Electrophysiol. 29, 619–626. doi:10.1111/j.1540-8159.2006.00409.x
Burgess, E. S., Quigley, J. F., Moran, G., Sutton, F. J., and Goodman, M. (1997).Predictors of psychosocial adjustment in patients with implantable cardioverterdefibrillators. Pacing Clin. Electrophysiol. 20, 1790–1795.
Burke, J. L., Hallas, C. N., Clark-Carter, D., White, D., and Connelly, D.(2003). The psychosocial impact of the implantable cardioverter defib-rillator: a meta-analytic review. Br. J. Health Psychol. 8, 165–178. doi:10.1348/135910703321649141
Buxton, A. E., Lee, K. L., Fisher, J. D., Josephson, M. E., Prystowsky, E.N., and Hafley, G. (1999). A randomized study of the prevention of sud-den death in patients with coronary artery disease. Multicenter unsus-tained tachycardia trial investigators. N. Engl. J. Med. 341, 1882–1890. doi:10.1056/NEJM199912163412503
Carroll, D. L., and Hamilton, G. A. (2005). Quality of life in implanted cardioverterdefibrillator recipients: the impact of a device shock. Heart Lung. 34, 169–178.doi: 10.1016/j.hrtlng.2004.10.002
Chevalier, P., Verrier, P., Kirkorian, G., Touboul, P., and Cottraux, J. (1996).Improved appraisal of the quality of life in patients with automatic implantablecardioverter defibrillator: a psychometric study. Psychother. Psychosom. 65,49–56.
Connolly, S. J., Gent, M., Roberts, R. S., Dorian, P., Roy, D., Sheldon, R. S., et al.(2000a). Canadian implantable defibrillator study (CIDS): a randomized trial ofthe implantable cardioverter defibrillator against amiodarone. Circulation 101,1297–1302. doi: 10.1161/01.CIR.101.11.1297
Connolly, S. J., Hallstrom, A. P., Cappato, R., Schron, E. B., Kuck, K. H.,Zipes, D. P., et al. (2000b). Meta-analysis of the implantable cardioverterdefibrillator secondary prevention trials. AVID, CASH and CIDS studies.Antiarrhythmics vs Implantable Defibrillator study. Cardiac Arrest StudyHamburg. Canadian Implantable Defibrillator Study. Eur. Heart J. 21,2071–2078. doi: 10.1053/euhj.2000.2476 S0195668X0092476X [pii]
Crossmann, A., Pauli, P., Dengler, W., Kuhlkamp, V., and Wiedemann, G. (2007).Stability and cause of anxiety in patients with an implantable cardioverter-defibrillator: a longitudinal two-year follow-up. Heart Lung. 36, 87–95. doi:10.1016/j.hrtlng.2006.08.001
Cuculi, F., Herzig, W., Kobza, R., and Erne, P. (2006). Psychological distressin patients with ICD recall. Pacing Clin. Electrophysiol. 29, 1261–1265. doi:10.1111/j.1540-8159.2006.00523.x
Dickerson, S. S., Kennedy, M., Wu, Y. W., Underhill, M., and Othman, A. (2010).Factors related to quality-of-life pattern changes in recipients of implantabledefibrillators. Heart Lung. 39, 466–476. doi: 10.1016/j.hrtlng.2009.10.022
Dougherty, C. M. (1995). Psychological reactions and family adjustment in shockversus no shock groups after implantation of internal cardioverter defibrillator.Heart Lung. 24, 281–291.
Dunbar, S. B., Jenkins, L. S., Hawthorne, M., Kimble, L. P., Dudley, W. N.,Slemmons, M., et al. (1999). Factors associated with outcomes 3 months afterimplantable cardioverter defibrillator insertion. Heart Lung. 28, 303–315. doi:10.1053/hl.1999.v28.a101052
Duru, F., Buchi, S., Klaghofer, R., Mattmann, H., Sensky, T., Buddeberg, C., et al.(2001). How different from pacemaker patients are recipients of implantablecardioverter-defibrillators with respect to psychosocial adaptation, affectivedisorders, and quality of life? Heart 85, 375–379. doi: 10.1136/heart.85.4.375
Godemann, F., Ahrens, B., Behrens, S., Berthold, R., Gandor, C., Lampe, F., et al.(2001). Classic conditioning and dysfunctional cognitions in patients with panicdisorder and agoraphobia treated with an implantable cardioverter/defibrillator.Psychosom Med 63, 231–238. doi: 10.1097/00006842-200103000-00006
Godemann, F., Butter, C., Lampe, F., Linden, M., Schlegl, M., Schultheiss, H.P., et al. (2004a). Panic disorders and agoraphobia: side effects of treatmentwith an implantable cardioverter/defibrillator. Clin. Cardiol. 27, 321–326. doi:10.1002/clc.4960270604
Godemann, F., Butter, C., Lampe, F., Linden, M., Werner, S., and Behrens,S. (2004b). Determinants of the quality of life (QoL) in patients with animplantable cardioverter/defibrillator (ICD). Qual. Life Res. 13, 411–416.
Goodman, M., and Hess, B. (1999). Could implantable cardioverter defibrilla-tors provide a human model supporting the learned helplessness theory ofdepression? Gen. Hosp. Psychiatry 21, 382–385.
Habibovic, M., Van Den Broek, K. C., Alings, M., Van Der Voort, P. H., andDenollet, J. (2012). Posttraumatic stress 18 months following cardioverterdefibrillator implantation: shocks, anxiety, and personality. Health Psychol. 31,186–193. doi: 10.1037/a0024701
Heller, S. S., Ormont, M. A., Lidagoster, L., Sciacca, R. R., and Steinberg, S. (1998).Psychosocial outcome after ICD implantation: a current perspective. PacingClin. Electrophysiol. 21, 1207–1215.
Herbst, J. H., Goodman, M., Feldstein, S., and Reilly, J. M. (1999). Health-related quality-of-life assessment of patients with life-threatening ventriculararrhythmias. Pacing Clin. Electrophysiol. 22(6 Pt 1), 915–926.
Herrmann, C., Von Zur Muhen, F., Schaumann, A., Buss, U., Kemper, S.,Wantzen, C., et al. (1997). Standardized assessment of psychological well-being and quality-of-life in patients with implanted defibrillators. Pacing Clin.Electrophysiol. 20, 95–103.
Irvine, J., Dorian, P., Baker, B., O’brien, B. J., Roberts, R., Gent, M., et al. (2002).Quality of life in the Canadian Implantable Defibrillator Study (CIDS). Am.Heart J. 144, 282–289. doi: 10.1067/mjh.2002.124049
Jacq, F., Foulldrin, G., Savoure, A., Anselme, F., Baguelin-Pinaud, A., Cribier,A., et al. (2009). A comparison of anxiety, depression and quality oflife between device shock and nonshock groups in implantable car-dioverter defibrillator recipients. Gen. Hosp. Psychiatry 31, 266–273. doi:10.1016/j.genhosppsych.2009.01.003
Johansen, J. B., Pedersen, S. S., Spindler, H., Andersen, K., Nielsen, J. C., andMortensen, P. T. (2008). Symptomatic heart failure is the most important
www.frontiersin.org February 2015 | Volume 6 | Article 39 | 25

Manzoni et al. ICD shocks and psychological effect
clinical correlate of impaired quality of life, anxiety, and depression inimplantable cardioverter-defibrillator patients: a single-centre, cross-sectionalstudy in 610 patients. Europace 10, 545–551. doi: 10.1093/europace/eun073
Kamphuis, H. C., De Leeuw, J. R., Derksen, R., Hauer, R., and Winnubst, J. A.(2002). A 12-month quality of life assessment of cardiac arrest survivors treatedwith or without an implantable cardioverter defibrillator. Europace 4, 417–425.doi: 10.1053/eupc.2002.0258
Kamphuis, H. C., De Leeuw, J. R., Derksen, R., Hauer, R. N., and Winnubst, J. A.(2003). Implantable cardioverter defibrillator recipients: quality of life in recip-ients with and without ICD shock delivery: a prospective study. Europace 5,381–389. doi: 10.1016/S1099-5129(03)00078-3
Kapa, S., Rotondi-Trevisan, D., Mariano, Z., Aves, T., Irvine, J., Dorian, P.,et al. (2010). Psychopathology in patients with ICDs over time: results of aprospective study. Pacing Clin. Electrophysiol. 33, 198–208. doi: 10.1111/j.1540-8159.2009.02599.x
Keren, A., Sears, S. F., Nery, P., Shaw, J., Green, M. S., Lemery, R., et al. (2011).Psychological adjustment in ICD patients living with advisory fidelis leads.J. Cardiovasc. Electrophysiol. 22, 57–63. doi: 10.1111/j.1540-8167.2010.01867.x
Keren, R., Aarons, D., and Veltri, E. P. (1991). Anxiety and depression in patientswith life-threatening ventricular arrhythmias: impact of the implantablecardioverter-defibrillator. Pacing Clin. Electrophysiol. 14, 181–187.
Kuck, K. H., Cappato, R., Siebels, J., and Ruppel, R. (2000). Randomized compar-ison of antiarrhythmic drug therapy with implantable defibrillators in patientsresuscitated from cardiac arrest: the Cardiac Arrest Study Hamburg (CASH).Circulation 102, 748–754. doi: 10.1161/01.CIR.102.7.748
Ladwig, K. H., Baumert, J., Marten-Mittag, B., Kolb, C., Zrenner, B., and Schmitt,C. (2008). Posttraumatic stress symptoms and predicted mortality in patientswith implantable cardioverter-defibrillators: results from the prospective liv-ing with an implanted cardioverter-defibrillator study. Arch. Gen. Psychiatry 65,1324–1330. doi: 10.1001/archpsyc.65.11.1324
Leosdottir, M., Sigurdsson, E., Reimarsdottir, G., Gottskalksson, G., Torfason,B., Vigfusdottir, M., et al. (2006). Health-related quality of life of patientswith implantable cardioverter defibrillators compared with that of pacemakerrecipients. Europace 8, 168–174. doi: 10.1093/europace/euj052
Liberati, A., Altman, D. G., Tetzlaff, J., Mulrow, C., Gotzsche, P. C., Ioannidis, J.P., et al. (2009). The PRISMA statement for reporting systematic reviews andmeta-analyses of studies that evaluate health care interventions: explanation andelaboration. Ann. Intern. Med. 151, W65–W94. doi: 10.7326/0003-4819-151-4-200908180-00136
Luderitz, B., Jung, W., Deister, A., Marneros, A., and Manz, M. (1993). Patientacceptance of the implantable cardioverter defibrillator in ventricular tach-yarrhythmias. Pacing Clin. Electrophysiol. 16, 1815–1821.
Luyster, F. S., Hughes, J. W., Waechter, D., and Josephson, R. (2006). Resource losspredicts depression and anxiety among patients treated with an implantablecardioverter defibrillator. Psychosom. Med. 68, 794–800. doi: 10.1097/01.psy.0000227722.92307.35
Mark, D. B., Anstrom, K. J., Sun, J. L., Clapp-Channing, N. E., Tsiatis, A.A., Davidson-Ray, L., et al. (2008). Quality of life with defibrillator ther-apy or amiodarone in heart failure. N. Engl. J. Med. 359, 999–1008. doi:10.1056/NEJMoa0706719
Mishkin, J. D., Saxonhouse, S. J., Woo, G. W., Burkart, T. A., Miles, W. M., Conti, J.B., et al. (2009). Appropriate evaluation and treatment of heart failure patientsafter implantable cardioverter-defibrillator discharge: time to go beyond theinitial shock. J. Am. Coll. Cardiol. 54, 1993–2000. doi: 10.1016/j.jacc.2009.07.039
Morris, P. L., Badger, J., Chmielewski, C., Berger, E., and Goldberg, R. J. (1991).Psychiatric morbidity following implantation of the automatic implantablecardioverter defibrillator. Psychosomatics 32, 58–64.
Moss, A. J., Zareba, W., Hall, W. J., Klein, H., Wilber, D. J., Cannom, D. S.,et al. (2002). Prophylactic implantation of a defibrillator in patients withmyocardial infarction and reduced ejection fraction. Multicenter AutomaticDefibrillator Implantation Trial II Investigators. N. Engl. J. Med. 346, 877–883.doi: 10.1056/NEJMoa013474 NEJMoa013474 [pii]
Namerow, P. B., Firth, B. R., Heywood, G. M., Windle, J. R., and Parides, M. K.(1999). Quality-of-life six months after CABG surgery in patients randomizedto ICD versus no ICD therapy: findings from the CABG Patch Trial. Pacing Clin.Electrophysiol. 22, 1305–1313.
Newman, D. M., Dorian, P., Paquette, M., Sulke, N., Gold, M. R., Schwartzman, D.S., et al. (2003). Effect of an implantable cardioverter defibrillator with atrial
detection and shock therapies on patient-perceived, health-related quality oflife. Am. Heart J. 145, 841–846. doi: 10.1016/S0002-8703(02)94817-9
Noyes, K., Corona, E., Veazie, P., Dick, A. W., Zhao, H., and Moss, A. J.(2009). Examination of the effect of implantable cardioverter-defibrillatorson health-related quality of life: based on results from the MulticenterAutomatic Defibrillator Trial-II. Am. J. Cardiovasc. Drugs 9, 393–400. doi:10.2165/11317980-000000000-00000
Passman, R., Subacius, H., Ruo, B., Schaechter, A., Howard, A., Sears, S. F., et al.(2007). Implantable cardioverter defibrillators and quality of life: results fromthe defibrillators in nonischemic cardiomyopathy treatment evaluation study.Arch. Intern. Med. 167, 2226–2232. doi: 10.1001/archinte.167.20.2226
Pauli, P., Wiedemann, G., Dengler, W., Blaumann-Benninghoff, G., and Kuhlkamp,V. (1999). Anxiety in patients with an automatic implantable cardioverter defib-rillator: what differentiates them from panic patients? Psychosom. Med. 61,69–76.
Pedersen, S. S., den Broek, K. C., Theuns, D. A., Erdman, R. A., Alings, M., Meijer,A., et al. (2011). Risk of chronic anxiety in implantable defibrillator patients:a multi-center study. Int. J. Cardiol. 147, 420–423. doi: 10.1016/j.ijcard.2009.09.549
Pedersen, S. S., Spindler, H., Johansen, J. B., and Mortensen, P. T. (2009). Clusteringof poor device acceptance and Type D personality is associated with increaseddistress in Danish cardioverter-defibrillator patients. Pacing Clin. Electrophysiol.32, 29–36. doi: 10.1111/j.1540-8159.2009.02173.x
Pedersen, S. S., Spindler, H., Johansen, J. B., Mortensen, P. T., and Sears, S. F.(2008a). Correlates of patient acceptance of the cardioverter defibrillator: cross-validation of the Florida patient acceptance survey in Danish patients. PacingClin. Electrophysiol. 31, 1168–1177. doi: 10.1111/j.1540-8159.2008.01158.x
Pedersen, S. S., Theuns, D. A., Erdman, R. A., and Jordaens, L. (2008b). Clusteringof device-related concerns and type D personality predicts increased distress inICD patients independent of shocks. Pacing Clin. Electrophysiol. 31, 20–27. doi:10.1111/j.1540-8159.2007.00921.x
Pedersen, S. S., Theuns, D. A., Jordaens, L., and Kupper, N. (2010a). Courseof anxiety and device-related concerns in implantable cardioverter defibril-lator patients the first year post implantation. Europace 12, 1119–1126. doi:10.1093/europace/euq154
Pedersen, S. S., Theuns, D. A., Muskens-Heemskerk, A., Erdman, R.A., and Jordaens, L. (2007). Type-D personality but not implantablecardioverter-defibrillator indication is associated with mpaired health-related quality of life 3 months post-implantation. Europace 9, 675–680. doi:10.1093/europace/eum041
Pedersen, S. S., and Van Den Broek, K. C. (2008). Implantable cardioverter-defibrillator shocks and their adverse impact on patient-centered outcomes: factor fiction? J. Am. Coll. Cardiol. 52, 1037–1038. doi: 10.1016/j.jacc.2008.04.066
Pedersen, S. S., Van Den Broek, K. C., Van Den Berg, M., and Theuns, D. A. (2010b).Shock as a determinant of poor patient-centered outcomes in implantable car-dioverter defibrillator patients: is there more to it than meets the eye? PacingClin. Electrophysiol. 33, 1430–1436. doi: 10.1111/j.1540-8159.2010.02845.x
Pedersen, S. S., Van Domburg, R. T., Theuns, D. A., Jordaens, L., andErdman, R. A. (2004). Type D personality is associated with increasedanxiety and depressive symptoms in patients with an implantable car-dioverter defibrillator and their partners. Psychosom Med. 66, 714–719. doi:10.1097/01.psy.0000132874.52202.21 66/5/714 [pii]
Pedersen, S. S., Van Domburg, R. T., Theuns, D. A., Jordaens, L., and Erdman, R. A.(2005). Concerns about the implantable cardioverter defibrillator: a determi-nant of anxiety and depressive symptoms independent of experienced shocks.Am. Heart J. 149, 664–669. doi: 10.1016/j.ahj.2004.06.031
Piotrowicz, K., Noyes, K., Lyness, J. M., Mcnitt, S., Andrews, M. L., Dick, A.,et al. (2007). Physical functioning and mental well-being in association withhealth outcome in patients enrolled in the multicenter automatic defibrilla-tor implantation Trial II. Eur. Heart J. 28, 601–607. doi: 10.1093/eurheartj/ehl485
Redhead, A. P., Turkington, D., Rao, S., Tynan, M. M., and Bourke, J. P. (2010).Psychopathology in postinfarction patients implanted with cardioverter-defibrillators for secondary prevention. A cross-sectional, case-controlled study.J. Psychosom. Res. 69, 555–563. doi: 10.1016/j.jpsychores.2010.06.002
Schron, E. B., Exner, D. V., Yao, Q., Jenkins, L. S., Steinberg, J. S., Cook, J. R., et al.(2002). Quality of life in the antiarrhythmics versus implantable defibrillatorstrial: impact of therapy and influence of adverse symptoms and defibrillatorshocks. Circulation 105, 589–594. doi: 10.1161/hc0502.103330
Frontiers in Psychology | Psychology for Clinical Settings February 2015 | Volume 6 | Article 39 | 26

Manzoni et al. ICD shocks and psychological effect
Sears, S. F., and Kirian, K. (2010). Shock and patient-centered outcomes research:is an ICD shock still a critical event? Pacing Clin. Electrophysiol. 33, 1437–1441.doi: 10.1111/j.1540-8159.2010.02872.x
Sears, S. F., Lewis, T. S., Kuhl, E. A., and Conti, J. B. (2005). Predictors of quality oflife in patients with implantable cardioverter defibrillators. Psychosomatics 46,451–457. doi: 10.1176/appi.psy.46.5.451
Sears, S. F., Sowell, L. V., Kuhl, E. A., Handberg, E. M., Kron, J., Aranda, J. M.Jr., et al. (2006). Quality of death: implantable cardioverter defibrillators andproactive care. Pacing Clin. Electrophysiol. 29, 637–642. doi: 10.1111/j.1540-8159.2006.00412.x
Sears, S. F. Jr., Todaro, J. F., Lewis, T. S., Sotile, W., and Conti, J. B. (1999).Examining the psychosocial impact of implantable cardioverter defibrillators:a literature review. Clin. Cardiol. 22, 481–489.
Sossong, A. (2007). Living with an implantable cardioverter defibrillator: patientoutcomes and the nurse’s role. J. Cardiovasc. Nurs. 22, 99–104.
Spindler, H., Johansen, J. B., Andersen, K., Mortensen, P., and Pedersen, S. S.(2009). Gender differences in anxiety and concerns about the cardioverterdefibrillator. Pacing Clin. Electrophysiol. 32, 614–621. doi: 10.1111/j.1540-8159.2009.02334.x
Strickberger, S. A., Hummel, J. D., Bartlett, T. G., Frumin, H. I., Schuger, C. D.,Beau, S. L., et al. (2003). Amiodarone versus implantable cardioverter-defibrillator:randomized trial in patients with nonischemic dilatedcardiomyopathy and asymptomatic nonsustained ventricular tachycardia–AMIOVIRT. J. Am. Coll. Cardiol. 41, 1707–1712. doi: 10.1016/S0735-1097(03)00297-3
Suzuki, T., Shiga, T., Kuwahara, K., Kobayashi, S., Suzuki, S., Nishimura, K., et al.(2010). Prevalence and persistence of depression in patients with implantablecardioverter defibrillator: a 2-year longitudinal study. Pacing Clin. Electrophysiol.33, 1455–1461. doi: 10.1111/j.1540-8159.2010.02887.x
Thomas, S. A., Friedmann, E., Gottlieb, S. S., Liu, F., Morton, P. G., Chapa, D. W.,et al. (2009). Changes in psychosocial distress in outpatients with heart failurewith implantable cardioverter defibrillators. Heart and Lung: the J. Critical Care38, 109–120.
Van Den Broek, K. C., Nyklicek, I., and Denollet, J. (2009). Anxiety predicts poorperceived health in patients with an implantable defibrillator. Psychosomatics 50,483–492. doi: 10.1176/appi.psy.50.5.483
Van Den Broek, K. C., Nyklicek, I., Van Der Voort, P. H., Alings, M., and Denollet,J. (2008). Shocks, personality, and anxiety in patients with an implantable
defibrillator. Pacing Clin. Electrophysiol. 31, 850–857. doi: 10.1111/j.1540-8159.2008.01099.x
Versteeg, H., Theuns, D. A., Erdman, R. A., Jordaens, L., and Pedersen, S. S.(2010). Posttraumatic stress in implantable cardioverter defibrillator patients:the role of pre-implantation distress and shocks. Int. J. Cardiol. 146, 438–439.doi: 10.1016/j.ijcard.2010.10.108
Von Känel, R., Baumert, J., Kolb, C., Cho, E.-Y. N., and Ladwig, K.-H. (2011).Chronic posttraumatic stress and its predictors in patients living with animplantable cardioverter defibrillator. J. Affect. Disord. 131, 344–352. doi:10.1016/j.jad.2010.12.002
Wallace, R. L., Sears, S. F. Jr., Lewis, T. S., Griffis, J. T., Curtis, A., and Conti, J.B. (2002). Predictors of quality of life in long-term recipients of implantablecardioverter defibrillators. J. Cardiopulm. Rehabil. 22, 278–281.
Wathen, M. S., Degroot, P. J., Sweeney, M. O., Stark, A. J., Otterness, M. F.,Adkisson, W. O., et al. (2004). Prospective randomized multicenter trial ofempirical antitachycardia pacing versus shocks for spontaneous rapid ven-tricular tachycardia in patients with implantable cardioverter-defibrillators:pacing fast ventricular tachycardia reduces shock therapies (PainFREE Rx II)trial results. Circulation 110, 2591–2596. doi: 10.1161/01.CIR.0000145610.64014.E4
Conflict of Interest Statement: The authors declare that the research was con-ducted in the absence of any commercial or financial relationships that could beconstrued as a potential conflict of interest.
Received: 05 September 2014; paper pending published: 05 November 2014; accepted:08 January 2015; published online: 04 February 2015.Citation: Manzoni GM, Castelnuovo G, Compare A, Pagnini F, Essebag V and ProiettiR (2015) Psychological effects of implantable cardioverter defibrillator shocks. A reviewof study methods. Front. Psychol. 6:39. doi: 10.3389/fpsyg.2015.00039This article was submitted to Psychology for Clinical Settings, a section of the journalFrontiers in Psychology.Copyright © 2015 Manzoni, Castelnuovo, Compare, Pagnini, Essebag and Proietti.This is an open-access article distributed under the terms of the Creative CommonsAttribution License (CC BY). The use, distribution or reproduction in other forums ispermitted, provided the original author(s) or licensor are credited and that the originalpublication in this journal is cited, in accordance with accepted academic practice. Nouse, distribution or reproduction is permitted which does not comply with these terms.
www.frontiersin.org February 2015 | Volume 6 | Article 39 | 27
Related Documents











