767 Myopotential Sensing by a Dual Chamber Implantable Cardioverter Defibrillator: Two Case Reports PRAMOD DESHMUKH, M.D., and KATHY ANDERSON, B.S.N. From the Cardiology Division, Robert Packer Hospital, Sayre, Pennsylvania Myopotential Oversensing by a Dual Chamber ICD. Introduction: Inappropriate discharges and/or improper inhibition of bradycardia pacing due to oversensing of extraneous signals in implantable cardioverter deflbrillators (ICDs) have been described. With one excep- tion, no previous report involving an intact lead system bas cited myopotential oversensing as tbe cause. Methods and Results: Two case reports of myopotential oversensing by a dual cbamber ICD system are reported. In the first patient suffering from chronic pulmonary obstructive disease, intermittent myopotential seasing during labored respiration resulted in episodic inbibition of bradycardia pacing. In the second patient, oversensing of sustained myopotentials generated during strenuous isometric activity resulted in an inappropriate ICD discbarge. For botb, the ICD system consisted of a CPI model 1810 Ventak AV used in conjunction with a model 0125 Rndotak lead, incorporating integrated bipolar sensing. Conclusion: Althougb modern ICDs bave proven to be bigbly effective in detecting and ter- minating malignant tachyarrhytbmias, tbe opportunity for improving their detection speci- ficity remains. (J Cardiovasc Electrophysiol. Vol. 9, pp. 767-772, July J99H) implantable cardioverter deftbrillator, oversensing, myopotentials Introduction The safety atid effectiveness of implantable car- dioverter deribrillators (ICDs) for the detection and protnpt treatment of rtialignant ventricular tachy- arrhythtiiia.s is well established,'^ particularly when compared with antiarrhyLhmic drug therapy.^ De- spite advances in technology, newer generation ICDs have been shown to be susceptible to de- tection of endogenous far-field biopotentials. De- pending on the continuous or sporadic nature and/or frequency of the interfering signals, adverse con- sequences of ICD oversensing have included ei- ther intemiittent inhibition of bradycardia pacing'^ and/or inappropriate delivery of antitachyarrhyth- mia therapy.'^'- Two cases involving ICD interference by my- opotential oversensing are described. In one case, the source of the tnyopotentials was demonstrated Address for correspondence: Pramod Deshmukh. M.D.. F.A.C.C., Robert Packer Hospital, Arrhythmia Center. Gulhrie Square. Sayre, PA 18840. Fax: 7I7-S82-5827. Manuscript received 7 January 1998; Accepted for publication 15 April 1998. to be diaphragtnatic during labored breathing. In the second case, the interfering myopotentials occurred during a sustained isometric contraction involving the muscles of the abdominal compart- ment, including the diaphragm. Case Report 1 A 73-year-old man with a significant cardio- vascular history including ischemie heart disease, a > I-year-old myocardial infarction, left ventricu- lar ejection fraction (EF) of 40%, and symptotn- atic runs of wide cornplex tachycardia ptesented for electrophysiologic study (EPS). Associated di- agnoses included hypertension, severe chronic ob- structive pulmonary disease, and persistent drug- refractory atrial ftbrillation. Provocative electrical stimulation during EPS elicited a sustained monomorphic tachycardia with characteristics sim- ilar to that of his clinical tachycardia with a cycle length of 330 msec (182 beats/min) that was read- ily restored to normal sinus rhythm using a 2(X)- J tran.sthoracic cardioversion. Due to his frequent episodes of poorly toler- ated, rapidly conducted atrial fibrillation despite

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

767
Myopotential Sensing by a Dual Chamber ImplantableCardioverter Defibrillator: Two Case Reports
PRAMOD DESHMUKH, M.D., and KATHY ANDERSON, B.S.N.
From the Cardiology Division, Robert Packer Hospital, Sayre, Pennsylvania
Myopotential Oversensing by a Dual Chamber ICD. Introduction: Inappropriatedischarges and/or improper inhibition of bradycardia pacing due to oversensing of extraneoussignals in implantable cardioverter deflbrillators (ICDs) have been described. With one excep-tion, no previous report involving an intact lead system bas cited myopotential oversensing astbe cause.
Methods and Results: Two case reports of myopotential oversensing by a dual cbamber ICDsystem are reported. In the first patient suffering from chronic pulmonary obstructive disease,intermittent myopotential seasing during labored respiration resulted in episodic inbibition ofbradycardia pacing. In the second patient, oversensing of sustained myopotentials generatedduring strenuous isometric activity resulted in an inappropriate ICD discbarge. For botb, theICD system consisted of a CPI model 1810 Ventak AV used in conjunction with a model 0125Rndotak lead, incorporating integrated bipolar sensing.
Conclusion: Althougb modern ICDs bave proven to be bigbly effective in detecting and ter-minating malignant tachyarrhytbmias, tbe opportunity for improving their detection speci-ficity remains. (J Cardiovasc Electrophysiol. Vol. 9, pp. 767-772, July J99H)
implantable cardioverter deftbrillator, oversensing, myopotentials
Introduction
The safety atid effectiveness of implantable car-dioverter deribrillators (ICDs) for the detection andprotnpt treatment of rtialignant ventricular tachy-arrhythtiiia.s is well established,'^ particularly whencompared with antiarrhyLhmic drug therapy.̂ De-spite advances in technology, newer generationICDs have been shown to be susceptible to de-tection of endogenous far-field biopotentials. De-pending on the continuous or sporadic nature and/orfrequency of the interfering signals, adverse con-sequences of ICD oversensing have included ei-ther intemiittent inhibition of bradycardia pacing'̂and/or inappropriate delivery of antitachyarrhyth-mia therapy.'^'-
Two cases involving ICD interference by my-opotential oversensing are described. In one case,the source of the tnyopotentials was demonstrated
Address for correspondence: Pramod Deshmukh. M.D.. F.A.C.C.,Robert Packer Hospital, Arrhythmia Center. Gulhrie Square.Sayre, PA 18840. Fax: 7I7-S82-5827.
Manuscript received 7 January 1998; Accepted for publication 15April 1998.
to be diaphragtnatic during labored breathing. Inthe second case, the interfering myopotentialsoccurred during a sustained isometric contractioninvolving the muscles of the abdominal compart-ment, including the diaphragm.
Case Report 1
A 73-year-old man with a significant cardio-vascular history including ischemie heart disease,a > I-year-old myocardial infarction, left ventricu-lar ejection fraction (EF) of 40%, and symptotn-atic runs of wide cornplex tachycardia ptesentedfor electrophysiologic study (EPS). Associated di-agnoses included hypertension, severe chronic ob-structive pulmonary disease, and persistent drug-refractory atrial ftbrillation. Provocative electricalstimulation during EPS elicited a sustainedmonomorphic tachycardia with characteristics sim-ilar to that of his clinical tachycardia with a cyclelength of 330 msec (182 beats/min) that was read-ily restored to normal sinus rhythm using a 2(X)-J tran.sthoracic cardioversion.
Due to his frequent episodes of poorly toler-ated, rapidly conducted atrial fibrillation despite
Journal of Cardiovascular Electrophysiology Vol. 9. No- 7. July 1998
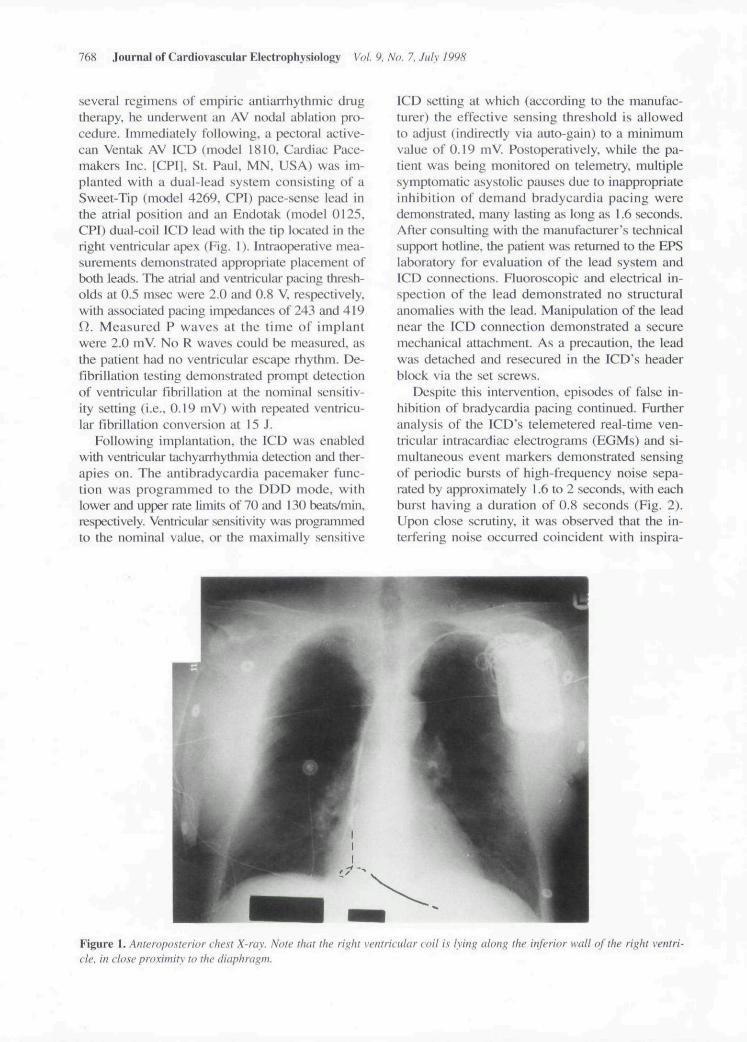
several regimens of empiric antiarrhythmic drugtherapy, he undeiAvcnt an AV nodal ablation pro-cedure. Immediately following, a pectoral active-can Ventak AV ICD (model 1810. Cardiac Pace-makers Inc. [CPIJ. St. Paul. MN. USA) was im-planted with a dual-lead system consisting of aSweet-Tip (model 4269, CPI) pace-sense lead inthe atrial position and an Endotak (model 0125,CPI) dual-coil ICD lead with the tip located in theright ventricular apex (Fig. 1). Intraoperative mea-surements demonstrated appropriate placement ofboth leads. The atrial and ventricular pacing thresh-olds at 0.5 msec were 2.0 and 0.8 V. respectively,with associated pacing impedances of 243 and 419i}. Measured P waves at the time of implantwere 2.0 mV. No R waves could be measured, asthe patient had no ventricular escape rhythm. De-fibrillation testing demonstrated prompt detectionof ventricular fibrillation at the nominal sensitiv-ity setting (i.e.. 0.19 mV) with repeated ventricu-lar fibrillation conversion at 15 J.
Following implantation, the ICD was enabledwith ventricular tachyarrhythmia detection and ther-apies on. The antibradycardia pacemaker func-tion was programmed to the DDD mode, withlower and upper rate limits of 70 iind 130 beats/min.respectively. Ventricular sensitivity was programmedto the nominal value, or the maximally sensitive
ICD setting at which (according to the manufac-turer) the effective sensing threshold is allowedto adjust (indirectly via auto-gain) to a minimumvalue of 0.19 mV. Postoperatively. while the pa-tient was being monitored on telemetry, multiplesymptomatic asystolic pauses due to inappropriateinhibition of demand bradycardia pacing weredemonstrated, many lasting as long as 1.6 seconds.After consulting with ihe manufacturer's technicalsupport hotline, the patient was returned to the EPSlaboratory for evaluation of the lead system andICD connections. Eluoroscopic and electrical in-spection of the lead demonstrated no structuralanomalies with the lead. Manipulation of the leadnear the ICD connection demonstrated a securemechanical attachment. As a precaution, the leadwas detached and resecured in the ICD's headerblock via the set screws.
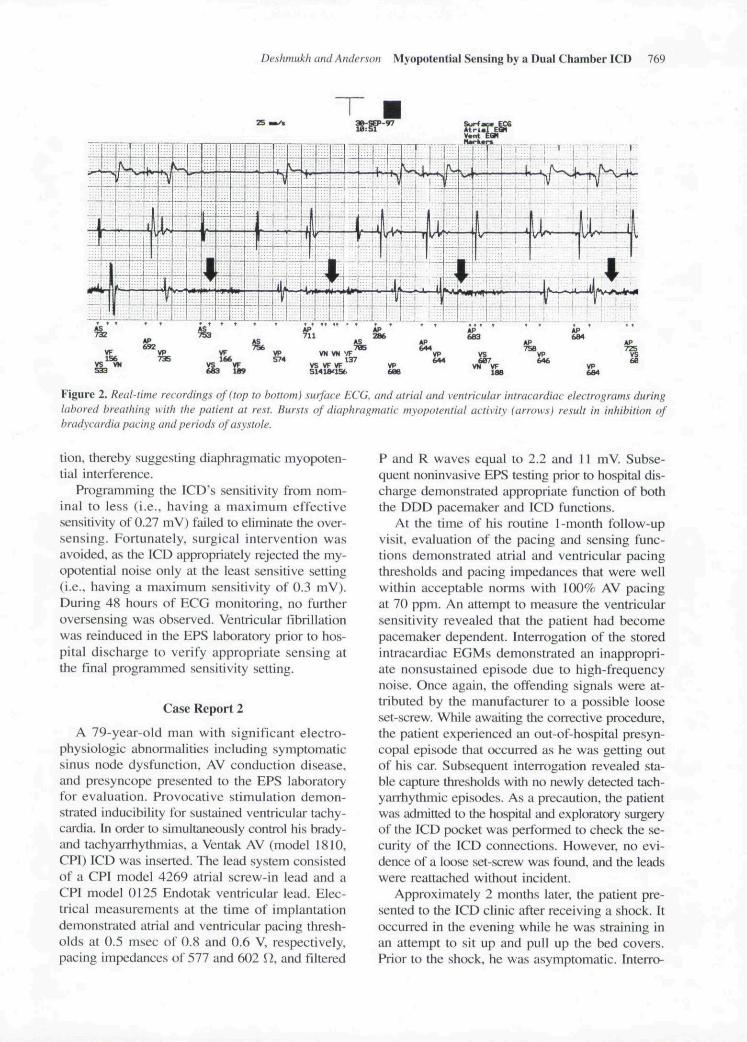
Despite this intervention, episodes of false in-hibition of bradycardia pacing continued. Furtheranalysis of the ICD's telemetered real-time ven-tricular intracardiac electrograms (EGMs) and si-multaneous event markers demonstrated sensingof periodic bursts of high-frequency noise sepa-rated by approximately 1.6 to 2 seconds, with eachburst having a duration of 0.8 seconds (Fig. 2).Upon close scrutiny, it was ob.served that the in-terfering noise occurred coincident with inspira-
Figure 1. Anteroposterior chest X-ray. Note that the right ventricular coil is tying along the inferior watt of the right ventri-cle, in close proximity to the diaphragm.
Deshmukh and Anderson Myopotential Sensing by a Dual Chamber ICD 769
Figure 2. Real-time recordings of (top to bottom) surface ECG, and atrial and ventricular intracardiac electrograms duringlabored breathing with the patient at rest. Bursts of diaphragmatic myopotential activity (arrows) result in inhibition ofbradycardia pacing and periods t>f asystole.
tion. thereby suggesting diaphragmatic myopoten-tial interference.
Programming the ICD's sensitivity from nom-inal to less (i.e., having a maximum effectivesensitivity of 0.27 mV) failed to eliminate the over-sensing. Fortunately, surgical intervention wasavoided, as the ICD appropriately rejected the my-opotential noise only at the least sensitive setting(i.e., having a maximum sensitivity of 0.3 mV).During 48 hours of ECG monitoring, no furtheroversensing was observed. Ventricular fibrillationwas reinduced in the EPS laboratory prior to hos-pital discharge to verify appropriate sensing atthe final programmed sensitivity setting.
Case Report 2
A 79-year-old man with significant electro-physiologic abnomialities including symptomaticsinus node dysfunction. AV conduction disease,and presyncope presented to the EPS laboratoryfor evaluation. Provocative stimulation demon-strated inducibility for sustained ventricular tachy-caidia. In order to simultaneously control his brady-and tachyarrhythmias, a Ventak AV (model 1810,CPI) ICD was inserted. The lead system consistedof a CPI model 4269 atrial screw-in lead and aCPI model 0125 Endotak ventricular lead. Elec-trical measurements at the time of implantationdemonstrated atrial and ventricular pacing thresh-olds at 0.5 msec of 0.8 and 0.6 V, respectively,pacing impedances of 577 and 602 H. and filtered
P and R waves equal to 2.2 and 11 mV. Subse-quent noninvasive EPS testing prior to hospital dis-charge demonstrated appropriate function of boththe DDD pacemaker and ICD functions.
At the time of his routine 1-month follow-upvisit, evaluation of the pacing and sensing func-tions demonstrated atrial and ventricular pacingthresholds and pacing impedances that were wellwithin acceptable norms with 100% AV pacingat 70 ppm. An attempt to measure the ventricularsensitivity revealed that the patient had becomepacemaker dependent. Interrogation of the storedintracardiac EGMs demonstrated an inappropri-ate nonsustained episode due to high-frequencynoise. Once again, the offending signals were at-tributed by the manufacturer to a possible looseset-screw. While awaiting the corrective procedure,the patient experienced an out-of-hospital presyn-copal episode Ihat occurred as he was getting outof his car. Subsequent interrogation revealed sta-ble capture thresholds with no newly detected tach-yarrhythmic episodes. As a precaution, the patientwas admitted to the hospital and exploratory surgeryof the ICD pocket was pertbrmed to check the se-curity of the ICD connections. However, no evi-dence of a loose set-screw was found, and the leadswere reattached without incident.
Approximately 2 months later, the patient pre-sented to the ICD clinic after receiving a shock. Itoccurred in the evening while he was straining inan attempt to sit up and pull up the bed covers.Prior to the shock, he was asymptomatic. Interro-
770 Journal of Cardiovascular Electrophysiology Vol. 9. No. 7, July 1998
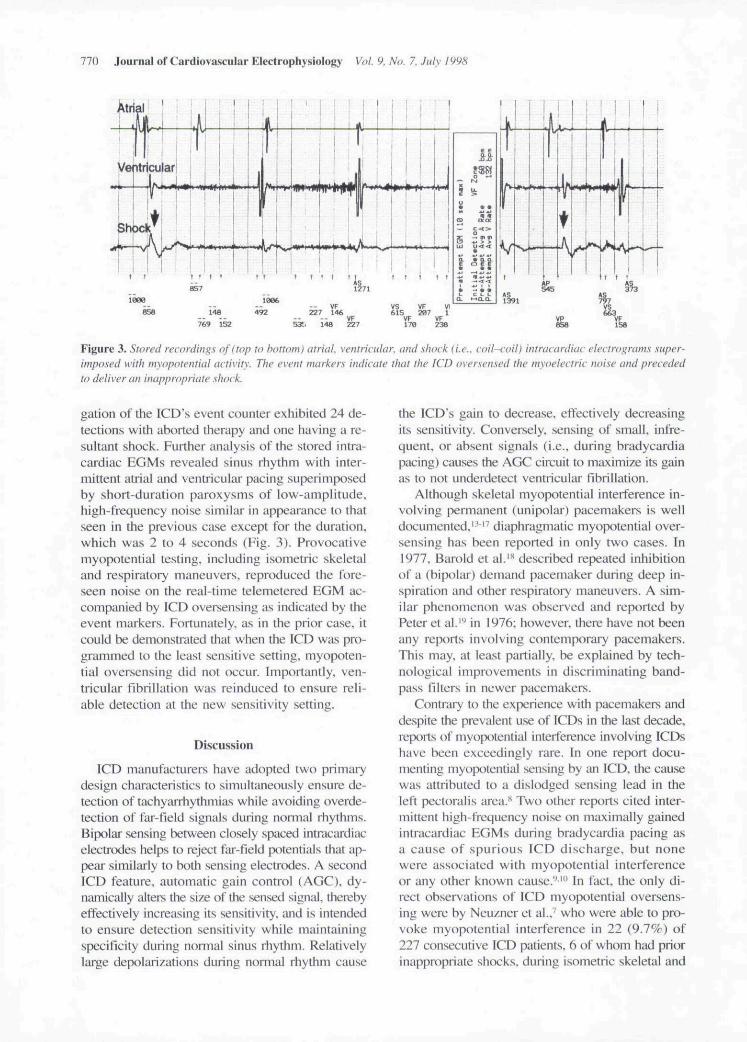
Figure 3. Stored recordings of I top to bottom) atriai. ventricular, and .shock {i.e.. coil-coil) intracardiac electrograms super-imposed with myopotential activity- The event markers indicate that the ICD oversensed the myoelectric noise and precededto deliver an inappropriate shock.
gation of the ICD's event counter exhibited 24 de-tections with aborted therapy and one having a re-sultant shock. Further analysis of the stored intra-cardiac EGMs revealed sinus rhythm with inter-mittent atrial and ventricular pacing superimposedby short-duration paroxysms of low-amplitude,high-frequency noise similar in appearance to thatseen in the previous case except for the duration,which was 2 to 4 seconds (Fig. 3). Provocativemyopotential testing, including isometric skeletaland respiratory maneuvers, reproduced the fore-seen noise on the real-time telemetered EGM ac-companied by ICD oversensing as indicated by theevent markers. Fortunately, as in the prior case, itcould be demonstrated that when the ICD was pro-grammed to the least sensitive setting, myopoten-tial oversensing did not occur. Impottantly, ven-tricular fibrillation was reinduced to ensure reli-able detection at the new sensitivity setting.
Discussion
ICD manufacturers have adopted two primarydesign characteristics to simultaneously ensure de-tection of tachyiurhythmias while avoiding overde-tection of far-field signais during normal ihythms.Bipolar sensing between closely spaced intracardiacelectrodes helps to reject far-field ptncntials that ap-pear similiirly to both .sensing electrodes. A secondICD feature, automatic gain control (AGC). dy-namically alters the size of the sensed signal, therebyeffectively increasing its sensitivity, and is intendedto ensure detection sensitivity while maintainingspecificity during nonnal sinus rhythm. Relativelylarge depolarizations during normal rhythm cause
the ICD's gain to decrease, clfectively decreiLsingits sensitivity. Conversely, sensing of small, infre-quent, or absent signals (i.e., during bradycardiapacing) causes the AGC circuit lo maximize its gainas to not underdetect ventricular fibrillation.
Although skeletal myopotential interference in-volving petmanent (unipolar) pacemakers is welldocumented." " diaphragmatic myopotential over-sensing has been reported in only two cases. In1977, Barold et al.'** described repeated inhibitionof a (bipolar) demand pacemaker during deep in-spiration and other respiratory niiuieuvers. A sim-ilar phenomenon was observed and reported byPeter et al.''' in 1976; however, there have not beenany reports involving contemporary pacemakers.This may, at least partially, be explained by tech-nological impiovements in discriminating band-pass filters in newer pacemakers.
Contrary to the experience with pacemakers anddespite the prevalent use of ICDs in the last decade,reports of myopotential interference involving ICDshave been exceedingly rare. In one report docu-menting myopt:)tential sensing by an ICD. the causewas attributed to a dislodged sensing lead in theleft pectoraiis area.** Two other reports cited inter-mittent high-frequency noise on maximally gainedintracardiac EGMs during bradyciirdia pacing asa cause of spurious ICD discharge, but nonewere associated with myopotential interferenceor any other known cause.'^'" In fact, the only di-rect observations of ICD myopotential oversens-ing were by Neuzner et al.,^ who were able to pro-voke myopotential interference in 22 (9.7%) of227 consecutive ICD patients, 6 of whom had priorinappropriate shocks, during isometric skeletal and

Deshmukh and Anderson Mj'oputential Sensing by a Dual Chamber ICD 771
respiratory maneuvers. Importantly, all patients hadtransvenous ICD systems incorporating integratedbipolar sensing, an adaptation of trtie bipolar sens-ing wbereby the large surface, right ventricularshocking coil is shated as the anode for sensing(and pacing).
These case studies illustrate a lingering sus-ceptibility of ICDs incorporating integrated bipo-lar sensing and highly sensitive AGC detection al-gorithms shared for both the antitachyarrhythmiaand anti bradycardia rhythm control features. Incase 1, long periods of maximally gained intra-cardiac signals during continuous AV bradycar-dia pacing resulted in intermittent inhibition bymyopotentials elicited Irom a hypertrophied di-aphragm overworked by obstructive pulmonarydisease. Unfortunately, a prompt diagnosis was notmade (despite consultation with the manufacturer),and the patient underwent an unnecessarysurgery in an attempt to rectify the ptoblem. Incase 2, maximum gain during constant bradycai-dia pacing again contributed to the oversensing.Although this also was misinterpreted as a kx>seset-screw problem, tbe correct diagnosis was even-tually made on tbe basis of what was learned intbe interim from the first case. Tbe similar ap-pearance of the high-frequency interfering signalson the stored EGM prompted the investigation ofmyopotentiai sensing as the possible cause.
Althougb the advent of dual chamber ICDsystems is considered a significant technologicaladvance, the availability of real-time and stored in-tracardiac EGMs as a standard feature in newerICDs may further reveal extraneous biopotentialoversensing as a clinical issue. Moreover, this phe-nomenon may become more evident as more oftbese integrated pacemaker-ICD systems are im-planted in pacemaker-dependent patients, many ofwbom previously would have received a separatedual pacemaker system (having a Hxed ventricu-lar sensitivity on the order of 2.5 mV). Importantly,tbese observations me made at a time wben a greatdeal of effort is being put forth by ICD manufac-turers to develop smaller-diatneter single- and dual-coil ICD leads. In fact, at tbe time of this writing,every ICD tnanufacturer provides a lead havingintegrated bipolar sensing.
Conclusion
Based on these findings, we advocate an in-creased awareness of the possibility of myopo-tential sensing in ICD patients exhibiting inap-propriate inhibition of bradycardia pacing and/or
false ICD shocks accompanied by high-frequencynoise on the stored EGM. Suggested maneuversfor testing for myopotential oversensing includ-ing provocative .skeletal isometric exercises in-volving the upper extremities and abdominal mus-cles as well as active diaphragmatic maneuversincluding deep inspiration, expiration. Valsalva,and coughing to ensure that inhibition cannotoccut. In those who do exhibit oversensing. a pos-sible solution may be to safely decrease the pace-maker/ICD's ventricular sensitivity only afterdemonstrating that ventricular fibrillation detec-tion is unimpaired. As a last resoit. insertion of aseparate dedicated bipolar sensing lead (or ICDlead replacement by one incorporating true bipo-lar sensing lead) is warranted.
References
1. Winkle RA. Mead RH. Ruder MA. et al: Long termoutcome with the automatic implantyble carcliDverterdellbrillator. J Am Coll Cardio! 1989:13:1353-1361.
2. Bardy GH. Trotitman C. Poole JH, et al: Clinical ex-perience wilh ii tiered-lherapy multiprogrammableantitachycardia device. Circulation I992:S6:1689-1698.
3. Saksena S. Pocqobutt-Johanos M. Castle L. et al:Long-terin multicenter experience with a second gener-ation implantable pacemaker cardioverier-defibrillator.J Am Coll Cardiol 1991:19:490-499.
4. The Antiarrhythmic versus Implantable Defibrillators(AVID) Invesiigators: A comparison of antiarrhythtnicdrug therapy with implantable deribrillators in patientsresuscitated from near fatal ventricular arrhythmias. NEngl J Med 1997;337:1576-1583.
5. Curwin JH. Roeike M. Ruskin JN: Inhibition oC brady-cardia pacing caused by far-field sensing in a third-generation cardioverter defibrillator with an automaticgain feature. PACE 1996; 19:124-126.
6. Sticherling C. Klingenheben T. Hohnloser SH: An un-usual cause of ICD shock. PACE 1997:20:2263-2267.
7. Neu/ner J. Durch M, Sper/,el J. et ai: Myopotentialsensing: Cause of inappropriate arrhythmia detectiotiand device discharges in implantable deiibrillaior ther-apy. (Abstracl) PACE l997:2()(Pt ll):i22.S.
8. Sandier MJ. Kutaiek SP: Inappropriate discharge by animplantable cardioverter defibrillator: Recognition ofmyopotential .sensing using telemetered intracardiacelectrograms. PACE 1994; 17:665-671.
9. Kelly PA. Mann DE. Damie RS. et a!: Oversensingduring ventricular pacing in patients with a third-gen-eration impiantable cardioverter-defibrillator. J AmCollCai-diol 1994:23:1531-1534.
10. Nuitian SO. Roeike M. Troutan T, ei al: Limitationsand late compiicaiions of third-generation automaticcardioverter-defibrillators. Circulation 1995:91:
•2204-2213.
772 Journal of Cardiovasfular Kletirophysiology Vol. 9. No. 7, July 1998
11. Schecter SO. Greenbcrg SM, Hoch DH: IniippropriatL'discharges of nn implanuibk cardioverter defibrillatorsecondary to automatic adjustable gain of atrial tachy-cardia. PACE 1997;20:172 1-1722.
12. Peters W. Kowallik P. Wittenberg G: Inappropriate dis-charge of an implantable cardioverter defibrillator dur-ing atrial flutter and intermittent antibradycardia pac-ing. J Cardiovasc Electrophysiol \991:H: 1167-1174.
13. Fetter J. Bobeldyk GL. Engman FJ: The clinical inci-dence and significance of myopotential sensing withunipolar pacemakers. PACE 1984;7:871-881.
14. Secemsky SI. Hauser RG. Denes P. et al: Unipolarsensing abnormalities: Incidence and clinical signifi-cance of skeletal muscle interference and undersensingin 228 patients. PACE I982;5:I(M9.
15. Ito H. Eesaka Y, Taniquchi K. et al: Comparison ofsusceptibility of myopotential inhibition between AAIand VVI pacemakers. Jpn Heart J 1987;28:I57-164,
16. Gialofos J. Miallis A. Kandilas J: Pacemaker inhibitionby myopotentials associated with wall motion and ex-ercise. Eur Head J 1987:80:149-154.
17. Gross JN. Platt S. Ritacco R. et al: The clinical rele-vance of electromyopotential oversensing in currentunipolar devices. PACE 1992:15:2023-2027.
18. Barotd SS. Ong LS. Falkoff MD. et al: Inhibition ofbipolar demand pacemaker by diaphragmatic myopo-tentials. Circulation 1977:56:679-683.
19. Peter T, Harper R, Sloman G: Inhibition of demandpacemakers caused by potentials associated with inspi-ration. Br Heart J 1976:38:21 1-212.
South end of elephant, Ngonmgoro Crater

Related Documents











